Chapter 37 Diseases of the Hematopoietic and Hemolymphatic Systems
DISEASES ASSOCIATED WITH BLOOD LOSS OR HEMOSTATIC DYSFUNCTION
Blood loss may be acute or chronic, and the clinical and laboratory manifestations differ widely because physiologic adaptation occurs in the chronic state.
ACUTE BLOOD LOSS
Common causes for acute blood loss include trauma (e.g., severe lacerations), surgical procedures (e.g., dehorning, castration), and erosion of the carotid artery by guttural pouch mycosis in horses. External hemorrhage is immediately obvious, but hemorrhage into a major body cavity may be occult (e.g., spontaneous rupture of middle uterine artery; splenic rupture resulting from trauma or erosion of major vessel by abscess, aneurysm, or neoplasia). Hemoperitoneum may induce signs of colic, and hemothorax is generally attended by dyspnea. Acute massive blood loss induces hypovolemic shock characterized by tachycardia, tachypnea, cold extremities, pale mucous membranes, muscle weakness, and eventual death resulting from cardiovascular collapse.
Acute blood loss does not initially cause a change in the packed cell volume (PCV) or total plasma protein (TPP), although rapid mobilization of extracellular fluid to maintain circulating blood volume causes the PCV and TPP to decline within 12 to 24 hours. The severity of blood loss may be partially masked by splenic contraction because shock causes activation of the sympathetic nervous system. Icterus is absent, and bone marrow erythroid hyperplasia is delayed by 3 to 4 days. Peripheral signs of erythroid regeneration in horses are limited to mild anisocytosis with a variable increase in mean corpuscular volume. Ruminants show erythrocyte polychromasia, basophilic stippling, Howell-Jolly bodies, and occasionally, nucleated erythrocytes within 4 days of the onset of hemorrhage.
Diagnosis
Diagnosis of acute blood loss is based on clinical signs, evidence of recent hemorrhage, and anemia accompanied by hypoproteinemia. Hemoperitoneum and hemothorax may be suggested by ultrasound and by abdominocentesis and thoracocentesis, respectively.
Treatment
Treatment of acute blood loss should initially be aimed at stopping the hemorrhage. External hemorrhage may be managed by pressure wraps or appropriately placed ligatures; however, it may be inadvisable to attempt to control internal hemorrhage when the patient is a poor risk for general anesthesia and the source of hemorrhage may not be found. Hypovolemic shock should be treated by prompt intravenous (IV) administration of 40 to 80 mL/kg body weight of sodium-containing crystalloid solutions. Studies indicate that a small volume of hypertonic saline (4 to 6 mL/kg of 7.2% sodium chloride) may temporarily reverse the pathophysiologic sequelae of severe hemorrhagic shock.1,2 The total volume of necessary crystalloid solution is usually much greater than the volume of blood lost because crystalloid solutions distribute throughout the extracellular space. The clinical response to fluid administration should be evaluated in light of ongoing losses to determine the necessary replacement volume.
If anemia becomes life threatening, whole-blood transfusion must be considered. A PCV less than 20% in an animal with acute blood loss suggests depletion of erythrocyte reserves, and persistent reduction of the PCV to 12% or less over 24 to 48 hours indicates the need for blood transfusion. A low but stable PCV (12% to 20%) does not necessitate transfusion because transfusion should be reserved for cases in which oxygen delivery to the tissues is inadequate to support life. Blood transfusion can only be viewed as a temporary therapeutic procedure because even crossmatch-compatible, allogeneic erythrocytes are removed from the circulation by the mononuclear phagocyte system within 2 to 4 days of transfusion.3 Horses and cattle display a high degree of blood type polymorphism, and minor antigenic incompatibilities are only delineated by blood typing.4 Serum antibodies against nonhost erythrocyte antigens (erythrocyte alloantibodies) probably mediate the short lifespan of transfused erythrocytes. Compatibility testing is used to avert life-threatening antigen-antibody reactions caused by major blood group mismatching.
The routine crossmatch involves incubating washed erythrocytes from donor (major) and recipient (minor) with serum from the other. Gross and microscopic examination for clumping demonstrates serum agglutinins in horses. Sensitized cattle erythrocytes do not become clumped in saline solution but do lyse in the presence of rabbit complement, so only a hemolytic crossmatch can be performed in this species. Not all equine erythrocyte alloantibodies act as agglutinins, and hemolysins must be detected by adding complement to the reaction mixture. Pooled rabbit serum must first be absorbed with equine erythrocytes to remove naturally occurring antibodies. The need for special handling and storage of rabbit serum makes hemolytic crossmatch procedures impractical for most veterinarians. These tests are best performed by veterinary hematology laboratories (e.g., Veterinary Genetics Laboratory, School of Veterinary Medicine, University of California, Davis), which usually require serum and whole blood in sodium citrate or acid-citrate-dextrose (ACD) to crossmatch.
The first transfusion of whole blood to a horse or ruminant that has not been previously transfused or sensitized by immunization or pregnancy is usually well tolerated because natural alloantibodies are of low concentration and weak activity. After incompatible transfusions, alloantibodies develop rapidly, making subsequent transfusions more hazardous.
Blood for transfusion should be collected aseptically into sterile containers containing sodium citrate (2.5% to 4%) or ACD solution and used immediately. The necessary dosage can only be estimated, but in most cases, replacing 20% to 40% of the calculated blood loss is sufficient to maintain life until the bone marrow can respond. A drop in PCV from 36% to 12% in a 500-kg animal (8% body weight blood) represents a loss of 27 L of blood. In this case, 6 to 8 L of whole blood would be therapeutic and easily donated by another 500-kg individual. Blood warmed to 37° C (98.6° F) should be administered through an in-line filter to remove clots. After pretransfusion vital parameters have been recorded, 0.1 mL blood/kg body weight is given over 5 to 10 minutes and the evaluation repeated. If parameters and attitude are unchanged, the transfusion can be continued at a rate not to exceed 20 mL/kg/hr. The recipient should be continuously monitored so that the transfusion can be stopped if adverse reactions occur, such as tachypnea, dyspnea, restlessness, defecation, tachycardia, piloerection, muscle fasciculations, or sudden collapse. Although these signs may not indicate anaphylaxis, severe reactions should be treated with epinephrine (0.01 to 0.02 mL/kg, 1:1000). Mild signs may respond to a slowed transfusion rate or administration of corticosteroids or flunixin meglumine. Because it is often not possible to delineate the cause of transfusion reactions, the safest approach is to discontinue the blood and administer isotonic crystalloid solutions.
The prognosis is good for most cases of acute blood loss if hypovolemic shock is quickly treated and the bleeding stops. The normal bone marrow begins to replace lost cells within 5 days. Sequential analysis of the PCV will be necessary to determine whether blood loss is controlled. Examples of specific disorders follow.
Hemoperitoneum in Horses
Hemoperitoneum is the accumulation of blood in the abdominal cavity, which can be a life-threatening problem. Causes associated with hemoperitoneum in the horse include trauma, postoperative abdominal hemorrhage, neoplasia, complications from pregnancy and foaling (uteroovarian, middle uterine, and external iliac artery rupture), organ rupture, mesenteric injury, coagulopathies, ovarian hematoma, systemic amyloidosis, and idiopathic causes.5-11 The underlying cause of hemoperitoneum may be identified in the majority of the cases (78%).11 Trauma (mainly of spleen, as well as reproductive tract with associated vessels in mares) and neoplasia are the most common causes of hemoperitoneum.7,11
A recent retrospective study of 67 horses with hemoperitoneum revealed that thoroughbreds and Arabians were overrepresented breeds.11 In addition, middle-aged and older horses (>13 years old) were also overrepresented. Females may be overrepresented.10,11 The most clinical signs include abdominal discomfort, lethargy, hypovolemic shock, pale mucous membranes, prolonged capillary refill time, tachycardia, and tachypnea.10,11 Other clinical signs are anorexia, reluctance to move, weakness, trembling, cool extremities, and abdominal distention.10
Clinicopathologic abnormalities include anemia, neutrophilia, lymphopenia, thrombocytopenia, hypoproteinemia, hypocalcemia, and azotemia.10 Abnormalities in clotting parameters may be observed, depending on the cause. Hemorrhagic abdominal effusion is characterized by high red blood cell (RBC) count (>2.4 million RBCs/μL), PCV (≥18%), and total protein (≥3.2 g/dL), with a normal to high leukocyte count.10 Central venous pressure and blood lactate concentration appear to be early indicators of hypovolemia caused by acute blood loss.12 Swirling fluid and the site of hemorrhage may be evident on abdominal ultrasound.
Primary goals of therapy consist of treating hypovolemic shock, restoring perfusion and oxygen delivery to tissues, correcting fluid deficits, stopping further blood loss, and preventing complications. Blood transfusion should be considered if anemia becomes life threatening. The use of antifibrinolytic and procoagulant agents have been reported in the literature, but controlled studies on its efficacy and safety in the horse with acute blood loss are lacking. Physical activity must be restricted in affected patients.
The short-term outcome is strongly associated with the underlying cause.11 Horses with neoplasia, uterine artery rupture, mesenteric injury, or disseminated intravascular coagulation (DIC) are a greater risk of death. The survival rate has been reported to range from 51% to 74%.10,11 Poor short-term outcome was significantly associated with high respiratory rate in one study.11 Prepartum hemorrhage appears to be associated with a poorer prognosis than postpartum hemorrhage (100% vs. 20% mortality, respectively).11
Hemothorax
Hemothorax may occur secondary to trauma (including lung biopsy), neoplasia, and strenuous exercise13 (see Chapter 31). Hemothorax in neonatal foals may be the result of lacerated lungs and vessels from fractured ribs14 (see Chapter 19).
Exercise-Induced Pulmonary Hemorrhage
Exercise-induced pulmonary hemorrhage (EIPH) has not been associated as a major cause of blood loss. EIPH is associated with high intensity exercise in horses. An estimated 14% to 75% of racehorses examined by endoscopy have EIPH.15 Based on bronchoalveolar lavage analysis, a study suggested that 100% of horses performing strenuous exercise have EIPH.16 EIPH has been reported in various breeds. A recent study reported that the frequency of EIPH is associated with race type, distance, gender, and age. In one study, epistaxis was more common in females, in older horses than in horses less than 2 years old, after steeplechase races than flat races, and with shorter distances (≤1600 m [1 mile] long).17 Recurrence rate in that study was reported to be 4.64%. The pathophysiology of EIPH is not completely known. For a complete description of this disorder, see Chapter 31.
CHRONIC BLOOD LOSS
A number of diseases can result in chronic loss of blood that is insidious until clinical signs of anemia develop. Physiologic adaptation to gradually developing tissue hypoxia generally masks signs of anemia until the PCV is less than 15%. Causes for chronic blood loss include bleeding gastrointestinal (GI) lesions, certain renal diseases, hemostatic dysfunction, bloodsucking external parasites, and haemonchosis (especially in goats and sheep).
Gastrointestinal hemorrhage is usually caused by neoplasia (especially gastric squamous cell carcinoma in horses and abomasal lymphoma in cattle), parasitism, or mucosal ulceration (e.g., abomasal ulcers in cattle, nonsteroidal antiinflammatory drug [NSAID] toxicity in horses). Significant hemorrhage may occur in ruminants heavily infested with Haemonchus contortus shortly after they are treated with an anthelmintic. Generally, GI hemorrhage is best detected by chemical determination of fecal occult blood because melena rarely occurs in horses, and bleeding abomasal ulcers cannot be excluded in cattle when melena is absent. Because of the low specificity of tests for fecal occult blood, the diagnosis of chronic GI blood loss is usually supported by strong clinical suspicion and ruling out other sources of hemorrhage.
Although renal papillary necrosis (caused by NSAID therapy) and urinary calculi cause hematuria, anemia rarely results. Renal neoplasia or congenital renal vascular anomalies rarely may be associated with chronic blood loss anemia. Other causes of blood loss include idiopathic hematuria and idiopathic recurrent hematuria of Arabian horses.
Disorders of hemostasis may cause internal or external hemorrhage that leads to anemia if enough blood is lost. Qualitative or quantitative abnormalities of blood vessels, platelets, or coagulation factors result in hemostatic dysfunction (see next section). Loss of erythrocyte iron secondary to chronic severe blood loss may result in iron deficiency anemia. Hypoferremia or reduced serum ferritin develops with increased total iron-binding capacity and reduction in marrow iron.
The aim in management of chronic blood loss is to determine the primary cause. Treatment of the anemia itself is rarely indicated. Iron deficiency may be alleviated by oral supplementation with ferrous sulfate, although good-quality forages contain more than adequate amounts of iron. Parenteral iron supplementation as iron dextran should be avoided because it has been associated with anaphylactoid reactions in large animals. Examples of specific disorders follow.
Gastric Ulceration
Gastric ulceration in horses is also known as equine gastric ulceration syndrome (EGUS). Although EGUS is not an important cause of blood loss, it has a high prevalence among adult horses. Thoroughbred racehorses have the greatest prevalence (82% to 93%), followed by endurance horses (67%), show horses (58%), hospitalized horses (49%), and geriatric patients with abdominal pain (18%).18-22 Gastric ulcers were found in 66.6% of pregnant and 75.9% of nonpregnant mares in a thoroughbred breeding farm.23 Clinical signs may include poor hair coat, decreased appetite, poor performance, nervous disposition, abdominal pain, teeth grinding, and salivation. Proposed causes of gastric ulceration include exercise, transportation, grazing deprivation, alternating periods of feeding and fasting, diets with high concentrate content, and confinement. For a complete description of gastric ulceration, see Chapter 32.
Right Dorsal Colitis
Right dorsal colitis (RDC) is an enteropathy associated with administration of NSAIDs, most often phenylbutazone.24,25 Other proposed factors that predispose to RDC include infection, immune-mediated response, genetics, and stress. The pathogenesis of RDC is unknown. NSAIDs act by inhibiting cyclooxygenase (more inhibition of constitutively expressed COX-1 than inducible expressed COX-2 during states of inflammation), which will cause inhibition of the production of prostaglandin E resulting in hypoxic or ischemic GI mucosal damage and may delay mucosal healing.25
Ponies and young performance horses appear to be predisposed to RDC. The clinical signs include inappetence, lethargy, intermittent or episodic colic, diarrhea, and weight loss.
Clinicopathologic abnormalities may include mild anemia, moderate to severe hypoproteinemia with hypoalbuminemia, hypocalcemia, and in some cases azotemia. Although mild anemia may be seen in most cases, horses occasionally present with severe anemia and hematochezia. RDC often develops over days or weeks. (See Chapter 32.)
HEMOSTATIC DYSFUNCTION
Basic Physiology of Normal Hemostasis
Understanding the pathogenesis and manifestations of hemostatic disorders is based on knowledge of the normal physiologic mechanism of hemostasis. Hemostasis can be viewed as two interrelated components, coagulation and fibrinolysis (both with their respective inhibitors), which function to stop bleeding from a damaged blood vessel and maintain nutrient blood flow.
Coagulation is mediated by blood vessels, platelets, and blood procoagulant proteins. When a blood vessel is damaged, vasoconstriction occurs, followed by rapid adherence of platelets to subendothelial collagen. Platelet adhesion causes membrane conformational changes that trigger aggregation, contraction, and granule secretion (the basic platelet reaction). Platelet phospholipoprotein (platelet factor 3) provides the necessary surface to catalyze interactions among the activated coagulation proteins that result in thrombin formation. Coagulant proteins are localized to this hemostatic plug because the platelet surface protects them from plasma anticoagulants. Through an incompletely understood mechanism, platelets also prevent spontaneous hemorrhage into the skin and mucous membranes by maintaining “vascular integrity.”
Procoagulant proteins circulate in the blood as precursive forms (zymogens) that must be altered during coagulation to become active. Numerous communications exist between the traditional extrinsic and intrinsic pathways, although initiating mechanisms remain distinct.26 The extrinsic system is initiated when lipoprotein tissue factor (TF) gains access to the bloodstream. TF is widely distributed in most tissues, including endothelial cells and monocytes, and may be increased or secreted in response to numerous pathologic stimuli, such as bacterial endotoxin. Intrinsic coagulation is initiated when blood is exposed to a negatively charged surface such as activated platelets. Because of reciprocal activation between factor XII and prekallikrein, the intrinsic coagulation pathway stimulates formation of numerous inflammatory mediators (e.g., kinins, complement). Both coagulation pathways culminate in the formation of activated factor X (Xa), by which thrombin is generated. In addition to catalyzing the conversion of fibrinogen to fibrin, thrombin promotes platelet aggregation, enhances cofactor activities of factors V and VIII, and activates factor XIII and protein C.27 Mechanisms to localize coagulation to the site of vascular injury are critical to protect against generalized thrombosis.28 Plasma anticoagulant proteins include the serpins, which inhibit activated coagulation factors, and the protein C system, which is directed against cofactors V and VIII.29 Antithrombin III (AT III), the main physiologic inhibitor of thrombin and Xa, normally provides 70% of the anticoagulant activity of plasma. Although not absolutely needed, heparin accelerates AT III action by 2000-fold.30 Activated protein C destroys factors V and VIII, ultimately limiting its own activation, which depends on thrombin and endothelial cofactor, thrombomodulin. Protein S enhances the anticoagulant ability of protein C.
The fibrinolytic system is activated simultaneously with coagulation and functions to prevent tissue ischemia by limiting the extent of fibrin clot formation. Plasmin, primarily responsible for degradation of fibrin, exists in the plasma as the zymogen plasminogen. Plasminogen has a high affinity for fibrin, as does tissue plasminogen activator (tPA); therefore, clots contain the necessary components to allow lysis from within, and systemic plasmin formation is avoided. Alpha-2-antiplasmin (α2-AP), the main physiologic inhibitor of plasmin, competes with the binding of plasminogen to fibrin, and the clot contains equal amounts of both glycoproteins. Because of this molar balance between α2-AP and plasminogen, a normal blood clot does not lyse spontaneously, despite fixation of tPA. Physiologic inhibitors of tPA (PAIs) are found in plasma, platelets, and endothelial cells, and platelet-derived PAI also protects a blood clot against premature lysis. Clot lysis is initiated if additional tPA is taken up from the surrounding tissues; stasis upstream from the occluded vessel is a potent stimulus for release of endothelial tPA. Conversion of plasminogen to plasmin allows partial digestion of fibrin and exposure of additional plasminogen-binding sites. When this additional plasminogen is converted to plasmin, the inhibitory effect of α2-AP is overcome, and clot lysis is accelerated. Plasmin hydrolyzes fibrinogen and fibrin with equal affinity, as well as numerous other procoagulants, and it can activate complement and kininogen. The physiologic actions of plasmin are limited to the fibrin clot by the affinity between the latter and plasminogen and the presence of α2-AP in blood. Because of multiple interactions between the coagulation and fibrinolytic systems, the most important factor that determines the rate of fibrinolysis is the rate of fibrin formation.31
Inherited Coagulation Disorders
Inherited deficiencies of factors VIII,32 IX, XI,33 and prekallikrein34 have been described in horses. Holstein cattle may have inherent factor XI deficiency.35 Congenital factor VIII deficiency (hemophilia A) is sex linked and recessive, occurring only in males. Factor XI deficiency in cattle is transmitted as an autosomal recessive trait.35 The inheritance pattern of the other deficiencies has not been proved.
Clinical signs of clotting factor deficiency reflect the tendency for abnormal hemorrhage from larger vessels (e.g., subcutaneous hematomas; hemarthroses; epistaxis; melena; hematuria; prolonged bleeding after trauma, diagnostic procedures, or surgery). Petechiae are a feature of vascular or platelet disorders and are not caused by clotting factor deficiency. Clinical signs do not always result from inherited clotting factor deficiencies. Cattle deficient for factor XI and horses with prekallikrein deficiency have complete in vivo coagulation competency. Prekallikrein appears to perform an accelerating rather than required role in activation of factor XII.26 Activated factor XII activates factor XI, which then catalyzes the remainder of the clotting sequence. Factor XII is also capable of activating factor VII in the extrinsic pathway,26 which may explain why factor XI deficiency does not cause a hemorrhagic diathesis. Values for the coagulant part of factor VIII (VIII:C) or factor IX must be reduced to less than 5% of normal before spontaneous hemorrhage occurs. Less severe deficiencies may result in excessive hemorrhage only after trauma.
The major differential diagnoses for heritable factor deficiencies include the acquired coagulation factor—deficient states, DIC, warfarin toxicosis (horses), moldy sweet clover toxicosis, and acute hepatic disease. The heritable clotting factor deficiencies involve proteins in the intrinsic pathway; thus a prolonged activated partial thromboplastin time (aPTT) is the only hemostatic abnormality. Acquired coagulation factor deficiencies involve proteins in the extrinsic or common pathways as well, causing a trend toward prolongation of both the prothrombin time (PT) and aPTT. The definitive diagnosis of heritable clotting factor deficiency must be based on specific quantitative assays of intrinsic clotting factors. The only possible treatment for heritable clotting factor deficiency is replacement of clotting factors through the administration of fresh plasma. Specific clotting factor concentrates are not commercially available for large animals, and the rarity of specific factor-deficiency states that produce clinical signs makes the development of these products unlikely. Because of the expense of therapy and the potential for complications, the long-term prognosis for horses with hemophilia A or multiple congenital coagulation factor defects is poor. Cattle with factor XI deficiency apparently live a normal life but may be more susceptible to secondary diseases.35
Thrombasthenia in Horses
GLANZMANN’S THROMBASTHENIA
Glanzmann’s thrombasthenia (GT) is a rare inherited platelet defect caused by quantitative or qualitative change in the platelet glycoprotein complex IIb-IIIa (integrin αIIbβ3). These subunits are encoded by separate genes, and in order to form a stable functional complex on the platelet surface, both subunits must be expressed. This complex was recognized as the receptor that mediated platelet aggregation and was termed the fibrinogen receptor. GT has been documented in humans and dogs.36,37 Clinical signs in these species include purpura, epistaxis, and gingival bleeding. There have been four reports of thrombasthenia in the horse, two of which (4-year-old quarter horse, 7-year-old cross-thoroughbred gelding) were confirmed with various tests, including genetic analysis.38-41 The prominent clinical sign is chronic, intermittent epistaxis unrelated to exercise. Other signs include petechial and ecchymotic hemorrhages in the nasopharynx.
Mild anemia may be observed. Platelet count, activated coagulation time, PTT, PT, thrombin time (TT), fibrin degradation products (FDPs), and plasma concentrations of von Willebrand (vW) factor antigen are normal. However, gingival bleeding time is prolonged (>60 minutes, control horses <2 minutes), clot retraction test is greatly reduced, and platelet aggregation in response to various agonists (as measured by aggregometry) is greatly impaired. Platelet morphology is normal on electron microscopy. Flow cytometric studies using CD41/CD61 monoclonal antibodies have revealed a reduction in the αIIbβ3 integrin on platelet surfaces.40 These findings are the basis for the diagnosis of GT.
Christopherson et al.41 found a single nucleotide change in codon 41 in exon 2 of the gene encoding integrin αIIb in two affected horses. This mutation would encode a proline instead of an arginine, which would result in an aberrant conformation that would prevent association of αIIb with integrin β3 with ultimate lack of expression of the complex on platelet surface. Currently, treatment is not available.
HERITABLE BLEEDING DIATHESIS (OTHER THAN GLANZMANN’S THROMBASTHENIA)
Severe bleeding diathesis was reported in a 2-year-old thoroughbred filly presented for prolonged bleeding time after minor insults.42 The filly’s template bleeding time was longer than 120 minutes, versus 5.5 minutes in control horses.42 Platelet concentration, PT, PTT, antithrombin III, and coagulation factors (vW, VIII, IX, XI, XII) were unremarkable. Platelet-rich plasma (PRP) aggregated normally in response to a range of agonists (adenosine diphosphate, thromboxane A2) but was slightly prolonged in response to thrombin and collagen.43 Several integral platelet membrane glycoproteins involved in aggregation and clotting (e.g., GPIb, GPVI, αIIbβ3) were present in this filly. However, this filly had a reduced prothrombinase activity, production of thrombin, and binding of fibrinogen.43 The mare’s disorder results in decreased platelet aggregation and ineffective clotting. Offspring of the affected mare were also affected.
