Health Promotion of the School-Age Child and Family

http://evolve.elsevier.com/wong/ncic

Dental Health, Ch. 14
Eating Disorders, Ch. 21
Health Problems of Middle Childhood, Ch. 18
Injuries and Health Problems Related to Sports Participation, Ch. 39
Injuries—the Leading Killer, Ch. 1
Limit Setting and Discipline, Ch. 3
Nutrition, Ch. 13
Physical and Developmental Assessment of the Child, Ch. 6
Psychosocial History, Ch. 6
Sleep Problems, Chs. 12 and 15
Television, Ch. 2
Promoting Optimum Growth and Development
The segment of the life span that extends from age 6 years to approximately age 12 years has a variety of labels, each of which describes an important characteristic of the period. The middle years are most often referred to as school age or the school years. This period begins with entrance into the wider sphere of influence represented by the school environment, which has a significant impact on development and relationships.
Physiologically the middle years begin with the shedding of the first deciduous tooth and end at puberty with the acquisition of the final permanent teeth (with the exception of the wisdom teeth). In the 5 to 6 years before the school-age period, children progressed from helpless infants to sturdy, complicated individuals with the capacity to communicate, conceptualize in a limited way, and become involved in complex social and motor behavior. Physical growth was been equally rapid. In contrast, the period of middle childhood— between the rapid growth of early childhood and the prepubescent growth spurt—is a time of gradual growth and development, with more even progress in both physical and emotional aspects.
Biologic Development
During middle childhood, growth in height and weight assumes a slower but steady pace compared with the earlier years. Between the ages of 6 and 12 years, children grow an average of 5 cm (2 inches) per year to gain 30 to 60 cm (1 to 2 feet) in height and will almost double in weight, increasing 2 to 3 kg (4.4 to 6.6 lb) per year. The average 6-year-old child is about 116 cm (46 inches) tall and weighs about 21 kg (46.3 lb); the average 12-year-old child stands about 150 cm (59 inches) tall and weighs approximately 40 kg (88.2 lb). During this age period girls and boys differ little in size, although boys tend to be slightly taller and somewhat heavier than girls. Toward the end of the school-age years both boys and girls begin to increase in size, although most girls begin to surpass boys in both height and weight, to the acute discomfort of both sexes.
Physical Changes
School-age children are more graceful than they were as preschoolers, and they are steadier on their feet. Their bodies take on a slimmer look with longer legs, varying body proportions, and a lower center of gravity. Posture improves over that of the preschool period to facilitate locomotion and efficiency in using the arms and trunk. These proportions make climbing, bicycle riding, and other activities much easier. Fat gradually diminishes, and its distribution patterns change, which contributes to the thinner appearance of children during the middle years.
Accompanying the skeletal lengthening and fat diminution is an increase in the percentage of body weight represented by muscle tissue. By the end of this age period, both boys and girls have doubled their strength and physical capabilities, and their steady and relatively consistent acquisition of refined coordination increases their poise and skill. However, this increased strength is often misleading. Although strength increases, muscles are still functionally immature when compared with those of the adolescent, and they are more readily injured by overuse.
The most pronounced changes that seem best to indicate increasing maturity in children are a decrease in head circumference in relation to standing height, a decrease in waist circumference in relation to height, and an increase in leg length related to height. These indicators often provide a clue to a child’s degree of maturity and have proved useful in predicting readiness for meeting the demands of school. There appears to be a correlation between physical indicators of maturity and success in school.
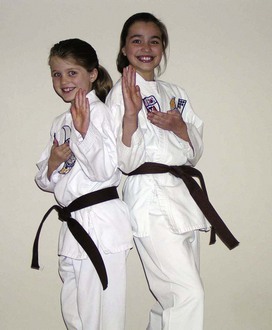
Certain physiologic and anatomic characteristics are typical of school-age children. Facial proportions change as the face grows faster in relation to the remainder of the cranium. The skull and brain grow very slowly during this period and increase little in size thereafter. Because all of the primary (deciduous) teeth are lost during this age span, middle childhood is sometimes known as the age of the loose tooth (Fig. 17-1) and the early years of middle childhood as the ugly duckling stage, when the new secondary (permanent) teeth appear to be much too large for the smaller face.

Maturation of Systems
As the gastrointestinal system matures, the child has fewer stomach upsets; better maintenance of blood sugar levels; and an increased stomach capacity, which permits retention of food for longer periods. The school-age child does not need to be fed as carefully, as promptly, or as frequently as before. Caloric needs are lower than they were in the preschool years and lower than they will be during the coming adolescent growth spurt.
Physical maturation occurs in other body tissues and organs. Bladder capacity, although differing widely among individual children, is generally greater in girls than in boys. There are individual variations in frequency of urination and differences in the same child according to circumstances such as temperature, humidity, time of day, amount of fluids ingested, and emotional state.
The heart grows more slowly during the middle years and is smaller in relation to the rest of the body than at any other period of life. Heart and respiratory rates steadily decrease, and blood pressure increases between ages 6 to 12 (see inside back cover).
The immune system becomes more competent in its ability to localize infections and produce an antibody-antigen response. Because of increased exposure to others in school classes, children can have several infections in the first 1 to 2 years of school while immunity develops.
Bones continue to ossify throughout childhood, but because mineralization is not completed until maturity, children’s bones resist pressure, and muscles pull less than with mature bones. Consequently, parents must be careful to prevent alterations in bone structure and provide children with well-fitted shoes and with chairs and desks that allow correct sitting posture with the feet able to reach the floor and the hips able to fit well back in the seat. Children should have ample opportunity to move around and be cautious about carrying heavy loads. For example, they should shift books and/or tote bags from one arm to the other. Back packs, when worn correctly, distribute weight more evenly.
Wider differences between children are seen at the end of middle childhood than at the beginning; such differences are sometimes striking. These differences become increasingly apparent and, if extreme or unique, may create emotional problems. The nurse should explain the associated characteristics of height and weight relationships, rapid or slow growth, and other important features of development to children and their families. Physical maturity is not necessarily correlated with emotional and social maturity. Seven-year-old children who look like 10-year-old children will think and act like 7-year-olds. To expect behavior appropriate for 10-year-old children from them is unrealistic and can be detrimental to their development of competence and self-esteem. Conversely, to treat 10-year-old children as though they were 7 years old is an equal disservice to them.
Prepubescence
Preadolescence is the period that begins toward the end of middle childhood and ends with the thirteenth birthday. Puberty signals the beginning of the development of secondary sex characteristics, and prepubescence, the 2-year period that precedes puberty, typically occurs during preadolescence.
Toward the end of middle childhood the discrepancies in growth and maturation between boys and girls become apparent. On the average, there is a difference of approximately 2 years between girls and boys in the age of onset of pubescence. For many, especially for girls, preadolescence is a period of rapid growth. For others, mostly boys, it is generally a period of continued steady growth in height and weight.
There is no universal age at which children assume the characteristics of preadolescence. The first physiologic signs appear at about 9 years (particularly in girls) and are usually clearly evident in 11- to 12-year-old children. Although preadolescent children do not want to be different, variability in physical growth and physiologic changes among children of the same sex, and between the two sexes, is often striking at this time. This variability, especially in relation to the onset of secondary sex characteristics, is of utmost concern to the preadolescent. Either early or late appearance of these characteristics is a source of embarrassment and uneasiness to both sexes. Early appearance of secondary sex characteristics in girls is often associated with dissatisfaction with physical appearance, greater general unhappiness, and lower self-esteem. Late-developing boys often have a negative self-concept. Both early appearance of physical characteristics in girls and late appearance in boys have been linked to participation in risk-taking behaviors (early sexual activity, substance use, and reckless vehicle use).
Preadolescence is a time when considerable overlapping of developmental characteristics occurs, with elements of both middle childhood and early adolescence apparent. However, there are sufficient unique characteristics to set this period apart as an age category. Generally, puberty begins no earlier than 10 years in girls and 12 years in boys, but its onset in either sex after the age of 8 years is considered normal. The average age of puberty is 12 years in girls and 14 years in boys. Boys experience little sexual maturation during preadolescence.
Psychosocial Development
Middle childhood is the period of psychosexual development that Freud described as the latency period, a time of tranquility between the oedipal phase of early childhood and the eroticism of adolescence. During this time children experience relationships with same-sex peers following the indifference of earlier years and preceding the heterosexual fascination that occurs for most boys and girls in puberty.
Developing a Sense of Industry (Erikson)
Successful mastery of Erikson’s first three stages of psychosocial development is probably the most important accomplishment in terms of development of a healthy personality (Erikson, 1963). Successful completion of these stages requires a loving environment within a stable family unit that has prepared the child to engage in experiences and relationships beyond this intimate group. During childhood, children affiliate with age-mates, receive the systematic instruction prescribed by their individual cultures, and develop the skills needed to become useful, contributing members of their social communities.
A sense of industry, or a stage of accomplishment, occurs somewhere between age 6 years and adolescence. The goal of this stage of development is to achieve a sense of personal and interpersonal competence through the acquisition of technologic and social skills. School-age children are eager to build skills and participate in meaningful and socially useful work. Interests expand, and, with a growing sense of independence, children want to engage in tasks that they can complete (Fig. 17-2). Failure to develop a sense of accomplishment may result in a sense of inferiority.

Fig. 17-2 School-age children are motivated to complete tasks. A, Working alone. B, Working with others.
Many aspects of industry contribute to the child’s sense of competence and mastery. Intrinsic motivation is associated with increased competence in mastering new skills and assuming new responsibilities. Children gain a great deal of satisfaction from independent behavior in exploring and manipulating their environment and from interaction with peers. Extrinsic sources of reinforcement in the form of grades, material rewards, additional privileges, and recognition provide encouragement and stimulation. Often the acquisition of skills is a means for achieving success in special activities such as athletics or social organizations. Peer approval is a strong motivating factor.
The danger inherent in this period of personality development is the occurrence of situations that might result in a sense of inadequacy or inferiority. This may happen if the previous stages have not been successfully mastered or if a child is incapable of or unprepared to assume the responsibilities associated with developing a sense of accomplishment. Feelings of inferiority or lack of worth come from children themselves or from the social environment. Children with physical or mental limitations are sometimes at a disadvantage for acquisition of certain skills. When the reward structure is based on evidence of mastery, children who are incapable of developing these skills are at risk for feeling inadequate and inferior.
Even children without chronic disabilities show such a wide range of individual differences in capabilities and preferences that they experience feelings of inadequacy in some areas. No child is able to do well in everything, and children must learn that they will not be able to master each skill that they attempt. All children, even children who in most instances have positive attitudes toward work and their own capabilities, feel some degree of inferiority in regard to a specific skill that they cannot master.
For some children, success or aptitude in one area may compensate for failure or ineptitude in another. However, the differences in reinforcement provided for success in various areas have significant effects on feelings of adequacy. For example, in the United States, reading proficiency is more highly rewarded than the mechanical aptitude needed for tinkering with broken automobile engines. Society places a higher value on success in team sports than on success in repairing a bicycle. Compensating for the inability to excel in more socially valued skills through mastery of other, less valued skills is difficult for children. If the social environment places a negative value on any failure, feelings of inferiority may be increased in the less capable child. Repeated failures can generate such strong feelings that eventually the child is reluctant to attempt any new task or is fearful of not being able to perform as well as his or her peers. Thus intrinsic motivation toward engaging in a task for the pleasure of the challenge conflicts with the external forces that cause feelings of doubt and inferiority. Consequently, the child may no longer try.
A child’s concept of success or failure is important. Children who aspire to more than they are capable of usually experience failure. In contrast, children who set their aspirations lower than their level of achievement are likely to experience success. Most accomplishments during the school years are very public. Family, teachers, and peers are all aware of success or failure in school. In school and sometimes at home, feelings of inferiority may be produced through comparisons with others that suggest the child is not as good as a peer, sibling, or member of another group. This inadequacy becomes a source of embarrassment. The child may even be shamed for the failure. Earlier conflicts of doubt and guilt are closely associated with feelings of inferiority.
A sense of accomplishment also involves the ability to cooperate, to compete with others, and to cope effectively with people. Middle childhood is the time when children learn the value of doing things with others and the benefits derived from division of labor in the accomplishment of goals. Children need and want real achievement. When they can accomplish tasks that need to be done and perform well despite individual differences in capacities and emotional development, and when they are suitably rewarded, children develop a sense of industry and accomplishment that prepares them for establishing a stable identity later in life.
Temperament
The reactivity patterns or temperamental traits identified in infancy may continue to influence behavior in middle childhood. Analyzing behavioral patterns observed in past situations can provide clues to the way that a child may react to new situations, although long-range projections are not always successful. Through interaction with the environment, experiences, motives, and abilities, many children change. In some children major temperamental characteristics persist into adolescence; in others they do not.
Many children tend to be identified with one of three broad temperament categories: easy, slow to warm up, and difficult. Parents and teachers are in an excellent position to assess a child’s behavioral style and to try to make their demands and expectations consonant with the individual child’s temperamental characteristics. With easy children this rarely poses a problem. They adapt readily to many childrearing programs and new situations. School entry and other changes usually go smoothly and are accomplished with minimal stress. Difficulties arise with children who are slow to warm up or are difficult or easily distracted.
Slow-to-warm-up children usually exhibit discomfort when introduced to new situations and need time to become accustomed to a new environment, authority figures, and expectations. These children may respond with tears, somatic complaints, or other maneuvers to avoid the event. The nurse should encourage them to try new experiences but allow them to adapt to their surroundings at their own speed. Pressure to move quickly into new situations only strengthens the tendency to withdraw. After-school activities can be a cause for reaction, but attending with a friend or contracting for permission to withdraw after a trial of a specified number of times may provide them with sufficient incentive to try (see Critical Thinking Exercise).
 CRITICAL THINKING EXERCISE
CRITICAL THINKING EXERCISE
Temperament in the School-Age Child
Mary’s teacher asks the school nurse for guidance. Mary is 8 years old and has just entered the third grade. In the classroom Mary is quiet and passive, and she frequently cries when the teacher talks with her. Mary’s mother describes her daughter as a healthy child who has always required more time and effort to adapt to changes in her routine. In counseling Mary’s teacher, what should the nurse encourage the teacher to do?
1. Evidence—Is there sufficient evidence to draw any conclusions about Mary’s behavior?
2. Assumptions—Describe the underlying assumptions about each of the following:
a. Factors and timing related to establishment of a child’s temperament
b. Ease or difficulty of adapting to new situations in relation to temperament
c. Helping the slow-to-warm-up child adjust to new situations
3. What priorities for nursing care can be drawn from this situation?
Difficult or easily distracted children may benefit from “practice” sessions in which they are prepared for a given event by role playing, visiting the site, or reading or listening to stories, or use of other methods to acquaint them with what to expect. Children who are persistent need to know when to stop what they are doing so that the signal to stop will not come as a surprise or trigger a reaction. Nurses need to handle children with difficult temperaments with exceptional patience, firmness, and understanding so that they can learn appropriate behavior in their interactions with others. If possible, teachers’ styles and characteristics should match the temperament of children to ensure a good fit.
Cognitive Development (Piaget)
When they enter the school years, children begin to acquire the ability to relate a series of events and actions to mental representations that they can express both verbally and symbolically. This is the stage that Piaget describes as concrete operations, when children are able to use their thought processes to experience events and actions. The term operation implies an action that is performed on an object or set of objects; thus a mental operation is an alteration or transformation that an individual carries out in thought rather than in action. Toddlers or preschool children can perform acts that involve ordering, such as correctly arranging a graduated set of circles from largest to smallest on a stick, and can find their way to a friend’s house, but they are unable to verbalize the actions involved in the process. School-age children are able to articulate the process and perform the actions mentally without the need to carry out the behaviors.
As children move from the preschool years into the school years, their conceptual abilities become increasingly flexible. During the concrete operational period, they acquire the ability to perform cognitive operations and apply these new skills when thinking about objects, situations, and events. Their rigid, egocentric outlook is replaced by thought processes that allow them to see things from another’s point of view. They become aware of a variety of perspectives and become more sensitive to the fact that others do not always perceive events exactly as they do. They are able to delay an action until they have evaluated alternative responses to situations. Their steady reduction in egocentricity helps form the basis for logical thought and the development and maturation of morality.
The concrete operational stage occurs between the ages of 7 and 11 years. During this stage children develop an understanding of relationships between things and ideas. They progress from making judgments based on what they see (perceptual thinking) to making judgments based on what they reason (conceptual thinking). They are increasingly able to master symbols and to use their memory store of past experiences to evaluate and interpret the present.
One of the major cognitive tasks of school-age children is mastering the concept of conservation—that physical matter does not appear and disappear by magic. They learn that certain properties of the environment are not changed simply by altering their disposition in space. They are able to resist perceptual cues that suggest alterations in the physical state of an object.
The nurse can use commonplace items to demonstrate the conservation of liquid, mass, number, length, area, and volume (Fig. 17-3). To explain the observation that the mass of the clay in the figure has not been altered, children use one of three concepts:
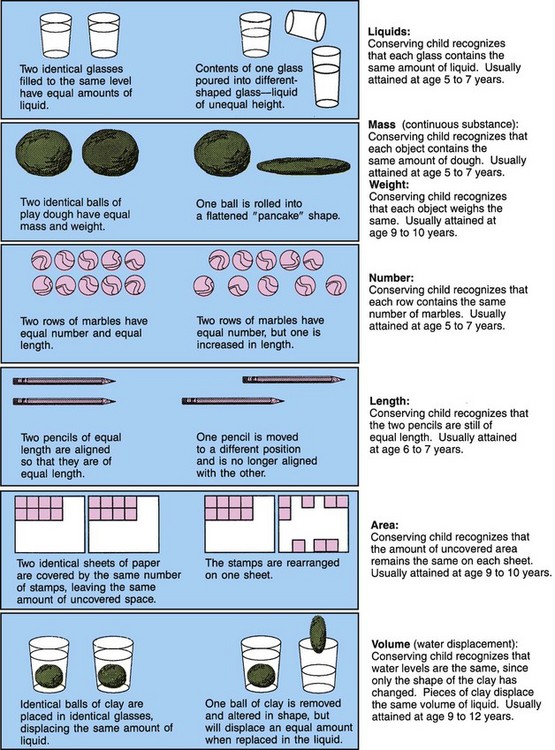
1. Identity—Because nothing has been added and nothing has been taken away, the pancake is still the same clay. Nothing has changed but the shape.
2. Reversibility—The clay can be reshaped into its original form (a ball).
3. Reciprocity—Although the pancake appears larger in circumference, the ball is much thicker. In this instance the child demonstrates the ability to deal with two dimensions at the same time and to comprehend that a change in one dimension compensates for a change in another.
When children are able to use the concepts of identity, reversibility, and reciprocity, they can conserve along any physical dimension. They perceive the concept of volume in relation to container size and shape, recognize that size is not necessarily related to weight or volume, and are able to manipulate or “see” in a concrete manner. They recognize that logical operations move in two directions (such as addition and subtraction or multiplication and division) and that certain properties are invariant (e.g., 7 remains 7 whether it is represented by 3 + 4, 2 + 5, seven buttons, seven stars, or seven boys).
