The reproductive system
The breast examination
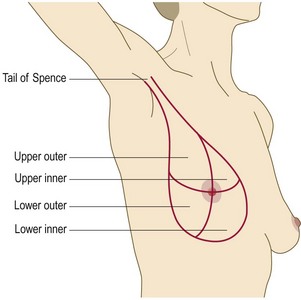
The breasts are modified sweat glands. Pigmented skin covers the areola and the nipple, which is erectile tissue. The openings of the lactiferous ducts are on the apex of the nipple. The nipple is in the fourth intercostal space in the mid-clavicular line, but accessory breast/nipple tissue may develop anywhere down the nipple line (axilla to groin) (Figs 10.2 and 10.3). The adult breast is divided into the nipple, the areola and four quadrants, upper and lower, inner and outer, with an axillary tail projecting from the upper outer quadrant (Fig. 10.4).

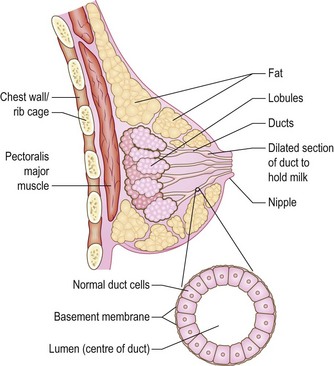
The size and shape of the breasts are influenced by age, hereditary factors, sexual maturity, phase of the menstrual cycle, parity, pregnancy, lactation and general state of nutrition. Fat and stroma surrounding the glandular tissue determine the size of the breast, except during lactation, when enlargement is mostly glandular. The breast responds to fluctuations in oestrogen and progesterone levels. Swelling and tenderness are more common in the premenstrual phase. The amount of glandular tissue reduces and fat increases with age, so that the breasts are softer and more pendulous. Lactating breasts are swollen and engorged with milk, and are best examined after breastfeeding.
Symptoms and definitions
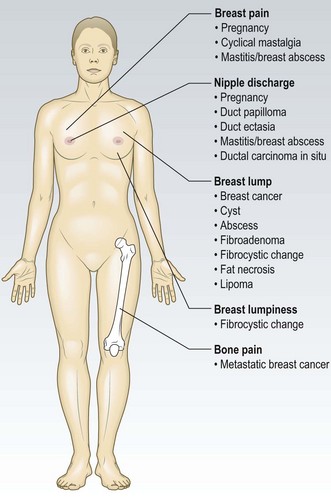
Breast cancer: Cancers are solid masses with an irregular outline. They are usually, but not always, painless, firm and hard, contrasting in consistency with the surrounding breast tissue. The cancer may extend directly into the overlying tissues such as skin, pectoral fascia and pectoral muscle, or metastasise to regional lymph nodes or the systemic circulation. In the UK, this cancer affects 1 in 9 women. The incidence increases with age, but manage any mass as potentially malignant until proven otherwise. Cancer of the male breast is uncommon and can have a strong genetic factor.
Fibrocystic changes: Fibrocystic changes are rubbery, bilateral and benign, and most prominent premenstrually, but investigate any new focal change in young women which persists after menstruation. These changes and irregular nodularity of the breast are common, especially in the upper outer quadrant in young women.
Fibroadenomas: These smooth, mobile, discrete and rubbery lumps are the second most common cause of a breast mass in women under 35 years old. These are benign overgrowths of parts of the terminal duct lobules.
Breast cysts: These are smooth fluid-filled sacs, most common in women aged 35–55 years. They are soft and fluctuant when the sac pressure is low but hard and painful if the pressure is high. Cysts may occur in multiple clusters. Most are benign, but investigate any cyst with blood-stained aspirate or a residual mass following aspiration, or which recurs after aspiration.
Breast abscesses: There are two types:
• lactational abscesses in women who are breastfeeding, usually peripheral
• non-lactational abscesses, which occur as an extension of periductal mastitis and are usually found under the areola, often associated with nipple inversion. They usually occur in young female smokers. Occasionally, a non-lactating abscess may discharge spontaneously through a fistula, classically at the areolocutaneous border (Fig. 10.5).

Breast pain
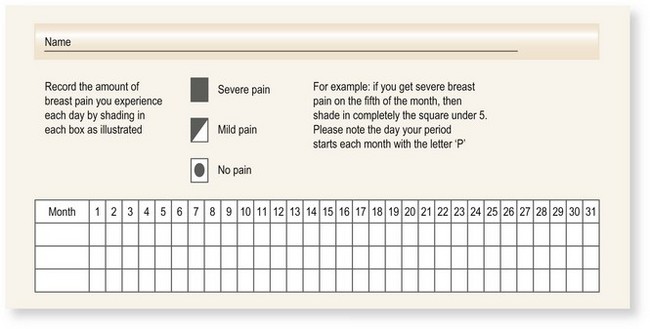
Most women suffer cyclical mastalgia at some stage (Box 10.1). Chest wall pain may be confused with breast pain.
Skin changes
Simple skin dimpling: The skin remains mobile over the cancer (Fig. 10.6).

Lymphoedema of the breast: The skin is swollen between the hair follicles and looks like orange peel (peau d’orange; Fig. 10.7). The most common causes are infection or tumour and it may be accompanied by redness, warmth and tenderness. Investigate any ‘infection’ which does not respond to one course of antibiotics to exclude an inflammatory cancer. These are aggressive tumours with a poor prognosis.

Eczema of the nipple and areola: This may be part of a generalised skin disorder. If it affects the true nipple, it may be due to Paget’s disease of the nipple (Fig. 10.8), or invasion of the epidermis by an intraductal cancer.

Nipple changes
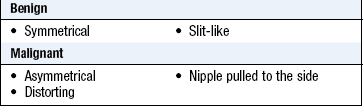
Nipple inversion: Retraction of the nipple is common and is often benign; however it can be the first subtle sign of malignancy when it is usually asymmetrical (Fig. 10.9 and Box 10.2).

Nipple discharge: A small amount of fluid may be expressed from multiple ducts by massaging the breast. It may be clear, yellow, white or green in colour. Investigate persistent single duct discharge or blood-stained (macroscopic or microscopic) discharge to exclude duct ectasia, periductal mastitis, intraduct papilloma or intraduct cancer.
Gynaecomastia
Gynaecomastia is enlargement of the male breast and often occurs in pubertal boys. In chronic liver disease gynaecomastia is caused by high levels of circulating oestrogens which are not metabolised by the liver. Many drugs can cause breast enlargement (Box 10.3 and Fig. 10.10).
 10.3
10.3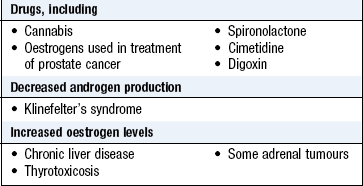

