Frameworks
A framework is an abstract, logical structure of meaning. It guides the development of the study and enables you to link the findings to the body of knowledge used in nursing. Frameworks are used in both quantitative and qualitative research. In quantitative studies, the framework is a testable theory that may emerge from a conceptual model or may develop inductively from published research or clinical observations. In qualitative research, the initial framework is a philosophy or worldview; a theory consistent with the philosophy may be developed as an outcome of the study.
Every quantitative study has a framework, even when that framework is not explicitly expressed. The framework should be well integrated with the methodology, carefully structured, and clearly presented. When you critically appraise studies to determine if you will apply them in clinical practice or to develop a study, you must be able to identify and evaluate the framework. Your ability to understand the meaning of study findings will depend on your ability to understand the logic within the framework and determines how you will use the findings. Thus, your ability to apply the findings of a study grows when you understand the framework and can relate it to the findings for use in your nursing practice. To help you build the knowledge and skills needed to develop a framework, this chapter explains relevant terms, describes how frameworks are constructed, and discusses the critical analysis of frameworks.
DEFINITION OF TERMS
The first step in understanding theories and frameworks is to familiarize yourself with the terms related to theoretical ideas and their application. These terms and the ways they are used come from the philosophy of science, where the main concern is the nature of scientific knowledge. As nurses have studied philosophies of science, philosophies of nursing science are beginning to emerge.
In the following section, we explain terms such as concept, relational statement, conceptual model, theory, and conceptual map. Within philosophies of science, the term theory is used in a variety of ways that could include both theories and conceptual models (Suppe & Jacox, 1985). In philosophies of nursing science, however, theory tends to be defined narrowly and is different from the term conceptual model.
Concept
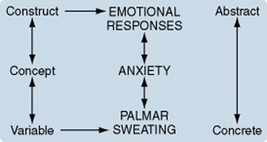
A concept is a term that abstractly describes and names an object, a phenomenon, or an idea, thus providing it with a separate identity or meaning. An example of a concept is the term anxiety. At high levels of abstraction, such as is found in conceptual models, concepts have general meanings and are sometimes referred to as constructs. For example, a construct associated with the concept of anxiety might be “emotional responses.”
At a more concrete level, terms are referred to as variables and have narrow definitions. A variable is more specific than a concept and implies that the term is defined so that it is measurable. The word variable implies that the numerical values associated with the term vary from one instance to another. A variable related to anxiety might be “palmar sweating,” which the researcher can measure by assigning numerical values to different amounts of sweat on the subject’s palm. The links among constructs, concepts, and variables are illustrated here:
Defining concepts allows us to be consistent in the way we use a term in the discipline, apply it to a theory, and incorporate it in a field of study. A conceptual definition differs from the denotative (or dictionary) definition of a word. A conceptual definition (connotative meaning) is more comprehensive than a denotative definition because it includes associated meanings the word may have. For example, we may connotatively associate the term “fireplace” with images of hospitality and warm comfort, whereas the dictionary definition would be more concrete and narrower. A conceptual definition can be established through concept synthesis, concept derivation, or concept analysis.
Concept Synthesis
In nursing, many phenomena have not yet been identified as discrete entities. However, recognizing, naming, and describing these phenomena are often critical steps to understanding the process and outcomes of nursing practice. The process of describing and naming a previously unrecognized concept is concept synthesis. In the discipline of medicine, Selye (1976) performed concept synthesis to identify and define the concept of stress. Before his work, stress was not known as a phenomenon. Nursing studies often involve previously unrecognized and unnamed phenomena that must be named and carefully defined. Concept synthesis is also important in the development of nursing theory (Walker & Avant, 2004).
Concept Derivation
In some cases, the researcher may obtain conceptual definitions from theories in other disciplines. A conceptual definition obtained in this way will explain a phenomenon important to a non-nursing discipline. Therefore, it will need to be carefully evaluated to determine whether or not it has the same conceptual meaning within nursing. The conceptual definition may need to be modified so that it is meaningful within nursing and consistent with nursing thought (Walker & Avant, 2004). This process, referred to as concept derivation, may require a concept analysis that examines the use of the concept in nursing literature, compares the results with the existing conceptual definition, and, if the two are different, modifies the definition to be consistent with nursing usage.
Concept Analysis
Concept analysis is a strategy that identifies a set of characteristics essential to the connotative meaning of a concept. The procedure will require you to explore the various ways the term is used and to identify a set of characteristics that clarify the range of objects or ideas to which that concept may be applied. You will also use these characteristics to distinguish the concept from similar concepts. Several approaches to concept analysis have been described in the literature, and the authors of these strategies are listed in Table 7-1. In addition, a number of concept analyses have been published in the nursing literature, such as those listed in Table 7-2. Concept analysis is a type of philosophical inquiry, although not all concept analyses follow the philosophical format; an example of a philosophical concept analysis is provided in Chapter 23. Multiple concept analyses are often performed related to a selected concept until there is some degree of consensus within the discipline regarding the conceptual definition. Conceptual definition often leads to methods for measuring the concept and to theories as well.
TABLE 7-1
Publications on How to Conduct a Concept Analysis
| Author | Date | Publication |
| Avant | 2000 | The Wilson method of concept analysis. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Broome | 2000 | Integrated literature reviews in the development of concepts. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Caron & Bowers | 2000 | Methods and applications of dimensional analysis: A contribution to concept and knowledge development in nursing. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Chinn & Kramer | 2007 | Integrated Theory and Knowledge Development in Nursing. |
| Haase, Leidy, Coward, Britt, & Penn | 2000 | Simultaneous concept analysis: A strategy for developing multiple interrelated concepts. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Lackey | 2000 | Concept clarification: Using the Norris method in clinical research. Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Maas et al. | 2000 | Concept development of nursing-sensitive outcomes. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Morse | 2000 | Exploring pragmatic utility: Concept analysis by critically appraising the literature. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Rodgers | 2000 | Concept analysis: An evolutionary view. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Sadler | 2000 | A multiphase approach to concept analysis and development. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Schwartz-Barcott & Kim | 2000 | An expansion and elaboration of the hybrid model of concept development. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
| Walker & Avant | 2004 | Strategies for Theory Construction in Nursing. |
| Wuest | 2000 | Concept development situated in the critical paradigm. In Concept Development in Nursing: Foundations, Techniques, and Applications. |
Importance of a Conceptual Definition: An Example
Morse, Solberg, Neander, Bottorff, and Johnson (1990) illustrated the importance of a conceptual definition. They analyzed published definitions of the concept of caring in a project funded by the National Center for Nursing Research. In examining previous conceptual definitions of caring, Morse and colleagues found that authors had difficulty separating meanings for caring, care, and nursing care. Caring may be an action, such as “taking care of,” or a concern, such as “caring about.” On the other hand, caring may be viewed from the perspective of the nurse or of the patient. Each of these perspectives alters how caring is conceptually defined. How might a nurse practitioner define caring?
Morse et al. (1990) used content analysis to examine how 35 authors defined the term caring. The analysis included definitions of caring from three nursing theorists: Orem, Watson, and Leininger. The researchers identified five categories of caring: (1) caring as a human trait, (2) caring as a moral imperative, (3) caring as an affect, (4) caring as an interpersonal relationship, and (5) caring as a therapeutic intervention. In addition, they identified two outcomes of caring: (1) the subjective experience of the patient and (2) the physical response of the patient. The following questions emerged from the analysis:
1. “Is caring a constant and uniform characteristic, or may caring be present in various degrees within individuals?” (Morse et al., 1990, p. 9).
2. Is caring an emotional state that can be depleted?
3. “Can caring be nontherapeutic? Can a nurse care too much?” (Morse et al., 1990, p. 10).
4. Can cure occur without caring? Can a nurse engage in safe practice without caring?
5. “What difference does caring make to the patient?” (Morse et al., 1990, p. 11)
These researchers concluded that, at the time of their analysis, a clear conceptual definition of caring did not exist. Their careful analysis has stimulated curiosity within the nursing practice as nurse scholars continue to seek a better understand of the concept of caring as it is used in nursing. Since their study, theoretical work—including additional literature reviews and concept analyses on caring—has increased, not just in the United States but across the world (Table 7-3).
TABLE 7-3
| Year | Author | Title |
| 1990 | Marck | Therapeutic reciprocity: A caring phenomenon |
| 1991 | Roberts & Fitzgerald | Serenity: Caring with perspective |
| 1992 | Eriksson | The alleviation of suffering: The idea of caring |
| 1992 | Eriksson | Different forms of caring communion |
| 1992 | O’Berle & Davies | Support and caring: Exploring the concepts |
| 1992 | Pepin | Family caring and caring in nursing |
| 1993 | Jones & Alexander | The technology of caring: A synthesis of technology and caring for nursing administration |
| 1995 | Buchanan & Ross | A concept analysis of caring |
| 1995 | Fealy | Professional caring: The moral dimension |
| 1995 | Kyle | The concept of caring: A review of the literature |
| 1995 | Scott | Correlates of health promotion in elders |
| 1995 | Smith | An analysis of altruism: A concept of caring |
| 1997 | McCance, McKenna, & Boore | Caring: Dealing with a difficult concept |
| 1997 | Sherwood | Meta-synthesis of qualitative analyses of caring: Defining a therapeutic model of nursing |
| 1997 | Sourial | An analysis of caring |
| 1997 | Wilde | The caring connection in nursing: A concept analysis |
| 1998 | Kelly | Caring and cancer nursing: Framing the reality using selected social science theory |
| 1998 | Wilkes & Wallis | A model of professional nurse caring: Nursing students’ experience |
| 1998 | Wilkinson | What it means to care |
| 1999 | Fredriksson | Modes of relating in a caring conversation: A research synthesis on presence, touch, and listening |
| 1999 | Patistea | Nurses’ perceptions of caring as documented in theory and research |
| 1999 | Rodriquez | Medicine or caring science in ancient Greece [Spanish] |
| 1999 | Smith | Caring and the science of unitary human beings |
| 1999 | Swanson | What is known about caring in nursing science: A literary meta-analysis |
| 1999 | Swanson | Effects of caring, measurement, and time on miscarriage impact and women’s well-being |
| 2000 | Priest | Focus: the use of narrative in the study of caring: A critique |
| 2001 | Kunyk & Olson | Clarification of conceptualizations of empathy |
| 2001 | Mattsson-Lidsle & Lindström | Consolation: A concept analysis [Swedish] |
| 2001 | McCance, McKenna, & Boore | Exploring caring using narrative methodology: An analysis of the approach |
| 2003 | Covington | Caring presence: Delineation of a concept for holistic nursing |
| 2003 | Duffy & Hoskins | The quality-caring model: Blending dual paradigms |
| 2003 | Lewis | Practice applications: Caring as being in nursing: Unique or ubiquitous? |
| 2003 | Lin & Chiou | Concept analysis of caring [Chinese] |
| 2004 | Coffey | Development of the concept of covenant between nurse and patient |
| 2004 | Pang et al. | Towards a Chinese definition of nursing |
| 2004 | Sadler | Descriptions of caring uncovered in student’s baccalaureate program admission essays |
| 2005 | Brilowski & Wendler | An evolutionary concept analysis of caring |
| 2005 | Brunelli | A concept analysis: the grieving process for nurses |
| 2005 | Cowling & Taliaferro | Emergence of a healing-caring perspective: Contemporary conceptual and theoretical directions |
| 2005 | Niu | The philosophy of nursing management: A concept analysis [Chinese] |
| 2006 | Fridh & Bergbom | To watch: A study of the concept [Norwegian] |
| 2006 | Coffey | The nurse-patient relationship in cancer care as a shared covenant: A concept analysis |
| 2006 | Sadler | In response to Brilowski & Wendler (2005) |
| 2006 | Sumner | Concept analysis: The moral construct of caring in nursing as communicative action |
| 2007 | Anderberg, Lepp, M., Berglund, A.L., & Segesten | Preserving dignity in caring for older adults: A concept analysis |
| 2007 | Schantz | Compassion: A concept analysis |
| 2007 | Finfgeld-Connett | Concept comparison of caring and social support |
A number of scales have been developed worldwide to measure caring in nursing (Table 7-4), and a number of qualitative studies have been conducted to gain insight on caring (Table 7-5). This work is increasing our understanding of caring in nursing, and enabling us to further implement caring in our practice. How might caring be measured in the work of nurse practitioners? Might qualitative studies increase the insight on caring in the primary care role?
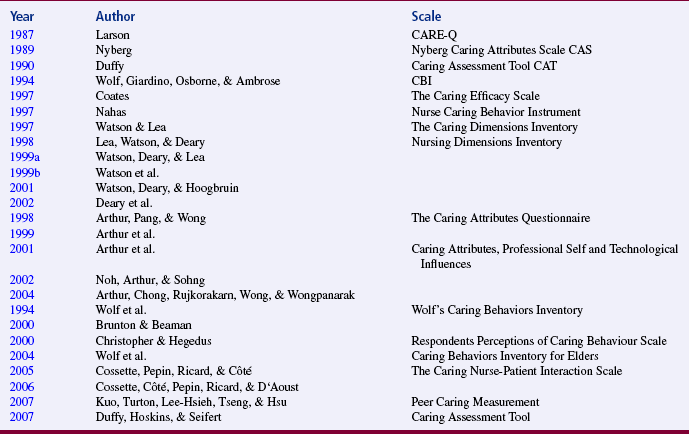
TABLE 7-5
| Year | Author | Title |
| 1995 | Fealy | Professional caring: The moral dimension |
| 1998 | Amendola | Toward a caring curriculum |
| 1998 | Fagerström, Eriksson, & Engberg | The patient’s perceived caring needs as a message of suffering |
| 1999 | Fredriksson | Modes of relating in a caring conversation: A research synthesis on presence, touch and listening |
| 1999 | Joudrey & Gough | Caring and curing revisited: Student nurses’ perceptions of nurses’ and physicians’ ethical stances |
| 1999 | Patistea | Nurses’ perceptions of caring as documented in theory and research |
| 1999 | Rodriquez | Medicine or caring science in ancient Greece [Spanish] |
| 1999 | Smith | Caring and the science of unitary human beings |
| 1999 | Smith-Campbell | A case study on expanding the concept of caring from individuals to communities |
| 2001 | Henderson | Emotional labor and nursing: An under-appreciated aspect of caring work |
| 2001 | Johns | Reflective practice: Revealing the [he]art of caring |
| 2001 | Turkel, Ray & Malinski | Relational complexity: From grounded theory to instrument development and theoretical testing |
| 2002 | Barnhill | The perception of caring in labor and delivery: a phenomenological study |
| 2002 | Schoenhofer | Theoretical concerns: Philosophical underpinnings of an emergent methodology for nursing as caring inquiry |
| 2002 | Yonge & Molzahn | Exceptional nontraditional caring practices of nurses |
| 2003 | Cortis & Kendrick | Nursing ethics, caring and culture |
| 2003 | Fredriksson & Eriksson | The ethics of the caring conversation |
| 2003 | Helin & Lindström | Sacrifice: An ethical dimension of caring that makes suffering meaningful |
| 2003 | McCance | Caring in nursing practice: The development of a conceptual framework |
| 2003 | Rogers | Nursing: An ethic of caring |
| 2003 | Söderlund | Qualitative research approaches of relevance for caring sciences [Swedish] |
| 2004 | Celich & Crossetti | Being with the carer: A dimension of the caring process [Portuguese] |
| 2004 | Clark | Human caring theory: Expansion and explication |
| 2004 | Coffman | Cultural caring in nursing practice: A meta-synthesis of qualitative research |
| 2004 | Cowling & Taliaferro | Emergence of a healing-caring perspective: Contemporary conceptual and theoretical directions |
| 2004 | Forbat | The care and abuse of minoritized ethnic groups: The role of statutory services |
| 2004 | Gramling | Ice chips and hope: The coach’s story of caring art |
| 2004 | Gregg & Magilvy | Values in clinical nursing practice and caring |
| 2004 | Lake | Transformation: Student nurses’ experiences in learning the caring process in nursing |
| 2004 | Lucena & Crossetti | The meaning of caring in the intensive care unit [Portuguese] |
| 2004 | McIntosh | Nurses’ experiences with healing and spirituality |
| 2005 | Biley & Bauer | Bringing the heart back to nursing: Human caring practice and education in Germany and the UK |
| 2005 | Brand | The lived experiences of six women during adjuvant chemotherapy for stage l or ll breast cancer |
| 2005 | Budo & Saupe | Ways of care in rural communities: Culture permeating the nursing care [Portuguese] |
| 2005 | Schumacher | Caring behaviors of preceptors as perceived by new nursing graduate orientees |
| 2005 | Wannapornsiri, Sindhu, Phancharoenworakul, & Gasemgitvatana | Caring process of Thai women with breast cancer receiving chemotherapy |
| 2006 | Coelho | Caring gestures in nursing [Portuguese] |
| 2006 | Delmar | Caring-ethical phronetic research: Epistemological considerations |
| 2006 | Hupcey & Miller | Community dwelling adults’ perception of interpersonal trust vs. trust in health care providers |
| 2006 | Jensen | To see with the heart’s eye [Danish] |
| 2006 | Lindholm, Nieminen, Mäkelä, & Rantanen-Siljamäki | Clinical application research: A Hermeneutical approach to the appropriation of caring science |
| 2006 | Liu, Mok, & Wong | Caring in nursing: Investigating the meaning of caring from the perspective of cancer patients in Beijing, China |
| 2006 | Nåden & Saeteren | Cancer patients’ perception of being or not being confirmed |
| 2006 | Perini et al. | The meaning of caring from the viewpoint of patients with wounds due to peripheral vascular disease [German] |
| 2006 | Sun, Long, Boore, & Tsao | Patients and nurses’ perceptions of ward environmental factors and support systems in the care of suicidal patients |
Relational Statements
A relational statement declares that a relationship of some kind exists between or among two or more concepts (Walker & Avant, 2004). Relational statements form the core of a framework. Skills in expressing statements are essential for constructing an integrated framework that will, in turn, lead to a well-designed study. The statements expressed in your framework will determine (1) your objective, question, or hypothesis; (2) your study’s design; (3) the statistical analyses you will perform; and (4) the type of findings you can expect. Frameworks developed with inadequate expression of statements provide only a broad orientation for the study and do not guide the research process.
Understanding relational statements is essential also for appraising frameworks. Being able to evaluate the links among the hypotheses, the design, and the framework is also an essential part of determining the quality of a study. Judging whether the study was successful depends, in part, on identifying the statements in the framework and tracking their examination by the study.
Characteristics of Relational Statements
Relational statements describe the direction, shape, strength, symmetry, sequencing, probability of occurrence, necessity, and sufficiency of a relationship (Fawcett, 1999; Stember, 1986; Walker & Avant, 2004). One statement may have several of these characteristics; each characteristic is not exclusive of the others. Statements may be expressed in literary form (such as a sentence), in diagrammatic form (such as a conceptual map), or in mathematical form (such as an equation). Statements in nursing tend to be expressed in literary and diagrammatic forms.
Direction: The direction of a relationship may be positive, negative, or unknown. A positive linear relationship implies that as one concept changes (the value or amount of the concept increases or decreases), the second concept will also change in the same direction. For example, the literary statement “The risk of illness (A) increases as stress (B) increases” expresses a positive relationship. This positive relational statement could also be expressed as “The risk of illness decreases as stress decreases.” This relationship could be diagramed as follows:

