The Evolution of Evidence-Based Practice in Nursing
Initially, nursing research evolved slowly, from Florence Nightingale’s investigations in the nineteenth century to the studies of nursing education in the 1930s and 1940s and the research of nurses and nursing roles in the 1950s and 1960s. However, in the late 1970s and 1980s, numerous studies focused on improving nursing practice. This emphasis continued in the 1990s with research focused on testing the effectiveness of nursing interventions and examining patient outcomes. The goal in the new millennium is the development of an evidence-based practice for nursing, with the current best research evidence being used to deliver patient care.
Evidence-based practice (EBP) is the conscientious integration of best research evidence with clinical expertise and patient values and needs in the delivery of quality, cost-effective health care. Chapter 1 presents a model depicting the elements of evidence-based practice (see Figure 1-2). You probably have many questions about evidence-based practice, because this is a relative new and evolving concept for the profession of nursing. What does best research evidence mean? How is this research evidence developed? Are there levels of quality in the types of research evidence? How is the best research evidence implemented in nursing practice? This chapter will increase your understanding of how nursing research has evolved over the past 150 years and the current movement of the profession toward evidence-based practice. The chapter describes the historical events relevant to nursing research in building an evidence-based practice for nursing, identifies the methodologies used in nursing to develop research evidence, and concludes with a discussion of the best research evidence needed to build an EBP.
HISTORICAL DEVELOPMENT OF RESEARCH IN NURSING
Some people think that research is relatively new to nursing, but Florence Nightingale initiated nursing research more than 150 years ago (Nightingale, 1859). Following Nightingale’s work (1850–1910), research received minimal attention until the mid-1900s. In the 1960s, nurses gradually recognized the value of research, but few had the educational background to conduct studies until the 1970s. However, in the 1980s and 1990s, research became a major force in developing a scientific knowledge base for the nursing practice. Today, nurses obtain federal and corporate funding for their research, conduct complex studies in multiple settings, and generate sound research evidence for practice. Table 2-1 identifies some of the key historical events that have influenced the development of nursing research and the movement toward EBP in nursing. These events are discussed in the following section.
TABLE 2-1
Historical Events Influencing Nursing Research
| Year | Historical Event |
| 1850 | Florence Nightingale is the first nurse researcher. |
| 1859 | Nightingale’s Notes on Nursing is published. |
| 1900 | American Journal of Nursing is first published. |
| 1923 | Teacher’s College at Columbia University offers the first educational doctoral program for nurses. |
| 1929 | First master of nursing degree is offered at Yale University. |
| 1932 | Association of Collegiate Schools of Nursing is organized. |
| 1950 | American Nurses Association (ANA) publishes study of nursing functions and activities. |
| 1952 | Nursing Research is first published. |
| 1953 | Institute of Research and Service in Nursing Education is established. |
| 1955 | American Nurses Foundation is established to fund nursing research. |
| 1963 | International Journal of Nursing Studies is first published. |
| 1965 | ANA sponsors first nursing research conferences. |
| 1967 | Image (Sigma Theta Tau publication) is first published. |
| Stetler/Marram Model for Application of Research Findings to Practice is first published. | |
| 1970 | ANA Commission on Nursing Research is established. |
| 1972 | Professor Archie Cochrane, a Scottish epidemiologist, publishes his book Effectiveness and Efficiency: Random Reflections on Health Services, which promotes the acceptance of the concepts behind evidence-based practice. |
| ANA Council of Nurse Researchers is established. | |
| 1973 | First Nursing Diagnosis Conference is held. |
| 1978 | Research in Nursing & Health is first published. Advances in Nursing Science is first published. |
| Western Interstate Commission for Higher Education (WICHE) Project focused on research utilization is published. | |
| 1979 | Western Journal of Nursing Research is first published. |
| 1980s–1990s | David Sackett and his research team develop methodologies to determine “best evidence” for practice. |
| 1982–1983 | Conduct and Utilization of Research in Nursing (CURN) Project is published. |
| 1983 | Annual Review of Nursing Research is first published. |
| 1985 | National Center for Nursing Research (NCNR) is established within the National Institutes of Health. |
| 1987 | Scholarly Inquiry for Nursing Practice is first published. |
| 1988 | Applied Nursing Research is first published. |
| Nursing Science Quarterly is first published. | |
| 1989 | Agency for Health Care Policy and Research (AHCPR) is established. |
| AHCPR first publishes clinical practice guidelines. | |
| 1992 | U.S. Department of Health and Human Services publishes the Healthy People 2000 document. |
| Cochrane Center, rooted on the evidence-based practice efforts of Dr. Cochrane, is launched. | |
| Clinical Nursing Research is first published. | |
| 1993 | NCNR is renamed the National Institute of Nursing Research (NINR). |
| Cochrane Collaboration is initiated providing systematic reviews and evidence-based guidelines for practice (www.cochrane.org). | |
| 1994 | Qualitative Health Research is first published. |
| 1999 | AHCPR is renamed Agency for Healthcare Research and Quality (AHRQ). |
| American Association of Colleges of Nursing publishes its Position Statement on Nursing Research. | |
| Institute of Medicine Study is published, which focuses on quality care issues and emphasizes the need for evidence-based practice. | |
| 2000 | The U.S. Department of Health and Human Services publishes the Healthy People 2010 document. |
| Biological Research for Nursing is first published. | |
| 2001 | Stetler publishes her model “Steps of Research Utilization to Facilitate Evidence-Based Practice.” |
| 2002 | Joint Commission revises accreditation policies, emphasizing patient care quality through the use of the most current research evidence in practice. |
| 2004 | Worldviews on Evidence-Based Nursing is first published. |
| 2007 | NINR identifies mission and funding themes for the future (www.nih.gov/ninr). |
| 2007 | AHRQ identifies mission and goals for the future (www.ahrq.gov). |
Florence Nightingale
Nightingale has been described as a reformer, reactionary, and researcher who has influenced nursing specifically and health care in general. Nightingale’s book, Notes on Nursing (1859), described her initial research activities, which focused on the importance of a healthy environment in promoting the patient’s physical and mental well-being. She identified the need to gather data on the environment, such as ventilation, cleanliness, temperature, purity of water, and diet, to determine their influence on the patient’s health (Herbert, 1981).
Nightingale is most noted for her data collection and statistical analyses during the Crimean War. She gathered data on soldier morbidity and mortality rates and the factors influencing them and presented her results in tables and pie charts, a sophisticated type of data presentation for the period (Palmer, 1977). Nightingale’s research enabled her to instigate attitudinal, organizational, and social changes. She changed the attitudes of the military and society toward the care of the sick. The military began to view the sick as having the right to adequate food, suitable quarters, and appropriate medical treatment. These interventions drastically reduced the mortality rate from 43% to 2% in the Crimean War (Cook, 1913). Nightingale improved the organization of army administration, hospital management, and hospital construction. Because of Nightingale’s research evidence and influence, society began to accept responsibility for testing public water, improving sanitation, preventing starvation, and decreasing morbidity and mortality rates (Palmer, 1977).
Early 1900s
From 1900 to 1950, research activities in nursing were limited, but a few studies advanced nursing education. These studies included the Nutting Report, 1912; Goldmark Report, 1923; and Burgess Report, 1926 (Abdellah, 1972; Johnson, 1977). On the basis of recommendations of the Goldmark Report, more schools of nursing were established in university settings. The baccalaureate degree in nursing provided a basis for graduate nursing education, with the first master of nursing degree offered by Yale University in 1929. Teachers College at Columbia University offered the first doctoral program for nurses in 1923 and granted a degree in education (Ed.D.) to prepare teachers for the profession. The Association of Collegiate Schools of Nursing, organized in 1932, promoted the conduct of research to improve education and practice. This organization also sponsored the publication of the first research journal in nursing, Nursing Research, in 1952 (Fitzpatrick, 1978).
