The Nurse-Client Relationship
At the end of the chapter, the reader will be able to:
1 Define key concepts in the nurse-client relationship.
2 Describe the characteristics of therapeutic nurse-client relationships.
3 Discuss therapeutic use of self in nurse-client relationships.
4 Describe the four phases of a nurse-client relationship.
5 Discuss tasks in each of the four phases of the relationship.
6 Compare and contrast adaptations for short-term relationships.
This chapter focuses on the characteristics and structure of nurse-client relationships in clinical practice. Included in the chapter is a comprehensive discussion of the therapeutic relationship as the cornerstone of professional nursing practice (Carter, 2009). Characteristics of the helping relationship related to authenticity, presence, boundaries, and self-awareness are explored as essential components of effective therapeutic relationships. Developmental stages of relationship are identified, and strategies nurses can apply to long- and short-term relationships are addressed.
Basic concepts
The Joint Commission (2001) affirms the role of the nurse in therapeutic relationships with clients and families: “Nearly every person’s every health care experience involves the contribution of a registered nurse. Birth and death, and all the various forms of care in between, are attended by the knowledge, support and comforting of nurses” (p. 5). It is an awesome responsibility, and of particular importance as nursing moves into the community with shorter term, less structured therapeutic relationships between nurse and client/family.
Key concepts in therapeutic relationships
A therapeutic relationship is a professional, interpersonal alliance in which the nurse and client join together for a defined period to achieve health-related treatment goals. The time spent in the relationship may be short, spanning up to an 8-hour shift in a hospital, or it can be longer term, lasting weeks or months in a rehabilitation center. Because each nurse and client has a distinctive personality, the human interactions within each relationship are unique (Chauhan & Long, 2000). Regardless of the time spent, each relationship with a client can be meaningful and important to clients.
The term client can refer to any individual, family, group, or community with an identified health care need requiring nursing intervention. Nurses enter therapeutic relationships with a specialized body of knowledge, a genuine desire to help others, and an openness to the client’s experience. Guiding principles (e.g., presence, purpose, mutuality, authenticity, empathy, active listening, confidentiality, and respect for the dignity of the client) strengthen the healing influence of a therapeutic relationship (McGrath, 2005). Box 5-1 identifies strategies to facilitate empathy.
The nurse-client relationship is an interdependent relationship. Martin Buber’s (1958) I and Thou relation in which each is aware of and respects the other in building a shared reality forms the foundation for therapeutic conversations. He described an I-thou relationship as an equal relationship marked by respect, mutuality, and reciprocity. Neither is an “object” of study. Instead, there is a process of mutual discovery and each person feels free to be authentic. The essence of the I-thou relationship allows each person to be who he or she is as a unique human being worthy of respect even when the person is being difficult.
Buber’s work forms a theoretical foundation for using confirming responses in which the helping person identifies an observable strength of another person and comments on it. He described this way of responding as follows: “Man wishes to be confirmed in his being by man and wishes to have a presence in the being of the other. Secretly and bashfully, he watches for a yes which allows him to be” (Buber, 1957, p. 104).
With the current emphasis on team collaboration in health service care delivery, collaborative relationships with other professionals have become increasingly important. LaSala (2009) notes, “The core values of human dignity, respect, caring, and compassion are not only central to the care of patients but also to nurses’ interactions with one another, members of the interdisciplinary team, and others” (p. 427).
Characteristics of therapeutic relationships
Although therapeutic helping relationships share many characteristics of a social relationship, there are distinct structural and functional distinctions. Table 5-1 presents the differences between a therapeutic helping relationship and a social relationship. The goal of a therapeutic relationship is ultimately promotion of the client’s health and well-being. This is true even when the client is dying or is uncooperative.
TABLE 5-1
Differences Between Helping Relationships and Social Relationships
| Helping Relationships | Social Relationships |
| Helper takes responsibility for the conduct of the relationship and for maintaining appropriate boundaries. | Both parties have equal responsibility for the conduct of the relationship. |
| Relationship has a specific purpose and a health-related goal. | Relationship may or may not have a specific purpose or goals. |
| Relationship terminates when the identified goal is met. | Relationship can last a lifetime or terminate without goal achievement. |
| Focus of the relationship is on needs of the helpee. | The needs of both partners should receive equal attention. |
| Relationship is entered through necessity. | Relationship is entered into spontaneously, accompanied by feelings of liking. |
| Choice of who to be in relationship is not available to either helper or helpee. | Behavior for both participants is spontaneous; people choose companions. |
| Self-disclosure is limited for the helper, encouraged for the helpee. | Self-disclosure for both parties in the relationship is expected. |
| Understanding should always be put into words. | Understanding does not necessarily need to be put into words. |
Client Centered
A therapeutic relationship is client or patient centered. Client-centered approaches, first described by Carl Rogers (1958), are based on the belief that each person has within him or herself the capacity to heal, given support from a helping person who treats the client with the utmost respect and unconditional regard in a caring, authentic relationship (Anderson, 2001). Client-centered care includes the client’s individual preferences, values, beliefs, and needs as a fundamental consideration in all nursing interventions.
In therapeutic relationships, clients are the personal experts on their life experiences; the nurse is the consultive expert on health care matters. The nurse’s expertise derives from integrated empirical, personal, aesthetic, and ethical ways of knowing. This knowledge helps guide the client to reflect on and clarify what is important in the dialogue, and offers professional insights that the client may not have considered previously.

In recent decades, patient- or client-centered care has been acknowledged as a core value in service delivery. Its relevance as an essential component of quality health care measures was strongly stated in the Institute of Medicine (2001) published report “Crossing the Quality Chasm: A New Health System for the 21st Century.” This document charged health care systems to
• Respect patients’ values, preferences and expressed needs
• Coordinate and integrate care across boundaries of the system
• Provide the information, communication, and education that people need and want
• Guarantee physical comfort, emotional support, and the involvement of family and friends (pp. 52–53)
From a functional perspective, client-centered relationships require nurses to step back and compassionately listen to each individual client or family concerns. Keeping in mind that each person’s experience is different, despite similarities in diagnosis, relevant questions are: “What is this person’s human experience of living with this illness or injury” and “How can I as a health care professional help you at this point in time?”