A negative linear relationship implies that as one concept changes, the other concept changes in the opposite direction. For example, the literary statement “As relaxation (A) increases, blood pressure (B) decreases” expresses a negative linear relationship. This relationship could be diagrammed as follows:

If a relationship is believed to exist but the nature of the relationship is unclear, the following diagram could be used to depict it:

This last type of statement might be appropriate for discussing the relationship between coping and social support. We might say that although there is evidence that a relationship exists between these two concepts, the studies examining that relationship have conflicting findings. For example, some researchers find coping to be positively related to social support—that is, as social support increases, coping increases. However, others may find a negative relationship—that is, as social support increases, coping decreases. Thus, the nature of the relationship between coping and social support is uncertain. It is possible that the conflicting findings may result from differences in how the two concepts have been defined and measured in various studies. But perhaps there is a confounding variable that has not been identified that changes the relationship between coping and social support.
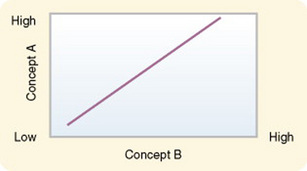
Shape: Most relationships are assumed to be linear, and statistical tests are conducted to look for linear relationships. In a linear relationship, the relationship between the two concepts remains consistent regardless of the values of each of the concepts. For example, if the value of A increases by 1 point each time the value of B increases by 1 point, then the values continue to increase at the same rate whether the value is 2 or 200. The relationship can be illustrated by a straight line, as shown in Figure 7-1.
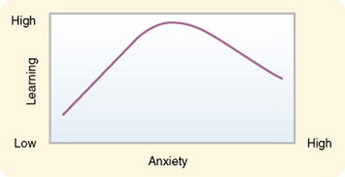
Relationships can also be curvilinear or form some other shape. In a curvilinear relationship, the relationship between two concepts varies according to the relative values of the concepts. The relationship between anxiety and learning is a good example of a curvilinear relationship. Very high or very low levels of anxiety are associated with low levels of learning, whereas moderate levels of anxiety are associated with high levels of learning (Fawcett, 1999). This type of relationship is illustrated by a curved line, as shown in Figure 7-2.
Strength: The strength of a relationship is the amount of variation explained by the relationship. Some of the variation in a concept, but not all, is associated with variation in another concept. In discussing the strength of a relationship, researchers sometimes use the term effect size. The effect size explains how much “effect” variation in one concept has on variation in a second concept.
In some cases, a large portion of the variation can be explained by the relationship; in others, only a moderate or a small portion of the variation can be explained by the relationship. For example, one might examine the strength of the relationship between coping and compliance. A portion of the variance in a measure of compliance is associated with the measure of a person’s coping ability, but the remaining portion of this variation cannot be explained by how well a person copes. Conversely, only a portion of variation in a measure of a person’s ability to cope can be explained by variation in a measure of his or her compliance. The portions of the two concepts that are associated are explained by the strength of the relationship.
Strength is usually determined by correlational analysis and is expressed mathematically by a correlation coefficient such as the following:

The statistic r is the coefficient obtained by performing the statistical procedure known as Pearson’s product moment correlation. A value of 0 indicates no strength, whereas a +1 or a –1 indicates the greatest strength, as signified in the following diagram:
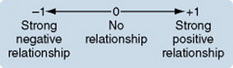
The + or – does not have an impact on strength. For example, r = –0.35 is as strong as r = +0.35. A weak relationship is usually considered one with an r value of 0.1 to 0.3; a moderate relationship is one with an r value of 0.31 to 0.5; and a strong relationship is one with an r value greater than 0.5. The greater the strength of a relationship, the easier it is to detect relationships between the variables being studied. We explore this idea further in the chapters on sampling, measurement, and data analysis.
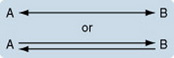
Symmetry: Relationships may be symmetrical or asymmetrical. In an asymmetrical relationship, if A occurs (or changes), then B will occur (or change); but there may be no indication that if B occurs (or changes), A will occur (or change) (Fawcett, 1999). A previously cited example showed that when changes in a person’s relaxation level (A) occurred, changes in blood pressure (B) occurred. However, one cannot say that when changes in blood pressure occur, changes in relaxation levels occur. Therefore, the relationship is asymmetrical. An asymmetrical relationship may be diagrammed as follows:

A symmetrical relationship is complex and contains two statements, such as if A occurs (or changes), B will occur (or change); if B occurs (or changes), A will occur (or change) (Fawcett, 1999). An example is the symmetrical relationship between the occurrences of cancer and impaired immunity. As the cancer increases, impaired immunity increases; as impaired immunity increases, cancer increases. A symmetrical relationship may be diagrammed as follows:
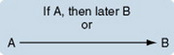
Sequencing: Time is the important factor in explaining the sequential nature of a relationship. If both concepts occur simultaneously, the relationship is concurrent (Fawcett, 1999). The relationship between relaxation (A) and blood pressure (B) may seem to be concurrent. If so, it would be expressed as follows:

If one concept occurs later than the other, the relationship is sequential. If relaxation (A) was thought to occur first, and then blood pressure (B) decreased, the relationship is sequential. This relationship is expressed as follows:
Probability of Occurrence: A relationship can be deterministic or probabilistic depending on the degree of certainty that it will occur. Deterministic (or causal) relationships are statements of what always occurs in a particular situation. A scientific law is one example of a deterministic relationship (Fawcett, 1999). It is expressed as follows:

Another deterministic relationship describes what always happens if no conditions interfere. This is referred to as a tendency statement. A tendency statement might propose that an immobilized patient lying in a typical hospital bed (A) will always develop pressure sores (B) after 6 weeks if there are no interfering conditions. A tendency statement would be expressed in the following form:

A probability statement expresses the probability that something will happen in a given situation (Fawcett, 1999). This relationship is expressed as follows:

Probability statements are tested statistically to determine the extent of probability that B will occur in the event of A. For example, one could state that there is greater than a 50% probability that a patient who has an indwelling catheter for 1 week will experience a urinary bladder infection. This probability could be expressed mathematically as follows:

The p is a symbol for probability. The > is a symbol for “greater than.” This mathematical statement asserts that there is more than a 50% probability that the relationship will occur.
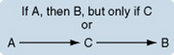
Necessity: In a necessary relationship, one concept must occur for the second concept to occur. For example, one could propose that if sufficient fluids are administered (A), and only if sufficient fluids are administered, then the unconscious patient will remain hydrated (B). This relationship is expressed as follows:

In a substitutable relationship, a similar concept can be substituted for the first concept and the second concept will still occur. For example, a substitutable relationship might propose that if tube feedings are administered (A1), or if hyperalimentation is administered (A2), the unconscious patient can remain nourished (B). This relationship is expressed as follows:

Sufficiency: A sufficient relationship states that when the first concept occurs, the second concept will occur, regardless of the presence or absence of other factors (Fawcett, 1999). A statement could propose that if a patient is immobilized in bed longer than a week, he or she will lose bone calcium, regardless of anything else. This relationship is expressed as follows:

