Chapter 27 Differential diagnosis of radiolucent lesions of the jaws
INTRODUCTION
This chapter is designed to simplify the process of arriving at a radiological differential diagnosis when confronted with a radiolucency of unknown cause on a plain radiograph. This process requires clinicians to follow a methodical step-by-step approach and to know the typical features of the various possibilities. Such a step-by-step guide is suggested and summarized in Figure 27.1. Although most lesions are still detected using plain radiographs, this process can be greatly facilitated in many cases if advanced imaging modalities, described in Chapter 19, such as computed tomography (CT), cone beam CT or magnetic resonance (MR) are available.
Unfortunately, most of the lesions encountered share several similar features and often individual conditions can present in many different ways. Thus the summary of features for the more important conditions included in this chapter is an attempt to unravel some of the inevitable confusion. Also, for simplicity, the frequency with which the various lesions present has been divided arbitrarily into common, uncommon and rare. It is hoped and intended, that the reader should expand on this short-notes style framework by referring to the suggested reading list.
Step-by-step guide
Step II
Step III
If the pathological radiolucency is acquired, decide within which of the following main disease categories it may be placed:
Step IV
Consider the classification and subdivision of cysts and other similar radiolucencies within each of the other main disease categories, as shown in Table 27.1. This resultant list includes most of the more likely diagnostic possibilities for the unknown radiolucent lesion.
Table 27.1 Classification of the main cysts and tumours and other bone-related conditions that can present as a cyst-like radiolucency (based broadly on the 2005 WHO Classification)
| Cysts | |
| Odontogenic | |
| Non-odontogenic | |
| Tumours and tumour-like lesions | |
| Benign odontogenic (epithelial with mature, fibrous stroma without odontogenic ectomesenchyme) | |
| Benign odontogenic (epithelial with odontogenic ectomesenchyme, with or without hard tissue formation) | |
| Benign odontogenic (Mesenchymal and/or odontogenic ectomesenchyme with or witout odontogenic epithelium) | |
| Malignant odontogenic | |
| Non-odontogenic intrinsic primary bone tumours | |
| Extrinsic primary tumours involving bone Secondary metastatic bone tumours Lymphoreticular tumours of bone | |
| Langerhans cell disease (Histiocystosis X) | |
| Bone-related lesions | |
| Giant cell lesions | |
| Osseous dysplasias (Fibro-cemento-osseous lesions) (early stages) | |
| Other lesions | |
Step V
Compare the radiological features of the unknown radiolucency with the typical radiological features of these possible conditions. Then construct a list showing, in order of likelihood, all the conditions that the lesion might be. This list forms the radiological differential diagnosis.
Infection is described elsewhere (apical, Ch. 22, spreading, Ch. 32) and trauma is described in Chapter 30. The rest of this chapter is devoted principally to differentiating between the different cysts — the most common of the remaining categories — and the other lesions which often present as very similar radiolucencies.
TYPICAL RADIOGRAPHIC FEATURES OF CYSTS
Inflammatory odontogenic cysts
Radicular (dental) cyst (Fig. 27.2)
This inflammatory cyst develops from the epithelial remnants of Hertwig’s root sheath — the cell rests of Malassez.
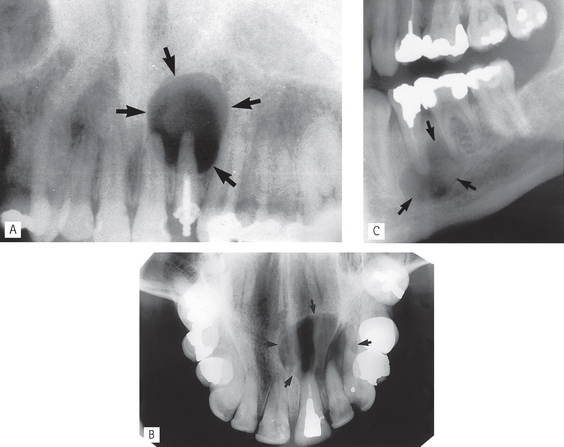
Fig. 27.2 A Static panoramic (Panoral) radiograph showing a typical radicular (dental) cyst (arrowed) associated with the non-vital  . B Upper standard occlusal showing a large radicular cyst associated with the root-filled
. B Upper standard occlusal showing a large radicular cyst associated with the root-filled  . C Part of a panoramic radiograph showing a typical unilocular radicular cyst associated with the non-vital
. C Part of a panoramic radiograph showing a typical unilocular radicular cyst associated with the non-vital  .
.
• Age: Usually adults, 20–50 year-olds.
• Frequency: Most common of all jaw cysts (about 70%).
• Site: Apex of any non-vital tooth, particularly upper lateral incisors.
• Size: 1.5–3 cm in diameter (if smaller the radiographic distinction between cyst and granuloma cannot usually be made).
Note: The term buccal bifurcation cyst is used to describe an inflammatory odontogenic cyst which develops on the side of a molar tooth in relation to a buccal enamel spur or pearl.
Residual radicular cyst (Fig. 27.3)
This term refers to a radicular (dental) cyst remaining after the causative tooth has been extracted.

Fig. 27.3 Part of a panoramic radiograph showing two residual radicular cysts (arrowed), one in the maxilla and one in the mandible.
Developmental odontogenic cysts
Lateral periodontal cyst (Fig. 27.4)
The diagnosis of this rare developmental cyst should be reserved for a cyst in the lateral periodontal region that is not an inflammatory cyst or an atypical odontogenic keratocyst. It is thought to develop from either the cell rests of the dental lamina or from remains of the reduced enamel epithelium on the lateral surface of the root.

Fig. 27.4 Periapical showing a typically small lateral periodontal cyst (arrowed) between the  and
and  . Although the adjacent premolar was restored, it was vital and symptom free.
. Although the adjacent premolar was restored, it was vital and symptom free.
(Kindly provided by Mr N. Drage.)
• Age: Adults over 30 years old.
• Site: Lateral surface of the roots of vital teeth in the lower canine/premolar region or upper lateral incisor region.
• Size: Small, less than 1cm in diameter.
• Shape: — Unilocular, very occasionally multilocular
• Radiodensity: Uniformly radiolucent.
