27 FIBER-REINFORCED COMPOSITE FIXED PROSTHESES
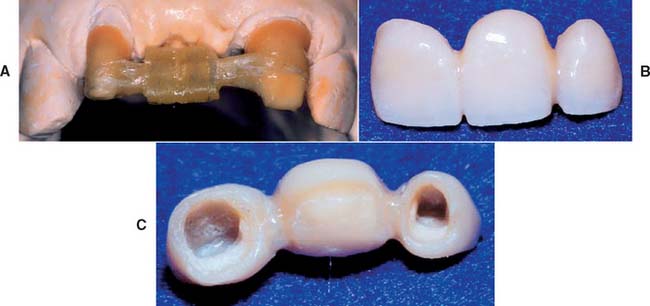
Fiber-reinforced fixed prostheses are an innovative alternative to traditional metal-ceramic restorations. They should be considered for certain patients because they provide a conservative approach to replacing missing teeth and overcome some of the drawbacks of conventional prostheses. The restoration consists of a fiber-reinforced composite (FRC) substructure veneered with a particulate composite material. The substructure provides strength, and the veneer, because it is laboratory processed, exhibits better physical properties and esthetics than do direct placement composite restoratives (Fig. 27-1). The following topics are included in this chapter:

Fig. 27-1 A, Fiber-reinforced composite (FRC) substructure. B, Completed polymer fixed prostheses consisting of the substructure and particulate composite veneer material. C, Tissue side view of the completed polymer fixed prostheses. D, Cemented FRC prostheses cemented in mouth.
ADVANTAGES AND DISADVANTAGES
As discussed in Chapter 24, the most common fixed prostheses are composed of a metal substructure veneered with a ceramic material. The substructure provides mechanical integrity, whereas the ceramic imparts the necessary esthetics. The metal-ceramic prosthesis has an excellent clinical service record but continues to exhibit several drawbacks. Although the metal substructure is strong and durable, there are biologic concerns, especially when base metal alloys (commonly used in clinical practice) are selected. They may undergo corrosion1-3 and/or may elicit an allergic reaction from some patients.4-8 Certain constituents of some base metal alloys may cause acute and chronic health hazards for laboratory personnel.9,10 In addition, the metal framework is opaque with a dark oxide layer, which is not esthetically pleasing. This must be covered with a porcelain veneer to produce a lifelike appearance.
Porcelain is a brittle material and can fracture, which is a leading cause of restoration failure.11-14 When this occurs, porcelain can sometimes be repaired with acrylic or composite resin15-18 bonded with silane coupling agents or 4-methacryloxyethyl-trimellitic anhydride (4-META) to promote adhesion (see Chapter 32). Porcelain is also abrasive to opposing enamel and can severely damage unrestored opposing teeth.19-23 Porcelain has been implicated in severe occlusal wear, particularly when it is not glazed or highly polished (see Chapter 19). In one survey, less wear on opposing teeth was cited as the single major need for change in posterior tooth-colored crowns.24
Because of these problems and concerns, alternatives to metal-ceramic materials continue to be explored. All-ceramic and all-particulate composite prostheses have been described in the dental literature.25,26 Recorded problems include low resilience and toughness, which result in clinical failure.
As with the porcelain surfaces of metal-ceramic prostheses, the surfaces of the all-ceramic prostheses are abrasive to tooth enamel and can potentially damage unrestored opposing teeth. Conversely, the composite materials have historically exhibited less than adequate occlusal wear resistance and color stability over time, but newer composites continue to improve with regard to these characteristics. Light-, heat-, and vacuum-polymerized laboratory-processed particulate composite materials are now commercially available and are made of new polymer formulations with improved filler particle distribution.27 These improved materials demonstrate better physical properties, such as hardness and wear resistance. However, particulate composites are brittle and need the support of a substructure with good flexure properties.
FRCs have good flexure strength and other physical characteristics that make them suitable fixed prosthesis substructure materials.28-30 In addition, the FRC substructure is translucent and requires no opaque masking. This allows a relatively thin layer of particulate covering composite and excellent esthetics. FRCs have been used to make two-phase all-polymer prostheses composed of an internal glass fiber–reinforced composite substructure covered by a particulate composite (Fig. 27-2).
