STRUCTURE AND FUNCTION OF THE NEUROLOGIC SYSTEM


The human nervous system is a remarkable structure that is responsible for the body’s ability to reciprocally interact with the environment and for the regulation of activities involving internal organs. The nervous system drives the other systems of the body. It is a network composed of complex structures that transmit electrical and chemical signals between the body’s many organs and tissues and the brain.
OVERVIEW AND ORGANIZATION OF THE NERVOUS SYSTEM
Although the nervous system functions as a unified whole, structures and functions of the nervous system have been divided to facilitate understanding. Structurally, the nervous system is divided into the central nervous system and the peripheral nervous system. The central nervous system (CNS) consists of the brain and spinal cord, enclosed within the protective cranial vault and vertebrae, respectively. The peripheral nervous system (PNS) is composed of the cranial nerves, which project from the brain and pass through foramina (openings) in the skull, and the spinal nerves, which project from the spinal cord and pass through intervertebral foramina of the vertebrae. Peripheral nerve pathways are differentiated into afferent pathways (ascending pathways) that carry sensory impulses toward the CNS and efferent pathways (descending pathways) that innervate effector organs, such as skeletal, cardiac, and smooth muscle, as well as glands, by transmitting motor impulses away from the CNS. Organs innervated by specific components of the nervous system are called effector organs. Cranial nerves are viewed most correctly as modified spinal nerves. Some cranial nerves function similarly to spinal nerves, whereas others have specialized sensory tasks, such as smell, taste, sight, and hearing.
Functionally the PNS can be divided into the somatic nervous system and the autonomic nervous system. The somatic nervous system consists of motor and sensory pathways regulating voluntary motor control of skeletal muscle. The autonomic nervous system (ANS) also consists of motor and sensory components and is involved with regulation of the body’s internal environment (viscera) through involuntary control of organ systems. The ANS is further divided into sympathetic and parasympathetic divisions. Today we understand that some aspects of the ANS can be controlled through mental practice with or without biofeedback techniques.
CELLS OF THE NERVOUS SYSTEM
The two basic types of cells that make up nervous tissue are neurons and neuroglial cells. The neuron is the primary information/communication cell of the nervous system. Working in parallel systems, neurons can scan the environment, integrate many systems at higher cognitive levels, and initiate body responses to maintain homeostasis. The neuroglial cells are found in the CNS and PNS and can provide structural support and nutrition for neurons, remove debris, increase the speed of nerve impulses, and play a significant role, along with neurons, in processing and storing information (i.e., memory).1
Neurons
Neuronal structure varies considerably throughout the CNS. Neurons vary in size from micrometers to several meters long and have from one to many cell processes. Even the shapes and complexity of the processes can vary considerably. Neurons are specialized cells that share many of the same metabolic activities and constituents as other types of cells. The fuel source for the neuron is predominantly glucose; insulin, however, is not required for cellular glucose uptake in the CNS. Neurons contain many cellular constituents, namely, microtubules, neurofibrils, microfilaments, and Nissl substances. Microfilaments and neurofibrils are composed of structural proteins and are responsible for structural support within the cell and movement of neuron processes, as seen in amoebas and white blood cells. Microtubules also are made of protein and are believed to be involved in the transport of cellular products. Nissl substances consist of endoplasmic reticulum and ribosomes and are involved in protein synthesis. The CNS starts out with more neurons than it needs, and those neurons that do not become involved in functional systems die. Some neurons continue to divide after birth. Olfactory neurons in the nose continue to divide throughout life.
A neuron (Figure 14-1) has three components: a cell body (soma) and the thin processes of the cell—the dendrites and axons. Most cell bodies are located within the CNS. Dense, packed cell bodies in the CNS are called nuclei. Cell bodies in the PNS are usually found in groups called ganglia or plexuses. The dendrites are extensions that carry nerve impulses toward the cell body. The dendritic zone is the receptive portion of a neuron that receives a stimulus and continues further conduction. Axons are long, conductive projections from the cell body that carry nerve impulses away from the cell body. The axon hillock is the cone-shaped, Nissl-free area where the axon leaves the cell body. In large nerves, axons are bundled together as fascicles. The initial segment of the axon has the lowest threshold for stimulation, and as a result, action potentials begin there.
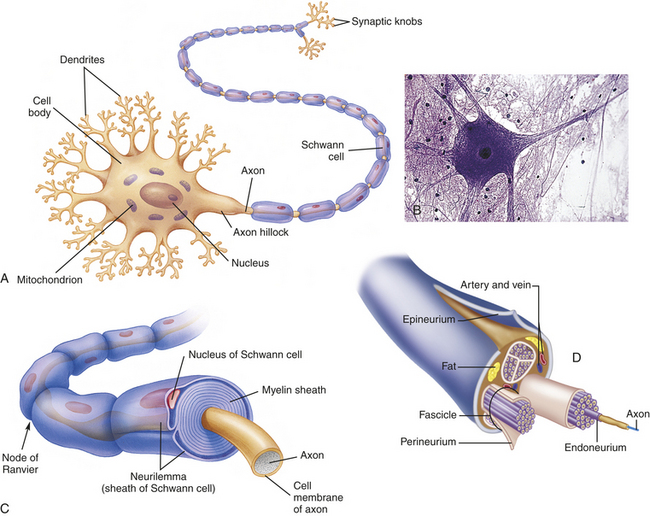
Figure 14-1 Structure of a typical neuron. A, Many dendrites carry nerve impulses to the cell body, which then send the nerve impulses along a single, long axon. Long axons are encased at intervals by a myelin sheath. B, Photomicrograph of a neuron. C, A segment of myelinated fiber in cross section, showing myelin sheath composed of several layers of myelin, which insulate the axon. D, Axons bundled into fascicles. (A and C from Thibodeau GA, Patton KT: Structure and function of the human body, ed 12, St Louis, 2004, Mosby; B, copyright Edward Reschke; D from Patton KT, Thibodeau GA: Anatomy & physiology, ed 7, St Louis, 2010, Mosby.)
A typical neuron has only one axon, which may be covered with a segmented layer of lipid material called myelin, which acts as an insulating substance. This entire membrane is referred to as the myelin sheath; the thin membrane between the myelin sheath and the endoneurium, a delicate connective tissue around each axon in the PNS (see Figure 14-23, B), is the neurilemma (Schwann sheath). The neurilemma and the myelin sheath are interrupted at regular intervals by the nodes of Ranvier. The Schwann cell forms and maintains the myelin sheath, and the nodes of Ranvier form the spaces on either side of the Schwann cell. If the myelin layer is tightly wrapped many times around the axon forming nodes of Ranvier, it increases conduction velocity and the neuron is referred to as myelinated (see Figure 14-1).
Myelin acts as an insulator that allows ions to flow between segments rather than along the entire length of the membrane, resulting in increased velocity. This mechanism is referred to as saltatory conduction. If the Schwann cells are loosely wrapped around the axon, it is referred to as unmyelinated, and conduction velocity is not increased. Axons are capable of extensive branching, which occurs at the nodes of Ranvier. Two major principles of information processing in the nervous system are divergence and convergence. Divergence refers to the ability of these branching axons to influence many different neurons. Convergence is the term applied to branches of numerous neurons converging on and influencing one or a few neurons. Disorders of the myelin sheath (demyelinating diseases), such as multiple sclerosis and Guillain-Barré syndrome, demonstrate the important role myelin plays in nerve function (see Chapter 17). Besides depending on the myelin coating, conduction velocities also depend on the diameter of the axon. Larger axons transmit impulses at a faster rate.
Neurons are structurally classified on the basis of the number of processes (projections) extending from the cell body. There are four basic types of cell configuration: (1) unipolar, (2) pseudounipolar, (3) bipolar, and (4) multipolar (Figure 14-2). Unipolar neurons have one process that branches shortly after leaving the cell body. One example is found in the retina. Pseudounipolar neurons (some authors call them unipolar) have one process that has its dendritic portion extending away from the CNS and its axon portion projecting into the CNS (see Figure 14-2). The configuration is typical of sensory neurons in both cranial and spinal nerves. Bipolar neurons have two distinct processes arising from the cell body. This type of neuron connects to rod and cone cells of the retina. Multipolar neurons are the most common and have multiple processes capable of extensive branching. A motor neuron is typically multipolar.
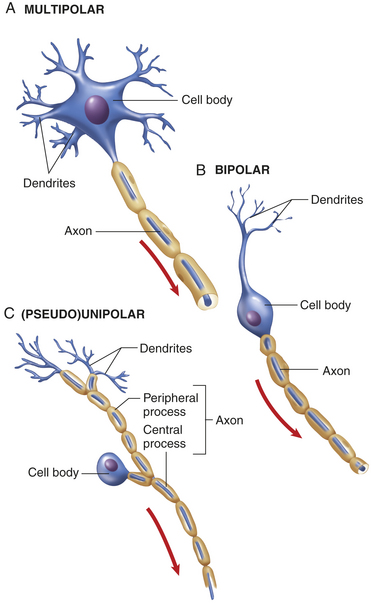
Figure 14-2 Structural classification of neurons. (From Patton KT, Thibodeau GA: Anatomy & physiology, ed 7, St Louis, 2010, Mosby.)
Functionally there are three types of neurons (with their direction of transmission and typical configuration noted in parentheses): (1) sensory (afferent, mostly pseudounipolar), (2) associational (interneurons, multipolar), and (3) motor (efferent, multipolar). Sensory neurons carry impulses from peripheral sensory receptors to the CNS (Box 14-1). Associational neurons (interneurons) transmit impulses from neuron to neuron, for example, from sensory to motor neurons, and are also involved in cognitive function. Motor neurons transmit impulses away from the CNS to an effector organ. In skeletal muscle the end processes form a complex neuromuscular (myoneural) junction.
Neuroglia and Schwann Cells
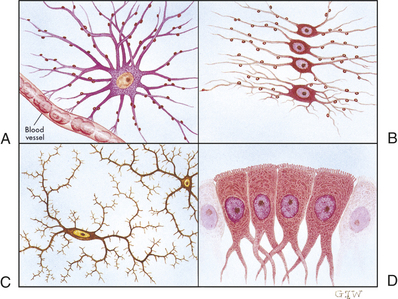
Neuroglia (“nerve glue”) comprise the general classification of cells that support the neurons of the CNS. They make up approximately half of the total brain and spinal cord volume and are 5 to 10 times more numerous than neurons. Different types of neuroglia serve different functions. Astrocytes, for example, fill the spaces between neurons and surround blood vessels in the CNS; oligodendroglia (oligodendrocytes) function to deposit myelin within the CNS. Oligodendroglia are the CNS counterpart of the Schwann cells. Ependymal cells line the cerebrospinal fluid (CSF)–filled cavities of the CNS. Microglia remove debris (phagocytosis) in the CNS. Characteristics of neuroglia and Schwann cells are summarized in Figure 14-3 and Table 14-1.
Table 14-1
Support Cells of the Nervous System
| Cell Type | Primary Functions |
| Astrocytes | Form specialized contacts between neuronal surfaces and blood vessels |
| Provide rapid transport for nutrients and metabolites | |
| Believed to form an essential component of the blood-brain barrier | |
| Appear to be the scar-forming cells of the CNS, which may be the foci for seizures | |
| Appear to work with neurons in processing information and memory storage | |
| Oligodendroglia (oligodendrocytes) | Formation of myelin sheath and neurilemma in the CNS |
| Schwann cells (neurolemmocytes) | Formation of myelin sheath and neurilemma in the PNS |
| Microglia | Responsible for clearing cellular debris (phagocytic properties) |
| Ependymal cells | Serve as a lining for ventricles and choroid plexuses involved in production of cerebrospinal fluid |
CNS, Central nervous system; PNS, peripheral nervous system.
Nerve Injury and Regeneration
When an axon is severed, a typical sequence of events, known as wallerian degeneration, occurs in the portion of the axon distal to the cut: (1) a characteristic swelling appears, (2) the neurofilaments hypertrophy, (3) the myelin sheath shrinks and disintegrates, and (4) this axon portion degenerates and disappears. The myelin sheaths reform into Schwann cells that line up in a column between the cut and the effector organ.
At the proximal end of the injured axon, similar changes occur, but only back as far as the next node of Ranvier. The cell body responds to trauma by swelling and then dispersing the Nissl substance (chromatolysis). During the repair process the cell increases in metabolic activity, protein synthesis, and mitochondrial activity. Approximately 7 to 14 days after the injury, new terminal sprouts project from the proximal segment and may enter the remaining Schwann cell pathway. (Figure 14-4 contains a more detailed representation of these events.) This process, however, is limited to myelinated fibers and generally occurs only in the PNS. The regeneration of axonal constituents in the CNS is limited by increased scar formation and the different nature of myelin formation by the oligodendrocyte.
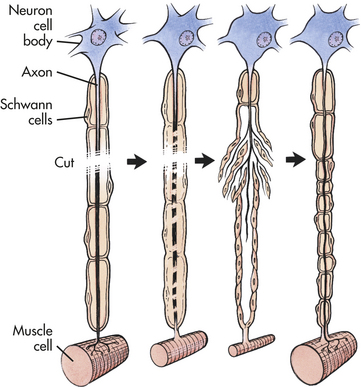
Figure 14-4 Repair of a peripheral nerve fiber. When cut, a damaged motor axon can regrow to its distal connection only if the neurilemma remains intact (to form a guiding tunnel) and if scar tissue does not block its way.
Nerve regeneration depends on many factors, such as location of the injury, type of injury, the inflammatory responses, and the process of scarring. The closer to the cell body of the nerve, the greater the chances that the nerve cell will die and not regenerate. A crushing injury allows recovery more fully than does a cut injury. Crushed nerves sometimes recover fully, whereas cut nerves often form connective tissue scars that block or slow regenerating axonal branches.
NERVE IMPULSE
Neurons generate and conduct electrical and chemical impulses by selectively changing the electrical portion of their plasma membranes and influencing other nearby neurons by the release of chemicals (neurotransmitters). A neuron in its unexcited state maintains a resting membrane potential (see Chapter 1). When the membrane potential is raised sufficiently, an action potential is generated (see Figure 1-32), and the nerve impulse then flows to all parts of the neuron. The action potential response occurs only when the stimulus is strong enough; if it is too weak, the membrane remains unexcited. This property is sometimes termed the all-or-none response.
Synapses
Neurons are not physically continuous with one another. The region between adjacent neurons is called a synapse. Impulses are transmitted across the synapse by chemical (see Figures 14-5 and 14-14) and electrical conduction (Chapter 1); only chemical conduction is discussed here. The neurons that conduct a nerve impulse are named according to whether they relay impulses toward the synapse (presynaptic neurons) or away from the synapse (postsynaptic neurons). Four basic types of connections occur in regions of contact between the presynaptic and postsynaptic neurons. These are between axons (axoaxonic), from axon to cell body (axosomatic), from axon to dendrite (axodendritic), and from dendrite to dendrite (dendrodendritic).