Acquired Hemostatic Disorders*
Acquired defects of hemostasis may be divided into those involving blood vessels, platelets, and coagulation factors, although some diseases affect more than one component.
VASCULITIS
Vasculitis is a clinicopathologic process that involves inflammation and necrosis of blood vessel walls, regardless of size, location, or cause.44 Vasculitis in large animals is generally a secondary manifestation of a primary infectious, toxic, or neoplastic disorder and has characteristics of hypersensitivity vasculitis in humans. The predominant involvement of small vessels in the skin (e.g., venules, arterioles) is the hallmark of hypersensitivity vasculitis.
The clinical manifestations of vasculitis include demarcated areas of dermal or subcutaneous edema, which may progress to skin infarction, necrosis, and exudation.45 Hyperemia, petechial and ecchymotic hemorrhages, and ulceration of mucous membranes are common. Although the skin and mucous membranes are predominantly involved, hemorrhage and necrosis may occur in any organ system, resulting in conditions such as lameness, colic, dyspnea, and ataxia. Subclinical renal disease may also occur. Vasculitis is often accompanied by adverse sequelae such as cellulitis, thrombophlebitis, laminitis, and pneumonia. Characterized vasculitis syndromes with predominant cutaneous involvement in horses include equine purpura hemorrhagica (EPH), equine viral arteritis (EVA), equine infectious anemia (EIA), and equine granulocytic ehrlichiosis (EGE). In addition, for a number of vasculitis syndromes in horses, the cause, pathogenesis, and clinical course are poorly defined.46,47
Vasculitis is apparently uncommon in ruminants but may accompany certain septicemic diseases, such as malignant catarrhal fever of cattle and bluetongue of sheep.48
Hematologic and serum biochemical findings in vasculitis are determined by the underlying disease, length of illness, organ involvement, and secondary complications. Chronic inflammation may involve neutrophilia, mild anemia, hyperglobulinemia, and hyperfibrinogenemia. Some horses with EPH develop a moderate anemia (PCV, 20% to 25%) thought to be caused by increased erythrocyte destruction.49 The platelet count is generally normal. Muscle damage may be reflected by increased serum concentrations of creatine phosphokinase (CPK) and aspartate aminotransferase (AST). The creatinine may be elevated, and urinalysis may rarely show trace hematuria or proteinuria if there is glomerulonephritis.
The definitive diagnosis of vasculitis is made by demonstration of the characteristic histopathology of involved vessels. Full-thickness punch biopsies (at least 6 mm in diameter) of skin in an affected area should be obtained and preserved in 10% formalin and Michel’s transport medium. Multiple biopsies from different sites may be necessary to reach the diagnosis. The most common inflammatory pattern is neutrophilic infiltration of venules in the dermis and subcutaneous tissue, with nuclear debris in and around involved vessels (leukocytoclasis) and fibrinoid necrosis. Immunofluorescence on biopsies preserved in Michel’s medium may reveal immune complexes. Considerable evidence suggests that most vasculitis syndromes are mediated by immunologic mechanisms, that is, an allergic reaction to a microbe, drug, toxin, or protein.44 In some cases an exogenous stimulus cannot be identified, and an autoimmune pathogenesis is suspected. Immune complex deposition in vessel walls, with subsequent complement activation and chemoattractant production, seems to be the major pathogenic mechanism. Infiltrating neutrophils and macrophages release proteolytic enzymes that cause vessel wall necrosis, with subsequent edema, hemorrhage, and infarction of supplied tissues. Size and physiochemical properties of immune complexes, blood flow turbulence in sites of vessel bifurcation, and hydrostatic forces in dependent areas account for preferential formation of lesions in certain disease states and anatomic locations. Horses and cattle with idiopathic vasculitis may have incomplete response to therapy with an unpredictable, poor prognosis.48,49
Equine Purpura Hemorrhagica (MA, DDM)
EPH is a noncontagious disease of horses characterized by vasculitis leading to extensive edema and hemorrhage of the mucosa and subcutaneous tissue. The disease has been recognized as a sequela to infection or exposure to Streptococcus equi, S. zooepidemicus, Rhodococcus equi, Corynebacterium pseudotuberculosis, and other species and to vaccination against S. equi.45,50
Young to middle-aged horses are usually affected (mean, 8.4 years; range, 6 months to 19 years).50 The clinical signs usually develop acutely within 2 to 4 weeks of a respiratory infection.51 The predominant signs are well demarcated subcutaneous edema of all four limbs, lethargy, anorexia, hemorrhages on mucous membranes, fever, and tachycardia. Other signs include tachypnea, reluctance to move, exudation from the skin, colic, and epistaxis.
The predominant laboratory abnormalities include anemia, neutrophilia, hyperproteinemia, hyperfibrinogenemia, hyperglobulinemia, and elevated muscle enzymes. Thrombocytopenia is rarely detected in horses with EPH.
Skin biopsy shows evidence of acute leukocytoclastic or nonleukocytoclastic vasculitis with necrosis of blood vessels. The lesions consist of marked dermal and subcutaneous hemorrhage, protein-rich edema, and multifocal areas of dermal infarction. Small arteries and capillaries are swollen and infiltrated by degenerate or nondegenerate neutrophils. Hyaline thrombi may be observed.50 Immune complexes primarily composed of IgM or IgA, and streptococcal M protein may be present in capillaries and small blood vessels of horses with EPH, leading to type III hypersensitivity reaction.52 Deposition of complement in immune complexes in vessel walls may result in cell death. Extensive hemorrhages in the dermis, subcutis, skeletal muscles, lungs, kidneys, spleen, intestinal walls, and blood vessels have been observed on postmortem examination.
Horses with infarctive EPH can present with colic, lameness, muscle swelling, and stiffness.53 Extensive GI infarction results in severe colic signs. The significant findings in these horses include leukocytoclastic vasculitis and necrosis of various tissues, neutrophilia with a left shift, hypoalbuminemia, and high serum creatine kinase.53
Treatment is initiated to address the primary cause if identified, reduce the immune and inflammatory response, and provide antimicrobial therapy in cases of active infection, or to prevent infection if indicated, provide supportive care, and prevent complications. Horses with known streptococcal infection should receive penicillin (22,000 IU/kg of procaine penicillin G intramuscularly [IM] twice daily, or potassium penicillin G intravenously [IV] every 6 hours) for at least 2 weeks. Hydrotherapy, limb bandages, and light exercise (hand walk) have been helpful in reducing limb edema. Fluids administered through nasogastric tube or IV may be necessary for animals that become severely lethargic and fail to drink or those that develop dysphagia from laryngeal edema. Stridor and dyspnea may indicate the need for tracheostomy. Prolonged treatment with corticosteroids (2 to 4 weeks) has resulted in favorable outcome and low relapse rate. However, some horses may require more than 4 weeks. Depending on severity of clinical signs, proposed dosage is 0.04 to 0.2 mg/kg of dexamethasone (IV, IM, or orally [PO]) once (morning) or twice daily, or 0.5 to 1.0 mg/kg of prednisolone PO once (morning) or twice daily, with a gradual reduction of the dosage.50 Use of antimicrobials has been suggested throughout corticosteroid therapy to reduce the prevalence of secondary sepsis.45
The outcome will depend on early detection, early aggressive treatment, and extent of organ involvement. Skin sloughing, laminitis, cellulitis, pneumonia, and diarrhea may be seen and may significantly prolong convalescence. Although the prognosis has been thought to be fair with early aggressive therapy and supportive care, a recent retrospective study of 53 horses with EPH reported a mortality rate of 7.5%.50
Equine Viral Arteritis (MA)
EVA is an infectious disease characterized by panvasculitis, edema, hemorrhage, and abortion in pregnant mares. EVA is caused by an enveloped, spherical, positive-stranded RNA virus with a diameter of 50 to 70 nm. Equine arteritis virus (EAV) is a non-arthropod-borne virus classified as a member of the new order Nidovirales within the family Arteriviridae.54 EAV was first isolated from fetal lung collected during an epizootic of abortion in Bucyrus, Ohio.55 Clinical signs may be absent or may develop 1 to 10 days after infection and include pyrexia, lethargy, anorexia, limb edema, stiffness, rhinorrhea, epiphora, conjunctivitis, rhinitis, and abortion. Edema of several regions may be observed, including periorbital, supraorbital, ventral abdomen, mammary gland, scrotum, and limbs.56 Other signs include urticarial rash, abortion, respiratory signs, ataxia, mucosal eruptions, submaxillary lymphadenopathy, and intermandibular and shoulder edema. EAV can present as epidemic abortion, with occasional fatalities in foals and adults. In natural exposure, abortion rate varies from less than 10% to more than 60% and can occur from 3 to 10 months of gestation.57 Infected mares do not become EAV carriers or chronic shedders and do not appear to have fertility problems.
Laboratory abnormalities are variable and not diagnostic for EVA. Experimentally infected mature horses had a consistent leukopenia from neutropenia and lymphopenia.58 After infection, EAV can be localized in macrophages and lymph nodes within 24 and 48 hours, respectively. Various tissues are affected, but blood vessels are the principal target of EAV. Within vessels, EAV localizes in endothelium, medial myocytes, and pericytes. The virus causes vasculitis with fibrinoid necrosis of tunica media, abundant vascular and perivascular lymphocytic and lesser granulocytic infiltration with karyorrhexis, loss of endothelium, and formation of large, fibrinocellular, stratified thrombi.56 Body cavity effusion may be seen.
The virus is mainly transmitted through aerosols from respiratory, urinary, or aborted secretions of acutely infected animals. The other route of transmission is through semen from shedding stallion. The virus remains viable in fresh, chilled, and frozen semen.57 Horizontal transmission by fomites is possible.59 Natural EAV exposure results in long-term immunity to disease. Mares and geldings eliminate virus within 60 days, but 30% to 60% of acutely infected stallions will become persistently infected, temporarily or permanently shedding virus in the semen.56 The virus is maintained in the accessory organs of the male reproductive tract (ampullae, vasa deferentia).57 An outbreak of EVA occurred in the quarter horse population in 2006.60
A fourfold or more increase in serum neutralizing antibodies between acute and convalescent samples (3 weeks apart) is required for diagnosis. Stallions with positive titers of 1:4 should be tested for persistent infection by virus isolation from sperm-rich ejaculate.57 Viral isolation can be attempted from fetal and placental tissues. Semen can be tested for viral shedding by culture, isolation, or polymerase chain reaction (PCR). Identification of carrier stallions is crucial in preventing dissemination of EAV. A modified live vaccine is available.* Vaccination will result in the development of a serum titer that will be detected on EVA testing and cannot be distinguished from active infection. Horses vaccinated for the first time may temporarily shed the modified virus.
ANAPLASMA PHAGOCYTOPHILA INFECTION IN HORSES (MA, JEM)
Definition and Etiology
Equine granulocytic ehrlichiosis (EGE) was first reported in the late 1960s in the foothills of northern California.61 The disease is caused by Anaplasma phagocytophila, formerly known as Ehrlichia equi but reclassified in the Anaplasma genus based on genetic analysis.62 Recently, the agent of human granulocytic ehrlichiosis (HGE)—Ehrlichia phagocytophila—and E. equi have been grouped into a single species and named Anaplasma phagocytophila.62 These organisms are identical based on 16S rRNA gene sequences and have similar morphology, host cell tropism, and indirect fluorescent antibody (IFA) response.63 Furthermore, injection of infected blood from patients with HGE into horses causes EGE.
The organism is found within vacuoles (1.5 to 5 μm in diameter) in the cytoplasm of infected granulocytes, primarily neutrophils and eosinophils. These vacuoles, or inclusion bodies, are pleomorphic and contain one or more coccibacilli or large, granular aggregates called morulae. The organisms are visible under light microscopy as deep-blue to pale-blue gray with Giemsa or Wright-Leishman stains.
Epidemiology
Since the disease was first reported in California,64 cases have been diagnosed in Colorado, Connecticut,65 Florida, Illinois, Minnesota, New Jersey, New York, Oregon, Washington, Wisconsin, Canada, Brazil, northern Europe, and Israel. Equine cases occur during late fall, winter, and spring. There is no apparent gender or age predilection. However, EGE appears to be less severe in younger horses. Persistent, chronic, or latent infections and carrier status have not been demonstrated and are unlikely to occur because the presence of A. phagocytophila is limited to the acute phase. Therefore, it is also unlikely that infected horses could serve as reservoirs. The disease is not contagious but could be readily transmitted through the administration of infected blood. The vectors of granulocytic ehrlichiosis are Ixodes pacificus in California, Ixodes scapularis in the East and Midwest (U.S.), and Ixodes ricinus in Europe.66-69 Potential or proposed reservoirs are white-footed mice, chipmunks, white-tailed deer, dusky-footed wood rats, cervids, lizards, and birds.69
Pathogenesis
The pathogenesis of EGE is unknown. Entry of the organism occurs after inoculation from a biting tick and presumed spread by blood and lymphatics. The organism has cell tropism toward neutrophils and eosinophils, where it replicates within vacuoles, forming characteristic morulae. Presumed cytolysis, induction of inflammation, and cell sequestration, consumption, or destruction result in the observed clinical signs and pancytopenia.70 Cell-mediated and humoral-mediated immune responses develop in affected animals. Antibody titers peak at 19 to 81 days after the onset of clinical signs, and immunity may persist for a long time (2 years).71
Clinical Signs
Signs include reluctance to move, fever ranging from 39.4° to 41.3° C (102.9° to 106.3° F), mild to moderate tachycardia (50 to 60 beats/min), lethargy, decreased appetite, limb edema, petechiation, icterus, weakness, ataxia, and recumbency (reported in one case). Secondary trauma may result from falling in severely ataxic horses. These clinical signs appear to be less profound in younger horses. The presumptive incubation period after natural infection is believed to be less than 14 days. The prepatent period after experimental exposure to infected ticks or inoculation with infected blood is 8 to 12 days and 3 to 10 days, respectively. The disease is self-limiting and nonfatal provided no complications develop. However, affected horses may be predisposed to secondary bacterial, fungal, and viral infections.61 Abortions and laminitis have not been reported in affected horses.
Clinical Pathology
Laboratory alterations include anemia, leukopenia characterized by granulocytopenia and lymphopenia, and thrombocytopenia. Morulae may be observed within the cytoplasm of neutrophils and eosinophils during the acute phase of the infection.
Diagnosis
The definitive diagnosis is based on the presence of characteristic morulae (minimum of three) within the cytoplasm of neutrophils and eosinophils or positive PCR assay for A. phagocytophila in peripheral blood (buffy coat).72 Morulae may be observed in less than 1% of cells in the initial stages of the infection, up to 20% to 50% of the cells few days later. A-fourfold or greater increase in IFA titer of paired samples confirms recent exposure.73
Pathologic Findings
Petechiae and ecchymosis of subcutaneous tissues and edema of the ventral abdomen, limbs, and prepuce are characteristic in infected animals. Proliferative and necrotizing vasculitis, thromboses, and perivascular cuffing in subcutaneous tissue, fascia, kidneys, heart, brain, lungs, ovaries, and testes have been reported.61,70
Treatment, Prognosis, and Prevention
The treatment of choice is IV oxytetracycline, 7 mg/kg once daily for 5 to 7 days. Prompt response to treatment is seen within the first 24 hours. Supportive therapy may be necessary in some cases. The disease can be self-limiting in 2 to 3 weeks if untreated. The prognosis of the disease is excellent provided secondary complications are prevented. At present, prevention is limited to tick control.
THROMBOCYTOPENIA (DDM)
Thrombocytopenia (platelet count <100,000/μL) can result from one or more of three basic mechanisms: (1) decreased or ineffective platelet production, (2) abnormal sequestration (usually in spleen), or (3) shortened platelet survival (consumption or destruction). Thrombocytopenia causes a hemorrhagic diathesis characterized by multiple sites of small-vessel bleeding. Petechial hemorrhages with or without ecchymotic hemorrhages are generally found on the oral, nasal, or vaginal mucous membranes, as well as on the nictitans and sclera. Epistaxis, melena, hyphema, or microscopic hematuria may occur, but spontaneous hemorrhage is unusual unless the platelet count is less than 10,000/μL. Prolonged bleeding from wounds, injections, or surgical procedures and the propensity to form hematomas after minor trauma are common when the platelet count drops below 40,000/μL. The platelet count below which bleeding occurs varies among individuals and seems to be determined by concurrent diseases.
The interaction of blood platelets with a discontinuous vascular surface constitutes the basis for primary hemostasis. In addition, platelets provide the phospholipoprotein surface necessary to catalyze interactions among the activated coagulation proteins that culminate in fibrin formation. The platelet surface also protects activated clotting factors from destruction by plasma anticoagulants, thereby localizing coagulation to the hemostatic plug. Finally, platelets maintain “vascular integrity” through obscure mechanisms and prevent spontaneous hemorrhage into the skin and mucous membranes. Severe thrombocytopenia produces prolonged bleeding time and abnormal clot retraction without affecting clotting times or plasma fibrinogen.
Persistent life-threatening hemorrhage caused by thrombocytopenia may be treated with a transfusion of compatible fresh whole blood or, preferably, PRP, which may be produced by centrifugation thrombocytopheresis74 or by centrifugation of freshly collected blood, 3 to 5 minutes at 250 g.75 Blood or plasma must be used immediately and contact with glass prevented to avoid platelet adhesion and activation. Platelet transfusion is a very transient lifesaving measure, and the ultimate prognosis for thrombocytopenia depends on the cause.
Decreased production of platelets may result from replacement of the normal marrow architecture by neoplastic or inflammatory tissue (myelophthisic disease) or from bone marrow aplasia. Both conditions are characterized by peripheral pancytopenia of variable severity and are extremely unusual in large animals. Myelophthisic disease with thrombocytopenia has been described in horses with various forms of myelogenous neoplasia76-78 and eosinophilic myeloproliferative disorder.79
Hypoplastic anemia with leukopenia and thrombocytopenia has been reported in horses and cattle, as discussed later under Aplastic Anemia. Shortened platelet lifespan is by far the most common cause of thrombocytopenia in large animals. Increased platelet consumption accompanies DIC (discussed in the next section) and rare cases of vasculitis. Immune-mediated mechanisms result in platelet destruction.
Immune-mediated thrombocytopenia (IMTP) may be primary (idiopathic) or secondary to drug administration, infections, neoplasia, or other immunologic disorders.75 This disease is most common in horses and has been reported secondary to EIA,80 lymphoma,81 and autoimmune hemolytic anemia.82 The clinical signs of IMTP include mucosal hemorrhages and the propensity to bleed from small blood vessels. Horses with idiopathic IMTP are usually bright, afebrile, and without overt hemorrhage despite severely reduced platelet numbers. Thrombocytopenia in a horse with obvious primary disease should prompt a thorough hemostatic workup to rule out DIC.
Alloimmune thrombocytopenia of neonates has been recognized as a spontaneous disease of human infants, piglets, foals, and possibly mule foals.83 Clinical signs include depression, loss of suckle, a bleeding tendency, blood loss, and rapidly developing anemia because of a profound thrombocytopenia. The condition occurs in multiparous dams, and immunoglobulins may be found in the mare’s plasma, serum, and milk that bind to the foal’s platelets. Alloimmune thrombocytopenia should be considered in neonates with severe thrombocytopenia when other causes can be excluded, and platelet antibody assays should be used to support this diagnosis. Differential considerations include neonatal sepsis, neonatal maladjustment syndrome, and neonatal isoerythrolysis.
Laboratory findings of IMTP include severe thrombocytopenia (<40,000/μL), prolonged bleeding time, and abnormal clot retraction with normal TT, PT, aPTT, and plasma fibrinogen. FDPs may be mildly increased, and anemia with hypoproteinemia develops if blood loss is ongoing. In most cases of IMTP and other causes of shortened platelet lifespan, megakaryocytic hyperplasia is evident on examination of bone marrow aspirates or biopsies. Megakaryocytic destruction by the immunologic process could induce megakaryocytic hypoplasia, although this is apparently rare in horses.
The definitive diagnosis of IMTP requires demonstration of increased quantities of platelet-associated IgG or C3 or antiplatelet activity in the serum. Unfortunately, methods to detect platelet-associated immunoreactants have not been adapted for horses, although it appears they affect platelet function.84 Therefore the diagnosis of IMTP must be based on small-vessel hemorrhagic diathesis and severe thrombocytopenia in a horse with normal coagulation times and no other evidence of DIC. Response to therapy (see next section) supports the diagnosis. A tentative diagnosis of IMTP in the horse should prompt a thorough search for an underlying disorder, especially lymphoma.
Platelet destruction in IMTP is apparently mediated by antibodies coating the platelet surface that cause premature platelet removal from circulation by the mononuclear phagocyte system (MPS).85 In primary IMTP the platelet-associated immunoglobulin is directed against a membrane antigen, is usually of the IgG class, is produced in the spleen, fixes complement, and can be absorbed from serum by platelets from a normal individual of the same species. Autoantibodies may attach to megakaryocytes, but the latter are not necessarily destroyed because they do not circulate through the spleen or liver. In secondary IMTP the immunoglobulin bound to the platelet surface is part of an immune complex composed of antibody directed against a drug, microbe, or neoplastic antigen that is nonspecifically attached to the platelet Fc receptor. For secondary IMTP to be perpetuated, the foreign antigen must be constantly replenished or difficult to excrete. Drug-induced IMTP generally subsides within a few days of drug discontinuation, although thrombocytopenia secondary to chrysotherapy (gold therapy) may persist for weeks to years. Because gold is occasionally used to treat pemphigus foliaceus in horses, thrombocytopenia should be considered as a potential side effect. The spleen is the major site of platelet phagocytosis because (1) much antiplatelet antibody is secreted locally, (2) more than 30% of circulating platelets are normally stored there, and (3) the stagnant splenic blood flow allows sensitized platelets to pass slowly through a dense network of phagocytic cells. The mean cell life of circulating platelets and the platelet count are inversely proportional to the quantity of platelet-associated IgG.
When any unexplained case of thrombocytopenia is treated, all current medication should be stopped. If a drug is absolutely necessary, it must be replaced by the chemically most-dissimilar substitute. Drug-induced IMTP usually responds within 14 days of drug withdrawal. Most animals with suspected IMTP improve when treated with corticosteroids. Although their precise mechanisms of action are speculative, corticosteroids improve capillary integrity, impair clearance by the MPS, decrease the number and avidity of macrophage Fc receptors, impair antiplatelet antibody production, impede platelet-antibody interactions, and increase thrombocytopoiesis.
Dexamethasone (0.05 to 0.2 mg/kg IV or IM) given once daily generally results in an elevation in the platelet count within 4 to 7 days. Once the platelet count is greater than 100,000/μL, the dose of dexamethasone can be reduced by 10% to 20% daily, while the platelet count is monitored for a relapse. Occasionally, animals with IMTP are refractory to dexamethasone, in which case prednisolone (1 mg/kg IM twice daily) may be tried. Treatment with corticosteroids can usually be discontinued after 10 to 21 days, provided the platelet count has been normal for at least 5 days.
Most horses with IMTP have a favorable prognosis, and the disease resolves within 14 to 21 days. This suggests that many cases may be secondary, although the initiating cause is rarely found. Chronic or recurrent IMTP requiring prolonged corticosteroid therapy has been reported.86 Alternative treatment modalities for IMTP are largely unproved in horses because most cases respond to corticosteroids.87-89
DISORDERS OF COAGULATION FACTORS (DDM)
Normal blood coagulation proceeds in an integrated sequence that can be simplistically viewed as three key reactions: formation of activated factor X, formation of thrombin, and formation of fibrin. Other protein interactions serve to accelerate or inhibit the reaction rate of the coagulation factors.26 Excessive use or inhibition of these proteins produces a relative deficiency that causes hemorrhagic diathesis. Alterations in the coagulation cascade, including thrombocytopenia and procoagulant and anticoagulant effects, can be observed with snakebite (e.g., rattlesnake) envenomation (see Chapter 54).
