Chapter 1 Assessment and investigation of patients’ problems
INTRODUCTION
The aim of assessment is to define the patient’s problems accurately. It is based on both a subjective and an objective assessment of the patient. Without an accurate assessment, it is impossible to develop an appropriate plan of treatment. Equally, a sound theoretical knowledge is required to develop an appropriate treatment plan for those problems that may be improved by physiotherapy. Once treatment has started, it is important to assess its effectiveness regularly in relation to both the problems and goals.
The system of patient management used in this book is based on the problem-oriented medical system (POMS) first described by Weed in 1968. This system has three components:
The POMR is now widely used as the method of recording the assessment, management and progress of a patient. It is divided into five sections, as shown in Figure 1.1 and summarized below.
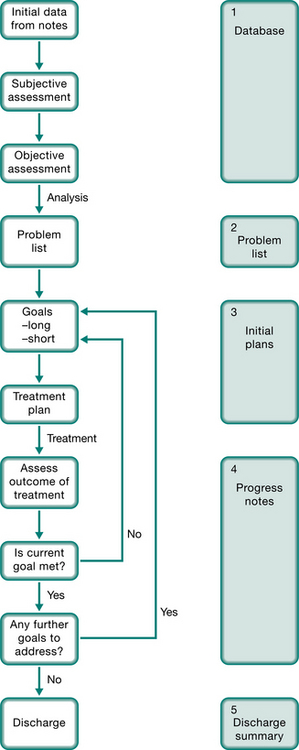
 Database. Here personal details, medical history, relevant social history, results of investigations and tests, together with the physiotherapist’s assessment of the patient are recorded. Problem list. This is a concise list of the patient’s problems, compiled after the assessment is complete. Problems are not always written in order of priority. The list includes problems both amenable to physiotherapy and problems that must be taken into consideration during treatment. The resolution of problems and the appearance of new ones are noted appropriately. Initial plan and goals. A treatment plan is formulated to address the physiotherapy-related problems, with consideration given to the patient’s other problems. Long- and short-term goals are then formulated. Long-term goals are what the patient and the physio-therapist want to achieve finally, and should relate to the problems. Short-term goals are the stages by which the long-term goals should be achieved.
Database. Here personal details, medical history, relevant social history, results of investigations and tests, together with the physiotherapist’s assessment of the patient are recorded. Problem list. This is a concise list of the patient’s problems, compiled after the assessment is complete. Problems are not always written in order of priority. The list includes problems both amenable to physiotherapy and problems that must be taken into consideration during treatment. The resolution of problems and the appearance of new ones are noted appropriately. Initial plan and goals. A treatment plan is formulated to address the physiotherapy-related problems, with consideration given to the patient’s other problems. Long- and short-term goals are then formulated. Long-term goals are what the patient and the physio-therapist want to achieve finally, and should relate to the problems. Short-term goals are the stages by which the long-term goals should be achieved.DATABASE
The database contains a concise summary of the relevant information about the patient taken from the medical notes, together with the subjective and objective assessment made by the physiotherapist. The format may differ from hospital to hospital, but will contain the same information.
The first part contains the patient’s personal details including name, date of birth, address, hospital number, and referring doctor. It may also contain the diagnosis and reason for referral. The second part summarizes the history from the medical notes and the physiotherapy assessment. This is often divided into several sections.