A contingent relationship will occur only if a third concept is present. For example, a statement might claim that if a person experiences a stressor (A), the person will manage the stress (B), but only if she or he uses effective coping strategies (C). The third concept, in this case effective coping strategies, is referred to as an intervening (or mediating) variable. Intervening variables can affect the occurrence, strength, or direction of a relationship. A contingent relationship can be expressed as follows:
Statement Hierarchy
Statements about the same two conceptual ideas can be made at various levels of abstractness. The statements found in conceptual models (general propositions) are at a high level of abstraction. Statements found in theories (specific propositions) are at a moderate level of abstraction. Hypotheses, which are a form of statement, are at a low level of abstraction and are specific. As statements become less abstract, they become narrower in scope (Fawcett, 1999), as shown in the following diagram:
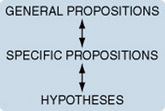
Statements at varying levels of abstraction that express relationships between or among the same conceptual ideas can be arranged in hierarchical form, from general to specific. This arrangement allows you to see (or evaluate) the logical links among the various levels of abstraction. Statement sets link the relationships expressed in the framework with the hypotheses, research questions, or objectives that guide the methodology of the study.
Roy and Roberts (1981) developed statement sets related to Roy’s nursing model that could be used in frameworks for research, as shown in the following excerpts.
“The magnitude of the internal and external stimuli will positively influence the magnitude of the physiological response of an intact system.” (Roy & Roberts, 1981, p. 90)
“The amount of mobility in the form of exercising positively influences the level of muscle integrity.” (Roy & Roberts, 1981, p. 90)
“If the nurse helps the patient maintain muscle tone through proper exercising, the patient will experience fewer problems associated with immobility.” (Roy & Roberts, 1981, p. 90)
Conceptual Models
A conceptual model is a set of highly abstract, related constructs. It broadly explains phenomena of interest, expresses assumptions, and reflects a philosophical stance. A number of conceptual models have been developed in nursing. For example, Roy’s (1984, 1988, 1990) model describes adaptation as the primary phenomenon of interest to nursing. This model identifies the constructs she considers essential to adaptation and how these constructs interact to produce adaptation. Orem (2001) considered self-care to be the phenomenon central to nursing. Her model explains how nurses facilitate the self-care of clients. Rogers (1970, 1980, 1983, 1986, 1988) regarded human beings as the central phenomenon of interest to nursing, and her model is designed to explain the nature of human beings. A conceptual model may use the same or similar constructs as other models but define them in different ways. Thus, Roy, Orem, and Rogers may all use the construct health but define it in different ways.
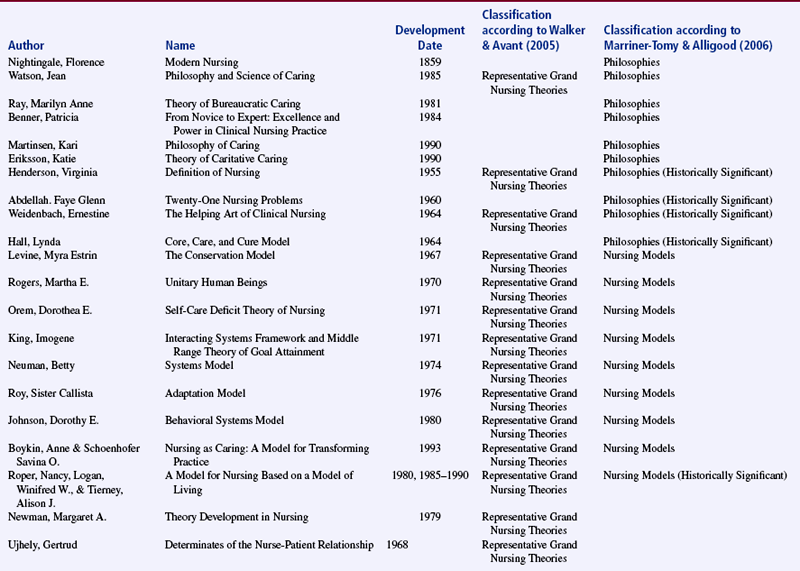
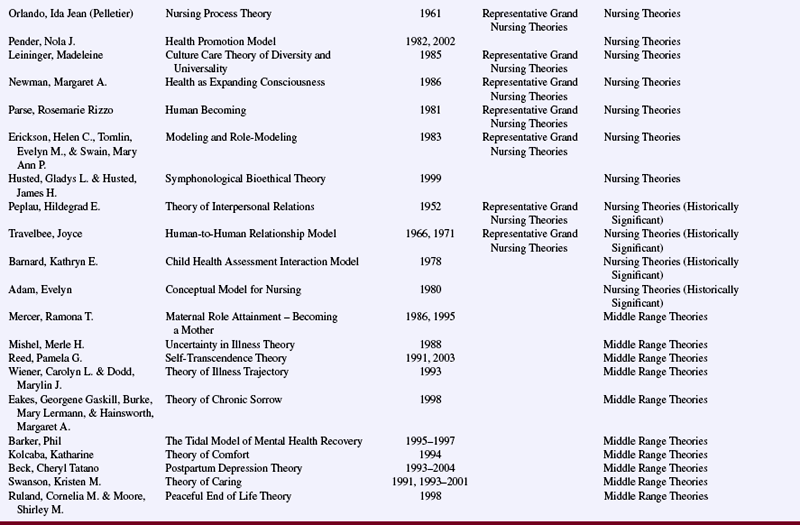
Most disciplines have several conceptual models, each with a distinctive vocabulary. Table 7-6 lists some of the conceptual models or grand theories in nursing. These philosophical and theoretical statements of nursing vary in their level of abstraction and the breadth of phenomena they explain. However, each provides an overall picture, a gestalt of the phenomena they explain. It is not their purpose to provide detail or to be specific. Most are not directly testable through research and thus cannot be used alone as the framework for a study (Fawcett, 1999; Walker & Avant, 2004). However, a framework can include a combination of a more abstract conceptualization of nursing and a theory.
An organized program of research is important for building a body of knowledge related to the phenomena explained by a particular conceptual model. This program of research is referred to as a research tradition. To develop a research tradition for a particular model, a group of scholars must be willing to dedicate time and energy to this endeavor. Middle-range theories compatible with the model must be developed. The research tradition for the conceptual model must be defined. The definition must (1) identify acceptable strategies for developing and testing theory on the basis of the model, (2) define the phenomena to be studied, (3) establish priorities for testing theory statements, (4) develop research methods and measurement techniques, (5) describe data collection strategies, and (6) select acceptable approaches to data analyses (Fawcett, 1999). These research traditions should include the advanced practice roles in nursing and their phenomena.
Researchers conducting studies consistent with a particular tradition may be scattered across the country (or the world), but they often maintain a network of communication about their work. In some cases, they hold annual conferences that focus on the model. These gatherings give researchers the opportunity to share findings, discuss methods, explore theoretical ideas, identify priorities for future research, and maintain network contacts. The organizations of advanced practice nurses should interface with organizations that conduct studies according to a particular tradition; this type of interaction will facilitate studies relevant to advanced nursing practice.
One example of a conceptual nursing model with an emerging research tradition is Orem’s model of self-care. Orem’s (2001) model focuses on the domain of nursing practice and on what nurses actually do. She proposed that individuals generally know how to take care of themselves (self-care). If they are dependent in some way, as are children, the aged, or the handicapped, family members take on this responsibility (dependent care). If individuals are ill or have some health problem (such as diabetes or a colostomy), they or their family members acquire special skills to provide that care (therapeutic self-care). An individual’s capacity to provide self-care is referred to as self-care agency. A self-care deficit occurs when self-care demand exceeds self-care agency (Hartweg & Orem, 1991).
An individual obtains nursing care only when there is a deficit in the self-care or dependent care that the individual and his or her family can provide (self-care deficit). In this case, the nurse or nurses develop a system to provide the needed care. This system involves prescribing, designing, and providing care. The goal of nursing care is to help the individual resume self-care independently or with family assistance. There are three types of nursing systems: wholly compensatory, partly compensatory, and supportive-educative. The system chosen is based on the person’s capacity to perform self-care.
A research tradition related to the testing of propositions of the theory requires a commitment to develop valid and reliable scales to measure the concepts of the theory. Instruments based on Orem’s model are shown in Table 7-7. Orem (2001) has developed three theories related to her model: the theory of self-care deficits, the theory of self-care, and the theory of nursing systems (also referred to as the general theory of nursing). Studies testing statements that have emerged from Orem’s theories appear in the literature (Table 7-8). Research methodologies acceptable for testing Orem’s theories have not been specified in the literature. Orem has suggested that researchers examine the qualitative characteristics of self-care, as well as its presence or absence. She also recommended studying the phases in which individuals (1) investigate the possibility of caring for themselves, (2) make the decision to do so, and (3) begin to engage in self-care behaviors. The focus of self-care in Orem’s work should provide a basis for research by nurse practitioners who, in most cases, must depend on the client’s self-care abilities to implement the instructions provided during primary care. Are there strategies that nurse practitioners could use to increase the self-care capabilities of their clients? Could the effectiveness of a new strategy be tested through research and published to guide other nurse practitioners?
TABLE 7-7
Development of Instruments to Measure Concepts in Orem’s Theories and Use in Studies
| Year | Instrument | Authors |
| 1979 | Exercise of Self-Care Agency Scale (translated to Chinese) | Ailinger & Deer, 1993; Beatty, 1991; Beauchesne, 1989; Brown, 1996; Carroll, 1995; Folden, 1990; Kearney & Fleischer, 1979; Mapanga, 1994; McBride, 1987, 1991 Pressly, 1995; Riesch & Hauck, 1988; St. Onge, 1988; Wang & Laffrey, 2001 |
| 1980 | Denyes Self-Care Agency Instrument–90 | Baker, 1991; Campbell & Soeken, 1999; Canty, 1993; Denyes, 1980; Hurst, 1991; James, 1991; Jesek-Hale, 1994; McBride, 1991; Monsen, 1988; Robinson, 1995; Schott-Baer, 1993; Slusher, 1999 |
| 1982 | Self-Care Agency in Adolescents | Denyes, 1982 |
| 1984 | Self-Care Behavior Log | Dodd, 1984b, 1987 |
| 1984 | Self-Care Behavior Questionnaire | Dodd 1984a, 1984b, 1987 |
| 1985 | Perception of Self-Care Agency | Greenfeld, 1989; Hanson & Bickel, 1985; McBride, 1991; McDermott, 1989; Weaver, 1987 |
| 1987 | ADL Self-Care Scale | Gulick, 1987, 1988, 1989; Mosher & Moore, 1998 |
| 1987 | Appraisal of Self-Care Agency Scale (translated to Chinese, Dutch, Norwegian, and Danish) Turkish, 2004 | Brown, 1996; Evers, Isenberg, Philipsen, Senten, & Brouns, 1993; Fok, Alexander, M.F., Wong, T.K., & McFayden, 2002; Hart, 1993; Hart & Foster, 1998; Isenberg, Evers, G., & Brouns, 1987; Lorensen, Holter, Evers, Isenberg, & van Achterberg, 1993; Nahcivan, 2004; Simmons, 1990; Soderhamn & Cliffordson, 2001; van Achterberg et al., 1991; Vannoy, 1989 |
| 1988 | Nurse Performance Evaluation Tool | Kostopoulos, 1988 |
| 1988 | Self-Care Agency Questionnaire | Bottorff, 1988; Koster, 1995; St. Onge, 1988 |
| 1988 | Self-Care Questionnaire | Riley, 1988 |
| 1989 | Denyes/Fildey Dependent-Care Agency Instrument | Haas, 1990; Moore & Gaffney, 1989; Moore & Mosher, 1997 |
| 1989 | Mother’s Performance of Self-Care Activities for Children | Moore & Gaffney, 1989 |
| 1990 | Denyes Health Status Instrument | Frey & Fox, 1990 |
| 1990 | Functional Status Instrument | Willard, 1990 |
| 1991 | Conditioning Factor Profile | Cull, 1995; McCaleb, 1991 |
| 1991 | Diabetes Self-Care Practices Instrument | Frey & Fox, 1990 |
| 1991 | Self-as-Carer Inventory | Freeman, 1992; Geden & Taylor, 1991; Lukkarinen & Hentinen, 1997; Metcalfe, 1996; White, 2000 |
| 1991 | Self-Care Agency Assessment | Gammon, 1991 |
| 1991 | Cystic Fibrosis Self-Care Practice Instrument | Baker, 1991 |
| 1992 | HIV-Specific Therapeutic Self-Care Demand Inventory | Freeman, 1992 |
| 1992 | HIV-Related Self-Care Behaviors Checklist | Freeman, 1992 |
| 1993 | Children’s Self-Care Performance Questionnaire | Moore, 1993; Moore & Mosher, 1997 |
| 1993 | Hart Prenatal Care Actions Scale | Hart, 1993 |
| 1993 | Task Scale (measures dependent care) | Schott-Baer, 1993 |
| 1995 | Bess’s Measurement of Diabetes Self-Care Practices Scale | Bess, 1995 |
| 1995 | Health Self-Determinism Index for Children | Koster, 1995 |
| 1995 | Maieutic Dimensions of Self-Care Agency | O’Connor, 1995 |
| 1995 | Self-Care of Older Persons Evaluation | Dellasega, 1995 |
| 1995 | Self-Care Practices of Children and Adolescents | Moore, 1995 |
| 1996 | Basic Conditioning Factors Form | Metcalfe, 1996 |
| 1996 | COPD Self-Care Knowledge Questionnaire | Metcalfe, 1996 |
| 1996 | COPD Self-Care Action Scale | Metcalfe, 1996 |
| 1996 | Self-Care Needs Inventory (French) | Page & Ricard, 1996 |
| 1998 | Self-Care Management and Life-Quality Amongst Elderly | Lorensen, 1998 |
| 2001 | Characterization of therapeutic self-care needs of an individual submitted to bone marrow transplantation (Portuguese) | da Silva, 2001 |
| 2001 | Heart Failure Self-Care Inventory | Ahrens, 2001 |
| 2002 | Revised Heart Failure Self-Care Behavior Scale | Artinian, Magnan, Sloan, & Lange, 2002 |
| 2003 | Facts on Osteoporosis Quiz – revised | Ailinger, Lasus, & Braun, 2003 |
| 2003 | Psychiatric Patients Caregiver Burden Scale | Pipatananond & Hanucharurnkul, 2003 |
| 2004 | Self-care scale for dysmenorrhic adolescents | Hsieh, Gau, Mao, & Li, 2004 |
TABLE 7-8
Studies Testing Statements from Orem’s Theories
| Year | Number of Studies | Researchers |
| 1988 | 2 | Alexander, Younger, Cohen, & Crawford; Hartley |
| 1989 | 2 | Frey & Denyes; Hanucharurnkul |
| 1990 | 1 | Weintraub & Hagopian |
| 1991 | 2 | Baker; Hartweg |
| 1993 | 8 | Ailinger & Deer; Baker; Canty; Dodd & Dibble; Folden; Hart; Moore; Schott-Baer |
| 1994 | 4 | Dowd; Jesek-Hale; Mapanga; McCaleb & Edgil |
| 1995 | 8 | Bess; Carroll; Cull; Hart; Koster; Robinson; Schott-Baer, Fisher, & Gregory; Villarruel |
| 1996 | 6 | Aish & Isenberg; Dodd et al.; Gaffney & Moore; Hagopian; Metcalfe; Wang & Fenske |
| 1997 | 4 | Ailinger & Deer; Lukkarinen & Hentinen; Moore & Mosher; Wang |
| 1998 | 2 | Hart & Foster; Mosher & Moore |
| 1999 | 5 | Campbell & Soeken; Lee; Renker; Slusher; Torres, Davim, & da Nobrega |
| 2000 | 3 | Dodd & Miaskowski; Weber; White |
| 2001 | 2 | Cade; Wang & Laffrey |
| 2002 | 3 | Artinian, Magnan, Sloan, & Lange; Fialho, Pagliuca, & Soares; Monteiro, da Nobraga, & de Lima |
| 2003 | 7 | Callaghan; Dashiff; Fok & Daly; Fok & Wong; Phelan, Oliveria, Christos, Dusza, & Halpern; Sousa; Wattanawech, Srimoragot, Kasemkitwattana, & Kimpee |
| 2004 | 3 | Harris; Velsor-Friedrich, Pigott, & Louloudes et al.; Williams & Schreier |
| 2005 | 6 | Callaghan; Hurst, Montgomery, Davis, Killion, & Baker; Sousa & Zauszniewski; Velsor-Friedrich, Pigott, & Srof; Zrinyi & Rimar |
| 2006 | 7 | Ailinger, Moore, Nguyen, & Lasus; Callaghan; Kongsaktrakul et al.; Santos & da Silva; Su, Songwathana, & Naka; Wilson, Brown, & Stephens-Ferris |
| 2007 | 1 | Zrinyi & Zekanyne |
Theory
A theory is more narrow and specific than a conceptual model and is directly testable. A theory consists of an integrated set of defined concepts, existence statements, and relational statements that can be used to describe, explain, predict, or control that phenomenon. Existence statements declare that a given concept exists or that a given relationship occurs. For example, an existence statement might claim that a condition referred to as stress exists and that there is a relationship between stress and health.
Relational statements clarify the relationship that exists between or among concepts. For example, a relational statement might propose that high levels of stress are related to declining levels of health. It is the statements of a theory that are tested through research, not the theory itself. Thus, identifying statements within the theory is critical to the research endeavor and forms the basis of the study’s framework. The types of theory discussed here are scientific, substantive, and tentative.
Middle-Range Theories
Middle-range theories present a partial view of nursing reality. Merton, a sociologist, developed middle-range theories, in 1968. These theories are less abstract and address more specific phenomena than grand theories do. They directly apply to practice and focus on explanation and implementation. Middle-range theories may emerge from grand theories or may develop inductively from research findings. Qualitative studies have been a good source of middle range theory. Some middle-range theories have been developed by combining nursing theories with theories from other disciplines. Recently, some middle-range theories have been developed from clinical practice guidelines.
Middle-range theories are useful in both research and practice. They often help the practitioner to understanding the client’s behavior, enabling more effective interventions. Because of their usefulness in practice, some authors refer to middle-range theories as practice theories. Middle-range theories are used more commonly than grand theories as frameworks for research. As a researcher, it will be important for you to carefully consider what aspects of a particular middle-range theory are appropriate for before using it. Table 7-9 identifies some of the more frequently used middle-range theories.
TABLE 7-9
Middle Range Theories Commonly Used in Nursing
| Author | Reference | Philosophy/Theory |
| Abdellah, Faye Glenn | Abdellah, F. G., Beland, I. I., Martin, A., & Matheney, R. V. (1960). Patient-centered approaches in nursing. New York: Macmillan. | Twenty-One Nursing Problems (1960) |
| Adam, Evelyn | Adam, E. (1980). To be a nurse. Toronto, Canada: W.B. Saunders | Conceptual Model for Nursing (1980) |
| Barker, Phil | Barker, P. (1998). The Tidal Model: An integrative framework for caring within an interpersonal paradigm. Newcastle: University of Newcastle. | The Tidal Model of Mental Health Recovery (1995-1997) |
| Barnard, Kathryn E. | Barnard, K. (1979). Nursing child assessment satellite teaching manual. Seattle: NCAST Publications | Child Health Assessment Interaction Model (1978) |
| Beck, Cheryl Tatano | Beck, C. T. (1993). Teetering on the edge: A substantive theory of postpartum depression. Nursing Research, 42(1): 42–48. | Postpartum Depression Theory (1993) |
| Benner, Patricia | Benner, P. (1984). From novice to expert: Promoting excellence and power in clinical nursing practice. Menlo Park, CA: Addison-Wesley | From Novice to Expert: Excellence and Power in Clinical Nursing Practice (1984) |
| Boykin, Anne & Schoenhofer, Savina O. | Boykin, A., & Schoenhofer, S. (1993) Nursing as caring: A model for transforming practice. New York: National League for Nursing | Nursing as Caring: A Model for Transforming Practice (1993) |
| Eakes, Georgene, Burke, Mary, & Hainsworth, Margaret | Eakes, G. G., Burke, M. L., & Hainsworth, M. A. (1998). Middle-range theory of chronic sorrow. Image: Journal of Nursing Scholarship,30(2): 179–184. | Theory of Chronic Sorrow (1998) |
| Erickson, Helen, Tomlin, Evelyn, & Swain, Mary Ann | Erickson, H. C., Tomlin, E., & Swain, M. A. (1983). Modeling and role-modeling: A theory and paradigm for nursing. Englewood Cliffs, NJ: Prentice Hall. | Modeling and Role Modeling (1983) |
| Eriksson, Katie | Eriksson, K. (1990). Systematic and contextual caring science: A study of the basic motive of caring and context. Scandinavian Journal of Caring Sciences, 4(1), 3–5. | Theory of Caritative Caring (1990) |
| Hall, Lynda | Hall, L. E. (1964). Nursing: What is it? The Canadian Nurse, 60, 150-154. | Core, Care, and Cure Model (1964) |
| Henderson, Virginia | Henderson, V. (1966) The nature of nursing. New York: Macmillan. | Definition of Nursing (1955) |
| Husted, Gladys, & Husted, James | Husted, J. H., & Husted, G. L. (1999). Agreement: the origin of ethical action. Critical Care Nursing Quarterly, 22(3): 12-18. | Symphonological Bioethical Theory (1999) |
| Johnson, Dorothy | Johnson, D. E. (1980). The behavioral system model for nursing. In J. P. Riehl & C. Roy (Eds.), Conceptual models for nursing practice (pp. 207–216). New York: Appleton-Century-Crofts. | Behavioral Systems Model (1980) |
| King, Imogene | King, I. M. (1981). A theory for nursing: Systems, concepts, process. New York: John Wiley & Sons. | Interacting Systems Framework and Middle Range Theory of Goal Attainment (1971) |
| Kolcaba, Katharine | Kolcaba, K. Y. (1994). A theory of holistic comfort for nursing. Journal of Advanced Nursing, 19(6): 1178-1184. | Theory of Comfort (1994) |
| Author | Reference | Philosophy/Theory |
| Leininger, Madeleine | Leininger, M. M. (1985). Transcultural care diversity and universality: A theory of nursing. Nursing and Health Care, 6(4), 208-212. | Culture Care Theory of Diversity and Universality (1985) |
| Levine, Myra | Levine, M. E. (1967). The four conservation principles of nursing. Nursing Forum, 6(1): 45-59. | The Conservation Model (1967) |
| Martinsen, Kari | Martinsen, K. (1990). Moral practice and documentation in practical nursing. In T. K. Jensen (Ed.), Foundational problems in nursing ethics, theories of science, leadership and society [Norwegian]. Philosophia, Aarhus. | Philosophy of Caring (1990) |
| Mercer, Ramona | Mercer, R. (1986). First-time motherhood: Experiences from teens to forties. New York: Springer. Mercer, R. (1995). Becoming a mother: Research on maternal identity from Rubin to the present. New York: Springer. | Maternal Role Attainment—Becoming a Mother (1986, 1995) |
| Mishel, Merle | Mishel, M. (1988). The theory of uncertainty in illness. Image, 20(4), 225-232. | Uncertainty in Illness Theory (1988) |
| Neuman, Betty | Neuman, B. (1974). The Betty Neuman Health-Care Systems Model: A total person approach to patient problems. In J. P. Riehl & C. Roy (Eds.), Conceptual models for nursing practice (pp. 99–114). New York: Appleton-Century-Crofts. | Systems Model (1974) |
| Newman, Margaret | Newman, M. A. (1979). Theory Development in Nursing, Philadelphia: F.A. Davis. (see particularly Chapter 6) | Theory Development in Nursing (1979) |
| Newman, Margaret | Newman, M. A. (1986). Health as expanding consciousness. St. Louis: C.V. Mosby. | Health as Expanding Consciousness (1986) |
| Nightingale, Florence | Nightingale, F. (1957). Notes on nursing. Philadelphia: J.B. Lippincott. (Original publication in 1859) | Modern Nursing (1859) |
| Orem, Dorothea | Orem, D. E. (1971). Nursing: Concepts of practice.New York: McGraw-Hill | Self-Care Deficit Theory of Nursing (1971) |
| Orlando, Ida Jean (Pelletier) | Orlando, I. J. (1961). The dynamic nurse-patient relationship: Function, process and principles. New York: G.P. Putnam. | Nursing Process Theory (1961) |
| Parse, Rosemarie | Parse, R. R. (1981). Man-living-health: A theory of nursing. New York: Wiley. | Human Becoming (1981) |
| Pender, Nola | Pender, N. J. (1982). Health promotion in nursing practice. New York: Appleton-Century-Crofts. Most recent edition, 2005 | Health Promotion Model (1982; 2005) |
| Peplau, Hildegard | Peplau, H. E. (1952). Interpersonal relations in nursing. New York: G.P. Putnam. | Theory of Interpersonal Relations (1952) |
| Ray, Marilyn | Ray, M. (1981). A philosophical analysis of caring within nursing. In M. Leininger (Ed.): Caring: An essential human need (pp. 25–36). Thorofare, NJ: Charles B. Slack. | Theory of Bureaucratic Caring (1981) |
| Reed, Pamela | Reed, P. G. (1991). Toward a nursing theory of self-transcendence: Deductive reformulation using developmental theories. Advances in Nursing Science 13(4), 64-77. | Self-Transcendence Theory (1991; 2003) |
| Rogers, Martha | Rogers, M. E. (1970). An introduction to the theoretical basis of nursing. Philadelphia: F.A. Davis. | Unitary Human Beings (1970) |
| Roper, Nancy, Logan, Winifred, & Tierney, Alison | Roper, N., Logan, W., & Tierney, A. (1980, 1985, 1990, 1996). Elements of Nursing. Edinburgh: Churchill Livingstone. Roper, N, Logan, W., & Tierney, A. (1996) The Roper-Logan-Tierney Model: a model in nursing practice. The Roper-Logan-Tierney Model: a model in nursing practice. In P.H. Walker (Ed.), Blueprint for use of nursing models: education, research, practice, and administration. National League for Nursing, pp. 289–314. | A Model for Nursing Based on a Model of Living (1980, 1985, 1990) |
| Roy, Sister Callista | Roy, C. (1976). Introduction to nursing: An adaptation model. Englewood Cliffs, NJ: Prentice-Hall. | Adaptation Model (1976) |
| Ruland, Cornelia, & Moore, Shirley | Ruland, C. M., & Moore, S. M. (1998). Theory construction based on standards of care: a proposed theory of the peaceful end of life. Nursing Outlook, 46(4): 169–175. | Peaceful End of Life Theory (1998) |
| Swanson, Kristen | Swanson, K. M. (1991). Empirical development of a middle range theory of caring. Nursing Research, 40(3): 161–166. | Theory of Caring (1991) |
| Travelbee, Joyce | Travelbee, J. (1966). Interpersonal aspects of nursing. Philadelphia: F.A. Davis. | Human-to-Human Relationship Model (1966, 1971) |
| Ujhely, Gertrud | Ujhely, G. (1968).Determinants of the nurse-patient relationship. New York: Springer. | Determinants of the Nurse-Patient Relationship (1968) |
| Watson, Jean | Watson, J. (1985). Nursing: Human science and human care. New York: Appleton-Century-Crofts. | Philosophy and Science of Caring (1985) |
| Wiedenbach, Ernestine | Weidenbach, E. (1964). Clinical nursing: A helping art. New York: Springer. | The Helping Art of Clinical Nursing (1964) |
| Wiener, Carolyn, & Dodd, Marylin | Wiener, C. L., & Dodd, M. J. (1993). Coping amid uncertainty: An illness trajectory perspective. Scholarly Inquiry for Nursing Practice, 7(1): 17-31. | Theory of Illness Trajectory (1993) |
Developed by Helen Hough, Nursing Librarian, University of Texas at Arlington.
Scientific Theory
The term scientific theory is restricted to a theory that has valid and reliable methods of measuring each concept and whose relational statements have been tested through research and demonstrated to be valid. Scientific theories have empirical generalizations, statements that have been repeatedly tested and have not been disproved. There are no scientific theories within nursing. Scientific theories from other disciplines are commonly used within the nursing practice. For example, most physiological theories are scientific in nature.
Substantive Theory
Substantive theory is useful for explaining important phenomena within the discipline. The knowledge you gain from a substantive theory may be valuable in practice settings. An example of a substantive theory is the theory of reasoned action (Ajzen & Fishbein, 1980; Fishbein & Ajzen, 1975), which proposes that a person’s expectation that a particular behavior will lead to a given outcome increases his or her intention to perform the behavior. Research has shown that intention predicts behavior. Blue (1995) has reviewed studies that examine the capacity of this theory to predict a person’s willingness to participate in exercise programs.
Substantive theories do not have the validity of a scientific theory. Some of the statements may have been tested and verified, but others have not. In some cases, the statements in the theory may not have been clearly identified by the theorist or by those using the theory.
Tentative Theory
A tentative theory is newly proposed, has had minimal critical appraisal, and has undergone little testing. Tentative theories propose an integrated set of relationships among concepts that have not been satisfactorily addressed in a substantive theory. Because tentative theories are newly emerging and untested, they tend to be less well developed than substantive theories. Many tentative theories have short lives, but others may eventually be more extensively developed and validated through multiple studies.
Tentative theories may be developed from clinical insights, from elements of existing theories not previously related, as outcomes of qualitative studies, or from conceptual models. One type of tentative theory of great importance in nursing today is intervention theories. These middle-range theories seek to explain the dynamics of a patient problem and exactly how a specific nursing intervention is expected to change patient outcomes. Currently, these new theories are tentative, but some will likely become substantive in the future. Intervention theories are discussed in detail in Chapter 13.
Tentative theories developed in nursing often contain concepts and relational statements derived from sociological, psychosocial, psychological, and physiological theories. In some cases, the framework may require that the nurse researcher merge concepts using theory from other sciences with concepts from nursing science theories. Tentative theories in nursing often emerge from questions related to identified nursing problems or from the clinical insight that a relationship exists between or among elements important to desired outcomes. These situations tend to be concrete and require that the researcher express these concrete ideas in more abstract language. This issue is particularly difficult for the beginning researcher. The neophyte researcher’s awareness of theoretical ideas related to the situation may be limited, or the researcher may perceive the situation in such concrete terms that even though the researcher knows the theories, he or she fails to link them to the situation.
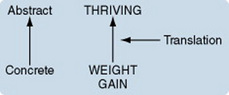
For example, one nurse, a novice researcher who worked in a newborn intensive care unit, was convinced from her clinical experiences that a mother’s frequent visits to the hospital were related to her infant’s weight gain. The nurse’s ideas could be diagrammed as follows:

