Family Influences on Child Health Promotion

http://evolve.elsevier.com/Wong/NCIC

Adolescent Pregnancy, Ch. 17
Alternate Child Care Arrangements, Ch. 10
Communicating with Families, Ch. 6
History Taking and Physical Examination, Ch. 6
Impact of Chronic Illness or Disability on the Child, Ch. 22
Preschool and Kindergarten Experience, Ch. 15
Promote Parent-Infant Bonding (Attachment), Ch. 8
Sibling Rivalry, Ch. 12
General Concepts
The term family has been defined in many different ways according to the individual’s own frame of reference, values, or discipline. There is no universal definition of family; a family is what an individual considers it to be. Biology describes the family as fulfilling the biologic function of perpetuation of the species. Psychology emphasizes the interpersonal aspects of the family and its responsibility for personality development. Economics views the family as a productive unit providing for material needs. Sociology depicts the family as a social unit interacting with the larger society, creating the context within which cultural values and identity are formed. Others define family in terms of the relationships of the persons who make up the family unit. The most common type of relationships are consanguineous (blood relationships), affinal (marital relationships), and family of origin (family unit a person is born into).
Earlier definitions of family emphasized that family members were related by legal ties or genetic relationships and lived in the same household with specific roles. Later definitions have been broadened to reflect both structural and functional changes. A family can be defined as an institution where individuals, related through biology or enduring commitments, and representing similar or different generations and genders, participate in roles involving mutual socialization, nurturance, and emotional commitment (Hanson, Gedaly-Duff, and Kaakinen, 2005).
Considerable controversy has surrounded the newer concepts of family, such as communal families, single-parent families, and homosexual families. To accommodate these and other varieties of family styles, the descriptive term household is frequently used.
 NURSING ALERT
NURSING ALERT
The nurse’s knowledge and the sensitivity with which he or she assesses a household will determine the types of interventions that are appropriate to support family members.
Nursing care of infants and children is intimately involved with care of the child and the family. Family structure and dynamics can have an enduring influence on a child, affecting the child’s health and well-being (American Academy of Pediatrics, 2003). Consequently, nurses must be aware of the functions of the family, various types of family structures, and theories that provide a foundation for understanding the changes within a family and for directing family-oriented interventions.
Family Theories
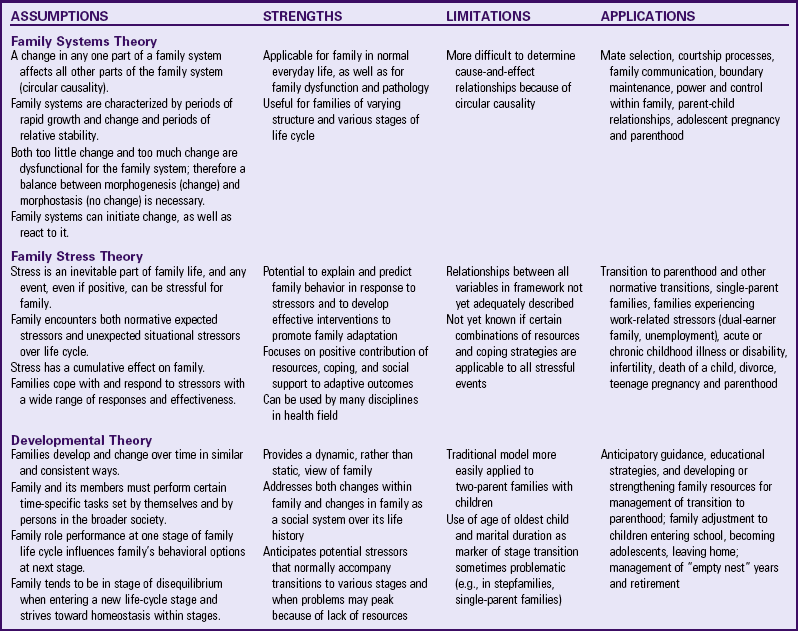
A family theory can be used to describe families and how the family unit responds to events both within and outside the family. Each family theory makes assumptions about the family and has inherent strengths and limitations (Hanson, Gedaly-Duff, and Kaakinen, 2005). Most nurses use a combination of theories in their work with children and families. Commonly used theories are family systems theory, family stress theory, and developmental theory (Table 3-1).
Family Systems Theory
Family systems theory is derived from general systems theory, a science of “wholeness” that is characterized by interaction among the components of the system and between the system and the environment (Bomar, 2004). General systems theory expanded scientific thought from a simplistic view of direct cause and effect (A causes B) to a more complex and interrelated theory (A influences B, but B also affects A). In family systems theory, the family is viewed as a system that continually interacts with its members and the environment. The emphasis is on the interaction between the members; a change in one family member creates a change in other members, which in turn results in a new change in the original member. Consequently, a problem or dysfunction does not lie in any one member but rather in the type of interactions used by the family. Because the interactions, not the individual members, are viewed as the source of the problem, the family becomes the patient and the focus of care. Examples of the application of family systems theory to clinical problems are nonorganic failure to thrive and child abuse. According to family systems theory, the problem does not rest solely with the parent or child but with the type of interactions between the parent and the child and the factors that affect their relationship.
The family is viewed as a whole that is different from the sum of the individual members. For example, a household of parents and one child consists of not only three individuals, but also four interactive units. These units include three dyads (the marital relationship, the mother-child relationship, and the father-child relationship) and a triangle (the mother-father-child relationship). In this ecologic model, the family system functions within a larger system, with the family dyads in the center of a circle surrounded by the extended family, the subculture, and the culture, with the larger society at the periphery.
Bowen’s family systems theory (Hanson, Gedaly-Duff, and Kaakinen, 2005) emphasizes that the key to healthy family function is the members’ ability to distinguish themselves from each other both emotionally and intellectually. The family unit has a high level of adaptability. When problems arise within the family, change occurs by altering the interaction or feedback messages that perpetuate disruptive behavior. Feedback refers to processes in the family that help identify strengths and needs and determine how well goals are accomplished. Positive feedback initiates change; negative feedback resists change (Goldenberg and Goldenberg, 2008). When the family system is disrupted, change can occur at any point in the system.
A major factor that influences a family’s adaptability is its boundary, an imaginary line that exists between the family and its environment (Hanson, Gedaly-Duff, and Kaakinen, 2005). Families have varying degrees of openness and closure in these boundaries. For example, one family has the capacity to reach out for help, whereas another considers help threatening. Knowledge of boundaries is critical when teaching or counseling families. Families with open boundaries may demonstrate a greater receptivity to interventions, whereas families demonstrating closed boundaries often require increased sensitivity and skill on the part of the nurse to gain their trust and acceptance. The nurse who uses family systems theory should assess the family’s ability to accept new ideas, information, resources, and opportunities and to plan strategies.
Family Stress Theory
Family stress theory explains how families react to stressful events and suggests factors that promote adaptation to stress (Hanson, Gedaly-Duff, and Kaakinen, 2005). Families encounter stressors (events that cause stress and have the potential to effect a change in the family social system), including those that are predictable (e.g., parenthood) and those that are unpredictable (e.g., illness, unemployment). These stressors are cumulative, involving simultaneous demands from work, family, and community life. Too many stressful events occurring within a relatively short period (usually 1 year) can overwhelm the family’s ability to cope and place it at risk for breakdown or physical and emotional health problems among its members. When the family experiences too many stressors for it to cope adequately, a state of crisis ensues. For adaptation to occur, a change in family structure or interaction is necessary.
The resiliency model of family stress, adjustment, and adaptation emphasizes that the stressful situation is not necessarily pathologic or detrimental to the family but demonstrates that the family needs to make fundamental structural or systemic changes to adapt to the situation (McCubbin and McCubbin, 1994).
Developmental Theory
Developmental theory is an outgrowth of several theories of development. Duvall (1977) described eight developmental tasks of the family throughout its life span (Box 3-1). The family is described as a small group, a semiclosed system of personalities that interacts with the larger cultural social system. As an interrelated system, the family does not have changes in one part without a series of changes in other parts.
Developmental theory addresses family change over time using Duvall’s family life cycle stages, based on the predictable changes in the family’s structure, function, and roles, with the age of the oldest child as the marker for stage transition. The arrival of the first child marks the transition from stage I to stage II. As the first child grows and develops, the family enters subsequent stages. In every stage the family faces certain developmental tasks. At the same time, each family member must achieve individual developmental tasks as part of each family life cycle stage.
Developmental theory can be applied to nursing practice. For example, the nurse can assess how well new parents are accomplishing the individual and family developmental tasks associated with transition to parenthood. New applications should emerge as more is learned about developmental stages for nonnuclear and nontraditional families.
Family Nursing Interventions
In working with children, the nurse must include family members in their care plan. Research confirms parents’ desire and expectation to participate in their child’s care (Power and Franck, 2008). To discover family dynamics, strengths, and weaknesses, a thorough family assessment is necessary (see Chapter 6). The nurse’s choice of interventions depends on the theoretic family model that is used (Box 3-2). For example, in family systems theory, the focus is on the interaction of family members within the larger environment (Goldenberg and Goldenberg, 2008). In this case, using group dynamics to involve all members in the intervention process and being a skillful communicator are essential. Systems theory also presents excellent opportunities for anticipatory guidance. Because each family member reacts to every stress experienced by that system, nurses can intervene to help the family prepare for and cope with changes. In family stress theory the nurse employs crisis intervention strategies to help family members cope with the challenging event. In developmental theory the nurse provides anticipatory guidance to prepare members for transition to the next family stage. Nurses who think family involvement plays a key role in the care of a child are more likely to include families in the child’s daily care (Fisher, Lindhorst, Matthews, et al, 2008).
