The frail elderly
Examination of the frail elderly
Assessment of the frail elderly
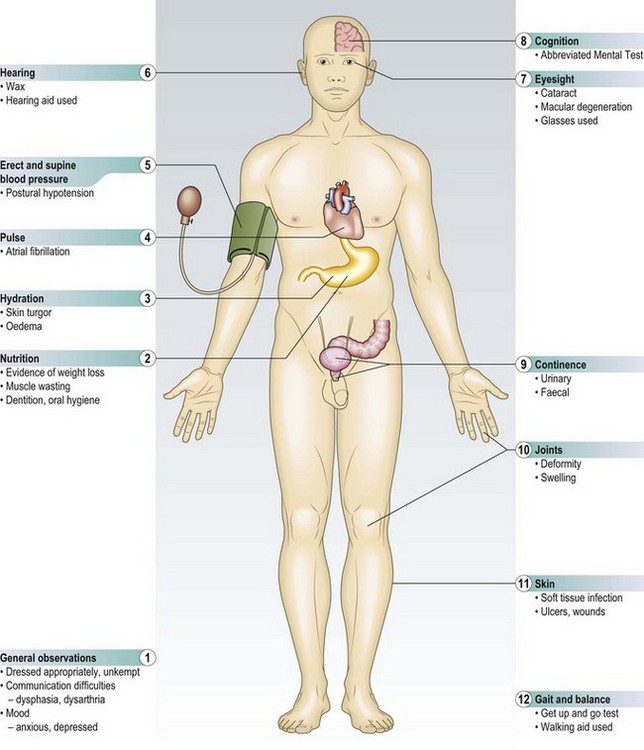
Comprehensive geriatric assessment is an evidence-based process which improves outcomes. It involves taking the history from the patient and, with the patient’s consent, that of a carer or relative, and is followed by a systematic examination, including assessment of:
Ideally the multiprofessional team (Box 16.1) work together to create a comprehensive assessment and individualised management plan.
 16.1 The multiprofessional team
16.1 The multiprofessional team
| Professional | Key roles in assessment of: |
| Physician | Physical state, including diagnosis and therapeutic intervention |
| Psychiatrist | Cognition, mood and capacity |
| Physiotherapist | Mobility, balance, gait and falls risk |
| Occupational therapist | Practical functional activities (self-care and domestic) |
| Nurse | Skin health, nutrition and continence |
| Dietician | Nutrition |
| Speech and language therapist | Speech and swallowing |
| Social worker | Social care needs |
The extent and focus of the assessment required depend on the clinical presentation. In non-acute settings, e.g. GP/outpatient clinic or day hospital, do not focus only on establishing what diseases are present, but also which functional impairments and problems most affect the patient’s life.
In acute settings, e.g. following acute hospital referral, primarily focus on what has changed; detect any new symptoms or signs of illness and any changes from baseline physical or cognitive function.
The complexity of problems presented, and need for comprehensive and systematic analysis, means that assessment is divided into components undertaken at different times, by different members of the multiprofessional team.
Definitions
Elderly: There is no specific age when a patient is ‘elderly’ and although >65 years is commonly used as the definition, there is no biological basis for this. There is considerable variation in ageing with many chronologically elderly patients appearing biologically and functionally younger and vice versa.
Frailty: Frailty becomes more common with advancing age and is a response to chronic disease and ageing itself. A frail elderly person typically suffers multimorbidity, often with cognitive impairment, visual and hearing loss, and may be on multiple medications. His general functional reserve and the capacity of individual organs and physiological systems are impaired, making the individual vulnerable to the effects of minor illness.
Multimorbidity: Multimorbidity (multiple illnesses) and disability (impaired capacity to undertake specific functions) are defining features of frailty (Box 16.2).
