Qualitative Research Methodology
The methodology of qualitative studies is guided by the broad qualitative research paradigm, as well as by a specific philosophical base (see Chapter 4). Strategies for methods of sampling, data gathering, and analyses are not as tightly controlled as those of the quantitative paradigm. Because data analysis begins as data are gathered, insights from early data may suggest fruitful methods of sampling, data gathering, or analyses that were not originally planned. In qualitative studies, the researcher is free to modify the original methodology based on these insights.
This chapter allows you to understand the process and to envision what the experience will be like if you conduct a qualitative study. However, we suggest that you seek additional sources of guidance for understanding the philosophical base you plan to use, as well as the process of collecting and analyzing qualitative data. Developing a mentorship with someone experienced in the type of qualitative analysis you wish to perform is still the most useful approach to learning these skills (Morse, 1997; Sandelowski, 1997).
The steps of the qualitative research process are similar to those used in quantitative research, which include reviewing the literature, developing a framework, developing objectives or questions, and sampling. These aspects of qualitative studies are explored in the chapters that focus on each of these topics. However, researchers conducting a qualitative study use some methods of data collection and analysis that are unique to qualitative research and will be discussed in this chapter. Other methods, similar to quantitative methods, are applied differently in qualitative studies. Because data analysis occurs concurrently with data collection, the researcher is attempting to simultaneously gather the data, manage a growing bulk of collected data, and interpret the meaning of the data. Qualitative analysis techniques use words rather than numbers as the basis of analysis. However, qualitative researchers need the same careful skills in analytical reasoning as those needed for quantitative analysis. In qualitative analysis, reasoning flows from concreteness to increasing abstraction. This reasoning process guides the organization, reduction, and clustering of the findings and leads to theoretical explanations. Even though the researcher may change data collection or analysis strategies during the study, the process is not as spontaneous and impulsive as one might think. The procedures must be carefully planned.
This chapter begins with a description of some of the frequently used approaches for collecting and analyzing qualitative data. Next, research methodologies and designs of specific approaches are presented. These include phenomenology, grounded theory, ethnographical methodology, historical research methodology, philosophical studies, and critical social theory methodology. The chapter ends with a discussion of issues that are important to qualitative research: theoretical frameworks for qualitative studies, researcher-participant relationships, participatory research, reflexivity, auditability, and appraisal of qualitative studies.
DATA COLLECTION METHODS
Because data collection occurs simultaneously with data analysis in qualitative studies, the process is complex. Collecting data is not a mechanical process that can be completely planned before it is initiated. The researcher as a whole person is totally involved—perceiving, reacting, interacting, reflecting, attaching meaning, and recording. Such is the case whether the study involves observing and participating in social situations, as would occur in phenomenological, grounded theory, ethnographical, or critical social theory research, or whether the study deals with written communications, as might occur in phenomenological, historical, philosophical, or critical social theory studies. For a particular study, the researcher may need to address data collection issues related to relationships between the researcher and the participants, reflections of the researcher on the meanings obtained from the data, and management and reduction of large volumes of data. Methods of gathering data include making unstructured observations, conducting unstructured interviews, observing focus groups, collecting stories, constructing life stories, and interpreting case studies.
Unstructured Observations
Unstructured observation involves spontaneously observing and recording what one sees with a minimum of planning. Although unstructured observations give the observer freedom, there is a risk that the observer may lose objectivity or may not remember all of the details of the event. If possible, the researcher should take notes during the observation periods. If this is not possible, the researcher needs to record the observations soon afterward. You may even find it useful to photograph or videotape the observation period so that you can examine it extensively at a later time (Harrison, 2002; Mullhall, 2002).
Unstructured observations are not unsystematic or sloppy as the term might suggest. Rather, unstructured means that the researcher has few predetermined notions as to what he or she might observe. What notions the researcher does have may change over time as data are collected. As Mulhall (2003) pointed out:
The way people move, dress, interact and use space is very much a part of how particular social settings are constructed. Observation is the key method for collecting data about such matter…. Observers have a great degree of freedom and autonomy regarding what they choose to observe, how they filter that information, and how it is analysed.… Observation also captures the whole social setting in which people function, by recording the context in which they work…. Finally, observation is valuable because it informs about the influence of the physical environment. This aspect of observation is quite lacking in nursing research. Observations are made of people’s behaviour, but data about the physical environment seldom are collected. (pp. 307, 308)
Hamilton and Manias (2007) studied the observational methods of psychiatric nurses and their invisibility in an acute inpatient setting. This excellent study not only gives you as reader a clear understanding of the careful observation conducted during this study, but it also enables you to understand how detailed observation must be in a qualitative study and gives you a chance to think about how you might conduct your own observations. Hamilton and Manias (2007) described their study as follows.
The postmodern approach used in the study was informed by Foucault (1973, 1980, 1995, 1994) and by researchers after him (Fox, 1993; Rhodes, 1991; Silverman, 2005). A postmodern epistemology informed both the positioning of the first author during fieldwork and the emphasis on discourses, power relations and particular concepts in data analysis. A postmodern epistemology informed both the positioning of the first author during fieldwork and the emphasis on discourses, power relations and particular concepts in data analysis. In postmodern ethnography, the ethnographers’ power in the portrayal of the field is made explicitly (Alvesson, 2002). Accordingly the first author, an experienced psychiatric nurse, was cast as an objective observer, but as an active participant, recognizing and exposing her own subjectivity in shaping the research. (p. 334)
The study was based in a 44-bed acute psychiatric inpatient unit, on the site of metropolitan acute teaching hospital in Victoria, Australia. Ethics approval was gained from the hospital, in accordance with national guidelines in Australia.
Ethnography has been widely used to study workplaces as subcultures (Silverman, 2005). This study centered on the work of 11 participating psychiatric nurses and the first author, who worked part time as a psychiatric nurse alongside the participants for 18 months. Fieldwork data were generated through: participant observations (180 h; 13 individual interviews and two focus groups with the participating psychiatric nurses; transcriptions of their file notes and other documents related to assessment; and the first author’s journal that detailed 170 h of her work as a registered nurse in the unit. (p. 334)
The ethnography focused on nurses’ activities and on nurse-nurse and nurse-patient interactions. The psychiatric nursing experience of the 11 nurses recruited ranged from 2 to 30 years and ages ranged from 28 to 67 years. Six nurses were women, a gender ratio in keeping with the current psychiatric nursing workforce in Australia (Clinton, 2001), which includes a much higher proportion of men than in other specialties of nursing. Nurse participants were positioned as key informants who provided insight into the social life of the unit (Riley & Manias, 2006). Participant observations extended across participants’ rostered working shifts, through all days of the week and all three shifts (morning, afternoon and night), in order to attend to a variety of contexts, routines, experiences and practices. (p. 334)
Central to our analysis of how inpatient psychiatric nurses observed patients were the Foucauldian concepts of the gaze and of discipline, both given form in nurses’ discursive practices (Roberts, 2005). Analysis was focused on discursive practices of assessment, understood to be the micro-politics of nurses’ language and action (Fox, 1993, p. 161). Everyday nursing practices identified in the fieldwork texts were highlighted as discursive practices when we could show how these practices were imbued with power through social, historical and political conditions, and in the wider context of psychiatric discourse (Irving, 2002). (pp. 334–335)
We present three identified modes of nurses’ observations: nurses’ scanning of patients, nurses’ obvious and direct probing of patients, and nurses’ discreet and hidden observations of patients.
The term scan is used here to encompass nurses’ frequent sweeping of eyes across rooms, surfaces and spaces of the unit, taking in features and contents of the space as well as impressions of the people occupying it. Nurses relied on their sight, supplemented by other senses to inform the scan. Through scanning, nurses monitored the physical spaces and their objects, commenting on noise, smells and temperature, and noticing and moving hazards. Nurses also scanned for emotional tone in the unit: for potential areas of distress and conflict that might encompass patients, staff and visitors. The nurses’ scan took in the demeanour and behaviour of individual patients and groups of patients. Nurses scanned in passing patients’ bodies, expressions, movements, gestures and tones of voice…
…nurses’ visual observations were supplemented by their tuning into sounds of movement, or ‘listening in’ to patients talk. Whether in the office or circulating in the unit, nurses were alert to voices and other sounds in the ward environment. Three nurses might all glance or move toward a doorway, in response to a sound such as a heavy footfall, even as they were engaged in other work. Nurses gleaned valuable information about patients through this form of aural surveillance (Riley, 2005), a partner to their visual surveillance. Nurses embraced their scanning role, to the extent that they permitted sounds and conversations to frequently interrupt their own planned work. They were often drawn away from planned work to go and see the event or person at the source of an interruption.
Nurses scanned the unit on arrival, when entering a different area of the unit, or when returning after an absence, such as a tea break. Their scan was brief, capturing the physical and social condition of the unit at that moment. From such activity, details were reported to colleagues, in snatches of conversation and handovers. Nurses exercised the scan both as a baseline form of monitoring and as a prelude to more focused work with individuals and groups of patients, assisting them to determine work priorities and issues for the working shift. (p. 336)
Nurses’ Probing Observations of Patients
Nurses focused on patients who were assigned to their care. As they scanned the ward space and occupants, their attention was drawn also to patients who were assigned to other nurses. The probing observation of a patient was a distinctive activity in that nurses stopped circulating, and looked in a more considered way at a patient’s body, social interactions and behaviour. From this probing, nurses gleaned clues about the patient’s feelings, thoughts and motivations, the patient’s ways of interacting, the patient’s coping abilities or strengths, as well as evidence of symptoms. On occasions, nurses withdrew after a period of sharp observation, without interrupting the patient’s activity or speaking at all … (p. 337)
Through observations, nurses elicited evidence of symptoms and also absence of symptoms. Nurses identified evidence of the person ‘getting along’ in the social sense with other patients, of the person coping with the demands of an activity and even exhibiting prowess in the activity. Nurses’ counterbalancing of psychiatric symptoms with a lack of such symptoms, coping and prowess, in the context of unstructured activity, was an element of nurses’ assessment. Nurses’ accounts of symptoms, based in the behaviour they observed in the unit, were potentially important accounts in the ongoing construction of illness by the treating team. (p. 337)
Nurses’ Discreet Observation: Clinical and Civil Surveillance
Nurses’ observations of patients in the acute psychiatry unit were shaped substantially by the legal status and admission circumstances of patients, most of whom were detained and treated under the Mental Health Act (1986). The loss of fundamental rights to freedom and choice in psychiatric treatment could cause great offence to patients, many of whom flatly disagreed with the medical diagnosis and bitterly resented being detained and given psychotropic medications.
The ward environment was a place where direct contact with clinicians frequently provoked patients’ ire. Since nurses were the group of clinicians in most frequent and close contact with patients, they were attuned to and dealt with patients’ rising emotions by avoiding direct discussion about the terms and legitimacy of their hospital admission, including discussion of symptoms, in marked contrast to the probing of psychiatrists or psychologists. Evasion and distraction were common strategies used by nurses, in the moment-to-moment and daily work of maintaining civility and relative calm among inhabitants of the unit, in the face of such a perennial conflict of views.
In the process of examining a patient and with the main aim of not angering the patient, nurses often avoided looking directly at a patient, instead glancing briefly or discreetly…. A feature of surveillance was the nurses’ ability to tune in to patient conversations at some distance, or whilst engaged in another conversation themselves. Being the third party to patient’s talk gave nurses material from which to construct two valued forms of knowledge: patients’ speech related to mental status and patients’ coping ability in social situations. (p. 338)
Unstructured Interviews
Unstructured interviews are used primarily in descriptive quantitative and qualitative studies. According to market research, in-depth interviews provide more quality data for less money than do focus groups (Palmerino, 1999). However, the interviewer seeks information from a number of individuals, whereas the focus group strategy is designed to obtain the perspective of the normative group, not individual perspectives.
Learning to Interview
Interviewing is a skill. Researchers must give themselves the opportunity to develop this skill before they initiate an interview for a study. A skilled interviewer can elicit higher-quality data than an inexperienced interviewer. Unskilled interviewers may not know how or when to intervene, when to encourage the participant to continue to elaborate, or when to divert to another subject. The interviewer must know how to handle intrusive questions.
Establishing a Positive Environment for an Interview
When preparing for an interview, establish an environment that encourages a comfortable conversation. If you are going to audio- or videotape the exchange, make sure that the recording equipment is placed unobtrusively. Likewise, using batteries rather than plug-in sources of power tends to be less intrusive. A sensitive microphone will allow you to pick up even faint or distorted voices, thereby increasing your ability to make an accurate transcription later.
Conducting an Effective Interview
For practice, conduct interviews with individuals who meet the sampling criteria. These rehearsals will help you to identify problems before initiating the study. Practice sessions also allow you to determine a realistic time estimate for the interviews.
There are power issues in an interview. As the researcher, you have the power to shape the interview agenda. Participants have the power to choose the level of responses they will provide. You might begin the interview by asking a broad question such as “Describe for me your experience with…” or “Tell me about…” Ideally, the participant will respond as though she or he is telling a story. It is important that the narrative be from the participant’s, and not the interviewer’s, perspective. Ask your interviewees to speak freely about their experiences.
Once the interview begins, the role of the interviewer is to encourage the subject to continue talking. Nod your head or make sounds that indicate interest. When it seems appropriate, encourage your subject to elaborate further on a particular dimension of the topic (known as probing). Participants may need validation that they are providing the needed information. Some participants may give short answers, so you may need to encourage them to elaborate. The interviewer becomes a detective in his or her search for important information. McEvoy (2001) pointed out that the interviewer is not after factual information. From the perspective of qualitative research, interviews generate socially constructed knowledge. The interviewer influences the interviewee in terms of “how she or he listens, attends, encourages, interrupts, digresses, initiates topics and terminates responses” (p. 51).
Problems with Interviewing
You may encounter some challenges during an interview. Common problems include interruptions such as telephone calls, “stage fright” that often arises when the participant realizes he or she is being recorded, failure to establish a rapport with your subject, verbose participants, and those who tend to wander off the subject. You may need to tactfully guide the interview back to the topic. If the participant is emotionally distressed as a result of the interview, remain with the individual until the participant is able to restore his or her composure. Researchers and interviewers tend to underestimate the amount of time required for an interview. If the participant is hurried, the quality of data is affected.
When the study focuses on families, issues arise regarding which members are interviewed. In some cases, a single member is selected to represent the family. This strategy biases the results because other family members may have different perspectives of the situation. Select two family members and interview each separately. The best strategy, of course, is to interview each member separately, but this requires an inordinate amount of time (Astedt-Kurki, Paavilainen, & Lehti, 2001).
Particular concerns arise when a researcher is interviewing colleagues. The interviewer (an insider) lacks the social distance that facilitates a balanced, objective perspective. Common experiences tend to be taken for granted. Aspects of the social world that should be questioned are overlooked. You may find it difficult to ask questions about sensitive issues of someone in your own social group. However, there are advantages. Because of their unique position, insiders are familiar with the social world and thus can interpret and attach meaning that may elude an outsider. As an insider, you may find that you read between the lines of participants’ comments rather than taking them at face value. This capability may be particularly important if the group under study is a minority group or otherwise marginalized (McEvoy, 2001).
From an ethical perspective, interviews tend to be viewed as noninvasive and thus as posing no threat to the interviewee. However, interviews are an invasion of the psyche. For some, this may be therapeutic. However, an interview is capable of producing risks to the health of the participant. Therefore, the interviewer must always avoid inflicting unnecessary harm upon the participant (Munhall, 1991; Sullivan, 1998).
The data you obtain are affected by characteristics of the person being interviewed. These may include age, ethnicity, gender, professional background, educational level, and relative status of interviewer and interviewee, as well as impairments in vision or hearing, speech impediments, fatigue, pain, poor memory, disorientation, emotional state, or language difficulties. Interviews with children may require special considerations (Deatrick & Ledlie, 2000). In some studies, interviewers may be profoundly affected by participants’ stories and may need debriefing. This need may extend to those transcribing the interviews and to researchers analyzing the data. Because of privacy issues, study participants are not able to share their feelings with those who usually provide support and comfort. In these cases, a person or persons should be designated to address these needs (Moyle, 2002; Price, 2002; Sullivan, 1998; Wilmpenny & Gass, 2000).
Berg (1998) has identified the following “ten commandments” of interviewing:
1. Never begin an interview cold. Remember to spend several minutes chatting and making small talk with the subject. If you are in the subject’s home, use what’s there for this chatting. Look around the room and ask about such things as photographs, banners, books, and so forth. The idea here is to set the subject at ease and establish a warm and comfortable rapport.
2. Remember your purpose. You are conducting an interview in order to obtain information. Try to keep the subject on track, and if you are working with an interview schedule, always have a copy of it in front of you—even though you should have your questions memorized.
3. Present a natural front. Because your questions are memorized, you should be able to ask each one as if it had just popped into your head. Be relaxed, affirmative, and as natural as you can.
4. Demonstrate aware hearing. Be sure to offer the subjects appropriate nonverbal responses. If they describe something funny, smile. If they tell you something sad, look sad. If they say that something upset them, try to console them. Do not present yourself as uninterested or unaware.
5. Think about appearance. Be sure you have dressed appropriately for both the setting and the kind of subject you are working with. Generally, business attire is most appropriate. If you are interviewing children, a more casual appearance may be more effective. Remember to think about how you look to other people.
6. Interview in a comfortable place. Be sure that the location of the interview is somewhere the subject feels comfortable. If the subject is fearful about being overheard or being seen, your interview may be over before it ever starts.