From Mutuality to Partnership
Health care consumers are increasingly expected to be active partners in their own health care (McGrath, 2005; McQueen, 2000). Nurse-client relationships are designed to empower clients and families to assume as much responsibility as possible in self-management of chronic illness. Both nurse and client have responsibilities, and work toward agreed-on goals. Shared knowledge, mutual decision-making power, and respect for the capacities of client to actively contribute to his or her health care to whatever extent is possible are active components of the partnership required of client centered care. Exercise 5-1 looks at shared decision making.
A client-centered partnership honors the client’s right to self-determination and gives the client and family maximum control over health care decisions. The client always has the right to choose personal goals and courses of action, even when they are at odds with the nurse’s ideas. An effective collaborative partnership between nurse and client results in enhanced self-management, better health care utilization, and improved health outcomes (Hook, 2006).
Professional Boundaries
Emotional integrity in the nurse-client relationship is “reliant on maintaining relational boundaries” (LaSala, 2009, p. 424). Professional boundaries represent invisible structures imposed by legal, ethical, and professional standards of nursing that respect nurse and client rights, and protect the functional integrity of the alliance between nurse and client. Bruner and Yonge (2006) suggest that “rather than a line, boundaries represent a continuum with issues related to boundaries ranging from a lack of involvement to overinvolvement” (p. 39). Examples of relationship boundaries involve the setting, time, purpose, and length of contact, maintaining confidentiality, and use of appropriate professional behaviors.
Professional boundaries define how nurses should relate to clients as a helping person, that is, not as a friend, not as a judge, but as a skilled professional companion committed to helping the client achieve mutually defined health care goals (Briant & Freshwater, 1998). Maintaining appropriate professional behavior is a clear interpersonal boundary that makes the relationship safe for the client in much the same way as guardrails protect the public from falling into danger when observing a tourist attraction. Professional boundaries spell out the parameters of the health care relationship (Fronek, Kendall, Ungerer, Malt, Eugarde, & Geraghty, 2009). Nurses are ethically bound to observe the boundaries needed to make a relationship therapeutic (Sheets, 2001). When clients seek health care, they are in a vulnerable position and look to their health care providers as responsive guides to helping them achieve optimum health and well-being.
Boundary Violations and Crossings
The National Council of State Boards of Nursing (NCSBN, 2007) describes professional boundaries as the spaces between the nurse’s position power and client vulnerability. The nurse, not the client, is responsible for maintaining professional boundaries. Boundary violations take advantage of the client’s vulnerability and represent a conflict of interest that usually is harmful to the goals of the therapeutic relationship. Examples of boundary violations include sexual encounters with clients, excessive personal disclosures, personal or business relationships, and requests/acceptance of special favors or expensive gifts. Extensive following of a client after discharge is a common boundary violation. Boundary violations are ethically wrong.
Boundary crossings are less serious infractions. They give the appearance of impropriety but do not actually violate prevailing ethical standards. Hartley (2002) suggests, “With boundary crossings, context is everything. What is appropriate behavior in one context may not be in another” (p. 7). Examples of boundary crossings include meetings outside of the relationship or disclosing personal intimate details about aspects of the nurse’s life that would not be common knowledge (Bruner & Yonge, 2006). Repeated boundary crossings such as continuing a biased, rather than an impartial, relationship with a client should be avoided.
Nurses need to carefully examine their behaviors, look for possible misinterpretations or unintended consequences, and seek supervision when boundary crossings occur. For example, suppose the client perceives your extra involvement as more than a responsive gesture. How will other clients or family members view the extra attention? Is reliance on the extra time or effort spent with a client likely to jeopardize that client’s journey to independence (Hartley, 2002)?
Level of Involvement
An important feature of a therapeutic relationship is the helping person’s level of involvement. The term involvement relates to the degree of the nurse’s attachment and active participation in the client’s care. The level of involvement may fluctuate, depending on the needs of the client, but it should never exceed the boundaries of professional behavior (see Figure 5-1). It becomes problematic when the nurse limits the level of involvement to perfunctory tasks or becomes emotionally overinvolved in the client’s care. To be effective, nurses must maintain emotional objectivity, whilst remaining human and present to clients. Heinrich (1992) notes that nurses constantly walk a thin line between having compassion for a client and developing a relationship that is too close, resulting in a friendship with potential serious complications for the client, as well as the nurse.
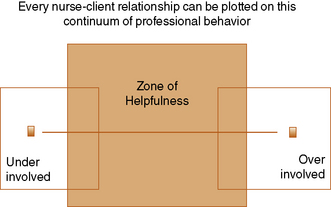
Figure 5-1 Levels of Involvement: A Continuum of professional Behavior. From: National Council of State Boards of Nursing (NCSBN) Professional Boundaries. www.ncsbn.org/Professional_Boundaries_2007_Web.pdf, 2007.
Overinvolvement can be associated with countertransference (O’Kelly, 1998), resulting from the nurse’s unresolved feelings about previous relationships. It often occurs when the client is particularly needy, or feeds the nurse’s ego by considering him or her as special, or the only one who understands.
Overinvolvement results in the nurse’s loss of an essential objectivity needed to support the client in meeting health goals (Kines, 1999). In addition to its impact on the nurse-client relationship, overinvolvement can compromise the nurse’s obligation to the service agency, a professional commitment to the treatment regimen, collegial relationships with other health team members, and professional responsibilities to other clients (Morse, 1991).
Warning signs that the nurse is becoming overinvolved include the following:
• Giving extra time and attention to certain clients
• Visiting clients in off hours
• Doing things for clients that the clients could do for themselves
• Discounting the actions of other professionals
• Keeping secrets with the client
• Believing that the nurse is the only one who understands the client’s needs
The opposite of overinvolvement is disengagement, which occurs when nurses find themselves withdrawing from clients because of a client’s behavior or the intensity of client suffering. Deaths and high stress levels on a unit can create compassion fatigue, which can lead to disengagement as a self-protective mechanism (Hofmann, 2009). Nurses tend to disengage from clients who are sexually provocative, complaining, hostile, or extremely anxious or depressed. Physical characteristics such as poor hygiene, marked physical disability, socially stigmatized illness, or an unusual or altered appearance can negatively affect the nurse’s willingness to engage with a client.
Signs of disengagement include withdrawal, limited perfunctory contacts, minimizing the client’s suffering, and defensive or judgmental communication. Regardless of the reason, the outcome of disengagement is that the client feels isolated and sometimes abandoned when care is mechanically delivered with limited human connection.