• Effects: — Adjacent teeth — displaced if cyst becomes large, rarely resorbed
Dentigerous (follicular) cyst (Fig. 27.5)
This cyst develops from the remnants of the reduced enamel epithelium after the tooth has formed.
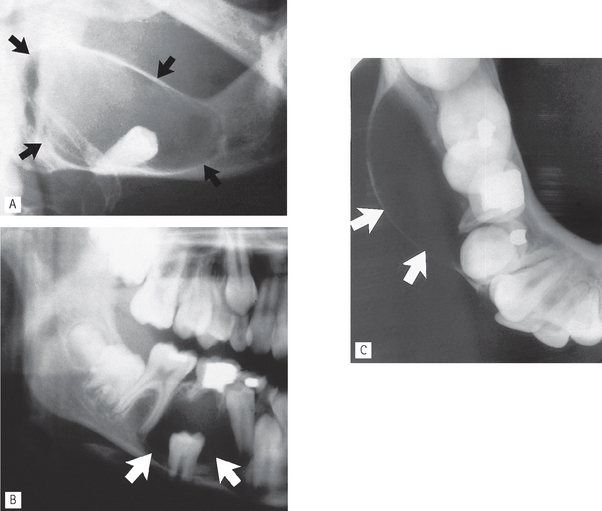
Fig. 27.5 A Oblique lateral of the right side of the mandible showing a typical circumferential dentigerous cyst (arrowed) associated with the unerupted and displaced  . B Part of a panoramic radiograph showing a unilocular central dentigerous cyst (arrowed) associated with the unerupted and inferiorly displaced
. B Part of a panoramic radiograph showing a unilocular central dentigerous cyst (arrowed) associated with the unerupted and inferiorly displaced  . C Right side of a lower 90° occlusal of the same patient showing the typical buccal expansion (arrowed).
. C Right side of a lower 90° occlusal of the same patient showing the typical buccal expansion (arrowed).
• Age: Usually adolescents or young adults, 20–40 year-olds, occasionally the elderly.
• Frequency: About 20% of all cysts.
• Site: Associated with the crown of an unerupted and displaced tooth, typically teeth where eruption is impeded, e.g.  and
and  .
.
• Size: Very variable, cyst suspected if follicular space exceeds 3 mm but may grow to several centimetres in diameter and extend up into the ramus.
• Shape: — Round or oval, typically enveloping the crown symmetrically
Note: The term eruption cyst is used to describe a dentigerous cyst when it is in the soft tissues overlying the unerupted tooth.
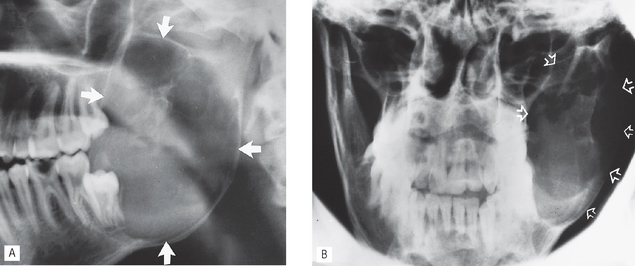
Odontogenic keratocyst (keratocystic odontogenic tumour) (Fig. 27.6)
Somewhat controversially in 2005 the WHO Working Group recommended that the odontogenic keratocyst be renamed the keratocystic odontogenic tumour as they felt this name better reflected its neoplastic nature. The WHO now define this lesion as a benign uni- or multicystic intraosseous tumour of odontogenic origin with a histologically characteristic lining of parakeratinized stratified squamous epithelium with a potentially aggressive, infiltrative behaviour. It is believed to develop from the epithelium of the dental lamina — the cell rests of Serres — instead of the normal tooth which is therefore typically missing from the series. Lesions are typically solitary but multiple odontogenic keratocysts are a feature of nevoid basal cell carcinoma syndrome (Gorlin’s syndrome), which also includes multiple basal cell carcinomas, and skeletal anomalies, e.g. bifid ribs and calcification of the falx cerebri.
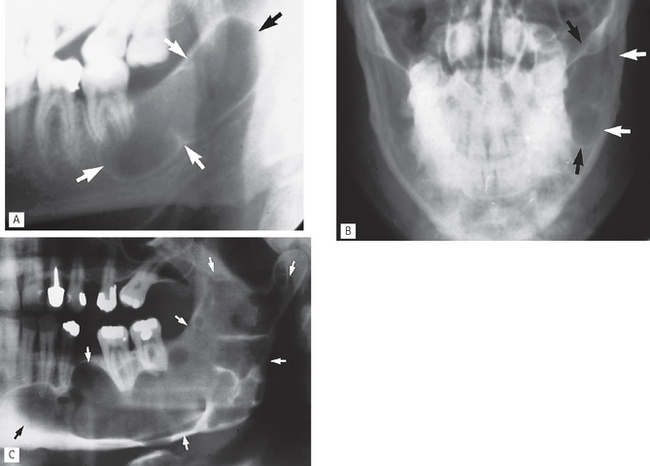
Fig. 27.6 A Oblique lateral of the left side of the mandible showing a typically extensive pseudolocular odontogenic keratocyst (arrowed) which has apparently developed instead of  . B PA jaws of the same patient showing that it has caused minimal mediolateral expansion (arrowed). CLeft side of a panoramic radiograph showing a very large multilocular odontogenic keratocyst (arrowed) occupying almost all the left side of the mandible.
. B PA jaws of the same patient showing that it has caused minimal mediolateral expansion (arrowed). CLeft side of a panoramic radiograph showing a very large multilocular odontogenic keratocyst (arrowed) occupying almost all the left side of the mandible.
• Age: Very variable, peak incidence between second and third decades.
• Site: — Posterior body/angle of the mandible extending into the ramus
• Size: Variable, but often large in the mandible.
• Shape: — Oval, extending along the body of the mandible with little mediolateral expansion
• Outline: — Smooth and scalloped
• Radiodensity: Uniformly radiolucent.
• Effects: — Adjacent teeth — minimal displacement, rarely resorbed
 . by enfolding so resembling a dentigerous cyst.
. by enfolding so resembling a dentigerous cyst.Non-odontogenic cysts
Nasopalatine duct / incisive canal cyst (Fig. 27.7)
This cyst develops from epithelial remnants of the nasopalatine duct or incisive canal.