She wanted to study this relationship but was having difficulty expressing her ideas as a framework. Number of visits and weight gain are concrete ideas. From the perspective of research, these ideas are variables. However, to develop a framework, the researcher must express the variables in a more abstract and general way as concepts. This novice researcher lacked the knowledge and skills needed to accomplish this task. She was “stuck” at a concrete level of viewing her problem.
Many students recognize that they are concrete thinkers and believe that they are incapable of moving beyond that limited way of thinking. However, the capacity for abstract thinking is not an innate ability; it is a learned skill. Acquiring it simply requires that one invest the energy to obtain the knowledge and practice the skills.
Converting a concretely expressed term to a higher level of abstractness—from a variable to a concept—is a form of translation. Because the translation in this case is from a lower level of abstractness to a higher level (as shown in the following diagram), we can apply inductive reasoning:
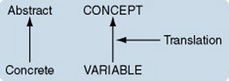
However, the researcher must know of equivalent terms at both the concrete and abstract levels in order to perform the translation. Conducting a literature search can be useful in identifying equivalent abstract terms. The search may be difficult if the novice researcher is blind to the theoretical ideas presented in the literature and picks up only the concrete ideas.
Sometimes, probing questions can help a researcher to move from concrete to more abstract thinking. For example, one could ask, “Why is it important that the mother visit?” “What happens when the mother visits?” Answering these questions may help the researcher to label what happens when the mother visits; existing theories have named this process bonding or attachment. The following diagram could be used to describe this process:

One can then ask, “What happens when the baby gains weight?” “Why is this important?” “How is it different from the baby who gains weight more slowly or fails to gain weight?” One name for this phenomenon is growth; another is thriving. There might be other ways to express the phenomenon. The following diagram could be used to describe this process:
At this point, the novice nurse researcher is ready to search the literature more thoroughly. Theories related to bonding, attachment, growth, and thriving can be examined. The novice researcher may find literature that proposes a positive relationship between attachment and thriving. This relationship could be expressed as follows:

When the aforementioned ideas are linked, we have the beginning of a tentative theory. The diagram—really the beginning of a conceptual map—has the following appearance:
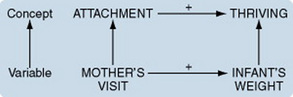
However, the ideas for a framework and a tentative theory are still incomplete. What other factors are important in influencing the relationship between mother’s visits and infant’s weight gain, between attachment and thriving? Again, the researcher can consult the literature. Researchers in this field have examined elements relevant to this question. What concepts did they include? What relationships did they find? Are their findings consistent with the emerging framework? Clinically, what other elements seem to be associated with this phenomenon? Do the newly found concepts need to be included in the framework? While pondering these questions, the researcher can obtain conceptual definitions for attachment and thriving and statements expressing the relationship between the two concepts from existing theories, from synthesis of the literature, or from qualitative data analysis.
As the framework expressing a tentative theory takes shape, it is time to consider moving to an even higher level of abstraction, that of conceptual models. Is there a possible fit between a conceptual model in nursing and the tentative theory expressed in the developing framework? Can the study concepts be translated to the even more abstract constructs of a conceptual model? Are the study statements linked in any way with the broad statements of a conceptual model? If a conceptual nursing model is included in the framework, the links between the conceptual model and the tentative theory must be made clear.
Conceptual Maps
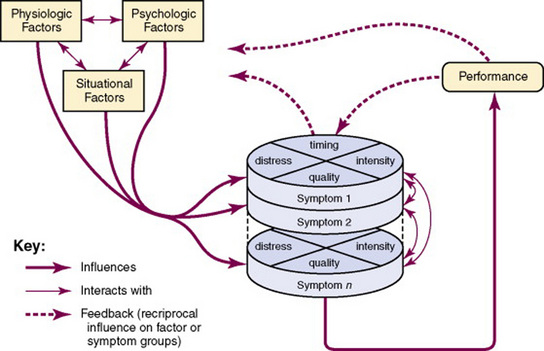
One strategy for expressing a framework is a conceptual map that diagrams the interrelationships of the concepts and statements (Artinian, 1982; Fawcett, 1999; Moody, 1989; Newman, 1979, 1999; Silva, 1981). Figures 7-3 through 7-7 are examples of conceptual maps. A conceptual map summarizes and integrates what we know about a phenomenon more succinctly and clearly than a literary explanation and allows us to grasp the gestalt of a phenomenon. A conceptual map should be supported by references from the literature.
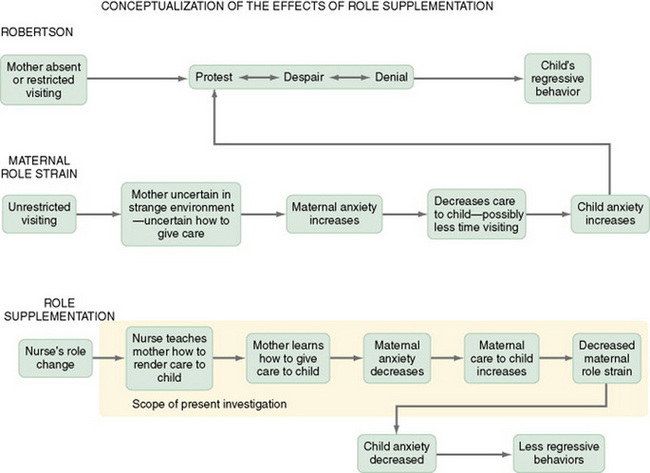
Figure 7-3 Conceptual map outlining scope of present study: conceptualization of the effects of role supplementation.
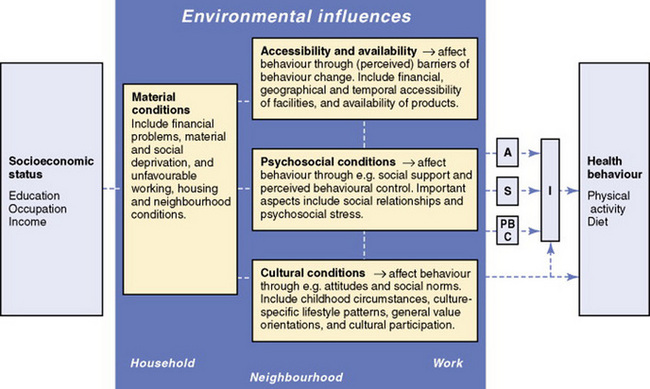
Figure 7-4 Framework of environmental determinants contributing to the explanation of socioeconomic inequalities in health behaviors. The gray panel incorporates four boxes of environmental determinants. The terms household, neighborhood, and work are examples of the different settings in which these determinants may influence health behaviors. The abbreviations in the right-hand side boxes represent the following constructs: A = attitude; S = social influences, like social support, subjective norms, and modeling; PBC = perceived behavioral control; I = intention. These constructs are derived from the theory of planned behavior (see Ajzen [1991] for more information).
A conceptual map explains which concepts contribute to or partially cause an outcome. Conditions, both direct and indirect, that may produce the outcome are specified. A conceptual map illustrates the process in which factors must cumulatively interact over time in some sequence to have a causal effect. Conceptual maps vary in complexity and accuracy, depending on the available body of knowledge related to the phenomenon. Mapping can also identify gaps in the logic of the theory being used as a framework and reveals inconsistencies, incompleteness, and errors.
Conceptual maps are useful beyond the study for which they were developed. A conceptual map may suggest hypotheses that can be tested in future studies. In addition, through map development, the researcher may gain insight about different situations in which the same process may be occurring. Publication of the map may stimulate the interest of other researchers, who may then use it in their own studies. Thus, a well-developed conceptual map may help to build a body of knowledge related to a particular theory. In addition to conceptual maps included as the framework for a study, more maps are being published that are outcomes of extensive reviews of the literature expressed as tentative theories.
THE STEPS FOR CONSTRUCTING A STUDY FRAMEWORK
Developing a framework is one of the most important steps in the research process but, perhaps, also one of the most difficult. Examples of frameworks from the literature are helpful but not sufficient as a guide to framework development. The brief but impressive presentation of a framework in a published study belies the careful, thoughtful work required to arrive at that point. Yet, as a neophyte researcher you will need to learn how to perform that thoughtful work.
As the body of knowledge related to a phenomenon grows, it becomes easier for researchers to develop a framework to express that knowledge. Therefore, frameworks for quasi-experimental and experimental studies, which should have a background of descriptive and correlational studies and perhaps some substantive theory, should be more easily and fully developed than those for descriptive studies. Descriptive studies and qualitative studies often examine multiple factors to explore a phenomenon not previously well studied. Previous theoretical work related to the phenomenon may be tentative or nonexistent. Therefore, the framework may be less comprehensive. In qualitative studies, in which the framework development is an outcome of the study, even identifying concepts may not be clear at the beginning of the study, and statements will be synthesized from the data. The basis for developing qualitative studies is more philosophical than theoretical.
To illustrate the development of a framework, we will use a middle-range theory by Kamphuis, van Lenthe, Giskes, Brug, and Mackenback (2007) that explains socioeconomic inequalities in health behavior using constructs from the theory of planned behavior (Ajzen, 1991). As you read through the extracts from this study, however, keep in mind that the nicely turned phrases in a framework require much time, effort, thought, and reflection. They do not easily and miraculously appear in their present form. You are examining the finished framework and will not be able to see the process of thinking or the work involved as ideas develop.
The following steps introduce the reasoning used to develop a framework. The steps of the process are (1) selecting and defining concepts, (2) developing statements relating the concepts, (3) expressing the statements in hierarchical fashion, and (4) developing a conceptual map that expresses the framework. The steps are not usually performed in order. In reality, there is a flow of thought from one step to another, back and forth, as ideas are developed and refined.
Selecting and Defining Concepts
Concepts are selected for a framework on the basis of their relevance to the phenomenon you are studying. Thus, the problem statement, which describes the phenomenon, is a rich source of concepts for the framework. If you begin from a concrete clinical perspective, the ideas may be first identified as variables and then translated to concepts. Every major variable included in the study should reflect a concept included in the framework. You may modify the framework as you develop the rest of the study. As you gain additional insight into the phenomenon through a thorough search of theoretical, research, and clinical publications, you may identify additional relevant concepts or propose new relationships. While incorporating these new elements into the framework, consider their implications for the study design.
The framework presented here was developed by researchers from the public health field, not nursing, but it is imminently relevant for nursing research. As Kamphuis and colleagues indicated:
Poorer people experience worse health (Mackenbach et al., 2003; Van Herton, 2002) with higher rates of mortality and morbidity from cardiovascular diseases, obesity, type 2 diabetes and cancers (Choiniere et al., 2000; Kaplffan & Lynch, 1997; Van Lenthe & Mackenback, 2002). Fruit and vegetable consumption and physical activity play a protective role in the onset of these chronic diseases (Ness & Powles, 1977; US DHHS [U.S. Department of Health and Human Services], 1996; Van Duyn & Pivonka, 2000; Wannamethee et al., 2000). Low socioeconomic groups consume less fruits and vegetables(Smith & Brunner, 1997; James et al., 1997)and do less physical activity (Droomers et al., 1998; US DHHS, 1996) than people from higher socioeconomic backgrounds, which is considered one of the explanations for socioeconomic inequalities in health. (p. 493)
Their framework “specifies the pathways between socioeconomic status (SES), environmental factors, personal level factors (constructs from the Theory of Planned Behaviour: see Ajzen, 1991) and health behaviours” (p. 494).
Each concept included in a framework must be defined conceptually. When available and appropriate, use conceptual definitions from existing theoretical works, with definitions quoted and sources cited. If theories that define the concept are not available, you will need to develop the definition. Conceptual definitions may be available in the literature in the absence of theories that use the concept. For an example of the extraction of conceptual definitions from the literature, see Chapter 6 in Understanding Nursing Research (Burns & Grove, 2007).
One source of conceptual definitions is published concept analyses. Previous studies using the concept may also provide a conceptual definition. Another source of a conceptual definition is literature associated with instrument development related to the concept. Although the instrument itself is an operational definition of the concept, the author will often provide a conceptual definition on which the instrument development was based. The general literature can sometimes provide a conceptual definition. Although it may not have been as carefully thought out as the definitions in a theory or a concept analysis, this conceptual definition may reflect the only definition available in the discipline.
When acceptable conceptual definitions are not available, perform concept synthesis or concept analysis to develop the definition. You must present various definitions of the concept from the literature to validate the conceptual definition you selected for the study.
Kamphuis et al. (2007) provided the conceptual definitions in the following excerpts.
 ACCESSIBILITY AND AVAILABILITY
ACCESSIBILITY AND AVAILABILITY
Including financial, geographical and temporal accessibility of products and facilities that are needed for (un)healthy behaviour, and interventions to support behaviour change. (Kamphuis et al., 2007, p. 494)
Including social relationships, and psychosocial stress. (Kamphuis et al., 2007, p. 494)
Including culture-specific lifestyle patterns, childhood circumstances, general value orientations, and cultural participation. (Kamphuis et al., 2007, p. 494)
Including financial problems, material and social deprivation, and unfavourable working, housing and neighbourhood conditions. These may affect behaviour factors. For instance, a person’s budgetary situation may partly determine one’s access to products and facilities, or in what neighbourhood one can afford to live. (Kamphuis et al., 2007, p. 494)
Developing Relational Statements
The next step in framework development is to link all of the concepts through relational statements. Whenever possible, obtain relational statements from theoretical works and the sources cited. If such statements are unavailable, propose the relationships. Provide evidence from the literature for the validity of each relational statement whenever available. This support must include a discussion of previous quantitative or qualitative studies (or both) that have examined the proposed relationship and published observations from the clinical practice perspective.
As you develop the framework, you may have to extract statements that are embedded in the literary text of an existing theory, published research, or clinical literature. When you first begin extracting statements, the task can be overwhelming because every sentence in the text seems to be a relational statement. A little practice makes the task easier. The steps in the process of extracting statements are as follows:
1. Select a portion of a theory that discusses the relationships between or among two or three concepts.
2. Write down a single sentence from the theory that seems to be a relational statement.
3. Express it by using the statement diagrams presented earlier in the chapter.
4. Move to the next statement, and express it with diagrams.
5. Continue until all of the statements related to the selected concepts have been expressed using statement diagrams.
6. Examine the links among the diagrammatic statements you have developed. The logic of what the theorist is saying will gradually become clearer.
This process is illustrated in greater detail in Chapter 6 of Understanding Nursing Research (Burns & Grove, 2007).
If statements relating the concepts of interest are not available in the literature, statement synthesis is necessary. Develop statements that propose specific relationships among the concepts you are studying. You may gain the knowledge for your statement synthesis through clinical observation and integrative literature review (Walker & Avant, 2004).
In descriptive studies, theoretical statements related to the phenomenon may be sparse. In this case, developing a framework requires more synthesis and has a higher level of uncertainty. You may note in the statement that a relationship between A and B is proposed but the type of relationship is unknown. Follow this statement with a research question based on this relationship rather than a hypothesis. For example, ask, “What is the nature of the relationship between A and B?” An objective might be to examine the nature of the relationship between A and B.
Kamphuis et al. (2007) offered the relational statements shown in the following excerpts, each of which is followed by a diagram of the relationship.
1. Rates of physical activity is associated with neighbourhood attractiveness, accessibility and proximity of neighbourhood facilities and neighbourhood safety. (Kamphuis et al., 2007, p. 494)