History of presenting condition (HPC) summarizes the patient’s current problems, including relevant information from the medical notes. Previous medical history (PMH) summarizes the entire list of medical and surgical problems that the patient has had in the past. It may be written in disease- specific groupings or as a chronological account. Drug history (DH) is a list of the patient’s current medications (including dosage) taken from the medication charts. Drug allergies should also be noted. Family history (FH) includes a list of any major diseases suffered by members of the immediate family. Social history (SH) provides a picture of the patient’s social situation. It is important to specifically question the patient about the level of support available at home, and to gain an idea of the patient’s expected contribution to household duties. The layout of the patient’s home should also be ascertained with particular emphasis on stairs. Occupation and hobbies, both past and present, give further information about the patient’s lifestyle. Finally, history of smoking and alcohol use should be noted. Patient examination includes all information collected in the physiotherapist’s subjective and objective assessment of the patient. Test results contain any significant findings as they become available. These may include arterial blood gases, spirometry, blood tests, sputum analysis, chest radiographs, computed tomography (CT) and any other relevant tests (e.g. hepatitis B positive).Subjective assessment
Subjective assessment is based on an interview with the patient. It should generally start with open-ended questions What is the main problem? What troubles you most? allowing the patient to discuss the problems that are most important to them at that time. Indeed, by asking such questions, previously unmentioned problems may surface. As the interview progresses, questioning may become more focused on those important features that need clarification. There are five main symptoms of respiratory disease:
With each of these symptoms, enquiries should be made concerning:
duration – both the absolute time since first recognition of the symptom (months, years) and the duration of the present symptoms (days, weeks)Breathlessness
Breathlessness is the subjective awareness of an increased work of breathing. It is the predominant symptom of both cardiac and respiratory disease. It also occurs in anaemia where the oxygen-carrying capacity of the blood is reduced, in neuromuscular disorders where the respiratory muscles are affected, and in metabolic disorders where there is a change in the acid–base equilibrium (Chapter 3) or metabolic rate (e.g. hyperthyroid disorders). Breathlessness is also found in hyperventilation syndrome or dysfunctional breathing where psychological factors (e.g. anxiety) may be contributory factors.
The pathophysiological mechanisms causing breathlessness are still the subject of intensive investigation. Many factors are involved, including respiratory muscle length–tension relationships, respiratory muscle fatigue, stimulation of pulmonary stretch receptors, and alterations in central respiratory drive.
The duration and severity of breathlessness is most easily assessed through enquiries about the level of functioning in the recent and distant past. For example, a patient may say that 3 years ago he could walk up five flights of stairs without stopping, but now cannot manage even one flight. Some patients may deny breathlessness as they have (unconsciously) decreased their activity levels so that they do not get breathless. They may acknowledge breathlessness only when it interferes with important activities, e.g. bathing. The physio-therapist should always relate breathlessness to the level of function that the patient can achieve.
Comparison of the severity of breathlessness between patients is difficult because of differences in perception and expectations. To overcome these difficulties, numerous gradings have been proposed. The New York Heart Association classification of breathlessness, shown in Box 1.1, was developed for patients with cardiac disease, but is also applicable to respiratory patients. The Borg Rating of Perceived Exertion Scale (Borg 1982) is another scale that is frequently used for both respiratory and cardiac patients. No scale is universal and it is important that all staff within one institution use the same scale.
Box 1.1 The New York Heart Association classification of breathlessness
Breathlessness is usually worse during exercise and better with rest. An exception is hyperventilation syndrome where breathlessness may improve with exercise. Two patterns of breathlessness have been given specific names:
In the cardiac patient, lying flat increases venous return from the legs so that blood pools in the lungs, causing breathlessness. A similar pattern may be described in patients with severe asthma, but here the breathlessness is caused by nocturnal bronchoconstriction.
Further insight into a patient’s breathlessness may be gained by enquiring about precipitating and relieving factors. Breathlessness associated with exposure to allergens and relieved by bronchodilators is typically found in asthma.
Cough
Coughing is a protective reflex that rids the airways of secretions or foreign bodies. Any stimulation of receptors located in the pharynx, larynx, trachea or bronchi may induce cough. Cough is a difficult symptom to clarify as most people cough normally every day, yet a repetitive persistent cough is both troublesome and distressing. Smokers may discount their early morning cough as being ‘normal’ when in fact it signifies chronic bronchitis.