The history
Benign and malignant conditions cause similar symptoms but benign changes are more common. Not all patients have symptoms. Women may have an abnormality on screening mammography; asymptomatic women may present with concerns about their family history. Breast cancer may present with symptoms of metastatic disease. Men may present with gynaecomastia. Explore the patient’s ICE (p. 8). Women are often worried that they have breast cancer.
Presenting complaint
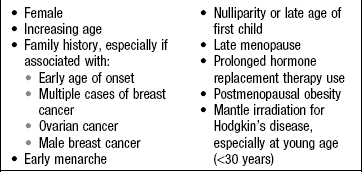
Evaluate potential risk factors (Box 10.4) and menopausal status. Use a pain chart to establish the timing of symptoms (Fig. 10.11).
The physical examination
Offer a chaperone and record that person’s name; if the patient declines, note this. Male doctors should always have a chaperone. Ask the patient to undress to the waist and sit upright on a well-illuminated chair or on the side of a bed.
Examination sequence
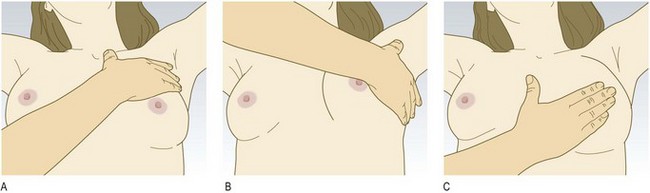
 Ask her to rest her hands on her thighs to relax the pectoral muscles (Fig. 10.12A).
Ask her to rest her hands on her thighs to relax the pectoral muscles (Fig. 10.12A).
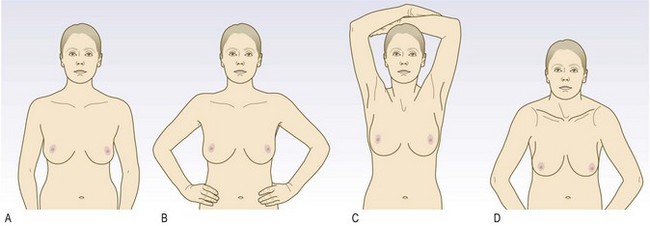
Fig. 10.12 Positions for inspecting the breasts.
(A) Hands resting on thighs. (B) Hands pressed on to hips. (C) Arms above head. (D) Leaning forward with breasts pendulous.
Face the patient and look at the breasts for:
Ask the patient to press her hands firmly on her hips to contract the pectoral muscles and inspect again (Fig. 10.12B).
Ask her to raise her arms above her head and then lean forward to expose the whole breast and exacerbate skin dimpling (Fig. 10.12C and D).
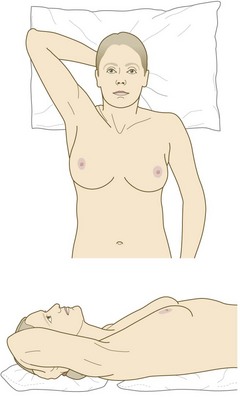
Ask her to lie with her head on one pillow and her hand under her head on the side to be examined (Fig. 10.13).
Hold your hand flat to her skin and palpate the breast tissue, using the palmar surface of your middle three fingers. Compress the breast tissue firmly against her chest wall.
View the breast as a clock face. Examine each ‘hour of the clock’ from the outside towards the nipple, including under the nipple (Fig. 10.14). Compare the texture of one breast with the other. Examine all the breast tissue. The breast extends from the clavicle to the upper abdomen and from the midline to the anterior border of latissimus dorsi (posterior axillary fold). Define the characteristics of any mass (Box 3.11).
Elevate the breast with your hand to uncover dimpling overlying a tumour which may not be obvious on inspection.
Is the mass fixed underneath? With the patient’s hands on her hips, hold the mass between your thumb and forefinger. Ask her to contract and relax the pectoral muscles alternately by pushing into her hips. As the pectoral muscle contracts, note whether the mass moves with it and if it is separate when the muscle is relaxed. Infiltration suggests malignancy.
Examine the axillary tail between your finger and thumb as it extends towards the axilla.
Palpate the nipple by holding it gently between your index finger and thumb. Try to express any discharge. Massage the breast towards the nipple to uncover any discharge. Note the colour and consistency of any discharge, along with the number and position of the affected ducts. Test any nipple discharge for blood using urine-testing sticks.
Palpate the regional lymph nodes, including the supraclavicular group. Ask the patient to sit facing you, and support the full weight of her arm at the wrist with your opposite hand. Move the flat of your other hand high into the axilla and upwards over the chest to the apex. This can be uncomfortable for patients, so warn them beforehand and check for any discomfort. Compress the contents of the axilla against the chest wall. Assess any palpable masses for:
Examine the supraclavicular fossa, looking for any visual abnormality. Palpate the neck from behind and systematically review all cervical lymphatic chains (p. 54).
Investigations
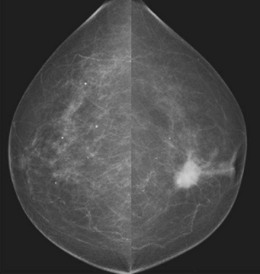
Accurate diagnosis of breast lesions depends on clinical assessment, backed up by mammography and/or breast ultrasound and pathological diagnosis, either by fine-needle aspiration cytology or core biopsy (‘triple assessment’) (Box 10.5 and Figs 10.15 and 10.16). Up to 5% of malignant lesions require excision biopsy for the diagnosis to be made. Magnetic resonance imaging is useful to investigate possible implant rupture, extent of cancer in a mammographically dense breast and as a screening tool in those with genetic markers – BRCA1 or 2. In the UK there are specific guidelines for the appropriate referral of patients with breast symptoms to specialist units where this assessment is carried out.
 10.5 Investigation of breast lumps
10.5 Investigation of breast lumps
| Investigation | Indication/comment |
| Ultrasound | Lump |
| Mammography | Not in women under 35 unless there is a strong suspicion of cancer |
| Magnetic resonance imaging | Dense breasts/ruptured implant |
| Fine-needle aspiration | Aspirate lesion using a 21 or 23 G needle |
| Core biopsy | To differentiate invasive or in situ cancer |
| Large-core vacuum-assisted core biopsy | |
| Open surgical biopsy |

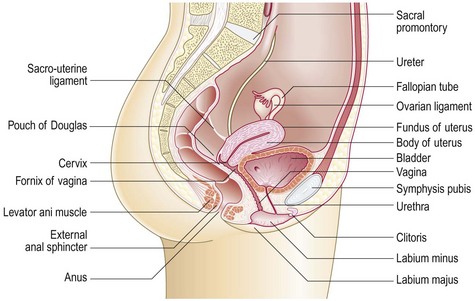
The gynaecological examination
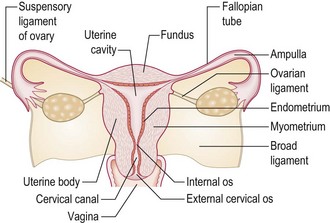
The uterus
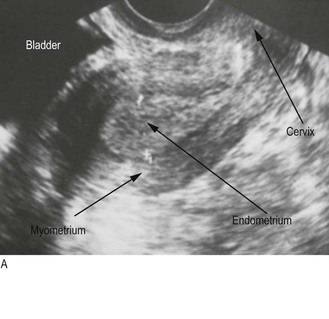
Pear-shaped, about 6–8 cm long, 4–6 cm wide and stabilised by the broad ligament, the uterus lies between the bladder and rectum and consists of muscular myometrium surrounding a cavity lined by endometrium (Figs 10.17 and 10.18). Ovarian hormones stimulate the endometrium to proliferate; secretion and breakdown (menstruation) follow.
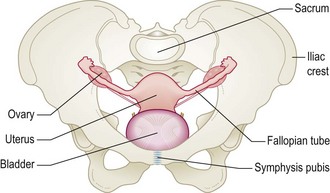
The Fallopian tubes
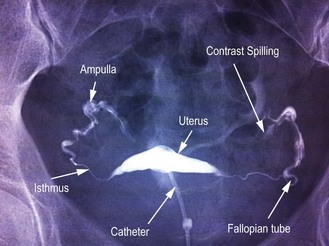
Approximately 10 cm long, the Fallopian tubes run from the lateral border of the uterine fundus to the ovary. The distal ampulla is mobile and ends with finger-like fimbria (Fig. 10.19).
The ovaries
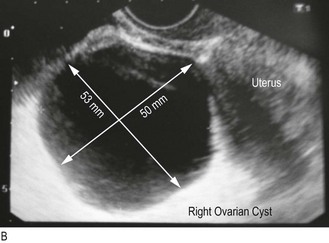
Oval, sitting behind and above the uterus close to the pelvic side-wall, and 1–2 × 2–3 cm, the ovaries increase in size during the follicular phase of the menstrual cycle when a dominant follicle develops.
The cervix
Connecting the uterine body to the upper vagina, this fibrous tube 2 × 3 cm has the external cervical os visible on its surface. Inside the cervix, where the single-layer epithelium changes to multilayered epithelium, is the transition zone where malignant transformation occurs (Fig. 10.20).
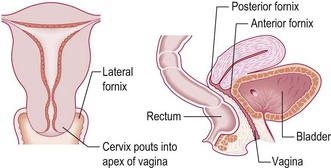
The vagina
The vagina is a rugged tube 10–15 cm in length with the cervix invaginating the top, forming lateral fornices on either side and anterior and posterior fornices. Two centimetres into the vagina is a ring of tissue, the remnant hymen (Fig. 10.20).
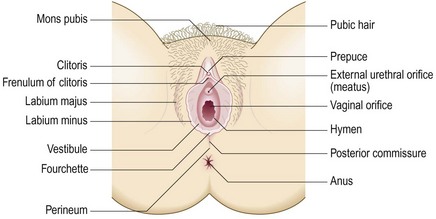
The external female genitalia
The vulva consists of labia majora – fat pads covered with hair. The labia minora are hairless skin flaps at each side of the vulval vestibule, which contains the urethral opening and the vaginal orifice. The fourchette, the posterior part of the clitoris, is anterior and usually obscured by a prepuce or hood. The perineum is the fibrous tissue; muscle and skin separate the vestibule from the anus (Fig. 10.21).
Symptoms and definitions
The first day of one period (menstrual bleeding) to the first day of the next lasts 22–35 days (average 28 days) with bleeding for 3–6 days. Record bleeding for 4–5 days during a cycle of 25–29 days as 4–5/25–29.
Abnormal uterine bleeding
Heavy menstrual bleeding affects 20% of premenopausal women over 35 (Box 10.6). Average blood loss is 35 ml but is subjective. Ask how many sanitary pads and tampons the patient uses and how often she changes them overnight. Flooding, where menstrual blood soaks through protection, passing blood clots or anaemia implies heavy bleeding.
 10.6
10.6
Postmenopausal bleeding
Postmenopausal bleeding occurs in 1.5% of women. It must be investigated, since 10% have endometrial cancer.
SIGN guidelines 61. Investigation of postmenopausal bleeding. Available online at: http://www.sign.ac.uk/guidelines/fulltext/61/section2.html.
Intermenstrual bleeding and postcoital bleeding suggest cervical pathology.
Amenorrhoea is absent periods. Primary amenorrhoea is when a girl has not started her periods by 16 years old and secondary amenorrhoea is no periods for 3 months or more in a woman who has previously menstruated. The commonest cause of secondary amenorrhoea is pregnancy. Otherwise, secondary amenorrhoea is due to hypothalamic–pituitary–ovarian axis dysfunction and affects 5–7% of woman in their reproductive years (Box 10.7).
 10.7 Gynaecological symptoms and definitions
10.7 Gynaecological symptoms and definitions
| Menarche | Age at first period (average in UK 12 years) |
| Menopause | Age at last menstrual period. Only determined retrospectively after 1 year with no periods |
| Perimenopause (climacteric) | The time before the menopause (2–5 years) when periods become irregular and flushes and sweats occur |
| Heavy menstrual bleeding | Excess blood loss (80 ml+) during a period, previously called menorrhagia |
| Intermenstrual bleeding | Bleeding between periods, suggesting hormonal, endometrial or cervical pathology |
| Postcoital bleeding | Bleeding after intercourse, suggesting cervical pathology |
| Postmenopausal bleeding | Bleeding more than 1 year after menopause |
| Primary amenorrhoea | No periods by age 16 |
| Secondary amenorrhoea | No periods for 3 months in a woman who has previously menstruated |
| Oligomenorrhoea | Periods with a cycle more than 35 days |
Urinary incontinence
Inappropriate and involuntary voiding of urine severely affects 10% of women, and its prevalence increases with age. Stress incontinence occurs on exertion, coughing, laughing or sneezing and is associated with pelvic floor weakness. Urge incontinence, an overwhelming desire to urinate when the bladder is not full, is due to detrusor muscle dysfunction.
Prolapse
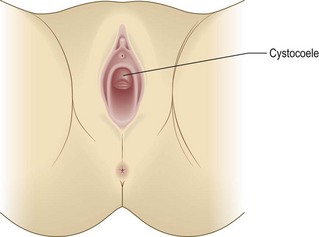
The pelvic contents may bulge into (Fig. 10.22) or beyond (Fig. 10.23) the vagina in 30% of women. Women feel something ‘coming down’, particularly when standing or straining. It is associated with previous childbirth (Box 10.8).
10.8 Definitions related to prolapse
| Cystocoele | Bulge of the anterior vaginal wall containing the bladder |
| Rectocoele | Bulge of the posterior vaginal wall containing the rectum |
| Enterocoele | Bulge of the distal wall posteriorly containing small bowel and peritoneum |
| Urethrocoele | Prolapse of the urethra into the vagina, often occurring with a cystocoele |
| Uterine prolapse | Grade 1 is descent halfway to the hymen, grade 2 is to the hymen and grade 3 is past the hymen within the vagina |
| Procidentia | External prolapse of the uterus (grade 4) |
| Vault prolapse | Bulge of the roof of the vagina after hysterectomy |