Presentation of disease
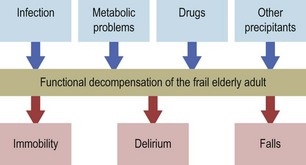
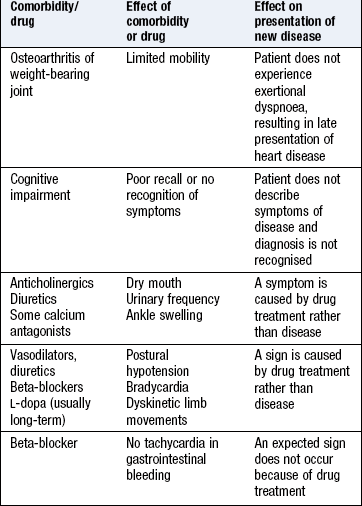
Classical patterns of symptoms and signs do occur in the frail elderly, but modified or non-specific presentations are common due to the effects of co-morbidity, drug treatment and the ageing process itself. As the combination of these factors is unique for each individual, the presentation of disease is distinct in each patient. In the frail elderly the first sign of new illness may not be a specific new symptom but a change in their functional status; typically, reduced mobility, altered cognition or impairment of balance leading to falls. Common precipitants are infections, changes in drug treatment and metabolic derangements but almost any acute insult can produce this response (Fig. 16.1).
Communication difficulties, cognition and mood: Communication can be challenging (Box 16.3). The history can be incomplete, difficult to interpret or misleading and the whole assessment, including physical examination, time-consuming.
 16.3 Communication difficulties – the seven Ds
16.3 Communication difficulties – the seven Ds
| Problem | Comment/causes |
| Deafness | Nerve or conductive |
| Dysphasia | Most commonly due to stroke disease but sometimes a feature of dementia |
| Dysarthria | Cerebrovascular disease, motor neurone disease, Parkinson’s disease |
| Dysphonia | Parkinson’s disease |
| Dementia | Global impairment of cognitive function |
| Delirium | Impaired attention, disturbance of arousal and perceptual disturbances |
| Depression | May mimic dementia or delirium |
Whenever possible, assess the patient somewhere quiet with few distractions. Make your patient comfortable, with access to a drink of water. Patients should wear any glasses, hearing aids or dentures they need. Help them to switch on and adjust their hearing aid if necessary. If they still cannot hear you clearly, use an electronic communicator. If communication remains difficult and they can read, write down simple questions and instructions.
Cognitive function includes the processes of perception, attention, memory, reasoning, decision making and problem solving. Cognitive impairment increases with age and has implications for assessment, treatment, consent and prognosis. Be alert to cognitive impairment with evidence of poor recall or limited ability to cooperate. Patients may not recall their medical history or may deny all symptoms, even when they are clearly unwell. Consider the possibility of cognitive impairment early, and tailor your assessment appropriately. Dementia and delirium commonly cause cognitive impairment and are underrecognised in community and hospital settings (p. 24).
Use the Mini Mental State Examination (MMSE) or Abbreviated Mental Test (AMT) or Addenbrooke’s Cognitive Examination (p. 26) to help detect cognitive impairment, but recognise that these should not be used alone to diagnose dementia or delirium.
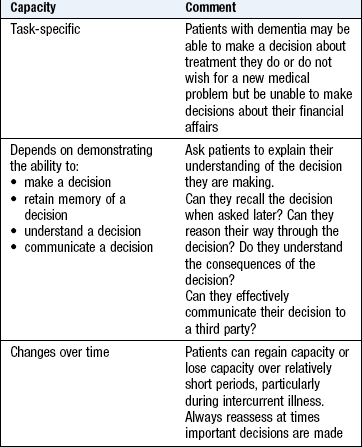
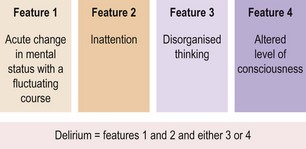
In acute presentations, consider delirium and use a validated screening tool, e.g. the Confusion Assessment Method (CAM) score to distinguish between delirium and dementia (Fig. 16.2). Remember that patients with delirium need not be agitated and are frequently quiet and withdrawn (hypoactive). Assessing capacity to make decisions is part of assessing cognitive function but specialised psychiatric assessment may be required (Box 16.4).
