Family-Centered Care of the Child During Illness and Hospitalization
On completion of this chapter the reader will be able to:
 Identify the stressors of illness and hospitalization for children during each developmental stage.
Identify the stressors of illness and hospitalization for children during each developmental stage.
List essential priorities of nursing care for a child on admission to the hospital.
Outline nursing interventions that prevent or minimize the stress of separation during hospitalization.
Outline nursing interventions that minimize the stress of loss of control during hospitalization.
Outline nursing interventions that minimize the fear of bodily injury during hospitalization.
Outline nursing interventions that support parents, siblings, and family during a child’s illness and hospitalization.
Describe nursing interventions needed when children are admitted to special units such as the emergency department.
RELATED TOPICS and ADDITIONAL RESOURCES
 IN TEXT
IN TEXTAdministration of Medication, Ch. 22
Compliance, Ch. 22
Cultural and Religious Influences on Health Care, Ch. 4
Developmental Assessment, Ch. 5
Family-Centered Care, Ch. 18
Family-Centered Home Care, Ch. 20
Impact of the Child’s Chronic Illness or Disability, Ch. 18
Neonatal Pain, Ch. 9
Normalization, Ch. 18
Nursing Diagnosis, Ch. 1
Pain Assessment and Management in Children, Ch. 7
Physical Examination, Ch. 6
Preparation for Diagnostic and Therapeutic Procedures, Ch. 22
Surgical Procedures, Ch. 22
STRESSORS OF HOSPITALIZATION AND CHILDREN’S REACTIONS
Often, illness and hospitalization are the first crises children must face. Especially during the early years, children are particularly vulnerable to the crises of illness and hospitalization because (1) stress represents a change from the usual state of health and environmental routine and (2) children have a limited number of coping mechanisms to resolve stressors (those events that produce stress). Major stressors of hospitalization include separation, loss of control, bodily injury, and pain. Children’s reactions to these crises are influenced by their developmental age; their previous experience with illness, separation, or hospitalization; their innate and acquired coping skills; the seriousness of the diagnosis; and the support system available.
SEPARATION ANXIETY
The major stress from middle infancy throughout the preschool years, especially for children ages 6 to 30 months, is separation anxiety, also called anaclitic depression. The principal behavioral responses to this stressor during early childhood are summarized in Box 21-1. During the phase of protest, children react aggressively to the separation from the parent. They cry and scream for their parents, refuse the attention of anyone else, and are inconsolable in their grief (Fig. 21-1). During the phase of despair, the crying stops and depression is evident. The child is much less active, is uninterested in play or food, and withdraws from others (Fig. 21-2).
BOX 21-1 Manifestations of Separation Anxiety in Young Children
Behaviors observed during later infancy include:
Additional behaviors observed during toddlerhood include:
Verbally attacks strangers (e.g., “Go away”)
Physically attacks strangers (e.g., kicks, bites, hits, pinches)
Behaviors may last from hours to days.
Protest, such as crying, may be continuous, ceasing only with physical exhaustion.
Observed behaviors include:
Behaviors may last for variable length of time.
Child’s physical condition may deteriorate from refusal to eat, drink, or move.

FIG. 21-1 In the protest phase of separation anxiety, children cry loudly and are inconsolable in their grief for the parent. (Courtesy James DeLeon, Texas Children’s Hospital, Houston.)
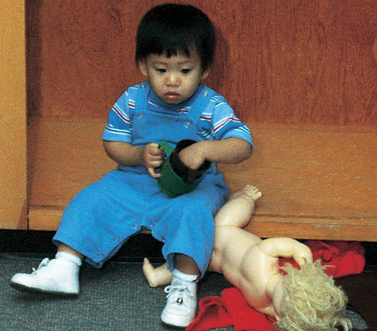
FIG. 21-2 During the despair phase of separation anxiety, children are sad, lonely, and uninterested in food and play.
The third stage is detachment, also called denial. Superficially it appears that the child has finally adjusted to the loss. The child becomes more interested in the surroundings, plays with others, and seems to form new relationships. However, this behavior is the result of resignation and is not a sign of contentment. The child detaches from the parent in an effort to escape the emotional pain of desiring the parent’s presence and copes by forming shallow relationships with others, becoming increasingly self-centered, and attaching primary importance to material objects. This is the most serious stage in that reversal of the potential adverse effects is less likely to occur after detachment is established. However, in most situations, the temporary separations imposed by hospitalization do not cause such prolonged parental absences that the child enters into detachment. In addition, considerable evidence suggests that even with stressors such as separation, children are remarkably adaptable and permanent ill effects are rare.
Although progression to the stage of detachment is uncommon, the initial stages are frequently observed even with brief separations from either parent. Unless health team members understand the meaning of each stage of behavior, they may erroneously label the behaviors as positive or negative. For example, they may see the loud crying of the protest phase as “bad” behavior. Because the protests increase when a stranger approaches the child, they may interpret that reaction as meaning they should stay away. During the quiet, withdrawn phase of despair, health team members may think that the child is finally “settling in” to the new surroundings, and they may see the detachment behaviors as proof of a “good adjustment.” The faster this stage is reached, the more likely it is that the child will be regarded as the “ideal patient.”
Because children seem to react “negatively” to visits by their parents, uninformed observers feel justified in restricting parental visiting privileges. For example, during the protest stage, children outwardly do not appear happy to see their parents (Fig. 21-3). In fact, they may even cry louder. If they are depressed, they may reject their parents or begin to protest again. Often they cling to their parents in an effort to ensure their continued presence. Consequently, such reactions may be regarded as “disturbing” the child’s adjustment to the new surroundings. If the separation has progressed to the phase of detachment, children will respond no differently to their parents than they would to any other person.

FIG. 21-3 Young children may appear withdrawn and sad even in the presence of a parent. (Courtesy E. Jacob, Texas Children’s Hospital, Houston.)
Such reactions are distressing to parents, who are unaware of their meaning. If parents are regarded as intruders, they will see their absence as “beneficial” to the child’s adjustment and recovery. They may respond to the child’s behavior by staying for only short periods, visiting less frequently, or deceiving the child when it is time to leave. The result is a destructive cycle of misunderstanding and unmet needs.
Early Childhood
Separation anxiety is the greatest stress imposed by hospitalization during early childhood. If separation is avoided, young children have a tremendous capacity to withstand any other stress. During this age period, the typical reactions just described are seen. However, children in the toddler stage demonstrate more goal-directed behaviors. For example, they may plead with the parents to stay and physically try to keep the parents with them or try to find parents who have left. They may demonstrate displeasure on the parents’ return or departure by having temper tantrums; refusing to comply with the usual routines of mealtime, bedtime, or toileting; or regressing to more primitive levels of development. However, temper tantrums, bed-wetting, or other behaviors may also be expressions of anger, a physiologic response to stress, or symptoms of illness.
Because preschoolers are more secure interpersonally than toddlers, they can tolerate brief periods of separation from their parents and are more inclined to develop substitute trust in other significant adults. However, the stress of illness usually renders preschoolers less able to cope with separation; as a result, they manifest many of the stage behaviors of separation anxiety, although in general the protest behaviors are more subtle and passive than those seen in younger children. Preschoolers may demonstrate separation anxiety by refusing to eat, experiencing difficulty in sleeping, crying quietly for their parents, continually asking when the parents will visit, or withdrawing from others. They may express anger indirectly by breaking their toys, hitting other children, or refusing to cooperate during usual self-care activities. Nurses need to be sensitive to these less obvious signs of separation anxiety in order to intervene appropriately.
Later Childhood and Adolescence
Previous research, usually based on adult recollections, indicated that the family does not play as important a role for school-age children as it does during the toddler and preschool years. However, in a recent study that asked children about their fears when hospitalized, children listed their greatest fears regarding hospitalization as being separated from family and friends, being in an unfamiliar environment, receiving investigations or treatments, and losing self-determination or choices (Coyne, 2006).
Although school-age children are better able to cope with separation in general, the stress and often accompanying regression imposed by illness or hospitalization may increase their need for parental security and guidance. This is particularly true for young school-age children who have only recently left the safety of the home and are struggling with the crisis of school adjustment. Middle and late school-age children may react more to the separation from their usual activities and peers than to the absence of their parents. These children have a high level of physical and mental activity that frequently finds no suitable outlets in the hospital environment, and even when they dislike school, they admit to missing its routine and worry that they will not be able to compete or “fit in” with their classmates when they return. Feelings of loneliness, boredom, isolation, and depression are common. Such reactions may occur more as a result of separation than of concern over the illness, treatment, or hospital setting.
School-age children may need and desire parental guidance or support from other adult figures but may be unable or unwilling to ask for it. Because the goal of attaining independence is so important to them, they are reluctant to seek help directly, fearing that they will appear weak, childish, or dependent. Cultural expectations to “act like a man” or to “be brave and strong” weigh heavily on these children, especially boys, who tend to react to stress with stoicism, withdrawal, or passive acceptance. Often the need to express hostile, angry, or other negative feelings finds outlets in alternate ways, such as irritability and aggression toward parents, withdrawal from hospital personnel, inability to relate to peers, rejection of siblings, or subsequent behavioral problems in school.
For adolescents, separation from home and parents may produce varied emotions, ranging from difficulty coping to welcoming the event. However, loss of peer-group contact may pose a severe emotional threat because of loss of group status, inability to exert group control or leadership, and loss of group acceptance. Deviations within peer groups are poorly tolerated, and although group members may express concern for the adolescent’s illness or need for hospitalization, they continue their group activities, quickly filling the gap of the absent member. During the temporary separation from their usual group, ill adolescents may benefit from group associations with other hospitalized teens.
LOSS OF CONTROL
One of the factors influencing the amount of stress imposed by hospitalization is the amount of control that persons perceive themselves as having. Lack of control increases the perception of threat and can affect children’s coping skills. Many hospital situations decrease the amount of control a child feels. Although the usual sensory stimulations are lacking, the additional hospital stimuli of sight, sound, and smell may be overwhelming. Without an insight into the type of environment conducive to children’s optimal growth, the hospital experience can at best temporarily slow development and at worst permanently restrict it. Because children’s needs vary greatly depending on their age, the major areas of loss of control in terms of physical restriction, altered routine or rituals, and dependency are discussed for each age-group.
Infants
Infants are developing the most important attribute of a healthy personality—trust. Trust is established through consistent, loving care by a nurturing person. Infants attempt to control their environment through emotional expressions, such as crying or smiling. In the hospital setting, cues may be missed or misinterpreted, and routines may be established to meet the hospital staff’s needs instead of the infant’s needs. Inconsistent care and deviations from the infant’s daily routine may lead to mistrust and a decreased sense of control.
Toddlers
Toddlers are striving for autonomy, and this goal is evident in most of their behaviors: motor skills, play, interpersonal relationships, activities of daily living, and communication. When their egocentric pleasures meet with obstacles, toddlers react with negativism, especially temper tantrums. Any restriction or limitation of movement, such as the simple act of making toddlers lie down, can cause forceful resistance and noncompliance.
Loss of control also results from altered routines and rituals. Toddlers rely on the consistency and familiarity of daily rituals to provide a measure of stability and control in their complex world of growing and developing. The experience of hospitalization or illness severely limits their sense of expectation and predictability, since practically every detail of the hospital environment differs from that of the home.
Toddlers’ main areas for rituals include eating, sleeping, bathing, toileting, and play. When the routines are disrupted, difficulties can occur in any or all of these areas. The principal reaction to such change is regression. For example, when mealtime and food choices differ from those at home, toddlers often refuse to eat, demand a bottle, or ask others to feed them. Although regression to earlier forms of behavior may seem to increase toddlers’ security and comfort, in reality it is threatening for them to relinquish their most recently acquired achievements.
Enforced dependency is a chief characteristic of the sick role and accounts for the numerous instances of toddler negativism. For example, rigid schedules, different clothes, altered caregiving activities, unfamiliar surroundings, separation from parents, and medical procedures usurp toddlers’ control over their world. Although most toddlers initially react negatively and aggressively to such dependency, prolonged loss of autonomy may result in passive withdrawal from interpersonal relationships and regression in all areas of development. Therefore the effects of the sick role are most severe in instances of chronic, long-term illnesses or in those families who foster the sick role despite the child’s improved state of health.
Preschoolers
Preschoolers also suffer from loss of control caused by physical restriction, altered routines, and enforced dependency. However, their specific cognitive abilities, which make them feel all-powerful, also make them feel out of control. This loss of control in the context of their sense of self-power is a critical influencing factor in their perception of and reaction to separation, pain, illness, and hospitalization.
Preschoolers’ egocentric and magical thinking limits their ability to understand events because they view all experiences from their own self-referenced (egocentric) perspective. Without adequate preparation for unfamiliar settings or experiences, preschoolers’ fantasy explanations for such events are usually more exaggerated, bizarre, and frightening than the facts. One typical fantasy to explain the illness or hospitalization is that it represents punishment for real or imagined misdeeds. In response to such thinking the child usually feels shame, guilt, and fear.
Preschoolers’ preoperational thinking means that they understand explanations only in terms of real events. Purely verbal instructions are often inadequate for them because they are unable to abstract and synthesize beyond what their senses tell them. When combined with their egocentric and magical thinking, this characteristic may lead them to interpret messages according to their particular past experiences. Even with the best preparation for a procedure, they may misconstrue the details.
Transductive reasoning implies that preschoolers deduct from the particular to the particular, rather than from the specific to the general, or vice versa. For example, if preschoolers’ concept of nurses is that they inflict pain, preschoolers will think that every nurse, or everyone wearing a similar uniform, will also inflict pain.
