The febrile adult
Examination of the febrile adult
Symptoms and definitions
Fever (pyrexia) is a body temperature >99th percentile of the healthy adult maximum (p. 61). Fever is present if the oral temperature is >37.7°C, or tympanic temperature >37.5°C. In immunodeficient or neutropenic patients, fever is a single temperature >38.3°C, or a temperature >38°C sustained for >1 hour.
Body temperature is tightly controlled to maintain normal metabolic processes. The set point is controlled by the hypothalamus and modified by infection, inflammation and, rarely, other conditions, e.g. hypothyroidism, lymphoma. Infection is the most common cause but in very young or elderly patients and those with impaired immune function (due to primary disease, e.g. human immunodeficiency virus (HIV), or following treatment, e.g. oral steroids, immunosuppressants) it may not produce fever.
Body temperature depends upon the balance between heat generation and loss, and the ambient environment. Heat-related illness occurs with exercise in high temperatures and humidity. It is more common at the extremes of age and may be precipitated or aggravated by drugs which affect thermoregulation, e.g. phenothiazines, alcohol, or which are associated with excessive exercise, e.g. ‘rave’ drugs, including ecstasy, amphetamines (Boxes 17.1 and 17.2).
 17.2
17.2
Fever
A patient who reports fever or whose forehead feels abnormally warm is highly likely to have a fever.
Buckley RG, Conine M. Reliability of subjective fever in triage of adult patients. Ann Emerg Med 1996;27:693–695. Hung OL, Kwan NS, Cole AE et al. Evaluation of the physician’s ability to recognize the presence or absence of anaemia, fever and jaundice. Acad Emerg Med 2000;7:146–156.
Fictitious fever is produced artificially by the patient or an attendant. It may form part of a Munchausen or Munchausen-by-proxy syndrome (Box 17.3).
 17.3 Clues to fictitious fever
17.3 Clues to fictitious fever
Extreme fever (>41°C) is life-threatening and is usually associated with:
• central problems with temperature regulation, e.g. following intracranial haemorrhage or head injury
• drug reactions, e.g. to anaesthetic agents, or drugs associated with the neuroleptic malignant syndrome
• severe environmental conditions often with strenuous unaccustomed exertion (heatstroke)
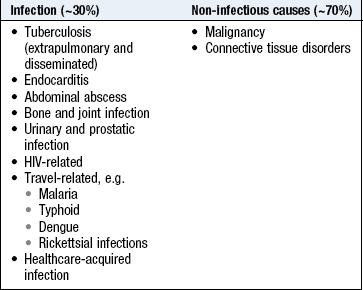
Fever (pyrexia) of unknown origin (FUO or PUO) is documented fever which remains unexplained after 2–3 weeks’ investigation. Healthcare-acquired PUO is fever in patients hospitalised for >48 hours with no infection evident at admission, and in whom the diagnosis remains uncertain after ≥3 days of appropriate evaluation (Box 17.4).
Rigors (chills) are bouts of uncontrollable muscular shaking, often with ‘chattering’ teeth, lasting for minutes. They are associated with rapid temperature rises and may be caused by cytokines and acute-phase proteins resetting the hypothalamic temperature set point. Subjectively the patient feels cold and unwell and the episode may be followed by sweating. A rigor may be associated with bacteraemia or malaria and is of poor diagnostic value.
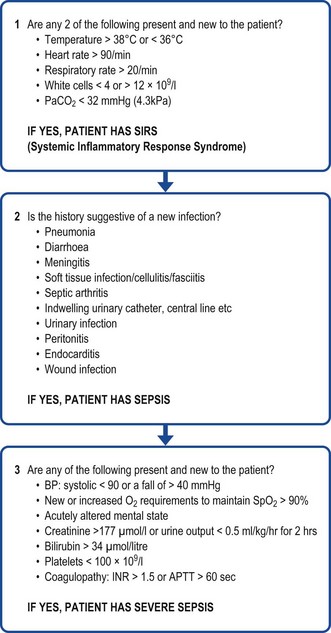
The terms systemic inflammatory response syndrome (SIRS), sepsis, severe sepsis and septic shock reflect progressively increasing morbidity and mortality in response to infection. Multiple organ failure and death ensue if recognition or treatment is delayed (Fig. 17.1). The term SIRS is not specific to infection.