AVAILABLE MATERIALS
FRC materials are categorized according to the following characteristics:
The most commonly used fibers in dental applications are glass, polyethylene, and carbon. Fiber architectures in dentistry include “unidirectional” patterns, in which all fibers are parallel, and braided and woven patterns. Commercially available non–resin-impregnated materials include polyethylene weaves (e.g., Ribbond* and Construct†) and glass weaves (e.g., GlasSpan‡). These products need to have the resin added to the fibers by hand. Resin-preimpregnated materials include everStick and StickNET,§ which are hand formed and available in both unidirectional and woven-glass forms; FibreKor,‖ which is hand formed and available as a unidirectional glass material; and Splint-It,¶ which is also hand formed and available in both unidirectional and woven glass forms (Fig. 27-3).
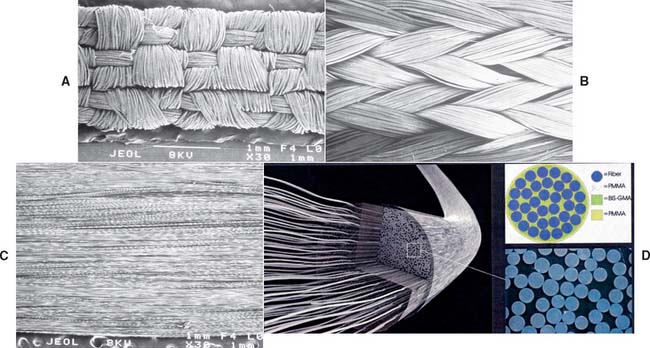
Fig. 27-3 Scanning electron micrographs. A, Woven polyethylene fiber-reinforced composite (FRC) (Construct, Kerr Corporation). B, Braided polyethylene FRC (Ribbond, Ribbond, Inc.). C, Unidirectional long glass fiber FRC (FibreKor, Pentron Clinical Technologies, LLC). D, Unidirectional long glass fibers with a polymethylmethacrylate (PMMA) outer membrane (everStick, StickTech).
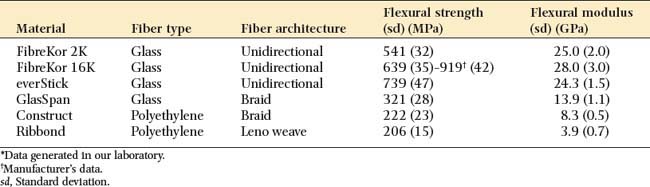
Different FRC materials exhibit different handling and mechanical properties. Fiber type, fiber orientation, and the quality of fiber impregnation with the resin matrix have a substantial effect on handling characteristics and physical properties. As seen in Table 27-1, glass materials with a unidirectional architecture exhibit flexural properties that are superior to the polyethylene materials with a woven or braided architecture. These glass materials have a flexural strength that is more than twice the strength of polyethylene materials and a flexural modulus almost eight times as great.16 Because of their good handling characteristics, the braided and woven polyethylene products may be useful for other dental applications (e.g., operatory fabrication of periodontal splints).
INDICATIONS
Indications for selecting a fiber-reinforced polymer prosthesis include the following:
These materials can be used anywhere in the mouth where esthetics is important. The lack of metal or opaque materials provides good translucency and a very natural appearance. This natural appearance at the cervical aspect of the prosthesis retainer eliminates the need to hide margins subgingivally, where they may create periodontal problems for the patient. Supragingival margins of this polymer prosthesis blend in easily with the nonprepared tooth structure apical to the tooth preparation finish line, just as the overall prosthesis blends in with the adjacent natural teeth. Resin composite luting materials that bond to the internal aspect of the polymer prosthesis retainers and to the dentin and enamel of the abutment teeth improve retention of the prosthesis. This feature may provide crucial retention of a polymer prosthesis on abutment teeth that cannot be made to exhibit optimum geometric retention form; however, the bonding process requires careful control of moisture and soft tissues.
An early prosthodontic application of an experimental thermoplastic unidirectional FRC31-33 was the fabrication of a single tooth replacement bonded fixed dental prosthesis (FDP).34 These prostheses were formed in the laboratory and then bonded to the teeth (Fig. 27-4).