School-Age Children
Because of their striving for independence and productivity, school-age children are particularly vulnerable to events that may lessen their feeling of control and power. In particular, altered family roles; physical disability; fears of death, abandonment, or permanent injury; loss of peer acceptance; lack of productivity; and inability to cope with stress according to perceived cultural expectation may result in loss of control.
Because of the nature of the patient role, many routine hospital activities usurp individual power and identity. For school-age children, dependent activities such as enforced bed rest, use of a bedpan, inability to choose a menu, lack of privacy, help with a bed bath, or transport by a wheelchair or stretcher can be a direct threat to their security. Although all these procedures seem routine and inconsequential, they allow no freedom of choice to children who want to “act grown-up.” However, when children are allowed to exert a measure of control, regardless of how limited it may be, they generally respond well to any procedure. For example, some of the most cooperative, satisfied, and contented patients are school-age children who help make their beds, choose their schedule of activities, and assist in their own care. An increased sense of control usually results from a feeling of usefulness and productivity.
In addition to the hospital environment, illness may also cause a feeling of loss of control. One of the most significant problems of children in this age-group is boredom. When physical or enforced limitations curtail their usual ability to care for themselves or to engage in favorite activities, school-age children generally respond with depression, hostility, or frustration. Keeping a normally active child on bed rest is difficult. However, emphasizing areas of control and capitalizing on quiet activities, particularly hobbies such as building models or playing age-appropriate video or board games, promotes their adjustment to physical restriction.
Adolescents
Adolescents’ struggle for independence, self-assertion, and liberation centers on the quest for personal identity. Anything that interferes with this poses a threat to their sense of identity and results in a loss of control. Illness, which limits one’s physical abilities, and hospitalization, which separates one from one’s usual support systems, constitute major situational crises.
The patient role fosters dependency and depersonalization. Adolescents may react to dependency with rejection, uncooperativeness, or withdrawal. They may respond to depersonalization with self-assertion, anger, or frustration. Regardless of the response elicited, hospital personnel often regard them as difficult, unmanageable patients. Parents may not be a source of help because these behaviors serve to isolate them further from understanding the adolescent. Although peers may visit, they may not be able to offer the kind of support and guidance needed. Sick adolescents often voluntarily isolate themselves from age-mates until they feel they can compete on an equal basis and meet group expectations. As a result, ill adolescents may be left with virtually no support system.
Loss of control also occurs for many of the reasons discussed for school-age children. However, adolescents are more sensitive to potential instances of loss of control and dependency than are younger children. For example, both groups seek information about their physical status and rely heavily on anticipatory preparation to decrease fear and anxiety. However, adolescents react not only to the kinds of information supplied them, but also to the means by which it is conveyed. They may feel threatened by others who convey facts in a condescending manner. Adolescents want to know that others can relate to them on their own level. This necessitates a careful assessment of their intellectual abilities, previous knowledge, and present needs. It may also require the nurse’s willingness to learn the adolescent’s language.
EFFECTS OF HOSPITALIZATION ON THE CHILD
Children may react to the stresses of hospitalization before admission, during hospitalization, and after discharge. A child’s concept of illness is even more important than age and intellectual maturity in predicting the level of anxiety before hospitalization (Clatworthy, Simon, and Tiedeman, 1999). This may or may not be affected by the duration of the condition or prior hospitalizations; therefore nurses should avoid overestimating the illness concepts of children with prior medical experience (Box 21-2).
Individual Risk Factors
A number of risk factors make certain children more vulnerable than others to the stresses of hospitalization (Box 21-3). Rural children may exhibit significantly greater degrees of psychologic upset than urban children, possibly because urban children have opportunities to become familiar with a local hospital. Because separation is such an important issue surrounding hospitalization for young children, children who are active and strong willed tend to fare better when hospitalized than youngsters who are passive. Consequently, nurses should be alert to children who passively accept all changes and requests; these children may need more support than the “oppositional” child.
The stressors of hospitalization may cause young children to experience short- and long-term negative outcomes. Adverse outcomes may be related to the length and number of admissions, multiple invasive procedures, and the parents’ anxiety. Common responses include regression, separation anxiety, apathy, fears, and sleeping disturbances, especially for children younger than 7 years of age (Melnyk, 2000). Supportive practices, such as family-centered care and frequent family visiting, may lessen the detrimental effects of such admissions. Research also indicates that a child’s pain experience determines how the overall hospitalization is experienced (Woodgate and Kristjanson, 1996). Consequently, nurses should attempt to identify children at risk for poor coping strategies (Small, 2002).
Changes in the Pediatric Population.: The pediatric population in hospitals has changed dramatically over the past two decades. With a growing trend toward shortened hospital stays and outpatient surgery, a greater percentage of the children hospitalized today have more serious and complex problems than those hospitalized in the past. Many of these children are fragile newborns and children with severe injuries or disabilities who have survived because of major technologic advances, yet have been left with chronic or disabling conditions that require often frequent and lengthy hospital stays. The nature of their conditions increases the likelihood that they will experience more invasive and traumatic procedures while they are hospitalized. These factors make them more vulnerable to the emotional consequences of hospitalization and result in their needs being significantly different from those of the short-term patients of the past (see Chapter 18 for further discussion on children with special needs). The majority of these children are infants and toddlers, the age-group most vulnerable to the effects of hospitalization.
Concern in recent years has focused on the increasing length of hospitalization because of complex medical and nursing care, elusive diagnoses, and complicated psychosocial issues. Without special attention devoted to meeting the child’s psychosocial and developmental needs in the hospital environment, the detrimental consequences of prolonged hospitalization may be severe.
Beneficial Effects of Hospitalization
Although hospitalization can be and usually is stressful for children, it can also be beneficial. The most obvious benefit is the recovery from illness, but hospitalization also can present an opportunity for children to master stress and feel competent in their coping abilities. The hospital environment can provide children with new socialization experiences that can broaden their interpersonal relationships. The psychologic benefits need to be considered and maximized during hospitalization. Appropriate nursing strategies to achieve this goal are presented on p. 668.
STRESSORS AND REACTIONS OF THE FAMILY OF THE CHILD WHO IS HOSPITALIZED
The crisis of childhood illness and hospitalization affects every member of the family. Parents’ reactions to illness in their child depend on a variety of factors. Although one cannot predict which factors are most likely to influence their response, a number of variables have been identified (Box 21-4). (See also Chapter 18.)
BOX 21-4 Factors Affecting Parents’ Reactions to Their Child’s Illness
Recent research has identified common themes among parents whose children were hospitalized, including feeling an overall sense of helplessness, questioning the skills of staff, accepting the reality of hospitalization, needing to have information explained in simple language, dealing with fear, coping with uncertainty, and seeking reassurance from caregivers. This reassurance involves staff being compassionate, expressing concern for the child, and attending to detail in the child’s care (Stranton, 2004).
SIBLING REACTIONS
Siblings’ reactions to a sister’s or brother’s illness or hospitalization are discussed in Chapter 18 and differ little when a child becomes temporarily ill. Siblings experience loneliness, fear, and worry, as well as anger, resentment, jealousy, and guilt. Various factors have been identified that influence the effects of the child’s hospitalization on siblings. Although these factors are similar to those seen when a child has a chronic illness, Craft (1993) reported that the following factors regarding siblings are related specifically to the hospital experience and increase the effects on the sibling:
Being younger and experiencing many changes
Being cared for outside the home by care providers who are not relatives
Receiving little information about their ill brother or sister
Perceiving that their parents treat them differently compared with before their sibling’s hospitalization
Parents are often unaware of the number of effects that siblings experience during the sick child’s hospitalization and the benefit of simple interventions to minimize such effects, such as explicit explanations about the illness and provisions for the siblings to remain at home. Sibling visitation is usually beneficial to the patient, sibling, and parent but should be evaluated on an individual basis. Siblings should be prepared for the visit with developmentally appropriate information and be given the opportunity to ask questions.
ALTERED FAMILY ROLES
In addition to the effects of separation on family roles, loss of parenting, sibling, and offspring roles may affect each family member differently. One of the most common reactions of parents is specialized and intensified attention toward the sick child. The other siblings may regard this as unfair and interpret the parents’ attitude toward them as rejection. Although such responses are usually unconscious and unintended, they place unique burdens on ill children. For example, the ill child may feel obligated to play the sick role to meet parents’ expectations, especially those children who have had limited physical ability and regain normal health status, such as after corrective heart surgery. Parents may be unable to perceive the child’s recovery and therefore continue the pattern of overprotection and indulgent attention.
Ill children may also feel jealousy and resentment from other siblings. Because of their singular position in the family, they may be denied the companionship of their brothers and sisters. Rivalry between siblings tends to be greatest for the sibling who is nearest in age to the ill child. Without an understanding of the interpersonal dynamics between siblings, parents are likely to blame the well children for antisocial behavior. Illness may also result in children’s loss of status within either their family or social group. For example, illness in the oldest child may temporarily terminate special privileges as “big” brother or sister.
NURSING CARE OF THE CHILD WHO IS HOSPITALIZED
PREPARATION FOR HOSPITALIZATION
Children and families require individualized care to minimize the potential negative effects of hospitalization. One method that can decrease negative feelings and fear in children is preparation for hospitalization. The rationale for preparing children for the hospital experience and related procedures is based on the principle that fear of the unknown (fantasy) exceeds fear of the known. When children do not have paralyzing fear to cope with, they are able to direct their energies toward dealing with the other, unavoidable stresses of hospitalization.
Although preparation for hospitalization is a common practice, there is no universal standard or program for all settings. The preparation process may be elaborate with tours, puppet shows, and playtime with miniature hospital equipment; it may involve the use of books, videos, or films; or it may be limited to a brief description of the major aspects of any hospital stay (Stewart, Algren, and Arnold, 1994). No consensus exists on the timing of preparation. Some authorities recommend preparing children 4 to 7 years of age about 1 week in advance so that they can assimilate the information and ask questions. For older children the time may be longer. However, for young children, who may begin to fantasize about what they observed, 1 or 2 days before admission is sufficient time for anticipatory preparation. The length of the session should be tailored to the children’s attention span— the younger the child, the shorter the program. The optimal approach is one that is individualized for each child and family.
Regardless of the specific type of program, all children, even those who have been hospitalized before, benefit from an introduction to the environment and routine of the unit. Sometimes it is not possible to prepare children and families for hospitalization, such as in the event of sudden, acute illness. However, care should be taken to orient the child and family to hospital routines, establish expectations, and allow for questions.
Admission Assessment
The nursing admission history refers to a systematic collection of data about the child and family that allows the nurse to plan individualized care. The nursing admission history presented in Box 21-5 is organized according to the Functional Health Patterns outlined by Gordon (1994, 2002) (see Nursing Diagnosis, Chapter 1). This assessment framework is a guideline for formulating nursing diagnoses. One of the main purposes of the history is to assess the child’s usual health habits at home to promote a more normal environment in the hospital. Therefore questions related to activities of daily living in the nutritional-metabolic, elimination, sleep-rest, and activity-exercise patterns are a major part of the assessment. The questions found under the health perception–health management pattern are directed toward evaluation of the child’s preparation for hospitalization and are key factors in determining whether additional preparation is needed. The questions included in the self-perception–self-concept and role-relationship patterns offer insight into the child’s potential reaction to hospitalization, especially in terms of separation.
BOX 21-5 Nursing Admission History According to Functional Health Patterns*
HEALTH PERCEPTION–HEALTH MANAGEMENT PATTERN
Why has your child been admitted?
How has your child’s general health been?
What does your child know about this hospitalization?
Ask the child why he or she came to the hospital.
If the answer is “For an operation or for tests,” ask the child to tell you about what will happen before, during, and after the operation or tests.
Has your child ever been in the hospital before?
How was that hospital experience?
What things were important to you and your child during that hospitalization? How can we be most helpful now?
What medications does your child take at home?
How are they given (if a liquid, with a spoon; if a tablet, swallowed with water; or other)?
Does your child have any trouble taking medication? If so, what helps?
What, if any, forms of complementary medicine practices are being used?
What are the family’s usual mealtimes?
Do family members eat together or at separate times?
What are your child’s favorite foods, beverages, and snacks?
Average amounts consumed or usual size of portions
Special cultural practices, such as family eats only ethnic food
What foods and beverages does your child dislike?
What are your child’s feeding habits (bottle, cup, spoon, eats by self, needs assistance, any special devices)?
How does your child like the food served (warmed, cold, one item at a time)?
How would you describe your child’s usual appetite (hearty eater, picky eater)?
Are there any known or suspected food allergies?
Is your child on a special diet?
Are there any feeding problems (excessive fussiness, spitting up, colic); any dental or gum problems that affect feeding?
What are your child’s toilet habits (diaper, toilet trained—day only or day and night, use of word to communicate urination or defecation, potty chair, regular toilet, other routines)?
What is your child’s usual pattern of elimination (bowel movements)?
Do you have any concerns about elimination (bed-wetting, constipation, diarrhea)?
What is your child’s usual hour of sleep and awakening?
What is your child’s schedule for naps; length of naps?
Is there a special routine before sleeping (bottle, drink of water, bedtime story, night-light, favorite blanket or toy, prayers)?
Is there a special routine during sleep time, such as waking to go to the bathroom?
What type of bed does your child sleep in?
Does your child have a separate room or share a room; if shares, with whom?
Does your child sleep with someone or alone (e.g., sibling, parent, other person)?
What is your child’s favorite sleeping position?
Are there any sleeping problems (falling asleep, waking during night, nightmares, sleep walking)?
Are there any problems in awakening and getting ready in the morning?
What is your child’s schedule during the day (preschool, daycare center, regular school, extracurricular activities)?
