TCM diagnosis and treatment of recurrent miscarriage
Once physical uterine and cervical disorders, inherited genetic disorders, sperm and ova defects due to occupational toxic exposure and complications from other diseases or medications are all ruled out, then the Chinese medicine practitioner can apply his diagnostic skills and determine if there is another, perhaps more subtle, reason for recurrent miscarriage.
Acupuncture and Chinese herbs have been used for many centuries in the treatment of recurrent miscarriage. Of course, if pregnancy loss is recurrent, then it is reasonable to think that there is a persistent factor in one or both of the would-be parents. Thus, recurrent miscarriage lends itself a little more to the sort of treatment that TCM offers (i.e., preventative treatment ahead of the fact) than does a miscarriage, which is already threatening and which in many cases is due to a lethal chromosomal defect.
The TCM doctor would traditionally diagnose the nature of the recurrent miscarriage according to the constitution of the female partner. Nowadays, in the light of new knowledge, the male partner will be assessed too.
The categories into which TCM divides recurrent miscarriage are the same as those for threatened miscarriage with subtle differences. The clinical approach, however, is quite distinct in the two cases. In the former, we have an acute situation with little time in which to make a difference. Treatment must be applied to address the disorder and at the same time, calm the fetus. If the disorder is serious, then there may be little chance of saving the pregnancy. However, in the case of recurrent miscarriage, we can allow plenty of time (preferably ≥6 months) to correct the problem before conception is attempted again. Herbs which calm the fetus are not necessary and, more importantly, we do not have to avoid herbs or points which are contraindicated in pregnancy.
Categories of recurrent miscarriage are as follows:
Kidney deficiency
Kidney deficiency is the most common pathology underlying both infertility and miscarriage. For threatened miscarriage due to Kidney deficiency, Kidney Yang was our prime treatment target. In the case of recurrent miscarriage, we will treat both Kidney Yin and Yang if necessary. Kidney Yin deficiency is a prime cause of infertility and women with Kidney Yin deficiency may have as much difficulty becoming pregnant as they do staying pregnant. Treatment of such women is necessarily quite long term – the Yin must be recovered so that the egg develops well and the endometrium is thick and secretory. This can take time in the case of a woman who is very Yin-deficient and, since this happens more often in older women, we are confronted with a dilemma. Older women (and Yin-deficient women with Yin-deficient Heat) are impatient to conceive and it is often a difficult task for the practitioner to persuade them of the wisdom of preparing their body first. In cases of recurrent miscarriage due to Kidney Yin deficiency, pregnancy attempts should be avoided for at least three or four menstrual cycles to give time to build the Yin. Most women can understand that risking having repeated miscarriages is very damaging, but the pressure of time ticking by is strong once the woman is already in her late 30s or has turned 40.
For most women who miscarry more than once, it is important to build and balance the Kidney Yin and Yang before the next attempt to conceive. This is achieved best by following a simplified version of the protocols described in Chapter 4. Thus, building Kidney Yin is emphasized in the pre-ovulatory or post-menstrual phase and Kidney Yang in the post-ovulatory phase.
Post-menstrual phase
Herbal formula: The formula of choice is:
Gui Shao Di Huang Tang (Angelica Peonia Rehmannia decoction)
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Bai Shao | 9 g | Radix Paeoniae Lactiflorae |
| Shu Di | 9 g | Radix Rehmanniae Glutinosae Conquitae |
| Shan Zhu Yu | 9 g | Fructus Corni Officinalis |
| Shan Yao | 9 g | Radix Dioscorea Oppositae |
| Fu Ling | 12 g | Sclerotium Poriae Cocos |
| Mu Dan Pi | 6 g | Cortex Moutan Radicis |
| Ze Xie | 9 g | Rhizoma Alismatis |
This is the well-known formula for strengthening Kidney and Liver Yin, Lui Wei Di Huang Wan, with the addition of two Blood tonics Dang Gui and Bai Shao. (It is explained in Ch. 4.)