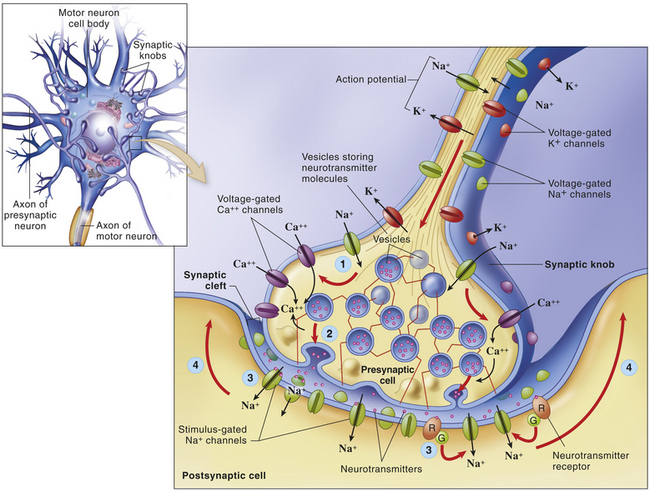
Figure 14-5 Neuronal transmission and synaptic cleft. Electrical impulse travels along axon of first neuron to synapse at synaptic knobs. Chemical transmitter is secreted into synaptic space to depolarize membrane (dendrite or cell body) of the next neuron in pathway. Details illustrate the synaptic knob (axon terminal) of a presynaptic neuron, the plasma membrane of a postsynaptic neuron, and a synaptic cleft. At step (1) the arrival of an action potential at the synaptic knob, voltage-gated Ca++ channels open and allow extracellular Ca++ to diffuse into the presynaptic cell. At step (2) the Ca++ triggers the rapid exocytosis of neurotransmitter molecules from vesicles in the knob. At step (3) neurotransmitter diffuses into the synaptic cleft and binds to receptor molecules in the plasma membrane of the postsynaptic neuron. The postsynaptic receptors directly or indirectly trigger the opening of stimulus-gated ion channels, initiating a local potential in the postsynaptic neuron. At step (4) the local potential may move toward the axon, where an action potential may begin. (From Patton KT, Thibodeau GA: Anatomy & physiology, ed 7, St Louis, 2010, Mosby.)
Impulses are transmitted across the synapse by chemical conduction. The conducting substance is called a neurotransmitter, and it is often formed in the synaptic knobs (boutons) of the presynaptic neuron’s axon and stored in synaptic vesicles within the knobs. Action potentials in the presynaptic neuron cause the synaptic vesicles to release their neurotransmitter or neurotransmitters through the plasma membrane into the synaptic cleft (the space between the neurons), where they bind to receptor sites on the plasma membrane of the postsynaptic neuron (see Figure 14-5). Neurons can synthesize more than one neurotransmitter, and postsynaptic membranes can contain more than one type of transmitter-specific receptor.
Neurotransmitters
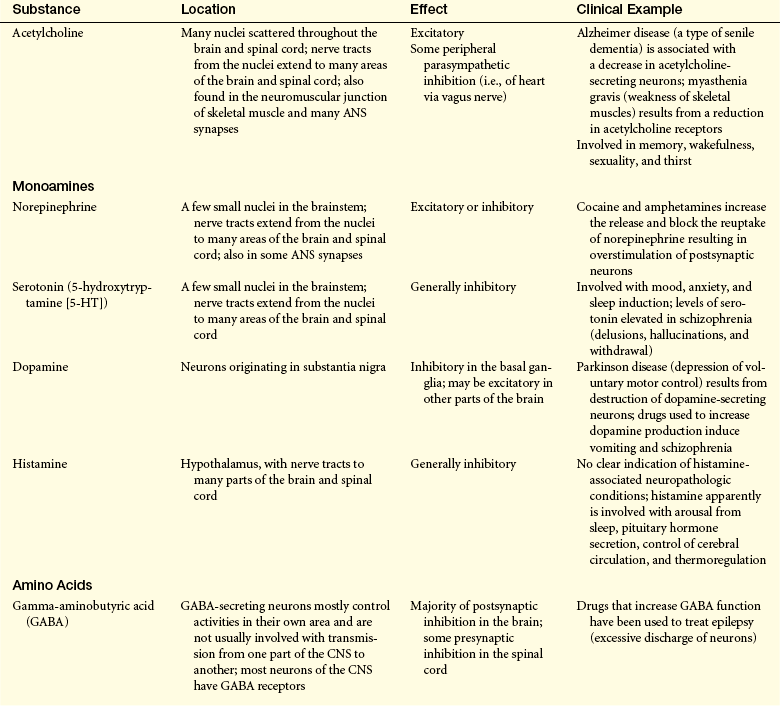
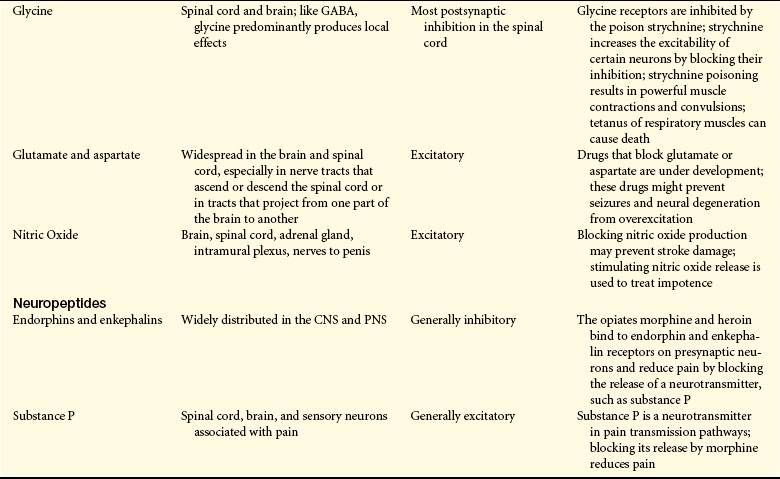
A neurotransmitter is defined as a chemical that “must be synthesized in the neuron, become localized in the presynaptic terminal [synaptic bouton], be released into the synaptic cleft, bind to a receptor site [binding site] on the postsynaptic membrane of another neuron or effector where it affects ion channels, and last, be removed by a specific mechanism from its site of action.” More than 39 substances are thought to be neurotransmitters, including norepinephrine, acetylcholine, dopamine, histamine, gamma-aminobutyric acid (GABA), and serotonin.2,3 Many of these transmitters have more than one function. For example, norepinephrine in the brain probably helps regulate mood, functions in dream sleep, and maintains arousal. Several neurotransmitters are amino acids, including GABA, glutamic acid, and aspartic acid. Small chains of amino acids, such as enkephalins and endorphins, also function as neurotransmitters. They (neuropeptides) are involved in the perception and integration of pain, as well as in emotional experiences. Neurotransmitter and neuromodulator substances are listed in Table 14-2.
Table 14-2
Neurotransmitter and/or Neuromodulator Substances
ANS, Autonomic nervous system; CNS, central nervous system; PNS, peripheral nervous system.
From Seeley R, Stephens TD, Tate P: Anatomy & physiology, ed 6, St Louis, 2003, Mosby.
Because the neurotransmitter is normally stored on one side of the synaptic cleft and the receptor sites are on the other side, chemical synapses operate in one direction. Therefore, action potentials are transmitted along a multineuronal pathway in one direction. The binding of the neurotransmitter at the receptor site changes the permeability of the postsynaptic neuron and, consequently, its membrane potential. Two possible scenarios can then follow: (1) the postsynaptic neuron may be excited (depolarized; excitatory postsynaptic potentials [EPSPs]) or (2) the postsynaptic neuron’s plasma membrane may be inhibited (hyperpolarized; inhibitory postsynaptic potentials [IPSPs]). It has recently been discovered that cannabinoid transmitters are released from postsynaptic neurons that modulate neurotransmitter release from presynaptic neurons.4,5 (Chapter 1 contains a review of electrical impulses and membrane potentials.)
Usually, a single EPSP cannot induce a neuron’s action potential and the propagation of the nerve impulse. Whether an action potential occurs depends on the number and frequency of potentials the postsynaptic neuron receives—a concept known as summation. Temporal summation (time relationship) refers to the effects of successive, rapid impulses received from a single neuron on the same synapse. Spatial summation (spacing effect) is the combined effects of impulses from a number of neurons on a single synapse at the same time. Facilitation refers to the effect of EPSPs on the plasma membrane potential. The plasma membrane is facilitated when summation brings the membrane closer to the threshold potential and decreases the stimulus required to induce an action potential. The effect that a neurotransmitter has on the plasma membrane potential depends on the balance of these effects. The mechanisms of convergence, divergence, summation, and facilitation allow for the integrative processes of the nervous system.
Two points could be helpful in understanding the complexity of brain physiology. First, the aforementioned neuromodulators appear to function to raise or lower the membrane potentials of neurons. These chemicals facilitate or inhibit the effect of neurotransmitters. Second, reciprocal synapses between dendrites—that is, one dendrite being able to depolarize or hyperpolarize the membrane potential of another dendrite through the use of neurotransmitters—demonstrate that the interactions between neurons are far more complicated than postulated by simple on-off models of brain function.
CENTRAL NERVOUS SYSTEM
The human brain enables individuals to reason, function intellectually, express personality and mood, and interact with the environment. The brain is a pinkish gray organ that weighs approximately 3 pounds and has the consistency of tofu or custard. It receives approximately 15% to 20% of the total cardiac output. The three major divisions of the brain, based on embryologic origin, are (1) the forebrain, formed by the two cerebral hemispheres; (2) the midbrain, which includes the corpora quadrigemina, tegmentum, and cerebral peduncles; and (3) the hindbrain, which includes the cerebellum, pons, and medulla (Table 14-3). The midbrain, medulla oblongata, and pons make up the brainstem, which connects the hemispheres of the brain, cerebellum, and spinal cord. A collection of nuclei (nerve cell bodies) within the brainstem collectively constitute the reticular formation (Figure 14-6). The reticular formation is a large network of connected tissue nuclei that regulate vital reflexes, such as cardiovascular function and respiration. The reticular formation is essential for maintaining wakefulness and in conjunction with the cerebral cortex is referred to as the reticular activating system. Some nuclei within the reticular formation are involved in motor movements.1
Table 14-3
Divisions of the Central Nervous System
| Primary Vesicles | Secondary Vesicles | Associated Structures |
| Forebrain (prosencephalon) | Telencephalon | Cerebral hemispheres |
| Cerebral cortex | ||
| Rhinencephalon | ||
| Basal ganglia | ||
| Diencephalon | Epithalamus | |
| Thalamus | ||
| Hypothalamus | ||
| Subthalamus | ||
| Midbrain (mesencephalon) | Mesencephalon | Corpora quadrigemina |
| Tegmentum | ||
| Cerebral peduncles | ||
| Hindbrain (rhombencephalon) | Metencephalon | Cerebellum |
| Pons | ||
| Myelencephalon | Medulla oblongata | |
| Spinal cord | Spinal cord | Spinal cord |
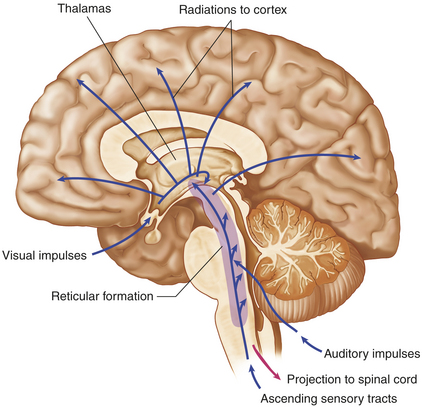
Figure 14-6 Reticular activating system. System consists of nuclei in the brainstem reticular formation plus fibers (axons) that conduct to the nuclei from below and fibers that conduct from the nuclei to widespread areas of the cerebral cortex. Functioning of the reticular activating system is essential for consciousness. (From Patton KT, Thibodeau GA: Anatomy & physiology, ed 7, St Louis, 2010, Mosby.)
In general, many major divisions of the brain are associated with specific functions, such as the occipital lobe and vision, but attributing specific functions to definite regions of the brain is not entirely accurate. Many activities, such as motor movements and memory, may actually be performed in several regions. Understanding functional specificity is very useful to clinical personnel, especially when attempting to localize pathologic conditions in the nervous system. A neurologist often can localize the site of a tumor, stroke, or bullet wound in an individual just by performing a neurologic examination.
Many attempts have been made to ascribe function to various regions of the cerebral cortex. A German neuropsychiatrist, Korbinian Brodmann (1868-1918), is credited with postulating the correlation of various activities to many regions of the cerebral cortex. (Figure 14-7, B and C, illustrates these regions and identifies some functional areas.) Another basic CNS principle, plasticity, holds that the CNS is capable of change. For example, children with brain damage may experience “relocation” of some functional areas to other parts of the brain. This propensity for plasticity decreases with age, which explains why older individuals tend not to recover from brain injuries as well as younger individuals. This varying balance between specificity and plasticity makes understanding brain functions difficult.
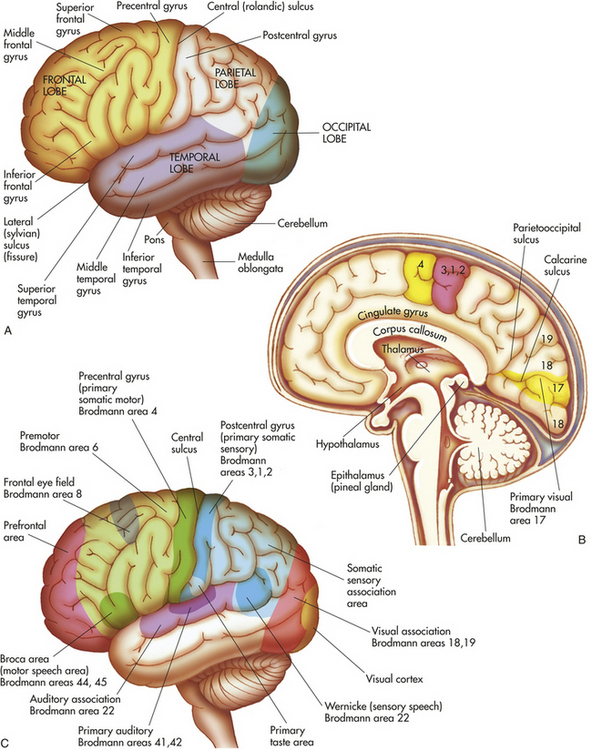
Figure 14-7 Cerebral hemispheres. A, Left hemisphere of cerebrum, lateral view. B, Functional areas of the cerebral cortex, midsagittal view. C, Functional areas of the cerebral cortex, lateral view.
Forebrain
Telencephalon: The telencephalon consists of the cerebrum (the largest portion of the brain), which includes the cerebral cortex and basal ganglia. The surface of the cerebrum is characterized by numerous convolutions called gyri (see Figure 14-7, A). The gyri greatly increase the cortical surface area. Grooves between adjacent gyri are called sulci. Deeper grooves are referred to as fissures. The cerebral cortex contains the cell bodies and dendrites of neurons, which often are referred to as gray matter. Gray matter is organized into columns perpendicular to the surface that receive, integrate, store, and transmit information. White matter lies beneath the cerebral cortex and is composed of myelinated nerve fibers.
The two cerebral hemispheres are separated by the longitudinal fissure. The surface of each hemisphere is divided into lobes that take their names from the region of the skull under which each of them lies. The posterior margin of the frontal lobe is the central sulcus (fissure of Rolando, central fissure); it borders inferiorly on the lateral sulcus (sylvian fissure, lateral fissure) (see Figure 14-7, A). The prefrontal area is responsible for goal-oriented behavior (i.e., ability to concentrate), short-term or recall memory, and the elaboration of thought and inhibition on the limbic (emotional) areas of the CNS. The premotor area (Brodmann area 6) (see Figure 14-7, C) is involved in programming motor movements. This area also contains the cell bodies that form part of the basal ganglia system (extrapyramidal system—efferent pathways outside the pyramids of the medulla oblongata). The frontal eye fields (the lower portion of Brodmann area 8), which are involved in controlling eye movements, are located in the middle frontal gyrus.