CONTRAINDICATIONS
Contraindications to selecting an FRC fixed prosthesis include the following:
Patient selection criteria are summarized in Box 27-1. Composite resin luting materials and an adhesive cementation technique can be used only in situations in which the operator can maintain a contamination-free field. Rubber dam isolation is ideal and should be used whenever possible. At this time, FDPs that replace more than two teeth are not recommended because the material’s ability to support longer edentulous spans has not been documented. An increased susceptibility to wear or fracture may occur in patients who brux or clench, and surface degradation of the particulate composite is likely to be a problem in alcoholic patients. Because there are no clinical data to substantiate how the FRC fixed prosthesis would perform when subjected to these conditions, it should not be considered until more information is available.
A number of clinical studies have evaluated FRC full- or partial-coverage fixed prostheses, ranging from 1 to 4 years.35-41 These have yielded variable results on the basis of the material and fabrication method. Survival rates ranged from 58.8% to 95%, depending on the criteria used and the type of FRC/particulate resin composite system employed. The FRC frameworks performed well with few fractures. Most of the problems involved the wear, discoloration, degradation, and fracture of the particulate resin composite veneer materials. These veneering resin composite problems were associated with the two types of commercially available FRC systems for laboratory-generated partial fixed dental prostheses—Targis/Vectris (Ivoclar/Vivadent, Inc.) and Sculpture/FibreKor (Pentron, Inc.)—but at a much higher reported rate for the Targis/Vectris system. Ivoclar/Vivadent removed their system from the market because of the frequency of these problems. These data also indicated that the adequacy of tooth preparation (Fig. 27-5) and volume of the FRC framework, particularly in the pontic support area, play crucial roles in the performance of an FRC fixed prosthesis.
EXTRACORONAL COMPLETE-COVERAGE FIXED PROSTHESES
Newer, lighter, heat/vacuum laboratory-polymerized FRC formulations have been developed and tested. They demonstrate excellent esthetics, good handling characteristics, and good flexure properties.29,42-45 Commercial products have been based on these formulations. The fabrication of a complete-coverage prosthesis with a commercially available, preimpregnated unidirectional FRC (FibreKor, Pentron Clinical Technologies, LLC) and a hand-fabricated technique are shown in Figure 27-6.
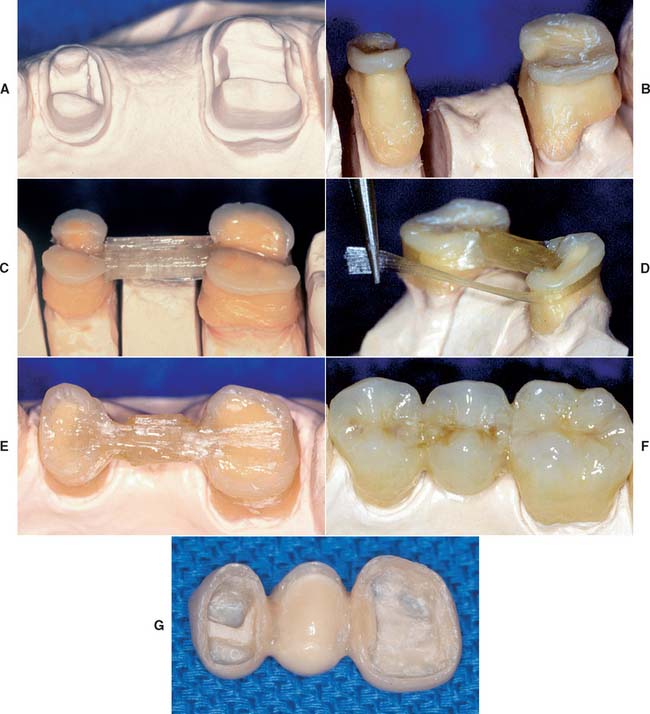
Fig. 27-6 The step-by-step fabrication of a complete-coverage fiber-reinforced composite (FRC) prosthesis with a unidirectional glass material (FibreKor, Pentron Clinical Technologies, LLC), accomplished with a hand-fabricated technique. A, Dies showing posterior abutment preparations for an FRC polymer bridge. B, Thin coping of opacious body particulate composite adapted to the die. C, Bar of multiple layers of FRC spanning the pontic region, bonding the copings together. D, Continuous strip of FRC bonded to one end of the pontic bar and then wrapped around the axial surfaces of the copings while being polymerized. E, Occlusal view of the completed FRC substructure. F, Completed prosthesis with particulate resin veneers on model. G, Tissue side view of completed prosthesis, showing the internal adaptation to preparation design of the abutment teeth.