Family Structure and Function
The family structure, or family composition, consists of individuals, each with a socially recognized status and position, who interact with one another on a regular, recurring basis in socially sanctioned ways (Hanson, Gedaly-Duff, and Kaakinen, 2005). When members are gained or lost through events such as marriage, divorce, birth, death, abandonment, or incarceration, the family composition is altered and roles must be redefined or redistributed.
Traditionally, the family structure was either a nuclear or extended family. In recent years, family composition has assumed new configurations, with the single-parent family and blended family becoming prominent forms. The predominant structural pattern in any society depends on the mobility of families as they pursue economic goals and as relationships change. It is not uncommon for children to belong to several different family groups during their lifetime.
Nurses must be able to meet the needs of children from many diverse family structures and home situations. A family’s particular structure affects the direction of nursing care. The U.S. Census Bureau uses four definitions for families: the traditional nuclear family, the nuclear family, the blended family or household, and the extended family or household.
Traditional Nuclear Family
A traditional nuclear family consists of a married couple and their biologic children. Children in this type of family live with both biologic parents and, if siblings are present, only full brothers and sisters (i.e., siblings who share the same two biologic parents). No other persons are present in the household (i.e., no steprelatives, foster or adopted children, half-siblings, other relatives, or nonrelatives).
Nuclear Family
The nuclear family is composed of two parents and their children. The parent-child relationship may be biologic, step, adoptive, or foster. Sibling ties may be biologic, step, half, or adoptive. The parents are not necessarily married. No other relatives or nonrelatives are present in the household.
Blended Family
A blended family or household, also called a reconstituted family, includes at least one stepparent, stepsibling, or half-sibling. A stepparent is the spouse of a child’s biologic parent but is not the child’s biologic parent. Stepsiblings do not share a common biologic parent; the biologic parent of one child is the stepparent of the other. Half-siblings share only one biologic parent.
Extended Family
An extended family or household includes at least one parent, one or more children, and one or more members (related or unrelated) other than a parent or sibling. Parent-child and sibling relationships may be biologic, step, adoptive, or foster.
In many nations and among many ethnic and cultural groups, households with extended families are common. Within the extended family, grandparents often find themselves rearing their grandchildren (Fig. 3-1). Young parents are often considered too young or too inexperienced to make decisions independently. Often, the older relative holds the authority and makes decisions in consultation with the young parents. Sharing residence with relatives also assists with the management of scarce resources and provides child care for working families. A resource for extended families is the Grandparent Information Center.*

Single-Parent Family
In the United States an estimated 21.7 million children live in single-parent families (Annie E Casey Foundation, 2009). The contemporary single-parent family has emerged partially as a consequence of the women’s rights movement and also as a result of more women (and men) establishing separate households because of divorce, death, desertion, or single parenthood. In addition, a more liberal attitude in the courts has made it possible for single people, both male and female, to adopt children. Although mothers usually head single-parent families, it is becoming more common for fathers to be awarded custody of dependent children in divorce settlements. With women’s increased psychologic and financial independence and the increased acceptability of single parents in society, more unmarried women are deliberately choosing mother-child families. Frequently, these mothers and children are absorbed into the extended family. The challenges of single-parent families are discussed on p. 63.
Binuclear Family
The term binuclear family refers to parents continuing the parenting role while terminating the spousal unit. The degree of cooperation between households and the time the child spends with each can vary. In joint custody the court assigns divorcing parents equal rights and responsibilities concerning the minor child or children. These alternate family forms are efforts to view divorce as a process of reorganization and redefinition of a family rather than as a family dissolution. Joint custody and coparenting are discussed further on p. 63.
Polygamous Family
Although it is not legally sanctioned in the United States, the conjugal unit is sometimes extended by the addition of spouses in polygamous matings. Polygamy refers to either multiple wives (polygyny) or, rarely, husbands (polyandry). Many societies practice polygyny that is further designated as sororal, in which the wives are sisters, or nonsororal, in which the wives are unrelated. Sororal polygyny is widespread throughout the world. Most often, mothers and their children share a husband and father, with each mother and her children living in the same or separate household.
Communal Family
The communal family emerged from disenchantment with most contemporary life choices. Although communal families may have divergent beliefs, practices, and organization, the basic impetus for formation is often dissatisfaction with the nuclear family structure, social systems, and goals of the larger community. Relatively uncommon today, communal groups share common ownership of property. In cooperatives, property ownership is private, but certain goods and services are shared and exchanged without monetary consideration. There is strong reliance on group members and material interdependence. Both provide collective security for nonproductive members, share homemaking and childrearing functions, and help overcome the problem of interpersonal isolation or loneliness.
Gay, Lesbian, Bisexual, and Transgender Families
A same-sex, homosexual, or gay/lesbian/bisexual/transgender (GLBT) family is one in which there is a legal or common-law tie between two persons of the same sex who have children (Blackwell, 2007). There are a growing number of families with same-sex parents in the United States, with an estimated one fourth of all same-sex couples raising children (Pawelski, Perrin, Foy, et al, 2006). Although some children in gay/lesbian households are biologic from a former marriage or relationship, children may be present in other circumstances. They may be foster or adoptive parents, lesbian mothers may conceive through artificial fertilization, or a gay male couple may become parents through use of a surrogate mother.
When children are brought up in GLBT families, the relationships seem as natural to them as heterosexual parents do to their offspring. In other cases, however, disclosure of parental homosexuality (“coming out”) to children can be a concern for families. There are a number of factors to consider before disclosing this information to children. Parents should be comfortable with their own sexual preference and should discuss this with the children as they become old enough to understand relationships. Discussions should be planned and take place in a quiet setting where interruptions are unlikely.
Nurses need to be nonjudgmental and to learn to accept differences rather than demonstrate prejudice that can have a detrimental effect on the nurse-child-family relationship (Blackwell, 2007). Moreover, the more nurses know about the child’s family and lifestyle, the more they can help the parents and the child.
Family Strengths and Functioning Style
 Family function refers to the interactions of family members, especially the quality of those relationships and interactions (Bomar, 2004). Researchers are interested in family characteristics that help families function effectively. Knowledge of these factors guides the nurse throughout the nursing process and helps the nurse to predict ways that families may cope and respond to a stressful event, to provide individualized support that builds on family strengths and unique functioning style, and to assist family members in obtaining resources.
Family function refers to the interactions of family members, especially the quality of those relationships and interactions (Bomar, 2004). Researchers are interested in family characteristics that help families function effectively. Knowledge of these factors guides the nurse throughout the nursing process and helps the nurse to predict ways that families may cope and respond to a stressful event, to provide individualized support that builds on family strengths and unique functioning style, and to assist family members in obtaining resources.
 Case Study—Family Functioning
Case Study—Family FunctioningFamily strengths and unique functioning styles (Box 3-3) are significant resources that nurses can use to meet family needs. Building on qualities that make a family work well and strengthening family resources make the family unit even stronger. All families have strengths as well as vulnerabilities.
Family Roles and Relationships
Each individual has a position, or status, in the family structure and plays culturally and socially defined roles in interactions within the family. Each family also has its own traditions and values and sets its own standards for interaction within and outside the group. Each determines the experiences the children should have, those they are to be shielded from, and how each of these experiences meets the needs of family members. When family ties are strong, social control is highly effective, and most members conform to their roles willingly and with commitment. Conflicts arise when people do not fulfill their roles in ways that meet other family members’ expectations, either because they are unaware of the expectations or because they choose not to meet them.
Parental Roles
In all family groups the socially recognized status of father and mother exists with socially sanctioned roles that prescribe appropriate sexual behavior and childrearing responsibilities. The guides for behavior in these roles serve to control sexual conflict in society and provide for prolonged care of children. The degree to which parents are committed and the way they play their roles are influenced by a number of variables and by the parents’ unique socialization experience.
Parental role definitions have changed as a result of the changing economy and increased opportunities for women (Bomar, 2004). As the woman’s role has changed, the complementary role of the man has also changed. Many fathers are more active in childrearing and household tasks. As the redefinition of sex roles continues in American families, role conflicts may arise in many families because of a cultural lag of the persisting traditional role definitions.
Role Learning
Roles are learned through the socialization process. During all stages of development children learn and practice, through interaction with others and in their play, a set of social roles and the characteristics of other roles. They behave in patterned and more or less predictable ways because they learn roles that define mutual expectations in typical social relationships. Although role definitions are changing, the basic determinants of parenting remain the same. Several determinants of parenting infants and young children are parental personality and mental well-being, systems of support, and child characteristics. These determinants have been used as consistent measurements to determine a person’s success in fulfilling the parental role.
Parents, peers, authority figures, and other socializing agents who use positive and negative sanctions to ensure conformity to their norms transmit role conceptions. Role behaviors positively reinforced by rewards such as love, affection, friendship, and honors are strengthened. Negative reinforcement takes the form of ridicule, withdrawal of love, expressions of disapproval, or banishment.
In some cultures the role behavior expected of children conflicts with desirable adult behavior. One of the family’s responsibilities is to develop culturally appropriate role behavior in children. Children learn to perform in expected ways consistent with their position in the family and culture. The observed behavior of each child is a single manifestation—a combination of social influences and individual psychologic processes. In this way the uniting of the child’s intrapersonal system (the self) with the interpersonal system (the family) is simultaneously understood as the child’s conduct.
Role structuring initially takes place within the family unit, in which the children fulfill a set of roles and respond to the roles of their parents and other family members (Hanson, Gedaly-Duff, and Kaakinen, 2005). Children’s roles are shaped primarily by the parents, who apply direct or indirect pressures to induce or force children into the desired patterns of behavior or direct their efforts toward modification of the role responses of the child on a mutually acceptable basis. Parents have their own techniques and determine the course that the socialization process follows.
