Pediatric Variations of Nursing Interventions
GENERAL CONCEPTS RELATED TO PEDIATRIC PROCEDURES
Preparation for Diagnostic and Therapeutic Procedures
Subcutaneous and Intradermal Administration
Nasogastric, Orogastric, or Gastrostomy Administration
PROCEDURES FOR MAINTAINING RESPIRATORY FUNCTION
On completion of this chapter the reader will be able to:
 Identify those instances in which informed consent is required and in which minors may be considered emancipated.
Identify those instances in which informed consent is required and in which minors may be considered emancipated.
Formulate general guidelines for preparing children for procedures, including surgery.
Implement play in therapeutic procedures.
List general strategies for enhancing compliance in children and families.
Outline general hygiene and care procedures for hospitalized children.
Implement feeding techniques that encourage food and fluid intake.
Describe methods of reducing temperature of child with fever or hyperthermia.
Describe systems that can be used for infection control.
Describe safe methods of administering oral, parenteral, rectal, optic, otic, and nasal medications to children.
Identify nursing responsibilities in maintaining fluid balance.
Demonstrate correct procedures for postural drainage and tracheostomy care.
Describe the procedures involved in providing nutrition via gavage, gastrostomy, and parenteral routes.
Describe the procedures involved in administering an enema and ostomy care to children.
RELATED TOPICS and ADDITIONAL RESOURCES
 IN TEXT
IN TEXTCommunicating with Families, Ch. 6
Dental Health: Infant, Ch. 10; Toddler, Ch. 12; Preschooler, Ch. 13; School-Age Child, Ch. 15; Adolescent, Ch. 16
Family-Centered Home Care, Ch. 20
Febrile Seizures, Ch. 28
Feeding Resistance, Ch. 9
Injury Prevention: Infant, Ch. 10; Toddler, Ch. 12; Preschooler, Ch. 13; School-Age Child, Ch. 15; Adolescent, Ch. 16
Limit Setting and Discipline, Ch. 3
Nutritional Assessment, Ch. 6
Pain Assessment and Management in Children, Ch. 7
Preparation for Hospitalization, Ch. 21
Providing Opportunities for Play and Expressive Activities, Ch. 21
Spina Bifida (Myelomeningocele), Ch. 32
Temperature (Measurement), Ch. 6
Wounds, Ch. 30
GENERAL CONCEPTS RELATED TO PEDIATRIC PROCEDURES
Before undergoing any invasive procedure, the patient or the patient’s legal surrogate must receive sufficient information on which to make an informed health care decision. Informed consent should include the expected care or treatment, potential risks, benefits, alternatives, and what might happen if the patient chooses not to consent. To obtain valid informed consent, the following three conditions must be met:
1. The person must be capable of giving consent; he or she must be over the age of majority (usually age 18) and must be considered competent (i.e., possessing the mental capacity to make choices and understand their consequences).
2. The person must receive the information needed to make an intelligent decision.
3. The person must act voluntarily when exercising freedom of choice without force, fraud, deceit, duress, or other forms of constraint or coercion.
The patient has the right to accept or refuse any health care. If the patient is treated without consent, the hospital or health care provider may be charged with assault and held liable for damages.
Requirements for Obtaining Informed Consent
Written informed consent of the parent or legal guardian is usually required for medical or surgical treatment, including many diagnostic procedures. One universal consent is not sufficient. Separate informed permissions must be obtained for each surgical or diagnostic procedure, including major or minor surgery, diagnostic tests with an element of risk (e.g., bronchoscopy), and medical treatments with an element of risk (e.g., blood transfusion, radiotherapy).
Other situations that require parental consent include:
Photographs for medical, educational, or public use
Removal of the child from the health care institution against medical advice
Postmortem examinations, except in unexplained deaths, such as sudden infant death, violent death, or suicide
Informed Consent and Assent in Children
Janet DeJean
CRITICALLY ANALYZE THE EVIDENCE
There are numerous opinions on when and how a child should be involved in the medical decision-making process. The determining factor is the child’s developmental readiness and the medical procedure involved.
The American Academy of Pediatrics’ (1995) position is that patients should participate in decision making commensurate with their development. No specific minimum age for a child is identified.
The Children’s Oncology Group (2005) states that in clinical research trials for cancer treatment, a child needs to be at least 9 years of age before he or she would have the ability to understand research-related information.
Two research studies evaluated the understanding of assent. Each recommended a different age of understanding:
1. Ondrusek, Abramovitch, Pencharz, and others (1998) found that in subjects younger than 9 years, understanding of most aspects of a clinical nutrition study involving a nontherapeutic blood sample was poor to nonexistent.
2. Tait, Voepel-Lewis, and Malviya (2003) found children ages 11 years and older had significantly greater understanding of the study protocol, benefits, and freedom to withdraw from a clinical anesthesia or surgical study.
Wendler (2006) suggests that children are capable of assent when they become able to understand the research in question at approximately 14 years of age. Assent is not required when the prospect of direct benefit of treatment is available only within the context of research. Sustained dissent should be respected in all cases.
Two research studies were found examining institutional review board (IRB) practices of determining when assent should be attained. All of the IRBs in these two studies support obtaining assent for children before clinical trials.
1. Kimberly, Hoehn, Feudtner, and others (2006) compared 55 different IRBs across the United States. The majority of the IRBs (83%) included methods for documenting assent, whereas only 45% identified specific age ranges for obtaining assent. The ages ranged from 7 to 18 years.
2. Whittle, Shah, Wilfond, and others (2004) interviewed 188 chairpersons of IRBs nationwide. Half the IRBs had a method, most commonly an age cutoff, they required investigators to follow in determining which children are capable of assent.
APPLY THE EVIDENCE: NURSING IMPLICATIONS
Children should be assessed for understanding and ability to participate in the assent process.
The age for assent ranged from 7 to 14 years in numerous published articles on obtaining assent in children.
The complex nature of some research studies and interventions may preclude children younger than 7, 9, 11, or 14 years of age from complete understanding.
Assent should not be sought when the prospect of direct treatment benefit is available only within the context of research.
REFERENCES
American Academy of Pediatrics Committee on Bioethics. Informed consent, parental permission, and assent in pediatric practice. Pediatrics. 1995;95(2):314–317.
Children’s Oncology Group. Guidelines for involving children in decision-making about research participation. http://www.childrensoncologygroup.org, 2005. [retrieved Aug 21, 2006, from].
Kimberly, M, Hoehn, K, Feudtner, C, et al. Variation in standards of research compensation and child assent practices: a comparison of 69 institutional review board–approved informed permission and assent forms for three multicenter pediatric clinical trials. Pediatrics. 2006;117:1706–1711.
Ondrusek, N, Abramovitch, R, Pencharz, P, et al. Empirical examination of the ability of children to consent to clinical research. J Med Ethics. 1998;24(3):158–165.
Tait, A, Voepel-Lewis, T, Malviya, S. Do they understand? part II, Assent of children participating in clinical anesthesia and surgery research. Anesthesiology. 2003;98(3):609–614.
Wendler, D. Assent in paediatric research: theoretical and practical considerations. J Med Ethics. 2006;32(4):229–234.
Whittle, A, Shah, S, Wilfond, B, et al. Institutional review board practices regarding assent in pediatric research. Pediatrics. 2004;113(6):1747–1752.
Decision making involving the care of older children and adolescents should include, to the extent feasible, the patient’s assent as well as that of the parents (see Evidence-Based Practice box). Assent means the child or adolescent has been informed about what will happen during the treatment or procedure and is willing to permit a health care provider to perform it. Assent should include the following elements:
Helping the patient achieve a developmentally appropriate awareness of the nature of his or her condition
Telling the patient what he or she can expect
Making a clinical assessment of the patient’s understanding
Soliciting an expression of the patient’s willingness to accept the proposed procedure of care
Multiple methods should be used to provide information, including age-appropriate methods (e.g., videotapes, peer discussion, diagrams, and written materials). An assent form should be provided to each child to sign, and the child should keep a copy (Broome, 1999). By including children in the decision-making process and gaining their acceptance, staff members demonstrate respect for the child. Assent is not a legal requirement but an ethical one to protect the rights of children.
Eligibility for Giving Informed Consent
Informed Consent of Parents or Legal Guardians: Parents have full responsibility for the care and rearing of their minor children, including legal control over them. As long as children are minors, their parents or legal guardians are required to give informed consent before medical treatment is rendered or any procedure is performed. If parents are married to each other, consent from only one parent is required for nonurgent pediatric care. If the parents are divorced, consent usually rests with the parent who has legal custody (Berger and AAP Committee on Medical Liability, 2003). Parents also have a right to withdraw consent at any time.
Evidence of Consent.: Obtaining informed consent varies from state to state, and policies differ at each health care facility. It is the physician’s responsibility to explain the procedure, risks, benefits, and alternatives. The nurse witnesses the patient’s, parent’s, or legal guardian’s signature on the consent form and may reinforce what the patient has been told. A signed consent form is the legal document that signifies that the process of informed consent has occurred. If parents are unavailable to sign consent forms, verbal consent may be obtained via the telephone in the presence of two witnesses. Both witnesses record that informed consent was given and by whom. Their signatures indicate that they witnessed the verbal consent.
Informed Consent of Mature and Emancipated Minors.: State laws differ with regard to the so-called age of majority, the age at which a person is considered to have all the legal rights and responsibilities of an adult. In most states, 18 is the age of majority. Competent adults can give informed consent on their own behalf. An emancipated minor is one who is legally under the age of majority but is recognized as having the legal capacity of an adult under circumstances prescribed by state law, such as pregnancy, marriage, high school graduation, living independently, or military service.
Treatment Without Parental Consent.: Exceptions to requiring parental consent before treating minor children occur when children need urgent medical or surgical treatment and a parent is not readily available or refuses to give consent. For example, a child may be brought to an emergency department accompanied by a grandparent, child care provider, teacher, or others. In the absence of parents or legal guardians, persons in charge of the child may be given permission by the parents to give informed consent by proxy. In emergencies, including danger to life or the possibility of permanent injury, appropriate care should not be withheld or delayed because of problems obtaining consent (Berger and AAP Committee on Medical Liability, 2003; American Academy of Pediatrics, 2003). Efforts made to obtain consent should be documented.
Refusal to give consent can occur when the treatment, such as blood transfusions, conflicts with the parents’ religious beliefs. All states recognize such exceptions and have statutory procedures to permit treatment if the life or health of such a minor is in jeopardy or if delayed treatment would create a risk to the minor’s health. In most states evaluation for child abuse or neglect can occur without parental consent and without notification of the state prior to evaluation.
Adolescents, Consent, and Confidentiality.: The Health Insurance Portability and Accountability Act of 1996 (HIPAA) was passed to help protect and safeguard the security and confidentiality of a person’s health information. Because adolescents are not yet adults, parents have the right to make most decisions on their behalf and receive information. Adolescents, however, are more likely to seek care in a setting in which they believe their privacy will be maintained. All 50 states have enacted legislation that entitles adolescents to consent to treatment without their parents’ knowledge for one or more “medically emancipated” conditions, such as sexually transmitted infections, alcohol and drug abuse, and need for contraceptive advice (Anderson, Schaechter, and Brosco, 2005; Tillett, 2005). Consent to abortion is controversial, and statutes vary widely by state. State law preempts HIPAA regardless of whether that law prohibits, mandates, or allows discretion about a disclosure.
Informed Consent and Parental Right to the Child’s Medical Chart.: Some state statutes give parents the unrestricted right to a copy of children’s medical records. In states without statutes, the best practice is to allow parents to review or have a copy of minors’ charts under reasonable circumstances. Practitioners should avoid restrictive requirements such as review permitted only in the presence of a clinician. Rather, an appropriate practitioner should be available to answer any questions that parents may have during reviews.
PREPARATION FOR DIAGNOSTIC AND THERAPEUTIC PROCEDURES
Technologic advances and changes in health care have resulted in more pediatric procedures being performed in a variety of settings. Many procedures are both stressful and painful experiences. For most procedures the focus of care is psychologic preparation of the child and family. However, some procedures require the administration of sedatives or analgesics.
Psychologic Preparation
Preparing children for procedures decreases their anxiety, promotes their cooperation, supports their coping skills and may teach them new ones, and facilitates a feeling of mastery in experiencing a potentially stressful event. Many institutions have developed preadmission teaching programs designed to educate the pediatric patient and family by offering hands-on experience with hospital equipment, information about the procedure to be performed, and an overview of departments they may visit (Algren, Ireland, and Stewart, 1998). Preparatory methods may be formal, such as group preparation for hospitalization. Most preparation strategies used by nurses are informal, focus on providing information about the experience, and are directed at stressful or painful procedures. The most effective preparation includes providing sensory-procedural information and helping the child develop coping skills, such as imagery, distraction, or relaxation (Broome, Rehwaldt, and Fogg, 1998).
General guidelines for preparing children for procedures are described in Box 22-1, and age-specific guidelines that consider children’s developmental needs and cognitive abilities are presented in Box 22-2. In addition to these suggestions, nurses should consider the child’s temperament, existing coping strategies, and previous experiences. Children who are distractible and highly active, as well as those who are “slow to warm up,” may need individualized sessions that are shorter for the active child but more slowly paced for the shy child. Youngsters who tend to cope well may need more emphasis on using their present skills, whereas those who appear to cope less adequately can benefit from more time devoted to simple coping strategies, such as relaxing, breathing, counting, squeezing a hand, or singing.