INTRACORONAL PARTIAL-COVERAGE FIXED PROSTHESES
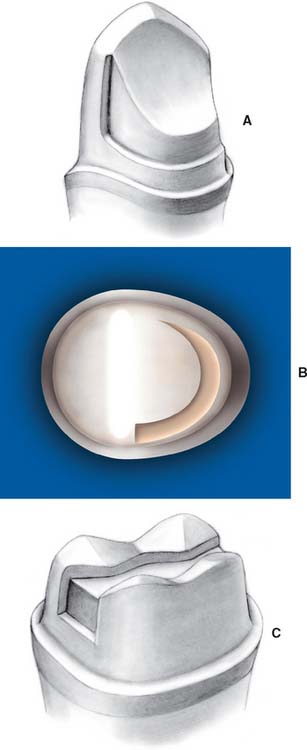
The FRC partial-coverage FDP allows a conservative design when the abutment teeth are unrestored or have modest intracoronal restorations. When an implant is not possible, an etched metal resin-retained FDP (see Chapter 26) is the only other conservative fixed treatment alternative. However, these prostheses have problems with retention, graying of abutment teeth (as a result of metal showing through), and overcontoured retainers. The advantages discussed for the complete-coverage FDP (esthetics, metal-free framework, ease of laboratory fabrication, and use of an adhesive cementation technique) also apply to the partial-coverage FDP. The fabrication of a partial-coverage intracoronal prosthesis with a commercially available, preimpregnated unidirectional FRC (FibreKor, Pentron Clinical Technologies, LLC) and a hand-fabricated technique are shown in Figure 27-7.
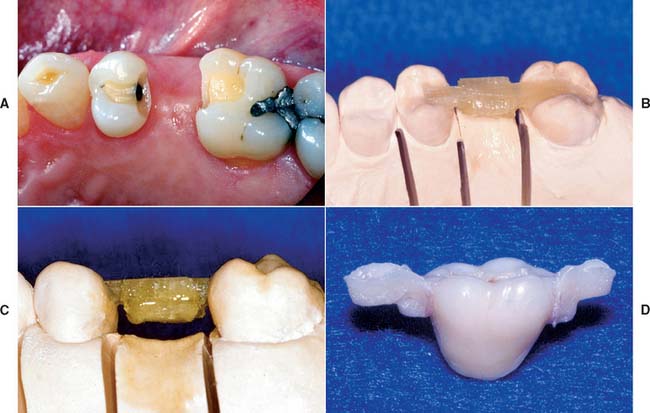
Fig. 27-7 The tooth preparation and step-by-step fabrication of a partial-coverage intracoronal fiber-reinforced composite (FRC) prosthesis with a unidirectional glass material (FibreKor, Pentron Clinical Technologies, LLC) and a hand-fabricated technique. A, Intracoronal tooth preparation. B, Placement of the unidirectional FRC bar into unpolymerized opacious body particulate composite. C, Completed FRC substructure. D, Completed prosthesis as viewed from the buccal surface.
CHAIRSIDE PROSTHESES
One of the most exciting and potentially useful applications for preimpregnated FRC technology is its use in replacing missing teeth in a timely and cost-effective manner. The ability to deliver a functional, esthetic tooth replacement with no to minimal tooth preparation of the adjacent abutment teeth in a single visit is now a realistic treatment option with the current adhesive technologies and reinforced composites. The increase in physical properties that fiber reinforcement provides to particulate composites allows for an improved approach versus earlier methods in which denture teeth have been used as pontics.46,47 This new approach eliminates the disadvantages posed by the incompatibility of the different chemistries between the particulate luting composite and the acrylic resin pontic and also results in a much stronger connector between the pontic and the abutment teeth in comparison with particulate composite alone. This provides the potential for long-term clinical service.42 Potential clinical applications for chairside-fabricated FRC prostheses include situations in which the abutment teeth may be of questionable prognosis or in place of an interim removable prosthesis immediately after anterior implant placement but before loading. The latter situation is seen in Figure 27-8. In addition, this technology can be used for immediate fixed tooth replacement after extraction, after traumatic loss of a tooth, or for space maintenance in pediatric or adolescent patients, in whom it acts as a transitional prosthesis until a more permanent solution can be delivered.