Children respond to life situations according to behaviors learned in reciprocal transactions. As they acquire important role-taking skills, their relationships with others change. For instance, when a teenager is also the mother but lives in a household with the grandmother, the teenager may be viewed more as an adolescent than as a mother. Children become proficient at understanding others as they acquire the ability to discriminate their own perspectives from those of others. Children who get along well with others and attain status in the peer group have well-developed role-taking skills.
Family Size and Configuration
Parenting practices differ between small and large families. Small families place more emphasis on the individual development of the children. Parenting is intensive rather than extensive, and there is constant pressure to measure up to family expectations. Children’s development and achievement are measured against those of other children in the neighborhood and social class. In small families, children have more democratic participation than in larger families. Adolescents in small families identify more strongly with their parents and rely more on them for advice. They have well-developed, autonomous inner controls as contrasted with adolescents from larger families, who rely more on adult authority.
Children in a large family are able to adjust to a variety of changes and crises. There is more emphasis on the group and less on the individual (Fig. 3-2). Cooperation is essential, often because of economic necessity. The large number of people sharing a limited amount of space requires a greater degree of organization, administration, and authoritarian control. A dominant family member (a parent or older child) wields control. The number of children reduces the intimate, one-to-one contact between the parent and any individual child. Consequently, children turn to each other for what they cannot get from their parents. The reduced parent-child contact encourages individual children to adopt specialized roles to gain recognition in the family.

Older siblings in large families often administer discipline. Siblings are usually attuned to what constitutes misbehavior. Sibling disapproval or ostracism is frequently a more meaningful disciplinary measure than parental interventions. In situations such as death or illness of a parent, an older sibling often assumes responsibility for the family at considerable personal sacrifice. Large families generate a sense of security in the children that is fostered by sibling support and cooperation. However, adolescents from a large family are more peer oriented than family oriented.
Sibling Interactions
Spacing of Children: Age differences between siblings affect the childhood environment, but to a lesser extent than does the sex of the sibling. The arrival of a sibling is difficult for toddlers and preschool children, especially between the ages of 2 and 3 years old. At this age, they are still very attached to their parents and do not understand the concept of sharing. An older child is able to understand the situation and is less likely to see the newcomer as a threat, although the child does feel the loss of the only-child status (Hanson, Gedaly-Duff, and Kaakinen, 2005). In general, the narrower the spacing between siblings, the more the children influence one another, especially in emotional characteristics. The wider the spacing, the greater the influence of the parents.
Traditionally, sibling relationships were viewed from a Freudian perspective that emphasized the concept of sibling rivalry. Researchers have viewed siblings through developmental or ecologic frameworks that focus on interactions within family systems (Friedman, Bowden, and Jones, 2003). The results of these broader perspectives provide a picture of rich and varied sibling interactions (Fig. 3-3).
Sibling Functions: The sibling relationship’s most unique feature is its duration. The longest relationship one will share with another human being is the sibling relationship, which lasts through a lifetime (often 50 to 80 years), compared with the child-parent relationship of approximately 30 to 50 years. Siblings spend long periods together and get to know each other at their best and worst.
Siblings exert power, exchange services, and express feelings in reciprocal ways that are often not revealed in the presence of the parents. They see themselves in their brother or sister, experience life vicariously through their sibling’s behavior, and begin to expand on their own possibilities. Siblings can also be touchstones for what the other would not like to be, and they use each other as yardsticks for comparison. They provide a sounding board for each other and offer a safe forum for experimenting with new behaviors and roles. Brothers and sisters provide each other with tangible services (e.g., lending money, clothing, toys, or sports equipment; teaching a skill), help each other with childhood problems, provide support in dealing with parents or others outside the family, and provide introductions to new friendship groups. Children learn to negotiate and bargain, and sometimes to manipulate, from their siblings. Their interactions with each other provide opportunities for conflict and conflict resolution. They protect one another from parental-executive abuse of power and can form a coalition to deal with the issues of authority, power, and emotional support. Negotiating with parents is stronger when siblings act together rather than singly.
Tattling can be an important lever in sibling interactions. On the other hand, siblings often have a conspiracy of silence, leaving the parents feeling isolated and excluded. A willingness to maintain each other’s privacy often forges a powerful bond of loyalty that distinguishes the relationship between siblings from that between friends.
More Active Sibling Relationships: Sibling relationships vary among cultures. Some factors may be giving the sibling relationship greater significance in American families than in the past. Shrinking family size, longer life spans, divorce and remarriage, geographic mobility, maternal employment, alternative sources of child care, competitive pressures, stress, and parental insufficiency may be propelling siblings into greater contact and emotional interdependence than ever before. Siblings often join forces to confront the trauma of divorce, and they frequently rely on each other for support when parents remarry. The large number of working mothers means that young siblings today have significant amounts of time when a personally committed adult does not monitor their relationship. Often an older sibling is required to baby-sit, resulting in children spending more and more time together unsupervised. In a worried, mobile, small-family, high-stress, fast-paced, parent-absent society, children often turn to a brother or sister to meet their needs for contact, constancy, and permanency.
Ordinal Position
Researchers have observed that the birth position of children affects their personalities. Parents treat children differently, and sibling interactions are different, depending on the child’s position within the family. Power is unequally distributed among siblings. Older siblings attempt to dominate younger ones. Therefore younger siblings develop interpersonal skills, the ability to negotiate, and an ability to accept unfavorable outcomes to a greater extent than older siblings. Later-born children are obliged to interact with other siblings from birth and seem to be more outgoing and make friends more easily than firstborns. Children vary tremendously, and generalizations do not always apply to the individual. General characteristics of children in the various ordinal positions are presented in Box 3-4.
The Only Child: Being the only child in a family has traditionally been considered a disadvantage. Only children have been described as selfish, spoiled, dependent, and lonely. However, they do not demonstrate more evidence of maladjustment or self-centeredness than other children and tend to strongly resemble firstborn children in respects such as higher educational goals. Only children perform better on cognitive tests, are more mature, are more socially sensitive, and demonstrate superiority in language facility compared with other children.
Only children also enjoy the advantage of having parents who can devote more time to them, talk to them, and stimulate them in intellectual activities. However, parents also exert greater pressure for mature behavior at an early age and for achievement. Relative isolation from peers contributes to intellectual pursuits and encourages a rich fantasy life, independence, and originality.
Multiple Births
A deviation in early development that occurs with variable frequency is multiple births. Twins are not uncommon in the population, but triplets are rare and quadruplets or quintuplets are extremely unusual. In any of these situations, the offspring can be of the like or unlike sex (i.e., derived from a single ovum; from multiple ova; or from a combination of the two, which can involve one or more cell divisions). The cause of twinning is unknown, but the increase in the number of larger multiples (quintuplets, sextuplets) in recent years has been associated with fertility treatments such as ovulation-inducing drugs or in vitro fertilization. Because women in their thirties are almost 2.5 times as likely as women in their twenties to have higher-order plural births, increased childbearing among older women and the expanded use of fertility drugs have been associated with a rise in the multiple-birth ratio (Hamilton, Minino, Martin, et al, 2007).
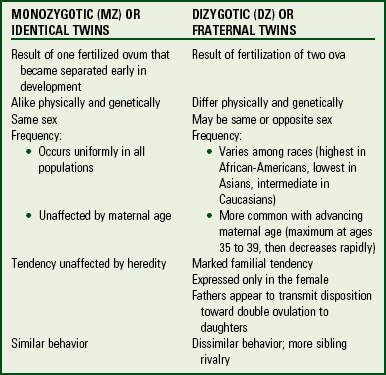
Twins are of two distinct types: identical, or monozygotic (MZ), and fraternal (Fig. 3-4), or dizygotic (DZ) (Box 3-5). In 2004 in the United States the overall rate of twin birth was 32.2 per 1000 births, a record high (Martin, Kung, Mathews, et al, 2008); one third are MZ twins, and two thirds are DZ twins.
A special kind of sibling relationship is observed in twins, although getting along with each other and quarreling are not much different from these behaviors in any other two siblings, especially if they are different-sex fraternal twins. Twins tend to work out a relationship that is reasonably satisfactory to both and demonstrate early independence from parental attention. They develop a remarkable capacity for cooperative play and considerable loyalty and generosity toward each other. It is not uncommon for them to evolve a private language between themselves that may interfere with the development of the family language.
In a twinship, one member of the pair, to a greater or lesser extent, is more dominant, outgoing, and assertive than the other, often to the consternation of their parents. However, the seemingly more passive twin is able to accomplish as much and get his or her way as frequently as the more assertive twin.
Researchers have also observed a difference in behavior between identical and fraternal twins. There is near-unison in the actions of identical twins (although they alternate in assuming the leadership), but fraternal twins, even of the same sex, do not display this quality. Sibling rivalry can be pronounced in fraternal twins, especially in different-sex twins.
Identical twins also differ in their response to the tendency of some parents to treat twins exactly alike. The present philosophy is to determine the degree to which the children demonstrate an inclination toward togetherness. Some twins thrive best when they are constantly in each other’s company; others prefer more individuality and separateness. Early years of togetherness are often the basis of the children’s security, and separating them too early may produce unnecessary stresses. Fostering individual differences as they become evident could ease the process of separation when it becomes advisable.