7. Don’t be satisfied with monosyllabic answers. Be aware when subjects begin giving yes-and-no answers. Answers like these will not offer much information during analysis. When this does occur, be sure to probe with questions such as, “Can you tell me a little bit more about that?” or “What else happened?” Even a simple pause and an uncomfortable silence might yield additional information.
8. Be respectful. Be sure the subject feels that he or she is an integral part of your research and that any answer he or she offers is absolutely wonderful. Often subjects will say things like, “You don’t really want to know how I feel about that.” Assure them that you really do!
9. Practice, practice, and practice some more. The only way to actually become proficient at interviewing is to interview. Although this book [Berg, 1998] and other manuals can offer guidelines, it is up to you as a researcher to develop your own repertoire of actions. The best way to accomplish this task is to go out and do interviews.
10. Be cordial and appreciative. Remember to thank the subject when you finish, and answer any questions he or she might have about the research. Remember, you are always a research emissary. Other researchers may someday want to interview this subject or gain access to the setting you were in. If you mess things up through inappropriate actions, you may close the door for future researchers. (Berg, 1998, pp. 87–88)
The following is an abstract of a study on Ph.D.- prepared nurses in the clinical setting (McNett, 2006).
Focus Groups
Focus groups were designed to obtain the participants’ perceptions in a focused area in a setting that is permissive and nonthreatening. One of the assumptions underlying the use of focus groups is that group dynamics can help people to express and clarify their views in ways that are less likely to occur in a one-to-one interview. The group may give a sense of “safety in numbers” to those wary of researchers or those who are anxious.
Focus groups are a relatively recent strategy that was used initially in nursing studies in the late 1980s. However, they have been used in other fields for a long time. The idea of focus groups emerged in the 1920s as an approach for examining the effectiveness of marketing strategies. The concept reemerged during World War II with efforts to determine ways to improve the morale of the troops. The technique serves a variety of purposes in nursing research. It has been used to perform qualitative studies (Twinn, 1998), make policy analyses (Straw & Smith, 1995), assess consumer satisfaction, evaluate the quality of care (Beaudin & Pelletier, 1996), examine the effectiveness of public health programs, assist in professional decision making (Bulmer, 1998; Southern et al., 1999), develop instruments, explore patient care problems and strategies for developing effective interventions, develop education programs (Halloran & Grimes, 1995), and study various patient populations (Disney & May, 1998; Goss, 1998; Quine & Cameron, 1995; Reed & Payton, 1997). It has also been employed as a data collection strategy in participatory research. A focus group study might include from 6 to 50 groups.
The following assumptions underlie focus groups (Morrison & Peoples, 1999):
1. A homogeneous group provides the participants with freedom to express thoughts, feelings, and behaviors candidly.
2. Individuals are important resources of information.
3. People are able to report and verbalize their thoughts and feelings.
4. A group’s dynamics can generate authentic information.
5. Group interviews are superior to individual interviews.
6. The facilitator can help people recover forgotten information by focusing the interview.
The effective use of focus groups requires careful planning. Questions that must be addressed include the following:
1. What are the aims of the focus groups?
2. How many focus groups should be assembled?
3. How many individuals should be in each focus group?
4. How will you recruit for the focus groups?
5. Can you locate sufficient people for the focus groups?
6. Are you selecting the right people for the focus groups?
7. Where should the focus groups meet?
8. What skills should the groups’ moderators have?
9. How will moderators interact with participants?
Many different communication forms are used in focus groups, including teasing, arguing, joking, anecdotes, and nonverbal approaches such as gesturing, facial expressions, and other body language. Kitzinger (1995, pp. 299–300) has suggested that
people’s knowledge and attitudes are not entirely encapsulated in reasoned responses to direct questions. Everyday forms of communication may tell us as much, if not more, about what people know or experience. In this sense focus groups reach the parts that other methods cannot reach, revealing dimensions of understanding that often remain untapped by more conventional data collection techniques. (full text available in Health Source Nursing/ Academic edition)
Recruiting appropriate participants for each of the focus groups is critical, because recruitment is the most common source of failure. Each focus group should include 6 to 10 participants. If there are fewer participants, the discussion tends to be inadequate. In most cases, participants are expected to be unknown to each other. However, when targeting professional groups such as clinical nurses or nurse educators, such anonymity usually is not possible. You may use purposive sampling to seek out individuals known to have the desired expertise. In other cases, you may look for participants through the media, posters, or advertisements. A single contact with an individual who agrees to attend a focus group does not ensure that this person will attend the group session. You will need to make repeated phone calls and remind the candidates by mail. Inform them at the time of consent that you will be calling to remind them of the group and to verify that the phone number they gave you is the best number to call. You may need to offer incentives. Cash payments are, of course, the most effective if the resources are available through funding. Other incentives include refreshments at the focus group meeting, T-shirts, coffee mugs, gift certificates, or coupons. Overrecruiting may be necessary; a good rule is to invite two more potential participants than you need for the group (Morgan, 1995).
Segmentation is the process of sorting participants into focus groups with common characteristics. Selecting participants who are similar to each other in lifestyle or experiences, views, and characteristics facilitates more open discussion. And you can increase the group’s validity by conducting multiple focus groups and placing participants with differing characteristics into separate groups. These characteristics might be age, gender, social class, ethnicity, culture, lifestyle, or health status. Strickland (1999) pointed out the problems that could occur if differing cultural groups are included in the same focus group. Communication patterns, roles, relationships, and traditions might interfere with the interactions within the focus group. In some cases, groups may occur naturally such as those who work together. Be cautious about bringing together participants with considerable variation in social standing, education, or authority because some group members may hesitate to participate fully, whereas others may discount the input of those with perceived lower standing (Kitzinger, 1995; Morgan, 1995).
Establish a setting for your focus group that is relaxed. There should be space for participants to sit comfortably in a circle or U-shape and maintain eye contact with all participants. Ensure that the acoustics of the room will allow you to obtain a quality tape recording of the sessions. As with the one-on-one interview discussed earlier, place your tape or video recorders unobtrusively, and use batteries rather than plugging your equipment into a power source as this is less invasive. Use a highly sensitive microphone. However, it may be necessary for the moderator or assistant moderator to take notes when the speaker’s voice is soft or when several individuals are speaking at once. Making notes on the dynamics of the group is also useful. Note how group members interact with one another. Sessions will usually last 1 to 2 hours, although some may extend to an entire afternoon or continue as part of a series of meetings.
It is important for the researcher to clarify the aims of the focus groups and communicate these aims to the moderators and the participants before the group session. Instruct participants that all points of view are valid and helpful and that speakers should not have to defend their positions. Make clear to the group that the facilitator’s role is to moderate the discussion, not to contribute. Carefully plan the questions that are to be asked during the focus group, and, if time permits, pilot-test them. Limit the number of questions to those most essential so that sufficient time is left for discussion. You may elect to give participants some of the questions before the group meeting to enable them to give careful thought to their responses. Questions should be posed in such a way that group members can build on the responses of others in the group, raise their own questions, and question each other. Probes can be used to elicit richer details using questions such as “How would that make a difference?” or “What makes you think that?” “Why” questions are not good because they tend to push a participant toward taking a stand and defending it. Then it is difficult to move away from the stand if the group begins moving toward some consensus. The act of questioning or challenging ideas offers a stimulating learning experience for group members. Their thinking may be supported or tested, and participants may be presented with new ways of thinking about a problem (Hollis Openshaw, & Goble, 2002).
A common problem in focus groups is to dive right into the topic of interest to the researcher with little emphasis on the interests of the participants. Early in the session, provide opportunities for participants to express their views on the topic of discussion. Next, proceed with the questions. Use probes if the discussion wanders too far. A good facilitator will weave questions into the discussion naturally. The facilitator’s role is to clarify, paraphrase, and reflect back what group members have said. These discussions tend to express group norms, and individual voices of dissent may be stifled. However, when the discussion is on sensitive topics, the group may actively facilitate the discussion because less inhibited members break the ice for those who are more reticent. Participants may also provide group support for expressing feelings, opinions, or experiences. Late in the session, the moderator may encourage group members to go beyond the current discussion or debate and discuss inconsistencies among participants and within their own thinking. The moderator can use disagreements among group members to encourage participants to state their points of view more clearly and provide a rationale for their position (Kitzinger, 1995).
Moderator Role
Selecting effective moderators is as critical as selecting appropriate participants. The moderator must encourage participants to talk about the topic. Sim (1998) pointed out that “the focus group moderator will influence powerfully the process of interaction that takes place, and the way in which the moderator behaves, and the verbal and non-verbal cues that he or she gives to the group, are crucial in this respect” (p. 347). Because expertise in the topic may make participants reluctant to speak, the moderator should make it clear that he or she is there to learn from the group members. In some cases, you will want to include an assistant moderator as well as a moderator. Participants should be encouraged to talk to one another rather than addressing all comments to the moderator. A successful moderator encourages participants to interact with one another, formulates ideas, and draws out cognitive structures not previously articulated. Moderators should remain neutral and nonjudgmental. If the topic is sensitive, moderators need to be able to put participants at ease. To accomplish this goal, use a moderator with characteristics similar to those of the group participants. Extreme dominance or extreme passiveness on the part of the moderator will lead to problems (Kitzinger, 1995; Morgan, 1995; Morrison & Peoples, 1999).
Data Collection
Sim (1998) recommended that the following data be collected:
2. How participants interact with one another
3. Accurate attribution of quotations to individual group members
Data collection should not interfere with the coordination of the group. The method of data collection should not have reactive effects on the participants.
Berg (1998), citing the work of Reinharz (1992) and Kramer (1983), suggested using a computer group diary as a strategy, combining focus group interviewing and unobtrusive observation to gather information. Participants are given a web site where each individual can enter his or her thoughts. All participants have access to each participant’s comments and can enter their own thoughts or respond to comments of others. Thus, these become unguided focus groups in which the discourse is “similar to synergistically created convergence of ideas and experiences” (Berg, 1998, p. 108).
Kelly and Patterson (2006) conducted a study titled “Childhood Nutrition: Perceptions of Caretakers in a Low-Income Urban Setting” in which they used focus groups. The following abstract describes their research.
Collecting Stories
During observation and interviewing, the researcher may record stories shared by participants. Banks-Wallace (1998) described a story as “an event or series of events, encompassed by temporal or spatial boundaries, that are shared with others using an oral medium or sign language. Storytelling is the process or interaction used to share stories. People sharing a story (storytellers) and those listening to a story (storytakers) are the main elements of storytelling” (p. 17). Stories can help researchers to understand a phenomenon of interest. In some qualitative studies, the focus of the research may be the gathering of stories. Gathering of stories can enable health care providers to develop storytelling as a powerful means to increase insight and promote health behavior in clients. For example, Nwoga (1997, 2000) studied how African-American mothers use storytelling to guide their adolescent daughters regarding sexuality. The stories could assist other mothers who are struggling to help their daughters deal with sexuality issues.
Coffey and Atkinson (1996) discussed the importance of capturing stories in qualitative studies.
Mattingly and Lawlor (2000) described their research in which they solicit “illness stories.” These authors skillfully guide you in interpreting the process of the story, identifying key turning points as the story progresses.
Constructing Life Stories
A life story is designed to reconstruct and interpret the life of an ordinary person. The methodology, which emerged from history, from anthropology, and more recently from phenomenology, has been described by a number of scholars (Bateson, 1989; Bertaux, 1981; Frank, 1979; Gergen & Gergen, 1983; Josselson & Lieblich, 1995; Linde, 1993; Mattingly & Garro, 1994; Polkinghorne, 1988; Sarbin, 1986; Tanner et al., 1993; Ventres, 1994). The life story can be used to clarify the meanings of various states of health, chronic illness, and disability in the lives of patients, their families, and other caregivers. These stories can help us understand the meaning to patients of their health behavior, lifestyles, illnesses, or impairments; the meaning of symptoms; their experiences of treatment; how they adapt; and their hopes and possibilities of reconstructing their lives. Interviews are tape-recorded and transcribed. Notes from observations may be important, and personal documents such as diaries or historical records may be used. Analysis involves more than just stringing events together; events should be linked in an interpretation through which the researcher can create theoretical sense. Materials are organized and analyzed according to theoretical interests. Constructing a life story often requires a long-term contact and extensive collaboration with the participant (Frank, 1996; Larson & Fanchiang, 1996; Mallinson, Kielhofner, & Mattingly, 1996).
Roesler (2006) provided a life story of Herr Bittner in an article describing a narratological methodology for identifying archetypal story patterns in autobiographical narratives. The article is translated from German.
Case Studies
A case study examines a single unit within the context of its real-life environment. The unit may be a person, a family, a nursing unit, or an organization. In the early twentieth century, the most common nursing study was a case study. Medical case studies were also common. Nursing case studies were published in the American Journal of Nursing and initiated a variety of nursing studies of patient care. As nursing research began to use more rigorous methods, the case study fell into disrepute. However, the importance of information from case studies is again being recognized. Case studies can use quantitative, qualitative, or mixed methods of data collection. It is important for the researcher to consider the multiple aspects that affect a particular case and to include this essential information in the plan for data collection and analysis.
Research questions, as well as the qualitative method chosen for the study, guide the data collection. However, as with most qualitative studies, as an understanding of the situation begins to emerge, other questions arise and new data may be gathered to address the new question. A researcher might want to understand the multiplicity of factors that affect patient care, all of the elements that affect the emotional state of a person with a particular illness, or the factors that affect learning from a particular approach to patient education. Factors might include the social and political environment in which care is being provided. Thus, identifying all of the variables to be examined is a critical component to planning the study. Multiple sources of information for as many of the variables as possible give the study greater validity. This is referred to as data triangulation. A field diary is also useful because insights can be recorded as they occur. The researcher might also recognize new variables that need to be examined. Personal response to events should also be recorded. If the case is a person, multiple interviews may need to be conducted, requiring a strong commitment from the respondent. Documentary evidence is also a valuable source of details related to the case. Analysis focuses on providing a rich, in-depth description of the case. Generalization, as with many qualitative studies, is not possible. However, comparisons with similar situations are sometimes possible.
Benderix and Sivberg (2007) provided an example of a case study.
DATA MANAGEMENT AND REDUCTION
Using the Computer for Qualitative Analysis
Traditionally, qualitative data collection and analysis were performed manually. The researcher recorded the data on small bits of paper or note cards, which were then carefully coded, organized, and filed at the end of a day. Manual analysis requires cross-checking each bit of data with all the other bits of data on little pieces of paper. It is easy to lose data in the mass of paper. Keeping track of connections between various bits of data requires meticulous record keeping. This method was developed because it was important for the qualitative researcher to maintain a close link with—or become immersed in—the data being analyzed.
Some qualitative researchers believe that using the computer can make analysis of qualitative data quicker and easier without the researcher losing touch with the data (Anderson, 1987; Miles & Huberman, 1994; Pateman, 1998; St John & Johnson, 2000; Taft, 1993). Taft has suggested that because of the ease of coding and recoding, the researcher feels more free to play with the data and experiment with alternative ways of coding. This freedom fosters analytical insight and thus facilitates data analysis. Researchers can also search for codes that tend to occur together. Also, easy access to the data facilitates team research. Pateman (1998; full text available in Nursing Collection) suggested that “some would argue that scientific, mathematically-minded people are more computer literate than those with more artistic, humanistic interests, in which case affinity with computing may have something to do with personal traits.… Some of the … arguments [by qualitative researchers against using computers] could simply be rationalisation by computer-phobic researchers.” However, Taft expressed concern about the dark side of computer technology for qualitative researchers. The researcher may be tempted to study larger samples and sacrifice depth for breadth. Meaningful understanding of the data may also be sacrificed. Sandelowski (1995a) expressed concern that the use of computers will alter the aesthetics of qualitative research and suggested that the key motivation for using computer technology in qualitative research is to legitimize the claim that qualitative researchers are doing science. She stated, “computer technology permits qualitative researchers to have computer printouts of data (with the veneer of objectivity they confer) comparable to their quantitative counterparts whose claims to doing science are often not questioned. Even so-called soft data can become hard when produced by hardware. Qualitative work can now have the look and feel, or aesthetic features, of science” (p. 205).
The computer can assist researchers in activities such as processing, storage, retrieval, cataloging, and sorting and leaves the analysis activities up to the researcher. Anderson (1987) pointed out that “the computer does not perform the thinking, reviewing, interpretative, and analytic functions that the researcher must do for himself or herself. Rather, the computer makes the researcher more efficient and effective in those high-level functions, and eases some of the tedious ‘mindless’ tasks that otherwise consume so much time and energy” (pp. 629–630). However, Sandelowski (1995a) has argued that replacing and streamlining the cutting and pasting activities may be seen as desirable by some because they are uncomfortably reminiscent of childhood play. She argued against the claim that machine technology saves human labor and suggested that it may actually increase labor because more data are stored and retrieved and once the data are stored, one has more of a sense that it must all be accounted for in the report of results.
Computer use has several advantages over the more traditional methods of recording and storing data. Multiple copies can be made with ease, and files can be copied onto backup disks and stored at another site without the need for a large amount of storage space. Blocks of data can also be moved around in the file or copied to another file when data are being sorted by category. The same block of data could be inserted within several categories, if desired. At the same time, interviews or descriptions of observations can be kept intact for reference as needed. In addition, most word processing programs can perform sort operations and can search throughout a text file for a selected word or a string of words. Many of these activities can be performed with a traditional word processing program (Burnard, 1998). Files in a word processing program can be transferred to a database spreadsheet such as Excel, dBase, or Lotus 1–2–3 to organize the data into matrices.
