Bridges and Barriers in the Therapeutic Relationship
At the end of the chapter, the reader will be able to:
1 Identify concepts that enhance development of therapeutic relationships: caring, empowerment, trust, empathy, mutuality, and confidentiality.
2 Describe nursing actions designed to promote trust, empowerment, empathy, mutuality, and confidentiality.
3 Describe barriers to the development of therapeutic relationships: anxiety, stereotyping, and lack of personal space.
4 Identify nursing actions that can be used to reduce anxiety and respect personal space and confidentiality.
5 Identify research-supported relationships between communication outcomes, such as client empowerment and improvements in self-care.
6 Discuss how findings from research studies can be applied to clinical practice.
This chapter focuses on the components of the nurse-client relationship, showing how nursing communication affects client health outcomes and satisfaction. Health communication is a multidimensional process and includes aspects from both the sender and the receiver of the message. Your communication skills influence outcomes such as anxiety, adherence to treatments, and satisfaction with care. To establish a therapeutic relationship, you need to understand and apply the concepts of respect, caring, empowerment, trust, empathy, and mutuality, as well as confidentiality and veracity (Figure 6-1). Additional bridges fostering the relationship are your ability to put into practice the ethical aspects of respecting the client’s autonomy and treating your client in a just and beneficent manner. Understanding communication barriers in the relationship (e.g., anxiety, stereotyping, or violations of personal space or confidentiality) affects the quality of the relationship. Implementing actions that convey feelings of respect, caring, warmth, acceptance, and understanding to the client is an interpersonal skill that requires practice. Caring for others in a meaningful way improves with experience. Novice students may encounter interpersonal situations that leave them feeling helpless and inadequate. Feelings of sadness, anger, or embarrassment, although overwhelming, are common. Through discussion of these feelings in peer groups and experiential learning practice activities, you gain skill. The self-awareness strategies identified in Chapter 4 and the use of educational groups described in Chapter 12 provide useful guidelines for working through your feelings.
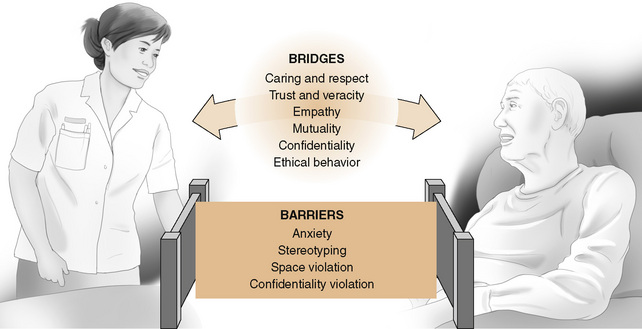
Figure 6-1 Relationships can move in a positive or negative direction. Nursing actions can be bridges or barriers to a good nurse-client interaction.
Basic concepts
Nursing communication is crucial to efficient provision of quality care for your clients (Finke, 2008). Your communication skills affect client outcomes such as satisfaction with care, improved coping, adherence to treatment, adaptation to institutional care, peaceful death, and level of anxiety. Communication also affects us as providers in terms of our job satisfaction and stress levels (Sheldon & Ellington, 2008). The following concepts will help you improve your communication. Barriers to use of each concept are described.
Respect
Conveying genuine respect for your client assists in building a professional relationship with him or her. As your mutual goal is to maximize the client’s health status, you convey respect for his values and opinions. Asking clients what they prefer to be called and always addressing them as such is a correct initial step. Of course, you avoid the sort of casual addresses portrayed in bad television shows, such as “How are you feeling, honey?” “Mom, hold your baby,” or “How are we feeling today?” We try to remember that hospitalized clients feel a loss of control in relation to interpersonal relationships with staff.
Barrier: Lack of Respect: In the Williams and Irurita study (2004), clients felt devalued when they perceived that staff were avoiding talking with them or were unfriendly; they felt comforted when a little “chitchat” was exchanged. Lack of respect among members of the team has also been often cited as a cause of adverse client outcomes. Lack of respect for the nurse by the physician has been cited as a factor leading to communication failures resulting in harm to the client (Sutcliffe, Leewton, & Rosenthal, 2004). Safety issues and communication is discussed in Chapter 22.
Caring
Caring is an intentional human action characterized by commitment and a sufficient level of knowledge and skill to allow you to support the basic integrity of your client. You offer caring to your client by means of the therapeutic relationship. Your ability to care develops from a natural response to help those in need, from the knowledge that caring is a part of nursing ethics, and from respect for self and others. As a caring nurse, you will involve clients in their struggle for health and well-being rather than simply doing things for your clients.
Provision of a caring relationship that facilitates health and healing is identified as an essential feature of contemporary nursing practice in the Social Policy Statement of the American Nurses Association (ANA, 1995). In the professional literature, the focus of the caring relationship is clearly placed on meeting the client’s needs. A formal model is even titled “patient-centered care.” It involves understanding the client’s perceived needs and expectations for health. This is a shift away from the old “I am the provider of treatment for this disease” kind of thinking. The behavior of “caring” is not an emotional feeling. Rather, it is a chosen response to your client’s need. You willingly give of yourself to another through your compassion, concern, and interest. Caring is an ethical responsibility that guides a health care provider to advocate for the client.