Parental Adjustment: The entrance of any new member into a household creates stress, but with multiple births two or more new members must be incorporated into the family at the same time. The problems are obvious. Two infants must be provided with physical care, including feeding, diapering, and all of the purchasing and preparation that accompanies the care of any infant. Scheduling becomes crucial, and advancement in development brings new problems and adjustments (e.g., space and sleeping arrangements, selection of a stroller and other equipment). Care must be observed in selecting toys. As play becomes a serious business, some toys that would be safe and appropriate for a single child become weapons when two infants share a playpen. It is a good idea to select different toys for each child as they grow older and encourage sharing.
It is especially important for parents to maintain relationships with each other and other family members. Parents need to arrange time together as often as possible. The National Organization of Mothers of Twins Clubs, Inc.,* has local chapters throughout the United States to offer information and support to parents of twins and is highly recommended as a resource. Twins Magazine (www.twinsmagazine.com) is a place to seek and give advice about parenting multiples.
PARENTING
A dominant characteristic in all societies is that adults are expected to become parents and to be gratified by the experience. Pressures of tradition, sentiment regarding the state of parenthood, and religious beliefs influence decision making because conformity to social-role expectations is a strong influence in family planning.
Factors that influence family size are social class, religion, race, financial stability, type of conjugal-role relationships, and the social-psychologic aspects of sexual relations (Hanson, Gedaly-Duff, and Kaakinen, 2005). In the case of divorce and remarriage, an individual may decide to have more children with the new spouse.
Preparation for Parenthood
The basic goals of parenting are to promote the physical survival and health of children, to foster the skills and abilities necessary to be self-sustaining adults, and to foster behavioral capabilities for optimizing cultural values and beliefs (Deave, Johnson, and Ingram, 2008). However, new parents often approach parenthood with limited experience and knowledge. Parents learn by trial and error, committing the same mistakes that have been committed by countless other parents, but they somehow manage to accomplish the task, becoming more skilled with each additional child.
Tradition, rather than rational planning, furnishes the chief norms for childrearing. Experience in having been nurtured as a child is an essential component of successful parenting. Their own parents are probably the only persons whom parents observe intimately in the parental role. This results in a generational continuity—parents rear their own children in much the same way that they themselves were reared. Other essential skills that parents need to feel comfortable in the parenting role include a basic understanding of childhood growth and development, bathing, feeding, use of play, and interpersonal communication skills.
Transition to Parenthood
Although experts disagree as to whether the birth of the first child should be labeled a crisis, the early weeks of an infant’s life call for parents to make drastic adjustments. A child’s birth presents the challenge of providing total care 24 hours a day for a new member of the family (Deave, Johnson, and Ingram, 2008). A crisis may occur if the event is perceived as disturbing old habits and relationships and eliciting new responses. The birth requires role changes and significantly modifies former relationships. In addition to the roles of husband and wife, the couple must assume the roles of father and mother.
The advent of a new family member requires that the family cope with greater financial responsibilities, a possible loss of income, changes in sleeping habits, and less time for the parents to spend with each other (especially if it is a firstborn) and with other children. If these events are perceived as aversive, it can disrupt the couple’s bond and reduce their intimacy and affection.
Parental Factors Affecting Transition to Parenthood
No amount of preparation can fully prepare prospective parents for an infant’s constant and immediate needs. The importance of early parent-infant interactions is addressed in the discussion of the neonate, especially the attachment process (see Chapter 8). Factors affecting parenting are the age of the parents, the quality of the parental relationship, the amount of previous experience with childrearing, parental support systems, and the effects of stress on parental behavior (Deave, Johnson, and Ingram, 2008).
Parental Age: From a physiologic health perspective, the most satisfactory ages for childbearing are the years between 18 and 35. During this time, parents are considered to be in optimum health, with a predicted life span that allows sufficient time and vigor to raise a family. However, the age at which parents begin their families has changed over the past few decades in the United States, with a substantial increase in the birth rate for women 30 to 44 years of age and a decline for women ages 20 to 29 years.
Father Involvement: Current practices that encourage early father-infant interaction indicate that fathers are as intrigued with their newborns as mothers are (see discussion on paternal engrossment under Promote Parent-Infant Bonding [Attachment], Chapter 8). Even fathers who have little initial contact with their newborn become involved with them over the next few months (Fig. 3-5), although the type of interaction is different from that of the mother. For example, mothers are more likely to hold, soothe, care for, or play quietly with their infants, whereas fathers are more boisterous and engage in more physically stimulating activities. However, fathers are more than just playmates. They are often successful at soothing a distressed infant. A secure attachment to the father can help offset the consequences of an insecure attachment to the mother.

Parenting Education: First-time parents who have prepared themselves to be parents experience less stress adjusting to the birth of a new baby than those who have not. Programs designed to take place near the time of birth or soon after can be more helpful in easing transitional stress than earlier programs (Deave, Johnson, and Ingram, 2008).
Many parents are looking for ways to be a better parent. Nurses can offer a number of suggestions, including being an active listener, having an active role in education, keeping up with technology, keeping up with regular visits to the child’s health care provider and vaccinations, ensuring safety in and out of the home, spending quality time with the child, and focusing on improving overall family communication (Fig. 3-6).

Other factors influencing the transition to the parental role include the following:
• Parents with previous experience, such as another child, appear to be more relaxed, have less conflict in disciplinary relationships, and are more aware of normal growth and development.
• The amount of stress experienced by one or both parents may interfere with their ability to be patient and understanding and to cope with their children’s behavior.
• Special characteristics of the infant, such as being temperamentally difficult, can cause the parents to lose confidence and doubt their abilities. Infants with special care needs (such as those associated with a disability) can be a significant source of added stress.
• Stressed marital relationships can have a negative effect on parental transition because marital tension can alter caregiving routines and interfere with enjoyment of the infant. Conversely, parents’ support and encouragement of one another serve as positive influences on establishing a satisfying parental role.
Support Systems: Successful adaptation to the stress of transition to parenthood involves at least two types of family resources (McCubbin and McCubbin, 1994). Internal resources such as adaptability and integration are the first type of resource. Changing from an orderly, predictable life to a relatively disordered, unpredictable one is a universal adaptation that families must make. Rigid schedules are impossible to maintain, and former activities must be curtailed or abandoned. Adaptation is reflected in learning to be patient, becoming better organized, and becoming more flexible. Integration refers to the couple’s attempt to continue some activities they engaged in before they became parents. In this way couples are able to maintain a sense of continuity and appreciate the importance of the husband-wife relationship (McCubbin and McCubbin, 1994).
The second resource is the use of coping strategies that strengthen the family’s organization and functioning. These include the use of social support systems and community resources and the adoption of a future orientation. Interpersonal supports that provide information, advice, and caretaking can be derived from friends, relatives, and neighbors. Relationships with family, friends, and community are essential. For parents, positive, supportive work relationships are important. Equally important is time spent with friends. Arranging for time away from the child or children is also beneficial. One parent can assume care of the family to allow the other parent some time to himself or herself. Adoption of a future orientation reassures parents that things will get better, that they will cope, and that it is realistic to plan for the time when they will be able to engage in self-fulfilling activities.
It is also reassuring to know that others experience ambivalent feelings toward parenthood and share the same difficulties and frustrations. Exchanging ideas and experiences with other parents and each other provides an opportunity to voice concerns and to learn new ways to cope with multiple childrearing problems (Fig. 3-7).

Parenting Behaviors
Parenting styles have been described in many different ways. Within a social interactional learning model, parenting can be positive or coercive (Liddle, Santisteban, Levant, et al, 2002). A positive approach to parenting encourages skill development, whereas a coercive approach uses negative reinforcement and often causes a destructive effect on relationships.
Parenting styles are often classified as authoritarian, permissive, or authoritative (Hoeve, Dubas, Eichelsheim, et al, 2009; Hubbs-Tait, Kennedy, Page, et al, 2008). Authoritarian or dictatorial parents try to control their children’s behavior and attitudes through unquestioned mandates. They establish rules and regulations or standards of conduct that they expect to be followed rigidly and unquestioningly. The message is: “Do it because I say so.” Punishment need not be corporal but may be stern withdrawal of love and approval. Careful training often results in rigidly conforming behavior in the children, who tend to be sensitive, shy, self-conscious, retiring, and submissive. They are more likely to be courteous, loyal, honest, and dependable but docile. These behaviors are more typically observed when close supervision and affection accompany parental authority. If not, this style of parenting may be associated with both defiant and antisocial behavior.
Permissive parents exert little or no control over their children’s actions. They avoid imposing their own standards of conduct and allow their children to regulate their own activity as much as possible. These parents consider themselves to be resources for the children, not role models. If rules do exist, the parents explain the underlying reason, elicit the children’s opinions, and consult them in decision-making processes. They employ lax, inconsistent discipline; do not set sensible limits; and do not prevent the children from upsetting the home routine. These parents rarely punish the children.
Authoritative or democratic parents combine practices from both of the previously described parenting styles. They direct their children’s behavior and attitudes by emphasizing the reason for rules and negatively reinforcing deviations. They respect the individuality of each child and allow the child to voice objections to family standards or regulations. Parental control is firm and consistent but tempered with encouragement, understanding, and security. Control is focused on the issue, not on withdrawal of love or the fear of punishment. These parents foster “inner-directedness,” a conscience that regulates behavior based on feelings of guilt or shame for wrongdoing, not on fear of being caught or punished. Parents’ realistic standards and reasonable expectations produce children with high self-esteem who are self-reliant, assertive, inquisitive, content, and highly interactive with other children.
There are differing philosophies in regard to parenting. Childrearing is a culturally bound phenomenon, and children are socialized to behave in ways that are important to their family. In the authoritative style, authority is shared and children are included in discussions, fostering an independent and assertive style of participation in family life. When working with individual families, nurses should give these differing styles equal respect.