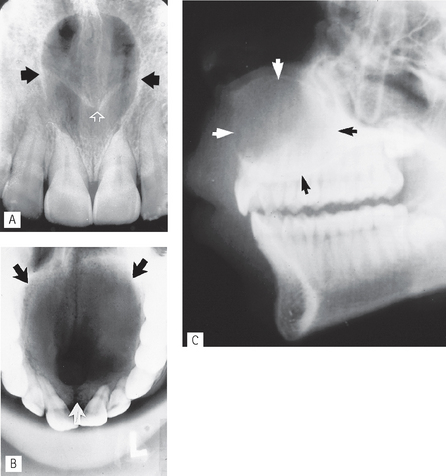
Fig. 27.7 A Periapical showing a typical nasopalatine duct cyst (solid arrows) in the midline between the upper central incisors. Note the superimposed shadow of the anterior nasal spine (open white arrows). B Upper occlusal showing a very extensive nasopalatine duct cyst (arrowed) occupying nearly the entire palate. C Lateral view of the same patient showing the expansion of the cyst into the nasal cavity and palate (arrowed).
• Age: Variable, but most frequently detected in middle age (40–60 year-olds).
• Frequency: Most common of all non-odontogenic cysts, affecting about 1% of total population.
• Site: Midline, anterior maxilla just posterior to the upper central incisors.
• Size: Variable, but usually from 6 mm to several centimetres in diameter.
• Shape: — Round or oval (superimposition of the nasal septum or anterior nasal spine may cause the cyst to appear heart-shaped or resemble an inverted tear drop)
• Radiodensity: Uniformly radiolucent but radiopaque shadows sometimes superimposed.
• Effects: — Adjacent teeth — distal displacement, rarely resorbed
Note: Differentiation is sometimes required between a nasopalatine duct cyst and a large normal nasopalatine foramen. Several features need to be considered including:
Bone cysts or pseudocysts
Despite their names — simple bone cyst and aneurymal bone cyst — these entities are no longer categorized as cysts. In the new WHO Classification they come under the heading of bone-related lesions. They more commonly affect the skeleton and only relatively rarely affect the jaws.
Simple (solitary) bone cyst (Fig. 27.8)
Defined as an intra-osseous pseudocyst, devoid of an epithelial lining and either empty or filled with serous or sanguinous fluid. The aetiology is unknown.
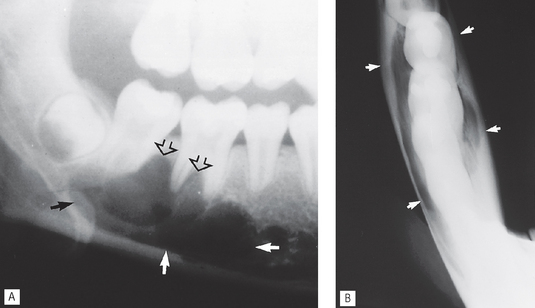
Fig. 27.8 A Oblique lateral of the right side of the mandible of a teenager showing a typical solitary bone cyst (solid arrows) in the body of the mandible. Note the upper border arching up between the roots of the molar teeth (open arrows). B Oblique lower occlusal of the same patient showing no apparent buccolingual expansion (arrowed).
• Age: Children or young adults, peak incidence in second decade.
• Site: — Mandible, particularly anteriorly and in the premolar/molar region.
• Size: Variable, up to several centimetres in diameter.
• Outline: — Smooth and undulating
• Radiodensity: Uniformly radiolucent.
• Effects: — Adjacent teeth — minimal or no displacement, very rarely resorbed
Aneurysmal bone cyst (see Fig. 27.21)
This rare lesion is defined as an expansile osteolytic lesion, often multilocular with histologically blood filled spaces separated by fibrous septa containing osteoclast type giant cells and reactive bone. It is categorized as a giant cell lesion and described later.
 . B PA jaws of the same patient showing ballooning expansion (arrowed).
. B PA jaws of the same patient showing ballooning expansion (arrowed).TYPICAL RADIOGRAPHIC FEATURES OF TUMOURS AND TUMOUR-LIKE LESIONS
Odontogenic tumours
Ameloblastoma (Fig. 27.9)
An aggressive but non-metastasizing tumour originating from remnants of the odontogenic epithelium of the enamel organ or dental lamina. Four main types include:
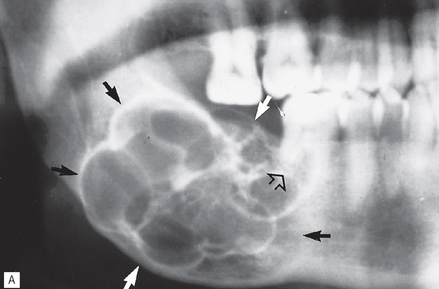
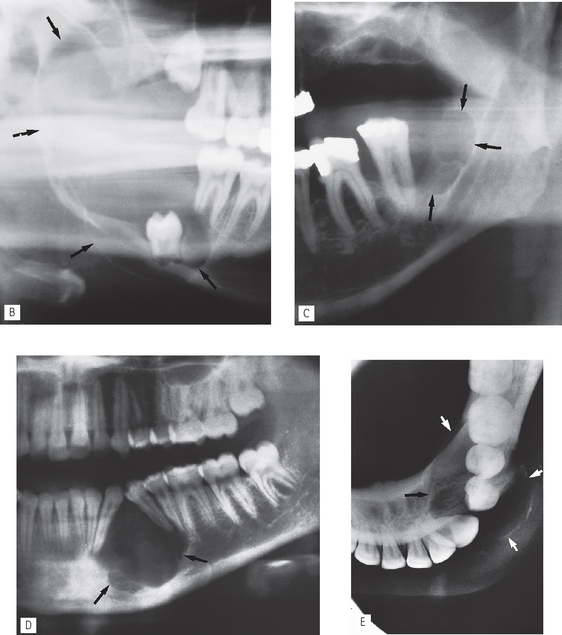
Fig. 27.9 A Part of a panoramic radiograph showing the typical multilocular appearance of a large ameloblastoma at the angle of the mandible, with extensive expansion (solid arrows) and resorption of adjacent teeth (open arrow).