Coexisting problems, including impaired hearing, low mood or bradykinesia, can mimic cognitive impairment. Some patients present with apparently good social skills or ‘façade’ and cover their impaired memory by diverting the conversation to another topic. Do not ascribe changes in cognition to age alone without excluding dementia or delirium. Never use terms such as ‘vague’ or ‘poor historian’.
Depression is common in frail elderly people and may be difficult to diagnose. A formal psychiatric assessment and corroborating history from a carer or friend may be valuable. Standardised rating scales are available, e.g. the Geriatric Depression Scale. Consider using these for all patients >80 years.
Patients are often fearful that they will not return home after admission to hospital, and accordingly play down their symptoms or functional limitations. Always try to corroborate the history from a carer, relative or friend, with the patient’s consent.
The history
Frail elderly patients often have multiple symptoms. Take time to detail each symptom, and separate those arising from new acute illness from those due to background disabilities. Ask the patient:
If the patient focuses on a functional change such as difficulty walking, find out what the patient feels is the specific cause. Is there pain when moving? Is balance difficult or is there weakness, and if so, in one limb or both?
Try and gauge baseline health status. Find out what the patient’s symptoms, functional abilities and mental status were before the new presenting problem. This helps set realistic goals.
The patient’s perspective may vary from yours, particularly when you are assessing an acute episode. For example, a patient referred following sudden loss of consciousness may be unconcerned by this but anxious about long standing back pain. These symptoms are not coincidental; if it is important to your patient, it should be important to you.
Past history
Detail the past history and known comorbidities using all sources, including any previous records. Comorbidity may not relate directly to the current problem but may influence new problems and the feasibility and appropriateness of potential treatments (Box 16.5).
Drug history
Polypharmacy, drug interactions, adverse events and difficulties with compliance are common. Take a detailed drug history (p. 14), supplemented by additional information.
• Identify all medications, including over-the-counter preparations.
• Ask about any drugs that have been started or stopped recently, and if doses of regular medications have been altered.
• Explore ability to self-administer drugs; ask if the patient uses a dosette box or if a carer helps with administration.
• Explore ability to read labels, open bottles or use inhalers correctly.
• If patients have their drugs with them, go through them together. Ask patients what they believe each one is for, how it affects them and how often they take it.
• Ask if there are any drugs that they sometimes omit, e.g. diuretics on days that they are going out.
• Ask carers if there are partially used supplies of drugs in the house.
• Clarify any ‘allergies’ or previous adverse events; if in doubt, regard the allergy as significant.
• Explore which symptoms patients believe are caused by their drugs.
• Contact the prescriber, if necessary, to confirm details of drug history.
Some patients describe multiple drug intolerances, often imprecisely or inconsistently. Clarify what symptoms the patient believes to be adverse effects of drug treatment, as some may be unrelated. Failure to do so may deny the use of potentially useful treatment.
Family history
New presentation of disease with a strong genetic predisposition is unlikely, but family history may be important to patients who have lost siblings or their own children to specific conditions. They may think their own symptoms relate to the same problem.
Social and functional history
Complement a comprehensive social history with information about the patient’s functional capability as this affects their ability to cope at home, and what assistance they need to support their function there. Establish the patient’s current level of function, what it was before the onset of any new problem, and the time course of any functional deterioration. Abrupt functional decline suggests a more acute underlying precipitant or disease. Insidious decline suggests alternate pathologies or progression of underlying chronic disease. Get corroboration from a friend, relative or carer, but interpret all information obtained in association with objective functional assessment by yourself and other members of the multiprofessional team (Box 16.1).
Mobility and transfers: Can the person transfer from chair to bed or toilet and walk alone? Does he use a walking aid and can he manage stairs?