Limit Setting and Discipline
In its broadest sense, discipline means to teach or refers to a set of rules governing conduct. In a narrower sense, it refers to the action taken to enforce the rules after noncompliance. Limit setting refers to establishing the rules or guidelines for behavior. For example, parents can place limits on the amount of time children spend watching television or chatting online. The clearer the limits that are set and the more consistently they are enforced, the less need there is for disciplinary action.
Nurses can help parents establish realistic and concrete “rules.” Limit setting and discipline are positive, necessary components of childrearing and serve several useful functions as they help children:
• Test their limits of control
• Achieve in areas appropriate for mastery at their level
• Channel undesirable feelings into constructive activity
Children want and need limits. Unrestricted freedom is a threat to their security and safety. By testing the limits imposed on them, children learn the extent to which they can manipulate their environment and gain reassurance from knowing that others are there to protect them from potential harm.
Minimizing Misbehavior
The reasons for misbehavior may include attention, power, defiance, and a display of inadequacy (e.g., the child misses classes because of a fear that he or she is unable to do the work). Children may also misbehave because the rules are not clear or consistently applied. Acting-out behavior, such as a temper tantrum, may represent uncontrolled frustration, anger, depression, or pain. The best approach is to structure interactions with children to prevent or minimize unacceptable behavior (see Family-Centered Care box).
 FAMILY-CENTERED CARE
FAMILY-CENTERED CARE
Minimizing Misbehavior
• Set realistic goals for acceptable behavior and expected achievements.
• Structure opportunities for small successes to lessen feelings of inadequacy.
• Praise children for desirable behavior with attention and verbal approval.
• Structure the environment to prevent unnecessary difficulties (e.g., place fragile objects in inaccessible area).
• Set clear and reasonable rules; expect the same behavior regardless of the circumstances; if exceptions are made, clarify that the change is for one time only.
• Teach desirable behavior through own example, such as using a quiet, calm voice rather than screaming.
• Review expected behavior before special or unusual events, such as visiting a relative or having dinner in a restaurant.
• Phrase requests for appropriate behavior positively, such as “Put the book down,” rather than “Don’t touch the book.”
• Call attention to unacceptable behavior as soon as it begins; use distraction to change the behavior or offer alternatives to annoying actions, such as exchanging a quiet toy for one that is too noisy.
• Give advance notice or “friendly reminders,” such as “When the TV program is over, it is time for dinner” or “I’ll give you to the count of three and then we have to go.”
• Be attentive to situations that increase the likelihood of misbehaving, such as overexcitement or fatigue, or decreased personal tolerance to minor infractions.
• Offer sympathetic explanations for not granting a request, such as “I am sorry I can’t read you a story now, but I have to finish dinner. Then we can spend time together.”
• Keep any promises made to children.
• Avoid outright conflicts; temper discussions with statements such as “Let’s talk about it and see what we can decide together” or “I have to think about it first.”
• Provide children with opportunities for power and control.
General Guidelines for Implementing Discipline
Regardless of the type of discipline used, certain principles are essential to ensure the efficacy of the approach (see Family-Centered Care box). Many strategies, such as behavior modification, can only be implemented effectively when principles of consistency and timing are followed. A pattern of intermittent or occasional enforcement of limits actually prolongs the undesired behavior because children learn that if they are persistent, the behavior is permitted eventually. Delaying punishment weakens its intent, and practices such as telling the child, “Wait until your father comes home,” are not only ineffectual, but also convey negative messages about the other parent.*
FAMILY-CENTERED CARE
Implementing Discipline
Consistency—Implement disciplinary action exactly as agreed on and for each infraction.
Timing—Initiate discipline as soon as child misbehaves; if delays are necessary, such as to avoid embarrassment, verbally disapprove of the behavior and state that disciplinary action will be implemented.
Commitment—Follow through with the details of the discipline, such as timing of minutes; avoid distractions that may interfere with the plan, such as telephone calls.
Unity—Make certain that all caregivers agree on the plan and are familiar with the details to prevent confusion and alliances between child and one parent.
Flexibility—Choose disciplinary strategies that are appropriate to child’s age and temperament and the severity of the misbehavior.
Planning—Plan disciplinary strategies in advance and prepare child if feasible (e.g., explain use of time-out); for unexpected misbehavior, try to discipline when you are calm.
Behavior orientation—Always disapprove of the behavior, not the child, with such statements as “That was a wrong thing to do. I am unhappy when I see behavior like that.”
Privacy—Administer discipline in private, especially with older children, who may feel ashamed in front of others.
Termination—After the discipline is administered, consider child as having a “clean slate,” and avoid bringing up the incident or lecturing.
Types of Discipline
To deal with misbehavior, parents need to implement appropriate disciplinary action. Many approaches are available. Reasoning involves explaining why an act is wrong and is usually appropriate for older children, especially when moral issues are involved. However, young children cannot be expected to “see the other side” because of their egocentrism. Children in the preoperative stage of cognitive development (toddlers and preschoolers) have a limited ability to distinguish between their point of view and that of others. Sometimes children use “reasoning” as a way of gaining attention. For example, they may misbehave thinking the parents will give them a lengthy explanation of the wrongdoing and knowing that negative attention is better than no attention. When children use this technique, parents should end the explanation by stating, “This is the rule, and this is how I expect you to behave. I won’t explain it any further.”
Unfortunately, reasoning is often combined with scolding, which sometimes takes the form of shame or criticism. For example, the parent may state, “You are a bad boy for hitting your brother.” Children take such remarks seriously and personally, believing that they are bad.
NURSING ALERT
When reprimanding children, focus only on the misbehavior, not on the child. Use of “I” messages rather than “you” messages expresses personal feelings without accusation or ridicule. For example, an “I” message attacks the behavior—”I am upset when Johnny is punched; I don’t like to see him hurt”—not the child.
Positive and negative reinforcement is the basis of behavior modification theory—behavior that is rewarded will be repeated; behavior that is not rewarded will be extinguished. Using rewards is a positive approach. By encouraging children to behave in specified ways, the parents can decrease the tendency to misbehave. With young children, using paper stars is an effective method. For older children, the “token system” is appropriate, especially if a certain number of stars or tokens yields a special reward, such as a trip to the movies or a new book. In planning a reward system, the parents must explain expected behaviors to the child and establish rewards that are reinforcing. They should use a chart to record the stars or tokens and always give an earned reward promptly. Verbal approval should always accompany extrinsic rewards.
Consistently ignoring behavior will eventually extinguish or minimize the act. Although this approach sounds simple, it is difficult to implement consistently. Parents frequently “give in” and resort to previous patterns of discipline. Consequently, the behavior is actually reinforced because the child learns that persistence gains parental attention. For ignoring to be effective, parents should (1) understand the process, (2) record the undesired behavior before using ignoring to determine whether a problem exists and to compare results after ignoring is begun, (3) determine whether parental attention acts as a reinforcer, and (4) be aware of “response burst.” Response burst is a phenomenon that occurs when the undesired behavior increases after ignoring is initiated because the child is “testing” the parents to see if they are serious about the plan.
The strategy of consequences involves allowing children to experience the results of their misbehavior. It includes three types:
1. Natural—Those that occur without any intervention, such as being late and having to clean up the dinner table
2. Logical—Those that are directly related to the rule, such as not being allowed to play with another toy until the used ones are put away
3. Unrelated—Those that are imposed deliberately, such as no playing until homework is completed or the use of time-out
Natural or logical consequences are preferred and effective if they are meaningful to children. For example, the natural consequence of living in a messy room may do little to encourage cleaning up, but allowing no friends over until the room is neat can be motivating! Withdrawing privileges is often an unrelated consequence. After the child experiences the consequence, the parent should refrain from any comment, because the usual tendency is for the child to try to place blame for imposing the rule.
Time-out is a refinement of the common practice of sending the child to his or her room and is a type of unrelated consequence. It is based on the premise of removing the reinforcer (i.e., the satisfaction or attention the child is receiving from the activity). When placed in an unstimulating and isolated place, children become bored and consequently agree to behave in order to reenter the family group (Fig. 3-8). Time-out avoids many of the problems of other disciplinary approaches. No physical punishment is involved; no reasoning or scolding is given; and the parent does not need to be present for all of the time-out, thus facilitating consistent application of this type of discipline. Time-out offers both the child and the parent a “cooling off” time. To be effective, however, time-out must be planned in advance (see Family-Centered Care box).
FAMILY-CENTERED CARE
Using Time-Out
Select an area for time-out that is safe, convenient, and unstimulating, but where the child can be monitored, such as the bathroom, hallway, or laundry room.
Determine what behaviors warrant a time-out.
Make certain children understand the “rules” and how they are expected to behave.
Explain to children the process of time-out:
• When they misbehave, they will be given one warning.
• If they do not obey, they will be sent to the place designated for time-out.
• They are to sit there for a specified period.
• If they cry, refuse, or display any disruptive behavior, the time-out period will begin after they quiet down.
• When they are quiet for the duration of the time, they can then leave the room.
A rule for the length of time-out is 1 minute per year of age; use a kitchen timer with an audible bell to record the time rather than a watch.
Implement time-out in a public place by selecting a suitable area, or explain to children that time-out will be spent immediately on returning home.
Corporal or physical punishment most often takes the form of spanking (Larzelere, 2008). Based on the principles of aversive therapy, inflicting pain through spanking causes a dramatic short-term decrease in the behavior. However, this approach has serious flaws: (1) it teaches children that violence is acceptable; (2) it may physically harm the child if it is the result of parental rage; and (3) children become “accustomed” to spanking, requiring more severe corporal punishment over time. Spanking can result in severe physical and psychologic injury, and it interferes with effective parent-child interaction (Cain, 2008). In addition, when the parents are not around, children are likely to misbehave, since they have not learned to behave well for their own sake. Parental use of corporal punishment may also interfere with the child’s development of moral reasoning.