B Right side of a panoramic radiograph showing a very extensive ameloblastoma (arrowed) with a less multilocular appearance but still causing considerable expansion and displacement of  . C Left side of a panoramic radiograph showing bilocular ameloblastoma (arrowed) distal to the molar. D Part of a panoramic radiograph showing an ameloblastoma in a more unusual anterior position causing displacement of the adjacent teeth. E Lower occlusal of the same patient showing the bucolingual extent of the lesion (arrowed).
. C Left side of a panoramic radiograph showing bilocular ameloblastoma (arrowed) distal to the molar. D Part of a panoramic radiograph showing an ameloblastoma in a more unusual anterior position causing displacement of the adjacent teeth. E Lower occlusal of the same patient showing the bucolingual extent of the lesion (arrowed).
Solid/multicystic ameloblastoma
• Age: Adults 30–60 years old.
• Frequency: Rare, but still the most common odontogenic tumour.
• Site: — 80% posterior body/angle/ramus of mandible
• Size: Very variable depending on the age of the lesion, may become very large if neglected and cause gross facial asymmetry.
• Shape: — Multilocular, distinct septa dividing the lesion into compartments with large, apparently discrete areas centrally and with smaller areas on the periphery
• Outline: — Smooth and scalloped
• Radiodensity: Radiolucent with internal radiopaque septa.
• Effects: — Adjacent teeth displaced, loosened, often resorbed
Unicystic ameloblastoma
Accounts for 5–15% of all ameloblastomas and is found equally in the mandible and the maxilla. It usually presents as a unilocular radiolucency associated with the crown of an unerupted tooth (peak age: 16 years), or as a unilocular radiolucency at the apices of teeth, resembling a radicular cyst (peak age: 35 years).
Note: Since different ameloblastomas can mimic a large variety of other radiolucent lesions, this possibility must always be borne in mind when formulating a radiological differential diagnosis.
Ameloblastic fibroma (Fig. 27.10)
A rare, benign, mixed odontogenic tumour originating from both the odontogenic epithelium and the connective tissue of the developing tooth germ. Histologically, it consists of odontogenic ectomesenchyme resembling dental papilla and epithelial strands and rests resembling dental lamina and enamel organ. Radiographically these tumours closely resemble ameloblastomas but develop in a younger age group.
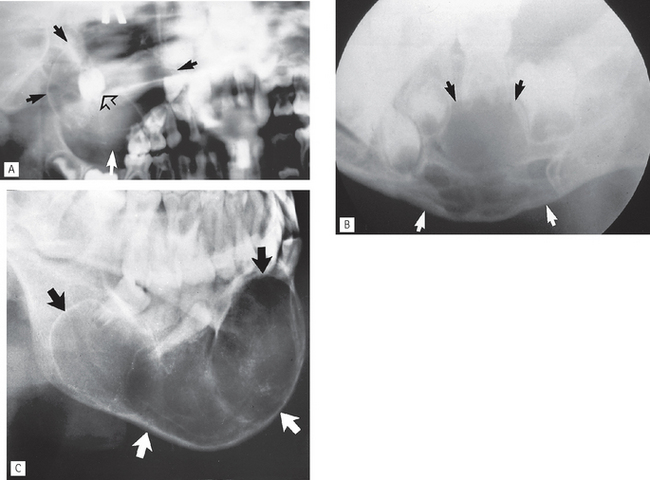
Fig. 27.10 A Part of a panoramic radiograph of a 4-year-old showing a large ameloblastic fibroma in the right maxilla, causing marked expansion (solid arrows) and displacement of the developing first molar (open arrow). B Oblique lateral of another small child showing a multilocular ameloblastic fibroma (arrowed) in the left body of the mandible causing displacement of the developing premolars and expansion of the lower border.
C Oblique lateral showing a very extensive ameloblastic fibroma (arrowed) of the right side in a 17-year-old.
(Kindly provided by Mrs J. E. Brown.)
Other epithelial odontogenic tumours
The other more important epithelial odontogenic tumours, with or without odontogenic ectomesenchyme, that can present as a radiolucency include:
• Calcifying epithelial odontogenic tumour (CEOT) or Pindborg tumour
• Adenomatoid odontogenic tumour (AOT)
• Calcifying cystic odontogenic tumour (calcifying odontogenic cyst).
However, as the name of a couple of them suggests, these lesions often develop internal calcifications and more typically present as lesions of variable radiopacity. They are therefore described in detail with appropriate examples in Chapter 28. A brief summary of each is outlined below.
Calcifying epithelial odontogenic tumour (CEOT), Pindborg tumour
This rare odontogenic tumour usually presents in the premolar/molar region of the mandible in 20–60 year-old adults. They can be either unilocular or multilocular, but tend to remain relatively small although they can cause expansion of surrounding cortical bone. They are often associated with an unerupted tooth particularly  . The outline of the lesion tends to be of variable definition and cortication but is frequently scalloped. They are often radiolucent in their early stages; then numerous scattered radiopacities usually become evident within the lesion, often most prominent around the crown of any associated unerupted tooth. This appearance is sometimes described as driven snow. Adjacent teeth can be either displaced and/or resorbed (see Fig. 28.8).
. The outline of the lesion tends to be of variable definition and cortication but is frequently scalloped. They are often radiolucent in their early stages; then numerous scattered radiopacities usually become evident within the lesion, often most prominent around the crown of any associated unerupted tooth. This appearance is sometimes described as driven snow. Adjacent teeth can be either displaced and/or resorbed (see Fig. 28.8).
Ameloblastic fibro-odontoma
These rare, unilocular or multilocular odontogenic tumours resemble closely ameloblastic fibromas (see Fig. 27.10), and also affect children. However, they are often associated with an unerupted tooth and usually contain enamel or dentine, either as multiple small opacities or as a solid mass (see Fig. 28.9).
Adenomatoid odontogenic tumour (AOT)
Another rare odontogenic tumour, but unusually the most frequent site affected, is the anterior maxilla in the incisor/canine region. Young adults are usually affected. The lesion tends to be unilocular, round or oval, and often surrounds an entire unerupted tooth. When radiolucent in their early stages, they can closely resemble a dentigerous cyst. However, as the lesion matures, small opacities (snowflakes) within the central radiolucency may be seen peripherally. Adjacent teeth are often displaced as the lesion expands but are rarely resorbed (see Fig. 28.10).