Home environment: Find out who is at home with the patient. If the patient lives alone, he may require additional support. Has the patient lived there long? A recent move may cause problems. What is access like to the house/bedroom/toilets? Does the patient need to use stairs, inside or outside? If the patient lives in sheltered accommodation, are meals provided, and is there an on-site warden or personal safety alarms? How does the patient feel about living there?
Daily activities: Can patients wash and dress themselves? Do they do their own shopping and prepare their own meals? Patients may need a carer to help them with these tasks.
Support: Find out what formal carer support the patient has, e.g. home help. Establish how often any carer visits and what that person does for the patient. Do family or friends help? If so, how much and how often?
Social interaction: Social isolation can contribute to mood disorders. Can patients still get out of the house by themselves or accompanied, or are they house-bound? How many visitors do they have?
Occupation: Do they still have a job and if so, what? If retired, find out about what they did as it may be relevant to current disease as well as allow you to see another side to them.
Systematic enquiry
The systematic enquiry forms part of a screening process and is important because many diseases present with non-specific functional deterioration, e.g. immobility, and you need clues to specific underlying precipitants. Because comorbidity is common, many conditions are underdiagnosed.
Use standard framework questions to concentrate on certain areas.
Cognitive impairment: Have patients noticed any memory problems or has anyone else commented on their memory? Does anyone help them with letters and bills?
Mood: Ask about how they sleep at night. How would they describe their mood and appetite? Are they still interested in previous pursuits, such as reading or following favourite television programmes?
Nutrition: Has their weight been steady over the past few months? Ask the patient whether they have noticed their clothes getting loose; this helps establish weight loss. How many meals do they have in the day and do they eat meat, fish, vegetables and fruit? Who prepares their meals?
Oral health: Do they have any problems with their teeth or gums? If they wear dentures, do they fit well? Ask if their mouth is dry.
Continence: Sensitively ask whether patients ever notice incontinence or leakage from their bladder or bowels. Are they aware when they are about to pass urine or a stool? Do they ever find it hard to get to the toilet in time? Do these problems stop them doing activities?
The physical examination
Physical examination is easiest when your patient can comply with your instructions. All patients benefit from clear, careful instruction and this is particularly important for the frail elderly who may have communication problems or find the examination routine demanding. Many have low levels of stamina and movement may be limited by physical disability. Integrate your physical examination to minimise movement for patients and maximise their understanding and cooperation. Help them to move around the room, to get on and off the examination couch and recognise that they will take longer to undress and dress. Some patients feel more comfortable if a family member, carer or friend is present, but always check that this is what they wish.
It may be challenging to examine a frail elderly person comprehensively because of communication barriers, the patient’s reduced physical stamina and functional impairment. Often the patient, doctor and carer have different goals or concerns. This means there are additional elements in the physical examination and an altered emphasis. It takes time and patience to perform a detailed assessment of a frail elderly patient.
Some elderly people have difficulty maintaining personal hygiene, grooming or appearance. Their hair and clothes may be unclean, nails unkempt and facial hair longer than in younger life. These findings may reflect underlying functional or cognitive impairment, social isolation or low mood, and are relevant to the patient’s overall functional status, condition and outlook, or need for social support.
Be aware of the common clinical signs found in frail elderly patients. Just as the history elicits multiple diverse and unexpected symptoms, a careful examination will often reveal many clinical signs in different clinical systems. In acute presentations, be alert to those signs that may, misleadingly, be absent (Box 16.6).