The primary motor area (Brodmann area 4) is located along the precentral gyrus forming the primary voluntary motor area, which has a somatotopic organization that often is referred to as a homunculus (little man) (Figure 14-8). Electrical stimulation of specific areas of this cortex causes specific muscles of the body to move. The medial part of the cortex in the longitudinal fissure (midline space between the two cerebral hemispheres) affects the lower limb and foot, whereas on the lateral surface, the superior third controls the torso and arm, the middle third the hand, and the lowest third the face and mouth/throat. The axons traveling from the cell bodies in and on either side of this gyrus project fibers (axons) that form the corticospinal tracts (pyramidal system) that descend into the spinal cord. Cerebral impulses control function in the opposite side of the body, a phenomenon called contralateral control (Figure 14-9, A). The Broca speech area (Brodmann areas 44, 45) is rostral to the inferior edge of the premotor area (Brodmann area 6) on the inferior frontal gyrus. It is usually on the left hemisphere and is responsible for the motor aspects of speech. Damage to this area, commonly as a result of a cerebrovascular accident (stroke), results in the inability to form, or difficulty in forming, words (expressive aphasia or dysphasia) (see Chapter 17).
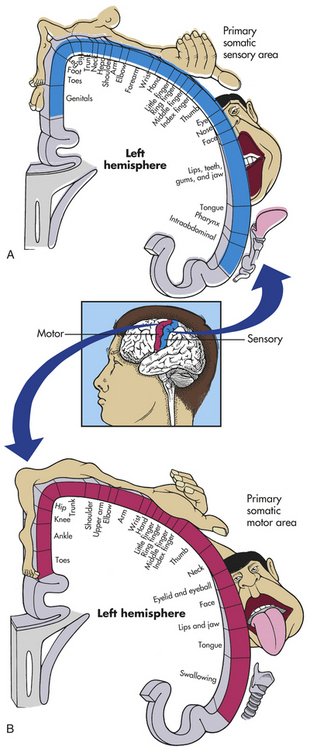
Figure 14-8 Primary somatic sensory (A) and motor (B) areas of the cortex. (From Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
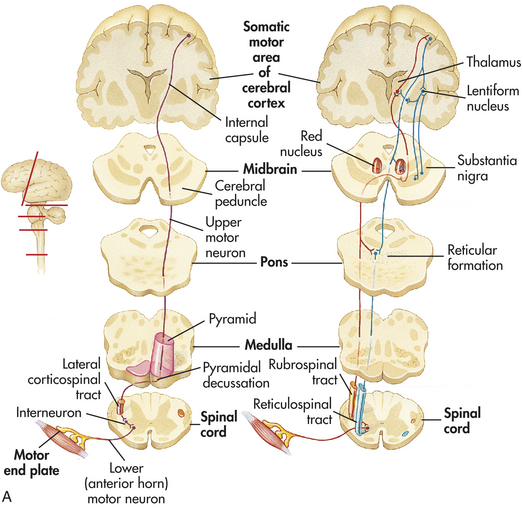
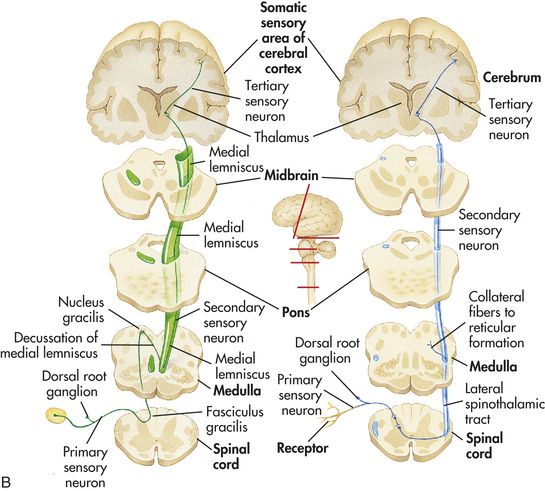
Figure 14-9 Examples of somatic motor and sensory pathways. A, Motor: the pyramidal pathway through the lateral corticospinal tract and the extrapyramidal pathways through the rubrospinal and reticulospinal tracts. Note that the pyramidal tracts decussate (cross over) to control the opposite side of the body. B, Sensory: pathways of the medial lemniscal system that conducts information about discriminating touch and kinesthesis and the spinothalamic pathway that conducts information about pain and temperature. (From Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
The parietal lobe lies within the borders of the central, parietooccipital, and lateral sulci. This lobe contains the major area for somatic sensory input, located primarily along the postcentral gyrus (Brodmann areas 3, 1, 2), which is adjacent to the primary motor area. Communication between the motor and sensory areas (and among other regions in the cortex) is provided by association fibers (i.e., axons from association fibers). Much of this region is involved in sensory association (storage, analysis, and interpretation of stimuli). (Figure 14-8 shows the distribution of functions associated with both the primary motor area and the primary sensory area of the cerebral cortex.)
The occipital lobe lies caudal to the parietooccipital sulci and superior to the cerebellum. The primary visual cortex (Brodmann area 17) is located in this region and receives input from the retinas. Much of the remainder of this lobe is involved in visual association (Brodmann areas 18, 19). The temporal lobe lies inferior to the lateral sulcus and is composed of the superior, middle, and inferior temporal gyri. The primary auditory cortex (Brodmann area 41) and its related association area (Brodmann area 42) lie deep within the lateral sulcus on the superior temporal gyrus. The Wernicke area (posterior portion of Brodmann area 22) is located on the superior temporal gyrus. This area is responsible for reception and interpretation of speech, and dysfunction may result in receptive aphasia or dysphasia. The Wernicke area, along with adjacent portions of the parietal lobe, constitutes a sensory speech area. The temporal lobe also is involved as a major area for long-term memory and secondary functions, such as balance, taste, and smell.
Another lobe, the insula, lies hidden from view deep in the lateral sulcus. Lying directly beneath the longitudinal fissure is a massive white matter pathway called the corpus callosum (commissural fibers). The corpus callosum connects the two cerebral hemispheres and is essential in the coordination of activities between hemispheres, especially specific tasks that may be present in only one hemisphere (see Figures 14-7, C, and 14-15). As a last resort, part or all of the corpus callosum is cut to prevent the spread of epileptic loci (site of seizure activity) through the corpus callosum to the opposite cerebral hemisphere. Epileptic loci often are found in the temporal lobe. This procedure, evolved in the well-known split-brain studies, results initially in temporary aphasia and paralysis.
Inside the cerebrum are numerous tracts (white matter) and nuclei (gray matter). The major cerebral nuclei are called basal ganglia and include the corpus striatum and amygdala. The corpus striatum consists of the lentiform nucleus (lens shaped), the putamen and globus pallidus, and the ram’s horn–shaped caudate nucleus. The internal capsule is a thick white-matter region in which afferent and efferent pathways, to and from the cerebral cortex, pass through the center of the cerebral hemispheres. The corpus striatum appears striped because of the rostral connections between its gray matter and the white matter of the internal capsule.
Functionally, the basal ganglia include, in addition to the corpus striatum, the subthalamic nucleus of the diencephalon and the substantia nigra of the mesencephalon. The basal ganglia plus their interconnections with the thalamus, premotor cortex, red nucleus, reticular formation, and spinal cord are part of the basal ganglia system (extrapyramidal system). The basal ganglia system is believed to exert a fine-tuning effect on motor movements. Parkinson disease and Huntington disease are conditions associated with defects of the basal ganglia (Box 14-2). They are characterized by various involuntary or exaggerated motor movements (see Chapter 16).
The limbic system, first described in 1878 by Broca, is composed of the Papez circuit (amygdala, parahippocampal gyrus, hippocampus, fornix, mamillary body of the hypothalamus, thalamus, and cingulate gyrus), septal area, habenula, other portions of the hypothalamus, and related autonomic nuclei. It is an extension or modification of the olfactory system. Its principal effects are believed to be involved with primitive behavioral responses, visceral reaction to emotion, feeding behaviors, biologic rhythms, and the sense of smell. Expression of affect (emotional and behavioral states) is mediated by extensive connections with the limbic system and prefrontal cortex. Interestingly, the Papez circuit, first postulated in 1937, appears to have as one of its major functions the consolidation of memory through a reverberating circuit.
Diencephalon: The diencephalon, surrounded by the cerebrum, is made up of four divisions: epithalamus, thalamus, hypothalamus, and subthalamus (see Table 14-3 and Figure 14-7, B). The epithalamus (pineal gland) forms the roof of the third ventricle (a brain cavity) and composes the most superior portion of the diencephalon. It has connections and functions closely associated with those of the limbic system. For example, the hormones of the pineal body have been shown to influence reproductive ability, and the secretion of melatonin is associated with circadian rhythms (see Chapters 10 and 20).
The largest component of the diencephalon is the thalamus. It is approximately the size and volume of the thumb from the tip to the first joint. It borders and surrounds the third ventricle, and it is a major integrating center for afferent impulses to the cerebral cortex, except for olfaction. The perception of various sensations occurs at this level but requires cortical processing for interpretation. The thalamus also serves as a relay center for sensory aspects of motor information from the basal ganglia and cerebellum to appropriate cortical motor areas. Cerebral cortical information also projects to the thalamus, creating reverberating circuits.
The hypothalamus forms the base of the diencephalon. Hypothalamic function falls into two major areas: (1) maintenance of a constant internal environment and (2) implementation of behavioral patterns. Integrative centers control ANS function, regulation of body temperature, endocrine function, and regulation of emotional expression. (Temperature regulation is discussed in Chapter 15.) The hypothalamus exerts its influence through the endocrine system, as well as through neural pathways (Box 14-3). (For endocrine functions of the hypothalamus and pituitary, see Chapter 20.)
The subthalamus flanks the hypothalamus laterally. The subthalamus contains the subthalamic nucleus, which is part of the basal ganglia system.
Midbrain
The midbrain (mesencephalon) is composed of three structures: the corpora quadrigemina, or tectum (composed of the superior and inferior colliculi); the tegmentum (containing the red nucleus and substantia nigra); and the basis pedunculi. (The tegmentum and basis pedunculi are collectively the cerebral peduncles.)
The superior colliculi are involved with voluntary and involuntary visual motor movements (e.g., the ability of the eyes to track moving objects in the visual field). The inferior colliculi accomplish similar motor activities but involve movements affecting the auditory system (e.g., positioning the head to improve hearing). The inferior colliculus is also a major relay center along the auditory pathway. The red nucleus is a major motor output center that is influenced by the cerebellum. The inferior-most portion of the basal ganglia is the substantia nigra, which synthesizes dopamine, a neurotransmitter and precursor of norepinephrine. Its dysfunction is associated with Parkinson disease (see Chapter 16). The basis pedunculi are made up of efferent fibers of the corticospinal, corticobulbar, and corticopontocerebellar tracts.
Other notable structures of this region are the nuclei and tracts of the third and fourth cranial nerves. The cerebral aqueduct (aqueduct of Sylvius), which carries CSF, also traverses this structure. The plugging of this aqueduct is often the cause of hydrocephalus.
Hindbrain
Metencephalon: The major structures of the metencephalon are the cerebellum and the pons. The cerebellum (see Figure 14-7, A and B) is composed of two cerebellar hemispheres covered with small convolutions called folia. Each hemisphere is divided by the primary fissure into two lobes (anterior and posterior) that are connected by a midline structure called the vermis, meaning worm.
The cerebellum is responsible for conscious and unconscious muscle synergy and for maintaining balance and posture. This is accomplished through extensive neural connections from the spinal cord and medulla oblongata through the inferior cerebellar peduncle and with the midbrain and higher structures through the superior cerebellar peduncle. The two cerebellar hemispheres receive massive cerebral cortical input through the middle cerebellar pedunculi. These connections allow extensive sampling of visual, vestibular, and proprioceptive data from other regions of the CNS and periphery. Damage to the cerebellum is characterized by ipsilateral (same side) loss of equilibrium, balance, and motor coordination. The cerebellum has ipsilateral control of the body, in contrast to the cerebral cortex, which has contralateral (opposite side) control of the body.
The pons (bridge) is easily recognized by its bulging appearance below the midbrain and above the medulla oblongata. Primarily, it transmits information from the cerebellum to the brainstem nuclei and relays motor information from the cerebral cortex to the contralateral cerebellar hemisphere. The pons is an important center for the control of respiration (i.e., rate and relationship of inspiration to expiration). The nuclei of cranial nerves V through VIII are located in this structure.
Myelencephalon: The medulla oblongata makes up the myelencephalon and is the lowest portion of the brainstem. Reflex activities, such as heart rate, respiration, blood pressure, coughing, sneezing, swallowing, and vomiting, are controlled in this area. The nuclei of cranial nerves IX through XII (see Table 14-6 for discussion) are located in this region. The lowest portion of the reticular formation is found here as well.
A major portion of the descending motor pathways (i.e., corticospinal tracts) crosses to the contralateral side, or decussate, at the inferior medulla oblongata (see Figure 14-9, A). These pathways, together with other areas of decussation in the CNS, are the basis for the phenomenon of contralateral control.
Spinal Cord
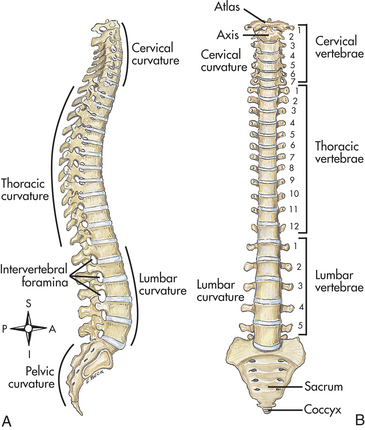
The spinal cord is the portion of the CNS that lies within the vertebral canal and is surrounded and protected by the vertebral column. The spinal cord has many functions, which include being a long nerve cable that connects the brain and body, conducting somatic and autonomic reflexes, providing motor pattern control centers, and serving as a sensory and motor modulation center. It continues from the medulla oblongata and ends at the level of the first or second lumbar vertebra in adults (Figure 14-10). The end of the spinal cord, the conus medullaris, is cone shaped. Spinal nerves continue from the end of the spinal cord and form a nerve bundle called the cauda equina. The filament anchor from the conus medullaris to the coccyx is the filum terminale (see Figure 14-10).
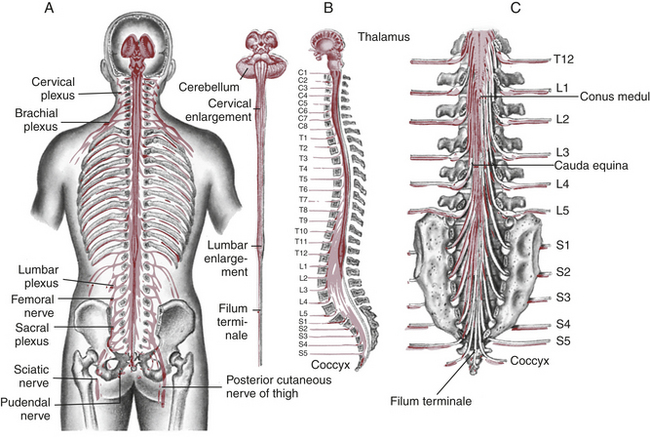
Figure 14-10 Spinal cord within vertebral canal and exiting spinal nerves. A, Posterior view of brainstem and spinal cord in situ with spinal nerves and plexus. B, Anterior view of brainstem and spinal cord. C, Enlargement of caudal area showing termination of spinal cord (conus medullaris) and group of nerve fibers constituting the cauda equina. (From Rudy EB, editor: Advanced neurological and neurosurgical nursing, St Louis, 1984, Mosby.)