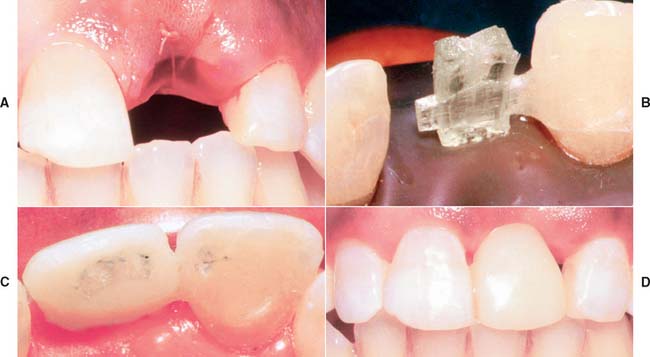
Fig. 27-8 An example of a prefabricated fiber-reinforced composite (FRC) framework used as a fixed interim prosthesis after tooth extraction and before implant placement. A, Appearance after lateral incisor has been extracted. B, A cantilever prefabricated framework placed. The wing is attached to the central incisor. C, Lingual view of completed interim prosthesis, showing the adaptation of the particulate composite veneer. D, Facial view of interim FRC prosthesis.
Methods have been developed whereby preformed substructures can be used to quickly provide a platform for creating a prosthesis at chairside, rather than having to fabricate a chairside prosthesis from scratch by using particulate composite and FRC components.48-50 This helps reduce time and technique sensitivity in the delivery of chairside prostheses. FRC can be easily manipulated into a preformed (prefabricated) substructure that has both polymerized and nonpolymerized elements. The “wing” element is not yet polymerized and provides an attachment to the adjacent abutment teeth as they are adapted, polymerized, and bonded to the facial or lingual surfaces. The “pontic” element is rigid because it is already polymerized and also consists of unidirectional FRC but in greater bulk. After attaching the wings to the abutment teeth, the dentist veneers the pontic element with light polymerized particulate (restorative) composite.
IMPLANT-SUPPORTED FIXED PROSTHESES
The advantages of using FRC materials to fabricate implant-supported fixed prostheses (see Chapter 13) include good flexure properties of the preimpregnated FRCs, time saving as a result of lack of casting and soldering, and the chemical bond of the resin veneer to substructure. Implant-supported FRC prostheses can either be retained by screws or luted to the implant abutment.51 In contrast to tooth-supported prostheses, the component of the FRC prosthesis retainer that provides an attachment to the implant abutment can be premanufactured. This is because the implant abutment is generally not custom made but machined by the manufacturer. For luted prostheses, a woven FRC coping can be used to make the underside or foundation of the retainer. The remainder of the FRC substructure can be bonded directly to these copings. An example of a luted FRC framework and a definitive prosthesis can be seen in Figure 27-9. For screw-retained FRC framework, a cylinder with a screw channel that fits directly to the implant abutment becomes an integral component of the substructure. An example of titanium-ceramic cylinders with horizontal grooves on the facial and lingual surfaces and proximal boxes can be seen in Figure 27-10. These design characteristics of the cylinder enable the FRC to be reliably attached. The horizontal grooves provide macromechanical retention, and the proximal boxes provide vertical support to the FRC (Fig. 27-11). The etched and silanated ceramic coating (titanium-ceramic, Vident) provides an opaque mask of the alloy and micromechanical retention for the FRC.
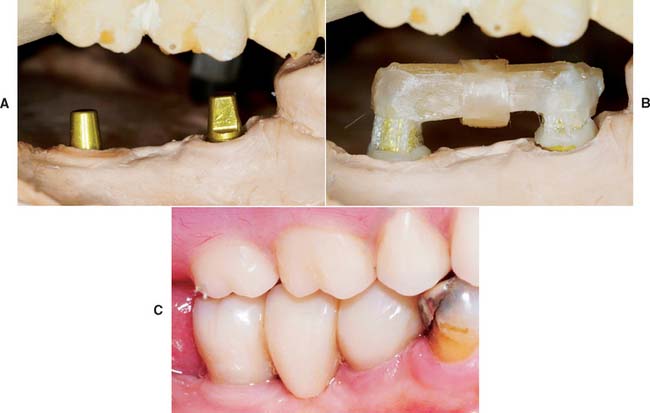
Fig. 27-9 Example of an implant-supported three-unit fiber-reinforced composite (FRC) fixed prosthesis. A, Cast with solid analogs for a cemented three-unit FRC polymer prosthesis. B, Framework completed, buccal view. C, Completed FRC polymer prosthesis.