To reinforce the Yin further, add:
| Nu Zhen Zi | 12 g | Fructus Ligustri Lucidi |
| Han Lian Cao | 9 g | Herba Ecliptae Prostratae |
Where Kidney Yang is constitutionally weak (sore lower back, frequent urination), add:
| Tu Si Zi | 9 g | Semen Cuscatae |
Acupuncture points: Choose from the following points (and see Table 8.9):
Table 8.9
Acupuncture pointsa used in the treatment of recurrent miscarriage due to Kidney weakness, post-menstrual phase
| Treatment goal | Acupuncture points |
| To reinforce Kidney Yin | Ren-4 and KI-3 |
| To reinforce Kidney Yin and clear Heat | KI-6 |
| To regulate the activity of the Chong and Ren vessels | Ren-7, KI-5 and KI-13 |
| To influence Kidney Jing | ST-27 |
| To supplement Liver Yin and Blood | LIV-8 |
| Ren-4 | Guanyuan |
| KI-13 | Qixue |
| Ren-7 | Yinjiao |
| ST-27 | Daju |
| KI-3 | Taixi |
| KI-5 | Shuiquan |
| LIV-8 | Ququan |
| KI-6 | Zhaohai |
Post-ovulation phase
Herbal formula: The formula of choice is:
Bu Shen Gu Chong Tang (Reinforce the Kidneys, Consolidate the Chong Channel decoction) modified
| Xu Duan | 9 g | Radix Dipsaci |
| Ba Ji Tian | 9 g | Radix Morindae Officinalis |
| Du Zhong | 9 g | Cortex Eucommiae Ulmoidis |
| Tu Si Zi | 9 g | Semen Cuscatae |
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Shu Di | 9 g | Radix Rehmanniae Glutinosae Conquitae |
| Gou Qi Zi | 12 g | Fructus Lycii Chinensis |
| Dang Shen | 12 g | Radix Codonopsis Pilulosae |
| Bai Zhu | 12 g | Rhizoma Atractylodis Macrocephalae |
| Da Zao | 3 pieces | Fructus Zizyphi Jujuba |
| Sha Ren | 3 g | Fructus seu Semen Amomi |
Xu Duan, Ba Ji Tian, Du Zhong, and Tu Si Zi all support the Kidney Yang, whereas Shu Di and Gou Qi Zi reinforce Kidney and Liver Yin and with Dang Gui, the Blood. Dang Shen, Bai Zhu, Da Zao, and Sha Ren are added to invigorate Spleen Qi. This formula can be continued during the first few weeks of pregnancy.
Acupuncture points: Choose from the following points (and see Table 8.10):
Table 8.10
Acupuncture pointsa used in the treatment of recurrent miscarriage due to Kidney deficiency, post-ovulation phase
| Treatment goal | Acupuncture points |
| To supplement Kidney Yang | Ren-4b, BL-23 and KI-3 |
| To support the Kidney and stabilize the emotions | KI-4 |
| To clear Liver-Heat | LIV-2 |
aPoints are reinforced with the exception of LIV-2, which is reduced.
bRen-4 is used only before and at midcycle in cycles where pregnancy is attempted. In other cycles, it can be used with no restriction.
| Ren-4 | Guanyuan |
| BL-23 | Shenshu |
| KI-3 | Taixi |
| KI-4 | Dazhong |
| LIV-2 | Xingjian |
Watching clinical markers such as the quality of the cervical mucus, the shape of the BBT chart and the nature of the period can help us to assess progress. Of course, the vitality and well-being of the woman will also tell us about improved Kidney energy.
Women with Kidney deficiency tend to miscarry early in the pregnancy. In the case of Kidney Yang failing, this can be so early, as to seem like a slightly late period and the miscarriage may only be detected if BBT charts have been kept.
It may also be the case that there is significant preimplantation loss in women with Kidney deficiency; some of these women may have been told they have a luteal phase defect (see Ch. 4). We prescribe the herbs discussed above to help prepare the endometrium for successful implantation and establishment of a pregnancy. Whether this is by promoting upregulation of implantation factors or modulation of immune factors or increasing progesterone levels, we don’t yet know. Studies of some Kidney tonic formulas have reported significant increases in the expression of growth factors and receptors and suggested that these could promote implantation and reduce risk of pregnancy loss.71
CASE HISTORY – ARIELLA
Ariella (38) said she fell pregnant as soon as she looked at a double bed. But just as soon as she got the positive test result, she would start bleeding. Once she got as far as 7 weeks, but then the bleeding came again. After four miscarriages, she was emotionally wrung out and terrified of becoming pregnant and miscarrying again. All her blood tests showed nothing wrong, and her chromosomes did not seem to be incompatible with her husband’s.