What are your child’s favorite activities or toys (both active and quiet interests)?
What is your child’s usual television-viewing schedule at home?
What are your child’s favorite programs?
Are there any television restrictions?
Does your child have any illness or disabilities that limit activity? If so, how?
What are your child’s usual habits and schedule for bathing (bath in tub or shower, sponge bath, shampoo)?
What are your child’s dental habits (brushing, flossing, fluoride supplements or rinses, favorite toothpaste); schedule of daily dental care?
Does your child need help with dressing or grooming, such as hair combing?
Are there any problems with these patterns (dislike of or refusal to bathe, shampoo hair, or brush teeth)?
Are there special devices that your child requires help in managing (eyeglasses, contact lenses, hearing aid, orthodontic appliances, artificial elimination appliances, orthopedic devices)?
note: Use the following code to assess functional self-care level for feeding, bathing/hygiene, dressing/grooming, toileting:
Does your child have any hearing difficulty?
Does your child have any vision problems?
Does your child have any learning difficulties?
What is the child’s grade in school?
For information on pain, see Chapter 7.
SELF-PERCEPTION–SELF-CONCEPT PATTERN
How would you describe your child (e.g., takes time to adjust, settles in easily, shy, friendly, quiet, talkative, serious, playful, stubborn, easygoing)?
What makes your child angry, annoyed, anxious, or sad? What helps?
How does your child act when annoyed or upset?
What have been your child’s experiences with and reactions to temporary separation from you (parent)?
Does your child have any fears (places, objects, animals, people, situations)?
Do you think your child’s illness has changed the way he or she thinks about self (e.g., more shy, embarrassed about appearance, less competitive with friends, stays at home more)?
Does your child have a favorite nickname?
What are the names of other family members or others who live in the home (relatives, friends, pets)?
Who usually takes care of your child during the day/night (especially if other than parent, such as baby-sitter, relative)?
What are the parents’ occupations and work schedules?
Are there any special family considerations (adoption, foster child, stepparent, divorce, single parent)?
Have any major changes in the family occurred lately (death, divorce, separation, birth of a sibling, loss of a job, financial strain, mother beginning a career, other)? Describe child’s reaction.
Who are your child’s play companions or social groups (peers, younger or older children, adults, prefers to be alone)?
Do things generally go well for your child in school or with friends?
Does your child have “security” objects at home (pacifier, bottle, blanket, stuffed animal or doll)? Did you bring any of these to the hospital?
How do you handle discipline problems at home? Are these methods always effective?
Does your child have any condition that interferes with communication? If so, what are your suggestions for communicating with your child?
Will your child’s hospitalization affect the family’s financial support or care of other family members (e.g., other children)?
What concerns do you have about your child’s illness and hospitalization?
Who will be staying with your child while hospitalized?
How can we contact you or another close family member outside of the hospital?
SEXUALITY-REPRODUCTIVE PATTERN
(Answer questions that apply to your child’s age-group.)
Has your child begun puberty (developing physical sexual characteristics, menstruation)? Have you or your child had any concerns?
Does your daughter know how to do breast self-examination?
Does your son know how to do testicular self-examination?
How have you approached topics of sexuality with your child?
Do you think you might need some help with some topics?
Has your child’s illness affected the way he or she feels about being a boy or a girl? If so, how?
Do you have any concerns with behaviors in your child, such as masturbation, asking many questions or talking about sex, not respecting others’ privacy, or wanting too much privacy?
Initiate a conversation about an adolescent’s sexual concerns with open-ended to more direct questions and using the terms “friends” or “partners” rather than “girlfriend” or “boyfriend”:
Tell me about your social life.
Who are your closest friends? (If one friend is identified, could ask more about that relationship, such as how much time they spend together, how serious they are about each other, if the relationship is going the way the teenager hoped.)
Might ask about dating and sexual issues, such as the teenager’s views on sexuality education, “going steady,” “living together,” or premarital sex.
COPING-STRESS TOLERANCE PATTERN
(Answer questions that apply to your child’s age-group.)
What does your child do when tired or upset?
If your child has temper tantrums, what causes them and how do you handle them?
Whom does your child talk to when worried about something?
How does your child usually handle problems or disappointments?
Have there been any big changes or problems in your family recently? If so, how have you handled them?
Has your child ever had a problem with drugs or alcohol or tried to commit suicide?
Do you think your child is “accident prone”? If so, explain.
What is your religion?
How is religion or faith important in your child’s life?
What religious practices would you like continued in the hospital (e.g., prayers before meals or bedtime; visit by minister, priest, or rabbi; prayer group)?
*The focus of the admission history is the child’s psychosocial environment. Most of the questions are worded in terms of parental responses. Depending on the child’s age, they should be addressed directly to the child when appropriate.
The nurse should also inquire about the use of any medications at home, including complementary medicine practices (Box 21-6). In a study of children with cancer, 42% had used alternative or complementary therapies simultaneously with or after conventional treatments (Fernandez, Pyesmany, and Stutzer, 1999). It is important that the use of any herbal or complementary therapy be noted in a preoperative assessment because of possible anesthesia or surgical complications related to herbal products (Flanagan, 2001) (see Critical Thinking Exercise).
After collecting the admission data, the nurse must apply the information to the nursing process and communicate it to other staff. Information gathered in the nursing admission assessment can offer insight into family dynamics, assist in normalization of the hospital environment, and aid staff members in meeting the child’s and family’s needs. Asking questions and seeking information directly from the child in an age-appropriate manner can yield a wealth of information regarding understanding of their illness and hospitalization.
Besides completing the nursing admission history, nurses should also perform a physical assessment (see Chapter 6) before planning care. At the very least, the nurse’s physical assessment of the child should include observation of the body for any bruises, rashes, signs of neglect, deformities, or physical limitations. The nurse should also listen to the heart and lungs to assess overall physical status. For example, it is impossible to evaluate improvement in respiratory function in a child admitted with pulmonary disease unless there are baseline data with which to compare subsequent findings.
Preparing Child for Admission
The preparation that children require on the day of admission depends on the kind of prehospital counseling they have received. If they have been prepared in a formalized program, they will usually know what to expect in terms of initial medical procedures, inpatient facilities, and nursing staff. However, prehospital counseling does not preclude the need for support during procedures such as obtaining blood specimens, x-ray tests, or physical examination. For example, undressing young children before they feel comfortable in their new surroundings can be upsetting. Causing needless anxiety and fear during admission may adversely affect the nurse’s establishment of trust with these children. Therefore nursing assistance during the admission procedure is vital, regardless of how well prepared any child is for the experience of hospitalization. In addition, spending this time with the child gives the nurse an opportunity to evaluate the child’s understanding of subsequent procedures (Fig. 21-4). Ideally, a primary nurse is assigned whenever possible to allow for individualized care and to provide a substitute support person for the child.

FIG. 21-4 The initial admission procedures give the nurse an opportunity to get to know the child and to assess the child’s understanding of the hospital experience.
Complementary and Alternative Medicine
Maria, a 10-year-old Hispanic girl, has had severe nosebleeds. She is admitted to the hospital for a complete workup in an attempt to determine the cause. Her parents and grandparents have gathered around her bed. When you enter her room to begin admitting procedures, you notice an unusual scent. Maria’s mother is rubbing the contents from an unfamiliar bottle of liquid on Maria. Meanwhile, the grandmother is rubbing Maria’s head. She is startled at your entry and drops something on the floor near your feet. You bend over to pick it up and discover that it is a penny.
1. Evidence—Is there sufficient evidence to draw any conclusions?
2. Assumptions—What are some underlying assumptions that may be drawn from the data about the following:
a. Complementary or alternative medical remedies
b. The role of ethnic or folk remedies in modern health care practice
c. The nurse’s role in cases where alternative medicine is practiced (vs traditional medicine)
3. What implications and priorities for nursing care can be drawn at this time?
4. Does the evidence objectively support your argument (conclusion)?
5. Are there alternative perspectives to your arguments? If so, what are they?
When a child is admitted, nurses follow several fairly universal admission procedures (Box 21-7). One particularly important decision is room assignment. The minimum considerations for room assignment are age, sex, and nature of the illness. No absolute rules govern room selection, but in general, placing children of the same age-group and with similar types of illness in the same room is both psychologically and medically advantageous. However, there are many exceptions. For example, a child in traction may be therapeutic for another child confined to bed because of a serious illness. A child who is independent despite physical disabilities may help another child with similar or different limitations, and the parents of the child with disabilities may achieve deeper insight and acceptance of their child’s disorder.
Age-grouping is especially important for adolescents. Many hospitals make an effort to place teenagers on their own unit or in a separate, designated section of the pediatric or general unit whenever possible.
NURSING INTERVENTIONS
Preventing or Minimizing Separation
A primary nursing goal is to prevent separation, particularly in children younger than 5 years of age. Changes in hospitals’ policies over recent years reflect a changed attitude toward parents; many hospitals no longer consider parents “visitors” and welcome their presence at all times throughout the child’s hospitalization. Many hospitals have developed a system of family-centered care. This philosophy of care recognizes the integral role of the family in a child’s life and acknowledges the family as an essential part of the child’s care and illness experience. The family is considered to be partners in the care of the child (Smith and Conant Rees, 2000) (see Chapter 1). Family-centered care also supports the family by establishing priorities based on the needs and values of the family unit (Lewandowski and Tesler, 2003).
At the very least, most hospitals welcome parents at any time. Many provide facilities such as a chair or bed for at least one person per child, unit kitchen privileges, and other amenities that create a welcoming atmosphere for parents. However, not all hospitals provide such amenities, and parents’ own schedules may prevent rooming-in (see Ethical Case Study). In such instances, strategies to minimize the effects of separation must be implemented.
Nurses must have an appreciation of the child’s separation behaviors. As discussed earlier, the phases of protest and despair are normal. The child is allowed to cry. Even if the child rejects strangers, the nurse provides support through physical presence. Presence is defined as spending time being physically close to the child while using a quiet tone of voice, appropriate choice of words, eye contact, and touch in ways that establish rapport and communicate empathy. If behaviors of detachment are evident, the nurse maintains the child’s contact with the parents by frequently talking about them; encouraging the child to remember them; and stressing the significance of their visits, telephone calls, or letters. The use of cellular phones can increase the contact between the hospitalized child and parents or other significant family members and friends. However, many cell phone signals are not compatible with medical equipment, and use may be restricted in certain areas within the hospital.
 ETHICAL CASE STUDY Maternal Absence During Infant Hospitalization
ETHICAL CASE STUDY Maternal Absence During Infant Hospitalization
Carrie is a 3-month-old infant who has been admitted to the hospital for bronchiolitis and respiratory syncytial virus (RSV). She also is diagnosed with failure to thrive. Carrie’s mother is 18 years of age and has a history of substance abuse. On arrival at the hospital, Carrie’s mother informs the nurse that she cannot stay with Carrie because she has to go to work. She leaves shortly after the nurse completes the admission history and has not returned to the hospital for 2 days. No other family members are listed in the chart, and no one has visited Carrie since her mother left.
The first priority is Carrie’s recovery from bronchiolitis and RSV. The hospital policies for supervision of a young infant without family presence should be followed. Social services should be involved, and an investigation of the mother should occur before Carrie’s discharge. A review of any past hospital or emergency department visits could be helpful in trying to locate a family member and obtain additional information on Carrie’s health.
Treat All Involved with Respect
It is difficult for nursing staff not to judge a mother who has left her young child in a hospital for 2 days without visiting. Nurses who realize the difficulties facing this mother with a history of substance abuse can provide support and serve as resources for helping the mother receive care and improve parenting skills.
Assumptions are easily made in this case because the mother is young and has a history of substance abuse. It is important for the nursing staff to remember to be objective during the investigation of the mother and to provide professional support for needed referrals for counseling and guidance.
Carrie’s situation warrants immediate action to begin plans for her care outside the hospital. If the mother cannot be found, social services must begin working with outside resources to place Carrie in a foster home. While investigation of Carrie’s mother continues, comfort and support for Carrie should be provided by child life specialists, volunteers, and the nursing staff.
There are a number of outcomes to consider that could positively affect Carrie’s well-being. One is that the mother would receive the appropriate counseling needed to cope with her problems without depending on substances or drugs that could affect her and her daughter. If the mother demonstrates the capacity to adequately care for Carrie at home, it would be best for the child to remain in the home setting with her mother. Carrie’s failure to thrive must be adequately addressed before such actions take place. The second scenario would entail Carrie recovering from the bronchiolitis and RSV and going into a temporary foster home while her mother receives appropriate assistance for substance abuse. Carrie needs a constant, stable primary caretaker and home environment to be able to grow and develop appropriately. The issue of her failure to thrive must be investigated to ensure that organic problems are not contributing factors. If the lack of an appropriate and consistent home environment is the cause of her failure to thrive, this must be addressed by the nursing staff and social services.
Separation may be equally difficult for parents, especially when they do not understand the behaviors of separation anxiety. To avoid the immediate protest, parents may sneak out or lie to the child about leaving. As a result, instead of learning that absence is associated with a guaranteed return, the child learns that absence means loss of parents. Helping parents recognize that separation behaviors are normal and expected can decrease the parents’ anxiety and may ease their fears about leaving their child. Explaining to parents how the child reacts after they leave may also be helpful. Many parents imagine that the child cries for hours after they leave, whereas in reality the child may cry for a few minutes but settle down when comforted by someone else.