The history
How has the fever been documented? What is its severity and time course? Have there been rigors or sweating?
Has there been a rash or skin changes? If yes, ask about its timing in relation to the fever, the distribution and direction of any progression and associated symptoms, e.g. pruritus, local lymphadenopathy.
Systematically ask about localising symptoms, e.g. cough, pleuritic chest pain, purulent sputum, vomiting, abdominal pain, jaundice, diarrhoea, dysuria, urinary frequency, headache, photophobia, neck stiffness, altered consciousness, joint pain, muscle aches, throat or ear discomfort and nasal discharge.
Are there constitutional symptoms, including easy fatigability, anorexia, weight loss, falls, change in daily activities or behaviour? Such symptoms may indicate infection in the elderly or immunocompromised.
Past medical history
Have there been previous or recurrent infections, illnesses, surgical operations or dental treatment?
Has there been contact or residence in a healthcare facility (including long-term care facility)?
Ask about a history of immunosuppression, e.g. HIV infection, chemotherapy, steroid therapy, transplantation, diabetes mellitus. Ask about indwelling catheters, e.g. urethral, intravenous (IV) or implants, e.g. pacemakers, joint replacements.
Drug history
Find out about all prescribed and non-prescribed medications, e.g. herbal remedies taken and ask specifically about immunosuppressants (including oral steroids), antibiotics, antipyretics. Have any ‘recreational’ drugs been taken; if so, have they ever been injected?
Note any history of adverse reactions, allergies or hypersensitivity to any drugs, particularly antibiotics.
Family and social history
Has the patient had contact with anyone with a similar illness? Find out about exposure to animals, birds or pets and if so, is the animal unwell? Note the patient’s occupation and hobbies. Are there clusters of similar symptoms or infections among family, friends or workmates?
Travel history
Has there been recent (in the past year) travel abroad? If so, take a detailed travel history including:
• travel destinations: dates, duration, mode of travel, stop-overs (Box 2.18)
• environment abroad: accommodation, altitude, climate, activities
• lifestyle: including diet, e.g. raw or unpasteurised products, sexual contact (who, when, how many partners), water sports, healthcare, piercings, tattoos
• medical history: including vaccination status, pre-existing conditions, antimalarial measures, particularly type, duration and compliance (Boxes 17.5 and 17.6).