Maintaining a helpful level of involvement is always the responsibility of the professional nurse (see Figure 5-1). Carmack (1997) suggests that nurses can take the following actions to regain perspective:
• Assume full responsibility for the process of care while acknowledging that the outcome usually is not within your control.
• Focus on the things that you can change while acknowledging that there are things over which you have no control.
• Be aware and accepting of your professional limits and boundaries.
• Monitor your reactions, and seek assistance when you feel uncomfortable about any aspect of the relationship.
• Balance giving care to a client with taking care of yourself, without feeling guilty.
Debriefing after a highly emotional event helps nurses resolve and put strong feelings into perspective. Support groups for nurses working in high-acuity nursing situations and mentoring of new nurses are recommended.
Therapeutic use of self
The therapeutic relationship is not simply about what the nurse does, but who the nurse is in relation to clients and families. One of the most important tools nurses have at their disposal is the use of self. LaSala (2009) uses the words of Florence Nightingale, that a nurse achieves “the moral ideal” whenever he or she uses “the whole self” to form relationships with “the whole of the person receiving care” (p. 423) to explain the optimum involvement of self in the nurse-client relationship. The relationships that nurses establish with clients and their families and other practitioners in which “the whole self” is drawn into the process serves as the primary means for putting into action health treatments and healing interventions needed for client support and self-care.
Authenticity
Authenticity is a precondition for the therapeutic use of self in the nurse-client relationship. Authenticity requires recognizing personal vulnerabilities, strengths, and limitations, working within this knowledge in the service of the client, and seeking help when needed to further relationship goals. Self-awareness allows you to fully engage with a client, knowing that parts of the relationship may be painful, distasteful, or uncomfortable. Daniels (1998) suggests that when nurses recognize parts of themselves in their clients, they humanize the nurse-client relationship.
Nurses need to be clear about their personal values, beliefs, stereotypes, and personal perspectives because of their potential influence on client decisions (McCormack & McCance, 2006; Morse, Havens, & Wilson, 1997). There are some clients whom nurses simply don’t like working with (Erlen & Jones, 1999). It is up to the nurse, not the client, to resolve interpersonal issues that get in the way of the relationship. Nurses need to acknowledge overinvolvement, avoidance, anger, frustration, or detachment from a client when it occurs. A useful strategy in such situations is to seek further understanding of the client as a person by acknowledging your knowledge deficit and seeking to correct it.
Authenticity requires admitting mistakes. For example, a nurse might promise a client to return immediately with a pain medication and then forget to do so because of other pressing demands. When the nurse brings the medication, the client might accuse the nurse of being uncaring and incompetent. It would be appropriate for the nurse to apologize for forgetting the medication, and for the extra discomfort suffered by the client.
Presence
Nursing presence involves being with the client in the moment, in a manner that both nurse and client can recognize. McDonough-Means, Kreitzer and Bell (2004) describe presence as having two dimensions: “being there” and “being with” (p. S25). The sense of connectivity is simultaneously experienced by those involved in the process: nurse, client, family. Nursing presence is evidenced through active listening, relevant caring communication, and sharing of skills, knowledge, and competencies related to client-specific problems (McCormack & McCance, 2006; Morse et al., 1997). Presence involves the nurse’s capacity to know when to provide help and when to stand back, when to speak frankly, and when to withhold comments because the client is not ready to hear them. The gift of presence enriches the sense of self, and life of both patient and nurse, in ways that are unique to each person and situation (Covington, 2003; Easter, 2000).
Self-awareness
Peplau (1997) notes that nurses must observe their own behavior, as well as the client’s, with “unflinching self-scrutiny and total honesty in assessment of their behavior in interactions with patients” (p. 162). Self-awareness requires a reflective process that seeks to understand one’s personal values, feelings, attitudes, motivations, strengths, and limitations—and how these affect practice and client relationships. By critically and simultaneously examining the behaviors of the client and the nurse, and what is going on in the relationship, nurses can create a safe, trustworthy, and caring relational structure (Lowry, 2005). Questions developed by Carl Rogers (1958) that nurses can ask themselves to promote the professional self-awareness needed in nurse-client relationships are presented in Box 5-2.
Applications
Peplau (1952) described four sequential phases of a nurse-client relationship, each characterized by specific tasks and interpersonal skills: preinteraction, orientation, working (problem identification and exploitation), and termination. The phases are overlapping and serve to broaden as well as deepen the emotional connection with clients (Reynolds, 1997). Although her theoretical model of relationships is better applied to long-term relationships, the concepts hold true for short encounters. Peplau identified six professional roles the nurse can assume during the course of the nurse-client relationship (Box 5-3).
Peplau’s developmental stages parallel the nursing process. The orientation phase correlates with the assessment phase of the nursing process. The identification component of the working phase corresponds to the planning phase, whereas the exploitation phase parallels the implementation phase. The final resolution phase of the relationship corresponds to the evaluation phase of the nursing process (see Chapter 2 for details on the nursing process). Table 5-2 identifies interviewing strategies associated with each phase of the nurse-client relationship.
TABLE 5-2
Interviewing and Relationship Skills
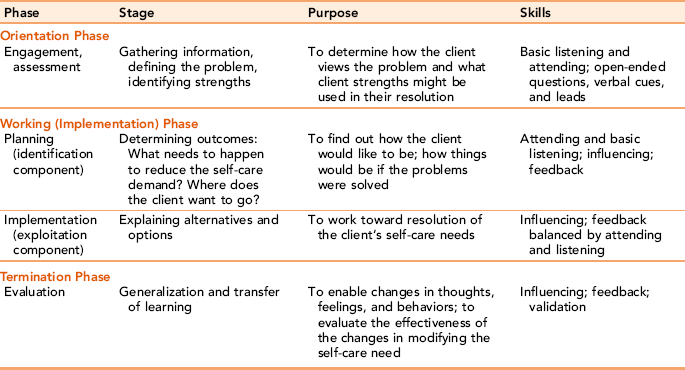
Data Sources: Ivey A, Ivey M: Ivey’s five stage model of interviewing. In Ivey A, editor, Intentional interviewing and counseling, Monterey, CA, 2002, Brooks/Cole; and Richmond V, McCroskey J, Payne S: Nonverbal behavior in interpersonal relations, Englewood Cliffs, NJ, 1987, Prentice Hall; Peplau H: Peplau’s theory of interpersonal relations, Nursing Science Quarterly 10(4):162–167, 1997.

