Communicating in Groups
At the end of the chapter, the reader will be able to:
2 Identify the stages of group development.
3 Discuss theory-based concepts of group dynamics.
4 Apply group concepts in therapeutic groups.
5 Compare and contrast different types of therapeutic groups.
This chapter describes concepts related to group dynamics in therapeutic and organizational settings. Theoretical frameworks related to the stages of group development and role functioning provide a background. Different types of group formats and the stages of group relationships are identified. Applications of group concepts in therapeutic and in work groups complete chapter content.
Basic concepts
A group is more than a random number of individuals occupying the same space. Forsyth (2009) defines group as “two or more individuals who are connected by and within social relationships” (p. 3). Relationships among members are interdependent; each member’s behavior affects the behavior of other group members. Group cultures develop through shared images, values, and meanings that over time become the stories, myths, and metaphors about the group and how it functions.
Primary and secondary groups
Groups are categorized as primary or secondary groups. Primary groups are characterized by an informal structure and social process. Group membership is automatic (e.g., in a family) or is voluntarily chosen because of a common interest (e.g., in scouting, religious, or civic groups). Primary groups are an important part of a person’s self-concept, revealed in self-descriptions such as “I am Jamie’s mother.”
Secondary groups differ from primary groups in structure and purpose; they have a planned, time-limited association; a prescribed structure; a designated leader; and a specific, identified purpose. When groups achieve their goals, the group disbands. Examples include focus groups, therapy and health-related groups, discipline-specific work groups, interdisciplinary health care teams, and educational groups. People join secondary groups for one of three reasons: to meet personally established goals, to develop more effective coping skills, or because it is required by the larger community system to which the individual belongs. Exercise 12-1 identifies the role that group communication plays in a person’s life.

Therapeutic groups
The value of group communication as a therapeutic tool was first introduced by Joseph Pratt, who found that he was able to expand positive outcomes with people treated for tuberculosis (TB), through group classes. Group therapy for psychological issues became apparent during World War II when it was used as a primary treatment modality to treat soldiers for war-related stress (Corey & Corey, 2008). The outcomes were so successful that mental health professionals continued to use group therapy to treat people with psychological problems. Jacob Moreno later developed psychodrama as an experiential form of group therapy, and introduced sociometry as a way to diagram group participation. In the 1930s, Samuel Slavson introduced the idea of using therapeutic activity groups for disturbed children (Rutan, Stone, & Shay, 2007). Many others contributed to the development of group communication as a treatment modality for psychological problems and general medical issues. Some health related groups are one session; most meet on a regular basis to share common concerns and experiences, and to learn new skills. With the exception of self-help groups, and some support groups, a trained group facilitator guides groups in health care.
Irvin Yalom’s classic work (2005) on interactional group process is recognized as the gold standard for describing group communication processes and dynamics in therapeutic settings. Curative changes occur in therapy groups as a result of 11 therapeutic process factors. Yalom and Leszcz (2005) identify these as follows:
5. The corrective recapitulation of the primary family group
6. Development of socializing techniques
11. Existential factors (pp. 1–2).
Group dynamics
Group dynamics is a term used to describe the communication processes and behaviors occurring during the life of the group. They represent a complex blend of individual and group characteristics that interact with each other to achieve a group purpose. Factors that influence dynamics are illustrated in Figure 12-1.
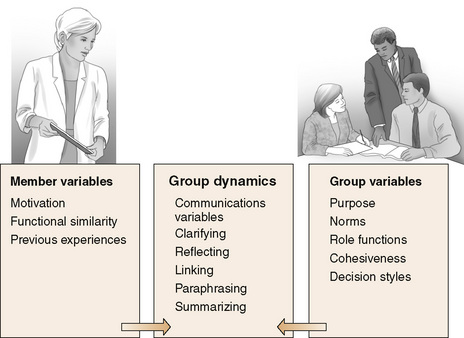
Functional Similarity: Careful selection of group members, based on the person’s capacity to derive benefit from the group and to contribute to group goals, is a critical variable in successful groups. One variable is functional similarity, defined as choosing group members who have enough in common intellectually, emotionally, and experientially to interact with each other in a meaningful way. Exercise 12-2 shows the value of finding things in common. An older, highly educated adult placed in a group of young adults with limited verbal and educational skills can be a group casualty or scapegoat simply because there is not enough in common to be viewed as a peer. Placed in a different group, with clients of a similar intellectual, emotional, and experiential level, the outcome might be quite different.
Whereas it is important that group members have enough in common to understand each other, differences in interpersonal styles help clients learn a broader range of behavioral responses.
Group Purpose: Group purpose supplies the rationale for each group’s existence (Powles, 2007). It provides direction for decisions, encourages the development of relevant group norms, and determines the type of communication and activities required to meet group goals. For example, if a group’s purpose relates to medication compliance, the interventions would be educational. The purpose of a therapy group would be to improve interpersonal functioning and insight into behavior. Purposes of different group types are presented in Table 12-1.
TABLE 12-1
| Group | Purpose |
| Therapy | Reality testing, encouraging personal growth, inspiring hope, strengthening personal resources, developing interpersonal skills |
| Support | Giving and receiving practical information and advice, supporting coping skills, promoting self-esteem, enhancing problem-solving skills, encouraging client autonomy, strengthening hope and resiliency |
| Activity | Getting people in touch with their bodies, releasing energy, enhancing self-esteem, encouraging cooperation, stimulating spontaneous interaction, supporting creativity |
| Education | Learning new knowledge, promoting skill development, providing support and feedback, supporting development of competency, promoting discussion of important health-related issues |
Norms: Group norms refer to the behavioral rules of conduct expected of group members. Norms provide needed predictability for effective group functioning and make the group safe for its members. There are two types of group norms: universal and group specific. Universal norms are stated behavioral standards that must be present in all groups for effective outcomes. Examples include confidentiality, regular attendance, and not socializing with members outside of group (Burlingame et al., 2006). Unless group members can trust that personal information will not be shared outside the group setting (confidentiality), trust will not develop. Regular attendance at group meetings is critical to group stability and goal achievement. Personal relationships between group members outside of the group threaten the integrity of the group as the therapeutic arena for the group’s work.
Group-specific norms evolve from the group itself in the storming phase. They represent the shared beliefs, values, and unspoken operational rules governing group function. Examples include tolerance for latecomers, use of humor or confrontation, and talking directly to other group members rather than about them. Exercise 12-3 will help you develop a deeper understanding of group norms.