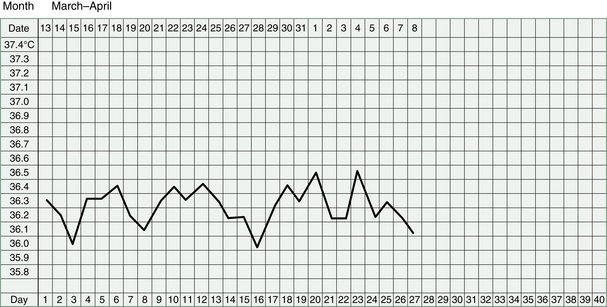
Ariella agreed to not ‘look at a double bed’ for 3 months, while we fortified her Kidney Yang. Her cycle was short and her BBT charts showed a low and short luteal phase. Her health, however, was for the most part, excellent. Occasionally, she felt some period pain but this was mild, and slightly loose stools before her periods was the only clear symptom of Kidney Yang deficiency. In situations like this, the BBT chart (Fig. 8.3) plays an essential role in diagnosis.
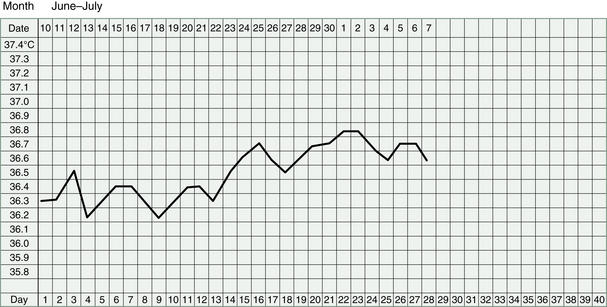
She took herbs to increase her Kidney Yang throughout her menstrual cycle and by the 3rd month, her BBT chart showed a convincing luteal phase (Fig. 8.4). This type of recurrent miscarriage (or infertility) is one of the most rewarding to treat because results usually come quickly, unlike problems with Kidney Yin deficiency.
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Bai Shao | 9 g | Radix Paeoniae Lactiflorae |
| Shu Di | 9 g | Radix Rehmanniae Glutinosae Conquitae |
| Shan Zhu Yu | 9 g | Fructus Corni Officinalis |
| Shan Yao | 9 g | Radix Dioscorea Oppositae |
| Fu Ling | 12 g | Sclerotium Poriae Cocos |
| Mu Dan Pi | 6 g | Cortex Moutan Radicis |
| Ze Xie | 9 g | Rhizoma Alismatis |
| Ba Ji Tian | 6 g | Radix Morindae Officinalis |
| Tu Si Zi | 9 g | Semen Cuscatae |
This formula she took each month before ovulation.
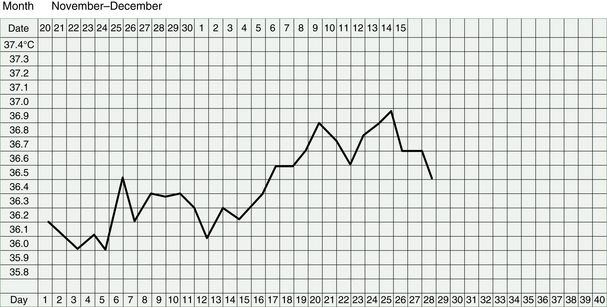
Figure 8.4 Case history – Ariella. This chart shows an improved luteal phase after having treatment for 3 cycles.
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Shu Di | 9 g | Radix Rehmanniae Glutinosae Conquitae |
| Gou Qi Zi | 12 g | Fructus Lycii Chinensis |
| Dang Shen | 12 g | Radix Codonopsis Pilulosae |
| Bai Zhu | 12 g | Rhizoma Atractylodis Macrocephalae |
| Shan Yao | 9 g | Radix Dioscorea Oppositae |
| Ba Ji Tian | 6 g | Radix Morindae Officinalis |
| Tu Si Zi | 15 g | Semen Cuscatae |
| Du Zhong | 9 g | Cortex Eucommiae Ulmoidis |
| Xu Duan | 9 g | Radix Dipsaci |
| Da Zao | 3 pieces | Fructus Zizyphi Jujuba |
| Sha Ren | 3 g | Fructus seu Semen Amomi |
This formula she took each month after ovulation.
Ariella fell pregnant soon after, and took more herbs to prevent miscarriage:
| Tu Si Zi | 15 g | Semen Cuscatae |
| Sang Ji Sheng | 15 g | Ramulus Sangjisheng |
| Du Zhong | 9 g | Cortex Eucommiae Ulmoidis |
| Xu Duan | 9 g | Radix Dipsaci |
| Bai Zhu | 9 g | Rhizoma Atractylodis Macrocephalae |
| E Jiao | 6 g | Gelatinum Asini |
Qi deficiency
If Spleen Qi deficiency is seriously compromised, there may be a problem with the uterus dropping and the cervix not staying firmly closed and holding the pregnancy. Cervical incompetence usually causes a problem after about 14 or 15 weeks of pregnancy, when the fetus is starting to grow larger and the Uterus to stretch. Several months of treatment to lift and strengthen the uterus prior to conception may help in future pregnancies. However, the woman with a history of cervical incompetence would always be well advised to get a suture in the cervix as well, once she was 14 weeks into a pregnancy.