BOX 22-1 General Guidelines for Preparing Children for Procedures
Determine details of exact procedure to be performed.
Review parents’ and child’s present understanding.
Base teaching on developmental age and existing knowledge.
Incorporate parents in the teaching if they desire, especially if they plan to participate in care.
Inform parents of their supportive role during procedure, such as standing near child’s head or in child’s line of vision and talking softly to child.
Allow for ample discussion to prevent information overload and ensure adequate feedback.
Use concrete, not abstract, terms and visual aids to describe procedure. For example, use a simple line drawing of a boy or girl and mark the body part that will be involved in the procedure. Use nonthreatening but realistic models.*
Emphasize that no other body part will be involved.
If the body part is associated with a specific function, stress the change in or noninvolvement of that ability (e.g., after tonsillectomy, child can still speak).
Use words appropriate to child’s level of understanding.
Avoid words and phrases with dual meanings (see Nursing Care Guidelines box, p. 693) unless child understands such words.
Clarify all unfamiliar words (e.g., “Anesthesia is a special sleep”).
Emphasize sensory aspects of procedure–what child will feel, see, hear, smell, and touch and what child can do during procedure (e.g., lie still, count out loud, squeeze a hand, hug a doll).
Allow child to practice procedures that require cooperation (e.g., turning, deep breathing, incentive spirometry).
Introduce anxiety-laden information last (e.g., starting an intravenous line).
Be honest with child about unpleasant aspects of a procedure but avoid creating undue concern. When discussing that a procedure may be uncomfortable, state that it feels differently to different people.
Emphasize end of procedure and any pleasurable events afterward (e.g., going home, seeing parents).
Stress positive benefits of procedure (e.g., “After your tonsils are fixed, you won’t have as many sore throats”).
*Soft-sculptured dolls and customized adapters and overlays for preparing children and families about procedures and as teaching models for technical care are available from Legacy Products, Inc., 508 Green St., Cambridge City, IN 47327; (800) 238-7951; e-mail: info@legacyproductsinc.com; http://www.legacyproductsinc.com.
Children differ in their “information-seeking dimension.” Some actively solicit information about the intended procedure, whereas others avoid information. Parents can often guide nurses in deciding how much information is enough, since parents know whether the child is typically inquisitive or satisfied with short answers. Asking older children their preferences about the amount of explanation is also important. Drawings may also be helpful in preparing children for procedures.
The exact timing of the preparation for a procedure varies with the child’s age and type of procedure. No exact guidelines govern timing, but in general the younger the child, the closer the explanation should be to the actual procedure to prevent undue fantasizing and worrying. With complex procedures, more time may be needed for assimilation of information, especially with older children. For example, the explanation for an injection can immediately precede the procedure for all ages, whereas preparation for surgery may begin the day before for young children and a few days before for older children (although older children’s preferences should be elicited).
Establish Trust and Provide Support.: The nurse who has spent time with and established a positive relationship with a child will usually find it easier to gain cooperation. If the relationship is based on trust, the child will associate the nurse with caregiving activities that give comfort and pleasure most of the time rather than discomfort and stress. If the nurse does not know the child, it is best to be introduced by another staff person whom the child trusts. The first visit with the child should not include any painful procedure and ideally should focus on the child first, then on the explanation of the procedure.
Parental Presence and Support.: Children need support during procedures, and for young children the greatest source of support is the parents. They represent security, safety, and comfort. Controversy exists regarding the role parents should assume during the procedure, especially if discomfort is involved. Parental presence is preferable, however, since it can reduce patient and parent anxiety and decrease the need for sedation (Nelson, 1999). The nurse should assess the parents’ preferences for assisting, observing, or waiting outside the room, as well as the child’s preference for parental presence. The child’s and parents’ choice should be respected. Parents who wish to stay should be given appropriate explanation about the procedure and coached about what to do, where to sit or stand, and what to say to help the child through the procedure. Simple instructions such as clarifying where parents can stand or sit in the room and positioning them where they have eye contact with the child provide support and lessen anxiety. Parents who do not want to be present or participate are supported in their decision and encouraged to remain close by so that they can be available to console the child immediately after the procedure. Parents should also know that someone will be with their child to provide support. Ideally, this person should inform the parents after the procedure about how the child did.
Provide an Explanation.: Age-appropriate explanations are one of the most widely used interventions for reducing anxiety in children undergoing procedures. Before performing a procedure, explain what is to be done and what is expected of the child. The explanation should be short, simple, and appropriate to the child’s level of comprehension. Long explanations may increase anxiety in a young child. When explaining the procedure to parents with the child present, the nurse uses language appropriate to the child because unfamiliar words can be misunderstood (see Nursing Care Guidelines box). If the parents need additional preparation, this is done in an area away from the child. Teaching sessions are planned at times most conducive to the child’s learning (e.g., after a rest period) and for the usual span of attention.
Special equipment is not necessary for preparing a child, but for young children who cannot yet think in concepts, using objects to supplement verbal explanation is important. Allowing children to handle actual items that will be used in their care, such as a stethoscope, sphygmomanometer, or oxygen mask, helps them develop familiarity with these items and reduces the threat often associated with their use. Miniature versions of hospital items such as gurneys and x-ray and intravenous (IV) equipment can be used to explain what the children can expect and permit them to safely experience situations that are unfamiliar and potentially frightening. Written and illustrated materials are also valuable aids to preparation.*
Physical Preparation.: One area of special concern is the administration of sedation and analgesia before stressful procedures. Refer to Chapter 7 for information on sedating children.
Performance of the Procedure
Supportive care continues during the procedure and can be a major factor in a child’s ability to cooperate. Ideally, the same nurse who explains the procedure should perform or assist with the procedure. Before beginning, all equipment is assembled and the room is readied to prevent unnecessary delays and interruptions that increase the child’s anxiety.
If possible, procedures should be performed in a special treatment room rather than the child’s hospital room. Traumatic procedures should never be performed in “safe” areas, such as the playroom. If the procedure is lengthy, avoid conversation that could be misinterpreted by the child. As the procedure is nearing completion, inform the child that it is almost over in language the child understands.
Expect Success.: Nurses who approach children with confidence and who convey the impression that they expect to be successful are less likely to encounter difficulty. It is best to approach a child as though cooperation is expected. Children sense anxiety and uncertainty in an adult and respond by striking out or actively resisting. Although it is not possible to eliminate such behavior in every child, a firm approach with a positive attitude tends to convey a feeling of security to most children.
Involve the Child.: Involving children helps to gain their cooperation. Permitting choices gives them some measure of control. However, a choice is given only in situations in which one is available. Asking children, “Do you want to take your medicine now?” leads them to believe they have an option and provides them with the opportunity to legitimately refuse or delay the medication. This places the nurse in an awkward, if not impossible, position. It is much better to state firmly, “It’s time to drink your medicine now.” Children usually like to make choices, but the choice must be one that they do indeed have (e.g., “It’s time for your medicine. Do you want to drink it plain or with a little water?”).
Many children respond to tactics that appeal to their maturity or courage. This also gives them a sense of participation and achievement. For example, preschool children will be proud that they can hold the dressing during the procedure or remove the tape. The same is true for the school-age child, who often cooperates with minimal resistance.
Provide Distraction.: Distraction is a powerful coping strategy during painful procedures (Algren and Algren, 1997). It is accomplished by focusing the child’s attention on something other than the procedure. Singing favorite songs, listening to music, counting aloud, or blowing bubbles to “blow the hurt away” are effective techniques.
For other nonpharmacologic interventions that may lessen discomfort, see Pain Management, Chapter 7.
Allow Expression of Feelings.: The child should be allowed to express feelings of anger, anxiety, fear, frustration, or any other emotion. It is natural for children to strike out in frustration or to try to avoid stress-provoking situations. The child needs to know that it is all right to cry. Behavior is children’s primary means of communication and coping and should be permitted unless it inflicts harm on them or those caring for them.
Postprocedural Support
After the procedure, the child continues to need reassurance that he or she performed well and is accepted and loved. If the parents did not participate, the child is united with them as soon as possible so that they can provide comfort.
Encourage Expression of Feelings.: Planned activity after the procedure is helpful in encouraging constructive expression of feelings. For verbal children, reviewing the details of the procedure can clarify misconceptions and garner feedback for improving the nurse’s preparatory strategies. Play is an excellent activity for all children. Infants and young children are given the opportunity for gross motor movement. Older children are able to vent their anger and frustration in acceptable pounding or throwing activities. Play-Doh is a remarkably versatile medium for pounding and shaping. Dramatic play provides an outlet for anger and places the child in a position of control, in contrast to the position of helplessness in the real situation. Puppets can also allow the child to communicate feelings in a nonthreatening way. One of the most effective interventions is therapeutic play, which includes well-supervised activities such as permitting the child to give an injection to a doll or stuffed toy to reduce the stress of injections (Fig. 22-1).

Provide Positive Reinforcement.: Children need to hear from adults that they know the youngsters did the best they could in the situation, no matter how they behaved. It is important for children to know that their worth is not being judged on the basis of their behavior in a stressful situation. Reward systems, such as earning stars, stickers, or a badge of courage, are appealing to children.
Returning to the child a short while after the procedure helps the nurse strengthen a supportive relationship. Relating with the child in a relaxed and nonstressful period allows him or her to see the nurse not only as someone associated with stressful situations but as someone with whom to share pleasurable experiences.
Use of Play in Procedures
The use of play is an integral part of relationships with children. As such, its value in specific situations is discussed throughout this book, such as in Chapter 21, in relation to hospitalization. Many institutions have elaborate and well-organized play areas and programs under the direction of child life specialists; other institutions have limited facilities. No matter what the institution provides for children, nurses can include play activities as part of nursing care. Play can be used to teach, express feelings, or achieve a therapeutic goal. Consequently, it should be included in preparing children for and encouraging their cooperation during procedures. Play sessions after procedures can be structured, such as directed toward needle play, or general, with a wide variety of equipment available for children to play with. Routine procedures such as measuring blood pressure and oral administration of medication may be of concern to children. Box 22-3 offers suggestions for incorporating play into nursing procedures and activities for the hospitalized child that facilitate learning and adjustment to a new situation.
SURGICAL PROCEDURES
Children experiencing surgical procedures require both psychologic and physical preparation. In general, psychologic preparation is similar to that previously discussed for any procedure and employs many of the same techniques used in preparing a child for hospitalization, such as films, books, brochures, play, and tours. However, some important differences exist. Even though children are asleep for the actual surgical intervention, they are subjected to numerous preoperative and postoperative procedures. Stress points before and after surgery include the admission process, blood tests, injection of preoperative medication (if prescribed), transport to the operating room, and the stay in the postanesthesia care unit (PACU).
Psychologic intervention consisting of systematic preparation, rehearsal of the forthcoming events, and supportive care at each of these points has been shown to be more effective than a single-session preparation or consistent supportive care without systematic preparation and rehearsal. Play is always an effective strategy in preparing children, and increased familiarity with medical procedures decreases anxiety.
Surprisingly little research has been conducted on children’s perception of the surgical experience and their fears of the event. Although fear of anesthesia is thought to be a major concern among children, little evidence exists. School-age children report few remembered events and even fewer fears. Those events recalled most often were riding to and arriving in the operating room, receiving the preoperative or induction injection, waking up in pain, and not being allowed to eat or drink. The most feared events were the preoperative injection and the mask on the face.
Parental presence during induction of anesthesia is allowed in some institutions (Fig. 22-2). Potential benefits include minimizing the need for premedication and reducing the struggle that often occurs during separation (Kain, Caldwell-Andrews, and Wang, 2002). Other benefits are controversial but may include decreasing the child’s anxiety during induction (e.g., breath holding and laryngospasm) and decreasing long-term behavioral effects of surgery (Romino, Keatley, Secrest, and others, 2005). Although few institutions endorse the policy, reports from parents who attend the induction are favorable (Kain, Caldwell-Andrews, Krivutza, and others, 2004). Even though some parents may become anxious, most control their anxiety, do not disrupt the induction, and support the child (Hall, Payne, Stack, and others, 1995; LaRosa-Nash and Murphy, 1997; Munro and D–Errico, 2000). Clinical observations show parental presence decreases anxiety in the child and reduces the need for heavy doses of preoperative sedation (Fennell, 1999).

FIG. 22-2 Parental presence during induction of anesthesia can minimize child’s and parents’ anxiety during the preoperative period.
Some concern exists regarding the appropriateness of this practice for all parents. Some parents may become upset by the rapid succession of induction events, by observing their child becoming limp, and by leaving the child in the care of strangers. Parents who are anxious before surgery tend to become even more anxious after the induction, whereas the reverse is true of parents with little anxiety.
However, based on the parents’ favorable response to the practice and most children’s desire to have parents with them during any stressful procedure, parents should have the option of attending the induction. Appropriate education is essential to help parents understand the stages of anesthesia, what to expect, and how to support their child (Fennell, 1999), combined with a program that prepares them for what to expect and what is expected of them. When parents choose not to or are not allowed to attend this induction, leaving a favorite possession with the child and uniting the child and parents as soon as possible after surgery (preferably in the PACU) are important interventions. During surgery the family should have a designated place to wait and should be kept informed of the child’s progress. They also should know where and when they can visit the child after surgery.