Toddlers and preschoolers have a limited concept of time. Time is measured in associations, such as eating dinner “when Daddy comes home.” Therefore, when helping parents with children’s fears of separation, nurses need to suggest ways of explaining leaving and returning. For example, if parents must leave to go to work or to make meals for the other family members, they should tell the child the reason for leaving. They also need to convey the expected time of return in terms of anticipated events. For example, if the parents will return in the morning, they can say to the child, “We’ll see you after the sun comes up” or “We–ll come back when [a favorite program] is on television.”
The young child’s ability to tolerate parental absence is limited. Therefore parental visits should be frequent (e.g., visiting three times a day for short periods rather than once a day for an extended time). This may necessitate that each parent visit at different times to lessen the length of separation. When parents cannot visit, the presence of other significant people can be most comforting for the child (Fig. 21-5).

FIG. 21-5 When parents cannot visit, other significant persons can provide comfort to the hospitalized child.
If parents leave after the child is asleep, they still need to communicate their absence. The parents of a 5-year-old boy solved this problem by devising a sign; on one side they drew a picture of a telephone, and on the other they drew a hamburger. Before they left, they turned the sign to the appropriate side to tell the child when he awoke that they were out using the telephone or eating.
Older children who know how to tell time may find it helpful to have a clock or watch. However, these children have the same need for honesty from their parents regarding visiting schedules. Because their peer groups are important, adolescents often appreciate planning visiting hours with their parents to ensure that the patient has some private time for friends.
Familiar surroundings also increase the child’s adjustment to separation. If parents cannot stay with the child, they should leave favorite articles from home with the child, such as a blanket, toy, bottle, feeding utensil, or article of clothing. Because young children associate such inanimate objects with significant people, they gain comfort and reassurance from these possessions. They make the association that if the parents left this, the parents will surely return. Placing an identification band on the toy lessens the chances of its being misplaced and provides a symbol that the toy is experiencing the same needs as the child. Other mementos of home include photographs and audiotape or videocassette recordings of family members reading a story, singing a song, saying prayers before bedtime, relating events at home, or taking a “talking walk” through the home. The tapes can be played at lonely times, such as on awakening or before sleeping. Some units allow pets to visit, which can have therapeutic benefits for a child. Animals should be carefully screened for medical or behavioral problems, and patients should be screened for allergies.
Older children also appreciate familiar articles from home, particularly photographs, a radio, a favorite toy or game, and their own pajamas. Often the importance of treasured objects to school-age children is overlooked or criticized. However, many school-age children have a special object to which they formed an attachment in early childhood. Therefore such treasured or transitional objects can help even older children feel more comfortable in a strange environment.
The strange sights, smells, and sounds in the hospital that are commonplace for the nurse can be frightening and confusing for children. It is important for the nurse to try to evaluate stimuli in the environment from the child’s point of view (considering also what the child may see or hear happening to other patients) and to make every effort to protect the child from frightening and unfamiliar sights, sounds, and equipment. The nurse should offer explanations or prepare the child for those experiences that are unavoidable. Combining familiar or comforting sights with the unfamiliar can relieve much of the harshness of medical equipment.
Helping children maintain their usual contacts also minimizes the effects of separation imposed by hospitalization. This includes continuing school lessons during the illness and confinement, visiting with friends either directly or through letter writing or telephone calls, and participating in stimulating projects whenever possible (Fig. 21-6). For extended hospitalizations, youngsters enjoy personalizing the hospital room to make it “home” by decorating the walls with posters and cards, rearranging the furniture (when possible), and displaying a collection or hobby.

Minimizing Loss of Control
Feelings of loss of control result from separation, physical restriction, changed routines, enforced dependency, and magical thinking. Although some of these cannot be prevented, most can be minimized through individualized planning of nursing care.
Promoting Freedom of Movement.: Younger children react most strenuously to any type of physical restriction or immobilization. Although temporary immobilization may be necessary for some interventions such as maintaining an intravenous line, most physical restriction can be prevented if the nurse gains the child’s cooperation.
For young children, particularly infants and toddlers, preserving parent-child contact is the best means of decreasing the need for or stress of restraint. For example, almost the entire physical examination can be done in a parent’s lap, with the parent hugging the child for procedures such as otoscopy. For painful procedures, the nurse should assess the parents’ preferences for assisting, observing, or waiting outside the room.
Environmental factors may also restrict movement. Keeping children in cribs or playpens may not represent immobilization in a concrete sense, but it certainly limits sensory stimulation. Increasing mobility by transporting children in carriages, wheelchairs, carts, or wagons provides them with a sense of freedom.
In some cases, physical restraint or isolation is necessary due to the child’s medical diagnosis. In these cases, the environment can be altered to increase sensory freedom (e.g., moving the bed toward the window; opening window shades; providing musical, visual, or tactile activities).
Maintaining Child’s Routine.: Altered daily schedules and loss of rituals are particularly stressful for toddlers and early preschoolers and may increase the stress of separation. The nursing admission history provides a baseline for planning care around the child’s usual home activities. A frequently neglected aspect of altered routines is the change in the child’s daily activities. A nonhospitalized child’s day, especially during the school years, is structured with specific times for eating, dressing, going to school, playing, and sleeping. However, this time structure vanishes when the child is hospitalized. Although nurses have a set schedule, the child is frequently unaware of it, and the new schedules that are imposed may be rigid. For example, some units have uniform nap times and bedtimes for all children, whereas others allow children to stay up late at night. Many children obtain significantly less sleep in the hospital than at home; the primary causes are delay in sleep onset and early termination of sleep because of hospital routines. Not only are hours of sleep disrupted, but waking hours are spent in passive activities. For example, few institutions impose any limits on the amount of time the child spends watching television. This may lead to the child being less “tired” at bedtime and delay the onset of sleep.
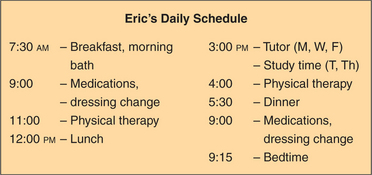
One technique that can minimize the disruption in the child’s routine is establishing a daily schedule. This approach is most suitable for the non–critically ill school-age or adolescent child who has mastered the concept of time. It involves scheduling the child’s day to include all those activities that are important to the child and nurse, such as treatment procedures, schoolwork, exercise, television, playroom, and hobbies. Together, the nurse, parent, and child then plan a daily schedule with times and activities written down (Fig. 21-7). This is left in the child’s room, and a clock or watch is available for the child’s use. Whenever possible, a calendar is also constructed with special events marked, such as favorite television programs, visits by friends or relatives, events in the playroom, and holidays or birthdays. If specific changes in treatment are expected (e.g., “beginning physical therapy in 2 days”), these are added.
Encouraging Independence.: The dependent role of the hospitalized patient imposes tremendous feelings of loss on older children. Principal interventions should focus on respect for individuality and the opportunity for decision making. Although these sound simple, their efficacy lies with nurses who are flexible and tolerant. It is also important for the nurse to empower the patient while not feeling threatened by a sense of lessened control.
Enabling children’s control involves helping them maintain independence and promoting the concept of self-care. Self-care refers to the practice of activities that individuals personally initiate and perform on their own behalf in maintaining life, health, and well-being (Orem, 2001). Although self-care is limited by the child’s age and physical condition, most children beyond infancy can perform some activities with little or no help. Whenever possible, these activities are encouraged in the hospital. Other approaches include jointly planning care, time structuring, wearing street clothes, making choices in food selections and bedtime, continuing school activities, and rooming with an appropriate age-mate.
Promoting Understanding.: Loss of control can occur from feelings of having too little influence on one’s destiny or from sensing overwhelming control or power over fate. Although preschoolers’ cognitive abilities predispose them most to magical thinking and delusions of power, all children are vulnerable to misinterpreting causes for stresses such as illness and hospitalization.
Most children feel more in control when they know what to expect, since the element of fear is reduced. Anticipatory preparation and provision of information help to lessen stress and increase understanding (see Preparation for Diagnostic and Therapeutic Procedures, Chapter 22).
Informing children of their rights while hospitalized fosters greater understanding and may relieve some of the feelings of powerlessness they typically experience. Hospitals providing services to children should have a hospital-wide policy on the rights and responsibilities of these patients and of their parents or guardians (The Joint Commission, 2004). An increasing number of hospitals and organizations have developed a patient “bill of rights” that is prominently displayed throughout the hospital or is presented to children and their families on admission (Box 21-8).
BOX 21-8 Bill of Rights for Children and Teens
In this hospital you and your family have the right to:
Care that supports you and your family
Information you can understand
From Association for the Care of Children’s Health: A pediatric bill of rights, Bethesda, Md, 1991, The Association. The Association
Preventing or Minimizing Fear of Bodily Injury
Beyond early infancy all children fear bodily injury from mutilation, bodily intrusion, body-image change, disability, or death. In general, preparation of children for painful procedures decreases their fears and increases cooperation. Manipulating procedural techniques for children in each age-group also minimizes fear of bodily injury. For example, because toddlers and young preschoolers are traumatized by insertion of a rectal thermometer, axillary temperatures or temperatures taken with electronic or tympanic membrane devices can effectively be substituted. Whenever procedures are performed on young children, the most supportive intervention is to do the procedure as quickly as possible while maintaining parent-child contact.
Because of toddler and preschool children’s poorly defined body boundaries, the use of bandages may be particularly helpful. For example, telling children that the bleeding will stop after the needle is removed does little to relieve their fears, whereas applying a small Band-Aid usually reassures them. The size of bandages is also significant to children in this age-group; the larger the bandage, the more importance is attached to the wound. Watching their surgical dressings become successively smaller is one way young children can measure healing and improvement. Prematurely removing a dressing may cause these children considerable concern for their well-being. Specific pain management strategies are discussed in Chapter 7.
For children who fear mutilation of body parts, it is essential that the nurse repeatedly stress the reason for a procedure and evaluate the child’s understanding. For example, explaining cast removal to preschoolers may seem simple enough, but children’s comprehension of the details may vary considerably from the explanation. Asking them to draw a picture of what they think will happen presents substantial evidence of how they perceive events.
Children may fear bodily injury from a great variety of sources. Imaging machines, strange equipment used for examination, unfamiliar rooms, or awkward positions can be perceived as potentially hazardous. In addition, thoughts and actions can be imagined sources of bodily damage. Therefore it is important to investigate imagined reasons, particularly of a sexual nature, for illness. Because children may fear revealing such thoughts, using techniques such as drawing or doll play may elicit previously undisclosed misconceptions.
Older children fear bodily injury of both internal and external origins. For example, school-age children are aware of the significance of the heart and may fear the actual operation as much as the pain, the stitches, and the possible scar. Adolescents may express concern about the actual procedure but be much more anxious over the resulting scar.
Children can grasp information only if it is presented on or close to their level of cognitive development. This necessitates an awareness of the words used to describe events or processes. For example, young children told that they are going to have a CAT (i.e., CT, computed tomography) scan may wonder, “Will there be cats? Or something that scratches?” It is clearer to describe the procedure in simple terms and explain what the letters of the common name stand for. Therefore, to prevent or alleviate fears, nurses must be keenly aware of the medical terminology and vocabulary that they use every day.
When children are upset about their illness, their perception can be changed by (1) providing a somewhat different and less negative account of the disease or (2) offering an explanation that is characteristic of the next stage of cognitive development. An example of the first strategy is reassuring a preschooler who fears that after a tonsillectomy, another sore throat means a second operation. Explaining that after tonsils are “fixed” they do not need fixing again can help relieve the fear. An example of the latter strategy is to explain that germs made the tonsils sick and even though germs can cause another sore throat, they cannot cause the tonsils to ever be sick again. This higher-level explanation is based on the school-age child’s concept of germs as a cause of disease.
Providing Developmentally Appropriate Activities
A primary goal of nursing care for the child who is hospitalized is to minimize threats to the child’s development. Many strategies (e.g., minimizing separation) have been discussed and may be all that the short-term patient requires. However, children who experience prolonged or repeated hospitalization are at greater risk for developmental delays or regression. The nurse who provides opportunities for the child to participate in developmentally appropriate activities further normalizes the child’s environment and helps reduce interference with the child’s ongoing development (see Normalization, Chapter 18).
Interference with normal development may have long-term implications for the developing infant and toddler. The nurse plays a primary role in identifying children at risk and helping to plan, implement, and evaluate developmental intervention (see Chapters 10 and 12).
School is an integral part of the school-age child’s and adolescent’s development. Accreditation standards for hospitals serving children consider access to appropriate educational services a key factor in the accreditation decision process when a child’s treatment requires a significant absence from school (The Joint Commission, 2004). The nurse can encourage children to resume schoolwork as quickly as their condition permits, help them schedule and protect a selected time for studies, and help the family coordinate hospital educational services with their children’s schools. Children should have the opportunity to continue art and music classes, as well as their academic subjects.
To meet the unique developmental needs of adolescents, special units may be developed that provide privacy, increased socialization, and appropriate activities for these young people. Typically these units can be set apart from the general pediatric facility so that the teenagers do not share space with younger children, who are often perceived as a threat to their maturity.
In caring for the adolescent patient, it is essential to provide flexible routines and activities, such as more group activity, wearing of street clothes, and access to the items so critical to adolescents—telephones, compact disc players, DVD players, videocassette recorders, computers, e-mail, video games, and televisions. Because adolescents’ food habits are rarely limited to the three traditional meals a day, a ready supply of snacks should be available. However, the most important benefit of these units is increased socialization with peers. In addition, staff members usually enjoy working with this age-group and are able to establish the trust so essential for communication.
Although regression is expected and normal for all age-groups, nurses have the responsibility for fostering the child’s growth and development. Hospitalization can become a significant opportunity for learning and advancing. Extended hospitalizations for long-term chronic illness or situations of failure to thrive, abuse, or neglect represent instances in which regression must be seen as an adjustment period, to be followed by plans for promoting appropriate developmental skills.