Herbal formula: The formula of choice is:
Bu Zhong Yi Qi Tang (Reinforce the Center and Benefit the Qi decoction) modified
| Huang Qi | 15 g | Radix Astragali |
| Dang Shen | 12 g | Radix Codonopsis Pilulosae |
| Bai Zhu | 9 g | Rhizoma Atractylodis Macrocephalae |
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Chen Pi | 6 g | Pericarpium Citri Reticulate |
| Sheng Ma | 6 g | Rhizoma Cimicifugae |
| Chai Hu | 6 g | Radix Bupleuri |
| Gan Cao | 3 g | Radix Glycyrrhizae Uralensis |
| Wu Zei Gu | 9 g | Os Sepia seu Sepiellae |
Dang Shen, Bai Zhu, and Gan Cao invigorate the Spleen Qi, Huang Qi, Sheng Ma, and Chai Hu lift the Uterus, and Chen Pi keeps the Qi moving. Dang Gui and Bai Zhu are often used together to both nourish the Blood and the Qi to help prevent further miscarriages. Wu Zei Gu provides an astringent action to prevent leakage and opening of the Uterus.
To concurrently reinforce the Kidneys, add:
| Tu Si Zi | 9 g | Semen Cuscatae |
| Bu Gu Zhi | 9 g | Fructus Psoraleae |
| Shan Yao | 9 g | Dioscorea Oppositae |
Tu Si Zi builds Kidney Yin and Yang and the Spleen, Bu Gu Zhi builds both Spleen and Kidney Yang, and Shan Yao reinforces Spleen Qi and Yin and the Kidneys.
Acupuncture points: Choose from the following points (and see Table 8.11):
Table 8.11
Acupuncture pointsa used in the treatment of recurrent miscarriage due to Qi deficiency
| Treatment goal | Acupuncture points |
| To lift the Qi and the organs, in this case the Uterus | DU-20 |
| To reinforce the Spleen Qi | ST-36, Ren-12, Ren-6 |
| To supplement the Kidney Yin and Yang | Ren-4b |
| To regulate the Qi in the Spleen, Liver and Kidney channels | SP-6 |
aReinforcing or even method is used.
bRen-4 and SP-6 are used only before and at midcycle in cycles where pregnancy is attempted. In other cycles, they can be used with no restriction.
| DU-20 | Baihui |
| Ren-6 | Qihai |
| Ren-12 | Zhongwan |
| Ren-4 | Guanyuan |
| ST-36 | Zusanli |
| SP-6 | Sanyinjiao |
Blood deficiency
If Yin deficiency leads to Blood deficiency, then the endometrium will be thin and may not be conducive to effective implantation, or may not be able to nourish a fetus adequately if implantation is successful. If Qi deficiency is accompanied by Blood deficiency, then the fetus may fail to grow and thrive and will appear small-for-dates on ultrasound tests.
Herbal formula: Give Gui Shao Di Huang Tang (Angelica Peonia Rehmannia decoction) for Yin and Blood deficiency or give the following guiding formula for Blood deficiency with Qi deficiency:
Ba Zhen Tang (Eight Precious decoction)
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Bai Shao | 9 g | Radix Paeoniae Lactiflorae |
| Chuan Xiong | 6 g | Radix Ligustici Wallichii |
| Shu Di | 9 g | Radix Rehmanniae Glutinosae Conquitae |
| Dang Shen | 12 g | Radix Codonopsis Pilulosae |
| Bai Zhu | 9 g | Rhizoma Atractylodis Macrocephalae |
| Fu Ling | 12 g | Sclerotium Poriae Cocos |
| Gan Cao | 3 g | Radix Glycyrrhizae Uralensis |
This formula was mentioned above, where it was prescribed for recovery after miscarriage with an increased dose of Dang Gui.
When treating recurrent miscarriage, it is appropriate to add more Kidney tonics to the formula, e.g.:
| Huang Jing | 9 g | Rhizoma Polygonati |
| Tu Si Zi | 9 g | Semen Cuscatae |
| Sang Ji Sheng | 15 g | Ramulus Sangjisheng |
| Shan Zhu Yu | 9 g | Fructus Corni Officinalis |
Huang Jing reinforces Qi and Kidneys; Tu Si Zi reinforces Kidney Yin and Yang; Sang Ji Sheng nourishes the Blood, Kidneys, and Liver; Shan Zhu Yu nourishes Kidney Yin and Jing, and provides an astringing action to prevent leakage from the uterus.
