STOOL SPECIMENS
Stool specimens are frequently collected in children to identify parasites and other organisms that cause diarrhea, to assess gastrointestinal function, and to check for occult (hidden) blood. Ideally, stool should be collected without contamination with urine, but in children wearing diapers this is difficult unless a urine bag is applied. Children who are toilet trained should urinate first, flush the toilet, then defecate in the toilet, a bedpan (preferably one that is placed on the toilet to avoid embarrassment), or a commercial potty hat.
Stool specimens should be large enough to obtain an ample sampling, not merely a fecal fragment. Specimens are placed in an appropriate container, which is covered and labeled. If several specimens are needed, the containers are marked with the date and time and kept in a specimen refrigerator. Care is exercised in handling the specimen because of the risk of contamination.
BLOOD SPECIMENS
Whether the specimen is collected by the nurse or others, the nurse is responsible for making certain that specimens, such as serial examinations and fasting specimens, are collected on time and the proper equipment is available. Collecting, transporting, and storing specimens can have a major impact on laboratory results.
Venous blood samples can be obtained by venipuncture or by aspiration from a peripheral or central access device (see Evidence-Based Practice box). Withdrawing blood specimens through peripheral lock devices in small peripheral veins has met with varying degrees of success. Although it avoids an additional venipuncture for the child, attempting to aspirate blood from the peripheral lock may shorten the life of the device. When using an IV infusion site for specimen collection, consider the type of fluid being infused. For example, a specimen collected for glucose level would be inaccurate if removed from a catheter through which glucose-containing solution was being administered.
 To obtain a blood specimen from a peripheral lock when the infusion solution may interfere with tests results, first aspirate a quantity of blood equal to the volume of fluid in the catheter and discard; then aspirate the blood sample.
To obtain a blood specimen from a peripheral lock when the infusion solution may interfere with tests results, first aspirate a quantity of blood equal to the volume of fluid in the catheter and discard; then aspirate the blood sample.
For a blood culture, use the first sample of blood, since organisms are most likely to collect within the catheter itself.
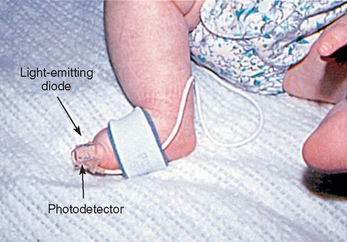
Arterial blood samples are sometimes needed for blood gas measurement, although noninvasive techniques, such as transcutaneous oxygen monitoring and pulse oximetry, are used frequently. Arterial samples may be obtained by arterial puncture using the radial, brachial, or femoral arteries; by deep heel puncture; or from indwelling arterial catheters. Adequate circulation should be assessed before arterial puncture by observing capillary refill or performing the Allen test, a procedure that assesses the circulation of the radial, ulnar, or brachial arteries. Because unclotted blood is required, only heparinized collection tubes are used. In addition, no air bubbles should enter the tube, since they can alter blood gas concentration. Crying, fear, and agitation also affect blood gas values; therefore every effort is made to comfort the child. The nurse should pack the sample in ice to reduce blood cell metabolism and take it to the laboratory for immediate analysis.
Capillary blood samples are taken from children by a finger stick. A common method for taking peripheral blood samples from infants younger than 6 months of age is by a heel stick. Before the blood sample is taken, the heel is warmed for 3 minutes. The area is cleansed with alcohol, the infant’s foot firmly restrained with the free hand, and the heel punctured with an automatic lancet device (Clinical and Laboratory Standards Institute, 2006). An automatic device delivers a more precise puncture depth and is less painful than using a lance (Vertanen, Fellman, Brommels, and others, 2001). A surgical blade of any kind is contraindicated. An example of a safe device is the BD Quickheel Safety Lancet. The Tenderfoot Preemie device was compared with the Monolet lancet and was found to be safer than the lancet and required fewer heel punctures, less collection time, and lower recollection rates (Kellam, Sacks, Wailer, and others, 2001). Shepherd, Glenesk, Niven, and others (2006) reported the Tenderfoot device was more effective and safer than a lancet for newborn screening tests. Although obtaining capillary blood gases is a common practice, these measures may not accurately reflect arterial values.
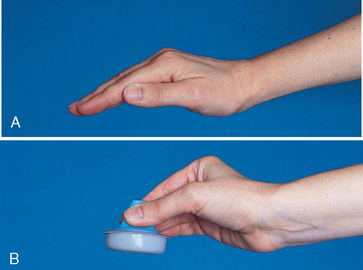
The most serious complications of infant heel puncture are necrotizing osteochondritis from lancet penetration of the underlying calcaneus bone, infection, or abscess (Meehan, 1998). To avoid osteochondritis, the puncture should be no deeper than 2 mm and should be made at the outer aspect of the heel. The boundaries of the calcaneus can be marked by an imaginary line extending posteriorly from a point between the fourth and fifth toes and running parallel to the lateral aspect of the heel and another line extending posteriorly from the middle of the great toe and running parallel to the medial aspect of the heel (Fig. 22-11). Repeated trauma to the walking surface of the heel can cause fibrosis and scarring that may interfere with locomotion.