There appears to be a developmental sequence in children’s capacity to conserve matter. Children usually grasp conservation of numbers (ages 5 to 6) before conservation of substance. Conservation of liquids, mass, and length usually is accomplished at about ages 6 to 7, conservation of weight sometime later (ages 9 to 10), and conservation of volume or displacement last (ages 9 to 12).
Children use reversibility in selecting a course of action, which thus provides greater control over themselves and their environment. They have the ability to think through an action sequence, anticipate the consequences, and, if needed, return to the beginning and rethink the action in a different direction. They no longer need to experience an action before they can anticipate the results. Reversibility allows mental action and enables children to disassemble and reassemble certain kinds of things in their thoughts.
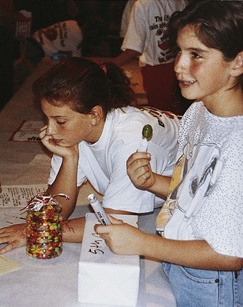
Classification skills involve the ability to group objects according to the attributes that they have in common. School-age children can place things in a sensible and logical order, group and sort, and hold a concept in their minds while they make decisions based on that concept. In middle childhood children get a great deal of enjoyment from classifying and ordering their environment. They become occupied with numerous and varied collections of objects, such as stamps, shells, dolls, cars, stones, cards, stuffed animals, and anything that is classifiable (Fig. 17-4). They even begin to order friends and relationships (e.g., first best friend, second best friend).

As children mature, they progress from collecting simply for the sake of collecting and become more selective and discriminating. Their classification systems become more complex and are based on abstract ideas rather than on perception and experience. Much of the pleasure of collections is in the appraising, ordering, and reordering of the parts.
School-age children are able to serialize, or to arrange objects according to some ordinal scale or quantified dimension such as size, weight, or color. They develop the ability to understand relational terms and concepts, such as bigger and smaller; darker and paler; heavier and lighter; to the right of and to the left of; first, last, and intermediate (e.g., fourth, second); and more than and less than. They can see family relationships in terms of reciprocal roles; for example, to be a brother, one must have a sibling.
During the school-age years children develop combinatorial skills—the ability to manipulate numbers and to learn the skills of addition, subtraction, multiplication, and division. They learn to apply the basic operations to any object or quantity. They learn the alphabet and the ever-widening world of symbols called words that can be arranged in terms of structure and their relationship to the alphabet. They learn to tell time, to see the relationship of events in time (history) and places in space (geography), and to combine time and space relationships (geology and astronomy).
The most significant skill, the ability to read, is acquired during the school years and becomes the most valuable tool for independent inquiry. Children’s capacity for exploration, imagination, and expansion of knowledge is enhanced by the ability to read as they progress from the repetition and confusion of early efforts to increasing facility and comprehension. Formal academic learning begins at ages 5 to 6 years, when children’s intellectual capabilities and cognitive processes allow them to attain intellectual achievements.
Moral Development (Kohlberg)
As children move from egocentrism to more logical patterns of thought, they also move through stages in the development of conscience and moral standards. Young children do not believe that standards of behavior come from within themselves but that others establish and enforce these rules. During preschool years, children perceive rules as definite and require no reason or explanation. Children learn the standards for acceptable behavior, act according to these standards, and feel guilty when they violate the standards. Although children 6 or 7 years old know the rules and what they are supposed to do, they do not understand the reasons behind them. Young children usually judge an act by its consequences. Rewards and punishment guide their judgment; a “bad” act is one that breaks a rule or causes harm. When a child and an adult differ in judging an act, the adult is right. Children may believe that what other people tell them to do is right and that what they themselves think is wrong. Consequently, children 6 or 7 years old are more likely to interpret accidents and misfortunes as punishment for misdeeds or “bad” acts.
Older school-age children are able to judge an act by the intentions that prompted it rather than just by the consequences. Rules and judgments become less absolute and authoritarian and begin to be founded more on the needs and desires of others. Rules of conduct are more readily considered in terms of mutual agreement and are based on cooperation and respect for others. Older children will likely view a rule violation in relation to the total context in which it appears; reactions are influenced by the situation as well as by the morality of the rule itself. However, it is not until adolescence or beyond that children are able to view morality on an abstract basis with sound reasoning and principled thinking. Although younger children can judge an act only according to whether it is right or wrong, older children take into account a different point of view to make a judgment. They are able to understand and accept the concept of treating others as they would like to be treated.
Spiritual Development
Children at this age think in very concrete terms but are avid learners and have a great desire to learn about their God or deity. They picture God as human and use adjectives such as “loving” and “helping” to describe their deity. They are fascinated by heaven and hell and, with a developing conscience and concern about rules, they fear going to hell for misbehavior. School-age children want and expect to be punished for misbehavior and, if given the option, tend to choose a punishment that “fits the crime.” Often they view illness or injury as a punishment for a real or imagined misdeed. The beliefs and ideals of family and religious personages are more influential than those of their peers in matters of faith.
School-age children begin to learn the difference between the natural and the supernatural but have difficulty understanding symbols. Consequently, religious concepts must be presented to them in concrete terms. They try to relate phenomena in the world in a logical, systematic manner, which is both satisfying and occasionally disheartening. Religion is a means whereby children can relate to their deity in a direct and personal way.
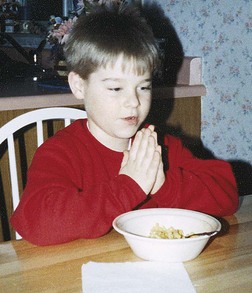
Prayer and other religious rituals are often a comfort to children, and if these activities are a part of children’s daily lives, they can help children cope with threatening situations (Fig. 17-5). Their petitions to their God in prayers tend to be for tangible rewards. Although younger children expect their prayers to be answered, as children get older they begin to recognize that this does not always occur and become less concerned when prayers are not answered. They are able to discuss their feelings about their faith and how it relates to their lives (see Cultural Competence box).
 CULTURAL COMPETENCE
CULTURAL COMPETENCE
Religious Orientation
Many schools and communities have a Judeo-Christian orientation toward prayer, holidays, and values. This may result in conflict and discomfort for children of other religious and ethnic groups. Schools should exercise sensitivity so as not to offend and confuse children from other religious backgrounds, such as the Buddhist, Hindu, and Muslim faiths.
Language Development
Children enter middle childhood with remarkably efficient language skills, but they make many important linguistic achievements during the school-age years. During the elementary school years they learn to correct previous syntactic errors and begin to use more complex grammatical forms, such as correct past tenses for irregular verbs, correct plurals for irregular nouns, and correct personal pronouns.
Word usage and the ability to find and retrieve words quickly when called on to produce what they know in a relatively short time grow considerably during the school years. Children learn to apply the minimum-distance principle—the rule that the subject of a verb in an active sentence is the noun or pronoun that immediately precedes it. For example, a 6-year-old child will understand the sentence “Ask Mary her last name” but until age 9 or 10 years will be confused by the sentence “Ask Mary what to bring to the party.”
Narrative skills improve markedly. School-age children are increasingly able to provide directives that others can correctly interpret without visual data (e.g., explain directions over the telephone). By age 10 to 12 years the child should be able to use factitive words (such as know, think, and believe), as well as complex pronouns and conjunctions, and be able to form grammatically correct sentences. School-age children gradually become more proficient at making inferences about meanings and learn the subtle exceptions to grammatical rules. This makes them less likely to engage in literal interpretation of messages.
They rapidly develop metalinguistic awareness—an ability to think about language and to comment on its properties. This enables them to appreciate jokes, riddles, and puns that involve play on words, sounds, or double meanings. They are beginning to understand metaphors and figurative statements, such as “A stitch in time saves nine.” The acquisition of cognitive skills enables them to think about the quality of their own and others’ speech and to evaluate and clarify messages.
Social Development
At the beginning of middle childhood, children enter a period of less intense emotions, secure in their dependency on their parents and family and with self-confidence tempered by a more realistic perspective. They have the energy to explore the environment beyond the family, to gradually increase the scope of interpersonal interactions, and to invest their curiosity in understanding the world.
Identification with peers is a strong influence in children’s gaining independence from parents. The aid and support of peers provides children with enough security to risk the moderate parental rejection brought about by each small victory in their development of independence.
Questions of masculinity and femininity take on importance as sex-role learning assumes more prominence. Boys associate with boys, and girls with girls, each group pursuing its own interests, with communication between the sexes confined to that which is necessary. Much of the child’s concept of the appropriate sex role is acquired through relationships with peers. During the early school years there is little difference relative to sex in the play experiences of children. Both girls and boys share games and other activities. However, in the later school years the differences become marked.
Social Relationships and Cooperation
Daily relationships with age-mates provide the most important social interactions for school-age children. For the first time, children are able to join in group activities with unrestrained enthusiasm and steady participation. Previously, interactions were limited to short periods under considerable adult supervision. With increased skills and wider opportunities, children become involved with one or several peer groups in which they can gain status as respected members.
Valuable lessons are learned from daily interaction with age-mates. First, children learn to appreciate the numerous and varied points of view that are represented in the peer group. As they play together, children discover that there are many occupations for fathers and mothers, more than one version of the same song, different rules for the same game, and different customs for celebrating the same holiday. As children interact with peers who see the world in ways that are somewhat different from their own, they become aware of the limits of their own point of view. Because age-mates are peers and are not forced to accept one another’s ideas as they are expected to accept those of adults, other children have a significant influence on decreasing the egocentric outlook of the individual child. Consequently, children learn to argue, persuade, bargain, cooperate, and compromise to maintain friendships.
Second, children become increasingly sensitive to the social norms and pressures of the peer group. The peer group establishes standards for acceptance and rejection, and children may be willing to modify their behavior to be accepted by the group. They are judged by the physical impression they convey, the skills they possess, and other abilities they can demonstrate. The need for peer approval becomes a powerful influence toward conformity. Children learn to dress, talk, and otherwise behave in a manner acceptable to the group. A variety of roles, such as class joker or class hero, may be assumed by the individual child to gain approval from the group. However, no child can adapt perfectly to all the requirements of the peer group. If some children find differences between the values of the peer group and the values of their families to be too great, they may relinquish the pleasure of interaction with the group to abide by the regulations established in the home. Thus, to diminish conflict within the family, some children may be forced into a position outside the peer group.
Third, the interaction among peers leads to the formation of intimate friendships between same-sex peers (Fig. 17-6). School age is the time when children have “best friends” with whom they share secrets, private jokes, and adventures; they come to one another’s aid in times of trouble. In the course of these friendships, children also fight, threaten, break up, and reunite. These dyadic relationships, in which children experience love for and closeness with a peer, seem to be important as a foundation for heterosexual relationships in adulthood. The conflicts encountered in the relationship are usually resolved in terms that children are able to control. Because neither child has authority over the other, as in an adult-child relationship, children must work through their differences within the framework of their commitment to each other.
Clubs and Peer Groups: One of the outstanding characteristics of middle childhood is the formation of formalized groups or clubs. Initially, children in the early middle years merely hang around the periphery of the formalized group, watching, learning, practicing various skills, and participating in group activities whenever the members of the group allow them to do so. As they age, children eventually take their places as full-fledged participating group members.
A prominent feature of middle childhood groups is the code of rigid rules imposed on the members. Exclusiveness is evident in the selection of persons given the privilege of joining. Acceptance in the group often depends on a pass-fail basis according to social or behavioral criteria. Conformity is the core of the group structure. There are often secret codes, shared interests, special modes of dress, and special words that signify membership in the group. Each child must follow a standard of behavior established by the group. Conforming to the rules provides children with feelings of security and relieves them of the responsibility of making decisions.
Membership in the group provides children with a comfortable place in society. Many of the qualities valued by the group, such as physical strength, daring, ingenuity, and comradeship, have not been stressed in the family. However, these are values that contribute to an individual child’s total personality. By merging their identity with the identities of their peers, children move from the family group to an outside group as a step toward further independence. They substitute conformity to a peer-group pattern for conformity to a family pattern while they are still too insecure to function independently.
During the early school years, groups are small and loosely organized, with changing membership and little formal structure. They do not demonstrate the elements of give and take, cooperation, and order that are seen in groups of older children. As a rule, girls’ groups are less formalized than boys’ groups, and although there may be a mixture of both sexes in groups in the earlier school years, those of later school years are composed predominantly of children of the same sex. Common interests are frequently the central element around which a group is structured.
Children’s strong desire not to be different creates problems for those who are, for various reasons, unable to meet the accepted standards of the peer group. Children with disabilities or those who are in some way unable to compete have a difficult time. Children become self-consciousness when they are unable to dress like other children, do not have spending money like other children, or appear different from other children.
Children who have physical characteristics that are obviously different (such as birthmarks, ears that “stick out,” or physical defects) may be set apart from the peer group and become a target for the criticism and ridicule. Peer-group identification and association are essential to socialization.
Poor relationships with peers and a lack of group identification can also contribute to bullying behavior. Bullying is the infliction of repetitive physical, verbal, or emotional abuse by one or more individuals intended to harm or bother another who is perceived as being less physically or psychologically powerful than the aggressor(s). Bullying can occur in varying degrees of severity in a physical, social, or emotional context. Boys usually participate in more direct or physical acts of bullying, whereas girls are commonly more involved with indirect acts such as spreading rumors or social exclusion. Although bullying can occur in any setting, it usually takes place in a classroom or on the playground when supervision is minimal (Vreeman and Carroll, 2007). Approximately 25% of students engage in bullying or are victims of bullying during elementary school, with bullying peaking on transition from elementary to secondary school (Jenson and Dieterich, 2007). Children who are bullies are often defiant, antisocial, impulsive, easily frustrated, and likely to break school rules.
Bullies and victims of bullying are at risk for long-term psychologic disturbances and psychiatric symptoms. Future problems of bullies include a higher risk for conduct problems, hyperactivity, school drop-out, and participation in criminal behavior (Gini, 2007; Jenson and Dieterich, 2007). Victims of bullying are at increased risk for low self-esteem; anxiety; feelings of insecurity; poor academic performance; and psychosomatic complaints such as feeling tense, tired, or dizzy (Gini, 2007; Jenson and Dieterich, 2007). Bullying can be reduced or prevented through supportive relationships with family, intervention of school personnel, and involvement with positive peer groups.* Many school districts have developed bullying prevention programs in response to local circumstances; however, these programs have yet to be critically evaluated for their effectiveness.
Although peer-group identification and association are essential to a child’s emergence into the world, dangers are inherent in strong peer-group attachment. Peer pressure may force children into taking risks, even against their better judgment. Peer-group activities that result in unacceptable, unlawful, or criminal gang violence are increasing in the United States and represent a significant challenge for health professionals and teachers who work with children (see Community Focus box).
 COMMUNITY FOCUS
COMMUNITY FOCUS
Providing Guidance About Gangs
Parents of school-age children often worry about the informal and unstructured social groups that their children are attracted to and wish to join. Parents of boys seem particularly concerned about “boys only” groups and the possibility that such groups could become gangs and participate in violent activities.
To help parents cope with these fears, nurses can encourage parents to become aware of any gang-related activities in their community. Typically, activities of organized gangs are illegal, and children involved in gang activities may experience frequent accidents or trips to the emergency department or police station. In addition, gang members frequently have characteristics that parents can identify, such as graffiti, a particular clothing style, unique tattoos, hand signals, or violent illegal initiation rituals. Nurses can also encourage parents to become acquainted with their child’s friends and to become involved in providing positive recreational activities for their children.
The community’s awareness of gangs that promote violence is essential to stop the spread of gang membership among youth. The media can inform the community of gang influx, identification, and activities to raise parents’ awareness of the potential dangers to their children. Community services that promote a sense of belonging among children and offer structured recreational and social events can help youth find alternatives to being a gang member.
Relationships with Families
Although the peer group is highly influential and necessary to normal child development, parents are the primary influence in shaping children’s personalities, setting standards for behavior, and establishing value systems. Family values usually predominate when parental and peer value systems come into conflict. Although children may appear to reject parental values while testing the new values of the peer group, ultimately they retain and incorporate many parental values into their own value systems. Peer associations seem to remain within the social class system.
As children move into a wider world of peer-group relationships, parents are faced with the task of letting go of control. Parents may find it difficult to face the rejection that children demonstrate as they become more involved with their peer groups. Children may want to spend more time in the company of their peers, may seem eager to leave the house, and often prefer activities of the peer group to family activities. During this time, children discover that parents can be wrong, and they begin to question the knowledge and authority of the parents who previously were considered to be all-knowing and all-powerful. Parents can best serve the interests of their children through tolerant understanding and support.
Although increased independence is the goal of middle childhood, children are not yet prepared to abandon parental control. Children need and want restrictions placed on their behavior; they are not yet prepared to cope with all of the problems of their expanding environment. They feel more secure knowing that there is an authority greater than themselves to implement controls and restrictions. Children may complain loudly about the restrictions and try to break down parental barriers, but they are uneasy if they succeed in doing so. Children feel secure with reasonable, consistent controls. They respect the adults on whom they can rely to prevent them from acting on each and every urge. Children see this behavior as an expression of love and concern for their welfare.
Children also need their parents as adults, not as “pals.” Sometimes parents, hurt by their children’s rejection, attempt to maintain their children’s love and gratitude by assuming the role of pal. Children need the stable, secure strength provided by mature adults to whom they can turn during troubled relationships with peers or stressful changes in their world. During a disruption in their lives, such as times of failure, periods of illness, or a move that separates them from the security of friends, children need the firm, secure anchor of parental interest and concern. With a secure base in a loving family, children are able to develop the self-confidence and maturity needed to stand independently.
Children’s relationships with siblings change during the middle years. Children view siblings as equal in power and status. In earlier years, older siblings were influential in the younger siblings’ learning. In the middle years the relationship becomes one of companionship. Positive emotional tone increases, but sibling conflict also increases as the siblings get older. Middle childhood is a period of transition for sibling relationships, a juncture between the open bickering of early childhood and the supportive relationships observed in adult siblings.
Development of Self-Concept
Closely associated with developing a sense of industry is developing a concept of one’s value and worth. With the emphasis on skill building and broadened social relationships, children are continually occupied in the process of self-evaluation. Children’s self-concepts are composed of their own critical self-assessments plus their interpretations of the opinions of others. Self-concept refers to a conscious awareness of a variety of self-perceptions, such as one’s physical characteristics, abilities, values, and self-ideals, and one’s idea of self in relation to others.
Body Image
Body image is what children think about their bodies. School-age children are knowledgeable about the human body, and social development during this period focuses to a large extent on the body and its capabilities. School-age children can draw a recognizable human figure, although individually their portrayal of body parts may vary considerably. They are acutely aware of their own bodies as well as those of their peers and those of adults. It is important that children know body functions and that adults correct any misinformation children have about the body (e.g., what is fat).
During the school years, children focus on peer relationships and conform to group norms. They evaluate how their physical appearance, body configuration, and coordination compare with those of their peers. The head is the most noticeable and, to them, important part of the body. They also model themselves after their parents and compare themselves to favored peers and images observed in the media.