Acupuncture points: Choose from the following points (and see Table 8.12):
Table 8.12
Acupuncture pointsa used in the treatment of recurrent miscarriage due to Blood deficiency
| Treatment goal | Acupuncture points |
| To strengthen Spleen and Stomach and encourage Blood production | BL-17, BL-20, BL-23, Ren-12, ST-36 |
| To build Blood in the uterus | Ren-4b |
| To regulate Blood in the uterus | ST-28b |
aReinforcing or even method is used.
bRen-4 and ST-28 are used only before and at midcycle in cycles where pregnancy is attempted. In other cycles, they can be used with no restriction.
| BL-17 | Geshu |
| BL-20 | Pishu |
| BL-23 | Shenshu |
| Ren-12 | Zhongwan |
| ST-36 | Zusanli |
| Ren-4 | Guanyuan |
| ST-28 | Shuidao |
Heat in the Blood
As was the case for threatened miscarriage, the Heat which causes repeated miscarriages mostly arises from Kidney Yin deficiency. In some cases, it comes from severe mental agitation, causing Liver- or Heart-Fire; this latter can interfere with the normal ‘opening and closing’ functions of the uterus. The timing of ovulation and periods may be affected, as well as the ability of the uterus to hold a pregnancy. We can use the same guiding formula here as we used for a pregnancy under threat by Heat in the Blood, but because we are applying preventative treatment, we can expand on the formula and use acupuncture points we may have been hesitant to use on a pregnant woman.
Herbal formula: In the case of long-term endometritis or PID causing the Heat, a combination of herbal medicine, acupuncture and allopathic medicine may be necessary.
Bao Yin Jian (Protecting Yin decoction) modified
| Sheng Di | 9 g | Radix Rehmanniae Glutinosae |
| Xuan Shen | 9 g | Radix Scrophulariae |
| Shan Yao | 12 g | Radix Dioscorea Oppositae |
| Bai Shao | 9 g | Radix Paeoniae Lactiflorae |
| Huang Qin | 6 g | Radix Scutellariae Baicalensis |
| Huang Bai | 6 g | Cortex Phellodendri |
| Di Gu Pi | 9 g | Cortex Lycii Chinensis |
| Nu Zhen Zi | 9 g | Fructus Ligustri Lucidi |
| Han Lian Cao | 9 g | Herba Ecliptae Prostratae |
| Suan Zao Ren | 15 g | Semen Ziziphi Spinosae |
| Gan Cao | 3 g | Radix Glycyrrhizae Uralensis |
Sheng Di and Xuan Shen cool the Blood; Di Gu Pi clears Yin deficient Heat, while Huang Bai and Huang Qin are used to remove Heat and Damp specifically from the pelvic area. Bai Shao and Suan Zao Ren soothe the Liver; Nu Zhen Zi and Han Lian Cao protect the Yin, and Shan Yao the Spleen.
Acupuncture points: Choose appropriate points from the following (and see Table 8.13):
Table 8.13
Acupuncture pointsa used in the treatment of recurrent miscarriage due to Heat in the Blood
| Treatment goal | Acupuncture points |
| To cool the Blood | SP-10 and CO-11 |
| To clear Yin-deficient Heat from the Uterus | KI-6 and KI-2 |
| To clear Liver-Fire | LIV-2 |
| To clear Heart-Fire and Heat in the Blood and safeguard the Bao vessels | HE-5 |
| To cool the Blood and calm the spirit | PC-3 |
| To harmonize Heart and Kidney | KI-3 |
aReducing or even method is applied except in the case of KI-6, which is reinforced.
| SP-10 | Xuehai |
| KI-6 | Zhaohai |
| KI-2 | Rangu |
| LIV-2 | Xingjian |
| HE-5 | Tongli |
| PC-3 | Quze |
| CO-11 | Quchi |
| KI-3 | Taixi |
If Heat in the Blood is contributed to by diet, then this should be adjusted in the ways suggested in Chapter 9. If Heat in the Blood is contributed to by emotional factors, then steps to reduce stress should be taken. Even where emotional factors are not the initial cause of Heat in the Blood, they should be considered in women who suffer recurrent miscarriages because there will always be a degree of anxiety and fear. Restlessness and anxiety can be particularly marked in this pattern due to the Heat but should respond favorably to acupuncture and herbal treatment.