A number of computer programs have been developed specifically to perform qualitative analyses. Podolefsky and McCarty (1983) described one of the earliest attempts. This program, Computer Assisted Topical Sorting (CATS), allowed users to insert codes, designated as numbers, into a text file. A mainframe text editor gave users the capacity to search for strings of characters such as words or phrases. St John and Johnson (2000) explored the pros and cons of various data analysis software for qualitative research.
Transcribing Interviews
Tape-recorded interviews are generally transcribed word for word. Field and Morse (1985) provided the following instructions for transcribing a tape-recorded interview.
Sandelowski (1994) indicated that the researcher must choose which features about the interview to preserve in print. These choices directly influence the nature and direction of the analysis. Once the interview has been transcribed, the transcript takes on an independent reality and becomes the researcher’s raw data. Sandelowski suggested that the process of transcription alters reality. The text is “many transformations removed from the so-called unadulterated reality it was intended to represent” (p. 312). She recommended asking the following questions regarding transcription:
1. Is a transcript necessary to achieve the research goals?
2. If a transcription is required, what features of the interview event should be preserved (if at all possible) and what features can be safely ignored?
3. What notation system should be used?
4. What purposes besides investigator analysis per se will the transcript serve? (Sandelowski, 1994, pp. 312–313)
Sandelowski pointed out that transcriptions require about 3.5 hours for each 1 hour of interview time. The cost for this work may be $20/hour for an experienced typist.
Hutchinson (2005) has developed an innovative method of data analysis that uses audio-editing software to save selected audio bytes from digital audio recordings. The data are never transcribed but remain in audio form. A database is used to code and manage the linked audio files and generate detailed and summary reports. Although the system is time consuming to set up, it negates the need for expensive and time-intensive transcription of recorded data.
Listen to the tape recordings as soon after the interview as possible. Listen carefully to voice tone, inflection, and pauses of the researcher and the participant, as well as the content. These features may indicate that the topic is very emotional or very important. While you are listening, read the written transcript of the tape. Make notations of your observations on the transcript.
Ayers and Poirier (1996) pointed out that “qualitative analysis results from the recontextualization of chunks of data, always with the caveat that the new context must in some way be faithful to its origins. Narrative data are meaningless without context” (p. 164). Using the reader response theory emerging from the work of Iser (1980) and Kermode (1983), Ayers and Poirier indicated that “the meaning of a text arises from the interaction of the mind (including the personal history) of the reader with the content of the text (which in turn arose from the mind and personal history of the interview respondent)” (p. 164). Reading the text results in an interaction between the mind and personal history of the respondent and the mind and personal history of the researcher. This interaction results in the emergence of a “virtual text,” which is the entity being interpreted. Thus, there is no real objective, authentic information from which only one correct interpretation can be made. The text does not explain everything. “Motives, histories, antecedents, and causal links, sometimes entire subplots are left to the reader, to the researcher, to infer” (Ayers & Poirier, 1996, p. 165). The process of interpretation occurs in the mind of the reader. The virtual text grows in size and complexity as the researcher reads and rereads. Throughout the process of analysis, the virtual text develops and evolves. Although multiple valid interpretations may occur if different researchers examine the text, all findings must remain trustworthy to the data. This trustworthiness applies to the unspoken meanings emerging from the totality of the data, not just the written words of the text.
Immersion in the Data
Data collected during a qualitative study may be narrative descriptions of observations, transcripts from tape recordings of interviews, entries in the researcher’s diary reflecting on the dynamics of the setting, or notes taken while reading written documents. In the initial phases of data analysis, you need to become familiar with the data as you gather them. This process may involve reading and rereading notes and transcripts, recalling observations and experiences, listening to tapes, and viewing videotapes until you have become immersed in the data. Tapes contain more than words; they contain feeling, emphasis, and nonverbal communications. These aspects are at least as important to the communication as the words are. In phenomenology, this immersion in the data is referred to as dwelling with the data.
Data Reduction
Because of the volumes of data acquired in a qualitative study, initial efforts at analysis focus on reducing the volume of data so that the researcher can more effectively examine them, a process referred to as data reduction. During data reduction, you begin attaching meaning to elements in your data. You will discover classes of things, persons, and events and detect properties that characterize things, persons, and events. You will also note regularities in the setting or the people. These discoveries will lead to classifying elements in your data. In some cases, you may apply the classification scheme used by participants or authors. In other cases, you may wish to construct your own classification scheme.
According to Sandelowski (1995b),
Although data preparation is a distinctive stage in qualitative work where data are put into a form that will permit analysis, a rudimentary kind of analysis often begins when the researcher proofs transcripts against the audiotaped interviews from which they were prepared. Indeed, the proofing process is often the first time a researcher gets a sense of the interview as a whole; it is, occasionally, the first time investigators will hear something said, even though they conducted the interview. During the proofing process, researchers will often underline key phrases, simply because they make some as yet inchoate impression on them. They may jot down ideas in the margins next to the text that triggered them, just because they do not want to lose some line of thinking. (p. 373)
Data Analysis
The following is a description of some of the techniques qualitative researchers use during the process of data analysis and interpretation. These techniques include coding, reflective remarks, marginal remarks, memoing, and developing propositions.
Codes and Coding
Coding is a means of categorizing. A code is a symbol or abbreviation used to classify words or phrases in the data. Codes may be placed in the data at the time of data collection, when entering data into the computer, or during later examination. Through the selection of categories, or codes, the researcher defines the domain of the study. Therefore, it is important that the codes be consistent with the philosophical base of the study. Organization of data, selection of specific elements of the data for categories, and naming of these categories all reflect the philosophical base used for the study. Later in the study, coding may progress to the development of a taxonomy. For example, you might develop a taxonomy of types of pain, types of patients, or types of patient education. Initial categories should be as broad as possible, but categories should not overlap. As you collect more data in relation to a particular category, you can section the major category into smaller categories.
SmithBattle (2007) described her coding process as follows.
The types of codes that can be used are descriptive, interpretative, and explanatory. Descriptive codes classify elements of the data by using terms that describe how the researcher is organizing the data. It is the simplest method of classification and is commonly used in the initial stages of data analysis. Descriptive codes remain close to the terms that the participant used during the interview. For example, if you were reading a transcribed interview in which a participant described experiences in the first days after surgery, you might use descriptive codes such as PAIN, MOVING, FEAR, and REST.
Interpretative codes are usually developed later in the data-collecting process as the researcher gains some insight into the processes occurring and begins to move beyond simply sorting statements. The participant’s terms are used to attach meanings to these statements. For example, in a study of postoperative experiences, you might begin to recognize that the participant was investing much energy in seeking to relieve symptoms and seeking information about how the health care providers believed that he or she was doing. These might be classified by using interpretative codes of RELIEF and INFO.
Explanatory codes are developed late in the data-collecting process after theoretical ideas from the study have begun to emerge. The explanatory codes are part of the researcher’s attempt to unravel the meanings inherent in the situation. These codes connect the data to the emerging theory, and the codes used may be specific to the theory or be more general, such as PATT (pattern), TH (theme), or CL (causal link). Typically, codes will not stay the same throughout the study. Some codes will have to be divided into subclassifications. Other codes may be discontinued because they do not work.
Reflective Remarks
While she or he is recording notes, thoughts or insights often emerge into the researcher’s consciousness. These thoughts are generally included within the notes as reflective remarks and are separated from the rest of the notes by double parentheses (()). Later, they may need to be extracted and used for memoing (Miles & Huberman, 1994).
Marginal Remarks
As you are reviewing your notes, immediately write down any observations you may have about them. These remarks are usually placed in the right-hand margin of the notes. The remarks often connect the notes with other parts of the data or suggest new interpretations. Reviewing notes can become boring, which is a signal that thinking has ceased. Making marginal remarks assists the researcher in “retaining a thoughtful stance” (Miles & Huberman, 1994, p. 65).
Memoing
The researcher develops a memo to record insights or ideas related to notes, transcripts, or codes. Memos move the researcher toward theorizing and are conceptual rather than factual. They may link pieces of data together or use a specific piece of data as an example of a conceptual idea. The memo may be written to someone else in the study or may be just a note you make to yourself. The important thing is to value your ideas and get them written down quickly. Whenever an idea emerges, even if it is vague and not well thought out, develop the habit of writing it down immediately. Initially you might feel that the idea is so clear in your mind that you can write it down later. However, you may soon forget the thought and be unable to retrieve it. As you becomes immersed in the data, these ideas will occur at odd times, such as 2 am, when you are driving, or when you are preparing a meal. Therefore, keep paper and pencil handy. If an idea wakes you up, write it down immediately; it may be gone by morning. Make sure that your memos are dated, titled with the key concept discussed, and connected by codes with the field notes or forms that generated the thoughts (Miles & Huberman, 1994).
Developing Propositions
As the study progresses, relationships among categories, participants, actions, and events will begin to emerge. You will develop hunches about relationships that you can then use to formulate tentative propositions. If the study is being conducted by a team of researchers, everyone involved in the study can participate in the development of propositions. Statements or propositions can be written on index cards and sorted into categories or entered into the computer. A working list can then be printed and shared among the researchers to generate further discussion (Miles & Huberman, 1994).
Multimedia Analysis
The purpose of any sort of analysis of transcripts is to ascertain meaning. The type of meaning sought may vary. However, meaning in an interaction is not conveyed totally through the words that are used. The way in which the words were expressed may be critical to the meaning being conveyed. In addition, approximately 70% of communication is nonverbal. As Burnard (1995) wisely pointed out, “often the words used are not particularly relevant or are not ‘registered’ by the parties involved in a conversation. We do not, after all, usually pick our words very carefully when we speak, nor do we continually ‘check each other’ to ascertain that understanding has occurred. And yet we do understand one another, most of the time” (full text available in Nursing Collection). In some cases, the words used have little or no meaning. They are used to convey unstated meanings. The meanings are behind the words. It may be impossible to capture this meaning by analyzing transcripts. The participant, asked for an exact interpretation of what was meant, may not be able to explain the meaning. Sometimes,
words do not convey any meaning at all but instead create a mood.… Sometimes words can be used as “fillers” between pieces of information.… In summary, then, it seems possible that we communicate, using words, in many different ways. First, we may use words precisely and to convey very definite concepts. Second, we may use words to convey or to ‘create moods. In this case, we are not conveying particular or precise meanings. Third, it may be that we communicate in chunks of words and phrases. Finally, in this summation, we may note that not everything we say is of equal importance—either to ourselves or to the listener. All of these factors make the likelihood of a researcher, using textual data and a method of textual analysis, uncovering the precise meaning of pieces of communication an unlikely scenario. … Transcripts are always post hoc—they always occur after and, sometimes, at some distance from the original interviews. This means that the reader of the transcripts—the researcher—always comes to the transcripts too late. What “really happened” in the interview has been lost. (Burnard, 1995; full text available in Nursing Collection)
One way to address this problem is to use multiple data collection methods. Interviews might be videotaped as well as audiotaped. The researcher might strengthen his or her analysis by simultaneously reviewing video and audio transmissions while reviewing the transcript. Parse (1990) referred to this process as immersion in the data. Multimedia computers are now available in which text, video, graphical media, and sound can be used for such immersion. Burnard (1995) foresees a time when CD-ROM disks might be used to store these multimedia data sets. This type of integrated and triangulated approach to analysis would provide a richer understanding of meaning.
Analysis of Focus Group Data
Historically, content analysis has been used to analyze focus group data. However, data from focus groups are complex in that analysis is required at both the individual level and at the group level, considering interactions among individuals and the group, and making comparisons across groups. It is important to attend to the amount of consensus and interest in topics generated in the discussion. Analysis of deviance and minority opinions is important. Attending to the context within which statements were made is critical to the analysis (Morgan, 1995).
Carey (1995) made the following suggestions regarding analyzing focus group data.
It is important in analyzing the data to determine who said what. If only tape-recording is available, this may be a problem. Video recording can help you to obtain this information; if this is not feasible, the cofacilitator can take notes that may provide some information that will help you to make this determination. One useful analysis strategy is to examine all the input of a particular individual and the extent to which this individual’s comments influenced the position of other group members. Nonverbal interaction should also be noted. Dominant members of the group may suppress dissonant views that increase the richness of the data. According to Sim (1998):
Generalization from Focus Group Analysis
The common view of focus groups was that they were representative of a target population and thus generalization to the target group was acceptable. However, participants are not obtained using probability sampling, and one is on shaky ground justifying generalization using this argument. The type of person likely to agree to participate in a focus group is probably different from those who decline. The focus group is a carefully constructed environment, with the setting designed to facilitate the group dynamics so that data are generated. The contrived social situation is not a natural one. What a person says in the focus group cannot be assumed to be what the person would say in other settings. Sim (1998) concluded that “it is not clear that any process of analysis can meaningfully separate out from the data the social factors which operate within the context of a focus group—indeed, the very idea of a context-neutral perspective may not even make sense within this sort of epistemological framework” (p. 350). Rather than considering empirical generalization, Sim (1998) recommended theoretical generalization, based on commonalities of the focus group participants with other groups. Different degrees of generalization may be possible based on the extent of commonality.
Displaying Data for Analysis and Presentation
Displays contain highly condensed versions of the outcomes of qualitative research. They are equivalent to the summary tables of statistical outcomes developed in quantitative research and allow the researcher to get the main ideas of the research across succinctly. Strategies for achieving displays are limited only by the researcher’s imagination. Some suggested ideas follow. It is relatively easy to develop displays by using computer spreadsheets, graphics programs, or desktop publishing programs. Miles and Huberman (1994) provided helpful guidelines for developing displays of qualitative data. Williamson and Long (2005) described techniques of qualitative data analysis using data displays, including the use of computer packages for making displays.
Critical Incident Chart
In some studies, the researcher, in an effort to gain increased insight into the dynamics of a process, identifies critical incidents occurring in the course of that process. The researcher can then compare these critical incidents in various subgroups of participants. The critical incidents and the subgroups can then be placed in a matrix listing the critical incidents in relation to time. The matrix can make it easier to compare critical incidents in terms of timing and variation across participants or subgroups.
Causal Network
As the data are collected and analyzed, the researcher’s understanding of the dynamics involved in the process under study grows. This understanding might be considered a tentative theory. The first tentative theories are vague and poorly pieced together. In some cases, they are altogether wrong. The best way to verify a tentative theory is to share it with others, particularly informants in the study situation. Informants have their own tentative theories that have never been clearly expressed. The tentative theory needs to be expressed as a map. Developing a good map of the tentative theory is difficult and requires some hard work. The development of a tentative theory and an associated map is presented in Chapter 7.
The validity of predictions developed in a tentative theory must be tested. However, finding effective ways to perform such testing is difficult. Predictions are usually developed near the end of the study. Because the findings are often context specific, the predictions must be tested on the same sample or on a sample that is very similar. One strategy is to predict outcomes expected to occur 6 months after the study has been completed. Six months later, send these predictions to informants who participated in the study. Ask the informants to respond to the accuracy of (1) the predictions and (2) the explanation of why the prediction was expected to occur (Miles & Huberman, 1994).
Cognitive Mapping
Cognitive mapping has been used for analysis and display as an alternative to transcribing taped interview data (Northcott, 1996). The technique might also be used as an adjunct to other approaches to analysis. A cognitive map is a visual representation of the information provided by a participant. It represents the researcher’s conceptualizations and interpretations of the participant. The researcher maps the ideas onto a single page, including codes (concepts) and relationships among the codes (similar to the conceptual maps described in Chapter 7), as the researcher listens repeatedly to the taped interview. The interview is not transcribed. The procedure is designed to condense the process of coding, categorizing, and interpreting into one activity. Mapping is performed within 4 days of the interview. For a 45-minute interview, the researcher should allow 3 hours for cognitive mapping. Guidelines for performing cognitive mapping are as follows:
1. Generate field notes immediately after the interview and have them available for the cognitive mapping.
2. Use a large sheet of paper and a black pen (to facilitate photocopying) for the mapping.
3. Listen to the tape without stopping to write comments and rewind the tape.
4. Begin mapping. Start in the center of the paper with a pivotal word (code) and branch out as needed. Listen to the tape repeatedly as you develop the map to ensure that the map accurately reflects the participant’s ideas.
5. Consider the data cognitively. This process may require formulating codes, establishing relationships (or propositions), and recording nonverbal data. You may need to take breaks to allow time for thought.
6. Keep verbatim quotes from the tape separately and indicate where they emerge on the map.
7. Annotate the map to indicate connections and respondent or researcher input.
8. As a second-level analysis, develop a “macro” map that combines content from all the individual cognitive maps. This map will initiate theory building from the analysis.
Drawing and Verifying Conclusions
Unlike the case in quantitative research, conclusions are formed throughout the data analysis process. Conclusions are similar to the findings in a quantitative study. Miles and Huberman (1994) identified 12 tactics used to draw and verify conclusions.
Counting
Qualitative researchers have tended to avoid any use of numbers. However, when judgments of qualities are made, counting is occurring. The researcher states that a pattern occurs “frequently” or “more often.” Something is considered “important” or “significant.” These judgments are made in part by counting. If the researcher is counting, it should be recognized and planned. Counting can help researchers see what they have, it can help verify a hypothesis, and it can help keep one intellectually honest. Qualitative researchers work by insight and intuition; however, their conclusions can be wrong. It is easier to see confirming evidence than to see disconfirming evidence. Comparing insights with numbers can be a good method of verification (Miles & Huberman, 1994).