Providing Opportunities for Play and Expressive Activities
Play is one of the most important aspects of a child’s life and one of the most effective tools for managing stress. Because illness and hospitalization constitute crises in a child’s life and often involve overwhelming stresses, children need to act out their fears and anxieties as a means of coping with these stresses. Play is essential to children’s mental, emotional, and social well-being. As with their other developmental needs, play does not stop when children are ill or in the hospital. On the contrary, play in the hospital serves many functions (Box 21-9). Of all hospital facilities, no room probably alleviates the stressors of hospitalization more than the playroom (or activity room). In the playroom, children temporarily distance themselves from their illness, hospitalization, and the associated stressors. This room should be a safe haven for children, free from medical or nursing procedures (including medication administration), strange faces, and probing questions. The playroom then becomes a sanctuary in an otherwise frightening environment.
BOX 21-9 Functions of Play in the Hospital
Provides diversion and brings about relaxation
Helps the child feel more secure in a strange environment
Lessens the stress of separation and the feeling of homesickness
Provides a means for release of tension and expression of feelings
Encourages interaction and development of positive attitudes toward others
Provides an expressive outlet for creative ideas and interests
Provides a means for accomplishing therapeutic goals (see Use of Play in Procedures, Chapter 22)
Places child in active role and provides opportunity to make choices and be in control
Engaging in play activities gives children a sense of control. In the hospital environment, most decisions are made for the child; play and other expressive activities offer the child much-needed opportunities to make choices for themselves. Even if a child chooses not to participate in a particular activity, the nurse has offered the child a choice, perhaps one of only a few real choices the child has had that day.
The hospitalized child typically has lower energy levels than healthy children of the same age. Therefore children may not appear engaged and enthusiastic about an activity, even though they are enjoying the experience. Activities may need to be adjusted or limited based on the child’s age, endurance, and any special needs.
Diversional Activities.: Almost any form of play can be used for diversion and recreation, but the activity should be selected on the basis of the child’s age, interests, and limitations (Fig. 21-8). Children do not necessarily need special direction for using play materials. All they require is the raw materials with which to work and adult approval and supervision to help keep their natural enthusiasm or expression of feelings from getting out of control. Small children enjoy a variety of small, colorful toys that they can play with in bed or in their room, or more elaborate play equipment, such as playhouses, sandboxes, rhythm instruments, or large boxes and blocks, that may be a part of the hospital playroom.

FIG. 21-8 Play materials for children in the hospital need to be appropriate for their age, interests, and limitations.
Games that can be played alone or with another child or an adult are popular with older children, as are puzzles; reading material; quiet, individual activities, such as sewing, stringing beads, and weaving; and Lego blocks and other building materials. Assembling models is an excellent pastime, but one should make certain that all pieces and necessary materials are included in the package so that the child is not disappointed and frustrated.
Well-selected books are of infinite value to the child. Children never tire of stories; having someone read aloud gives them endless hours of pleasure and is of special value to the child who has limited energy to expend in play. A radio, DVD player, electronic games, and television, included among most hospital room equipment, are useful tools for entertaining a child. Computers with access to the Internet can provide diversion, educational opportunities, and online support groups.
When supervising play for ill or convalescent children, it is best to select activities that are simpler than would normally be chosen for the child’s specific developmental level. These children usually do not have the energy to cope with more challenging activities. Other limitations also influence the type of activities. Special consideration must be given to the child who is confined in terms of movement, has a restricted extremity, or is isolated. Toys for isolated children must be disposable or need to be disinfected after every use. Therefore toys that are not able to be disinfected (e.g., stuffed animals) cannot be used as community toys.
Toys.: Parents of hospitalized children often ask nurses about the types of toys that would be best to bring for their child. Although parents often want to buy new toys for the hospitalized child to offer cheer and comfort, it is often better to wait to bring new things, especially in the case of younger children. Small children need the comfort and reassurance of familiar things, such as the stuffed animal the child hugs for comfort and takes to bed at night. These familiar items are a link with home and the world outside the hospital. All toys brought into the hospital should be assessed for safety.
Large numbers of toys often confuse and frustrate a small child. A few small, well-chosen toys are usually preferred to one large, expensive one. Children who are hospitalized for an extended time benefit from changes. Rather than a confusing accumulation of toys, older toys should be replaced periodically as interest wanes.
A highly successful diversion for a child who is hospitalized for a length of time and whose parents are unable to visit frequently is having the parents bring a box with several small, inexpensive, brightly wrapped items with a different day of the week printed on the outside of each package. The child will eagerly anticipate the time for opening each one. If the parents know when their next visit will be, they can provide the number of packages that corresponds to the time between visits. In this way the child knows that the diminishing packages also represent the anticipated visit from the parent.
Expressive Activities.: Play and other expressive activities provide one of the best opportunities for encouraging emotional expression, including the safe release of anger and hostility. Nondirective play that allows children freedom for expression can be tremendously therapeutic. Therapeutic play, however, should not be confused with play therapy, a psychologic technique reserved for use by trained and qualified therapists as an interpretative method with emotionally disturbed children. Therapeutic play, on the other hand, is an effective, nondirective modality for helping children deal with their concerns and fears, and at the same time it often helps the nurse gain insights into children’s needs and feelings.
Tension release can be facilitated through almost any activity; with younger ambulatory children, large-muscle activity such as use of tricycles and wagons is especially beneficial. Much aggression can be safely directed into pounding and throwing games or activities. Beanbags are often thrown at a target or open receptacle with surprising vigor and hostility. A pounding board is employed with enthusiasm by young children; clay and Play-Doh are beneficial for use at any age.
Creative Expression.: Although all children derive physical, social, emotional, and cognitive benefits from engaging in art or other creative activities, children’s need for such activities is intensified when they are hospitalized. Drawing and painting are excellent media for expression. Children are more at ease expressing their thoughts and feelings through art, since humans think first in images and later learn to translate these images into words. The child needs only to be supplied with the raw materials, such as crayons and paper; large brushes and an ample supply of newsprint supported on easels; or materials for finger painting (Fig. 21-9). Children can work individually or work together on a group project, such as a mural painted on a long piece of paper.
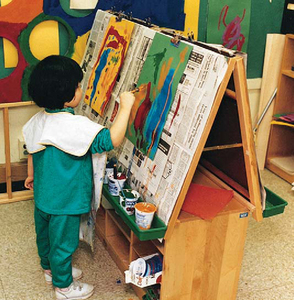
Although interpretation of children’s drawings requires special training, observing changes in a series of the child’s drawings over time can be helpful in assessing psychosocial adjustment and coping. The nurse can use children’s drawings, stories, poetry, and other products of creative expression as a springboard for discussion of thoughts, fears, and understanding of concepts or events (see Communication Techniques, Chapter 6). A child’s drawing before surgery, for example, may reveal unvoiced concerns about mutilation, body changes, and loss of self-control.
Nurses can incorporate opportunities for musical expression into routine nursing care. For example, simple musicalinstruments, such as bracelets with bells, can be placed on infants’ legs for them to shake to accompany mealtime music or dressing changes. Dance and movement suggestions may encourage a child to ambulate.
Holidays provide stimulus and direction for unlimited creative projects. Children can participate in decorating the pediatric unit; making pictures and decorations for their rooms gives the children a sense of pride and accomplishment. This is especially beneficial for children who are immobilized and isolated. Making gifts for someone at home helps to maintain interpersonal ties.
Dramatic Play.: Dramatic play is a well-recognized technique for emotional release, allowing children to reenact frightening or puzzling hospital experiences. Through use of puppets, replicas of hospital equipment, or some actual hospital equipment, children can act out the situations that are a part of their hospital experience. Dramatic play enables children to learn about procedures and events that concern them and to assume the roles of the adults in the hospital environment.
Puppets are universally effective for communicating with children. Most children see them as peers and readily communicate with them. Children will tell the puppet feelings that they hesitate to express to adults. Puppets can share children’s own experiences and help them to find solutions to their problems. Puppets dressed to represent figures in the child’s environment—for example, a physician, nurse, child patient, therapist, and members of the child’s own family—are especially useful. Small, appropriately attired dolls are equally effective in encouraging the child to play out situations, although puppets are usually best for direct conversation.
Play must consider medical needs, but at times a procedure can be postponed briefly to allow the child to complete a special activity (see Critical Thinking Exercise). Play must consider any limitations imposed by the child’s condition. For example, small children may eat paste and other creative media; therefore a child who is allergic to wheat should not be given finger paint made from wallpaper paste or modeling dough made with flour. A child on a restricted salt intake should not play with modeling dough because salt is one of its major constituents. At home the play program can be planned around the therapy regimen. However, play can be satisfactorily incorporated into the child’s care if the nurse and others involved allow some flexibility and use creativity in planning for play.
Maximizing Potential Benefits of Hospitalization
Although hospitalization generally represents a stressful time for children and families, it also represents an opportunity for facilitating positive change within the child and among family members. For some families the stress of a child’s illness, hospitalization, or both can lead to strengthening of family coping behaviors and the emergence of new coping strategies.
Playroom and Hospital Procedures
Hannah, a 7-year-old with cystic fibrosis, has been hospitalized numerous times with complications from the condition. She is playing Candyland with her brother, sister, and several other children in the playroom on the pediatric unit. A pediatric phlebotomist enters the playroom and says, “Hannah, I need to take some blood. I can see that you are playing a game, so I–ll just do it while you play. It will just take a minute.” Hannah nods her head indicating that she agrees to let the phlebotomist draw the blood at this time. The playroom is usually off-limits for invasive procedures. As Hannah’s nurse, you are aware that Dr. Lung wants the results of the laboratory studies as soon as possible to make a decision about her course of therapy.
1. Evidence—Is there sufficient evidence to draw any conclusions about this situation at this time?
2. Assumptions—What are some underlying assumptions about the following:
a. Children and painful procedures such as venipunctures
b. The function of play in a hospitalized child
3. What implications and priorities for nursing care can be drawn at this time (i.e., what will you do)?
4. Does the evidence objectively support your argument (conclusion)?
5. Are there alternative perspectives to your conclusions? If so, what are they?
Fostering Parent-Child Relationships.: The crisis of illness or hospitalization can mobilize parents into more acute awareness of their child’s needs. For example, hospitalization provides opportunities for parents to learn more about their children’s growth and development. When parents are helped to understand children’s usual reactions to stress, such as regression or aggression, they are not only better able to support the child through the hospital experience, but also may extend their insights into childrearing practices after discharge.
Difficulties in parent-child relationships that existed before hospitalization that are characterized by feeding problems, negative behavior, and sleep disturbances may decrease during hospitalization. The temporary cessation of such problems sometimes alerts parents to the role they may be playing in propagating the negative behavior. With assistance from health professionals, parents can restructure ways of relating to their children to foster more positive behavior.
Hospitalization may also represent a temporary reprieve or refuge from a disturbed home. Typically, abused or neglected children’s dramatic physical and social improvement during hospitalization is proof of the benefits and potential growth that can occur during hospitalization. These children temporarily are able to seek support, reassurance, and security from new relationships, particularly with nurses and hospitalized peers.
Providing Educational Opportunities.: Illness and hospitalization represent excellent opportunities for children and other family members to learn more about their bodies, each other, and the health professions. For example, during a hospital admission for a diabetic crisis, the child may learn about the disease; the parents may learn about the child’s needs for independence, normalcy, and appropriate limits; and each of them may find a new support system in the hospital staff.
Illness or hospitalization can also help older children in choosing a career. Frequently, children have impressions of physicians or nurses that are disproportionately positive or negative. Actual experience with different health professionals can influence their attitude about health professionals and even a decision regarding a career in healthcare.
Promoting Self-Mastery.: The experience of facing a crisis such as illness or hospitalization, coping successfully with it, and maturing as a result of it constitutes an opportunity for self-mastery. Younger children have the chance to test fantasy vs reality fears. They realize that they were not abandoned, mutilated, or punished. In fact, they were loved, cared for, and treated with respect for their individual concerns. It is not unusual for children who have undergone hospitalization or surgery to tell others that “it was nothing” or to display proudly their scars or bandages. For older children, hospitalization may represent an opportunity for decision making, independence, and self-reliance. They are proud of having survived the experience and may feel a genuine self-respect for their achievements. Nurses can facilitate such feelings of self-mastery by emphasizing aspects of personal competence in the child and not focusing on uncooperative or negative behavior.
Providing Socialization.: Hospitalization may offer children a special opportunity for social acceptance. Lonely, asocial, and even delinquent children find a sympathetic environment in the hospital. Children who have a physical handicap or are in some other way “different” from their age-mates may find an accepting social peer group (Fig. 21-10). Although this does not always spontaneously occur, nurses can structure the environment to foster a supportive child group. For example, selection of a compatible roommate can help children gain a new friend and learn more about themselves. Forming relationships with significant members of the health care team, such as the physician, nurse, child life specialist, or social worker, can greatly enhance children’s adjustment in many areas of life.

FIG. 21-10 Placing children of the same age-group with similar illnesses near each other on the unit is both psychologically and medically supportive. (Courtesy E. Jacob, Texas Children’s Hospital, Houston.)
Parents may also encounter a new social group in other parents who have similar problems. The waiting room or hallway “self-help” groups are inherent to every institution. Parents meet while in the hospital or clinic and discuss their children’s illnesses and treatments. Nurses can capitalize on this informal gathering by encouraging parents to discuss collectively their concerns and feelings. Nurses can also refer parents to organized parent groups or can use the help and support of parents of recovered hospitalized patients. It is important that nurses emphasize to families that each child responds differently to disease, treatments, and care. Any questions raised during group discussions should be clarified with a nurse or physician.