Clients want us to understand why they are suffering. We tend to speak in a language in medicine that values facts and events. Clients, in contrast, value associations and causes. To bridge this potential gap, you need to convey a sense that you truly care about your client’s perspective. Caring has a positive influence on health status and healing. Clients can focus on accomplishing the goals of health care instead of worrying about whether care is forthcoming. The nurse gains from the caring relationship by experiencing satisfaction in meeting the client needs.
Families also need to experience a sense of caring from the nurse. Many families do not believe we have a clear understanding of the problems they are encountering while caring for their ill family member. This is especially true if the illness is not easily observable. One French study of effects of proactive communication with families of dying clients found that “caring” interventions in the form of longer conferences where family members could express emotions and talk with ethics and palliative care experts in conjunction with written materials did decrease their anxiety and depression (Lautrette et al., 2007).
Barrier: Lack of Caring: Although nursing has had a long-standing commitment to client-focused care, sometimes you may observe a situation in which you feel a nurse is apathetic, trying to meet her own needs rather than the client’s needs. Some nurses develop a detachment that interferes with expressions of caring behaviors. At other times, a nurse can be so rushed to meet multiple demands that she seems unable to focus on the client. Exercise 6-1 will help you focus on the concept of caring.
Empowerment
Empowerment is assisting the client to take charge of his own life. We use the interpersonal process to provide information, tools, and resources that help our clients build skills to reach their health goals. Empowerment is an important aim in every nurse-client relationship, and is addressed by nursing theories such as Orem’s view of the client as an agent of self-care. Studies demonstrate that the more involved a client is in his own care, the better the health outcome.
At a personal level, empowered clients feel valued, adopt successful coping methods, and think positively. Empowerment has to do with people power: In helping our clients to take control of their lives, we identify and build on their existing strengths.
Barriers: Empowerment is purposeful. It encourages clients to assume responsibility for their own health. This is in direct contrast with the paternalistic attitude formerly found in medicine and characterized by the attitude of “I know what is best for you or I can do it better.” An Australian study showed that lack of information about giving care, managing medicines, or recognizing approaching crises was the major impediment to empowering family members to care for sick relatives (Wilkes, White, & O’Riordan, 2000). Failure to allow our client to assume personal responsibility, or failure to provide him with appropriate resources and support, undermines empowerment.
Trust
Establishing trust is the foundation in all relationships. The development of a sense of interpersonal trust, a sense of feeling safe, is the keystone in the nurse-client relationship. Trust provides a nonthreatening interpersonal climate in which the client feels comfortable revealing his needs. The nurse is perceived as dependable. Establishment of this trust is crucial toward enabling you to make an accurate assessment of your client’s needs.
Trust is also the key to establishing workable relationships. Lack of trust in the workplace has detrimental effects for the organization and coworkers, undermining performance and commitment (Laschinger & Finegan, 2005). According to Erikson (1963), trust is developed by experiencing consistency, sameness, and continuity during care by a familiar caregiver. Trust develops based on past experiences. In the nurse-client relationship, maintaining an open exchange of information contributes to trust. For the client, trust implies a willingness to place oneself in a position of vulnerability, relying on health providers to perform as expected. Honesty is a basic building block in establishing trust. Studies show that clients or their surrogates want “complete honesty” and most prefer complete disclosure (Evans et al., 2009). Box 6-1 lists interpersonal strategies that help promote a trusting relationship.
Barrier: Mistrust: Mistrust has an impact not only on communication but on healing process outcomes. Trust can be replaced with mistrust between nurse and client. Just as some agency managers treat employees as though they are not trustworthy, some nurses treat some clients as though they are misbehaving children. Such would be the case if a client fails to follow the treatment regimen and is labeled with the nursing diagnosis of “noncompliant.” In other examples, the community health nurse who is inconsistent about keeping client appointments or the pediatric nurse who indicates falsely that an injection will not hurt are both jeopardizing client trust. It is hard to maintain trust when one person cannot depend on another. Energy that should be directed toward coping with health problems is rechanneled into assessing the nurse’s commitment and trustworthiness. Having confidence in the nurse’s skills, commitment, and caring allows the client to place full attention on the situation requiring resolution. Clients can also jeopardize the trust a nurse has in them. Sometimes clients “test” a nurse’s trustworthiness by sending the nurse on unnecessary errands or talking endlessly on superficial topics. As long as nurses recognize testing behaviors and set clear limits on their roles and the client’s role, it is possible to develop trust. Exercise 6-2 is designed to help students become more familiar with the concept of trust.