The specimens are quickly collected, and pressure is applied to the puncture site with dry gauze until bleeding stops. The arm is kept extended, not flexed, while pressure is applied for a few minutes after venipuncture in the antecubital fossa to reduce bruising. The site is covered with an adhesive bandage. In young children, adhesive bandages pose an aspiration hazard; they should be avoided or removed as soon as the bleeding stops. Applying warm compresses to ecchymotic areas increases circulation, helps remove extravasated blood, and decreases pain.
No matter how or by whom the specimen is collected, children, even some older ones, fear the loss of their blood. This is particularly true for children whose condition requires frequent blood specimens. They mistakenly believe that blood removed from their bodies is a threat to their lives. Explaining to them that their body is continuously producing blood provides them with a measure of reassurance. When the blood is drawn, a comment such as “Just look how red it is. You–re really making a lot of nice red blood,” confirms this information and affords them an opportunity to express their concern. An adhesive bandage gives them added reassurance that the vital fluids will not leak out.
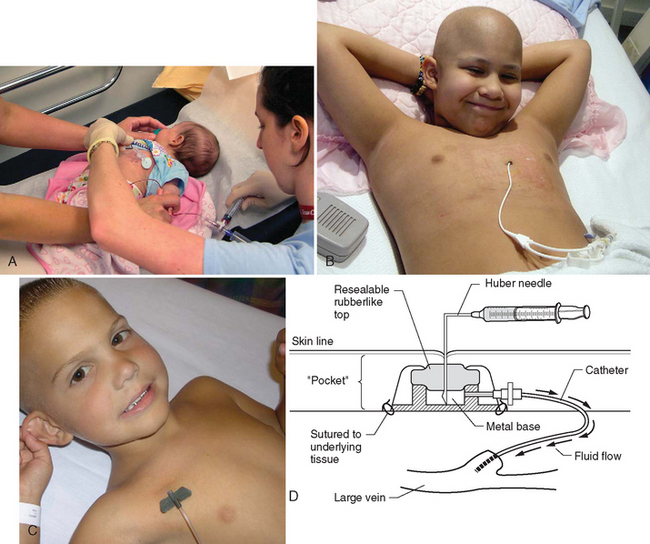
Obtaining Blood Specimens from Central Venous Catheters in Children
Joy Hesselgrave
In children, do blood specimens obtained from central venous catheters using the discard, reinfusion, or push-pull method yield more accurate samples?
CRITICALLY ANALYZE THE EVIDENCE
Limited scientific research exists that describes the optimal method for drawing blood samples from central venous access devices (VAD) in the pediatric patient.
A convenience sample of paired specimens compared blood drawn from central lines via push-pull method and discard method on 28 pediatric patients 6 months to 12 years of age. Of the 438 pairs of measurements that were compared, 420, or 95.9%, were within limits of agreement for hemograms, electrolytes, and glucose. The push-pull method eliminates loss of blood and decreases the amount of times the central line is accessed (Barton, Chase, Latham, and others, 2004).
Forty-two nonneutropenic pediatric patients ages 2 to 20 years were randomly assigned to one of two syringe-handling methods for blood sampling. The discard specimen, routinely reinfused, was collected using the usual clean procedure and an exaggerated unclean alternative procedure. Neither the sterile specimens nor the unclean specimens grew organisms, thus suggesting that the reinfusion of the blood specimen would be safe. This study did not evaluate for clots in the discard specimen (Hinds, Wentz, Hughes, and others, 1991).
Thirty bone marrow transplant units were surveyed to evaluate how blood samples were drawn from central VADs. The average patient age was 5 to 16 years. Seventy-five percent of the units used the discard method, with the volume of discard ranging from 0.5 to 10 ml and an average of 4 to 6 ml. Fourteen percent used the reinfusion method, and 11% used the push-pull or mixing method (Keller, 1994).
The Infusion Nurses Society (2006) recommends that the discard method be used when drawing blood samples from central VADs. The discard volume should be 1.5 to 2 times the fill volume of the central VAD.
Frey (2003) summarizes evidence for the practice of all three blood sampling methods. The discard method is most widely reported, with disadvantages including blood loss, blood exposure risk for clinicians, and the potential to confuse the discard specimen for the blood sample. The reinfusion method does not deplete blood volume but risks blood exposure for clinician and potential to reinfuse a contaminated specimen or clots in the discard volume. The push-pull or mixing method demonstrates accuracy for studies other than coagulation and drug levels and reduces blood loss and clinician exposure risk.