 17.5 Common causes of fever in travellers
17.5 Common causes of fever in travellers
| Developing countries | Worldwide |
| Malaria | Influenza |
| Schistosomiasis | Pneumonia |
| Dengue | Upper respiratory tract infection |
| Typhoid | Urinary infection |
| Tick typhus | Traveller’s diarrhoea |
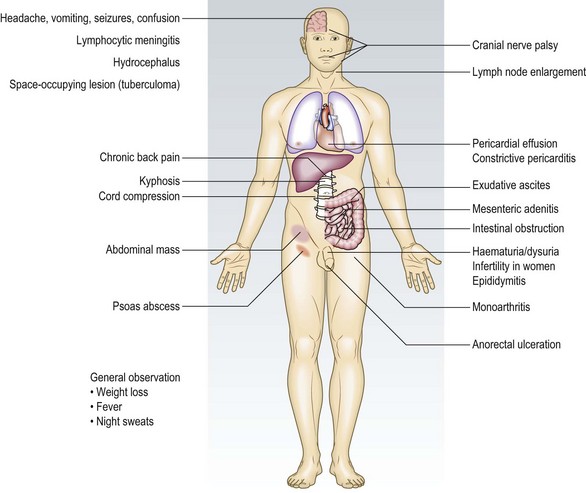
| Tuberculosis | |
| Dysentery | |
| Hepatitis A | |
| Amoebiasis |
17.6 Specific exposures and causes of fever in the tropics
| Exposure | Infection or disease |
| Mosquito bite | Malaria, dengue fever, chikungunya, filariasis, tularaemia |
| Tsetse fly bite | African trypanosomiasis |
| Tick bite | Rickettsial infections, including typhus, Lyme disease, tularaemia, Crimean–Congo haemorrhagic fever, Kyasanur forest disease, babesiosis, tick-borne encephalitis |
| Louse bite | Typhus |
| Flea bite | Plague |
| Sandfly bite | Leishmaniasis, arbovirus infection |
| Reduviid bug | Chagas’ disease |
| Animal contact | Q fever, brucellosis, anthrax, plague, tularaemia, viral haemorrhagic fevers, rabies |
| Fresh-water swimming | Schistosomiasis, leptospirosis, Naegleria fowleri |
| Exposure to soil | Inhalation: dimorphic fungi Inhalation or inoculation: Burkholderia pseudomallei Inoculation (most often when barefoot): hookworms, Strongyloides stercoralis |
| Raw or undercooked fruit and vegetables | Enteric bacterial infections, hepatitis A or E virus, Fasciola hepatica, Toxocara spp., Echinococcus granulosus (hydatid disease), Entamoeba histolytica |
| Undercooked pork | Taenia solium (cysticercosis) |
| Crustaceans or molluscs | Paragonimiasis, gnathostomiasis, Angiostrongylus cantonensis infection, hepatitis A virus, cholera |
| Unpasteurised dairy products | Brucellosis, salmonellosis, abdominal tuberculosis, listeriosis |
| Untreated water | Enteric bacterial infections, giardiasis, Cryptosporidium spp. (chronic in immunocompromised), hepatitis A or E virus |
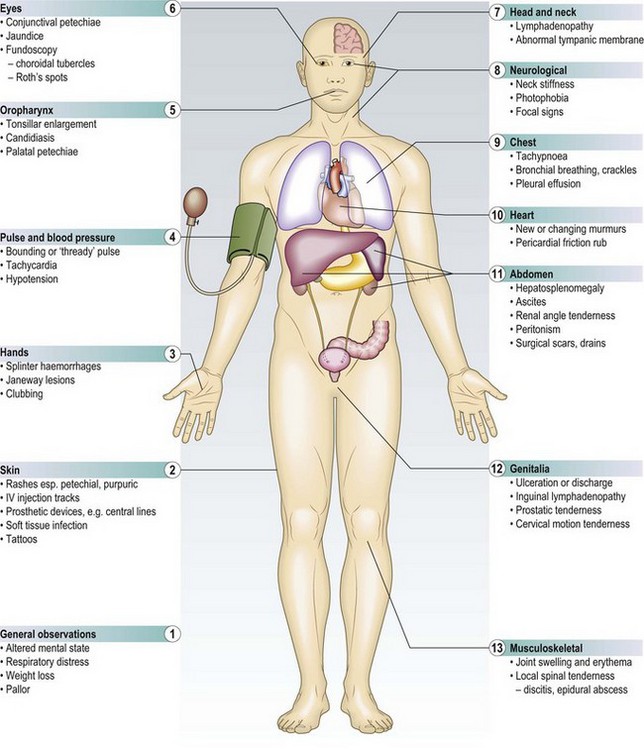
The physical examination
Examination sequence
 Record the temperature and the site of measurement (p. 61). Fever may be intermittent or be suppressed or modified by antipyretic or antimicrobial drugs. With one exception (Box 17.7), fever ‘patterns’, e.g. sustained, intermittent, relapsing, are of little diagnostic value.
Record the temperature and the site of measurement (p. 61). Fever may be intermittent or be suppressed or modified by antipyretic or antimicrobial drugs. With one exception (Box 17.7), fever ‘patterns’, e.g. sustained, intermittent, relapsing, are of little diagnostic value.