Empathy
Empathy is the ability to be sensitive to and communicate understanding of the client’s feelings. It is a crucial characteristic of a helping relationship. Empathy is an important element of effective communication and is associated with improved client satisfaction and adherence to treatments (Morse et al., 2008). The American Academy of Pediatrics has a policy statement emphasizing the need to communicate empathy to clients and family (Levetown, 2008). An empathetic nurse perceives and understands the client’s emotions accurately. Empathy is the ability to put oneself into the client’s position. Some nurses might term this as compassion, which has been identified by staff nurses as being crucial to the nurse-client relationship. Communication skills are used to convey respect and empathy. Although expert nurses recognize the emotions a client feels, they hold on to their objectivity, maintaining their own separate identities. As a nurse, you should try not to overidentify with or internalize the feelings of the client. If internalization occurs, objectivity is lost, together with the ability to help the client move through his or her feelings. It is important to recognize that the client’s feelings belong to the client, not to you.
Communicate your understanding of the meaning of a client’s feelings by using both verbal and nonverbal communication behaviors. Maintain direct eye contact, use attending open body language, and keep a calm tone of voice. Acknowledge your client’s message about his feelings by restating what you understand him to be conveying. Then, have him validate that this is accurate. If you need more information about his feelings, ask him to expand on his message, perhaps asking, “Are there other things about this that are bothering you?” Now that you have full information, you can directly make interventions to address his needs. Armed with accurate data, you can communicate your client’s feelings to other providers if necessary.
Barrier: Lack of Empathy: Failure to understand the needs of clients may lead you to fail to provide essential client education or to provide needed emotional support. The literature indicates that major barriers to empathy exist in the clinical environment, including lack of time, lack of trust, lack of privacy, or lack of support. Several studies suggest that lack of empathy will affect the quality of care, result in less favorable health outcomes, and lower client satisfaction (Levetown, 2008). However, providers can be taught to express empathy.
Mutuality
Mutuality basically means that the nurse and the client agree on the client’s health problems and the means for resolving them, and that both parties are committed to enhancing the client’s well-being. This is characterized by mutual respect for the autonomy and value system of the other. In developing mutuality, you maximize your client’s involvement in all phases of the nursing process. Mutuality is collaboration in problem solving and “drives” the communication at the initial encounter (Feldman-Stewart & Brundage, 2008). Evidence of mutuality is seen in the development of individualized client goals and nursing actions that meet a client’s unique health needs. Exercise 6-3 gives practice in evaluating mutuality.
Nurses need to respect interpersonal differences. We involve clients in the decision-making process. We accept their decisions even if we do not agree with them. Effective use of values clarification as described in Chapter 3 assists clients in decision making. Clients who clearly identify their own personal values are better able to solve problems effectively. Decisions then have meaning to the client. There is a greater probability he will work to achieve success. When a mutual relationship is terminated, both parties experience a sense of shared accomplishment and satisfaction.
Veracity
As described in Chapters 2 and 3, legal and ethical standards mandate specific nursing behaviors, such as confidentiality, beneficence, and respect for client autonomy. These behaviors are based on professional nursing values that stem from the ethical principles. By adhering to these “rules,” nurses build their therapeutic relationships with individual clients. Veracity contributes to the establishment of a therapeutic relationship. When the client knows he can expect the truth, the development of trust is promoted and helps build the relationship.
Other barriers to the relationship
A few additional barriers that affect the development of the nurse-client relationship include anxiety, stereotyping, and lack of personal space. Barriers inherent in the health care system are also commonly discussed in the professional literature. Under managed care, barriers often reflect cost-containment measures. Such barriers include lack of consistent assignment of nurse to client and increased use of temporary staff such as agency nurses or “floats.” Lack of time can result from low staff/client ratios or early discharge. The primary care literature describes agency demand for minimal appointment time with clients. Primary care providers such as nurse practitioners are often constrained to focus just on the chief complaint to maximize the number of clients seen, leading to “the 15-minute office visit.” Other system barriers include communication conflicts with other health professionals, conflicting values, poor physical arrangements, and lack of value placed on caring by for-profit agencies. These system barriers limit the nurse’s ability to develop substantial rapport with clients. Adequate time is essential to develop therapeutic communication to achieve effective care responsive to client needs. Try Exercise 6-4.
Anxiety: Anxiety is a vague, persistent feeling of impending doom. It is a universal feeling; no one fully escapes it. The impact on the self is always uncomfortable. It occurs when a threat (real or imagined) to one’s self-concept is perceived. Lower satisfaction with communication is associated with increased client anxiety. Anxiety is usually observed through the physical and behavioral manifestations of the attempt to relieve the anxious feelings. Although individuals experiencing anxiety may not know they are anxious, specific behaviors provide clues that anxiety is present Exercise 6-5 identifies behaviors associated with anxiety. Table 6-1 shows how an individual’s sensory perceptions, cognitive abilities, coping skills, and behaviors relate to the intensity and level of anxiety experienced.