APPLY THE EVIDENCE: NURSING IMPLICATIONS
There is limited pediatric research that clearly supports any particular central line blood sampling method as being superior. All three methods yield accurate results and appear safe. The discard method is the most frequently reported in the literature and benchmarking. However, if there is a concern about blood volume, the push-pull or reinfusion method should be considered.
If the catheter has multiple lumens, use the distal lumen for laboratory specimen collection.
Infusions should be stopped and lumens clamped before blood sampling.
Cleanse the injection cap with antiseptic agent and allow to dry before drawing laboratory specimens.
REFERENCES
Barton, S, Chase, T, Latham, B, et al. Comparing two methods to obtain blood specimens from pediatric central venous catheters. J Pediatr Oncol Nurs. 2004;21(6):320–326.
Frey, M. Drawing blood samples from vascular access devices. J Infus Nurs. 2003;26(5):285–293.
Hinds, PS, Wentz, T, Hughes, W, et al. An investigation of the safety of the blood reinfusion step used with tunneled venous access devices in children with cancer. J Pediatr Oncol Nurs. 1991;8(4):59–64.
Infusion Nurses Society. Policies and procedures for infusion nursing, ed 3. South Norwood, Mass: The Society, 2006.
Keller, CA. Methods of drawing blood samples through central venous catheters in pediatric patients undergoing bone marrow transplant: results of a national survey. Oncol Nurs Forum. 1994;21(5):879–884.
Children also dislike the discomfort associated with venous, arterial, or capillary punctures. Children have identified these procedures as the ones most frequently causing pain during hospitalization and arterial punctures as being one of the most painful of all procedures experienced (Van Cleve, Johnson, and Pothier, 1996). The ones most distressed by venipunctures are toddlers, followed by school-age children and then adolescents. Consequently nurses need to institute pain reduction techniques to lessen the discomfort of these procedures (see Atraumatic Care box).
 ATRAUMATIC CARE
ATRAUMATIC CAREGuidelines for Skin and Vessel Punctures
FOR REDUCTION OF PAIN ASSOCIATED WITH HEEL, FINGER, VENOUS, OR ARTERIAL PUNCTURES
Apply EMLA (an eutectic mixture of lidocaine and prilocaine) topically over the site if time permits (at least 60 minutes). LMX (lidocaine) cream also may be used and requires a shorter application time (30 minutes).
To remove the Tegaderm dressing atraumatically, grasp opposite sides of the film and pull the sides away from each other to stretch and loosen the film. After the film begins to loosen, grasp the other two sides of the film and pull.
Use iontophoresis (Numby Stuff) over the site if time permits (8 to 20 minutes, depending on the amount of current), a vapocoolant spray, or buffered lidocaine (injected intradermally near the vein with a 30-gauge needle) to numb the skin.
Use nonpharmacologic methods of pain and anxiety control (e.g., ask child to take a deep breath when the needle is inserted and again when the needle is withdrawn; exhale a large breath or blow bubbles to “blow hurt away”; count slowly and then faster and louder if pain is felt).
Keep all equipment out of sight until used.
Enlist parents’ presence or assistance if they wish.
Restrain child only as needed to perform the procedure safely; use therapeutic holding (p. 708).
Allow the skin preparation to dry completely before penetrating the skin.
Use the smallest-gauge needle (e.g., 25 gauge) that permits free flow of blood; a 27-gauge needle can be used for obtaining 1 to 1.5 ml blood and for prominent veins (needle length is only ½ inch).
Emphasize that blood entering the syringe or tube does not hurt, and reassure young children that you did not “take their blood” away and that they have a lot more inside.
Place a small bandage over the puncture site to make removal easy and less painful and to reassure young children that their blood will not “leak out.”
Have a “two-try” only policy to reduce excessive insertion attempts–two operators each have two insertion attempts; if insertion is not successful after four punctures, consider alternative venous access, such as a peripherally inserted central catheter (PICC); have a policy for identifying children with difficult access and appropriate interventions (e.g., most experienced operator for the first attempt).
Use an intermittent infusion device (saline lock) to collect additional samples; consider PICC lines early, not as a last resort.
Coordinate care to allow several tests to be performed on one blood sample using micromethods of testing.
Anticipate tests (e.g., drug levels, chemistry, immunoglobulin levels) and ask the laboratory to save blood for additional testing.
Heel lancing has been shown to be more painful than venipuncture (Larsson, Tannfeldt, Lagercrantz, and others, 1998); consider venipuncture when the amount of blood from the heel would require much squeezing (e.g., genetic screening tests).