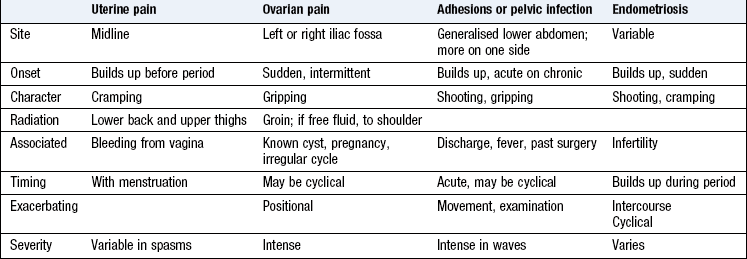
Pain
Pain in either iliac fossa may be due to ovarian cysts, cyst conditions, e.g. haemorrhage, rupture or torsion, or diseased Fallopian tubes. Infection, pelvic adhesions and endometriosis can cause generalised pain (Boxes 10.9 and 10.10).
10.9 Pelvic pain definitions
| Primary dysmenorrhea | Ongoing pain during a period that is most intense just before and during a period, caused by uterine contraction |
| Secondary or progressive dysmenorrhea | Worsening pain that deteriorates during a period, suggesting pathology such as endometriosis or chronic infection |
| Ovarian torsion | Twisting of an ovarian cyst on its vascular pedicle, causing acute ischaemia |
| Dyspareunia | Pain with intercourse, suggesting endometriosis or pelvic adhesions |
| Vaginismus | Pain on penetration secondary to involuntary contraction of the pelvic floor |
| Mittelschmertz | Pain associated with follicle rupture during ovulation |
Vaginal discharge
This may be normal and variable during the menstrual cycle. Prior to ovulation it is clear, abundant and stretches like egg white; after ovulation it is thicker, does not stretch and is less abundant. Abnormal vaginal discharge occurs with infection. The most common non-sexually transmitted infection (caused by Candida species) gives a thick, white, curdy discharge often associated with marked vulval itching. Bacterial vaginosis is a common, non-sexually acquired infection, usually caused by Gardnerella vaginalis, producing a watery, fishy-smelling discharge. The pH of normal vaginal secretions is usually <4.5 but in bacterial vaginosis it is >5. Sexually transmitted infections (STIs) can cause discharge, vulval ulceration or pain, dysuria, lower abdominal pain and general malaise. They may also be asymptomatic.
Pelvic masses
These can cause abdominal distension and pressure effects or be asymptomatic. The most common is a pregnant uterus. Uterine leiomyoma (fibroids) or ovarian cysts are other causes.
Dyspareunia
This is pain during intercourse, which may be felt around the entrance to the vagina (superficial) or within the pelvis. Pain due to involuntary spasm of muscles at the vaginal entrance (vaginismus) may make intercourse impossible. Persistent deep dyspareunia suggests underlying pelvic pathology. Dyspareunia can occur due to vaginal dryness following the menopause.
The history
Ensure you understand what the woman’s main problems are, how these developed, how they affect her from day to day and how she copes. She may have no specific problems and have come for a routine cervical smear. Find out her ICE (p. 8) and any previous investigations and management.
Clarify the presenting complaint and take a general gynaecological history. Always consider that she may be pregnant and ask about her last menstrual period (LMP) and whether this was normal. Ask about past and present contraceptive use as well as plans for fertility and any weight changes (Box 10.11).
 10.11 Menstrual history checklist
10.11 Menstrual history checklist
| Ask about: | Information to obtain | Comment |
| Menarche | Age at which periods began | Not essential in older women with children |
| Last menstrual period | Date of the first day of the last period | If the period is late, exclude pregnancy. If the patient is menopausal, record the age at which periods stopped |
| Length of period | Number of days the period lasts | Normal 4–7 days |
| Amount of bleeding | How heavy the bleeding is each month (light, normal or heavy). Any episodes of flooding or passed clots? | If heavy, how many sanitary pads and tampons are used? Does the patient get up at night to change her sanitary protection? How many times? |
| Regularity of periods | Number of days between each period. Is the pattern regular or irregular? | Normal 22–35 days. Around the menopause, cycles lengthen until they stop altogether |
| Erratic bleeding | Bleeding between periods or after intercourse | May indicate serious underlying disease |
| Pain | Association with menstruation. Does the pain precede or occur during the period? | Common in early adolescence; usually no underlying pathology. Painful periods starting in older women may be associated with underlying disease |
| Pregnancies | Record any births, miscarriages or abortions | Some women may not disclose an abortion or baby given up for adoption |
| Infertility | Is the patient trying to become pregnant? | How long has she been trying to conceive? |
| Contraception | Record current and previous methods. Note that the patient’s partner may have had a vasectomy or she may be in a same-sex relationship | Hormonal and intrauterine contraception can affect menstrual bleeding patterns |
| Lifestyle | Ask about weight, dieting and exercise | Rapid or extreme weight loss and excessive exercise often cause oligoamenorrhoea. Obesity causes hormonal abnormalities, menstrual changes and infertility. Acne and hirsutism may be signs of an underlying hormonal disorder |
People often find it difficult talking about sexual matters. It is important that you are at ease and ask questions in a straightforward and non-judgemental manner (p. 9). Do not perform a pelvic examination in someone who has not been sexually active (Box 10.12).
10.12 Taking a sexual history
• Are you currently in a relationship?
• How long have you been with your partner?
• Is it a sexual relationship?
• Have you had any (other) sexual partners in the last 12 months?
• How many were male? How many female?
• When did you last have sex with:
• Do you use barrier contraception – sometimes, always or never?
Past history
Ask about the patient’s cervical smears, when taken and the results, along with any treatment required for abnormalities. Note any abdominal surgery, pelvic infection or previous sexually transmitted disease. Document each pregnancy, its outcome and any interventions.
Drug history
Ask about contraception. Document current or previous use of hormone replacement therapy or hormonal preparations, e.g. tamoxifen. Antibiotic use can be associated with vaginal candidiasis and some antipsychotic drugs can cause hyperprolactinaemia. Other prescribed medications may reduce the effectiveness of the contraceptive pill, e.g. women on some antiepileptic drugs require a high-dose combined oral contraceptive (Box 10.13).
10.13 Methods of contraception
• Combined oral contraceptive pill (or combined transdermal patch)
• Progestogen-only pill (‘mini pill’)
• Depot progestogen injection (Depo-Provera)
• Progestogen implant (Implanon)
• Copper intrauterine device (IUD or coil)
• Progestogen-releasing intrauterine system (IUS or Mirena)
• Female barrier method: diaphragm, cervical cap or female condom
• Natural methods: rhythm method, Persona, lactational amenorrhoea
Family history
Ovarian cancer can be familial and a family history of diabetes is associated with some reproductive abnormalities, such as polycystic ovarian syndrome (PCOS). Hereditary bleeding disorders can present with heavy menstrual bleeding.
Social history
Smoking, occupation and lifestyle affect many gynaecological conditions, e.g. obesity and PCOS reduce fertility.
Sexual history
The patient may find these questions embarrassing so put her at ease and be comfortable yourself about these issues. Explain why you need to ask these questions and be non-judgemental. Ask clear unambiguous questions (Box 10.12).
The sexual partners of women with STIs should be informed and treated to prevent further transmission of the infection or reinfection of the treated person. Confidentiality is paramount, so do not give information to a third party.
The physical examination
Assess the woman’s demeanour and for signs of anaemia or evidence of weight change. In amenorrhoeic patients note any hirsuitism, acanthosis nigricans (Fig. 5.13A) or galactorrhoea. Measure blood pressure and body mass index.
Offer a female chaperone, record her name and whether the patient declines. The examination area should be private, with the equipment to hand and an adjustable light source. The woman should have an empty bladder and remove her clothing from the waist down along with any sanitary protection. Leave her in privacy to do this.
Abdominal examination
Note any masses arising from the pelvis, tenderness, ascites or inguinal lymph nodes (p. 53).
Pelvic examination
Explain what you are going to do, why it is necessary (Box 10.14) and obtain verbal consent. Use a vaginal speculum to see the cervix and the vaginal walls, to carry out a cervical smear and to take swabs. Specula are metal or plastic and come in various sizes and lengths. Metal specula may be sterilised and reused. Plastic specula are always disposable. A metal speculum is cold, so warm it under the hot tap. Most women find a speculum examination mildly uncomfortable, so put a small amount of lubricating gel on the tip of each blade, even if you are carrying out a cervical smear.
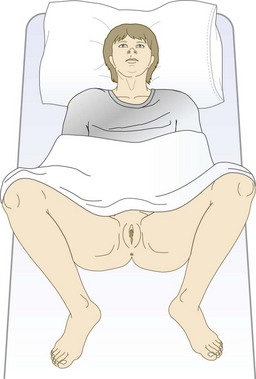
Ask the patient to lie on her back on the couch, covered with a modesty sheet to the waist, with her knees bent and knees apart (Fig. 10.24).
Wash your hands and put on medical gloves.
Examination sequence
Look at the perineum for any deficiency associated with childbirth; note abnormal hair distribution and cliteromegaly (associated with hyperandrogenism) (Fig. 5.22). Note any skin abnormalities, discharge or swellings of the vulva, such as the Bartholin’s glands on each side of the fourchette (Fig. 10.25).