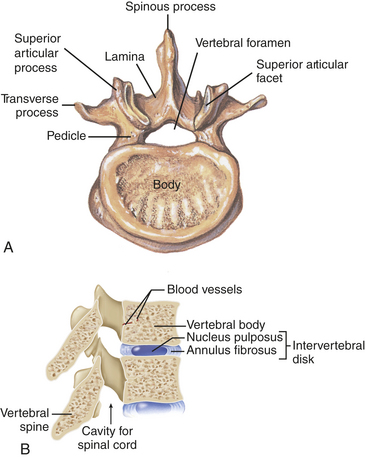
Grossly, the spinal cord is divided into sections (8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal) that correspond to paired nerves (see Figure 14-10). A cross section of the spinal cord (Figure 14-11) is characterized by a butterfly-shaped inner core of gray matter (containing nerve cell bodies). The central canal lies in the center of this region and extends through the spinal cord from its origin in the fourth ventricle. The gray matter of the spinal cord is divided into three regions with specific functional characteristics. These regions include the posterior horn (dorsal horn), which is composed primarily of interneurons and axons from sensory neurons whose cell bodies lie in the sensory ganglion (dorsal root ganglion). At the tip of the posterior horn is the substantia gelatinosa, a structure involved in pain transmission (see Chapter 15). The intermediolateral gray (lateral horn) contains cell bodies involved with the ANS. The anterior horn (ventral horn) contains the nerve cell bodies for efferent pathways leaving the spinal cord by way of spinal nerves. The terms anterior and posterior are preferred by many authors for describing human spinal cord anatomy, whereas dorsal and ventral are the common zoologic (“cat and dog”) terms.
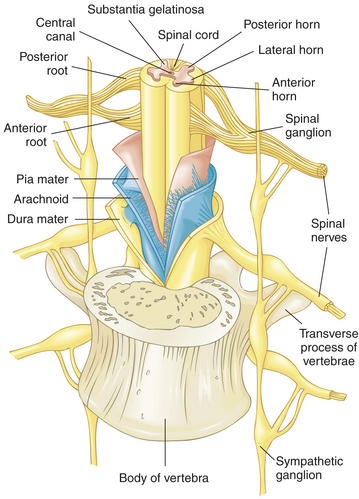
Figure 14-11 Coverings of the spinal cord. Note how the dura mater extends to cover the spinal nerve roots and nerves. The arachnoid is highlighted in blue and the pia mater in pink. (Modified from Thibodeau GA, Patton KT: Structure and function of the body, ed 12, St Louis, 2004, Mosby.)
Surrounding the gray matter is white matter that forms ascending and descending pathways called spinal tracts and short ascending and descending integrative pathways. Spinal tracts are named to denote their beginning and ending points. For example, the spinothalamic tract carries nerve impulses from the spinal cord to the thalamus in the diencephalon. The white matter is subdivided into columns. These consist of the anterior column (ventral column), lateral column, and posterior column (dorsal column), that is, the fasciculus gracilis and fasciculus cuneatus. (Figure 14-12 identifies the location and principal activities of the major spinal tracts.)
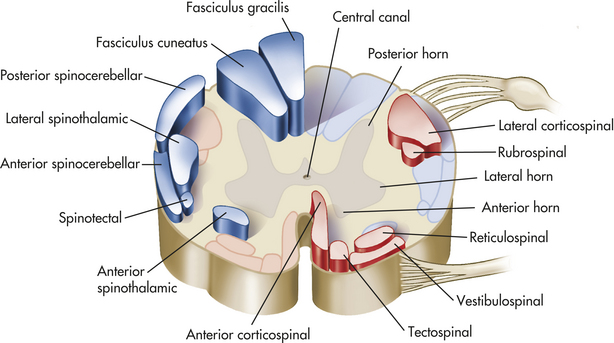
Figure 14-12 Major tracts of the spinal cord. The major ascending (sensory) tracts, shown only on the left here, are highlighted in blue. The major descending (motor) tracts, shown only on the right, are highlighted in red. (From Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
Neural circuits in the spinal cord, when activated, display specific sets of motor responses. Reflex arcs form basic units that respond to stimuli and provide protective circuitry for motor output. Structures mandatory for a reflex arc are a receptor, an afferent (sensory) neuron, an efferent (motor) neuron, and an effector muscle or gland. The afferent neuron is a pseudounipolar neuron, with its cell body in the sensory ganglion. A simple reflex arc may contain only two neurons. (Figure 14-13 illustrates a simple reflex arc.) Most reflex arcs consist of three neurons that include an interneuron or association neuron between the afferent and efferent neurons. Transmission time for three-neuron reflexes is slower than in simple reflexes because there are two synaptic delays, rather than one, as well as the delay involved in crossing the interneuron. The afferent neuron of the reflex arc simultaneously sends sensory information to the effector organ and to higher CNS centers (see Figure 14-9, B, and Figure 15-3). The motor effects from reflex arcs generally occur before perception of the event in the higher centers of the brain. Much of the regulation of the internal environment is mediated by ANS reflexes.
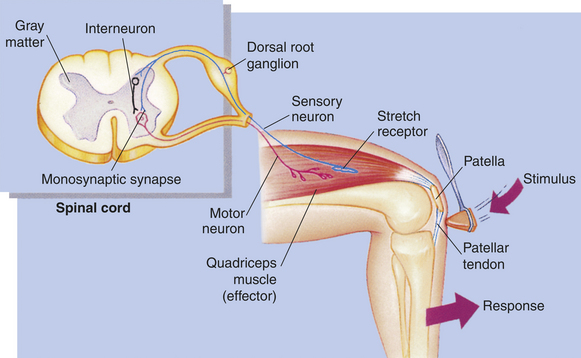
Figure 14-13 Cross section of spinal cord showing simple reflex arc. (From Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
Afferent pathways transmit information from peripheral receptors and eventually terminate in the cerebral or cerebellar cortex or both. Efferent pathways primarily relay information from the cerebrum to the brainstem or spinal cord (see Figure 14-9, A). Upper motor neurons (i.e., corticospinal tract) are the classification of motor pathways completely contained within the CNS. Their primary roles include directing, influencing, and modifying reflex arcs, lower-level control centers, and motor (and some sensory) neurons. Generally, upper motor neurons form synapses with interneurons, which then form synapses with lower motor neurons before projecting into the periphery. Lower motor neurons (i.e., cranial and spinal efferent neurons) are responsible for direct influence on muscles. Their cell bodies lie in the gray matter of the spinal cord, but their processes extend into the PNS (see Figure 16-26). Destruction of upper motor neurons usually results in initial paralysis followed within days or weeks by partial recovery, whereas destruction of the lower motor neurons often leads to permanent paralysis. Peripheral nerve damage may be followed by nerve regeneration and recovery. (Injury to motor neurons is discussed in Chapter 17.)
Muscle activity (i.e., stimulation and contraction) is regulated by nerve impulses. Motor neurons innervate one or more muscle cells, forming motor units consisting of a neuron and the skeletal muscles it stimulates. The junction between the axon of the motor neuron and the plasma membrane of the muscle cell is called the neuromuscular (myoneural) junction (Figure 14-14). The skeletal muscle neuromuscular junction is more elaborate than the simpler smooth muscle neuromuscular junction.
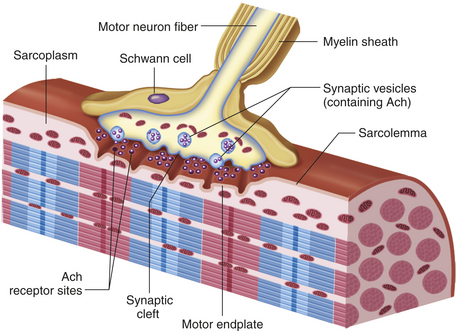
Figure 14-14 Neuromuscular junction. This figure shows how the distal end of a motor neuron fiber forms a synapse, or “chemical junction,” with an adjacent muscle fiber. Neurotransmitters (specifically, acetylcholine) are released from the neuron’s synaptic vesicles and diffuse across the synaptic cleft where they stimulate receptors in the motor end-plate region of the sarcolemma. (From Patton KT, Thibodeau GA: Anatomy & physiology, ed 7, St Louis, 2010, Mosby)
Motor Pathways
The four clinically relevant motor pathways are the lateral corticospinal, corticobulbar, basal ganglia, and vestibulospinal pathways. The corticospinal (see Figure 14-9, A) and corticobulbar (see Figure 16-25) are essentially the same tract and consist of a two-neuron chain. The cell bodies originate in and around the precentral gyrus; pass through the corona radiata of the cerebrum, the internal capsule, middle three fifths of the basis pedunculus, pons, and pyramid; decussate (cross contralaterally) in the medulla oblongata; and form the lateral corticospinal tract of the spinal cord (see Figure 14-12). The lateral corticospinal tract axons (upper motor neurons) leave the tract to go to specific interneurons or motor neurons in the anterior horn. The lateral corticospinal tract has the same somatotopic organization as the body. These spinal motor neurons project to specific motor units and are lower motor neurons. The corticobulbar (bulbar refers to brainstem) tract can be thought of as the part of the corticospinal tract that innervates the cranial motor nuclei for eye, face, tongue, throat, and neck movement. This tract innervates all the cranial motor nuclei bilaterally except for the facial (spinal), accessory, and hypoglossal nuclei, which receive primarily contralateral innervation. These tracts are involved in precise motor movements. The basal ganglia are part of a system that drives the reticular descending tracts (Figure 14-12 shows only one of the two reticulospinal tracts). These tracts modulate motor movement by inhibiting and exciting spinal activity. The vestibulospinal tract arises from the lateral vestibular nucleus in the pons and causes the extensor muscles of the body to rapidly contract, most dramatically witnessed when a person starts to fall backward.
Sensory Pathways
The three clinically important spinal afferent pathways are the posterior (dorsal) column, anterior spinothalamic, and lateral spinothalamic (see Figures 14-9, B, and 14-12). The posterior column has a somatotopic organization with the fasciculus gracilis and fasciculus cuneatus, respectively, carrying lower body and upper body fine touch, two-point discrimination, and proprioceptive information (i.e., epicritic). The posterior column is formed by a three-neuron chain. The first neuron of the chain is the primary afferent neuron. It is also the sensory neuron of the reflex arc. After entering the spinal cord it sends its axon ipsilaterally up the spinal cord in a specific part of the posterior funiculus and synapses in one of three posterior column nuclei in the hindbrain. A basketball center has primary afferent neurons that run from the great toe up to the pons, which could be more than 6 feet long. The second-order neuron has its cell body in one of the posterior column nuclei and sends its axon contralaterally and ascends to a specific nucleus of the thalamus and synapses. The third-order neuron, originating in the thalamus, continues the tract into the internal capsule, corona radiata, and postcentral gyrus (Brodmann areas 3, 1, 2) (see Figure 14-7, C). The anterior and lateral spinothalamic tracts are responsible for vague touch and pain and temperature, respectively (see Figure 14-9, B). These modalities are referred to as protopathic.
Today the anterior and lateral spinothalamic tracts are combined by many neuroanatomists into the anterolateral system because these modalities are difficult to localize into finite tracts in the spinal cord. These tracts also form a three-neuron chain. However, the primary afferent neurons synapse in the posterior horn of the spinal cord, not just at the level they enter the intervertebral foramen but in a number of spinal segments above and below their point of entry. This is an example of divergence. The second-order neurons in the posterior horn cross to the contralateral side in the spinal cord and ascend to the same thalamic nucleus as the posterior column pathway and continue on with the posterior column pathway to the postcentral gyrus.
Protective Structures
The cranium is composed of eight bones. The cranial vault functions to enclose and protect the brain and its associated structures. The galea aponeurotica, which is a thick, fibrous band of tissue overlying the cranium between the frontal and occipital muscles, affords added protection to the bony structure of the skull. The subgaleal space has venous connections with the dural sinuses, and with increased intracranial pressure, blood can be shunted to the space, thus reducing pressure in the intracranial cavity. The subgaleal space is also a common site for wound drains to be placed after intracranial surgery.
The floor of the cranial vault is irregular and contains many foramina (openings) for cranial nerves, blood vessels, and the spinal cord to exit. The cranial floor is divided into three fossae (depressions). The frontal lobes lie in the anterior fossa; temporal lobes and base of the diencephalon lie in the middle fossa (temporal fossa); and the cerebellum lies in the posterior fossa. These terms are commonly used anatomic landmarks to describe the location of intracranial lesions.
Meninges
Surrounding the brain and spinal cord are three protective membranes: the dura mater, the arachnoid, and the pia mater. Collectively they are called the meninges (Figure 14-15). The dura mater (meaning literally “hard mother”) is composed of two layers, with the venous sinuses formed between them. The outermost layer forms the periosteum (endosteal layer) of the skull, and the inner dura, or meningeal layer, is responsible for the formation of rigid, double-thickness membranous plates that serve to support and separate various brain structures.
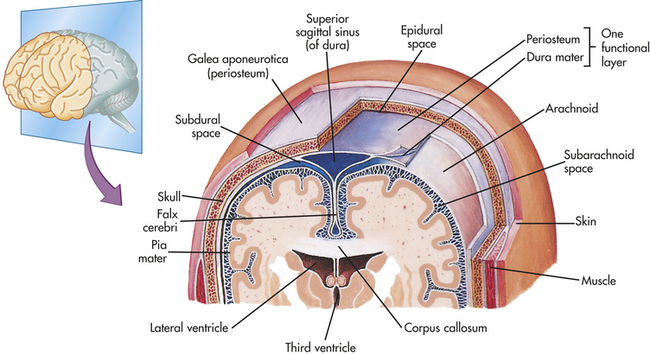
Figure 14-15 Coverings of the brain. Frontal section of the superior portion of the head, as viewed from the front. The bony and the membranous coverings of the brain can be seen. (From Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
One of these membranous plates (see Figure 14-15), the falx cerebri, dips between the two cerebral hemispheres along the longitudinal fissure. The falx cerebri is anchored anteriorly to the base of the brain at the crista galli of the ethmoid bone. The tentorium cerebelli is a membrane that separates the cerebellum below from the cerebral structures above. The tentorium may become involved during periods of increased intracranial pressure caused by an injury to the brain. An injury within the cranial cavity tends to shift intracranial contents, and as structures shift, they tend to be compressed against these rigid membranes, resulting in damage or destruction. A common example is tentorial herniation.
Below the dura mater lies the arachnoid membrane, characterized by its filmy, weblike structure. It loosely follows the contours of the cerebral structures but goes over the sulci.
The subdural space lies between the dura and arachnoid. Many small bridging veins that have little support traverse the subdural space. Their disruption results in a subdural hematoma (see Chapter 17). The subarachnoid space, which contains CSF, lies between the arachnoid and the pia mater (see Figure 14-15). Damage to intracranial vessels can lead to a condition called subarachnoid hemorrhage, which frequently results in signs of meningeal irritation, such as neck stiffness, Kernig sign, and low back pain.