NURSING CARE OF THE FAMILY
Although it is not possible to predict exactly which factors are most likely to have an effect on the family’s reactions, important variables are (1) the seriousness of the child’s illness, (2) the family’s previous experience with hospitalization, and (3) the medical procedures involved in the diagnosis and treatment. Important information is also obtained in the nursing admission history (see Box 21-5).
SUPPORTING FAMILY MEMBERS
Support involves the willingness to stay and listen to parents’ verbal and nonverbal messages. Sometimes the nurse does not give this support directly. For example, the nurse may offer to stay with the child to allow the parents time alone or may discuss with other family members the parents’ need for extra relief. Often relatives and friends want to help but do not know how. Suggesting ways, such as baby-sitting, preparing meals, doing laundry, or transporting the siblings to school, can prompt others to help reduce the responsibilities that burden parents. An ongoing parent support group held on the pediatric unit during the children’s traditional nap time has also proved effective in helping parents share emotions and concerns related to hospitalization (Bracht, Ardal, Bot, and others, 1998).
Support may also be provided through the clergy. Parents with deep religious beliefs may appreciate the counsel of a clergy member, but because of their stress they may not have sufficient energy to initiate the contact. Nurses can be supportive by arranging for clergy to visit, upholding parents’ religious beliefs, and respecting the individual meaning and significance of those beliefs (Feudtner, Haney, and Dimmers, 2003).
Support involves accepting cultural, socioeconomic, and ethnic values. For example, health and illness are defined differently by various ethnic groups. For some, a disorder that has few outward manifestations of illness, such as diabetes,hypertension, or cardiac problems, is not a sickness. Consequently, following a prescribed treatment may be seen as unnecessary. Nurses who appreciate the influences of culture are more likely to intervene therapeutically. (See also Cultural and Religious Influences on Healthcare, Chapter 4.)
 FAMILY-CENTERED CARE
FAMILY-CENTERED CARESupporting Siblings During Hospitalization
Trade off staying at the hospital with spouse or have a surrogate who knows the siblings well stay in the home.
Offer information about the child’s condition to young siblings as well as older siblings; respect the sibling who avoids information as a means of coping with the situation.
Arrange for children to visit their brother or sister in the hospital if possible.
Encourage phone visits and mail between brothers and sisters; provide children with phone numbers, writing supplies, and stamps.
Help each sibling identify an extended family member or friend to be their support person and provide extra attention during parental absence.
Make or buy inexpensive toys or trinkets for siblings, one gift for each day the child will be hospitalized.
Wrap each gift separately and place in a basket, box, or other container at each child’s bedside.
Instruct siblings to open one gift each night at bedtime and to remember that he or she is in the parent’s thoughts.
If the child’s condition is stable and distance is not prohibitive, plan a special time at home with the siblings or have spouse or another relative or friend bring the children to meet parent(s) at a restaurant or other location near the hospital.
Modified from Craft M, Craft J: Perceived changes in siblings of hospitalized children: a comparison of sibling and parent reports, Child Health Care 18(1):42-48, 1989; Rollins J: Brothers and sisters: a discussion guide for families, Landover, Md, 1992, Epilepsy Foundation of America.
Parents need help in accepting their own feelings toward the ill child. If given the opportunity, parents often disclose their feelings of loss of control, anger, and guilt. They often resist admitting to such feelings because they expect others to disapprove of behavior that is less than perfect. Unfortunately, health personnel, including nurses, sometimes do exercise little tolerance for deviation from the norm. This only increases the psychologic impact of a child’s illness on family members. Helping parents identify the specific reason for such feelings and emphasizing that each is a normal, expected, and healthy response to stress may reduce the parents’ emotional burden.
Family-centered care also addresses the needs of siblings. Support may involve preparing siblings for hospital visits, assessing their adjustment, and providing appropriate interventions or referrals when needed. The Family-Centered Care box suggests ways that parents can support siblings during hospitalization.
PROVIDING INFORMATION
One of the most important nursing interventions is providing information about (1) the disease, its treatment, prognosis, and home care; (2) the child’s emotional and physical reactions to illness and hospitalization; and (3) the probable emotional reactions of family members to the crisis.
For many families the child’s illness is the first contact they have with the hospital experience. Often parents are not prepared for the child’s behavioral reactions to hospitalization, such as separation behaviors, regression, aggression, and hostility. Providing the parents with information about these normal and expected behavioral responses can lessen the parents’ anxiety during the hospital admission. The family is equally unfamiliar with hospital rules, which often compounds their confusion and anxiety. Therefore the family needs clear explanations about what to expect and what is expected of them.
Parents also need to be aware of the effects of illness on the family and strategies that prevent negative changes. Specifically, parents should keep the family well informed and communicate with everyone as much as possible. They should treat all the children equally and as normally as before the illness occurred. Discipline, which initially may be lessened for the ill child, should be continued to provide a measure of security and predictability. When ill children know that their parents expect certain standards of conduct from them, they feel certain that they will recover. Conversely, when all limits are removed, they fear that something catastrophic will happen.
Helping parents understand the meaning of posthospitalization behaviors in the sick child is necessary for them to tolerate and support such behaviors. In addition, parents should be forewarned of the common reactions following discharge (see Box 21-2). Parents who do not expect such reactions may misinterpret them as evidence of the child’s “being spoiled” and demand perfect behavior at a time when the child is still reacting to the stress of illness and hospitalization. If the behaviors, especially the demand for attention, are dealt with in a supportive manner, most children are able to relinquish them and assume precrisis levels of functioning.
Nurses should also prepare parents for the reactions of siblings—particularly anger, jealousy, and resentment. Older siblings may deny such reactions because they provoke feelings of guilt. However, everyone needs outlets for emotions, and the repressed feelings may surface as problems in school or with age-mates, as psychosomatic illnesses, or in delinquent behavior.
Probably one of the most neglected areas of communication involves giving information to siblings. Frequently, age becomes the only factor that leads to an awareness of this problem, since older children may begin to ask questions or request explanations. Even in this situation, however, the information may be seriously inadequate. Children in every age-group deserve some explanation of the sibling’s illness or hospitalization. Although the exact wording may differ, the explanation should focus on the following concerns: (1) “Will I get sick and have to go to the hospital?” (2) “Did I cause the illness?” (for actual or imagined reasons), and (3) “Will my parents abandon me if my brother or sister doesn’t recover?” If parents or nurses address these three questions, the siblings’ own fears of illness, guilt, and abandonment are minimized (Melnyk and Alpert-Gillis, 1998).
ENCOURAGING PARENT PARTICIPATION
Preventing or minimizing separation is a key nursing goal with the child who is hospitalized, but maintaining parent-child contact is also beneficial for the family. One of the best approaches is encouraging parents to stay with their child and to participate in the care whenever possible. Although some health facilities provide special accommodations for parents, the concept of rooming in can be instituted anywhere. The first requirement is the staff’s positive attitude toward parents. A negative attitude toward parent participation can create barriers to collaborative working relationships.
When hospital staff genuinely appreciate the importance of continued parent-child attachment, they foster an environment that encourages parents to stay. When parents are included in the care planning and understand that they are a contributing factor to the child’s recovery, they are more inclined to remain with their child and have more emotional reserves to support themselves and the child through the crisis. An empowerment model of helping allows the nurse to focus on parents’ strengths and seek ways to promote growth and family functioning so that the parents become empowered in caring for their child.
Because the mother tends to be the usual family caregiver, she usually spends more time in the hospital than the father. However, not all mothers (or fathers) feel equally comfortable assuming responsibility for their child’s care. Some may be under such great emotional stress that they need a temporary reprieve from total participation in caregiving activities (see Ethical Case Study). Others may feel insecure in participating in specialized areas of care, such as bathing the child after surgery. On the other hand, some mothers may feel a great need to control their child’s care. This seems particularly true of young mothers, who have recently established their role as a parent; mothers of children too young to verbalize their needs; and ethnic minority mothers when the hospital setting is predominantly staffed by nonminority personnel. Individual assessment of each parent’s preferred involvement is necessary to prevent the effects of separation while supporting parents in their needs as well.
With lifestyles and gender roles changing, fathers may assume all or some of the usual “mothering” roles in the household. In this case it may be the father-child relationship that requires preservation. Fathers need to be included in the care plan and respected for their parental role. For some fathers the child’s hospitalization may represent an opportunity to alter their usual caregiving role and increase their involvement. In single-parent families the caregiver may not be a parent but an extended family member, such as a grandparent or aunt.
One of the potential problems with continuous parent involvement is neglect of the parent’s need for sleep, nutrition, and relaxation. Often the sleeping accommodations are limited to a chair, and sleep is disrupted by nursing procedures. Encouraging the parents to leave for brief periods, arranging for sleeping quarters on the unit but outside the child’s room, and planning a schedule of alternating visits with another family member can minimize the stresses for the parent.
All too often, nurses respond to parent participation by abandoning their patient responsibilities. Nurses need to restructure their roles to complement and augment the caregiving functions of parents. Even in units structured to provide care by parents, parents frequently feel anxiety in their caregiving responsibilities; those more involved in direct care may feel more anxiety than those less involved in direct care. Therefore 24-hour responsibility may be too much for some parents. Assistance and relief by nursing personnel should always be available to these families, and nurses may need to work diligently to establish the strong bond of trust some parents need to take advantage of these opportunities.
PREPARING FOR DISCHARGE AND HOME CARE
Most hospitalizations necessitate some type of discharge preparation. Often this involves education of the family for continued care and follow-up in the home. Depending on the diagnosis, this may be relatively simple or highly complex. Preparing the family for home care demands a high degree of competence in planning and implementing discharge instructions. This usually is best accomplished using an interdisciplinary team approach, which requires a shift from the multidisciplinary team approach used during an acute phase of a child’s illness (Hornick, 1996).
Nurses are often key individuals in initiating and carrying out the discharge process. They collaborate with others in the planning and implementation phases to ensure appropriate care after hospitalization. Throughout the hospitalization the nurse should be aware of the need for discharge planning and those assessment factors that affect the family’s ability to provide home care. A thorough assessment of the family and home environment should be performed to ensure that the family’s emotional and physical resources are sufficient to manage the tasks of home care. (For a discussion of family and home assessment strategies, see Chapter 6.) In addition to adequate family resources, an investigation of community services, including respite care, is needed to ensure that appropriate support agencies are available, such as emergency facilities, home health agencies, and equipment vendors. Financial resources are also a consideration. To coordinate the immense task of assessment and to plan implementation, a care coordinator or manager should be appointed early in the discharge process.
The preparation for hospital discharge and home care begins during the admission assessment. Short- and long-term goals are established to meet the child’s physical and psychosocial needs. For children with complex care needs, discharge planning focuses on obtaining appropriate equipment and healthcare personnel for the home. Discharge planning is also concerned with those treatments that parents or children are expected to continue at home. In planning appropriate teaching, nurses need to assess (1) the actual and perceived complexity of the skill, (2) the parents’ or child’s ability to learn the skill, and (3) the parents’ or child’s previous or present experience with such procedures.
The teaching plan incorporates levels of learning, such as observing, participating with assistance, and finally, acting without help or guidance. The skill is divided into discrete steps, and each step is taught to the family member until it is learned. Return demonstration of the skill is requested before new skills are introduced. A record of teaching and performance provides an efficient checklist for evaluation. All families need to receive detailed written instructions about home care, with telephone numbers for assistance, before they leave the hospital. Communication between the nurse performing discharge planning and home health care is essential for ensuring a smooth transition for the child and family.
After the family is competent in performing the skill, they are given responsibility for the care. When possible, the family should have a transition or trial period to assume care with minimal health care supervision. This may be arranged on the unit; during a home pass; or in a facility, such as a motel, near the hospital. Such transitions provide a safe practice period for the family, with assistance readily available when needed, and are especially valuable when the family lives far from the hospital.
In many instances parents need only simple instructions and understanding of follow-up care. However, the often overwhelming care assumed by some families, coupled with other stressors they may be experiencing, necessitates continued professional support after discharge. A follow-up home visit or telephone call gives the nurse an opportunity to individualize care and provide information in perhaps a less stressful learning environment than the hospital. Appropriate referrals and resources may include visiting nurse or home health agencies, private nurse services, the school system, a physical therapist, a mental health counselor, a social worker, and any number of community agencies. Sharing the important issues surrounding the child’s and family’s needs is essential. Referral summaries should be concise, specific, and factual. When numerous support services are required, periodic collaboration among the professionals involved and the family is an excellent strategy to ensure efficient usage and comprehensive delivery of services.
CARE OF THE CHILD AND FAMILY IN SPECIAL HOSPITAL SITUATIONS
In addition to a general pediatric unit, children may be admitted to special facilities such as an ambulatory or outpatient setting, an isolation room, or intensive care.
AMBULATORY OR OUTPATIENT SETTING
The ambulatory or outpatient setting provides needed medical services for the child while eliminating the necessity of overnight admission. Among the benefits of ambulatory care are (1) minimization of the stressors of hospitalization, especially separation from the family; (2) reduced chance of infection; and (3) cost savings. Admission to the ambulatory or outpatient hospital setting usually is for surgical or diagnostic procedures, such as insertion of tympanostomy tubes, hernia repair, adenoidectomy, tonsillectomy, cystoscopy, or bronchoscopy.