Aside from possibly being separated from the parents before and after surgery, children may be cared for by a number of unfamiliar practitioners, which promotes fear and uncertainty. Although the same supportive nurse should remain with the child through as many of the procedures as possible, the child may have other nurses, especially if the patient returns to a special care unit postoperatively. Many hospitals have surgical tours for children and parents to familiarize them with the strange environment and to introduce them to other individuals who will be involved in their care.
An important concern is restriction of food and fluids before surgery to avoid aspiration during anesthesia. Infants require special attention to fluid needs. They should not be without oral fluids for an extended period preoperatively to avoid glycogen depletion and dehydration. Current preoperative fasting guidelines are found in Table 22-1.
TABLE 22-1
Fasting Recommendations to Reduce the Risk of Pulmonary Aspiration*
| INGESTED MATERIAL | MINIMUM FASTING PERIOD (hours)† |
| Clear liquids‡ | 2 |
| Breast milk | 4 |
| Infant formula | 6 |
| Nonhuman milk§ | 6 |
| Light meal¶ | 6 |
*These recommendations apply to healthy patients who are undergoing elective procedures. They are not intended for women in labor. Following the guidelines does not guarantee a complete gastric emptying has occurred.
†Fasting periods noted in chart apply to all ages.
‡Examples of clear liquids include water, fruit juices without pulp, carbonated beverages, clear tea, and black coffee.
§Because nonhuman milk is similar to solids in gastric emptying time, the amount ingested must be considered when determining appropriate fasting period.
¶A light meal typically consists of toast and clear liquids. Meals that include fried or fatty foods or meat may prolong gastric emptying time. Both the amount and type of foods ingested must be considered when determining appropriate fasting period.
From American Society of Anesthesiologists: Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures, Anesthesiology 90(3):896-905, 1999; retrieved from http://www.asahq.org/publicationsAndServices/NPO.pdf.
Although most preoperative care procedures are routine, nurses should keep in mind that they can be anxiety provoking for children and parents. For example, wearing a hospital gown without the security of underpants or pajama bottoms can be traumatic. Therefore these articles of clothing should be allowed to be worn into the operating room and removed after induction of anesthesia.
Preoperative Sedation.: Historically the most upsetting event for children has been the preoperative injection. Significant increases have recently occurred in the number of anesthesiologists who use preoperative sedatives, usually midazolam (Versed), and parental presence for children undergoing surgery (Kain, Caldwell-Andrews, Krivutza, and others, 2004). When drugs are administered, they should be delivered atraumatically via oral or IV routes. Numerous preanesthetic drug regimens are used with children, and no consensus exists on the optimal method. The goals for using preoperative medications include (1) anxiety reduction, (2) amnesia, (3) sedation, (4) antiemetic effect, and (5) reduction of secretions (Landsman and Cook, 1998; Manworren and Fledderman, 2000). Midazolam provides excellent preoperative anxiety reduction, amnesia, and sedation. It is popular because of its short duration, predictable onset, and rare occurrence of respiratory depression. Oral transmucosal fentanyl (OTFC, or Oralet) is available as a sweetened lozenge on a plastic stick. When first approved, this appeared to be an excellent, atraumatic route of administration. However, associated nausea and vomiting, respiratory depression, and the need for more intensive monitoring and observation than with other oral sedatives have limited its popularity (Klein, Diekema, Paris, and others, 2002). If children have no preoperative pain, are well prepared psychologically for surgery, and have their parents nearby, preoperative medication may be unnecessary.
Anesthesia induction of the pediatric patient is commonly accomplished by administering inhalation agents in combination with nitrous oxide and oxygen by mask. Children may fear induction of anesthesia by mask. Practices that can minimize anxiety related to inhalation anesthesia are (1) disguising the unpleasant odor of anesthetic gases by applying a pleasant-smelling substance on the mask; (2) using a transparent plastic mask rather than an opaque black mask and gradually bringing it toward the face; (3) directing a stream of gas toward the child’s face from the bare tube until the child becomes drowsy, then using the mask; (4) allowing the child to sit up rather than lie down for anesthesia induction; and (5) allowing preoperative play with a mask and a doll or manikin.
Postoperative Care
Various psychologic and physical interventions and observations are required to prevent or minimize possible untoward effects from anesthesia and the surgical procedure (see Nursing Care Guidelines box). Although the incidence of serious postoperative complications in healthy children undergoing surgery is less than 1% (Maxwell and Yaster, 2000), continuous monitoring of cardiopulmonary status is essential during the immediate postoperative period. Postanesthesia complications such as airway obstruction, postextubation croup, laryngospasm, and bronchospasm make maintaining a patent airway and maximum ventilation critical.
Monitoring oxygen saturation and providing supplemental oxygen as needed, maintaining body temperature, and promoting fluid and electrolyte balance are important aspects of immediate postoperative care. Vital signs are continuously monitored, and each vital sign is evaluated in terms of side effects from anesthesia, shock, or respiratory compromise (Table 22-2).
TABLE 22-2
Potential Causes of Postoperative Vital Sign Alterations in Children
From Smith DP: Comprehensive child and family nursing skills, St Louis, 1991, Mosby.
A change in vital signs that demands immediate attention in the perioperative period is caused by malignant hyperthermia (MH), a potentially fatal genetic myopathy. In susceptible children, anesthetics such as succinylcholine and halothane trigger the disorder, producing hypermetabolism, muscle rigidity, and an elevated temperature. Early symptoms of MH include tachycardia and tachyarrhythmias, tachypnea, hypercarbia, and metabolic and respiratory acidosis. An elevated temperature is considered by many to be a late sign of the disorder (Redmond, 2001). A family or previous history of sudden high fever associated with a surgical procedure and certain neuromuscular disorders increase risk for MH; children who have successfully undergone prior surgery without adverse effects may still be considered susceptible. Treatment includes immediate discontinuation of the triggering agent and surgical procedure, hyperventilation with 100% oxygen, and IV dantrolene sodium. Infusions of cool saline, cooling blankets, gastric or peritoneal lavage, packed ice bags in the axillae and groin, and, possibly, cardiopulmonary bypass reduce core temperature (Redmond, 2001). The patient should be transferred to an intensive care unit and closely monitored for stabilization of vital signs, metabolic state, and possible recurrence of symptoms.
Managing pain is a major nursing responsibility after surgery (see Chapter 7). The nurse should assess pain frequently and administer analgesics to provide comfort and facilitate cooperation with postoperative care such as ambulation and deep breathing. Opioids are the most commonly used analgesics. Routinely scheduled IV analgesics, patient-controlled analgesia, and epidural infusions, rather than as needed (PRN) orders, provide excellent analgesia in postoperative pediatric patients.
Ensure that preparations are made to receive child:
Take vital signs, including blood pressure; keep blood pressure cuff in place and deflated to lessen amount of disturbance to child.
Take and record vital signs more frequently if any value fluctuates.
– Outline any bleeding area on dressing or cast with pen.
– Reinforce, but do not remove, loose dressing.
– Observe areas below surgical site for blood that may have drained toward bed.
– Assess for bleeding and other symptoms in areas not covered with a dressing, such as throat after tonsillectomy.
Notify physician of any irregularities in child’s condition.
Assess for evidence of pain (see Pain Assessment, Chapter 7).
Review surgeon’s orders after completing initial assessment, and check that any preoperative orders, such as seizure or cardiac medications, have been reordered and can be given by available routes (oral preparations may be contraindicated).
Monitor vital signs as ordered and more often if indicated.
Check dressings for bleeding or other abnormalities.
Observe for signs of shock, abdominal distention, and bleeding.
Assess for bladder distention.
Because respiratory infections are a potential complication, every effort is taken to aerate the lungs and remove secretions. The lungs are auscultated regularly to identify abnormal sounds or any areas of diminished or absent breath sounds. To prevent hypostatic pneumonia, respiratory movement can be encouraged with incentive spirometers or other motivating activities (see Box 22-3). If these measures are presented as games, the child is more likely to comply. The child’s position is changed every 2 hours, and deep breathing is encouraged.
During the recovery period, some time should be spent with children to assess their perception of surgery. Play, drawing, and storytelling are excellent methods of discovering their thoughts. With such information the nurse can support or correct their perceptions and boost children’s self-esteem for having endured a stressful procedure.
COMPLIANCE
Compliance, also termed adherence, refers to the extent to which the patient’s behavior coincides with the prescribed regimen in terms of taking medication, following diets, or executing other lifestyle changes. In developing strategies to promote compliance, the nurse must first assess level of compliance. Because many children are too young to assume partial or total responsibility for their care, parents are usually primarily responsible for home management.
Factors relating to the care setting are important in ensuring compliance and should be considered in planning strategies to improve compliance. Basically, any aspect of the health care environment that increases the family’s satisfaction with the physical setting and the relationship with the practitioner positively influences adherence to the treatment regimen. However, the more complex, expensive, inconvenient, and disruptive the treatment protocol, the less likely the family is to comply. During long-term conditions that involve multiple treatments and considerable rearrangement of lifestyle, compliance is severely affected.
Although it is helpful to know those factors that influence compliance, assessment must include more direct measurement techniques. A number of methods exist, each with advantages and disadvantages. The most successful approach includes a combination of at least two of the following methods:
Clinical judgment—This is subject to bias and inaccuracy unless the nurse carefully evaluates the criteria used in assessment.
Self-reporting—Most people overestimate compliance by about 20% even when they admit to lapses.
Direct observation—This is difficult to employ outside the health care setting, and awareness of being observed frequently affects performance.
Monitoring appointments—Keeping appointments indirectly indicates compliance with the prescribed care.
Monitoring therapeutic response—Few treatments yield directly measurable results (e.g., decreased blood pressure, weight loss); record on a graph or chart.
Pill counts—The nurse counts the number of pills remaining in the original container and compares the number missing with the number of times the medication should have been taken. Families may forget to bring the container or deliberately alter the number of pills to avoid detection. This method is also poorly suited to liquid medication. Another technique is the use of pill container caps that record every opening as a presumptive dose.
Chemical assay—For certain drugs, such as digoxin and phenytoin, measurement of plasma drug levels provides information on the amount of drug recently ingested. However, this method is expensive, indicates only short-term compliance, and requires precise timing of the assay for accurate results.
Compliance Strategies
Strategies to improve compliance are composed of interventions that encourage families to follow the prescribed treatment regimen. Some evidence suggests that higher levels of self-esteem and increased autonomy favorably affect adolescent compliance (KyngAs, Kroll, and Duffy, 2000). However, family factors are important, and characteristics associated with good compliance include family support, family reminders, good communication, and expectations for successful completion of the therapeutic regimen (KyngAs, Kroll, and Duffy, 2000). No one approach is always successful, and the best results occur when at least two strategies are used.
Organizational strategies involve the care setting and the therapeutic plan. They include manipulating the factors listed in Box 22-4 that positively affect compliance. This may involve increasing the frequency of appointments, designating a primary practitioner, reducing the cost of medication by prescribing generic brands, reducing the treatment’s disruption of the family’s lifestyle, and using cues to minimize forgetting. Numerous devices are available commercially or can be improvised for cueing, such as pill dispensers; watches with alarms; charts to record completed therapy; messages on the refrigerator or morning coffee pot; and treatment schedules that incorporate the treatment plan into the daily routine, such as physical therapy after the evening bath.
Educational strategies instruct the family about the treatment plan. Although education is an important factor in enhancing compliance and patients who are more knowledgeable about their condition are more likely to comply, education alone does not ensure compliant behavior. The nurse should incorporate teaching principles known to enhance understanding and retention of material (see Nursing Care Guidelines box). Written materials are essential, especially in any regimen requiring multiple or complex treatments, and they need to be understandable to the average individual, who reads at about the fourth-grade level. Involvement of the immediate and extended family (e.g., grandparents) in education sessions may enhance compliance.
Effective Teaching of Family Members
Establish rapport; reduce anxiety and fear.
Assess what family members know and expect to learn and address their concerns before beginning teaching.
Assess learning style; ask if they prefer to have everything explained in detail or if they prefer knowing only the major facts.
Use a variety of teaching materials (lecture, demonstration, video, written material).
Be specific when giving information.
Divide the information into small steps.
Keep information short, simple, and concrete.
Introduce most important information first.
Use “verbal” headings to organize information, such as “There are two things you need to learn: how to give the medicine and what side effects to look for. First, how to give…. Second, what side effects….”
Stress how important the instructions are and the expected benefits; explain the detrimental effects of inadequate treatment, but avoid fear tactics.
Evaluate the teaching by eliciting feedback to ensure that family members understand the information.
Reward family for learning through verbal praise.
Use “teachable moments”–times when family members are most likely to accept new information (e.g., when a member asks a question or when symptoms are present).
Use hands-on demonstration and return demonstration to encourage mastery of skills and retention of information.
Treatment strategies relate to the child’s refusal or inability to take the prescribed medication. The family may also have difficulty following a prescribed treatment regimen. They may remember and understand the instructions but may not be able to give the medicine as prescribed. Assess the reason for refusal. For example, the child may not be able to swallow pills. In this case, perhaps pills can be crushed or a liquid medication substituted (always review medication to ensure that crushing is acceptable before giving this instruction).