Ask the woman to cough and look for any prolapse or incontinence.
Gently part the labia using your left hand (Fig. 10.26). With your right hand gently insert a lightly lubricated bivalve speculum (Figs 10.27 and 10.28A), with the blades vertical, fully into the vagina, rotating the speculum 90o so that the handles point anteriorly and the blades are now horizontal (Fig. 10.28B). A woman who has been pregnant will need a larger or longer speculum if the cervix is very posterior. If the woman finds the examination difficult, ask her to try and insert the speculum herself.
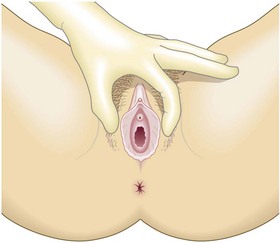
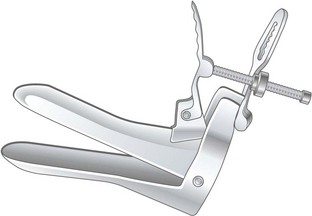
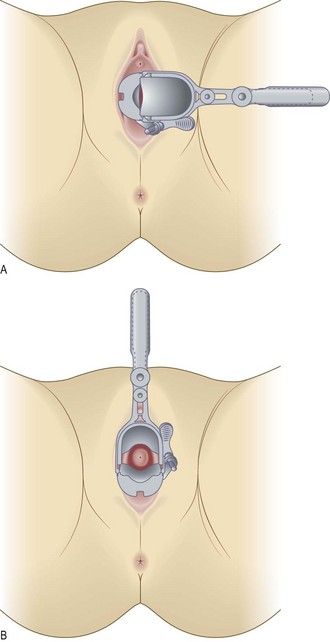
Fig. 10.28 Bivalve speculum examination.
(A) Insertion of speculum. (B) Visualisation of cervix after rotation through 90°.
Slowly open the blades and see the cervix between them. If you cannot see it, reinsert the speculum at a more downward angle as the cervix may be behind the posterior blade. Note any discharge or vaginal or cervical abnormalities.
Ask the woman to lie on her left side and bring her knees up to her chest.
Place a small amount of lubricating jelly on the blade of the speculum.
Insert the blade to hold back the posterior wall.
Ask the women to cough and look for uterine descent and the bulge of a cystocoele (Fig. 10.29).