TABLE 6-1
Levels of Anxiety with Degree of Sensory Perceptions, Cognitive and Coping Abilities, and Manifest Behaviors
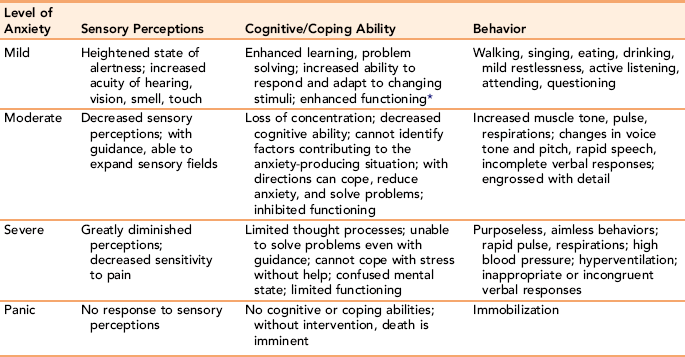
*Functioning refers to the ability to perform activities of daily living for survival purposes.
A mild level of anxiety heightens one’s awareness of the surrounding environment, and fosters learning and decision making. Therefore, it may be desirable to allow a mild degree of anxiety when health teaching is needed or when problem solving is necessary. It is not prudent, however, to prolong even a mild state of anxiety.
Greater levels of anxiety decrease perceptual ability. The anxious state is accompanied by verbal and nonverbal behaviors that inhibit effective individual functioning. For example, anxiety causes you to hold your breath, which can lead to even greater levels of anxiety (Puetz, 2005). Moderate-to-severe anxiety on the part of either nurse or client hinders the development of the therapeutic relationship. To accomplish goals and attain mutuality, greater levels of anxiety must be reduced. Once the presence of anxiety has been identified, the nurse needs to take appropriate action. Strategies to reduce anxiety are listed in Box 6-2.
Severe anxiety requires medical and psychiatric intervention to alleviate the stress. A prolonged panic state is incompatible with life. It is such an extreme level of anxiety that, without immediate medical and psychiatric assistance, suicide or homicide may ensue. Some of these interpersonal strategies used to reduce moderate anxiety also are used during severe anxiety and panic attacks as part of a team approach to client care.
Choosing from various strategies to reduce client anxiety can be difficult. Not all methods are appropriate or work equally well with all clients. If a nurse attempting to build trust pushes a client too fast into revealing what he is not yet ready to discuss, this can increase anxiety. You need to accurately identify your client’s level of anxiety. You should also identify and reduce your own anxiety. Anxiety can cloud your perceptions and interfere with relationships.
Stereotyping and Bias: Stereotyping is the process of attributing characteristics to a group of people as though all persons in the identified group possessed them. People may be stereotyped according to ethnic origin, culture, religion, social class, occupation, age, and other factors. Even health issues can be the stimulus for stereotyping individuals. For example, alcoholism, mental illness, and sexually transmitted diseases are fertile grounds for the development of stereotypes. Stereotypes have been shown to be consistent across cultures and somewhat across generations, although the value placed on a stereotype changes.
Stereotypes are learned during childhood and reinforced by life experiences. They may carry positive or negative connotations. For example, Harding, North, and Perkins (2008) suggest that our culture has stereotyped an image of men as less feeling than women. We all have personal biases, usually based on unconscious past learning. As nurses, we may act on these unknowingly. Stereotypes negate empathy and erode the nurse-client relationship. As nurses, we must work to develop insight into our own expectations and prejudgments about people. Telenurses in Hoglund and Holmstrom’s (2008) study revealed distrust in fathers’ competence to provide care for ill children, an example of stereotyping by nurses. Stewart and Payne’s (2008) study showed that mentally making an intentional resolution to avoid a stereotype enables one to change.
Stereotypes are never completely accurate. No attribute applies to every member of a group. All of us like to think that our way is the correct way, and that everyone else thinks about life experiences just as we do. The reality is that there are many roads in life, and one road is not necessarily any better than another.
Emotions play a role in the value we place on negative stereotypes. Stereotypes based on strong emotions are called prejudices. Highly emotionally charged stereotypes are less amenable to change. In the extreme, this can result in discrimination. Discrimination as a legal statute refers to actions in which a person is denied a legitimate opportunity offered to others because of prejudice. In the United States, federal laws prohibit workplace discrimination based on age, creed, gender, sexual preference, disability, race, religion, or genetics.
Everyone has biases. If nurses bring their biases with them to the clinical situation, they will distort their perception, prevent client change, and disrupt the provider-client relationship. Nurses need to make it a goal to reduce bias. We do this by recognizing a client as a unique individual, both different from and similar to self. Acceptance of the other person needs to be total. This unconditional acceptance, as described by Carl Rogers (1961), is an essential element in the helping relationship. It does not imply agreement or approval; acceptance occurs without judgment. Mr. Fred Rogers, the children’s television show host, ended his programs by telling his audience, “I like you just the way you are.” How wonderful if we, as nurses, could convey this type of acceptance to our clients through our words and actions. Exercise 6-6 examines ways of reducing clinical bias.