Special Parenting Situations
Parenting is a demanding task under ideal circumstances, but when parents and children face situations that deviate from “the norm,” the potential for family disruption is increased. Situations that are encountered frequently are divorce, single parenthood, blended families, adoption, and dual-career families. In addition, as cultural diversity increases in our communities, many immigrants are making the transition to parenthood and a new country, culture, and language simultaneously. Other situations that create unique parenting challenges are parental alcoholism, homelessness, and incarceration. Although these topics are not addressed here, the reader may wish to investigate them further.
Parenting the Adopted Child
Adoption establishes a legal relationship between a child and parents who are not related by birth, but who have the same rights and obligations that exist between children and their biologic parents. In the past the biologic mother alone made the decision to relinquish the rights to her child. In recent years the courts have acknowledged the legal rights of the biologic father regarding this decision. Concerned child advocates have questioned whether decisions that honor the father’s rights are in the best interests of the child. As the child’s rights have become recognized, older children have successfully dissolved their legal bond with their biologic parents to pursue adoption by adults of their choice. Furthermore, there is a growing interest and demand within the gay and lesbian (GLBT) community to adopt.
Unlike biologic parents, who prepare for their child’s birth with prenatal classes and the support of friends and relatives, adoptive parents have fewer sources of support and preparation for the new addition to their family. Nurses can provide the information, support, and reassurance needed to reduce parental anxiety regarding the adoptive process and refer adoptive parents to state parental support groups. Such sources can be contacted through a state or county welfare office.
The sooner infants enter their adoptive home, the better the chances of parent-infant attachment. However, the more caregivers the infant had before adoption, the greater the risk for attachment problems. The infant must break the bond with the previous caregiver and form a new bond with the adoptive parents. Difficulties in forming an attachment depend on the amount of time he or she has spent with caregivers early in life as well as the number of caregivers (e.g., the birth mother, nurse, adoption agency personnel).
Siblings, adopted or biologic, who are old enough to understand should be included in decisions regarding the commitment to adopt, with reassurance that they are not being replaced. Ways that the siblings can interact with the adopted child should be stressed (Fig. 3-9).

Issues of Origin
The task of telling children that they are adopted can be a cause of deep concern and anxiety. There are no clear-cut guidelines for parents to follow in determining when and at what age children are ready for the information. Parents are naturally reluctant to present such potentially unsettling news. However, it is important that parents not withhold the adoption from the child, since it is an essential component of the child’s identity (see Critical Thinking Exercise).
 CRITICAL THINKING EXERCISE
CRITICAL THINKING EXERCISE
Parenting the Adopted Child
Twelve-month-old Justin was adopted at birth. His parents tell you that they wonder when they should tell Justin that he is adopted. As the nurse, what counseling and advice should you give Justin’s parents?
1. Evidence—Is there sufficient information to draw any conclusions about this situation?
2. Assumptions—Describe some underlying assumptions about the following:
a. The best time to tell children that they are adopted
b. The manner in which parents should tell their child about adoption
3. What implications for nursing care can be drawn at this time?
The timing arises naturally as parents become aware of the child’s readiness. Most authorities believe that children should be informed at an age young enough so that, as they grow older, they do not remember a time when they did not know they were adopted. The time is highly individual, but must be right for both the parents and the child. It may be when children ask where babies come from, at which time children can also be told the facts of their adoption. If they are told in a way that conveys the idea that they were active participants in the selection process, they will be less likely to feel that they were abandoned victims in a helpless situation. For example, parents can tell children that their personal qualities drew the parents to them. It is wise for parents who have not previously discussed adoption to tell children that they are adopted before the children enter school to avoid having them learn it from third parties. Complete honesty between parents and children strengthens the relationship.
Parents should anticipate behavior changes after the disclosure, especially in older children. Children who are struggling with the revelation that they are adopted may benefit from individual and family counseling. Children may use the fact of their adoption as a weapon to manipulate and threaten parents. Statements such as “My real mother would not treat me like this” or “You don’t love me as much because I’m adopted” hurt parents and increase their feelings of insecurity. Such statements may also cause parents to become overpermissive. Adopted children need the same undemanding love, combined with firm discipline and limit setting, as any other child.
Adolescence
Adolescence may be an especially trying time for parents of adopted children. The normal confrontations of adolescents and parents assume more painful aspects in adoptive families. Adolescents may use their adoption to defy parental authority or as a justification for aberrant behavior. As they attempt to master the task of identity formation, they may begin to have feelings of abandonment by their biologic parents. Gender differences in reacting to adoption may surface.
Adopted children fantasize about their biologic parents and may feel the need to discover their parents’ identity to define themselves and their own identity. It is important for parents to keep the lines of communication open and to reassure their child that they understand the need to search for their identity. In some states, birth certificates are made legally available to adopted children when they come of age. Parents should be honest with questioning adolescents and tell them of this possibility (the parents themselves are unable to obtain the birth certificate; it is the children’s responsibility if they desire it).
Cross-Racial and International Adoption
Adoption of children from racial backgrounds different from that of the family is commonplace. In addition to the problems faced by adopted children in general, children of a cross-racial adoption must deal with physical and sometimes cultural differences. It is advised that parents who adopt children with different ethnic background do everything to preserve the adopted children’s racial heritage.
NURSING ALERT
As a health care provider, it is important not to ask the wrong questions, such as “Is she yours, or is she adopted?” “What do you know about the ‘real’ mother?” “Do they have the same father?” or “How much did it cost to adopt him?”
Although the children are full-fledged members of an adopting family and citizens of the adopted country, if they have a strikingly different appearance from other family members or exhibit distinct racial or ethnic characteristics, challenges may be encountered outside the family. Bigotry may appear among relatives and friends. Strangers may make thoughtless comments and talk about the children as though they were not members of the family. It is vital that family members declare to others that this is their child and a cherished member of the family.
In international adoptions the medical information the parents receive may be incomplete or sketchy; weight, height, and head circumference are often the only objective information present in the child’s medical record. Many internationally adopted children were born prematurely, and common health problems such as infant diarrhea and malnutrition delay growth and development. Some children have serious or multiple health problems that can be stressful for the parents.
Parenting and Divorce
Since the mid-1960s, a marked change in the stability of families has been reflected in increased rates of divorce, single parenthood, and remarriage. In 2008 the divorce rate for the United States was 3.6 per 1000 total population (Centers for Disease Control and Prevention, 2008). The divorce rate has changed little since 1987. In the decade before that, the rate increased yearly, with a peak in 1979. Although almost half of all divorcing couples are childless, it is estimated that more than 1 million children experience divorce each year.
The process of divorce begins with a period of marital conflict of varying length and intensity, followed by a separation, the actual legal divorce, and the reestablishment of different living arrangements (Box 3-6). Because a function of parenthood is to provide for the security and emotional welfare of children, disruption of the family structure often engenders strong feelings of guilt in the divorcing parents.
During a divorce, parents’ coping abilities may be compromised. The parents may be preoccupied with their own feelings, needs, and life changes and be unavailable to support their children. Newly employed parents, usually mothers, are likely to leave children with new caregivers, in strange settings, or alone after school. The parent may also spend more time away from home, searching for or establishing new relationships. Sometimes, however, the adult feels frightened and alone and begins to depend on the child as a substitute for the absent parent. This dependence places an enormous burden on the child.
Common characteristics in the custodial household after separation and divorce include disorder, coercive types of control, inflammable tempers in both parents and children, reduced parental competence, a greater sense of parental helplessness, poorly enforced discipline, and diminished regularity in household routines. Noncustodial parents are seldom prepared for the role of visitor, may assume the role of recreational and “fun” parent, and may not have a residence suitable for children’s visits. They may also be concerned about maintaining the arrangement over the years to follow.
Impact of Divorce on Children
Parental divorce is an additional childhood adversity that contributes to poor mental health outcomes, especially when combined with child abuse. Parental psychopathology may be one possible mechanism to explain the relationships between child abuse, parental divorce, and psychiatric disorders and suicide attempts (Afifi, Boman, Fleisher, et al, 2009). Even when a divorce is amicable and open, children recall parental separation with the same emotions felt by victims of a natural disaster: loss, grief, and vulnerability to forces beyond their control.
The impact of divorce on children depends on several factors, including the age and sex of the children, the outcome of the divorce, and the quality of the parent-child relationship and parental care during the years following the divorce. Family characteristics are more crucial to the child’s well-being than specific child characteristics, such as age or sex. High levels of ongoing family conflict are related to problems of social development, emotional stability, and cognitive skills for the child (see Research Focus box).
 RESEARCH FOCUS
RESEARCH FOCUS
Impact of Divorce
Children who reported that their divorced parents were cooperative had better relationships with their parents, grandparents, stepparents, and siblings (Ahrons, 2007). Complications associated with divorce include efforts on the part of one parent to subvert the child’s loyalties to the other, abandonment to other caregivers, and adjustment to a stepparent.
A major problem occurs when children are “caught in the middle” between the divorced parents. They become the message bearer between the parents, are often quizzed about the other parent’s activities, and have to listen to one parent criticize the other. A nurse may be able to help the child get out of the middle by stating “I messages” based on the formula of “I feel (state the feeling) when you (state the source). I would like it if you . . . .” An example of an “I message” is: “I do not feel comfortable when you ask me questions about mom; maybe you could ask her yourself.” This approach enables the child to feel in control.