16.6 Modified signs in acutely unwell frail elderly patients
| Feature | Clinical context | Modification |
| Temperature | Possible sepsis | Systemic inflammatory response obtunded, may not mount pyrexia (or may become hypothermic) Core temperature normally lower and diurnal variation lost – → temperature may occur, but not > 37°C |
| Pulse rate | Volume status, response to sepsis or pain | Altered baroreceptor function may attenuate the rise in heart rate typically associated with these stressors |
| Blood pressure | Volume status, response to sepsis or pain | Altered baroreceptor function may modify BP response to acute illness |
| Postural blood pressure | Volume status | May be found in volume-replete patients due to primary autonomic dysfunction. Less reliable indicator of volume depletion |
| Skin turgor | Hydration | ↓ but less specific because of reduction in subcutaneous fat |
Document all signs. Try to determine their relevance to the presentation and care of each individual patient. Your history and subsequent targeted investigations will help determine the significance of examination findings. Assume that a physical sign is due to disease, which may be treatable, rather than ageing, which is not.
General examination
Hydration and nutrition: Disorders of hydration are common in frail elderly patients but accurate clinical assessment is difficult and classical signs less reliable (Box 16.7).
16.7 Assessment of dehydration
| Classical feature of dehydration | Interpretation in frail elderly |
| Postural hypotension | Less specific than in younger patients; may be caused by drugs, disease or age-related abnormal autonomic responses to postural change |
| Decreased skin turgor | Decreased collagen elasticity and reduced subcutaneous fat can mimic reduced turgor. Best assessed at the sternum |
| Impaired capillary refill time | Less reliable in the frail elderly because less specific |
| Dry mouth | A non-specific finding caused by other problems such as anticholinergic drugs or mouth breathing |
| Tachycardia in hypovolaemia | Less sensitive due to drug- or age-related abnormal autonomic responses |
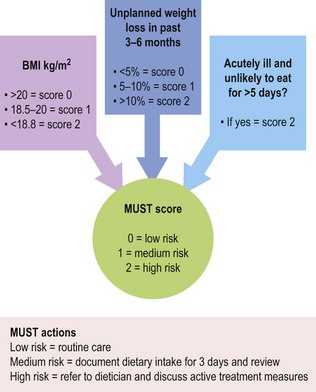
Undernutrition and low body weight are common features of frailty that may develop rapidly in hospitalised patients. They are frequently multifactorial so seek reversible factors. Consider chronic disease, e.g. COPD, new serious disease, e.g. cancer, poor social support or isolation and depression or dementia as these may present with low body weight. Other factors that contribute are poor oral health, poor function (being unable to obtain/prepare food) and cognitive impairment (being unable to prepare food or remember to eat it) (Fig. 16.3).
The skin: Bruising may suggest past or present steroid use, but is often simply age-related due to the reduction in subcutaneous supporting tissue. Rarely, it is due to scurvy (p. 56). Soft-tissue infections often cause functional decompensation and consequent confusion, immobility and falls (Fig. 16.1). Leg ulcers are common and frequently have multifactorial causes (p. 135). Pain from ulcers may reduce mobility. On admission to hospital many frail elderly patients have skin wounds that have been dressed in the community. Always remove these dressings, with the help of a nurse when possible, and assess the underlying lesion.
Frail elderly patients with limited mobility are vulnerable to the rapid development of pressure sores, particularly at times of intercurrent acute illness. Standardised assessment scores, e.g. the Waterlow Score, help identify patients at risk of skin breakdown.
Pain: In patients with impairment of communication or cognitive impairment, look for pain-related behaviour (Box 16.8).
16.8 Signs and behaviours associated with pain
| Type | Description |
| Autonomic changes | Pallor, sweating, tachypnoea, altered breathing patterns, tachycardia, hypertension |
| Facial expressions | Grimacing, wincing, frowning, rapid blinking, brow raising, brow lowering, cheek raising, eyelid tightening, nose wrinkling, lip corner pulling, chin raising, lip puckering |
| Body movements | Altered gait, pacing, rocking, hand wringing, repetitive movements, increased tone, guarding,* bracing† |
| Verbalisation/vocalisation | Sighing, grunting, groaning, moaning, screaming, calling out, aggressive/offensive speech |
| Interpersonal interactions | Aggression, withdrawal, resisting |
| Changes in activity patterns | Wandering, altered sleep, altered rest patterns |
| Mental status changes | Confusion, crying, distress, irritability |
*Guarding = abnormal stiff, rigid or interrupted movement while changing position.