17.7
Typhoid
In tropical countries, a ‘stepladder’ pattern of remittent fever is highly specific for typhoid.
Haq SA, Alam MN, Hossain SM et al. Value of clinical features in the diagnosis of enteric fever. Bangladesh Med Res Council Bull 1997;23:42–46.
Look for ‘red flag’ features indicating serious infection (Box 17.8).
 17.8 ‘Red flag’ features
17.8 ‘Red flag’ features
• Petechial/purpuric skin rash
• Hypotension – systolic blood pressure <90 mmHg
• Tachycardia – heart rate >90 bpm –with narrowed pulse pressure and ‘thready’ pulse
• Tachypnoea – respiratory rate >20 breaths/min
• Recent travel to or recent arrival from malaria or tuberculosis endemic area
• Recent use of immunosuppressant drugs
• Significant active comorbidities (cancer, HIV, organ transplantation)
Assess the general appearance: look for any weakness, lethargy, cachexia, distress or altered conscious state (use the Abbreviated Mental Test and the Mini-Mental State Examination: p. 26).
Inspect the entire body for rashes, particularly petechial or haemorrhagic (Fig. 17.2). If a rash is present, characterise the lesions (Box 17.9) and note any change in morphology, e.g. papules to vesicles or petechiae, and whether the rashes are coalescing or denuding.
17.9 Some infections associated with rash and fever
| Macular/maculopapular | Vesicular |
| Measles | Chickenpox (varicella virus) |
| Rubella | Shingles (zoster virus) |
| Enterovirus | Herpes simplex virus |
| Human herpes virus 6 | Herpangina (Coxsackie virus) |
| Epstein–Barr virus | Hand, foot and mouth disease (Coxsackie virus) |
| Cytomegalovirus | Erythematous |
| Human parvovirus B19 | Scarlet fever |
| HIV | Toxic shock syndrome |
| Typhoid | Lyme disease (erythema chronica migrans) |
| Dengue | Human parvovirus B19 |
| Secondary syphilis | Petechial/haemorrhage |
| Rickettsial spotted fevers | Meningococcal septicaemia |
| Urticarial (worm infestations) | Septicaemia with disseminated intravascular coagulation |
| Toxocara | Rickettsiae |
| Schistosomiasis | Yellow fever |
| Strongyloides | Ebola and Marburg virus |
| Cutaneous larva migrans | Lassa fever |
| Other | Dengue |
| Primary syphilis (chancre) | Rift valley fever |
| Tick typhus (eschar) |

Fig. 17.2 Examples of serious infections.
(A) Meningococcal rash. (B) Necrotising fasciitis with fasciotomy. (C) Anthrax eschar.
Look for areas of erythema, swelling or blistering, suggesting skin or soft-tissue infection (Fig. 17.2).
Examine the neck, axillae, epitrochlear and groin areas for lymphadenopathy and feel for the spleen (p. 185).
In hospitalised patients, look for evidence of inflammation at the site of IV lines or devices (Fig. 17.2) or urinary catheters.
Carefully inspect recent surgical wound sites for signs of infection.
Look at hands and feet for splinter haemorrhages (Fig. 4.15A) and Janeway lesions (non-tender haemorrhagic macules on the palms or soles) (Fig. 6.8B).
Systemic examination
Examination sequence
If a febrile patient looks unwell, rapidly assess the mental state, pulse rate, respiratory rate, blood pressure and pulse oximetry (SpO2). If the history and general examination suggest severe sepsis or septic shock, begin resuscitation immediately (Ch. 19).
Most patients with bacterial infection have localising symptoms or signs, e.g. tender swelling of an abscess or murmurs of bacterial endocarditis, but it is essential to examine the patient from head to toe because clues may be in any system.
Look at the tympanic membranes with an otoscope for middle-ear infection.