Disseminated Intravascular Coagulation
The most common form of hemostatic dysfunction in large animals is a syndrome known variously as DIC, consumption coagulopathy, defibrination syndrome, or intravascular coagulation fibrinolysis.90-91 The pathologic process is characterized by widespread fibrin deposition in the microcirculation, with subsequent ischemic damage, and the development of a hemorrhagic diathesis caused by the consumption of procoagulants and hyperactivity of fibrinolysis.26 Never a primary disease entity, DIC represents an intermediary mechanism of underlying disease. In large animals, DIC has been described in association with forms of localized or systemic septic processes,91-94 neoplasia,91 GI disorders,49,95 renal disease,95 and hemolytic anemia.94,96 Diffuse activation of the hemostatic system is particularly prevalent in horses with acute GI disorders that cause colic31,94,95 and is a likely initiating factor for laminitis.97,98 Because of the dynamic nature of DIC, clinical manifestations range from diffuse thrombosis leading to ischemic organ failure to severe hemorrhagic diathesis. The most important determinants are the rate of thrombin generation, which depends on the triggering disease, adequacy of fibrinolysis, and functional state of the MPS, which is largely determined by peripheral circulation. Coagulopathy usually occurs in a compensated form in horses and cattle and is rarely accompanied by overt hemorrhage; however, microvascular thrombosis and subsequent ischemia to vital tissues leads to organ malfunction (e.g., renal failure), which contributes to the morbidity and mortality of the primary disease process.
Renal involvement is common in DIC, which produces ischemic cortical necrosis followed by acute tubular necrosis. Renal disease may be manifested by oliguria, depression, and ileus caused by azotemia and electrolyte imbalances. GI microthrombosis may induce colic as a result of submucosal necrosis and superficial ulceration. Spontaneous GI hemorrhage caused by DIC may cause melena in ruminants and occult fecal blood loss in horses. Rarely, pulmonary function may be compromised by microvascular thrombosis in DIC, causing tachypnea and variable hypoxemia. Altered consciousness, delirium, convulsions, or coma may follow cerebral microvascular thrombosis, although these signs are not common in large animals with DIC. Although reported in both horses99 and cattle,96 microangiopathic hemolysis is rare in large animals with DIC because of their small erythrocyte size.
Digital ischemia frequently accompanies DIC in horses and may play a role in the development of acute laminitis. Laboratory evidence of DIC has been documented during the developmental phase of equine laminitis,98 and digital microvascular thrombosis occurs in horses that develop laminitis with colic or septic conditions.97 The tendency for thrombosis of major peripheral veins is another prominent manifestation of coagulopathy in horses. Venous thrombosis occurs in horses and is associated with needle- or catheter-induced intimal trauma, nonsterility during catheterization, blood sampling or treatment procedures, and thrombogenic catheter materials. However, the strong clinical impression remains that severely ill horses with diseases known to induce coagulopathy have a greater tendency toward venous thrombosis. Spontaneous thrombosis of smaller cutaneous vessels also occurs.
As the thrombotic stimulus continues or intensifies, the tendency for hemorrhage develops because of clotting factors and platelet depletion or generation of excessive fibrinolytic by-products (FDPs). Petechial or ecchymotic hemorrhages on mucosae and sclerae and a tendency to bleed from venipuncture or after minor trauma are the principal signs. Spontaneous life-threatening hemorrhage is very rare; however, trauma or surgery may induce uncontrollable hemorrhage. Once signs of blood incoagulability develop, the prognosis is poor.
Horses may develop a chronic, compensated form of DIC with few or no clinical signs. This entity develops in patients with illnesses that produce a low-grade or intermittent procoagulant stimulus that allows used coagulant proteins and platelets to be partially or totally replenished and activated clotting factors and FDPs to be cleared by the MPS. Localized sepsis (e.g., pleuritis), neoplasia, protein-losing enteropathy, and immune-mediated disorders (vasculitis, anemia) are common initiating diseases. This compensated state may become imbalanced by stress, concurrent diseases, or worsening of the primary process, resulting in clinically obvious DIC. Diseases that must be differentiated from DIC include IMTP, warfarin toxicosis (horses), moldy sweet clover toxicosis, and inherited coagulation abnormalities.
Numerous laboratory tests of hemostasis may be abnormal during DIC; however, no one test consistently or specifically provides a definitive diagnosis. Lack of test sensitivity results from the dynamic nature of DIC; laboratory findings are determined by the balance between coagulation and fibrinolytic forces, as well as MPS integrity at blood sampling.
The most widely used hemostatic function tests in large animals include the platelet count, plasma fibrinogen, PT, aPTT, and serum FDPs. Because clinical manifestations of DIC vary widely, clarification of the most frequent laboratory abnormalities in large animals with DIC is hindered by lack of a definitive diagnosis in most cases. A disseminated coagulopathy is manifested by multiple hemostatic abnormalities, and serial analyses should reveal reduced platelet numbers and a trend toward prolongation of the PT, aPTT, and TT. Repeated hemostatic testing is advised when there is strong suspicion for DIC. Serum FDPs are most often elevated by DIC, but they are usually normal in the early or compensated form of the disease. Hypofibrinogenemia is an uncommon manifestation of DIC in large animals and, when present, should strongly suggest concomitant liver dysfunction. Hemostatic function tests are totally unreliable unless blood samples are collected and handled properly.
Criteria used for diagnosis of DIC are extremely arbitrary, and laboratory results must be interpreted in light of the patient’s underlying disease. The combination of thrombocytopenia with mild to moderate prolongation of the PT or aPTT strongly suggests DIC. The clinician should seek laboratory assistance when considering the diagnosis of DIC but should appreciate that the findings are often not helpful. Clinical signs and specific situations suggest the possibility of DIC, and laboratory tests are only used to provide support.
Diseases initiate DIC by two major mechanisms: (1) generation of excessive procoagulant activity within the blood and (2) contact of blood with abnormal surfaces. Many diseases act by more than one mechanism to induce the overwhelming stimulus needed to trigger DIC. The nature and intensity of the procoagulant force (which determines the rate of thrombin formation), the concentration of natural coagulation inhibitors, and the functional capacity of the MPS determine (1) whether an individual with a given disease process develops DIC and (2) the clinical manifestations of DIC. Many diseases that produce DIC have the propensity to cause endotoxemia. The intestinal tract in large animals normally contains large quantities of endotoxins, only a small part of which is absorbed through the portal vein and removed by the liver. Conditions that cause intestinal mucosal edema or disruption allow endotoxins to gain access to the peripheral circulation and initiate many morbid sequelae, one of which is DIC. Intestinal strangulating obstruction, thromboembolic infarction, and severe colitis induce mucosal abnormalities, allowing endotoxemia to occur. The proliferation of gram-negative bacteria within tissues and the blood is also accompanied by endotoxemia.
Gram-negative endotoxins are capable of direct factor XII activation. However, most studies indicate that the procoagulant effects of endotoxin are primarily mediated by cytokine production by mononuclear phagocytes.27,100 After endotoxin stimulation, phagocytes produce a platelet-activating factor (PAF), tissue factor, prostaglandins, interleukins, tumor necrosis factor (TNF), and other mediators with procoagulant activity.27,101
The net result of any triggering mechanism for DIC is the exaggerated generation of systemic thrombin, which causes widespread microcirculatory thrombosis. In addition to the cleavage of fibrinogen to produce fibrin monomers, thrombin activates factor XIII to render fibrin more resistant to fibrinolysis, enhances the cofactor activity of factors V and VIII, and induces platelet aggregation and exposure of platelet phospholipid. Circulatory obstruction produces organ hypoperfusion, leading to ischemic necrosis.
The counterbalance fibrinolytic system is also activated by DIC and plasmin contributes to factor consumption by destroying factors V, VIII, XIIa, IX, and XI, in addition to fibrin and fibrinogen. FDPs contribute greatly to the hemorrhagic manifestations of DIC because they have antithrombin activity, interfere with fibrin monomer polymerization, and cause platelet dysfunction.28 Paradoxically, the combination of consumption and anticoagulation predisposes to hemorrhage at the same time that disseminated thromboses occur.
The MPS plays a vital role in the pathogenesis of DIC. The tissue-fixed macrophages of the spleen and liver normally remove FDPs and activated clotting factors from the peripheral circulation, and FDPs only increase when their rate of formation exceeds the ability of the MPS to clear them. Shock and hypoperfusion of the liver and spleen or diseases associated with excessive tissue debris that must be removed by the MPS (e.g., sepsis, metastatic neoplasia) reduce the function of the MPS and predispose to or perpetuate DIC.
Therapy for DIC is highly controversial, and the only noncontended modalities are those directed toward identification and treatment of the primary disorder, along with general supportive measures to combat shock and maintain tissue perfusion.26,88,102,103 Intravenous fluid administration helps to prevent organ dysfunction after microvascular thrombosis and can correct existing acid-base or electrolyte imbalances. Septic conditions should be treated with appropriate antimicrobial agents, and necrotic tissue or purulent exudate removed whenever possible (e.g., immediate surgical intervention to resect nonviable bowel). Flunixin meglumine mitigates the deleterious effects of endotoxin caused by eicosanoids and is used in horses at 0.25 mg/kg IV every 8 hours.49 Corticosteroids may worsen DIC because they reduce the phagocytic action of the MPS and potentiate the vasoconstrictor effects of catecholamines.
Significant life-threatening hemorrhage is rare in large animals with DIC; however, if it occurs, fresh plasma should be administered (15 to 30 mL/kg) to replace used coagulant and anticoagulant proteins. The use of heparin in DIC has been recommended in various regimens to stall the disseminated microvascular thrombosis that precipitates organ failure; however, its efficacy is still controversial.88,103 In dogs, minidose heparin therapy (5 to 10 U/kg subcutaneously [SC] three times daily) is often used with blood products in treatment of DIC.88,102 Efficacy of heparin for DIC in horses is unproven. Heparin in all species can predispose to hemorrhage, thrombosis, and thrombocytopenia104 and causes anemia and erythrocyte agglutination in horses.105 If considering heparin therapy, the clinician must ensure there is adequate plasma AT III, which is necessary for heparin action. Because AT III is often depleted by DIC, plasma may be necessary. Clinical trials in humans have not indicated therapeutic benefit of anticoagulants in chronic DIC.
The prognosis for DIC in large animals depends largely on the nature and severity of the underlying disease and how effectively the latter is treated. Once DIC has progressed to the stage at which signs of blood incoagulability predominate, the prognosis generally is extremely poor.
Warfarin Toxicosis
Horses may develop a hemorrhagic diathesis caused by warfarin toxicosis.106 Some use this coumarin-derivative anticoagulant to treat horses with navicular disease.107 Rarely, horses and other animals may be exposed to coumarins used as rodenticides in grains or other feedstuffs. Therapeutic concentrations of warfarin can have a cumulative toxic effect if the diet is altered to contain less vitamin K or if there is concurrent protein-bound drug therapy. The clinical signs of warfarin toxicosis include hematomas, ecchymoses of mucous membranes, epistaxis, and hematuria. The earliest laboratory indication of warfarin toxicosis is a prolongation of PT because the plasma half-life of factor VII is shorter than the other clotting factors.108 As the disease progresses, the aPTT becomes prolonged, and the animal may develop blood-loss anemia and hypoproteinemia. The diagnosis of warfarin toxicosis is based on a history of exposure, clinical signs of large-vessel hemorrhagic diathesis, and prolonged PT with or without aPTT and with no other abnormalities of the clotting profile.
Warfarin acts through competitive inhibition of vitamin K, which is necessary for liver production of clotting factors II, VII, IX, and X.107 Factor activity is reduced in the blood at a rate that depends on its individual half-life. In most species, factors VII, IX, X, and XI have increasingly greater half-lives, accounting for the greater sensitivity of PT for the early diagnosis of warfarin toxicosis. After GI absorption, warfarin is highly bound to plasma proteins. Drugs that are normally protein bound (e.g., phenylbutazone, chloral hydrate) can enhance the toxicity of warfarin by allowing a greater proportion of the administered drug to be unbound and active.109 In the same manner, hypoalbuminemia may increase the likelihood of warfarin toxicosis. Corticosteroids and thyroxin can lower the necessary therapeutic dose of warfarin by increasing both the receptor affinity and the clotting factor catabolism. Drugs that induce hepatic microsomal enzyme activity (e.g., barbiturates, rifampin, chloramphenicol) can accelerate warfarin metabolism and reduce therapeutic response to a given dose. Finally, any reduction in hepatic function or content of vitamin K in the diet can precipitate warfarin toxicosis.
Treatment of warfarin toxicosis depends on clinical signs. Warfarin therapy should be stopped if PT exceeds twice the pretherapeutic value. Vitamin K1 (0.5 to 1 mg/kg SC) must be given every 6 hours until PT is again normal and stable. Significant hemorrhage can be controlled by the administration of fresh plasma to provide necessary clotting factors. If the anemia is life threatening, whole-blood transfusion should be considered. Although warfarin is eliminated rapidly, some potentiated coumarins have a prolonged half-life, requiring a longer course of vitamin K therapy. The prognosis for warfarin toxicosis is good with early diagnosis and prompt administration of vitamin K. It is imperative that vitamin K3 not be used because it has poor therapeutic action and is highly nephrotoxic for horses.110
Prevention of warfarin toxicosis is based on limiting access of livestock to rodenticides and carefully monitoring the therapeutic use of warfarin in horses. The benefits of warfarin in horses are highly controversial, and many question whether advantages outweigh the risks.
Sweet Clover Toxicosis
Sweet clover (Melilotus species) toxicosis is caused by the ingestion of moldy sweet clover hay or silage containing dicoumarol. Natural coumarins in sweet clover can be converted to dicoumarol when hay or silage is improperly cured and mold forms. The toxin persists in moldy hay or silage and is palatable. This disease can occur in all species but is most often seen in cattle fed sweet clover hay in the northern plains states. Early signs include epistaxis and melena, with the development of subcutaneous hematomas and periarticular swellings as the disease progresses. Visible swellings occur at points of trauma (e.g., brisket, tuber coxae, carpi) and are not hot or painful, although they may cause stiffness and disinclination to move. Accidental and surgical wounds cause severe hemorrhage and may precipitate fatal blood-loss anemia.
Clinical pathology in sweet clover toxicosis is similar to that described for warfarin toxicosis, with prolonged PT being the earliest abnormality (detected before clinical evidence of hemorrhage). The platelet count remains normal, which differentiates this syndrome from DIC and bracken fern toxicosis. Other diagnostic rule-outs include mycotoxicosis, and toxicosis from trichloroethylene-extracted soybean meal.48 In the absence of fever and anorexia, coagulopathy should make moldy sweet clover toxicosis a strong tentative diagnosis in animals with a history of access. Chemical analysis for dicoumarol in suspected feed or in the blood and liver of affected animals aids in the diagnosis111; however, the disease cannot be excluded if dicoumarol is not detected.
The pathogenesis of moldy sweet clover toxicosis is identical to that of warfarin toxicosis. Dicoumarol interferes with hepatic synthesis of clotting factors II, VII, IX, and X by inhibiting vitamin K. Usually the syndrome appears in cattle 2 to 7 days after they ingest the moldy hay. Lower levels of dicoumarol (<70 mg/kg) in feed may prolong the onset of signs for up to 3 months.48
The succulent nature of sweet clover creates a high incidence of molding in hay. Grazing the crop is not dangerous. Because of its high forage yield, sweet clover is usually harvested as silage, which should carry less danger of molding when properly cured. The toxic level of dicoumarol in sweet clover feed samples is 10 mg/kg of feed.111
Treatment of sweet clover toxicosis involves discontinuing the use of contaminated feed and administering vitamin K1.109 Dosages between 1.1 and 3.3 mg/kg should be administered IM; response occurs within 24 hours. Animals with severe blood-loss anemia or ongoing hemorrhage should be treated with plasma or whole fresh blood. Sweet clover toxicosis can be prevented by careful forage preparation, followed by the inspection of hay and silage before feeding. When the disease is suspected, questionable feed should be removed from the diet.
DISEASES ASSOCIATED WITH INCREASED ERYTHROCYTE DESTRUCTION (HEMOLYTIC ANEMIA)
Hemolytic disorders are characterized by an increased rate of red blood cell (RBC, erythrocyte) destruction. Anemia occurs when the rate of RBC destruction exceeds the bone marrow capacity for increased proliferative response. Although intravascular hemolysis occurs in some circumstances, these anemias are primarily caused by an increased rate of extravascular erythrocyte destruction and shortened intravascular lifespan.
Hemolytic anemias are associated with a wide range of systemic disease processes. The mechanisms responsible for the enhanced RBC destruction also vary greatly. Box 37-1 lists differential considerations of possible causal factors for hemolytic anemia in large animals. Clinical manifestations of hemolytic anemia vary with the degree of anemia, rate of RBC destruction, and primary or underlying disease process. Regardless of the cause, however, several common clinical signs are seen in animals with a severe hemolytic anemia, including pallor of the mucous membranes, fatigue, depression, and anorexia. Clinical icterus can be quite variable, depending on the rate of RBC destruction and the ability of the liver to excrete bilirubin. Icterus is a characteristic feature in hemolytic anemia, but intense icterus is noted only after massive RBC destruction and often is transient. With continued low-level hemolytic processes, the liver may be able to excrete bilirubin at a rate sufficient to avoid clinical icterus. Hemolytic icterus must be differentiated from other potential causes, such as liver disease or anorexia, in horses. If icterus is caused by hemolytic processes, clear clinical and hematologic evidence of anemia should exist. Massive intravascular hemolysis may result in an orange to reddish discoloration of the mucous membranes. Modest to marked and often variable febrile responses are frequently encountered in hemolytic anemias caused by infectious agents and during periods of active erythrocyte destruction. With advanced anemia the pulse and respiratory rates are elevated at rest. Death losses may occur, and neurologic abnormalities ranging from bizarre behavior to mania, collapse, and death may be associated with handling animals with a severe anemia.
The hematologic manifestations of hemolytic anemia also vary with the rate of RBC destruction, time course of the anemia, and primary or underlying disease process. The anemia may be modest to severe; after the first few days in all species except the horse, there is usually hematologic evidence of enhanced erythropoietic response, manifested by increased anisocytosis, polychromasia, reticulocytosis, and the presence of nucleated RBCs in the circulation. Morphologic abnormalities of diagnostic significance (e.g., intracellular/epicellular parasites, granulocytic inclusion bodies, Heinz bodies, spherocytes, schistocytes, poikilocytes) may be noted on examination of stained blood smears. Responsive anemias often are accompanied by a neutrophilia and regenerative left shift. The bone marrow usually shows an active erythropoietic response with a decreased myeloid/erythroid (M/E) ratio. The serum concentration of haptoglobin is decreased, and serum lactate dehydrogenase (LDH) enzyme activity may be elevated during acute hemolytic episodes. An increase in serum bilirubin concentration, caused primarily by an increase in indirect reacting bilirubin, is a reflection of active RBC destruction.
Specific serologic diagnostic procedures are available for many of the infectious causes of hemolytic anemia. Immunohematologic procedures such as the direct and indirect Coombs’ test show that immune-mediated processes contribute to enhanced erythrocyte destruction. The principal mechanisms responsible for increased rate of RBC destruction associated with many of the infectious causes of hemolytic anemia (parasitic, bacterial, viral) are immunologically mediated, and affected animals may be transiently Coombs’ positive.
INFECTIOUS CAUSES OF HEMOLYTIC ANEMIA
Definition and Etiology
In veterinary medicine, anaplasmosis traditionally refers to disease characterized by progressive anemia caused by intraerythrocytic infection with Anaplasma marginale in cattle and Anaplasma ovis in sheep and goats. In addition, A. marginale subspecies centrale (also known as Anaplasma centrale) causes mild disease in cattle and has been used as a live vaccine to induce partial protection against A. marginale.
In the recent taxonomic reclassification of the tick-borne bacteria in the genera Anaplasma and Ehrlichia, Ehrlichia equi (cause of equine granulocytic ehrlichiosis), Ehrlichia phagocytophila (the cause of tick-borne fever in sheep, not recognized as a significant disease problem in North America), and the agent of human granulocytic ehrlichiosis (HGE) have been reclassified and unified as a single species, Anaplasma phagocytophila.62 Correspondingly, the disease caused by A. phagocytophila in humans is designated as human granulocytic anaplasmosis (HGA) and in horses as equine granulocytic anaplasmosis. In addition, A. phagocytophila is an emerging disease of dogs.112 Although this discussion primarily addresses bovine anaplasmosis and, to a lesser degree, ovine and caprine anaplasmosis, it is important to emphasize that any descriptions of human anaplasmosis are in reference to infection with A. phagocytophila. There is no evidence that A. marginale or A. ovis are capable of infecting humans or any nonruminant mammalian species.
Clinical Signs and Differential Diagnosis
Clinical signs are highly variable, from acute severe disease to subclinical infection, and reflect variation in virulence among pathogen strains and age- and breed-related differences in host susceptibility. Age at the time of initial infection is a primary determinant of host susceptibility. Disease is often mild in calves in the first 6 to 9 months of life and increasingly severe in older cattle. The typical incubation period ranges from 15 to 30 days. Infections in calves are often asymptomatic, but mild lethargy and anorexia may be seen for 24 to 48 hours. In contrast, the early stage of acute anaplasmosis in adult cattle is typified by fever, with rectal temperatures ranging from 39.5° C to 41° C (103° F to 106° F). Within 12 to 24 hours the fever subsides, and the temperature may drop to normal and become subnormal before the animal dies. Anorexia and, in dairy cows, a dramatic decrease in milk production can usually be observed soon after a fever is detected. Concurrently, there is suppression of rumination, dryness of the muzzle, and lethargy. Cattle may stagger or become aggressive as a result of cerebral hypoxia associated with anemia. Care must be taken not to stress severely anemic cattle because this may result in collapse and death. Early, the mucous membranes are pallid, but they may be icteric if an animal has survived for 2 to 3 days past the acute crisis. Constipation is a consistent sign, with the feces dark brown and covered with mucus, and pollakiuria is characterized by dark-yellow urine. Hemoglobinuria does not occur. Abortion may occur when infection occurs late in gestation. If an animal survives the acute crisis, the convalescent period is protracted and depends on the severity of the anemia. Icterus and weight loss are more frequently observed in the convalescent period, which may last for 3 to 4 weeks. Recovered animals remain persistently infected for life and, as described later, are epidemiologically important as a reservoir for ongoing transmission. However, persistent infection is not associated with any disease or decrease in production status; therefore, no basis exists for a diagnosis of “chronic anaplasmosis.” Although A. ovis infection in sheep and goats is often asymptomatic, anemia occasionally becomes severe enough to produce signs similar to those seen during A. marginale infection of cattle.
Definitive diagnosis of acute anaplasmosis requires identification of A. marginale— or A. ovis—infected erythrocytes by microscopic examination of blood smears, concomitant with a significant decrease in hematocrit (see next section). The differential diagnosis requires consideration of the diseases that can produce anemia or icterus, including babesiosis, bacillary hemoglobinuria, and leptospirosis. In pastured cattle, hepatotoxic plant poisonings (Senecio) and other causes of liver disease that produce icterus must also be considered. Copper poisoning is considered in sheep.
Clinical Pathology and Serology
Because acute bovine anaplasmosis is characterized by anemia, a falling hematocrit is an excellent criterion for prognostic purposes and for determining the severity of infection. The packed cell volume (PCV) drops below 30% when the first clinical signs are observed and may drop precipitously within 24 to 48 hours. Death can occur during this period despite a PCV above 20%. In other cases, PCV may decrease below 10% before death. During this acute phase, A. marginale can be detected within the erythrocytes by microscopic examination of blood smears stained with Wright’s, new methylene blue, or Giemsa stain. The inclusion is composed of a small morula of two to eight individual organisms, and over 5%, up to 20% to 70%, of the erythrocytes may be infected. Later, after several days of anemia, the percentage of infected erythrocytes decreases dramatically, and evidence of RBC regeneration can be detected. There is anisocytosis, basophilic stippling, poikilocytosis, polychromatophilia, and reticulocytosis.