Preinteraction phase
The preinteraction phase is the only one in which the client does not directly participate. Awareness of professional goals is important. Developing professional goals helps the nurse select concrete, specific nursing actions that are purposeful and aligned with individualized client needs.
Professional goals differ from client goals, having to do with the nurse’s knowledge, competence, and control of role responsibilities in the nurse-client relationship. Although professional goals are not communicated directly to clients, they are present as professional behaviors in all aspects of nursing care.
Having an idea of potential client issues before meeting with the client is helpful. For example, a different approach is required for a client whose infant is in the neonatal intensive care unit, than for a client who is rooming in with a healthy infant.
If the relationship is to be ongoing, for example, in a subacute, rehabilitation, or psychiatric setting, it is important to share initial plans related to time, purpose, and other details with staff. This simple strategy helps avoid scheduling conflicts.
Creating the Physical Environment: Specific client needs dictate the most appropriate interpersonal setting. When the interview takes place at the client’s bed in a hospital setting, the curtain should be drawn and the nurse can sit at an angle facing the client. One-on-one relationships with psychiatric clients commonly take place in a designated, noiseless room apart from the client’s bedroom. In the client’s home, the nurse is always the client’s guest. A private space in which the nurse and client can talk without being uninterrupted is essential. Each time a nurse is sensitive to the environment in a nurse-client relationship, the nurse models thoughtfulness, respect, and empathy.
Orientation phase
The nurse enters the relationship in the “stranger” role and begins the process of developing trust by providing the client with basic information about the nurse (e.g., name and professional status) and essential information about the purpose, nature, and time available for the relationship (Peplau, 1997). It can be a simple introduction: “I am Susan Smith, a registered nurse, and I am going to be your nurse on this shift.” Nonverbal supporting behaviors of a handshake, eye contact, and a smile reinforce spoken words. Introductions are important even with clients who are confused, aphasic, comatose, or unable to make a cogent response because of mental illness or dementia. Introductions may need to be repeated, particularly for cognitively disabled clients.
Next, the nurse can ask the client, “How would you prefer to be addressed?” Assure the client that personal information will be treated as confidential (Heery, 2000). Explain that data will be shared with other members of the health care team as needed for making relevant clinical decisions and informing the client about the general composition of the health care team. Exercise 5-2 is designed to give you practice in making introductory statements.
Clarifying the Purpose of the Relationship: Clarity of purpose related to identifiable health needs is an essential dimension of the nurse-client relationship (LaSala, 2009). It is difficult to fully participate in any working partnership without understanding its purpose and expectations. Clients need basic information about the purpose and nature of the interview or relationship, including what information is needed and how the information will be used, how the client can participate in the treatment process, and what the client can expect from the encounter. To understand the importance of orientation information, consider the value of having a clear syllabus for your nursing courses.
The length of the relationship dictates the depth of the orientation. An orientation given to a client by a nurse assigned for a shift would be different from that given to a client when the nurse assumes the role of primary care nurse over an extended period. When the relationship is of longer duration, the nurse should discuss the parameters of the relationship (e.g., length of sessions, frequency of meetings, and role expectations of the nurse and client).
Initial meetings should have two outcomes: First, the client should emerge from the encounter with a better idea of the most relevant health issues; second, the client should feel that the nurse is interested in him or her as a person. At the end of the contact, the nurse should thank the client for his or her participation and indicate what will happen next.
Establishing Trust: Carter (2009) defines trust as “a relational process, one that is dynamic and fragile, yet involving the deepest needs and vulnerabilities of individuals” (p. 404). Starting with the first encounter, clients begin to assess the nurse’s trustworthiness. Kindness, competence, and a willingness to become involved are communicated through the nurse’s words, tone of voice, and actions. Does the nurse seem to know what he or she is doing? Is the nurse tactful and respectful of cultural differences? Data regarding the level of the nurse’s interest and knowledge base are factored into the client’s decision to engage actively in a therapeutic relationship. Confidentiality, sensitivity to client needs, and honesty strengthen the relationship.
The level of trust fluctuates with illness, age, and successful and unsuccessful encounters with others (Carter, 2009). Knowledge of the client’s developmental level helps frame therapeutic conversations. For example, you would hold a different conversation with an adolescent client than you would with an elderly client. The acutely ill client will need short contacts that are to the point and related to providing comfort and care. The client’s current health situation is a good starting place for choice of topic.
Trusting the nurse is particularly difficult for the seriously mentally ill, for whom the idea of having a professional person care about them can be incomprehensible. Having this awareness helps the nurse look beyond the bizarre behaviors that these clients present in response to their fears about helping relationships. Many mentally ill clients will respond better to shorter, frequent contacts until trust is established. Schizophrenic clients often enter and leave the space occupied by the nurse, almost circling around a space that is within visual distance of the nurse. With patience and tact, the nurse engages the client slowly with a welcoming look and brief verbal contact. Over time, brief meetings that involve an invitation and a statement as to when the nurse will return help reduce the client’s anxiety, as indicated in the following dialogue.
Identifying Client Needs: Therapeutic relationships should directly revolve around the client’s needs and preferences. Each person’s experience and individualized expression of them will be different. How clients perceive their health status, reasons for seeking treatment at this time, and expectations for health care are critical data, which you can begin to elicit by simply asking the client why he or she is seeking treatment at this time. Using questions that follow a logical sequence and asking only one question at a time help clients feel more comfortable, and is likely to elicit more complete data.
Client and family expectations can facilitate or hinder the treatment process. When health professionals treat elderly, adolescent, or physically handicapped clients as though they are mentally incapacitated in assessment interviews, it devalues them as a person. On the other hand, family members are sometimes reluctant to challenge a client’s perceptions in front of the client and may need a private interview. Nurses need to include both perspectives for accurate assessment.
Similarities and differences between client and family perceptions of illness and treatment are important data. If there is reason to suspect the reliability of the client as a historian, interviewing significant others assumes greater importance. Family/client agreement or disagreement about diagnosis, treatment goals, or ways to provide care are critical data. For example, if a client has one perception about personal self-care abilities and family members have a completely different awareness, these differences can become a nursing concern.