Noting Patterns and Themes
People easily identify patterns, themes, and gestalts from their observations—almost too easily. The difficulty is in seeking real additional evidence of that pattern while remaining open to disconfirming evidence. Any pattern that is identified should be subjected to skepticism—that of the researcher and that of others (Miles & Huberman, 1994).
Seeing Plausibility
Often during analysis, a conclusion is seen as plausible. It seems to fit; it “makes good sense.” When asked how one arrived at that point, the researcher may state that it “just feels right.” These intuitive feelings are important in both qualitative and quantitative research. However, plausibility cannot stand alone. After plausibility must come systematic analysis. First, intuition occurs and, then, the data are carefully examined to verify the validity of that intuition (Miles & Huberman, 1994).
Clustering
Clustering is the process of sorting elements into categories or groups. It is the first step in inductive theorizing. To cluster objects, people, or behavior into a group, one must first conceptualize them as having similar patterns or characteristics. Clusters, however, like patterns, must be viewed with caution and verified. Alternative ways to cluster may be found that would be more meaningful (Miles & Huberman, 1994).
Making Metaphors
Miles and Huberman (1994) have suggested that qualitative researchers should think and write metaphorically. A metaphor uses figurative language to suggest a likeness or analogy of one kind of idea used in the place of another. Metaphors provide a strong image with a feeling tone that is powerful in communicating meaning. For example, stating rationally and logically that you are in a heavy work situation does not provide the emotional appeal and meaning that you could express by saying, “I am up to my ears in work!” Miles and Huberman also believe that metaphors add meaning to the findings and use the example of a mother’s separation anxiety, a phrase “which is less appealing, less suggestive, and less theoretically powerful than the empty nest syndrome” (p. 221). The phrase “empty nest syndrome” communicates images loaded with meaning far beyond that conveyed by the words alone.
Metaphors are also data-reducing devices that involve generalizing from the particulars. They are pattern-making devices that place the pattern into a larger context. Metaphors are also effective decentering devices. They force the viewer to step back from the mass of particular observations to see the larger picture. Metaphors are also ways of connecting findings to theory. They are what initiates the researcher to think in more general terms. A few suggestions about developing metaphors may be of use: (1) It is unwise to look for metaphors early in the study. (2) To develop metaphors, one must be cognitively playful and move from the denotative to the connotative. Interacting with others in a cognitively playful environment can be useful. (3) Metaphors can be taken too far in terms of meaning; therefore, one must know when to stop.
Splitting Variables
Qualitative research is strongly oriented toward integrating concepts. However, in some cases, researchers must recognize the need for differentiation. They must have the courage to question; Miles and Huberman (1994) have referred to this early integration as premature parsimony. Splitting variables is particularly important during the initial stages of the analysis to allow more detailed examination of the processes that are occurring. It also often occurs with the development of matrices. During theorizing, if the variable does not seem to relate well with the rest of the framework, it may have to be split to allow a more coherent, integrated model to be developed (Miles & Huberman, 1994).
Subsuming Particulars into the General
This process is similar to clustering in that it involves clumping things together. Clustering tends to be intuitive and is similar to coding. Subsuming particulars into the general is a move from the specific and concrete to the abstract and theoretical.
Factoring
The idea of factoring is taken from the quantitative procedure of factor analysis. If you have a list of characteristics, are there general themes within the list that allow you to explain more clearly what is going on? As with factor analysis, when clusters have been identified, they must be named. Factoring can occur at several levels of abstraction in the data. The important consideration is that they make a meaningful difference in clarity (Miles & Huberman, 1994).
Noting Relationships between Variables
Earlier we discussed the development of relationships between variables. However, at this point, it is important to go beyond verifying that a relationship in fact exists; the next step is to explain the relationship. The relationships described in Chapter 7 can be used to describe qualitative findings. Some relationships that might occur are as follows (Miles & Huberman, 1994, p. 257):
1. A+, B+ (both are high, or both low at the same time)
2. A+, B– (A is high, B is low, or vice versa)
3. A↑, B↑ (A has increased, and B has increased)
4. A↑, B↓ (A has increased, and B has decreased)
5. A ↑ then → B ↑ A ↓ (A increased first, then B increased)
6. A↑ then → B ↑ then A↑ (A increased, then B increased, then A increased some more)
Finding Intervening Variables
In some cases, the researcher believes that two variables should go together; however, the findings do not verify this thinking. In other cases, two variables are found during data analysis to go together, but their connection cannot be explained. In both these situations, a third variable may be responsible for the confusion. Therefore, the third variable must be identified. The matrices described earlier can help researchers to search for this variable, and the search often requires some careful detective work. Finding an intervening variable is easiest when multiple cases of the two- variable relationship can be examined (Miles & Huberman, 1994).
Building a Logical Chain of Evidence
At first glance, this step would seem to be the same activity described earlier that resulted in the development of a tentative theory; however, this activity assumes the prior development of a tentative theory. Building a logical chain of evidence involves testing that theory. The researcher must go back and carefully trace evidence from the data through development of the tentative theory; the elements, relationships, and propositions of the theory are then tested against new data. The researcher looks for cases that closely fit the theory and for those that clearly do not fit the theory. The theory may then be modified.
This process is referred to as analytical induction and uses two interlocking cycles. The first cycle is enumerative induction, in which a number and variety of instances are collected that verify the model. The second cycle, eliminative induction, requires that the hypothesis be tested against alternatives. The researcher is required to check carefully for limits to generalizability of the theory. The process of constant comparisons used in grounded theory is related to eliminative induction (Miles & Huberman, 1994).
Making Conceptual/Theoretical Coherence
The previous steps have described a gradual move from empirical data to a conceptual overview of the findings. Inferences have been made as the analysis moved from the concrete to the more abstract. The steps then moved from metaphors to interrelationships, then to constructs, and from there to theories. The theory must now be connected with existing theories in the body of knowledge. To accomplish this step, you must become familiar with a wide variety of theories that could explain the current phenomenon. If you can connect the new theory with other theories, it further strengthens the present theoretical explanation (Miles & Huberman, 1994).
Content Analysis
Content analysis is designed to classify the words in a text into a few categories chosen because of their theoretical importance. Because content analysis uses counting, many qualitative researchers do not consider it to be a qualitative analysis technique. Content analysis is frequently used in historical research. It is the primary approach to analysis used by Kalisch and Kalisch (1977); Kalisch, Kalisch, and Belcher (1985); Kalisch, Kalisch, and Young (1983); and Kalisch, Kalisch, and Clinton, J. (1982) in their series of studies examining the image of nursing as reflected in news media and primetime television.
The technique provides a systematic means of measuring the frequency, order, or intensity of the occurrence of words, phrases, or sentences. Initially, the specific characteristics of the content to be measured must be defined, and then the researcher develops rules for identifying and recording these characteristics. The researcher first selects a specific unit of analysis, which may be individual words, word combinations, or themes. This unit of analysis is considered a symbolic entity and often indicates an abstract concept. Downe-Wamboldt (1992, p. 314) pointed out that “content analysis is more than a counting game; it is concerned with meanings, intentions, consequences, and context. To describe the occurrences of words, phrases, or sentences without consideration of the contextual environment of the data is inappropriate and inadequate.”
To perform content analysis, text is divided into units of meaning (idea categories). These units are then quantified according to specific rules. Idea categories are constructed and words considered representative of these idea categories are selected; this is a crucial phase of content analysis. In more complex studies, more than one categorizing scheme may be used. One common approach to categorization is the use of a dictionary to identify terms and delineate their meaning (Kelly & Sime, 1990).
In some studies, the researcher is searching for latent meaning within the text. In these studies, the text cannot be analyzed by directly observing or identifying specific terms. The researcher may have to infer meaning by more indirect means, such as by looking for relationships among ideas, reality, and language (Kelly & Sime, 1990).
Narrative Analysis
Narrative analysis is a qualitative means of formally analyzing text including stories. When stories are analyzed, the researcher “unpacks” the structure of the story. A story includes a sequence of events with a beginning, a middle, and an end. Stories have their own logic and are temporal (Coffey & Atkinson, 1996; Denzin, 1989). The structures can also be used to determine how people tell stories, how they give shape to the events that they describe, how they make a point, how they “package” events and react to them, and how they communicate their stories to audiences. The structure used for narrative analysis as identified by Coffey and Atkinson (1996, p. 58) is as follows:
| Structure | Question |
| Abstract | What is this about? |
| Orientation | Who? What? When? Where? |
| Complication | Then what happened? |
| Evaluation | So what? |
| Result | What finally happened? |
| Coda | Finish narrative |
The abstract initiates the narrative by summarizing the point of the story or by giving a statement of the proposition that the narrative will illustrate. Orientation provides an introduction to the major events central to the story. Complication continues the narrative by describing complications in the event that make it a story; it takes the form “And then what happened?” Evaluation is the point of the narrative, followed by the result, which gives the outcome or resolution of events. The coda ends the story and is a transition point at which talk may revert to other topics.
The narrative analysis can focus on social action embedded in the text or examine the effect of the story. Stories serve a purpose. They may make a point or be moralistic. They may be success stories or may be a reminder of what not to do or how not to be, with guidance on how to avoid the fate described in the story. The purpose of the story can be the starting point for a more extensive narrative analysis. Narrative analysis may examine multiple stories of key life events and gain greater understanding of the impact of these key events; it may help to explain the relationship between social processes and personal lives; and it may be used to elucidate the cultural values, meanings, and personal experiences. Issues related to power, dominance, and opposition can be examined. Through stories, silenced groups can be given voice (Coffey & Atkinson, 1996). You could perform a narrative analysis of Barbara’s story under Collecting Stories.
Coding is not used in narrative analysis. Coding breaks data up into separate segments and is not useful in analyzing a story; the researcher can lose the sense that informants are providing an account or narrative of events.
Qualitative researchers may choose to communicate the findings of their study as a story. A story can be a powerful way to make a point. Stories can be presented to readers from a variety of perspectives: chronological order, the order in which the story was originally presented, progressive focusing, focusing only on a critical or key event in the story, describing the plot and characters as one would stage a play, following an analytical framework, providing versions of an event from the stories of several viewers, or presenting the story as one would write a mystery and thus appealing to problem solvers.
Reporting Results
In any qualitative study, the first section of a research report should be a detailed description of the participants, the setting, and observing and experiencing the environment in which the data were gathered. This description should be so vivid that the readers or listeners will feel that they are there with you. To accomplish this goal, the qualitative author must go beyond the skills required for technical writing to creative writing skills. Many qualitative authors suggest that researchers are so eager to get right into the results of data analysis, such as those described in this section, that they pay only brief attention to writing the description. The final part of a qualitative research report should express the theoretical ideas emerging from the data analysis.
RESEARCH METHODOLOGY OF SPECIFIC QUALITATIVE APPROACHES
Historically in qualitative research in nursing, the researcher selected a particular research method for conducting studies. A researcher might spend considerable time becoming familiar with the philosophy and strategies used by that method. These researchers were expected to continue to use this same method throughout their careers. This approach has faded over time and now, qualitative researchers commonly use one method for one study and switch to another method for the next study. In many cases, the researcher will use a mixed collection of strategies from various methods for a study. It is rare now that a study rigidly adheres to a particular method. However, we will present the strategies of each method in their “pure” form as a heuristic.
Phenomenological Research Methods
In phenomenological studies, the researcher can use several strategies for data collection, and it is possible to use combinations of strategies. To conduct these data collection strategies, you will involve your personality and use intuiting. Intuiting is the process of actually looking at the phenomenon. During intuiting, you will focus all awareness and energy on the subject of interest to allow an increase in insight. Thus, this process requires absolute concentration and complete absorption with the experience being studied. Intuiting is a strange idea to those of us in the Western world. It is a more common practice in Eastern thought and is related to meditation practices and the directing of personal energy forces.
Data Collection Strategies
In one data collection strategy, participants are asked to describe verbally their experiences of a phenomenon. These verbal data need to be collected in a relaxed atmosphere, and the respondent must be allowed sufficient time to provide complete description. Alternatively, informants can be asked to provide a written description of their experiences. Ruffing-Rahal (1986) has recommended the use of personal documents, particularly autobiographical accounts, as a source of data.
Another strategy requires that the researcher be more directly involved in the experience. During the participant’s experience, the researcher simultaneously observes verbal and nonverbal behavior, the environment, and his or her own responses to the situation. Written notes may be used, or the experience may be tape-recorded or videotaped. When observed behavior is being recorded, the researcher describes rather than evaluates observations.
Several variations may be used to analyze phenomenological data. Porter (1998) clarified the steps of the Husserlian method in Table 23-1. Beck (1994) compared the three methods of Van Kaam, Giorgi, and Colaizzi in Table 23-2. Within nursing, Parse (1990) developed a methodology that is now being used in phenomenological nursing studies.
TABLE 23-1
| Step | Philosophical* |
| 1. Explore the diversity of one’s consciousness. | “Each has his place whence he sees the things that are present, and each enjoys accordingly different appearances of the things” (p. 95) |
| 2. Reflect on experiences Choose an experience to study. Develop a phenomenological framework. Specify a research question. | It is through reflection, one of the many spontaneities of consciousness that experiences are “brought under … [the] glance of the Ego [p. 197] [and become] objects for the Ego” (p. 196) |
| 3. Bracket or perform the phenomenological reduction. | “Not a single theorem [should] … be taken from any of the related sciences, nor allowed as premises for phenomenological purposes” (p. 165) |
| 4. Explore the participants’ life-world. | Engage in a “thorough inspection, analysis, and description of the life-word as we encounter it” (p. 161) |
| 5. Intuit the structures through descriptive analysis. Perform the eidetic reduction (intuit the principle shared by the facts). Create a taxonomy for the experience: intention, component phenomenon. Create a taxonomy for the context of experience: element, descriptor, and feature. |
“We … must strive … to describe faithfully what we really see from our own point of view and after the most earnest consideration” (p. 259) “A living picture of the fruitfulness of phenomenology … can be won only when domain after domain has been actually tramped and the problem-vistas it possesses opened up for all to see” (p. 258) |
| 6. Engage in intersubjective dialogue about the phenomena and contextual features. | To develop a phenomenon fully, two “formations in the constituting of the Thing” (p. 387) are needed: the first formation (reflection, bracketing, and intuiting by the researcher) and the second formation (“the intersubjective identical thing” [p. 387]) to discuss phenomena and “counter-case” (p. 388) |
| 7. Attempt to fill out the phenomena and features. Cycle through reflection, bracketing, and intuiting.Cycle between the first and second formations. Integrate the bracketed material into the analysis. | “The possibility remains of changes in apprehension [but the goal is a] harmonious filling out” (131, 356) of phenomena |
| 8. Determine uses for the phenomena and features. | “In the end, the conjectures must be redeemed by the real vision of the essential connections” (p. 193) |
*From Husserl, E., & Gibson, W. R. B. (1962). Ideas: General introduction to pure phenomenology, (Trans.). New York: Macmillan (original work published 1913).
From Porter, E. J. (1998). On “being inspired” by Husserl’s phenomenology: Reflections on Omery’s exposition of phenomenology as a method of nursing research. Advances in Nursing Research, 21(1), 16–28.
TABLE 23-2
Comparison of Three Phenomenological Methods
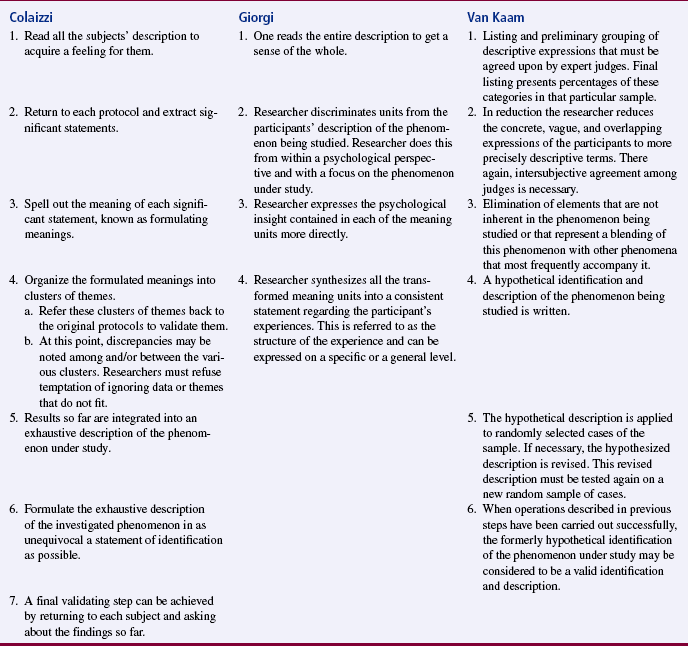
From Beck, C. T. (1994). Reliability and validity issues in phenomenology. Western Journal of Nursing Research, 16(3), 254–267.
Van Kaam: Van Kaam (1966) suggested classifying data and ranking the classifications according to the frequency of occurrence. A panel of judges verifies this ranking. The number of categories is then reduced to eliminate overlapping, vague, or intricate categories, and again, agreement of the panel of judges is sought. Hypotheses are developed to explain the categories theoretically, and these hypotheses are tested on a new sample. This process continues until no new categories emerge.
Giorgi: Giorgi (1970) recommended a similar process but prefers to maintain more of the sense of wholeness. Although individual elements of the phenomenon are identified, their importance to the phenomenon is not established by the frequency of their occurrence but rather by the intuitive judgment of the researcher. Giorgi considered it important to identify the relationships of the units to each other and to the whole. In Table 23-3, Pallikkathayil and Morgan (1991) illustrated the steps of the Giorgi method of analysis by using examples from their study of suicide attempters.