Unlike the dura mater and arachnoid, the delicate pia mater (see Figure 14-15) closely adheres to the surface of the brain and spinal cord and even follows the sulci and fissures. It provides support for blood vessels serving brain tissue. The choroid plexuses, structures that produce CSF, arise from the pia mater. The spinal cord is anchored to the vertebrae by extensions of the meninges called denticulate ligaments. The meninges continue beyond the end of the spinal cord to the lower portion of the sacrum. CSF, contained within the subarachnoid space, also circulates down to the large lumbar cistern, which extends from the second lumbar vertebra to the second sacral vertebra. Cisterns are expanded areas of the subarachnoid space. The cerebellomedullary cistern (cisterna magna) and the pontine cisterns are two other important cisterns.
The meninges form potential and real spaces important to understanding functional and pathologic mechanisms. For example, between the dura mater and skull lies a potential space termed the epidural space (see Figure 14-15). In the spinal canal is a real epidural space filled with fatty tissue and a venous plexus. The arterial supply to the meninges consists of blood vessels that lie within grooves in the skull. As a result of trauma, the skull can be fractured and the blood vessels disrupted. The ruptured vessels can lead to an accumulation of blood within the epidural space, called an epidural hematoma (see Chapter 17). Persons with alcoholism often fall and injure their head, resulting in an epidural hematoma. An inflammation of the meninges (meningitis) also can have life-threatening implications because of the relative proximity to the brain. (Disorders of the CNS are discussed in Chapter 17.)
Cerebrospinal Fluid and the Ventricular System
Cerebrospinal fluid (CSF) is a clear, colorless fluid similar to blood plasma and interstitial fluid. The intracranial and spinal cord structures float in CSF and are thereby protected from jolts and blows. The buoyant properties of the CSF also prevent the brain from tugging on meninges, nerve roots, and blood vessels. (Constituents of CSF are listed in Table 14-4.) Between 125 and 150 ml of CSF, approximately the quantity of a small cup of coffee, is circulating within the ventricles (small cavities) and subarachnoid space at any given time. Approximately 600 ml of CSF is produced daily.
Table 14-4
Composition of Cerebrospinal Fluid
| Constituent | Normal Value |
| Na+ | 148 mM |
| K+ | 2.9 mM |
| Cl− | 125 mM |
| HCO3− | 22.9 mM |
| Glucose (fasting) | 50-75 mg/dl (60% of serum glucose) |
| Ph | 7.3 |
| Protein | 15-45 mg/dl |
| Albumin | 80% |
| Gamma globulin | 6%-10% |
| Cells | |
| White (lymphocytes) | 0-6/mm3 |
| Red (red blood cell [RBC]) | 0/mm3 |
Cl−, Chloride; HCO3−, bicarbonate; K+, potassium; Na+, sodium.
The choroid plexuses in the lateral, third, and fourth ventricles produce the major portion of CSF. (Ventricles are illustrated in Figure 14-15.) These plexuses are characterized by a rich network of blood vessels, supplied by the pia mater, that lie in close contact with the ependymal cells of the ventricles.
The CSF exerts pressure within the brain and spinal cord. When a person is lying down, CSF pressure is approximately 120 to 180 mm of water pressure, or approximately 9 to 14 mmHg pressure. CSF flow is a result of a pressure gradient between the arterial system and the CSF-filled cavities. Beginning in the lateral ventricles, the CSF flows through the interventricular foramen (foramen of Monro) into the third ventricle and then passes through the cerebral aqueduct (aqueduct of Sylvius) into the fourth ventricle. From the fourth ventricle, the CSF may pass through either the paired lateral apertures (foramina of Luschka) into the pontine cisterns, located along the basal pons, or the midline median aperture (foramen of Magendie) into the cerebellomedullary cistern before communicating with the subarachnoid spaces of the brain and spinal cord. The CSF does not, however, accumulate. Instead, it is reabsorbed into the venous circulation through the arachnoid villi, primarily located superior to the falx cerebri in the superior sagittal sinus. The arachnoid villi protrude from the arachnoid space, through the dura mater, and lie within the blood flow of the venous sinuses. CSF is reabsorbed by means of a pressure gradient between the arachnoid villi and the cerebral venous sinuses. The villi function as one-way valves directing CSF outflow into the blood but preventing blood flow into the subarachnoid space. Thus CSF is derived from the blood, and after circulating throughout the CNS, it returns to the blood.
Samples of CSF are withdrawn for diagnostic purposes either (1) by inserting a needle between the third and fourth lumbar vertebrae into the lumbar cistern (subarachnoid space)—a procedure called lumbar puncture—or (2) from an intraventricular catheter. Spinal anesthesias (blocks) are administered in a manner similar to the lumbar puncture.
Vertebral Column
The vertebral column (Figure 14-16) is composed of 33 vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 fused sacral, and 4 fused coccygeal. Between each interspace (except the fused sacral and coccygeal vertebrae) is an intervertebral disk (Figure 14-17). At the center of the intervertebral disk is the nucleus pulposus, a pulpy mass of elastic fibers. The intervertebral disk functions to absorb shocks, preventing damage to the vertebrae. The intervertebral disk is also a common source of back problems. If too much stress is applied to the vertebral column, the disk contents may rupture and protrude into the spinal canal, causing compression of the spinal cord or nerve roots. The disks also can degenerate.
Blood Supply
The brain receives approximately 20% of the cardiac output, or 800 to 1000 ml of blood flow per minute. Carbon dioxide serves as a primary regulator for blood flow within the CNS. It is a potent vasodilator in the CNS, and its effects ensure an adequate blood supply.
The brain derives its arterial supply from two systems: the internal carotid arteries and the vertebral arteries (Figure 14-18). The internal carotid arteries, anteriorly, supply a proportionately greater amount of blood flow. They take their origin from the common carotid arteries, enter the cranium through the base of the skull, and pass through the caver-nous sinus. After giving off some small branches, they divide into the anterior and middle cerebral arteries (Figure 14-19). The vertebral arteries, posteriorly, originate as branches off the subclavian arteries, pass through the transverse foramina of the cervical vertebrae, and enter the cranium through the foramen magnum. They join at the junction of the pons and medulla oblongata to form the basilar artery. The basilar artery divides at the level of the midbrain to form paired posterior cerebral arteries. Three major paired arteries perfuse the cerebellum and brainstem and originate from the posterior arterial supply: the posterior inferior cerebellar artery, off the vertebral artery; and the anterior inferior cerebellar and superior cerebellar arteries, off the basilar artery. The basilar artery also gives rise to small pontine arteries. The large arteries on the surface of the brain and their branches are called superficial arteries (conducting arteries). The small branches that project into the brain are termed projecting arteries (nutrient arteries). Occluding any of these vessels can cause neurologic signs and symptoms that are often diagnostically unique.
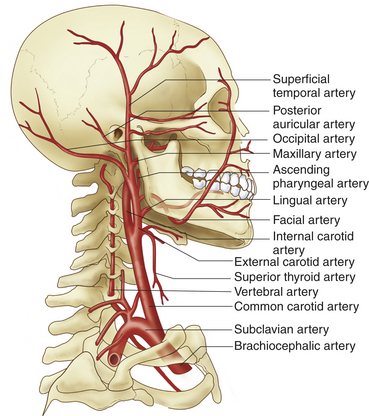
Figure 14-18 Major arteries of the head and neck. (From Patton KT, Thibodeau GA: Anatomy & physiology, ed 7, St Louis, 2010, Mosby.)
The arterial circle (circle of Willis) (see Figure 14-19) is a structure credited with the ability to compensate for reduced blood flow from any one of the major contributors (collateral blood flow). The arterial circle is formed by the posterior cerebral arteries, posterior communicating arteries, internal carotid arteries, anterior cerebral arteries, and anterior communicating artery. The anterior cerebral, middle cerebral, and posterior cerebral arteries leave the arterial circle and extend to various brain structures. (Table 14-5 and Figure 14-20 illustrate structures served, functional relationships, and pathologic considerations related to occlusion of cerebral arteries.)
Table 14-5
Arterial Systems Supplying the Brain
| Arterial Origin | Structures Served | Conditions Caused by Occlusion |
| Anterior cerebral artery | Basal ganglia; corpus callosum; medial surface of cerebral hemispheres; superior surface of frontal and parietal lobes | Hemiplegia on contralateral side of body, greater in lower than in upper extremities |
| Middle cerebral artery | Frontal lobe; parietal lobe; temporal lobe (primarily cortical surfaces) | Aphasia in dominant hemisphere and contralateral hemiplegia (see Chapter 16) |
| Posterior cerebral artery | Part of diencephalon and temporal lobe; occipital lobe | Visual loss; sensory loss; contralateral hemiplegia if cerebral peduncle affected |
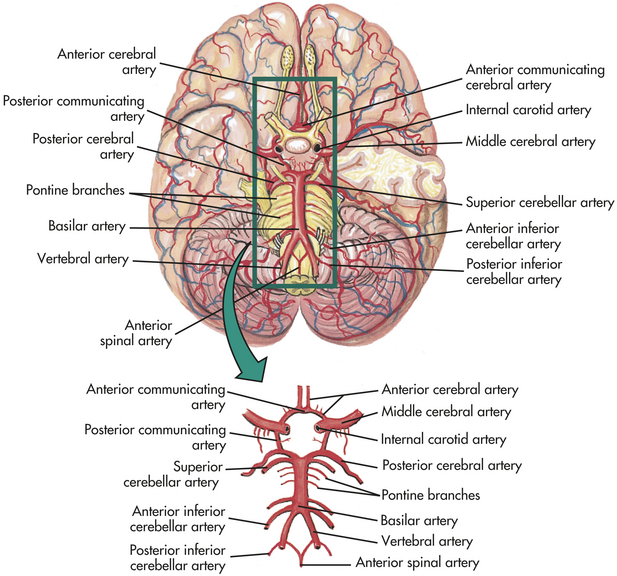
Figure 14-19 Arteries at the base of the brain. The arteries that compose the circle of Willis are the two anterior cerebral arteries, joined to each other by the anterior communicating two short segments of the internal carotids, off of which the posterior communicating arteries connect to the posterior cerebral arteries. (Modified from Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
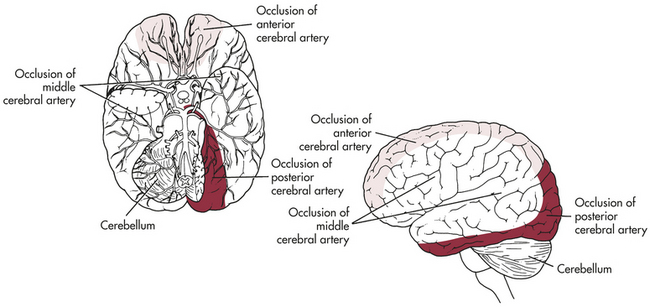
Figure 14-20 Areas of the brain affected by occlusion of the anterior, middle, and posterior cerebral artery branches. A, Inferior view. B, Lateral view.
Cerebral venous drainage does not parallel (lie side by side) its arterial supply, whereas the venous drainage of the brainstem and cerebellum does parallel the arterial supply of the structures. The cerebral veins are classified as superficial veins and deep cerebral veins. The veins drain into venous plexuses and dural sinuses (formed between the dural layers) and eventually join the internal jugular veins at the base of the skull (Figure 14-21). Adequacy of venous outflow can have a significant effect on intracranial pressure. For example, in individuals with head injury, turning or letting the head fall to the side partially occludes venous return and can increase intracranial pressure because of decreased flow through the jugular veins.
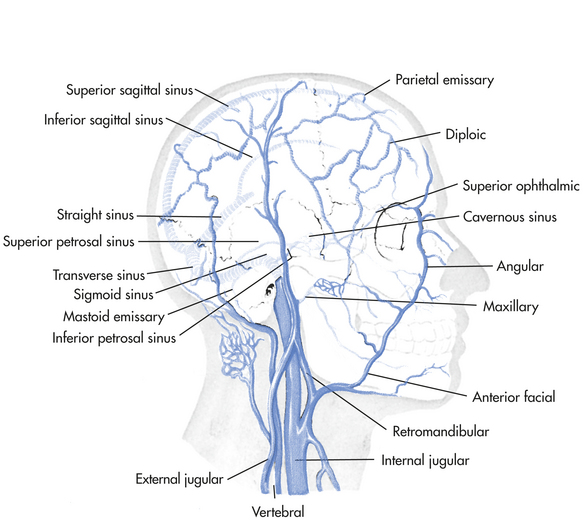
Figure 14-21 Large veins of the head. Deep veins and dural sinuses are projected on the skull. Note connections (emissary veins) between the superficial and deep veins. (From Rudy EB, editor: Advanced neurological and neurosurgical nursing, St Louis, 1984, Mosby.)
The blood-brain barrier is discussed in Box 14-4.
Blood Supply to the Spinal Cord
The spinal cord derives its blood supply from branches off the vertebral arteries and from branches from various regions of the aorta (Figure 14-22). The anterior spinal arteries and the paired posterior spinal arteries branch off the vertebral artery at the base of the cranium and descend alongside the spinal cord. Arterial branches from vessels exterior to the spinal cord follow the spinal nerve through the intervertebral foramina, pass through the dura, and divide into the anterior and posterior radicular arteries.
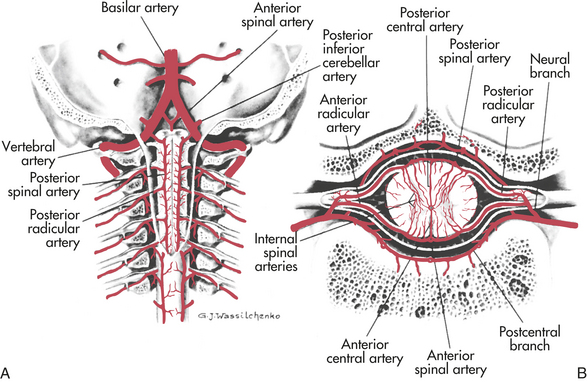
Figure 14-22 Arteries of the spinal cord. A, Arteries of cervical cord exposed, posterior view. B, Arteries of spinal cord diagrammatically shown in horizontal section. (From Rudy EB, editor: Advanced neurological and neurosurgical nursing, St Louis, 1984, Mosby.)
The radicular arteries eventually reconnect to the spinal arteries. Branches from the radicular and spinal arteries form plexuses whose branches penetrate the spinal cord, supplying the deeper tissues. Venous drainage parallels the arterial supply closely and drains into venous sinuses located between the dura and periosteum of the vertebrae.
PERIPHERAL NERVOUS SYSTEM
The cranial and spinal nerves, including their branches and ganglia, constitute the PNS. A peripheral nerve (cranial or spinal) is composed of individual axons/dendrites, with most wrapped in a myelin sheath. These individual fibers are arranged in bundles called fascicles (see Figure 14-1 and Figure 14-23, B). The coverings supply structural support, a blood supply, and interstitial compartments necessary for the supply of essential electrolytes to support nerve impulse conduction.