Assess the treatment and medication schedule to determine if it is reasonable for a home situation. Although an every-6-hour or every-8-hour schedule is reasonable for hospitals, a parent would have difficulty getting up once or twice nightly; instead a medication could be given during the day at times that would be easy to remember.
Behavioral strategies are designed to modify behavior directly. Several strategies encouraging the desired behavior are effective with children. Ideally, positive reinforcement should be employed to strengthen the behavior and may consist of earning stars or tokens, which gains the child a special privilege or gift. At times, however, disciplinary techniques such as time-out for young children or withholding privileges for older children may be needed to improve compliance (see Limit Setting and Discipline, Chapter 3). Contracting, a formal process in which exact elements of desired behavior are explicitly outlined along with rewards or negative consequences, is an effective method with older children.
GENERAL HYGIENE AND CARE
MAINTAINING HEALTHY SKIN*
Maintaining an IV line, removing a dressing, positioning a child in bed, changing a diaper, using electrodes, and using restraints have the potential to contribute to skin injury. Skin care must go beyond the daily bath and become a part of each nursing intervention (see Nursing Care Guidelines box). Specific guidelines for skin care of neonates are provided in Skin Care, Chapter 9.
Assessment of the skin is most easily accomplished during the bath. Examine for early signs of injury. Risk factors include impaired mobility, protein malnutrition, edema, incontinence, sensory loss, anemia, infection, failure to turn the patient, and intubation. Critically ill children often are at higher risk of pressure ulcers and skin breakdown, since they often have several risk factors combined. Identification of risk factors helps to determine those children who need a more thorough skin assessment. Assessment should occur within 24 hours of admission so that pressure ulcers and wounds that occurred before admission can be identified (Ratliff and Rodheaver, 1999; Quigley and Curley, 1996).
Cleanse skin with mild nonalkaline soap or soap-free cleaning agents for routine bathing.
Provide daily cleansing of eyes, oral and diaper or perineal areas, and any areas of skin breakdown.
Apply moisturizing agents during or immediately after bathing; cleanse skin of old cream before adding a new layer.
Use minimum tape and adhesives. On very sensitive skin, use a protective, pectin-based or hydrocolloid skin barrier between skin and tape or adhesives.
Use water or adhesive remover (if skin is not fragile) when removing tape or adhesives.
Place pectin-based or hydrocolloid skin barriers directly over excoriated skin. Leave barrier undisturbed until it begins to peel off, or for 5 to 7 days. With wet, oozing excoriations, place a small amount of stoma powder on site, remove excess powder, and apply skin barrier. Hold barrier in place for several minutes to allow barrier to soften and mold to skin surface.
Alternate electrode placement and thoroughly assess skin underneath electrodes at least every 24 hours. Alcohol-free skin sealant under leads protects skin from epidermal stripping.
Be certain fingers or toes are visible whenever extremity is used for intravenous (IV) or arterial line.
Keep skin dry (may apply absorbent powder, e.g., cornstarch) and use soft, smooth bed linen and clothes.
Use a draw sheet to move a child in bed or onto a gurney; do not drag the child from under the arms.
Identify children at risk for skin breakdown before it occurs. Employ measures such as pressure-reducing or pressure-relieving devices (e.g., mattress overlay, low–air-loss bed, gel pillows).
Do not massage reddened bony prominences, since this can cause deep tissue damage; provide pressure relief to those areas instead.
Keep skin free of excess moisture (e.g., urine or fecal incontinence, wound drainage, excessive perspiration).
Routinely assess the child’s nutritional status. A child who is NPO (nothing by mouth) for several days and is receiving only IV fluid is nutritionally at risk, which can also affect the skin’s ability to maintain its integrity. Consider parenteral nutrition.
When capillary blood flow is interrupted by pressure, the blood flows back into the tissue when the pressure is relieved. As the body attempts to reoxygenate the area, a bright red flush appears. This reactive hyperemia, or flush, is the earliest sign of tissue compromise and pressure-related ischemia. If pressure is prolonged, reactive hyperemia will not be sufficient to revitalize ischemic tissue (Calianno, 1999).
Staging of pressure ulcers is used to classify the amount of tissue damage.* Necrotic tissue must be removed so that the tissue depth can accurately be assessed. Accurate documentation of redness or obvious skin breakdown is essential. Color, size (diameter and depth), location, presence of sinus tracts, odor, exudate, and response to treatment are observed and recorded at least daily. (For treatment of wounds, see Chapter 30.)
Pressure ulcers can develop when the pressure on the skin and underlying tissues is greater than the capillary closing pressure, causing capillary occlusion. If the pressure remains unrelieved, vessels can collapse, resulting in tissue anoxia and cellular death. Pressure ulcers most often occur over bony prominences and are usually very deep, extending into subcutaneous tissue or even deeper into muscle, tendon, or bone. A pressure-reduction device reduces pressure but does not prevent pressure from causing capillary closure; therefore turning and repositioning are always included when using these devices. Most of these items are overlays that are placed on top of the regular mattress. A pressure-relief device maintains pressure below that which would cause capillary closure. These devices are usually high-technology beds that are used for patients who have multiple problems and cannot be turned effectively.
Friction and shear contribute to pressure ulcers. Friction occurs when the surface of the skin rubs against another surface, such as the bed sheets. Skin damage most often occurs over the elbows, heels, or occiput; is usually limited to the epidermal and upper layers; and may have the appearance of an abrasion. Prevention of friction injury includes the use of protective sheepskin over the elbows or heels; gel pillows under the head of infants and toddlers; moisturizing agents; transparent dressings over susceptible areas; and soft, smooth bed linen and clothing. Shear is the result of the force of gravity pushing down on the body and friction of the body against a surface, such as the bed or chair. For example, when a patient is in the semi-Fowler position and begins to slide to the foot of the bed, the skin over the sacral area remains in the same place because of the resistance of the bed surface. The blood vessels in the area are stretched and may cause small-vessel thrombosis and tissue death (Bryant and Doughty, 2000). Prevention of shear injury includes using lift sheets when repositioning a patient, elevating the bed no more than 30 degrees for short periods, and using the knee gatch to interrupt the pull of gravity on the body toward the foot of the bed.
Epidermal stripping results when the epidermis is unintentionally removed with tape removal. These lesions are usually shallow and irregularly shaped and may blister or weep. Babies are at increased risk for epidermal injury. Prevention includes using no tape when possible, securing dressings with laced binders (Montgomery straps) or stretchy netting (Spandage or stockinette). Using porous or low-tack tapes (e.g., Medipore, paper, hydrogel), using alcohol-free skin sealants (No Sting Barrier Film), or picture framing wounds with hydrocolloid or wafer barriers (e.g., DuoDERM, Coloplast, Stomahesive) and then taping on top of the barrier also will reduce epidermal stripping.
Tape is placed so that there is no tension, traction, or wrinkles on the skin. To remove tape, slowly peel the tape away while stabilizing the underlying skin. Adhesive remover may be used to break the adhesive bond but may be drying to the skin; adhesive removers should be avoided in preterm neonates, since absorption rates vary and toxicity may occur. The adhesive is removed with water to prevent absorption and irritation. Wetting the tape with water or alcohol-based foam hand cleansers may facilitate removal.
Chemical factors can also lead to skin damage. Fecal incontinence, especially when mixed with urine; wound drainage; or gastric drainage around gastrostomy tubes can erode epidermis. The skin can quickly progress from redness to denudement if exposure continues. Moisture barriers, gentle cleansing as soon after exposure as possible, and skin barriers can be used to prevent damage caused by chemical factors (see also Diaper Dermatitis, Chapter 30). In addition, foam dressings that wick moisture away from the skin are helpful around gastrostomy tubes and tracheostomy sites.
BATHING
Most infants and children can be bathed in a basin at the bedside, on the bed, or in a standard bathtub or shower. For infants and young children confined to bed, the towel method can be used. Two towels are immersed in a diluted soap solution and wrung damp. With the child lying supine on a dry towel, one damp towel is placed on top of the child and used to gently clean the body. This towel is discarded, and the child is dried and turned prone. The procedure is repeated using the second damp towel. Commercially available bath cloths may also be used.
Infants and small children are never left unattended in a bathtub, and infants who are unable to sit alone are securely held with one hand during the bath. The nurse should securely support the infant’s head with one hand, or grasp the farther arm firmly while the head rests comfortably on the nurse’s arm. Children who are able to sit without assistance need only close supervision and a pad placed in the bottom of the tub to prevent slipping and loss of balance.
School-age children and adolescents may shower or bathe. Nurses need to use judgment regarding the amount of supervision the child requires. Some can assume this responsibility unaided, whereas others will need someone in constant attendance. Children with cognitive impairments, physical limitations, or suicidal or psychotic problems (who may commit bodily harm) require close supervision.
Areas that require special attention are ears, between skinfolds, neck, back, and genital area. The genital area should be carefully cleansed and dried with particular care given to skinfolds, and in uncircumcised boys, usually those older than 3 years of age, the foreskin should be gently retracted, the exposed surfaces cleansed, and the foreskin then replaced. If the condition of the glans indicates inadequate cleaning, such as accumulated smegma, inflammation, phimosis, or foreskin adhesions, teaching proper hygiene is indicated. In the Vietnamese and Cambodian cultures the foreskin is traditionally not retracted until adulthood. Older children have the tendency to avoid cleaning the genitalia; therefore they may need a gentle reminder.
Children who are ill or debilitated need more extensive assistance with bathing, but should be encouraged to perform as much as they can without overtaxing their energies. Expect increasing involvement with improved strength and endurance.
ORAL HYGIENE
Mouth care is an integral part of daily hygiene and should be continued in the hospital. Infants and debilitated children require the nurse or a family member to perform mouth care. Although young children can manage a toothbrush and are encouraged to use it, most need assistance to perform satisfactorily. Older children, although capable of brushing and flossing without assistance, sometimes need to be reminded. (See Dental Health, Chapters 10 and 12, for specific oral hygiene techniques; mouth care of children with mucosal ulcers is discussed under nursing care of the child with leukemia in Chapter 26.)
HAIR CARE
Children should have their hair brushed and combed at least once daily. The hair is styled for comfort and in a manner pleasing to the child and parents. The hair should not be cut without parental permission, although clipping hair to provide access to a scalp vein for IV insertion may be necessary.
If children are hospitalized for more than a few days, the hair may need shampooing. With infants the hair may be washed during the daily bath or less frequently. For most children, washing the hair and scalp once or twice weekly is sufficient unless there is an indication for more frequent washing, such as following a high fever and profuse sweating. Adolescents normally have increased oily sebaceous secretions that require frequent hair care and more frequent shampoos.
Almost any child can be transported to an accessible sink for shampooing. Those who are unable to be transported can receive a shampoo in their beds with adequate protection, specially adapted equipment or positioning, or dry shampoo caps. When necessary, a shampoo basin may be used or the child may be positioned near the edge of the bed, towels placed under the shoulders, a large plastic garbage bag draped at the edge of the bed with one open end under the shoulders, and the hair placed inside the opening. The other end is opened and placed in a collection container. Water can be transported in a basin.
African-American children require special hair care. For the child with curly hair, most standard combs are inadequate and may cause hair breakage and discomfort. Use a special comb with widely spaced teeth. It is also much easier to comb the hair after shampooing when it is wet. Use a special hair dressing or pomade, which usually has a coconut oil base. The preparation is rubbed on the hands and then transferred to the hair to make it more pliable and manageable. Consult the parents regarding the preparation to use on their child’s hair and ask if they can provide some for use during the hospitalization. Petroleum jelly should not be used. If braiding or plaiting the hair, the nurse should weave it loosely while the hair is damp. The hair tightens as it dries, which could result in tension folliculitis.
FEEDING THE SICK CHILD
Loss of appetite is a symptom common to most childhood illnesses. Because an acute illness is usually short, the nutritional state is seldom compromised. Urging foods on the sick child may precipitate nausea and vomiting, and in most cases children can be permitted to determine their own need for food.
Refusing to eat may also be one way children can exert power and control in an otherwise helpless situation. For young children, loss of appetite may be related to the depression caused by separation from their parents. Parents’ concern with eating can intensify the problem. Forcing a child to eat meets with rebellion and reinforces the behavior as a control mechanism. Parents are encouraged to relax any pressure during an acute illness. Although it is best to encourage high-quality nutritious foods, the child may desire foods and liquids that contain mostly empty or nonnutritional calories. Some well-tolerated foods include gelatin, diluted clear soups, carbonated drinks, flavored ice pops, dry toast, and crackers. Even though these substances are not nutritious, they can provide necessary fluid and calories.
Dehydration is always a hazard when children are febrile or anorexic, especially when accompanied by vomiting or diarrhea. Offer small amounts of favored fluids at frequent intervals and provide salty foods (which increase thirst) if allowed. If diarrhea is present, avoid high-carbohydrate liquids (e.g., carbonated beverages, gelatin, flavored ice pops) because they may aggravate the diarrhea by an osmotic effect. Replacing abnormal losses with plain water or undiluted broth may worsen the electrolyte imbalance. Fluids should not be forced, and the child is not awakened to take fluids. Forcing fluids may create the same difficulties as urging unwanted food. Gentle persuasion with preferred beverages will usually meet with success. Using play techniques can also be very effective (see Nursing Care Guidelines box).