A research trend that started in the 1940s and continued in the 1950s focused on the organization and delivery of nursing services. Studies were conducted on the numbers and kinds of nursing personnel, staffing patterns, patient classification systems, patient and personnel satisfaction, and unit arrangement. Types of care such as comprehensive care, home care, and progressive patient care were evaluated. These evaluations of care laid the foundation for the development of self-study manuals, which are similar to the quality assurance manuals of today (Gortner & Nahm, 1977).
Nursing Research in the 1950s and 1960s
In 1950, the American Nurses Association (ANA) initiated a 5-year study on nursing functions and activities. The findings were reported in Twenty Thousand Nurses Tell Their Story, and this study enabled the ANA to develop statements on functions, standards, and qualifications for professional nurses in 1959. Also during this time, clinical research began expanding as specialty groups, such as community health, psychiatric, medical-surgical, pediatrics, and obstetrics, developed standards of care. The research conducted by ANA and the specialty groups provided the basis for the nursing practice standards that currently guide professional nursing practice (Gortner & Nahm, 1977).
Educational studies were conducted in the 1950s and 1960s to determine the most effective educational preparation for the registered nurse. A nurse educator, Mildred Montag, developed and evaluated the 2-year nursing preparation (associate degree) in the junior colleges. Student characteristics, such as admission and retention patterns and the elements that promoted success in nursing education and practice, were studied for both associate- and baccalaureate degree–prepared nurses (Downs & Fleming, 1979).
In 1953, an Institute for Research and Service in Nursing Education was established at Teacher’s College, Columbia University, which provided research-learning experiences for doctoral students (Werley, 1977). The American Nurse’s Foundation, chartered in 1955, was responsible for receiving and administering research funds, conducting research programs, consulting with nursing students, and engaging in research. In 1956, a Committee on Research and Studies was established to guide ANA research (See, 1977).
A Department of Nursing Research was established in the Walter Reed Army Institute of Research in 1957. This was the first nursing unit in a research institution that emphasized clinical nursing research (Werley, 1977). Also in 1957, the Southern Regional Educational Board (SREB), the Western Interstate Commission on Higher Education (WICHE), and the New England Board of Higher Education (NEBHE) were developed. These organizations are actively involved in promoting research and disseminating the findings. The ANA sponsored the first of a series of research conferences in 1965, and the conference sponsors required that the studies presented be relevant to nursing and conducted by a nurse researcher (See, 1977). These ANA conferences continue to be an important means of disseminating nursing research findings.
In the 1960s, a growing number of clinical studies focused on quality care and the development of criteria to measure patient outcomes. Intensive care units were being developed, which promoted the investigation of nursing interventions, staffing patterns, and cost-effectiveness of care (Gortner & Nahm, 1977).
Nursing Research in the 1970s
In the 1970s, the nursing process became the focus of many studies, with the investigations of assessment techniques and guidelines, goal-setting methods, and specific nursing interventions. In 1973, the first Nursing Diagnosis Conference was held; these conferences continue to be held every 2 to 3 years. Studies have focused on identifying appropriate diagnoses for nursing and generating an effective diagnostic process (Carlson-Catalano & Lunney, 1995). Many of the studies conducted in the 1970s were not being used in practice, so Stetler and Marram (1976) developed a model to promote the communication and use of research findings in practice.
The educational studies of the 1970s evaluated teaching methods and student learning experiences. A number of studies were conducted to differentiate the practices of nurses with baccalaureate and associate degrees. These studies, which primarily measured abilities to perform technical skills, were ineffective in differentiating between the two levels of education.
In the service setting, primary nursing care, which involves the delivery of patient care predominantly by registered nurse, was the trend of the 1970s. Studies were conducted to examine the implementation and outcomes of primary nursing care delivery models. The number of nurse practitioners (NPs) and clinical nurse specialists (CNSs) with master’s degrees increased rapidly during the 1970s. Limited research has been conducted on the CNS role; however, the NP and nurse midwifery roles have been researched extensively to determine their positive impact on productivity, quality, and cost of health care (Brown & Grimes, 1995; Mundinger et al., 2000). In addition, those clinicians with master’s degrees were provided the background to conduct research and to use research findings in practice.
In the 1970s, nursing scholars began developing models, conceptual frameworks, and theories to guide nursing practice. The works of these nursing theorists also directed future nursing research. In 1978, a new journal, Advances in Nursing Science, began publishing the works of nursing theorists and the research related to their theories. The number of doctoral programs in nursing and the number of nurses prepared at the doctoral level greatly expanded in the 1970s (Jacox, 1980). Some of the nurses with doctoral degrees increased the conduct and complexity of nursing research; however, many doctorally prepared nurses did not become actively involved in research. In 1970, the ANA Commission on Nursing Research was established; in turn, this commission established the Council of Nurse Researchers in 1972 to advance research activities, provide an exchange of ideas, and recognize excellence in research. The commission also prepared position papers on subjects’ rights in research and on federal guidelines concerning research and human subjects, and it sponsored research programs nationally and internationally (See, 1977).
Federal funds for nursing research increased significantly, with a total of slightly more than $39 million awarded for research in nursing from 1955 to 1976. Even though federal funding for nursing studies rose, the funding was not comparable to the $493 million in federal research funds received by those doing medical research in 1974 alone (de Tornyay, 1977).
The dissemination of research findings was a major focus in the 1970s. Sigma Theta Tau, the International Honor Society for Nursing, sponsored national and international research conferences, and the chapters of this organization sponsored many local conferences to promote the dissemination of research findings. Image, a journal initially published in 1967 by Sigma Theta Tau, contains many nursing studies and articles about research methodology. A major goal of Sigma Theta Tau is to advance scholarship in nursing by promoting the conduct, communication, and utilization of research in nursing. The addition of two new research journals in the 1970s, Research in Nursing & Health in 1978 and Western Journal of Nursing Research in 1979, also increased the communication of nursing research findings.
Professor Archie Cochrane originated the concepts of evidence-based practice with a book he published in 1972 titled Effectiveness and Efficiency: Random Reflections on Health Services. Cochrane advocated the provision of health care based on research to improve the quality of care and patient outcomes. To facilitate the use of research evidence in practice, the Cochrane Center was established in 1992 and the Cochrane Collaboration in 1993. The Cochrane Collaboration and Library house numerous resources to promote EBP, such as systematic reviews of research and evidence-based guidelines for practice (discussed later in this chapter) (see the Cochrane Collaboration at www.cochrane.org).
Nursing Research in the 1980s and 1990s
The conduct of clinical nursing research was the focus in the 1980s and 1990s. A variety of clinical journals (Cancer Nursing; Cardiovascular Nursing; Dimensions of Critical Care Nursing; Heart & Lung; Journal of Obstetric, Gynecologic, and Neonate Nursing; Journal of Neurosurgical Nursing; Oncology Nursing Forum; Pediatric Nursing; and Rehabilitation Nursing) published an increasing number of studies. One new research journal was published in 1987, Scholarly Inquiry for Nursing Practice, and two in 1988, Applied Nursing Research and Nursing Science Quarterly.
Even though the body of empirical knowledge generated through clinical research grew rapidly in the 1970s and 1980s, little of this knowledge was used in practice. Two major projects were launched to promote the use of research-based nursing interventions in practice: the Western Interstate Commission for Higher Education (WICHE) Regional Nursing Research Development Project and the Conduct and Utilization of Research in Nursing (CURN) Project. In these projects, nurse researchers, with the assistance of federal funding, designed and implemented strategies for using research findings in practice. The WICHE Project participants selected a research-based intervention for use in practice and then functioned as change agents to implement the selected intervention in a clinical agency. Because of the limited amount of research that had been conducted, the project staff and participants had difficulty identifying adequate clinical studies with findings ready for use in practice (Krueger, Nelson, & Wolanin, 1978).