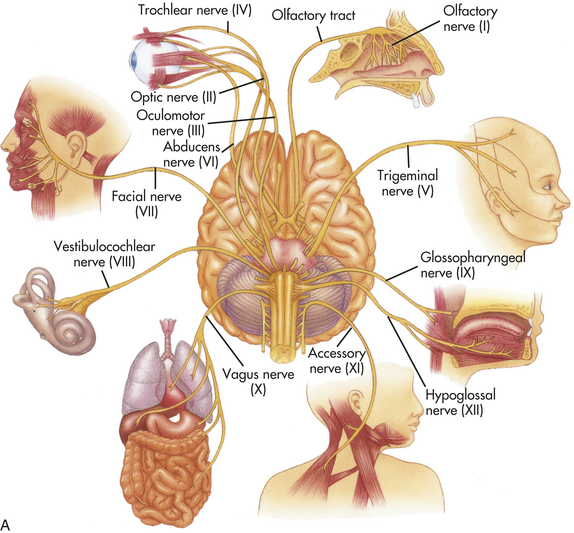
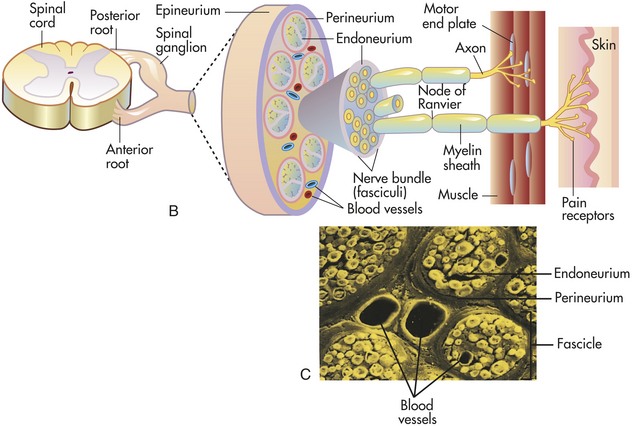
Figure 14-23 Cranial and peripheral nerves. A, Ventral surface of the brain showing attachment of the cranial nerves. B, Peripheral nerve trunk and coverings. C, Scanning electron micrograph of a freeze-fractured preparation of peripheral nerve. (A and C from Thibodeau GA, Patton KT: Anatomy & physiology, ed 6, St Louis, 2007, Mosby.)
The 31 pairs of spinal nerves derive their names from the vertebral level from which they exit. There are eight cervical spinal nerves. The first cervical nerve exits above the first cervical vertebra, and the rest of the spinal nerves exit below their corresponding vertebrae. From the thoracic region (and inferiorly) nerves correspond to the vertebral level above their exit (see Figure 14-10).
Spinal nerves contain both sensory and motor neurons and are called mixed nerves. They arise as rootlets from the anterior and posterior horn cells of the spinal cord. These two spinal nerve roots converge in the region of the intervertebral foramen to form the spinal nerve (see Figure 14-11). Shortly after converging, the spinal nerve divides into anterior and posterior rami (branches). The anterior rami (except the thoracic) initially form plexuses (networks of nerve fibers), which then branch into the peripheral nerves. Instead of forming plexuses, the thoracic nerves pass through the intercostal spaces and innervate regions of the thorax.
The main spinal nerve plexuses innervate the skin and the underlying muscles of the limbs. The brachial plexus, for example, is formed by the last four cervical nerves (C5-C8) and the first thoracic nerve (T1). The brachial plexus innervates the nerves of the arm, wrist, and hand. The lumbar plexus (L2-L4) and sacral plexus (L5-S5) contain nerves that innervate the anterior and posterior portions of the lower body, respectively.
The posterior rami of each spinal nerve, with their many processes, are distributed to a specific area in the body. Sensory signals thus arise from specific sites associated with a specific spinal cord segment. Specific areas of cutaneous (skin) innervation at these spinal cord segments are called dermatomes. The dermatomes of various spinal nerves are distributed in a fairly regular pattern, although adjacent regions between dermatomes can be innervated by more than one spinal nerve.
Like spinal nerves, cranial nerves are categorized as peripheral nerves. Most of these are mixed nerves (like the spinal nerves), although some are purely sensory or motor. Cranial nerves arise from nuclei in the brain and brainstem. (Figure 14-23, A, illustrates their location, and Table 14-6 describes structural and functional characteristics.)

AUTONOMIC NERVOUS SYSTEM
Components of the ANS are located in both the CNS and PNS; however, the ANS is considered part of the efferent division of the PNS, even though visceral afferent neurons are an important part of this system. Many neurons of the ANS travel in spinal nerves and certain cranial nerves. The widespread activity of this system indicates that its components are distributed all over the body. The peripheral autonomic nerves carry mainly efferent fibers. The motor component of the ANS is a two-neuron system consisting of preganglionic neurons (myelinated) and postganglionic neurons (unmyelinated). This arrangement contrasts with the somatic nervous system, in which a single motor neuron travels from the CNS to the innervated structure. Visceral afferent neurons have their cell bodies in some sensory and cranial ganglia and their fiber processes traveling in peripheral nerves. The CNS has autonomic areas in the intermediolateral horns of the spinal cord, cardiovascular and respiratory centers in the reticular formation, and both sympathetic and parasympathetic areas in the hypothalamus. CNS pathways interconnect all these areas.
The ANS coordinates and maintains a steady-state among visceral (internal) organs, such as regulation of cardiac muscle, smooth muscle, and the glands of the body. This system is considered an involuntary system because one generally cannot will these functions to happen. The ANS is separated structurally and functionally into two divisions: (1) the sympathetic nervous system (Figure 14-24) and (2) the parasympathetic nervous system (Figure 14-25).
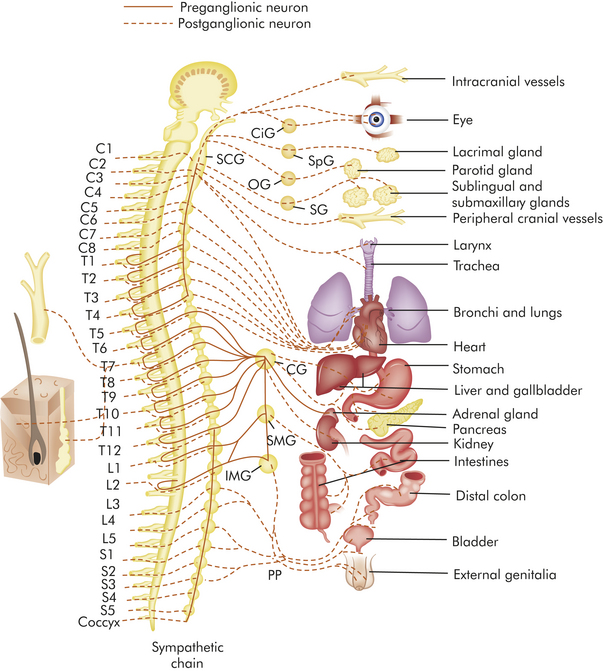
Figure 14-24 Sympathetic division of the autonomic nervous system. Fibers of the parasympathetic system pass through the CG and SMG, but these ganglia are not part of the parasympathetic system. CG, Celiac ganglion; CiG, ciliary ganglion; IMG, inferior mesenteric ganglion; OG, otic ganglion; PP, pelvic plexus; SCG, superior cervical ganglion; SG, submandibular ganglion; SMG, superior mesenteric ganglion; SpG, sphenopalatine ganglion. (Redrawn from Rudy EB, editor: Advanced neurological and neurosurgical nursing, St Louis, 1984, Mosby.)
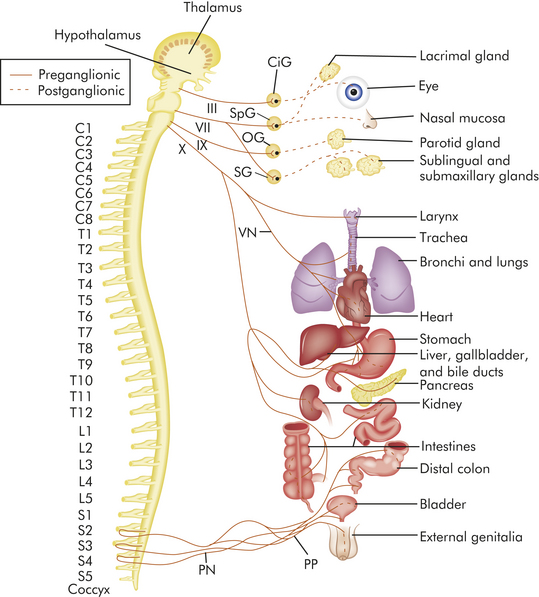
Figure 14-25 Parasympathetic division of the autonomic nervous system. CiG, Ciliary ganglion; OG, otic ganglion; PN, pelvic nerve; PP, pelvic plexus; SG, submandibular ganglion; SpG, sphenopalatine ganglion; VN, vagus nerve. Fibers of the parasympathetic system pass through the CG and SMG, but these ganglia are not part of the parasympathetic system. (From Rudy EB, editor: Advanced neurological and neurosurgical nursing, St Louis, 1984, Mosby.)
Anatomy of the Sympathetic Nervous System
The sympathetic nervous system functions to mobilize energy stores in times of need (e.g., in the fight-or-flight response) (see Figure 10-2; see also Chapter 10). The sympathetic division receives its innervation from cell bodies located from the first thoracic (T1) through the second lumbar (L2) regions of the spinal cord and is therefore called the thoracolumbar division. The preganglionic axons of the sympathetic division form synapses shortly after leaving the cord in the sympathetic (paravertebral) ganglia. At this point the impulse may travel several ways: (1) directly across the same ganglion level and form a synapse with the cell bodies of the postganglionic neuron, (2) up or down the sympathetic chain before forming synapses with a higher or lower postganglionic neuron (divergence), or (3) through the chain ganglion without synapsing (see Figure 14-24). Some preganglionic axons form pathways called splanchnic nerves, which lead to collateral ganglia surrounding the abdominal aorta. The collateral ganglia are named according to the branches of the aorta nearest them, namely, the celiac, superior mesenteric, and inferior mesenteric. The preganglionic neurons synapse with postganglionic neurons within the collateral ganglia. These postganglionic neurons leave the collateral ganglia and innervate the viscera below the diaphragm.
Preganglionic sympathetic neurons that innervate the adrenal medulla also travel in the splanchnic nerves and do not synapse before reaching the gland. The secretory cells in the adrenal medulla are considered modified postganglionic neurons. Because preganglionic sympathetic fibers are all myelinated, travel to the adrenal medulla is quick, and innervation causes the rapid release of epinephrine and norepinephrine. Epinephrine and norepinephrine are mediators of the fight-or-flight response (see Chapter 10).
Anatomy of the Parasympathetic Nervous System
The parasympathetic nervous system functions to conserve and restore energy. The nerve cell bodies of this division are located in the cranial nerve nuclei and in the sacral region of the spinal cord and therefore constitute the craniosacral division. Unlike the sympathetic division, the preganglionic fibers in the parasympathetic division travel to ganglia close to the organs they innervate before forming synapses with the relatively short postganglionic neurons (see Figure 14-25). Parasympathetic nerves arising from nuclei in the brainstem travel to the viscera of the head, thorax, and abdomen within cranial nerves—including the oculomotor (III), facial (VII), glossopharyngeal (IX), and vagus (X) nerves.
Preganglionic parasympathetic nerves that originate from the sacral region of the spinal cord run either separately or together with some spinal nerves. The preganglionic axons join to form the pelvic nerve, which innervates the viscera of the pelvic cavity. These preganglionic axons synapse with postganglionic neurons in terminal ganglia located close to the organs they innervate.
Neurotransmitters and Neuroreceptors
Sympathetic preganglionic fibers and parasympathetic preganglionic and postganglionic fibers release acetylcholine—the same neurotransmitter released by somatic efferent neurons (Figure 14-26; also see Figure 14-23). These fibers are characterized by cholinergic transmission. Most postganglionic sympathetic fibers release norepinephrine (adrenaline) and thus are considered to function by adrenergic transmission. A few postganglionic sympathetic fibers, such as those that innervate the sweat glands, release acetylcholine.
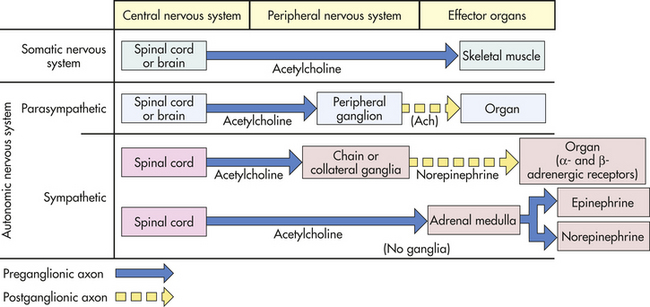
Figure 14-26 The autonomic nervous system and the type of neurotransmitters secreted by preganglionic and postganglionic fibers. Note that all preganglionic fibers are cholinergic (Ach). A somatic nerve is used for comparison.
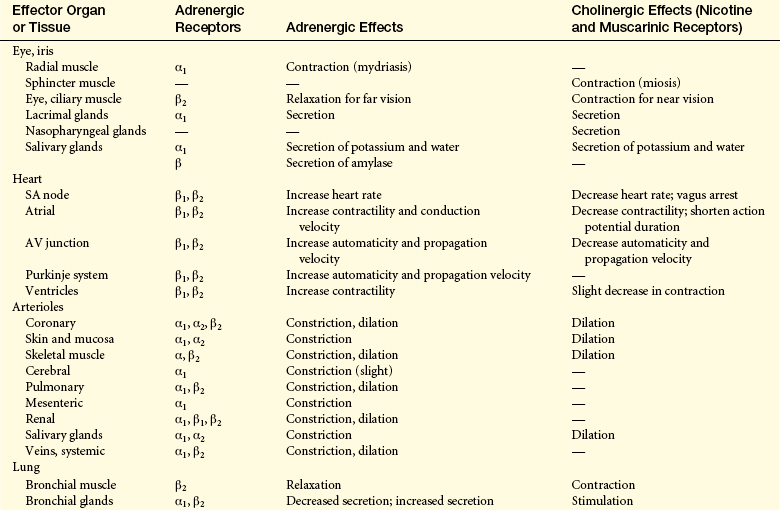
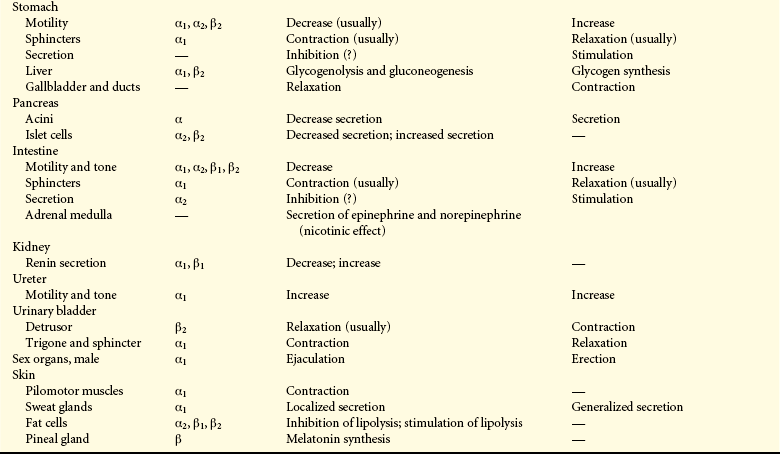
The action of catecholamines (epinephrine, norepinephrine, dopa) varies with the type of neuroreceptor stimulated. It should be remembered that catecholamines also are released by the adrenal medulla gland that physiologically and biochemically resembles the sympathetic nervous system. Two types of adrenergic receptors exist: α- and β-adrenergic receptors. Cells of the effector organs may have only one or both types of adrenergic receptors. The α-adrenergic receptors have been further subdivided according to the action produced: α1-adrenergic activity is associated mostly with excitation or stimulation; α2-adrenergic activity is associated with relaxation or inhibition. Most of the α-adrenergic receptors on effector organs belong to the α1-adrenergic class. The β-adrenergic receptors are classified as β1-adrenergic receptors (which facilitate increased heart rate and contractility and cause the release of renin from the kidney) and β2-adrenergic receptors (which facilitate all of the remaining effects attributed to β-adrenergic receptors).6 Norepinephrine stimulates all α-adrenergic and β1-adrenergic receptors and only certain β2-adrenergic receptors. The primary response from norepinephrine, however, is stimulation of the α1-adrenergic receptors that cause vasoconstriction. Epinephrine strongly stimulates all four types of receptors and induces general vasodilation because of the predominance of β-adrenergic receptors in muscle vasculatures. (Table 14-7 summarizes the effects of neuroreceptors on their effector organs.)