Blood stagnation
Women with a history of endometriosis, endometritis, fibroids, cysts, and abdominal surgery are likely to have a degree of Blood stagnation. Sometimes, this can impact unfavorably on pregnancy, especially if there is obstruction, scarring or damage to the endometrium which interferes with placental attachment. If large fibroids are deemed to be a risk for implantation, then surgery is often recommended, as is also the case for polyps. In the case of endometriosis, in which Kidney Yang is frequently a contributing factor, pregnancies may be at risk from inadequate corpus luteum function, increased inflammation, immune system disturbance and disordered blood supply to the endometrium, all of which can impede successful implantation and development of the placenta and therefore increase the risk of miscarriage.
Herbal formula: Our guiding formula in this case can be stronger than that employed for threatened miscarriage with Blood stagnation. While the following herbs are being consumed, it is important that pregnancy is avoided.
Shao Fu Zhu Yu Tang (Lower Abdomen Eliminating Stasis decoction)
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Chi Shao | 6 g | Radix Paeoniae Rubra |
| Chuan Xiong | 6 g | Radix Ligustici Wallichii |
| Yan Hu Suo | 9 g | Rhizoma Corydalis Yanhusuo |
| Mo Yao | 6 g | Myrrha |
| Pu Huang | 9 g | Pollen Typhae |
| Wu Ling Zhi | 6 g | Excrementum Trogopterori |
| Xiao Hui Xiang | 6 g | Fructus Foeniculi Vulgaris |
| Gan Jiang | 3 g | Rhizoma Zingiberis Officinalis |
| Rou Gui | 3 g | Cortex Cinnamomi Cassiae |
Dang Gui, Chi Shao, Chuan Xiong, Yan Hu Suo, Mo Yao, Pu Huang, and Wu Ling Zhi all help to invigorate the Blood. Xiao Hui Xiang, Gan Jiang, and Rou Gui warm the uterus and expel Cold: in cases where this formula is too heating for a patient, these last three herbs will be reduced or removed.
This formula should be administered before and during the period to regulate Blood stagnation. If there are symptoms of Blood stagnation (i.e., pain) at other times of the cycle, it may be administered then too. At other times, Kidney tonic formulas should be given (see Kidney deficiency, above) or, alternatively, Kidney tonic herbs can be added to Shao Fu Zhu Yu Tang, namely:
| Nu Zhen Zi | 9 g | Fructus Ligustri Lucidi |
| Xu Duan | 12 g | Radix Dipsaci |
| Tu Si Zi | 9 g | Semen Cuscatae |
In the case of large submucosal fibroids (where surgery is not appropriate or desired), with little complication by Kidney deficiency, consider a variation of Gui Zhi Fu Ling Wan.
Gui Zhi Fu Ling Tang (Ramulus Cinnamomi-Poria decoction) modified
| Dang Gui | 12 g | Radix Angelicae Sinensis |
| Bai Shao | 12 g | Radix Paeoniae Lactiflorae |
| Chuan Xiong | 6 g | Radix Ligustici Wallichii |
| Yi Mu Cao | 9 g | Herba Leonuri Heterophylli |
| San Leng | 12 g | Rhizoma Sparganii |
| E. Zhu | 12 g | Rhizoma Curcumae Zedoariae |
| Tao Ren | 6 g | Semen Persicae |
| Gui Zhi | 6 g | Ramulus Cinnamomi Cassiae |
| Fu Ling | 15 g | Sclerotium Poriae Cocos |
| San Qi | 9 g | Radix Pseudoginseng |
| Wu Ling Zhi | 6 g | Excrementum Trogopterori |
This is a strong formula for reducing fibroid size and should not be taken at the same time as trying to conceive. Gui Zhi Fu Ling Wan, a well known formula for the treatment of masses, disperses Blood stasis and Phlegm Damp accumulation. Stronger stasis moving herbs in the shape of San Leng and E Zhu are added alongside additional Blood moving herbs San Qi, Yi Mu Cao, and Wu Ling Zhi. This formula can also be considered if other factors such as endometriosis, endometritis, or polyps are contributing to recurrent miscarriage.
See also formulas discussed for endometriosis in Chapter 5.