†Bracing = a stationary position in which a fully extended limb maintains and supports an abnormal weight distribution for at least 3 seconds.
Continence: Urinary incontinence is common. The acute onset of incontinence can be caused by specific disease (p. 202), but can also be a non-specific feature of any acute illness or insult. It is common with advanced cognitive impairment. Faecal incontinence is less common, but has a major impact on care needs.
Vision and hearing: Hearing loss and visual symptoms, including impairment of visual acuity, are common (Box 16.9). They are often not noted and this will adversely affect communication, interaction and function. Hearing loss may be misinterpreted as cognitive impairment and vice versa. Use a Snellen chart (Fig. 12.17) or ask the patient to read from a newspaper to assess vision.
16.9 Sensory problems
| Visual | Underlying disease process |
| Loss of near vision (presbyopia) | Common in elderly because lens less pliable |
| Loss of central vision | Macular degeneration |
| Loss of peripheral vision | Glaucoma Stroke disease (homonymous hemianopia) |
| Glare from lights at night | Cataracts |
| Eye pain | Glaucoma |
| Auditory | |
| High-frequency loss | Presbyacusis Conductive deafness commoner due to otosclerosis |
| Generalised loss | Conductive – otosclerosis; wax Nerve – Paget’s disease, drug-induced ototoxicity; acoustic neuroma |
Make sure the external auditory meatus is not blocked with wax. Ensure patients wear their hearing aids with a functioning battery so you do not incorrectly diagnose cognitive impairment simply because they could not hear you properly. Assess hearing using the whispered voice test if they do not have hearing aids (p. 304).
Systems examination
Fully examine each system, but particularly note the differences that may occur in the frail elderly.
Cardiovascular system: Corneal arcus increases in prevalence in the elderly but is a poor sign of dyslipidaemia (Fig. 6.8C).
Blood pressure: A widened pulse pressure occurs because there is decreased arterial compliance. Isolated systolic hypertension and postural hypotension occur more frequently. The latter may result from age-related baroreceptor reflex change, disease or drugs. It may not be symptomatic but increases the risk of a fall.
Respiratory system: The significance of localised crackles is uncertain and they may not represent acute disease. Always exclude new respiratory disease.
Gastrointestinal system: Dry mouth and tongue are common side-effects of drugs and may affect taste and swallowing. Abnormal dentition or oral thrush or mouth ulcers may reduce oral intake and nutrition.
Nervous system: Cognitive impairment may reduce the accuracy of the history and affect consent for investigation and treatment. It will reduce the person’s awareness of safety and compliance. Impaired vibration and position sense occur in old age but always exclude correctable causes, e.g. vitamin B12 deficiency. They may impair balance and increase the risk of falls. Bilateral absent ankle reflexes may be normal, but unilateral loss is likely to indicate pathology.
Musculoskeletal system: Osteoarthritic changes in the hands and weight-bearing joints may predispose to falls or unsteadiness even if relatively asymptomatic or painless. Gouty tophi may be asymptomatic and reflect underlying renal dysfunction and influence the choice of drug therapy. Kyphosis occurs frequently from painless osteoporotic vertebral collapse. It may affect postural stability and even respiratory function. Low muscle mass is a frailty indicator and a risk factor for falls.
Gait: Gait abnormalities are risk factors for falls or exacerbate joint problems. They may indicate undiagnosed neurological disease, such as Parkinson’s disease. Sometimes gait problems may be helped by orthoses or mobility supports (Fig. 3.2).
Functional assessment
Functional assessment is divided into assessment of:
• The ability to undertake activities of daily living (ADLs), those activities required for self-care and domestic tasks:
• personal activities of daily living (PADL)
• domestic activities of daily living (DADL) (Box 16.10).