Group Role Positions: People in groups assume and/or are ascribed roles that influence their communication and the responses of others. A person’s role position in the group corresponds with the status, power, and internal image that other members in the group have of the member. Group members usually have trouble breaking away from roles they have been cast in despite their best efforts. For example, people will look to the “helper” group member for advice, even when that person lacks expertise or personally needs the group’s help. Other times, group members “project” a role position onto a particular group member that represents a hidden agenda or unresolved issue for the group as a whole (Gans & Alonso, 1998). If the group as a whole seems to scapegoat, ignore, defer to, or consistently idealize one of its members, this group phenomenon can signify a group projection (Moreno, 2007). Exercise 12-4 considers group role position expectations.
Group dynamics
Phases of the group life cycle
Group process refers to the structural development of the group, and describes the phases of its life cycle. Tuckman’s (1965, 1977) model of small-group development provides a framework for examining group process at different stages in the life of the group. He describes five stages: forming, storming, norming, performing, and adjourning (see Figure 12-2). Stages of group development are applicable to work groups, as well as therapeutic groups. Each sequential phase has its own set of tasks that build and expand on the work of previous phases. The concept of stage development is operationalized in the application section of the chapter.
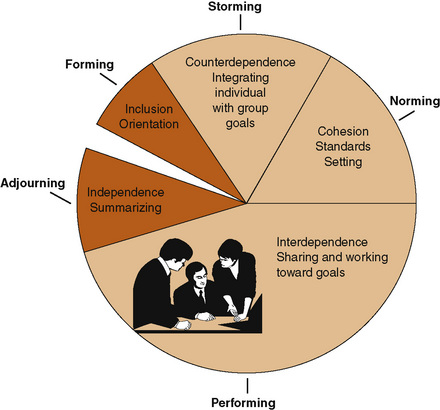
Forming Phase: The forming phase begins when members come together to form a group. Members enter group relationships as strangers to each other. There is high dependence on the leader for direction, and orientation of members to purpose and expectations for behavior is a fundamental leadership responsibility. Getting to know each other, finding common threads in personal experience, and learning about group goals and tasks are emphasized. Members have a basic need for acceptance. Minimal work on the task is accomplished, but this phase cannot be shortchanged without having a serious impact on the evolving effectiveness of the group (Yalom & Leszcz, 2005).
Storming Phase: When a group moves into the storming phase, the gloves come off. This phase is characterized by conflict around interpersonal issues. Members focus on power and control issues. They use testing behaviors around boundaries, communication styles, and personal reactions with other members and the leader. Characteristic behaviors include disagreement with the group format, topics for discussion, the best ways to achieve group goals, and comparisons of member contributions. Although the storming phase is uncomfortable, successful resolution leads to the development of group-specific norms.
Norming Phase: In the norming phase, cohesiveness develops as standards evolved by members are accepted as operational norms. Individual goals become aligned with group goals. The group holds members accountable and challenges individual members who fail to adhere to expected behaviors. Group norms make the group safe, and members begin to experience the cohesiveness of the group as “their group.”
Performing Stage: The group’s “work” is accomplished in the performing phase, which is characterized by interdependence and cohesion. People feel loyal to the group and to individual members. Members are comfortable taking risks, and are invested enough in each other and the group process to offer constructive comments.
Adjourning Phase: Tuckman introduced the adjourning phase as a final phase of group development at a later date (Tuckman & Jensen, 1977). This phase is characterized by reviewing what has been accomplished, reflecting on the meaning of the group’s work together, and making plans to move on in different directions.
Functional group roles
Functional roles differ from positional roles group members assume in that they are related to the type of member contributions needed to achieve group goals. Benne and Sheats (1948) described constructive role functions as the behaviors members use to move toward goal achievement (task functions) and behaviors designed to ensure personal satisfaction (maintenance functions).
Balance between task and maintenance functions increases group productivity. When task functions predominate, member satisfaction decreases and a collaborative atmosphere is diminished. When maintenance functions override task functions, members have trouble reaching goals. Members do not confront controversial issues, so the creative tension needed for successful group growth does not occur. Task and maintenance role functions found in successful small groups are listed in Box 12-1. Exercise 12-5 provides practice in identifying task and maintenance functions.
Benne and Sheats (1948) also identified nonfunctional role functions. Self-roles are roles a person uses to meet self-needs at the expense of other members’ needs, group values, and goal achievement. Self-roles, identified in Table 12-2, detract from the group’s work and compromise goal achievement by taking time away from group issues and creating discomfort among group members.
TABLE 12-2
| Role | Characteristics |
| Aggressor | Criticizes or blames others, personally attacks other members, uses sarcasm and hostility in interactions |
| Blocker | Instantly rejects ideas or argues an idea to death, cites tangential ideas and opinions, obstructs decision making |
| Joker | Disrupts work of the group by constantly joking and refusing to take group task seriously |
| Avoider | Whispers to others, daydreams, doodles, acts indifferent and passive |
| Self-confessor | Uses the group to express personal views and feelings unrelated to group task |
| Recognition | Seeks attention by excessive talking, seeker trying to gain leader’s favor, expressing extreme ideas, or demonstrating peculiar behavior |
Modified from Benne KD, Sheats P: Functional roles of group members, J Soc Issues 4(2):41–49, 1948.
Group leadership
Two basic assumptions support the function of group leadership: (1) Group leaders have a significant influence on group process; and (2) most problems in groups can be avoided or reworked productively if the leader is aware of and responsive to the needs of individual group members, including the needs of the leader (Corey & Corey, 2008).
Effective leadership behaviors require adequate preparation, professional leadership attitudes and behavior, responsible selection of members, and use of a responsible scientific rationale for determining a specific group approach. Personal characteristics demonstrated by effective group leaders include commitment to the group purpose, self-awareness of personal biases and interpersonal limitations, careful preparation for the group and with the group, and an open attitude toward group members. Knowledge of group dynamics, training, and supervision are additional requirements for leaders of psychotherapy groups. Educational group leaders need to have expertise on the topic for discussion.
Throughout the group’s life, the leader models attitudes of caring, objectivity, and integrity. Effective leaders are good listeners, and are able to adapt their leadership style to fit the changing needs of the group. They respectfully support the integrity of group members as equal partners in meeting group goals. Successful leaders trust the group process enough to know that group members can work through conflict and difficult situations. They know that even mistakes can be used to promote group member growth (Rubel & Kline, 2008).