Fig. 27-10 Examples of titanium-ceramic cylinders used to receive fiber-reinforced composite (FRC) for fixed implant-supported prosthesis. A, Titanium-ceramic cylinders on definitive cast in position to receive FRC bundles. B, Close-up view of a titanium-ceramic cylinder, showing horizontal groove and proximal box, which act as receptors for FRC bundles/wrap.

Fig. 27-11 Completed fiber-reinforced composite (FRC) framework before polymethylmethacrylate (PMMA) denture base and denture tooth addition.
These fixed partial and complete FRC implant prostheses continue to be developed and tested by our research group. The implant prosthesis framework exhibits the “high-volume” design features and external surface air-inhibited layer. An example of a complete arch implant-supported prosthesis framework and definitive prosthesis can be seen in Figure 27-12. For the partial prostheses, a light-/heat-/vacuum-polymerized particulate composite veneer is placed over the FRC substructure. For complete, fixed prostheses, polymethylmethacrylate (PMMA) and denture teeth are used to provide final form and occlusal function. These materials are applied through the use of many widely accepted fabrication techniques commonly employed by the dentist and laboratory technician. These include procedures for the verification of the accuracy of the definitive cast, wax evaluation of the denture teeth, and the processing of the PMMA prosthesis suprastructure.51,52

CEMENTATION
As with porcelain veneers (see Chapter 31), the shade of the complete coverage or inlay prosthesis should be assessed with a water-soluble paste that corresponds to the selected luting composite. Minor adjustments in value can be obtained by selecting darker or lighter luting resins. The translucency of the FRC prosthesis allows the luting composite to play a role in the final shade of the prosthesis. Luting an FRC prosthesis involves the procedures that accompany any bonded restorative procedure: isolation of the abutment teeth, treatment of the inner surface of the FRC retainers, and conditioning of the abutment teeth.
SUMMARY
The natural, esthetic appearance of this metal-free prosthesis and its inherent adhesive nature make the fiber-reinforced prosthesis a successful fixed tooth replacement. Its adhesive qualities may enable the use of abutment teeth that do not exhibit classic geometric retention and resistance form without the need for elective endodontics, surgical crown-lengthening procedures, and the apical placement of finish margins. Furthermore, its favorable strength, esthetics, and adhesive properties make the intracoronal fiber-reinforced prosthesis uniquely qualified for the minimally invasive replacement of a single missing tooth adjacent to unrestored or minimally restored abutment teeth. Multiyear clinical studies are currently in progress to determine the value and efficacy of the FRC prosthesis as a long-term tooth replacement.
 GLOSSARY*
GLOSSARY*
all-polymer prosthesis: a fixed dental prosthesis fabricated from non-metallic or ceramic components typically composed of an internal glass fiber-reinforced composite framework covered by a particulate composite resin
bond strength \b nd str
nd str ngkth, strngth\: the force required to break a bonded assembly with failure occurring in or near the adhesive/adherens interface
ngkth, strngth\: the force required to break a bonded assembly with failure occurring in or near the adhesive/adherens interface
bond·ing \bn′d ng\ n (1976) 1: joining together securely with an adhesive substance such as cement or glue 2: the procedure of using an adhesive, cementing material or fusible ingredient to combine, unite, or strengthen 3: adhesive technique in dentistry involving conditioning of enamel and/or dentin so as to create tags in the tooth structure for mechanical retention of restorative material.
ng\ n (1976) 1: joining together securely with an adhesive substance such as cement or glue 2: the procedure of using an adhesive, cementing material or fusible ingredient to combine, unite, or strengthen 3: adhesive technique in dentistry involving conditioning of enamel and/or dentin so as to create tags in the tooth structure for mechanical retention of restorative material.
bonding agent \bn′dng ā′jent\: a material used to promote adhesion or cohesion between two different substances, or between a material and natural tooth structures
resin-bonded splint \rz′n bn′dd splnt\: a fixed splint made of heavy wire, fibrous resin materials or/and cast metal that is bonded to the labial or lingual surface of natural teeth with an acid etch technique. It is used to stabilize traumatically displaced or periodontally compromised teeth
STUDY QUESTIONS
1 Johansson BI, et al. Corrosion of copper, nickel, and gold dental casting alloys: an in vitro and in vivo study. J Biomed Mater Res. 1989;23(A3 Suppl):349.