Overinvolvement as a Barrier: Objectivity is important if you are to provide competent, professional care. This may be more likely to occur in a long-term relationship. Sharing too much information about yourself, your job problems, or about your other clients can become a barrier if your client becomes unclear about his role in your relationship. Many of us enjoy warm relationships with our clients, but if we are to remain effective, we need to be alert to the disadvantages of overinvolvement.
Violation of Personal Space: Personal space is an invisible boundary around an individual. The emotional personal space boundary provides a sense of comfort and protection. It is defined by past experiences, current circumstances, and our culture.
Proxemics is the study of an individual’s use of space. Optimal territorial space needed by most individuals living in Western culture: 86 to 108 square feet of personal space. Other research has found that 60 square feet is the minimum needed for each client in multiple-occupancy rooms, and 80 square feet is the minimum for private rooms in hospitals and institutions. Critical care units offer even less square footage.
Among the many factors that affect the individual’s need for personal distance are cultural dictates. In some cultures, people approach each other closely, whereas in others, more personal space is required. In most cultures, men need more space than women do. People generally need less space in the morning. The elderly need more control over their space, whereas small children generally like to touch and be touched by others. Although the elderly appreciate human touch, they generally do not like it to be applied indiscriminately. Situational anxiety causes a need for more space. Persons with low self-esteem prefer more space, as well as some control over who enters their space and in what manner. Usually people will tolerate a person standing close to them at their side more readily than directly in front of them. Direct eye contact causes a need for more space. Placing oneself at the same level (e.g., sitting while the client is sitting, or standing at eye level when the client is standing) allows the nurse more access to the client’s personal space because such a stance is perceived as less threatening.
Hospitals are not home. Many nursing care procedures are a direct intrusion into your client’s personal space. Commonly, procedures that require tubes (e.g., nasal gastric intubation, administration of oxygen, catheterization, and intravenous initiation) restrict the mobility of the client and the client’s sense of control over personal territory. When more than one health professional is involved, the impact of the intrusion on the client may be even stronger. In many instances, personal space requirements are an integral part of a person’s self-image. When clients lose control over personal space, they may experience a loss of identity and self-esteem. It’s recommended you maintain a social physical body distance of 4 feet when not actually giving care. Consider the issue of respect for personal space in the clinical examples presented in Box 6-3.
When institutionalized clients are able to incorporate parts of their rooms into their personal space, it increases their self-esteem and helps them to maintain a sense of identity. This feeling of security is evidenced when a client asks, “Close my door, please.” Freedom from worry about personal space allows the client to trust the nurse and fosters a therapeutic relationship. When invasions of personal space are necessary while performing a procedure, you can minimize impact by explaining why a procedure is needed. Conversation with clients at such times reinforces their feelings that they are human beings worthy of respect and not just objects being worked on. Advocating for the client’s personal space needs is an aspect of the nursing role. This is done by communicating your clients preferences to the members of the health team and including them in their care plan.
Home is not quite home when the home health nurse, infusion nurse, or other aides invade the client’s personal space. Some modification of “take-charge” behavior is required when giving care in a client’s home.
Cultural Barriers: Cross-cultural communication is discussed extensively in Chapter 11. Every interaction encounters a basic challenge of communicating between the culture of a client and the medical culture of the health professional (Teal & Street, 2009). Cultural background and level of health literacy may have a powerful influence on communication practices. For example, Gordon and associates (2006) found lower levels of participation in cancer communication by ethnic minority clients. It is important to identify any cultural issues that will influence how your client or their family responds to your type of health communication. In some cultures, the sick role is no longer valid after symptoms disappear, so when your client’s diabetes is under control, he and his family may no longer see the need for special diet or medication (Chang & Kelly, 2007). As we move into a more multicultural society, all health care providers need to work to become culturally competent communicators.
Cultural competence requires us to become aware of the arbitrary nature of our own cultural beliefs. Culturally competent communication is characterized by a willingness to try to understand and respond to your client’s beliefs. Knowledge of the client’s cultural preferences helps you avoid stereotyping and allows you to adapt your communication (Ngo-Metzger, August, Srinivasan, Liao, & Meyskens, 2008; Teal & Street, 2008).
Gender Differences: Gender is defined as the culture’s attributions of masculine or feminine. Recently, more attention has been given to gender role, communication barriers, and health inequalities. In Hoglund and Holmstrom’s (2008) study, phone calls by male clients to female telenurses revealed expressions of disrespect related to the nurse’s gender, as well as her professional advice. Earlier studies seemed to show little communication or outcome difference relevant to the gender of the care provider. But Harding and coauthors’ (2008) more recent study indicated that male nurses’ touching of clients is problematic. This is because although our culture equates female touch with caring, being touched by a male individual is perceived as sexual. Women traditionally were considered to be better communicators, but some studies found no differences. Although results are mixed, it appears that gender need not be a factor in developing therapeutic communication with clients.