After recovery from acute disease, cattle and sheep remain persistently infected, with 0.000001% to 0.1% of erythrocytes being infected. These extremely low levels cannot be reliably detected by microscopic examination, and persistently infected animals, which serve as reservoirs for transmission, need to be detected serologically. Serologic diagnosis is most often accomplished through competitive enzyme-linked immunosorbent assay (cELISA),* which provides both high specificity and, unlike the complement fixation test, high sensitivity in detection of persistently infected carrier cattle.113,114 The cELISA, approved as an official test by the U.S. Department of Agriculture (USDA) and the Office of International Epizootics (OIE), is conducted by most, if not all, state diagnostic laboratories. Currently, negative status with the cELISA is required for importation of live cattle into Canada. Although cattle will seroconvert by cELISA during acute infection, serology generally is of minimal utility in diagnosis of acute anaplasmosis.
Pathophysiology
Anaplasma species are naturally transmitted by Ixodidae ticks, most often the genera Dermacentor in the mainland United States and Rhipicephalus (including tick species previously classified in Boophilus) in tropical and subtropical regions worldwide. Although there is strong epidemiologic evidence of transmission by hematophagous flies, under experimental conditions this is very inefficient,115 and thus the field conditions that allow transmission remain poorly understood. In addition, direct iatrogenic transfer of infected blood (contaminated needles; dehorning, castrating, hormone-implanting, or ear-tagging instruments) can result in transmission. After transmission, sequential rounds of bacterial invasion of mature erythrocytes, replication, and egress result in a progressively increasing, cell-associated bacteremia, with a doubling time of approximately 24 hours. Clinical signs appear when greater than 1% of erythrocytes are infected and the severity roughly correlates with the percentage of infected erythrocytes. Anemia is at least partly caused by splenic and hepatic macrophage-mediated phagocytosis of both infected and uninfected erythrocytes. This appears to reflect both induction of autoantibodies against the RBC surface and induction of acute-phase reactants, including complement activation, during high-level rickettsemia. The regenerative response to anemia can be vigorous and does not appear to be suppressed by the infection.
Protective immunity appears to require induction of both antibody against the outer membrane proteins and macrophage activation for enhanced phagocytosis and bacterial killing.116 Although the immune response controls the acute phase of infection, organisms are not completely cleared from the blood because of the emergence of antigenic variants.117 These variants are responsible for persistent infection, characterized by recurring waves of bacteremia that reflect sequential emergence and then immune control of antigenically variant organisms.
Epidemiology
A. marginale is the most prevalent of the tick-borne infections of cattle worldwide and remains a serious constraint to livestock production in tropical and subtropical regions. However, anaplasmosis is also a significant problem in temperate regions. In the United States, infection is endemic in much of the West and occurs episodically in many historically nonendemic regions; anaplasmosis has been detected in at least 40 states. Canada is considered to be free of endemic anaplasmosis. Endemic regions are maintained by the prevalence of both competent arthropod vectors and persistently infected carrier cattle. These carrier cattle, which are typically asymptomatic, are efficient reservoirs for tick-borne transmission.115,118 Vector activity varies by region, but outbreaks of anaplasmosis generally occur most frequently in the late spring and summer, when arthropod activity is highest. However, it should be emphasized that the determinants of tick-borne and fly-borne transmission are not well understood, and transmission is often unpredictable. In contrast, iatrogenic transmission can occur at any time and can be controlled by avoiding blood contamination during veterinary medical procedures. Although wild ruminants (e.g., deer, elk, bison) rarely have clinical disease and generally are asymptomatic, persistently infected carriers, their overall importance in the epidemiology of infection is unclear. Currently, wild ruminants are thought to play at most only a minor role in natural transmission.
Pathology
At necropsy, there are no pathognomonic lesions for the diagnosis of anaplasmosis. In acute anaplasmosis the blood is thin and watery and fails to clot readily. Mucous membranes, subcutaneous tissues, and skeletal musculature are pale (anemic pallor). In later stages of acute disease, however, the same tissues exhibit varying degrees of icterus. Splenomegaly is a consistent finding; hepatomegaly and distention of the gallbladder are common but seen less often. Urine is deep yellow, but neither hemoglobinuria nor hematuria occurs. The absence of hemoglobinuria helps differentiate anaplasmosis from other hemolytic diseases (babesiosis, bacillary hemoglobinuria, leptospirosis, onion toxicity, copper poisoning in sheep). Occasionally, petechiae may be found in the subepicardium, subendocardium, and other serous membranes. Detection of A. marginale—infected erythrocytes within capillaries of Giemsa-stained histologic sections can be used to confirm a diagnosis of anaplasmosis.
Treatment
Tetracyclines are the antibiotic of choice for treating acute disease, and resistance has not been reported. In acute anaplasmosis, oxytetracycline at 11 mg/kg IV every 24 hours for 3 to 5 days is effective. One to two administrations of long-acting oxytetracycline at 20 mg/kg IM at 72-hour intervals is also an effective treatment. In addition to antibiotic therapy, supportive therapy is important. If the PCV is 12% or lower, whole-blood transfusion may be indicated to prevent death and shorten the convalescent period; 4 to 8 L of whole blood is usually administered to an adult animal. A PCV of 8% or lower indicates an unfavorable prognosis, and death often occurs despite appropriate antibiotic and supportive therapy. Importantly, the oxytetracycline regimen used to treat acute anaplasmosis is not effective in completely clearing the animal of the organism, and recovered animals become persistently infected carriers. Although prior studies showed that long-acting oxytetracycline at 20 mg/kg every 3 days for four successive treatments resulted in clearance, more recent studies using this regimen and variations of this regimen have indicated that clearance is not achieved.119 If required for exportation, clearance should be confirmed by conversion to seronegative status.
Prevention and Control
Control measures vary depending on the geographic region and type of livestock production system. In endemic regions with high transmission rates, such as those in tropical countries, beef cattle are often allowed to become naturally infected at a young age and remain asymptomatic carriers with minimal risk of later acute disease. In regions with lower transmission rates, live blood-based vaccines may be used to ensure infection of cattle at a young age. This is exemplified by the use of trivalent (A. marginale, Babesia bovis, Babesia bigemina) live vaccine in Australia. Similarly, live vaccines based on A. centrale or weakly virulent strains of A. marginale are typically used in Africa, Asia, and Central and South America. However, these are not licensed for use in the United States, largely because of the risk of transmitting known or newly emergent pathogens contaminating the blood-based vaccine. The exception to this is the licensing of a live vaccine* for use in California. Importantly, these live vaccines should only be used in young animals and are contraindicated for use in older and especially pregnant animals. Killed vaccines are less efficacious and require multiple immunizations, but these can induce at least partial protection against severe morbidity and mortality. Unfortunately, none of the federally licensed killed vaccines previously marketed in the United States are currently available. However, an experimental killed vaccine* has been licensed for use in 14 states and Puerto Rico.
In the absence of immunoprophylaxis, anaplasmosis is usually controlled by preventing transmission. Although it is difficult to prevent completely the contact of ticks and biting flies with cattle grazing on open ranges or farm pastures, strategic use of acaricides and insecticides can reduce transmission during periods of high vector activity. Periodic spraying for tick control and the use of insecticide-impregnated ear tags or insecticide dust bags for biting-fly control are cost-effective, not only for control of anaplasmosis but also for control of pinkeye and for directly reducing irritation and increasing weight gain. Because blood-contaminated instruments and needles can mechanically transmit infection, appropriate sanitary measures should be implemented when injections or surgical procedures are performed.
Maintenance of an A. marginale–free herd in nonendemic areas can be accomplished by quarantine and serologic screening of all additions using the USDA-approved cELISA. Within endemic regions, however, this requires extreme vigilance in screening and prevention of both direct contact and sharing pasture with other domestic and wild ruminants, which may result in vector-borne transmission. The risk of maintaining a fully susceptible herd within an endemic region should not be taken lightly.
Babesiosis
Babesiosis is a tick-borne intraerythrocytic disease of domestic and wild mammals and humans caused by protozoan parasites of the genera Babesia and Theileria. The acute disease is characterized by fever, hemolytic anemia, icterus, hemoglobinuria, and death. Although both morphologic and serologic differentiation is needed for specific identification of the various disease-producing species, all can be categorized as being either “large” or “small” in size. Table 37-1 presents common Babesia species (and Theileria equi), their usual biologic vectors, and livestock hosts. Babesiosis has a wide geographic distribution, particularly in the tropics and subtropics, largely related to the distribution of vector ticks. Of the different diseases, the economically most important infections of livestock are those of cattle and horses.
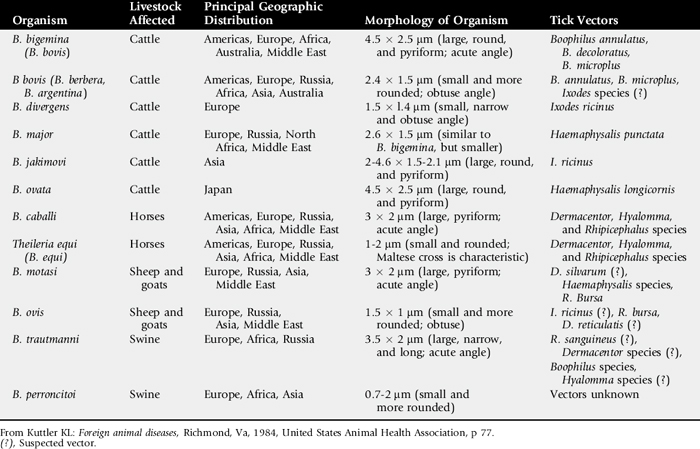
BABESIOSIS IN THE BOVINE
Etiology
Known variously by such names as bovine babesiosis, piroplasmosis, Texas fever, redwater, tick fever, and tristeza, the disease may be caused by at least six Babesia species (see Table 37-1). Animals other than cattle known to be susceptible to agents of bovine babesiosis include white-tailed deer, American bison, water buffalo, reindeer, and African buffalo. Infections in these other animals are nominal, and except under unusual conditions, such hosts are probably not significant reservoirs.
Of greatest concern in the Western Hemisphere are the species B. bigemina and B. bovis. Babesia bigemina is a large species characteristically appearing within mature erythrocytes as nonpigmented, paired, pear-shaped bodies joined at an acute angle. Irregularly shaped, round, or amoeboid forms are also seen. Babesia bovis is a small, pleomorphic species often identified as a single round body or as paired, pear-shaped bodies joined at an obtuse angle within mature erythrocytes. Of the two species, B. bovis is usually considered the most virulent.
Natural transmission of both species occurs primarily by the feeding of various stages of the one-host ticks of the genus Boophilus. Ticks are most often infected transovarially (vertically). The female tick becomes infected by the ingestion of parasites during engorgement. After it drops off the host, the babesial organisms reproduce within the tick’s tissues. Some of the reproducing organisms are incorporated within developing tick embryos, and the disease agents are transmitted to new vertebrate hosts by the feeding of ensuing tick larvae, nymphs, or adults. Larval ticks may transmit B. bovis, but B. bigemina is not transmitted until the larvae have molted into the nymphal or adult stages. Both Babesia species may also be transmitted iatrogenically through blood-contaminated fomites, as described under Anaplasmosis.
Clinical Signs
Clinical signs manifest 2 to 3 weeks after tick infestation. The incubation period after blood inoculation may be less than 5 days to more than 3 weeks, depending on the volume of inoculum. Clinical signs of fever (40° C to 42° C, 104° F to 107.6° F), depression, icterus, anorexia, tachycardia, tachypnea, anemia, hemoglobinemia, hemoglobinuria, abortion, and death are seen. Anemia is caused by intravascular destruction of erythrocytes by escaping merozoites after intraerythrocytic reproduction of the babesias by binary fission. In addition, the osmotic fragility of the whole-erythrocyte population increases terminally, such that massive lysis occurs, even though the parasitemia may be less than 1%.120 Additionally, as also seen with anaplasmosis, an autoimmune condition may result in which the spleen removes damaged and apparently healthy erythrocytes from circulation. Thus, the degree of anemia may exceed that expected with a low parasitemia. The anemia may occur rapidly, with 75% or more of the erythrocytes destroyed in a few days. The exit of B. bigemina and B. bovis parasites from infected erythrocytes releases two or more parasite-associated proteolytic enzymes into the plasma. These enzymes and other parasite metabolic products are believed to interact with blood components and are responsible for such clinical signs as metabolic acidosis and anoxia. Tachycardia may be dramatic and the heartbeat pronounced.
Cerebral babesiosis, characterized by hyperexcitability, convulsions, opisthotonos, coma, and death, may be observed in cattle infected with either B. bigemina or B. bovis, but especially with the latter. Central nervous system (CNS) signs are caused by brain anoxia resulting from severe anemia and erythrocyte blockage of cerebral capillaries.
Death is caused by a shocklike syndrome associated with the accumulation of toxins, release of vasoactive substances, and anemic anoxia. Most cases with cerebral involvement are fatal; however, mortality is extremely variable, depending on Babesia species involved, susceptibility of the host, and management and environmental stress factors. Many cattle that survive the acute phase recover but become chronic carriers. Other survivors often experience episodes of recrudescence, eventually succumbing to the disease, or they may die as a result of secondary infections contracted during their debilitated state.
Cattle of all breeds are susceptible to babesiosis. However, Bos indicus breeds exhibit a definite degree of resistance to both Babesia species and the tick vectors.121 Calves possess a natural immunity to babesiosis. Such immunity was believed to be reinforced by colostral antibodies for calves born to previously infected dams.122 However, erythrocytes of young bovines may contain factor(s) independent of antibody that provide an innate resistance to severe babesiosis.123 Thus, calves infected up to the age of 9 months experience a minimum reaction to the disease, becoming asymptomatic carriers. Carriers remain resistant to clinical disease for at least 4 years.124 The carrier state can be overcome, however, by such stressors as calving, malnutrition, and concurrent disease.125
Clinical Pathology
Clinical signs observed in cattle in enzootic areas with Boophilus ticks may provide sufficient data for a presumptive diagnosis. Other conditions that may exhibit similar signs as babesiosis are anaplasmosis, trypanosomiasis, theileriosis, leptospirosis, chronic copper toxicity, and bacillary hemoglobinuria. The cerebral signs may be confused with rabies and other encephalitides. A positive diagnosis requires identification of the Babesia species on Giemsa-stained thin blood smears, positive serologic tests, or inoculation of splenectomized calves with infective blood. In acute infection, Babesia species can usually be detected in smears made from peripheral blood. In chronic cases, numbers of parasitized erythrocytes diminish, becoming so sparse as to make detection difficult. This is especially true with B. bovis, which shows a marked tendency to accumulate in capillaries, particularly those of the brain. B. bovis may favor capillaries in the brain and kidney because the major energy-producing pathway of Babesia appears to be anaerobic glycolysis. The blockage of cerebral and renal capillaries by parasitized erythrocytes results in an anaerobic condition that enables the parasites to absorb preformed substrates by pinocytosis and diffusion through their surface membranes. PCV values drop rapidly from a normal of 35% to below 10% in less than a week after onset of clinical signs.126 Serum potassium levels decrease in some infected animals, whereas urine potassium levels increase in almost all cases.127
Specific anti-Babesia antibodies are detectable in cattle sera less than 7 days after infection.128 Such antibodies also exist for at least 252 days after the disappearance of detectable parasites.129 The complement fixation (CF) and indirect fluorescent antibody (IFA) tests are the most widely used.128 The CF test follows the same basic procedure used in anaplasmosis CF testing130 with a Babesia antigen.131 The test is effective, but approximately 100 days after infection, the CF antibodies drop below a reliable diagnostic level.128 The IFA test uses the whole intraerythrocytic parasite as antigen rather than an extract and commercially prepared rabbit antibovine γ-globulin conjugated to fluorescein.128 Other serologic tests include gel precipitation,132 latex particle agglutination,133 rapid card agglutination,134 and enzyme-labeling immunoassay (EIA).135 The immunologic assays, however, are indirect methods and do not detect the causal organisms in samples obtained from a suspected infected animal. Recombinant DNA techniques using selected clones containing inserts of Babesia genomic DNA sequences are now available to be used as specific, highly sensitive DNA or RNA probes to detect the presence of the hemoparasite DNA in an infected animal or a tick vector.136
Necropsy Findings
Postmortem findings in cattle that die peracutely are characteristic of an acute hemolytic crisis. Such findings include a generalized pallor or icterus throughout the carcass; an enlarged icteric liver; gallbladder distended with thick, dark-green bile; and a greatly enlarged, dark, soft spleen. Hydropericardium and subepicardial/subendocardial petechiation may be seen. The blood is thin and watery. The urinary bladder is frequently distended with dark-red urine. There may be subserosal ecchymotic hemorrhages in abomasal and intestinal mucosa, and the lymph nodes are edematous. The carcass of an animal that dies after a prolonged illness is generally emaciated and icteric. The intermuscular fascia is also edematous. The kidneys are pale and edematous, and the bladder may contain pink-tinged or normal urine. The liver is enlarged and jaundiced, and the bile may contain flakes of semisolid material.
Treatment and Prognosis
After the onset of hemoglobinuria or cerebral signs, the prognosis is poor. Acute cases with PCV values above 12% usually respond well to treatment. The prognosis decreases for cases with PCV values below 10%. Successful treatment depends on early diagnosis and prompt therapy. In addition to specific treatment, supportive therapy such as blood transfusions (4 L of whole blood per 250 kg of body weight), fluids, hematinics, and prophylactic antibiotics are important. However, wild, excitable cattle may best be left alone. With severe hemolytic anemias, any exertion associated with restraint and treatment may precipitate an anoxic crisis.
The small Babesia species are more resistant to chemotherapy and may require increased dosages or additional treatments. The most frequently used, effective, and relatively less toxic specific babesiacides are diminazine aceturate* at 3 to 5 mg/kg; phenamidine diisethionate† at 8 to 13 mg/kg; imidocarb dipropionate‡ at 1 to 3 mg/kg; and amicarbalide diisethionate§ at 5 to 10 mg/kg.137 Generally, treated cattle become chronic carriers and are resistant to further clinical episodes of the disease. However, treatment of B. bigemina may be so effective that sterilization occurs, eventually leaving the animal susceptible to reinfection. Imidocarb has both therapeutic and prophylactic activities. In enzootic areas, its use prevents clinical infection for as long as 2 months but at the same time allows mild, subclinical infections to occur, resulting in premunition immunity.138,139
Prevention and Control
Eradication of Boophilus tick vectors has provided effective control in the United States. Other such projects attempted elsewhere have not been successful because of such diverse reasons as tick resistance to acaricides; ability of some ticks to infest alternate, nonbovine hosts; failure to obtain 100% cooperation of cattle producers; and lack of financial resources to sustain a prolonged program.
Most procedures aimed at reducing tick infestations (acaricide applications [on host or over environment], controlled range burning, cultivation, prolonged pasture rest, use of repellents) are beneficial. Care should be taken to prevent accidental transfer of blood from one animal to another in routine surgery (e.g., dehorning, castration, ear marking, hormone implantation) and vaccination procedures.
The most common form of immunization consists of inoculating live organisms (virulent or attenuated) into susceptible calves to induce a state of premunition. Inoculation of older animals is followed by nonsterilizing chemotherapy as needed to modify clinical effects.140 Although a premunition approach is useful in endemic areas, it is less desirable in areas with low infection rates because the premunized carriers provide a large reservoir of infection. Some killed adjuvant vaccines have proved successful in limited trials.141 In vitro cell cultivation techniques have yielded highly immunogenic soluble antigens of B. bovis.142 Subunit vaccines derived from monoclonal technologies were proved effective in protecting against severe clinical disease.143 The monoclonal antibodies apparently inhibit merozoite invasion of the erythrocytes. Vaccines of such noninfectious material generally do not prevent disease, but they do moderate the effects of infection and do not directly produce carriers.
BABESIOSIS IN THE HORSE
Etiology
Babesiosis/theileriosis of equids (piroplasmosis) is a febrile, tick-borne disease caused by Babesia caballi and Theileria equi. Until recently, T. equi was known as Babesia equi. However, because the organism more closely resembles members of the genus Theileria with its exoerythrocytic (lymphocytic) stages within the vertebrate host, with development of microschizonts and macroschizonts, B. equi is now classified as Theileria equi144 (see Table 37-1). Babesia caballi is a large species resembling Babesia bigemina, which affects cattle. Although T. equi is not a member of the genus Babesia, for practical purposes it is still considered a “small” parasite, similar to B. bovis on stained thin blood smears. However, a unique characteristic of T. equi is that the intraerythrocytic parasites divide into four cells to form a Maltese cross.145
Equine piroplasmosis is widely distributed throughout the tropics and subtropics and to a lesser extent in temperature regions. The distribution roughly corresponds to those of the tick vectors. Both species are naturally transmitted by ticks of the genera Dermacentor, Hyalomma, and Rhipicephalus. B. caballi is passed transovarially (vertically) from one tick generation to the next. Transmission of T. equi apparently occurs only transstadially (horizontally); one tick stage (larvae or nymphs) becomes infected, and the disease agent is passed to the next vertebrate host in the next tick stage (nymph or adult). Because of the widespread prevalence of potential tick vectors in the United States (Dermacentor albipictus, D. iteus, and D. variablis), it is unknown why equine piroplasmosis is not a problem in the United States.
Clinical Signs
All equids apparently are susceptible to both parasite species. The zebra in Africa is naturally infected with T. equi but not with B. caballi. Once infected, survivors remain chronic carriers. T. equi can be transmitted transplacentally. Clinical features after an incubation period of 5 to 28 days include fever (39° C to 42° C; 102° F to 107.6° F), hemolytic anemia, jaundice, hemoglobinuria, and death. Generalized signs of depression, anorexia, incoordination, lacrimation, mucous nasal discharge, swelling of the eyelids, and frequent lying down are seen. T. equi is considered the most pathogenic of the two species and is responsible for a greater incidence of hemoglobinuria and death. B. caballi causes a more persistent fever and anemia. Differential diagnoses include equine monocytic ehrlichiosis, equine infectious anemia, liver failure with hemolytic anemia, and other hemolytic anemias of the horse.
Clinical Pathology
A fever associated with anemia, jaundice, and hemoglobinuria, with the detection of parasite-infected erythrocytes in Geimsa-stained blood smears, is diagnostic. A significant increase in relative and absolute numbers of monocytes and absence of eosinophils may be observed in horses infected with T. equi. Hemoglobinuria is rare in animals infected with B. caballi, but urine is often dark yellow. The most frequently used serologic tests are CF and IFA tests. Blood from spleen-intact horses can become CF positive within 14 days after parasite exposure. There is also a cELISA test for T. equi and a polymerase chain reaction (PCR) test for both equine diseases. Further, as with the bovine infections, both B. caballi and T. equi infections can be specifically detected with nucleic acid probes.136
Necropsy Findings
Postmortem features are similar to those seen in bovine babesiosis, but jaundice is even more prominent throughout the carcass. There is excessive fluid in the body cavities, especially the pericardial sac. Pulmonary edema is evident. The liver is swollen, and hepatic vessels contain large, yellowish clots. The spleen in enlarged with rounded edges.