Some individuals, because of the force of their personalities, knowledge, or experience, will emerge as informal leaders within the group. Power is given to members who best clarify the needs of the other group members, or who move the group toward goal achievement. They are not always the group members making the most statements.
Emergent informal leaders such as Al are recognized by other group members as being powerful, and their comments are equated with those of the designated leader. Ideally, group leadership is a shared function of all group members, with many opportunities to divide up responsibility for achieving group goals. Exercise 12-6 is designed to help you develop an appreciation of leadership role preferences.
Co-Leadership: Yalom and Leszcz (2005) suggest that co-leadership has advantages and disadvantages. The advantages are that co-leaders can complement and support each other. Co-leaders provide a wider variety of responses, dual points of view that can be helpful to group members, and feedback to each other. When one leader is under fire, it can increase the other’s confidence, knowing that in-group support and an opportunity to process the session afterward is available.
Problems arise when co-leaders have different theoretical orientations or are competitive. Needing to pursue solo interpretations rather than explore or support the meaning of co-leader’s interventions is distracting to the group. Yalom and Leszcz (2005) state, “You are far better off leading a solo group with good supervision than being locked into an incompatible co-therapy relationship” (p. 447).
If you decide to co-lead a group, you need to spend sufficient prep time together before meeting with a therapy group to ensure personal compatibility, and that you have the same understanding of the group purpose. Depending on time availability, it is sometimes advantageous for both group co-leaders to hold pregroup interviews with clients. You will also need to process the group dynamics together, preferably after each meeting.
It is important for co-leaders to work together harmoniously. This requires developing respect for each other’s skills, maintaining authenticity for yourself, and sensitivity to your co-leaders style of communicating (Corey & Corey, 2008).
Applications
Applying group concepts to therapeutic groups
Differences between individual and group communication
Group communication encompasses characteristics of individual communication. Acceptance, respect, understanding, and listening responses found in individual relationships are essential components of effective group communication. Similar therapeutic strategies of using open-ended questions, listening responses, and minimal cues are important in group communication.
There also are key differences. Group communication is more complex than individual communication because each member brings to the group a different set of perspectives, perception of reality, communication style, and personal agenda. Counselman (2008) suggests, “Group demonstrates that there truly are multiple realities” (p. 270). Group themes, rather than individual feelings with situations, form the basis for conversation.
In therapeutic groups, clients are sources of help, as well as recipients. Groups offer a simulated forum for learning. Members not only talk about interpersonal issues; they can practice interpersonal skills with other group members. Disclosures from other group members help individuals recognize the universality of their problems at a personal level (Forsyth, 2009; Yalom & Leszcz, 2005). The leader relates to the group as a whole, instead of with only one person.
Group structure and format
Group purpose and goals dictate group structure, membership, and format. For example, a medication group would have an educational purpose. A group for parents with critically ill children would have a supportive design, whereas a therapy group would have restorative functions. Exploration of personal feelings would be limited and related to the topic under discussion in an education group. In a therapy group, such probing would be encouraged.
Group size
The size of the group depends on its purpose. In general, therapy and personal growth groups consist of six to eight members. Generally, therapy groups should not have fewer than five members. With less than this number, interaction tends to be limited, and if one or more members are absent, the group interaction can become intense and uncomfortable for the remaining members. Powles (2007) argues, “The threesome rarely leads to solid group formation or a productive group work” (p. 107). Support, education, and skills training groups can have from 10 to 30 members.
Group Membership Issues: Groups are categorized as closed or open groups, and as having homogeneous or heterogeneous membership (Corey, 2007). Closed groups have a predefined selected membership with an expectation of regular attendance for an extended time period, usually at least 12 sessions. Group members may be added, but their inclusion depends on a match with group-defined criteria. Most psychotherapy groups fall into this category. Open groups do not have a defined membership. Individuals come and go depending on their needs. One week the group might consist of 2 or 3 members and the next week 15 members. Most community support groups are open groups. Some groups, such as Alcoholics Anonymous, have “open” meetings, which anyone can attend, and “closed” meetings, which only alcoholic members can attend.
Therapeutic groups are composed of a homogeneous or heterogeneous membership. Homogeneous groups share common characteristics, for example, diagnosis (e.g., breast cancer support group) or a personal attribute (e.g., gender or age). Twelve-step programs for alcohol or drug addiction, eating disorder groups, and gender-specific consciousness-raising groups are familiar examples of homogeneous groups.
Heterogeneous groups represent a wider diversity of human experience and problems. Members vary in age, gender, and psychodynamics. Most psychotherapy and insight-oriented personal growth groups have a heterogeneous membership. Educational groups held on inpatient units (e.g., medication groups) may have a homogeneous membership related to diagnosis or specific learning needs.
Group Goals: Group goals define the therapeutic outcome that a group hopes to achieve. Group goals need to be achievable, measurable, and within the capabilities of group membership. Identifying a group goal helps the leader determine the time frame and type of membership needed to achieve the goal. Evidence of goal achievement justifies the existence of the group and increases client satisfaction.
Matching group goals with client needs and characteristics is essential. The leader needs to ask, “How will being in this group enhance a client’s health and well-being?” When there is a good match and the mix of clients has the capacity to contribute to the group (functional similarity), members develop commitment and perceive the group as having value.
Creating a safe group environment
Privacy and freedom from interruptions are key considerations in selecting an appropriate location. A sign on the door indicating the group is in session promotes privacy. Seating should be comfortable and arranged in a circle so that each member has face-to-face contact with all other group members. Being able to see facial expressions and to respond to several individuals at one time is essential to effective group communication.
The number of sessions, times, and frequency of meetings depend on the type of group and group goals. Therapy groups usually meet weekly. Support groups meet at regular intervals, ranging from weekly to monthly. Educational groups meet for a predetermined number of sessions and then disband. Once established, agreed-on times and days should be maintained, except for emergency situations. Meetings should start and end on time.
Most groups, other than educational groups, meet for 60 to 90 minutes on a regular basis with established, agreed-on meeting times. A regular time that does not conflict with a member’s other obligations should be established. Groups that begin and end on time foster trust and predictability. Characteristics of effective and ineffective groups are presented in Table 12-3.