Calcifying cystic odontogenic tumour (calcifying odontogenic cyst or Gorlin’s cyst)
The new name of this lesion reflects its classification by the WHO as an odontogenic tumour. It presents typically anteriorly in either the mandible or the maxilla as a unilocular, well-defined, well-corticated radiolucency resembling any other odontogenic cyst. It can affect any age group having been reported in patients from 5–92 years old. One third of cases are associated with an unerupted tooth or odontome. As the lesion matures, a variable amount of calcified material, of tooth-like density, becomes evident scattered throughout the radiolucency. The opacities can range from small flecks to large masses. Adjacent teeth are usually displaced and/or resorbed (see Fig. 28.11).
Odontogenic fibroma (Fig. 27.11)
Controversy still exists as to the concept and definition of the odontogenic fibroma as a distinct lesion. The WHO classify it separately and describe it as a rare neoplasm characterized histologically by varying amounts of inactive looking odontogenic epithelium embedded in a mature fibrous stroma. Two sub-types are described, thought to develop from different parts of the tooth germ:
• Epithelium-poor originating from the dental follicle
• Epithelium-rich originating from the periodontal ligament.
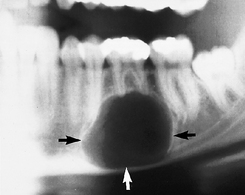
Fig. 27.11 Part of a panoramic radiograph showing a round, unilocular, well-defined radiolucency (arrowed) at the apex of  which was clinically vital. Histopathology confirmed an odontogenic fibroma.
which was clinically vital. Histopathology confirmed an odontogenic fibroma.
Typically lesions present as cyst-like well defined, unilocular radiolucencies with dense corticated margin. Rarely calcified material may develop internally and adjacent teeth may be displaced.
Odontogenic myxoma (Fig. 27.12)
An intra-osseous neoplasm characterized histologically by stellate and spindle-shaped cells embedded in an abundant myxoid or mucoid extracellular matrix originating from the odontogenic connective tissue fibroblasts of the developing tooth germ.
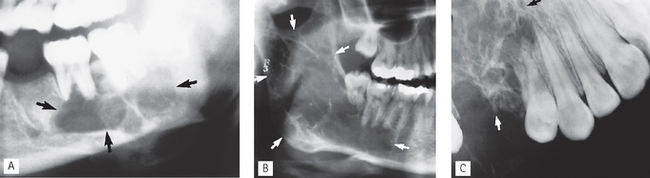
Fig. 27.12 A Left side of a panoramic radiograph showing the typical multilocular appearance of an odontogein myxoma (arrowed) in the body of the mandible. B Right side of a panoramic radiograph showing an extensive odontogenic myxoma (arrowed) with final internal septa. C Part of an upper oblique occusal showing a multilocular almost honeycomb appearance of an odontogenic myxoma (arrowed) in the maxilla.
• Age: Young adults — most diagnosed in the 2nd–4th decades.
• Frequency: Rare, but the third most common odontogenic tumour.
• Site: Posterior mandible or posterior maxilla.
• Size: Variable, but may become very large if untreated.
• Shape:—Multilocular (honeycomb or soap-bubble)
• Outline: — Smooth and often scalloped
• Radiodensity: Radiolucent with fine internal radiopaque septa or trabeculae often arranged at right angles to one another, producing an appearance sometimes described as resembling the strings of a tennis racket or the letters X and Y.
• Effects:—Adjacent teeth displaced and loosened, occasionally resorbed
Radiolucent non-odontogenic tumours
Intrinsic primary benign bone tumours
Central haemangioma (Fig. 27.13)
This is a rare, benign tumour that occasionally affects the jaws, particularly the mandible. It is usually regarded as a developmental malformation (hamartoma) of the blood vessels in the marrow spaces, rather than a true neoplasm.
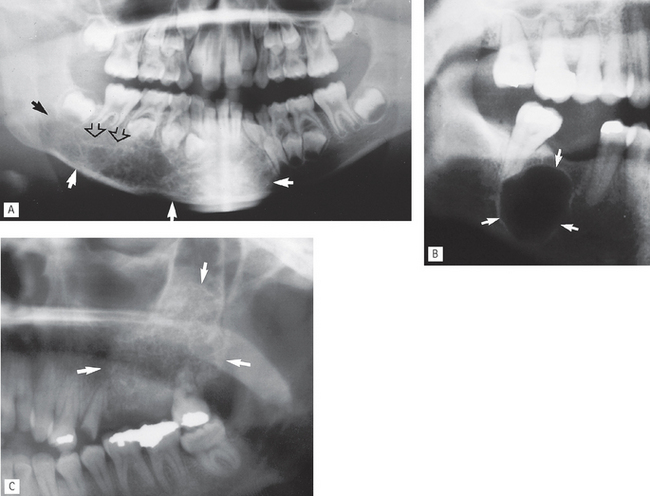
Fig. 27.13 A Part of a panoramic radiograph of an 8-year-old showing a large central haemangioma occupying most of the body of the mandible (solid arrows). The typical honeycomb appearance is evident on the right (open arrows) and there is evidence of root resorption. B Part of a panoramic radiograph showing a unilocular cyst-like haemangioma (arrowed). These two examples highlight the very variable appearance of this important lesion. C Left side of a panoramic radiograph showing the multilocular honeycomb appearance of a large haemangioma in the posterior maxilla (arrowed).
(Kindly provided by Mr K. Hussain.)
Central haemangioma can present at any age but is usually discovered in adolescents. It can produce a very variable radiographic appearance. These variations are important because of the life-threatening nature of the lesion; they include:
• Most commonly a multilocular, expanding lesion which may be associated with displacement and resorption of associated teeth. The size and number of locules can vary considerably, and, if numerous, can present with a honeycomb appearance.
• A moderately well-defined zone of radiolucency within which the trabecular spaces are enlarged and the trabeculae themselves are coarse and thick and are said to be arranged like a hub or the spokes of a wheel.
• Rarely, a relatively well-defined, round, cyst-like radiolucency — not distinctive in any way.
• Large lesions may cause cortical expansion, occasionally producing the sunray or sunburst appearance.