Acupuncture points: Choose points from the following (and see Table 8.14):
Table 8.14
Acupuncture pointsa used in the treatment of recurrent miscarriage due to Blood stagnation
| Treatment goal | Acupuncture points |
| To clear stagnant Blood in the Chong vessel | KI-14b and KI-18 |
| To regulate the Blood in the Chong and Ren vessels | KI-5 |
| To move Blood stagnation from the Uterus, especially if it is associated with Cold | ST-28b and ST-29b |
| To reinforce Kidney function | Ren-4b and Ren-6 |
| To regulate Blood in the Uterus | SP-8 and SP-10 |
| To regulate Qi and Blood in the Bao vessel | PC-5 |
| To release the menstrual flow if it is obstructed and painful | CO-4 with SP-6 |
aPoints are used with reducing method to clear stagnation and stop pain.
bUsed with caution and no manipulation after ovulation in cycles where conception is attempted.
| ST-28 | Shuidao |
| ST-29 | Guilai |
| SP-10 | Xuehai |
| SP-8 | Diji |
| SP-6 | Sanyinjiao |
| KI-14 | Siman |
| KI-18 | Shiguan |
| KI-5 | Shuiquan |
| Ren-4 | Guanyuan |
| Ren-6 | Qihai |
| PC-5 | Jianshi |
| CO-4 | Hegu |
These acupuncture points are applied just before and during the period or when there is pain. Applying moxa to abdomen points can facilitate the moving of Qi and Blood stagnation, providing there is no Heat (inflammation).
CASE HISTORY – GERALDINE
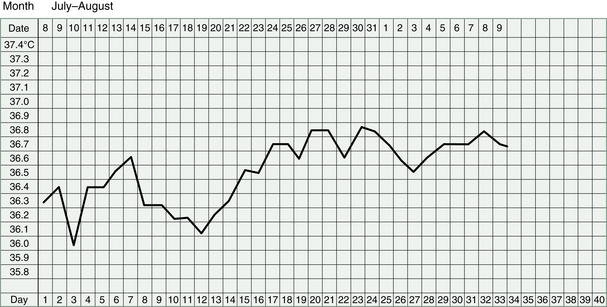
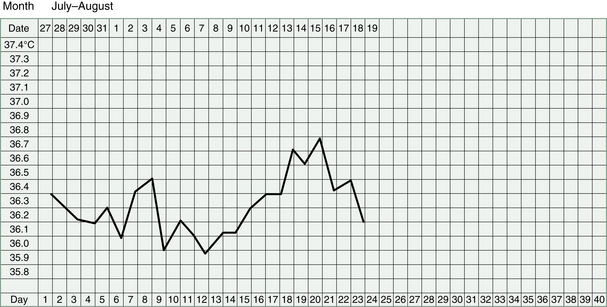
Geraldine (29) had endometriosis, diagnosed on laparoscopy. It was a mild case according to the surgeon who removed some of the lesions and, he explained, it was probably the reason she hadn’t succeeded in becoming pregnant. She had been trying for 2 years: 1 year before and 1 year since the surgery. Her cycle was long and irregular; premenstrually, she experienced breast soreness and abdomen distension; her periods were heavy and clotty and associated with strong pain in the back and abdomen. After the surgery, her periods were less heavy but still somewhat clotty and painful. She had been recording her BBT for the last 9 cycles and a disturbing pattern was evident. In four of the nine charts, her luteal phase was between 19 and 21 days long before a period arrived, indicating early miscarriage (Fig. 8.5). Geraldine didn’t register this possibility because her cycle had always been irregular and her premenstrual symptoms mimicked pregnancy ones.
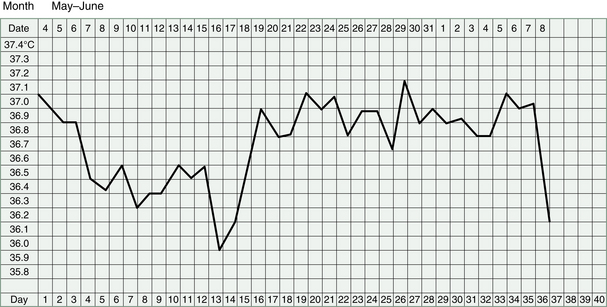
Figure 8.5 Case history – Geraldine. The luteal phase on Geraldine’s BBT charts was sometimes as long as 21 days.
Her pulse was wiry and choppy. Her tongue was normal, except for slight dark discoloration on the right side.
TCM treatment aimed to clear Blood stagnation, regulate Liver Qi, and boost Kidney Yang. She agreed to avoid attempts at pregnancy for 2 cycles, during which time she took strong herbs to remove any endometriosis.