Participant Observation: Peplau describes the role of the nurse in all phases of the relationship as being a participant observer. This means that the nurse simultaneously participates in and observes the progress of the relationship from the nurse and the client perspective. When validated with the client, observations about the client’s behavior and words serve as guides for subsequent dialogue and actions in the relationship. According to Peplau, observation includes self-awareness and self-reflection on the part of the nurse. This is as critical to the success of the relationship as is the assessment of the client’s situation (McCarthy and Aquino-Russell, 2009).
By linking the emotional context with the content of the client’s message, the nurse enters into the client’s world and shows a desire to understand the situation from the client’s perspective. Nurses need to be aware of the different physical and nonverbal cues clients give with their verbal messages. Noting facial expressions and nonverbal cues with “You look exhausted” or “You look worried” acknowledges the presence of these factors and normalizes them. Exercise 5-3 is designed to help you to critically observe a person’s nonverbal cues.
EXERCISE 5-3 Nonverbal Messages
Purpose: To provide practice in validation skills in a nonthreatening environment.

Defining the Problem: Nurses act as a sounding board, asking questions about parts of the communication that are not understood and helping clients to describe their problems in concrete terms. The nurse asks for specific details to bring the client’s needs into sharper focus, for example, “Could you describe for me what happened next,” or “Tell me something about your reaction to (your problem),” or “how do you feel about…”? Time should be allowed between questions for the client to respond fully. Commonly, such questions are asked but not enough time is allowed for the client to respond.
Clients usually find it easier to talk about factual data related to a problem rather than to express the feelings associated with the issue. For example, saying “It sounds as if you feel ____________ because of ____________” helps the client to articulate the relationships between situational data and its emotional impact.
Once the nurse and client develop a working definition of the problem, they can begin to brainstorm the best ways to meet treatment goals. The brainstorming process occurs more easily when nurses are relaxed and willing to understand views different from their own. Brainstorming involves generating multiple ideas and suspending judgment until after all possibilities are presented. The next step is to look realistically at ideas that could work given the resources the client has available right now. Resistance can be worked through with empathetic reality testing. Peplau (1997) suggests that a general rule of thumb in working with clients is to “struggle with the problem, not with the patient” (p. 164). The last part of the process relates to determining the kind of help needed and who can best provide it. Assessment of the most appropriate source of help is an important but often overlooked part of the evaluation needed in the orientation phase.
Defining Goals: Unless clients are physically or emotionally unable to participate in their care, they should be treated as active partners in developing personal goals. Goals should have meaning to the client. For example, modifying the exchange lists with a diabetic adolescent’s input so that they include substitutions that follow normal adolescent eating habits can facilitate acceptance of unwelcome dietary restrictions. The nurse conveys confidence in the client’s capacity to solve his or her own problems by expecting the client to provide data, to make constructive suggestions, and develop realistic goals.
Working (exploitation/active intervention) phase
With relevant treatment goals to guide nursing interventions and client actions, the conversation in the working phase turns to active problem solving related to assessed health care needs. Clients are able to discuss deeper, more difficult issues and to experiment with new roles and actions. Corresponding to the implementation phase of the nursing process, the working phase focuses on self-direction and self-management to whatever extent is possible in promoting the client’s health and well-being.
Peplau (1997) has categorized the client role as dependent, interdependent, or independent, based on the amount of responsibility the client is willing or able to assume for his or her care. Nurses should provide enough structure and guidelines for clients to explore problem issues and develop realistic solutions, but no more than are needed (Ballou, 1998). Avoid taking more responsibility for actions than the client or situation requires. For example, it may seem more efficient to give a bath to a stroke victim than to watch the client struggle through the bathing process with the nurse providing coaching when the client falters. However, what happens when the client goes home if she has not learned to bathe herself?
Breaking a seemingly insoluble problem down into simpler chunks is a nursing strategy that makes doing difficult tasks more manageable. For example, a goal of eating three meals a day may seem overwhelming to a person suffering from nausea and loss of appetite associated with gastric cancer. A smaller goal of having applesauce or chicken soup and a glass of milk three times a day may sound more achievable, particularly if the client can choose the times.
In even the most difficult nursing situations, there are options, even if the choice is to die with dignity or to change one’s attitude toward an illness or a family member. The client’s right to make decisions, provided they do not violate self or others, needs to be accepted by the nurse, even when it runs contrary to the nurse’s thinking. This protects the client’s right to autonomy.
Tuning in to Client Response Patterns: The art of nursing requires that nurses recognize differences in client response patterns. Elderly adults may need a slower pace, and people in crisis will need a simple structured level of support. Throughout the working phase, nurses need to be sensitive about whether the client is still responding at a useful level. Looking at difficult problems and developing strategies to resolve those problems is not an easy process, especially when resolution requires significant behavioral changes. If the nurse is perceived as inquisitive rather than facilitative, communication breaks down.
It is the responsibility of the nurse, not the client, to pace interactions in ways that offer support, as well as challenge. Deciding whether to proceed is a clinical judgment that should be based on the client’s response and overall body language. Examples of warning signs that the pace may need adjustment include loss of eye contact, fidgeting, abrupt changes in subject, or asking to be left alone. At the same time, strong emotion should not necessarily be interpreted as reflecting a level of interaction stretching beyond the client’s tolerance. Tears or an emotional outburst may reflect honestly felt emotion. A well-placed comment, such as, “I can see that this is difficult for you,” acknowledges the feeling and may stimulate further discussion.
The working phase may produce uneven results, with two steps forward and one backward, even when the plan is appropriate. Mistakes are to be expected. They should be treated as temporary setbacks and new information requiring a modification in strategy. Developing alternative constructive coping mechanisms is as important to support as the actual plan. Coping with unexpected responses can strengthen the client’s problem-solving abilities by compelling the person to consider alternative options (i.e., a Plan B) when the original plan does not bring about the desired results. Exercise 5-4 examines the role of brainstorming in generating alternative strategies.
As clients use the relationship to support coping with health-related situations, nurses can offer anticipatory guidance and role rehearsal for difficult aspects of this process. Sometimes, simply anticipating the worst-case scenario for a given action allows the client to see that even the worst possibility is manageable.
Defusing Challenging Behaviors: Challenging behaviors can sabotage the therapeutic relationship if they are not addressed early in the relationship process. There is no one way to approach a client, and no single interpersonal strategy that works equally well with every client. Some clients clearly are more emotionally accessible and attractive to work with than others. When a client seems unapproachable or uninterested in human contact, it can be quite disheartening for the nurse. It is not uncommon for the nurse to report the kind of initial contact with a client seen in the following case examples.