Important features concerning cough are its effectiveness, and whether it is productive or dry. The severity of cough may range from an occasional disturbance to continual trouble. A loud, barking cough, which is often termed ‘bovine’, may signify laryngeal or tracheal disease. Recurrent coughing after eating or drinking is an important symptom of aspiration. A chronic productive cough every day is a fundamental feature of chronic bronchitis and bronchiectasis. Interstitial lung disease is characterized by a persistent, dry cough. Nocturnal cough is an important symptom of asthma in children and young adults, but in older patients it is more commonly due to cardiac failure. Drugs, especially beta-blockers and some other antihypertensive agents, can cause a chronic cough. Chronic cough may cause fractured ribs (cough fractures) and hernias. Stress incontinence is a common complication of chronic cough, especially in women. As this subject is often embarrassing to the patient, specific questioning may be required (see below).
Postoperatively, the strength and effectiveness of cough is important for the physiotherapist to assess.
Sputum
In a normal adult, up to 100 ml of tracheobronchial secretions are produced daily and cleared subconsciously by swallowing. Sputum is the excess tracheobronchial secretions that are cleared from the airways by coughing or huffing. It may contain mucus, cellular debris, microorganisms, blood and foreign particles. Questioning should determine the colour, consistency and quantity of sputum produced each day. This may clarify the diagnosis and the severity of disease (Table 1.1).
| Description | Causes | |
|---|---|---|
| Saliva | Clear watery fluid | |
| Mucoid | Opalescent or white | Chronic bronchitis without infection, asthma |
| Mucopurulent | Slightly discoloured, but not frank pus | Bronchiectasis, cystic fibrosis, pneumonia |
| Purulent | Thick, viscous: | |
| Frothy | Pink or white | Pulmonary oedema |
| Haemoptysis | Ranging from blood specks to frank blood, old blood (dark brown) | Infection (tuberculosis, bronchiectasis), infarction, carcinoma, vasculitis, trauma, also coagulation disorders, cardiac disease |
| Black | Black specks in mucoid secretions | Smoke inhalation (fires, tobacco, heroin), coal dust |
A number of grading systems for mucoid, mucopurulent, purulent sputum have been proposed. For example, Miller (1963) suggested:
| M1 | mucoid with no suspicion of pus |
| M2 | predominantly mucoid, suspicion of pus |
| P1 | 1/3 purulent, 2/3 mucoid |
| P2 | 2/3 purulent, 1/3 mucoid |
| P3 | >2/3 purulent. |
However, in clinical practice sputum is often classified as mucoid, mucopurulent or purulent, together with an estimation of the volume (1 teaspoon, 1 egg cup, half a cup, 1 cup). Odour emanating from sputum signifies infection. In general, particularly offensive odours suggest infection with anaerobic organisms (e.g. aspiration pneumonia, lung abscess).
In patients with allergic bronchopulmonary aspergillosis (ABPA), asthma and occasionally bronchiectasis, sputum ‘casts’ may be expectorated. Classically these take the shape of the bronchial tree.
Haemoptysis is the presence of blood in the sputum. It may range from slight streaking of the sputum to frank blood. Frank haemoptysis can be life threatening, requiring bronchial artery embolization or surgery. Isolated haemoptysis may be the first sign of bronchogenic carcinoma, even when the chest radiograph is normal. Patients with chronic infective lung disease often suffer from recurrent haemoptyses.
Wheeze
Wheeze is a whistling or musical sound produced by turbulent airflow through narrowed airways. These sounds are generally noted by patients when audible at the mouth. Stridor, the sound of an upper airway obstruction, is often mistakenly called ‘wheeze’ by patients. Heart failure may also cause wheezing in those patients with significant mucosal oedema. Wheezing is discussed in more detail later in this chapter.
Chest pain
Chest pain in respiratory patients usually originates from musculoskeletal, pleural or tracheal inflammation, as the lung parenchyma and small airways contain no pain fibres.
Pleuritic chest pain is caused by inflammation of the parietal pleura, and is usually described as a severe, sharp, stabbing pain that is worse on inspiration. It is not reproduced by palpation.
Tracheitis generally causes a constant burning pain in the centre of the chest, aggravated by breathing.