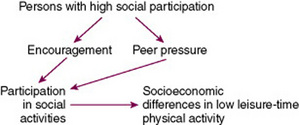
2. Participation in social activities is a strong predictor of socioeconomic differences in low leisure-time physical activity, which may be mediated by a higher extent of encouragement or peer pressure to participate in physical activities experienced by persons with high social participation. (Kamphuis et al., 2007, p. 494)
3. A range of possible mediating environmental factors between area deprivation and an unhealthy diet includes a lower prevalence of supermarkets, a higher prevalence of fast food restaurants and a relatively higher premium on the price of healthy compared to less healthy food in deprived areas. (Kamphuis et al., 2007, p. 494)

4. Social participation and social support may play a role in inequalities in fruit and vegetable consumption, as a lack of social participation might indicate a less extensive social network and less social support for adhering to a healthy diet. (Kamphuis et al., 2007, p. 494)
5. Cultural influences, such as traditional beliefs about appropriate or healthy diets may contribute to socioeconomic differences in fruit and vegetable consumption. (Kamphuis et al., 2007, p. 494)

Developing Hierarchical Statement Sets
A hierarchical statement set is composed of a specific proposition and a hypothesis or research question. If a conceptual model is included in the framework, the statement set may also contain a general proposition. The proposition is listed first, with the hypothesis or research question immediately following. In some cases, more than one hypothesis may be related to a particular proposition. However, there must be a proposition for each hypothesis stated. This statement set indicates the link between the framework and the methodology.
Constructing a Conceptual Map
Conceptual maps are initiated early in the development of the framework, but refining the map will probably be one of your last steps. Before you can complete the map, the following information must be available:
1. A clear problem and purpose statement.
2. Concepts of interest, including conceptual definitions.
3. Results of an integrative review of the theoretical and empirical literature.
4. Relational statements linking the concepts, expressed literally and diagrammatically.
5. Identification and analysis of existing theories that address the relationships of interest.
6. Identification of existing conceptual models congruent with the developing framework.
7. Linking of proposed relationships with hypotheses, questions, or objectives (hierarchical statement sets).
Some nursing scholars believe that the map should be limited to those concepts included in the study (Fawcett, 1999). However, Artinian (1982) recommended that the map include all the concepts necessary to explain the phenomenon, plainly delineating that portion of the map to be studied. We agree with Artinian. It is important that the map be a full expression of the phenomenon of concern. This strategy is illustrated by Artinian’s map of the conceptualization of the effects of role supplementation, presented in Figure 7-3. In this map, the scope of the study is enclosed by a yellow box.
Developing your own concept map entails the following steps. First, arrange the concepts on the page in sequence of occurrence (or causal linkage) from left to right, with the concepts reflecting the outcomes located on the far right. Concepts that are elements of a more abstract construct can be placed in a frame or box. Sets of closely interrelated concepts can be linked by enclosing them in a frame or circle. Second, using arrows, link the concepts in a way that is consistent with the statement diagrams you previously developed. For some studies, at some point on the map, the path of relationships may diverge, so that there are then two or more paths of concepts. The paths may converge at a later point. Every concept should be linked to at least one other concept. Third, examine the map for completeness by asking yourself the following questions:
• Are all of the concepts in the study also included on the map?
• Are all the concepts on the map defined?
• Does the map clearly portray the phenomenon?
• Does the map accurately reflect all the statements?
• Is there a statement for each of the links portrayed by the map? Is the sequence accurate?
Developing a well-constructed conceptual map requires repeated tries, but persistence pays off. You may need to reexamine the statements identified. Are there some missing links? Are some of the links inaccurately expressed?
As the map takes shape and begins to seem right, show it to trusted colleagues. Can they follow your logic? Do they agree with your links? Can they identify missing elements? Can you explain the map to them? Seek out individuals who have experienced the phenomenon you are mapping. Does the process depicted seem valid to them? Find someone more experienced than you in conceptual mapping to examine your map closely and critically.
Continue to revise your conceptual map until you achieve some degree of consensus with the people you have consulted and you feel a sense of rightness about it. Examine the conceptual map by Kamphuis et al. that is presented in Figure 7-4. Is it consistent with their concepts and statements? Does the process described seem valid to you?
Constructing a Study Framework from Substantive Theory
Developing a framework designed to test statements in a substantive theory requires that all concepts in the framework be obtained from the substantive theory. These concepts must be defined as the theorist defines them. If the theorist has failed to define a concept, develop one that is consistent with the theorist’s perspective. Operational definitions must be consistent with the conceptual definitions and should be accepted methods of measurement used for testing the selected theory. Statements (propositions) from the substantive theory must be identified. In a substantive theory, previous studies will have tested at least some of the relational statements. Findings from these studies must be discussed in the literature review or in the presentation of the framework in terms of evidence validating or refuting the relational statements. Hypotheses for the present study must be designed to test one or more statements from the substantive theory.
Hoffman, Given, von Eye, Gift, and Given (2007) developed a study to test the theory of unpleasant symptoms (Lenz, Pugh, Milligan, Gift, & Suppe, 1997). The framework for the theory of unpleasant symptoms is shown in Figure 7-5. The authors described the theory as follows.
The TOUS theorizes that concurrent symptoms (pain, fatigue, and insomnia) may interact and catalyze each other, worsening the overall level of symptom severity experienced by people with lung cancer… The TOUS also highlights four dimensions that characterize the symptom experience: timing (frequency of occurrence and duration), intensity (severity), quality (description of qualifiers), and distress (bother).… Although symptoms comprise a chief component of the TOUS, the theoretical framework has two other components: the antecedent patient factors influencing the symptom experience and the consequences of the symptom experience. Patient factors that influence symptoms include physiologic, psychological, and situational factors… The last component of the TOUS is the consequences of the symptom experience, including performance outcomes such as symptom status.… Finally, the three components of the TOUS are reciprocal, and each component influences every other component (Hoffman et al., 2007, p. 787).
WHAT IS ALREADY KNOWN IN TESTING THIS THEORY
Studies have examined symptom experiences and reported no differences by gender. (Kurtz et al., 2000; Cooley et al., 2003; Gift et al., 2003; Gift et al., 2004).
• Some studies have found differences by gender (Degner & Sloan, 1995; Hopwood & Stephens, 1995).
• Pain and fatigue were the most common and distressing symptoms among patients with lung cancer (Cooley et al., 2003)
• The presence of pain and fatigue may affect the number of symptoms that people with cancer experience (Given et al., 2001b).
• More than one-third of people diagnosed with lung cancer report insomnia (Cooley et al., 2003).
• Pain, fatigue, and insomnia are the most common and severe symptoms (Fox & Lyon, 2006; Gift et al., 2004; Hoekstra et al., 2006; Miaskowski et al., 2004; Walsh & Rybicki, 2006).
• Four research teams have highlighted the effects of the concurrence of pain, fatigue and insomnia in people with cancer (Beck et al., 2005; Dodd et al., 2001; Given et al., 2001a; Sarna, 1993a; Sarna, 1993b).
The current, gender based study acknowledged the importance of directing research according to a realistic clinical picture of people with lung cancer and focusing on the most common and severe symptoms of pain, fatigue, and insomnia. If pain, fatigue, and insomnia cluster together and are found to interact differently according to gender, then strategies may be developed and implemented to ameliorate the synergistic effects of the symptoms (Hoffman et al., 2007, p. 786).
For people within 56 days of starting chemotherapy for a new diagnosis of lung cancer:
1. What are the most frequently occurring symptoms in people with lung cancer, and do they differ between men and women?
2. What are the mean severity scores for pain, fatigue, insomnia, and gender?
3. If a relationship exists among pain, fatigue, insomnia, and gender, do the differences remain statistically significant after controlling for age, comorbidities, and stage of cancer?
Constructing a Study Framework on the Basis of a Conceptual Model
Although the testing of extant nursing models is a critical need within nursing, few published studies have been designed for this purpose. One reason is the level of complexity required for such testing. Because conceptual models cannot be tested directly, a middle-range theory based on the conceptual model must be available (or must be developed as a tentative theory). The framework must include both the conceptual model and the middle-range theory. Thus, the conceptual map for the study must illustrate relationships among the constructs of the model, the concepts of the middle-range theory, and the link between the concepts and relationships in the model and the concepts and relationships in the middle-range theory. Because of this complexity, in our opinion, master’s-level students should not attempt the process unless they are collaborating with doctorally prepared nurses. However, master’s-level students will be involved in critiquing published studies with such frameworks and applying them in practice situations.
A framework that includes a conceptual model has the following elements:
• Constructs from the conceptual model
• Definitions of constructs from the conceptual model
• Statements linking the constructs
• Concepts that represent portions of the selected constructs
• Conceptual definitions compatible with construct definitions
• Statements linking the concepts that express a tentative or substantive theory
• Selection of variables that represent portions of the concepts
• Operational definitions of the variables compatible with conceptual definitions
• A conceptual map linking the constructs, concepts, and variables
In some cases, rather than beginning with the choice of a model, the researcher begins developing the framework by identifying concepts relevant to a particular nursing problem. The researcher identifies or develops a theory related to the phenomenon of interest; simultaneously, or perhaps later, the researcher selects all or a portion of a conceptual model compatible with his or her interests. The important issue is not where the development of the framework begins but rather how logically the various elements of the framework are linked and how complete the end product is.
Whittemore and Roy (2002) have developed a middle-range theory of adapting to diabetes mellitus that is derived from the Roy adaptation model, developed through theory and concept synthesis using relevant empirical evidence. The following excerpt contains their description of the process of developing the theoretical model:
The researchers conducted an extensive literature review to identify concepts within the nursing literature that are relevant to chronic illness. They selected Pollock’s middle-range theory of chronic illness (1986, 1993), based on Roy’s adaptation model (Figure 7-6), because it captured key aspects of adapting to DM. The authors analyzed the theory in terms of its origin, meaning, logical adequacy, usefulness, and testability. Several concepts in the DM literature were identified that had the potential to enhance the understanding of the theory—namely, self-management, integration, and health-within-illness. Analyzing the concepts from the Pollock model and from the literature review provided new insights into adapting to DM. A synthesis of Roy’s model, Pollock’s chronic illness theory, and findings from existing diabetes research were used to develop a new middle-range theory—adapting to DM.
Definitions of adaptation and health from Roy’s model and Pollock’s theory were expanded, and assumptions of individual creativity and human potential have been added. These additions are consistent with the relationships and propositions from Roy’s model and Pollock’s middle-range theory.
The goal of nursing in Pollock’s theory and the newly developed theory of adapting to diabetes mellitus, consistent with Roy’s model, is to facilitate this adaptation. The conceptual map of the newly developed theory of adapting to diabetes mellitus is shown in Figure 7-7. Examine the progression of ideas expressed in the maps illustrating Roy’s conceptual map, Pollock’s map, and the map of the new theory.
THE CRITICAL ANALYSIS OF FRAMEWORKS: THEORETICAL SUBSTRUCTION
Hinshaw (1979) developed the initial methods for evaluating study frameworks, using theoretical substruction as a strategy. Dulock and Holzemer (1991) have further refined the process. The term substruction is the opposite of construction and means “to take apart.” With theoretical substruction, a framework of a published study is separated into component parts to evaluate (1) the logical consistency of the theoretical system and (2) the interaction of the framework with the study methodology. It essentially reverses the process for developing a framework described in this chapter. If components of the framework are inferred rather than clearly stated, the evaluator extracts those components and states them as clearly as possible. If a conceptual map is not presented, the evaluator may construct one.
Theoretical substruction must answer two questions: “Is the framework logically adequate?” and “Did the framework guide the methodology of the study?” Gaps and inconsistencies are identified. The conclusions of the study are evaluated in terms of whether they are logical, defensible, and congruent with the framework.
To perform theoretical substruction, an evaluator must extract the following elements from the published description of the framework:
• Concepts (and constructs if included)
• Conceptual definitions (and construct definitions if used)
• Operational definitions of concepts
• Conceptual sets linking constructs, concepts, and variables
• General propositions linking the constructs
• Specific propositions linking the concepts
• Hypotheses, research questions, or objectives
• Statement sets linking (a) general propositions, (b) specific propositions, and (c) hypotheses, questions, or objectives
• Data analysis performed in relation to each hypothesis, question, or objective
• Findings related to each hypothesis, question, or objective
• Author’s interpretation of findings in relation to the framework
The extracted information is used to analyze the logical structure of the framework and its link with the methodology. The following questions can be used to guide that analysis:
1. Is the framework based on a substantive theory or a tentative theory?
2. Was a conceptual model included in the framework?
3. Are the definitions of constructs consistent with the theorist’s definitions?
4. Do the concepts reflect the constructs identified in the framework?
5. Do the variables reflect the concepts identified in the framework?
6. Are the conceptual definitions validated by references to the literature?
7. Do the operational definitions reflect the conceptual definitions?
8. Are the reliability and validity of the operational definitions adequate?
9. Are the propositions logical and defensible?
10. Is evidence from the literature used to validate the propositions?
11. Are the hypotheses, questions, or objectives logically linked to the propositions?
12. Can diagrams of the propositions be linked to the conceptual map?
13. Does the conceptual map adequately explain the phenomenon of concern?
14. Is the design appropriate to test the propositions?
15. Is the sample size adequate to avoid a type II error? (Type II errors are discussed in Chapter 18.)
16. Are the data analyses appropriate for the hypotheses, questions, or objectives?
17. Are the findings for each hypothesis, question, or objective consistent with that proposed by the framework? If not, was the methodology adequate to test the hypothesis, question, or objective?
18. Did the author interpret the findings in terms of the framework?
19. Do the findings validate the framework?
20. Are the findings consistent with those of other studies using the same framework (or testing the same propositions)?