Mobility is a key determinant of physical function (Box 16.11). A wide variety of pathologies can impair mobility and produce distinctive abnormalities of gait (Box 11.13). Other diseases may affect mobility by causing decreased muscle strength or joint function. Frailty causes generally impaired muscle strength, function and poor mobility but no specific clinical findings on examination of muscle, nerves, joints or gait (Fig. 16.4).
 16.11
16.11
Mobility
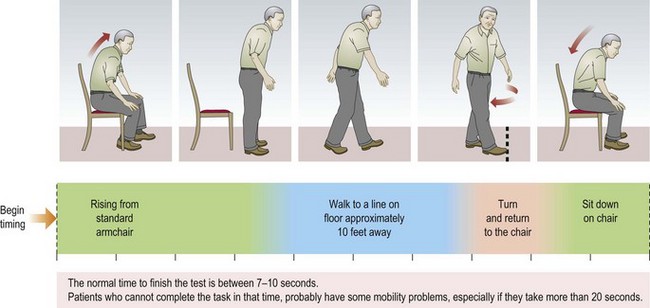
The Timed Get-Up and Go test is a simple measurement of mobility. Perform it in all patients presenting in non-acute settings.
Podsiadio D, Richardson S. The timed ‘Up & Go’: a test of basic functional mobility for frail elderly patients. J Am Geriatr Soc 1991;39:142–148.
Standardised rating scales are used for different components of function, e.g. the modified Barthel Index for activities of daily living and the Elderly Mobility Score for mobility. Use these scales to describe the patient’s abilities succinctly and, using sequential recording over time, objectively assess improvement or deterioration.
Common presentations
The frail elderly person with immobility: Establish patients’ normal mobility, when it changed and if the change was abrupt. Have they fallen? Is there any history of recent head injury, fevers or rigors, dizziness or poor balance? Have they noticed lower limb weakness, numbness or paraesthesia? Ask about joint pain, especially in the back, neck or lower limbs, and if there are any bladder or bowel symptoms. What is their current drug treatment and has this changed recently?
Examination sequence
 General examination: look particularly for signs of acute illness (Box 16.6). If they are able to walk, assess the posture and gait and any inappropriate footwear. Are they visually impaired? (Box 16.9). Are there signs of sepsis, or a distended bladder?
General examination: look particularly for signs of acute illness (Box 16.6). If they are able to walk, assess the posture and gait and any inappropriate footwear. Are they visually impaired? (Box 16.9). Are there signs of sepsis, or a distended bladder?
Cardiovascular system: check for postural hypotension.
Nervous system: note any neurological signs, particularly in the lower limbs, and look for evidence of Parkinson’s disease (p. 346).
Locomotor system: look for muscle wasting or fasciculation, joint abnormality and foot deformity.
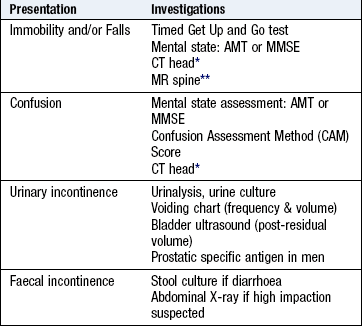
Consider specific investigations (Box 16.12).
The acutely confused frail elderly person: Always take a collateral history. Establish the person’s normal cognitive state and whether the change has been abrupt or gradual. Ask about symptoms of common acute illness, particularly infection, such as urinary frequency, productive cough, fever or rigors. Has the person complained of pain and if so, where? What is the current drug treatment and compliance? In particular, have there been any recent changes to drug treatment?
Examination sequence
Look for signs of acute illness (Box 16.6) and pain (Box 16.8).
Examine the skin, large joints, heart valves, prostheses and abdomen, e.g. biliary tract, colonic diverticulae, meninges, bladder and lungs.