Musculoskeletal (chest wall) pain may originate from the muscles, bones, joints or nerves of the thoracic cage. It is usually well localized and exacerbated by chest and/or arm movement. Palpation will usually reproduce the pain.
Angina pectoris is a major symptom of cardiac disease. Myocardial ischaemia characteristically causes a dull central retrosternal gripping or band-like sensation, which may radiate to either arm, neck or jaw.
Pericarditis may cause pain similar to angina or pleurisy.
A differential diagnosis of chest pain is given in Table 1.2.
Table 1.2 Syndromes of chest pain
| Condition | Description | Causes |
|---|---|---|
| Pulmonary | ||
| Pleurisy | Sharp, stabbing, rapid onset, limits inspiration, well localized, often ‘catches’ at a certain lung volume, not tender on palpation | Pleural infection or inflammation of the pleura, trauma (haemothorax), malignancy |
| Pulmonary embolus | Usually has pleuritic pain, with or without severe central pain | Pulmonary infarction |
| Pneumothorax | Severe central chest discomfort, with or without pleuritic component, severity depends on extent of mediastinal shift | Trauma, spontaneous, lung diseases (e.g. cystic fibrosis, AIDS) |
| Tumours | May mimic any form of chest pain, depending on site and structures involved | Primary or secondary carcinoma, mesothelioma |
| Musculoskeletal | ||
| Rib fracture | Localized point tenderness, often sudden onset, increases with inspiration | Trauma, tumour, cough fractures (e.g. in chronic lung diseases, osteoporosis) |
| Muscular | Superficial, increases on inspiration and some body movements, with or without palpable muscle spasm | Trauma, unaccustomed exercise (excessive coughing during exacerbations of lung disease), accessory muscles may be affected |
| Costochondritis (Tietze’s syndrome) | Localized to one or more costochondral joints, with or without generalized, non-specific chest pain | Viral infection |
| Neuralgia | Pain or paraesthesia in a dermatomal distribution | Thoracic spine dysfunction, tumour, trauma, herpes zoster (shingles) |
| Cardiac | ||
| Ischaemic heart disease (angina or infarct) | Dull, central, retrosternal discomfort like a weight or band with or without radiation to the jaw and/or either arm, may be associated with palpitations, nausea or vomiting | Myocardial ischaemia, onset at rest is more suggestive of infarction |
| Pericarditis | Often retrosternal, exacerbated by respiration, may mimic cardiac ischaemia or pleurisy, often relieved by sitting | Infection, inflammation, trauma, tumour |
| Mediastinum | ||
| Dissecting aortic aneurysm | Sudden onset, severe, poorly localized central chest pain | Trauma, atherosclerosis, Marfan’s syndrome |
| Oesophageal | Retrosternal burning discomfort, but can mimic all other pains, worse lying flat or bending forward | Oesophageal reflux, trauma, tumour |
| Mediastinal shift | Severe, poorly localized central discomfort | Pneumothorax, rapid drainage of a large pleural effusion |
Incontinence
Incontinence is a problem that is often aggravated by chronic cough (Orr et al 2001, Scottish Intercollegiate Guidelines Network 2004, Thakar & Stanton 2000). Coughing and huffing increase intra-abdominal pressure, which may precipitate urine leakage. Fear of this may influence compliance with physiotherapy. Thus, identification and treatment of incontinence is important. Questions may need to be specific to elicit this symptom: ‘When you cough, do you find that you leak some urine? ‘Does this interfere with your physiotherapy?’
Other symptoms
Of the other symptoms a patient may report, a number have particular importance:
Fever (pyrexia) is one of the common features of infection, but low-grade fevers can also occur with malignancy and connective tissue disorders. Equally, infection may occur without fever, especially in immunosuppressed (e.g. chemotherapy) patients or those on corticosteroids. High fevers occurring at night, with associated sweating (night sweats), may be the first indicator of pulmonary tuberculosis.