Treatment and Prognosis
Generally, both B. caballi and T. equi respond to the same babesiacidal drugs used to treat bovine babesiosis, but T. equi is more refractory to treatment than B. caballi. If diagnosed early and treated promptly, recovery is the rule. The drug of choice for eliminating the carrier state of infected animals is imidocarb; at 2.2 mg/kg twice in 24 hours, imidocarb is effective against B. caballi; 4 mg/kg four times over 72 hours is effective against T. equi of Eastern Hemisphere origin.137 However, donkeys receiving similar treatment died from drug toxicosis.121 The higher doses of imidocarb often produce transient side effects in horses similar to signs seen in colic. To date, attempts to eliminate consistently the carrier state of T. equi of Eastern European origin have been unsuccessful.146 However, as proposed in 1993,147 irregular chemical sterilization success has been obtained with concurrent IV buparvaquone* at 4 mg/kg and IM imidocarb at 4 mg/kg.
Prevention and Control
Control of the tick infestations does much to reduce disease incidence, as does care to prevent blood transfer during such routine surgical procedures as castration. No vaccines effectively prevent equine babesiosis. Premunition (as used in bovine babesiosis) is of limited value in some enzootic areas, but it is not widely practiced because early treatment without sterilization is effective, and the resulting chronic carriers resist further disease challenge.
Hemobartonellosis (Eperythrozoonosis)
Haemobartonella bovis is an epicellular organism that is closely associated with the surface of erythrocytes. It may appear as a rod shape, an ovoid, or in chains with conventional stains. Hemobartonellosis is primarily of academic interest in North America because it is rarely a cause of anemia.148 The organism has been found in association with other rickettsial diseases and has been experimentally transmitted in splenectomized calves. The agent may be visualized as delicate ovoid, rod, or dumbbell forms arranged in chains or tight groups or randomly distributed epicellularly throughout appropriately stained blood smears.
EPERYTHROZOONOSIS IN CATTLE
The causal agent is Eperythrozoon wenyoni (Mycoplasma wenyoni). Infection is usually latent, producing no clinical signs in normal cattle, but it may become apparent in animals that have been severely stressed by some other systemic disease. The disease can be produced experimentally if infected blood is administered to splenectomized calves. Even under experimental circumstances, clinical signs consist of mild depression, fever, and modest anemia. The disease in cattle is of little clinical consequence, except for the potential for confusion should the organism be seen on stained blood films. Occasionally, cattle may have swollen and tender teats and legs.148
EPERYTHROZOONOSIS IN SHEEP AND GOATS
The causal organism in sheep and goats is Mycoplasma ovis (Eperythrozoon ovis), which appears to be very similar morphologically and serologically to the species found in cattle. The disease can produce more prominent clinical signs in sheep, with profound depression, anemia, and significant death losses in young lambs.149 Erythrocyte destruction is thought to be caused by intravascular hemolysis and erythrophagocytosis.
Theileriasis
Theileriasis is caused by small hemoparasite of the genus Theileria that infects lymphocytes and erythrocytes of ruminants and is most common in tropical and subtropical climates. The organism is spread by bloodsucking arthropods, particularly ticks of the Ixodidae family. Theileria parva is the cause of East Coast fever, a highly fatal disease of cattle in Africa. Other members of the genus Theileria (T. annulata, T. mutans, T. hirci, and T. ovis) tend to be less pathogenic and produce diseases with a wider geographic distribution.149 T. cervi has been seen in North American deer. T. mutans has been seen in erythrocytes of both cattle and deer in North America. Theileriosis caused by an agent indistinguishable from T. buffeli has been described in cattle from Texas and North Carolina with parasitemia, but clinical signs were not reported.150 Recently, T. buffeli was reported as the cause of a hemolytic anemia in a 6-month-old Simmental calf.151 There was serologic evidence of a high herd prevalence of Theileria infection, and the agent was transmitted to splenectomized calves, which developed mild anemia. The organism produces a brief illness characterized by mild fever, anorexia, and modest anemia, followed by rapid recovery.
Trypanosomiasis
Trypanosomes are flagellated protozoal organisms that can produce a variety of serious diseases of humans and animals, although many are nonpathogenic. Nagana, a disease of cattle in Africa, is caused by Trypanosoma congolensi. Trypanosoma evansi is the cause of surra, a disease of cattle in India, and Trypanosoma equiperdium produces dourine in horses. In North America, Trypanosoma theileri (Trypanosoma americanum) is the only agent reported and is principally of academic interest because it is relatively nonpathogenic. The organism is occasionally seen free in the plasma in small numbers on stained blood films from cattle as a large, flagellated protozoan with an undulating membrane.149 The organism is best visualized in buffy coat smears, which tend to concentrate it. T. theileri rarely produces clinical signs, but occasionally a fulminating parasitemia may develop, resulting in fever, depression, and decreased milk production.
Leptospirosis
Leptospira infections produce disease in several species, including cattle, sheep, swine, horses, dogs, and humans, but the acute hemolytic syndrome associated with these infections is seen most often in calves and lambs. Leptospira interrogans serovars pomona and icterohaemorrhagiae are the serotypes usually involved in the hemolytic syndrome. Clinical signs of the hemolytic syndrome vary but generally include fever, lethargy, icterus, anemia, and petechial hemorrhages. The anemia results, at least in part, from immune-mediated mechanisms. Cold-reacting immunoglobulin M (IgM) antibodies have been implicated in the hemolytic anemia seen in lambs. The degree of anemia is variable but can be severe, with evidence of erythropoietic response apparent in the peripheral blood within 4 to 7 days. A moderate leukocytosis and elevation in plasma fibrinogen are often associated with the hemolytic anemia. The diagnosis is generally made on demonstration of the organism in the urine, PCR, and an increase in serum antibody titer. Discussion of leptospirosis as a reproductive, renal, and ocular problem can be found in other chapters.
Equine Leptospirosis
Leptospirosis is a bacterial zoonotic disease that is prevalent worldwide.152 The organism can be readily transmitted between mammalian species (cattle, pigs, horses, dogs, and humans) through infected urine, body fluids, and contaminated soil or water.153 In horses from North America, infections are primarily caused by Leptospira interrogans serovar pomona kennewicki.154 There are various maintenance hosts for this serovar, with the skunk being the most common host. Leptospira bratislava has been considered the host-adapted serovar of the horse, although this has been controversial. Some researchers believe this serovar is also pathogenic to the horse, and when the horse is infected, the organism can be shed indefinitely in urine and possibly the reproductive tract.154
Leptospira pomona can cause uveitis, placentitis, abortion, stillbirth, renal disease, and hemolysis. Clinical signs include fever, jaundice, anorexia, and lethargy. Leptospirosis is a sporadic cause of abortions, although in endemic areas it may account for 13% of bacterial abortions.155 In general, abortions occur during late-term gestation. The organism can be found in the placenta, umbilical cord, kidney, and liver of the aborted fetus. L. pomona can be shed in urine for up to 14 weeks after infection. Leptospira grippotyphosa and L. hardjo are serovars also known to cause equine abortions.154
Renal disease, tubulointerstitial nephritis, pyuria, and rarely acute renal failure have been reported in horses with leptospirosis. More often, two ocular disorders appear to be associated with L. pomona infection in horses: equine recurrent uveitis (ERU) and immune-mediated keratitis. The immune-mediated response is postulated to result from the cross-reaction between leptospiral antigens and uveal tissue, cornea, lens, vitreous body, and retina.156 Recent reports have confirmed the presence of live Leptospira in the uveal tissue of horses with uveitis through isolation of the organism, positive PCR, or high antibody titer in the aqueous humor.156
Diagnosis
Diagnosis of leptospirosis can be challenging because of variable serologic results. Microscopic agglutination titer (MAT) in serum and fluorescent antibody titer (FAT) in infected tissues have been routinely used for diagnosis. The sensitivity and specificity of FAT in tissues of aborted fetuses are almost 100%.155 In cases of uveitis, high antibody titers in aqueous humor may be found despite variable serum titers, suggesting local antigenic stimulation.156 Serum titers of 1:6400 are considered significant and consistent with infection.157 Serum titers of 1:3200 that are stable for 2 to 3 weeks are not considered significant. Rising titers after 2 to 3 weeks are considered significant, and the patient should be isolated and treated. Other diagnostic modalities are PCR, histology, and bacterial isolation. Recently, Divers155 isolated genes of two surface proteins of L. pomona (immunoglobulin-like proteins A and B) that are expressed only during active infection. These proteins may improve the diagnosis and development of a protective vaccine for leptospirosis.
Treatment
Treatment for leptospirosis has been advocated with ampicillin, amoxicillin, procaine penicillin (22,000 IU/kg IM every 12 hours), oxytetracycline (5 to 10 mg/kg IV every 24 hours, slow in fluids not containing calcium), or doxycycline (7 to 10 mg/kg PO every 12 hours) for 7 days. The inflammatory response in horses with ERU and immune-mediated keratitis has been managed with corticosteroids and cyclosporine, but this may provide only temporary relief. Affected horses tend to develop ocular complications (e.g., cataracts, glaucoma, blindness, intractable pain) that may result in enucleation. The inability to cure many cases of ERU may be caused by the lack of treatment for the possibly active infection. Therefore, treatment should be directed toward controlling the ocular inflammatory response and ongoing infection, if indicated. Systemic antimicrobial therapy may not be successful in ERU cases resulting from an intact blood ocular barrier despite being inflamed.155
Prevention
Prevention must be aimed at controlling exposure to shedding hosts, infected animals, and contaminated fomites. Thorough cleaning and disinfection of contaminated areas and proper disposal of infected material are essential measures to minimize exposure. Pregnant mares should be isolated from other animals because bacterial shedding may last several weeks. If abortions occur in endemic areas, it is recommended to test horses for leptospiral antibodies and isolate those horses with a serum titer of 1:6400 or higher.157 Also, horses with a negative or low titer should be retested in 2 to 3 weeks. Horses with rising titers should be isolated. Attempts to decrease shedding in horses with oxytetracycline, penicillin G, and streptomycin have not been effective. Vaccination is sometimes performed on farms with endemic abortions or high rates of uveitis.155
Bacillary Hemoglobinuria (Redwater)
Bacillary hemoglobinuria is an acute hemolytic disorder caused by Clostridium haemolyticum (Clostridium novyi type D). Also known as “Nevada redwater,” it has been reported as a naturally occurring disease in cattle and has been experimentally produced in sheep. Clinical signs develop rapidly, and death losses are often seen. Affected animals may manifest severe depression, anorexia, fever, hemoglobinemia, and hemoglobinuria. The disease is endemic in certain poorly drained areas of the western United States and is caused by ingestion of infectious spores. The organism finds a favorable environment for development in areas of preexisting liver damage, most often produced by migrating liver flukes. The hemolytic syndrome results from toxins elaborated by the organism, which also produce a characteristic focal liver lesion. The anemia produced may be marked, and both icterus and evidence of erythropoietic response may be seen in animals that survive for more than a few days. (See Chapter 33.)
Equine Infectious Anemia
Equine infectious anemia virus (EIAV) is an RNA virus, a member of the Retroviridae family, belonging to the Lentivirus genus. It has a structure and genome organization similar to other animal and human lentiviruses. Lentiviruses use virally encoded reverse transcriptase to convert the RNA genome to a DNA intermediate that is integrated into the host’s genome by another virally encoded enzyme, integrase. The integrated DNA intermediate, or provirus, usurps the host cell to replicate its genome, manufacture viral proteins, and assemble the virally encoded proteins into virions, which subsequently bud from the cell. Thus, infection by a lentivirus results in a lifelong, persistent infection. EIAV causes the disease, equine infectious anemia (EIA), first described in 1843 by Lignée.158 In 1904, Carré and Vallée159 determined that EIA was associated with a filterable agent, making it the first animal disease determined to be caused by a virus.
Serosurveillance and Detection
EIA is a USDA-regulated disease. In 2003 the USDA estimated that serosurveillance of almost 2 million samples cost U.S. horse owners more than $48 million. USDA-accredited laboratories use a testing scheme that detects the presence of serum antibody to the virus. The Coggins’ test, developed by Dr. Leroy Coggins in 1970, provided the first efficient serologic test for detection of EIAV-infected animals; it remains a USDA-accepted test.160,161 In addition, four ELISAs are licensed tests, one of which is a competitive ELISA (cELISA). These ELISAs detect antibody directed at the transmembrane glycoprotein (gp45) and the p26 antigen.162 All areas in the United States, Canada, and Mexico accept either the Coggins’ test or one of the licensed ELISAs when testing for EIA is required for entry. Equids that cross state lines or that attend many equestrian events are required to be seronegative for EIA; however, the required period of seronegativity between tests varies according to the state. No tests are currently approved by the USDA for diagnosis of EIA based on detection of viral nucleic acid.
Serosurveillance can lead to the detection of horses that are infected with EIAV but that otherwise appear healthy. Indeed, most infected horses are inapparent carriers. However, blood transferred from an inapparent carrier to another horse, through instruments (e.g., needles, nasogastric tubes, dental equipment), blood products, or insect vectors (primarily tabanids), can lead to infection with a fatal outcome.
Clinical Findings
The clinical form of EIA is characterized by three defined, temporal stages of disease: acute, chronic, and inapparent. The acute stage occurs with the initial burst of viremia and is characterized by high fever, thrombocytopenia, and nonspecific signs of malaise, including lethargy and inappetence. Ecchymoses and petechiae may also be detected on the mucous membranes. During the chronic stage, similar clinical features occur during recurrent episodes of viremia, interspersed with periods of clinical quiescence and low viremia. Throughout the chronic stage the clinical episodes tend to diminish gradually in severity and duration. The inapparent stage occurs once levels of viremia are immunologically contained and no clinical signs are detected. Horses experiencing clinical disease at any point may develop DIC and die. In addition, episodes of stress, including transportation, racing, and extreme temperatures, may precipitate clinical disease. Furthermore, corticosteroids have been used experimentally to induce recrudescence of clinical disease.163
Other chronic manifestations of EIA include the development of dependent edema, weight loss, anemia, and other ill-thrift signs. Rare manifestations that may develop include leukoencephalitis and enterocolitis.164 The expression of clinical disease, particularly during acute infection, likely involves multiple factors, including inoculating dose, virulence factors of the inoculating viral strain, immune status and immunogenetics of the host, age, and stress. Indeed, clinical disease occurs concomitantly with high-titer viremia. Horses with high-titer viremia pose the greatest risk of transmission to uninfected horses.
Lentiviruses have a DNA-dependent RNA polymerase (reverse transcriptase) that misincorporates nucleotides, resulting in changes in the viral genome.165 This mechanism allows for generation of viral variants that differ genetically from preexisting ones. As a result, genetic and antigenic variation of epitopes for neutralizing antibody and cytotoxic T lymphocytes allows viral escape from adaptive immune responses.166,167 Antigenic variation plays a central role in recurrence of clinical disease throughout the chronic stage of infection and thwarts attempts to develop an effective vaccine.165
The EIA virus can replicate effectively in monocytes, dendritic cells, and tissue macrophages.168-170 In addition, EIAV has been shown to replicate in endothelial cells.171 EIAV replication in endothelial cells may play a role in the development of DIC by viral damage to endothelial cells, with subsequent exposure of subendothelium.171 This in turn could lead to platelet aggregation and formation of thrombi.172 In addition, damaged endothelium may result in development of dependent tissue edema by transudation of fluid through compromised small vessels.171
Necropsy Findings and Clinical Pathology
Necropsy examination of horses that die of EIA may demonstrate splenomegaly, lymphadenopathy, hepatomegaly, pronounced hepatic lobular architecture, ecchymoses of the mucosa and viscera, dependent subcutaneous edema, and thrombotic disease of small vessels. Histologic findings may include a mononuclear cell infiltrate of periportal regions of the liver, adrenals, spleen, lymph nodes, meninges, and lungs. Hemosiderophages are frequently detected in the spleen, lymph nodes, liver, and bone marrow. Glomerulonephritis from immune complex deposition is often observed.
Clinicopathologic abnormalities vary depending on the stage and severity of infection. During clinical disease, a frequently profound thrombocytopenia develops concurrently with each successive episode of fever. Platelet function of EIAV-infected horses has been demonstrated to be hypofunctional, possibly exacerbating bleeding tendencies and the progression to DIC in clinically affected equids.173 Anemia from intravascular hemolysis, extravascular hemolysis, and depression of bone marrow erythropoiesis may progressively develop during the chronic stage of infection.174 During the inapparent stage, horses typically have increased plasma total solids and globulin concentrations, mild anemia, and decreased albumin concentration.175 Polyclonal B-cell activation is also evident, suggesting chronic antigenic stimulation despite clinical quiescence.175 Concomitant fever and thrombocytopenia should prompt immediate consideration of EIA. A history of recurring fever is also suggestive of EIA, particularly when other causes of fever have been ruled out.
Prevention, Control, and Regulatory Considerations
It is well recognized that EIAV seroprevalence varies with the region of the United States.174 States considered at a high risk include Texas, Oklahoma, Louisiana, and Arkansas, whereas the mid-Atlantic area, New England, Alaska, and Hawaii are considered low-risk regions. The remaining states are classified as intermediate-risk areas. Despite regional differences in risk to noninfected horses, sporadic outbreaks do occur. Veterinarians should therefore encourage all horse owners to test for EIAV annually, test new arrivals, and maintain good fly control. In addition, the veterinary community should encourage organizers of equestrian events to require proof of seronegativity of attending horses.
Once a seroreactor is identified, all contact horses are quarantined and undergo testing until two negative test results at 30- to 60-day intervals are obtained for all individuals in the quarantined herd.162 The required interval is based on the need to allow recently infected horses to seroconvert. Seroreactors may be either quarantined or euthanized, depending on state regulations. Quarantined horses must be at least 200 yards (180 m) from seronegative animals, the distance shown to be sufficient to obviate viral spread by insect vectors. In addition, seroreactors remaining in permanent quarantine need to be identified. A USDA code number followed by the letter A is assigned to the quarantined horse and permanently applied to the horse as a brand or lip tattoo.
Because an eradication program has never been implemented in the United States for EIA, persistence of reservoirs of horses infected with EIAV must be expected. Indeed, the vast majority of horses in the United States are not tested on an annual basis. To encourage horse owners voluntarily to maintain vigorous surveillance testing, the veterinary community needs to educate owners about the consequences of infection by EIAV. Horse owners are often unprepared to deal with the financial and emotional losses associated with detection of a horse seropositive for EIAV.
IMMUNE-MEDIATED HEMOLYTIC ANEMIA
Autoimmune Hemolytic Anemia
Definition and Etiology
Autoimmune hemolytic anemia is associated with the production of autologous antibodies directed against the patient’s own RBCs. These antibodies combine with complement and antigens on the RBC membrane, leading to the rapid removal of affected RBCs from the circulation and their accelerated destruction. Autoimmune hemolytic anemia occurs rarely as a primary idiopathic disorder176,177; more often it is found secondarily associated with some other primary disease process.176 An idiopathic immune-mediated hemolytic anemia has been reported in a calf177 and pony.178
Clinical Signs and Differential Diagnosis
The presenting clinical signs of animals with autoimmune hemolytic anemia are quite variable, depending on the degree of anemia and the primary disease. Animals with marked anemia (PCV <15%) manifest signs typical of those seen in any animal with a severe hemolytic anemia (i.e., depression, pale mucous membranes, variable icterus, elevated heart and respiratory rate, variable to intermittent fever). Secondary autoimmune hemolytic anemia in horses has been associated most often with some other primary problem, such as purpura hemorrhagica, lymphoma, other neoplasms, protein-losing enteropathy, or chronic bacterial infections.179,180 Clinical features are typical of the primary problem, with additional findings of a hemolytic anemia. In humans, exposure to a wide variety of drugs has been causally associated with the development of autoimmune hemolytic anemia. A number of studies report an association between procaine penicillin and autoimmune hemolytic anemia in horses.82,181-185 Autoimmune hemolytic anemia was reported in a 10-year-old horse treated with trimethoprim-sulfamethoxazole.186 This apparently occurs rarely, perhaps only in specific individuals, but drug history should be ascertained in all animals with an otherwise unexplained hemolytic anemia.
The anemia in cattle with anaplasmosis and babesiosis or in horses with equine infectious anemia, piroplasmosis, or ehrlichiosis is largely the result of an immune-mediated hemolytic process. These diseases are discussed fully elsewhere in this book.
Clinical Pathology
The hemolytic process often is rapid and persistent, leading to a pronounced anemia. The hematologic features are those typically expected for a responsive hemolytic anemia. The anemia often is progressive and may become severe, even life threatening (i.e., PCV <10%). Erythrophagocytosis and autoagglutination may be noted on blood smears. Spherocytosis may be difficult to recognize in large animals because of the relatively small cell size and lack of a clear area or central pallor of the erythrocytes from these species. If the process has been present for 4 days or more, hematologic evidence of active erythropoietic response may be seen in the peripheral blood of all species except the horse. This evidence of bone marrow response is a favorable prognostic indicator, even when the anemia is quite advanced. A moderate neutrophilic leukocytosis is a common feature, and thrombocytopenia may be noted in some individuals if the autoimmune process is directed at platelets and megakaryocytes, as well as the erythrocytes.
Diagnosis
Documentation of the presence of antierythrocyte antibodies and complement on the RBC membrane is based on the direct Coombs’ test. The indirect Coombs’ test detects antierythrocyte antibody in the serum. It is important to remember that the Coombs’ test is based on species-specific reagents. These reagents are commercially available in the United States for small animals and horses, and not all diagnostic laboratories will have suitable Coombs’ reagents for other species. Special procedures may be necessary to adsorb these reagents to avoid nonspecific reactions. Multivalent Coombs’ reagent directed against IgG, IgM, and complement is most often used. The Coombs’ test usually is conducted at body temperature and also in the cold. A positive reaction at body temperature indicates that the antibodies are primarily IgG. These warm antibodies are associated more frequently with anemia, generally produce a more severe anemia, and tend to be more responsive to corticosteroids than the cold-reacting antibodies. The cold-reacting antibodies detected with the saline agglutination test run at 25° C and 4° C (39° F and 77° F) are primarily of the IgM class. Exposure to a cold environment may be necessary to produce clinical signs associated with cold agglutinin disease. Both the warm-reacting and the cold-reacting antibodies are capable of fixing complement. Unfortunately, the Coombs’ test is not always positive in affected animals. Approximately one third of human and canine patients with autoimmune hemolytic anemia have a negative direct Coombs’ test, possibly because of low concentrations of antibody or low binding to the RBC membrane. The diagnosis in these patients depends on ruling out other causes of a responsive hemolytic anemia and on the response to corticosteroid therapy. Direct immunofluorescence with flow cytometry was used to determine the classes of antibody bound to erythrocytes in three horses and 12 dogs with immune-mediated hemolytic anemia. The three horses had surface-bound IgG, including a horse with suspected penicillin-induced hemolytic anemia, a foal with neonatal isoerythrolysis, and a foal with clostridial septicemia.187
A substantial proportion of otherwise normal horses have small amounts of cold-reacting Coombs’ antibodies, and spontaneous agglutination may be noted in blood sample tubes exposed to the cold. In most cases these cold agglutinins appear to occur naturally and, at low levels, are of little clinical significance. Prior treatment with corticosteroids may inhibit antibody production and could lead to a false-negative Coombs’ test.
Pathophysiology
Autoimmune hemolytic anemia rarely has been reported as a primary or idiopathic process in large animals; however, immune-mediated anemia occurs more often as a secondary problem (1) in association with certain types of neoplasia; (2) with a variety of viral, bacterial, rickettsial, and protozoal infections; (3) after exposure to certain drugs; or (4) in association with other immune-mediated disorders, such as systemic lupus erythematosus.188 The initiating factors for this autoimmune disorder are not completely understood but may be related to alterations in the RBC membrane through direct or indirect injury, which elicits an abnormal response by the immune system. The RBC membrane is no longer recognized as “self” and is treated as a foreign antigen. Alternately, changes in the immune system or stimulation by some other antigenic source may result in production of antibodies with a misdirected cross-reactivity with the patient’s own normal erythrocytes. Structural and functional changes in the RBC membrane are induced by the antigen-antibody reaction and complement fixation. The complement-fixing IgG or IgM antigen-antibody reaction may produce sufficient RBC damage to result in intravascular lysis of erythrocytes, but more often, affected cells are removed from the circulation at a rapid rate by the reticuloendothelial system of the liver and spleen. Partial phagocytosis of affected cells may result in spherocyte formation. Although the presence of spherocytes on blood smears is a characteristic diagnostic feature in human and canine patients with autoimmune hemolytic anemia, the relatively small size of RBCs of most large domestic animals may make it difficult to recognize spherocytes.