The CURN Project was a 5-year venture (1975–1980) directed by Horsley, Crane, Crabtree, and Wood (1983) to increase the utilization of research findings by (1) disseminating findings, (2) facilitating organizational modifications necessary for implementation, and (3) encouraging collaborative research that was directly transferable to clinical practice. Research utilization was seen as a process to be implemented by an organization rather than by an individual practitioner. Activities of the research utilization included (1) identification and synthesis of multiple studies in a common conceptual area (research base), (2) transformation of the knowledge derived from a research base into a solution or clinical protocol, (3) transformation of the clinical protocol into specific nursing actions (innovations) that are administered to patients, and (4) clinical evaluation of the new practice to ascertain whether it produced the predicted result (Horsley et al., 1983). The clinical protocols developed during the project were published to encourage nurses in other health care agencies to use these research-based intervention protocols in their practice (CURN Project, 1981–1982).
To ensure that the studies were incorporated into nursing practice, the findings needed to be synthesized for different topics. In 1983, the first volume of the Annual Review of Nursing Research was published (Werley & Fitzpatrick, 1983). This annual publication contains experts’ reviews of research in selected areas of nursing practice, nursing care delivery, nursing education, and the profession of nursing. The Annual Review of Nursing Research continues to be published each year to (1) expand the synthesis and dissemination of research findings, (2) promote the use of research findings in practice, and (3) identify directions for future research.
Many nurses obtained master’s and doctoral degrees during the 1980s and 1990s, and postdoctoral education was encouraged for nurse researchers. The ANA Cabinet on Nursing Research identified the research participation for various levels of educational preparation. As indicated in Figure 2-1, nurses at all levels of education have a role in research (ANA, 1989). The nursing educational preparation provides a background for nurses at the following levels:
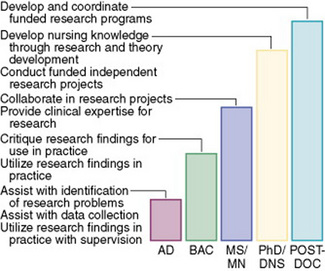
• The nurse with an associate degree to assist with problem identification and data collection
• The nurse with a baccalaureate degree to use research findings in practice
• The nurse with a master’s degree to collaborate in research projects
• The nurse with a doctoral degree to conduct independent, funded research projects
• The nurse with a postdoctoral degree to implement a funded program of research
These research expectations for each level of nursing education were supported by the American Association of Colleges of Nursing’s (AACN’s) 1999 position statement on nursing research (AACN, 1999).
Another priority of the 1980s and 1990s was to obtain greater funding for nursing research. Most of the federal funds in the 1980s were designated for studies involving the diagnosis and cure of diseases. Therefore, nursing received a small percentage of the federal research and development (R&D) funds (approximately 2% to 3%) compared with medicine (approximately 90%), even though nursing personnel greatly outnumber medical personnel (Larson, 1984). However, the ANA achieved a major political victory for nursing research with the creation of the National Center for Nursing Research (NCNR) in 1985. This center was created after years of work and two presidential vetoes (Bauknecht, 1986). The purpose of the NCNR was to support the conduct of basic and clinical nursing research and the dissemination of findings. The NCNR was established under the National Institutes of Health (NIH) and provided visibility for nursing research at the federal level. In 1993, during the tenure of its first director, Dr. Ada Sue Hinshaw, the NCNR became the National Institute of Nursing Research (NINR). This change in title enhanced the recognition of nursing as a research discipline and expanded the funding for nursing research.
Outcomes research emerged as an important methodology for documenting the effectiveness of health care services in the 1980s and 1990s. This type of research evolved from the quality assessment and quality assurance functions that originated with the professional standards review organizations (PSROs) in 1972. During the 1980s, William Roper, the director of the Health Care Finance Administration (HCFA), promoted outcomes research for determining the quality and cost-effectiveness of patient care (Johnson, 1993).
In 1989, the Agency for Health Care Policy and Research (AHCPR) was established to facilitate the conduct of outcomes research (Rettig, 1991). The AHCPR also had an active role in communicating research findings to health care practitioners and was responsible for publishing the first clinical practice guidelines in 1989. Several of these guidelines, including the latest research findings with directives for practice, were published in the 1990s. The Healthcare Research and Quality Act of 1999 reauthorized the AHCPR, changing its name to the Agency for Healthcare Research and Quality (AHRQ). This significant change positioned the AHRQ as a scientific partner with the public and private sectors to improve the quality and safety of patient care by promoting the use of the best research evidence available in practice (see www.ahcpr.gov).
Building on the process of research utilization, physicians, nurses, and other health care professions focused on the development of EBP for health care during the 1990s. A research group led by Dr. David Sackett at McMaster University in Canada developed explicit research methodologies to determine the “best evidence” for practice. The term evidence based was first used by David Eddy in 1990 with the focus on providing EBP for medicine (Craig & Smyth, 2007; Sackett, Straus, Richardson, Rosenberg, & Haynes, 2000). In 2002, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) revised the accreditation policies for hospitals to support the implementation of evidence-based health care. To facilitate the movement of nursing toward EBP, Stetler (2001) develop the “Research Utilization to Facilitate EBP” model (see Chapter 27 for a description of this model).
Nursing Research in the Twenty-First Century
The vision for nursing in the twenty-first century includes conducting quality studies, synthesizing the study findings into the best research evidence available, and using that research evidence effectively in practice (Brown, 1999; Craig & Smyth, 2007; Malloch & Porter-O’Grady, 2006; Melnyk & Fineout-Overholt, 2005; Pearson, Field, & Jordan, 2007). This vision is consistent with the mission of the NINR, which is to support the conduct of biological and clinical research and facilitate the communication of this research to promote an EBP for nursing (NINR, 2007, at www.nih.gov/ninr). With the conduct of biological research a priority for the NINR, the journal Biological Research for Nursing was initiated in 2000. The focus on EBP in nursing was supported with the initiation of the Worldviews on Evidence-Base Nursing journal in 2004.
The AHRQ has been designated the lead agency supporting research designed to improve the quality of health care, reduce its cost, improve patient safety, decrease medical errors, and broaden access to essential services. The AHRQ sponsors and conducts research that provides evidence-based information on health care outcomes, quality, cost, use, and access. This research information promotes effective health care decision making by patients, clinicians, health system executives, and policy makers. The three future goals of the AHRQ are to (1) support improvements in health outcomes; (2) strengthen quality measurements and improvements; and (3) identify strategies to improve access, foster appropriate use of health care resources, and reduce unnecessary expenditures (AHRQ, 2007, www.ahrq.gov). Currently, the AHRQ and NINR work collaboratively to promote funding for nursing studies. These agencies often jointly call for proposals for studies of high priority to both agencies.
The focus of health care research and funding is expanding from the treatment of illness to include health promotion and illness prevention interventions. Healthy People 2000 and Healthy People 2010, government documents published by the U.S. Department of Health and Human Services (1992, 2000), have increased the visibility of and identified priorities for health promotion research. In the twenty-first century, nurses can have a major role in the development of interventions to promote health and prevent illness in individuals, families, and communities.
To ensure an effective research enterprise in nursing, the discipline must do the following:
2. Provide quality educational (baccalaureate, master’s, doctoral, and postdoctoral) programs to prepare a workforce of nurse scientists.