In the ambulatory or outpatient setting, adequate preparation is particularly challenging. Ideally, the child and parents hould receive preadmission preparation, including a tour of the facility and a review of the day’s events (Brewer and Lambert, 1997). Parents need information in advance to help prepare the child and themselves for surgery and enable them to care for the child at home after the procedure. Parents also appreciate suggestions for items to bring to the hospital, such as blankets or stuffed animals. When preadmission preparation is not possible, time should be allowed on the day of the procedure for children to become acquainted with their surroundings and for nurses to assess, plan, and implement appropriate teaching.
Waiting is usually inevitable in ambulatory settings. Families frequently report waiting to be the most stressful part of the experience. Providing a pager is one way to allow the family (and at times the child) to leave the area and then be paged to return when needed (Ashenberg, Lambert, Maier, and others, 1996).
Explicit discharge instructions are important after outpatient surgery (see Family-Centered Care box and Preparing for Discharge and Home Care, p. 678). Parents need guidelines on when to call their practitioner regarding a change in the child’s condition. A follow-up telephone call system allows for nurses to check on the child’s progress within 48 to 72 hours after discharge. It also provides an opportunity for the nurse to review discharge information and answer questions.
Help the family prepare for the transportation home by offering these suggestions:
Have a blanket and pillow in the car. (Always use the car safety restraint system.)
Take a basin or plastic bag in case of vomiting.
Use a cup with a cap and straw for the child to drink fluids (except in cases of orofacial surgery where a straw may be contraindicated).
Give any prescribed pain medication before leaving facility.
Provide parents verbal and written information regarding potential side effects of pain medication for which they should be vigilant after discharge.
Discharge from Ambulatory Settings
Before beginning, explain that all instructions will also be presented in writing for the family to refer to later.
Provide an overview of the typical trajectory (expected pattern) of recovery.
Discuss expected progression of the child’s activity level during the postdischarge period (e.g., “Mary will probably sleep for the rest of the day, feel kind of tired most of tomorrow, but be back to her usual activities the next day”).
Explain which activities the child is allowed and what is not permitted (e.g., bed rest, bathing).
Discuss dietary restrictions, being very specific and giving examples of “clear fluids” or what is meant by a “full liquid diet.”
Discuss nausea and vomiting, if applicable, explaining how much is “normal” and what to do if more occurs (e.g., “Juan may be sick to his stomach and vomit. This is normal. However, if he vomits more than three times, please call us at this number right away.”).
Discuss fever and appropriate comfort measures, explaining how much fever is considered “normal,” and specifically what to do if the child goes beyond the range.
Explain the amount, location, and kind of pain or discomfort the child may experience.
Give any prescribed medication before leaving the facility.
Send a pain scale home with the family.
Explain how much pain and discomfort is “normal” and what to do if the child surpasses that level or if pain management interventions are unsuccessful.
Discuss pain management, including dosage for pain medications and details on how to administer them.
Describe appropriate nonpharmacologic comfort measures, such as holding, rocking, or swaddling.
Provide information about each medication that the child will be taking at home.
Review the details, including dose and route.
Demonstrate how to administer medications, if necessary (e.g., how to take wrapping off suppositories, how to insert).
Discuss guidelines for requesting other medications.
Request that all prescriptions be filled and given to the family before discharge.
Make certain the family has all of the equipment and supplies (e.g., gauze and tape for dressing changes) they will need at home.
Discuss complications that may occur and the steps to take if they do.
Ensure that appropriate measures are in place for safe transport home.
Remind family to use a seat belt or car seat for the child.
Determine if there will be one person whose sole responsibility is helping ensure the child’s safety and comfort during transport.
Discuss measures the driver may need to take if this is impossible (e.g., be certain a basin is within the child’s reach should vomiting occur; take a route that permits slower traffic and has places along the roadside to stop if necessary).
Determine the availability of a blanket, pillow, and cup with a lid and straw for the child’s use in the car.
Provide emergency phone numbers for the family to call with any concerns.
Explain that the family will be contacted (give an approximate time) to follow up on the child but that they should not hesitate to call if concerns arise before then.
Ask the family and child, if appropriate, if they have any questions, and problem solve with family members to meet their unique needs.
ISOLATION
Admission to an isolation room increases all of the stressors typically associated with hospitalization. There is further separation from familiar persons; additional loss of control; and added environmental changes, such as sensory deprivation and the strange appearance of visitors. Orientation to time and place is affected. These stressors are compounded by children’s limited understanding of isolation. Preschool children have difficulty understanding the rationale for isolation because they cannot comprehend the cause-and-effect relationship between germs and illness. They are likely to view isolation as punishment. Older children understand the causality better but still require information to decrease fantasizing or misinterpretation.
When a child is placed in isolation, preparation is essential for the child to feel in control. With young children the best approach is a simple explanation, such as “You need to be in this room to help you get better. This is a special place to make all the germs go away. The germs made you sick, and you could not help that.”
All children, but especially younger ones, need preparation in terms of what they will see, hear, or feel in isolation. Therefore they are shown the mask, gloves, and gown and are encouraged to “dress up” in them. Playing with the strange apparel lessens the fear of seeing “ghostlike” people walk into the room. Before entering the room, nurses and other health personnel should introduce themselves and let the child see their face before donning a mask. In this way the child associates them with significant experiences and gains a sense of familiarity in an otherwise strange and lonely environment.
When the child’s condition improves, appropriate play activities are provided to minimize boredom, stimulate the senses, provide a real or perceived sense of movement, orient the child to time and place, provide social interaction, and reduce depersonalization. For example, the environment can be manipulated to increase sensory freedom by moving the bed toward the door or window. Opening window shades; providing musical, visual, or tactile toys; and increasing interpersonal contact can substitute mental mobility for the limitations of physical movement. Rather than dwelling on the negative aspects of isolation, the child can be encouraged to view this experience as challenging and positive. For example, the nurse can help the child look at isolation as a method of keeping others out and letting only special people in. Children often think of intriguing signs for their doors, such as “Enter at your own risk.” These signs also encourage people “on the outside” to talk with the child about the ominous greeting.
EMERGENCY ADMISSION
One of the most traumatic hospital experiences for the child and parents is an emergency admission. The sudden onset of an illness or the occurrence of an injury leaves little time for preparation and explanation. Sometimes the emergency admission is compounded by admission to an intensive care unit (ICU) or the need for immediate surgery. However, even in those instances requiring only outpatient treatment, the child is exposed to a strange, frightening environment and to experiences that may elicit fear or cause pain.
There is a wide discrepancy between what constitutes a medically defined emergency and a client-defined emergency. A growing concern is the use of major emergency departments for routine primary care health visits. To offset overcrowding in emergency departments, many facilities have minor emergency units or pediatric minor emergency units for after-hours health care. Telephone triage for minor illnesses for patients is also emerging as a health care delivery mode to differentiate illnesses such as a common cold from true life-threatening conditions that require immediate practitioner attention and intervention. Other factors contributing to the overuse of emergency departments (as opposed to the primary practitioner’s office) include the increasing number of uninsured persons and households where both parents work full time and cannot afford to take off during the daytime to take the sick child to a practitioner.
In pediatric populations most visits to an emergency department are for respiratory infections, with skin conditions, gastrointestinal disorders, and trauma such as poisoning accounting for the remainder of cases. The most common reason parents give for bringing the child to the emergency department is concern about the illness worsening. However, practitioners may not think that the progressive symptoms necessitate immediate or emergency care. One of the nurse’s primary goals is to assess the parents’ perception of the event and their reasons for considering it serious or life threatening.
Lengthy preparatory admission procedures are often inappropriate for emergency situations. In such instances, nurses must focus their nursing interventions on the essential components of admission counseling (Box 21-10) and complete the process as soon as the child’s condition has stabilized.
BOX 21-10 Guidelines for Special Hospital Admission*
Lengthy preparatory admission procedures are often impossible and inappropriate for emergency situations.
Focus assessment on airway, breathing, and circulation; weigh child whenever possible for calculation of drug dosages.
Unless an emergency is life threatening, children need to participate in their care to maintain a sense of control.
Focus on essential components of admission counseling, including:
Appropriate introduction to the family
Use of child’s name, not terms such as “honey” or “dear”
Determination of child’s age and some judgment about developmental age (If the child is of school age, asking about the grade level will offer some evidence of intellectual ability.)
Information about child’s general state of health, any problems that may interfere with medical treatment (e.g., allergies), and previous experience with hospital facilities
Information about the chief complaint from both the parents and the child
ADMISSION TO INTENSIVE CARE UNIT (ICU)
Prepare child and parents for elective ICU admission, such as for postoperative care after cardiac surgery.
Prepare child and parents for unanticipated ICU admission by focusing primarily on the sensory aspects of the experience and on usual family concerns (e.g., persons in charge of child’s care, schedule for visiting, area where family can stay).
Prepare parents regarding child’s appearance and behavior when they first visit child in ICU.
Accompany family to bedside to provide emotional support and answer questions.
Prepare siblings for their visit; plan length of time for sibling visitation; monitor siblings’ reactions during visit to prevent them from becoming overwhelmed.
Encourage parents to stay with their child:
If visiting hours are limited, allow flexibility in schedule to accommodate parental needs.
Give family members a written schedule of visiting times.
If visiting hours are liberal, be aware of family members’ needs and suggest periodic respites.
Prepare parents for expected role changes and identify ways for parents to participate in child’s care without overwhelming them with responsibilities:
Provide information about child’s condition in understandable language:
Seek clarification of understanding.
During bedside conferences, interpret information for family members and child or, if appropriate, conduct report outside room.
Prepare child for procedures, even if this involves explanation while procedure is performed.
Assess and manage pain; recognize that a child who cannot talk, such as an infant or child in a coma or on mechanical ventilation, can be in pain.
Establish a routine that maintains some similarity to daily events in child’s life whenever possible:
Organize care during normal waking hours.
Keep regular bedtime schedules, including quiet times when television or radio is lowered or turned off.
Provide uninterrupted sleep cycles (60 minutes for infant, 90 minutes for older child).
Close and open drapes and dim lights to allow for day/night.
Place curtain around bed for privacy.
Orient child to day and time; have clocks or calendars in easy view for older children.
Schedule a time when child is left undisturbed (e.g., during naps, visit with family, playtime, or favorite program).
*See also Box 21-7.
Unless an emergency is life threatening, children need to participate in their care to maintain a sense of control. Because emergency departments are frequently hectic, there is a tendency to rush through procedures to save time. However, the extra few minutes needed to allow children to participate may save many more minutes of useless resistance and uncooperativeness during subsequent procedures. Other supportive measures include ensuring privacy, accepting various emotional responses to fear or pain, preserving parent-child contact, explaining all events before or as they occur, and personally remaining calm. Pain management strategies are discussed in Chapter 7.
At times, because of the child’s physical condition, little or no preparatory counseling for emergency hospitalization can be done. In such situations the implementation of postvention, or counseling subsequent to the event, has therapeutic value. The process of postvention involves evaluating children’s thoughts regarding admission and related procedures. It is similar to precounseling techniques; however, instead of supplying information, the nurse listens to the explanations offered by the child. Projective techniques such as drawing, doll play, or storytelling are especially effective. The nurse then bases additional information on what has already been understood.
INTENSIVE CARE UNIT
Admission to an ICU can be traumatic for both the child and parents (Fig. 21-11). The nature and severity of the illness and the circumstances surrounding the admission are major factors, especially for parents. Parents experience significantly more stress when the admission is unexpected rather than expected. One study found that parental anxiety reached near panic levels initially (Huckabay and Tilem-Kessler, 1999). Stressors for the child and parent are described in Box 21-11. Although several studies have described what parents perceive as most stressful, the most effective strategy may be to simply ask parents what is stressful and implement interventions that will enhance their ability to cope (Board and Ryan-Wenger, 2003; Melnyk and Alpert-Gillis, 1998). Assessment should be repeated periodically to account for changes in perceptions over time.
BOX 21-11 Neonatal or Pediatric Intensive Care Unit Stressors for the Child and Family
Pain and discomfort (e.g., injections, intubation, suctioning, dressing changes, other invasive procedures)
Unfamiliar surroundings (e.g., crowding)
Equipment noise (e.g., monitors, telephone, suctioning, computer printout)
Human sounds (e.g., talking, laughing, crying, coughing, moaning, retching, walking)
Unfamiliar people (e.g., health care professionals, patients, visitors)
Unfamiliar and unpleasant smells (e.g., alcohol, adhesive remover, body odors)
Constant lights (disturb day/night rhythms)

FIG. 21-11 Parental presence during hospitalization provides emotional support for the child and increases the parent’s sense of empowerment in the caregiver role. (Courtesy E. Jacob, Texas Children’s Hospital, Houston.)
 FAMILY FOCUS
FAMILY FOCUSA teenage boy with a rare genetic disorder, having made steady progress after awakening from a coma, relapsed and seemed very depressed. When told that a musician was visiting the pediatric intensive care unit, he immediately perked up and asked to have his room lights turned on. He whispered endless song requests to the musician. Family members and staff were treated to some of his first smiles in days; his biggest came when the musician held his hand and guided it across the guitar strings while they sang “Born to Be Wild” together at the boy’s request. His dad was misty eyed as he thanked the musician for the visit.
A few weeks later the boy’s condition worsened and he again lapsed into a coma. There was nothing more to be done. His parents began the necessary preparations to take their son home to die.
We continued to visit our friend and his family, offering a song, a story, or a simple hello. I hold a vivid picture of our final visit. We stood around the boy’s bed with his parents singing together songs they remembered from their youth, from more carefree times. Song and laughter filled the boy’s room.
Perhaps the boy heard his parents’ laughter and knew then that they would be okay. He died a few days later on the morning he was to have been discharged.
Modified from Rollins J: Placed in our keeping, 1995, Unpublished.