TABLE 23-3
Application of Giorgi’s Method of Analysis of Phenomenological Data
| Step No. | Theoretical Process | Pragmatic Process Used in Example |
| One | Reading of the entire disclosure of the phenomenon straight through to obtain a sense of the whole. | Reading and rereading the first three transcripts to look for emerging themes. Establishing the coding process and decision rules for coding. |
| Two | Rereading the same disclosure again in a purposeful manner to delineate each time that a transition in meaning occurs. This is done with the intention of discovering the essence of the phenomenon under study. The end result is a series of meaning units or themes. | Reading and coding each of the 20 transcripts for themes by each member of the research team. Weekly meetings of the coders to review the coding process and to reach consensus where questions or discrepancies had arisen. Intrarater and interrater reliability was established during this step. |
| Three | Examining the previously determined meaning units for redundancies, clarification, or elaboration by relating meaning units to each other and to a sense of the whole. | The meaning units or themes were examined and categories were developed that represented a higher level of abstraction. Themes not related to the research questions were categorized appropriately. The result was an extensive listing of data by categories. |
| Four | Reflecting on the meaning units (still expressed essentially in the language of the subject) and extrapolating the essence of the experience for each subject. Systematic interrogation of each unit is undertaken for what it reveals about the phenomenon under study for each subject. During this process, each unit is transformed into the language of psychological science when relevant. | After reflecting on the categories, such as thoughts, feelings, and responses of the subjects, a narrative capturing the essence of the phenomenon of an encounter with a suicide attempter was formulated for each subject. It was during this time that the true richness of the phenomenological method was realized. |
| Five | Formalizing a consistent description of the structure of the phenomenon under study across subjects by synthesizing and integrating the insights achieved in the previous steps. | Decisions were made regarding what to accept as the common experience for the phenomenon. Responses offered by 25% or more of the subjects were accepted as the structure of the phenomenon of an encounter with a suicide attempter. |
From Pallikkathayil, L., & Morgan, S. A. (1991). Phenomenology as a method for conducting clinical research. Applied Nursing Research, 4(4), 197.
Colaizzi: Colaizzi (1978) has developed a method that involves observing and analyzing human behavior within its environment to examine experiences that cannot be communicated. This strategy is useful in studying phenomena such as the behavior of preverbal children, subjects with Alzheimer’s disease, the combative behavior of an unconscious patient, and the body motion of subjects with new amputations.
Parse: Parse (1990) described a research methodology specific to the man-living-health theory. This methodology involves dialogical engagement, in which the researcher, and respondent participate in an unstructured discussion about a lived experience. The experience is described as an I-Thou intersubjective being with the participant during the discussion:
The researcher, in true presence with the participant, engages in a dialogue surfacing the remembered, the now, and the not-yet all at once. Before the dialogue with the participant, the researcher “dwells with” the meaning of the lived experience, centering self in a way to be open to a full discussion of the experience as shared by the participant. The discussion is audio and video tape-recorded (when possible), and the dialogue is transcribed to typed format for the extraction-synthesis process. Extraction-synthesis is a process of moving the descriptions from the language of the participants up the levels of abstraction to the language of science. (Parse, 1990, p. 11)
The researcher contemplates the phenomenon under study while listening to the tape, reading the transcribed dialogue, and viewing the videotape. Thus, the researcher is multisensorily immersed in the data. According to Parse (1990), the details of this process include the following:
1. Extracting essences from transcribed descriptions (participant’s language). An extracted essence is a complete expression of a core idea described by the participant.
2. Synthesizing essences (researcher’s language). A synthesized essence is an expression of the core idea of the extracted essence conceptualized by the researcher.
3. Formulating a proposition from each participant’s description. A proposition is a nondirectional statement conceptualized by the researcher joining the core idea of the synthesized essences from each participant.
4. Extracting core concepts from the formulated propositions of all participants. An extracted core concept is an idea (written in a phrase) that captures the central meaning of the propositions.
5. Synthesizing a structure of the lived experience from the extracted concepts. A synthesized structure is a statement conceptualized by the researcher joining the core concepts. The structure as evolved answers the research question, “What is the structure of this lived experience?” (Parse, 1990, p. 11)
The results of this analysis are then moved up another level of abstraction to represent the meaning of the lived experience at the level of theory. The findings are interpreted in terms of the principles of the Parse theory.
Outcomes
Findings are often described from the orientation of the participants studied rather than being translated into scientific or theoretical language. For example, the actual words participants use to describe an experience are often used when reporting the findings. The researcher identifies themes found in the data and uses them to develop a structural explanation of the findings.
Descriptions of human experience need to produce a feeling of understanding in the reader. To do so, the author must focus not only on issues related to truth (validity) but also on issues related to beauty (aesthetics). Therefore, the author must communicate in such a way that the reader is presented with both the structure and the texture of the experience (Todres, 1998).
Phenomenological Nursing Study
Bunkers (2007) conducted a phenomenological study titled “The experience of feeling unsure for women at end-of-life.” The following is an abstract of the study.
Grounded Theory Methodology
Data collection for a grounded theory study is referred to as fieldwork. Participant observation is a commonly used technique. Observation focuses on social interactions within the phenomenon of interest. Interviews may also be conducted to obtain the perceptions of participants. Data are coded in preparation for analysis, which begins with data collection. Stern (1980) and Turner (1981) described the methodology used for grounded theory analysis.
1. Category development. Categories derived from the data are identified and named. These categories are then used as codes for data analysis. This process is the beginning stage of the development of a tentative theory.
2. Category saturation. Examples of the categories identified are collected until the characteristics of items that fit into the category become clear to the researcher. The researcher then examines all instances of the category in the data to determine whether they fit the emerging pattern of characteristics identified.
3. Concept development. The researcher defines the category (now properly referred to as a concept) by using the characteristics verified in step 2.
4. Search for additional categories. The researcher continues to examine the data and collect additional data to search for categories that were not immediately obvious but seem to be essential to understand the phenomenon under study.
5. Category reduction. Categories, which at this point in the research may have become numerous, are clustered by merging them into higher-order categories.
6. Search for negative instances of categories. The researcher continually seeks instances that contradict or otherwise do not fit the characteristics developed to define a category.
7. Linking of categories. The researcher seeks to understand relationships among categories. To accomplish this goal, data collection becomes more selective as the researcher seeks to determine conditions under which the concepts occur. The researcher develops hypotheses and tests them with available data or by selecting additional interviews or observations specifically to examine proposed links among the categories. The researcher then develops a narrative of the emerging theory, including the concepts, conceptual definitions, and relationships. She or he rewrites the narrative repeatedly until the emerging theory has been clearly expressed, is logically explained, reflects the data, and is compatible with the knowledge base of nursing. A conceptual map may be provided to clarify the theory (Burns, 1989).
8. Selective sampling of the literature. Background and significance of the research question are validated through the literature, and the researcher conducts a brief review of previous research. A more extensive literature review is conducted during the interpretation phase to determine the fit of findings from earlier studies with the present findings and the fit of existing theory with the emerging grounded theory.
9. Emergence of the core variable. Through the aforementioned activities, the concept most important to the theory emerges. This concept, or core variable, becomes the central theme or focus of the theory.
10. Concept modification and integration. The researcher wraps up the process by finalizing the theory and again comparing it with the data. “As categories and patterns emerge, the researcher must engage in the critical act of challenging the very pattern that seems so apparent. The researcher must search for other, plausible explanations for the data and the linkages among them” (Marshall & Rossman, 1989, p. 119). Sometimes, the fit between the data and the emerging theory is poor. A poor fit can occur when patterns in the data are identified before the researcher can logically fit all the data within the emerging framework. In this case, the relationships proposed among the phenomena may be spurious. Miles and Huberman (1994) have suggested that plausibility is the opiate of the intellectual. If the emerging schema makes good sense and fits with other theorists’ explanations of the phenomena, the researcher may lock into it prematurely. Therefore, it is critical to test the schema by rechecking the fit between the emerging theory and the original data.
Zoffmann and Kirkevold (2007) conducted a grounded theory study of relationships and their potential for change developed in difficult type 1 diabetes. The abstract of the study is provided here.
Few researchers have explored how relationships between patients and providers might change problem solving in clinical practice. The authors used grounded theory to study dyads of 11 people with diabetes and poor glycemic control, and 8 nurses interacting in diabetes teams. Relational Potential for Change was identified as a core category that involved three types of relationships. Professionals mostly shifted between less effective relationships characterized by I-you-distant provider dominance and I-you-blurred sympathy. Although rarely seen, a third relationship, I-you-sorted mutuality proved more effective than the others in exploiting the Relational Potential for Change. The three types of relationship differed in (a) scope of problem solving, (b) the roles assigned to the patient and the professionals, (c) use of difficult feelings and different points of view, and (d) quality of knowledge achieved as the basis for problem solving and decision making. The authors discuss implications for practice and further research. (p. 625)
Ethnographical Methodology
One of the critical steps in any study is gaining entry into the area being studied. This step can be particularly sensitive in ethnographical studies. The mechanics of this process may vary greatly, depending on whether you are attempting to gain entrance to another country or into a specific institution. The researcher is responsible for explaining the purposes and methods of the study to those with the power to grant entrance.
Acquiring Informants
To understand the culture, seek out individuals who are willing to interpret the culture for you. These people (usually members of the culture) will not be research subjects in the usual sense of the word, but rather colleagues. You must have the support and confidence of these individuals to complete your research. Therefore, maintaining these relationships is of utmost importance. Not only will the informants answer questions, but they may also help you to formulate the questions because they understand the culture better than you do.
Immersion in the Culture
Ethnographical researchers must become familiar with the culture being studied by living in it (active participation) and by extensive questioning. The process of becoming immersed in the culture involves gaining increasing familiarity with the language, sociocultural norms, traditions, and other social dimensions, including family, communication patterns (verbal and nonverbal), religion, work patterns, and expression of emotion. Immersion also involves the researcher’s gradual acceptance into the culture.
Gathering Data (Elicitation Procedures)
The activity of collecting data is referred to as field research and requires taking extensive notes. The quality of these notes will depend on the expertise of the researcher. A skilled researcher experienced in qualitative research techniques will discern more easily what observations need to be noted than will a less experienced researcher or assistant. During observations, you and your research team will be bombarded with information. Intuition plays an important role in determining which data to collect. Although you must be actively involved in the culture you are studying, avoid “going native,” which will interfere with both data collection and analysis. In going native, the researcher becomes a part of the culture and loses all objectivity—and with it the ability to observe clearly.
Analysis of Data
Data analysis is essentially the analysis of the field notes and interviews. The notes themselves may be superficial. However, during the process of analysis, you will clarify, extend, and interpret those notes. Abstract thought processes (intuition, introspection, and reasoning, discussed in Chapter 1) are involved in analysis. Interpretations are checked out with the informants. The data are then formed into categories and relationships developed between categories. Patterns of behavior are identified.
Outcomes
The analysis process in ethnography provides detailed descriptions of cultures. These descriptions may be applied to existing theories of cultures. In some cases, the findings may lead to the development of hypotheses, theories, or both. The results are tested by whether another ethnographer, using the findings of the first ethnographical study, can accurately anticipate human behavior in the studied culture. Although the findings are not usually generalized from one culture or subculture to another, a case may be made for some degree of generalization to other similar cultures (Germain, 1986).
Ethnographical Study
Penney and Wellard (2007) conducted an ethnographic study of older consumers’ perceptions of participating in their care. The abstract follows.
Historical Research Methodology
The methodology of historical research consists of the following steps: (1) formulating an idea, (2) developing research questions, (3) developing an inventory of sources, (4) clarifying the validity and reliability of data, (5) developing a research outline, and (6) conducting data collection and analysis.
Formulating an Idea
The first step in historical research is selecting a topic. Some appropriate topics for historical research in nursing are “origins, epochs, events treated as units; movements, trends, patterns over stated periods; history of specific agencies or institutions; broad studies of the development of needs for specialized types of nursing; biographies and portrayals of the nurse in literature, art, or drama” (Newton, 1965, p. 20).
As with many types of research, the initial ideas for historical research tend to be broad. Once your initial ideas have been clearly stated and narrowed to a topic that is precisely defined, the time predicted to search for related materials is realistic. In addition to narrowing the topic, it is often important to limit the historical period to be studied. Limiting the period requires a knowledge of the broader social, political, and economic factors that would have an impact on the topic you are studying.
Spend much time extensively reading related literature before making a final decision about the precise topic. For example, Waring (1978) conducted her doctoral dissertation using historical research to examine the idea of the nurse experiencing a “calling” to practice nursing. In the following abstract from that dissertation, she describes the extensive process of developing a precise topic.
In historical research, there frequently is no problem statement. Rather than being defined in a problem statement, the research topic is usually expressed in the title of the study. For example, the title of Waring’s dissertation was American Nursing and the Concept of the Calling.
Developing Research Questions
After you have clearly defined your topic, identify the questions you will examine during the research process. These questions tend to be more general and analytical than those found in quantitative studies. In the following excerpt, Evans, then a doctoral student, describes the research questions she developed for her historical study.
Developing an Inventory of Sources
The next step is to determine whether sources of data for the study exist and are available. Many of the materials needed for historical research are contained within private archives in libraries or are privately owned. One must obtain written permission to gain access to library archives. Private materials are often difficult to ferret out, and when they are discovered, access to them may be a problem. However, Sorensen (1988) believes that the primary problem is the lack of experience of nurse researchers with the use of archival data. Sorensen (1988) and Fairman (1987) have identified the major sources of archival data for historical nursing studies (see Table 4-1). Lusk (1997) also provided an extensive discussion of sources for historical researchers. Lusk suggests that the pleasure of the pursuit for sources should not be underrated. The assistance of a librarian in selecting appropriate indexes is recommended.
Historical materials in nursing, such as letters, memos, handwritten materials, and mementos of significant leaders in nursing, are being discarded because no one recognizes their value. The same is true of materials related to the history of institutions and agencies within which nursing has been involved. Christy (1978, p. 9) observed, “It seems obvious that interest in the preservation of historical materials will only be stimulated if there is a concomitant interest in the value of historical research.”
Sometimes, when such material is found, it is in such poor condition that much of the data are unclear or completely lost. In the following excerpt, Christy describes one of her experiences in searching for historical data:
Currently, most historical nursing research has focused on nursing leaders. However, Noel (1988, p. 107) suggested that “women in general are woefully underrepresented in the biographical form.” She comments that worthy nurses are those controversial figures who have influenced broad segments of their cultures, although any life well told can help the reader understand and value the individual and his or her contributions. She suggests two prerequisites for selecting a subject: “the biographers’ interest, affinity, or fatal fascination for the subject (living or dead) … and the existence and availability of data” (Noel, 1988, p. 107).
Life histories can provide insight into the lives of significant nursing figures. Gathering data for life histories involves collecting the stories and interpretations of the individual being studied. This method allows the individuals to present their views of their lives in their own words. Life histories have been viewed with skepticism because findings are difficult to verify, results are vague, and generalization is limited. In-depth and repeated interviews longitudinally overcome some of these drawbacks, but selective memory of the subject can be problematic. Triangulation of data collection methods and verification with other sources reduce this limitation (Admi, 1995).
Rosenberg (1987) has identified eight areas that are important to examine from a nursing history perspective: (1) history from below—the life of ordinary men and women in nursing, (2) gender and the professions, (3) knowledge and authority, (4) the role of technology, (5) the new institutional history, (6) the hospital as problematic, (7) the nurse as worker, and (8) history as meaning.
There seems to have been no examination of historical patterns of nursing practice. Because so much of nursing knowledge has been transmitted verbally or by role modeling, we as nurses may lose much of the understanding of our roots unless studies are initiated to record them. We have no clear picture of how nursing practice has changed over the years (e.g., when, how, and for what reasons have nursing care patterns changed for individuals experiencing diabetes, cardiovascular disease, surgery, or stroke?). Changes in nursing procedures, such as bed baths, enemas, and the feeding of patients, could be examined. Procedure manuals, policy books, and nurses’ notes in patient charts are useful sources for examining changes in nursing practice.
Some possible research questions are as follows:
1. Which nursing practice changes were due to medical actions, and which were nursing innovations?
2. What factors in nursing influence changes in nursing practice?
3. What are the time patterns for changes in practice?
4. Have the time patterns for changes in practice remained fairly consistent, or have they changed over the history of nursing?
5. What has been the influence of levels of education on nursing practice?
6. What has been the influence of advanced nursing practice roles (clinical nurse specialist, nurse practitioner, nurse midwife, nurse anesthetist) on nursing practice?
7. How has the quality of nursing care changed over the past decade? Over the past century?
This type of information might provide greater insight into future directions for nursing practice, research, and theory development. However, to conduct quality historical research, those of us in the process of making history must accept responsibility for preserving the sources.
Historical researchers spend considerable time refining their research questions before they start collecting data. They identify sources of data relevant to the research question. Sources of data are often remote, so the researcher may need to make travel plans to obtain access to the data. In many cases, the researcher must obtain special written permission from the relevant library to obtain access to needed data. The validity and reliability of the data are an important concern in historical research.