Headache is an uncommon feature of respiratory disease. Morning headaches in patients with severe respiratory failure may signify nocturnal carbon dioxide retention. Early morning arterial blood gases or nocturnal transcutaneous carbon dioxide monitoring are required for confirmation.
Peripheral oedema in the respiratory patient suggests right heart failure, which may be due to cor pulmonale (right ventricular failure secondary to hypoxic pulmonary vasoconstriction). Peripheral oedema may also occur in patients taking high-dose corticosteroids, as a result of salt and water retention.
Functional ability
It is important to assess the patient as a whole, enquiring about their daily activities. If the patient is employed, what does the job actually entail? For example, a surveyor may sit behind a desk all day, or may be climbing 25-storey buildings. The home situation should also be documented, in particular the number of stairs to the front door and within the house. With whom does the patient live? What roles does the patient perform in the home (shopping, housework, cooking)? Finally, questions concerning activities and recreation often reveal areas where significant improvements in quality of life can be made.
Quality of life
Assessment of quality of life (QOL) is becoming increasingly important to assess the impact of disability on the patient and as a measure of response to treatment. QOL scales measure the effect of an illness and its management upon a patient as perceived by the patient. Often there is little correlation between physiological measures (e.g. lung function) and QOL. A number of both generic, for example SF-36 (Ware & Sherbourne 1992) and disease-specific QOL scales are available which allow data to be gathered principally by self-report questionnaires or interview. QOL scales available for assessment of patients with respiratory or cardiovascular disease are reviewed elsewhere (Juniper et al 1999, Kinney et al 1996, Mahler 2000, Pashkow et al 1995). The choice of a QOL measure requires an evaluation of QOL scales with respect to their reliability, validity, responsiveness and appropriateness (Aaronson 1989).
Objective assessment
Objective assessment is based on examination of the patient, together with the use of tests such as spirometry, arterial blood gases and chest radiographs. Although a full examination of the patient should be available from the medical notes, it is worthwhile to make a thorough examination at all times, as the patient’s condition may have changed since the last examination, and the physiotherapist may need greater detail of certain aspects than is available from the notes. A good examination will provide an objective baseline for future measurement of the patient’s progress. By developing a standard method of examination, the findings are quickly assimilated and the physiotherapist remains confident that nothing has been omitted. This chapter refers mainly to assessment of the adult patient, although much of the information is also relevant to the paediatric population. Specific details for the assessment of infants and children and normal values can be found in the relevant paediatric sections (Chapters 9 & 10).
General observation
Examination starts by observing the patient from the end of the bed. Is the patient short of breath, sitting on the edge of the bed, distressed? Is he obviously cyanosed? Is he on supplemental oxygen? If so, how much? What is the speech pattern – long fluent paragraphs without discernible pauses for breath, quick sentences, just a few words, or are they too breathless to speak? When he moves around or undresses, does he become distressed? With a little practice, these observations should become second nature and can be noted while introducing yourself to the patient.
In the intensive care patient there are a number of further features to be observed. The level of ventilatory support must be ascertained. This includes both the mode of ventilation (e.g. supplemental oxygen, continuous positive airway pressure, intermittent positive pressure ventilation) and the route of ventilation (mask, endotracheal tube, tracheostomy). The level of cardiovascular support should also be noted, including drugs to control blood pressure and cardiac output, pacemakers and other mechanical devices. The patient’s level of consciousness should also be noted. Any patient with a decreased level of consciousness is at risk of aspiration and retention of pulmonary secretions. In those patients who are not pharmacologically sedated, the level of consciousness is often measured using the Glasgow Coma Scale (Box 1.2). This gives the patient a score (from 3 to 15) based on his best motor, verbal and eye responses.