Repeat, using the speculum to hold back the anterior vaginal wall to see a rectocoele or enterocoele.
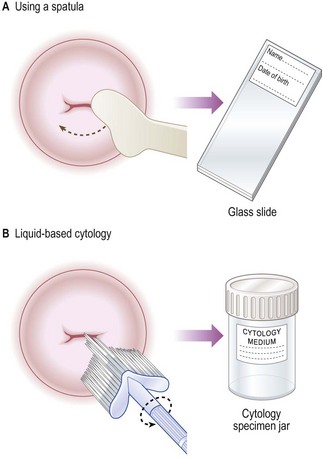
Taking a cervical smear: There are two ways of taking a smear:
Liquid-based cytology allows smears to be processed more efficiently and gives a smaller percentage of inadequate smears. Always label the microscope slide (in pencil) or the vial of cytological medium with the woman’s details before examining her so you do not mix up specimens (Fig. 10.30).
Examination sequence
Label the cytological medium or slide and fill in the request form before starting the examination.
Clearly visualise the entire cervix.
For a conventional smear, insert the longer blade of the spatula into the cervical os.
Rotate the spatula through 360°.
Spread once across the glass slide.
Place the slide immediately into fixative (methylated spirits) for 3–4 minutes.
Remove it and leave it to dry in air.
Insert the centre of the plastic broom into the cervical os.
Rotate the broom five times through 360° (Fig. 10.30).
Push the brush 10 times against the bottom of the specimen container.
Apply lubricating gel to your right index and middle finger.
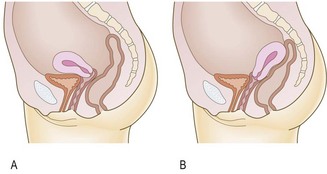
Gently insert them into the vagina and feel for the firm cervix. The uterus is usually anteverted (Fig. 10.31A) and you feel its firmness anterior to the cervix. If the uterus is retroverted (15%) and lying over the bowel, feel the firmness posterior to the cervix (Fig. 10.31B).
Push your fingers into the posterior fornix and lift the uterus while pushing on the abdomen with your left hand.
Place your left hand above the umbilicus and bring it down, palpating the uterus between both hands and note its size, regularity and any discomfort (Fig. 10.32).
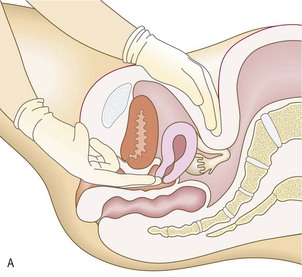
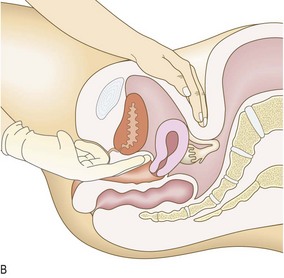
Fig. 10.32 Bimanual examination of the uterus.
(A) Use your vaginal fingers to push the cervix back and upwards, and feel the fundus with your abdominal hand. (B) Then move your vaginal fingers into the anterior fornix and palpate the anterior surface of the uterus, holding it in position with your abdominal hand.
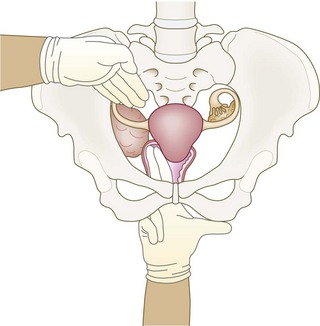
Move your fingers to the lateral fornix and, with your left hand above and lateral to the umbilicus, bring it down to assess any adnexal masses between your hands on each side (Fig. 10.33).
If stress incontinence occurs when the patient coughs, try lifting the anterior vaginal wall with your fingers and asking her to cough again. This stops genuine stress incontinence.
Normal findings: The cervix os may be a slit after childbirth. Vaginal squamous epithelium and the endocervical columnar epithelium meet on the cervix. The position of this squamocolumnar junction varies throughout reproductive life and so the cervix can look very different in individual women. The transition zone may be seen on the cervix. This is called an ectropion and looks red and friable; there may be small cysts called nabothian follicles.
The uterus should feel regular and be mobile and the size of a plum. The Fallopian tubes cannot be felt and normal ovaries are only palpated in very slim women.
Abnormal findings: Vulval changes include specific skin disease and infections such as herpes, thrush or malignancy. Visual abnormalities of the cervix such as ulceration or bleeding suggest cervical pathology, including polyps or malignancy. Tender nodules in the posterior fornix suggest endometriosis, and both endometriosis and pelvic adhesions cause fixation of the uterus. Acute pain when touching the cervix (cervical excitation) suggests an acute pelvic condition such as infection, cyst accident or tubal rupture.
Fibroids can cause uterine irregularity and enlargement. The size is related to that of the uterus in pregnancy. A tangerine-sized uterus is 6 weeks, an apple 8 weeks, an orange 10 weeks and a grapefruit 12 weeks.
It is hard to tell whether a large midline mass is ovarian or uterine. Push the mass upwards with your left hand and feel the cervix with your right hand. A mass which moves without the cervix suggests an ovarian mass.
Investigations
See Figures 10.33-35. Always consider carrying out a pregnancy test even if the woman says she cannot be pregnant (Box 10.15).
10.15 Investigations in gynaecological disease
| Full blood count | Heavy menstrual bleeding |
| White blood cell count | Pelvic infection |
| C-reactive protein | Pelvic infection |
| Renal and liver function tests | Pelvic masses |
| Gonadotrophins, sex steroids, prolactin | Ovarian dysfunction |
| High vaginal swab | Pelvic and vaginal infections |
| Midstream urine | Urinary infection |
| Endocervical swab | Chlamydia or gonorrhoea |
| Biopsy | Vulva, vagina and cervix |
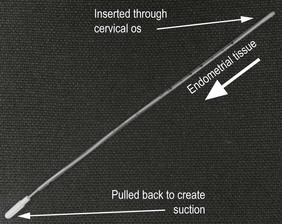
| Pipelle biopsy | Endometrial biopsy |
| Transabdominal or transvaginal ultrasound | Assess pelvic organs |
| X-ray | Assess tubal patency |
| Hysteroscopy | Intrauterine pathology |
| Laparoscopy | Pelvic visualisation and intervention |
| Urodynamic studies | Stress and urge incontinence |
| Colposcopy | Assess cervix for premalignant changes |
The obstetric examination
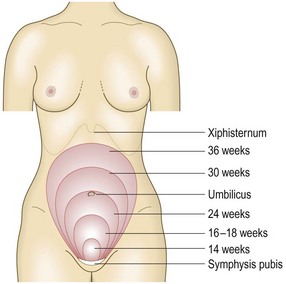
The size of the uterus increases as pregnancy advances (Fig. 10.37). At 20 weeks, the uterine fundus is at the umbilicus; by 36 weeks it reaches the xiphisternum. The distance from the pubic symphysis to the top of the uterine fundus is the symphyseal fundal height (SFH). If the baby is growing well, the SFH in centimetres approximates to the duration of pregnancy in weeks.
Symptoms and definitions
Estimated date of delivery (EDD)
This is the date that the baby is ‘due’ to deliver, 40 weeks from the first day of the LMP.
To calculate the EDD: add 1 year and 7 days and subtract 3 months from the date of the LMP. So, if the date of the LMP was 28 August 2013, the EDD is 4 June 2014.
However, only a very small proportion of babies deliver on the exact EDD; the majority deliver from 37 to 42 weeks’ gestation. The EDD is most accurately estimated from ultrasound measurement of fetal crown, rump length or head circumference in the first trimester of pregnancy.
Parity
The number of previous births is written in the format ‘para x + y’. x is the number of live births and any births over 24 weeks’ gestation. y is the number of births before 24 weeks of pregnancy of babies who did not show any signs of life, all ectopic pregnancies, miscarriages and terminations of pregnancy before 24 weeks’ gestation. For example, a woman who has had one baby by caesarean section at 39 weeks, a termination of pregnancy at 12 weeks and an ectopic pregnancy at 8 weeks is para 1 + 2. A woman is ‘parous’ if she has had one or more live births or births over 24 weeks (Box 10.16).
10.16 Examples of parity
| A women who: | Para | |
| is not pregnant, has had a single live birth, one miscarriage and one termination | 1 + 2 | |
| has had two previous pregnancies resulting in a live birth and a stillbirth | 2 + 0 | |
| is pregnant with a singleton pregnancy, has had live twins and a previous ectopic | 1 + 1 | |
| is not pregnant, has had a twin pregnancy resulting in two live births | 1 + 0 |
Gestation
The number of weeks that the woman has been pregnant is the gestation. It is counted from the LMP and expressed in weeks plus days, e.g. 24 + 6. Pregnancy is dated from the LMP for convenience. Fertilisation and implantation do not occur until after ovulation. Ovulation occurs 14 days before the next LMP. For example, a woman with a 28-day cycle ovulates on day 14 but a woman with a 32-day cycle ovulates on day 18.
The 40 weeks of a pregnancy are divided into first, second and third trimesters.
The lie
This describes the longitudinal axis of the fetus related to the longitudinal axis of the mother’s uterus. Most fetuses have a longitudinal lie in the third trimester (Fig. 10.38).
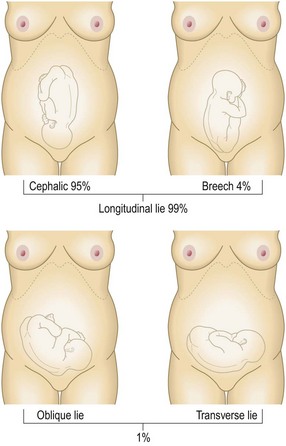
The presentation
This is the part of the fetus’s body which is expected to deliver first. With a longitudinal lie there is either a cephalic or a breech presentation (Fig. 10.38).
Oligoamnios and polyhydramnios
These terms describe too little or excess amounts of amniotic fluid respectively.
Live birth
Live birth is the spontaneous birth of a live baby, regardless of the length of time the baby lives for.
Stillbirth
The birth of a potentially viable baby who shows no signs of life is a stillbirth. In the UK it includes all births at 24 weeks’ gestation and above; in Australia it includes all births at 20 weeks’ gestation and above.
Fetal movements
Fetal movements are initially felt by pregnant women at 16–20 weeks’ gestation. Their frequency increases until about 32 weeks to an average of 30 movements per hour and this level remains unchanged until delivery. The ‘classic’ fetal movement is a kick, but any perceived fetal activity counts as movement. Movements may decrease if the mother is given sedative drugs, and may not be felt if the placenta is anterior. They also may decrease with intrauterine compromise which may precede stillbirth.
Physiological symptoms
Physiological symptoms are common. Breast tenderness, often the earliest symptom of pregnancy, may occur even before a missed period. Mild dyspnoea may be due to increased respiratory drive early in pregnancy or diaphragmatic compression by the growing uterus late in pregnancy. Heartburn increases in prevalence as pregnancy advances, affecting up to three-quarters of all pregnant women by the third trimester. Constipation, urinary frequency, nausea and vomiting (which usually resolve by 16–20 weeks) and aches and pains, especially backache, carpal tunnel syndrome and pubic symphyseal discomfort, also occur.
Secondary amenorrhoea is the most obvious symptom of early pregnancy.
Bleeding in pregnancy
Bleeding in pregnancy before 24 weeks may herald a miscarriage; after 24 weeks it is called an antepartum haemorrhage.
Pre-eclampsia
Pre-eclampsia is a multifactorial syndrome associated with high blood pressure, proteinuria and placental compromise and is a significant cause of maternal and fetal morbidity. It is often asymptomatic and is detected by blood pressure monitoring and urinalysis.
Pruritus
Pruritus (itching) occurs in one-quarter of pregnant women and may rarely be associated with liver cholestasis.
Breathlessness
Breathlessness is common in pregnancy but, if associated with chest pain, consider pulmonary embolism (p. 157).
Maternal mortality: This is the death of a woman while pregnant or within 42 days of delivery, miscarriage or termination. Death can be from any cause but must be related to or aggravated (directly or indirectly) by the pregnancy or its management. Deaths from accidents or incidental causes are not included. Late maternal deaths are those occurring between 42 days and 1 year. Deaths in pregnant women from conditions that are not unique to pregnancy are remaining constant in the UK and are commoner than maternal deaths due to complications arising directly as a result of pregnancy, delivery or its management.
The history
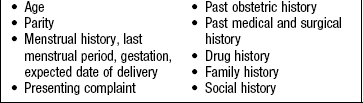
Take a full history at the first visit (the ‘booking’ visit) and establish the LMP (Box 10.17). At subsequent visits explore any new symptoms, symptoms relevant to ongoing conditions, and whether the patient feels the baby move. Remember that pregnant women can have illnesses that are not directly related to pregnancy.
Past history
Record information about each previous pregnancy (Box 10.17).
10.17 Information to be recorded for previous pregnancies
• Date and gestation of delivery
• Indication for and mode of delivery, e.g. spontaneous vaginal delivery, operative vaginal delivery (forceps or ventouse) or caesarean section
• Singleton or multiple pregnancy
• Any pregnancy complications (take a full history)
• Duration of first and second stage of labour
Note all past medical and surgical events. Pregnancy may adversely affect many diseases. Some conditions, e.g. asthma, may improve during pregnancy but worsen postnatally. Many illnesses adversely affect pregnancy outcome, and indirectly may cause maternal death.
Drug history
Ask about any prescribed medication, over-the-counter drugs, ‘natural’ remedies and illegal drugs. Find out at what gestation these drugs were taken. Advise the patient to stop smoking and abstain from alcohol. Check that she is taking 400 µg of folic acid until 12 weeks’ gestation to reduce the incidence of neural tube defects, including spina bifida.
Family history
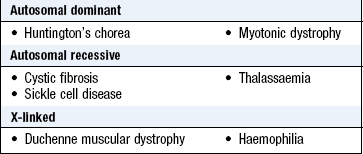
To explore possible inherited conditions, find out the full family history of both the pregnant woman and the father (Boxes 10.18 and 10.19).
Social history
Lower socioeconomic status is linked with increased perinatal and maternal mortality. Ask the patient who her partner is, how stable the relationship is, and if she is not in a relationship, who will give her support during and after her pregnancy. Was the pregnancy planned or not? If unplanned, find out how she feels about it. Encourage her to exercise regularly and to avoid certain foods, such as tuna (high mercury content), soft cheeses (risk of Listeria) and liver (high vitamin A content). Domestic violence can start or escalate in pregnancy and is associated with an increased risk of maternal death.
Occupational history
Ask what her job entails and whether she plans to return to it. Use this opportunity to give her advice on the safety (or otherwise) of continuing work. Occupations which involve exposure to ionising radiation have specific risks to the fetus or pregnant woman and her job profile may require modification. There is no definitive evidence of a link between heavy work and preterm labour or pre-eclampsia.
The physical examination
Booking visit: Do not perform a routine full physical examination (including breast and vaginal examination) in healthy pregnant women. It is unnecessarily intrusive and has a low sensitivity for disease identification. Calculate body mass index and fully examine any woman with poor general health. Take the blood pressure (p. 113) (Box 10.21).
10.21
Antenatal booking visits
Subsequent visits: 10 visits are recommended in an uncomplicated first pregnancy, seven for subsequent pregnancies.
National Collaborating Centre for Women’s and Children’s Health (2008) Antenatal care. Routine care for the healthy pregnant woman. Available online at: http://www.nice.org.uk/nicemedia/live/11947/40145/40145.pdf.
Examination sequence
Before examining the patient, measure her height and weight and ask her to empty her bladder. She should lie with her head on a low pillow, her abdomen exposed from the symphysis pubis to the xiphisternum.
Examine women in late pregnancy in the left lateral position, 15° to the horizontal, to avoid vena caval compression, which can cause hypotension for the mother and hypoxia for the fetus.
Note her general demeanour. Is she at ease or distressed by physical pain?
Note any scars, particularly from previous caesarean section, as well as a linea nigra and striae gravidarum. Note the swelling of the uterus arising from the pelvis and any other swellings.
Ask the patient to tell you about any tenderness and constantly observe her facial and verbal responses.
Place the flat of your hand on the uterine swelling. Gently flex your fingers to palpate the upper and lateral edges of its firm mass. Note any tenderness, rebound or guarding outside the uterus. Palpate lightly to avoid triggering myometrial contraction which makes fetal parts difficult to feel. Avoid deep palpation of any tender areas of the uterus. Note any contractions.
Face the woman’s head. Place both your hands on either side of the fundus and feel the fetal parts. Estimate if the liquor volume is normal. Assess how far from the surface the fetal parts are. If you can only feel them on deep palpation, this implies large amounts of fluid (Fig. 10.39A).
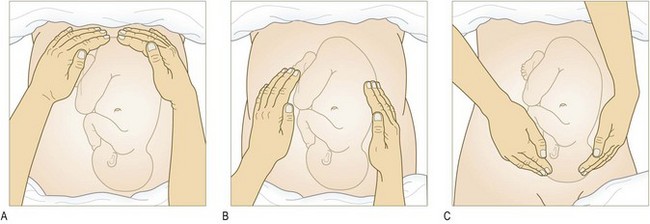
Fig. 10.39 Abdominal examination.
(A) Palpate the fundal area to identify which pole of the fetus (breech or head) is occupying the fundus. (B) Slip your hands gently down the sides of the uterus to identify which side the firm back and knobbly limbs of the fetus are positioned. (C) Turn to face the patient’s feet and slide your hands gently on the lower part of the uterus.
With your right hand on the woman’s left side, feel down both sides of the uterus. The side which is fuller suggests the fetal back is on that side (Fig. 10.39B).
Now face the woman’s feet. Place your hands on either side of the uterus, with your left hand on the woman’s left side, and feel the lower part of the uterus to try and identify the presenting part. Ballott the head by pushing it gently from one side to the other and feel its hardness move between your fingers (Fig. 10.39C).
After 20 weeks measure the SFH in centimetres. With a tape measure, fix the end at the highest point on the fundus (not always in the midline) and measure to the top of the symphysis pubis. To avoid bias, place the blank side of the tape facing you, lift the tape and read the measurement on the other side.
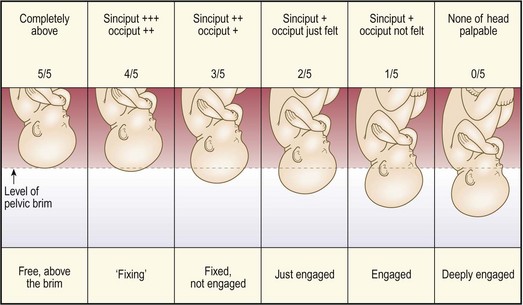
In late pregnancy or labour, assess whether more than 50% of the presenting part has entered the bony pelvis. This is usually the head and it is then said to be engaged (Fig. 10.40).
Percussion of the pregnant abdomen is unnecessary.
Listen for the fetal heart if you cannot feel fetal movements. A hand-held Doppler machine can be used from 14 weeks. From 28 weeks you can use a Pinard stethoscope over the anterior shoulder of the fetus. Face the mother’s feet and place your ear against the smaller end. Take your hand away and keep the stethoscope in place using only your head. Listen for the fetal heart which sounds distant, like listening to a clock through a pillow (Fig. 10.41).
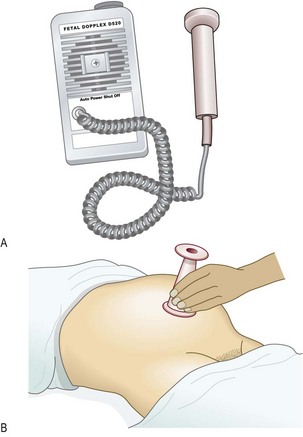
Fig. 10.41 Auscultation of the fetal heart.
(A) Doppler fetal heart rate monitor. (B) Pinard fetal stethoscope. The fetal rate varies between 110 and 160 bpm and should be regular.
Do not perform a vaginal examination routinely in pregnancy unless there is a specific indication.
Normal findings: Abdominal organs are displaced during pregnancy so swelling may be difficult to identify, e.g. ovarian cyst, and pain and tenderness may not be in usual sites. The kidneys and liver cannot be palpated and listening for bowel sounds may be difficult in late pregnancy. In tall or thin patients, the SFH may be less than expected; in obese patients, it may be larger. Ultrasound scanning is now routinely used to assess fetal development (Figs 10.42 and 10.43).