TABLE 12-3
Characteristics of Effective and Ineffective Groups
| Effective Groups | Ineffective Groups |
| Goals are clearly identified and collaboratively developed. | Goals are vague or imposed on the group without discussion. |
| Open, goal-directed communication of feelings and ideas is encouraged. | Communication is guarded; feelings are not always given attention. |
| Power is equally shared and rotates among members, depending on ability and group needs. | Power resides in the leader or is delegated with little regard to member needs. It is not shared. |
| Decision making is flexible and adapted to group needs. | Decision making occurs with little or no consultation. Consensus is expected rather than negotiated based on data. |
| Controversy is viewed as healthy because it builds member involvement and creates stronger solutions. | Controversy and open conflict are not tolerated. |
| There is a healthy balance between task and maintenance role functioning. | There is a one-sided focus on task or maintenance role functions to the exclusion of the complementary function. |
| Individual contributions are acknowledged and respected. Diversity is encouraged. | Individual resources are not used. Conformity, the “company man,” is rewarded. Diversity is not respected. |
| Interpersonal effectiveness, innovation, and problem-solving adequacy are evident. | Problem-solving abilities, morale, and interpersonal effectiveness are low and undervalued. |
Leader tasks applied to group stage development
Pregroup interview has several purposes. This individual interview is used to explain group goals and commitment, and affirm the client’s suitability for the group.
Adequate preparation of group members in pregroup interviews and the early stages of the group life cycle enhances the effectiveness of therapeutic groups (Corey, 2007; Yalom & Leszcz, 2005). Leaders should keep the description of the group and its members short and simple. Ask clients about previous group experiences and concerns. Allow ample time for questions and comments.
Forming stage
The forming stage is an orientation phase. Communication is tentative and structured to allow members to learn about each other and develop trust. The leader takes an active role in helping group members feel accepted during the forming stage. Members are asked to introduce themselves and share a little of their background or their reason for coming to the group. Corey and Corey (2008) state that how well leaders prepare themselves and group members has a direct impact on building the trust needed within the group.
In the first session, the leader identifies the purpose and goals of the group and allows ample time for questions. Although members may know the purpose ahead of time, taking the time to verbalize the purpose allows group members to hear it in the same way. The leader clarifies how the group will be conducted and what the group can expect from the leader and other members in achieving group goals. It is helpful to ask clients in round robin fashion about their personal expectations.
Clients need to be educated about the nature of the group process and the behaviors required to achieve group goals. Successful short-term groups focus on “here and now” interactions, giving practical feedback, sharing personal thoughts and feelings, and listening to each other (Corey & Corey, 2008). Orienting statements may need to be restated in subsequent early sessions if there is a lot of anxiety in the group.
The leader introduces universal behavioral norms such as confidentiality, attendance, and mutual respect (Corey & Corey, 2008). Confidentiality is harder to implement in group formats because members are not held to professional legal standards. However, for the integrity of the group, all members need to commit to confidentiality as a group norm (Lasky & Riva, 2006). Limits to confidentiality related to treatment disclosures to other providers for therapeutic purposes need to be clearly stated and agreed to by all members early in the group.
Storming phase
The storming phase helps group members move to a deeper level. In the storming phase, the gloves come off and communication can become controversial. The leader plays an important facilitative role in the storming phase by accepting differences in member perceptions as being normal and growth producing. By affirming genuine strengths in individual members, leaders model handling conflict with productive outcomes. Linking constructive themes while stating the nature of the disagreement is an effective modeling strategy.
Members who test boundaries through sexually provocative, flattering, or insulting remarks should have limits set promptly. Refer to the work of the group as being of the highest priority, and tactfully ask the person to align remarks with the group purpose. Resolution of the storming stage is evidenced in the willingness of members to take stands on their personal preferences without being defensive, and to compromise.
Norming phase
Once initial conflict is resolved in the storming phase, the group moves into the norming phase. Group-specific norms have developed from discussions in the previous phase. The leader encourages member contributions and emphasizes cooperation in recognizing each person’s talents related to group goals.
During the norming phase, cohesion begins to develop and is carried forward into the remaining stages of group development as a critical variable related to success. Similar to the concept of therapeutic alliance in individual relationships, cohesion is considered the most central therapeutic factor, influencing all others (Bernard et al., 2008). The group itself now becomes the agent of change.
Group Cohesion: Cohesion refers to the value a group holds for its members and their investment in being a part of the group. It describes the emotional bonds among members for each other and underscores their commitment to the group (Yalom & Leszcz, 2005). Evidence of group cohesion occurs when the group demonstrates a sense of common purpose, caring, collaboration in problem solving, a sense of feeling personally valued, and a team spirit (Powles, 2007). Research suggests that cohesive groups experience more personal satisfaction with goal achievement, and that members of such groups are more likely to join other group relationships. See Box 12-2 for communication principles that facilitate cohesiveness. Exercise 12-7 provides experience with understanding the relationship between individual involvement and group cohesion.
Facilitating the performing phase
In the performing stage of group development, members focus on problem solving. Working together and participating in another person’s personal growth allows members to experience one another’s personal strengths and the collective caring of the group. Of all the possibilities that can happen in a group, feeling affirmed and respected is most highly valued by group members (Table 12-4).
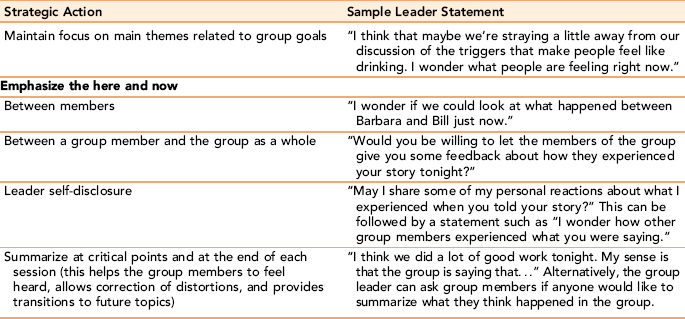
Dissent is expected, but because members function interdependently and respect each other, they are able to work through issues in ways that are acceptable to the individual and the group. Effective group leaders trust group members to develop their own solutions, but call attention to important group dynamics when needed. This can be done with a simple statement such as “I wonder what is going on with her right now” (Rubel & Kline, 2008).