Children are aware of physical disabilities in others, and it is not unusual for them to believe that their own bodies are not the right size or the right shape or are in some way defective. They respond to such concerns in a variety of ways. For example, they will conceal perceived shortcomings of body or performance, as in the obese child who refrains from going swimming, the child who conveniently forgets a gym suit, the child who conceals an imagined defect, or the child with enuresis who declines invitations to slumber parties. Children seldom express these concerns to families. However, they need reassurance about both the uniqueness and the sameness of their bodies while their privacy is respected and they are allowed appropriate protective strategies. Children who are different become aware of the differences and may find themselves excluded from the group. When children are teased or criticized about being different, the effect can last even into adulthood.
Self-Esteem
Self-esteem is children’s pictures of their individual worth and consists of both positive and negative qualities. Children actively strive to achieve internalized goals. At the same time, they continually receive feedback on the quality of their performance from individuals they consider to be authorities. By the time they reach school age, children have received messages regarding the extent to which they are able to accomplish tasks that have been delegated to them. For example, one child may have been given prestigious responsibilities at home or at school or received special commendation for an achievement. On the other hand, another child may have been sent to a special class for slow learners or may have been the last person selected when children chose sides for a game. These and other signs serve as clues to social worth that children incorporate as part of their self-evaluation.
Children approach the process of self-evaluation from a framework of either self-confidence or self-doubt. Children who have mastered the maturational crises of autonomy and initiative are able to face the world with feelings of pride rather than shame. At first, children’s self-concepts are formed exclusively from their perceptions of their parents’ evaluation of them. During middle childhood the opinions of peers and teachers are important. Criticisms and peer approval are additional sources of data for evaluation. Parents and other adults are no longer the only persons who respond to their skills, talents, and abilities; peers also identify skills and capabilities. Each child soon begins to internalize these outside opinions. If children regard themselves as worthwhile or satisfactory persons, they have high self-esteem, self-confidence, and a positive self-concept. If they view themselves as worthless, they have low self-esteem.
Pets also influence a child’s self-esteem. Pets can have a positive effect on physical and emotional health and can teach children the importance of nurturing and nonverbal communication (Podberscek, 2006).
Children encounter difficulties assessing their own abilities because they rely on their own expectations or on the expectations expressed by others regarding their performance. They depend almost entirely on external evidence of worth, such as school grades, teachers’ comments, and parental and peer approval. Children do not yet have the capacity to develop their own independent criteria to evaluate their own accomplishments. It is especially difficult for them to assess their achievement in abstract skills.
Nothing succeeds like success. Significant adults in children’s lives can often manage to manipulate the environment so that children meet with success. Each small success can improve a child’s self-image. The more positive children feel about themselves, the more confident they feel in trying again for success. All children profit from feeling that they are special to significant adults. A positive self-image makes them feel likable, worthwhile, and capable of valuable contributions. Such feelings lead to self-respect, self-confidence, and a general feeling of happiness. Parents can help their school-age children develop self-esteem by being honest, by providing opportunities for creativity, by helping them succeed in activities, and by providing positive reinforcement. Nurses can enhance self-esteem by fostering supportive relationships between children and members of their families and by emphasizing children’s strengths and positive aspects of their behavior (see Community Focus box).
COMMUNITY FOCUS
Socialization of Boys and Girls
Health professionals have long been aware that boys and girls are socialized differently by parents and teachers. Girls are encouraged to express their emotions and to be sensitive and responsive to others. Boys, on the other hand, are often told to hide their feelings and are criticized if they are “too sensitive.” In school, boys are encouraged to take the most challenging courses, to do well in math and science, and to participate in athletic endeavors. Girls may be discouraged from taking math and science, ostracized socially if they take typically “male” courses, and penalized for joining athletic teams. These differences in socialization may contribute to stereotypic behavior and the way that boys and girls relate to each other. Boys may feel entitled to life’s opportunities and benefits, and girls may think that they need to be submissive and deferential to succeed. Such beliefs may ultimately influence participation in risk-taking behaviors in adolescence.
To prevent the development of a sense of entitlement in boys and to foster self-reliance in girls, parents can encourage boys to be socially and interpersonally sensitive and responsive to others, and teach boys that interrupting girls is rude and inappropriate behavior. Teachers can encourage girls, as well as boys, to take the challenging courses in math and science, foster cooperation between boys and girls on school projects, and facilitate the development of athletic endeavors for not only boys but also girls. Some schools are providing same-sex courses to provide a more neutral and nurturing environment for students.
Development of Sexuality
Evidence indicates that many children experience some form of sex play during or before preadolescence as a response to normal curiosity, not as a result of love or sexual urge. Children are experimentalists by nature, and this play is incidental and transitory. Adverse emotional consequences or guilt feelings depend on how the parents manage the behavior and whether children view their actions as wrong in the eyes of significant persons, particularly their parents.
Children’s attitudes toward sex are acquired indirectly at an early age and affect the way they respond to sexual information presented later. Many parents discourage sexual exploration, either through subtle substitution of activities that divert their children’s attention from the genitalia or by expressions of anger or disgust at their children’s behavior. These tactics clearly communicate to children that they should not engage in such activities, discourage questions about sex, and limit the sources of information.
Sex Education
Parents may not teach young children the correct terminology for sexual organs or sexual feelings. Often the only vocabulary available to children is one that identifies sexual organs with excretory functions. If children learn that excretory organs and functions are dirty, they may associate “dirtiness” with the reproductive organs and functions. If children learn the correct terminology for the organs and their functions, this will eliminate or reduce this association.
Because parents often either repress or avoid their children’s sexual curiosity, sexual information received in childhood may be acquired almost entirely from peers. Such information is often transmitted in secret conversations and contains considerable misinformation. These communications can also create anxiety in children and inhibit spontaneous expressions or questioning of their parents.
Although middle childhood is an ideal time for formal sex education, this subject has created considerable controversy. Many parents and groups are unconditionally opposed to the inclusion of sex education in the schools. Others believe that information relating to sexual maturation and the process of reproduction should be presented as naturally as information about other natural phenomena, such as the growth of plants, the changing seasons, and the migratory habits of birds. When sex education is presented from a life span perspective and treated as a normal part of growth and development, the information is less likely to contain overtones of uncertainty, guilt, or embarrassment that could in turn produce anxiety in children.
Sex education programs have been successfully incorporated into a number of elementary school curricula. In many of these programs, sexuality is presented in the context of its central role as a biologic mechanism for the survival of the culture. Children learn that sexual maturation and reproduction represent each individual’s contribution to the natural order of things. This approach provides a natural entry into discussion of sexuality as a basis for family units, marriage, and attitudes toward children, as well as an entry into a presentation of the biologic facts of sexuality. Many sex education programs also emphasize that sexual intimacy is part of a close, personal relationship and a means of conveying love, as well as a means for ensuring the survival of the species.
Nurse’s Role in Sex Education
No matter where nurses practice, they can provide information on human sexuality to both parents and children. To discuss the topic adequately, nurses must understand the physiologic aspects of sexuality; know the common myths and misconceptions associated with sex and the reproductive process; understand cultural and societal values; and be aware of their own attitudes, feelings, and biases.
When nurses present sexual information to children, they should treat sex as a normal part of growth and development. Nurses should answer questions honestly, matter-of-factly, and at the child’s level of understanding. School-age children may be more comfortable when boys and girls are segregated for discussions; however, each group needs information about both sexes.
Children need help to differentiate sex and sexuality. Exercises focused on clarifying values, identifying role models, solving problems, and accepting responsibility are important to prepare school-age children for early adolescence and puberty. In addition, care providers need to explain sexual information that is discussed via the media or jokes. A comprehensive sex education program including information about abstinence, contraception, and birth control methods should be presented during the middle school years (Eisenberg, Bernat, Bearinger, et al, 2008). Teaching a child to be sexually responsible is an important component of sex education. Health care providers should supply specific information concerning sexually transmitted infections, human immunodeficiency virus (HIV), and acquired immunodeficiency syndrome (AIDS). Anticipatory guidance should include information about prevention, transmission, and implications of sexually transmitted infections.
Preadolescents need precise and concrete information that will allow them to answer questions such as “What if I start my period in the middle of class?” or “How can I keep people from telling I have an erection?” It is important to tell them what they want to know and what they can expect to happen as they mature sexually.
During encounters with parents, nurses can be open and available for questions and discussion. They can set an example by the language they use in discussing body parts and their function and by the way in which they deal with problems that have emotional overtones, such as exploratory sex play and masturbation. Parents need help to understand normal behaviors and to view sexual curiosity in their children as a part of the developmental process. Assessing the parents’ level of knowledge and understanding of sexuality provides cues to their need for supplemental information that will prepare them for increasingly complex explanations as their children grow older.
Children with developmental disabilities need emotional and sexual relationships. Parents of children with developmental disabilities may need special assistance and help with sex education. In 1996 the American Academy of Pediatrics developed specific guidelines that discuss ways to teach these children about human anatomy, pubertal changes, expression of physical affection, protection from sexual abuse or exploitation, and independence in personal hygiene and self-care. Sex education for children with disabilities requires individualized techniques, depending on the type and degree of disability (Murphy and Young, 2005). Nurses must bring the issue of sexuality out in the open and promote the idea that sexuality is a part of every individual’s identity in order to address educational needs (Murphy and Young, 2005).
Sometimes participation in short classes or group discussions can help parents address disturbing behaviors and anticipate their children’s questions and learning needs. It is wise to include both parents in such activities when possible. Both parents should assume responsibility for sex education in the home so that the children will not acquire a distorted view of either the male or the female role that may alter relationships with the opposite sex in later life.
Play
As children enter the school years, their play takes on new dimensions that reflect a new stage of development. Not only does play involve increased physical skill, intellectual ability, and fantasy, but as children form groups and cliques, they begin to evolve a sense of belonging to a team or club. To belong to a group is of vital importance. Clubs, societies, and organizations are important parts of the culture of childhood.
Rules and Rituals
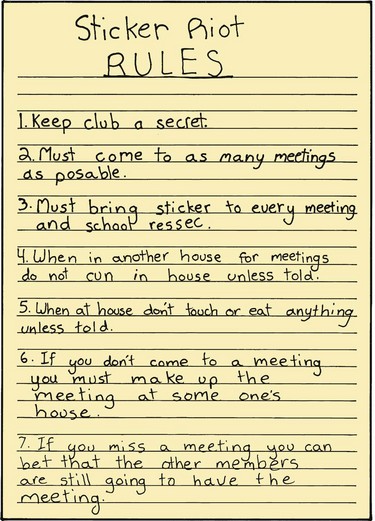
The need for conformity in middle childhood is strongly manifested in the activities and games so important in the life of school-age children. Up to this point, they have either played games they have invented themselves or have played in the company of a friend or an adult, and rules more or less evolved with the game. Now they begin to see the need for rules, and the games they play have fixed and unvarying rules that may be bizarre and extraordinarily rigid (especially those made up by the group). But part of the enjoyment of the game is knowing the rules, because knowing means belonging. Once the rules are established and agreed on, the demand for conformity is strong (Fig. 17-7).
Conformity and ritual characterize the play of school-age children, not only in games, but also in behavior and language. Childhood is full of chants and taunts, such as “Eeny, meeny, miney, mo,” “Last one is a rotten egg,” and “Step on a crack, break your mother’s back.” Children receive a great deal of pleasure and power from such sayings, which have been handed down with few changes through generations.
Team Play: A more complex form of group play that develops from the need for peer interaction involves the team games and sports that are part of the school years. Such games may require a referee, umpire, or person of authority so the rules can be followed more accurately. Team membership has several characteristics that promote child development during the middle years.
Children learn to subordinate personal goals to group goals. Team membership means that each child is accountable to the other team members and that each member’s acts may affect the success or failure of the entire group. Each member’s behavior is open to public evaluation, and children risk ostracism, ridicule, or scapegoating if they contribute to a team loss. Although individual skills are recognized, team successes and failures are shared by all members. Children learn the concept of interdependence and the reliance of all players on one another.
Children learn that division of labor is an effective strategy for the attainment of a goal. Each person on a team has a specific function, which increases the team’s chances of winning. Once children learn that certain goals are best accomplished by dividing tasks among several individuals, they can transfer this knowledge to other social situations. Children also learn that some children are best equipped to perform one part of the task and other children are best suited to another aspect of the task.
Team play helps children learn about the nature of competition. In all team play there is a winning side and a losing side. Because losing is often interpreted as failure, children go to great lengths to avoid the public embarrassment and personal shame that accompany failure. The more a child identifies with the team and values membership in the group, the more distasteful losing becomes. Fear of losing and the failure it implies are strong incentives for group commitment; however, winning is not universally given high value. Some cultures and subcultures emphasize the game and consideration for one’s companions rather than the outcome.
Team play also contributes to children’s social, intellectual, and skill growth. Children work hard to develop the skills needed to become members of a team, to improve their contribution to the group effort, and to anticipate the consequences of their behavior for the group. Team play helps stimulate cognitive growth as children are called on to learn many complex rules, make judgments about those rules, plan strategies, and assess the strengths and weaknesses of members of their own and the opposing teams (Fig. 17-8).

Quiet Games and Activities
Although the play of school-age children can be highly active, they also enjoy many quiet and solitary activities. The middle childhood years are the time for collections, and young school-age children’s collections are an odd assortment of unrelated objects in messy, disorganized piles. Collections of later years are more orderly and selective and often are organized neatly in scrapbooks, on shelves, or in boxes.
School-age children become fascinated with increasingly complex board, card, and computer games. Children play these games alone or in groups. As in all games, the adherence to rules is fanatic. There is usually much discussion and argument, but children easily resolve disagreement by learning the appropriate rules of the game.
The newly acquired skill of reading becomes increasingly satisfying as school-age children begin to expand their knowledge of the world through books (Fig. 17-9). School-age children never tire of stories, and, like preschool children, they love to have stories read aloud. They also enjoy sewing, cooking, carpentry, gardening, and creative endeavors such as painting. Many creative skills, such as those involving music and art, and athletic skills, such as swimming, riding, hiking, dancing, and karate, are acquired during childhood and continue to be enjoyed into adolescence and adulthood (Fig. 17-10).

Hero worship is another characteristic of children and adolescents. The object of the adoration can be a friend, relative, teacher, or national sports or entertainment figure. However, problems can arise when the idol proves to be an inappropriate role model.
Ego Mastery
Play also affords children the means to acquire representational mastery over themselves, their environment, and other persons. Through play, children can feel as big, as powerful, and as skillful as their imaginations will allow, and they can attain vicarious mastery and power over whomever and whatever they choose. They need to feel in control in their play. School-age children still need the opportunity to use large muscles in exuberant outdoor play and the freedom to exert their newfound autonomy and initiative. They need space in which to exercise large muscles and to work off tensions, frustrations, and hostility. Physical skills practiced and mastered in play help to develop a feeling of personal competence, which contributes to a sense of accomplishment and helps provide a place of status in the peer group.
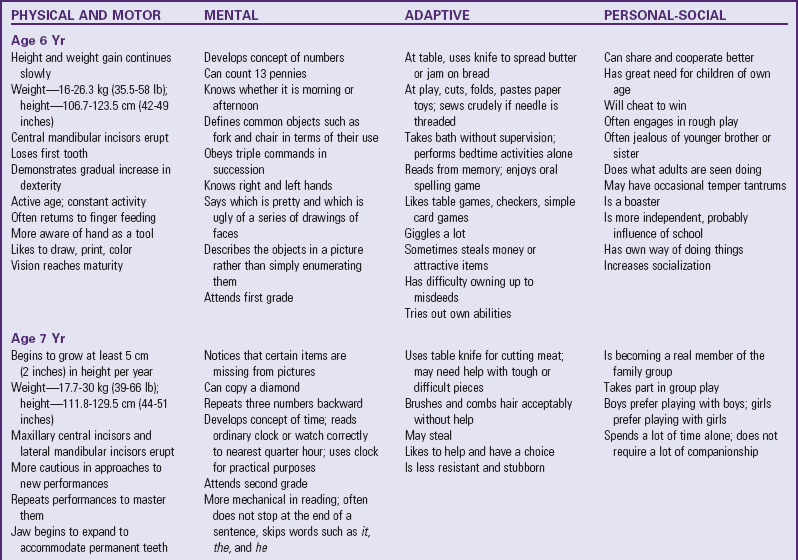
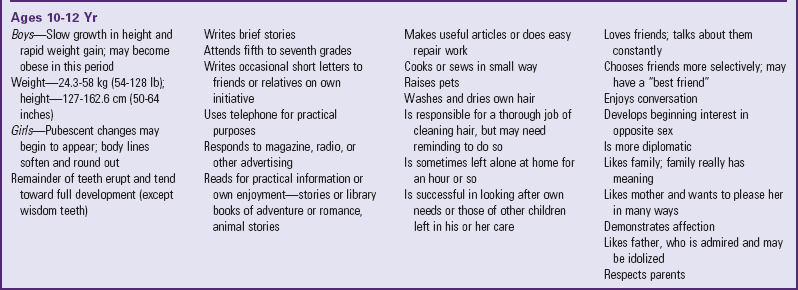
Table 17-1 presents a summary of growth and development in middle childhood. Because each child has a unique developmental pattern, any descriptions of the typical child of any age-group can represent only an average and should not be considered as absolute criteria for any given child.

Coping with Concerns Related to Normal Growth and Development
School serves as an agent for transmitting societal values to each succeeding generation of children and as a setting for many peer relationships. As a socializing agent second only to the family, school exerts a profound influence on the social development of children.
School entrance causes a sharp break in the structure of a child’s world. For some children it is their first experience in conforming to a group pattern imposed by an adult who is not a parent and who has responsibility for too many children to be constantly aware of each child as an individual. Children want to go to school and usually adapt to the new environment with little difficulty. Successful adjustment is directly related to the child’s physical and emotional maturity and the parents’ readiness to accept the separation associated with school entrance. Cooperation among parents and support for the child are successful ways of coping with school entry stress. Unfortunately, some parents express their unconscious attempts to delay their child’s maturity by clinging behavior, particularly with their youngest child.
Anticipatory Socialization
By the time they enter school, most children have a fairly realistic concept of what school involves. They receive information regarding the role of pupil from parents, playmates, and the media. In addition, most children have had experience with daycare or preschool and kindergarten.
Children’s attitudes toward school and the extent of their adjustment are strongly influenced by their parents’ attitudes. Middle-class children have fewer adjustments to make and less to learn about expected behavior because the school tends to reflect dominant middle-class customs and values, although this may be tempered by the school’s location and predominant teachers and student body. Parents who view school as a place that they have helped to create and support and that is directed toward the same objectives for socialization as their own usually prepare their children with useful anticipatory socialization and furnish them with confidence to meet the challenge. Parents who view the school as an alien culture and one that they have little, if any, power to affect may unknowingly teach their children to be fearful and resentful toward school, even though the parents agree with its purposes and objectives.