3. Develop a sound research infrastructure.
4. Obtain sufficient funding for essential research (AACN, 1999).
METHODOLOGIES FOR DEVELOPING RESEARCH EVIDENCE IN NURSING
Scientific method incorporates all procedures that scientists have used, currently use, or may use in the future to pursue knowledge (Kaplan, 1964). This broad definition dispels the belief that there is one way to conduct research and embraces the use of both quantitative and qualitative research methodologies in developing research evidence for practice.
Since the 1930s, many researchers have narrowly defined scientific method to include only quantitative research. This research method is based in the philosophy of logical empiricism or positivism (Norbeck, 1987; Scheffler, 1967). Therefore, scientific knowledge is generated through an application of logical principles and reasoning, whereby the researcher adopts a distant and noninteractive posture with the research subject to prevent bias (Silva & Rothbart, 1984). Quantitative research is a formal, objective, systematic process in which numerical data are used to obtain information about the world. This research method is used to describe variables, examine relationships among variables, and determine cause-and-effect interactions between variables. Currently, the predominantly used method of scientific investigation in nursing is quantitative research.
Qualitative research is a systematic, interactive, subjective approach used to describe life experiences and give them meaning (Marshall & Rossman, 2006; Munhall, 2001). Qualitative research is not a new idea in the social and behavioral sciences (Baumrind, 1980; Glaser & Strauss, 1967). This type of research is conducted to describe and promote our understanding of human experiences such as pain, caring, and comfort.
Comparison of Quantitative and Qualitative Research
The quantitative and qualitative types of research complement each other because they generate different kinds of knowledge that are useful in nursing practice. The problem and purpose to be studied determines the type of research to be conducted, and the researcher’s knowledge of both types of research promotes accurate selection of the methodology for the problem identified (McPherson & Leydon, 2002). Quantitative and qualitative research methodologies have some similarities, because both require researcher expertise, involve rigor in implementation, and result in the generation of scientific knowledge for nursing practice. Some of the differences between the two methodologies are presented in Table 2-2.
TABLE 2-2
Quantitative and Qualitative Research Characteristics
| Characteristic | Quantitative Research | Qualitative Research |
| Philosophical origin | Logical positivism | Naturalistic, interpretive, humanistic |
| Focus | Concise, objective, reductionistic | Broad, subjective, holistic |
| Reasoning | Logistic, deductive | Dialectic, inductive |
| Basis of knowing | Cause-and-effect relationships | Meaning, discovery, understanding |
| Theoretical focus | Tests theory | Develops theory |
| Researcher involvement | Control | Shared interpretation |
| Methods of measurement | Structured interviews, questionnaires, observations, scales, or physiological instruments | Unstructured interviews and observations |
| Data | Numbers | Words |
| Analysis | Statistical analysis | Individual interpretation |
| Findings | Generalization, accept or reject theoretical propositions | Uniqueness, dynamic, understanding of phenomena, and new theory |
Philosophical Origin of Quantitative and Qualitative Research
The quantitative approach to scientific inquiry emerged from a branch of philosophy called logical positivism, which operates on strict rules of logic, truth, laws, axioms, and predictions. Quantitative researchers hold the position that truth is absolute and that there is a single reality that one could define by careful measurement. To find truth as a quantitative researcher, you must be completely objective, meaning that values, feelings, and personal perceptions cannot enter into the measurement of reality. Quantitative researchers believe that all human behavior is objective, purposeful, and measurable. The researcher needs only to find or develop the “right” instrument or tool to measure the behavior.
Today, however, many nurse researchers base their quantitative studies on more of a postpositivist philosophy (Clark, 1998). This philosophy evolved from positivism but focuses on the discovery of reality that is characterized by patterns and trends that can be used to describe, explain, and predict phenomena. With postpositivism, “truth can be discovered only imperfectly and in a probabilistic sense, in contrast to the positivist ideal of establishing cause-and-effect explanations of immutable facts” (Ford-Gilboe, Campbell, & Berman, 1995, p. 16). The postpositivist approach also rejects the idea that the researcher is completely objective about what is to be discovered but continues to emphasize the need to control environmental influences (Newman, 1992).
Qualitative research is an interpretive methodological approach that is thought to produce more of a subjective science than quantitative research. Qualitative research evolved from the behavioral and social sciences as a method of understanding the unique, dynamic, holistic nature of human beings. The philosophical base of qualitative research is interpretive, humanistic, and naturalistic and is concerned with helping those involved to understand the meaning of their social interactions. Qualitative researchers believe that truth is both complex and dynamic and can be found only by studying persons as they interact with and within their sociohistorical settings (Marshall & Rossman, 2006; Munhall, 2001).
Focus of Quantitative and Qualitative Research
The focus or perspective for quantitative research is usually concise and reductionistic. Reductionism involves breaking the whole into parts so that the parts can be examined. Quantitative researchers remain detached from the study and try not to influence it with their values (objectivity). Researcher involvement in the study is thought to bias or sway the study toward the perceptions and values of the researcher, and biasing a study is considered poor scientific technique (Kerlinger & Lee, 2000).
The focus of qualitative research is usually broad, and the intent is to give meaning to the whole (holistic). The qualitative researcher has an active part in the study, and the researcher’s values and perceptions influence the findings. Thus, this research approach is subjective, but the approach assumes that subjectivity is essential for the understanding of human experiences (Marshall & Rossman, 2006; Munhall, 2001).
Uniqueness of Conducting Quantitative and Qualitative Research
Quantitative research describes and examines relationships and determines causality among variables. Thus, this method is useful for testing a theory by testing the validity of the relationships that compose the theory. Quantitative research incorporates logistic, deductive reasoning as the researcher examines particulars to make generalizations about the universe.
Qualitative research generates knowledge about meaning and discovery. Inductive and dialectic reasoning are predominant in these studies. For example, the qualitative researcher studies the whole person’s response to pain by examining premises about human pain and determining the meaning that pain has for a particular person. Because qualitative research is concerned with meaning and understanding, the findings from these studies can be used to identify the relationships among the variables, and these relational statements are used to develop theories.
Quantitative research requires control (see Table 2-2). The investigator uses control to identify and limit the problem to be researched and attempts to limit the effects of extraneous or outside variables that are not the focus of the study. For example, as a quantitative researcher, you might study the effects of nutritional education on serum lipid levels (total serum cholesterol, low-density lipoprotein [LDL], and high-density lipoprotein [HDL]). You would control the educational program by manipulating the type of education provided, the teaching methods, the length of the program, the setting for the program, and the instructor. You could also control other extraneous variables, such as participant’s age, history of cardiovascular disease, and exercise level, because they might affect the serum lipid levels. The intent of this control is to more precisely examine the effects of nutritional education on serum lipid levels.
Quantitative research also requires the use of (1) structured interviews, questionnaires, or observations; (2) scales; or (3) physiological instruments that generate numerical data. Statistical analyses are conducted to reduce and organize data, determine significant relationships, and identify differences among groups. Control, instruments, and statistical analyses are used to ensure that the research findings accurately reflect reality so that the study findings can be generalized. Generalization involves the application of trends or general tendencies (which are identified by studying a sample) to the population from which the research sample was drawn. Researchers must be cautious in making generalizations, because a sound generalization requires the support of many studies with a variety of samples.
Qualitative researchers use unstructured observations and interviews to gather data. The data include the shared interpretations of the researcher and the subjects, and no attempts are made to control the interaction. For example, the researcher and subjects might share their experiences of powerlessness in the health care system. The data are subjective and incorporate the perceptions and beliefs of the researcher and the subjects (Munhall, 2001).
Qualitative data take the form of words and are analyzed in terms of individual responses, descriptive summaries, or both. The researcher identifies categories for sorting and organizing the data (Miles & Huberman, 1994). The intent of the analysis is to organize the data into a meaningful, individualized interpretation, framework, or theory that describes the phenomenon studied. The findings from a qualitative study are unique to that study, and it is not the researcher’s intent to generalize the findings to a larger population. However, understanding the meaning of a phenomenon in a particular situation is useful for understanding similar phenomena in similar situations.