Once the child is feeling better, appetite usually begins to improve. It is best to take advantage of any hungry period by serving high-quality foods and snacks. If the child still refuses to eat, nutritious fluids, such as prepared breakfast drinks, should be encouraged. Parents can help by bringing in food items from home, especially if the family’s cultural eating habits differ from the hospital food. A clinical dietitian may also be consulted for alternative food choices.
When children are placed on special diets, such as clear liquids after surgery or during episodes of diarrhea, assessment of their intake and readiness to advance to more complex foods is essential. Regardless of the type of diet, charting of the amount consumed is an important nursing responsibility. Descriptions need to be detailed and accurate, such as “4 ounces of orange juice, one pancake, and 8 ounces of milk.” Comments such as “ate well” or “ate poorly” are inadequate. Charting the percentage of the meal eaten is also inadequate unless food is measured before serving.
If parents are involved in the child’s care, they are encouraged to keep a list of everything eaten. Using a premeasured cup for fluids ensures a more accurate estimate of intake. A comparison of the intake at each meal can isolate food deficiencies, such as insufficient intake of meat or vegetables. Behaviors associated with mealtime also may point to possible factors influencing appetite. For example, the observation that “child eats well when with other children but plays with food if left alone in room” helps the nurse plan mealtime activities that stimulate the appetite.
CONTROLLING ELEVATED TEMPERATURES
An elevated temperature, most frequently from fever but occasionally caused by hyperthermia, is one of the most common symptoms of illness in children. This manifestation is of great concern to parents. To facilitate an understanding of fever, the following terms are defined:
Set point—The temperature around which body temperature is regulated by a thermostat-like mechanism in the hypothalamus
Fever (hyperpyrexia)—An elevation in set point such that body temperature is regulated at a higher level; may be arbitrarily defined as temperature above 38° C (100.4° F)
Take a dietary history (see Chapter 6) and use information to make eating time as much like home as possible.
Encourage parents or other family members to feed child or to be present at mealtimes.
Make mealtimes pleasant; avoid any procedures immediately before or after eating; make certain child is rested and pain free.
Serve small, frequent meals rather than three large meals or serve three meals and nutritious between-meal snacks.
Provide finger foods for young children.
Involve children in food selection and preparation whenever possible.
Serve small portions, and serve each course separately, such as soup first; followed by meat, potatoes, and vegetables; and ending with dessert.
With young children, camouflage size of food by cutting meat thicker so that less appears on plate or by folding a cheese slice in half.
Ensure a variety of foods, textures, and colors.
Provide food selections that are favorites of most children, such as peanut butter and jelly sandwiches, hot dogs, hamburgers, macaroni and cheese, pizza, spaghetti, tacos, fried chicken, corn, and fruit yogurt.
Avoid foods that are highly seasoned, have strong odors, or are all mixed together, unless typical of cultural practices.
Provide fluid selections that are favorites of most children, such as fruit punch, cola, ginger ale, sweetened tea, flavored ice pops, sherbet, ice cream, milk, milkshakes, eggnog, pudding, gelatin, clear broth, or creamed soups.
Offer nutritious snacks, such as frozen yogurt or pudding, ice cream, oatmeal or peanut butter cookies, hot cocoa, cheese slices, pieces of raw vegetable or fruit, and dried fruit or cereal.
Make food attractive and different; for example:
Serve a “picnic lunch” in a paper bag.
Pack food in a Chinese take-out container; decorate container.
Put a “face” or a “flower” on a hamburger or sandwich with pieces of vegetable.
Use a cookie cutter to shape a sandwich.
Serve pudding, yogurt, or juice frozen as an ice pop.
Make Slurpies or snow cones by pouring flavored syrup on crushed ice.
Add food coloring to water or milk.
Serve fluids through brightly colored or unusually shaped straws.
Make “bowtie” sandwiches by cutting them in triangles and placing two points together.
Slice sandwiches into “fingers.”
Cut apples horizontally to make circles.
Put a banana on a hot dog bun and spread with peanut butter.
Break uncooked spaghetti into toothpick lengths and skewer cheese, cold meat, vegetables, or fruit chunks.
Praise children for what they do eat.
Do not punish children for not eating by removing their dessert or putting them to bed
Hyperthermia—Body temperature exceeding the set point, which usually results from the body or external conditions creating more heat than the body can eliminate, such as in heatstroke, aspirin toxicity, seizures, or hyperthyroidism
Body temperature is regulated by a thermostat-like mechanism in the hypothalamus. This mechanism receives input from centrally and peripherally located receptors. When temperature changes occur, these receptors relay the information to the thermostat, which either increases or decreases heat production to maintain a constant set point temperature. However, during an infection, pyrogenic substances cause an increase in the body’s normal set point, a process that is mediated by prostaglandins. Consequently, the hypothalamus increases heat production until the core temperature reaches the new set point.
Most fevers in children are of brief duration with limited consequences and are viral in origin. When fever is caused by bacteria, endotoxins are produced that activate the inflammatory process and produce fever (Rote, Huether, and McCance, 2000). Contrary to popular belief, neither the rise in temperature nor its response to antipyretics indicates the severity or etiology of infection, which casts doubt on the value of using fever as a diagnostic or prognostic indicator.
Therapeutic management of elevated temperature depends on whether it is due to a fever or hyperthermia. Because the set point is normal in hyperthermia but increased in fever, different approaches must be used to lower body temperature successfully.
Fever
The principal reason for treating fever is the relief of discomfort. Relief measures include pharmacologic or environmental intervention. The most effective intervention is the use of antipyretics to lower the set point.
Antipyretic drugs include acetaminophen, aspirin, and nonsteroidal antiinflammatory drugs (NSAIDs). Acetaminophen is the preferred drug; aspirin should not be given to children because of the association between aspirin use in children and influenza virus or chickenpox and Reye syndrome. One nonprescription NSAID, ibuprofen, is approved for fever reduction in children as young as 6 months of age. Dosage is based on the initial temperature level: 5 mg/kg of body weight for temperatures less than 39.2° C (102.6° F) or 10 mg/kg for temperatures greater than 39.2° C. The recommended dosage for pain is 10 mg/kg every 6 to 8 hours, and the recommended maximum daily dose for pain and fever is 40 mg/kg. The duration of fever reduction is generally 6 to 8 hours and is longer with the higher dose (see Chapter 6). It may be given every 4 hours but no more than five times in 24 hours. Because body temperature normally decreases at night, three or four doses in 24 hours will control most fevers. The nurse should retake the temperature 30 minutes after the antipyretic is given to assess its effect, but temperature should not be repeatedly measured; the child’s level of discomfort is the best indication for continued treatment.
Environmental measures to reduce fever may be used if tolerated by the child and if they do not induce shivering. Shivering is the body’s way of maintaining the elevated set point by producing heat. Compensatory shivering greatly increases metabolic requirements above those already caused by the fever.
Traditional cooling measures, such as wearing minimum clothing, exposing the skin to the air, reducing room temperature, increasing air circulation, and applying cool, moist compresses to the skin (e.g., the forehead), are effective if employed approximately 1 hour after an antipyretic is given so that the set point is lowered. Cooling procedures such as sponging or tepid baths are ineffective in treating febrile children (these measures are effective for hyperthermia) either when used alone or in combination with antipyretics, and they cause considerable discomfort (Sharber, 1997).
Seizures associated with a fever occur in 3% to 4% of all children, usually those 3 months to 5 years of age. Although most children never have febrile seizures after the first occurrence, a younger age at onset and a family history of febrile seizures are associated with recurring episodes (Berg, Shinnar, Levy, and others, 1999; Shinnar, Pellock, Berg, and others, 2001). There is little evidence to support the use of antipyretic drugs to prevent febrile seizures; nursing interventions should focus on ways to provide care and comfort during a febrile illness (Purssell, 2000).
Hyperthermia
Unlike fever, antipyretics are of no value in hyperthermia because the set point is already normal. Consequently, cooling measures are used. Cool applications to the skin help reduce the core temperature. Cooled blood from the skin surface is conducted to inner organs and tissues, and warm blood is circulated to the surface, where it is cooled and recirculated. The surface blood vessels dilate as the body attempts to dissipate heat to the environment and facilitate the cooling process.
Commercial cooling devices, such as cooling blankets or mattresses, are available to reduce body temperature. Place on the bed and cover with a sheet or lightweight blanket. Frequent temperature monitoring is essential to prevent excessive cooling of the body.
Traditionally, cool compresses have been used to decrease high temperature. For tepid tub baths it is usually best to start with warm water and gradually add cool water until the desired water temperature of 37° C (98.6° F) is reached to accustom the child to the lower water temperature. Generally, the temperature of the water only has to be 1° C or 2° F less than the child’s temperature to be effective. The child is placed directly in the tub of tepid water for 15 to 20 minutes while water is gently squeezed from a washcloth over the back and chest or gently sprayed over the body from a sprayer. In the bed or crib, cool washcloths or towels are used, exposing only one area of the body at a time. The sponging is continued for approximately 20 minutes. After the tub or sponge bath, the child is dried and dressed in lightweight pajamas, a nightgown, or a diaper and placed in a dry bed. The child is dried by gently rubbing the skin surface with a towel to stimulate circulation. The temperature is retaken 30 minutes after the tub bath or sponge bath. The tub or sponge bath should not be continued or restarted until the skin surface is warm or if the child feels chilled. Chilling causes vasoconstriction, which defeats the purpose of the cool applications. In this condition, little blood is carried to the skin surface; the blood remains primarily in the viscera to become heated.
Whether a temperature elevation in the critically ill child is caused by fever or hyperthermia, it should be treated aggressively. The metabolic rate increases 10% for every 1° C increase in temperature and three to five times during shivering, thus increasing oxygen, fluid, and caloric requirements. If the child’s cardiovascular or neurologic system is already compromised, these increased needs are especially hazardous. In all children with elevated temperature, attention to adequate hydration is essential. Most children’s needs can be met through additional oral fluids.
FAMILY TEACHING AND HOME CARE
Although most children have learned self-care and hygiene in the home or at school, many have not. For some young children, this is their first introduction to the use of a toothbrush. Much health teaching can be accomplished even when the child is hospitalized for only a short time. The daily bath, hand washing before meals and after bowel and bladder evacuation, and conscientious dental hygiene are taught during routine care. Clean hair, nails, and clothing and good grooming are emphasized as being essential to a pleasing appearance. Positive reinforcement of good hygiene practices helps create a positive body image, enhances self-esteem, and prevents health problems (e.g., teaching girls to wipe the genital area from front to back after toileting).
Although sick children’s appetites may be poor and not characteristic of their home eating habits, the hospital stay provides numerous opportunities for nurses to assess the family’s knowledge of good nutrition and to implement teaching as needed to improve nutritional intake.
Fever is one of the most common problems for which parents seek health care. Parental anxiety increases with temperature elevation and its management (Liebman and Barnsteiner, 2001). Parents need to know that sponging is indicated for elevated temperatures from hyperthermia rather than fever and that ice water and alcohol are inappropriate, potentially dangerous solutions (Axelrod, 2000). Parents should know how to take the child’s temperature and read the thermometer accurately and should have guidelines for seeking professional care (see Family-Centered Care box). Some of the newer temperature-measuring devices, such as plastic strips or digital thermometers, may be better suited for home use than hospital use (see Temperature, Chapter 6). If the use of acetaminophen or ibuprofen is indicated, the parents need instruction in administering the drug. Emphasize accuracy in both the amount of drug given and the time intervals at which the drug is administered.
 FAMILY-CENTERED CARE
FAMILY-CENTERED CARECALL THE OFFICE IMMEDIATELY IF:
Your child is younger than 2 months old.
The fever is over 40.6° C (105° F).
Your child looks or acts very sick: stiff neck, persistent vomiting, purplish spots on skin, confusion, trouble breathing after you have cleaned his nose, or inability to be comforted.
The fever is between 40° and 40.6° C (104° and 105° F), especially if your child is younger than 2 years old.
Had a fever for more than 24 hours without an obvious cause or location of infection
Had a fever for more than 3 days
The fever went away for more than 24 hours and then returned.
Modified from Schmitt BD: Instructions for pediatric patients, ed 2, Philadelphia, 1999, Saunders.
SAFETY
Safety is an essential component of any patient’s care, but children have special characteristics that require an even greater concern for safety. Because small children in the hospital are separated from their usual environment and do not possess the capacity for abstract thinking and reasoning, it is the responsibility of everyone who comes in contact with them to maintain protective measures throughout their hospital stay. Nurses need to understand the age level at which each child is operating and plan for safety accordingly.
Identification bands are particularly important for children. Infants and unconscious patients are unable to tell or respond to their names. Toddlers may answer to any name or to a nickname only. Older children may exchange places, give an erroneous name, or choose not to respond to their own names as a form of joke, unaware of the hazards of such practices.
ENVIRONMENTAL FACTORS
All of the environmental safety measures for the protection of adults apply to children, including good illumination, floors clear of fluid or objects that might contribute to falls, and nonskid surfaces in showers and tubs. All staff members should be familiar with the area-specific fire plan. Elevators and stairways should be made safe
All windows should be secured. Blind and curtain cords should be out of reach, with split cords to prevent strangulation.
Electrical equipment is maintained in good working order, is operated only by personnel familiar with its use, and is not in contact with moisture or situated near tubs. Electrical outlets should be provided with covers to prevent burns in small children, whose exploratory activities may extend to inserting objects into the small openings.