The television, which influences the acquisition of information and attitudes, also provides anticipatory socialization. Television viewing has the potential to increase a child’s vocabulary, extend the child’s horizons, and enrich the school experience. However, television relies heavily on images to convey information. Consequently, it is difficult to explore complex issues by this medium. Extensive television viewing may also encourage children to seek simple answers to tough problems and to believe that violence is the most effective and quick solution to conflict.
Although most children have had some experience with schooling before they enter the first grade, the extent to which early childhood education prepares children for primary school varies. Some preschool programs provide custodial care; others also emphasize emotional, social, and intellectual development. Early childhood programming that stresses cognitive more than social aspects appears to be more effective in facilitating later academic achievement.
Role of the Teacher
To facilitate the transition from home to school, teachers should have personality characteristics that allow them to deal with the needs of young children. Because they react to the teacher on the basis of past experience, children respond best to teachers with attributes that they would find in a warm, loving parent. As a parental surrogate, teachers in the early grades perform many of the activities formerly assumed by the parents, such as recognizing the children’s personal needs (e.g., a need to go to the bathroom or for assistance with clothing) and helping to develop their social behavior (e.g., manners).
Teachers, like parents, are concerned about the psychologic and emotional welfare of children. Although the functions of teachers and parents differ, both place constraints on behavior, and both are in a position to enforce standards of conduct. However, the teacher’s primary responsibility is stimulating and guiding children’s intellectual development as opposed to providing for their physical welfare beyond the school setting.
Teachers share the parental influence in shaping a child’s attitudes and values. They serve as models with whom children can identify and whom they try to emulate. Children seek a teacher’s approval and avoid a teacher’s disapproval. The teacher is a significant person in the life of the early school-age child, and hero worship of a teacher may extend into late childhood and preadolescence. It is not uncommon for the first or second grader to be heartbroken and tearful at leaving a familiar teacher at the end of the school term or to be upset when faced with a substitute teacher for even a short period.
Children’s interest in school and learning and much of their social interaction and self-concept are related to interactions with the teacher (Fig. 17-11). The differential systems of reward and punishment administered by teachers affect the emotional adjustment and self-concept of children and how they respond to school in general.

Fig. 17-11 School represents an important change in a child’s life, and teachers exert a significant influence on the child.
The interaction between the teacher and an individual pupil affects the pupil’s acceptance by other children, which in turn affects the child’s self-concept. Behaviors praised by the teacher usually acquire a positive value, whereas those viewed negatively by the teacher are devalued by the children. In this way the teacher exerts considerable influence in a number of areas, such as attitudes toward minority groups, the disabled, or less favorably endowed children. Teacher approval of children and their self-acceptance are closely related.
The teacher sets the emotional tone of the classroom. Those who are able to establish a positive social climate are usually concerned about the mental health and social dynamics of children. Feeling a responsibility for personality development in their pupils, they are alert and sensitive to a child’s anxieties, peer-group relationships, self-concepts, and general attitudes toward school. Learner-centered behaviors, such as supportive statements that reassure or commend children, accepting and clarifying statements that help them refine ideas and feelings to provide a sense of being understood, and constructive assistance that aids them with their own problem solving, contribute to the expansion and development of a positive self-concept.
Role of the Parents
Parents share responsibility with the schools for helping children achieve their maximum potential. Parents can supplement the school program in numerous ways (see Family-Centered Care box). Cultivating responsibility is the goal of parental assistance. Being responsible for schoolwork helps children learn to keep promises, meet deadlines, and succeed at their jobs as adults. Responsible children may occasionally ask for help (e.g., with a spelling list), but usually they like to think through their work by themselves. Excessive pressure or lack of encouragement from parents may inhibit the development of these desirable traits.
 FAMILY-CENTERED CARE
FAMILY-CENTERED CARE
Helping Children in School
Be supportive; through companionship, share ideas and thoughts.
Be positive; every child should experience some success each day.
Share an interest in reading; use the library, discuss books they are reading.
Support and encourage activity rather than passivity.
Encourage originality; help children make their own projects from discarded articles or other available materials.
Foster the development of hobbies and collections.
Encourage children to wonder and reflect during free time.
Encourage family experiences and trips to places of interest.
Encourage questions; help children discover sources for information or places to explore and investigate.
Stimulate creative thinking and problem solving; help children try out new solutions to problems without fear of making mistakes.
Meet the teacher at the beginning of school and plan to visit the school to see what is taught and expected.
Send the child to school every day. Teachers are concerned when parents make other plans for their children; it conveys the impression that school is unimportant.
Demonstrate an interest in what the child is learning.
Demonstrate an interest in content and growth more than in grades.
Make it clear to the child that schoolwork is between the child and the teacher; teacher and child should set goals for better school performance to allow the child to feel responsible for school successes and failures.
Take advantage of situations that support and reinforce school learning.
Share information with teachers that will help them understand the child better.
Communicate with the teacher if there appears to be a problem; avoid waiting for a scheduled conference.
Provide a quiet, well-lit area for study that is safe from interruption; do not allow television or radio.
Avoid dictating a study time, but do enforce rules, such as no television until homework is done; accept the child’s word that work is complete.
Help with homework should focus on explaining the question, not giving the answer.
Teach the child to break large tasks (such as a report) into smaller, manageable tasks spread over the allotted time rather than to attempt the entire project the night before it is due.
Request special help for children with learning problems.
Support the school staff by showing respect for both the school system and the teacher, at least in the child’s presence.
Discipline
Numerous factors influence the amount and manner of discipline imposed on school-age children: the parents’ psychosocial maturity, their own childrearing experiences during childhood, the children’s temperament, the context of the children’s misconduct, and the children’s response to rewards and punishments. Discipline serves many purposes: (1) to help the child interrupt or inhibit a forbidden action; (2) to point out a more acceptable form of behavior so that the child knows what is right in a future situation; (3) to provide some reason, understandable to the child, that explains why one action is inappropriate and another action is more desirable; and (4) to stimulate the child’s ability to empathize with the victim of a misdeed.
As children are increasingly able to see a situation from the point of view of another, they are able to understand the effects of their reactions on others and themselves. Disciplinary techniques should help children control their own behavior.
To be effective, discipline should take place in an environment characterized by positive, supportive parent-child relationships and should involve strategies that instruct and guide desired behaviors and eliminate undesired or ineffective behaviors (Towe-Goodman and Teti, 2008). Parents should not use punitive actions or corporal punishment, since these methods are of limited value and are associated with increasingly disruptive behavior in children. Negative outcomes associated with corporal punishment are discussed in Chapter 3. In particular, physically aggressive parenting practices that involve spanking are linked to children with poor psychologic adjustment, including depression, anxiety, hopelessness, and destructive behavior such as aggression and violence (Durrant, 2008). Reasoning, on the other hand, is an effective disciplinary technique for school-age children; however, use of a time-out may be necessary to stop the behavior acutely (Towe-Goodman and Teti, 2008).
As their cognitive skills advance, school-age children are able to benefit from more complex disciplinary strategies. For example, withholding privileges, requiring recompense, imposing penalties, and contracting can be used with great success. Problem solving is the best approach to limit setting, and children themselves can be included in the process of determining appropriate disciplinary measures.
Dishonest Behavior
During middle childhood, children may engage in what is considered to be antisocial behavior. Lying, stealing, and cheating may become manifest in previously well-behaved children. This is especially disturbing to parents, who may have difficulty coping with such behavior.
Lying can occur for a number of reasons. Preschool children often have difficulty distinguishing between fact and fantasy. They do not have the cognitive capacity to deliberately mislead. Sometimes they misperceive or fail to remember an event. By the time they reach school age, they still tell stories but can distinguish between what is real and what is make-believe. If not, they need to learn to distinguish between fantasy and reality. Often children will exaggerate a story or situation as a means to impress their family or friends.
Young children lie to escape punishment or get out of some difficulty, even when the evidence of their misbehavior is before their eyes. Lying is more common in families in which punishment is severe. When parents model honesty and veracity, the children will often behave in the same way. If parents lie, the children will emulate their behavior. Older children may lie to meet expectations set by others to which they have been unable to measure up. They may also lie because of low self-esteem or as a means of getting ahead or acquiring something with little effort. However, most children are concerned with the wrongfulness of lying and cheating—especially in their friends. They are quick to tell on others when they detect cheating.
Parents need to be reassured that all children lie sometimes and that they often have difficulty separating fantasy from reality. Providers should help parents to understand the importance of their own behavior as role models and of being truthful in their relationships with children. Parents can discuss the issue with the children directly to impress on them how much of their own security and respect is lost when they are not believed.
Cheating is most common in young children, ages 5 to 6 years. They find it difficult to lose at a game or contest, and they cheat to win. They have not yet acquired the full realization of the wrongfulness of this behavior and do it almost automatically. It usually disappears as they mature. However, when children observe parental behaviors such as boasting about cheating on income taxes, they assume this to be appropriate behavior. Parents need to be aware of the types of behaviors they model for their children. When they set examples of honesty, children are more likely to conform to these standards.
As with other ethically related behavior, stealing is not an unexpected event in the younger child. Between ages 5 and 8 years, children’s sense of property rights is limited; they tend to take something simply because they are attracted to it, or they take money for what it will buy. They are equally likely to give away something valuable that belongs to them. When young children are caught and punished, they are penitent—they “didn’t mean to” and promise “never to do it again,” but they may well repeat the performance the following day. Often they not only steal but lie about it as well or attempt to justify the act with excuses. It is seldom helpful to trap children into admission by asking directly if they did the offensive thing. Children do not take on such responsibility until nearer the end of middle childhood.
Children steal for several reasons: lack of a sense of property rights, an attempt to acquire the means with which to bribe other children for favors, a strong desire to own the coveted item, or a wish for revenge to “get back at someone” (usually a parent) for what they consider to be unfair treatment. Older children may steal to supplement an inadequate income from other sources. Sometimes stealing is an indication that something is seriously wrong or lacking in the child’s life. Children may steal to make up for a perceived lack of love or another satisfaction.
In some settings in which living arrangements are crowded, children have little privacy, and much of the family property is communal, children may fail to develop a sense of property rights. Sometimes parents unintentionally confuse children with seemingly conflicting values. In an attempt to teach unselfishness, they may force children to share belongings with others, with the result that the children fail to understand property rights.
If children are told not to take money from their mother’s purse or their father’s pocket but observe the parents doing the same thing, they receive conflicting messages. Parents may go through a child’s pockets or other private areas at night and even discard, without explanation, items of which they do not approve. Children should have a place that is private to them alone that other family members respect. If children’s personal rights are respected, they are more likely to respect the rights of others.
It is difficult for many parents to cope with stealing by their children. In most situations it is best not to attempt to find a hidden or deep meaning to the stealing. A reprimand, together with an appropriate and reasonable punishment, such as having the older child pay back the money or return the stolen items, will ordinarily take care of most cases. Most children can learn to respect the property rights of others with little difficulty despite temptations and opportunities. Some children simply need more time to learn the importance of the culture’s rules regarding private property.
Coping with Stress
Children today experience more stress than children in previous generations. This stress comes from a variety of sources. Other sections in this book discuss dealing with specific types of stresses, especially those in which nurses assume a major role, such as hospitalization, illness, abuse, disabling injuries, and death or the threat of death.
In the normal course of growing up, children are pressured by their peers to identify with their friends; to eat, dress, and look like their friends; to talk about the same things that their friends talk about; to engage in the same activities as their friends; and yet to compete with them. They are pressured by parents to excel in school, in athletics, and in social situations at ever-younger ages. Children in the middle school years are often over-programmed with activities such as ballet lessons, music lessons, athletics, and other activities until the cumulative effect is overwhelming.
Although children receive better treatment than in earlier times, when beatings and child labor were common, their physical and emotional well-being is threatened by different stresses, especially violence. Children are stressed by conflict within the home. The high divorce rate and the number of single-parent families result in altered relationships and increasing responsibilities for children.
Children’s exposure to domestic violence is a significant problem in the United States. Approximately 3.3 million children in the United States witness domestic violence every year (Murrell, Christoff, and Henning, 2007). Children who are exposed to domestic violence are 15 times more likely to be physically abused or neglected than children without exposure (Holt, Buckley, and Whelan, 2008). Parents of violent households may be unable to meet their children’s needs and may have ineffective relationships with their children (Holt, Buckley, and Whelan, 2008). These children are often more aggressive, participate in delinquent behaviors, experience developmental and academic deficits, and have difficulties maintaining peer relationships (Murrell, Christoff, and Henning, 2007). In addition, longitudinal studies have shown that children exposed to domestic violence are more likely to display antisocial behavior and become involved in violent crimes and substance abuse as adults (Holt, Buckley, and Whelan, 2008).
Exposure to violence in the family, school, or community affects children’s ability to concentrate and function. Children may be traumatized by witnessing violence and develop fear, insecurity, and a sense of helplessness (Fredland, 2008). Children exposed to repeated violence can display hyperarousal symptoms leading to posttraumatic stress disorder and symptoms such as nightmares, flashbacks, a fatalistic orientation to the future, depression, and anxiety (Fowler, Tompsett, Braciszewski, et al, 2009).
School itself is stressful for many children, and school has become a more violent environment. A recent national survey found that 6.5% of students brought a weapon such as a gun, knife, or club to school in the last 30 days, and 8% of students reported being threatened or injured with a weapon (Fredland, 2008). Nearly 30% of students reported that their property was stolen or damaged one or more times while at school (Fredland, 2008).
The school environment may also pose a threat to the middle schooler’s self-image. School-age children have a high fear of failure and criticism (Weems and Costa, 2005). Competing with classmates for grades and teacher recognition, failing an examination, being teased or made fun of in school, or being labeled as “stupid” or “learning disabled” all result in emotional distress. Teachers or parents may not always recognize or appreciate the worries or sources of stress for school-age children.
Students’ interactions with their teachers are an important component of the school day and can affect student behavior (Eisenbraun, 2007). Children become distressed when teachers raise their voices, yell or scream, or use fear of physical punishment in the classroom. Students exposed to such behavior may show symptoms of stress, express excessive worry about school, demonstrate negative self-perceptions, and verbalize fear of physical harm by the teacher. Although parents and nurses should be cautious in interpreting such behaviors (they are in many ways similar to school phobia; see Chapter 18), a high degree of suspicion might be justified if the symptoms are not explained by other factors or if they represent a marked change from previous patterns.
Some children are encouraged to feel, think, and behave at a level of maturity far beyond what could reasonably be expected of individuals their age. They are expected to take on many adult-type responsibilities, to make decisions they are not really able to make, and to achieve more. A school’s emphasis on high test score achievement can increase stress. Children have little time for being young and enjoying the spontaneous activities of childhood.
When asked to describe sources of worry, school-age children identified concerns such as social threats (e.g., being teased), personal harm, medical procedures, punishment, death, and school performance (Weems and Costa, 2005). Girls are often more sensitive to critical comments at school or other social settings than boys (Li and Prevatt, 2007). Other potential sources of stress are listed in Box 17-1.
Children respond to stress by using coping mechanisms that include internalizing symptoms such as withdrawal, delaying tactics, and daydreaming, along with externalizing symptoms such as aggression and delinquency (Fowler, Tompsett, Braciszewski, et al, 2009). Variables that contribute to children’s ability to cope with stress include socioeconomic status, family relationships, social support, gender, and previous life experiences.
 NURSING ALERT
NURSING ALERT
The nurse who observes the following signs of stress in a child should explore the situation further:
To help children cope with the stresses in their lives, the parent, teacher, or health care worker must recognize signs that indicate that a child is undergoing stress (see Box 17-1) and identify the source promptly. Children need to learn how to recognize signs of stress in themselves, such as a pounding heart, rapid breathing, or “butterflies” in the stomach. Once they are able to recognize that they are stressed, they can employ techniques for managing their stress. Probably the most useful technique is to help them plan a process for dealing with any stress through problem solving.
Children can learn relaxation techniques such as deep-breathing exercises, progressive relaxation of muscle groups, and positive imagery. Encouraging them to “blow off steam” through physical activity reduces tension and anxiety. Children need to learn to identify their stress reactions. Those involving situations or actions of others are easy to identify. Feelings within themselves are sometimes more difficult. Alternative actions must be explored. Children should list all possibilities, including those that they know will not work. They need to examine what might happen as a consequence of each alternative. The final step is to select what they perceive to be the best option. It is sometimes helpful to have children model their behavior after that of someone they know who has successfully coped with a similar problem. When children work through this process a few times, they are able to apply problem solving automatically.
Fears
Several anxiety symptoms, including fear of the dark, excessive worry about past behavior, self-consciousness, social withdrawal, and an excessive need for reassurance, are considered normal developmental events for children. School-age children are less fearful of body safety than they were as preschoolers, although they still fear being hurt, kidnapped, or having to undergo surgery. They also fear death and are fascinated by all aspects of death and dying. They have less fear of noises, darkness, storms, and dogs. Most new fears that trouble school-age children are related to school and family (e.g., fear of failing, fear of teachers and bullies, or fear of something bad happening to their parents).
Parents and other persons involved with children should discuss children’s fears with them individually or through group activities. Their viewpoints must be respected, and their need to communicate their concerns should be recognized. Sometimes school-age children are inclined to hide their fears to avoid being ridiculed or labeled as a “baby” or “chicken.” Hiding fears does not end them, and children who are afraid to communicate their fears may develop displaced fears or phobias. Children need to know that their concerns are heard and understood. Parents who convey this to their children without becoming overprotective help their children to feel less lonely and less frightened.
Latchkey Children
The term latchkey children is used to describe children in elementary school who are left to care for themselves before or after school without supervision of an adult (Fig. 17-12). The increasing numbers of single-parent families and working mothers, together with a lack of available child care, have created a stress-provoking situation for many school-age children. Some latchkey children may have a chronic illness as well.

Inadequate adult supervision after school leaves children at greater risk for injury and delinquent behavior. Latchkey children feel more lonely, isolated, and fearful than children who have someone to care for them. To cope with their fears and anxieties while alone, these children may devise strategies such as hiding (in a bathroom, closet, or shower or under a bed), playing the television loudly to drown out noises, and using pets as a comfort.
Many communities and persons concerned about such children’s welfare are trying to help children and their parents deal with this potentially serious problem. School-age child care programs have been implemented by some communities and employers. Some guidelines appropriate for presentation to parents and/or children to help alleviate their stress and increase the children’s safety are listed in the Family-Centered Care box. Other types of programs include those designed to teach self-help skills to children, hotlines that provide telephone check-in and reassurance programs for children, and programs that link latchkey children with reassuring older persons in their community.
FAMILY CENTERED-CARE
Latchkey Children
Teach the child not to display keys and to always lock doors.
Tell the child not to enter the house after school if the door is ajar, a window is open, or anything appears unusual.
Talk through the after-school routine with the child.
Consult with public safety officials about burglar-proofing and fireproofing the home.
Teach the child first-aid procedures.
Teach safety rules to the child who is expected to cook (microwave ovens are safest).
Emphasize fire safety rules and conduct practice fire drills.
Teach and reinforce traffic and bicycle safety.
Teach the child weather-related safety (e.g., stay inside but do not take a bath during an electrical storm; go to and stay in a storm cellar during a tornado warning).