Clarifying Validity and Reliability of Data
The validity and reliability concerns in historical research are related to the sources from which data are collected. The most valued source of data is the primary source. A primary source is material most likely to shed true light on the information you are seeking. For example, material written by a person who experienced an event or letters and other mementos saved by the person being studied are primary source material. A secondary source is material written by those who have previously read and summarized the primary source material. History books and textbooks are secondary source materials. Primary sources are considered more valid and reliable than secondary sources:
The presumption is that an eyewitness can give a more accurate account of an occurrence than a person not present. If the author was an eyewitness, he is considered a primary source. If the author has been told about the occurrence by someone else, the author is a secondary source. The further the author moves from an eyewitness account, the less reliable are his statements. (Christy, 1975, p. 191)
Historiographers use primary sources whenever possible.
The historical researcher must consider the validity and reliability of primary sources used in the study. To do so, the researcher uses principles of historical criticism.
One does not merely pick up a copy of Grandmother’s diary and gleefully assume that all the things Grandma wrote were the unvarnished facts. Grandmother’s glasses may at times have been clouded, at other times rose-colored. The well-prepared researcher will scrutinize, criticize, and analyze the diary before even accepting that Grandma wrote it! Even after the document has been validated, the researcher must make every attempt to uncover bias, prejudice, or just plain exaggeration on Grandmother’s part. Healthy skepticism becomes a way of life for the serious historiographer (Christy, 1978, p. 6). Two strategies have been developed to determine the authenticity and accuracy of the source: external and internal criticism.
External criticism determines the validity of source material. The researcher needs to know where, when, why, and by whom a document was written, which may involve verifying the handwriting or determining the age of the paper on which it was written. Christy (1975) described some difficulties she experienced in establishing the validity of documents:
Internal criticism involves establishing the reliability of the document. The researcher must determine possible biases of the author. To verify the accuracy of a statement, the researcher should have two independent sources that provide the same information. In addition, the researcher should ensure that he or she understands the writer’s statements, because words and their meanings change across time and across cultures. It is also possible to read into a document meaning that the author did not originally intend. This shortcoming is most likely to happen when one is seeking a particular meaning. Sometimes, words can be taken out of context (Christy, 1975).
Developing a Research Outline
The research outline is a guide for the broad topics to be examined and also serves as a basis for a filing system for classifying the data collected. For example, you may file data by time period and cross-reference the material for easy access. One piece of data may be filed under several classifications, and you can place a note in one file referring to data stored in another file. The research outline will provide you with a checkpoint during the process of data collection and can be used to help you to identify gaps in the data collection process.
Data Collection
Data collection may require months or years of dedicated searching for pertinent material. Sometimes, one small source may open a door to an entire new field of facts. In addition, data collection has no clear, obvious end. By examining the research outline, the researcher must decide to stop collecting data. Newton (1965) described these facets of data collection.
Careful attention to note taking is critical. Lusk (1997) provided the following instructions related to note taking:
Analysis of Data
Data analysis involves synthesizing all the data collected. The researcher must sift data and make choices about which to accept and which to reject. Sometimes, interesting data that do not contribute to the questions of the study are difficult to discard. Also, conflicting evidence must be reconciled. For example, if two primary sources give opposite information about an incident, you will need to interpret the differences and determine, as nearly as possible, what actually occurred.
Outcomes
The perspective of the researcher influences interpretations about the outcomes of a historical study inasmuch as competing explanations can be created from the same data set. Evidence for conclusions is always partial because of missing data. Historical interpretation is not about describing the progress of events but about ascribing meaning to them. Thus, the responsibilities of interpreting historical data are great. Lynaugh and Reverby (1987, p. 4) suggested that “historical scholarship is judged on its ability to assemble the best facts and generate the most cogent explanation of a given situation or period.”
Developing a Writing Outline
Before proceeding to write the research report, you must decide the most appropriate means of presenting the data. Some options include a biography, a chronology, and a paper organized to focus on issues. If your outline has been well organized and detailed, the writing that follows should flow easily and smoothly.
Writing the Research Report
Historical research reports do not follow the traditional formalized style of much research. The studies are designed to attract the interest of the reader and may appear deceptively simple. An untrained eye may not recognize the extensive work required to write the paper. As Christy explained (1975, p. 192), “The reader is never aware of the painstaking work, the careful attention to detail, nor the arduous pursuit of clues endured by the writer of history. Perhaps that is why so many nurses have failed to recognize historiography as a legitimate research endeavor. It looks so easy.”
Example of a Historical Study
Mu and Lin (2007) provided an oral historical study of the development of the discipline of military nursing in Taiwan from 1948 to 1970. The following abstract describes their study.
Another recently published historical study of significance is Benedict and Georges (2006) study of nurses’ involvement in the sterilization experiments of Auschwitz.
Philosophical Studies
The purpose of philosophical research is to clarify meanings, make values manifest, identify ethics, and study the nature of knowledge (Ellis, 1983). A philosophical researcher is expected to consider a philosophical question from all perspectives by examining conceptual meaning, raising further questions, proposing answers, and suggesting the implications of those answers. The data source for most philosophical studies is written material and verbally expressed ideas relevant to the topic of interest. The researcher critically examines the text or the ideas for flaws in logic. A key element of the analysis is the posing of philosophical questions. The data are then searched for information relevant to the question. Ideas or values implied in the text are an important source of information because many philosophical analyses address abstract topics. The researcher attempts to maintain an objective distance from perspectives in the data so that the logic of the idea can be abstractly examined. Ideas, questions, answers, and consequences are often explored, debated, or both with colleagues during the analysis phase.
Three types of philosophical studies are foundational inquiry, philosophical analyses, and ethical analyses.
Foundational Inquiries Methodology
Foundational inquiries are critical and exploratory. The researcher asks questions that reveal flaws in the logic with which the ideas of the science were developed. These flaws may be ambiguities, discrepancies, or puzzles in the way those within the science speak, think, and act. Generally, those within the science do not see this knowledge as having logic problems. The knowledge questioned could be in the form of ideas, concepts, facts, theories, or even various sorts of experiences and ways of doing things (Manchester, 1986). For example, one might question whether adaptation is a desired outcome of nursing action consistent with nursing’s definition of health.
Outcomes: Foundational studies provide critical analyses of ideas and thought within a discipline and thereby facilitate further development of the body of knowledge. The critique of studies within the science is guided by the outcomes of foundational studies and entails the use of five traditional criteria for scientific thinking: accuracy, consistency, scope, simplicity, and fruitfulness (Manchester, 1986).
Example of a Foundational Study: By far, the best-known foundational inquiry in nursing is Carper’s (1978) study of the ways of knowing in nursing. This study was her doctoral dissertation, and only a portion of it has been published. In conducting the study, Carper examined nursing textbooks and journals from 1964 to 1974. She identified four ways of knowing in nursing: empirical, aesthetic, personal, and ethical.
Philosophical Research
The primary purpose of philosophical analysis is to examine meaning and to develop theories of meaning. This objective is usually accomplished through concept analysis or linguistic analysis (Rodgers, 1989). Concept analyses have become common exercises for graduate nursing students, although most have not been performed with philosophical research strategies. Many of them have been published and are providing an important addition to the body of knowledge in nursing. One of the best-known analyses, Smith’s (1986) idea of health, was performed by philosophical inquiry.
Example of Philosophical Inquiry: Smith searched the literature for fundamental concepts on the nature of health. Regardless of how health was defined, it was considered one extreme on a continuum of health and illness. Health was a relative term. A person was judged healthy when measured against some ideal of health. Who was considered healthy was based on the particular ideal of health being used. Smith identified four models (or ideals) of health: the eudaimonistic model, the adaptive model, the role performance model, and the clinical model. This analysis has proved useful in exploring many issues related to nursing, including differing expectations of clients in relation to their health. An instrument has been developed to put this concept into operation and will allow it to be examined in relation to a number of variables important to nursing (Smith, 1986).
Ethical Analysis
In ethical inquiry, the researcher identifies principles to guide conduct that are based on ethical theories. Problems in ethics are related to obligation, rights, duty, right and wrong, conscience, justice, choice, intention, and responsibility. An analysis using a selected ethical theory is performed. The actions prescribed by the analysis may vary with the ethical theory used. The ideas are submitted to colleagues for critique and debate. Conclusions are associated with rights and duties rather than preferences.
Example of Ethical Analysis: Happ et al. (2007) conducted an ethical analysis of communication with patients related to ethical decision making during prolonged mechanical ventilation. Their abstract follows.
Critical Social Theory Methodology
Three means of collecting data for a critical social theory study may be used: verbal or written questions posed to individuals or groups, observation, or use of written documents. Data may be quantitative or qualitative and include numbers and stories. Methods are selected that are expected to yield the most compelling evidence, which is most likely to be a combination of stories and numbers. This strategy may use one of three basic approaches:
1. Numbers foreground, stories background. These studies are primarily quantitative with a lesser qualitative focus. Use this approach when the purpose of the study is to influence those in positions of power and the general public who are most likely to be influenced by “hard evidence” (numbers). In this case, stories are used to “put a face” on the numbers so that the intended audience can hear the voices of the participants and consider the meaning of the numbers.
2. Stories foreground, numbers background. These studies are primarily qualitative with a lesser quantitative focus. The purpose of these studies is to provide opportunities for researchers and participants to engage in dialogue, reflection, and critique in relation to the phenomenon being studied. Telling a story enables the participants to name their reality and explore strategies for changing that reality. Emphasis is on personal change, growth, and empowerment. However, problems and concerns of individuals do not occur in isolation and are often beyond the control of the individual. Lasting changes must occur on many levels.
3. Stories and numbers with equal emphasis. A research program fostering individual empowerment and system change may use a full range of methods and types of data. This approach might include a combination of standardized instruments and various interview techniques. Use these data to specify a theory, establish the prevalence of a phenomenon, explore the context of a phenomenon, test a nursing intervention, or any combination of these objectives (Berman et al., 1998).
The research process of critical social theory requires that researchers use oppositional thinking to perform a critique of the social situation under study by applying the following four steps: (1) critical examination of the implicit rules and assumptions of the situation under study in a historical, cultural, and political context; (2) use of reflection to identify the conditions that would make uncoerced knowledge and action possible; (3) analysis of the constraints on communication and human action to develop a theoretical framework that uses causal relationships to explain distortions in communications and repression, the theoretical framework is then tested against individual cases (Hedin, 1986); and, finally, (4) participation in dialogue with those oppressed individuals within the social situation. Dialogue raises the collective consciousness and identifies ways to take action against oppressive forces. The action for change must come from the groups and communities rather than from the researcher. The groups and communities must consider “(a) their common interests; (b) the risks they are willing to undergo; (c) the consequences they can expect; and (d) their knowledge of the circumstances of their own lives” (Hedin, 1986, p. 146).
As with most qualitative research methodologies, it is difficult to separate the steps. Dialogue is used both to collect and to interpret the data, and researchers constantly move back and forth between collection and interpretation. Dialogue, which uses some of the techniques of phenomenology, includes conversations between the researcher and persons within the society and requires a relationship of equality and active reciprocity. In addition, by reflection and insight, the researcher dialogues with the data while collecting, analyzing, and interpreting it. “New meanings emerge, and phrases that have always been ignored suddenly come alive and demand explanation” (Thompson, 1987, p. 33). The process “exposes ways in which the self has been formed (or deformed) through the influence of coercive power relations. The work of critical scholarship is to make these power relations transparent, for these relations lose power when they become transparent” (Thompson, 1987, p. 33). Knowledge is created, and this knowledge furthers autonomy and responsibility by enlightening individuals about how they may rationally act to realize their own best interests (Holter, 1988).
Example of a Critical Social Theory Study
Cueto (2004) conducted a critical social theory analysis of the origins of primary health care and selective primary health care in Latin America. The abstract follows.
Feminist Research Methodology
Purpose: The purpose of feminist research is transformational and directed at social structures and social relationships, including logical arguments (Rafael, 1997).
Review of Literature: The review of literature focuses on a search for evidence of the relationship between power and knowledge. For example, who decides what counts as knowledge? How is power produced? What resistance to power exists? Whose interests are silenced, marginalized, or excluded? How open is power to change (Rafael, 1997)?
Participant-Researcher Relationships: The feminist method requires a leveling of the usual power imbalance between researcher and participant. The perspective of participants is considered primary, yet they are assisted in gaining some distance from their views. The method promotes a balance between objectivity and subjectivity (Rafael, 1997).
Example of Critical Social Theory (Feminist) Study
Ismail, Berman, and Ward-Griffin (2007) conducted a feminist study of dating violence. An abstract is provided here.
QUALITATIVE RESEARCH ISSUES
It has been the position of qualitative researchers that they do not use theoretical frameworks as do quantitative researchers. In some cases, theory was developed as an emerging part of the analysis process. Two recent texts are changing that stance by arguing that atheoretical research is impossible. Flinders and Mills (1993), in their text Theory and Concepts in Qualitative Research, first addressed the issue saying, “Few of us now claim that we enter the field tabula rasa, unencumbered by notions of the phenomena we seek to understand” (p. xi). Anfara and Mertz (2006) in their text Theoretical Frameworks in Qualitative Research, stated that “no comprehensive discussion of theoretical frameworks exists to assist those engaged in qualitative research” (p. xiii). Their goal is to describe what a theoretical framework is and how it is used in qualitative research as well as the effects it has on the qualitative research process. Each chapter in their text offers the framework of a qualitative researcher as a guide for qualitative researchers as they develop frameworks.
The framework development process for qualitative studies is not unlike that described in Chapter 7 of this text. The role that theory plays in qualitative research will likely differ from that of quantitative research. Some qualitative researchers may refer to a theoretical stance, whereas others may not be quite ready to take the leap to frameworks. Strategies for using frameworks to guide the development of qualitative studies, and in the interpretation of results, are not yet clear. It will be interesting to see how the move to frameworks in qualitative research plays out over the next few years.
Researcher-Participant Relationships
One of the important differences between quantitative and qualitative research is the nature of relationships between the researcher and the individuals being studied. The nature of these relationships has an impact on the data collected and their interpretation. In many qualitative studies, the researcher observes social behavior and may participate in social interactions with those being studied. Four types of participant observation are commonly distinguished: (1) complete participation, in which the observer becomes a member of the group and conceals the researcher role; (2) participant as observer, in which participants are aware of the dual roles of the researcher; (3) observer as participant, in which most of the researcher’s time is spent observing and interviewing and less in the participation role; and (4) complete observer, in which the researcher is passive and has no direct social interaction in the setting. You must carefully consider the type(s) of researcher-participant relationships that you will use in your study and specify them when describing your methodology.
In varying degrees, the researcher influences the individuals being studied and, in turn, is influenced by them. The mere presence of the researcher may alter behavior in the setting. Although this involvement is considered a source of bias in quantitative research, qualitative researchers consider it to be a natural and necessary element of the research process. The researcher’s personality is a key factor in qualitative research as skills in empathy and intuition are cultivated. You will need to become closely involved in the subject’s experience to interpret it. It is necessary to be open to the perceptions of the participants rather than attaching your own meaning to the experience. Individuals being studied often participate in determining research questions, guiding data collection, and interpreting results. Watts (2006) described challenges in feminist research when researching women who do not identify with feminist aims. She discussed the impact the insider researcher role has on “truth telling.” She pointed out that there is a fine line between empathy and exploitation. Dickson-Swift, James, Kippen, and Liamputtong (2006) conducted a study examining the blurring of boundaries between the researcher and the participants. Many researchers conducting research in sensitive areas found themselves becoming friends with the participants. Poor boundary management adds stress to research work. A number of researchers described emotional exhaustion and feeling overwhelmed. The authors recommend that you develop protocols for studies of sensitive areas before initiating the study. Training is also recommended for managing boundary issues before commencing such studies.
The interface between the participant-observer role and the nurse role of the researcher is a concern. Because of the possible impact of the nursing role on the study, Robinson and Thorne (1988) claimed that the nurse researcher has an obligation to explain in the study report the influence that his or her professional perspective had on the process and outcomes of the study. In some studies, the researcher is expected to interact with participants but to stay in the role of researcher and avoid relating to participants as a nurse. Some insist that the nurse researcher must always relate first as a nurse and second as a researcher (Cooper, 1988; Fowler, 1988). Connors (1988) suggested that qualitative researchers must be authentic and engaged as a whole person rather than just as a researcher or as a nurse. Colbourne and Sque (2005) pointed out that nurse researchers, while in the role of qualitative researcher, “may offer the participant a mechanism for reflection, greater self-awareness, finding a voice, obtaining information, and venting repressed emotions.” Positive and negative aspects of this therapeutic component are explored along with cautions that the nurse researcher think carefully about the stance taken in the field.
In addition to the role you will take in the relationship, carefully consider the expectations of your study. Munhall (1988) pointed out that ethically, it is essential that the qualitative researcher think through both the aims and the means of the study and determine whether these aims and means are consistent with those of the participants. For example, if your desire as a researcher is to change the behavior of the participants, the participants need to share this goal. During the study, a level of trust develops between the researcher and the participant, who may provide information labeled as secret. Establishing relationships with participants, however, can cause harm. Participant observation requires a close relationship that invades the privacy of the individual. Although participants may experience confidence, commitment, and friendship from the encounter, they may also experience disappointment, perceived betrayal, and desertion as the researcher functions in the researcher role and then leaves (Munhall, 1988). The relationship can also harm the researcher. Cowles (1988) described emotional pain and difficulty sleeping as she collected data from family members of murdered individuals. She frequently required support and opportunities to explore her feelings with colleagues during the process. Draucker (1999) cautioned that little is known about the effects on participants in studies of sexual violence.
Participatory Research
In some qualitative studies, participants partner with the researchers in planning and conducting the study. This is referred to as participatory research. The method began in ethnographical research and is now being used in some quantitative and outcome studies as well.