Intrinsic primary malignant bone tumours
Osteosarcoma (Fig. 27.14)
Rare, rapidly destructive malignant tumour of bone. From a radiological viewpoint, there are three main types:
• Osteolytic — no neoplastic bone formation.
• Osteosclerotic — neoplastic osteoid and bone formed.
• Mixed lytic and sclerotic — patches of neoplastic bone formed.
• Age: Young adults under 30 years old.
• Frequency: Rare, but the most common primary malignant bone tumour.
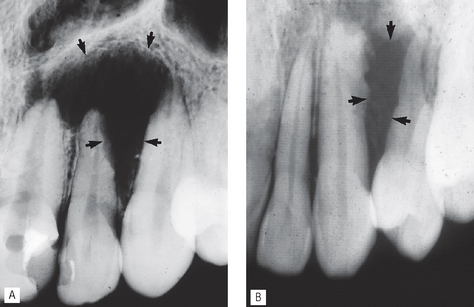
Fig. 27.14 A Periapical of  showing a poorly defined ragged area of radiolucency (arrowed) with resorption of the lateral aspect of
showing a poorly defined ragged area of radiolucency (arrowed) with resorption of the lateral aspect of  root. Biposy revealed an osteolytic osteosarcoma. B Periapical showing a similar smaller poorly defined area of bone destruction between
root. Biposy revealed an osteolytic osteosarcoma. B Periapical showing a similar smaller poorly defined area of bone destruction between  (arrowed) which was again shown to be an osteosarcoma.
(arrowed) which was again shown to be an osteosarcoma.
Later features:
• Osteosclerotic and mixed lesions:
Extrinsic primary malignant tumours involving bone
Squamous cell carcinoma (Fig. 27.15)
Squamous cell carcinomas of the oral mucosa directly overlying bone, in their latter stages, often invade the underlying bone to produce a destructive radiolucency.
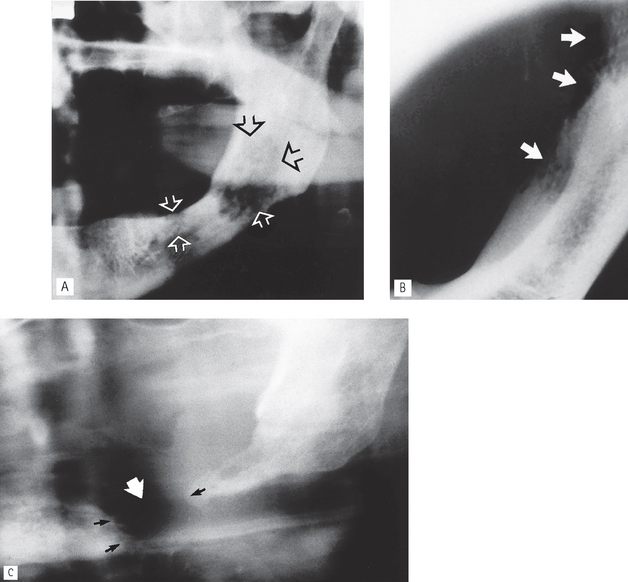
Fig. 27.15 A Part of a panoramic radiograph of a patient who presented with a large squamous cell carcinoma on the left ventral surface of his tongue and the floor of his mouth. The radiograph shows two areas of poorly defined radiolucency (arrowed) with a ragged or moth-eaten appearance. B Left side of a lower 90° occlusal of the same patient showing the bony destruction (arrowed) of the lingual surface of the mandible as the soft tissue tumour invades the bone. C Part of a panoramic radiograph of another patient who presented with a very large squamous cell carcinoma of the floor of the mouth that had penetrated through the mandible (white arrow) causing a pathological fracture. The ragged bone edges are marked with the black arrows.
• Age: Adults over 50 years old.
• Frequency: Rare, but the most common oral malignant tumour.
• Site: Mandible, or maxilla if originating in the antrum.
• Shape: Irregular area of bone destruction often initially saucer-shaped.
• Outline: — Irregular and moth-eaten
• Radiodensity: Radiolucent, radiodensity dependent on degree of destruction.
• Effects: — Adjacent teeth may be displaced, loosened and/or resorbed or left floating in space
Secondary (metastatic) bone tumours (Fig. 27.16)
Carcinomas from the bronchus, breast, prostate, kidney and thyroid sometimes metastasize to the jaws and produce the typical destructive radiolucency of a malignant lesion (see Ch. 22).
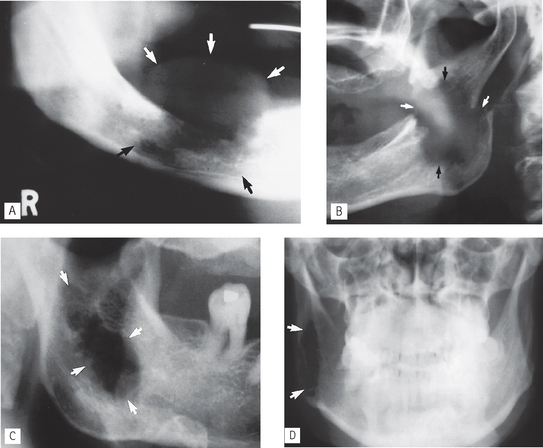
Fig. 27.16 A Right side of a panoramic radiograph showing the typical destructive, moth-eaten radiolucency of a malignant lesion (black arrows). Overlying soft tissue involvement is also evident (white arrows). Subsequent investigation showed this to be a secondary metastatic tumour from the breast. B Left side of a panoramic radiograph showing a large irregular destructive secondary metastatic tumour in the ascending ramus (black arrows). There is an associated pathological fracture (white arrows). C Left side of a panoramic radiograph and D PA jaws of the same patient showing a poorly defined radiolucent secondary metastastic deposit, from the lung, presenting centrally in the ramus (arrowed).
• Age: Adults over 40 years old.
• Frequency: Rare, but the second most common malignant tumours of the jaws.
• Site: Usually centrally in the mandible, molar and premolar regions, occasionally at the apex of a tooth.
• Size: Variable, dependent on the length of time the lesion has been present.
• Shape: Irregular area or areas of bone destruction.