Classification for the Research Methodologies Presented in This Text
Research methods used frequently in nursing have been classified in different ways, so a classification system was developed for this text and is presented in Table 2-3. The quantitative research methods are classified into four categories: (1) descriptive, (2) correlational, (3) quasi-experimental, and (4) experimental. Types of quantitative research are used to test theories and generate and refine knowledge for nursing practice. Quantitative research methods are introduced in this section and described in more detail in Chapter 3.
TABLE 2-3
Classification System of Nursing Research Methods for This Textbook
Types of Quantitative Research
Descriptive research
Correlational research
Quasi-experimental research
Experimental research
Types of Qualitative Research
Phenomenological research
Grounded theory research
Ethnographic research
Historical research
Philosophical inquiry:
Critical social theory methodology
Outcomes Research
Intervention Research
The qualitative research methods included in this textbook are (1) phenomenological research, (2) grounded theory research, (3) ethnographic research, (4) historical research, (5) philosophical inquiry, and (6) critical social theory. These approaches, all methodologies for discovering knowledge, are introduced in this section and described in depth in Chapters 4 and 23. Unit Two of this textbook focuses on understanding the research process and includes discussions of both quantitative and qualitative research.
Quantitative Research Methods
Descriptive Research: Descriptive research provides an accurate portrayal or account of characteristics of a particular individual, situation, or group (Kerlinger & Lee, 2000). Descriptive studies offer researchers a way to (1) discover new meaning, (2) describe what exists, (3) determine the frequency with which something occurs, and (4) categorize information. Descriptive studies are usually conducted when little is known about a phenomenon and provide the basis for the conduct of correlational, quasi-experimental, and experimental studies.
Correlational Research: Correlational research involves the systematic investigation of relationships between or among two or more variables that have been identified in theories, observed in practice, or both. If the relationships exist, the researcher determines the type (positive or negative) and the degree or strength of the relationships. The primary intent of correlational studies is to explain the nature of relationships, not to determine cause and effect. However, correlational studies are the means for generating hypotheses to guide quasi-experimental and experimental studies that focus on examining cause-and-effect interactions.
Quasi-Experimental Research: The purposes of quasi-experimental research are (1) to identify causal relationships, (2) to examine the significance of causal relationships, (3) to clarify why certain events happened, or (4) a combination of these objectives (Cook & Campbell, 1979). These studies test the effectiveness of nursing interventions that can then be implemented to control the patient and family outcomes in nursing practice.
Quasi-experimental studies are less powerful than experimental studies because they involve a lower level of control in at least one of three areas: (1) manipulation of the treatment or independent variable, (2) manipulation of the setting, and (3) selection of subjects. When studying human behavior, especially in clinical areas, researchers are commonly unable to manipulate or control certain variables. Also, subjects are not randomly selected but are selected on the basis of convenience. Thus, as a nurse researcher you will probably conduct more quasi-experimental than experimental studies.
Experimental Research: Experimental research is an objective, systematic, controlled investigation conducted for the purpose of predicting and controlling phenomena. This type of research examines causality (Kerlinger & Lee, 2000). Experimental research is considered the most powerful quantitative method because of the rigorous control of variables. Experimental studies have three main characteristics: (1) a controlled manipulation of at least one treatment variable (independent variable), (2) administration of the treatment to some of the subjects in the study (experimental group) and not to others (control group), and (3) random selection of subjects or random assignment of subjects to groups, or both. Experimental studies usually have highly controlled settings in laboratories or research units in clinical agencies. A randomized controlled trial (RCT) is a type of experimental research that produces the strongest research evidence for practice.
Qualitative Research Methods
Phenomenological Research: Phenomenological research is a humanistic study of phenomena that is conducted in a variety of ways according to the philosophy of the researcher. The aim of phenomenology is to explore an experience as it is lived by the study participants and interpreted by the researcher. During the study, the researcher’s experiences, reflections, and interpretations influence the data collected from the study participants (Munhall, 2001). Thus, the participants’ lived experiences are expressed through the researcher’s interpretations and based on the underlying philosophy of the phenomenological study. Phenomenological research is an effective methodology to discover the meaning of a complex experience as it is lived by a person, such as the lived experience of health or dealing with chronic illness.
Grounded Theory Research: Grounded theory research is an inductive research method initially described by Glaser and Strauss (1967). This research approach is useful for discovering what problems exist in a social setting and the process people use to handle them. Grounded theory methodology emphasizes observation and the development of practice-based intuitive relationships among variables. Throughout the study, the researcher formulates, tests, and redevelops propositions until a theory evolves. The theory developed is “grounded,” or has its roots in, the data from which it was derived.
Ethnographic Research: Ethnographic research was developed by anthropologists to investigate cultures through an in-depth study of the members of the culture. This type of research attempts to tell the story of people’s daily lives while describing the culture in which they live. The ethnographic research process is the systematic collection, description, and analysis of data to develop a theory of cultural behavior. The researcher (ethnographer) actually lives in or becomes a part of the cultural setting to gather the data. Through the use of ethnographic research, different cultures are described, compared, and contrasted to add to our understanding of the impact of culture on human behavior and health (Germain, 2001).
Historical Research: Historical research is a narrative description or analysis of events that occurred in the remote or recent past. Data are obtained from records, artifacts, or verbal reports. Through historical research, nursing has a way of understanding itself and interpreting the discipline and its contributions to others. The mistakes of the past can be examined to help nurses understand and respond to present situations affecting nurses and nursing practice. In addition, historical research has the potential to provide a foundation for and to direct the future movements of the profession (Fitzpatrick, 2001).
Philosophical Inquiry: Philosophical inquiry uses intellectual analyses to (1) clarify meanings, (2) make values manifest, (3) identify ethics, and (4) study the nature of knowledge (Ellis, 1983). As a philosophical researcher, you would consider an idea or issue from all perspectives by extensively exploring the literature, examining conceptual meaning, raising questions, proposing answers, and suggesting the implications of those answers. The research is guided by philosophical questions that have been posed.
This textbook covers three categories of philosophical inquiry: foundational inquiry, philosophical analysis, and ethical inquiry. Foundational inquiry involves the analysis of the structure of a science and the process of thinking about and valuing certain phenomena held in common by members of a scientific discipline. Philosophical analysis examines meaning and develops theories of meaning through concept analysis or linguistic analysis. Ethical inquiry, another type of philosophical inquiry, involves the intellectual analysis of problems of ethics related to obligation, rights, duty, right and wrong, conscience, justice, choice, intention, and responsibility. Ethical inquiry is a means of striving for rational ends when other people are involved.
Critical Social Theory: Critical social theory provides the basis for research that focuses on understanding how people communicate and develop symbolic meanings in a society. Many of the meanings occur in a world where certain facts of the society are taken for granted rather than being discussed or disputed. The established political, social, and cultural orders are perceived as closed to change and are not questioned. Critical social theory provides a philosophical basis for multiple research methods to generate knowledge that might promote empowerment and political change (Ford-Gilboe et al., 1995). Nurses need to be aware of constraints and power imbalances in society that affect areas such as access to care, care of the chronically ill and elderly, and pain management of the terminally ill. The health needs of patients and families and the health care system developed to meet these needs are continuously influenced by the social system that surrounds them.
Outcomes Research
The spiraling cost of health care has generated many questions about the quality and effectiveness of health care services and the patient outcomes. Consumers want to know what services they are buying and whether these services will improve their health. Health care policy makers want to know whether the care is cost-effective and high quality. These concerns have promoted the development of outcomes research, which examines the results of care and measures the changes in health status of patients (AHRQ, 2007; Doran, 2003). Key ideas related to outcomes research are addressed throughout the text, and Chapter 12 contains a detailed discussion of this methodology.