Participatory research is a strategy designed to include representatives of the community under study as members of the research team. It allows members of the community to have a voice in the way the study is conducted and the results that are disseminated. The strategy also serves as a check on the researchers’ biases and makes the scientific community directly accountable to the client communities. Commonly, issues related to imbalances in power between the researchers and the community representatives must be addressed.
In vulnerable populations, suspicion of researchers is prevalent. Many people fear being misused. Establishing and maintaining trust is the ongoing key to success. In a participatory research project, the partnership leads to the researchers and the people being studied being involved in all phases of the research process. Questions of immediate concern to the community may be added to the research program. Through dialogue, the researchers often gain new insights into the problem under study, as well as interventions that might be effective in addressing the problem. Change is one of the primary purposes of the project (Henderson, 1995; Seng, 1998).
Friere, a Brazilian scholar whose ideas were described in Chapter 4, originated participatory research strategies. The methods used to promote social change are those of critical social theory as described in Chapter 4. Participatory studies include a variety of designs, some qualitative, some quantitative, and some a triangulated mix of strategies. Some of the strategies that might be used in a participatory research project were described in more detail in Chapter 13, which describes another new paradigm in research, intervention research.
Mullings et al. (2001) used participatory research methods in their study of reproductive experiences in Harlem. The following quotes from this excellent study on a topic difficult to examine sheds light on how to implement participatory research methods.
We used four approaches for organizing community participation: 1) recruitment of organizations and researchers with longstanding relationships and commitment to the community, 2) development of a community advisory board, 3) community dialogue groups, and 4) community meetings.
The New York Urban League was chosen as the general contractor for the Harlem Birth Right Project because of its long-term links with the Harlem community and its involvement in a number of other health-related projects, including overseeing the Harlem Healthy Start program. In addition, all four principal investigators had long histories of residence, activism, or work in Harlem.
 DEVELOPMENT OF A COMMUNITY ADVISORY BOARD
DEVELOPMENT OF A COMMUNITY ADVISORY BOARD
To involve a broad cross-section of the community, the research team established a 24-member Community Advisory Board (CAB). This Board was composed of Harlem residents, who met quarterly with the researchers throughout the 4-year research period. In constituting the CAB, the researchers attempted to make it representative of the socioeconomic, occupational, gender, religious, age, and ethnic heterogeneity of Central Harlem. To operationalize this, CAB members were recruited from community organizations, unions, youth programs, and service organizations, and participated as individuals and not as representatives of their organizations. Some members were unaffiliated persons encountered in the course of fieldwork. The CAB actively participated in all phases of the research, including designing and facilitating the research (e.g., selection of the research sites, and development of the focus groups and the ethnographic questionnaire), facilitating research contracts and entry into research sites, representing the project at various public functions, serving as resources in the hiring of personnel (e.g., interviewers) from the community, and helping develop strategies for public dissemination of the project objectives and results. Furthermore, the CAB maintained continuous dialogue with the researchers, providing insight into research problems on the basis of their experiences as long-term residents or workers in Harlem.
In addition to the CAB, several Community Dialogue Groups (CDGs) of 5–10 persons each were convened during the active field research to discuss specific issues, such as selection of the sites for intensive ethnographic data collection, selection and recruitment of longitudinal participants, focus group criteria, structure and content of the ethnographic questionnaire, and improved community participation. The CDGs allowed the researchers to involve an even broader group of Harlem residents in the Project, to discuss specific issues in greater depth and to avoid overburdening the CAB members.
Additional participation was elicited through two general community meetings open to the public, which were held to provide information about the Harlem Birth Right Project and to solicit advice. Moreover, ethnographers provided persons at all participant observation sites and public meetings with detailed explanations about the research.
OPERATIONALIZING QUALITATIVE RESEARCH
In collaboration with the CAB and the CDG, the researchers developed an ethnographic research design with four components: participant observation, longitudinal case studies, focus groups, and ethnographic questionnaire. A thorough literature review and pilot fieldwork were conducted over the 6 months prior to initial data collection. Analysis of media reports, archival information, public documents, and academic literature was undertaken throughout the research to situate the Harlem data in a broader social and political context. (Mullings et al., 2001, pp. 86–87)
In this Project, community participation was critical to achieving new theoretical and methodological insights, and assisted in the ways in which material was prepared for presentation to the community. As many proponents have pointed out, community participation has an important role to play in facilitating access, trust, and implementation. But the incorporation of community participation also has real implications for addressing biases in traditional public health and social science research. (Mullings et al., 2001, p. 91)
Reflexivity
Qualitative researchers need to critically think through the dynamic interaction between the self and the data occurring during analysis. This interaction occurs whether the data are communicated person to person or through the written word. The critical thinking used to examine this interaction is referred to as reflexive thought or reflexivity (Lamb & Huttlinger, 1989). During this process, the researcher explores personal feelings and experiences that may influence the study and integrates this understanding into the study. The process requires a conscious awareness of self.
Drew (1989), in a paper recounting her experience conducting a phenomenological study of caregiving behavior, demonstrated reflexivity as she described the impact of relationships on her study.
In some phenomenological research, this critical thinking leads to bracketing, which researchers use to avoid misinterpreting the phenomenon as the individual experiences it. Bracketing is suspending or laying aside what is known about the experience being studied (Oiler, 1982). Researchers using the Husserl interpretation of phenomenology most commonly use bracketing. Other phenomenologists, especially those using Heideggerian phenomenology, do not believe bracketing is possible. However, they do identify beliefs, assumptions, and preconceptions about the research topic, which are put in writing at the beginning of the study for self-reflection and external review. These procedures are intended to facilitate openness and new insight.
Most researchers inexperienced in qualitative research require mentoring in reflexive thought. Part of this mentoring is developing a plan for reflexive thought during the conduct of the study. Dialogue with the mentor(s) during the study about the researcher’s experiences and reactions during the study and their implications are also critical. Walsh and Downe (2006), in developing criteria for appraising the quality of qualitative research, developed the following criteria for judging reflexivity. These criteria are especially helpful for students who seem to have difficulty grasping the idea of reflexivity.
Criteria for Judging Reflexivity
Walsh and Downe provide criteria for evaluating the presence and quality of reflexivity in a qualitative study.
Discussion of relationship between researcher and participants during fieldwork
Demonstration of researcher’s influence on stages of the research process
Evidence of self-awareness/insight
Documentation of the effects of the research on researcher
Evidence of how problems/complications were dealt with (Walsh & Downe, 2006, p. 115)
Auditability
The larger scientific community has in some cases seriously questioned the credibility of qualitative data analysis. The concerns relate to the inability to replicate the outcomes of a study, even when using the same data set. Miles and Huberman (1994) described the problem as follows.
To respond to this concern, some qualitative researchers have attempted to develop strategies by which other researchers, using the same data, can follow the logic of the original researcher and arrive at the same conclusions. Guba and Lincoln (1982) referred to this strategy as auditability.
Auditability requires that the researcher establish decision rules for categorizing data, arriving at ratings, or making judgments. A decision rule might say, for example, that a datum would be placed in a specific category if it met specified criteria. Another decision rule might say that an observed interaction would be considered an instance of an emerging theoretical explanation if it met specific criteria. A record is kept of all decision rules used in the data analysis. All raw data are stored so that they are available for review if requested. As the analysis progresses, the researcher documents the data and the decision rules on which each decision was based and the reasoning that entered into each decision. Thus, evidence is retained to support the study conclusions and the emerging theory and is made available on request (Burns, 1989). Marshall (1984, 1985), however, cautioned against undermining the strengths of qualitative research by overly mechanistic data analysis. Marshall and Rossman (1989, p. 113) expressed concern that efforts to increase validity will “filter out the unusual, the serendipitous—the puzzle that if tended to and pursued would provide a recasting of the entire research endeavor.”
If you intend to use auditability strategies, plan for auditability before you begin collecting data, because analysis is initiated at that point. You should include these plans in your research proposal.
Appraisal of Qualitative Studies
Synthesis of studies in preparation for evidence-based practice has, until recently, focused entirely on quantitative research. Qualitative research has been left out of the equation, not considered sufficiently relevant to evidence-based practice to be included. This decision has serious implications for the contribution of qualitative knowledge to clinical practice. Funding of studies, funding of educational programs, and valuing of qualitative knowledge is determined by the inclusion of these studies in the evidence base for practice. A small group of qualitative scholars have been working to persuade those in decision-making positions to include qualitative research in the studies examined for inclusion in evidence-based practice reports. A book describing their work, Handbook for Synthesizing Qualitative Research (Sandelowski & Barroso, 2007), is an excellent guide for qualitative researchers working in the teams to synthesize qualitative studies for inclusion of the evidence base. Of particular interest to a broader group of users, faculty, and students interested in qualitative research is a chapter titled “Appraising Reports of Qualitative Studies.” This chapter provides a detailed guide to the appraisal of individual qualitative studies and to the comparative appraisal of qualitative studies. This book takes the art of writing a qualitative research report and the application of findings well beyond auditability to a whole new level of analysis. We recommend it to students, faculty, and researchers who are invested in qualitative research.
SUMMARY
• Qualitative data analysis occurs concurrently with data collection rather than sequentially as is true in quantitative research.
• Methods of data collection include unstructured observations, unstructured interviews, focus groups, collecting stories, constructing life stories, and case studies.
• Some qualitative researchers use the computer for data analysis, whereas others perform their analysis manually.
• Data are often transcribed from tape recordings to typed manuscripts before analyses.
• After the analyses, a variety of methods are used to display data for analyses and presentation, including critical incident charts, causal networks, and cognitive mapping.
• Methods of analyzing the data may include content analysis and narrative analysis.
• Six research methodologies for qualitative studies are described: phenomenological, grounded theory, ethnographical, historical, philosophical, and critical social theory including feminist approaches.
• Although theoretical frameworks have not traditionally been used in qualitative studies, some researchers are beginning to include frameworks in their studies.
• Research-participant relationships are critical to the effective conduct of qualitative studies and are explored in the chapter.
• Participatory research, which began in ethnographical studies, is emerging as an important approach in both qualitative and quantitative studies.
• Reflexivity, in which the qualitative researcher critically thinks through the dynamic interaction between the self and the data, is an important element of qualitative studies.
• Auditability requires the researcher to establish decision rules for categorizing data, arriving at ratings, and making judgments so that another qualitative researcher, using the same data, can follow the logic of the first researcher and arrive at similar conclusions.
• Appraisal of qualitative studies is a newly developing strategy that provides methods to synthesize relevant qualitative studies so that qualitative findings can be included in evidence-based practice documents.
REFERENCES
Admi, H. The life history: A viable approach to nursing research. Nursing Research. 1995;44(3):186–188.
Alvesson, M. Postmodernism and social research. Buchingham: Open University Press, 2002.
Anderson, N.L.R. Computer-assisted analysis of textual field note data. Western Journal of Nursing Research. 1987;9(4):626–630.
Anfara, V.A., Jr., Mertz, N.T. Theoretical frameworks in qualitative research. Thousand Oaks, California: Sage, 2006.
Astedt-Kurki, P., Paavilainen, E., Lehti, K. Methodological issues in interviewing families in family nursing research. Journal of Advanced Nursing. 2001;35(2):288–293.
Atkinson, P. The ethnography of a medical setting: Reading, writing and rhetoric. Qualitative Health Research. 1992;2(4):451–474.
Ayers, L., Poirier, S. Virtual text and the growth of meaning in qualitative analysis. Research in Nursing & Health. 1996;19(2):163–169.
Banks-Wallace, J. Emancipatory potential of storytelling in a group. Image: Journal of Nursing Scholarship. 1998;30(1):17–21.
Bateson, M.C. Composing a life. New York: Penguin, 1989.
Beaudin, C.L., Pelletier, L.R. Consumer-based research: Using focus groups as a method for evaluating quality of care. Journal of Nursing Care Quality. 1996;10(3):28–33.
Beck, C.T. Phenomenology: Its use in nursing research. International Journal of Nursing Studies. 1994;31(6):499–510.
Benderix, Y., Sivberg, B. Siblings’ experiences of having a brother or sister with autism and mental retardation: A case study of 14 siblings from five families. Journal of Pediatric Nursing. 2007;22(5):410–418.
Benedict, S., Georges, J.M. Nurses and the sterilization experiments of Auschwitz: A postmodernist perspective. Nursing Inquiry. 2006;13(4):277–288.
Berg, B.L. Qualitative research methods for the social sciences. Boston: Allyn & Bacon, 1998.
Berman, H., Ford-Gilboe, M., Campbell, J.C. Combining stories and numbers: A methodologic approach for a critical nursing science. Advances in Nursing Science. 1998;21(1):1–15.
Bertaux, D. Biography and society: The life history approach in the social sciences. Beverly Hills, CA: Sage, 1981.
Bulmer, C. Clinical decisions: Defining meaning through focus groups. Nursing Standard. 1998;12(20):34–36.
Bunkers, S.S. The experience of feeling unsure for women at end-of-life. Nursing Science Quarterly. 2007;20(1):56–63.
Burnard, P. Unspoken meanings: Qualitative research and multi-media analysis. Nurse Researcher. 1995;3(1):55–64.
Burnard, P. Qualitative data analysis: Using a word processor to categorize qualitative data in social science research. Social Sciences in Health. 1998;4(1):55–61.
Burns, N. Standards for qualitative research. Nursing Science Quarterly. 1989;2(1):44–52.
Carey, M.A. Comment: Concerns in the analysis of focus group data. Qualitative Health Research. 1995;5(4):487–495.
Carper, B. Fundamental patterns of knowing in nursing. Advances in Nursing Science. 1978;1(1):13–24.
Christy, T.E. The methodology of historical research: A brief introduction. Nursing Research. 1975;24(3):189–192.
Christy, T.E. The hope of history. In: Fitzpatrick M.L., ed. Historical studies in nursing. New York: Teachers College, Columbia University; 1978:3–11.
Clinton, M. Scoping study of the Australian mental health nursing workforce 1999. Canberra: Mental Health and Special Programs Branch Commonwealth Department of Health and Aged Care, 2001. [(No. 0642735204)].
Coffey, A., Atkinson, P. Making sense of qualitative data: Complementary research strategies. Thousand Oaks, CA: Sage, 1996.
Colaizzi, P. Psychological research as the phenomenologist views it. In: Valle R.S., King M., eds. Existential phenomenological alternatives for psychology. New York: Oxford University Press; 1978:48–71.
Colbourne, L., Sque, M. The culture of cancer and the therapeutic impact of qualitative research interviews. Journal of Research in Nursing. 2005;10(5):551–567.
Connors, D.D. A continuum of researcher-participant relationships: An analysis and critique. Advances in Nursing Science. 1988;10(4):32–42.
Cooper, M.C. Covenantal relationships: Grounding for the nursing ethic. Advances in Nursing Science. 1988;10(4):48–59.
Cowles, K.V. Issues in qualitative research on sensitive topics. Western Journal of Nursing Research. 1988;10(2):163–179.
Cueto, M. The origins of primary health care and selective primary health care. American Journal of Public Health. 2004;94(11):1864–1874.
Deatrick, J.A., Ledlie, S.W. Qualitative research interviews with children and their families. Journal of Child and Family Nursing. 2000;3(2):152–158.
Denzin, N.K. Interpretive interactionism. Newbury Park, CA: Sage, 1989.
Dickson-Swift, V., James, E.L., Kippen, S., Liamputtong, P. Blurring boundaries in qualitative health research on sensitive topics. Qualitative Health Research. 2006;16(6):853–871.
Dingwall, R. Atrocity stories and professional relationships. Sociology of Work and Occupations. 1977;4(4):371–396.
Disney, J.A., May, K.M. Focus group method for nursing research: Pleasures and pitfalls. Nursing Research Methods: An Electronic Journal for Nursing Researchers [Online serial]. 1998, August;3:7.
Downe-Wamboldt, B. Content analysis: Method, applications, and issues. Health Care for Women International. 1992;13(3):313–321.
Draucker, C.B. The emotional impact of sexual violence research on participants. Archives of Psychiatric Nursing. 1999;13(4):161–169.
Drew, N. The interviewer’s experience as data in phenomenological research. Western Journal of Nursing Research. 1989;11(4):431–439.
Ellis, R., Philosophic inquiry. Werley, H.H., Fitzpatrick, J.J., eds., Annual review of nursing research, Vol. I. New York: Springer, 1983:211–228.
Evans, J.C. Formulating an idea. In: Fitzpatrick M.L., ed. Historical studies in nursing. New York: Teacher’s College; 1978:15–17.
Fairman, J.A. Sources and references for research in nursing history. Nursing Research. 1987;36(1):56–59.
Field, P.A., Morse, J.M. Nursing research: The application of qualitative approaches. Rockville, MD: Aspen, 1985.
Flinders, D.J., Mills, G.E. Theory and concepts in qualitative research: perspectives from the field. New York: Teachers College Press, 1993.
Foucault, M. The birth of the clinic: An archaeology of medical perception. New York: Vintage Books, 1973. [(A. M. S. Smith, Trans.)].
Foucault, M., Technologies of the Self. Rabinow, P., eds., Ethics: Subjectivity and truth, Vol. 1. New York: The New Press, 1994:223–251. [(R. Hurley & J. Faubion, Trans)].
Foucault, M. Discipline and punish: The birth of the prison. New York: Vintage, 1995. [(A. Sheridan, Trans.)].
Foucault, M. Power/knowledge: Selected interviews and other writings 1972–1977. New York: Pantheon Books, 1980. [(C. Gordon, L. Marshall, J. Mepham, & K. Soper, Trans.)].