Teach and reinforce water safety practices (e.g., warn the child not to go swimming alone; caution about safe bathing methods and keeping the toilet lid down when infants or toddlers are in their care).
Keep firearms securely locked away and teach the child that they are for adult use only.
Teach the child his or her home telephone number, address, and parents’ names.
Teach the child to tell callers that parents are “busy”; instruct the child not to tell a caller that parents are not at home.
Teach the child not to tell casual callers the home address; instruct the child to tell the caller that the parents cannot come to the phone right now and will call back later.
Keep a list of emergency numbers by the telephone. Make certain that the child knows how to report emergencies.
Have a list of telephone numbers of friends or neighbors who are available for help with emergencies.
Ask public safety officials to offer classes about when and how to call them.
If a telephone hotline for latchkey children exists, teach the child how to use it.
Arrange for the child to spend some afternoons with friends.
Provide structured activities for the child.
Have the child attend a public library–sponsored activity rather than watch television at home.
Discuss with the child things to do after school.
Emphasize positive aspects of independence and resourcefulness, but do not demand too much from the child.
Help the child feel successful in self-care.
Consider the potential problems of letting an older child assume care of younger ones before the child is developmentally ready.
Help the child talk about experiences and feelings about being alone after school.
Consider getting a pet to help provide company for the child.
Be punctual in arriving home. A child’s anxiety level accelerates when parents are not home when expected.
Call the child if there is a delay in arriving home.
Leave a tape-recorded message for the child to play on arrival home from school.
Form a group of parents with flex-time so that children can be cared for by one of the group after school.
Nurses should be aware of services in their communities designed to meet the needs of latchkey children and include this information in anticipatory guidance of school-age children and their families. It is vital that children have adequate supervision and companionship.
Promoting Optimum Health During the School Years
During the middle childhood years, children acquire increased cognitive skills that allow them to make decisions about health behaviors they will select and pursue. By the end of middle childhood, children should be able to assume personal responsibility for self-care in the areas of hygiene, nutrition, exercise, recreation, sleep, and safety.
Little is known about how school-age children acquire positive health behaviors. However, both boys and girls view themselves as healthy and can manage their own care in the areas of seat belt use, exercise, emergency situations, and dental health.
Health education is a primary component of comprehensive health care, and health education programs should promote desired health behavior through guided learning and modeling. An optimum program helps children learn about their bodies and about the effect of their behavior on their health.
Health promotion projects teach school-age children that social decision making to promote health is important. Children who attain skills in self-control, social awareness, and problem solving through classroom discussions and practice may engage in fewer risk-taking behaviors.
Children can also learn to take a more active role in relationships with health care providers. If asked what they would like to ask the health practitioner, most children are able to formulate several questions related to the reason for their visit. Providers can also teach children how to ask these questions so they can learn about their health during well-child visits to the pediatrician, nurse practitioner, or school nurse.
Nutrition
Although caloric needs are diminished in relation to body size during middle childhood, resources are being laid down for the increased growth needs of the adolescent period. It is important to impress on children and their parents the value of a balanced diet to promote growth (Box 17-2). When children enter school, they develop an eating style that is increasingly independent from parental influence and scrutiny. Parents do not know what their children eat when they are away from home. A parent may pack a lunch to be eaten at school but be unaware of how much is eaten, traded, sold, or thrown away.
Mealtime continues to be a central issue in many families. Although it should be a pleasant part of a child’s day, parents’ concern and emphasis on manners often make it a battleground. Likes and dislikes established at an early age continue in middle childhood, although the inclination for single-food preferences begins to end and children acquire a taste for an increasing variety of foods. Because children usually eat as the family does, the quality of their diet depends to a large extent on their family’s pattern of eating. Other interests and participation in outside activities often compete with mealtime.
Outside Influences
With the influence of the mass media and the temptation of an immense variety of “junk food,” it is all too easy for children to fill up on empty calories—foods that do not promote growth, such as sugars, starches, and excess fats. They have more freedom to move without parental supervision and often have small amounts of money to spend on candy, soft drinks, and other easily accessible treats. Midafternoon snacks are common, and it is wise to encourage consumption of fruit, nuts, and other wholesome finger foods to meet this need. Nutrition is a joint responsibility of both the child and the family.
The popularity of fast-food restaurants has aroused the interest of nutritionists and other health care professionals concerned with children’s nutrition. The restaurants provide fast service, they are relatively inexpensive and appealing to children, and their convenience makes them attractive to busy parents as an alternative to eating at home. Because the nutritional content of fast foods is usually available, it is easier for nutrition-conscious parents to help children select appropriate items from the available menu. Nurses can support consumer advocate groups to encourage restaurants to offer items higher in nutritional value (such as skimmed milk, broiled meats, and fresh fruits and vegetables) and to list ingredients on the menu as required for packaged foods.
Childhood obesity is an increasingly prevalent health problem in school-age children. It is estimated that approximately 17% of American children ages 6 to 11 years are overweight (Centers for Disease Control and Prevention, 2009b). The easy availability of high-calorie foods, the tendency toward more sedentary activities (such as watching television and playing or working at a computer), and the trend away from walking or cycling and toward transportation by automobile and bus have reduced caloric expenditure. The consumption of a high-fat diet also contributes to obesity. The problem of childhood obesity is discussed further in Chapter 21. Given the threat of obesity and a diet-conscious society, many school-age children start to diet in an effort to prevent obesity or lose weight or to conform to peer behaviors and pressures. Children need education about food selection and the importance of body-building nutrients as opposed to empty caloric intake.
School Programs
Working parents assume that their children are sufficiently mature and frequently leave the responsibility of meal preparation to them. Although most older school-age children are capable of preparing simple meals, all too often breakfast and lunch may be inadequate, makeshift, or nonexistent. In recognition of this problem, the federal government has established the National School Lunch Program and the School Breakfast Program in many areas. These meals must meet specified nutritional requirements and furnish one third of the daily recommended dietary allowance for children in the United States. Most schools subscribe to the programs, and although the results are difficult to measure directly, it is believed that these school meal programs positively influence the behavior and learning capacity of children. However, the average school lunch may also exceed the recommended dietary guidelines for saturated and total fat. In addition, children who purchase school lunches often select only the items they want. In general, food choices of American children do not meet recommended intakes outlined in the U.S. Department of Agriculture MyPyramid. Many Americans consume too many foods and drinks high in fat and carbohydrates and too little nutrient-dense foods and drinks such as fruits, vegetables, and low-fat milk (Wells and Buzby, 2008).
Nutrition Education: Nutrition education should be integrated throughout the school years into classroom learning. In school, children can learn daily food choices, serving sizes, portion control, and the elements of a wholesome diet using MyPlate (Box 17-3). (See Chapter 6.) Guidelines from the U.S. Department of Agriculture (2009) include the following:
BOX 17-3
SAMPLE MENU FOR SCHOOL-AGE CHILDREN BASED ON myplate
 cup shredded romaine lettuce, 2 slices tomato)
cup shredded romaine lettuce, 2 slices tomato) cup peas and onions with 1 tsp soft margarine
cup peas and onions with 1 tsp soft margarine cup dried apricots
cup dried apricotshttp://www.choosemyplate.gov/foodgroups/downloads/Sample_Menus-2000Cals-DG2010.pdf
• Balance food and physical activity: choose a lifestyle that combines sensible eating with regular physical activity.
• Choose a diet with plenty of nutrient-dense foods such as grain products, vegetables, and fruits.
• Choose a diet low in fat, saturated fat, and cholesterol.
• Choose protein foods that are lean.
The school nurse should take an active role in nutrition education and work with teachers to implement nutrition instruction that is relevant and interesting to children (see Box 17-2 and Critical Thinking Exercise). The U.S. Department of Agriculture also maintains a website called Team Nutrition that provides nutrition education information and resources for schools, students, parents, and communities.*
CRITICAL THINKING EXERCISE
Physical Growth in the School-Age Child
Janie, an 8-year-old girl, has just received her annual school physical examination. Janie weighs 30 kg (66 lb) and is 127 cm (50 inches) tall. Janie has gained 4.5 kg (10 lb) since last year and is otherwise reported as in good health with no acute illnesses.
1. Evidence—Is there sufficient evidence to draw conclusions about this situation?
2. Assumptions—Describe the underlying assumption about each of the following:
a. Changing eating patterns among children
b. Genetic, environmental, and societal risk factors associated with becoming overweight and obese
c. Comorbidities associated with overweight and obesity in children
3. What implications for nursing care can be drawn from this situation?
Sleep and Rest
The amount of sleep and rest required during middle childhood is highly individualized. The specific amount of needed sleep depends on the child’s age, activity level, and other factors such as health status. The growth rate has slowed; therefore less energy is expended in growth than during the preceding periods.
Sleep requirements decrease during school-age years; 5-year-olds generally require 11 hours of sleep, whereas 13-year-olds require approximately 9 hours of sleep (Smaldone, Honig, and Byrne, 2007). School-age children usually do not require a nap. Fewer bedtime problems occur during these years, but occasional difficulties are still associated with the necessary bedtime ritual.
Usually children 6 and 7 years old have few problems, and encouraging quiet activity before bedtime, such as coloring and reading, can facilitate the task of going to bed. Although most children in middle childhood must be reminded to go to bed, 8- to 9-year-old children and 11-year-old children are particularly resistant, with approximately 25% of all school-age children showing reluctance to go to bed (Spruyt, O’Brien, Cluydts, et al, 2005). Often children are unaware that they are tired; if they are allowed to remain up later than usual, they are fatigued the following day. Sometimes parents can resolve bedtime resistance by allowing a later bedtime in deference to their advancing age. Twelve-year-old children usually offer no difficulty in relation to bedtime. Some even retire early to enjoy slow preparations for bed, to read, or to listen to music.
A firm approach to bedtime is usually the most successful. Parents can help children by giving them a little advance warning, but children should realize that when the final bedtime is announced, the parents mean it.
Sleep Problems
During middle childhood, nighttime sleep is usually continuous, and the child has developed a repertoire of tactics (such as reading or playing quietly without involving the parents) to deal with occasional difficulties in falling asleep. If a child has a sleep problem, a thorough assessment may be necessary to plan appropriate interventions.
The cause of bedtime resistance is not always clear. For some children it is related to normal fears of their age, such as fear of the dark, strange noises, intruders, or other imagined phenomena. Children who are subject to frightening dreams are hesitant to retire, and their sleep is more likely to be disturbed after emotional stimulation before bedtime. Sometimes children are unwilling to give up an exciting or interesting activity, or they are reluctant to leave the protective social circle of the family. Another factor associated with reluctance to go to bed is related to status. For example, older children are given the privilege of a later bedtime than younger children. Promotion to a later bedtime is highly prestigious, and age-mates compare their bedtimes. This may explain why children who believe that playmates enjoy a more privileged position strongly oppose parental decisions. In some situations going to bed is used as a method of control. When going to bed early is imposed as a punishment or when staying up late is a reward, children may view bedtime as punitive or status degrading.
Some children resort to multiple “curtain calls,” such as wanting a drink of water, asking for one more story, needing to go to the bathroom, or wanting to watch television. Some children persist in coming out of their rooms repeatedly after being put back to bed. Some voice fears, such as “there is someone outside the window.” Parents may have difficulty determining whether the fear is legitimate or whether the behavior is a bid for attention. Consistent reassurance and limit setting usually resolve the problem. Children feel tense and insecure when limits are applied inconsistently, such as when parents grant permission one night and punish the next for the same behavior.
The night terrors of preschool children may be replaced by sleepwalking and sleep talking. Like night terrors, sleepwalking is associated with the transition from stage 4 to stage 1 of non–rapid eye movement sleep. When children arouse from stage 4 sleep, it is often difficult for them to reach a fully alert, wakeful state rapidly. Sleepwalking occurs in the first 3 to 4 hours of sleep. Children often have no memory of sleepwalking in the morning. The episode begins when the child sits up abruptly and walks. During sleepwalking, movements are clumsy and repetitive; parents often observe finger and hand movements. Most commonly, children move about restlessly, then lie down and return to sleep. However, they may get out of bed and engage in nonpurposeful walking. They rarely perform purposeful acts during sleepwalking. Any attempts to communicate with the child elicit only mumbled and slurred responses. Sleep talking, like sleepwalking, is not purposeful, and speech is usually incomprehensible and monosyllabic.
The best approach is to leave sleepwalking children alone unless they are in danger or may endanger others. However, clumsiness and stereotyped movements can make sleepwalking very dangerous. If the environment is not safe, children can get hurt. Instruct parents to gently redirect children back to bed without waking them, if possible. If children must be wakened, it is best to call them by name slowly and softly, orient them to where they are, explain that they were walking in their sleep, and assure them that it will not happen when they are more relaxed. Preventive measures include avoiding over-fatigue in children, making certain they get adequate rest, employing relaxation techniques, and relieving any stress the children may be experiencing.
Sleepwalking is usually self-limiting and requires no treatment. Persistent sleepwalking occurs in some older children and adolescents who are well behaved and tend to repress strong emotions, such as anger. They may benefit from learning to express their feelings and from doing self-relaxation before bedtime.
Nightmares are a part of the normal developmental process; 70% to 90% of young adults reported experiencing nightmares at some time during childhood (Schredl, Biemelt, Roos, et al, 2008). However, repetitive nightmares or increased nightmare frequency may indicate a specific underlying conflict or stressor that is strongly influencing the child’s behavior and thought. Resolving worries or stress will often reduce nightmares. If nightmares become chronic, parents should consider professional counseling (Schredl, Biemelt, Roos, et al, 2008).
A traumatic event often produces posttraumatic nightmares, which are anxiety provoking and literal in their depiction of the trauma. As time goes on, the dreams of affected children may consist of “modified repetitions” that may add more current material to the recurrent dreams (e.g., involving others who were not a part of the traumatic event). Current external stresses, movies, or stories may also precipitate a nightmare by reactivating old traumas. (For a comparison of nightmares and night [or sleep] terrors, see Table 15-2.)
Physical Activity
Exercise is essential for muscle development and tone, refinement of balance and coordination, gaining of strength and endurance, and stimulation of body functions and metabolic processes. Throughout middle childhood, children’s increasing capabilities and adaptability permit greater speed and effort in motor activities. Larger, stronger muscles with greater efficiency and skill permit longer and increasingly strenuous play without exhaustion. During this period children acquire the coordination, timing, and concentration that are required to participate in adult-type activities, even though they may lack the strength, stamina, and control of the adolescent and adult. Consequently, parents should expect and encourage a larger amount of physical activity during the school years.
Children should have opportunities that provide satisfying experiences to meet individual likes and dislikes. Children need space to run, jump, skip, and climb as well as safe facilities and equipment to use both inside and outside. Appropriate activities that promote coordination and development include running, rope skipping, swimming, roller skating, ice skating, and bicycle riding. Positive reinforcement achieved by experiencing increasingly smooth, rhythmic, and efficient use of the body conditions the child toward regular physical activity. However, one must keep in mind that although school-age children are large and appear to be strong, they may not be prepared for strenuous competitive athletics.
Most children need little encouragement to engage in physical activity. They have so much energy that they seldom know when to stop. However, children with disabilities or those who hesitate to become involved in active play, such as obese children, require special assessment and help in determining activities that appeal to them, are compatible with their limitations, and meet their developmental needs. Parents also need to limit television viewing to encourage outside activities.
Physical Fitness
The development of physical fitness is a goal for all children. This goal was easy to accomplish in the past when school-age children spent a considerable amount of time each day playing on playgrounds, walking to school, and participating in games or sports at school or in their communities. With the advent of technology and the information age, many children are less active physically and spend large portions of their day in front of a computer or television (see Research Focus box).
 RESEARCH FOCUS
RESEARCH FOCUS
Strategies to Increase Physical Activity in Children
Strategies focusing on increasing physical activity and reducing sedentary behavior have become a priority; however, only 8% of elementary schools and 6% of middle schools in America provide daily physical education classes (Bagby and Adams, 2007). Recent studies show less than 25 minutes of school time is spent in moderate to vigorous physical activity each week (Bagby and Adams, 2007). Furthermore, some students offset any increased activity during school with little to no exercise outside of school (Cawley, Meyerhoefer, and Newhouse, 2007).
Counseling should include developing goals, identifying fun and safe physical activities, addressing potential barriers, and encouraging support from family and friends. Nurses can further promote efforts to include physical fitness in school programs and encourage children to engage in aerobic physical activities during their free time. Such activities provide cardiopulmonary benefits, maintain normal weight, and have the potential to contribute to lifelong fitness.
Sports: Much controversy has surrounded the trend toward earlier participation in competitive athletics and the amount and type of competitive sports that are appropriate for children in the elementary grades. The current view is that virtually every child is suited for some type of sport, and authorities do not discourage participation if children are matched to the type of sport appropriate to their abilities and to their physical and emotional constitutions. School-age children enjoy competition, and when teachers, parents, and coaches understand children’s physical limitations and teach them the proper techniques and safety measures to avoid injury to developing bones and muscles, a safe and appropriate sport can be found for even the most unskilled and uncompetitive child.
During middle childhood, girls have the same basic structure as boys and thus have a similar response to systematic exercise training. At puberty, when boys become larger and have more muscle mass, it is usually recommended that girls compete only against other girls. Before puberty there is no essential difference in strength and size between girls and boys, which makes these precautions unnecessary.
Well-organized extracurricular sports programs based in the community or school encourage enjoyment of sports and fitness in childhood (Box 17-4). Preadolescence is a time to teach fundamental motor skills; develop fitness in a practical, safe, and gradual manner; and promote desired attitudes and values. Activities should include practice sessions and unstructured play. The actual game or event should be managed in a manner that stresses mastery of the sport and enhancement of self-image rather than winning or pleasing others. All children should have an opportunity to participate, and special ceremonies should recognize all participants rather than individuals.
In addition to ensuring the interest, suitability, and safety (Box 17-5) of the sport, parents must make certain that coaches (if involved in the sport) are skillful in managing children and do not engage in abusive behavior. Coaches, parents, and others involved in children’s sports play critical roles in shaping children’s self-esteem. Any sport for children should emphasize the pleasure of the activity. It is wise to expose children to a variety of individual sports. The overall emphasis of both team and individual sports should be on playing and learning. Parents who pressure their children to perform beyond their capabilities run the risk of the child’s being injured, developing a dislike for the activity, and developing a lowered self-image (see Family-Centered Care box).
FAMILY-CENTERED CARE
Athletic Stress in School-Age Children
Participating in a competitive sport should be an enjoyable experience for school-age children. For some children, however, this activity is associated with considerable stress and anxiety. Their parents’ reaction to their performance serves as the source of this stress. Children state that they feel awful when they strike out or are unable to catch a fly ball or when their team loses a game. These children report that their parents often yell at them and are more upset over a lost game than their coach is. Children notice that their mothers and fathers consider themselves a failure if their child is not a star player.