The family’s emotional needs are paramount when a child is admitted to an ICU. Although the same interventions discussed earlier for the stressors of separation and loss of control apply here, additional interventions may also benefit the family and child (see Box 21-11 and Family Focus box). In a qualitative study of 19 parents of 10 children in an ICU, parents reported that they simply wanted nurses to nurture the child in the same way the family would (Harbaugh, Tomlinson, and Kirschbaum, 2004). Nurse behaviors that exemplified caring and affection were perceived as helpful in decreasing stress. Behaviors perceived as not helpful included separating the child from the parents and communicating poorly with parents. Therefore even critical care must be centered on the family. It is important that visiting hours be liberal and flexible enough to accommodate parental needs and involvement (Hazinski, 1999).
Critically ill children become the focus of the parents’ lives, and parents’ most pressing need is for information (Scott, 1998). They want to know if their child will live and, if so, whether the child will be the same as before. They need to know why various interventions are being done for the child, that the child is being treated for pain or is comfortable, and that the child may be able to hear them even though not awake. When parents first visit the child in the ICU, they need preparation regarding the child’s appearance. Ideally, the nurse should accompany the parents to the bedside to provide emotional support and answer any questions.
Despite the stresses normally associated with ICU admission, a special security develops from being carefully monitored and receiving individualized care. Therefore planning for transition to the regular unit is essential and should include:
Assignment of a primary nurse on the regular unit
Continued visits by the ICU staff to assess the child’s and parents’ adjustment and to act as a temporary liaison with the nursing staff
Explanation of the differences between the two units and the rationale for the change to less intense monitoring of the child’s physical condition
Selection of an appropriate room, such as one that is close to the nursing station, and a compatible roommate
Children are particularly vulnerable to the stressors of illness and hospitalization because stress represents a change from the usual state of health and routine and because they possess limited coping mechanisms.
The three phases of separation anxiety are protest, despair, and detachment.
Feelings of loss of control are caused by unfamiliar environmental stimuli, physical restriction, altered routine, and dependency.
Fear of bodily pain may be manifested in the following ways: infants–facial expressions, body movements; toddlers—intense emotional upset, physical resistance; preschoolers—aggression, verbal expression, dependency; school-age children–precise verbalization of pain, passive requests for support or help, procrastination technique; adolescents–self-control, limited movement.
Because of their separation from significant people, children who are hospitalized may lack the opportunity to form new attachments in the strange environment of the hospital and exhibit negative behaviors after discharge.
Nursing care of the child in the hospital is aimed at preventing or minimizing separation, decreasing loss of control, minimizing fear of bodily injury, using play or expressive activities to lessen stress, and maximizing the potential benefits of hospitalization.
The nurse can maximize potential benefits of hospitalization by fostering parent-child relations, providing educational opportunities, promoting self-mastery, and encouraging socialization.
Family reactions are influenced by the seriousness of the illness, experience with illness or hospitalization and diagnostic or therapeutic procedures, available support systems, personal ego strengths, coping abilities, presence of additional stressors, cultural and religious beliefs, and family communication patterns.
Fear of contracting illness, their younger age, a close relationship with the ill sibling, substitute child care, minimal explanation of the illness, and perceived changes in parenting all increase the deleterious effects of a brother’s or sister’s illness and hospitalization on siblings.
Nursing care of the family involves listening to parents’ verbal and nonverbal messages; providing clergy support; accepting cultural, socioeconomic, and ethnic values; giving information to families and siblings; and preparing for discharge and home care.
Admission to an outpatient setting, emergency department, isolation room, or ICU requires additional intervention strategies to meet the child’s and family’s needs.
 answers to CRITICAL THINKING EXERCISES
answers to CRITICAL THINKING EXERCISES
COMPLEMENTARY AND ALTERNATIVE MEDICINE
1. There is limited evidence to draw certain conclusions without obtaining more data from the parents. It would be appropriate to gather more information before jumping to any major conclusions at this time.
a. Complementary and alternative medicine (CAM) is more common in U.S. households than previously reported. Much of the concern surrounding complementary therapies, especially in children, is the lack of sufficient data regarding their effectiveness, benefit, and the potential harm that may occur as a result of such treatments. In some cases CAM therapies may counteract certain medications or the effects of prescribed therapies. It has become more common for practitioners in emergency medicine to encounter patients who are taking CAM therapy in addition to prescription medications or treatments for conditions such as eczema, asthma, colds, and upper respiratory tract problems.
b. Folk remedies are common among certain ethnic groups and subgroups within the United States. Many are based on traditional family remedies that have been proven neither to be effective or entirely harmful in most cases. However, a few remedies could be potentially harmful, especially to children, if these remedies counteract the effects of prescribed treatments that are known to be effective.
c. The nurse’s role in such cases is to gather sufficient data from the family about the practice, discuss the treatment (CAM) in a nonjudgmental manner, and be cognizant of the effects of the treatment on the child’s current health status and potential effects on other medical treatment regimens.
3. Give the family their penny and open a dialog about the traditional practice they are using. Additional information should be gathered in a nonjudgmental manner, and the discussion should center on the family’s traditional beliefs regarding the practices, the prescribed medical regimen, and whether there is conflict or potential for harm. There is no need to stop the treatment unless potential harm to the child may occur. A discussion with the primary practitioner regarding the use of CAM for Maria should ensue, followed by a discussion with the entire family, if necessary. The contents of the bottle will more than likely be revealed during the discussion with the family. It is important to respect the family’s wishes regarding traditional folk or CAM rituals, yet remain mindful of potential harmful effects on the child. It is not likely that telling the family to stop the ritual will be successful because these beliefs are deeply ingrained into cultural, religious, and medical practice; the family is more likely to continue the ritual at home on discharge and further disregard other instructions for care should a confrontational approach be adopted by the nursing and medical staff. The important concept for the staff and family to focus on is the ultimate well-being of the child. What you have probably observed is Santeria, the African-Caribbean religion that was brought to the New World by slaves from West Africa. It is common among immigrants from Cuba, Puerto Rico, Brazil, and Santo Domingo, and it is believed that a majority of Latin American immigrants will have contact with Santeria sometime in their lives.
4. As yet, there is insufficient evidence to indicate that harm is being done by the CAM ritual. Further data need to be gathered, and then a decision about further discussion of the CAM practice may occur.
PLAYROOM AND HOSPITAL PROCEDURES
1. There is sufficient evidence regarding this incident to draw some conclusions.
a. Regardless of how minor a procedure such as a venipuncture may seem to an adult health care worker, it represents a major threat to a child. One must consider the child’s age, illness, developmental level, and previous experiences with venipunctures.
b. Play is an important function of childhood whether the child is sick or well. Through play children may act out fears, concerns, anger, and other behaviors they may not feel comfortable expressing to adults in a confrontational manner. Play is an important part of the hospitalized child’s life, and it is a vehicle for promoting optimal development.
c. It is important to have the blood drawn so Dr. Lung may plan a therapeutic regimen; however, one must consider another issue: there appears to have been no advance preparation of the child’s skin to minimize or prevent pain from the procedure. Regardless of the phlebotomist’s skill in performing the procedure, it is also important to consider the fact that the negative repercussions for performing the procedure at this point may outweigh the positive benefits.
d. All staff on the pediatric floor must be in agreement about respecting the child’s personal space in the playroom and about adhering to unit policies or rules so that respect is maintained. Failure to respect the child’s space may engender fear in other children who perceive that the playroom is not a safe place after all. The fear of having other procedures performed in the playroom may prevent children from going there to participate in therapeutic and interactive play.
3. It is important to maintain a fair balance between what constitutes therapeutic management of illness and childhood recreation. It would be appropriate in this situation to intervene and ask the phlebotomist to return in 30 minutes to an hour and indicate that the child will be ready for the venipuncture in the treatment room at that time. It is important to stress that the playroom is off-limits for procedures. It would be appropriate to discuss this plan with Hannah, indicating that the procedure will be performed at the designated time. It is also important to explore pain management issues with Hannah—does she usually use EMLA (an eutectic mix of local anesthetics) or other topical remedy to prevent pain at the site? If so, it will be necessary to make such arrangements in advance, possibly now, so her pain is managed appropriately. As the nurse, it is appropriate to discuss a delay in obtaining the laboratory results with Dr. Lung and the reasons for the delay. As workers on the pediatric floor, it is important for medical and nursing staff to communicate effectively. Should this arrangement not suit Dr. Lung’s time frame for accomplishing certain tasks, one might suggest a trade-off. The nurse may draw the blood in the treatment room after preparations are made and Hannah agrees on a time. Remember, however, that school-age children are prone to “bargain” for more time to delay or prevent the event because it is painful. One must be gently firm about the agreed-on time of the procedure and not allow further delays to accommodate the child who just does not want the procedure performed—ever, in most cases.
Even if one accepts the conclusion that it is okay with Hannah, it is important to consider the possible negative implications for the other children in the room, who may be confused about even a simple procedure (e.g., checking blood pressure) or the sanctuary status of the playroom for themselves. Drawing blood in the playroom would violate the child’s trust in what adult health care workers say regarding the purpose of the playroom as a sanctuary from painful procedures. Such action would likely result in less cooperation from the children who are present and may also make other parents present (or who learn about the incident) wonder about the staff’s sincerity. Interrupting the children’s game is not necessary because this does not represent a life-threatening condition at this time.
4. Yes, there is sufficient evidence to support these decisions and the plan of action.
5. An exception is sometimes made when all the children present are older and the procedure is a quick, painless one (e.g., checking blood pressure, giving oral medication) that all the children present have experienced. In such cases the patient and the other children are asked if it is okay and give permission before the procedure is undertaken.
REFERENCES
Ashenberg, MD, Lambert, SA, Maier, NP, et al. Easing the wait: development of a pager program for families. Pediatr Nurs. 1996;22(2):103–107.
Board, R, Ryan-Wenger, N. Stressors and symptoms of mothers with children in the PICU. J Pediatr Nurs. 2003;18(3):195–201.
Bracht, M, Ardal, F, Bot, A, et al. Initiation and maintenance of a hospital-based parent group for parents of premature infants: key factors for success. Neonatal Netw. 1998;17(3):33–37.
Brewer, S, Lambert, C. Preparing children for same day surgery: innovative approaches. J Pediatr Nurs. 1997;12(4):257–259.
Clatworthy, S, Simon, K, Tiedeman, ME. Child drawing: hospital—an instrument designed to measure the emotional status of hospitalized school-aged children. J Pediatr Nurs. 1999;14(1):2–9.
Coyne, I. Children’s experiences of hospitalization. J Child Health Care. 2006;10(4):326–336.
Craft, MJ. Siblings of hospitalized children: assessment and intervention. J Pediatr Nurs. 1993;8(5):289–297.
Fernandez, C, Pyesmany, A, Stutzer, C. Alternative therapies in childhood cancer. N Engl J Med. 1999;340(7):569–570.
Feudtner, HJ, Haney, J, Dimmers, MA. Spiritual care needs of hospitalized children and their families: a national survey of pastoral care providers’ perceptions. Pediatrics. 2003;111(1):e67–e72.
Flanagan, K. Preoperative assessment: safety considerations for patients taking herbal products. J Perianesth Nurs. 2001;16(1):19–26.
Gordon, M. Manual of nursing diagnosis, ed 10. St Louis: Mosby, 2002.
Gordon, M. Nursing diagnosis: process and application, ed 3. St Louis: Mosby, 1994.
Harbaugh, BL, Tomlinson, PS, Kirschbaum, M. Parents’ perceptions of nurses’ caregiving behaviors in the pediatric intensive care unit. Issues Compr Pediatr Nurs. 2004;27(3):163–178.
Hazinski, MF. Manual of pediatric critical care. St Louis: Mosby, 1999.
Hornick, R. Discharge teams. In: Gunter K, Manago R, eds. Beyond discharge: interdisciplinary perspectives for transitioning children with complex medical needs from hospital to home. Bethesda, Md: Association for the Care of Children’s Health, 1996.
Huckabay, LMD, Tilem-Kessler, D. Patterns of parental stress in PICU emergency admission. Dimens Crit Care Nurs. 1999;18(2):36–42.
Lewandowski, LA, Tesler, MD. Family centered care: putting it into action. Washington, DC: American Nurses Association, 2003.
Melnyk, BM. Intervention studies involving parents of hospitalized young children: an analysis of the past and future recommendations. J Pediatr Nurs. 2000;15(1):4–13.
Melnyk, B, Alpert-Gillis, L. The COPE Program: a strategy to improve outcomes of critically ill young children and their parents. Pediatr Nurs. 1998;24(6):521–527.
Orem, D. Nursing: concepts of practice, ed 5. New York: Mosby, 2001.
Scott, LD. Perceived needs of parents of critically ill children. J Soc Pediatr Nurs. 1998;3(1):4–12.
Small, L. Early predictors of poor coping outcomes in children following intensive care hospitalization and stressful medical encounters. Pediatr Nurs. 2002;28(4):393–401.
Smith, T, Conant Rees, HL. Making family-centered care a reality. Semin Nurs Manage. 2000;8(3):136–142.
Stewart, E, Algren, C, Arnold, S. Preparing children for a surgical experience. Today’s OR Nurse. 1994;16(2):9–14.
Stranton, KM. Parents’ experiences of their child’s care during hospitalization. J Cult Divers. 2004;11(1):4–11.
The Joint Commission on Accreditation of Healthcare Organizations. AMH92 accreditation manual for hospitals. Chicago: The Commission, 2004.
Woodgate, R, Kristjanson, L. “Getting better from my hurts”: toward a model of the young child’s pain experience. J Pediatr Nurs. 1996;11(4):233–242.