Treatment and Prognosis
The approach to treatment of autoimmune hemolytic anemia depends on the causal factors. If the animal has a history of drug therapy, it is advisable to discontinue medication or to change to another class of drug. Patients with primary or idiopathic autoimmune hemolytic anemia may be the best candidates for treatment. Immune-mediated hemolytic anemias secondary to other diseases can only be managed if the primary problem is amenable to treatment. Thus, treatment of an immune-mediated hemolytic anemia in a patient with extensive lymphoreticular neoplasia is likely to be unrewarding, and thorough diagnostic efforts should precede case selection for treatment. Although immune-mediated processes are responsible for hemolytic anemia in a number of infectious diseases, therapy must be directed at the primary agent, and corticosteroids are contraindicated in these diseases. Corticosteroids can cause recrudescence of viremia in horses with EIA, and a negative Coggins’ test should be a prerequisite to treatment of horses with an autoimmune hemolytic anemia of undetermined cause.
Treatment of autoimmune hemolytic anemia is directed at providing supportive care and interrupting the immune response responsible for antibody production. This is usually accomplished with systemic glucocorticoids. For a 450-kg horse, dexamethasone is recommended at an initial dosage of 30 to 40 mg/day given parenterally. This rate is continued for 3 to 5 days, then decreased gradually over 7 to 14 days, depending on the response to therapy; the hematologic response should be closely monitored. If there has been no response in 5 to 7 days, the diagnosis of autoimmune hemolytic anemia should be reviewed, and potential causes of bone marrow suppression should be evaluated. Once the hemolytic process is well under control, oral prednisolone can be given at 400 to 500 mg daily. Human patients and small animals with immune-mediated hemolytic anemia unresponsive to corticosteroids are often treated with cyclophosphamide. There is one report of successful management of a horse with cyclophosphamide and azathioprine when the anemia failed to respond to corticosteroids.189 Supportive care consists of providing a quiet, restful environment and good nutrition, including vitamin supplementation. Iron- and copper-containing hematinics are generally of little benefit because neither of these elements is lost with hemolytic anemia. Blood transfusion is also of little benefit because it is often impossible to find a compatible donor, and the transfused cells are rapidly removed from the circulation. Blood transfusion should not be administered unless the anemia is life threatening and the immune response can be controlled with corticosteroids.
Neonatal Isoerythrolysis in Horse and Mule Foals
Neonatal isoerythrolysis (NI) is the most common alloimmune disease in neonatal foals 7.5 hours to 12 days old (median. 2.5 days).190 NI is characterized by hemolytic anemia, icterus, and hemoglobinuria. Clinicopathologic abnormalities include anemia, high serum indirect and direct bilirubin concentrations, and sorbitol dehydrogenase activity. NI is caused by a blood group incompatibility between the foal and dam. The foal inherits from the sire and expresses an erythrocyte antigen (alloantigen) that is not present in the mare. The hemolytic syndrome is mediated by maternal antibodies against foal erythrocytes (alloantibodies) absorbed from colostrum. Blood factors associated with NI in horse foals are Qa, Qb, Qc, Aa, Pa, and Dg, and donkey factor in mule foals.190 The most common antigens are Qa and Aa. Foals with NI may also present with alloimmune thrombocytopenia. (See Chapters 19 and 53.)
HEINZ BODY HEMOLYTIC ANEMIA
Definition and Etiology
An acute hemolytic anemia can develop after exposure to a variety of oxidizing agents. These include drugs such as phenothiazine, methylene blue, and acetylphenylhydrazine and plants such as wild or domestic onions, members of the Brassica family (rape or kale), and wilted or dried leaves of the red maple (Acer rubrum).191-197 Red maple toxicosis (RMT) has been reported in horses, zebras, and alpacas.195,198-200 Heinz body hemolytic anemia also occurs in sheep on specially formulated diets that are low in molybdenum, which results in chronic copper toxicity, as herd problems in cattle grazing rye grass (Secale cereale)201 or selenium-deficient pastures in Florida,202 and with selenium deficiency as a contributing factor in postparturient hemoglobinuria of cattle in New Zealand.203 These agents produce or allow oxidative denaturation of hemoglobin and resultant aggregation of the protein globin, which appears as Heinz body inclusions within the RBCs. Heinz body anemia has been seen in association with lymphoma in a horse, possibly from failure of the reticuloendothelial system (RES) to remove the Heinz bodies, as reported in horses with EIA.204
Clinical Signs and Differential Diagnosis
Clinical signs vary with the species involved, specific toxin or toxic metabolites, amount of toxin ingested, time course of the disease process, and occurrence of complicating secondary factors, such as hemoglobin nephrosis and acute renal failure. Weakness, lethargy, anorexia, and exercise intolerance are the usual presenting complaints, and death losses can occur. Mucous membranes are generally pale with variable to marked icterus. The heart and respiratory rates are generally elevated, but rectal temperature is usually within normal limits. Horses with RMT may be subclinical or may present with lethargy, muddy or cyanotic mucous membranes, tachycardia, inappetence, weakness, colic, icterus, brown discoloration of the blood, and pigmenturia. Rarely, sudden death occurs.200 Pyrexia and hypothermia have also been documented. Most horses develop clinical RMT during summer and fall. The high mortality rate in horses with RMT may relate to the combination of a rapidly progressive hemolytic anemia and the formation of methemoglobin. Urine output may be reduced, and the urine may be dark because of the presence of hemoglobin, methemoglobin, or bilirubin.
It is not possible to differentiate Heinz body hemolytic anemia from other potential causes of hemolytic anemia without laboratory evaluation. The absence of fever may help to differentiate these anemias from infectious causes of hemolytic anemia. History of exposure to potential oxidizing agents and the fact that these toxic plants may produce death losses or clinical signs in multiple animals at the same time should help to differentiate these cases from autoimmune hemolytic anemia.
Clinical Pathology
Poisoning or intoxication resulting in Heinz body formation usually causes acute and profound anemia. In the early stages a very high percentage of erythrocytes may have Heinz body inclusions. Later, as these cells are removed from the circulation and replaced by young cells from the bone marrow, the relative number of affected cells may decrease greatly. Heinz bodies are round, oval to serrated, refractile granules usually located near the cell margin or protruding from the cell and best visualized with vital stains such as crystal violet or new methylene blue applied to unfixed blood smears. Heinz bodies appear as bluish green inclusions with the new methylene blue stain. Fixing of blood smears with methanol in preparation for staining with the classic Wright’s stain interferes with stain uptake, and Heinz bodies appear as a pale area within or projecting from the cell margin and can easily be missed. After the first 3 or 4 days, the anemia is usually associated with hematologic evidence of an active erythrogenic response in all species except the horse. The total plasma proteins usually remain within normal limits, and the Coombs’ test is negative. Red maple poisoning also results in depleted RBCs, reduced glutathione, methemoglobinemia, increased osmotic fragility, and modest elevations of liver-derived serum enzyme activities.
The rapid and profound erythrocyte destruction may lead to hemoglobinemia and hemoglobinuria. The development of renal failure secondary to hemoglobin nephrosis is a definite risk in these animals and is reflected by modest to marked increases in the blood urea nitrogen (BUN) and creatinine, as well as changes in the urinalysis.196,197 These parameters should be monitored in severely affected animals. As with other causes of hemolytic anemia, serum bilirubin, particularly the indirect reacting bilirubin, is elevated.
The clinicopathologic abnormalities of horses with RMT include anemia (PCV as low as 7.5%), eccentrocytes, Heinz bodies, and elevated plasma methemoglobin concentration.200 Other significant findings consist of inflammatory leukogram and renal insufficiency (75% and 40% of cases, respectively).200 Mild elevation of serum total bilirubin is observed in most cases, and hemoglobinuria is seen in all affected patients.
Pathophysiology
Heinz bodies are formed by the precipitation of oxidatively denatured hemoglobin. The hemoglobin contained within the RBC is constantly undergoing mild oxidative stress associated with oxygen transport, as well as generation of superoxide radicals and hydrogen peroxide within the cell. A number of reducing mechanisms within the RBC counteract these oxidative processes through production of NADPH and reduced glutathione. The occurrence of Heinz body hemolytic anemia could be viewed as a consequence of exposure to oxidative stresses that simply overwhelmed the cells’ reductive capacity. Selenium deficiency results in a decrease in glutathione peroxidase, a selenium-containing enzyme; in special circumstances, selenium deficiency may contribute to Heinz body formation by impeding the ability of the cells to respond to oxidative stress. Substantial species variation in the rate of Heinz body formation relates to the chemical structure of hemoglobin and the efficacy of erythrocyte-reducing mechanisms in the face of oxidative stress.191 RBCs with Heinz bodies are less deformable than normal cells and are rapidly removed from the circulation by the RES in the spleen, where they are phagocytized and broken down. Old or senescent erythrocytes are thought to be more prone to develop Heinz bodies. Splenectomy or corticosteroid therapy may alter Heinz body clearance mechanisms, allowing significant numbers of affected RBCs to remain in the circulation of otherwise normal animals.
Gallic acid is a strong oxidant present in red maple leaves. Gallic acid has been implicated in the oxidation of hemoglobin, methemoglobin formation, and Heinz body anemia.195,196,205 Methemoglobin is the result of oxidative change of hemoglobin iron to the nonfunctional ferric state (see discussion of nitrate poisoning, Chapter 54). This is normally prevented by glutathione reductase, ascorbic acid, and reduced glutathione. Methemoglobin cannot load or transport oxygen and, when present in sufficient quantities, results in a brown color of peripheral blood and mucous membranes. An estimation of methemoglobin concentration in a blood sample can be made by comparing the hemoglobin concentration measured by the cyanmethemoglobin method, which measures all forms of hemoglobin, with that measured by the oxyhemoglobin method, which only measures oxyhemoglobin, not other forms such as methemoglobin. Methemoglobinemia and hemolytic anemia have been reported in a mare and her dam in association with decreased levels of RBC glutathione and glutathione reductase, presumably as a result of an inherited enzymatic defect.206
Treatment
Treatment primarily involves removal from the source of toxicity and provision of supportive care. Blood transfusion can be very beneficial in severely anemic patients, particularly when there is insufficient evidence of active erythropoietic response. Iron-containing hematinics are of little benefit. Intravenous fluid therapy is indicated in animals with hemoglobinuria or azotemia to reduce the potential for further renal damage. High doses of vitamin C (ascorbic acid, 50 to 100 g IV daily), together with fluids and transfusion, were thought to aid recovery in two horses with red maple poisoning.207 One report suggests that vitamin C therapy may have little impact on survival of affected horses, and when methylene blue was used to treat the associated methemoglobinemia in two horses, both died.208 The goal of therapy should be to improve tissue oxygenation and perfusion and control inflammation and pain (use of NSAIDs). Horses treated with corticosteroids have an increased likelihood of death.200
Prognosis
Prognosis in animals with modest anemia and evidence of response is good if the inciting factor can be controlled or eliminated. The mortality rate of horses with experimental or naturally occurring RMT is reported to be 60% to 65%.208 In animals with rapidly progressive and profound anemia, prognosis is poor unless blood transfusion is undertaken. Complications are associated with hypoxia, hypoperfusion, and inflammation. Horses may develop acute renal failure, colic, pyrexia, and laminitis. A recent retrospective study of 32 horses reported a fatality rate of 59%.200 It has been proposed that the severity of anemia is associated with mortality, but the previous study showed no such association.200
OTHER CAUSES OF HEMOLYTIC ANEMIA
Intravascular Hemolysis Following Cutaneous Burns
Intravascular hemolysis has been reported in horses after severe cutaneous burns affecting more than 25% of their body surface. Plasma on admission showed hemolysis along with abnormal RBC morphology, increased osmotic fragility, hemoglobinuria, azotemia, and hemoglobin pigment nephropathy.209 The pathophysiology of hemolysis is unclear but suspected to be associated with the production of hydroxyl radicals by complement-activated neutrophils. Abnormal findings reported in humans include intravascular hemolysis, increased RBC osmotic fragility, decreased membrane deformability, RBC crenation, eccentrocytosis, spherocytosis, bud formation, fragmentation, and vesiculation.210 Presence of these abnormalities depends on the severity of burn trauma.210 Pseudothrombocytosis has been reported, presumably caused by the incorrect recognition by automatic counters of RBC microvesicles as platelets.210 Early fluid therapy and free-radical scavengers have been beneficial for the treatment of burns in humans, along with supportive and wound care, control of pain and inflammation, and prophylaxis of sepsis. A recent murine study suggested that the level of plasma free hemoglobin is related to the size and depth of burn injury, which may be difficult to determine in some cases.211
L-Tryptophan—Indole Intoxication
Experimental studies in ponies have demonstrated an acute hemolytic process associated with orally administered L-tryptophan, which is converted to indole in the GI tract.212 Intoxication was associated with an acute onset of restlessness, tachypnea, intravascular hemolysis, and hemoglobinuria. At necropsy there was evidence of hemoglobinuric nephrosis and bronchiolar degeneration in some ponies. Similar clinical signs were noted after oral administration of tryptophan at 0.35 to 0.60 g/kg and indole at 0.1 to 0.2 g/kg.212,213 Intravascular hemolysis was associated with increased osmotic fragility and with Heinz body formation in a few of the experimental ponies.
Water Intoxication
Massive water intake may produce marked hypotonicity of the body fluids, with subsequent intravascular hemolysis of erythrocytes.214 This problem has been described as a naturally occurring entity in milk-reared calves when first given access to unlimited quantities of water.215,216 Severe neurologic signs may be seen, including depression, convulsions, and coma; respiratory distress, hemoglobinuria, and death losses occur in some cases. Clinicopathologic features include hemolytic anemia, hypoproteinemia, hyponatremia, hypochloremia, hyposmolality, hemoglobinuria, and hyposthenuria. A sudden decrease in serum osmolality is believed to result in osmotic lysis of erythrocytes.217 Fragility of the erythrocytes to osmotic shock is greatest in calves between 4 and 5 months of age. Treatment is primarily a matter of temporarily restricting water and providing supportive care. Calves with marked hyponatremia (sodium 110 mmol/L) that are manifesting neurologic signs may benefit from hypertonic saline, mannitol, and corticosteroids. The goal of treatment is the restoration of serum sodium to 120 to 125 mmol/L without overcorrection. Death losses can occur in as soon as 2 hours, but most calves recover without long-term adverse effects.
Postparturient Hemoglobinuria
A syndrome of intravascular hemolysis, hemoglobinuria, and anemia has been recognized in postparturient dairy cattle worldwide.218 The disease occurs sporadically, and the incidence is relatively low. Affected animals are most often high-producing multiparous cows that develop clinical signs during the first month after calving.219 Depression, decreased feed consumption, and decreased milk production are associated with hemoglobinuria, anemia, and icterus. The anemia is often marked and after 4 or 5 days is associated with evidence of a strong erythropoietic response. The precise mechanism causing the intravascular hemolysis has not been fully defined. The condition has been related to the marked hypophosphatemia often found in affected cows and the moderately low phosphate levels in unaffected herdmates. Hypophosphatemia arises from inadequate dietary phosphorus intake in animals grazing phosphorus-deficient soils or fed fodder grown on such soils. Low intracellular phosphate concentration may interfere with energy metabolism, thus affecting cell viability and the ability of RBCs to deal with potential hemolysins, such as saponins from sugar beets or alfalfa. A postparturient hemolytic problem has been described as a herd problem in New Zealand associated with copper deficiency and Heinz body formation203 (see previous section).
Blood transfusion and supportive IV fluids are indicated in valuable cows with severe life-threatening anemia. Treatment of hypophosphatemia consists of provision of phosphate, initially as sodium acid phosphate (NaH2PO4H2O), 60 g/300 mL of water IV, followed by oral phosphorus supplementation. Correction of dietary imbalances is indicated.
Copper Toxicosis
Copper is an essential nutrient for domestic animals, but excessive supplementation can result in toxicity. Copper poisoning is a common intoxication in ruminants. The toxicodynamics and clinical syndromes have been reviewed.220-222 Lambs are most susceptible to the effects of copper, but poisonings have occurred in adult sheep, goats, and cattle. Merino sheep are more resistant than British breeds to the toxic effects of copper.223 Cattle have been poisoned by ingesting diets containing 37 mg of copper/kg of feed for 2 years.224 Cattle fed 12 mg or more of copper/kg have been reported to develop subclinical hepatic disease.225
Pathogenesis
Elemental copper is an essential trace mineral that has a narrow therapeutic window. Dietary requirements for growing sheep range between 4 and 6 parts per million (ppm), but toxicity can occur whenever sheep are exposed to diets containing as little as 10 to 20 ppm.226-228 Phytogenous copper poisoning results from concomitant ingestion of copper at 20 ppm of food, molybdenum, and sulfate. Ingested salts of copper are absorbed through enterocytes by carrier proteins and transported to blood in loose complexes with albumin and amino acids.229 Ionized copper is approximately 20% of the total plasma copper. Between 70% and 90% of the ionic copper is internalized by hepatocytes, where it is redistributed to bile, packaged in lysosomes in protein complexes, or used for the formation of ceruloplasmin.229 Accumulation of copper occurs because daily hepatic biliary copper excretion amounts to less than 1% of ingested copper in ruminants.230 Hepatic storage can buffer high levels of copper intake until the sites become saturated. At that time, hepatocytes die spontaneously or in response to environmental stress or dietary changes. Hepatocyte death causes the release of large amounts of cuprous copper into the blood. Animals that have preexisting hepatitis from pyrrolizidine alkaloids store less copper and are more susceptible to the hemolytic crisis.223,231
Free inorganic copper is an oxidant and can participate in Fenton’s reaction. Cellular damage is related to the production of oxidative hydroxides and peroxides, but not to copper oxidation. These reactive intermediates are thought to initiate lipid peroxidation and oxidative denaturation of proteins within erythrocytes. Oxidation of heme protein produces Heinz bodies, and oxidation of the hemin produces methemoglobinemia. Oxidized erythrocytes spontaneously lyse intravascularly, or they are sequestered in the spleen and degraded to constituent amino acids. Vitamin E is also denatured. This latter reaction removes a potent antioxidative protective factor and enhances the cellular susceptibility to additional oxidants. Differences in genetic susceptibility to copper poisoning are unknown.
The hemolytic phase of copper poisoning is often initiated by noxious stimuli that could include shipping, hierarchic change, administration of oxidative drugs, starvation, or change of housing.232 Feeding of high-protein diets has increased the resistance in sheep to the hemolytic crisis; however, the role of extra molybdenum intake in these supplemented animals was unclear.228,233 The mechanistic relationship between the stressful events and the hepatocyte release of copper is unknown.
Etiology
Sources of copper that have been responsible for copper accumulation in animals include trace-mineralized salt, inappropriately formulated cereal grain mixtures, forages from pastures fertilized by swine or chicken manure,234 orchard pastures contaminated by copper-containing fungicides, rations containing more than 20% chicken litter, and diets that contain high concentrations of palm kernel oil. Other potential sources of copper accumulation include fencing and copper piping and overdoses of parenterally administered copper salts. In one recent case at the University of California, Davis, dairy goats were poisoned by supplementation of trace minerals that were formulated for dairy cattle.
The toxic dose of copper for each species is variable and depends on the duration of exposure, the animal’s genetics, and the amount of molybdenum being fed. Diets that contain copper/molybdenum ratios greater than 6:1 are more likely to result in copper poisoning than diets with lower ratios. The interaction between the two minerals may occur in the solid phase of rumen ingesta, when insoluble and nonabsorbable complexes of copper, sulfur, molybdenum, and large—molecular-mass protein are formed. The highly complexed copper is unabsorbed and thus not toxic. High dietary intake of zinc and iron also inhibits absorption of copper, and although the precise mechanism of antagonism is unknown, the elements share a competitive affinity for metallothioneine.235-237 Competition for this protein could alter the storage capacity for copper. Soil sulfates reduce molybdenum absorption by plants, thereby increasing the potential for pathologic accumulation of copper in herbivores.
The respective single toxic doses of copper for sheep and cattle range from 20 to 110 mg/kg and 220 to 880 mg/kg body weight. Most poisonings occur after a long-term, low-dose ingestion of the element. Copper poisoning can occur in sheep after 2 months of daily dosing of 3.5 mg/kg copper, feeding a ration that contains 20 ppm copper for several months, or after a single subcutaneous injection of copper—ethylenediaminetetraacetic acid (EDTA) salt at 2.0 mg/kg.238 Sheep have been poisoned by subcutaneous injection of 3 to 4 mg/kg copper-calcium EDTA, but remained normal after 6 mg/kg copper methionate.239 Sheep have died after single injections of 2 mg/kg diethylamine copper oxyquinoline sulfonate.239 One study that fed 3.7 mg copper/kg daily for 84 days reported peak hepatic copper levels between 258 and 375 mg/kg wet weight by 26 days after the final copper feed.240 A single dose of 50 mg copper caused acute hemolytic crisis in sheep when treated during midpregnancy. The highest incidence of hemolytic anemia occurred in Welsh sheep, with a lower cumulative incidence in Cheviot sheep.241 Single doses of copper-calcium ETDA at 25 mg/animal has killed lambs.242 Cumulative doses of copper ranging between 12.8 and 22 g have produced hemolytic anemia in Suffolk lambs by 42 days.
Goats may show signs of copper poisoning by 144 days after daily feeding of a ration that contains 80 mg copper/kg. Placental transfer of copper occurs, but concentrations in the tissues of lambs are not toxic, even during the hemolytic phase in the dam.
Adult cattle may be poisoned by feeding 5 g copper sulfate daily for as long as 4 months. Calves may be poisoned after 6 to 8 weeks of feeding milk replacer containing 115 ppm copper.229,243 Horses are resistant to high dietary concentrations of copper and may remain clinically normal after prolonged feeding of diets containing levels as high as 791 ppm. In these horses, hepatic concentrations of copper at the end of the feeding period reached 4000 ppm. Adult ponies treated once with oral copper at 40 mg/kg did not develop hemolytic anemia.
Clinical Signs
Animals that have been exposed to high levels of copper are asymptomatic for weeks until the onset of hepatic necrosis.244,245 Signs develop rapidly after the onset of hepatic necrosis and reflect coexisting anemia, myopathy, and neurologic, renal, or hepatic disease. Clinical signs include inappetence, lethargy, weakness, recumbency, cool extremities, pallor, and grayish discoloration of the mucous membranes. Affected animals have a greatly increased pulse rate, tachypnea, hypotension, and hypothermia. The pulse amplitude of the linguofacial artery is decreased. Urine is dark red due to the presence of free hemoglobin products. The animals may have marked petechiation of the conjunctival mucosa. Pregnant animals often abort because of hypoxemia. Feces are dark or have yellowish discoloration, but are normally formed, and do not contain hemoglobin unless secondary abomasal ulceration has occurred. Recumbent patients usually expire without struggling. Exposed ewes that survive copper poisoning tend to have dystocia and dilation failure in subsequent lambing periods.
Pathology
The tissues of hemolyzing animals are pale and icteric. The serous surfaces are covered by petechial and ecchymotic hemorrhages. The liver is often pale and yellow, and the lungs are firm. The kidneys are black and have a metallic sheen because of entrapped hemoglobin. The urinary bladder of copper-poisoned animals is filled with serosanguineous urine. Microscopic changes include hemoglobinuric and tubular nephrosis, as well as necrosis of the splenic follicles and hepatocytes. There is also biliary ductular proliferation and pericholangitis.240,246 Hepatic necrosis may be detectable by microscopic examination for as long as 412 days after poisoning. Microscopic changes in the brain of poisoned animals include spongy degeneration of the pons and brainstem.