• Outline: — Irregular and moth-eaten
• Radiodensity: Radiolucent, but some carcinomas from the prostate and breast may be osteogenic and show areas of bone production/ sclerosis.
• Effects: — Adjacent teeth may be displaced, loosened and/or resorbed
Note: The radiographic appearance, while strongly indicating a destructive malignant lesion, does not enable the distinction between a primary or secondary tumour to be made.
Lymphoreticular tumours of bone (Fig. 27.17)
Multiple myeloma (Fig. 27.17)
Multifocal proliferation of the plasma cell series within the bone marrow, resulting in overproduction of immunoglobulins.
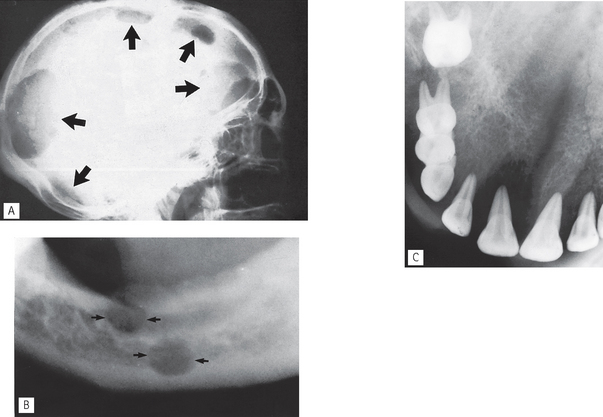
Fig. 27.17 A True lateral skull showing the typical multiple punched-out lesions (arrowed) of the skull vault of multiple myeloma. B Oblique lateral of the left side showing two similar lesions in the mandible (arrowed). C Upper oblique occlusal showing the typical appearance of destructive malignancy of Burkitt’s lymphoma. Almost all normal anatomical structures have been destroyed.
Others
• Large cell (anaplastic) lymphoma — adults under 40 years
• Burkitt’s (African) lymphoma — children (see Fig. 27.17C)
These lymphoreticular tumours are rare and apart from the age group predilection (shown above), they present in a similar, relatively non-specific manner. Radiographically they usually present as expansile, destructive, poorly defined, radiolucent areas — suggestive of malignant disease.
Langerhans cell disease (histiocytosis X)
Langerhans cell disease is used as a broad grouping of three different clinical manifestations of the same disease. All three manifestations produce tumour-like lesions in bone, caused by proliferation of Langerhans cells and eosinophilic leucocytes:
• Solitary eosinophilic granuloma — localized to the skeleton, affecting adolescents and young adults (see Fig. 27.18)
• Multifocal eosinophilic granuloma (Hand– Schüller–Christian disease) — chronic and wide-spread, begins in childhood but may not be fully developed until early adulthood, 20–30 years
• Letterer–Siwe disease — acute or subacute and widespread, affecting children under three years old.
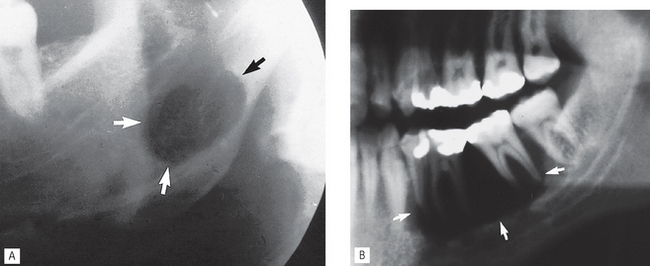
Fig. 27.18 A Oblique lateral of the left side of the mandible showing a well-defined, unilocular, punched-out, radiolucency (arrowed) beneath the inferior dental canal and therefore non-odontogenic, which proved to be an eosinophilic granuloma. B Left side of a panoramic radiograph showing an extensive punched-out destructive eosinophilic granuloma (arrowed) causing the  to appear to be floating in space.
to appear to be floating in space.
(Kindly provided by Dr J. Luker.)
Radiographically, the bone lesions (in whatever parts of the skeleton are affected) are similar in all three diseases.
• Site: Multiple lesions (in multifocal eosinophilic granuloma and Letterer–Siwe disease only) throughout the skeleton, occasionally solitary lesion, affecting:
• Size: Small, 1–2cm in diameter.
• Effects: — Adjacent teeth — not resorbed, but the periodontal bone support is sometimes destroyed so that they appear to be floating or standing in space
TYPICAL RADIOGRAPHIC FEATURES OF BONE-RELATED LESIONS
Giant cell lesions
Central giant cell lesion (granuloma) (Fig. 27.19)
A relatively rare lozalized, benign but sometimes aggressive osteolytic proliferation consisting histiologically of fibrous tissue with haemorrhage and haemosiderin deposits, presence of osteoclast- like giant cells and reactive bone formation producing an expansile radiolucent lesion.
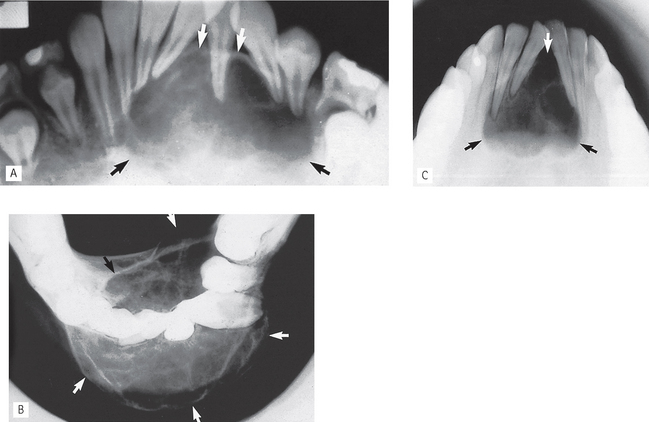
Fig. 27.19 Typical appearance of central giant cell lesion. A Anterior portion of a static panoramic showing the multilocular appearance, expansion (arrowed) and considerable displacement of the adjacent teeth. B Lower 90° occlusal showing the gross buccal and lingual expansion (arrowed) and the scalloped cortical border. C Lower 45° occlusal of another patient showing the appearance of a similar but much smaller central giant cell lesion (arrowed).
• Age: All ages can be affected but usually young adolescents and adults under 30 years old. One third of cases reported in patients under 20.
• Site: Mandible — all parts particularly premolar/molar region and anteriorly often crossing the midline.