Staff members should practice proper care and disposal of small objects such as syringe caps, needle covers, and temperature probe covers (Fig. 22-3).

FIG. 22-3 To prevent needlestick injuries, used needles (and other sharp instruments) are not capped or broken and are disposed of in a rigid, puncture-resistant container located near the site of use. Note placement of the container to prevent children’s access to the contents.
Bathwater is carefully checked before placing the child in it, and children must never be left alone in a bathtub. Infants are helpless in water, and small children (and some older ones) may turn on the hot water faucet and be severely burned.
Furniture is safest when it is scaled to the child’s proportions, is sturdy, and is well balanced to prevent its being easily tipped over. A special hazard for children is the danger of entrapment under an electronically controlled bed when it is activated to descend. Infants and small children must be securely strapped into infant seats, feeding chairs, and strollers. Baby walkers should not be used because they provide access to hazards and can cause injuries by tipping over. Infants; young children; and those who are weak, paralyzed, agitated, confused, sedated, or cognitively impaired are never left unattended on treatment tables, on scales, or in treatment areas. Even preterm infants are capable of surprising mobility; therefore portholes in incubators must be securely fastened when not in use. Beds of ambulatory patients should remain locked in place and at a height that allows easy access to the floor.
Crib sides are kept up and fastened securely unless an adult is at the bedside. It is safer to leave crib sides up, regardless of the child’s ability to get out and even when the crib is unoccupied, to remove the child’s temptation to climb in. Anyone attending an infant or small child in a crib with the sides down should never turn away without maintaining hand contact with the child; that is, one hand should be kept on the child’s back or abdomen to prevent the child from rolling, crawling, or jumping from the open crib (Fig. 22-4). A child who is apt to or has demonstrated the inclination to climb over the sides of the crib is safest when placed in a specially constructed crib with a cover.

Toy Safety
Toys play a vital role in the everyday life of children, and they are no less important in the hospital setting. Nurses are responsible for assessing the safety of toys brought to the hospital by well-meaning parents and friends. Toys should be appropriate to the child’s age, condition, and treatment. For example, if the child is receiving oxygen, electrical or friction toys are not safe, since sparks can cause oxygen to ignite. Inspect toys to ensure they are nonallergenic, washable, and unbreakable and have no small, removable parts that can be aspirated or swallowed or in other ways injure a child. All objects within reach of children younger than 3 years should pass the choke tube test. A toilet paper roll is a handy guide. If a toy or object fits into the cylinder (items less than 1¼ inches across or balls smaller than 1¾ inches), it is a potential choking danger to the child. Latex balloons pose a serious threat to children of all ages. If the balloon breaks, a child may put a piece of the latex in his or her mouth. If it is aspirated or swallowed, the latex piece is difficult to remove, resulting in choking. Latex balloons should never be permitted in the hospital setting.
Preventing Falls
Multiple interventions are needed to minimize pediatric patients’ risk of falling. Once individual children are identified as at risk for falling, visual identification and communication of the risk among all health care providers is essential. Reduce the risk of falling through patient, family, and staff education.
1. Identify children at risk of falling. Perform a fall risk assessment on patients on admission and throughout hospitalization to identify patients at high risk for falls. Risk factors for hospitalized children include:
Medication effects–postanesthesia or sedation; analgesics or narcotics, especially in those who have never had narcotics in the past and in whom effects are unknown
Altered mental status–secondary to seizures, brain tumors, or medications
Altered or limited mobility–reduced skill at ambulation secondary to developmental age, disease process, tubes, drains, casts, splints, or other appliances; new to ambulation with assistive devices such as walkers or crutches
Postoperative children–risk of hypotension or syncope secondary to large blood loss, a heart condition, or extended bed rest
Infants or toddlers in cribs with side rails down or on the daybed with family members
2. Visually identify patients at risk with one or more of the following:
Post signs on the door and at the bedside.
Apply a special colored armband labeled “Fall Precautions.”
Keep bed in lowest position, breaks locked, and side rails up.
Ensure that all necessary and desired items are within reach (e.g., water, glasses, tissues, snacks).
Offer toileting on a regular basis, especially if patient is taking diuretics or laxatives.
Keep lights on at all times, including dim lights while sleeping.
Lock wheelchairs before transferring patients.
Ensure that patient has appropriate size gown and nonskid footwear. Do not allow gowns or ties to drag on the floor when ambulating.
Keep floor clean and free of clutter. Post “wet floor” sign if floor is wet.
Ensure that patient has glasses on if he or she normally wears them.
4. Educate patients (as age appropriate):
Assist with ambulation even though the child may have ambulated well before hospitalization.
Patients who have been lying in bed will need to get up slowly, sitting on the side of the bed before standing.
Call the nursing staff for assistance, and do not allow patients to get up independently.
Keep the side rails of the crib or bed up whenever patient is in the crib or bed.
Do not leave infants on the daybed; put them in the crib with the side rails up.
When all family members need to leave the bedside, notify staff and ensure the patient is in the bed or crib with side rails up and call bell within reach (if appropriate).
INFECTION CONTROL
According to the Centers for Disease Control and Prevention, approximately 2 million patients each year develop nosocomial (hospital-acquired) infections. These infections occur when there is interaction among patients, health care personnel, equipment, and bacteria (Quality, equipment hold keys to infection control, 2006). Nosocomial infections are preventable if caregivers practice meticulous cleaning and disposal techniques. Standard precautions synthesize the major features of universal (blood and body fluid) precautions (designed to reduce the risk of transmission of blood-borne pathogens) and body substance isolation (designed to reduce the risk of transmission of pathogens from moist body substances). Standard precautions involve the use of barrier protection, such as gloves, goggles, gown, or mask, to prevent contamination from (1) blood; (2) all body fluids, secretions, and excretions except sweat, regardless of whether they contain visible blood; (3) nonintact skin; and (4) mucous membranes. Standard precautions are designed for the care of all patients to reduce the risk of transmission of microorganisms from both recognized and unrecognized sources of infection.
Transmission-based precautions are designed for patients with documented or suspected infection or colonization (presence of microorganism in or on patient but without clinical signs and symptoms of infection) with highly transmissible or epidemiologically important pathogens for which additional precautions beyond standard precautions are needed to interrupt transmission in hospitals. There are three types of transmission-based precautions: airborne precautions, droplet precautions, and contact precautions. They may be combined for diseases that have multiple routes of transmission (Box 22-5). They are to be used in addition to standard precautions.
BOX 22-5 Types of Precautions and Patients Requiring Them
In addition to standard precautions, use airborne precautions for patients known or suspected to have serious illnesses transmitted by airborne droplet nuclei. Examples of such illnesses include measles, varicella (including disseminated zoster), and tuberculosis.
In addition to standard precautions, use droplet precautions for patients known or suspected to have serious illnesses transmitted by large-particle droplets. Examples of such illnesses include:
Invasive Haemophilus influenzae type b, including meningitis, pneumonia, epiglottitis, and sepsis
Invasive Neisseria meningitidis, including meningitis, pneumonia, and sepsis
Other serious bacterial respiratory infections spread by droplet transmission, including diphtheria (pharyngeal), mycoplasmal pneumonia, pertussis, pneumonic plague, streptococcal pharyngitis, pneumonia, or scarlet fever in infants and young children
Serious viral infections spread by droplet transmission, including adenovirus, influenza, mumps, parvovirus B19, rubella
In addition to standard precautions, use contact precautions for patients known or suspected to have serious illnesses easily transmitted by direct patient contact or by contact with items in the patient’s environment. Examples of such illnesses include:
Gastrointestinal, respiratory, skin, or wound infections or colonization with multidrug-resistant bacteria judged by the infection control program, based on current state, regional, or national recommendations, to be of special clinical and epidemiologic significance
Enteric infections with a low infectious dose or prolonged environmental survival, including Clostridium difficile; for diapered or incontinent patients: enterohemorrhagic Escherichia coli 0157:H7, Shigella sp., hepatitis A, or rotavirus
Respiratory syncytial virus, parainfluenza virus, or enteroviral infections in infants and young children
Skin infections that are highly contagious or that may occur on dry skin, including diphtheria (cutaneous), herpes simplex virus (neonatal or mucocutaneous), impetigo, major (noncontained) abscesses, cellulitis or decubiti, pediculosis, scabies, staphylococcal furunculosis in infants and young children, zoster (disseminated or in the immunocompromised host)
From Garner JS: Guidelines for isolation precautions in hospitals, Infect Control Hosp Epidemiol 17(1):66, 1996.
Airborne precautions reduce the risk of airborne transmission of infectious agents. Airborne transmission occurs by dissemination of either airborne droplet nuclei (small-particle residue [5 mm or smaller in size] of evaporated droplets that may remain suspended in the air for long periods) or dust particles containing the infectious agent. Microorganisms carried in this manner can be dispersed widely by air currents and may become inhaled by or deposited on a susceptible host within the same room or over a longer distance from the source patient, depending on environmental factors. Special air handling and ventilation are required to prevent airborne transmission. Airborne precautions apply to patients with known or suspected infection with pathogens transmitted by the airborne route such as measles, varicella, and tuberculosis.
Droplet precautions reduce the risk of droplet transmission of infectious agents. Droplet transmission involves contact of the conjunctivae or the mucous membranes of the nose or mouth of a susceptible person with large-particle droplets (larger than 5 μm in size) containing microorganisms generated from a person who has a clinical disease or who is a carrier of the microorganism. Droplets are generated from the source person primarily during coughing, sneezing, or talking and during procedures such as suctioning and bronchoscopy. Transmission requires close contact between source and recipient persons, since droplets do not remain suspended in the air and generally travel only short distances, usually 3 feet or less, through the air. Because droplets do not remain suspended in the air, special air handling and ventilation are not required to prevent droplet transmission. Droplet precautions apply to any patient with known or suspected infection with pathogens that can be transmitted by infectious droplets (see Box 22-5).
Contact precautions reduce the risk of transmission of microorganisms by direct or indirect contact. Direct-contact transmission involves a skin-to-skin contact and physical transfer of microorganisms to a susceptible host from an infected or colonized person, such as occurs when turning or bathing patients. Direct-contact transmission also can occur between two patients (e.g., by hand contact). Indirect-contact transmission involves contact of a susceptible host with a contaminated intermediate object, usually inanimate, in the patient’s environment. Contact precautions apply to specified patients known or suspected to be infected or colonized with microorganisms that can be transmitted by direct or indirect contact.
Nurses caring for young children are frequently in contact with body substances, especially urine, feces, and vomitus. They should exercise judgment concerning those situations when gloves, gowns, or masks are necessary. For example, gloves and possibly gowns should be worn for changing diapers when there are loose or explosive stools. Otherwise, the plastic lining of disposable diapers provides a sufficient barrier between the hands and body substances. The type of diaper may be an important aspect of infection control. Super absorbent disposable diapers with elastic legs contain urine and feces better than cloth diapers.
Antimicrobial-resistant organisms are causing increasing numbers of nosocomial infections. Nearly 70% of nosocomial infections can be attributed to seven pathogens: the gram-positive organisms Staphylococcus aureus, coagulase-negative staphylococci, and enterococci; and the gram-negative organisms Escherichia coli, Pseudomonas aeruginosa, Enterobacter organisms, and Klebsiella pneumoniae. In hospitals, patients are the most significant sources of methicillin-resistant S. aureus (MRSA), and the main mode of transmission is patient to patient via the hands of a health care provider (Eaton, 2005; Quality, equipment hold keys to infection control, 2006).
During feedings, gowns should be worn if the child is likely to vomit or spit up, which often occurs during burping. When gloves are worn, wash hands thoroughly after removing the gloves, since gloves fail to provide complete protection. The absence of visible leakage does not indicate gloves are intact.
Another essential practice of infection control is that all needles (uncapped and unbroken) are disposed of in a rigid, puncture-resistant container located near the site of use. Consequently, these containers are installed in patients’ rooms. Since children are naturally curious, extra attention is needed in selecting a suitable type of container and a location that prevents access to disposed needles (see Fig. 22-3). The use of needleless systems allows secure syringe or IV tubing attachment to vascular access devices without the risk of needlestick injury to the child or nurse.
TRANSPORTING INFANTS AND CHILDREN
Infants and children usually need to be transported within the unit and to areas outside the pediatric unit. Infants and small children can be carried for short distances within the unit, but for more extended trips the child should be securely transported in a suitable conveyance.
Small infants can be held or carried in the horizontal position with the back supported and the thigh grasped firmly by the carrying arm (Fig. 22-5, A). In the football hold, the infant is carried on the nurse’s arm with the head supported by the hand and the body held securely between the nurse’s body and elbow (Fig. 22-5, B). Both of these holds leave the nurse’s other arm free for activity. The infant also can be held in the upright position with the buttocks on the nurse’s forearm and the front of the body resting against the nurse’s chest. The infant’s head and shoulders are supported by the nurse’s other arm in case the infant moves suddenly (Fig. 22-5, C). Older infants are able to hold their heads erect but are still subject to sudden movements.
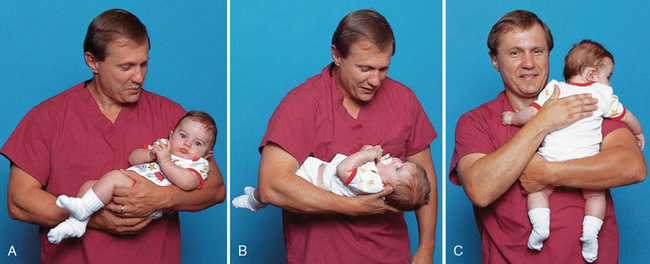
FIG. 22-5 Transporting infants. A, Infant’s thigh firmly grasped in nurse’s hand. B, Football hold. C, Back supported.