Critical reviews are now being published that examine studies related to selected areas of research. Theoretical substruction is being used to evaluate these studies. One example is Silva’s (1986) examination of studies asserting to test nursing models. The use of substruction should strengthen frameworks appearing in published studies. In addition, it will assist the researcher in building a body of knowledge related to a specific theory that can then be applied to clinical practice situations with greater confidence. For further information on critiquing frameworks, see Chapter 26.
SUMMARY
• A framework is the abstract, logical structure of meaning that guides the development of the study and enables the researcher to link the findings to the body of knowledge used in nursing.
• Every study has a framework.
• The framework should be well integrated with the methodology, carefully structured, and clearly presented, whether the study is physiological or psychosocial.
• If a well-established theory is being tested, the framework is derived deductively from the theory.
• A concept is a term that abstractly describes and names an object or a phenomenon, thus providing it with a separate identity or meaning.
• A relational statement declares that a relationship of some kind exists between two or more concepts.
• Relational statements are the core of the framework; it is these statements that are tested through research.
• Developing a framework for a study is one of the most important steps in the research process.
• The steps of the process are (1) selecting and defining concepts, (2) developing statements relating the concepts, (3) expressing the statements in hierarchical fashion, and (4) developing a conceptual map.
Ahrens, S.L.G. The development and testing of the Heart Failure Self-Care Inventory: An instrument for measuring heart failure self-care. Wayne State University, 2001. Unpublished doctoral dissertation
Ailinger, R.L., Deer, M.R. Self-care agency in persons with rheumatoid arthritis. Arthritis Care & Research. 1993;6(3):134–140.
Ailinger, R.L., Deer, M.R. An examination of the self-care needs of clients with rheumatoid arthritis [including commentary by N. Popovich]. Rehabilitation Nursing. 1997;22(3):135–140.
Ailinger, R.L., Lasus, H., Braun, M.A. Revision of the Facts on Osteoporosis Quiz. Nursing Research. 2003;52(3):198–201.
Ailinger, R.L., Moore, J.B., Nguyen, N., Lasus, H. Adherence to latent tuberculosis infection therapy among Latino immigrants. Public Health Nursing. 2006;23(4):307–313.
Aish, A.E., Isenberg, M. Effects of Orem-based nursing intervention on nutritional self-care of myocardial infarction patients. International Journal of Nursing Studies. 1996;33(3):259–270.
Ajzen, I. The theory of planned behaviour. Organizational Behaviour and Human Decision Processes. 1991;50(2):179. 121
Ajzen, I., Fishbein, M. Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice-Hall, 1980.
Alexander, J.S., Younger, R.E., Cohen, R.M., Crawford, L.V. Effectiveness of a nurse-managed program for children with chronic asthma. Journal of Pediatric Nursing. 1988;3(5):312–317.
Amendola, L.R. Toward a caring curriculum. University of North Carolina at Greensboro, 1998. Unpublished doctoral dissertation
Anderberg, P., Lepp, M., Berglund, A.L., Segesten, K. Preserving dignity in caring for older adults: A concept analysis. Journal of Advanced Nursing. 2007;59(6):635–643.
Arthur, D., Chong, C., Rujkorakarn, D., Wong, D., Wongpanarak, N. A profile of the caring attributes of Hong Kong and Thailand psychiatric nurses. International Journal of Mental Health Nursing. 2004;13(2):100–106.
Arthur, D., Pang, S., Wong, T. Caring in context: Caring practices in a sample of Hong Kong nurses. Contemporary Nurse: A Journal for the Australian Nursing Profession. 1998;7(4):198–204.
Arthur, D., Pang, S., Wong, T., Alexander, M.F., Drury, J., Eastwood, et al. Caring attributes, professional self concept and technological influences in a sample of Registered Nurses in eleven countries. International Journal of Nursing Studies. 1999;36(5):387–396.
Artinian, B.M. Conceptual mapping: Development of the strategy. Western Journal of Nursing Research. 1982;4(4):379–393.
Artinian, N.T., Magnan, M., Sloan, M., Lange, M.P. Self-care behaviors among patients with heart failure. Heart & Lung. 2002;31(3):161–172.
Avant, K. The Wilson method of concept analysis. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:55–64.
Baker, L.K. Predictors of self-care in adolescents with cystic fibrosis: A test and explication of Orem’s theories of self-care and self-care deficit. Wayne State University, 1991. Unpublished doctoral dissertation
Baker, S.P. The relationships of self care agency and self care actions to caregiver strain as perceived by female family caregivers of elderly parents. New York University, 1993. Unpublished doctoral dissertation
Barnhill, K.O. The perception of caring in labor and delivery: A phenomenological study. University of Idaho, 2002. Unpublished doctoral dissertation
Beatty, E.R. Locus-of-control, self-actualization and self-care agency among registered nurses. Columbia University Teachers College, 1991. Unpublished doctoral dissertation
Beauchesne, M.F. An investigation of the relationship between social support and the self care agency of mothers of developmentally disabled children. Boston University, 1989. Unpublished doctoral dissertation
Beck, S.L., Dudley, W.N., Barsevick, A. Pain, sleep disturbance, and fatigue in patients with cancer: Using a mediation model to test a symptom cluster [Online exclusive]. Oncology Nursing Forum. 2005;32(3):E48–E55. Retrieved October 20, 2007, from
Bess, C.J. Abilities and limitations of adult type II diabetic patients with integrating of self-care practices into their daily lives. University of Alabama at Birmingham, 1995. Unpublished doctoral dissertation
Biley, F.C., Bauer, R. Bringing the heart back to nursing: human caring practice and education in Germany and the UK. Theoria Journal of Nursing Theory. 2005;14(3):21–25.
Blue, C.L. The predictive capacity of the theory of reasoned action and the theory of planned behavior in exercise research: An integrated literature review. Research in Nursing & Health. 1995;18(2):105–121.
Bottorff, J.L. Assessing an instrument in a pilot project: The self-care agency questionnaire. Canadian Journal of Nursing Research. 1988;20(1):7–16.
Brand, J.M.E. The lived experiences of six women during adjuvant chemotherapy for stage I or II breast cancer. Ball State University, 2005. Unpublished doctoral dissertation
Brilowski, G.A., Wendler, M.C. An evolutionary concept analysis of caring. Journal of Advanced Nursing. 2005;50(6):641–650.
Broome, M.E. Integrative literature reviews in the development of concepts. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:231–250.
Brown, K.L.G. Grief as a conditioning factor affecting the self-care agency and self-care of family caregivers of persons with neurotrauma. Wayne State University, 1996. Unpublished doctoral dissertation
Brunelli, T. A concept analysis: the grieving process for nurses. Nursing Forum. 2005;40(4):123–128.
Brunton, B., Beaman, M. Nurse practitioners’ perceptions of their caring behaviors. Journal of the American Academy of Nurse Practitioners. 2000;12(11):451–456.
Buchanan, S., Ross, E.K. A concept analysis of caring. Perspectives: The Journal of the Gerontological Nursing Association. 1995;19(3):3–6.
Budo, M.L.D., Saupe, R. Ways of care in rural communities: Culture permeating the nursing care [Portuguese]. Texto & Contexto Enfermagem. 2005;14(2):177–185.
Burns, N., Grove, S. Understanding nursing research, (4th ed.). Philadelphia: W.B. Saunders; 2007.
Cade, N.V. Orem’s self care deficit theory applied to hypertensive people [Portuguese]. Revista Latino-Americana de Enfermagem. 2001;9(3):43–50.
Callaghan, D. Healthy behaviors, self-efficacy, self-care, and basic conditioning factors in older adults. Journal of Community Health Nursing. 2005;22(3):169–178.
Callaghan, D.M. The influence of spiritual growth on adolescents’ initiative and responsibility for self-care. Pediatric Nursing. 2005;31(2):91–95. 115
Callaghan, D. Basic conditioning factors influences on adolescents’ healthy behaviors, self-efficacy, and self-care. Issues in Comprehensive Pediatric Nursing. 2006;29(4):191–204.
Callaghan, D. The influence of basic conditioning factors on healthy behaviors, self-efficacy, and self-care in adults. Journal of Holistic Nursing. 2006;24(3):178–185.
Callaghan, D.M. Health-promoting self-care behaviors, self-care self-efficacy, and self-care agency. Nursing Science Quarterly. 2003;16(3):247–254.
Campbell, J.C., Soeken, K.L. Women’s responses to battering: A test of the model. Research in Nursing & Health. 1999;22(1):49–58.
Canty, J.L. An investigation of life change events, hope and self-care agency in inner city adolescents. University of Miami, 1993. Unpublished doctoral dissertation
Caron, C.D., Bowers, B.J. Methods and application of dimensional analysis: A contribution to concept and knowledge development in nursing. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:285–320.
Carroll, D.L. The importance of self-efficacy expectations in elderly patients recovering from coronary artery bypass surgery. Heart & Lung. 1995;24(1):50–59.
Celich, K.L., Crossetti, Mda. G. Being with the carer: A dimension of the caring process [Portuguese]. Revista Gaucha de Enfermagem. 2004;25(3):377–385.
Chang, M.C. Concept analysis of susceptibility [Chinese]. Chinese Journal of Nursing. 2007;54(4):88–93.
Chinn, P.L., Kramer, M.K. Integrated Theory and Knowledge Development in Nursing, (7th ed.). St. Louis: Elsevier; 2007.
Choiniere, R., Lafontaine, P., Edwards, A.C. Distribution of cardiovascular disease risk factors by socioeconomic status among Canadian adults. Canadian Medical Association Journal. 2000;162(9 Suppl):S13–S24.
Christopher, K.A., Hegedus, K. Oncology patients’ and oncology nurses’ perceptions of nurses caring behaviours. European Journal of Oncology Nursing. 2000;4(4):196–206.
Clark, C.S. Human caring theory: expansion and explication. California Institute of Integral Studies, 2004. Unpublished doctoral dissertation
Coates, C.J. The Caring Efficacy Scale: Nurses’ self-reports of caring in practice settings. Advanced Practice Nursing Quarterly. 1997;3(1):53–59.
Coelho, M.J. Revista Brasileira de Enfermagem. 2006;59(6):745–751.
Coffey, S. Development of the concept of covenant between nurse and patient. Catholic University of America, 2004. Unpublished doctoral dissertation
Coffey, S. The nurse-patient relationship in cancer care as a shared covenant: A concept analysis. Advances in Nursing Science. 2006;29(4):308–323.
Coffman, M.J. Cultural caring in nursing practice: A meta-synthesis of qualitative research. Journal of Cultural Diversity. 2004;11(3):100–109.
Cooley, M.E., Short, T.H., Moriarty, H.J. Symptom prevalence, distress, and change over time in adults receiving treatment for lung cancer. Psycho-Oncology. 2003;12(7):694–708.
Cortis, J.D., Kendrick, K. Nursing ethics, caring and culture. Nursing Ethics. 2003;10(1):77–88.
A dimensional structure of nurse-patient interactions from a caring perspective: Refinement of the Caring Nurse-Patient Interaction Scale (CNPI-Short Scale). Journal of Advanced Nursing. 2006;55(2):198–214.
Cossette, S., Pepin, J., Ricard, N., Côté, J. A factorial-dimensional structure of the Caring Nurse-Patient Interaction-Short Scale (CNPl-Short Scale). International Journal for Human Caring. 2005;9(2):31.
Covington, H. Caring presence: Delineation of a concept for holistic nursing. Journal of Holistic Nursing. 2003;21(3):301–317.
Cowling, W.R., III., Taliaferro, D. Emergence of a healing-caring perspective: Contemporary conceptual and theoretical directions. Journal of Theory Construction & Testing. 2004;8(2):54–59.
Cull, V.V. Exposure to violence and self-care practices of adolescents. University of Alabama at Birmingham, 1995. Unpublished doctoral dissertation
Dashiff, C.J. Self- and dependent-care responsibility of adolescents with IDDM and their parents. Journal of Family Nursing. 2003;9(2):166–183.
Deary, V., Deary, I.J., McKenna, H.P., McCance, T.V., Watson, R., Hoogbruin, A.L. Elisions in the field of caring. Journal of Advanced Nursing. 2002;39(1):96–102.
Degner, L.F., Sloan, J.A. Symptom distress in newly diagnosed ambulatory cancer patients and as a predictor of survival in lung cancer. Journal of Pain and Symptom Management. 1995;10(6):423–431.
Dellasega, C. SCOPE: A practical method for assessing the self-care status of elderly persons. Rehabilitation Nursing Research. 1995;4(4):128–135.
Delmar, C. Caring-ethical phronetic research: epistemological considerations. International Journal for Human Caring. 2006;10(1):22–27.
Denyes, M.J. Development of an instrument to measure self-care agency in adolescents. University of Michigan, Ann Arbor, 1980. Unpublished doctoral dissertation
Denyes, M.J. Measurement of self-care agency in adolescents [Abstract]. Nursing Research. 1982;31(1):63.
Dodd, M.J. Measuring informational intervention for chemotherapy knowledge and self-care behavior. Research in Nursing & Health. 1984;7(1):43–50.
Dodd, M.J. Patterns of self-care in cancer patients receiving radiation therapy. Oncology Nursing Forum. 1984;10(3):23–27.
Dodd, M.J. Efficacy of proactive information on self-care in radiation therapy patients. Heart & Lung. 1987;16(5):538–544.
Dodd, M.J., Dibble, S.L. Predictors of self-care: A test of Orem’s model. Oncology Nursing Forum. 1993;20(6):895–901.
Dodd, M.J., Larson, P.J., Dibble, S.L., Miaskowski, C., Greenspan, D., MacPhail, L., et al. Randomized clinical trial of chlorhexidine versus placebo for prevention of oral mucositis in patients receiving chemotherapy. Oncology Nursing Forum. 1996;23(6):921–927.
Dodd, M.J., Miaskowski, C. The PRO-SELF program: A self-care intervention program for patients receiving cancer treatment. Seminars in Oncology Nursing. 2000;16(4):300–314.
Dodd, M.J., Miaskowski, C., Paul, S.M. Symptom clusters and their effect on the functional status of patients with cancer. Oncology Nursing Forum. 2001;28(3):465–470.
Dowd, T.T. Relationship among health state factors, foundational capabilities and urinary incontinence self-care in women. Wayne State University, 1994. Unpublished doctoral dissertation
Droomers, M., Schrijvers, C.T., van de Mheen, H., Mackenback, J.P. Educational differences in leisure-time physical inactivity: a descriptive and explanatory study. Social Science and Medicine. 1998;47(11):1665–1676.
Duffy, J.R. An analysis of the relationships among nurse caring behaviors and selected outcomes of care in hospitalized medical and/or surgical patients. Catholic University of America, 1990. Doctoral Dissertation
Duffy, J.R., Hoskins, L.M. The quality-caring model: Blending dual paradigms. Advances in Nursing Science. 2003;26(1):77–88.
Duffy, J.R., Hoskins, L., Seifert, R.F. Advances in Nursing Science. 2007;30(3):235–245.
Dulock, H.L., Holzemer, W.L. Substruction: Improving the linkage from theory to method. Nursing Science Quarterly. 1991;4(2):83–87.
Easley, R. Harmony: a concept analysis. Journal of Advanced Nursing. 2007;59(5):551–556.
Eriksson, K. Nursing Science Quarterly. 1992;5(2):93.
Eriksson, K. Scandinavian Journal of Caring Sciences. 1992;6(2):119–123.
Evers, G.C. M., Isenberg, M.A., Philipsen, H., Senten, M., Brouns, G. Validity testing of the Dutch translation of the appraisal of the self-care agency A.S.A. scale. International Journal of Nursing Studies. 1993;30(4):331–342.
Fagerström, L., Eriksson, K., Engberg, I.B. The patient’s perceived caring needs as a message of suffering. Journal of Advanced Nursing. 1998;28(5):978–987.
Fain, J.A., Nettles, A., Funnell, M.M., Charron, D. Diabetes patient education research: An integrative literature review. Diabetes Educator. 1999;25(6, Suppl):7–15.
Fawcett, J. The relationship of theory and research. Norwalk, CT: Appleton-Century-Crofts, 1999.
Fealy, G.M. Professional caring: The moral dimension. Journal of Advanced Nursing. 1995;22(6):1135–1140.
Fialho, A.V. M., Pagliuca, L.M. F., Soares, E. The Self-Care Deficit Theory adjustment in home-care in the light of Barnum’s model [Portuguese]. Revista Latino-Americana de Enfermagem. 2002;10(5):715–720.
Finfgeld-Connent, D. Clarification of social support. Journal of Nursing Scholarship. 2005;37(1):4–9.
Finfgeld-Connent, D. Concept comparison of caring and social support. International Journal of Nursing Terminologies & Classifications. 2007;18(2):58–68.
Fishbein, M., Ajzen, I. Belief, attitude, intention and behavior. Boston: Addison-Wesley, 1975.
Fok, M.S., Alexander, M.F., Wong, T.K., McFayden, A.K. Contextualising the Appraisal of Self-Care Agency Scale in Hong Kong. Contemporary Nurse. 2002;12(2):124–134.
Fok, M.S., Wong, T.K. Testing Orem’s self-care agency and basic conditioning factors in a Chinese community undergoing haemodialysis. Contemporary Nurse: A Journal for the Australian Nursing Profession. 2003;15(3):262–272.
Fok, M.S., Daly, J., Clinical Application of Orem’s Self-care Model of Nursing in a Chinese Community. Advances in Contemporary Transcultural Nursing, v.1. eContent Management Pty Ltd, 2003:262–272.
Folden, S.L. The effect of supportive-educative nursing interventions on poststroke older adults’ self-care perceptions. University of Miami, 1990. Unpublished doctoral dissertation
Folden, S.L. Effect of a supportive-educative nursing intervention on older adults’ perception of self-care after a stroke. Rehabilitation Nursing. 1993;18(3):162–167.
Forbat, L. The care and abuse of minoritized ethnic groups: the role of statutory services. Critical Social Policy. 2004;24(3):312–331.
Fox, S.W., Lyon, D.E. Symptom clusters and quality of life in survivors of lung cancer. Oncology Nursing Forum. 2006;33(5):931–936.