Measure the pulse oximetry (SpO2).
Do a rectal examination (p. 189) to check for faecal impaction.
If patients have problems with vision or hearing, ensure they wear their glasses or working hearing aid.
Consider specific investigations (Box 16.12).
The frail elderly person with falls: What is patients’ normal mobility and have they had any blackouts? Find out how many falls they have had, over what timescale and if they have ever had any injury – in particular, a head injury. If they complain of dizziness, is this true vertigo (p. 245)? Ask systematically about palpitation, limb weakness, numbness or paraesthesia and any joint pain, especially in the back, neck or lower limbs. How is their vision? Have they had symptoms of infection recently, such as rigors or urinary symptoms? Ask about current drug treatment and any recent changes in drugs. A collateral history of a witnessed fall is helpful.
Examination sequence
Look for signs of bony or soft-tissue injury and acute illness, e.g. sepsis (Box 16.6).
Cardiovascular system: check for postural hypotension, arrhythmias and aortic stenosis.
Nervous system: are there neurological signs in lower limbs or evidence of Parkinson’s disease (p. 346)? Is there visual impairment?
Musculoskeletal system: look for joint or muscle abnormality and foot deformity. Do they have appropriate footwear? Note any posture or gait abnormality (Fig. 3.2).
Consider specific investigations (Box 16.12).
The incontinent frail elderly person: This may be either urinary or faecal incontinence or both.
Ask if patients can transfer and mobilise from a chair to toilet or commode?
Are they aware of the need to pass urine or defecate? Are they incontinent all the time or only intermittently? Is the stool formed or unformed?
Examination sequence
Nervous system: are they cognitively impaired? Is there other evidence of neurological disease? Palpate for the bladder and check that perianal sensation is normal.
Gastrointestinal: palpate for any abnormal abdominal masses. Examine the perineal skin and see if it is intact. Perform a rectal examination looking for anal fissure, haemorrhoids or other local disease. Note if the rectum is empty or impacted with faeces and assess anal tone. In a man, assess prostate enlargement; in a woman look for vaginal prolapse or atrophy.
Putting it all together
Comprehensive geriatric assessment requires excellent communication between members of the multiprofessional team. A problem-based approach helps to pull all this information together and formulate a clear individualised management plan.
Start by creating a problem list to summarise all the problems identified. Generate a provisional list after speaking with the patient and refine it after interviewing carers, undertaking the physical examination and hearing the outcome of functional assessments. Do not confine the list to medical diagnoses, but include symptoms, laboratory results and presenting features (Box 16.13).
 16.13 The problem-based approach
16.13 The problem-based approach
examples of how this might be used in a patient with falls and confusion
| Problem | Potential contributory factors | Management plan |
| Urinary incontinence | Urinary tract infection Faecal impaction |
Urinalysis Send midstream specimen of urine to confirm Rectal examination |
| Hyponatraemia | Bendroflumethiazide | Withhold bendroflumethiazide Monitor serum sodium |
| Confusion with features of delirium | Urinary infection Hyponatraemia Underlying dementia |
As above plus: Check MMSE Collateral history from carer Thyroid function Occupational therapy review |
| Foot ulcer | Absent pedal pulses | Check ankle brachial pressure index Discuss dressing with nurse |
| Poor mobility | Urinary infection Hyponatraemia Pain from foot ulcer Underlying cerebrovascular disease |
As above plus: Prescribe simple analgesia Full neurological/gait examination Assess vascular risk factors Physiotherapy review |
The problem list builds a complete picture of the patient and alerts you to how the different problems may interact. If a problem has several contributing factors, list them all. Use the list to develop a management plan addressing each problem and contributing factor. Include actions such as diagnostic investigations, treatment of identified disease, alteration of drug therapy and rehabilitation. Tailor your management plan specifically to the individual patient, considering the outcome goals you have agreed with the patient. Explain the proposed management plan to your patient and ensure that he understands and agrees.