Percuss the frontal and maxillary sinuses for tenderness (sinusitis).
Palpate the temporal arteries for tenderness (giant cell arteritis).
Examine the nose for congestion and discharge (clear or purulent).
Look in the mouth at the oropharynx and gums for inflammation (Fig. 13.21), oral candidiasis (Fig. 13.25A), immunodeficiency, e.g. HIV, or recent broad-spectrum antibiotic use.
Examine the sclerae for conjunctivitis or jaundice.
Use an ophthalmoscope to examine the retinae for Roth’s spots (endocarditis) (Fig. 6.6).
Gently flex the neck to detect discomfort, stiffness, or both, indicating meningism.
Palpate for neck lymphadenopathy (Fig. 17.3).
Percuss and auscultate the lungs for crackles, signs of consolidation (pneumonia) or effusion (empyema).
Listen to the heart for murmurs (endocarditis).
Examine the abdomen for enlargement and tenderness of the liver and spleen.
Percuss the flanks for renal tenderness (pyelonephritis).
In women, pelvic examination (p. 224) may reveal cervical motion or adnexal tenderness; in men, look for urethral discharge or local genital tenderness (p. 237).
Perform a rectal examination (p. 189) looking for tenderness and swelling, suggesting perirectal abscess (which may be occult in immunocompromised patients) and prostatic enlargement or tenderness (urinary or prostate infection).
Examine the major joints for swelling, erythema and tenderness (joint infection or rheumatologic disorder).
Specific situations
Injecting drug users: Injecting drug users are at particular risk of serious bacterial infection as well as viral diseases, e.g. HIV, hepatitis B and C. The commonest infections are of skin and soft tissue with bacteraemia leading to endocarditis (especially involving the tricuspid valve) and bone and joint infections. In an injecting drug user with fever, examine injection sites for discharge or signs of infection, listen to the chest for crackles or pleural rub (septic pulmonary emboli) and auscultate the heart for murmurs (right-sided valve endocarditis),
The immunocompromised patient: Although immunocompromised patients have less fever with infection, it is still the main presenting complaint. Because they are less able to mount an inflammatory response at the site of infection, the usual signs and symptoms may be absent, e.g. pneumonia without purulent sputum, tenderness without visible inflammation in a perirectal abscess.
In a febrile immunocompromised patient:
• symptoms are diminished or atypical
• obtain a detailed history for possible sources of infection
• expect atypical clinical and radiological findings
• expect the infection to be advanced at the time of presentation
• use computed tomography (CT) and magnetic resonance imaging (MR) scanning early for anatomic delineation of infection
• obtain tissue for histopathology and microbiology early for specific microbiologic diagnosis.
Use the examination sequence above, but additionally look for:
• cushingoid features (Fig. 5.18) suggestive of oral corticosteroid use
• malnourished or wasted appearance
• features of chronic alcohol consumption and liver cirrhosis (Fig. 8.11)
• changes related to renal failure and replacement therapy (Fig. 9.5)
• changes associated with diabetes mellitus (Ch. 5)
• subtle signs of infection around indwelling catheters and tubes
• constellations of lesions commonly seen in neutropenic patients, e.g. erythema, rash, erythema nodosum, soft-tissue infection, ulcers, furuncles, herpetic eruptions, paronychia, mucositis, dental or peritonsillar abscesses, perirectal infection
• constellations of lesions commonly seen in HIV infection – carefully examine the skin, mouth, genitalia and perianal area. In a severely immunocompromised patient avoid rectal examination as this may breach the rectal mucosa and cause iatrogenic infection (Boxes 17.10 and 17.11).