Although, from the nurse’s perspective, this client’s behavior may represent a lack of desire for a relationship, in most cases, the rejection is not personal. It can reflect boredom, insecurity, or physical discomfort. Anxiety expressed as anger or unresponsiveness may be the only way a client can control fear in a difficult situation. Rarely does it have much to do with the personal approach used by the nurse unless the nurse is truly insensitive to the client’s feelings or the needs of the situation. In this situation, the nurse might say, “It seems to me that you just want to be alone right now. But I would like to help you, so if you don’t mind, I’ll check back later with you. Would that be OK with you?” Most of the time, clients appreciate the nurse’s willingness to stay involved.
For novice nurses, it is important to recognize that all nurses have experienced some form of client rejection at one time or another. The nurse needs to explore whether the timing was right, whether the client was in pain, and what other circumstances might have contributed to the client’s attitude. Behaviors that initially seem maladaptive may appear quite adaptive when the full circumstances of the client’s situation are understood.
Before confronting a client, the nurse should anticipate possible outcomes. The nurse needs to appreciate the impact of the confrontation on a client’s self-esteem. Calling a client’s attention to a contradiction in behavioral response is usually threatening. Constructive feedback involves drawing the client’s attention to the existence of unacceptable behaviors or contradictory messages whereas respecting the fragility of the therapeutic alliance and the client’s need to protect the integrity of the self-concept. To be effective, constructive confrontations should be attempted only when the following criteria have been met:
• The nurse has established a firm, trusting bond with the client.
• The timing and environmental circumstances are appropriate.
• The confrontation is delivered in a private setting, and in a nonjudgmental and empathetic manner.
• Only those behaviors capable of being changed by the client are addressed.
• The nurse supports the client’s right to self-determination.
Self-disclosure: Self-disclosure by the nurse refers to the intentional revealing of personal experiences or feelings that are similar to or different from those of the client. The purpose of self-disclosure is to deepen trust, to role-model self-disclosure as a beneficial mode of communicating for people who have trouble disclosing information about themselves. Appropriate self-disclosure can facilitate the relationship, providing the client with information that is both immediate and personalized (Deering, 1999).
Quality, not quantity, is a key characteristic of effective sharing in the working phase. Sharing should be solely for the clinical benefit of the client and never to meet the personal agenda of the nurse. Nurses should not share intimate details of their lives with their clients. The nurse, not the client, is responsible for regulating the amount of disclosure needed to facilitate the relationship. If the client asks a nonoffensive, superficial question, the nurse may answer briefly with a minimum of information and return to a client focus. Simple questions such as, “Where did you go to nursing school?” and “Do you have any children?” may represent the client’s effort to establish common ground for conversation (Morse, 1991). Answering the client briefly and returning the focus to the client is appropriate. If the client persists with questions, the nurse may need to redirect the client by saying, “I’d like to spend this time talking about you,” or simply indicate that personal questions are not relevant to understanding the client’s health care needs.
Deering (1999) suggests the following guidelines for keeping self-disclosure at a therapeutic level: (a) use self-disclosure to help clients open up to you, not to meet your own needs; (b) keep your disclosure brief; and (c) don’t imply that your experience is exactly the same as the client’s. Exercise 5-5 provides an opportunity to explore self-disclosure in the nurse-client relationship.
Termination Phase
It is important to be clear from the beginning about how long a therapeutic relationship will last. During the course of the relationship, termination can be mentioned, and clients should be told well in advance of an impending termination date. In the termination phase, the nurse and client evaluate the client’s responses to treatment, and explore the meaning of the relationship and what goals have been achieved. Discussing client achievements, how the client and nurse feel about ending the relationship, and plans for the future are an important part of the termination phase.
Termination is a significant issue in long-term settings such as skilled nursing facilities, bone marrow transplant units, rehabilitation hospitals, and state psychiatric facilities. Significant long-term relationships can and do develop in these settings. If the relationship has been effective, real work has been accomplished. Nurses need to be sufficiently aware of their own feelings so that they may use them constructively without imposing them on the client. It is appropriate for nurses to share some of the meaning the relationship held for them, as long as such sharing fits the needs of the interpersonal situation and is not excessive or too emotionally intense.
Termination of a meaningful nurse-client relationship in long-term settings should be final. To provide the client with even a hint that the relationship will continue is unfair. It keeps the client emotionally involved in a relationship that no longer has a health-related goal. This is a difficult issue for nursing students, who either see no harm in telling the client they will continue to keep in contact or who feel they have used the client for their own learning needs and to completely close the door is unfair. However, this perception underestimates the positive things that the client received from the relationship and denies the fact that good-byes, painful as they may be, are a part of life and certainly not new for the client or for the nursing student.
Termination behaviors the nurse may encounter include avoidance, minimizing of the importance of the relationship, anger, demands, or additional reliance on the nurse. When the client is unable to express feelings about endings, the nurse may recognize them in the client’s nonverbal behavior.
Gift Giving: Clients sometimes wish to give nurses gifts at the end of a constructive relationship because they value the care nurses have given to them. Gift giving is a delicate matter that does not lend itself to absolute dictums, but instead invites reflection and professional judgment. Nurses should consider: What meaning does the gift have for the relationship, and in what ways might accepting it change the dynamics of the therapeutic alliance? Would giving or receiving a gift present issues for other clients or their families?
There is no one answer about whether gifts should or should not be exchanged. In fact, if the nurse handled every situation in the same fashion, the nurse would be denying the uniqueness of each nurse-client relationship. Each relationship has its own character and its own strengths and limitations, so what might be appropriate in one situation would be totally inappropriate in another. Token gifts such as chocolates or flowers may be acceptable. In general, nurses should not accept money or gifts of significant material value. Should this become an issue, you might suggest making the gift to the health care agency or a charity. It is always appropriate to simply thank the client for their generosity and thoughtfulness (Lambert, 2009). Exercise 5-6 is designed to help you think about the implications of gift giving in the nurse-client relationship.
Evaluation: Objective evaluation of clinical outcomes achieved in the nurse-client relationship should focus on the following:
• Was the problem definition adequate and appropriate for the client?
• Were the interventions chosen adequate and appropriate to resolve the client’s problem?