Applications
Many nursing actions recommended here are mandated by the American Nurses Association Code of Ethics for Nurses discussed in Chapter 2. The actions specified include confidentiality, autonomy, beneficence, veracity, and justice. Mutuality is addressed in the ANA position statement on human rights. Providers with good communication skills have greater professional satisfaction and experience less job-related stress (Maguire & Pitceathly, 2002; Rask et al., 2009). Studies of client perceptions generally show a correlation between good nurse communicators and good quality of care (Jha, Orav, & Zheng, 2008), although not all do so (Rask et al., 2009). Practice exercises provide you with opportunities to improve your skills. Part of any simulation exercise to strengthen nursing communication is the offering of feedback (Kim, Heerey, & Kols, 2008).
Steps in the caring process
Several articles identify four steps to help you communicate C.A.R.E. to your client:
C = First connect with your client. Offer your attention. Here you introduce your purpose in developing a relationship with your client (i.e., meeting his health needs). Use his formal name, and avoid terms of endearment such as “sweetie.” Show an intent to care. Attentiveness is a part of communication skill training that is probably decreased by work-related stress, time constraints, and so forth.
A = The second step is to appreciate the client’s situation. Although the health care environment is familiar to you, it is a strange and perhaps frightening situation for your client. Acknowledge his point of view and express concern.
R = The third step is to respond to what your client needs. What are his priorities? Expectations for health care?
E = The fourth step is to empower the client to problem-solve with you. Here he gains strength and confidence from interactions with providers enabling him to move toward achievement of goals.

The ability to become a caring professional is influenced by your previous experiences. A person who has received caring is more likely to be able to offer it to others. Caring should not be confused with caretaking. Although caretaking is a part of caring, it may lack the necessary intentional giving of self. Self-awareness about feelings, attitudes, values, and skills is essential for developing an effective, caring relationship.
Strategies for empowerment
Your goal is to assist the client to assume more responsibility for their health conditions by teaching them new roles and skills to manage their illnesses (Sullivan, 2008). We may never fully understand the decisions some clients make, but we support their right to do so. Your method for empowering should include the following key strategies:
• Accept your clients as they are by refraining from any negative judgments.
• Assess their level of understanding, exploring their perceptions and feelings about their conditions and discussing issues that may interfere with self-care.
• Establish mutual goals for client care by forming an alliance, mutually deciding about their care.
• Find out how much information your clients want to know.
• Reinforce the client autonomy, for example, by allowing them to choose the content in your teaching plan.
• Offer information in an environment that enables them to use it.
• Make sure your clients actively participate in their care plan.
• Encourage clients to network with a support group.
• Clarify with your clients that they hold the major responsibility for both the health care decisions they make and their consequences.
Application of empathy to levels of nursing actions
Nursing actions that facilitate empathy can be classified into three major skills: (a) recognition and classification of requests, (b) attending behaviors, and (c) empathetic responses.
Processing requests: Two types of requests are for information and action. These requests do not involve interpersonal concerns and are easier to manage. Another form of request is for understanding involvement, which entails the client’s need for empathetic understanding. This type of request requires greater interpersonal skills. It can be misinterpreted as a request for action or information. The nurse may have to clarify whether the client needs only what he or she specifically asks for, or whether further exploration of the meaning of the need is necessary.
Use attending behaviors: Attending behaviors facilitate empathy and include an attentive, open posture; responding to verbal and nonverbal cues through appropriate gestures and facial expressions; using eye contact; and allowing client self-expression. Verbally acknowledging nonverbal cues shows you are attending. As does offering time and attention, showing interest in the client’s issues, offering helpful information, and clarifying problem areas. These responses encourage clients to participate in their own healing.
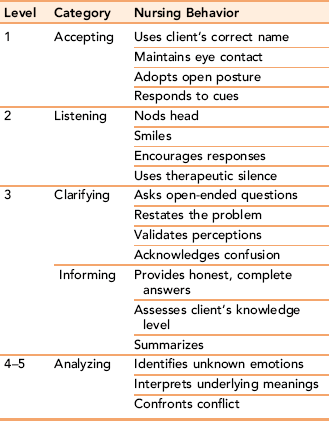
Make empathetic responses: You communicate empathy when you show your client that you understand how he is feeling. This helps him identify emotions that are not readily observable and connect them with the current situation. For example, observing nonverbal client cues such as worried facial expression and verbalizing this reaction with an empathetic comment, such as “I understand that this is very difficult for you,” validates what your client is feeling and tells him you understand him. Using the actions listed in Table 6-2, the nurse applies attending behaviors and nursing actions to express empathy. Verbal prompts such as “Hmm,” “Uh-huh,” “I see,” “Tell me more,” and “Go on” facilitate expression of feelings. The nurse uses open-ended questions to validate perceptions. Using informing behaviors listed in Table 6-2 enlarges the database by providing new information and gives feedback to your client. If your client’s condition prevents use of familiar communication strategies to demonstrate empathy, the nurse can use alternative techniques such as touch (refer to Chapter 17).