Abnormal findings: After 25 weeks’ gestation a difference of 3 or more between the number of completed weeks of pregnancy and the SFH in centimetres may suggest that the baby is small or large for dates. Investigate this with ultrasound. From 36 weeks a lie other than longitudinal is abnormal and requires further investigation or treatment. Do not routinely listen to the fetal heart unless the mother requests this.
Investigations
Perform dipstick urinalysis at each visit, looking for glycosuria or proteinuria. One + or more of protein may indicate a urinary tract infection or pre-eclampsia. Glycosuria requires a formal test for gestational diabetes (Boxes 10.22 and 10.23).
10.22
Gestational diabetes
The sensitivity of glycosuria in the detection of gestational diabetes is less than 30%.
NICE. Antenatal care. Routine care for healthy pregnant women. 2008. Available online at: www.nice.org.uk/CG062.
10.23 Antenatal investigations
| Urinary glucose | Every visit: if persists, consider glucose tolerance test |
| Urinary protein | Every visit: trace or +, check midstream specimen of urine; ++ or more, consider pre-eclampsia |
| Full blood count | Booking, 28 weeks, 36 weeks: treat if haemoglobin level falls <105 g/L |
| Haemoglobin electrophoresis | Booking: sickle cell and thalassaemias. Routine for patients of mixed ethnicity |
| Blood grouping and antibody screen | Booking and as advised by laboratory. Rhesus and Kell most common cause of isoimmunisation |
| Rubella | Booking |
| Hepatitis B and C | Booking |
| Human immunodeficiency virus (HIV) | Booking (unless patient opts out) |
| Syphilis testing | Booking |
| Plasma glucose | 28 weeks |
| Urine specimen for culture | As required |
| Combined biochemical screening and nuchal translucency measurement for trisomy 21 | 11–14 weeks: detects 80–90% of pregnancies affected by trisomy 21 |
| First-trimester ultrasound scan | 6–13 weeks: confirms viability, gestational age within 1 week, multiple pregnancy, adnexal mass |
| Detailed ultrasound scan | 18–22 weeks: detects 90% of major congenital abnormalities |
| Ultrasound scan for placental site | Antepartum haemorrhage after 24 weeks: more reliable as gestation advances when lower segment forms – 1 in 4 patients have a low placenta at 20 weeks; all patients with a previous caesarean section |
| Ultrasound scan for growth | Clinical suspicion of poor growth, usually after 24 weeks |
| Amniocentesis | 15 weeks for fetal karyotype: 0.5–1% risk of miscarriage |
| Chorionic villus biopsy | 10 weeks onwards for fetal karyotype, single-gene disorders 2% risk of miscarriage |
The male genital examination
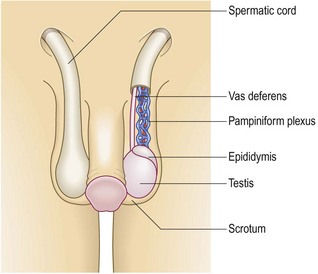
The male genitalia include the testes, epididymes and seminal vesicles, penis, scrotum and prostate gland (Fig. 10.44).
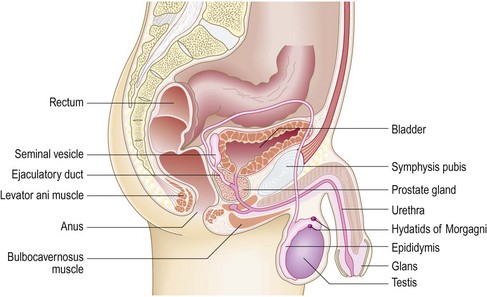
Fig. 10.44 Anatomy of the male genitalia.
The male genitalia include the external organs, seminal vesicles and the prostate gland.
The testes develop intra-abdominally near the embryonic kidneys and migrate through the inguinal canal into the scrotum, by birth. They have their own blood, lymphatic and nerve supply, so testicular problems may cause abdominal pain and tumours or inflammation may result in enlargement of the para-aortic lymph nodes. The testes lie within the scrotum separated from each other by a muscular septum; the left testis lies lower than the right. Each testis is oval and 3.5–4 cm long and covered by a fibrous layer, the tunica albuginea, which forms the posterior wall of the tunica vaginalis. This is a prolongation of the peritoneal tube that developmentally follows the testis down into the scrotum; if it persists, it is called the processus vaginalis and may be associated with an indirect inguinal hernial sac or cause a congenital hydrocoele. Along the posterior border of each testis the epididymis is formed by efferent tubules draining the seminiferous tubules through the rete testis. Multiple veins in the pampiniform plexus form one vein at the deep inguinal ring.
The testes produce sperm and hormones, predominantly testosterone. Sperm are produced from the germinal epithelium. They mature in the epididymis and pass down the vas deferens to the seminal vesicles for storage. They are ejaculated from the urethra, together with prostatic fluid, at orgasm. Testosterone is produced from the Leydig cells. Sperm and testosterone production commences at puberty, which occurs between 10 and 15 years of age (Fig. 15.19).
The penis has two cylinders of endothelial-lined spaces surrounded by smooth muscle, the corpora cavernosa (Fig. 10.45). These are bound with the bulbospongiosus surrounding the urethra and expanding into the glans penis. The penile skin is reflected over the glans, forming the prepuce (foreskin). The penis carries urine and semen. Sexual arousal causes a parasympathetically mediated increased blood flow into the corpora cavernosa with erection to enable vaginal penetration. Continued stimulation causes sympathetic-mediated contraction of the seminal vesicles and prostate, closure of the bladder neck and ejaculation. Following orgasm, reduction in blood inflow causes detumescence (Fig. 10.44).
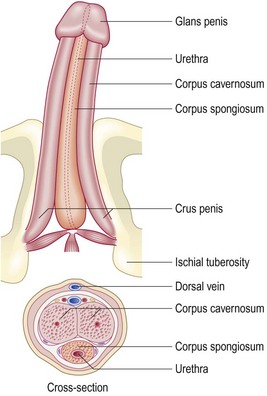
Fig. 10.45 Anatomy of the penis.
The shaft and glans penis are formed from the corpus spongiosum and the corpus cavernosum.
The scrotum is a pouch lying posterior to the penis which contains the testes. It has thin pigmented, ridged or wrinkled skin enclosing the dartos muscle (Fig. 10.46). The dartos is highly contractile and helps to regulate the temperature of the scrotal contents. The testes are held in the scrotum as sperm production is most efficient at temperatures lower than the body.
The prostate and seminal vesicles produce a fructose-rich fluid as an energy substrate for sperm. After age 40 the prostate develops a trilobar structure because of benign enlargement. Two lateral lobes and a variable median lobe protrude into the bladder and may cause urethral and bladder outflow obstruction. Prostate cancer develops in the peripheral tissue of the lateral lobes and sometimes may be detected by digital rectal examination. Only the posterior aspect and the lateral lobes of the prostate can be felt by rectal examination (p. 190).
Symptoms and definitions
Hydrocoeles: These are swellings due to fluid in the tunica vaginalis (Fig. 10.47). They are usually idiopathic but may be secondary to inflammatory conditions or tumours.
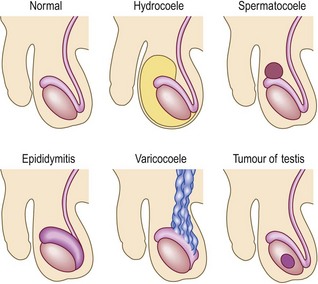
Epididymal cysts: Swellings of the epididymis which are completely separate from the body of the testis are epididymal cysts. They are isolated, adherent to the epididymis alone and virtually never malignant. Painful swellings at the superior pole of the testis, or adjacent to the head of the epididymis, are usually due to torsion of a paramesonephric duct remnant, the hydatids of Morgagni.
Varicocoeles: These are varicosities of the spermatic vein which feel like a ‘bag of worms’ in the scrotum.
Testicular tumours: These cause painless hard swellings of the body of the testis. Around 15% of tumours may occur close to the rete testis and may cause epididymal swelling and pain.
Epididymitis: Inflammation of the epididymus produces painful epididymal swelling, most often caused by STIs in young men, or coliform urinary infection in the elderly.
A single testis: This may be due to incomplete testicular descent of the ‘missing’ testis through the inguinal canal or an ectopic testis in the groin. Ask about previous surgery for a testicular tumour or testicular maldescent. Unilateral testicular atrophy may result from mumps infection, torsion of the testis, vascular compromise after inguinal hernia repair or from a late orchidopexy for undescended testis.
Bilateral testicular atrophy: This suggests primary, or secondary, hypogonadism or primary testicular failure. Look for hormonal abnormalities, or signs of anabolic steroid usage, and check the development of secondary sexual characteristics (Fig. 15.19).
Penile and urethral abnormalities
Urethritis: Inflammation of the urethra may cause dysuria (pain on micturition) or a urethral discharge. The most common causes are non-specific urethritis and gonococcal infection.
Phimosis: Narrowing of the preputial orifice which prevents retraction of the foreskin is called phimosis. This may produce balanitis (recurrent infection of the glans penis), posthitis (infection of the prepuce) or both (balanoposthitis).
Paraphimosis: This is an inability to pull the foreskin forward, after retraction, because of a constriction ring in the prepuce which jams behind the corona of the glans (Fig. 10.48).