Diagnosis
Normal hepatic copper concentrations in sheep have been reported as 173 ± 130 ppm (mean ± SD) and 129 ± 59 ppm (wet matter) for adults and lambs, respectively.247 Wet matter hepatic concentrations of copper in poisoned animals were 429 ± 249 ppm. Dry weight concentrations may be greater than 3000 ppm. Hepatic concentrations are usually high before and after the hemolytic episode, but normal hepatic copper concentrations in hemolyzing animals have been reported.238 The correlation between plasma and hepatic copper concentrations in prehemolytic animals is poor.248,249 Copper poisoning in animals with normal plasma concentrations and near-toxic liver levels has been reported.250 Normal plasma copper concentrations range from 13 to 20 μmol/L (0.8 to 1.2 μg/mL).240 Serum copper concentrations range between 0.60 and 1.50 μg/mL (0.6 to 1.5 ppm). Plasma copper concentrations that range between 2.4 and 20.0 μg/mL (2.4 to 20 ppm) are diagnostic of acute toxicosis.
Clinical Pathology
There are no consistent hematologic changes until 24 hours before the hemolytic crisis, when sudden concentrations of cytosolic hepatic enzymes increase coincidentally with a sharp rise in plasma copper concentration. Plasma copper concentrations fall rapidly after the hemolytic crisis and are often near normal by 4 days posthemolysis.244 The concentrations of copper within erythrocytes remain high.
Hepatic concentrations of 16 mmol copper/kg of dry matter are the threshold for development of hemolytic anemia. The half-life of copper in the liver of nontreated poisoned sheep has been estimated at 175 ± 91 days,240 and high copper concentrations in hepatic tissues can be found for as long as 100 days after the initiation of the hemolytic episode.248
Kidney concentrations of copper in animals with hemolytic crisis are 15 and 50 ppm for dry and wet weight volumes, respectively. Sheep may have increased plasma concentrations of γ-glutamyltransferase (GGT) and aspartate aminotransferase (AST) for 3 days before onset of hemolysis, and glutamate dehydrogenase may be increased for as long as 700 days after cessation of copper ingestion.240,251 Fecal copper concentrations may exceed 10,000 ppm during the hemolytic episode.
Clinicopathologic changes that occur during the acute hemolytic crisis include Heinz body formation; intravascular hemolysis; methemoglobinemia (as much as 5%); decreased PCV; increased concentrations of plasma bilirubin, AST, GGT, alkaline phosphatase, total bilirubin, creatine kinase, creatinine, and plasma urea nitrogen; and increased plasma ceruloplasmin. Urine is dark brown to black and contains high concentrations of protein, blood, and hemoglobin casts. Microscopic examination of urine may detect erythrocytic casts and inflammatory cells.252 Sheep that survive the hemolytic episode develop reticulocytosis by 4 days after onset of clinical signs.253
Treatment
Animals with acute hemolytic syndrome should be treated with insufflated oxygen and vitamin E (three to five daily doses of 3000 IU/dose). If PCV is less than 8%, animals should be given packed, washed homologous erythrocytes. Additional therapy should include D-penicillamine (Cuprimine* at 52 mg/kg daily for 6 days), anhydrous sodium sulphate (1 g/sheep daily for 6 days), and ammonium molybdate (100 mg/sheep daily for 6 days). D-Penicillamine therapy increases urinary copper excretion by 10- to 20-fold.254 Single-dose therapy with D-penicillamine (28 mg/kg) increases copper excretion, but the effect is transient and insignificant for reducing the total hepatic copper load.255
Dietary supplementation with 7.7 ppm ammonium molybdate also results in hepatic copper concentrations that are 40% lower than in unsupplemented controls. Addition of 7 or 15 mg molybdenum for 80 days to experimentally poisoned sheep has reduced hepatic copper concentration in sheep by 34% and 46%, respectively.256 Copper-poisoned cattle have been successfully treated with oral sodium molybdate (3 g daily) and sodium thiosulphate (5 g daily). When introduced into the sulfur-rich rumen contents, molybdenum salts complex with high—molecular-weight proteins in the solid phase of the digesta.257 The protein-bound thiomolybdate aggregates strongly chelate copper in insoluble and indigestible complexes. Molybdenum salts also enhance biliary copper excretion and remove copper selectively from hepatic metallothioneine.235,258,259 For poisoned cattle, top dressing of food with 500 to 1000 mg ammonium molybdate daily for 18 days greatly reduced the amount of hepatic copper.260
Parenterally administered ammonium tetrathiomolybdate has been recommended for treatment of acute hemolytic crises caused by copper poisoning. Intravenous administration of ammonium tetrathiomolybdate reduces both lysosomal and cytosolic copper in hepatocytes. The drug has been given at 0.2 mg/kg molybdenum (thiomolybdate), as IV injections of 50 to 100 mg twice weekly for up to 11 weeks, or as three doses of 3.4 mg/kg on alternate days and beginning at the onset of hemolytic crisis.261-265 Concomitant administration of 36 mg xylazine IV increased copper excretion in bile by as much as 2.25-fold over controls that were treated with thiomolybdate only.266 The parenteral administration of the thiomolybdate results in transient increases of copper concentrations in blood for as long as 24 hours. Because copper is acid insoluble, the effect is to protect the copper-exposed animals from hemolytic crises and reduce the tissue damage during an hemolytic event.267,268 Biweekly injection of 100 mg molybdenum as tetrathiomolybdate increased daily hepatic biliary copper excretion by a factor ranging between 150% and 300%.269
Prevention
Because of the sporadic nature of the poisoning and lack of signs during the accumulative phase, copper poisoning can be difficult to prevent. Clients should be counseled to purchase concentrates with label claims for the species that are being supplemented. Copper-supplemented salts should be restricted, especially in sheep. Heavily copper-contaminated pastures can be top-dressed with molybdenum phosphate at 113 g per acre. Fencing and plumbing that contain copper sulfate or metallic copper should be removed from the environment. One study controlled the hemolytic crisis and associated mortality from copper poisoning in sheep receiving 36 mg copper/kg daily for 18 months, by subcutaneous (SC) injection of sterile ammonium tetrathiomolybdate containing 3 to 4 mg molybdenum on alternate days for three injections.264 The sheep in this study were given either IV or SC molybdenum at dosages that amounted to 1.7 and 3.4 mg/kg ammonium tetrathiomolybdate. Addition of ammonium molybdate at 7.7 ppm and sodium sulfate at 4200 ppm reduced liver copper and decreased plasma ceruloplasmin in experimentally exposed lambs.249
Feeding of sodium molybdate and sodium sulfate at respective daily dosages of 20 mg and 6 g to experimentally poisoned lambs reduced hepatic copper content after 90 days.270
Molybdenum and sulfur protect sheep by converting ingested copper to nonabsorbable thiomolybdate complexes in the rumen. The antagonistic effects are greatest at times of rapid hepatic accumulation of copper. Addition of 3 mg/kg of food (dry matter) molybdenum as tetrathiomolybdate reduced hepatic copper accumulation by as much as 33-fold.263 Lambs that were fed diets containing 7.7 ppm ammonium molybdate after weaning until 14 weeks of age had reduced hepatic copper and decreased ceruloplasmin concentrations.249 Cattle can tolerate indefinite periods of feeding copper at dosages less than 0.6 mg/kg daily.250 Addition of 220 to 420 ppm zinc may be protective against copper poisoning in sheep, but this is not used in clinical situations.257
Hemolytic Syndrome in Horses with Liver Failure
A fulminant, intravascular hemolytic syndrome has been reported as a near-terminal event in horses with either acute or chronic liver failure.271 Marked hemoglobinemia and hemoglobinuria are associated with intense icterus. The sclera and conjunctiva often take on a distinctive, deep—reddish orange color. The onset of intravascular hemolysis is sudden and rapidly progressive. The prognosis is highly unfavorable because almost all horses that develop this syndrome die or must be euthanized because of clinical deterioration.272 Intravenous fluids, corticosteroids, and supportive care do not appear to alter the clinical course or the unfavorable outcome.
The cause of this syndrome has not been determined, but apparently it is not related to a release of hepatic copper stores. The hemolysis appears to be associated with increased erythrocyte osmotic fragility. Human patients with liver cirrhosis develop a hemolytic syndrome associated with alterations in the exchangeable lipoproteins of the RBC membrane. It is not known if a similar mechanism is responsible in horses, but morphologic alterations in the RBCs of these horses resemble the “burr cells” described in human patients.273 Bile acids and their salts are greatly increased in liver failure and could play a contributing role in the hemolytic process. At necropsy, widespread hemorrhagic lesions that resemble those described for DIC are often present.273 DIC and the activation of various mediators may play a role in the terminal stages of this almost invariably fatal process.
“Pink Tooth,” Congenital Erythropoietic Porphyria, Toxic Porphyria
A rare congenital disorder of hemoglobin production inherited as an autosomal recessive trait has been recognized primarily in Holstein cattle, but it has also been reported in Shorthorns and Jamaican cattle.274,275 This disorder is commonly called “pink tooth” and is characterized by slow growth rates in calves, photosensitization and exfoliation of nonpigmented skin when exposed to sunlight, reddish brown teeth, and modest anemia. The teeth and bones exhibit a pink fluorescence under ultraviolet (UV) light, and the urine is brownish red because of uroporphyrin. The condition is present at birth, and the metabolic defect in these cattle is a hereditary deficiency of the enzyme uroporphyrinogen III cosynthetase, which catalyzes an essential step in the synthesis of the porphyrin structure of hemoglobin.275 This leads to the accumulation of uroporphyrin and coproporphyrin, which deposit in the teeth, where porphyrin is concentrated in the dentine, bones, and other tissues. Several factors contribute to the variable anemia seen in these cattle. A reduced intravascular RBC lifespan is related to the high concentration of uroporphyrin and coproporphyrin within the cells. Porphyrins may induce hemolysis and also delay maturation of the RBC series in the bone marrow, although there is often evidence of active erythropoietic response in the peripheral blood.275
There is no treatment for this inherited disorder, but genetic counseling is advisable. Substantial efforts have been made to reduce the incidence of pink tooth in the Holstein breed. It may be possible to detect carrier animals. Affected cattle have much lower levels of uroporphyrinogen III cosynthetase than normal cattle, and carrier animals have intermediate levels of this enzyme. Despite their rather serious problems, these cattle do reasonably well if housed indoors out of direct sunlight. The principal differential consideration is chronic fluorosis, which also produces brown discoloration of the teeth. However, the teeth of cattle with chronic fluorosis do not fluoresce under UV light.
An additional form of altered porphyrin metabolism, congenital erythropoietic porphyria, has been described in humans and cattle.275 In humans the mode of inheritance is autosomal dominant, whereas in cattle the disorder appears to have a recessive pattern of inheritance and may be sex linked because it is only seen in females. The disease does not produce anemia, porphyrinuria, or discoloration of the teeth. This disorder is caused by a deficiency of ferrochelase (heme synthase), which leads to high concentrations of erythrocyte and fecal protoporphyrins. Porphyria has also been reported in swine, with a dominant pattern of inheritance.275 There is little effect on the health of the pigs and no photosensitivity, but the teeth have reddish brown discoloration. Although similarities exist with bovine congenital erythropoietic porphyria, the precise defect in swine has not been found.
Finally, animals may develop acquired toxic porphyrias. This can occur with heavy metal poisonings, principally lead, but has also been produced experimentally with hexachlorobenzene and other chemicals. Lead inhibits several key enzymes of heme synthesis. Inhibition of aminolevulinate dehydrase leads to an accumulation of aminolevulinic acid, and decreased aminolevulinate dehydrase activity is a sensitive indicator of lead poisoning. Lead also inhibits ferrochelase, leading to marked elevation of erythrocyte zinc protoporphyn IX, the measurement of which provides a means of monitoring lead exposure.275
DEPRESSION ANEMIA
The most common form of anemia in domestic animals is associated with inadequate erythropoiesis or bone marrow depression. Depression anemia can be caused by (1) deficiencies of vitamins or minerals that are essential for erythrocyte production, (2) systemic disease processes that interfere with normal erythropoiesis, and (3) processes that damage or displace normal bone marrow elements (Box 37-2). Depression anemia is often mild to moderate in severity and generally is only slowly progressive. Depressed erythropoiesis is occasionally associated with processes that also result in blood loss and increased rate of erythrocyte destruction. When this occurs, a profound, rapidly progressive, and potentially life-threatening anemia can develop.
With the possible exception of chronic iron or copper deficiency, depression anemia tends to be normocytic and normochromic. Bone marrow evaluation is an extremely useful diagnostic tool in animals with nutritional deficiencies or when bone marrow damage or dyscrasia is suspected. A thorough clinical evaluation and vigorous application of appropriate diagnostic procedures are necessary to establish a diagnosis of depression anemia and to determine the factors responsible for the anemia.
IRON DEFICIENCY ANEMIA
Iron is present in most forages and grains. In neonates the major source of iron is colostrum (∼0.79 mg/L in mare’s milk).276 Soil, dam’s feces, and milk are other important sources of iron.276 Iron deficiency most often is associated with chronic blood loss as the result of internal or external parasitism, bleeding GI lesions, or hemostatic defects.149 Dietary iron deficiency is seldom the sole cause of anemia, even in neonates on an all-milk diet, unless they are raised on cement or in barns or hutches with no access to the soil. A modest anemia is anticipated in veal calves. The anemia seen in some young calves during the first few days to weeks of life is apparently the result of congenital iron deficiency,277 but the causal factors have not been determined. Altered immune functions, high incidences of infection, and reduced growth performance are reported in veal calves on low-iron diets.278 Alterations in gastrointestinal pH may alter absorption of iron by the small intestine. States of inflammation and infection cause iron sequestration, not deficiency, by the reticuloendothelial system and lactoferrin. Iron deficiency has been well documented in calves and piglets that are housed exclusively indoors or hatches with no access to soil.279 Absolute iron deficiency anemia is not usually reported in horses.280-283
The circulating erythrocytes account for approximately two thirds of the total iron reserves found in the body. The remaining iron stores are distributed in the liver, spleen, and bone marrow. With chronic blood loss anemia, iron depletion is first indicated by decreased marrow iron, which can be appreciated with special staining of the bone marrow with Prussian blue stain for iron. As blood loss continues and iron deficiency progresses, serum iron is decreased, whereas iron binding capacity actually may increase. It is only late in this whole process that iron-deficient erythropoiesis results in the typical microcytic, hypochromic erythrocytes that generally are thought to be characteristic of iron deficiency anemia (decreased PCV, hemoglobin concentration, mean corpuscular volume, and mean corpuscular hemoglobin concentration).149,192 Other laboratory findings include echinocytosis, keratocytosis, schistocytosis, acanthocytosis, ovalocytosis, hypoferritinemia, and hypoferremia.280-283 The observed RBC morphologic abnormalities are thought to be caused by oxidative damage. The normal serum iron and iron-binding capacity for most domestic animals is 100 and 300 μg/dL, respectively. There is one report of a neonatal foal that had iron deficiency with refractory anemia and severe abnormal RBC morphology, but no microcytosis or hypochromasia.283
Treatment of iron deficiency anemia depends on evaluation of the cause and the correction or resolution of the process responsible for the chronic blood loss. Iron is usually supplied as an oral supplement or as a feed additive, and a variety of commercial preparations are available. Injectable iron dextran intended for use in baby pigs should be avoided in horses and cattle because it can induce an anaphylaxis, especially if administered repeatedly.284 Iron cacodylate was a safe parenteral iron preparation for use in horses but is no longer readily available. An injectable iron preparation intended for use in horses was reported to result in acute iron overload, massive hepatic necrosis, and severe death losses in a group of young cattle.285 Iron overload has resulted in acute death losses in neonatal foals fed an iron-containing microbial supplement. Iron accumulation resulting in hemochromatosis with extensive liver damage has also been reported in adult horses, although the mechanism responsible for the iron accumulation has not been explained.286
COPPER DEFICIENCY
Copper deficiency can occur as a primary problem in milk-fed animals or in pastured animals in copper-deficient areas. More often, copper deficiency occurs secondarily in association with other trace mineral imbalances (e.g., dietary molybdenum excess) and is influenced by the sulfur and zinc content of the diet. Copper is an essential cofactor for a variety of enzymatic reactions, and copper deficiency produces a constellation of clinical signs related to impairment of these reactions.287 Clinical signs of copper deficiency are most prominent in young, growing animals and may include reduced growth rate, rough and depigmented hair, diarrhea, osteoporosis with spontaneous fractures, and anemia. In lambs, copper deficiency can produce a demyelinating syndrome known as “swayback” or “enzootic ataxia.” Copper deficiency has also been associated with hemolytic anemia in postparturient dairy cattle in New Zealand.285
Copper plays an important role in the transport of iron from the gut to the marrow and in the incorporation of iron into the heme moiety. The anemia produced by copper deficiency is generally moderate, slowly progressive, and closely resembles iron deficiency in that it is usually a microcytic, hypochromic anemia. Bone marrow evaluation often reveals intracellular accumulations of iron known as sideroblasts. This finding indicates that the principal problem is a function of altered incorporation of iron into the erythrocyte hemoglobin rather than an actual deficiency of iron. Copper deficiency can be documented by measuring serum copper as ceruloplasmin, erythrocyte superoxide dismutase, or the copper content of hair, liver, or kidney. Serum iron tends to be low in animals with copper deficiency. Copper can be supplied as a dietary supplement or as an injectable copper glycinate preparation.
VITAMIN B12 AND FOLIC ACID DEFICIENCY
Almost all the vitamins are necessary for normal erythropoiesis, but in ruminants and horses, only deficiencies of vitamin B12 and folate have been associated with the development of anemia.149 These two vitamins play essential roles in DNA synthesis. When deficiencies of both vitamins coexist, as experimentally produced in pigs, a marked macrocytic anemia with hypersegmented circulating neutrophils and giant metamyelocytes and neutrophils in the bone marrow may be found. In ruminants, vitamin B12 deficiency has been associated with grazing cobalt-deficient pastures. A macrocytic to normocytic anemia may be noted in these animals. Folate deficiency has been reported as a cause of a mild seasonal decline in erythrocyte parameters in horses.
ANEMIA OF INFLAMMATORY DISEASE
A depression anemia associated with characteristic disturbances of iron metabolism is often found in animals with conditions that result in a chronic inflammatory response.288,289 These conditions include chronic internal or cutaneous infections, infectious diseases, or immune-mediated processes that result in chronic inflammation, severe traumatic injury or fractures, and active malignant neoplasia. The anemia tends to be mild, slowly progressive, and of itself, of little clinical consequence. Clinical signs relate to the primary disease process; and hematologic features are those of a mild, nonresponsive anemia, often with indications of a chronic inflammatory response (neutrophilic leukocytosis, as well as monocytosis with elevated fibrinogen, total protein, and globulin). Serum iron and iron-binding capacity are decreased, but marrow iron reserves and serum ferritin are increased.149,289
Anemia in these animals partly results from a modest decrease in the circulating RBC lifespan, but it is primarily caused by major alterations in iron metabolism and a depressed bone marrow response to the anemia. These alterations represent part of the body’s response to inflammation, which includes the release of interleukin and other mediators and the production and release of various “acute phase” proteins from the liver. The body tends to sequester iron from the circulation into storage forms primarily in the liver and bone marrow, where it is retained and is relatively unavailable for erythropoiesis. This general reaction may play a protective role by denying readily available iron to potential bacterial pathogens that require iron for rapid growth and multiplication. Iron supplementation is not indicated for the treatment of the anemia of chronic inflammation, and therapeutic effort should be directed at resolution of the primary disease process.
ANEMIA SECONDARY TO ORGAN DYSFUNCTION
A mild to moderate, nonresponsive anemia can develop in patients with chronic endocrine, hepatic, renal, or GI diseases. These disorders can produce bone marrow depression by (1) reducing the production or absorption processing and the distribution of elements essential for erythropoiesis, (2) allowing the elaboration or accumulation of toxic compounds, or (3) interfering with the production or action of erythropoietin.290,291 These effects can occur independent of alterations in iron metabolism that characterize the anemia of inflammatory disease.289 However, should inflammatory processes be responsible for the specific organ damage or dysfunction, the same pattern of anemia as described in the previous section would apply. Specific therapy for the anemia in these patients is not indicated, and resolution of the anemia depends on successful management of the primary disease process.
Internal parasitism, particularly that associated with Trichostrongylus species in ruminants, can result in a marked anemia. The anemia in these animals is primarily the result of bone marrow depression, in which failure to absorb iron, copper, and essential amino acids plays a major role.
MYELOID AND MEGAKARYOCYTIC BONE MARROW HYPOPLASIA
Myeloid and megakaryocytic bone marrow hypoplasia was reported in eight young standardbred horses sired by the same stallion.292 Clinical signs were variable and in individual horses included nonhealing wounds, nonresponive fevers, pleuritis, pneumonia, ataxia, hemoperitoneum, and bleeding into the bowel. Seven horses died or were euthanized. The principal laboratory findings were a variable RBC count from normal to modest to marked anemia, moderate to profound neutropenia, and an intermittent thrombocytopenia in most of the horses. There appeared to be a cyclic variation in neutrophil and platelet counts. A bone marrow microenvironment or growth factor defect is suspected as the cause of this problem because myeloid progenitor cells were present and were able to respond to exogenous growth factors. A familial basis for the disease is suspected.292
APLASTIC ANEMIA
Aplastic anemia is a stem cell disorder characterized by reduced marrow production of all blood components in the absence of a primary disease process infiltrating the bone marrow or suppressing hematopoiesis.293,294 Peripheral pancytopenia secondary to marrow aplasia is apparently very uncommon in horses, although idiopathic hypoplastic anemia has been reported,295-297 as well as rare cases associated with the use of phenylbutazone.290,298 Hemorrhagic diathesis caused by thrombocytopenia is often the first indication of disease, manifested by epistaxis, mucosal petechiae, or prolonged hemorrhage after trauma or injections. Pallor may be present, with other signs of anemia (e.g., reduced exercise tolerance) depending on the severity and rapidity by which aplasia progresses. Neutropenia causes increased susceptibility to infections, which may result in intermittent fever or weight loss. The production of lymphocytes is reportedly not impaired; however, absolute lymphopenia can occur in aplastic anemia. Circulating lymphocytes are often highly reactive, producing the suspicion of neoplasia or a preleukemic syndrome.290
Marrow aplasia in humans is usually termed idiopathic, although some cases are associated with exposure to a drug, chemical, ionizing radiation, or presence of another disease.294 Marrow failure results from damage to the hematopoietic stem cell compartment. This may be in the form of DNA damage to stem cells or depletion of later progenitor cells by a cycle-active agent. Some cases of marrow aplasia appear to be immune mediated, either genetically determined or incited by a particular viral infection or drug exposure.
The diagnosis of aplastic anemia is based on the combination of peripheral pancytopenia and bone marrow hypoplasia with fatty replacement. Because the normal erythrocyte lifespan in horses is approximately 140 days and in cattle exceeds 160 days,299 neutropenia with no left shift and thrombocytopenia are earlier hematologic manifestations.
The major aims in treatment of aplastic anemia are to remove the animal from suspected causative agents and to provide supportive care, in the hope that spontaneous remission will occur. Broad-spectrum antimicrobials are necessary to control infections. Blood transfusions are rarely indicated, and platelet transfusion should be reserved for severe bleeding episodes, which rarely occur. Bone marrow transplantation is used with some success in humans, although graft-versus-host disease poses significant risk. The latter would presumably limit this therapy in horses, and too few horses with aplastic anemia have been studied to give a clear indication of prognosis.