17.10 Features suggesting immunocompromise
• Severe infections that progress rapidly, or are associated with many complications
• Infections last longer, or are slower to respond to standard treatment
• Infections caused by a wider variety of microorganisms and/or unusual organisms
• Concurrent or close temporal proximity of infectious, autoimmune and malignant diseases
Healthcare-acquired infection (HAI): HAIs affect up to 10% of all hospital admissions. The close proximity of ill patients, coupled with the concentrated use of antimicrobial drugs and ease of transmission by healthcare workers, has led to multidrug-resistant organisms, e.g. meticillin-resistant Staphylococcus aureus (MRSA), Clostridium difficile. These infections are transmitted by many routes – contact, droplet spread, medication-related, transfusion, needlestick and air-borne. The commonest HAIs relate to indwelling urinary catheters and invasive devices, e.g. IV cannulae, and procedures. In a patient with fever and any invasive device find out how long the cannula, prosthesis or catheter has been present and look for redness or discharge at the entry site (Box 17.12).
17.12 Infections associated with invasive procedures and devices
| Procedure/device | Type of infection |
| Intravascular cannula | Bacteraemia, catheter site infection |
| Bladder catheter | Urinary tract infection, bacteraemia |
| Mechanical ventilation | Pneumonia, sinusitis |
| Stents, prosthesis, devices, grafts | Bacteraemia, subacute or chronic focal infection of device |
| Surgery | Surgical site infections, pneumonia |
| Endoscopy | Bacteraemia, pneumonia, cholangitis, gastroenteritis |
| Blood transfusion | Viral infection, bacteraemia, fungaemia |
Investigations
See Box 17.13.
 17.13 Investigations in the febrile adult
17.13 Investigations in the febrile adult
| Investigations | Indication/comment |
| Bedside | |
| Urinalysis and urine microscopy | Haematuria, white blood cells, bacteria or proteinuria in urinary infection Microscopic haematuria and proteinuria in endocarditis |
| Blood tests | |
| Full blood count* | White cell count >12 × 109/l or <4 × 109/l in septic shock CD4 lymphocyte count to assess HIV infection ↑ Eosinophil count in worm infestation and drug allergy |
| Blood film | Malarial parasites |
| Renal/liver function | Abnormal in bacteraemia with severe sepsis syndrome ↑ Transaminases in acute hepatitis |
| C-reactive protein | ↑ in bacterial infection |
| Serology | Less helpful in the immunocompromised: IgM in acute viral infection: IgG in previous viral infection, bacterial infection, e.g. syphilis; protozoal infection, e.g. amoebiasis, toxoplasmosis; worm infection, e.g. schistosomiasis |
| Culture | |
| Blood* | Bacteraemia, e.g. typhoid, endocarditis. Particularly useful during rigors |
| Sputum | e.g. Pneumococcal pneumonia, tuberculosis |
| Urine* | Urinary infection |
| Stool culture and microscopy + toxin | Culture: diarrhoea, e.g. Campylobacter, Salmonella. Microscopy for ova, cysts and parasites, e.g. giardiasis, amoebiasis. Toxin test: Clostridium difficile |
| Cerebrospinal fluid | Bacterial, viral and fungal meningitis |
| Joint fluid | Septic arthritis |
| Tissue biopsy | e.g. Tuberculosis lymph node |
| Polymerase chain reaction | |
| Cerebrospinal fluid | Viral meningitis, e.g. Herpes simplex Bacterial meningitis for pneumococcus and meningococcus |
| Throat swab | Viral infections, e.g. Influenza |
| Imaging | |
| Chest X-ray* | Pneumonia, tuberculosis. Perform in immunocompromised even if no apparent respiratory features |
| Ultrasound | Localising abscesses, empyema, gallstones |
| CT scan* | Intra-abdominal or intracranial abscesses, lymphadenopathy |
| MR scan* | Intracranial infections, bone and joint infections |
| Positron emission tomography/CT | Localising infections and pyrexia of unknown origin |
| Others | |
| Mantoux skin test and interferon-γ release assay Induced sputum or bronchoscopic lavage |
Latent tuberculosis Useful for Pneumocystis jirovecii pneumonia in HIV or ventilator-associated pneumonia |
*Investigations most often required in immunocompromised patients.