The effectiveness of EMLA is controversial, although application of 0.5 g for 30 minutes four times a day in preterm infants was found to be safe (Essink-Tebbes, Wuis, Liem, and others, 1999).
Place diapered newborn against mother’s bare chest in skin-to-skin contact 10 to 15 minutes before and during heel lance (Gray, Watt, and Blass, 2000).
During the procedure, allow newborn to suck a pacifier coated with a slurry of sucrose. When commercially manufactured 24% sucrose solution is unavailable, add 1 teaspoon of table sugar to 4 teaspoons of sterile water. Use this solution to coat the pacifier, or administer 2 ml to the tongue 2 minutes before the procedure (Blass and Watt, 1999).
RESPIRATORY SECRETION SPECIMENS
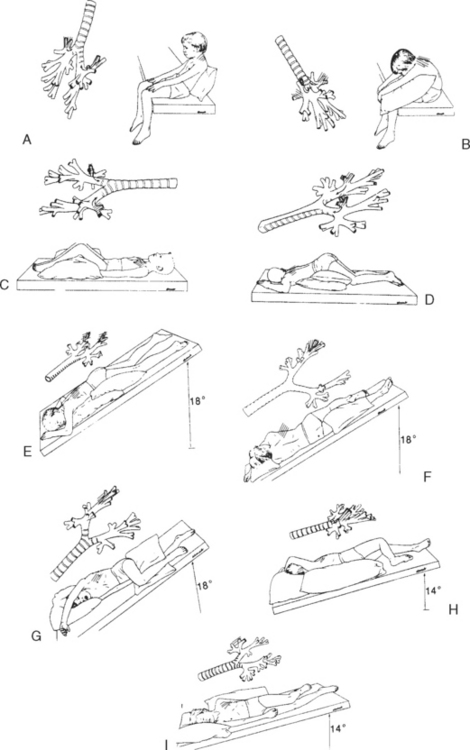
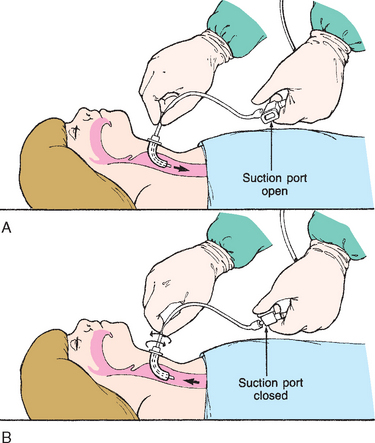
Collection of sputum or nasal discharge is sometimes required for diagnosis of respiratory infections, especially tuberculosis and respiratory syncytial virus (RSV). Older children and adolescents are able to cough and supply sputum specimens when given proper directions. It must be made clear to them that a coughed specimen, not mucus that is cleared from the throat, is needed. It is helpful to demonstrate a deep cough. Infants and small children are unable to follow directions to cough and will swallow any sputum produced; therefore gastric washings (lavage) may be used to collect a sputum specimen. Sometimes a satisfactory specimen can be obtained using a suction device such as a mucus trap if the catheter is inserted into the trachea and the cough reflex is elicited. A catheter inserted into the back of the throat is not sufficient. For children with a tracheostomy, a specimen is easily aspirated from the trachea or major bronchi by attaching a collecting device to the suction apparatus.
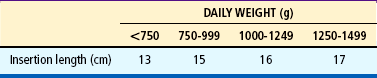
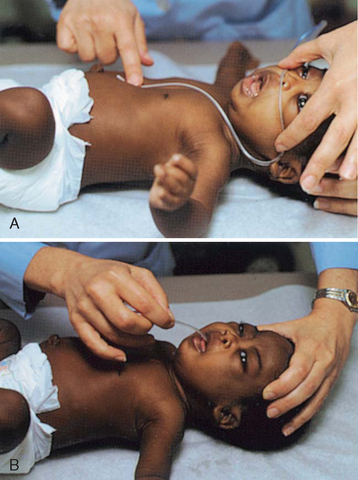
Nasal washings are usually obtained to diagnose an infection of RSV. The child is placed supine, and 1 to 3 ml sterile normal saline is instilled with a sterile syringe (without needle) into one nostril. The contents are aspirated using a small, sterile bulb syringe and are placed in a sterile container. Another method uses a syringe with 5 cm (2 inches) of 18- to 20-gauge tubing. The saline is quickly instilled and then aspirated to recover the nasal specimen. To prevent additional discomfort, all of the equipment should be ready before beginning the procedure.
Other respiratory secretion collection methods include nasopharyngeal swabs to diagnose Bordetella pertussis and throat cultures. The nurse swabs both the tonsils and the posterior pharynx when obtaining a throat culture. The swab stick is inserted into the culture tube. Some culture kits require squeezing an ampule to release the culture medium.