Reduction of barriers in nurse-client relationships
Recognition of barriers is the first step in eliminating them, and thus enhancing the therapeutic process. Practice with exercises in this chapter should increase your recognition of possible barriers. Findings from many studies (Evans et al., 2009) emphasize the crucial importance of honesty, cultural sensitivity, and caring, especially in listening actively to suggestions and complaints from client and family. Refer to Box 6-4 for a summary of strategies to reduce barriers to the nurse-client relationship.
Respect for personal space
Before providing care, you need to assess your client’s personal space needs. A comprehensive assessment includes cultural and developmental factors that affect perceptions of space and reactions to intrusions. (Discuss Exercise 6-7.) To increase your client’s sense of personal space, you can decrease close, direct eye contact. Instead, sit beside the client or position the chairs at angles for counseling or health teaching. Clients in intensive care units, where there are many intrusive procedures, benefit from decreased eye contact during certain times, such as when being bathed or during suction, wound care, and changing of dressings. At the same time, it is important for you to talk gently with your client during such procedures and to elicit feedback, if appropriate.
To minimize the loss of a sense of personal space, we should demonstrate regard for our client’s dignity and privacy. Closed doors for private rest and periods of uninterrupted relaxation are respected. Personal belongings are arranged and treated with care, particularly with very old and very young clients, for whom personal items may be highly significant as a link with a more familiar environment. Elderly clients can become profoundly disoriented in unfamiliar environments because their internal sensory skill in processing new information is often reduced. Encouraging persons in long-term facilities to bring pictures, clothing, and favorite mementos is an important nursing intervention with such clients.
Respect for personal space in hospital situations
Obviously, there is a discrepancy between the minimum amount of space an individual needs and the amount of space hospitals are able to provide in multiple-occupancy rooms. Actions to ensure private space and show respect include:
• Providing privacy when disturbing matters are to be discussed
• Explaining procedures before implementing them
• Entering another person’s personal space with warning (e.g., knocking or calling the client’s name) and, preferably, waiting for permission to enter
• Providing an identified space for personal belongings
• Encouraging the inclusion of personal and familiar objects on the client’s nightstand
• Decreasing direct eye contact during hands-on care
• Minimizing bodily exposure during care
• Using only the necessary number of people during any procedure
Violations of confidentiality
Discussing private information casually with others is an abuse of confidentiality. Nursing reports and interdisciplinary team case conferences are examples of acceptable forums for the discussion of privileged communication. This information is not discussed outside what is needed for nursing or medical care; to do so would undermine the basis for your therapeutic relationship with your client. Federal confidentiality regulations are discussed in Chapter 2.
Avoiding cross-cultural dissonance
The ANA’s statement on cultural diversity in nursing practice highlights the importance of recognizing intracultural variation and assessing each client as an individual (ANA, 1991). Becoming culturally sensitive includes avoiding barriers to communication that occur when generalizing about our client’s beliefs based on his membership, rather than taking the time to learn personal preferences. Identify your client’s health values, beliefs, health practices, or family factors that may affect his communication with you (Neuhauser & Kreps, 2008).
Summary
This chapter focuses on essential concepts needed to establish and maintain a therapeutic relationship in nursing practice: caring, empowerment, trust, empathy, mutuality, and confidentiality. Respect for the client as a unique person is a basic component of each concept.
Caring is described as a commitment by the nurse that involves profound respect and concern for the unique humanity of every client and a willingness to confirm the client’s personhood.
Empowerment is assisting the client to take charge of his or her own health.
Trust represents an individual’s emotional reliance on the consistency and continuity of experience. The client perceives the nurse as trustworthy, a safe person with whom to share difficult feelings about health-related needs.
Empathy is the ability to perceive accurately another person’s feelings and to convey their meaning to the client. Nursing behaviors that facilitate the development of empathy are accepting, listening, clarifying and informing, and analyzing. Each of these behaviors implicitly recognizes the client as a unique individual worthy of being listened to and respected.
Mutuality includes as much shared communication and collaboration in problem solving as the client is capable of providing. To foster mutuality within the relationship, nurses need to remain aware of their own feelings, attitudes, and beliefs.
Barriers that affect the development of the nurse-client relationship, such as anxiety, stereotyping, overfamiliarity, or intrusion into personal space, are described. High levels of anxiety decrease perceptual ability. The nurse needs to use anxiety- and stress-reduction strategies when clients demonstrate moderate anxiety levels. Stereotypes are generalizations representing an unsubstantiated belief that all individuals of a particular social group, race, or religion share the same characteristics. No allowance is made for individual differences. Developing a nonjudgmental, neutral attitude toward a client helps the nurse reduce clinical bias in nursing practice. Personal space, defined as an invisible boundary around an individual, is another conceptual variable worthy of attention in the nurse-client relationship. The emotional boundary needed for interpersonal comfort changes with different conditions. It is defined by past experiences and culture. Proxemics is the term given to the study of humans’ use of space. To minimize a decreased sense of personal space, you demonstrate a regard for your client’s dignity and privacy.