2 Hani H. Corrosive changes of dental alloys in oral environment—scanning electron microscopic observation and electron probe microanalysis on crown surfaces [in Japanese]. Kokubyo Gakkai Zasshi. 1993;60:372.
3 Ludwig K. Homogeneity and corrosion resistance of cast dental precious metal alloys compared with uncast alloys [in German]. Dtsch Zahnarztl Z. 1989;44:905.
4 American Dental Association, Council on Dental Materials, Instruments and Equipment. Biological effects of nickel-containing dental alloys. J Am Dent Assoc. 1982;104:501.
5 Association Report. Classification system for cast alloys. J Am Dent Assoc. 1984;109:838.
6 American Dental Association, Council on Dental Materials, Instruments, and Equipment. Report on base metal alloys for crown and bridge applications: benefits and risks. J Am Dent Assoc. 1985;111:479.
7 Covington JS, et al. Quantization of nickel and beryllium leakage from base metal casting alloys. J Prosthet Dent. 1985;54:127.
8 Marcusson JA. Contact allergies to nickel sulfate, gold sodium thiosulfate and palladium chloride in patients claiming side-effects from dental alloy components. Contact Dermatitis. 1996;34:320.
9 Moffa JP, et al. Allergic response to nickel containing dental alloys [Abstract no. 107]. J Dent Res. 1977;56:1378.
10 Morris HF. Veterans Administration Cooperative Studies Project No. 147. IV. Biocompatibility of base metal alloys. J Dent. 1987;58:1.
11 Walton JN, et al. A survey of crown and fixed partial denture failures: length of service and reasons for replacement. J Prosthet Dent. 1986;56:416.
12 Libby G, et al. Longevity of fixed partial dentures. J Prosthet Dent. 1997;78:127.
13 Sundh B, Odman P. A study of fixed prosthodontics performed at a university clinic 18 years after insertion. Int J Prosthodont. 1997;10:513.
14 Priest GF. Failure rates of restorations for single-tooth replacement. Int J Prosthodont. 1996;9:38.
15 Robbins JW. Intraoral repair of the fractured porcelain restoration. Oper Dent. 1998;23:203.
16 Chung KH, Hwang YC. Bonding strengths of porcelain repair systems with various surface treatments. J Prosthet Dent. 1997;78:267.
17 Kupiec KA, et al. Evaluation of porcelain surface treatments and agents for composite-to-porcelain repair. J Prosthet Dent. 1996;76:119.
18 Pameijer CH, et al. Repairing fractured porcelain: how surface preparation affects shear force resistance. J Am Dent Assoc. 1996;127:203.
19 Monasky GE, Taylor DF. Studies on the wear of porcelain, enamel, and gold. J Prosthet Dent. 1971;25:299.
20 Ekfeldt A, Øilo G. Occlusal contact wear of prosthodontic materials. Acta Odontol Scand. 1988;46:159.
21 Kelly JR, et al. Ceramics in dentistry: historical roots and current perspectives. J Prosthet Dent. 1996;75:18.
22 Hacker CH, et al. An in vitro investigation of the wear of enamel on porcelain and gold in saliva. J Prosthet Dent. 1996;75:14.
23 Ramp MH, et al. Evaluation of wear: enamel opposing three ceramic materials and a gold alloy. J Prosthet Dent. 1997;77:523.
24 Christensen GJ. The use of porcelain-fused-to-metal restorations in current dental practice: a survey. J Prosthet Dent. 1986;56:1.
25 Kern M, et al. The all-porcelain resin bonded bridge. Quintessence Int. 1991;22:257.
26 Dickerson WG. The Concept bridge. Dent Econ. 1994;84:67.
27 Yang Z, et al: Non-Diluent Dental Composite. Presented at the Fall National American Chemical Society Meeting, Las Vegas, September 7–11, 1997.
28 Karmaker AC, et al. Fiber reinforced composite materials for dental appliances. In: ANTEC 1996 Plastics: Plastics—Racing into the Future, Volume 3: Special Areas. Indianapolis: Society of Plastic Engineers; 1996:2777-2781.