Parents of children who participate in competitive sports need to praise and support their children regardless of whether games are won or lost. Parents need to avoid the temptation to identify with their child. Parents’ success and self-worth should not depend on whether their child wins. At the very minimum, parents should monitor their behavior at games and avoid criticizing their child, other players, the officials, or the coaches.
The same principles described in the preceding paragraphs apply to children with chronic illnesses, such as diabetes, epilepsy, asthma, or allergies, if the disorder is mild and can be controlled with medication. Children with cognitive impairment do not need to be excluded from sports competition if they are matched evenly against other children of equal abilities and provided with skilled supervision and coaching. Some activities need to be modified to accommodate the skills of these children.
Acquisition of Skills
School-age children demonstrate increasing capacity in fine muscle facility and complex artistic skills. Handedness is well established by the beginning of the school years, and children make great strides in writing and drawing during this age period. It is a time of energetic and vibrant creative productivity. With the tools of language and reading, children can create poems, stories, and plays. With more advanced fine motor skills, they are able to master an unlimited variety of handicrafts, such as ceramics, needlework, wood carving, and beadwork. They avidly pursue these skills in solitude, with a friend, or in programs offered through organizations such as boys’ or girls’ clubs or special interest groups that use crafts as a means to occupy, entertain, and educate children.
Music is a favorite form of expression in middle childhood (Fig. 17-13). Music stimulates and invigorates school-age children. They can sing in harmony, play instruments in orchestras and bands, and manage music at a more complex level. They can compose original songs, learn lyrics almost effortlessly, and turn any empty moment into an occasion for singing.

School-age children are capable of assuming responsibility for their own needs, although their distaste for soap and water and “dress” clothes is legendary. School-age children can and want to assume their share of household tasks, which usually are related to the male and female roles that have been defined by their culture (Fig. 17-14). Many also assume responsibility for tasks outside the home, such as baby-sitting, yard work, or paper routes.

Television, Videogames, and the Internet
For some time, child development specialists and parents have been concerned about the effect of media on child development and behavior. Children spend a significant amount of time each day involved in media-related activities, including the use of television, computers, videogames, and CD players. Children ages 8 to 18 years spend close to 4 hours every day watching television or videos, with 20% of these children watching more than 5 hours a day (Rideout, Roberts, and Foehr, 2005). Because of the long periods of exposure, the media have more time to develop children’s attitudes than do parents and teachers.
There is no doubt that children learn from television, but the values and attitudes depicted on television are not always realistic and may conflict with values that children were previously taught. School-age children can distinguish fantasy from reality, and some have had sufficient life experience to view television programs with skepticism. However, television rarely depicts the reality of day-to-day situations that confront children. When children view characters they admire using violence, such as Superheroes, it can teach them to become more violent (Christakis and Zimmerman, 2007). In addition, repeated exposure to violence can desensitize children to violence, can convey a message that violence is acceptable, and can teach children that initiating violent behavior is a way to protect themselves (Christakis and Zimmerman, 2007).
Violence in the media can also increase fear and anxiety in children. Events such as the 9/11 terrorist attacks and the war in Iraq have infiltrated television, frequently exposing children to real-life violence. Viewing violence in the news causes more fear and worry in children than viewing the same content in a fictional setting (Van Der Molen and Bushman, 2008).
Parents should make the ultimate decisions about which programs their child will watch. To reduce exposure to violence and maximize the beneficial effects of television, parents are advised to monitor program selection, view programs with their children, and discuss program content when the programs are finished (Christakis and Zimmerman, 2007). (See Chapter 2 for a more in-depth discussion of children and television.)
Videogames have been both criticized and supported in relation to their effect on children and adolescents. Critics maintain that videogames keep children from schoolwork and can cause tension, sleeplessness, and violence. Others support the activity as a means for improving eye-hand coordination and as a substitute for the inactivity of passive television viewing. Benefits may also include development of inductive reasoning (drawing generalizations from specific observations), improving spatial perception, and learning to handle multiple variables that interact simultaneously.
Research suggests that videogames may affect physical and psychologic functioning. Physical effects may include triggering of epileptic seizures. (See seizure discussion, Chapter 37.) However, research has noted some positive applications of videogames with dyslexic children (American Psychological Association, 2005).
Computers and the Internet are becoming a popular means for obtaining educational and recreational information. Children with home computers increased from 73% in 2000 to 86% in 2005, and an estimated 45 million U.S. children ages 10 to 17 years use the Internet every day (Rideout, Roberts, and Foehr, 2005; Williams and Guerra, 2007). Although the Internet provides valuable educational opportunities for children, there are also many risks that parents must acknowledge before children access the Internet. Major risks include exposure to inappropriate, dangerous, or illegal material; exposure to harassment through e-mail or chat rooms; revelation of financial information that leads to negative consequences; and safety issues relating to sharing personal information or meeting strangers (McColgan and Giardino, 2005). The best way to eliminate potential risks is to educate parents and children about the Internet and to provide adult supervision when children use the Internet.
Parent and teacher education relating to television, videogames, and the Internet should include recommendations to limit playing time, monitor game selection and content, and increase access to games and information that are educational.
Dental Health
The first permanent (secondary) teeth erupt at about 6 years of age. Before their appearance they have been developing in the jaw beneath the deciduous (primary) teeth. The roots of the latter are gradually absorbed, so that when a deciduous tooth is shed, only the crown remains. At 6 years of age, all of the primary teeth are present, and those of the secondary dentition are relatively well formed. Eruption of the permanent teeth begins with the 6-year molar, which erupts posterior to the deciduous molars. The others appear in approximately the same order as in eruption of the primary teeth and follow shedding of the deciduous teeth (Fig. 17-15).
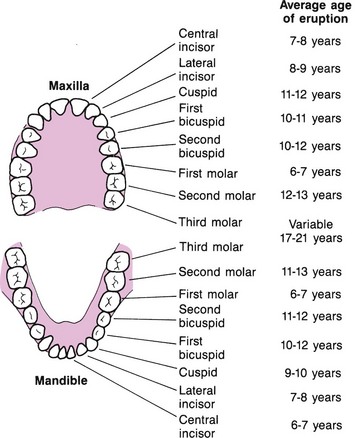
Fig. 17-15 Sequence of eruption of secondary teeth. (Data from Dean JA, McDonald RE, Avery DR: McDonald and Avery dentistry for the child and adolescent, ed 9, St Louis, 2011, Mosby.)
The pattern of shedding of primary teeth and eruption of secondary teeth is subject to wide variation among children. To allow the larger permanent teeth to occupy the limited space left by shed primary teeth, a series of complicated changes must take place in the jaws. At this time many of the difficulties created by crowding of teeth become apparent. With the appearance of the second permanent (12-year) molars, most of the permanent teeth are present. The third permanent molars, or wisdom teeth, may erupt from 18 to 25 years of age or later. Permanent dentition is somewhat more advanced in girls than in boys.
Because permanent teeth erupt during the school-age years, good dental hygiene and regular attention to dental caries are vital parts of health supervision during this period. Caries is a common problem, affecting as many as 57% of American school-age children (Wagner and Oskouian, 2008). Children of this age tend to become careless about oral hygiene unless they are carefully supervised. Although children are assuming more responsibility for their own care, they are not as motivated by improved appearance and odor as they will be during adolescence. School nurses should be alert for opportunities to teach correct brushing and flossing techniques; to reinforce avoidance of fermentable carbohydrates and sticky sweets; and to be alert for problems of malocclusion, toothache, and mouth infections.
Comprehensive dental supervision should be an integral part of the health maintenance program. Regular dental prophylaxis (teeth cleaning) by a dentist or dental hygienist and continued fluoride supplementation are essential to decrease the susceptibility of the tooth enamel to acid breakdown. (See Chapter 14 for a discussion of fluoride and other aspects of dental care.)
Brushing
The most effective means of preventing dental caries is a regimen of proper oral hygiene tailored to the individual child by the dentist. Children should learn to carry out their own dental care with the supervision and guidance of parents. Parents should learn proper brushing technique along with their children and should inspect their children’s efforts until the children can assume full responsibility for their own care.
Most practitioners believe that the majority of children do not possess the fine motor skills needed to brush their teeth properly until approximately second grade. Children under 10 years of age may need parental assistance to brush back teeth. Ideally, children should brush teeth after meals, after snacks, and at bedtime. The bedtime brushing is especially important because there is more time overnight for interaction between oral bacteria and unremoved substrate on the tooth substance. Children who brush their teeth frequently and become accustomed to the feel of a clean mouth at an early age usually maintain the habit throughout life.
The thoroughness of plaque removal (cleaning) can be checked using a plaque-disclosing agent that stains any remaining plaque red. The child should inspect the teeth closely with the aid of a mirror and under adequate light. The teeth then are again cleansed with a fluoridated dentifrice to remove the remaining plaque and provide further protection. This procedure may be carried out regularly or occasionally, according to instructions from the child’s dentist. Toothpastes recommended by the American Dental Association Council on Dental Therapeutics carry a seal of approval, which is easily identified on the package. They have been submitted to testing and demonstrate the ability to reduce the incidence of dental caries when used correctly.
For school-age children with mixed and permanent dentition, the best toothbrush is one with soft nylon bristles and an overall length of about 21 cm (8 inches). There are numerous methods of brushing the teeth for children, but no conclusive evidence indicates that one method is superior to another. The thoroughness of the cleaning is more important than the specific technique used. The dentist will assess all factors, such as the child’s manipulative skills and special needs, and suggest the most appropriate brushing technique and regimen. Flossing follows brushing. Parents usually floss until children acquire the manual dexterity needed. Most children are not able to floss properly until about 8 or 9 years of age.
School Health
Child health maintenance is ultimately the responsibility of parents; however, public schools and health departments in the United States have contributed to the improvement of child health by providing a healthful school environment, health services, and health education functions that emphasize sound health practices. These functions constitute major components of community health services and involve large amounts of public funds and many health professionals, including nurses.
A safe and healthful school environment is an essential element of any school health program. Conditions within the school must contribute to the physical, mental, and social development and well-being of the children. One model that has been used to provide information about the essential components of school health is the Coordinated School Health Program (Centers for Disease Control and Prevention, 2008). The eight basic components of this program are a healthy school environment; health services; health education; nutrition services; counseling, psychologic, and social services; health promotion for staff; physical education; and family and community involvement in school health (Centers for Disease Control and Prevention, 2008). See Boxes 17-6 and 17-7 for factors that contribute to a healthful school setting and for characteristics of school health programs.
Health Education
Health education of school-age children focuses on providing knowledge of health and influencing habits, attitudes, and conduct in relation to health (Box 17-8). A viable health education program is based on sound health concepts but should be adjusted to meet specific local needs, objectives, and legal requirements. Parents must understand and approve the health education curriculum so that its teaching will be reinforced at home. A comprehensive approach to health education is more successful in developing positive health practices than one in which the subjects are taught in isolation. Many topics presented in health education classes are associated with differing social and cultural attitudes and should be presented accurately and with sensitivity to these attitudes.
Health education concerning AIDS is a specific example. Most authorities agree that AIDS education should begin in the elementary grades to prevent high-risk behaviors. However, educational programs concerning AIDS must be developmentally appropriate and, to be effective, must be implemented with parental and community support. Young children need information on how HIV is transmitted, in simple, accurate terms without elaborate, unnecessary discussions of sex. Misconceptions that increase children’s anxiety about contracting the virus should be corrected. Although many children have heard that sex and drugs cause AIDS, some children also have misconceptions about AIDS. Children need information that HIV is transmitted through infected blood on shared drug needles and that the virus is not spread through common forms of expressing affection such as hugging and holding hands.
School Nursing Services
School nurses assume a major role in the school health program and can affect the lives of school-age children significantly. Working in collaboration with others in the school and community, school nurses provide health supervision, health counseling, and health education. The responsibilities of the school nurse can include providing education and interventions for acute and chronic illness, injuries, communicable diseases, obesity and nutrition, mental health, dental disease, and sexually transmitted infections (American Academy of Pediatrics, 2008b). These functions are not necessarily limited to the confines of the school environment but extend into the community in which the students live. As a health practitioner, the school nurse is in a position to promote and evaluate health services throughout the community as they affect children and to collaborate with agencies in planning for health and safety. For some children, especially those in poverty, the school nurse may be the only contact with illness prevention and health promotion. For children with chronic health conditions, the school nurse provides leadership within the school health team and assesses the student’s health status, identifies potential barriers of the educational process, and develops an individualized health care plan (American Academy of Pediatrics, 2008b).
Traditionally, school nurses have been viewed from a limited perspective that placed them in the role of disease detector, applier of bandages, and official caregiver in cases of illness and injury. Although these are still important functions, this traditional role has acquired much broader dimensions. School nurses develop, implement, and evaluate health care plans and programs. In some settings a school-based health center is near or within a school to provide additional health services. In these centers, school nurse practitioners provide primary health care, including assessment of physical, psychomedical, psychoeducational, behavioral, and learning disorder problems, as well as comprehensive well-child care (American Academy of Pediatrics, 2008b).
The minimum qualifications for a school nurse should include a baccalaureate degree from an accredited college or university and licensure as a registered nurse (American Academy of Pediatrics, 2008b). Unlicensed assistive personnel (UAP) may be a part of the school health care team. These paraprofessionals have a state certification and are trained to assist a professional but must be supervised by the school nurse (American Academy of Pediatrics, 2008b). The school nurse must use good assessment and professional judgment in deciding which procedures may be delegated to UAP.
NURSING ALERT
In the delegation or transfer of responsibility for the performance of an activity to an assistant, the nurse remains accountable for the outcome.
The passage of Public Laws 94-142 and 99-457 required the integration of children with chronic illness or disability into regular classrooms. School nurses are responsible for the medical and nursing needs of these children in the school setting. School nurses assess and monitor all health problems in children who come into the school and compile a health care list of all of these problems and their associated therapies. The nurse may call the parents of the child and arrange a visit to the home, made by either the school nurse or a public health nurse. After gathering information, the nurse can develop a nursing care plan for use in the school. The nurse collaborates with the family and includes their suggestions in the care plan. The nurse then discusses the plan with the child’s teachers and provides any needed education. School nurses are the only ones in the school system qualified to deal with medical problems. However, in many instances school nurses can collaborate with teachers to provide atraumatic care (see Community Focus box).
COMMUNITY FOCUS
Collaboration Between School Nurse and Teachers
• All students should have health cards completed by their parents.
• All teachers should receive a list of students who have health problems.
• Teachers should have a code to highlight students with health needs in their grade books so that substitute teachers can recognize these students and intervene immediately if problems occur in the classroom.
• Teachers should schedule students who miss physical education into an adaptive physical education class if possible.
• All students with asthma should have their metered-dose inhalers available to them for emergency use in physical education and all other classes.
• Adult volunteers should serve as team captains for games; selections of team members should be supervised so that one team is not stacked with all the good players.
• In physical education, evaluation of a skill or activity should be repeated several times if some students score extremely high and others extremely low, since every child has good and bad days.
• Teachers should never question a child’s ability in front of other students.
• Nurses should maintain privacy for height and weight checks and for vision and hearing tests (students should be taken into the nurse’s office individually so other students do not hear the test results).
Suggestions submitted by Linda L. Smith, Health/Physical Education Teacher.
Sometimes all that is required is conducting an assessment and making the teacher aware that the child has a health problem. In other cases more complex teaching is needed, such as how to observe for certain signs (e.g., insulin reaction), how to perform certain techniques (e.g., tracheostomy suctioning, gastrostomy or nasogastric tube feedings), and how to manage emergencies (e.g., care of a child during a seizure). School nurses instruct teachers in the necessary procedures and review their performance.
The American Academy of Pediatrics (2008a) has established guidelines for emergency medical care of children in schools. These guidelines include developing emergency policies and procedures, clarifying school staff roles, collecting emergency data on all school children, making emergency equipment and medication easily accessible, and adequately training staff. It is recommended that at least one staff member, in addition to the school nurse, have cardiopulmonary resuscitation, first aid, and automated external defibrillator training (American Academy of Pediatrics, 2008a).
A child who must take medication at school needs written authorization from his or her attending physician and/or written permission from the parents allowing the nurse to administer or supervise the administration of the medication. The medication must be brought to the school in a container appropriately labeled by the pharmacist or physician. Medications are kept locked up in the nurse’s office; usually the child is not allowed to carry medications at school. The policy may vary in some school districts or situations. For example, some children may be allowed to carry metered-dose inhalers that contain their asthma medication, provided that their physician and a parent provide the required authorization. Guidelines for administration of medications in schools are also available from the National Association of School Nurses.*
Injury Prevention
 Because school-age children have developed more refined muscular coordination and control and can apply their cognitive capacities to select a more judicious course of action, the incidence of unintentional injury is diminished in children in this age-group compared with the incidence in early childhood. School-age children have exposure to more environments in which they need protection, they acquire skills and interests that expose them to new perils, they have less supervision, and they take more responsibility as they begin to participate in the adult world.
Because school-age children have developed more refined muscular coordination and control and can apply their cognitive capacities to select a more judicious course of action, the incidence of unintentional injury is diminished in children in this age-group compared with the incidence in early childhood. School-age children have exposure to more environments in which they need protection, they acquire skills and interests that expose them to new perils, they have less supervision, and they take more responsibility as they begin to participate in the adult world.
 Critical Thinking Exercise—Injury Prevention
Critical Thinking Exercise—Injury Prevention
Injuries most prevalent in school-age children reflect their developmental stage. Table 17-2 outlines the developmental characteristics and accomplishments of middle childhood that predispose children to physical injury and offers guidelines for injury prevention.
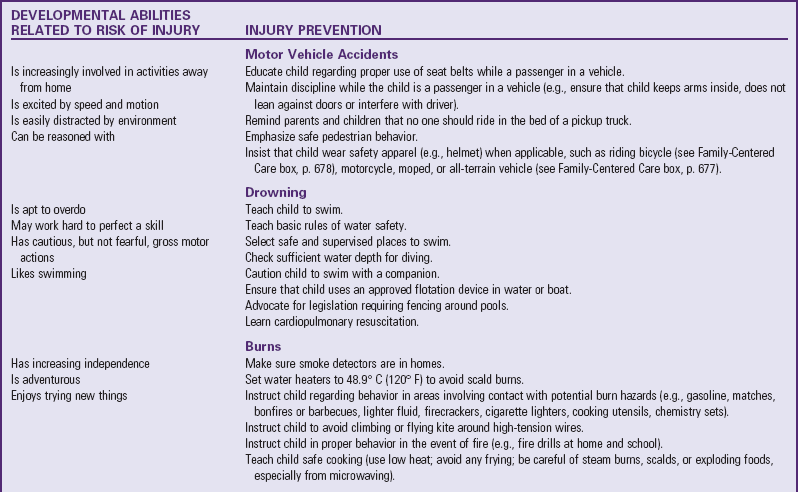
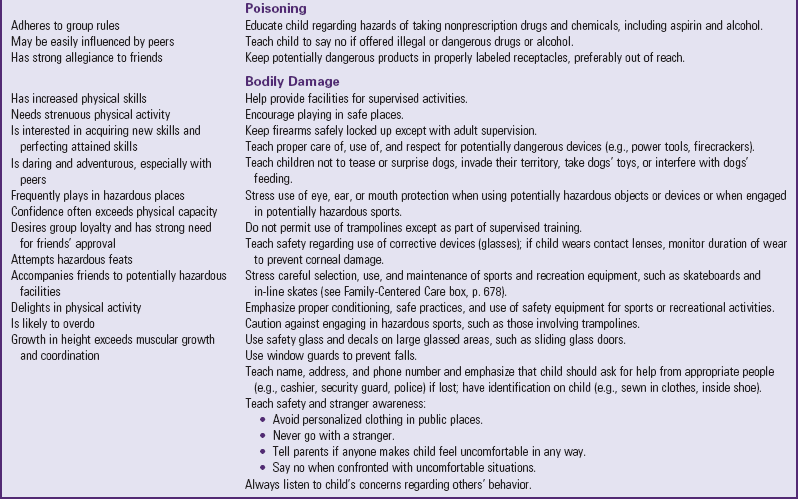
The incidence of injury during middle childhood is significantly higher in school-age boys than in school-age girls, and their death rate is twice that of girls. (See Chapter 1.) Most injuries occur in or near the home or school. The prevalence of injury depends on the dangers present in the environment, the protection offered by adults, and the behavior patterns of the children. Although school-age children are conscious of rules and frequently impose them in relationships with peers, they also tend to challenge established rules. It is often difficult to maintain a balance between the level of supervision and restriction needed by children and their need for freedom and independence.