Monopolizing: Despite clear operational roles, the performance stage can get bogged down when one person monopolizes conversation. Monopolizing is a negative form of power communication used to advance a personal agenda without considering the needs of others. When one person monopolizes the conversation, the leader should address the behavior, not an individual’s motivation. For example, the leader might affirm the monopolizer’s contribution and ask for group input: “Has anyone else had a similar experience?” Looking in the direction of positive group members as the statements are made also encourages member response. If a member continues to monopolize, the leader can respectfully acknowledge the person’s comment and refocus the issue within the group directly: “I appreciate your thoughts, but I think it would be important to hear from other people as well. What do you think about this, Jane?”
Completing the adjourning phase
The final phase of group development, termination or adjournment, ideally occurs when the group members have achieved desired outcomes. This phase is about task completion and disengagement. The leader encourages the group members to express their feelings about one another with the stipulation that any concerns the group may have about an individual member or suggestions for future growth should be stated in a constructive way. The leader closes the group with a summary of goal achievement. By being the last person to share closing comments, the leader has an opportunity to soften or clarify previous comments, and to connect cognitive with feeling elements that need to be addressed. The leader needs to remind members that the norm of confidentiality continues after the completion of the group (Mangione, Forti, & Iacuzzi, 2007). Referrals are handled on an individual basis. Exercise 12-8 considers group closure issues.
Types of therapeutic groups
Individuals tend to act in groups as they do in real life. The group provides a mirror with which clients can learn how others perceive them so that they can learn more adaptive responses.
The term therapeutic, as it applies to group relationships, refers to more than treatment of emotional and behavioral disorders. In today’s health care arena, short-term groups are being designed for a wide range of different client populations as a first-line intervention to either remediate problems or prevent them (Corey & Corey, 2008). Therapeutic groups offer a structured format that encourages a person to experience his or her natural healing potential (instillation of hope), and other group members reinforce individual group member’s resolve.
Therapeutic groups provide reality testing. People under stress lose perspective. Other group members can gently challenge cognitive distortions. They rarely accept unsubstantiated comments at face value and can say things to the client that friends and relatives are afraid to say. It is difficult to turn aside the energy and caring of five or six people when member comments are delivered in a caring, but reality-based way.
Therapy groups
Therapy groups are designed to remediate or correct behavioral disorders and issues that limit a person’s potential in personal and work relationships.
Group psychotherapy is a primary form of treatment for inpatient stabilization of mental disorders. In a number of studies, clients ranked group psychotherapy as one of the most valuable components of their treatment (Hoge & McLoughlin, 1991). Psychotherapy groups focus on “here and now group interaction” as the primary vehicle of treatment (Beiling, McCabe, & Antony, 2009). Treatment goals relate to modification of maladaptive interpersonal behaviors and development of constructive coping strategies. Clients are expected to share personal feelings, develop insights about personal behaviors, and practice new and more productive interpersonal responses. When situations cannot be changed, psychotherapy groups help clients accept that reality and move on with their lives by empowering and supporting their efforts to make constructive behavioral changes. A hidden benefit of group therapy is the opportunity to experience giving, as well as receiving help from others. Helping others enhances self-esteem (altruism), especially for people who feel they have little to offer others.
Therapy groups in inpatient settings are designed to stabilize the client’s behavior enough for them to functionally transition back into the community. Therapeutic groups in the community are particularly effective for adolescents as a preventive strategy because peer group interaction is such an intrinsic part of the adolescent’s life (Aronson, 2004).
Leading Groups for Psychotic Clients: Staff nurses are sometimes called on to lead or co-lead unit-based group psychotherapy on inpatient units for chronically ill clients (Clarke, Adamoski, & Joyce, 1998). Other times, staff nurses participate in community group meetings composed mostly of psychotic clients. Although acutely psychotic clients usually cannot participate until they are stabilized, community groups and small, structured therapy groups can be useful.
A directive, but flexible leadership approach is needed. Because the demands of leadership are so intense with psychotic clients, co-leadership is recommended. Co-therapists can share the group process interventions, model healthy behaviors, offset negative transference from group members, and provide useful feedback to each other. Every group session should be processed immediately after its completion.
If a group topic is not forthcoming from members, the leader can introduce a relevant, concrete, problem-centered topic of potential interest to the group. For example, the group might discuss how to handle a simple behavior in a more productive way. Other members can provide feedback, and the group can choose the best solution.
A primary goal in working with psychotic clients is to understand each person as a unique human being. Although their needs are disguised as symptoms, you can help clients “decode” a psychotic message by uncovering the underlying theme and translating it into understandable language. Sometimes other members will translate the message if called on by the nurse leader. The leader might say to the group, “I wonder if anyone in the group can help us understand better what John is trying to say.” Keep in mind how difficult it is for the psychotic client to tolerate close interaction, and how necessary it is interact with others, if the client is to succeed in the outside environment.
Therapeutic groups in long-term settings
Therapeutic groups in long-term settings offer opportunities for socially isolated individuals to engage with others. Common types of groups include reminiscence, reality orientation, resocialization, remotivation, and activity groups.
Reminiscence Groups: Reminiscence groups focus on life review and/or pleasurable memories (Stinson, 2009). They are not designed as insight groups, but rather to provide a supportive, ego-enhancing experience. Each group member is expected to share a few memories about a specific weekly group focus (holiday, first day of school, family photos, songs, favorite foods, pets, etc.). The leader encourages discussion. Depending on the cognitive abilities of members, the leader will need to be more or less directive. Sessions are held on a weekly basis and meet for an hour.
Reality Orientation Groups: Used with confused clients, reality orientation groups help clients maintain contact with the environment and reduce confusion about time, place, and person. Reality orientation groups are usually held each day for 30 minutes. Nurses can use everyday props such as a calendar, a clock, and pictures of the seasons to stimulate interest. The group should not be seen as an isolated activity; what occurs in the group should be reinforced throughout the 24-hour period. For example, on one unit, nurses placed pictures of the residents in earlier times on the doors to their bedrooms.
Resocialization Groups: Resocialization groups are used with confused clients who are too limited to benefit from a remotivation group but still need companionship and involvement with others. Resocialization groups focus on providing a simple social setting for clients to experience basic social skills again, for example, eating a small meal together. Although the senses and cognitive abilities may diminish in the elderly, basic needs for companionship, interpersonal relationships, and a place where one is accepted and understood remain the same throughout the life span. Improvement of social skills contributes to an improved sense of self-esteem.