Box 1.2 The Glasgow Coma Scale
| Eye opening | Spontaneous | 4 |
| To speech | 3 | |
| To pain | 2 | |
| None | 1 | |
| Best verbal response | Oriented | 5 |
| Confused speech | 4 | |
| Inappropriate words | 3 | |
| Incomprehensible sounds | 2 | |
| None | 1 | |
| Best motor response | Obeys commands | 6 |
| Localizes to pain | 5 | |
| Withdraws (generalized) | 4 | |
| Flexion | 3 | |
| Extension | 2 | |
| No response | 1 | |
| Maximum total score is 15; minimum total score is 3 (Teasdale and Jennett 1974) | ||
The patient’s chart should then be examined for recordings of temperature, pulse, blood pressure and respiratory rate. These measurements are usually performed by the nursing staff immediately on admission of the patient and regularly thereafter.
Body temperature.
Body temperature can be measured in a number of ways. Oral temperatures are the most convenient method in adults, but should not be performed for at least 15 minutes after smoking or consuming hot or cold food or drink. Aural, axillary and rectal temperature may also be measured.
Body temperature is maintained within the range 36.5–37.5°C. It is lowest in the early morning and highest in the afternoon.
Fever (pyrexia) is the elevation of the body temperature above 37.5°C, and is associated with an increased metabolic rate. For every 1°C rise in body temperature, there is an approximately 10% increase in oxygen consumption and carbon dioxide production (Manthous et al 1995). This places extra demand on the cardiorespiratory system, which causes a compensatory increase in heart rate and respiratory rate.
Heart rate.
Heart rate is most accurately measured by auscultation at the cardiac apex. The pulse rate is measured by palpating a peripheral artery (radial, femoral or carotid). In most situations, the heart rate and pulse rate are identical; a difference between the two is called the ‘pulse deficit’. This indicates that some heartbeats have not caused sufficient blood flow to reach the periphery and is commonly found in atrial fibrillation and some other arrhythmias. The normal adult heart rate is 60–100 beats per minute.
Tachycardia is defined as a heart rate greater than 100 beats/min at rest in adults. It is found with anxiety, exercise, fever, anaemia and hypoxia. It is also common in patients with cardiac disorders. Medications such as bronchodilators and some cardiac drugs may also increase heart rate.
Bradycardia is defined as a heart rate less than 60 beats/min. It may be a normal finding in athletes and may also be caused by some cardiac drugs (especially beta-blockers).
Blood pressure (BP).
With every contraction of the heart (systole) the arterial pressure increases, with the peak called the ‘systolic’ pressure. During the relaxation phase of the heart (diastole), the arterial pressure drops, with the minimum called the ‘diastolic’ pressure. Blood pressure is usually measured non-invasively by placing a sphygmomanometer cuff around the upper arm, and listening over the brachial artery with a stethoscope. The cuff width should be approximately one-half to two-thirds of the length of the upper arm, otherwise readings may be inaccurate. Cuff inflation to above systolic pressure collapses the artery, blocking flow. With release of the air, the cuff pressure gradually falls to a point just below systolic. At this point, the peak pressure within the artery is greater than the pressure outside the artery, so flow recommences. This turbulent flow is audible through the stethoscope. As the cuff is further deflated the noise continues. When the cuff pressure drops to just below diastolic, the pressure within the artery is greater than that of the cuff throughout the cardiac cycle, so turbulence abates and the noise ceases. The gauge to measure BP was previously a column of mercury, but with the increasing awareness of the risks of mercury, many devices now use pressure gauges or totally digital systems. Blood pressure is recorded as systolic/ diastolic pressure. Normal adult blood pressure is between 95/60 and 140/90 mmHg.
Hypertension is defined as a blood pressure greater than 145/95 mmHg, usually due to changes in vascular tone and/or aortic valve disease.
Hypotension is defined as a blood pressure less than 90/60 mmHg. It is often a normal finding during sleep. Daytime hypotension may be due to heart failure, blood loss or decreased vascular tone.
Postural hypotension is a drop in blood pressure of more than 5 mmHg between lying and sitting or standing, and may be due to decreased circulating blood volume, or loss of vascular tone.