Infants can be transported to other areas, such as the radiology department, in their bassinet or crib. Strollers and wheeled feeding chairs or tables are also convenient transporters in some situations, such as trips to the playroom or nurse’s station.
The method of transporting children is determined by their age, condition, and destination. Older children are safe in wheelchairs or on stretchers. Younger children can be transported in a crib, on a stretcher, in a wagon with raised sides, or in a wheelchair with a safety belt. Stretchers should be equipped with high sides and a safety belt, both of which are secured during transport.
RESTRAINING METHODS AND THERAPEUTIC HOLDING
The Joint Commission on Accreditation of Healthcare Organizations (now known as The Joint Commission) (2001) defines restraint as “any method, physical or mechanical, which restricts a person’s movement, physical activity, or normal access to his or her body.” Before initiating restraints, the nurse completes a comprehensive assessment of the patient to determine whether the need for a restraint outweighs the risk of not using one. Restraints can result in loss of dignity, violation of patient rights, psychologic harm, physical harm, and even death. Alternative methods should first be considered and documented in the patient’s record. The nurse is responsible for selecting the least restrictive type of restraint. Using less restrictive restraints is often possible by gaining the cooperation of the child and parents.
The two types of restraints used with children are classified as medical-surgical and behavioral restraints. When a standard or protocol states that immobilization is required 100% of the time as a part of the procedure or postprocedural care process, the restraint device is considered a part of routine care. For example, the postoperative use of elbow restraints after a cleft lip repair, if written in the protocol or standard of care and used for 100% of patients, would not fall under The Joint Commission or Centers for Medicare and Medicaid Services mandates for restraints.
Medical-surgical restraints are used for children with an artificial airway or airway adjunct for delivery of oxygen, indwelling catheters, tubes, drains, lines, pacemaker wires, or suture sites. The medical-surgical restraint is used to ensure that safe care is given to the patient. The potential risks of the restraint are offset by the potential benefit of providing safer care. Medical-surgical restraints may be instituted for any of the following reasons:
Risk for interruption of therapy used to maintain oxygenation or airway patency
Risk of harm if indwelling catheter, tube, drain, line, pacemaker wire, or sutures are removed, dislodged, or ruptured
Patient confusion, agitation, unconsciousness, or developmental inability to understand direct requests or instructions
Medical-surgical restraints can be initiated by an individual order or by protocol; the use of the protocol must be authorized by an individual order. Continued use of restraints must be renewed each day. Patients are monitored at least every 2 hours.
Behavioral restraints are limited to situations with a significant risk of patients physically harming themselves or others because of behavioral reasons and when nonphysical interventions are not effective. Before initiating a behavioral restraint, the nurse should assess the patient’s mental, behavioral, and physical status to determine the cause for the child’s behavior that may be harmful to the patient or others. If behavioral restraints are indicated, a collaborative approach involving the patient, if appropriate, the family, and the health care team should be used. An order must be obtained as soon as possible, but no longer than 1 hour after the initiation of behavioral restraints. Behavioral restraints for children must be reordered every 1 to 2 hours, based on age. A licensed independent practitioner must conduct an in-person evaluation within 1 hour and again every 4 hours until restraints are discontinued. Children in behavioral restraints must be continuously observed and assessed every 15 minutes. Assessment components include signs of injury associated with applying restraint, nutrition and hydration, circulation and range-of-motion of extremities, vital signs, hygiene and elimination, physical and psychologic status and comfort, and readiness for discontinuation of restraint. The nurse must use clinical judgment in setting a schedule for when each of these parameters needs to be evaluated because every parameter must be assessed during each 15-minute physical assessment.
Restraints with ties must be secured to the bed or crib frame, not the side rails. Suggestions for increasing safety and comfort while the child is in a restraint include leaving one finger breadth between skin and the device; tying knots that allow for quick release; ensuring the restraint does not tighten as the child moves; decreasing wrinkles or bulges in the restraint; placing jacket restraints over an article of clothing; placing limb restraints below waist level, below knee level, or distal to the IV; and tucking in dangling straps (Selekman and Snyder, 1997).
An alternative approach for temporary restraint is therapeutic holding. Therapeutic holding is the use of a secure, comfortable, temporary holding position that provides close physical contact with the parent or caregiver for 30 minutes or less (Fig. 22-6).

The use of restraints can often be avoided with adequate preparation of the child; parental or staff supervision of the child; or adequate protection of a vulnerable site, such as an infusion device. The nurse needs to assess the child’s development, mental status, potential to hurt others or self, and safety. The nurse should carefully consider alternatives to using restraints. Some examples of alternative measures include bringing a child to the nurses’ station for continuous observation, providing diversional activities such as music, or encouraging the participation of the parents.
Jacket Restraint
A jacket restraint is sometimes used to keep the child safe in various chairs. The jacket is put on the child with the ties in back so that the child is unable to manipulate them. The long tapes, secured to the understructure of the chair, keep the child inside the chair. The jacket restraint is also useful as a means of maintaining the child in a desired horizontal position.
Mummy Restraint or Swaddle
When an infant or small child requires short-term restraint for examination or treatment that involves the head and neck, such as venipuncture, throat examination, and gavage feeding, a papoose board with straps or a mummy wrap effectively controls the child’s movements. A blanket or sheet is opened on the bed or crib with one corner folded to the center. The infant is placed on the blanket with shoulders at the fold and feet toward the opposite corner. With the infant’s right arm straight down against the body, the right side of the blanket is pulled firmly across the infant’s right shoulder and chest and secured beneath the left side of the body (Fig. 22-7, A). The left arm is placed straight against the infant’s side, and the left side of the blanket is brought across the shoulder and chest and locked beneath the body on the right side. The lower corner is folded and brought over the body and tucked or fastened securely with safety pins. Safety pins can be used to fasten the blanket in place at any step in the process.

FIG. 22-7 Application of mummy restraint. A, Infant placed on folded corner of blanket and one corner of blanket brought across body and secured beneath body. B, Second corner brought across body and secured, and lower corner folded and tucked or pinned in place; modified mummy restraint with chest uncovered.
To modify the mummy restraint for chest examination, the folded edge of the blanket is brought over each arm and under the back, after which the loose edge is folded over and secured at a point below the chest to allow visualization of and access to the chest (Fig. 22-7, B).
Arm and Leg Restraints
Occasionally, one or more extremities must be restrained or limited in motion. Several commercial restraining devices are available, including disposable wrist and ankle restraints. The restraints must be appropriate to the child’s size and padded to prevent undue pressure, constriction, or tissue injury; and the extremity must be observed frequently for signs of irritation or impairment of circulation. The ends of the restraints are never tied to the side rails, since lowering the rail will disturb the extremity, frequently with a jerk that may hurt or injure the child.
Elbow Restraint
Sometimes it is important to prevent the child from reaching the head or face (e.g., after lip surgery, when a scalp vein infusion is in place, or to prevent scratching in skin disorders). Elbow restraints fashioned from a variety of materials function well. Commercial elbow restraints are available. An improvised form of elbow restraint consists of a piece of muslin long enough to reach comfortably from just below the axilla to the wrist with a number of vertical pockets into which tongue depressors are inserted. The restraint is wrapped around the arm and secured with tape or pins. It may be necessary to pin the top of the restraint to the undershirt sleeve to prevent the restraint from slipping.
POSITIONING FOR PROCEDURES
Infants and small children are unable to cooperate for many procedures; therefore the nurse is responsible for minimizing their movement and discomfort with proper positioning. Older children usually need only minimal, if any, restraint. Careful explanation and preparation beforehand and support and simple guidance during the procedure are usually sufficient. For painful procedures the child should receive adequate analgesia and sedation to minimize pain and the need for excessive restraint. For local anesthesia, use buffered lidocaine to reduce the stinging sensation or a topical anesthetic (see Pain Management, Chapter 7).
Femoral Venipuncture
The nurse places the child supine with the legs in a frog position to provide extensive exposure of the groin area. The infant’s legs can be effectively controlled by the nurse’s forearms and hands (Fig. 22-8). Only the side used for the venipuncture is uncovered, so the practitioner is protected should the infant urinate during the procedure. Apply pressure to the site to prevent oozing from the site.

Extremity Venipuncture
The most common sites of venipuncture are the veins of the extremities, especially the arm and hand. A convenient position is to place the child in the parent’s (or assistant’s) lap, with the child facing the parent and in the straddle position. Next, place the child’s arm for venipuncture on a firm surface, such as a treatment table. The child’s outstretched arm is partially stabilized by the technician drawing the blood. Then have the parent hug the child’s upper body, preventing movement, and use an arm to immobilize the venipuncture site. This type of restraint also comforts the child because of the close body contact and allows each person to maintain eye contact (see Fig. 22-6).
Lumbar Puncture
Pediatric lumbar puncture (LP) sets contain smaller spinal needles, but sometimes the practitioner will specify a different size or type of needle. The technique for LP in infants and children is similar to that in the adult, although modifications are suggested in neonates, who have less distress in a side-lying position with modified neck extension than in flexion or a sitting position.
Children are usually controlled best in the side-lying position, with the head flexed and the knees drawn up toward the chest. Even cooperative children need to be held gently to prevent possible trauma from unexpected, involuntary movement. They can be reassured that, although they are trusted, the holding will serve as a reminder to maintain the desired position. It also provides a measure of support and reassurance to them.
The child is placed on the side with the back close to the edge of the examining table on the side from which the practitioner is working. Maintain the child’s spine in a flexed position by holding the child with one arm behind the neck and the other behind the thighs (Fig. 22-9). The flexed position enlarges the spaces between the lumbar vertebrae, which facilitates access to the spinal fluid space. It is helpful to wrap the legs before positioning to decrease leg movement (see Atraumatic Care box).

 ATRAUMATIC CARE
ATRAUMATIC CARELumbar Puncture and Bone Marrow Test
Apply EMLA (an eutectic mixture of lidocaine and prilocaine) to the puncture site at least 60 minutes or LMX cream (lidocaine) at least 30 minutes before the procedure. To identify the lumbar puncture site, draw an imaginary line from the posterior iliac crest across the spine to the opposite iliac crest. The puncture site is intersected by the line at approximately L4. For additional anesthesia, buffered lidocaine with a 30-gauge needle can be used. Sedation with agents such as propofol (Diprivan) or ketamine is recommended for bone marrow biopsy and aspiration.
An alternate position used with small infants and some older children is the sitting position. The child is placed with the buttocks at the edge of the table and with the neck flexed so that the chin rests on the child’s chest or the nurse’s arm. The infant’s arms and legs are immobilized by the nurse’s hands.
Specimens and spinal fluid pressure are obtained, measured, and sent for analysis in the same manner as for the adult patient. Vital signs are taken as ordered, and the child is observed for any changes in level of consciousness, motor activity, or other neurologic signs. Post-LP headache may occur and is related to postural changes; this is less severe when the child lies flat. Headache is seen much less frequently in young children than in adolescents.
Bone Marrow Aspiration or Biopsy
The position for a bone marrow aspiration or biopsy depends on the chosen site. In children the posterior or anterior iliac crest is most frequently used, although in infants the tibia may be selected because of easy access to the site and holding of the child. The sternum, which is the most frequent site in adults, is generally avoided in children because the bone is more fragile and adjacent to vital organs.
If the posterior iliac crest is used, the child is positioned prone. Sometimes a small pillow or folded blanket is placed under the hips to facilitate obtaining the bone marrow specimen. Children should receive adequate analgesia or anesthesia to relieve pain. If the child may awaken, holding may be needed and is best done with two people–one person to immobilize the upper body and a second person to immobilize the lower extremities (see Atraumatic Care box).
COLLECTION OF SPECIMENS
Older children and adolescents can use a bedpan or urinal or can be trusted to follow directions for collection in the bathroom. However, they may have special needs. School-age children are cooperative but curious. They are concerned about the reasons behind things and are likely to ask questions regarding the disposition of their specimen and what one expects to discover from it. Self-conscious adolescents may be reluctant to carry a specimen through a hallway or waiting room and appreciate a paper bag or other means for disguising the container. The presence of menses may be an embarrassment or a concern to teenage girls; therefore it is a good idea to ask if they are menstruating and to make adjustments as necessary. The specimen can be delayed or a notation made on the laboratory slip to explain the presence of red blood cells.
Preschoolers and toddlers are usually unable to void on request. It is often best to offer them water or other liquids that they enjoy and wait about 30 minutes until they are ready to void voluntarily.
Children will better understand what is expected if the nurse uses familiar terms, such as “pee-pee,” “wee-wee,” “tee-tee,” or “tinkle.” Some will have difficulty voiding in an unfamiliar receptacle. Potty chairs or a potty hat placed on the toilet is usually satisfactory. Toddlers who have recently acquired bladder control may be especially reluctant, since they undoubtedly have been admonished for “going” in places other than those approved by parents. A useful approach is to enlist the help of parents; they are likely to be successful.