• Were the interventions implemented effectively and efficiently to both the client’s and the nurse’s satisfaction in the allotted time frame?
• Is the client progressing toward maximum health and well-being? Is the client satisfied with his or her progress and care received?
• If follow-up care is indicated, is the client satisfied and able to carry forward his or her treatment plan in the community.
Adaptations for short-term relationships
Hagerty and Patusky (2003) argue the need to reconceptualize the nurse-patient relationship to one of human relatedness, given the brevity of hospital stays in today’s evolving health care arena. Driven by the economics of managed care, nurses must help clients determine what they need and how to develop solutions that fit their situation much more quickly than previously. Although nurses can and should follow the phases of the relationship, developing a therapeutic relationship in short-term care could be more accurately termed a working alliance with active support.
The same recommendations for self-awareness, empathy, therapeutic boundaries, active listening, competence, mutual respect, partnership, and level of involvement hold true as key elements of brief therapeutic relationships.
Orientation Phase: The therapeutic alliance begins with the same type of introduction and description of purpose identified for long-term relationships, with a focus on the nurse and client working as partners to develop a shared understanding of the client’s health problems. Establishing a working alliance where time is an issue requires a “here and now” focus on problem identification and an emphasis on quickly understanding the context in which it arose.
Begin your client assessment by asking the client the reason for seeking care. Eliciting the client’s concerns and allowing the client to tell his or her story conveys respect and interest. Listen for what is left out and pay attention to what the client’s story elicits in you. Support and empathy help build trust quickly. Dealing with the client’s feelings with a statement such as “Tell me more about…” (with a theme picked up from the client’s choice of words, hesitancy, or nonverbal cues) keeps the conversation flowing.
As the nurse interacts with the client, there are opportunities to observe client strengths and to comment on them. Every client has healthy aspects of his or her personality, and personal strengths that can be drawn on to facilitate individual coping responses. Exercise 5-7 provides an opportunity to explore the value of acknowledging personal strengths.
An important component of brief therapeutic relationships is the rapid development of a central focus, which is developed during an initial client evaluation. Cappabianca, Julliard, Raso and Ruggiero (2009) suggest that a simple statement posed at the beginning of each shift, such as, “What is your most important need today?” or “What is the most important thing I can do for you today?” helps focus the relationship. This type of question demonstrates intent to understand and meet each client’s unique needs in a shortened time frame. It helps client and nurse develop a shared understanding of what is uniquely important to the client in the present moment.
Because the time frame for a therapeutic relationship may be a few hours or days, nurses need to focus on what is absolutely essential, rather than what would be nice to know. Finding out how much the client already knows can save a lot of time. Developed from this discussion are treatment goals that can be realistically achieved, and are consistent with client goals, beliefs, and preferences.
Planning will be smoother if the nurse and client choose problems that are of interest to the client and that offer the best return on investment. Included in the planning should be the risks and cost/benefits for each targeted clinical outcome given the shortened time frame. Looking at the client’s needs from a broader contextual perspective, one that takes into consideration which problems, if treated, would also help correct other health problems, has a double benefit in terms of client success and satisfaction. Engaging the client’s family early in the treatment process is helpful.
As nurses increasingly move from a bedside role into a managerial coordination role, they become increasingly responsible for clarifying, integrating, and coordinating different aspects of the client’s care, as part of an interdisciplinary team. An important component of this responsibility is ensuring that the client/family understands and is able to negotiate treatment initiatives with health care team providers.
Working Phase: Brief relationships need to be solution-focused right from the beginning. Giving clients your undivided attention and using concise active listening responses is absolutely essential to being able to frame issues in a solution focused way. A central focus, agreed on by nurse and client, allows for the small behavioral changes and related coping skills needed to meet client goals in short-term relationships. Finding ways to collaborate makes the most effective use of time, and confrontation should be avoided. Longer term issues are not examined in depth and support beyond what is needed to stabilize the client. Clients respond best to nurses who appear confident and empathetic. An excellent way of helping clients discover the solutions that fit them best is by engaging the client in determining and implementing activities to meet therapeutic goals at every realistic opportunity. Conveying a realistically hopeful attitude that the goals developed with the client are likely to be achieved is important. Action plans should be as simple and specific as possible. Changes in the client’s condition or other circumstances may require treatment modifications that should be expected in short term relationships. Keeping clients and families informed and working with them on alternative solutions is essential to maintaining trust in short term relationships.
Termination Phase: The termination phase in short-term relationships can include discharge planning, agency referrals, and arranging for follow-up appointments in the community for the client and family. Anticipatory guidance in the form of simple instructions or review of important skills also may be appropriate, depending on the circumstances. Interpersonal relationships with other health care disciplines, families, and communities to support positive client health changes should be the norm, not the exception with short-term therapeutic relationships.
The importance of the relationship, no matter how brief, should not be underestimated. Although the client may be one of several persons the nurse has taken care of during that shift, the relationship may represent the only interpersonal or professional contact available to a lonely and frightened person. Even if contact has been minimal, the nurse should endeavor to stop by the client’s room to say good-bye. The dialogue in such cases can be simple and short: “Mr. Jones, I will be going off duty in a few minutes. I enjoyed working with you. Miss Smith will be taking care of you this evening.” If you will not be returning at a later date, this information should be shared with the client.
Summary
The nurse-client relationship represents a purposeful use of self in all professional relations with clients and other people involved with the client. Respect for the dignity of the client and self, person-centered communication, and authenticity in conversation are process threads underlying all communication responses.
Therapeutic relationships have professional boundaries, purposes, and behaviors. Boundaries keep the relationship safe for the client. They spell out the parameters of the therapeutic relationship and nurses are ethically responsible for maintaining them throughout the relationship. Effective relationships enhance the well-being of the client and the professional growth of the nurse. The professional relationship goes through a developmental process characterized by four overlapping yet distinct stages: preinteraction, orientation, working phase, and termination phase. The preinteraction phase is the only phase of the relationship the client is not part of. During the preinteraction phase, the nurse develops the appropriate physical and interpersonal environment for an optimal relationship, in collaboration with other health professionals and significant others in the client’s life.
The orientation phase of the relationship defines the purpose, roles, and rules of the process, and provides a framework for assessing client needs. The nurse builds a sense of trust through consistency of actions. Data collection forms the basis for developing relevant nursing diagnoses. The orientation phase ends with a therapeutic contract mutually defined by nurse and client.