Fredriksson, L. Modes of relating in a caring conversation: A research synthesis on presence, touch and listening. Journal of Advanced Nursing. 1999;30(5):1167–1176.
Fredriksson, L., Eriksson, K. The ethics of the caring conversation. Nursing Ethics. 2003;10(2):138–148.
Freeman, E.M. Self-care agency in gay men with HIV infection. San Francisco: University of California, 1992. Unpublished doctoral dissertation
Frey, M.A., Denyes, M.J. Health and illness self-care in adolescents with IDDM: A test of Orem’s theory. Advances in Nursing Science. 1989;12(1):67–75.
Frey, M.A., Fox, M.A. Assessing and teaching self-care to youths with diabetes mellitus. Pediatric Nursing. 1990;16(6):597–599.
Fridh, I., Bergbom, I. To watch: A study of the concept [Norwegian]. Nordic Journal of Nursing Research & Clinical Studies. 2006;26(1):4–8.
Gaffney, K.F., Moore, J.B. Testing Orem’s theory of self-care deficit: Dependent care agent performance for children. Nursing Science Quarterly. 1996;9(4):160–164.
Gammon, J. Coping with cancer: The role of self-care. Nursing Practice. 1991;4(3):11–15.
Geden, E., Taylor, S. Construct and empirical validity of the Self-as-Carer Inventory. Nursing Research. 1991;40(1):47–50.
Gift, A.G., Jablonski, A., Stommel, M., Given, C.W. Symptom clusters in elderly patients with lung cancer. Oncology Nursing Forum. 2004;31(2):202–212.
Gift, A.G., Stommel, M., Jablonski, A., Given, W. A cluster of symptoms over time in patients with lung cancer. Nursing Research. 2003;52(6):393–400.
Given, B., Given, C., Azzouz, F., Stommel, M. Physical functioning of elderly cancer patients prior to diagnosis and following initial treatment. Nursing Research. 2001;50(4):222–232.
Given, C.W., Given, B., Azzouz, F., Kozachik, S., Stommel, M. Predictors of pain and fatigue in the year following diagnosis among elderly cancer patients. Journal of Pain and Symptom Management. 2001;21(6):456–466.
Gomes, M.M. A concept analysis of relational aggression. Journal of Psychiatric & Mental Health Nursing. 2007;14(5):510–515.
Gramling, K.L. Ice chips and hope: The coach’s story of caring art. International Journal for Human Caring. 2004;8(2):62–64.
Greenfield, P.H. A comparison of the self-care ability of employed women who have and have not maintained weight loss. Catholic University of America, 1989. Unpublished doctoral dissertation
Gregg, M.F., Magilvy, J.K. Values in clinical nursing practice and caring. Japan Journal of Nursing Science. 2004;1(1):11–18.
Gulick, E.E. Parsimony and model confirmation of the ADL self-care scale for multiple sclerosis persons. Nursing Research. 1987;36(5):278–283.
Gulick, E.E. The self-administered ADL scale for persons with multiple sclerosis. In: Waltz, C., Strickland, O., eds. The measurement of nursing outcomes, Vol. 1. New York: Springer; 1988:128–159.
Gulick, E.E. Model confirmation of the MS-related symptom checklist. Nursing Research. 1989;38(3):147–153.
Haas, D.L. The relationship between coping dispositions and power components of dependent-care agency in parents of children with special health care needs. Wayne State University, 1990. Unpublished doctoral dissertation
Haase, J.E., Leidy, N.K., Coward, T.B., Britt, T., Penn, P.E. Simultaneous concept analysis: A strategy for developing multiple interrelated concepts. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:209–230.
Hagopian, G.A. The effects of informational audiotapes on knowledge and self-care behaviors of patients undergoing radiation therapy. Oncology Nursing Forum. 1996;23(4):697–700.
Hanson, B.R., Bickel, L. Development and testing of the questionnaire on perception of self-care agency. In: The science and art of self-care. Norwalk, CT: Appleton-Century-Crofts; 1985:271–278.
Hanucharurnkul, S. Predictors of self-care in cancer patients receiving radiotherapy. Cancer Nursing. 1989;12(1):21–27.
Harris, M.A. Health-deviation self-care, dependent-care, disclosure, and health of children with perinatal HIV/AIDS. Wayne State University, 2004. Unpublished doctoral dissertation
Hart, M.A. Self-care agency and prenatal care actions: Relationships to pregnancy outcomes. Case Western Reserve University (Health Sciences), 1993. Unpublished doctoral dissertation
Hart, M.A. Orem’s Self-care Deficit Theory: Research with pregnant women. Nursing Science Quarterly. 1995;8(3):120–126.
Hart, M.A. Self-care agency before and after childbirth education classes. International Orem Society Newsletter. 1998;6(2):10–11.
Hart, M.A., Foster, S.N. Self-care agency in two groups of pregnant women. Nursing Science Quarterly. 1998;11(4):167–171.
Hartley, L.A. Congruence between teaching and learning self-care: A pilot study. Nursing Science Quarterly. 1988;1(4):161–167.
Hartweg, D.L. Health promotion self-care actions of healthy, middle-aged women. Wayne State University, 1991. Unpublished doctoral dissertation
Hartweg, D.L., Orem, D. Self-care deficit theory. Newbury Park, CA: Sage, 1991.
Helin, K., Lindström, U.A. Sacrifice: An ethical dimension of caring that makes suffering meaningful. Nursing Ethics. 2003;10(4):414–427.
Henderson, A. Emotional labor and nursing: An under-appreciated aspect of caring work. Nursing Inquiry. 2001;8(2):130–138.
Hinshaw, A.S. Theoretical substruction: An assessment process. Western Journal of Nursing Research. 1979;1(4):319–324.
Hoekstra, J., Vernooij-Dassen, M.J., de Vos, R., Bindels, P.J. The added value of assessing the “most troublesome” symptom among patients with cancer in the palliative phase. Patient Education and Counseling. 2006;65(2):223–229.
Hoffman, A.J., Given, B.A., von Eye, A., Gift, A.G., Given, C.W. Relationships among pain, fatigue, insomnia, and gender in persons with lung cancer. Oncology Nursing Forum. 2007;34(4):785–792.
Hopwood, P., Stephens, R.J. Symptoms at presentation for treatment in patients with lung cancer: Implications for the evaluation of palliative treatment. The Medical Research Council (MRC) Lung Cancer Working Party. British Journal of Cancer. 1995;71(3):633–636.
Hsieh, C., Gau, M., Mao, H., Li, C. The development and psychometric testing of a self-care scale for dysmenorrhic adolescents. Journal of Nursing Research. 2004;12(2):119–130.
Hupcey, J.E., Miller, J. Community dwelling adults’ perception of interpersonal trust vs. trust in health care providers. Journal of Clinical Nursing. 2006;15(9):1132–1139.
Hurst, C., Montgomery, A.J., Davis, B.L., Killion, C., Baker, S. The relationship between social support, self-care agency, and self-care practices of African American women who are HIV-positive. Journal of Multicultural Nursing & Health. 2005;11(3):11–22.
Hurst, J.D. The relationship among self-care agency, risk-taking, and health risks in adolescents. University of Alabama at Birmingham, 1991. Unpublished doctoral dissertation
Isenberg, M., Evers, G., Brouns, G. An international research project to test Orem’s self-care deficit theory. In: Proceedings of the International Research Congress. Edinburgh, Scotland: University of Edinburgh; 1987.
James, K.S. Factors related to self-care agency and self-care practices of obese adolescents. University of San Diego, 1991. Unpublished doctoral dissertation
James, W.P., Nelson, M., Ralph, A., Leather, S. Socioeconomic determinants of health. The contribution of nutrition to inequalities in health. British Medical Journal. 1997;314(7093):1545–1549.
Jensen, B.J. Sygeplejersken / Danish Journal of Nursing. 2006;106(15):40–43.
Jesek-Hale, S.R. Self-care agency and self care in pregnant adolescents: A test of Orem’s theory. College of Nursing, 1994. Unpublished doctoral dissertation, Rush University
Johns, C. Reflective practice: Revealing the [he]art of caring. International Journal of Nursing Practice. 2001;7(4):237–245.
Jones, C.B., Alexander, J.W. The technology of caring: A synthesis of technology and caring for nursing administration. Nursing Administration Quarterly. 1993;17(2):11–20.
Joudrey, R., Gough, J. Caring and curing revisited: student nurses’ perceptions of nurses’ and physicians’ ethical stances. Journal of Advanced Nursing. 1999;29(5):1154–1162.
Kamphuis, C.B. M., van Lenthe, F.J., Giskes, K., Brug, J., Mackenback, J.P. Perceived environmental determinants of physical activity and fruit and vegetable consumption among high and low socioeconomic groups in the Netherlands. Health & Place. 2007;13(2):493–503.
Kaplan, G.A., Lynch, J.W. Whither studies on the socioeconomic foundations of population health. American Journal of Public Health. 1997;87(9):1409–1411.
Kearney, B.Y., Fleischer, B.J. Development of an instrument to measure exercise of self-care agency. Research in Nursing & Health. 1979;2(1):25–34.
Kelly, D. Caring and cancer nursing: Framing the reality using selected social science theory. Journal of Advanced Nursing. 1998;28(4):728–736.
Kongsaktrakul, C., Suchaxaya, P., Kantawang, S., Schepp, K.G., Visudtibhan, A., Chinvarun, Y. A causal model of self-care behavior for adolescents with epilepsy. Thai Journal of Nursing Research. 2006;10(4):264–275.
Koster, M.K. A comparison of the relationship among self-care agency, self-determinism, and absenteeism in two groups of school-age children. University of Texas at Austin, 1995. Unpublished doctoral dissertation
Kostopoulos, M.R., The reliability and validity of a nurse performance evaluation tool. Measurement of nursing outcomes, Vol. 2. New York: Springer, 1988:77–95.
Kunyk, D., Olson, J.K. Clarification of conceptualizations of empathy. Journal of Advanced Nursing. 2001;35(3):317–325.
Kuo, C.L., Turton, M.A., Lee-Hsieh, J., Tseng, H.F., Hsu, C.L. Measuring peer caring behaviors of nursing students: Scale development. International Journal of Nursing Studies. 2007;44(2007):105–114.
Kurtz, M.E., Kurtz, J.C., Stommel, M., Given, C.W., Given, B.A. Symptomatology and loss of physical functioning among geriatric patients with lung cancer. Journal of Pain and Symptom Management. 2000;19(4):249–256.
Kyle, T.V. The concept of caring: A review of the literature. Journal of Advanced Nursing. 1995;21(3):506–514.
Lackey, N.R. Concept clarification: Using the Norris method in clinical research. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:193–208.
Lake, P.K. Transformation: student nurses’ experiences in learning the caring process in nursing. University of Texas at Tyler, 2004. Unpublished dissertation
Larson, P.J. Comparison of cancer patients’ and professional nurses’ perceptions of important caring behaviors. Heart & Lung. 1987;16(2):187–193.
Lea, A., Watson, R., Deary, I.J. Caring in nursing: a multivariate analysis. Journal of Advanced Nursing. 1998;28(3):662–671.
Lee, M.B. Power, self-care and health in women living in urban squatter settlements in Karachi, Pakistan: A test of Orem’s theory. Journal of Advanced Nursing. 1999;30(1):248–259.
Leh, S.K. Preconceptions: a concept analysis for nursing. Nursing Forum. 2007;42(3):109–122.
Lenz, E.R., Pugh, L.C., Milligan, R.A., Gift, A., Suppe, F. The middle-range theory of unpleasant symptoms: An update. Advances in Nursing Science. 1997;19(3):14–27.
Lewis, S.M. Practice applications. Caring as being in nursing: Unique or ubiquitous. Nursing Science Quarterly. 2003;16(1):37–43.
Lin, Y., Chiou, C. Concept analysis of caring [Chinese]. Chinese Journal of Nursing. 2003;50(6):74–78.
Lindholm, L., Nieminen, A., Mäkelä, C., Rantanen-Siljamäki, S. Clinical application research: A Hermeneutical approach to the appropriation of caring science. Qualitative Health Research. 2006;16(1):137–150.
Liu, J.E., Mok, E., Wong, T. Caring in nursing: Investigating the meaning of caring from the perspective of cancer patients in Beijing, China. Journal of Clinical Nursing. 2006;15(2):188–196.
Lorensen, M. Psychometric properties of self-care management and life-quality amongst elderly. Clinical Effectiveness in Nursing. 1998;2(2):78–85.
Lorensen, M., Holter, I., Evers, G., Isenberg, M., van Achterberg, T. Cross-cultural testing of the “appraisal of self-care agency”: ASA scale in Norway. International Journal of Nursing Studies. 1993;30(1):15–23.
Lorenz, S.G. Protection: Clarifying the concept for use in nursing practice. Holistic Nursing Practice. 2007;21(3):115–123.
Lucena, Ade.F., Crossetti, Mda.G. The meaning of caring in the intensive care unit [Portuguese]. Revista Gaucha de Enfermagem. 2004;25(2):243–256.
Lukkarinen, H., Hentinen, M. Self-care agency and factors relating this agency among patients with coronary health disease. International Journal of Nursing Studies. 1997;34(4):295–304.
Maas, M.L., Moorhead, S., Specht, J.P., Schoenfelder, D.P., Swanson, E.A., Johnson, M.L., et al. Concept development of nursing-sensitive outcomes. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:387–400.
Mackenbach, J.P., Bos, V., Andersen, O., Cardano, M., Costa, G., Hardin, S., et al. Widening socioeconomic inequalities in mortality in six Western European countries. International Journal of Epidemiology. 2003;32(5):830–837.
Mapanga, K.G. The influence of family and friends’ basic conditioning factors, and self-care agency on unmarried teenage primiparas’ engagement in a contraceptive practice. Case Western Reserve University (Health Sciences), 1994. Unpublished doctoral dissertation
Marck, P. Therapeutic reciprocity: A caring phenomenon. Advances in Nursing Science. 1990;13(1):49–59.
Mattsson-Lidsle, B., Lindström, U.A. Consolation: A concept analysis [Swedish]. Nordic Journal of Nursing Research & Clinical Studies. 2001;21(3):47–50.
McBride, S. Validation of an instrument to measure exercise of self-care agency. Research in Nursing & Health. 1987;10(5):311–316.
McBride, S.H. Comparative analysis of three instruments designed to measure self-care agency. Nursing Research. 1991;40(1):12–16.
McCaleb, A., Edgil, A. Self-concept and self-care practices of healthy adolescents. Journal of Pediatric Nursing. 1994;9(4):233–238.
McCaleb, K.A. Self-concept and self-care practices of healthy adolescents. University of Alabama at Birmingham, 1991. Unpublished doctoral dissertation
McCance, T.V. Caring in nursing practice: The development of a conceptual framework. Research & Theory for Nursing Practice. 2003;17(2):101–116.
McCance, T.V., McKenna, H.P., Boore, J.R. Caring: Dealing with a difficult concept. International Journal of Nursing Studies. 1997;34(4):241–248.
McCance, T.V., McKenna, H.P., Boore, J.R. Exploring caring using narrative methodology: An analysis of the approach. Journal of Advanced Nursing. 2001;33(3):350–356.
McDermott, M.A. The relationship between learned helplessness and self-care agency in adults as a function of gender and age. New York University, 1989. Unpublished doctoral dissertation
McIntosh, L.C. Nurses’ experiences with healing and spirituality. University of North Carolina at Greensboro, 2004. Unpublished dissertation
Metcalfe, S.A., Metcalfe, S.A. Self-care actions as a function of therapeutic self-care demand and self-care agency in individuals with chronic obstructive pulmonary disease. Wayne State University, 1996. Unpublished doctoral dissertation
Miaskowski, C., Dodd, M., Lee, K. Symptom clusters: The new frontier in symptom management research. Journal of the National Cancer Institute Monographs. 2004;32:17–21.
Monsen, R.B. Autonomy, coping, and self-care agency in healthy adolescents and in adolescents with spina bifida. University of Alabama at Birmingham, 1988. Unpublished doctoral dissertation
Monteiro, E.M., da Nobraga, M.M., de Lima, L.S. Self-care and the adult with asthma: The systematization of nursing assistance [Portuguese]. Revista Brasileira de Enfermagem. 2002;55(2):134–139.
Moody, L.E. Building a conceptual map to guide research. Florida Nursing Review. 1989;4(1):1–5.
Moore, J.B. Predictors of children’s self-care performance: Testing the theory of self-care deficit. Scholarly Inquiry for Nursing Practice: An International Journal. 1993;7(3):199–217.
Moore, J.B. Measuring the self-care practice of children and adolescents: Instrument development. Maternal-Child Nursing Journal. 1995;23(3):101–108.
Moore, J.B., Gaffney, K.F. Development of an instrument to measure mother’s performance of self-care activities for children. Advances in Nursing Science. 1989;12(1):76–84.
Moore, J.B., Mosher, R.B. Adjustment responses of children and their mothers to cancer self-care and anxiety. Oncology Nursing Forum. 1997;24(3):519–525.
Morse, J. Exploring pragmatic utility: Concept analysis by critically appraising the literature. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:333–352.
Morse, J.M., Solberg, S.M., Neander, W.L., Bottorff, J.L., Johnson, J.L. Concepts of caring and caring as a concept. Advances in Nursing Science. 1990;13(1):1–14.
Mosher, R.B., Moore, J.B. The relationship of self-concept and self-care in children with cancer. Nursing Science Quarterly. 1998;11(3):116–122.
Nåden, D., Saeteren, B. Cancer patients’ perception of being or not being confirmed. Nursing Ethics. 2006;13(3):222–235.
Nahas, V. Research feature. Muslim patients’ perceptions of a caring nurse [Singapore]. Professional Nurse. 1997;24(2):20–23.
Nahcivan, N.O. A Turnkish language equivalence of the exercise of self-care agency scale. Western Journal of Nursing Research. 2004;26(7):813–824.
Ness, A.R., Powles, J.W. Fruit and vegetables, and cardiovascular disease: A review. International Journal of Epidemiology. 1997;26(1):1–13.
Newman, M.A. Theory development in nursing. Philadelphia: F.A. Davis, 1979.
Newman, M.A. Health as expanding consciousness. Boston: Jones & Bartlett, 1999.
Niu, T. The philosophy of nursing management: A conceptual analysis [Chinese]. Chinese Journal of Nursing. 2005;52(5):5–9.
Noh, C.H., Arthur, D., Sohng, K.Y. Relationship between technological influences and caring attributes of Korean nurses. International Journal of Nursing Practice. 2002;8(5):247–256.