29 Freilich MA, et al. Flexure strength of fiber-reinforced composites designed for prosthodontic application [Abstract no. 999]. J Dent Res. 1997;76:138.
30 Freilich MA, et al. Flexure strength and handling characteristics of fiber-reinforced composites used in prosthodontics [Abstract no. 1561]. J Dent Res. 1997;76:184.
31 Goldberg AJ, et al. Flexure properties and fiber architecture of commercial fiber reinforced composites [Abstract no. 967]. J Dent Res. 1998;77:226.
32 Goldberg AJ, et al. Screening of matrices and fibers for reinforced thermoplastics intended for dental applications. J Biomed Mater Res. 1994;28:167.
33 Jancar J, DiBenedetto AT. Thermoplastic fiber reinforced composites for dentistry. II. Effect of moisture on flexural properties of unidirectional composites. J Mater Sci. 1993;4:562.
34 Altieri JV, et al. Longitudinal clinical evaluation of fiber-reinforced composite fixed partial dentures: a pilot study. J Prosthet Dent. 1994;71:16.
35 Gohring TN, et al. Two-year clinical and SEM evaluation of glass-fiber-reinforced inlay fixed partial dentures. Am J Dent. 2002;15:35.
36 Vallittu PK, Sevelius C. Resin-bonded, glass fiber–reinforced composite fixed partial dentures: a clinical study. J Prosthet Dent. 2000;84:413.
37 Freilich MA, et al. Clinical evaluation of fiber-reinforced fixed bridges. J Am Dent Assoc. 2002;133:1524.
38 Behr B, et al. Fiber-reinforced composite crowns and FPDs: a clinical report. Int J Prosthodont. 2003;16:239.
39 Monaco C, et al. Clinical evaluation of fiber-reinforced composite inlay FPDs. Int J Prosthodont. 2003;16:319.
40 Bohlsen F, Kern M. Clinical outcome of glass-fiber-reinforced crowns and fixed partial dentures: a three-year retrospective study. Quintessence Int. 2003;34:493.
41 Vallittu PK. Survival rates of resin-bonded, glass fiber–reinforced composite fixed partial dentures with a mean follow-up of 42 months: a pilot study. J Prosthet Dent. 2004;91:241.
42 Goldberg AJ, Burstone CJ. The use of continuous fiber reinforcement in dentistry. Dent Mater. 1992;8:197.
43 Karmaker AC, et al. Extent of conversion and its effect on the mechanical performance of Bis-GMA/PEGDMA-based resins and their composites with continuous glass fibers. J Mater Sci. 1997;8:369.
44 Freilich MA, et al. Preimpregnated, fiber-reinforced prostheses. I. Basic rationale and complete-coverage and intracoronal fixed partial denture designs. Quintessence Int. 1998;29:689.
45 Freilich MA, et al. Development and clinical applications of a light-polymerized fiber-reinforced composite. J Prosthet Dent. 1998;80:311.
46 Ibsen RL, Neville K. Adhesive Restorative Dentistry. Philadelphia: WB Saunders, 1974;139.
47 Littman H, et al. Provisional temporization with acid-etch resin technique. Clin Prev Dent. 1973;2:14.
48 Freilich MA, et al. Fiber-Reinforced Composites in Clinical Dentistry, Chapter 4. Chicago: Quintessence Publishing, 2000.
49 Meiers JC, Freilich MA. Chairside prefabricated fiber-reinforced resin composite fixed partial dentures. Quintessence Int. 2001;32:99.
50 Meiers JC, et al. Direct intra-oral applications of fiber-reinforced composites. The influence of FRC on particulate resin composite to enamel shear bond strengths. In: Vallittu PK, editor. The Second International Symposium on Fibre-Reinforced Plastics in Dentistry, Chapter 4. Turku, Finland: Department of Prosthetic Dentistry and Biomaterials Research, Institute of Dentistry, 2002.
51 Freilich MA, et al. The design and fabrication of fiber-reinforced implant prostheses. J Prosthet Dent. 2002;88:449.
52 Freilich MA, et al. Fiber-Reinforced Composites in Clinical Dentistry, Chapter 7. Chicago: Quintessence Publishing, 2000.