Feelings of children toward divorce vary with age (Box 3-7). Previously, researchers believed that divorce had a greater impact on younger children, but recent observations indicate that divorce constitutes a major disruption for children of all ages. The feelings and behaviors of children may be different for various ages and gender, but all children suffer stress second only to the stress produced by the death of a parent. Although considerable research has looked at sex differences in children’s adjustments to divorce, the findings are not conclusive.
Some children feel a sense of shame and embarrassment concerning the family situation. Sometimes children see themselves as different, inferior, or unworthy of love, especially if they feel responsible for the family dissolution. Although the social stigma attached to divorce no longer produces the emotions it did in the past, such feelings may still exist in small towns or in some cultural groups and can reinforce children’s negative self-image. The lasting effects of divorce depend on the children’s and the parents’ adjustment to the transition from an intact family to a single-parent family and, often, to a reconstituted family.
Although most studies have concentrated on the negative effects of divorce on youngsters, some positive outcomes of divorce have been reported. A successful postdivorce family, either a single-parent or a reconstituted family, can improve the quality of life for both adults and children. If conflict is resolved, a better relationship with one or both parents may result, and some children may have less contact with a disturbed parent. Greater stability in the home setting and the removal of arguing parents can be a positive outcome for the child’s long term well-being.
Telling the Children: Parents are understandably hesitant to tell children about their decision to divorce. Most parents neglect to discuss either the divorce or its inevitable changes with their preschool child. Without preparation, even children who remain in the family home are confused by the parental separation. Frequently, children are already experiencing vague, uneasy feelings that are more difficult to cope with than being told the truth about the situation.
If possible, the initial disclosure should include both parents and siblings, followed by individual discussions with each child. Sufficient time should be set aside for these discussions, and they should take place during a period of calm, not after an argument. Parents who physically hold or touch their children provide them with a feeling of warmth and reassurance. The discussions should include the reason for the divorce, if age appropriate, and reassurance that the divorce is not the fault of the children.
Parents should not fear crying in front of the children, because their crying gives the children permission to cry also. Children need to ventilate their feelings. Children may feel guilt, a sense of failure, or that they are being punished for misbehavior. They normally feel anger and resentment and should be allowed to communicate these feelings without punishment. They also have feelings of terror and abandonment. They need consistency and order in their lives. They want to know where they will live, who will take care of them, if they will be with their siblings, and if there will be enough money to live on. Children may also wonder what will happen on special days such as birthdays and holidays, whether both parents will come to school events, and whether they will still have the same friends. Children fear that if their parents stopped loving each other, they could stop loving them. Their need for love and reassurance is tremendous at this time.
Custody and Parenting Partnerships
In the past, when parents separated, the mother was given custody of the children with visitation agreements for the father. Now both parents and the courts are seeking alternatives. Current belief is that neither fathers nor mothers should be awarded custody automatically. Custody should be awarded to the parent who is best able to provide for the children’s welfare. In some cases, children experience severe stress when living or spending time with a parent. Many fathers have demonstrated both their competence and their commitment to care for their children.
Often overlooked are the changes that may occur in the children’s relationships with other relatives, especially grandparents. Grandparents are increasingly involved in the care of young children (Fergusson, Maughan, and Golding, 2008). Grandparents on the noncustodial side are often kept from their grandchildren, whereas those on the custodial side may be overwhelmed by their adult child’s return to the household with grandchildren.
Two other types of custody arrangements are divided custody and joint custody. Divided custody, or split custody, means that each parent is awarded custody of one or more of the children, thereby separating siblings. For example, sons might live with the father and daughters with the mother.
Joint custody takes one of two forms. In joint physical custody, the parents alternate the physical care and control of the children on an agreed-on basis while maintaining shared parenting responsibilities legally. This custody arrangement works well for families who live close to each other and whose occupations permit an active role in the care and rearing of the children. In joint legal custody, the children reside with one parent but both parents are the children’s legal guardians, and both participate in childrearing.
Coparenting offers substantial benefits for the family: children can be close to both parents, and life with each parent can be more normal (as opposed to having a disciplinarian mother and a recreational father). To be successful, parents in these arrangements must be highly committed to provide normal parenting and to separate their marital conflicts from their parenting roles. No matter what type of custody arrangement is awarded, the primary consideration is the welfare of the children.
Single Parenting
An individual may acquire single-parent status as a result of divorce, separation, death of a spouse, or birth or adoption of a child. Although divorce rates have stabilized, the number of single-parent households continues to rise. In 2007, 32% of children younger than 18 years of age lived in single-parent families, and the majority of single parents were women (Kreider and Elliott, 2009; Annie E Casey Foundation, 2009). Although some women are single parents by choice, most never planned on being single parents, and many feel pressure to marry or remarry.
Managing shortages of money, time, and energy is often a concern for single parents. Studies repeatedly confirm the financial difficulties of single-parent families, particularly single mothers. In 2004 only one third of mother-headed households received any child support or alimony (Annie E Casey Foundation, 2009). In fact, the stigma of poverty may be more keenly felt than the discrimination associated with being a single parent. These families are often forced by their financial status to live in communities with inadequate housing and personal safety concerns. Single parents often feel guilty about the time spent away from their children. Divorced mothers, from marriages in which the father assumed the role of breadwinner and the mother the household maintenance and parenting roles, have considerable difficulty adjusting to their new role of breadwinner. Many single parents have trouble arranging for adequate child care, particularly for a sick child.
Being a teenage parent adds to the financial burden of being a single parent and can have long-term consequences for the mother and child. Poverty is a well-known predictor of adverse effects on a child’s health and well-being. Approximately 78% of children born to a teenage mother who did not marry or graduate high school live in poverty. In contrast, only 9% of children born to women over 20 who marry and finish high school live in poverty (Annie E Casey Foundation, 2009).
Social supports and community resources needed by single-parent families include health care services that are open on evenings and weekends; high-quality child care; respite child care to relieve parental exhaustion and prevent burnout; and parent enhancement centers for advancing education and job skills, providing recreational activities, and offering parenting education. Single parents need social contacts separate from their children for their own emotional growth and that of their children. Parents Without Partners, Inc.,* is an organization designed to meet the needs of single parents.
Single Fathers
Fathers who have custody of their children have many of the same problems as divorced mothers. They feel overburdened by the responsibility; depressed; and concerned about their ability to cope with the emotional needs of the children, especially girls. Some fathers lack home-making skills. They may find it difficult at first to coordinate household tasks, school visits, and other activities associated with managing a household alone.
Parenting in Reconstituted Families
In the United States, many of the children living in homes where parents have divorced will experience another major change in their lives such as the addition of a stepparent or new siblings (Hanson, Gedaly-Duff, and Kaakinen, 2005). The entry of a stepparent into a ready-made family requires adjustments for all family members. Some obstacles to the role adjustments and family problem solving include disruption of previous lifestyles and interaction patterns, complexity in the formation of new ones, and lack of social supports. Despite these problems, most children from divorced families want to live in a two-parent home.
Cooperative parenting relationships can allow more time for each set of parents to be alone to establish their own relationship with the children. Under ideal circumstances, power conflicts between the two households can be reduced, and tension and anxiety can be lessened for all family members. In addition, the children’s self-esteem can be increased, and there is a greater likelihood of continued contact with grandparents. Flexibility, mutual support, and open communication are critical in successful relationships in stepfamilies and stepparenting situations.
Parenting in Dual-Earner Families
No change in family lifestyle has had more impact than the large numbers of women moving away from the traditional homemaker role and entering the workplace (Hanson, Gedaly-Duff, and Kaakinen, 2005). The trend toward increased numbers of dual-earner families is unlikely to diminish significantly. As a result, the family is subject to considerable stress as members attempt to meet often competing demands of occupational needs and those regarded as necessary for a rich family life.
Role definitions are frequently altered to arrange a more equitable division of time and labor, as well as to resolve conflict, especially conflict related to traditional cultural norms. Overload is a common source of stress in a dual-earner family, and social activities are significantly curtailed. Time demands and scheduling are major problems for all individuals who work. When the individuals are parents, the demands can be even more intense. Dual-earner couples may increase the strain on themselves to avoid creating stress for their children. Although there is no evidence to indicate that the dual-earner lifestyle is stressful to children, the stress experienced by the parents may affect the children indirectly.
Working Mothers
Working mothers have become the norm in the United States. Maternal employment may have variable effects on preschool children’s health (Mindlin, Jenkins, and Law, 2009). The quality of child care is a persistent concern for all working parents (see Evidence-Based Practice box). Determinants of child care quality are based on health and safety requirements, responsive and warm interaction between staff and children, developmentally appropriate activities, trained staff, limited group size, age-appropriate caregivers, adequate staff-to-child ratios, and adequate indoor and outdoor space. Nurses play an important role in helping families find suitable sources of child care and prepare children for this experience (see Alternate Child Care Arrangements, Chapter 10).
Foster Parenting
The term foster care is defined as placement in an approved living situation away from the family of origin (Annie E Casey Foundation, 2009; American Academy of Pediatrics, 2000). The living situation may be an approved foster home, possibly with other children, or a preadoptive home. Each state provides a standard for the role of foster parent and a process by which to become one. These “parents” contract with the state to provide a home for children for a limited duration. Most states require about 27 hours of training before being on contract and at least 12 hours of continuing education a year. Foster parents may be required to attend a foster parent support group that is often separate from a state agency. Each state has guidelines regarding the relative health of the prospective foster parents and their families, background checks regarding legal issues for the adults, personal interviews, and a safety inspection of the residence and surroundings (Chamberlain, Price, Leve, et al, 2008).