Pulsus paradoxus is the exaggeration of the drop in blood pressure that occurs with inspiration. Normally, during inspiration the negative intrathoracic pressure reduces venous return and drops cardiac output slightly. Exaggeration of this normal response where blood pressure drops by more than 10 mmHg is seen in situations where the intrathoracic pressure swings are greater, as occurs in severe airway obstruction.
Respiratory rate.
Respiratory rate should be measured with the patient seated comfortably. The normal adult respiratory rate is approximately 12–16 breaths/min.
Tachypnoea is defined as a respiratory rate greater than 20 breaths/min, and can be seen in any form of lung disease. It may also occur with metabolic acidosis and anxiety.
Bradypnoea is defined as a respiratory rate of less than 10 breaths/min. It is an uncommon finding, and is usually due to central nervous system depression by narcotics or trauma.
Body weight.
Weight is often recorded on the observation chart. Respiratory function can be compromised by both obesity and severe malnourishment. As ideal body weight has a large normal range, the body mass index (BMI) is a more valid measurement and is often expressed as a standard deviation score. This is calculated by dividing the weight in kilograms by the square of the height in metres (kg/m2); the normal range is 20–25 kg/m2. Patients with values below 20 are underweight, those with values of 25–30 are overweight, and those with values over 30 are classified as obese.
Malnourished patients often exhibit depression of their immune system with increased risk of infection. They also have weaker respiratory muscles, which are more likely to fatigue. Obesity causes an increase in residual volume (RV) and a decrease in functional residual capacity (FRC) (Rubinstein et al 1990). Thus tidal breathing occurs close to closing volumes. This is particularly important postoperatively, where the obese are more prone to subsegmental lung collapse.
An accurate daily weight gives a good estimate of fluid volume changes, as any change in weight of more than 250 g/day is usually due to fluid accumulation or loss. Daily weights are commonly used in intensive care, renal and cardiac patients to assess fluid balance.
Other measures.
In the intensive care patient there is a plethora of monitoring that can be performed. As well as the parameters listed above, measures of central venous pressure (CVP), pulmonary artery pressure (PAP) and intracranial pressure (ICP) will need to be reviewed as part of the physiotherapy assessment. Many intensive care units now record this information on bedside computer terminals. Further details of intensive care monitoring can be found in Chapters 8 & 9.
Apparatus.
The presence of lines and tubes should be noted. Venous lines provide constant direct access to the bloodstream, and vary widely in site, complexity and function. The simplest cannula in a small peripheral vein, usually in the forearm, is called a ‘drip’. It is used for the administration of intravenous (IV) fluids and most IV drugs. At the other end of the spectrum are the multilumen lines placed in the subclavian, internal jugular or femoral veins, ending in the venae cavae close to the heart. These central lines allow simultaneous administration of multiple drugs and can be used for central venous pressure monitoring. Central lines can be potentially dangerous, as disconnection of the line can quickly suck air into the central veins, causing an air embolus, which may be fatal.
Some patients, especially those in intensive care, may have an arterial line for continuous recording of blood pressure and for repeated sampling of arterial blood. These lines are usually inserted in the radial or brachial artery. If accidentally disconnected, rapid blood loss will occur.
After cardiac surgery, most patients have cardiac pacing wires that exit through the skin overlying the heart. In most cases these wires are not required and are removed routinely before discharge. In the event of clinically significant cardiac arrhythmias, these wires are connected to a pacing box that electrically stimulates the heart. In medical patients, pacemaker wires are introduced through one of the central veins and rest in the apex of the right ventricle. Care must be taken with all pacing wires as dislodgement may be life threatening.
Postoperatively, drains may be placed at any operation site (e.g. abdomen) to prevent the collection of fluid or blood. These are generally connected to sterile bags. Nasogastric tubes are placed for two reasons: soft, fine-bore tubes are used to facilitate feeding, while firm, wider-bore tubes allow aspiration of gastric contents.