The incidence of transportation-related injuries is higher in school-age children than in younger children, and the incidence of bicycle injury not involving a motor vehicle is higher than that in teenagers and preschool children. Injuries from burns and poisonings are lowest in school-age children. However, physically active school-age children are highly susceptible to cuts and abrasions, and the incidence of childhood fractures, strains, and sprains is impressive.
Risk-Taking Behavior
Achieving social acceptance is a primary objective for school-age children. They often attempt dangerous acts (sometimes extreme behaviors) to prove themselves worthy of acceptance and improve their status in the peer group. Peer pressure is a normal part of psychologic development, but it is also a major contributor to risk-taking behaviors. Peer challenges often encourage problem behaviors that place children at risk for injury or hazardous habits. School-age children are in the process of moving from preoperational to concrete operational thinking and are only beginning to understand causal relationships. Therefore they may attempt certain activities without planning or evaluating the consequences.
Children who are risk takers may have inadequate self-regulatory behavior. These children need to learn the motivation or the incentives for such behavior and to visualize the possible consequences if the risk-taking behavior ends in a tragic outcome.
Motor Vehicle Injury
As in all other age-groups, the most common cause of severe accidental injury and death in school-age children is involvement in motor vehicle accidents—either as a pedestrian or as a passenger. In 2007 approximately 18% of traffic-related fatalities involved pedestrians (National Highway Traffic Safety Administration, 2007). Most of the injuries occur when children misinterpret traffic signs or disobey common traffic safety regulations, cross the street against a red light, cross at places other than designated crosswalks, dart into the street, or walk in the same direction as the traffic. Parents consistently overestimate the street-crossing skills of young children ages 5 to 6 years and need education about their children’s developmental abilities and competence as pedestrians. Nurses can help parents to develop more realistic expectations of their children’s behavior and teach them to model safe street-crossing behaviors through pedestrian skills training programs.
Use of restraint systems, door-lock mechanisms, and appropriate passenger seating and behavior are simple but effective measures for eliminating noncrash injuries and reducing the severity of crash injuries. The importance of the correct use of seat restraints is essential. School-age children do not usually require special car seats. However, despite evidence that safety belt use saves lives and prevents injury, estimates of seat belt use in school-age children are still discouragingly low.
In 2006, 1335 children ages 0 to 14 years died in motor vehicle accidents and 184,000 received injuries requiring emergency department treatment (Centers for Disease Control and Prevention, 2009a). Investigations of motor vehicle accidents showed deployment of passenger-side air bags critically or fatally injured children seated in the right front seat (Newgard and Lewis, 2005). Therefore the National Highway Traffic Safety Administration recommends that children under age 13 years not ride in the front passenger seat of vehicles with air bags.* The American Academy of Pediatrics reiterates this view and strongly emphasizes that the rear seat of any vehicle is the safest place for children to ride. When in the car, school-age children should always be buckled properly in a weight-, height-, and age-appropriate seat. If the child weighs more than 18 kg (40 lb), a convertible safety seat that is positioned in the semiupright and forward-facing position may be used if the child fits in it well. If the child has outgrown the convertible safety seat but is still too small for a regular lap-shoulder belt, a booster seat restraint device equipped with a combination lap-shoulder belt should be used.
Injuries to children ages 5 to 9 years restrained in adult-type seat belts are related to anatomic differences between adults and children. The child’s sitting height is less than the adult’s, and the child’s center of gravity is located above the level of the lap belt. Consequently, the greater proportion of body mass above the belt may cause more forward motion and jackknifing over the belt, which increases the risk of head injury from impact with interior vehicle parts. The child’s smaller and less developed iliac crests are not suited to serve as an anchor for belts designed to restrain adults, and their intra-abdominal organs are less protected by the bony pelvis. The natural behavior of children, such as readjusting the seating position, moving about, and otherwise altering the fit of the restraint, also influences its effectiveness.
When children use adult-type seat belts, parents should make certain that the restraints are fitted to their children and fastened correctly. To reduce their risk of sliding beneath the standard seat belt during a collision, children should sit up straight and well back in the seat, and the seat should be moved forward until the feet fit firmly against the toe board. Caution children against assuming alternate seating positions, such as tailor fashion, while riding in the car. (See Chapter 14 for a comprehensive discussion of safety restraints.)
Each year 23.5 million children are transported to and from school on school buses. The majority of school travel–related injuries and deaths occur from passenger vehicles, while only 4% of school travel injuries and 2% of school travel deaths occur in school buses (American Academy of Pediatrics, 2007). However, the National Highway Traffic Safety Administration and the American Academy of Pediatrics have developed minimum standards to enhance school bus safety. These standards state that all children should travel to and from school in an age-appropriate, properly secured child-restraint system; all school buses should be equipped with lap-shoulder restraint systems that can accommodate safety seats, booster seats, and harness systems; and school districts should encourage appropriate education on safety devices (American Academy of Pediatrics, 2007).
All-terrain vehicles (ATVs), designed for off-road use by children and adolescents, are popular with children under 16 years of age but are responsible for a significant number of childhood injuries. These vehicles have a short wheelbase and low profile, which makes them relatively unstable and unable to be seen easily. The vehicles can also achieve substantial speed. Most injuries occur when the driver loses control of the vehicle, is thrown from the vehicle, or collides with fixed objects or other vehicles. Immature judgment and poorly developed motor skills also contribute to injury. The American Academy of Pediatrics views ATVs as a major hazard to the health of children, opposes their use by children younger than 16 years of age, and has created a safety bill outlining requirements to enhance ATV safety (Killingsworth, Tilford, Parker, et al, 2005). However, for parents who allow their use, the committee provides safety guidelines (see Family-Centered Care box).
FAMILY-CENTERED CARE
Safe Use of All-Terrain Vehicles
• Children under the age of 16 years should not operate an off-road vehicle.
• Vehicles should be sturdy and stable; quality construction is essential.
• Riders should receive instruction from a mature, experienced cyclist or a certified instructor.
• Riding should be supervised and allowed only after the rider has demonstrated competence in handling the machine on familiar terrain (preferably require licensing).
• Riders should wear approved helmets, eye protection, and protective reflective clothing (e.g., trousers, boots, gloves).
• Parents should prohibit street use of off-road vehicles.
• Riding should be restricted to familiar terrain.
• Nighttime riding should not be allowed.
• Vehicle should not carry more than one person.
• Vehicles should include seat belts, roll bars, and automatic headlights.
Modified from Killingsworth J, Tilford J, Parker J, et al: National hospitalization impact of pediatric all-terrain vehicle injuries, Pediatrics 115(3):e316-e321, 2005.
Bicycle Injury
The majority of school-age children have bicycles and love riding them, but this increases their risk of injury on streets and byways. In 2008 bicycle injuries in children ages 5 to 15 years accounted for approximately 13,000 nonfatal injuries and 89 fatal injuries (National Highway Traffic Safety Administration, 2008).
Many injuries are related to violations of traffic laws by the bicyclist, including wrong-way riding (facing traffic), failure to yield the right of way, and turning violations. Others are related to road conditions described as hazardous: bumps, potholes, and gravel. Bicycle-related injuries occur in young children playing in their own neighborhoods and in older children using their bicycles for transportation on streets with heavy traffic.
In addition to major injuries, cuts and bruises from falls and collisions account for a large number of injuries. Other injuries include trauma to internal organs. These injuries initially seem trivial, but injured children can develop serious symptoms (e.g., pain, vomiting, or collapse) hours later.
Many of the injuries to school-age children on bicycles occur because of the child’s developmentally limited range of vision and their inability to process perceptions of road situations sufficiently well and quickly enough to ride safely in traffic. Other important factors are lack of instruction in use of the equipment, lack of safety equipment, and unfamiliarity with the bicycle (e.g., having ridden the bicycle for less than a month).
To prevent bicycle injuries, both parents and children should learn and periodically review bicycle safety. Children need bicycles that are suited to their size and age; they should be able to stand with the balls of both feet on the ground when seated on the bicycle, be able to place both feet flat on the ground when straddling the center bar, and be able to grasp the brake lever comfortably and easily enough to apply sufficient pressure to brake the bicycle. Discourage parents from buying their child a bicycle that the child can “grow into.”
Because head injury is the major cause of bicycle-related fatalities, the single most important aspect of bicycle safety is to encourage the rider to wear a protective helmet (Fig. 17-16). Helmet use has caused an 88% reduction in head and brain injury and 65% reduction in face-related injuries (Okun and Adam, 2008). Hard-shelled helmets lined with expanded polystyrene (Styrofoam) provide the best head protection. The helmet should be one that can be adjusted to the individual child’s head, fits securely, and does not limit the child’s vision or hearing. A brightly colored helmet improves visibility. The helmet should carry a seal indicating that it is approved by the U.S. Consumer Product Safety Commission. All helmets should be replaced after any damage or crash.
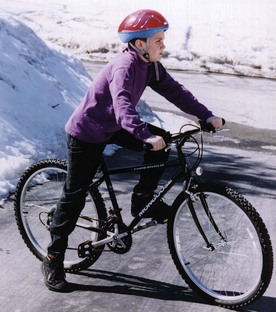
Fig. 17-16 The right-size bike is important; the child should be able to sit on the bike and place the balls of both feet on the ground. The foot should comfortably reach and manipulate the pedal in the down position. Wearing a protective helmet is mandatory for safe cycling. The helmet should sit on top of the head in a level position and should not rock back and forth or from side to side. The strap should always be fastened securely under the chin.
Legislative interventions and educational campaigns have significantly increased children’s usage of bicycle helmets, with two- to five-fold increases in some areas of the United States (Okun and Adam, 2008). Although most young riders acknowledge that wearing a helmet is important for safety, reasons for not wearing them include discomfort (especially heat), presumed lack of importance for casual riding, lack of style, and peer pressure.
Parental attitudes and behaviors also influence children’s use of bicycle helmets. Parental nonuse of a helmet is strongly associated with lack of intention to require the children to use helmets. Parents, as well as children, need to be educated on safety. The American Academy of Pediatrics recommends that (1) parents be informed of the dangers of riding without a helmet, (2) retail outlets carry inexpensive helmets available at the time of bicycle purchase, (3) state and local governments continue to enact legislation requiring helmet use by all bicyclists, (4) parents and community-based programs promote bicycle safety and helmet use, and (5) the media depict helmet use in all programs and promotional materials.
Schools, hospital emergency departments, and communities have developed numerous bicycle helmet promotion programs. Programs that are most successful are those that address the cost of helmets and peer pressure and combine multimedia public education announcements with the support of community organizations. The Family-Centered Care box lists guidelines for bicycle safety, and the Critical Thinking Exercise discusses bicycle helmets.
FAMILY-CENTERED CARE
Bicycle Safety
• Always wear a properly fitted helmet that is approved by the U.S. Consumer Product Safety Commission; replace a damaged helmet.
• Ride bicycles with traffic and away from parked cars.
• Walk bicycles through busy intersections and at crosswalks.
• Give hand signals well in advance of turning or stopping.
• Keep as close to the curb as practical.
• Watch for drain grates, potholes, soft shoulders, and loose dirt or gravel.
• Keep both hands on handlebars except when signaling.
• Never ride double on a bicycle.
• Do not carry packages that interfere with vision or control; do not drag objects behind bike.
• Watch for and yield to pedestrians.
• Watch for cars backing up or pulling out of driveways; be especially careful at intersections.
• Look left, right, then left before turning into traffic or roadway.
• Never hitch a ride on a truck or other vehicle.
• Learn rules of the road and respect for traffic officers.
• Wear shoes that fit securely while riding.
• Wear light colors at night, and attach fluorescent material to clothing and bicycle.
• Be certain the bicycle is the correct size.
• Equip the bicycle with proper lights and reflectors.
• Have the bicycle inspected to ensure good mechanical condition.
• When riding as a passenger, wear appropriate-size helmet and sit in a specially designed protective seat.
Modified from American Academy of Pediatrics, Committee on Injury and Poison Prevention: Bicycle helmets, Pediatrics 108(4):1030-1032, 2001.
CRITICAL THINKING EXERCISE
Bicycle Helmets
During the past month in your school district, one child died and another sustained a serious head injury from bicycle-vehicle collisions. Neither child wore a bicycle helmet. As a school nurse, you are considering effective approaches to increase the students’ use of bicycle helmets.
1. Evidence—Is there sufficient evidence to draw any conclusions?
2. Assumptions—Describe the underlying assumption about each of the following:
a. Potential hazards to children associated with bicycling
b. Intrinsic and extrinsic risk factors for bicycle injuries
c. Factors associated with deciding whether to wear a bicycle helmet
d. Strategies for pediatricians and nurses to help decrease bicycle-related injuries
3. What implications for nursing care can be drawn from this situation?
Other Vehicle-Related Injuries
After a short period of decline, skateboards are again becoming popular, with an accompanying resurgence of related injuries. Although the majority of injuries involve the extremities, severe injuries of the head and neck can occur. School-age children often use their skateboards on streets and highways, which increases the likelihood of high-speed collisions with objects or vehicles. Recommendations for safe skateboard use are in the Family-Centered Care box.
FAMILY-CENTERED CARE
Skateboard and In-Line Skate Safety
• Children younger than 10 years of age should not use skateboards without close supervision by an adult. They are not developmentally prepared to protect themselves from injury.
• The age when children are ready to use in-line skates safely is not known because of differences in the ability to acquire the skills needed to participate in the sport. Novice skaters should learn indoors on a flat, smooth surface.
• Children who use skateboards and in-line skates should wear helmets and protective padding, especially on wrists, knees, and elbows, to prevent injury.
• Skateboards and in-line skates should never be ridden near traffic. Their use should be prohibited on streets and highways. Activities that bring skateboards or in-line skates and cars together (e.g., “catching a ride”) are especially dangerous.
• Some types of use, such as riding homemade ramps on hard surfaces, may be particularly hazardous.
Modified from McGeehan J, Shields BJ, and Smith GA: Children should wear helmets while ice-skating: a comparison of skating-related injuries, Pediatrics 114(1):124-128, 2004.
Like skateboard injuries, roller skate or in-line skate injuries involve predominantly the upper extremities (especially the wrist and forearm) as children attempt to break a fall with outstretched arms. Safety measures are basically the same as for skateboards. Parents should carefully evaluate the skill level of the child before allowing the child to use skates. Younger children sustain injuries more frequently than older children. Some authorities believe that parents should not encourage children to engage in these activities until their bone strength and skills are sufficiently mature to decrease the risk of fracture.
Ride-on mower and other power mower injuries also occur among school-age children. Approximately 9400 children under the age of 18 years require emergency care for lawn mower–related injuries in the United States each year (Vollman and Smith, 2006). These injuries occur when children are allowed to operate a mower, when they are run over or backed over by another driver, or when they fall from a mower or from a trailer pulled by a mower. Although there are no age-specific criteria for the use of lawn mowers, children should not operate lawn mowers until they have appropriate levels of judgment, strength, coordination, and maturity, which is usually over the age of 12 years for walk-behind mowers and over the age of 16 years for riding mowers (Samson, 2006).
Similar injuries occur with snowmobiles. Most deaths and injuries involving snowmobiles occur when the vehicle collides with a stationary object or when riders fall or are ejected from the vehicle. The American Academy of Pediatrics recommends that persons under 16 years of age be prohibited from operating or riding snowmobiles (Nayci, Stavlo, Zarroug, et al, 2006).
Injuries at School
The risk of injury at school is relatively low, despite the amount of time children spend in that environment. Some injuries occur in gyms, shops, and laboratories, as well as on playgrounds and playing fields. Most injuries occur on the way to and from school. Many are related to sports activities. (See Chapter 39.) Persons concerned with child safety should be alert to hazards in the school environment and should become involved in efforts to make the environment safe in every aspect—physical facilities, equipment, training practices, and supervision.
Trampolines are popular with young children, and continue to cause significant injuries. In 2005 approximately 88,500 children suffered a trampoline related injury, with 66% of these patients ranging from 5 to 12 years old (Linakis, Mello, Machan, et al, 2007). Fractures, sprains, and head injuries have all been attributed to trampolines.
Farm Injuries
Many school-age children are involved in farm activities and play in the farm environment. They may be children of migrant workers, and as such, they constitute a significant proportion of agricultural workers. Most injuries take place during the summer when children are home from school and in the autumn when farming activity is brisk. Health facilities are also more scattered and less accessible for emergency treatment in farming areas than they are in urban communities.
Health workers need to be aware of the problems and to emphasize to the farm family the hazards related to their environment and ways to prevent injuries, especially when children are present. Rural schools should provide safety education regarding machinery operation, safety procedures, and injury prevention. Nurses in rural areas can be advocates for farm safety programs and for revision of the current farm safety legislation.
Other Injuries
Falls are still a source of injury in school-age children but less so than in preschool children and toddlers. “Flipping,” a popular activity in which children jump from an elevated surface and perform an aerial flip with the idea of landing upright, has resulted in serious injuries to the face and head and places children at risk for back and spinal cord injury. Seasonal injuries such as sledding accidents are common and more likely to occur when children ride sleds without adult supervision and in streets, as opposed to parks. Horseback riding injuries are another source of concern for parents of school-age children. The most common cause of death from horseback riding activities is head injury, followed by injuries to the chest and abdomen. Before enrolling children for riding lessons, parents should determine the instructor’s safety record with students, verify that safety helmets will be used, and confirm that the instructor is certified by a recognized organization. Injuries at public playgrounds and amusement parks (especially water slides) and around the home (power tools, ladders, fireworks) are ongoing concerns of parents and health care providers.