The working phase is the problem-solving phase of the relationship, paralleling the planning and implementation phases of the nursing process. As the client begins to explore difficult problems and feelings, the nurse uses a variety of interpersonal strategies to help the client develop new insights and methods of coping.
The final phase of the nurse-client relationship occurs when the essential work of the active intervention phase is finished. The ending should be thoroughly and compassionately defined early enough in the relationship that the client can process it appropriately. Primary tasks associated with the termination phase of the relationship include summarization and evaluation of completed activities, and referrals when indicated. Short-term relationships incorporate the same skills and competencies as traditional nurse-client relationships, but with a sharper focus on the here and now. The action plan needs to be as simple and specific as possible.
References
Anderson, H. Postmodern collaborative and person-centered therapies: what would Carl Rogers say? Journal of Family Therapy. 2001;23:339–360.
Ballou, K. A concept analysis of autonomy. J Prof Nurs. 1998;14(2):102–110.
Briant, S., Freshwater, D. Exploring mutuality within the nurse-patient relationship. Br J Nurs. 1998;7(4):204–206.
Bruner, K., Yonge, O. Boundaries and adolescents in residential treatment centers: what clinicians need to know. Journal of Psychosocial Nursing. 2006;44(9):38–44.
Buber, M.. Smith R.G., ed. I and thou. New York: Charles Scribner’s, 1958.
Buber, M. Distance and relation. Psychiatry. 1957;20:97–104.
Cappabianca, A., Julliard, K., Raso, R., Ruggiero, J. Strengthening the nurse-patient relationship: what is the most important thing I can do for you today. Creat Nurs. 2009;15(3):151–156.
Carmack, B. Balancing engagement and disengagement in caregiving. Image (IN). 1997;29(2):139–144.
Carter, M. Trust, power, and vulnerability: a discourse on helping in nursing. Nurs Clin North Am. 2009;44:393–405.
Chauhan, G., Long, A., Communication is the essence of nursing care, 2: ethical foundations. Br J Nurs, 2000;9(15):979–984. Available online:, http://www.cno.org/docs/prac/41033_Therapeutic.pdf.
Covington, H. Caring presence: delineation of a concept for holistic nursing. J Holist Nurs. 2003;21(3):301–317.
Daniels, L. Vulnerability as a key to authenticity. Image J Nurs Sch. 1998;30(2):191–193.
Deering, C.G. To speak or not to speak? Self-disclosure with clients. Am J Nurs. 1999;99(1 Pt 1):34–38.
Easter, A. Construct analysis of four modes of being present. J Holist Nurs. 2000;18(4):362–377.
Egan, G. The skilled helper, ed 7. Pacific Grove, CA: Brooks Cole Publishing, 2002.
Erlen, J.A., Jones, M. The patient no one liked. Orthop Nurs. 1999;18(4):76–79.
Fronek, P., Kendall, M., Ungerer, G., Malt, J., Eugarde, E., Geraghty, T. Towards healthy professional-client relationships: the value of an interprofessional training course. J Interprof Care. 2009;23(10):16–29.
Hagerty, B., Patusky, K. Reconceptualizing the nurse-patient relationship. J Nurs Scholarsh. 2003;35(2):145–150.
Hartley, S. Drawing the lines of professional boundaries. Renalink. 2002;3(2):7–9.
Heery, K. Straight talk about the patient interview. Nursing. 2000;30(6):66–67.
Heinrich, K. When a patient becomes too special. Am J Nurs. 1992;22(11):62–64.
Hofmann, P., Addressing compassion fatigue. Health Care Executive, 2009;Sept/Oct:40–42.
Hook, M. Partnering with patients—A concept ready for action. J Adv Nurs. 2006;56(2):133–143.
Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academy Press, 2001.
Joint Commission. The Health care at the crossroads: strategies for addressing the evolving nursing crisis. Washington, DC: Author, 2001.
Kines, M. The risks of caring too much. Can Nurs. 1999;95(8):27–30.
Lambert, K. Gifts and gratuities for the case manager. Professional Case Management. 2009;14(1):53–54.
LaSala, C. Moral accountability and integrity in nursing practice. Nurs Clin North Am. 2009;44:423–434.
Lowry, M. Self-awareness: is it crucial to clinical practice? Confessions of a self-aware-aholic. Am J Nurs. 105(11), 2005. [72CCC–72DDD].
McCarthy, C., Aquino-Russell, C.A. comparison of two nursing theories in practice: Peplau and Parse. Nurs Sci Q. 2009;22(1):34–40.
McDonough-Means, M.J., Kreitzer, Bell, I. Fostering a healing presence and investigating its mediators. J Altern Complement Med. 2004;10(Suppl 1):S25–S41.
McCormack, B., McCance, T.V. Development of a framework for person-centred nursing. J Adv Nurs. 2006;56(5):472–479.
McGrath, D. Healthy conversations: key to excellence in practice. Holist Nurs Pract. 2005;19(4):191–193.
McQueen, A. Nurse–patient relationships and partnership in hospital care. J Clin Nurs. 2000;9(5):723–731.
Morse, J. Negotiating commitment and involvement in the nurse-patient relationship. J Adv Nurs. 1991;16:455–468.
Morse, J.M., Havens, G.A., Wilson, S. The comforting interaction: developing a model of nurse-patient relationship. Sch Inq Nurs Pract. 1997;11(4):321–343.
National Council of State Boards of Nursing (NCSBN) Professional boundaries, Chicago, Author, 2007. Available online:, www.ncsbn.org/Professional_Boundaries_2007_Web.pdf. [Accessed December 15, 2009].
O’Kelly, E. Countertransference in the nurse-patient relationship: a review of the literature. J Adv Nurs. 1998;28(2):391–397.
Peplau, H.E. Interpersonal relations in nursing. New York: Putnam, 1952.
Peplau, H.E. Peplau’s theory of interpersonal relations. Nurs Sci Q. 1997;10(4):162–167.
Reynolds, W. Peplau’s theory in practice. Nurs Sci Q. 1997;10(4):168–170.
Rogers, C. The characteristics of the helping relationship. Personnel Guidance Journal. 1958;37(1):6–16.
Sheets, V. Professional boundaries: staying in the lines. Dimens Crit Care Nurs. 2001;20(5):36–40.