This formula she took for several days before and during the period:
| Gou Teng | 15 g | Ramulus Uncariae cum Uncis |
| Zi Bei Chi | 9 g | Mauritiae Concha |
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Chi Shao | 9 g | Radix Paeoniae Rubra |
| Wu Ling Zhi | 9 g | Excrementum Trogopterori |
| Yan Hu Suo | 9 g | Rhizoma Corydalis Yanhusuo |
| E. Zhu | 9 g | Rhizoma Curcumae Zedoariae |
| Rou Gui | 3 g | Cortex Cinnamomi Cassiae |
| Quan Xie | 1.5 g | Buthus Martensi |
| Wu Gong | 1.5 g | Scolopendra Subspinipes |
| Mu Xiang | 6 g | Radix Saussureae seu Vladimiriae |
| Xu Duan | 9 g | Radix Dipsaci |
The following formula Geraldine took after her period, until after she ovulated (i.e., her temperature rose on the BBT chart):
| Shu Di | 12 g | Radix Rehmanniae Glutinosae Conquitae |
| Shan Yao | 9 g | Radix Dioscorea Oppositae |
| Shan Zhu Yu | 9 g | Fructus Corni Officinalis |
| Fu Ling | 9 g | Sclerotium Poriae Cocos |
| Mu Dan Pi | 9 g | Cortex Moutan Radicis |
| Ze Xie | 12 g | Rhizoma Alismatis |
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Bai Shao | 9 g | Radix Paeoniae Lactiflorae |
| Tao Ren | 6 g | Semen Persicae |
| Hong Hua | 6 g | Flos Carthami Tinctorii |
| Wu Ling Zhi | 6 g | Excrementum Trogopterori |
| Tu Si Zi | 6 g | Semen Cuscatae |
| Rou Cong Rong | 6 g | Herba Cistanches |
| Xu Duan | 6 g | Radix Dipsaci |
The next formula she took for a week after ovulation:
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Chi Shao | 6 g | Radix Paeoniae Rubra |
| Chuan Xiong | 6 g | Radix Ligustici Wallichii |
| Dang Shen | 12 g | Radix Codonopsis Pilulosae |
| Tu Si Zi | 9 g | Semen Cuscatae |
| Lu Jiao Pian | 9 g | Cornu Cervi Parvum |
| Mo Yao | 6 g | Myrrha |
| Pu Huang | 9 g | Pollen Typhae |
| Wu Ling Zhi | 6 g | Excrementum Trogopterori |
| Rou Gui | 3 g | Cortex Cinnamomi Cassiae |
After two cycles, Geraldine once again tried to conceive, so the first formula (above) with the strong Blood-moving herbs was used only when the period arrived. In addition, we added another prescription to be taken for a few days just before and after ovulation:
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Chi Shao | 9 g | Radix Paeoniae Rubra |
| Bai Shao | 9 g | Radix Paeoniae Lactiflorae |
| Shan Yao | 9 g | Radix Dioscorea Oppositae |
| Shu Di | 9 g | Radix Rehmanniae Glutinosae Conquitae |
| Nu Zhen Zi | 9 g | Fructus Ligustri Lucidi |
| Mu Dan Pi | 9 g | Cortex Moutan Radicis |
| Fu Ling | 9 g | Sclerotium Poriae Cocos |
| Xu Duan | 9 g | Radix Dipsaci |
| Tu Si Zi | 9 g | Semen Cuscatae |
| Wu Ling Zhi | 9 g | Excrementum Trogopterori |
| Hong Hua | 6 g | Flos Carthami Tinctorii |
| (Sheng) Shan Zha | 9 g | Fructus Crataegi |
| Dan Shen | 9 g | Radix Salviae Miltiorrhizae |
She took these four different formulas at the appropriate time for the next 4 cycles. Her cycle was now a regular 29 days. The 5th month she fell pregnant and stayed pregnant. Her herbs were changed again:
| Xu Duan | 9 g | Radix Dipsaci |
| Ba Ji Tian | 9 g | Radix Morindae Officinalis |
| Du Zhong | 9 g | Cortex Eucommiae Ulmoidis |
| Tu Si Zi | 9 g | Semen Cuscatae |
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Shu Di | 9 g | Radix Rehmanniae Glutinosae Conquitae |
| Gou Qi Zi | 12 g | Fructus Lycii Chinensis |
| Dang Shen | 12 g | Radix Codonopsis Pilulosae |
| Bai Zhu | 12 g | Rhizoma Atractylodis Macrocephalae |
| Da Zao | 3 pieces | Fructus Zizyphi Jujuba |
| Sha Ren | 3 g | Fructus seu Semen Amomi |