• Shape: Multilocular, may be unilocular in early stages.
• Outline: — Smooth and scalloped
• Radiodensity: Radiolucent, larger lesions have thin internal septa or trabeculae producing the multilocular, or sometimes honeycomb appearance.
• Effects: — Adjacent teeth often displaced, sometimes resorbed
Based on their clinical and radiological effects on adjacent structures, central giant cell lesions are sometimes subdivided into two categories:
Brown tumours in hyperparathyroidism
The general radiological features of hyperparathyroidism are discussed in detail in Chapter 32. A few patients with this disease, in addition to the generalized decrease in bone density, also develop circumscribed, cyst-like radiolucencies. Histologically and radiologically these individual lesions (so-called brown tumours) are indistinguishable from central giant cell lesions (see earlier).
Cherubism (Fig. 27.20)
This rare disease of the jaws is inherited, usually as an autosomal dominant, but some cases appear spontaneously. Radiologically the lesions resemble closely other giant cell-containing lesions.
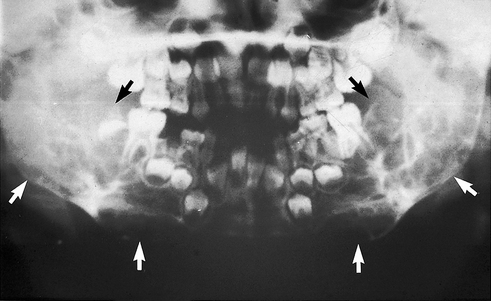
Fig. 27.20 Panoramic radiograph of a 5-year-old boy showing the typical bilateral multilocular lesions of cherubism affecting the mandible (arrowed).
• Age: Children, 2–6 years old.
• Site: — Angle/posterior mandible — bilateral
• Size: Variable, up to several centimetres in diameter, and may fill the whole jaw.
• Radiodensity: Radiolucent with internal radiopaque septa producing a multilocular appearance.
• Effects: — Adjacent teeth — gross displacement of deciduous and permanent teeth, occasionally resorbed, deciduous teeth sometimes exfoliated early
Aneurysmal bone cyst (Fig. 27.21)
As stated earlier, despite its name this rare lesion is categorized as a giant cell lesion and is defined as an expansile osteolytic lesion, often multilocular with histologically blood-filled spaces separated by fibrous septa containing osteoclast-type giant cells and reactive bone.
Bone-related lesions — osseous dysplasias
The 2005 WHO Classication, shown in Table 27.1, now categorizes fibro-cemento-osseous lesions as osseous dysplasias and includes four conditions:
They are all skeletal disorders in which bone is replaced by fibrous tissue which in turn is replaced by bone or mineralized tissue to a varying degree as the lesions age. Thus, in their early stages all the osseous dysplasias can present as cyst-like radiolucencies, although they are only sometimes seen clinically at this stage. It is more common to see them in their later stages when they present as mixed radiolucent/radiopaque lesions with varying degrees of opacity. Two radiolucent examples are shown here (Figs 27.22 and 27.23). The more radiopaque lesions are discussed and illustrated in Chapter 28.

Fig. 27.22 Periapicals of the lower incisors showing the early and intermediate stages of periapical osseous dysplasia. Several, small, discrete radiolucencies are evident at the apices. The more mature lesions at the apices  show evidence of internal calcification (open arrows).
show evidence of internal calcification (open arrows).
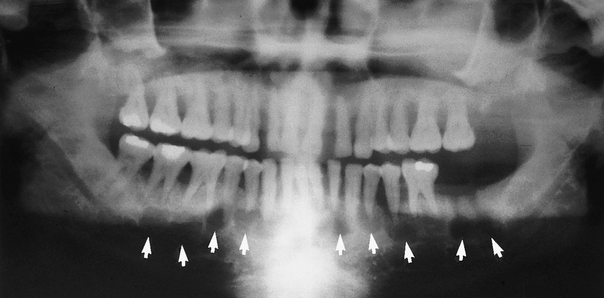
Fig. 27.23 Panoramic radiograph showing multiple radiolucent lesions (arrowed) in the mandible of early stage florid osseous dysplasia.
Periapical osseous dysplasia (Fig. 27.22)
• Age: Middle-aged adults (typically black women).
• Site: Apices of vital lower incisor teeth.
• Size: Small, usually only up to 5–6 mm in diameter.
• Outline: — Variable but usually poorly defined
• Radiodensity: — Early stage — radiolucent
• Effects: — Adjacent teeth — not displaced, not resorbed, typically vital, with intact periodontal ligament space, but lamina dura may be discontinuous
Florid osseous dysplasia (Fig. 27.23)
• Age: Middle-aged adults (typically black women).
• Site: Widespread, often in all four quadrants (dentulous and edentulous) but associated with the apices of the teeth if present.
• Size: Variable, but individual lesions up to 2 cm in diameter.
• Outline: — Smooth but lobular
• Radiodensity: — Early stage — multiple radiolucencies
• Effects: — Adjacent teeth — not displaced, not resorbed, typically vital
Other bone-related lesions
The other bone-related lesions that could present as a radiolucency include:
• Fibrous dysplasia (see Ch. 28 as more commonly mixed radiodensity)
• Ossifying fibroma (see Ch. 28 as more commonly mixed radiodensity)
Stafne’s bone cavity (Fig. 27.24)
A bone cavity or depression on the lingual aspect of the mandible near the lower border, frequently said to contain aberrant salivary gland tissue.

Fig. 27.24 Right side of a panoramic radiograph showing the typical cyst-like appearance of Stafne’s bone cavity at the angle of the mandible, below the inferior dental canal (arrowed).
FOOTNOTE
In view of this large number of radiolucent conditions, an ordered, systematic approach when producing a differential diagnosis is essential. Although the old adage that common things are commonly seen applies aptly to radiology, clinicians always have to be prepared for the possibility that they may be dealing with one of the rare, and perhaps sinister conditions.
For revision purposes, Table 27.2 summarizes those lesions which present typically as unilocular or multilocular radiolucencies.
Table 27.2 Summary of the main unilocular and multilocular radiolucent lesions
| Typically unilocular lesions | Typically multilocular or pseudolocular lesions |
|---|---|