For infants and toddlers who are not toilet trained, special urine collection bags with self-adhering material round the opening at the point of attachment are used. To prepare the infant, the genitalia, perineum, and surrounding skin are washed and dried thoroughly because the adhesive will not stick to a moist, powdered, or oily skin surface. The collection bag is easiest to apply if attached first to the perineum, progressing to the symphysis pubis (Fig. 22-10). With girls, the perineum is stretched taut during application to that area to ensure a leak-proof fit. With boys the penis and sometimes the scrotum are placed inside the bag. The adhesive portion of the bag must be firmly applied to the skin all around the genital area to avoid leakage. For low-birth-weight infants, small bags with adhesive that is gentle to the skin are available.* Anatomically correct urine collection bags are also available. The Bard Sure Catch is available from Bard Urological Division, C.R. Bard, Inc., 13183 Harland Drive, Covington, GA 30014; (888) 367-2273; http://www.crbard.com.† The diaper is carefully replaced. The bag is checked frequently and removed as soon as the specimen is available, since the moist bag may become loosened on an active child. When urine is collected for culture, the bag is removed immediately. For some types of urine testing, such as specific gravity, ketones, glucose, and protein, urine can be aspirated directly from the diaper. If the urine is not tested within 30 minutes, the specimen is refrigerated or placed in a sterile container with a preservative.
FIG. 22-10 Application of urine collection bag. A, On female infants, adhesive portion is applied to exposed and dried perineum first. B, Bag adheres firmly around perineal area to prevent urine leakage.
When using a urine collection bag, cut a small slit in the diaper and pull the bag through to allow room for urine to collect and to facilitate checking on the contents.
To obtain small amounts of urine, use a syringe without a needle to aspirate urine directly from the diaper; if diapers with absorbent gelling material that trap urine are used, place a small gauze dressing, some cotton balls, or a urine collection device‡ inside the diaper to collect urine and aspirate the urine with a syringe.
‡The Bard Sure Catch is available from Bard Urological Division, C.R. Bard, Inc., 13183 Harland Drive, Covington, GA 30014; (888) 367-2273; http://www.crbard.com.
At times parents may be asked to bring a urine sample to a health care facility for examination, especially when infants are unable to void during an outpatient visit. In this instance parents need instruction on applying the collection device and storing the specimen. Ideally, the specimen should be brought to the designated place as soon as possible; if there is a delay, the sample is refrigerated and the lapsed time reported to the examiner.
Clean-Catch Specimens
Clean-catch specimens traditionally refer to a urine sample obtained for culture after the urethral meatus is cleaned and the first few milliliters of urine are voided before the urine is collected (midstream specimen). In girls, the perineum is wiped with an antiseptic-soaked cotton ball or pad from front to back at least three times, using a new cotton ball or pad each time. In boys, the tip of the penis is cleansed. The area may be wiped with sterile water to prevent accidental contamination of the urine with a solution that may destroy pathogens.
Twenty-Four-Hour Collection
Collection bags are required to collect specimens from infants and small children. Older children require special instruction about notifying someone when they need to void or have a bowel movement so that urine can be collected separately and not discarded. Some older school-age children and adolescents can take responsibility for collection of their own 24-hour specimens and can keep output records and transfer each voiding to the 24-hour collection container.
The collection period always starts and ends with an empty bladder. At the time the collection begins, the child is instructed to void and the specimen is discarded. All urine voided in the subsequent 24 hours is saved in a container with a preservative or is placed on ice. Twenty-four hours from the time the precollection specimen was discarded, the child is again instructed to void, the specimen is added to the container, and the entire collection is taken to the laboratory.
Infants and small children who are bagged for a 24-hour urine collection require a special collection bag. Frequent removal and replacement of adhesive collection devices can produce skin irritation. A thin coating of sealant, such as Skin-Prep, applied to the skin helps to protect it and aids adhesion, unless its use is contraindicated, such as in a preterm infant or a child with irritated skin. Plastic collection bags with collection tubes attached are ideal when the container must be left in place for a time. These can be connected to a collecting device or emptied periodically by aspiration with a syringe. When such devices are not available, a regular bag with a feeding tube inserted through a puncture hole at the top of the bag serves as a satisfactory substitute. However, care is taken to empty the bag as soon as the infant urinates to prevent leakage and loss of contents. An indwelling catheter may also be placed for the collection period.
Bladder Catheterization and Other Techniques
Bladder catheterization or suprapubic aspiration is employed when a specimen is urgently needed or when the child is unable to void or otherwise provide an adequate specimen. Catheterization is used to obtain a sterile urine specimen and when urethral obstruction or anuria caused by renal failure is believed to be the cause of the child’s failure to void. The American Academy of Pediatrics recommends that urine collected by the bag can be used to determine whether it is necessary to obtain a catheterized urine specimen for culture (Wald, 2005). Suprapubic aspiration is useful in clarifying the diagnosis of suspected urinary tract infection in acutely ill infants.
Preparation for catheterization includes instruction on pelvic muscle relaxation. The toddler, preschooler, or younger child is taught to blow a pinwheel and to press the hips against the bed or procedure table during catheterization to relax the pelvic and periurethral muscles. The location and function of the pelvic muscles are described briefly to the older child or adolescent. The patient is then taught to contract and relax the pelvic muscles, and the relaxation procedure is repeated during catheter insertion. If the patient vigorously contracts the pelvic muscles when the catheter reaches the striated sphincter (proximal urethra in boys and midurethra in girls), catheter insertion is temporarily stopped. The catheter is neither removed nor advanced; instead, the child is helped to press the hips against the bed or examining table and relax the pelvic muscles. The catheter is then gently advanced into the bladder (Gray, 1996).
Children and adolescents experience some discomfort and anxiety during this procedure. Assistance and gentle holding may be necessary, especially for the younger child. Most children prefer to have the parents remain with them during the procedure. Encourage the parent to talk softly and hold the child’s hand as the catheter is inserted. Using distractions such as reading a book, singing a song, or playing with small toys may decrease the child’s anxiety. Older children and adolescents may wish to listen to music with headphones. Adolescents should be asked if they would like a parent to remain with them during the procedure. The decision should be made before the perineum is exposed and the sterile field is prepared.
Catheterization is a sterile procedure, and standard precautions for body substance protection should be followed. When placing a catheter to obtain a sterile urine specimen or to check for residual urine, the nurse may use a sterile feeding tube if a catheter is unavailable. If the catheter is to remain in place, a Foley catheter is used. Table 22-3 gives guidelines for choosing the appropriately sized catheter and length of insertion. The supplies needed for this procedure include sterile gloves, sterile lubricant anesthetic, an appropriately sized catheter, povidone-iodine (Betadine) swabs or an alternative cleansing agent and 4 3 4 inch gauze squares, a sterile drape, and a syringe with sterile water if a Foley catheter is used. Test the balloon of the Foley catheter by injecting sterile water before catheter insertion.
TABLE 22-3
Straight Catheter or Foley Catheter*
| SIZE (LENGTH OF INSERTION [cm]) FOR GIRLS | SIZE (LENGTH OF INSERTION [cm]) FOR BOYS | |
| Term neonate | 5-6 (5) | 5-6 (6) |
| Infant–3 years | 5-8 (5) | 5-8 (6) |
| 4-8 years | 8 (5-6) | 8 (6-9) |
| 8 years–prepubertal | 10-12 (6-8) | 8-10 (10-15) |
| Pubertal | 12-14 (6-8) | 12-14 (13-18) |
*Foley catheters are approximately 1 French size larger because of the circumference of the balloon. Example: 10 French Foley = approximately 12 French calibration.
Adolescent boys and children with a history of urethral surgery may be catheterized using a coudé-tipped catheter. The child with myelodysplasia or one who has been identified as being sensitive or allergic to latex is catheterized with a catheter manufactured from an alternative material. When an indwelling catheter is indicated for urinary drainage, a lubricious-coated or silicone catheter is selected because these materials produce less irritation of the urethral mucosa when compared with a Silastic or latex catheter when the catheter is left in place for more than 72 hours.
A 2% lidocaine lubricant with applicator is assembled according to the manufacturer’s instructions,* and several drops of the lubricant are placed at the meatus. Advise the child that the lubricant is used to reduce discomfort associated with inserting the catheter and that introduction of the lubricant and catheter into the urethra will produce a sensation of pressure and a desire to urinate (Gray, 1996) (see Evidence-Based Practice box).
In male patients, grasp the penis with the nondominant hand and retract the foreskin. In uncircumcised newborns and infants, the foreskin may be adhered to the shaft; use care when retracting. If the penis is pendulous, place a sterile drape under the penis. Using the sterile hand, swab the glans and meatus three times with povidone-iodine. Gently introduce the tip of the lidocaine jelly applicator into the urethra 1 to 2 cm (0.4 to 0.8 inch) so that the lubricant flows only into the urethra; insert 5 to 10 ml 2% lidocaine lubricant into the urethra and hold in place for 2 to 3 minutes by gently squeezing the distal penis. Lubricate the catheter and insert into the urethra while gently stretching the penis and lifting it to a 90-degree angle to the body. Resistance may occur when the catheter meets the urethral sphincter. Ask the patient to inhale deeply and advance the catheter. Do not force a catheter that does not easily enter the meatus, particularly if the child has had corrective surgery. For indwelling catheters, once urine is obtained, advance the catheter to the hub, inflate the balloon with sterile water, pull it back gently to test inflation, and connect it to the closed drainage system. Cleanse the glans and meatus and replace retracted foreskin. If blood is seen at any time during the procedure, discontinue the procedure and notify the practitioner.
Use of Lidocaine Lubricant for Urethral Catheterization
Marilyn J. Hockenberry
CRITICALLY ANALYZE THE EVIDENCE
Smith and Adams (1998) surveyed 46 children’s hospitals to determine the existence of standardized practice guidelines for urethral catheter insertion in children. Only 54% of the institutions had a written policy providing guidelines for the procedure, and the hospitals’ recommendations lacked consistency.
Grey (1996) published a review of strategies to minimize distress associated with urethral catheterization in children and supported the use of a local anesthetic that contains 2% lidocaine before insertion.
One prospective, double-blind, placebo-controlled trial evaluated the use of lidocaine lubricant for discomfort in 20 children before urethral catheterization. Findings revealed that lidocaine lubricant significantly reduced pain with pediatric urethral catheterization (Gerard, Cooper, Duethman, and others, 2003).
APPLY THE EVIDENCE: NURSING IMPLICATIONS
Although only one research study was found to support the use of a topical anesthetic before urethral catheterization, the study found significant reductions in procedural pain. Several publications support its effectiveness in clinical practice.
A topical anesthetic before urethral catheterization may be helpful, but further evidence is needed.
REFERENCES
Gerard, LL, Cooper, CS, Duethman, KS, et al. Effectiveness of lidocaine lubricant for discomfort during pediatric urethral catheterization. J Urol. 2003;170:564–567.
Grey, M. Atraumatic urethral catheterization of children. Pediatr Nurs. 1996;22(4):306–310.
Smith, AB, Adams, LL. Insertion of indwelling urethral catheters in infants and children: a survey of current nursing practice. Pediatr Nurs. 1998;24(3):229–234.
In female patients, place a sterile drape under the buttocks. Use the nondominant hand to gently separate and pull up the labia minora to visualize the meatus. Swab the meatus from front to back three times, using a different povidone-iodine swab each time. Place 1 to 2 ml 2% lidocaine lubricant on the periurethral mucosa, and insert 1 to 2 ml into the urethral meatus. Delay catheterization for 2 to 3 minutes to maximize absorption of the anesthetic into the periurethral and intraurethral mucosa. Add lubricant to the catheter, and gently insert into the urethra until urine returns then advance the catheter an additional 2.5 to 5 cm (1 to 2 inches). When using a Foley catheter, inflate the balloon with sterile water and gently pull back, then connect to a closed drainage system. Cleanse the meatus and labia (see Cultural Awareness box). Because the use of lidocaine jelly can increase the volume of intraurethral lubricant, urine return may not be as rapid as when minimal lubrication is used.
Suprapubic aspiration is mainly used when the bladder cannot be accessed through the urethra (such as with some congenital urologic birth defects) or to reduce the risk of contamination that may be present when passing a catheter. With the advent of small catheters (5 and 6 French), the need for suprapubic aspiration has decreased. Access to the bladder via the urethra has a much higher success rate than suprapubic aspiration, where success depends on the practitioner’s skill at assessing the location of the bladder and the amount of urine in the bladder. Suprapubic aspiration involves aspirating bladder contents by inserting a 20- or 21-gauge needle in the midline approximately 1 cm (0.4 inch) above the symphysis pubis and directed vertically downward. The skin is prepared as for any needle insertion, and the bladder should contain an adequate volume of urine. This can be assumed if the infant has not voided for at least 1 hour or the bladder can be palpated above the symphysis pubis. This technique is useful for obtaining sterile specimens from young infants, since the bladder is an abdominal organ and is easily accessed. Suprapubic aspiration is painful, and therefore pain management during the procedure is important.
 CULTURAL AWARENESS
CULTURAL AWARENESSParents may be upset when their child is catheterized. Aside from the trauma the child experiences, some parents may fear that the procedure affects the daughter’s virginity. To correct this misconception, the family may benefit from a detailed explanation of the genitourinary anatomy, preferably with a model that shows the separate vaginal and urethral openings. The nurse can also indicate that catheterization has no effect on virginity.