Functions of the Autonomic Nervous System
Many body organs are innervated by the sympathetic and parasympathetic nervous systems. The two divisions frequently cause opposite responses; for example, sympathetic stimulation of the gastrointestinal (GI) tract causes decreased peristalsis, whereas parasympathetic stimulation of the GI tract increases peristalsis. In general, sympathetic stimulation promotes responses that are concerned with the protection of the individual. For example, sympathetic activity increases blood sugar levels and temperature and raises blood pressure. In emergency situations a generalized and widespread discharge of the sympathetic system occurs. This is accomplished by an increased firing frequency of sympathetic fibers and by activation of sympathetic fibers normally silent and at rest (fibers to the sweat glands, pilomotor muscles, and the adrenal medulla, as well as vasodilator fibers to muscle). Regulation of vasomotor tone is considered the single most important function of the sympathetic nervous system. (Figure 14-27 illustrates some of the most important functions of the sympathetic nervous system; also see Figure 10-2.)
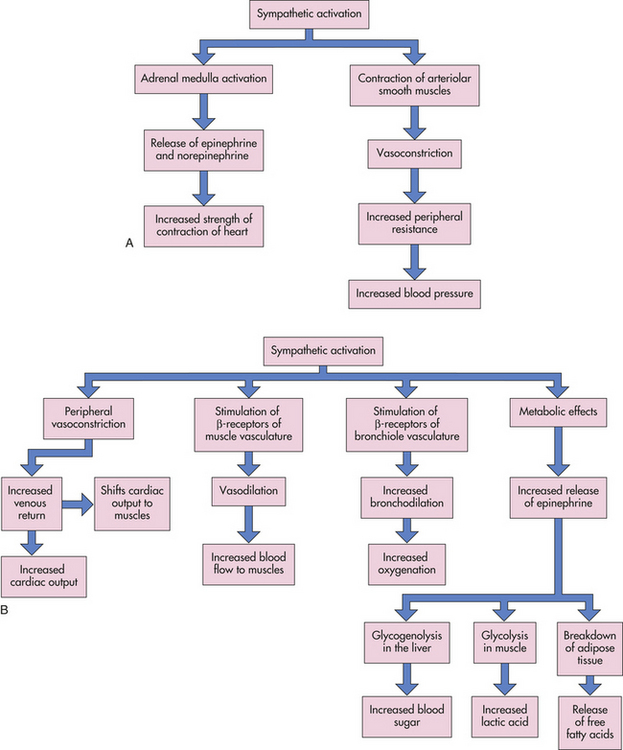
Figure 14-27 Some important functions of the sympathetic nervous system. A, Regulation of vasomotor tone. B, Regulation of strenuous muscular exercise (fight-or-flight response). (See also Chapter 10 and Figure 10-2 for more detail of the stress response.)
Increased parasympathetic activity promotes rest and tranquility and is characterized by reduced heart rate and enhanced visceral functions leading to digestion. Stimulation of the vagus nerve in the GI tract increases peristalsis and secretion, as well as relaxation of sphincters. Activation of parasympathetic fibers in the head, provided by cranial nerves III, VII, and IX, causes constriction of the pupil, tear secretion, and increased salivary secretion. Stimulation of the sacral division of the parasympathetic system contracts the urinary bladder and facilitates the process of genital erection.
The parasympathetic system lacks the generalized and widespread response of the sympathetic system. Specific parasympathetic fibers are activated to regulate particular functions. Although the actions of the parasympathetic and sympathetic systems usually are antagonistic, there are exceptions. Changes in the shape of the lens (for near vision) require only oculomotor parasympathetic activity. Most of the blood vessels involved in the control of blood pressure are innervated by sympathetic nerves. Peripheral vascular resistance is increased and decreased by the relative activity of the sympathetic division without a counteracting parasympathetic component. To decrease blood pressure, therefore, it is more important to block or paralyze the continuous (tonic) discharge of the sympathetic system than to promote parasympathetic activity.
Aging and the Nervous System
The CNS mechanisms involved in the aging process are extremely complex, and many questions concerning the neurologic effects of aging have yet to be answered. Some of the identified mechanisms associated with aging are pathologic, but the distinction between these mechanisms and those that are a part of the normal aging process remains somewhat cloudy.
Structural Changes with Aging
The CNS demonstrates many structural changes during the aging process. The primary mechanism responsible for most of these structural changes is a decrease in the number of neurons. Predominant external features of the aging brain include decreased brain weight and size (primarily the frontal hemispheres), increased adherence of the dura mater to the skull, fibrosis and thickening of the meninges, narrowed gyri, and widened sulci with a corresponding increase in the size of the subarachnoid space. The basal ganglia and ventricular system are internal structures that commonly reveal changes with aging. The basal ganglia reveal aberrations in vascular structures, and the ventricles (primarily the lateral and third ventricles) are enlarged, probably because they occupy much of the space left by dead neurons.
Cellular Changes with Aging
Practically every cell type within the CNS reflects specific responses to aging. A decrease in the number of neurons characterizes aging. Although neuronal cell loss is a general feature of aging, the effects are not consistent with deteriorating mental function or age of the individual.7,8 Controversy regarding the effects of neuronal cell loss is ongoing.
Principal cellular changes associated with aging include dendrite structure, lipofuscin deposition, and the presence of neurofibrillary tangles, senile plaques, and Lewy bodies. Kelly and colleagues9 described a decreased number of dendritic processes and their multiple synaptic connections. Lipofuscin, a yellow-brown fatty pigment, is found to be deposited intracellularly in increased amounts with age. Controversy still exists concerning whether increasing intracellular quantities of lipofuscin in aging brains and neuropathologic conditions cause these changes leading to cell death or if they are a result of some other underlying factors.10 For example, decreased circulation, genetic predisposition, or disruption of protein synthesis might be associated factors.
Senile plaques (areas of nerve degeneration) are found in the interstitial spaces of the cerebral cortex associated with tissue degeneration. Neurofibrillary tangles involve degenerative changes in neural protein fibers. These entities also are common in Alzheimer disease and some other forms of dementia. At present definitive evidence of a link between quantitative cellular changes and nervous system function in aging individuals is growing.
Closely paralleling cell function is a selective alteration in neurotransmitter function. One potentially fruitful area of research is investigation of possible correlations between the effects of acetylcholine (i.e., cholinergic transmission) and defects of memory and cognitive function associated with aging.11
Functional Changes with Aging
Because of integrative processes in the CNS, the consequences of aging have widespread implications for critical steady state, psychologic, and social function. Many theories have been proposed to explain the observations of progressive slowing of neurologic responses seen in older adults (Table 14-8). Studies of changes in brain electrical activity have been helpful in determining alterations in neural function. Timiras12 described the relationship between transmission of neural signals and slowing of responses observed in older adults: “It is evident that the efficacy of the signals may be disturbed not only by irregularities in the action of cells carrying the signals but also by the amount of random background activity.” This background activity is termed neural noise.
Table 14-8
Common Neurologic Signs in Aging
| Neurologic Sign | Examples | Changes in Response |
| Reflexes | Ankle reflex | Usually the first tendon reflex to be lost in older adults |
| Superficial reflex | Decreased or absent responsiveness | |
| Primitive reflexes (reflexes seen normally in infancy but that subside with maturity) | Suck and grasp | Reappearance with aging |
| Sensation | Taste and smell | Progressive deficit |
| Pain | Increased pain threshold, although subjective complaints increase | |
| Vibratory sense | Decreased | |
| Vision | Decreased visual color sense in a significant percentage of older adults; pupils commonly smaller; slowing of papillary relaxation and accommodation | |
| Motor function | Physiologic tremor | Exaggeration of normally unnoticeable resting tremor that is present at all ages |
| Neuromuscular control | Decreased, resulting in postural effects | |
| Posture | Stance commonly shows increased flexion of hips and knees; swaying motion while standing in one position more common | |
| Gait | Shuffling or shortened stride; loss of arm movement with walking | |
| Muscular atrophy | Age-associated loss of muscle fibers |
TESTS OF NERVOUS SYSTEM FUNCTION
Skull and Spine Roentgenograms
Roentgenograms (x-ray films) of the skull or spine from multiple angles (views) are used primarily to localize bony defects, bone density, erosion, or calcified structures. The pineal gland in older people becomes calcified and is useful as an internal brain landmark. X-ray films are probably the most commonly used radiologic studies.
Computed Tomography
Computed tomography (CT) creates two-dimensional reconstructions from multiple radiologic images (x-rays) using computer-assisted analysis. It is capable of demonstrating fine distinctions in densities of a variety of tissues. CT imaging is a safe and noninvasive procedure used in evaluating cranial and spinal structures, as well as hemorrhages, tumors, and distortions in the brain caused by pressure differences. A variety of contrast media also are commonly used in conjunction with this procedure to aid in enhanced delineation of selected structures. Spiral or helical CT uses a multidector scanner mounted on a rotating gantry to provide several axial images for imaging a large continuous anatomic area in a matter of seconds. Helical CT angiography uses contrast media for detection of aneurysms or ruptured aneurysms.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is a commonly used testing modality. It uses a static magnetic field, instead of x-rays, to orient physiologic atomic particles. Disruption of this orientation by excitation of the particles using serial radiofrequency pulsations provides the image data. The specific tissue reaction is computer analyzed to give an image of exquisite detail, similar to that provided by CT. The MRI also provides reconstruction of images in three views at right angles (i.e., axial, sagittal, coronal). MRI is reported to have none of the adverse effects associated with radiation examinations. Magnetic resonance spectroscopy can be completed at the same time as a standard MRI by analyzing the
WHAT’S NEW?
Reinforcement Center (Nucleus Accumbens)
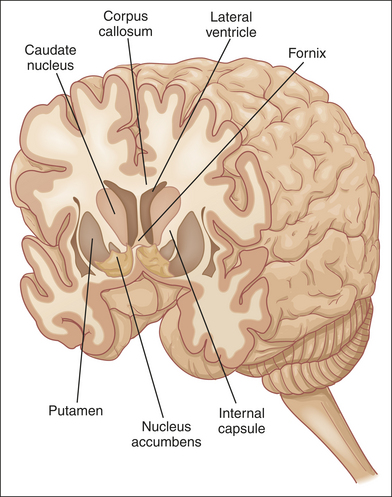
A small nucleus (see accompanying figure) in the septal area of the frontal lobe has become a center of intense research. The nucleus accumbens is considered to be the principal site of action for addictive drugs and the anatomic basis of positive reinforcement. The nucleus accumbens has input from the mesencephalon (ventral tegmental area) and many other neural areas. Mesencephalon neurons project dopamine to the nucleus accumbens and can affect its activity. Other neurotransmitters involved in this positive feedback system are gamma-aminobutyric acid (GABA), serotonin, and glutamate. Opiates can interfere with this system by allowing too much dopamine to go to the nucleus accumbens. The nucleus accumbens is involved in drug craving and withdrawal symptoms and therefore is clinically important.
Data from Wheeler RA, Carelli RM: Neuropharmacology 56 (Suppl 1):149-159, 2009; Goto Y, Grace AA: Trends Neurosci 31(11):552-558, 2008; Everitt BJ et al: Philos Trans R Soc Lond B Biol Sci 363(1507):3125-3135, 2008.
chemical composition of proton (hydrogen) or phosphorus-based molecules and is useful for evaluating the chemical composition and function of various regions of the brain.
Magnetic Resonance Angiography
A newer addition to MRI is magnetic resonance angiography (MRA). Special imaging techniques allow the visualization of blood vessels in great detail. MRA is likely to become indispensable, alone or in conjunction with cerebral angiography, in detecting and localizing pathologic lesions of the circulatory system of the brain.
Positron-Emission Tomography Scan
The positron-emission tomography (PET) scan uses CT imaging to detect the emission of positive electrons from radioactive substances. These substances are injected into the bloodstream or administered as inhaled gases. As they are distributed in tissues, they display characteristic patterns that indicate physiologic and metabolic processes, for example, glucose and oxygen uptake, cerebral blood flow, neural and neurotransmitter function, and the effects of drugs. As a research tool, PET is being used to visualize the specific brain sites that are involved in the processing of information in the brain.
Brain Scan
The brain scan images radionuclide substances (technetium [99mTc]) that have been introduced into the bloodstream. For example, visualization of tissue uptake of the radioactive agent provides an indication of blood-brain barrier integrity (increased uptake of the agent indicates disruption). This scanning technique also can identify abnormalities in blood flow dynamics and cellular metabolic function. The brain scan is particularly helpful in detecting abnormal vascularity resulting from neoplasms, abscesses, and vascular lesions.
Isotope cisternography is another radionuclide imaging technique that uses brain scan imaging to detect CSF flow, CSF resorption, and integrity of CSF pathways. The radionuclide agent in this case is injected directly into the subarachnoid space. Under normal conditions the agent passes over the cortical surface and is resorbed through the arachnoid villi. Demonstration of the agent in the ventricular system after a specific period of time indicates CSF obstruction; that is, the CSF back flows from the subarachnoid space into the ventricles.
Cerebral Angiography
Angiography is a radiologic technique that demonstrates cerebrovascular blood flow. This technique commonly is performed by the introduction of a small catheter into the femoral artery. The catheter is then passed to the level of the cerebral circulation and through the aorta, and a contrast dye is injected. Serial x-ray films are then taken. These films demonstrate flow of the dye through the cerebral vasculature and provide information on patency, location, size, and flow pattern of the vessels. Another technique used in cerebral angiography is the retrograde (reverse flow) injection of the dye through catheterization of a brachial, axillary, subclavian, or femoral vein.
Myelography
A myelogram demonstrates intraspinal anatomy by the introduction of a radiographic dye into the lumbar subarachnoid space or the cerebellomedullary cistern (cisterna magna). The dye is allowed to flow in a cephalic direction, as in the case of a lumbar injection, or inferiorly in a cerebellomedullary cistern puncture. X-ray films are then obtained. The distribution of the dye delineates spinal cord and nerve root structure and integrity.
Echoencephalography (Ultrasound)
Echoencephalography, or ultrasound, is a safe, noninvasive procedure using sound waves that are deflected at differing rates, depending on the density of the tissue. Information is processed and displayed on an oscilloscope screen. It is useful primarily in the detection of structural characteristics of intracranial space–occupying mass lesions and the determination of ventricular dimensions, especially in newborns.
Electroencephalography
The electroencephalograph (EEG) is a recording of electrical impulses, arising from the cortical surface of the brain, which is detected by scalp electrodes. The recording of brain wave patterns is analyzed for alterations or localization (or both) of specific electrical activity. This test is especially useful in detecting and localizing foci that initiate seizure activity. It is also an important technique in determining, from a person’s brain activity, whether the person is legally “brain dead.”
Evoked Potentials
Evoked potentials (EPs) are a method of detecting electrical brain activity that results from a stimulus—primarily auditory, visual, or peripheral sensory. Electrical activity is computer formatted to display changes in trends. The primary uses of EPs include perioperative detection of sensory pathway integrity and disease- or drug-related sensory dysfunction.