Intervention Research
Intervention research investigates the effectiveness of a nursing intervention in achieving the desired outcome or outcomes in a natural setting. “Interventions are defined as treatments, therapies, procedures, or actions implemented by health professionals to and with clients, in a particular situation, to move the clients’ condition toward desired health outcomes that are beneficial to the clients” (Sidani & Braden, 1998, p. 8). An intervention can be a specific treatment implemented to manage a well-defined patient problem or a program. A program intervention, such as a cardiac rehabilitation program, consists of multiple nursing actions that are implemented as a package to improve the health conditions of the participants (Brown, 2002). The goal of intervention research is to generate sound scientific knowledge for actions that nurses can use to provide evidence-based nursing care. The details of intervention research are presented in Chapter 13. In summary, nurse researchers conduct a variety of research methodologies (quantitative, qualitative, outcomes, and intervention research) to develop the research evidence needed for practice.
INTRODUCTION TO BEST RESEARCH EVIDENCE FOR PRACTICE
Evidence-based practice (EBP) involves the use of best research evidence to support clinical decisions in practice. As a nurse, you make numerous clinical decisions each day that impact the health outcomes of your patients and families. By using the best research evidence available, you can make quality clinical decisions that will improve the health outcomes for patients, families, and communities. This section introduces you to the concept of best research evidence for practice by providing the following: (1) a definition of the term best research evidence, (2) a model of the levels of research evidence available, and (3) a link of the best research evidence to evidence-based guidelines for practice.
Definition of Best Research Evidence
Best research evidence is a summary of the highest quality, current empirical knowledge in a specific area of health care that is developed from a synthesis of quality studies (quantitative, qualitative, outcomes, and intervention) in that area. The synthesis of study findings is a complex, highly structured process that is best conducted by at least two or even a team of expert researchers and health care providers. There are various types of research synthesis, and the type of synthesis conducted varies based on the quality and types of research evidence available.
The quality of the research evidence available in an area depends on the number and strength of the studies. Replicating or repeating of studies with similar methodology adds to the quality of the research evidence. The strengths and weaknesses of the studies are determined by critically appraising the validity or credibility of the study outcomes (see Chapter 26). The types of research commonly conducted in nursing were identified earlier in this chapter as quantitative, qualitative, outcomes, and intervention. The research synthesis process used to summarize knowledge varies for quantitative and qualitative research. In building the best research evidence for practice, the quantitative experimental study, such as a randomized controlled trial (RCT), has been identified as producing the strongest research evidence for practice (Craig & Smyth, 2007; Institute of Medicine, 2001; Malloch & Porter-O’Grady, 2006; Melnyk & Fineout-Overholt, 2005; Pearson et al., 2007; Sackett et al., 2000).
Research evidence in nursing and health care is synthesized by using the following processes: (1) systematic review, (2) meta-analysis, (3) integrative review, (4) metasummary, and (5) methasynthesis. Depending on the research findings available, the best research evidence might be synthesized by one or more of these five processes. Table 2-4 identifies the processes used in research evidence synthesis, the purpose of each synthesis process, the types of research included in the synthesis (sampling frame), and the analysis techniques used to achieve the synthesis of research evidence (Whittemore, 2005). A systematic review is a structured, comprehensive synthesis of quantitative studies in a particular health care area to determine the best research evidence available for expert clinicians to use to promote an EBP. Systematic reviews are conducted to synthesize research evidence from numerous, high-quality quantitative studies with similar methodologies (Craig & Smyth, 2007). These reviews are often conducted by teams or panels of expert researchers and clinicians, who use the results of these reviews to produce the national and international standardized guidelines for managing health care problems such as hypertension (Chobanian et al., 2003). These standardized guidelines are made available online, published in articles and books, and presented at conferences and professional meetings. Some of the common sources for these standardized guidelines are presented at the end of this chapter.
TABLE 2-4
Processes Used to Synthesize Research Evidence
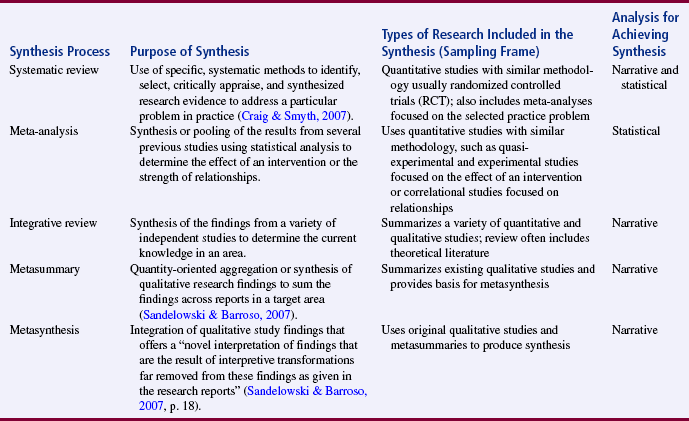
Table adapted from: Craig, J. V., & Smyth, R. L. (2007). The evidence-based practice manual for nurses. Edinburgh: Churchill Livingstone, Elsevier. Sandelowski, M., & Barroso, J. (2007). Handbook for synthesizing qualitative research. New York: Springer Publishing Company. Whittemore, R. (2005). Combining evidence in nursing research: Methods and implications. Nursing Research, 54(1), 56–62.
Meta-analysis is a type of study that statistically pools the results from previous, similar studies into a single quantitative analysis that provides one of the highest levels of evidence for an intervention’s efficacy (Conn & Rantz, 2003). The studies synthesized are usually quasi-experimental or experimental types of studies. In addition, a meta-analysis can be performed on correlational studies to determine the type (positive or negative) or strength of relationships among selected variables (see Table 2-4). Because meta-analyses involve statistical analysis to combine study findings, it is possible to be objective rather than subjective in synthesizing research evidence. Some of the strongest evidence for using an intervention in practice is generated from a meta-analysis of multiple, controlled quasi-experimental and experimental studies. Thus, many systematic reviews conducted to generate evidence-based guidelines include meta-analyses. The process for conducting a meta-analysis is presented in Chapter 27.
An integrative review of research identifies, analyzes, and synthesizes research findings from independent quantitative and qualitative studies to determine the current knowledge (what is known and not known) in a particular area. Most of the studies synthesized in an integrative review are quantitative (descriptive, correlational, quasi-experimental, and experimental), but some reviews also include important findings from qualitative studies and theoretical literature (see Table 2-4). Integrative reviews of research direct future studies and are sometimes included in systematic reviews. The value of an integrative review depends on the standards used to the conduct the review, which is similar to the standards of clarity, rigor, and replication required for conducting primary research. The process for conducting an integrative review of research is presented in Chapter 27.
Qualitative research synthesis is the process and product of systematically reviewing and formally integrating the findings from qualitative studies (Sandelowski & Barroso, 2007). Qualitative research synthesis includes two categories: qualitative metasummary and qualitative metasynthesis (see Table 2-4). Qualitative metasummary is the synthesis or summing of the findings across qualitative reports to determine the current knowledge in an area. Metasummary can be an end in itself to identify current knowledge or can provide a foundation for conducting qualitative metasynthesis. Qualitative metasynthesis provides a fully integrated, novel description or explanation of a target event or experience verses a summary view of that event or experience. Metasynthesis requires more complex, integrative thought in developing a new perspective or theory based of the findings of previous qualitative studies. These qualitative research synthesis processes have been used to generate research evidence that contributes to the knowledge needed for EBP. Sandelowski and Barroso (2007) have developed a book that focuses on the synthesis of qualitative research, and their processes for conducting metasummary and metasynthesis are addressed in Chapter 27.