Peyronie’s disease: Peyronie’s disease is a fibrotic condition of the shaft of the penis, of unknown aetiology, producing curvature, narrowing or shortening of the corpora cavernosa with erection.
Priapism: This persistent rigidity in the corpora cavernosa is characterised by longitudinal rigidity with a flaccid glans. Causes include leukaemia and sickle cell disease, pelvic malignancy and drugs.
Genital ulcer: A break in the mucosa or skin anywhere on the genitals is an ulcer. Painful ulcers are usually caused by herpes simplex; painless ulcers occur in reactive arthritis (p. 323), lichen simplex and (rarely) syphilis.
Sexual dysfunction: There are different problems and causes of sexual dysfunction, including psychological issues, alcohol, systemic disease (especially diabetes mellitus), peripheral vascular disease and drugs (Box 10.24).
Prostate abnormalities
Prostatitis: Inflammation of the prostate gland causes boggy, tender enlargement of the prostate. Usual causes are STI in younger men and Escherichia coli in older men.
Benign hyperplasia: This is common in men >60 years and associated with urinary symptoms (Box 9.2). The median sulcus is preserved and the prostate may feel smooth and rubbery.
The history
Ensure you understand what the man’s main genital or urinary problems are, the timescale of their development and how they affect his lifestyle. Be sensitive to his concerns but clarify the exact nature of any sexual activity (Ch. 9 and p. 9).
Take a general urological history, including a history about genital swelling, problems with micturition or discharge; be precise in asking about the site of any pain apparently emanating from the urinary tract. Ask about past, or intended, conceptions and about the man’s sexual function, when appropriate.
Past history
Ask about previous urological procedures, including neonatal surgery, hypertension and urinary infections. Relevant general surgical procedures, particularly pelvic operations, previous vasectomy and STIs and their complications, are important.
Drug history
Ask about previous urological drug treatments and obtain a full list of all medications and drugs taken recreationally. In particular note drugs such as α-adrenoreceptor blockers, which may cause retrograde ejaculation; antihypertensive agents, which may cause erectile dysfunction; vasoactive drugs, e.g. alprostadil, which may result in a prolonged erection, and antidepressants, which may affect sexual function.
The physical examination
Ensure privacy. Explain what you are going to do, why it is necessary and offer a chaperone. Record the chaperone’s name; if the offer is refused, record the fact. Allow the patient privacy to undress.
Have a warm, well-lit room with a moveable light source. Apply alcohol gel and put on gloves.
Ask the patient to stand and expose the area from his lower abdomen to the top of his thighs unless you are examining the inguinoscrotal area. In this case ask him to lie on his back initially.
The skin
Examination sequence
Look in turn at the groin, skin creases, perineum and scrotal skin for redness, swellings or ulcers. Note the hair distribution.
If you see any swellings in the groin palpate these and define them using SPACESPIT (Box 3.11).
Abnormal findings: There may be alopecia or infestation. Patients who shave their pubic hair may have dermatitis (inflammation of the dermis) or folliculitis (infection around the base of the hairs) causing an irritating red rash. Intertrigo (infected eczema) occurs in the skin creases and lymphadenopathy may be due to local or general causes.
Scrotal oedema can be caused by systemic or local disease. Heart and liver dysfunction may cause significant genital oedema, as may the nephrotic syndrome and lymphoedema due to para-aortic lymphadenopathy.
The penis
Examination sequence
Look at the shaft and check the position of the urethral opening to exclude hypospadias (urethra opening partway along the shaft of the penis) (p. 365).
Palpate the shaft for fibrous plaques (usually on the dorsum). Palpate any other lesions to define them.
Retract the prepuce and inspect the glans for red patches or vesicles.
Always draw the foreskin forward after examination to avoid a paraphimosis.
Take a urethral swab if your patient has a discharge or is having sexual health screening.
The scrotum
Examine the scrotum with the man standing. Then ask him to lie down if you find a swelling you can’t ‘get above’.
Ask the patient whether he has any genital pain. If the patient is cold or apprehensive the dartos muscle contracts and you will not be able to palpate the scrotal contents properly.
Examination sequence
Inspect the scrotum for redness, swelling or ulcers, lifting it to inspect the posterior surface.
Note the position of the testes and any paratesticular swelling and tenderness.
Palpate the scrotum gently using both hands. Check that both testes are present. If they are not, examine the inguinal canal and perineum, checking for ectopic testes.
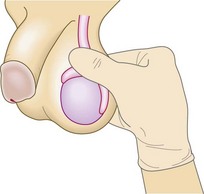
With each testis in turn, place the fingers of both your hands behind the testis to immobilise it and use your index finger and thumb to palpate the body of the testis methodically. Feel the anterior surface and medial border with your thumb and the lateral border with your index finger (Fig. 10.49).