Nyberg, J. Human care and economics: a nursing study. University of Colorado Health Sciences Center, 1989. Doctoral Dissertation
O’Berle, K., Davies, B. Support and caring: exploring the concepts. Oncology Nursing Forum. 1992;19(5):763–767.
O’Connor, N.A. Maieutic dimensions of self-care in aging: Instrument development. Wayne State University, 1995. Unpublished doctoral dissertation
Orem, D.E. Nursing: Concepts of practice, (6th ed.). New York: Mosby; 2001.
Page, C., Ricard, N. Conceptual and theoretical foundations for an instrument designed to identify self-care requisites in women treated for depression [French]. Canadian Journal of Nursing Research. 1996;28(3):95–112.
Pang, S.M., Wong, T.K., Wang, C.S., Zhang, Z.J., Chan, H.Y., Lam, C.W., et al. Towards a Chinese definition of nursing. Journal of Advanced Nursing. 2004;46(6):657–670.
Patistea, E. Nurses’ perceptions of caring as documented in theory and research. Journal of Clinical Nursing. 1999;8(5):487.
Pepin, J.I. Family caring and caring in nursing. Image: Journal of Nursing Scholarship. 1992;24(2):127–131.
Perini, C., Stauffer, Y., Grunder, M., Gandon, M., Datwyler, B., Hantikainen, V. The meaning of caring from the viewpoint of patients with wounds due to peripheral vascular disease [German]. Pflege. 2006;19(6):345–355.
Phelan, D.L., Oliveria, S.A., Christos, P.J., Dusza, S.W., Halpern, A.C. Skin self-examination in patients at high risk for melanoma: a pilot study. Oncology Nursing Forum. 2003;30(6):1029–1036.
Pipatananond, P., Hanucharurnkul, S. Development of the Psychiatric Patient’s Caregiver Burden Scale (The PPCBS). Thai Journal of Nursing Research. 2003;7(1):37–48.
Pollock, S.E. Human response to chronic illness: Physiologic and psychological adaptation. Nursing Research. 1986;35(2):90–95.
Pollock, S.E. Adaptation to chronic illness: A program of research for testing nursing theory. Nursing Science Quarterly. 1993;6(2):86–92.
Pressly, K.B. Psychosocial characteristics of CAPD patients and the occurrence of infectious complications. American Nephrology Nurses’ Association Journal. 1995;2(6):563–574.
Priest, H.M. The use of narrative in the study of caring: A critique. NT Research. 2000;5(4):245–252.
Reed, P. The theory of self-transcendence. In: Middle range theory for nursing. New York: Springer; 2003:145–165.
Renker, P.R. Physical abuse, social support, self-care, and pregnancy outcomes of older adolescents. JOGNN: Journal of Obstetric, Gynecologic, & Neonatal Nursing. 1999;28(4):377–388.
Riesch, S.K., Hauck, M.R. The exercise of self-care agency: An analysis of construct and discriminant validity. Research in Nursing & Health. 1988;11(4):245–255.
Riley, C.P. Effects of a pulmonary rehabilitation program on dyspnea, self care, and pulmonary function of patients with chronic obstructive pulmonary disease. University of Alabama at Birmingham, 1988. Unpublished doctoral dissertation
Roberts, K.T., Fitzgerald, L. Serenity: caring with perspective. Scholarly Inquiry for Nursing Practice. 1991;5(2):127–146.
Robinson, M.K. Determinants of functional status in chronically ill adults. University of Alabama at Birmingham, 1995. Unpublished doctoral dissertation
Rodgers, B.L. Concept analysis: An evolutionary view. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:77–102.
Rodriquez, D. Medicine or caring science in ancient Greece [Spanish]. Cultura de los Cuidados. 1999;3(5):33–37.
Rogers, B. Nursing: an ethic of caring. AAOHN Journal. 2003;51(4):155–157.
Rogers, M. Science of unitary human beings. In: Explorations on Martha Rogers’ science of unitary human beings. Norwalk, CT: Appleton-Century-Crofts; 1986:3–8.
Rogers, M.E. An introduction to the theoretical basis of nursing. Philadelphia: F.A. Davis, 1970.
Rogers, M.E. Nursing: A science of unitary man. In Conceptual models for nursing practice, (2nd ed.), Norwalk, CT: Appleton-Century-Crofts; 1980:329–337.
Rogers, M.E. A paradigm for nursing. In: Family health: A theoretical approach to nursing care. New York: Wiley; 1983:219–227.
Rogers, M.E. Nursing science and art: A prospective. Nursing Science Quarterly. 1988;1(3):99–102.
Roper, N., Logan, W., Tierney, A. The Roper-Logan-Tierney Model: a model in nursing practice. In: Blueprint for use of nursing models: education, research, practice, and administration. National League for Nursing; 1996:289–314.
Roy, C. Introduction to nursing: An adaptation model, (2nd ed.). Englewood Cliffs, NJ: Prentice-Hall; 1984.
Roy, C. An explication of the philosophical assumptions of the Roy adaptation model. Nursing Science Quarterly. 1988;1(1):26–34.
Roy, C. Response to dialogue on a theoretical issue: Strengthening the Roy adaptation model through conceptual clarification. Nursing Science Quarterly. 1990;3(2):64–66.
Roy, C. Future of the Roy model: Challenge to redefine adaptation. Nursing Science Quarterly. 1997;10(1):42–48.
Roy, C., Roberts, S.L. Theory construction in nursing: An adaptation model. Englewood Cliffs, NJ: Prentice-Hall, 1981.
Sadler, J., Brilowski, G.A., Wendler, M. An evolutionary concept analysis of caring. Journal of Advanced Nursing. 2006;50(6):641–650. In response to (2005)
Sadler, J.J. A multiphase approach to concept analysis and development. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:251–284.
Sadler, J.J. Descriptions of caring uncovered in students’ baccalaureate program admission essays. International Journal for Human Caring. 2004;8(3):37–46.
Santos, Z.M., da Silva, R.M. Self-care practice lived by hipertensive [sic] woman: Analysis on the health education focus [Portuguese]. Revista Brasileira de Enfermagem. 2006;59(2):206–211.
Sarna, L. Correlates of symptom distress in women with lung cancer. Cancer Practice. 1993;1(1):21–28.
Sarna, L. Fluctuations in physical function: Adults with non-small cell lung cancer. Journal of Advanced Nursing. 1993;18(5):714–724.
Schantz, M.L. Compassion: A concept analysis. Nursing Forum. 2007;42(2):48–55.
Schoenhofer, S.O. Theoretical concerns: Philosophical underpinnings of an emergent methodology for nursing as caring inquiry. Nursing Science Quarterly. 2002;15(4):275–280.
Schott-Baer, D. Dependent care, caregiver burden, and self-care agency of spouse caregivers. Cancer Nursing. 1993;16(3):230–236.
Schott-Baer, D., Fisher, L., Gregory, C. Dependent care, caregiver burden, hardiness and self-care agency of caregivers. Cancer Nursing. 1995;18(4):299–305.
Schumacher, D.L. Caring behaviors of preceptors as perceived by new nursing graduate orientees. Colorado State University, 2005. Unpublished dissertation
Schwartz-Barcott, D., Kim, H.S. An expansion and elaboration of the hybrid model of concept development. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:129–160.
Scott, L.D. Correlates of health promotion in elders. Louisiana State University Medical Center in New Orleans School of Nursing, 1995. Unpublished doctoral dissertation
Scott, P.A. Care, attention and imaginative identification in nursing practice. Journal of Advanced Nursing. 1995;21(6):1196–1200.
Selye, H. The stress of life. New York: McGraw-Hill, 1976.
Sherwood, G.D. Meta-synthesis of qualitative analyses of caring: Defining a therapeutic model of nursing. Advanced Practice Nursing Quarterly. 1997;3(1):32–42.
da Silva, L.M. A brief reflection on self-care in hospital discharge planning after a bone marrow transplantation (BMT): A case report [Portuguese]. Revista Latino-Americana de Enfermagem. 2001;9(4):75–82.
Silva, M.C. Selection of a theoretical framework. In: Readings for nursing research. St. Louis: Mosby; 1981:17–28.
Silva, M.C. Research testing nursing theory: State of the art. Advances in Nursing Science. 1986;9(1):1–11.
Simmons, S.J. Self-care agency and health-promoting behavior of a military population. Medical College of Georgia, 1990. Unpublished doctoral dissertation
Slusher, I.L. Self-care agency and self-care practice of adolescents. Issues in Comprehensive Pediatric Nursing. 1999;22(1):49–58.
Smith, A. An analysis of altruism: A concept of caring. Journal of Advanced Nursing. 1995;22(4):785–790.
Smith, G.D., Brunner, E. Socio-economic differentials in health: The role of nutrition. Proceedings of the Nutrition Society. 1997;56(1A):75–90.
Smith, M.C. Caring and the science of unitary human beings. Advances in Nursing Science. 1999;21(4):14–28.
Smith-Campbell, B. A case study on expanding the concept of caring from individuals to communities. Public Health Nursing. 1999;16(6):405–411.
Soderhamn, O., Cliffordson, C. The internal structure of the Appraisal of Self-care Agency (ASA) scale. Theoria Journal of Nursing Theory. 2001;10(4):5–12.
Söderlund, M. Qualitative research approaches of relevance for caring sciences [Swedish]. Nordic Journal of Nursing Research & Clinical Studies. 2003;23(2):9–15.
Sourial, S. An analysis of caring. Journal of Advanced Nursing. 1997;26(6):1189–1192.
Sousa, V.D. Testing a conceptual framework for diabetes self-management. Case Western Reserve University (Health Sciences), 2003. Unpublished doctoral dissertation
Sousa, V.D., Zauszniewski, J.A. Toward a theory of diabetes self-care management. Journal of Theory Construction & Testing. 2005;9(2):61–67.
St. Onge, J.L. The relationship of self-care agency to health-seeking behaviors in Caucasian and black U.S. veterans. University of South Africa, 1988. Unpublished doctoral dissertation
Stember, M.L. Model building as a strategy for theory development. In: Nursing research methodology: Issues and implementation. Rockville, MD: Aspen; 1986:103–119.
Su, Y., Songwathana, P., Naka, K. Factor related to self-care among Chinese women with mastectomy in Beijing. Thai Journal of Nursing Research. 2006;10(4):252–263.
Sumner, J. Concept analysis: the moral construct of caring in nursing as communicative action. International Journal for Human Caring. 2006;10(1):8–16.
Sun, F.K., Long, A., Boore, J., Tsao, L.I. Patients and nurses’ perceptions of ward environmental factors and support systems in the care of suicidal patients. Journal of Clinical Nursing. 2006;15(1):83–92.
Suppe, F., Jacox, A.K., Philosophy of science and the development of nursing theory. Annual review of nursing research, Vol. 3. New York: Springer, 1985:241–267.
Swanson, K.M. Nursing Research. 1999;48(6):288–298.
Swanson, K.M. What is known about caring in nursing science: A literary meta-analysis. In: Handbook of clinical nursing research. Thousand Oaks, CA: Sage; 1999.
Torres, Gde.V., Davim, R.M., da Nobrega, M.M. Application of the nursing process based in Orem’s theory: A case study with a pregnant adolescent [Spanish]. Revista Latino-Americana de Enfermagem. 1999;7(2):47–53.
Turkel, M.C., Ray, M.A., Malinski, V.M. Research issues. Relational complexity: from grounded theory to instrument development and theoretical testing … synthesis of the research findings from a 5-year program of qualitative and quantitative studies. Nursing Science Quarterly. 2001;14(4):281–287.
U.S. Department of Health and Human Services (US DHHS). Physical activity and health. A report of the Surgeon General U.S. Department of Health and Human Services, Center for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Atlanta, GA. 1996.
van Achterberg, T., Lorensen, M., Isenberg, M.A., Evers, G.C., Levin, E., Philipsen, H. The Danish and Dutch version of the Appraisal of Self-care Agency scale, comparing reliability aspects. Scandinavian Journal of Caring Sciences. 1991;5(2):101–108.
Van Duyn, M.A., Pivonka, E. Overview of the health benefits of fruit and vegetable consumption for the dietetics professional: Selected literature. Journal of the American Dietetic Association. 2000;100(12):1511–1521.
Van, L.M., Herten. Gezonde levensverwachting naar sociaal-economische status. TNO Preventie en Gezondheid. 2002.
Van Lenthe, F.M., Mackenbach, J.P. Neighbourhood deprivation and overweight: The GLOBE study. International Journal of Obesity and Related Metabolic Disorders. 2002;26(2):234–240.
Vannoy, B.E. Relationships among basic conditioning factors, motivational dispositions, and the power element of self-care agency in people beginning a weight loss program. Wayne State University, 1989. Unpublished doctoral dissertation
Velsor-Friedrich, B., Pigott, T.D., Louloudes, A. The effects of a school-based intervention on the self-care and health of African-American inner-city children with asthma. Journal of Pediatric Nursing. 2004;19(4):247–256.
Velsor-Friedrich, B., Pigott, T., Srof, B. A practitioner-based asthma intervention program with African American inner-city school children. Journal of Pediatric Healthcare. 2005;19(3):163–171.
Villarruel, A.M. Mexican-American cultural meanings, expressions, self-care and dependent-care actions associated with experiences of pain. Research in Nursing & Health. 1995;18(5):427–436.
Walker, L.O., Avant, K.C. Strategies for theory construction in nursing, (3rd ed.). Norwalk, CT: Appleton & Lange; 2004.
Walsh, D., Rybicki, L. Symptom clustering in advanced cancer. Supportive Care in Cancer. 2006;14(8):831–836.
Wang, C.Y. The cross-cultural applicability of Orem’s conceptual framework. Journal of Cultural Diversity. 1997;4(2):44–48.
Wang, C.Y., Fenske, M.M. Self-care of adults with non-insulin-dependent diabetes mellitus: Influences of family and friends. Diabetes Educator. 1996;22(5):465–470.
Wang, H.H., Laffrey, S.C. A predictive model of well-being and self-care for rural elderly women in Taiwan. Research in Nursing & Health. 2001;24(2):122–132.
Wannamethee, S.G., Shaper, A.G., Alberti, K.G. Physical activity, metabolic factors, and the incidence of coronary heart disease and type 2 diabetes. Archives of Internal Medicine. 2000;160(14):2108–2116.
Wannapornsiri, C., Sindhu, S., Phancharoenworakul, K., Gasemgitvatana, S. Caring process of Thai women with breast cancer receiving chemotherapy. Thai Journal of Nursing Research. 2005;9(2):121–132.
Watson, R., Deary, I.J., Hoogbruin, A.L. A 35-item version of the caring dimensions inventory (CDI-35): Multivariate analysis and application to a longitudinal study involving student nurses. International Journal of Nursing Studies. 2001;38(2001):511–521.
Watson, R., Deary, I.J., Lea, A. A longitudinal study into the perceptions of caring among student nurses using multivariate analysis of the Caring Dimensions Inventory. Journal of Advanced Nursing. 1999;30(5):1080–1089.
Watson, R., Deary, I.J., Lea, A. A longitudinal study into the perceptions of caring and nursing among student nurses. Journal of Advanced Nursing. 1999;29(5):1228–1237.
Watson, R., Lea, A. The caring dimensions inventory (CDI): Content validity, reliability and scaling. Journal of Advanced Nursing. 1997;25(1):87–94.
Wattanawech, T., Srimoragot, P., Kasemkitwattana, S., Kimpee, S. Influence of selected factors and self-care behavior on abdominal distention in patients with abdominal surgery. Self-care, Dependent-Care & Nursing. 2003;11(3):19–32.
Weaver, M.T. Perceived self-care agency: A LISREL factor analysis of Bickel and Hanson’s questionnaire. Nursing Research. 1987;36(6):381–387.
Weber, N.A. Explication of the structure of the secondary concept of women’s self-care developed within Orem’s self-care deficit theory: Instrumentation, psychometric evaluation and theory-testing. Wayne State University, 2000. Unpublished doctoral dissertation
Weintraub, F.N., Hagopian, G.A. The effect of nursing consultation on anxiety, side effects, and self-care of patients receiving radiation therapy. Oncology Nursing Forum. 1990;17(3 Suppl):31–36.
White, M.A.M. Predictors of self-care agency among community-dwelling older adults. University of Alabama at Birmingham, 2000. Unpublished doctoral dissertation
Whittemore, R., Roy, C. Adapting to diabetes mellitus: A theory synthesis. Nursing Science Quarterly. 2002;15(4):311–317.
Wilde, M.H. The caring connection in nursing: A concept analysis. International Journal for Human Caring. 1997;1(1):18–24.
Wilde, M.H., Garvin, S. A concept analysis of self- monitoring. Journal of Advanced Nursing. 2007;57(3):339–350.
Wilkes, L.M., Wallis, M.C. A model of professional nurse caring: Nursing students’ experience. Journal of Advanced Nursing. 1998;27(3):582–589.
Wilkinson, J.R. What it means to care. Curationis. 1998;21(2):2–8.
Willard, G.A. Development of an instrument to measure the functional status of hospitalized patients. University of Texas at Austin, 1990. Unpublished doctoral dissertation
Williams, S.A., Schreier, A.M. The effect of education in managing side effects in women receiving chemotherapy for treatment of breast cancer. Oncology Nursing Forum. 2004;31(1):E16–E23.
Wilson, F.L., Brown, D.L., Stephens-Ferris, M. Can easy-to-read immunization information increase knowledge in urban low-income mothers? Journal of Pediatric Nursing. 2006;21(1):4–12.
Wolf, Z., Giardino, E., Osborne, P., Ambrose, M. Dimensions of nurse caring. Image: Journal of Nursing Scholarship. 1994;26(2):107–111.
Wolf, Z.R., Zuzelo, P.R., Costello, R., Cattilico, D., Cooper, K.A., Crothers, R., et al. Development and testing of the Caring Behaviors Inventory for Elders. International Journal for Human Caring. 2004;8(1):48–54.
Wuest, J. Concept development situated in the critical paradigm. In Concept development in nursing: Foundations, techniques, and applications, (2nd ed.), Philadelphia: W.B. Saunders; 2000:369–387.
Yonge, O., Molzahn, A. Exceptional nontraditional caring practices of nurses. Scandinavian Journal of Caring Sciences. 2002;16(4):399–405.
Zrinyi, M., Rimar, I. The effect of nursing intervention on the patient’s self-care capability, between hospital admission and release. [Hungarian]. Nover. 2005;18(4):3–11.
Zrinyi, M., Zekanyne, R.I. Does self-care agency change between hospital admission and discharge? An Orem-based investigation. International Nursing Review. 2007;54(3):256–262.