Remotivation Groups: Remotivation groups are designed to stimulate self-esteem and socialization in a small group environment of acceptance and appreciation. Originally developed by Dorothy Hoskins Smith for use with patients with chronic mental illness, remotivation groups represent an effort to reach the unwounded healthy areas of the patient’s personality. It differs from other forms of therapy because of its exclusive focus on client strengths and abilities rather than on his or her disabilities (Dyer & Stotts, 2005).
Remotivation groups are composed of 10 to 15 members who sit in a circle. They focus on everyday topics, such as the way plants or trees grow, or they might consist of poetry reading or art appreciation. Visual props engage the participant and stimulate more responses. Steps for conducting remotivation groups are presented in Box 12-3.
Therapeutic activity groups
Activity groups offer clients a variety of self-expressive opportunities through creative activity rather than through words. The nurse may function as group leader or as a support to other disciplines in encouraging client participation. Activity groups include the following:
• Occupational therapy groups allow clients to work on individual projects or to participate with others in learning life skills. Examples are cooking, making ceramics, or activities of daily living groups. Tasks are selected for their therapeutic value, as well as for client interest. Life skills groups use a problem-solving approach to interpersonal situations.
• Recreational therapy groups offer opportunities to engage in leisure activities that release energy and provide a social format for learning interpersonal skills. Some people never learned how to build needed leisure activities into their lives.
• Exercise groups allow clients to engage in structured exercise. The nurse models the exercise behaviors, either with or without accompanying music, and encourages clients to participate. This type of group works well with chronically mentally ill clients.
• Art therapy groups encourage clients to reveal feelings through drawing or painting. It is used in different ways. The art can be the focus of discussion. Children and adolescents may engage in a combined group effort to make a mural. Clients are able to reveal feelings through expression of color and abstract forms that they have trouble putting into words.
• Poetry and bibliotherapy groups select readings of interest and invite clients to respond to literary works. Sluder (1990) describes an expressive therapy group for the elderly in which the nurse leader first read free verse poems and then invited the clients to compose group poems around feelings such as love or hate. Clients then wrote free verse poems and read them in the group. In the process of developing their poetry, clients got in touch with their personal creativity.
Self-help and support groups
Self-help and support groups provide emotional and practical support to clients and/or families experiencing chronic illness, crises, or the ill health of a family member. Held in the community, most support groups are led informally by group members rather than professionals, although often a health professional acts as an adviser. A suggested format for leading a support group is presented in Table 12-5.
TABLE 12-5
Sample Introductory Format for Support Group Leaders
| Steps | Examples |
| Introduce self. | “I am Christy Atkins, a staff nurse on the unit, and I am going to be your group facilitator tonight.” |
| Explain purpose of the group. | “Our goal in having the group is to provide a place for family members to get support from each other and to provide practical information to families caring for victims of Alzheimer’s disease.” |
| Identify norms. | “We have three basic rules in this group: (1) We respect one another’s feelings; (2) we don’t preach or tell you how to do something; and (3) the meetings are confidential, meaning that everything of a personal nature stays in this room.” |
| Ask members to identify themselves and have each one tell something about his or her situation. | “I’d like to go around the room and ask each of you to tell us your name and something about your situation.” |
| Link common themes. | “It seems as if feeling powerless and out of control is a common theme tonight. What strategies have you found help you to feel more in control?” |
| Allow time for informal networking (optional). | Providing a 10-minute break with or without refreshments allows members to talk informally with each other. |
| Provide closure. | “Now I’d like to go around the group and ask each of you to identify one thing you will do in the next week for yourself to help you feel more in control.” |
Self-help groups are voluntary groups, led by consumers and designed to provide peer support for individuals and their families struggling with mental health issues (Solomon, 2004). Examples include 12-step groups, On our own for chronic mentally ill clients, bipolar support alliance, and National Alliance on Mental Illness. Self-help groups are often associated with hospitals, clinics, and national health organizations.
Support groups, for example, for Alzheimer’s and related dementias, compassionate friends, and cancer support groups foster creative problem solving and provide community-based opportunities for people with serious health care problems to interact with others experiencing the same kinds of problems. Support groups have an informational function in addition to social support (Percy, Gibbs, Potter, & Boardman, 2009).
Nurses are encouraged to learn about support group networks in their community. Exercise 12-9 offers an opportunity to learn about them.
Educational groups
Community health agencies provide education groups to impart important knowledge about lifestyle changes needed to promote health and well-being and to prevent illness. Family education groups provide families of clients with the knowledge and skills they need to care for their loved ones.
Educational groups are reality-based and related to client needs. They are time-limited group applications (e.g., the group might be held as four 1-hour sessions over a 2-week period or as an 8-week, 2-hour seminar). Examples of primary prevention groups are childbirth education, parenting, stress reduction, and professional support groups for nurses working in critical care settings. Suitable adolescent groups include those that deal with values clarification, health education, and sex education, as well as groups to increase coping skills (e.g., avoiding peer pressure to use drugs).
Medication groups are an excellent example of educational group formats used in hospitals and community clinics. Clients are taught effective ways to carry out a therapeutic medication regimen while learning about their disorder. A typical sequence would be to provide clients with the following information:
• Details about their disorder and how the medication works to reduce symptoms
• Medications, including purpose, dosage, timing, and side effects; what to do when they do not take the medication as prescribed; what to avoid while on the medication (e.g., some medications cause sun sensitivity); and tests needed to monitor the medication
Giving homework, written instructions, and materials to be read between sessions can be helpful if the medication group is to last more than one session. You should allow sufficient time for questions and, by encouraging an open, informal discussion of the topic, engage individual members in the group activity.
Focus groups
Clark et al. (2003) describe a focus group as “a group of people who have personal experience of a topic of interest and who meet to discus their perceptions and perspectives on that topic” (p. 457). Focus groups are used to elicit feedback about important social and health issues as a basis for health policy recommendations. Focus groups allow qualitative researchers to “see the world from the participants’ perspectives” (Heary & Hennessy, 2002, p. 47). It is a very powerful and respected tool. In the process of participating in a focus group, clients learn more about health care issues affecting them, and have the opportunity to reflect on their own perceptions (Laube & Wieland, 1998).