References
American Nurses Association. Cultural diversity in nursing practice [position statement]. Washington, DC: Author, 1991.
American Nurses Association Nursing’s social policy statement, Washington, DC, Author, 1995. Available online:, http://nursingworld.org. [Accessed November 2004].
Chang, M., Kelly, A.E. Patient education: addressing cultural diversity and health literacy issues. Urol Nurs. 2007;27(5):411–417.
Erikson, E. Childhood and society, ed 2. New York: Norton, 1963.
Evans, L.R., Boyd, E.A., Malvar, G., et al. Surrogate decision-makers’ perspectives on discussing prognosis in the face of uncertainty. Respiratory & Critical Care Medicine. 2009;179(1):48–53.
Feldman-Stewart, D., Brundage, M.D. A conceptual framework for patient-provider communication: a tool in the PRO research tool box. Quality Life Res. 2008;18:109–114.
Finke, E.H., Light, J., Kitko, L. A systematic review of the effectiveness of nurse communication with patients with complex communication needs with a focus on the use of augmentive and alternative communication. J Clin Nurs. 2008;17(16):2102–2115.
Gordon, H.S., Street, R.L., Sharf, B.F., et al. Racial differences in doctors’ information giving and patients’ participation. Cancer. 2006;107(6):1313–1320.
Harding, T., North, N., Perkins, R. Sexualizing men’s touch: male nurses and the use of intimate touch in clinical practice. Res Theory for Nurs Pract. 2008;22(2):88–102.
Healthy People. Health Communication…, 2010. [Chapter 11], http://web.health.gov/healthypeople/.
Hoglund, A.T. Holmstrom I: ‘It’s easier to talk to a woman’: aspects of gender in Swedishtelenursing. J Clin Nurs. 2008;17:2979–2986.
Jha, A.K., Orav, E.J., Zheng, J., Epstein, A.M. Patients’ perceptions of hospital care in the United States. N Engl J Med. 2008;359(18):1921–1931.
Kim, Y.M., Heerey, M., Kols, A. Factors that enable nurse-patient communication in a family planning context: a positive deviance study. Int J Nurs Stud. 2008;45(10):1411–1421.
Laschinger, H.K., Finegan, J. Using empowerment to build trust and respect in the workplace: a strategy for addressing the nursing shortage. Nurs Econ. 2005;23(1):6–13.
Lautrette, A., Darmon, M., Megarbane, B., et al. A communication strategy and brochure for relatives of patients dying in the ICU. N Engl J Med. 2007;356(5):459–478.
Levetown, M. American Academy of Pediatrics Committee on Bioethics: Communicating with children and families: from everyday interactions to skill in conveying distressing information. Pediatrics. 2008;121(5):e1442–e1460.
Maguire, P., Pitceathly, C. Key communication skills and how to acquire them. Br Med J. 2002;325:697–700.
Morse, D.S., Edwardson, E.A., Gordon, H.S. Missed opportunities for interval empathy in lung cancer communications. Arch Intern Med. 2008;168(17):1853–1858.
Neuhauser, L., Kreps, G.L. Online cancer communication: meeting the literacy, cultural and linguistic needs of diverse audiences. Patient Educ Couns. 2008;71:365–377.
Ngo-Metzger, Q., August, K.J., Srinivasan, M., Liao, S., Meyskens, F.L. End-of-life care: guidelines for patient-centered communication. Am Fam Physician. 2008;77(2):167–174.
Puetz, B.E., The winning job interview. Am J Nurs, 2005;Career Guide 2005 Supp:30–32.
Rask, M.T., Jensen, M.L., Andersen, J., Zachariae, R. Effects of intervention aimed at improving nurse-patient communication in an oncology outpatient clinic. Cancer Nurs. 2009;32(1):E1–E11.
Rogers, C. On becoming a person. Boston: Houghton-Mifflin, 1961.
Sheldon, L.K., Ellington, L. Application of a model of social information processing to nursing theory: how nurses respond to patients. J Adv Nurs. 2008;64(4):388–398.
Stewart, B.D., Payne, B.K. Bringing automatic stereotyping under control: implementation intensions as efficient means of thought control. Pers Soc Psychol Bull. 2008;34(10):1332–1345.
Sullivan, C.F. Cybersupport: empowering asthma caregivers. Pediatr Nurs. 2008;34(3):217–224.
Sutcliffe, K.M., Leewton, E., Rosenthal, M.M. Communication failures: an insidious contributor to medical mishaps. Acad Med. 2004;79(2):186–194.
Teal, C.R., Street, R.L. Critical elements of culturally competent communication in the medical encounter: a review and model. Soc Sci Med. 2009;68(3):533–543.
Wilkes, L., White, K., O’Riordan, L. Empowerment through information. Austrian Journal of Rural Health. 2000;8(1):41–46.
Williams, A.M., Irurita, V.F. Therapeutic and non-therapeutic interpersonal interactions: the patient’s perspective. J Clin Nurs. 2004;13(7):806–815.