Bracken fern toxicosis in ruminants causes bone marrow depression and subsequent pancytopenia.48,299 Most field outbreaks of the disease occur in cattle. The toxic effects of the plant are cumulative, and clinical signs occur suddenly 2 to 8 weeks after cattle gain access to the plant. Clinical signs include fever, melena, epistaxis, hematuria, mucosal petechiae, hyphema, and bleeding from the eyes and vagina. Hematology reveals a platelet count less than 40,000/μL and profound leukopenia with essentially no neutrophils present. Death may follow in 1 to 3 days as a result of the combined effects of multiple internal hemorrhages and bacteremia. The aplastic anemia factor in bracken fern has not been identified, although ptaquiloside has been suggested.299 Necropsy of cattle with bracken fern toxicosis reveals multiple hemorrhages throughout most tissues, necrotic GI tract ulcers, and pale bone marrow. Antibiotics and blood and platelet transfusions may be appropriate but cattle with advanced bracken fern toxicosis (platelet count <50,000/μL; leukocyte count <2000/μL) usually die.
PARADOXIC ERYTHROID HYPOPLASIA
Recombinant human erythropoietin (rhEPO) has been used in racehorses to enhance their athletic activity by stimulating erythrocyte production in the bone marrow. Mild to moderate anemia and paradoxic erythroid hypoplasia based on bone marrow cytology were reported in two standardbred race horses after rhEPO administration.300 Serum from these horses inhibited the rhEPO-induced activity of mouse bone marrow in vitro. The degree of inhibition was inversely proportional to the amount of exogenous rhEPO added to the serum, suggesting the presence of anti-rhEPO antibodies. Anti-rhEPO antibodies to exogenous rhEPO likely cross-reacted with the horses’ endogenous rhEPO. These horses were treated with dexamethasone at adjustable dosages according to response and returned to their usual athletic activity.
ERYTHROCYTOSIS (POLYCYTHEMIA)
Absolute erythrocytosis is caused by increased erythropoiesis that creates a circulating erythrocyte mass above normal for the species. Relative erythrocytosis caused by hemoconcentration, endotoxemia, and splenic contraction (horses) must be ruled out because these conditions are much more common in large animals than absolute erythrocytosis. Diagnosis of absolute erythrocytosis is based on persistently elevated packed cell volume (PCV), hemoglobin, and erythrocyte count, without clinical evidence of shock or dehydration and without response to intravenous fluid therapy. Primary erythrocytosis is associated with normal arterial oxygen tension and reduced plasma erythropoietin, whereas secondary erythrocytosis is caused by increased production of erythropoietin.
All disorders characterized by an absolute erythrocytosis share clinical manifestations caused by expanded blood volume and increased blood viscosity. Generalized vascular expansion and venous engorgement cause the characteristic “muddy” hyperemia of mucous membranes. A marked decrease in cardiac output accompanies blood hyperviscosity and ultimately impairs tissue oxygenation, producing the vague signs of lethargy and weight loss. There may be an increase in thrombotic complications such as laminitis and renal failure.
CONGENITAL ERYTHROCYTOSIS
Familial erythrocytosis, described in cattle301 and humans,302 is caused by autonomous erythropoietin production without a demonstrable lesion. Congenital erythrocytosis is thus a form of inappropriate secondary erythrocytosis. Chronic hypoxia should be ruled out by measuring the arterial oxygen concentration. The only way to definitively differentiate secondary erythrocytosis from primary erythrocytosis is by determination of serum erythropoietin.
ACQUIRED ERYTHROCYTOSIS
Primary Erythrocytosis
Polycythemia vera, an idiopathic myeloproliferative disorder characterized by excessive proliferation of erythroid, myeloid, and megakaryocytic elements, has not been reported in large animals.
Secondary Erythrocytosis
PHYSIOLOGICALLY APPROPRIATE ERYTHROCYTOSIS
In domestic animals, absolute erythrocytosis is usually secondary to chronic diseases that produce tissue hypoxia. Chronic tissue hypoxia that attends residence at high altitude, congenital heart defects that produce right-to-left shunting, and some forms of chronic pulmonary disease induce a compensatory increase in plasma erythropoietin that results in absolute secondary erythrocytosis.303
The partial pressure of oxygen (PO2) in capillaries must be maintained close to 40 mm Hg to ensure adequate off-loading of oxygen to tissues. At elevated altitudes, diminished atmospheric oxygen tension produces a much smaller alveolar capillary PO2 gradient and an inadequate driving force for tissue oxygenation. Erythropoietin production in response to hypoxia causes erythrocytosis to increase the oxygen-carrying capacity of circulating blood. Cattle are most susceptible to the effects of high altitude, and some develop polycythemia at 1800 m (5940 ft) above sea level.48 Horses develop an increased erythrocyte mass above 2200 m (7260 ft), especially when in training. Sheep are similar to cattle, but goats are apparently least susceptible to elevation hypoxia.
Congenital cardiac disorders that produce right-to-left shunts are a common cause for absolute erythrocytosis in large animals. Tetralogy of Fallot is the most common defect to cause shunting of unoxygenated blood into the peripheral circulation, although a number of other defects, including the most common ventricular septal defect, may eventually result in right-to-left shunting and secondary erythrocytosis.304
Chronic impairment of alveolar ventilation may eventually cause erythrocytosis, although most chronic pulmonic diseases in large animals are not associated with significant hypoxemia. Chronic obstructive pulmonary disease in horses may produce enough ventilation/perfusion mismatching to reduce the pressure of arterial oxygen below normal, but the resultant hypoxemia is insufficient to induce erythrocytosis.
PHYSIOLOGICALLY INAPPROPRIATE ERYTHROCYTOSIS
Inappropriate elaboration of erythropoietin (i.e., normal PO2 and secondary erythrocytosis) may rarely accompany renal, hepatic, or endocrine disorders, especially those caused by neoplasia. Secondary erythrocytosis may accompany nonmalignant renal disorders, in which local intrarenal ischemia is believed to mediate increased erythropoietin production. Paraneoplastic erythrocytosis with normal serum erythropoietin is caused by tumor production of androgenic steroids or a protein with erythropoietin-like action.305 Increased plasma erythropoietin and secondary erythrocytosis have been identified in horses with hepatocellular carcinoma.303,306 Erythrocytosis was described in a horse with hepatoblastoma307 and in another with lymphoma,308 but serum erythropoietin levels (as measured by a human assay) were normal in both cases. In the horse with lymphoma, erythropoietin gene expression was identified in the lymphoma tissue. Typically, the diagnosis of inappropriate secondary erythrocytosis is based on elevated serum erythropoietin in the absence of hypoxemia. Elevated serum erythropoietin may not be demonstrated because of the nature of the assay or other compounds causing erythrocytosis.
TREATMENT OF ERYTHROCYTOSIS
When erythrocytosis is not in response to an appropriate physiologic stimulus (e.g., primary erythrocytosis, inappropriate secondary erythrocytosis), phlebotomy to keep the PCV less than 50% is the mainstay of the treatment to control hypervolemia and blood hyperviscosity. Initially, 2 to 4 L of blood may need to be removed every 2 to 3 days, but as iron deficiency supervenes, the frequency of phlebotomy may be reduced. The myelosuppressive drug hydroxyurea, used in humans and dogs with polycythemia vera,302,309 has not been tried in large animals.
The management of appropriate secondary erythrocytosis is more complex because there is a need for increased oxygen-carrying capacity of the blood. The beneficial effect of expanded RBC mass is ultimately offset by the detrimental effect of increased blood viscosity on oxygen delivery. Oxygen delivery is impaired when the PCV exceeds 60%, although continued erythropoietin output may result in overcompensation. Phlebotomy is indicated when the PCV is greater than 60%, but the optimum PCV for patients residing at high altitudes or those with right-to-left cardiac shunts must be determined by trial and error.
The long-term prognosis for patients with erythrocytosis is determined by the severity and cause of the disorder. Congenital cardiac defects, neoplastic diseases, and chronic organ insufficiency carry a guarded to poor prognosis. Familial or primary erythrocytosis may be managed by phlebotomy, although there are no long-term follow-ups for large animals with these disorders.
PROLIFERATIVE DISORDERS OF LYMPHOID AND MYELOID SYSTEMS
The lymphoproliferative disorders reported in horses include lymphoma, lymphocytic leukemia, and plasma cell myeloma. The myeloproliferative disorders include myeloid leukemias and malignant histiocytosis.310 The following sections describe lymphoma, leukemia, and myeloma.
BOVINE LYMPHOMA
Bovine lymphoma (lymphosarcoma) is characterized in terms of the frequency of occurrence (sporadic or endemic/enzootic), age at onset, organ involvement, and associated etiologic agent. Sporadic bovine lymphoma occurs as generalized lymphadenopathy in calves (calf or juvenile form), as thymic involvement in cattle between 6 months and 2 years of age (thymic or adolescent form), and as a cutaneous form in cattle between 1 and 3 years of age. Lymphoid tumors of cattle with sporadic bovine lymphoma are of the B-cell or T-cell lineage.311 The most common form of lymphoma appears endemically in adult cattle more than 2 years of age and is associated with bovine leukemia virus (BLV) infection and typically involves multiple organ systems; BLV-associated lymphomas of adult cattle are of the B-cell lineage.312 BLV is classified in the genus Deltaretrovirus, subfamily Orthoretrovirinae, and family Retroviridae.
Sporadic Lymphoma
CALF OR JUVENILE FORM
The prevalence rate of juvenile lymphoma is unknown, but this form of lymphoma is rare, and multiple cases may be seen in the same herd. The cause of juvenile sporadic lymphoma is unknown and does not appear to be associated with BLV infection.313
The age at onset ranges from 3 to 6 months, but can be seen in calves as young as 1 month or in cattle as old as 3 years. There have been reports of fetal involvement with the calf form.314 Calves generally present with a history of slight to moderate depression, weight loss, weakness (mainly in older calves and despite good appetite), or lymphadenopathy (mainly in younger calves).315 The onset of signs can be sudden (within a week).
Physical examination may reveal generalized bilateral enlargement of lymph nodes, particularly the deep cervical and parotid nodes and occasionally the popliteal and hemonodes. Moderate to marked enlargement may be noted for the iliac and mandibular nodes. Rarely, node enlargement is not generalized but is restricted to a regional anatomic site.313,315 Enlarged nodes tend to be smooth and firm and are not hot or painful. Mucous membranes are usually pale as a result of anemia. Tachycardia, tachypnea, hyperpnea, cough, and harsh respiratory sounds may be evident on auscultation. Less frequently reported signs include fever, ruminal tympany, an enlarged liver, ataxia, and diarrhea.315
Hematologic features include a microcytic hypochromic anemia, low hemoglobin concentration (<7 g/100 mL),316 low PCV (typically mid-20s), and a leukocytosis primarily caused by a lymphocytosis.313,315-317 Bone marrow examinations may reveal an elevated myeloid/erythroid ratio, with massive neoplastic infiltration in some calves.316 Affected calves also tend to have low serum globulin and elevated AST. Neoplastic involvement of a variety of organs, including the spleen, heart, kidney, liver, pancreas, uterus, and thymus, may occur.313,315,316 Less thymic involvement occurs compared with the thymic form of lymphoma; neoplastic tissue is found only as small, microscopic nodules.316 Subperiosteal neoplastic infiltration may produce spinal cord compression and result in paresis.316 The disease is rapidly progressive and usually fatal within 2 to 8 weeks of onset.
THYMIC OR ADOLESCENT FORM
The thymic form of lymphoma is very rare. The disease is usually seen in cattle 6 to 24 months of age but may occur in newborn calves and cattle up to 4 years of age.315 Clinical signs are produced by space-occupying lesions in the neck or thorax.318 Metastatic mammary lymphoma along with thymic lymphoma was reported in a 3-year-old beef heifer.319 Cattle with thymic lymphoma typically present with brisket enlargement or firm swelling in the presternal area of the brisket, associated with pitting edema.320 Loss in body condition, rumen tympany, and dysphagia are common. Bloat may occur as a result of inability to eructate ruminal gas as a result of a space-occupying lesion around the esophagus.318 Although generalized lymphadenopathy is uncommon, enlarged superficial cervical and prescapular nodes are usually observed. The jugular veins are distended and nonpulsating; there may be muffled heart sounds and diminished resonance on thoracic percussion. Tachycardia, dyspnea, coughing, or respiratory distress may be present. Hematologic features are generally unremarkable. Anemia is not a consistent feature, and lymphocytosis is only seen occasionally. The course of the disease from the time of recognition is generally from 2 to 9 weeks, but poor condition may have been present for several months before presentation.321 The disease is fatal, often as a consequence of bloat.
Although thymic lymphoma is not associated with BLV infection, there has been one report of a BLV-positive 18-month-old heifer with thymic lymphoma. In situ PCR was used to detect the presence of BLV proviral DNA in lymphocytes of the thymus and in liver and kidney epithelium.322
ATYPICAL FORMS
A 7-month-old Holstein heifer with diffuse swelling over the left thigh, difficult ambulation, and peroneal and tibial nerve deficit had an infiltrative B-cell lymphoma involving the semitendinosus, semimembranosus, and gluteal muscles.323 This heifer was serologically positive for BLV antibody, but the possibility of maternally derived antibody could not be ruled out. In another case report, the external and internal surfaces of the trachea of an 18-month-old Friesian heifer with cutaneous lymphoid tumors also had extensive lymphoid nodules covering the external and luminal surfaces of the trachea.324 An 8- to 9-year-old beef cow with weight loss was reported with pleural and pericardial invasion with a lymphoid tumor of T-cell lineage; the animal tested negative for BLV on PCR.325 Four of 10 cattle 3 years of age or younger diagnosed with sporadic lymphoma had BLV provirus in tumor DNA, as detected by PCR, and a possible role for BLV in some cases of sporadic lymphoma of cattle has been suggested.326
CUTANEOUS FORM
Cutaneous lymphoma is not as age specific as the other forms of sporadic lymphoma and may affect cattle between 1 and 3 years of age. The history may reveal an initial period of 1 to 3 months during which cutaneous swellings are observed around the anus, vulva, escutcheon, shoulders, or flank. These signs may regress and subsequently recur.327 Lesions tend to be raised and can be ulcerated. They are generally about 2 to 3 cm in diameter with necrotic centers and may be painful on palpation. Other clinical signs depend on additional organ system involvement of the tumor and may include cardiac insufficiency, with brisket edema extending along the ventral abdomen and jugular pulsation. Pulse and respiration may be elevated as a result of anemia. Hematologic features include anemia and presence of atypical lymphocytes. The mandibular, prescapular, prefemoral, and supramammary lymph nodes are usually enlarged.328
At necropsy, a variety of organs may be involved, including heart, brain, skin, spinal cord, liver, lung, kidney, and abomasum. The massive lymphoid infiltration of the skin resembles the clinical manifestations of mycosis fungoides of humans.314 In a report of a 12-month-old red Holstein heifer with cutaneous T-cell lymphoma, serum activity of lactate dehydrogenase (LDH) was moderately increased despite normal to minimally increased activities of liver and muscle specific enzymes.329
HEMONODE ENLARGEMENT (HEMAL LYMPH NODE)
A lymphoproliferative condition associated with hemonode enlargement and some generalized lymphadenopathy has been described for cattle infected with a lentivirus321 that is now called bovine immunodeficiency virus (BIV). BIV belongs in the genus Lentivirus, subfamily Orthoretrovirinae, and family Retroviridae. BIV has molecular similarity to human immunodeficiency virus (HIV) and is associated with persistent lymphocytosis, lymphadenopathy, central nervous system (CNS) lesions, progressive weakness, and emaciation.330 Infected calves may develop enlarged superficial nodes (hemonodes), mainly in the cervical region anterior and dorsal to the prescapular lymph node, over the spine of the scapula, in the paralumbar fossa, and dorsal to the prefemoral lymph node. Lymphocytosis may be related to an increase in B lymphocytes. In utero transmission of BIV has also been documented.331
Adult Lymphoma (Bovine Leukemia Virus)
The adult or enzootic form of lymphoma is the most common neoplastic disease of cattle and is associated with BLV infection. Rates of lymphoma in cattle vary considerably, probably reflecting variation in BLV infection rates. In 1978 the U.S. condemnation of carcasses because of lymphoma was reported to be 170 per 100,000 head slaughtered.332 A high condemnation rate, sometimes exceeding 1%, was reported for slaughtered California dairy cows,333 and about 1.73% of BLV-infected cattle had lymphoma.334 The rate of cattle condemnations resulting from lymphoma appears to have increased over time.333
Epidemiology
The epidemiology of adult lymphoma is not completely understood. Herd size might be positively correlated with a high rate of lymphoma, which may reflect higher rates of BLV infection in large herds or a preponderance of susceptible pedigrees in some of the herds studied.334,335 Susceptibility to BLV infection is associated with BoLA type,336,337 which may explain why higher rates of lymphoma are found in certain families of cattle. The progression of disease to lymphocytosis in some BLV-infected cows may also be influenced by BoLA type, suggesting a possible genetic predisposition to development of lymphoma through the antigens of the major histocompatibility complex (MHC) encoded at closely linked loci. Other potentially contributing factors, including nutrition, concurrent infections, and environmental/meteorologic stressors, have not been explored sufficiently. There is no evidence for a seasonally associated pattern to appearance of clinical lymphoma.333 Antigenic and molecular evidence for the presence of BLV in mammary glandular epithelium has been demonstrated.338 The effect of persistent mammary BLV infection on the mammary gland is not completely understood. Although one study identified increased average milk production in BLV-infected versus uninfected cattle,339 others report negative associations between milk production and BLV status.340,341
Economics
The economic importance of adult lymphoma varies according to production type.341,342 Producers incur losses from lymphoma associated with death of cattle (particularly genetically valuable livestock), loss of milk production, costs of treatment and diagnosis, and premature replacement costs for cattle dying or culled as a result of lymphoma. The latter may partly explain an observed increased rate of culling found for BLV-infected dairy cattle.339,343 In addition to premature culling and replacement, losses are incurred because of failure to retain salvage value of cows condemned for lymphoma at slaughter.333 A hidden cost of lymphoma also may be in the perpetuation of BLV-infected cattle through in utero infection of calves born to cows with lymphoma.344,345
Diagnosis
Cattle presented with the adult or enzootic form of lymphoma usually are older than 4 years but may be as young as 2 years. Cattle are often presented with a history of loss in condition, an abrupt drop in milk production (over a few days), enlarged peripheral nodes, exophthalmos, or partial to complete anorexia, particularly with regard to grain or concentrates. Because dry cows are not observed as closely as lactating cows and are not monitored for milk yield, lymphoma is less likely to be recognized until they freshen. Subclinical lymphoma may be diagnosed in cows submitted for routine reproduction examinations; other signs may include diarrhea, ataxia, paresis, ketosis, and infertility.
Physical examination often reveals an organ system failure resulting from tumor involvement. Thoracic auscultation may reveal cardiac dysrhythmia, tachycardia, tachypnea, and hyperpnea. Common sites of lymphoid tumor predilection in adult lymphoma include right atrium, uterus, retrobulbar space, abomasum, and spinal cord (epidural space); involvement of rumen, colon, and kidney is also seen. Dependent, pitting edema is common when cervical or supramammary lymph nodes are involved. Involvement of the intestinal lymphatics is often associated with generalized dependent edema anterior to the udder. Peripheral nodes typically found to be enlarged are the prescapular, femoral, and supramammary nodes. Feces may be scant, pasty, or watery and probably reflects the presence of lesions within the GI tract. Melena may be present in animals with ulceration of the abomasum and lymphoid cell infiltration in the abomasal wall. Rectal palpation can be a useful in cases lacking peripheral node enlargement or exophthalmos. Tumor masses palpated in the abdomen typically are multiple and range in size from only slightly enlarged lymph nodes to massive lesions half a meter in diameter. The internal iliac nodes are involved in most cattle with abdominal tumors.
Tumors tend to be firm but not hard and may feel slightly lobulated. Differentiation by palpation of lymphoma tumors from other masses is highly subjective. Carcinomas tend to be of similar consistency but are seldom larger than 15 cm in diameter and are usually associated with intestinal tissue. Lymph nodes of cows with a carcinoma are not usually enlarged unless a secondary infection is present. Melanomas are generally less than 15 cm in diameter and hard, sometimes with protrusions 1 to 2 cm high along the surface. They usually are not found associated with lymph nodes. Masses of fat necrosis tend to be firm and are usually associated with omental tissue. Internal abscesses are often single and associated with the uterus, as a consequence of uterine tear and infection during parturition, or with gluteal muscles of the pelvic ceiling, as a consequence of injection-related infections. Exploratory laparotomy may be indicated as an additional diagnostic tool in difficult cases, particularly in valuable cattle.
The hemogram of cattle with lymphoma often is generally unremarkable. Anemia, characterized as microcytic and hypochromic, may be present in cattle with GI hemorrhage. Fibrinogen levels have been inconsistent in lymphoma, and therefore its measurement may be helpful only in differentiating an abscess. Approximately 30% of cattle with BLV infection develop persistent lifelong lymphocytosis, composed mostly of B cells.346,347
Cytology of aspirates of tumors or tumorous nodes may not always be a reliable diagnostic tool, although it can be helpful. Discrimination cannot be made between a normal node responding to an infectious agent and a node involved with neoplastic lymphocytes; in both situations, cells resembling young, poorly differentiated lymphocytes may be present. Examination of nontumorous active lymph nodes may reveal an elevated proportion of large, young lymphocytes that could resemble those of lymphosarcoma. Histopathologic examination of biopsied tumors or nodes may be more useful than aspirates in making a diagnosis. However, cytology and culture of aspirates could be helpful in differentiating a tumor from an abscess. Failed attempts at collection of cerebrospinal (lumbosacral) fluid in cattle with recumbency or hindlimb weakness may be associated with the presence of lymphoid tumors in the vertebral canal; cytologic examination of cells from the collection needle in such cases may reveal abnormal lymphoid cells.
Standard serologic testing for BLV involves identification of antibody against the 51-kilodalton (kD) envelope glycoprotein (gp51). Although BLV diagnosis historically involved the use of the agar gel immunodiffusion (AGID) test, that method has been shown to be less sensitive than the enzyme-linked immunosorbent assay (ELISA).348 ELISA test kits are available commercially that detect antibodies to gp51 in serum and milk.* Diagnosis is also possible by use of PCR to detect BLV nucleic acid,349-351 as well as by a combined PCR-ELISA that is more sensitive than staining of PCR amplicons with ethidium bromide.352 ELISA-positive cattle that were not detected by PCR testing have been reported, most likely related to a low number of infected circulating lymphocytes at sample collection.353 The PCR by itself is considered unreliable for routine detection of BLV in herds with a high prevalence of disease.354 The ability of PCR to detect a BLV infected animal is improved by means of a nested PCR, which was reported to be effective in diagnosing infection when seroconversion had not yet occurred.355 The presence of antibodies to gp51 is generally considered to be a prerequisite to a diagnosis of lymphoma, except for cows during the periparturient period, when circulating antibodies may fall below the level detectable by a serologic test.356 The mere presence of BLV antibodies does not necessarily mean that an animal has lymphoma, which is found in only about 1.7% of BLV-infected cattle.357 However, serology can be helpful in predicting the chance of lymphoma in cattle seropositive to the gp51 antigen. Sera from cattle with lymphoma generally have high titers to the gp51 antigen (score of 3 or 4 on AGID), compared with those of infected cattle without lymphoma (score of 1 or 2). In addition, cattle that do not have lymphoma tend not to have antibodies to the p24 antigen of BLV, as detected by AGID. The percentage of cattle with histologically confirmed lymphoma but in which lymphoma was not diagnosed by a gp51-positive and p24-negative test result (false-negative rate of diagnostic test) has been found to be only 0.21%, using the AGID test.334 Unfortunately, most diagnostic laboratories do not have the capability to perform the test using the p24 antigen.
At necropsy, tumors are found enclosed in a capsular-like tissue that, when sectioned with a knife, results in an eversion of tumor stroma. Cut tumor tissue is cream colored and friable, with little binding structure. Centers of tumors may appear necrotic and mushy, whereas peripheral regions are firmer and pink to white. Histopathology provides the only definitive diagnosis. Tissue should be biopsied by surgical removal of as much of the node (or mass) as possible.