Discussion groups
Functional elements appropriate to discussion groups are found in Table 12-6. Careful preparation, formulation of relevant questions, and use of feedback ensure that personal learning needs are met. Group participation on an equal basis should be a group expectation. Although the level of participation is never quite equal, discussion groups in which only a few members actively participate are disheartening to group members and limited in learning potential. Because the primary purpose of a discussion group is to promote the learning of all group members, other members are charged with the responsibility of encouraging the participation of more silent members. Sometimes, when more verbal participants keep quiet, the more reticent group member begins to speak. Cooperation, not competition, needs to be developed as a conscious group norm in all discussion groups. Discussion group topics often include prepared data and group-generated material, which then is discussed in the group. Before the end of each meeting, the leader or a group member should summarize the major themes developed from the content material.
TABLE 12-6
Elements of Successful Discussion Groups
| Element | Rationale |
| Careful preparation | Thoughtful agenda and assignments establish a direction for the discussion and the expected contribution of each member. |
| Informed participants | Each member should come prepared so that all members are communicating with relatively the same level of information and each is able to contribute equally. |
| Shared leadership | Each member is responsible for contributing to the discussion. |
| Good listening skills | Members concentrate on the material and listen to content; challenge, anticipate, and weigh the evidence; they listen between the lines to emotions about the topic. |
| Relevant questions | Focused questions keep the discussion moving toward the group objectives. |
| Useful feedback | Thoughtful feedback maintains the momentum of the discussion by reflecting different perspectives of topics raised and confirming or questioning others’ views. |
Group principles applied to professional work groups
Multiple group membership is a fact of life in most organizations. Groups found in organizational settings (e.g., standing committees, ad hoc task forces, and quality circles) accomplish a wide range of tasks related to organizational goals.
In work groups, there are two main elements: content and process. Task group content is predetermined by an assignment or charge given to the group. Group process relates to the ways in which group members interact with each other to achieve goals.
Applying group concepts to work groups
Flexibility of leadership style is an essential characteristic of successful work groups. Effective leadership develops from leader characteristics, situational features, and member needs in combination with each other. Different groups require different leadership behaviors. Leadership is contingent on a proper match between a group situation and the leadership style.
Three types of leadership styles found in groups are authoritarian, democratic, and laissez-faire. Leaders demonstrating an authoritarian leadership style take full responsibility for group direction and control group interaction. Authoritarian leadership styles work best when the group needs structure and there is limited time to reach a decision. Democratic leadership involves members in active discussion and decision making. Democratic leaders are goal-directed but flexible. They offer members a functional structure, whereas preserving individual member autonomy, and members feel ownership of solutions. Members of a group with a laissez-faire leader function without significant leader input or structure. They are likely to be less productive or satisfying to group members.
Another way to look at leadership styles in professional group life is by using a situational leadership framework, originally developed by Hershey and Blanchard (Hershey, Fowler, Hawkins, et al., 2005). This format requires group leaders to match their leadership style to the situation and the maturity of the group members. The situational leader varies the amount of direction and support a group needs based on the complexity of the task and the follower’s experience and confidence with achieving task or group goals.
Group maturity involves two forms of maturity: job maturity and psychological maturity related to the work. Job maturity refers to the level of work abilities, skills, and knowledge. Psychological job maturity refers to the followers’ accurate knowledge of personal assets and limitations, feelings of confidence, willingness, and motivation. The capacity and readiness of situational maturity plays a role in the type of preferred leadership style to accomplish goals. A basic assumption is that leadership should be flexible and adapted to group needs. The situational leadership framework describe four leadership styles, matched to employee’s maturity level in a particular work situation and dependent on their need for structure and direction.
• Telling: high structure, low consideration
• Selling: high structure, high consideration
The leader must consistently monitor group member readiness level and must be willing to adapt to changes in the group’s maturity in working together. As the group matures, leaders turn more of the responsibility for the group to its members. Decision making is collaborative. The leader seeks member input, acts as discussion facilitator, and seeks consensus.
Leader and Member Responsibilities: Box 12-4 summarizes guidelines for groups charged with making organizational changes. The group leader takes the following responsibilities:
• Forms the committee structure and establishes the agenda
• Clarifies the group’s tasks and goals (providing background data and material if needed)
• Notifies each member of meeting dates, times, and place
Group members take responsibility for coming prepared to meetings, demonstrating respect for other members’ ideas, and taking an active participatory role in the development of viable solutions. Each member should take responsibility for the overall functioning of the group and the achievement of group goals.
Stage development leader tasks applied to work groups
Before the group starts, participants should have a clear idea of what the group task commitment will entail in terms of time, effort, and knowledge. Group members should have enough in common to engage in meaningful communication, relevant knowledge of the issues and/or expertise needed for resolution, a willingness to make a contribution to the group solution, and the ability to complete the task.
Forming
Even if members are known to each other, it is useful to have each person give a brief introduction that includes his or her reason for being part of the work group. The leader should explain the group’s purpose and structural components (e.g., time, place, and commitment). Member responsibilities should be outlined clearly with time for questions. A task group with vague or poorly understood goals or structure can breed boredom or frustration, and lead to power struggles and inadequate task resolution.
Norming
To be successful, group norms should support accomplishment of stated goals. In general, all data developed within the group context should be kept confidential until officially ready for publication. Otherwise, the “grapevine” can distort information and sabotage group efforts. Members should be accountable for regular attendance. If administrative staff is part of the group membership, they should attend all or designated meetings. Few circumstances are more threatening to a work-related group than having a supervisor enter and exit the task group at will.
Performing
In the performing phase, leader interventions should be consistent and well defined as the group works to fulfill its charge. Most of the group’s work is accomplished, including development of recommendations and preparation of final reports. Suggestions for leader feedback in work groups are presented in Box 12-5. Brainstorming is a commonly used strategy to generate solutions. Exercise 12-10 provides practice in the use of brainstorming. Guidelines for brainstorming include:
• Entertaining all ideas without censure
• Testing the more promising ideas for relevance
• Exploring consequences of each potential solution
• Identifying human and instrumental resources, including availability
Group formats are particularly useful for facilitating changes in organizational life.
Group Think: Although cohesiveness is an essential characteristic of effective work groups, carried to an extreme, it results in group think, defined by Janis (1971, 1982) as a phenomenon that occurs when loyalty and approval by other group members become so important that members are afraid to express conflicting ideas and opinions for fear of being excluded from the group. The group exerts pressure on members to act as one voice in decision making, so that realistic appraisal of issues gets lost. The warning signs of group think are listed in Box 12-6. Group think can create irrational decisions and dissatisfaction with goal achievement. Figure 12-3 displays the characteristics.