Cerebrospinal Fluid Analysis
CSF generally is obtained from the lumbar or cisternal subarachnoid space by means of a hollow needle that allows passive flow. The lumbar puncture is performed most often at the L3-L4 interspace (below the level of the spinal cord at L1-L2). Cisternal puncture is performed by the insertion of a needle into the cerebellomedullary cistern using an approach from the back of the neck in the region of the foramen magnum. CSF pressure is commonly measured during these procedures. The CSF can be analyzed also for gross characteristics and constituents (color, blood cells, electrolytes, and protein) and cultured for microorganisms (Table 14-9).
SUMMARY REVIEW
Overview and Organization of the Nervous System
Table 14-9
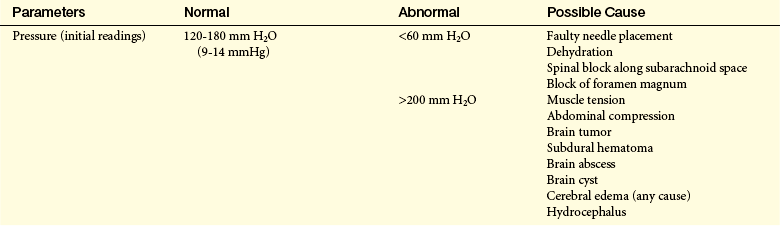
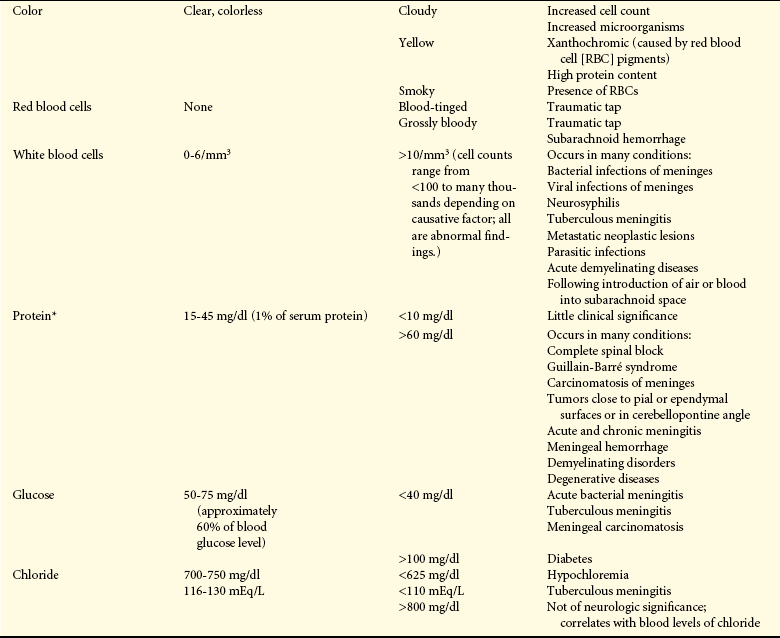
∗NOTE: If CSF contains blood, this will raise the protein level.
Data from Rudy EB, editor: Advanced neurological and neurosurgical nursing, St Louis, 1984, Mosby.
1. The divisions of the nervous system have been categorized as either structural (CNS and PNS) or functional (somatic nervous system and ANS).
2. The CNS is contained within the brain and spinal cord.
3. The PNS is composed of cranial and spinal nerves that carry impulses toward the CNS (afferent) and away from the CNS (efferent) to target organs or skeletal muscle.
1. The neuron and neuroglial cells make up nervous tissue. The neuron is specialized to transmit and receive electrical and chemical impulses, and the neuroglial cell provides supportive functions. The neuron is further divided into unipolar, pseudounipolar, bipolar, and multipolar categories, according to structure and particular mechanics of impulse transmission.
2. The neuron is composed of a cell body, one or more dendrites, and an axon. A myelin sheath around selected axons forms an insulation that allows quicker nerve impulse conduction, referred to as saltatory conduction.
3. Neurons have four basic types of cell configuration: (1) unipolar, (2) pseudounipolar, (3) bipolar, and (4) multipolar. The three function types of neurons are sensory, associational, and motor.
4. Neuroglial cells (“nerve glue”) support the CNS and make up approximately half of the total brain and spinal cord volume.
5. Nerve injury triggers a sequence of events known as wallerian degeneration. The degree of nerve regeneration that occurs depends on many factors.
1. The region between adjacent neurons is the synapse, and the region between the neuron and muscle is the myoneural junction.
2. Neurotransmitters are responsible for chemical conduction across the synapse and myoneural junction. Nerve impulse is predominantly regulated by a balance of IPSPs and EPSPs, temporal and spatial summation, and convergence and divergence.
1. The brain is contained within the cranial vault and is divided into three distinct regions: (a) forebrain, (b) midbrain, and (c) hindbrain.
2. The forebrain comprises the two cerebral hemispheres and allows conscious perception of internal and external stimuli, thought and memory processes, and voluntary control of skeletal muscles. The deep portion of the forebrain is termed the diencephalon and processes incoming sensory data. The center for voluntary control of skeletal muscle movements is located along the precentral gyrus in the frontal lobe, whereas the center for perception is along the postcentral gyrus in the parietal lobe. The Broca area (rostral to the postcentral gyrus) and the Wernicke area (superoposterior temporal lobe) are major speech centers.
3. The midbrain is primarily a relay center for motor and sensory tracts, as well as a center for auditory and visual reflexes.
4. The hindbrain allows sampling and comparison of sensory data from the periphery and motor impulses from the cerebral hemispheres for the purpose of coordination and refinement of skeletal muscle movement.
5. The spinal cord contains the majority of nerve fibers connecting the brain with the periphery. Reflex arcs are completed in the spinal cord and influenced by the higher centers in the brain.
6. The four clinically relevant motor pathways are the lateral corticospinal, corticobulbar, basal ganglia, and vestibulospinal.
7. The three clinically important afferent pathways are the posterior column, anterior spinothalamic, and lateral spinothalamic.
8. The CNS is protected by the scalp, bony cranium, meninges, vertebral column, and CSF. The CSF is formed from blood components in the choroid plexuses of the ventricles and is reabsorbed in the arachnoid villi (located in the dural venous sinuses) after circulating through the brain and spinal cord.
9. The paired carotid and vertebral arteries supply blood to the brain and connect to form the circle of Willis. The major branches projecting from the circle of Willis are the anterior, middle, and posterior cerebral arteries. Drainage of blood from the brain is accomplished through the venous sinuses and jugular veins.
10. Blood supply to the spinal cord originates from the vertebral arteries and branches arising from the aorta.
1. The ANS is responsible for the maintenance of a steady-state in the internal environment. Two opposing systems make up the ANS: (1) the sympathetic nervous system responds to stress by mobilizing energy stores and prepares the body to defend itself, and (2) the parasympathetic nervous system conserves energy and the body’s resources.
1. Major structural changes with aging include a decrease in number of neurons and a decrease in brain weight and size.
2. Deposition of lipofuscin and the presence of senile plaques, multiple neurofibrillary tangles, and Lewy bodies are common cellular changes with aging.
3. A progressive slowing of neurologic function occurs with advancing age.
α-Adrenergic receptor 469
β-Adrenergic receptor 469
Acetylcholine 467
Adrenergic transmission 469
Afferent pathway (ascending pathway) 443
Afferent (sensory) neuron 457
Amygdala 452
Angiography 476
Anterior cerebral artery 462
Anterior column (ventral column) 456
Anterior fossa 459
Anterior horn (ventral horn) 456
Anterior spinal artery 463
Anterior spinothalamic 458
Arachnoid membrane 460
Arachnoid villi 461
Arterial circle (circle of Willis) 462
Association fiber 452
Associational neuron (interneuron) 444
Astrocyte 445
Autonomic nervous system (ANS) 443
Axon 443
Axon hillock 443
Basal ganglia 452
Basal ganglia system 452
Basilar artery 462
Basis pedunculi 455
Bipolar neuron 444
Brachial plexus 465
Brain scan 475
Brainstem 450
Broca speech area 452
Cauda equina 456
Cavernous sinus 462
Celiac branch of aorta 467
Central canal 456
Central nervous system (CNS) 442
Central sulcus (fissure of Rolando) 452
Cerebellomedullary cistern (cisterna magna) 460
Cerebellum 455
Cerebral aqueduct (aqueduct of Sylvius) 455
Cerebral cortex 452
Cerebral nuclei 452
Cerebrospinal fluid (CSF) 461
Cerebrum 452
Cholinergic transmission 469
Choroid plexus 460
Collateral ganglia 467
Computed tomography (CT) 474
Contralateral control 452
Conus medullaris 456
Convergence 443
Corpora quadrigemina (tectum) 455
Corpus callosum (commissural fiber) 452
Corpus striatum 452
Corticobulbar 458
Corticospinal tract 452
Cranial nerves 443
Craniosacral division 467
Dendrite 443
Dendritic zone 443
Denticulate ligament 460
Dermatome 467
Diencephalon 453
Divergence 443
Dopamine 455
Dura mater 459
Echoencephalography (ultrasound) 476
Effector organ 443
Efferent (motor) neuron 457
Efferent pathway (descending pathway) 443
Electroencephalograph (EEG) 476
Endoneurium 443
Ependymal cells 445
Epicritic 458
Epidural space 460
Epithalamus 453
Evoked potential (EP) 476
Excitatory postsynaptic potential (EPSP) 448
Facilitation 449
Falx cerebri 460
Fascicle 443
Filum terminale 456
Fissure 452
Frontal lobe 452
Galea aponeurotica 459
Ganglia 443
Gray matter 452
Helical CT angiography 474
Hippocampus 453
Hypothalamus 453
Inferior colliculi 455
Inferior mesenteric branch of aorta 467
Inhibitory postsynaptic potential (IPSP) 448
Inner dura (meningeal layer) 459
Insula 452
Intermediolateral gray (lateral horn) 456
Internal capsule 452
Internal carotid artery 462
Interventricular foramen (foramen of Monro) 461
Intervertebral disk 461
Lateral aperture (foramen [pl., foramina] of Luschka) 461
Lateral column 456
Lateral corticospinal 458
Lateral spinothalamic 458
Lateral sulcus (sylvian fissure, lateral fissure) 452
Lentiform nucleus 452
Limbic system 453
Longitudinal fissure 452
Lower motor neuron 458
Lumbar cistern 460
Lumbar plexus 467
Lumbar puncture 461
Magnetic resonance angiography (MRA) 475
Magnetic resonance imaging (MRI) 474
Magnetic resonance spectroscopy 474
Median aperture (foramen of Magendie) 461
Medulla oblongata 455
Meninges 459
Metencephalon 455
Microfilament 443
Microglia 445
Microtubule 443
Midbrain (mesencephalon) 455
Middle cerebral artery 462
Middle fossa (temporal fossa) 459
Mixed nerve 465
Motor neuron 444
Motor unit 458
Multipolar neuron 444
Myelencephalon 455
Myelin 443
Myelin sheath 443
Myelogram 476
Neurilemma (Schwann sheath) 443
Neurofibril 443
Neurofibrillary tangle 471
Neuroglia 444
Neuroglial cell 443
Neuromuscular (myoneural) junction 458
Neuron 443
Neurotransmitter 447
Nissl substance 443
Nodes of Ranvier 443
Norepinephrine 469
Nucleus (pl., nuclei) 443
Nucleus pulposus 461
Occipital lobe 452
Oligodendroglia (oligodendrocyte) 445
Papez circuit 453
Parasympathetic nervous system 467
Parietal lobe 452
Pelvic nerve 467
Periosteum (endosteal layer) 459
Peripheral nervous system (PNS) 443
Pia mater 460
Plasticity 450
Plexus (pl., plexuses) 443
Pons 455
Positron-emission tomography (PET) scan 475
Postcentral gyrus 452
Posterior cerebral artery 462
Posterior column (dorsal column) 456
Posterior fossa 459
Posterior horn (dorsal horn) 456
Posterior spinal artery 463
Postganglionic neuron 467
Postsynaptic neuron 447
Precentral gyrus 452
Prefrontal area 452
Preganglionic neuron 467
Premotor area 452
Presynaptic neuron 447
Primary motor area 452
Primary voluntary motor area 452
Projecting artery (nutrient artery) 462
Protopathic 459
Pseudounipolar neuron 444
Red nucleus 455
Reflex arc 457
Reticular activating system 450
Reticular formation 450
Roentgenogram (x-ray film) 474
Sacral plexus 467
Saltatory conduction 443
Schwann cell 443
Senile plaque 471
Sensory ganglion (dorsal root ganglion) 456
Sensory neuron 457
Somatic nervous system 443
Spatial summation 449
Spinal cord 456
Spinal nerve 443
Spinal tract 456
Spinothalamic tract 456
Spiral (helical) CT 474
Splanchnic nerve 467
Subarachnoid space 460
Subdural space 460
Substantia gelatinosa 456
Substantia nigra 455
Subthalamic nucleus 455
Subthalamus 453
Sulci 452
Summation 449
Superficial artery (conducting artery) 462
Superior colliculi 455
Superior mesenteric branch of aorta 467
Superior sagittal sinus 461
Sympathetic nervous system 467
Sympathetic (paravertebral) ganglia 467
Synapse 446
Synaptic bouton 447
Synaptic cleft 447
Tegmentum 455
Telencephalon 452
Temporal lobe 452
Temporal summation 449
Tentorium cerebelli 460
Thalamus 453
Thoracolumbar division 467
Unipolar neuron 444
Upper motor neuron 457
Ventricle 461
Vermis 455
Vertebral artery 462
Vestibulospinal 458
Wallerian degeneration 445
Wernicke area 452
White matter 452
REFERENCES
1. Haines, D.E. Fundamental neuroscience for basic and clinical applications, ed 3. Philadelphia: Churchill Livingstone; 2006.
2. Kandel E.R., et al, eds. Principles of neural science, ed 4, New York: McGraw-Hill, 2000.
3. Purves, D., et al. Neuroscience, ed 4. Sunderland: Sinauer Associates; 2008.
4. Kolb, B., Whishaw, I.Q. An introduction to brain and behavior, ed 2. New York: Worth; 2006.
5. Szabo, B., Schicker, E., Effects of cannabinoids on neurotransmission. Handb Exp Pharmacol. 2005(168):327–365.
6. Benarroch, E.E., et al. Medical neurosciences: An Approach to Anatomy, Pathology, and Physiology by Systems and Levels, ed 5. Philadelphia: Lippincott Williams & Wilkins; 2008.
7. Brodal, P. The central nervous system, structure and function,, ed 3. New York: Oxford University Press; 2004.
8. Whitehouse, P.J., George, D. The myth of Alzheimer’s: what you aren’t being told about today’s most dreaded diagnosis. New York: St. Martin’s Press; 2008.
9. Kelly, et al. The neurobiology of aging. Epilepsy Res. 2006;68(Suppl 1):S5–S20.
10. Keller, J.N. Age related neuropathology, cognitive decline and Alzheimer’s disease. Ageing Res Rev. 2006;5(1):1–13.
11. Schliebs, R., Arendt, T. The significance of the cholinergic system in the brain during aging in Alzheimer’s disease,. J Neural Transm. 2006;113(11):1625–1644.
12. Timiras P.S., ed. Physiologic basis of aging and geriatrics, ed 3, Boca Raton, FL: CRC Press, 2003.