Fowler, M.D.M. Issues in qualitative research. Western Journal of Nursing Research. 1988;10(1):109–111.
Fox, N.J. Postmodernism, sociology and health. Buckingham: Open University Press, 1993.
Frank, G. Finding the common denominator: A phenomenological critique of life history method. Ethos. 1979;7(1):68–71.
Frank, G. Life histories in occupational therapy clinical practice. American Journal of Occupational Therapy. 1996;50(4):251–264.
Gergen, K.J., Gergen, M.M. Narratives of the self. In: Sarbin T.R., Scheibe K.E., eds. Studies in social identity. New York: Praeger; 1983:254–273.
Germain, C.P.H. Ethnography: The method. In: Munhall P.L., Oiler C.J., eds. Nursing research: A qualitative perspective. East Norwalk, CT: Appleton-Century- Crofts; 1986:147–162.
Giorgi, A. Psychology as a human science: A phenomenologically based approach. New York: Harper & Row, 1970.
Goss, G.I. Focus group interviews: A methodology for socially sensitive research. Clinical Excellence for Nurse Practitioners. 1998;2(1):30–34.
Guba, E.G., Lincoln, Y.S. Effective evaluation. Washington, DC: Jossey-Bass, 1982.
Halloran, J.P., Grimes, D.E. Application of the focus group methodology to educational program development. Qualitative Health Research. 1995;5(4):444–453.
Hamilton, B.E., Manias, E. Rethinking nurses’ observations: Psychiatric nursing skills and invisibility in an acute inpatient setting. Social Science & Medicine. 2007;65(2):331–343.
Happ, M.B., Swigart, V.A., Tate, J.A., Hoffman, L.A., Arnold, R.M. Patient involvement in health-related decisions during prolonged critical illness. Research in Nursing & Health. 2007;30(4):361–372.
Harrison, B. Seeing health and illness worlds—Using visual methodologies in a sociology of health and illness: A methodological review. Sociology of Health & Illness. 2002;24(6):856–872.
Hedin, B.A. Nursing, education, and emancipation: Applying the critical theoretical approach to nursing research. In: Chinn P.L., ed. Nursing research methodology: Issues and implementation. Rockville, MD: Aspen; 1986:133–146.
Henderson, D.J. Consciousness raising in participatory research: Method and methodology for emancipatory nursing inquiry. Advances in Nursing Science. 1995;17(3):58–69.
Hollis, V., Openshaw, S., Goble, R. Conducting focus groups: Purpose and practicalities. British Journal of Occupational Therapy. 2002;65(1):2–8.
Holter, I.M. Critical theory: A foundation for the development of nursing theories. Scholarly Inquiry for Nursing Practice: An International Journal. 1988;2(3):223–232.
Hutchinson, A.M. Analysing audio-recorded data: Using computer software applications. Nurse Researcher. 2005;12(3):20–31.
Irving, K. Governing the conduct of conduct: Are restraints inevitable? Journal of Advanced Nursing. 2002;40(4):405–512.
Ismail, F., Berman, H., Ward-Griffin, C. Dating violence and the health of young women: A feminist narrative study. Health Care for Women International. 2007;28(5):453–477.
Iser, W. The reading process: A phenomenological approach. In: Tompkins J., ed. Reader-response criticism. Baltimore: Johns Hopkins University Press; 1980:118–133.
Jensen, R. Text management—History and computing. III: Historians, computers and data, applications in research and teaching. Journal of Interdisciplinary History. 1992;22(4):711–722.
Josselson, R., Lieblich, A., eds. The narrative study of lives: Vol. 3. Interpreting experience. Newbury Park, CA: Sage, 1995.
Kalisch, B.J., Kalisch, P.A. An analysis of the sources of physician-nurse conflict. Journal of Nursing Administration. 1977;7(1):50–57.
Kalisch, B.J., Kalisch, P.A., Belcher, B. Forecasting for nursing policy: A news-based image approach. Nursing Research. 1985;34(1):44–49.
Kalisch, B.J., Kalisch, P.A., Young, R.L. Television news coverage of nurse strikes: A resource management perspective. Nursing Research. 1983;32(3):175–180.
Kalisch, P.A., Kalisch, B.J., Clinton, J. The world of nursing on prime time television, 1950 to 1980. Nursing Research. 1982;31(6):358–363.
Kelly, A.W., Sime, A.M. Language as research data: Application of computer content analysis in nursing research. Advances in Nursing Science. 1990;12(3):32–40.
Kelly, L.E., Patterson, B.J. Childhood nutrition: Perceptions of caretakers in a low-income urban setting. Journal of School Nursing. 2006;22(6):345–351.
Kermode, F. The art of telling: Essays on fiction. New York: Oxford University Press, 1983.
Kitzinger, J. Introducing focus groups. British Medical Journal. 1995;311(7000):299–302.
Kramer, T. The diary as a feminist research method. Newsletter of the Association for Women in Psychology. 1983:3–4. [Winter].
Kruman, M.W. Historical method: Implications for nursing research. In: Leininger M.M., ed. Qualitative research methods in nursing. New York: Grune & Stratton; 1985:109–118.
Lamb, G.S., Huttlinger, K. Reflexivity in nursing research. Western Journal of Nursing Research. 1989;11(6):765–772.
Larson, E.A., Fanchiang, S.C. Life history and narrative research: Generating a humanistic knowledge base for occupational therapy. American Journal of Occupational Therapy. 1996;50(4):247–250.
Linde, C. Life stories: The creation of coherence. New York: Oxford University Press, 1993.
Lusk, B. Historical methodology for nursing research. Image: Journal of Nursing Scholarship. 1997;29(4):355–359.
Lynaugh, J., Reverby, S. Thoughts on the nature of history. Nursing Research. 1987;36(1):4. [69].
Mallinson, T., Kielhofner, G., Mattingly, C. Metaphor and meaning in a clinical interview. American Journal of Occupational Therapy. 1996;50(5):338–346.
Manchester, P. Analytic philosophy and foundational inquiry: The method. In: Munhall P.L., Oiler C.J., eds. Nursing research: A qualitative perspective. East Norwalk, CT: Appleton-Century-Crofts; 1986:229–249.
Marshall, C. Elites, bureaucrats, ostriches, and pussycats: Managing research in policy settings. Anthropology and Education Quarterly. 1984;15(3):235–251.
Marshall, C. Appropriate criteria of trustworthiness and goodness for qualitative research on education organizations. Quality and Quantity. 1985;19(4):353–373.
Marshall, C., Rossman, G.B. Designing qualitative research. Newbury Park, CA: Sage, 1989.
Mattingly, C., Garro, L. Narrative representations of illness and healing: Introduction. Social Science and Medicine. 1994;38(6):771–774.
Mattingly, C., Lawlor, M. Learning from stories: Narrative interviewing in cross-cultural research. Scandinavian Journal of Occupational Therapy. 2000;7(1):1–4.
McEvoy, P. Interviewing colleagues: Addressing the issues of perspective, inquiry and representation. Nurse Researcher. 2001;9(2):49–59.
McNett, M.M. The PhD-prepared nurse in the clinical setting. Clinical Nurse Specialist. 2006;20(3):134–138.
Mental Health Act. Victorian Parliament. Legislative Assembly and Council, 1986.
Miles, M.B., Huberman, A.M. Qualitative data analysis: A sourcebook of new methods, (2nd ed.). Beverly Hills, CA: Sage; 1994.
Morgan, D.L. Why things (sometimes) go wrong in focus groups. Qualitative Health Research. 1995;5(4):516–523.
Morrison, R.S., Peoples, L. Using focus group methodology in nursing. Journal of Continuing Education in Nursing. 1999;30(2):62–65.
Morse, J.M. Learning to drive from a manual? Qualitative Health Research. 1997;7(2):181–183.
Moyle, W. Unstructured interviews: Challenges when participants have a major depressive illness. Journal of Advanced Nursing. 2002;39(3):266–273.
Mu, P., Lin, S. An oral historical study of the development of the discipline of military nursing in Taiwan from 1948 to 1970. Journal of Nursing Research. 2007;15(2):117–126.
Mulhall, A. In the field: Notes on observation in qualitative research. Journal of Advanced Nursing. 2003;41(3):306–313.
Mullings, L., Wali, A., McLean, D., Mitchell, J., Prince, S., Thomas, D. Qualitative methodologies and community participation in examining reproductive experiences: The Harlem Birth Right Project. Maternal and Child Health Journal. 2001;5(2):85–93.
Munhall, P.L. Ethical considerations in qualitative research. Western Journal of Nursing Research. 1988;10(2):150–162.
Munhall, P.L. Institutional review of qualitative research proposals: A task of no small consequence. In: Morse J.M., ed. Qualitative nursing research: A contemporary dialogue. London: Sage, 1991.
Munro, B.H. Doctorally prepared nurses in clinical settings. Clinical Nurse Specialist. 2001;15(5):197–198.
Newton, M.E. The case for historical research. Nursing Research. 1965;14(1):20–26.
Noel, N.L. Historiography: Biography of “Women Worthies” in nursing history. Western Journal of Nursing Research. 1988;10(1):106–108.
Northcott, N. Cognitive mapping: An approach to qualitative data analysis. NT Research. 1996;1(6):456–464.
Nwoga, I. Mother-daughter conversation related to sex-role socialization and adolescent pregnancy. Gainesville: University of Florida, 1997. [Unpublished doctoral dissertation].
Nwoga, I. African American mothers use stories for family sexuality education. MCN, American Journal of Maternal Child Nursing. 2000;25(1):31–36.
Oiler, C. The phenomenological approach in nursing research. Nursing Research. 1982;31(3):178–181.
Pallikkathayil, L., Morgan, S.A. Phenomenology as a method for conducting clinical research. Nursing Research. 1991;4(4):195–200.
Palmerino, M.B. Market research: Talk is best when it’s one-on-one. Take a quality approach to qualitative research. Marketing News. 1999, June 7;33(12):35.
Parse, R.R. Health: A personal commitment. Nursing Science Quarterly. 1990;3(3):136–140.
Pateman, B. Computer-aided qualitative data analysis: The value of NUD*IST and other programs. Nurse Researcher. 1998;5(3):77–89.
Patterson, B., Kelly, L. Lessons learned: One experience with focus groups in a school setting. Journal of School Nursing. 2005;21(3):6–11.
Penney, W., Wellard, S.J. Hearing what older consumers say about participation in their care. International Journal of Nursing Practice. 2007;13(1):61–68.
Podolefsky, A., McCarty, C. Topical sorting: A technique for computer assisted qualitative data analysis. American Anthropologist. 1983;85(4):886–890.
Polkinghorne, D.E. Narrative knowing and the human sciences. Albany, NY: State University of New York Press, 1988.
Porter, E.J. On “being inspired” by Husserl’s phenomenology: Reflections on Omery’s exposition of phenomenology as a method of nursing research. Advances in Nursing Science. 1998;21(1):16–28.
Price, B. Laddered questions and qualitative data research interviews. Journal of Advanced Nursing. 2002;37(3):273–281.
Quine, S., Cameron, I. The use of focus groups with the disabled elderly. Qualitative Health Research. 1995;5(4):454–462.
Rafael, A.R.F. Advocacy oral history: A research methodology for social activism in nursing; methods of clinical inquiry. Advances in Nursing Science. 1997;20(2):32–44.
Reed, J., Payton, V.R. Focus groups: Issues of analysis and interpretation. Journal of Advanced Nursing. 1997;26(4):765–771.
Reinharz, S. Feminist methods in social research. New York: Oxford University Press, 1992.
Rhodes, L.A. Emptying beds: The work of an emergency psychiatric unit. Berkeley: University of California Press, 1991.
Riley, R. Snapshots of live theatre: Rethinking the governance of operating room nursing through a discourse analysis of communication processes. Melbourne: University of Melbourse, 2005. [Unpublished Ph.D. thesis].
Riley, R.G., Manias, E. Governance in operating room nursing: Nurses’ knowledge of individual surgeons. Social Science & Medicine. 2006;62(6):1541–1551.
Roberts, M. The production of the psychiatric subject: Power, knowledge and Michel Foucault. Nursing Philosophy. 2005;6(1):33–42.
Robinson, C.A., Thorne, S.E. Dilemmas of ethics and validity in qualitative nursing research. Canadian Journal of Nursing Research. 1988;20(1):65–76.
Rodgers, B.L. Concepts, analysis and the development of nursing knowledge: The evolutionary cycle. Journal of Advanced Nursing. 1989;14(4):330–335.
Roesler, C. A narratological methodology for identifying archetypal story patterns in autobiographical narratives. Journal of Analytical Psychology. 2006;51(4):574–586.
Rosenberg, C. Clio and caring: An agenda for American historians and nursing. Nursing Research. 1987;36(1):67–68.
Ruffing-Rahal, M.A. Personal documents and nursing theory development. Advances in Nursing Science. 1986;8(3):50–57.
Sandelowski, M. Notes on transcription. Research in Nursing & Health. 1994;17(4):311–314.
Sandelowski, M. On the aesthetics of qualitative research. Image—Journal of Nursing Scholarship. 1995;27(3):205–209.
Sandelowski, M. Qualitative analysis: What it is and how to begin. Research in Nursing & Health. 1995;18(4):371–375.
Sandelowski, M. “To be of use”: Enhancing the utility of qualitative research. Nursing Outlook. 1997;45(3):125–132.
Sandelowski, M., Barroso, J. Handbook for synthesizing qualitative research. New York: Springer, 2007.
Sarbin, T.R., eds. Narrative psychology: The storied nature of human conduct. New York: Praeger, 1986.
Seng, J.S. Praxis as a conceptual framework for participatory research in nursing. Advances in Nursing Science. 1998;20(4):37–48.
Silverman, D. Doing qualitative research: A practical handbook, (2nd ed.). London: Sage, 2005.
Sim, J. Collecting and analyzing qualitative data: Issues raised by the focus group. Journal of Advanced Nursing. 1998;28(2):345–352.
Smith, J.A. The idea of health: Doing foundational inquiry. In: Munhall P.L., Oiler C.J., eds. Nursing research: A qualitative perspective. East Norwalk, CT: Appleton-Century-Crofts; 1986:251–262.
SmithBattle, L. Learning the baby: An interpretative study of teen mothers. Journal of Pediatric Nursing. 2007;22(4):261–271.
Sorensen, E.S. Historiography: Archives as sources of treasure in historical research. Western Journal of Nursing Research. 1988;10(5):666–670.
Southern, D.M., Batterham, R.W., Appleby, N.J., Young, D., Dunt, D., Guibert, R. The concept mapping method: An alternative to focus group inquiry in general practice. Australian Family Physician. 1999;28(Suppl. 1):35–40.
Sterling, Y., McNally, J. Clinical practice of doctorally prepared nurses. Clinical Nurse Specialist. 1999;13(6):296–301.
Stern, P.N. Grounded theory methodology: Its uses and processes. Image: Journal of Nursing Scholarship. 1980;12(1):20–23.
St John, W., Johnson, P. The pros and cons of data analysis software for qualitative research. Journal of Nursing Scholarship. 2000;32(4):393–397.
Straw, R.B., Smith, M.W. Potential uses of focus groups in federal policy and program evaluation studies. Qualitative Health Research. 1995;5(4):421–427.
Strickland, C.J. Conducting focus groups cross-culturally: Experiences with Pacific Northwest Indian people. Public Health Nursing. 1999;16(3):190–197.
Sullivan, K. Managing the “sensitive” research interview: A personal account. Nurse Researcher. 1998;6(2):72–85.
Taft, L.B. Computer-assisted qualitative research. Research in Nursing & Health. 1993;16(5):379–383.
Tanner, C.A., Benner, P., Chesla, C., Gordon, D.R. The phenomenology of knowing the patient. Image: Journal of Nursing Scholarship. 1993;25(4):273–280.
Thompson, J.L. Critical scholarship: The critique of domination in nursing. Advances in Nursing Science. 1987;10(1):27–38.
Todres, L. The qualitative description of human experience: The aesthetic dimension. Qualitative Health Research. 1998;8(1):121–127.
Turner, B. Some practical aspects of qualitative data analysis: One way of organizing the cognitive processes associated with the generation of grounded theory. Quality and Quantity. 1981;15(3):225–247.
Twinn, S. An analysis of the effectiveness of focus groups as a method of qualitative data collection with Chinese populations in nursing research. Journal of Advanced Nursing. 1998;28(3):654–661.
Van Kaam, A.L., Existential foundations of psychology, Vol. 3. Pittsburgh, PA: Duquesne University Press, 1966.
Ventres, W. Hearing the patient’s story: Exploring physician-patient communication using narrative case reports. Family Practice Research Journal. 1994;14(2):139–147.
Walsh, D., Downe, S. Appraising the quality of qualitative research. Midwifery. 2006;22(2):108–119.
Waring, L.M. Developing the research prospectus. In: Fitzpatrick M.L., ed. Historical studies in nursing. New York: Teachers College; 1978:18–20.
Watts, J. ”The outsider-within”: Dilemmas of qualitative feminist research within a culture of resistance. Qualitative Research. 2006;6(3):385–402.
Williamson, T., Long, A.F. Qualitative data analysis using data displays. Nurse Researcher. 2005;12(3):7–19.
Wilmpenny, P., Gass, J. Interviewing in phenomenology and grounded theory: Is there a difference? Journal of Advanced Nursing. 2000;31(6):1485–1492.
Zoffmann, V., Kirkevold, M. Relationships and their potential for change developed in difficult type 1 diabetes. Qualitative Health Research. 2007;17(5):625–638.