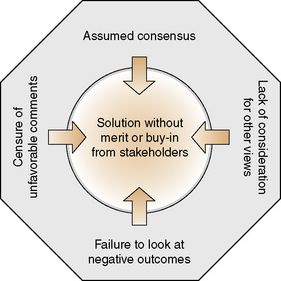
Ways to reduce the potential for group think in work groups include developing norms that make it acceptable to disagree with other group members, and to seek fresh information and outside opinions. Individual members who act as “devil’s advocate” about important issues should be respected and their ideas explored.
Adjourning phase
Termination in work groups takes place when the group task is accomplished. The leader should summarize the work of the group, allow time for processing level of goal achievement, and identify any follow-up. Work groups need to disband once the initial charge is satisfied. They should not simply move on into a never-ending commitment without negotiation and the agreement of participants to continue with another assignment.
Summary
This chapter outlines key concepts associated with group communication and explores how it is used to help clients cope with their health or personal issues more effectively. Differences between individual and group communication are described. Group dynamics include individual member commitment, functional similarity, and leadership style. Group concepts related to group dynamics consist of purpose, norms, cohesiveness, roles, and role functions.
Group processes refer to the structural phases of group development as described by Tuckman (1965, 1977): forming, storming, norming, performing, and adjourning. In the forming phase of group relationships, the basic need is for acceptance. The storming phase focuses on issues of power and control in groups. Behavioral standards are formed in the norming phase that will guide the group toward goal accomplishment, and the group becomes a safe environment in which to work and express feelings. Once this occurs, most of the group’s task is accomplished during the performing phase. Feelings of warmth, caring, and intimacy follow; members feel affirmed and valued. Finally, when the group task is completed to the satisfaction of the individual members, or of the group as a whole, the group enters an adjourning (termination) phase. Different types of groups found in health care include therapeutic, support, educational, and discussion focus groups. Group communication principles can be applied to task groups in work settings and strategies for conducting successful work groups are addressed.
References
Aronson, S. Where the wild things are: the power and challenge of adolescent group work. Mt Sinai J Med. 2004;71(3):174–180.
Beiling, P., McCabe, R., Antony, M., et al. Cognitive-behavioral therapy in groups. New York: Guilford Press, 2009.
Benne, K.D., Sheats, P. Functional roles of group members. J Soc Issues. 1948;4(2):41–49.
Bernard, H., Birlingame, G., Flores, P., et al. Clinical practice guidelines for group psychotherapy. Int J Group Psychother. 2008;58(4):455–542.
Burlingame, G., Strauss, B., Joyce, A., et al. Core battery—revised. New York: American Group Psychotherapy Association, 2006.
Clark, M., Cary, S., Diemert, G., et al. Involving communities in community assessment. Public Health Nurs. 2003;20(6):456–463.
Clarke, D., Adamoski, E., Joyce, B., et al. In-patient group psychotherapy: the role of the staff nurse. J Psychosoc Nurs Ment Health Serv. 1998;36(5):22–26.
Corey, G. Theory and practice of group counseling, ed 7. Pacific Grove, CA: Brooks Cole, 2007.
Corey, M., Corey, G. Groups: process and practice, ed 8. Pacific Grove, CA: Brooks/Cole, 2008.
Counselman, E. Reader’s forum: why study group therapy? Int J Group Psychother. 2008;58(2):265–272.
Dyer J., Stotts M., eds. Handbook of Remotivation Therapy. Binghamton NY: The Haworth Press, Inc, 2005.
Forsyth, D. Group dynamics, ed 5. Belmont, CA: Wadsworth Cengage Learning, 2009.
Gans, J., Alonso, A. Difficult patients: their construction in group therapy. Int J Group Psychother. 1998;48(3):311–326.
Heary, C., Hennessy, E. The use of focus group interviews in pediatric health care research. J Pediatr Psychol. 2002;27(1):47–57.
Hershey, K., Fowler, S., Hawkins, L., et al. Self Leadership and the One Minute Manager. New York: Harper Collins Publishers, 2005.
Hoge, M., McLoughlin, K. Group psychotherapy in acute treatment settings: theory and technique. Hosp Commun Psychiatry. 1991;42(2):153–157.
Janis, I. Groupthink. Psychol Today. 1971;5:43–46. [74–76].
Janis, I. Groupthink: Psychological studies of policy decisions and fiascos, ed 2. Boston: Houghton Mifflin, 1982.
Lasky, G., Riva, M. Confidentiality and privileged communication in group psychotherapy. Int J Group Psychother. 2006;56(4):455–476.
Laube, J., Wieland, V. Nourishing the body through use of process prescriptions in group therapy. Int J Eat Disord. 1998;24(1):1–11.
Mangione, L., Forti, R., Iacuzzi, C., et al. Ethics and endings in group psychotherapy: saying good-bye and saying it well. Int J Group Psychother. 2007;57(1):25–40.
Moreno, K.J. Scapegoating in group psychotherapy. Int J Group Psychother. 2007;57(1):93–104.
Percy, C., Gibbs, T., Potter, L., et al. Nurse-led peer support group: experiences of women with polycystic ovary syndrome. J Adv Nurs. 2009;65(10):2046–2055.
Powles, W. Reader’s forum: reflections on “what is a group?”. Int J Group Psychother. 2007;57(1):105–113.
Rogers, C. The process of the basic encounter group. In: Diedrich R., Dye H.A., eds. Group procedures: purposes, processes and outcomes. Boston: Houghton Mifflin, 1972.
Rubel, D., Kline, W. An exploratory study of expert group leadership. J Specialists Group Work. 2008;3(2):138–160.
Rutan, J.S., Stone, W., Shay, J., et al. Psychodynamic group psychotherapy. New York: The Guilford Press, 2007.
Sluder, H. The write way: using poetry for self-disclosure. J Psychosoc Nurs Ment Health Serv. 1990;28(7):26–28.
Solomon, P. Peer support/peer provided services underlying processes, benefits, and critical ingredients. Psychiatr Rehab J. 2004;27(4):392–401.
Stinson, C. Structured group reminiscence: an intervention for older adults. J Contin Educ Nurs. 2009;40(11):521–528.
Tuckman, B. Developmental sequence in small groups. Psychol Bull. 1965;63:384.
Tuckman, B., Jensen, M. Stages of small-group development revisited. Group Organ Manag. 1977;2(4):419–427.
Yalom, I., Leszcz, M. The theory and practice of group psychotherapy, ed 5. New York: Basic Books, 2005.