Levels of Research Evidence
The strength or validity of the best research evidence in an area depends on the quality and quantity of the studies conducted in the area. Quantitative studies, especially experimental studies like the RCT, are thought to provide the strongest research evidence. Also the replication or repetition of studies with similar methodology increases the strength of the research evidence generated. The levels of the research evidence can be thought of as a continuum with the highest quality of research evidence at one end and weakest research evidence at the other (see Figure 2-2) (Craig & Smyth, 2007; Malloch & Porter-O’Grady, 2006; Melnyk & Fineout-Overholt, 2005; Pearson et al., 2007). The systematic research reviews and meta-analyses of high-quality experimental studies provide the strongest or best research evidence for use by expert clinicians in practice. Meta-analyses and integrative reviews of quasi-experimental and experimental studies also provide strong research evidence for managing practice problems. Correlational, descriptive, and qualitative studies direct further research and provide some useful findings for practice (see Figure 2-2). The weakest evidence comes from expert opinions, which can include expert clinicians’ opinions or the opinions expressed in committee reports. When making a decision in your clinical practice, be sure to base that decision on the best research evidence available.
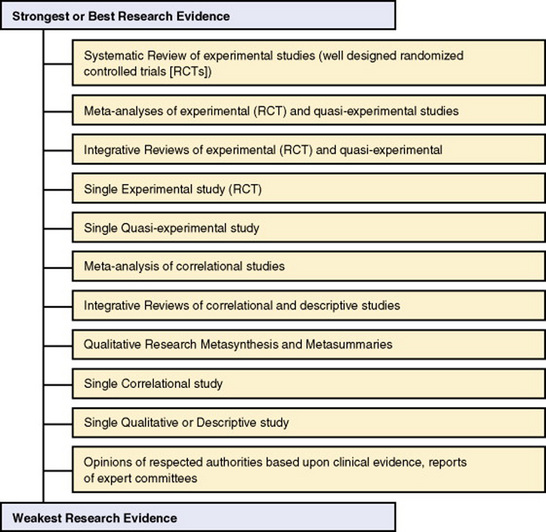
The levels of research evidence identified in Figure 2-2 will help nurses to determine the quality and validity of the evidence that is available for them to use in practice. Advance practice nurses must seek out the best research knowledge available in an area to ensure that they manage patients’ acute and chronic illnesses with a high quality of care (Kania-Lachance, Best, McDonah, & Ghosh, 2006). This best research evidence generated from systematic reviews, meta-analyses, and integrative reviews is used most often to develop standardized or evidence-based guidelines for practice.
Introduction to Evidence-Based Guidelines
Evidence-based practice guidelines are rigorous, explicit clinical guidelines that are based on the best research evidence available in that area. These guidelines are usually developed by a team or panel of expert researchers; expert clinicians (physicians, nurses, pharmacists, and other health professionals); and sometimes consumers, policy makers, and economists. The expert panel seeks consensus on the content of the guideline to provide clinicians with the best information for making clinical decisions in practice. There has been a dramatic growth in the production of evidence-based guidelines to assist health care providers in building an EBP and in improving health care outcomes for patients, families, providers, and health care agencies.
Every year, new guidelines are developed, and some of the existing guidelines are revised based on new research evidence. These guidelines have become the gold standard (or standard of excellence) for patient care, and nurses and other health care providers are encouraged to incorporate these standardized guidelines into their practice. Many of these evidence-based guidelines have been made available online by expert national and international government agencies, professional organizations, and centers of excellence. When selecting a guideline for practice, be sure that a credible agency or organization developed the guideline and that the reference list reflects the synthesis of extensive research evidence.
An extremely important source for evidence-based guidelines in the United States is the National Guideline Clearinghouse (NGC), which was initiated in 1998 by the Agency for Healthcare Research and Quality (AHRQ). The NGC started with 200 guidelines and has expanded to more than 1000 evidence-based guidelines (see www.guideline.gov). Another excellent source of systematic reviews and evidence-based guidelines is the Cochrane Collaboration and Library in the United Kingdom, which can be accessed at www.cochrane.org. Professional nursing organizations, such as the Oncology Nursing Society (www.ons.org) and the National Association of Neonatal Nurses (www.nann.org), have also developed evidence-based guidelines for nursing practice. These websites will introduce you to some of evidence-based guidelines that exist nationally and internationally. Chapter 27 will help you to critically appraise the quality of an evidence-based guideline and implement that guideline in your practice.
SUMMARY
• Florence Nightingale initiated nursing research more than 150 years ago; this was followed by years of limited research until the 1950s. During the 1950s and 1960s, research became a higher priority, with the development of graduate programs in nursing that increased the number of nurses with doctorates and master’s degrees. In the 1970s and 1980s, the major focus was on the conduct of clinical research to improve nursing practice.
• Outcomes research emerged as an important methodology for documenting the effectiveness of health care service in the 1980s and 1990s. In 1989, the Agency for Health Care Policy and Research (AHCPR) was established to facilitate the conduct of outcomes research.
• The vision for nursing in the twenty-first century is the development of a scientific knowledge base that enables nurses to implement an evidence-based practice (EBP).
• Nursing research incorporates both quantitative and qualitative research and two relatively new methodologies, outcomes research and intervention research.
• Quantitative research is classified into four types for this textbook: descriptive, correlational, quasi-experimental, and experimental.
• Qualitative research is classified into six types for this textbook: phenomenological research, grounded theory research, ethnographic research, historical research, philosophical inquiry, and critical social theory.
• Outcomes research focuses on determining the end results of care or a measure of the change in health status of the patient and family.
• Intervention research involves the investigation of the effectiveness of a nursing intervention in achieving the desired outcomes in a natural setting.
• Best research evidence is a summary of the highest quality, current empirical knowledge in a specific area of health care that is developed from a synthesis of high-quality studies (quantitative, qualitative, outcomes, and intervention) in that area. Research evidence in nursing and health care is synthesized using the following processes: (1) systematic review, (2) meta-analysis, (3) integrative review, (4) metasummary, and (5) methasynthesis.
• The levels of the research evidence can be thought of as a continuum with the highest quality of research evidence at one end and the weakest at the other. The best research evidence is synthesized by a team or panel of experts to develop evidence-based guidelines for clinicians in practice.
Abdellah, F.G. Evolution of nursing as a profession. International Nursing Review. 1972;19(3):219–235.
Agency for Healthcare Research and Quality (AHRQ). Agency for Healthcare Research and Quality homepage. Retrieved November 23, 2007, from www.ahrq.gov, 2007.
American Association of Colleges of Nursing (AACN). Position statement on nursing research. Journal of Professional Nursing. 1999;15(4):253–257.
American Nurses Association (ANA). Twenty thousand nurses tell their story. Kansas City: Author, 1950.
American Nurses Association (ANA). Education for participation in nursing research. Kansas City: Author, 1989.
Bauknecht, V.L. Congress overrides veto, nursing gets center for research. American Nurse. 1986;18(1):24.
Baumrind, D. New directions in socialization research. American Psychologist. 1980;35(7):639–652.
Brown, S.A., Grimes, D.E. A meta-analysis of nurse practitioners and nurse midwives in primary care. Nursing Research. 1995;44(5):332–339.
Brown, S.J. Knowledge for healthcare practice: A guide to using research evidence. Philadelphia: W.B. Saunders, 1999.
Brown, S.J. Focus on research methods. Nursing intervention studies: A descriptive analysis of issues important to clinicians. Research in Nursing & Health. 2002;25(4):317–327.
Carlson-Catalano, J., Lunney, M. Quantitative methods for clinical validation of nursing diagnoses. Clinical Nurse Specialist. 1995;9(6):306–311.