Check the size and consistency of the testis. Note any nodules or irregularities. Measure the testicular size in centimetres from one to the other.
Palpate the spermatic cord with your right hand. Gently pull the testis downward and place your fingers behind the neck of the scrotum. Feel the spermatic cord and within it the vas, like a thick piece of string.
Decide whether a swelling arises in the scrotum or from the inguinal canal. If you can feel above the swelling, it originates from the scrotum; if you can’t, the swelling usually originates in the inguinal region (Fig. 10.50).
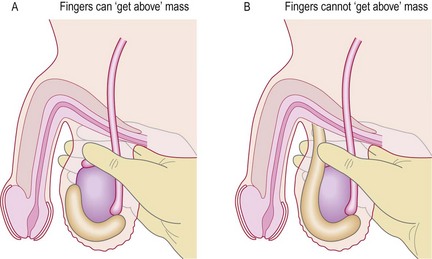
Fig. 10.50 Testing for scrotal swellings.
(A) It is possible to ‘get above’ a true scrotal swelling. (B) This is not possible if the swelling is caused by an inguinal hernia that has descended into the scrotum.
Place the bright end of a torch against a scrotal swelling (transillumination) (Fig. 15.5). Fluid-filled cysts allow light transmission and the scrotum glows bright red. This is an inconsistent sign which does not differentiate a hydrocoele from other causes of intrascrotal fluid, such as a large epididymal cyst. With thick-walled cysts transillumination may be absent (Fig. 15.5).
Normal findings: The right testicle is usually closer to the inguinal canal than the left but testes may be highly mobile (retractile). A normal testis is 5 cm long. The normal epididymis is barely palpable except for its head (Fig. 10.51), which feels like a pea separate from the superior pole of the body of the testicle.
Abnormal findings: Sebaceous cysts are common in the scrotal skin. If you can get above a scrotal swelling, it is a true scrotal swelling. If not, it may be a varicocoele or inguinal hernia which has descended into the scrotum. A varicocoele feels like a ‘bag of worms’ in the cord and should disappear when the patient lies down. If it does not, then consider a retroperitoneal mass compressing the testicular veins. A bulky or painful mass in the scrotum when you cannot palpate the testis needs an ultrasound scan to clarify the nature of the intrascrotal structures.
A retracted testicle accompanied by acute pain and swelling occurs in testicular torsion (Fig. 10.52).

The prostate
Ask the patient to lie in the left lateral position.
Examination sequence
Perform a rectal examination (p. 190).
Palpate the prostate anteriorly through the rectal wall.
Note any tenderness and assess the consistency. Is it hard, or boggy?
Withdraw your finger. Give the patient tissues to clean himself and privacy in which to get dressed.
Investigations
See Box 10.25.
10.25 Investigations in male genital disease
| Investigation | Indication/comment |
| Urinalysis | Protein and blood +++ in urinary tract infection and epididymitis |
| Serum prostate-specific antigen | Raised in prostate cancer but increases with age, prostatic volume, following prostatic trauma and in seminal or urinary tract infection |
| Serum beta-human chorionic gonadotrophin, alpha-fetoprotein and leukocyte alkaline phosphatase | Raised in some types of testicular cancer and in bony metastases |
| Serum follicle-stimulating hormone (FSH) and luteinising hormone (LH) | In azoospermia FSH and LH levels may be low due to pituitary dysfunction. FSH may be normal in obstructive azoospermia or maturation arrest and will be elevated in primary testicular failure |
| Serum prolactin | Raised prolactin suggests a pituitary tumour when libido is reduced |
| Serum testosterone and sex hormone-binding globulin (SHBG) | Low in lack of virilisation or sometimes in erectile dysfunction |
| Midstream urine | Urinary tract infection, testicular pain, epididymitis |
| Urinary chlamydial polymerase chain reaction | Sexually transmitted infection (STI), urethral discharge or epididymitis |
| Urethral swab | Suspected STI |
| Semen analysis/culture | In infertility to assess volume, number and quality of sperm in the ejaculate. Two separate samples should be analysed. Culture semen only when pus cells are found or haemospermia persists |
| Genital ultrasound examination | Hydrocoele, acute scrotal pain, testicular or penile mass |
| Colour Doppler imaging | To assess blood flow in suspected testicular torsion, priapism and erectile dysfunction |
| Transrectal ultrasound examination | Increases the sensitivity and specificity of digital rectal examination in suspected prostate cancer. Defines the anatomy of the prostate and the seminal vesicles in infertility or persisting haemospermia |
| CT scanning | To find the site of an undescended testis and to stage testicular cancer |
| MR scanning | To stage prostate cancer and delineate the seminal vesicles |