Injuries to eyes and teeth are a constant threat to school-age children involved in rough play. (See Chapter 24 [eyes] and Chapter 18 [teeth].) The normally shallow bony orbit of children in this age-group makes them particularly vulnerable to eye trauma, especially during contact sports or activities such as baseball or softball. Wearing protective eye and mouth gear is essential (Merriman, 2009).
Injuries have been reported from a variety of toys (slingshots, water balloons, lawn darts, chemistry sets) and household equipment (mowers, lawn trimmers). Gunshot wounds have become a significant problem during past years. The overall rate of firearm-related homicides for U.S. children younger than 15 years of age is nearly 12 times greater than that found in 25 other industrialized countries (Guralnick and Serwint, 2007). So-called toy firearms (air guns and air rifles) also cause frequent firearm injuries to children. Most of these injuries involve the face or eyes.
Nurse’s Role in Injury Prevention
Nurses are primary advocates for preventive care and guidance. Safety education and anticipatory guidance for both parents and school-age children can be incorporated in all nursing interventions. The most effective means of prevention is education of the child and family regarding the hazards of risk-taking behavior and improper use of equipment. No piece of equipment is safe unless a child is physically and mentally equipped to use it. A careful history and knowledge of normal growth and development serve as guidelines for both planned and impromptu education.
Parents are often unaware of hazards to their children at various ages, especially those related to normal developmental progress. Susceptibility to injuries and understanding of safety issues are influenced by children’s developmental level. Nurses who understand the growth and development of school-age children can provide effective safety education to parents and children and can correct misconceptions before injuries occur.
School nurses should be alert to hazards in the school and instrumental in evaluating safety risks and implementing safety programs. Characteristics of the school-age child and preventive measures are outlined in Table 17-2.
Anticipatory Guidance—Care of Families
The parents of the school-age child find themselves in the position of sharing their child’s time and interests with the increasingly important peer group. As a child feels the need to fit into a peer group and gain a sense of industry through individual and cooperative production and performance, he or she moves away from the close, familiar relationships of the family group. It is through these early peer relationships that children prepare for moving from narrow, sheltered family relationships to a broader world of relationships and increased independence. Parents must learn to provide support as unobtrusively as possible without feeling rejected, hurt, or angry. The nurse can help parents of the school-age child by providing anticipatory guidance and reassurance throughout this period of child development and maturation (see Family-Centered Care box).
FAMILY-CENTERED CARE
Guidance During School Years
Prepare parents to expect strong food preferences and frequent refusal of specific food items.
Prepare parents to expect increasingly ravenous appetite.
Prepare parents for emotional reactions as child experiences erratic mood changes.
Help parents anticipate continued susceptibility to illness.
Teach injury prevention and safety, especially bicycle safety.
Encourage parents to respect child’s need for privacy and to provide a separate bedroom for child, if possible.
Prepare parents for child’s increasing interests outside the home.
Help parents understand the need to encourage child’s interactions with peers.
Prepare parents to expect improvement in health with fewer illnesses, but warn them that allergies may increase or become apparent.
Prepare parents to expect an increase in minor injuries.
Emphasize caution in selecting and maintaining sports equipment and reemphasize safety.
Prepare parents to expect increased involvement with peers and interest in activities outside the home.
Emphasize the need to encourage independence while maintaining limit setting and discipline.
Prepare mothers to expect more demands at 8 years.
Prepare fathers to expect increasing admiration at 10 years; encourage father-child activities.
Help parents prepare child for body changes of pubescence.
Prepare parents to expect a growth spurt in girls.
Make certain child’s sex education is adequate with accurate information.
Prepare parents to expect energetic but stormy behavior at 11 years, with child becoming more even tempered at 12 years.
Encourage parents to support child’s desire to “grow up” but to allow regressive behavior when needed.
Prepare parents to expect an increase in masturbation.
Instruct parents that the child may need more rest.
Help parents educate child regarding experimentation with potentially harmful activities.
Help parents understand the importance of regular health and dental care for child.
Encourage parents to teach and model sound health practices, including diet, rest, activity, and exercise.
Stress the need to encourage children to engage in appropriate physical activities.
Emphasize providing a safe physical and emotional environment.
Key Points
• Middle childhood, also known as the school years, is a comfortable period of life that extends from 6 to 12 years of age.
• Although growth is slower than in previous years, there is a steady gain in height and weight with maturation of body systems; primary teeth are lost and replaced by permanent teeth.
• Skeletal lengthening, an increase in the ratio of muscle mass to fat, and maturation of the gastrointestinal system are major components of biologic development during middle childhood.
• Developing a sense of industry or accomplishment is a major task during the middle years (Erikson).
• Piaget’s theoretical stage of concrete operations refers to the school-age period, when children are able to use their thought processes to experience events and actions and make judgments based on what they reason.
• Through identity, reversibility, and reciprocity, children master the cognitive task of conservation.
• Children develop a conscience and are able to understand and adhere to rules and standards set by others.
• Spiritual development entails curiosity about deities, knowledge of the difference between the natural and the supernatural, and reliance on prayers or other religious rituals.
• Entertaining different points of view, becoming sensitive to social norms of peers, and forming peer friendships are the most important features of social development in the middle years.
• Children develop a self-concept from their own self-assessment and feedback from others.
• Increased socialization, earlier pubertal development, and constant media exposure make the school years an ideal time for sex education.
• Cooperative play, team activities, and acquisition of skills are prime elements of play during the school years; rules and rituals assume greater importance.
• Optimum nutrition is often hampered by an affinity for and availability of junk foods, irregular family meals, and schedules of working parents.
• Typical parental concerns during middle childhood include dishonest behavior, lying, cheating, stealing, and school-related stress.
• The school years are an ideal time for children to begin to take responsibility for their own health.
• School health centers ideally offer programs that include health appraisal, emergency care, safety education, communicable disease control, counseling, guidance, and health education, with adjustment to individual student needs.
• The major sources of accidental injury during middle childhood include a variety of conveyances, including motor vehicles, bicycles, skateboards, and in-line skates.
• Direct injury prevention toward safety education, provision of safe play areas and equipment, and good supervision of sports activities.
Answers to Critical Thinking Exercises
Temperament in the School-Age Child
1. Although many of Mary’s symptoms may be associated with her slow-to-warm-up temperament, it is difficult to rule out other health-related problems. Mary’s mother reports that she is in good health, but Mary could have an emotional or chronic illness that has not been identified. The nurse should encourage Mary’s mother to visit with her pediatrician if she has not done so already. The nurse should also instruct the teacher and parents about Mary’s temperament and offer suggestions to encourage Mary.
2. a. By the time a child reaches school-age years, his or her temperament has been defined. Most characteristics of a child’s temperament are innate; however, some characteristics can be modified by experiences and interactions with other people and with their environment, by their motives and abilities, and by the child’s health.
b A child’s behavioral adjustment can depend greatly on his or her temperament. Easy children adapt to new environments and people quickly; children who are slow to warm up may initially withdraw when encountering new situations; and difficult children usually adapt to new situations poorly, with explosive or stubborn behavior.
c Possible interventions include preparing the child for the specific activity in advance, allowing a friend to assist with the activity, offering praise and encouragement when the activity is completed, providing opportunities to do things the child is good at, and allowing the child extra time to get ready for the activity.
3. The first priority for the school nurse should be to discuss the situation with Mary’s mother to ensure that all potential causes of Mary’s behavior have been evaluated. If there is no evidence of other causes, Mary’s temperament characteristics should be discussed. The school nurse should educate Mary’s teachers and parents about her slow-to-warm-up temperament so that Mary’s needs can be accommodated to allow her to excel in all situations. The school nurse should evaluate what events are difficult for Mary and provide appropriate interventions for the teacher and parents to use when encountering these situations.
4. Yes. The information about Mary’s behavior provides a conclusion that Mary is either a slow-to-warm-up child or has an emotional or chronic illness. If emotional and chronic illnesses are ruled out, Mary’s behavior can be attributed to her temperament. Mary’s behavior fits into the slow-to-warm-up category and can be managed by assisting her in dealing with new situations.
Physical Growth in the School-Age Child
1. Yes. There is sufficient evidence to conclude that Janie is overweight. School-age children do not grow as quickly as they did in the preschool years; therefore caloric needs are diminished. Growth during school-age years is more even and steady with an average weight gain per year of 2.5 kg (5.5 lb). The 50th percentile for weight and height in an 8-year-old girl is 25.3 kg (55.8 lb) and 127 cm (50 inches), respectively.
2. a. Children’s eating patterns include increased restaurant food consumption, larger portion sizes, shifts in beverage consumption, and changes in meal patterns and meal frequency. Children are not eating the recommended servings of fruits, vegetables, and grains but are eating a diet high in fat, sweetened beverages, and salty foods.
b Risk factors include genetic factors such as high birth weight, maternal diabetes, and obesity in family members; environmental factors such as low economic status, lack of access to healthy food choices, and parental food choices; and societal factors such as increasingly sedentary leisure activities and decreased physical activity required in schools.
c Comorbidities include high blood pressure, insulin resistance and type 2 diabetes, hypercholesterolemia, dyslipidemia, and mental health issues such as depression and low self-esteem.
d Although parents exert a big influence on children’s attitudes and food choices, school-age children are starting to make decisions on their own. Parents do not know what or how much their children eat when they are away from home, such as during school lunch or at a friend’s house. Therefore educating the child about healthy food choices is essential so that the child can make appropriate food choices for his or her growing body.
3. Nursing care should include extensive education about nutrition and physical activity. This information should be shared with Janie and her family. Appropriate food consumption should include healthy eating patterns with nutritious snacks and suitable food portion sizes. Information about the importance and benefits of physical exercise should also be discussed, along with ideas for potential activities.
4. Yes. The data support the conclusion that Janie is overweight. Information about Janie’s food consumption and physical activity should be evaluated so that appropriate interventions can be identified.
Bicycle Helmets
1. Yes. There is a lack of bicycle helmet usage among children in your school district that is causing an increased risk for injury and deaths. Bicycling is one of the most popular recreational sports among children; however, it is also the leading cause of sports-related injuries when preventive gear is not used.
2. a. Hazards to children include serious brain injury, head injury, facial injury, broken bones, and abrasions.
b Intrinsic factors include children exceeding their ability level when riding or attempting to perform stunts; extrinsic factors include swerving to avoid a motor vehicle, striking a fixed object, and not wearing protective gear.
c The most influential factors associated with bicycle helmet use include helmet use by an accompanying parent and a state mandatory helmet law. Other factors include discomfort (especially heat), perceived lack of importance for casual riding, lack of style, and peer pressure.
d Pediatricians and nurses should serve as community and legislative advocates to encourage legislation requiring helmet use; encourage school districts to mandate helmet use when riding bicycles to and from school; assist in developing and implementing community- and school-based education programs to promote bicycle safety; urge retail stores to include helmets in the purchase of every new bicycle sold; and urge the media to consistently show helmets whenever bicycle riding is portrayed.
3. The major implication for nursing is the need to educate children and families on the importance of wearing helmets and other bicycle safety information.
4. Yes. Educating children and families about bicycle safety can reduce the number of bicycle-related injuries. Use of bicycle helmets can lessen the severity of brain injury and head trauma when used correctly. Other safety educational strategies add to the prevention of further injury.
References
American Academy of Pediatrics, Council on School Health. Medical emergencies occurring at school. Pediatrics. 2008;122(4):887–894.
American Academy of Pediatrics, Council on School Health. Role of the school nurse in providing school health services. Pediatrics. 2008;121(5):1052–1056.
American Academy of Pediatrics, Committee on Injury, Violence, and Poison Prevention and Council on School Health. School transportation safety. Pediatrics. 2007;120(1):213–220.
American Psychological Association. Undoing dyslexia via video games. available at www.psychologymatters.org/dyslexia.html, 2005. [(accessed February 26, 2009)].
Bagby, K, Adams, S. Evidence-based practice guideline: increasing physical activity in schools—kindergarten through 8th grade. J Sch Nurs. 2007;23(3):137–143.
Cawley, J, Meyerhoefer, C, Newhouse, D. The impact of state physical education requirements on youth physical activity and overweight. Health Economics. 2007;16:1287–1301.
Centers for Disease Control and Prevention. Motor vehicle safety. available at www.cdc.gov/MotorVehicleSafety/Child_Passenger_Safety/childseat-spot.html, 2009. [(accessed March 1, 2009)].
Centers for Disease Control and Prevention. Overweight and obesity. available at www.cdc.gov/nccdphp/dnpa/obesity/childhood/prevalence.htm, 2009. [(accessed February 22, 2009)].
Centers for Disease Control and Prevention. Healthy youth! Coordinated school health programs. available at www.cdc.gov/HealthyYouth/CSHP, 2008. [(accessed February 26, 2009)].
Christakis, D, Zimmerman, F. Children and television: a primer for pediatricians. Contemp Pediatr. 2007;24(3):31–42.
Durrant, J. Physical punishment, culture, and rights: current issues for professionals. J Dev Behav Pediatr. 2008;29(1):55–66.
Eisenberg, M, Bernat, D, Bearinger, L, et al. Support for comprehensive sexuality education: perspectives from parents of school-age youth. J Adolesc Health. 2008;42:352–359.
Eisenbraun, K. Violence in schools: prevalence, prediction, and prevention. Aggression Violent Behav. 2007;12:459–469.
Erikson, EH. Childhood and society, ed 2. New York: Norton; 1963.
Fowler, P, Tompsett, C, Braciszewski, J, et al. Community violence: a meta-analysis on the effect of exposure and mental health outcomes of children and adolescents. Dev Psychopathol. 2009;21:227–259.
Fredland, N. Nurturing hostile environments: the problem of school violence. Fam Commun Health. 2008;31(Suppl 1):S32–S41.
Gini, G. Association between bullying behaviour, psychosomatic complaints, emotional and behavioural problems. J Paediatr Child Health. 2007;44(9):492–497.
Guralnick, S, Serwint, J. Firearms. Pediatr Rev. 2007;28(10):396–397.
Holt, S, Buckley, H, Whelan, S. The impact of exposure to domestic violence on children and young people: a review of the literature. Child Abuse Negl. 2008;32(8):797–810.
Jenson, J, Dieterich, W. Effects of a skills-based prevention program on bullying and bully victimization among elementary school children. Prev Sci. 2007;8(4):285–296.
Killingsworth, J, Tilford, J, Parker, J, et al. National hospitalization impact of pediatric all-terrain vehicle injuries. Pediatrics. 2005;115(3):e316–e321.
Li, H, Prevatt, F. Fears and related anxieties across three age groups of Mexican American and white children with disabilities. J Genetic Psychol. 2007;168(4):381–400.
Linakis, J, Mello, M, Machan, J, et al. Emergency department visits for pediatric trampoline-related injuries: an update. Acad Emerg Med. 2007;14:539–544.
McColgan, MD, Giardino, AP. Internet poses multiple risks to children and adolescents. Pediatr Ann. 2005;34(5):405–414.
Merriman, J. Wearing protective sports gear. Contemp Pediatr. 2009;26(2):34.
Murphy, N, Young, P. Sexuality in children and adolescents with disabilities. Dev Med Child Neurol. 2005;47:640–644.
Murrell, A, Christoff, K, Henning, K. Characteristics of domestic violence offenders: associations with childhood exposure to violence. J Fam Violence. 2007;22:523–532.
National Highway Traffic Safety Administration. Traffic safety facts, bicyclists and other cyclists. available at www.nrd.nhtsa.dot.gov/Pubs/811156.PDF, 2008. [(accessed February 1, 2010)].
National Highway Traffic Safety Administration. Traffic safety facts, children. available at www.nhtsa.gov, 2007. [(accessed March 1, 2009)].
Nayci, A, Stavlo, P, Zarroug, A, et al. Snowmobile injuries in children and adolescents. Mayo Clin Proc. 2006;81(1):39–44.
Newgard, CD, Lewis, RJ. Effects of child age and body size on serious injury from passenger air-bag presence in motor vehicle crashes. Pediatrics. 2005;115(6):1579–1585.
Okun, A, Adam, H. Safety on bicycles, skateboards, scooters, and skates. Pediatr Rev. 2008;29(10):366–367.
Podberscek, AL. Positive and negative aspects of our relationship with companion animals. Vet Res Commun. 2006;30(S1):21–27.
Rideout, V, Roberts, D, Foehr, U. Generation M: media in the lives of 8-18 year olds. Kaiser Family Foundation, available at www.kff.org/entmedia/7251.cfm, 2005. [(accessed February 26, 2009)].
Samson, Z. Lawn-mowing fraught with danger. Am Acad Pediatr News. 2006;27(8):29–30.
Schredl, M, Biemelt, J, Roos, K, et al. Nightmares and stress in children. Sleep Hypnosis. 2008;10(1):19–25.
Smaldone, A, Honig, J, Byrne, M. Sleepless in America: inadequate sleep and relationships to health and well-being of our nation’s children. Pediatrics. 2007;119(S1):S29–S37.
Spruyt, K, O’Brien, L, Cluydts, R, et al. Odds, prevalence and predictors of sleep problems in school-age normal children. J Sleep Res. 2005;14:163–176.
Towe-Goodman, N, Teti, D. Power assertive discipline, maternal emotional involvement, and child adjustment. J Fam Psychol. 2008;22(3):648–651.
US Department of Agriculture. MyPlate. www.choosemyplate.gov, 2011. [available at (accessed September 8, 2011)].
Van Der Molen, JH, Bushman, BJ. Children’s direct fright and worry reactions to violence in fiction and news television programs. J Pediatr. 2008;153:420–424.
Vollman, D, Smith, GA. Epidemiology of lawn mower–related injuries to children in the United States. Pediatrics. 2006;118(2):e273–e278.
Vreeman, RC, Carroll, AE. A systematic review of school-based interventions to prevent bullying. Arch Pediatr Adolesc Med. 2007;161:78–88.
Wagner, R, Oskouian, R. The ECG epidemic. Contemp Pediatr. 2008;25(9):60–79.
Weems, CF, Costa, NM. Developmental differences in the expression of childhood anxiety symptoms and fears. J Am Acad Child Adolesc Psychiatry. 2005;44(7):656–663.
Wells, HF, Buzby, JC. Dietary assessment of major trends in U.S. food consumption. US Department of Agriculture, available at www.ers.usda.gov, 2008. [(accessed March 8, 2009)].
Williams, KR, Guerra, NG. Prevalence and predictors of Internet bullying. J Adolesc Health. 2007;41(6):S14–S21.
*For information on bullying and how to prevent it in the school setting, contact Educators for Social Responsibility, 23 Garden St., Cambridge, MA 02138; 617-492-1764 or 800-370-2515; www.esrnational.org.
*U.S. Department of Agriculture, Food and Nutrition Service, 3101 Park Center Drive, Alexandria, VA 22302; 703-305-1624; www.fns.usda.gov/tn.
*8484 Georgia Ave., Suite 420, Silver Springs, MD 20910; 866-627-6767; e-mail: nasn@nasn.org; www.nasn.org.
*Guidelines for car seat safety are also available in Wilson D and Hockenberry MJ: Wong’s clinical manual of pediatric nursing, ed 7, St Louis, 2008, Mosby.