Chobanian, A.V., Bakris, G.L., Black, H.R., Cushman, W.C., Green, L.A., Izzo, J.L., et al. The seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. Journal of the American Medical Association. 2003;289(19):2560–2572.
Clark, A.M. The qualitative-quantitative debate: Moving from positivism and confrontation to post-positivism and reconciliation. Journal of Advanced Nursing. 1998;27I(6):1242–1249.
Conduct and Utilization of Research in Nursing (CURN) Project. Using research to improve nursing practice. New York: Grune & Stratton, 1981–1982.
Conn, V.S., Rantz, M.J. Research methods: Managing primary study quality in meta-analyses. Research in Nursing & Health. 2003;26(4):322–333.
Cook, E., Sir., The life of Florence Nightingale, Vol. 1. London: Macmillan, 1913.
Cook, T.D., Campbell, D.T. Quasi- experimentation: Design and analysis issues for field settings. Chicago: Rand McNally, 1979.
Craig, J.V., Smyth, R.L. The evidence-based practice manual for nurses, (2nd ed.). Edinburgh: Churchill Livingstone; 2007.
de Tornyay, R. Nursing research: The road ahead. Nursing Research. 1977;26(6):404–407.
Doran, D.M. Nursing-sensitive outcomes: State of the science. Boston: Jones & Bartlett, 2003.
Downs, F.S., Fleming, W.J. Issues in nursing research. New York: Appleton-Century-Crofts, 1979.
Ellis, R., Philosophic inquiry. Werley, H.H., Fitzpatrick, J.J., eds., Annual review of nursing research, Vol. 1. New York: Springer, 1983:211–228.
Fitzpatrick, M.L. Historical studies in nursing. New York: Teachers College Press, 1978.
Fitzpatrick, M.L. Historical research: The method. In: Munhall P.L., ed. Nursing research: A qualitative perspective. 3rd ed. Sudbury, MA: Jones & Bartlett; 2001:403–415.
Ford-Gilboe, M., Campbell, J., Berman, H. Stories and numbers: Coexistence without compromise. Advances in Nursing Science. 1995;18(1):14–26.
Germain, C.P. Ethnography: The method. In: Munhall P.L., ed. Nursing research: A qualitative perspective. 3rd ed. New York: National League for Nursing; 2001:277–306.
Glaser, B.G., Strauss, A.L. The discovery of grounded theory: Strategies for qualitative research. Chicago: Aldine, 1967.
Gortner, S.R., Nahm, H. An overview of nursing research in the United States. Nursing Research. 1977;26(1):10–33.
Herbert, R.G. Florence Nightingale: Saint, reformer or rebel? Malabar, FL: Robert E. Krieger, 1981.
Horsley, J.A., Crane, J., Crabtree, M.K., Wood, D.J. Using research to improve nursing practice: A guide; CURN Project. New York: Grune & Stratton, 1983.
Institute of Medicine. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press, 2001.
Jacox, A. Strategies to promote nursing research. Nursing Research. 1980;29(4):213–218.
Johnson, J.E. Outcomes research and health care reform: Opportunities for nurses. Nursing Connections. 1993;6(4):1–3.
Johnson, W.L. Research programs of the National League for Nursing. Nursing Research. 1977;26(3):172–176.
Kania-Lachance, D.M., Best, P.J., McDonah, M.R., Ghosh, A.K. Evidence-based practice and the nurse practitioner. The Nurse Practitioner. 2006;31(10):46–53.
Kaplan, A. The conduct of inquiry: Methodology for behavioral science. New York: Chandler, 1964.
Kerlinger, F.N., Lee, H.B. Foundations of behavioral research, (4th ed.). Fort Worth, TX: Harcourt, 2000.
Krueger, J.C., Nelson, A.H., Wolanin, M.A. Nursing research: Development, collaboration, and utilization. Germantown, MD: Aspen, 1978.
Larson, E. Health policy and NIH: Implications for nursing research. Nursing Research. 1984;33(6):352–356.
Malloch, K., Porter-O’Grady, T. Introduction to evidence-based practice in nursing and health care. Sudbury, MA: Jones & Barlett, 2006.
Marshall, C., Rossman, G.B. Designing qualitative research, (4th ed.). Thousand Oaks, CA: Sage, 2006.
McPherson, K., Leydon, G. Quantitative and qualitative methods in UK health research: Then, now and …? European Journal of Cancer Care. 2002;11(3):225–231.
Melnyk, B.M., Fineout-Overholt, E. Evidence-based practice in nursing & healthcare: A guide to best practice. Philadelphia: Lippincott Williams & Wilkins, 2005.
Miles, M.B., Huberman, A.M. Qualitative data analysis: A sourcebook of new methods, (2nd ed.). Beverly Hills, CA: Sage, 1994.
Mundinger, M.O., Kane, R.L., Lenz, E.R., Totten, A.M., Tsai, W., Cleary, P.D., et al. Primary care outcomes in patients treated by nurse practitioners or physicians: A randomized trial. Journal of the American Medical Association. 2000;283(1):59–68.
Munhall, P.L. Research methods: A qualitative perspective, (3rd ed.). Sudbury, MA: Jones & Bartlett, 2001.
National Institute of Nursing Research. National Institute of Nursing Research mission and research agenda. Retrieved November 23, 2007, from www.nih.gov/ninr, 2007.
Newman, M.A. Prevailing paradigms in nursing. Nursing Outlook. 1992;40(1):10–13. 32
Nightingale, F. Notes on nursing: What it is, and what it is not. Philadelphia: Lippincott, 1859.
Norbeck, J.S. In defense of empiricism. Image: Journal of Nursing Scholarship. 1987;19(1):28–30.
Palmer, I.S. Florence Nightingale: Reformer, reactionary, researcher. Nursing Research. 1977;26(2):84–89.
Pearson, A., Field, J., Jordan, Z. Evidence-based clinical practice in nursing and health care: Assimilating research, experience, and expertise. Oxford: Blackwell, 2007.
Rettig, R. History, development, and importance to nursing of outcomes research. Journal of Nursing Quality Assurance. 1991;5(2):13–17.
Sackett, D.L., Straus, S.E., Richardson, W.S., Rosenberg, W., Haynes, R.B. Evidence-based medicine: How to practice & teach EBM, (2nd ed.). London: Churchill Livingstone, 2000.
Sandelowski, M., Barroso, J. Handbook for synthesizing qualitative research. New York: Springer, 2007.
Scheffler, I. Science and subjectivity. Indianapolis: Bobbs-Merrill, 1967.
See, E.M. The ANA and research in nursing. Nursing Research. 1977;26(3):165–171.
Sidani, S., Braden, C.P. Evaluating nursing interventions: A theory-driven approach. Thousand Oaks, CA: Sage, 1998.
Silva, M.C., Rothbart, D. An analysis of changing trends in philosophies of science on nursing theory development and testing. Advances in Nursing Science. 1984;6(2):1–13.
Stetler, C.B. Updating the Stetler model of research utilization to facilitate evidence-based practice. Nursing Outlook. 2001;49(6):272–279.
Stetler, C.B., Marram, G. Evaluating research findings for applicability in practice. Nursing Outlook. 1976;24(9):559–563.
U.S. Department of Health and Human Services. Healthy people 2000. Washington, DC: Author, 1992.
U.S. Department of Health and Human Services. Healthy people 2010. Washington, DC: Author, 2000.
Werley, H.H. Nursing research in perspective. International Nursing Review. 1977;24(3):75–83.
Werley, H.H., Fitzpatrick, J.J., eds. Annual review of nursing research, Vol. 1. New York: Springer, 1983.
Whittemore, R. Combining evidence in nursing research: Methods and implications. Nursing Research. 2005;54(1):56–62.