Foster homes include both kinship and nonrelative placements. Since the 1980s, the proportion of children in out-of-home care placed with relatives has increased rapidly and been accompanied by a decrease in the number of foster families. As with their nonfoster counterparts, much of the child’s adjustment depends on the family’s stability and available resources. Even though foster homes are designed to provide short-term care, it is not unusual for children to stay for many years.
Nurses should be aware that nearly 700,000 children spend time living in foster care in a given year, many of them facing developmental concerns (Annie E Casey Foundation, 2009; American Academy of Pediatrics, 2000). Children from lower-income, single-mother, and mother-partner families are considerably more likely to be living in foster care (Berger and Waldfogel, 2004). Children in foster care tend to have a higher than normal incidence of acute and chronic health problems and may experience feelings of isolation or confusion (Annie E Casey Foundation, 2009). Foster children are often at risk because of their previous caretaking environment. Nurses should strive to implement strategies to improve the health care for this group of children. In particular, assessment and case management skills are required to involve other disciplines in meeting their needs.
Accommodating Contemporary Parenting Situations
During recent years, both the private and government sectors have identified specific problems of contemporary families. Many of these issues involve working parents. One significant stressor for the working single parent or for dual-earner families is when a child becomes ill. The frequency of childhood illness, exclusion practices of most licensed child care programs, and employer’s limited sick-leave policies are other contributing factors. Most authorities agree that a familiar face and place are important components of sick-child care, and some argue that the only place for an ill child is at home with a parent or other relative.
Some employers have become more family focused and provide time off for parents to be with sick children. Increasing numbers are becoming more generous in the amount of time they allow parents (fathers as well as mothers) to remain at home after the birth or adoption of a child. Flexible work schedules and family-oriented legislation can ease the burden of managing family and work responsibilities. The passage of the Family and Medical Leave Act (FMLA) in 1993 set the stage for a greater focus on the issues of contemporary families. FMLA allows eligible employees to take up to 12 weeks of unpaid leave each year to care for newborn or newly adopted children, parents, or spouses who have serious health conditions, or to recover from their own serious health condition.
Key Points
• Because there is no agreement about the definition of family, a family is what an individual considers it to be.
• Three theories that have significant application to pediatric nursing are family systems theory, family stress theory, and developmental theory.
• Although the traditional family structure is nuclear or extended, in recent years other forms, such as the single-parent family, have become more prominent.
• Family size and position within the family structure have a strong impact on a child’s development.
• Interpersonal skills and a basic understanding of childhood growth and development are two essential areas of focus for parents.
• Parental control tends to be predominantly one of three types: authoritarian, permissive, or authoritative.
• Three areas of special concern to adoptive families include the initial attachment process, the task of telling the children they are adopted, and identity formation during adolescence.
• Marital factors within the home significantly influence a child’s development. The impact of divorce on a child depends on the child’s age, the outcome, and the quality of the parent-child relationship and parental care following the divorce.
• Single parenting and stepparenting create adjustment difficulties and add stress to the already demanding parental role. Significant numbers of children will live in a single-parent or reconstituted family at some point.
Answers to Critical Thinking Exercise
1. Yes. Although there is no one best time to tell children they are adopted, most authorities believe that children should be informed before they enter school to avoid learning about it from third parties. In addition, authorities agree that children should be told at an age young enough so that, as they grow older, they do not remember a time when they did not know they were adopted.
2. a.The best time is highly individualized and based on the child’s readiness. For some children, this may be when they ask about where babies come from. Children have a more difficult adjustment if disclosure occurs when they are older, and waiting until adolescence is too late.
b Parents should be completely honest with the child and provide information about the adoption in a matter-of-fact way. Sharing the story of adoption is an important parental responsibility and can be handled much like a parent shares birth experiences with a biologic child.
c Parents should anticipate that children may act out after being told that they are adopted. Some children use the fact of their adoption as a weapon to manipulate and threaten their parents. Allowing children to express their feelings and emotions after they have been told about their adoption is important.
3. Because Justin’s parents have requested guidance, it is appropriate for you, as the nurse, to provide information about how and when they should tell Justin he is adopted. However, the nurse’s first priority is to be certain that Justin’s parents are comfortable with this information, and that they feel free to ask any further questions and to obtain additional information. Because Justin is only 12 months old, his parents have time to think about how they will present this information to Justin and to prepare for the disclosure. They also have time to discuss how they will react to the feelings, emotions, and behaviors that Justin may demonstrate after he learns he is adopted.
4. Yes, at the present time, most authorities agree that children should be told about the fact that they are adopted, and that disclosure of this information should occur before the school-age years.
References
Afifi, TO, Boman, J, Fleisher, W, et al. The relationship between child abuse, parental divorce, and lifetime mental disorders and suicidality in a nationally representative adult sample. Child Abuse Negl. 2009;33(3):139–147.
Ahrons, CR. Family ties after divorce: long-term implications for children. Family Process. 2007;46(1):53–65.
American Academy of Pediatrics. Family pediatrics: report of the Task Force on the Family. Pediatrics. 2003;111(6):1541–1571.
American Academy of Pediatrics, Committee on Early Childhood, Adoption, and Dependent Care. Development issues for young children in foster care (RE0012). Pediatrics. 2000;106(5):1145–1150.
Annie, E, Casey Foundation. 2009 Kids count data book: state profiles of child well-being. Baltimore: The Foundation; 2009.
Berger, L, Waldfogel, J. Out-of-home placement of children and economic factors: an empirical analysis. Rev Econo Household. 2004;2(4):387–411.
Blackwell, CW. Belief in the “free choice” model of homosexuality: a correlate of homophobia in registered nurses. J LGBT Health Res. 2007;3(3):31–40.
Bomar, PJ. Promoting health in families, ed 3. Philadelphia: Saunders; 2004.
Cain, DS. Parenting online and lay literature on infant spanking: information readily available to parents. Soc Work Health Care. 2008;47(2):174–184.
Centers for Disease Control and Prevention. Births marriages, divorces, and deaths: provisional date for February 2008. Natl Vital Stat Rep. 2008;57(5):1–6.
Chamberlain, P, Price, J, Leve, LD, et al. Prevention of behavior problems for children in foster care: outcomes and mediation effects. Prev Sci. 2008;9(1):17–27.
Deave, T, Johnson, D, Ingram, J. Transition to parenthood: the needs of parents in pregnancy and early parenthood. BMC Pregnancy Childbirth. 2008;29(8):30.
Duvall, ER. Family development, ed 5. Philadelphia: Lippincott; 1977.
Fergusson, E, Maughan, B, Golding, J. Which children receive grandparental care and what effect does it have? Child Psychol Psychiatry. 2008;49(2):161–169.
Fisher, C, Lindhorst, H, Matthews, T, et al. Nursing staff attitudes and behaviors regarding family presence in the hospital setting. J Adv Nurs. 2008;64(6):615–624.
Friedman, MM, Bowden, VR, Jones, EG. Family nursing: research theory and practice, ed 5. Upper Saddle River, NJ: Prentice Hall; 2003.
Goldenberg, I, Goldenberg, H. Family theory: an overview, ed 7. Pacific Grove, Calif: Brooks-Cole Cengage Learning; 2008.
Hamilton, BE, Minino, AM, Martin, JA, et al. Annual summary of vital statistics: 2005. Pediatrics. 2007;119(2):345–360.
Hanson, SMH, Gedaly-Duff, V, Kaakinen, JR. Family health care nursing, ed 3. Philadelphia: Davis; 2005.
Hoeve, M, Dubas, JS, Eichelsheim, VI, et al. The relationship between parenting and delinquency: a meta-analysis. J Abnorm Child Psychol. 2009;37(6):749–775.
Hubbs-Tait, L, Kennedy, TS, Page, MC, et al. Parental feeding practices predict authoritative, authoritarian, and permissive parenting styles. J Am Diet Assoc. 2008;108(7):1154–1161.
Kreider, RM, Elliott, DB. America’s families and living arrangements: 2007. In: US Census Bureau: Current population reports. Washington, DC: The Bureau; 2009.
Larzelere, RE. Disciplinary spanking: the scientific evidence. J Dev Behav Pediatr. 2008;29(4):334–335.
Liddle, HA, Santisteban, DA, Levant, RF, et al. Family psychology. Washington, DC: American Psychological Association; 2002.
Martin, JA, Kung, KC, Mathews, TJ, et al. Annual summary of vital statistics: 2006. Pediatrics. 2008;121(4):788–801.
McCubbin, MA, McCubbin, HI. Families coping with illness: the resiliency model of family stress, adjustment, and adaptation. In: Danielson CB, Bissel BH, Winstead-Fry P, eds. Families, health, and illness. St. Louis: Mosby, 1994.
Mindlin, M, Jenkins, R, Law, C. Maternal employment and indicators of child health: a systemic review in pre-school children in OECD countries. J Epidemiol Commun Health. 2009;63(5):340–350.
Pawelski, JG, Perrin, EC, Foy, JM, et al. The effects of marriage, civil union, and domestic partnership laws on the health and well-being of children. Pediatrics. 2006;118(1):349–364.
Power, N, Franck, L. Parent participation in the care of hospitalized children: a systematic review. J Adv Nurs. 2008;62(6):622–641.
*For information, contact the local AARP representative or office; www.aarp.org/family/grandparenting.
*NOMOTC Executive Office, 2000 Mallory Lane, Suite 130-600, Franklin, TN 37067; www.nomotc.org.
*For parenting of kindergarten through sixth grade children, see http://childparenting.about.com and www.kidshealth.org.
*1650 South Dixie Hwy, Suite 402, Boca Raton, FL 33432; 800-637-7974; http://parentswithoutpartners.org.