Intercostal drains are placed between two ribs into the pleural space to remove air, fluid or pus which has accumulated. They are also used routinely after cardiothoracic surgery. In general, the tube is attached to a bottle partially filled with sterile water, called an ‘underwater seal drain’ (Chapter 11). The bottle should be positioned at least 0.5 metres below the patient’s chest (usually on the floor). Bubbling indicates that air is entering the tube from the pleural space at that time. Frequent observations must be made of the fluid level within the tube, which should oscillate or ‘swing’ with every breath. If the fluid does not swing, the tube is not patent and requires medical attention. In certain situations the bottle may be connected to continuous suction, which will dampen the fluid ‘swing’. Those patients who are producing large volumes of fluid or pus may be connected to a double bottle system, where the first bottle acts as a reservoir to collect the fluid and the second provides the underwater seal. Fully enclosed disposable plastic systems are now available. Any patient with a chest drain should have a pair of large forceps available at all times to clamp the tube if any connection becomes loosened.
The hands.
Significant findings can be identified by observing and examining the hands. A fine tremor will often be seen in association with high-dose bronchodilators. Warm and sweaty hands with an irregular flapping tremor may be due to acute carbon dioxide retention. Weakness and wasting of the small muscles in the hands may be an early sign of an upper lobe tumour involving the brachial plexus (Pancoast’s tumour). Examination of the fingers may show nicotine staining from smoking.
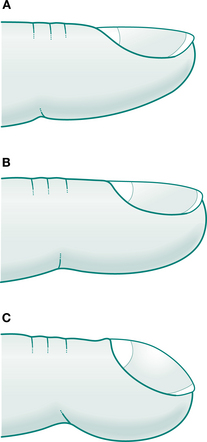
Clubbing is the term used to describe the changes in the fingers and toes as shown in Figure 1.2. The first sign of clubbing is the loss of the angle between the nail bed and the nail itself. Later, the finger pad becomes enlarged. The nail bed may also become ‘spongy’, but this is a difficult sign to elicit. A summary of the diseases associated with clubbing is given in Box 1.3. The exact cause of clubbing is unknown. It is interesting to note that clubbing in cystic fibrosis patients disappears after heart and lung or lung transplant.
The eyes.
The eyes should be examined for pallor (anaemia), plethora (high haemoglobin) or jaundice (yellow colour due to liver or blood disturbances). Drooping of one eyelid with enlargement of that pupil suggests Horner’s syndrome where there is a disturbance in the sympathetic nerve supply to that side of the head (sometimes seen in cancer of the lung).
Cyanosis.
This is a bluish discolouration of the skin and mucous membranes. Central cyanosis, seen on examination of the tongue and mouth, is caused by hypoxaemia where there is an increase in the amount of haemoglobin not bound to oxygen. The degree of blueness is related to the quantity of unbound haemoglobin. Thus a greater degree of hypoxia is necessary to produce cyanosis in an anaemic patient (low haemoglobin), while a patient with polycythaemia (increased haemoglobin) may appear cyanosed with only a small drop in oxygen levels. Peripheral cyanosis, affecting the toes, fingers and earlobes, may also be due to poor peripheral circulation, especially in cold weather.
Jugular venous pressure.
On the side of the neck the jugular venous pressure (JVP) is seen as a flickering impulse in the jugular vein. It is normally seen at the base of the neck when the patient is lying back at 45°. The JVP is usually measured in relation to the sternal angle as this point is relatively fixed in relation to the right atrium. A normal JVP at the base of the neck corresponds to a vertical height approximately 3–4 cm above the sternal angle. The JVP is generally expressed as the vertical height (in centimetres) above normal. The JVP provides a quick assessment of the volume of blood in the great vessels entering the heart. Most commonly it is elevated in right heart failure. This may occur in patients with chronic lung disease complicated by cor pulmonale. In contrast, dehydrated patients may only have a visible JVP when lying flat.
Peripheral oedema.
This is an important sign of cardiac failure, but may also be found in patients with a low albumin level, impaired venous or lymphatic function, or those on high-dose steroids. When mild, it may only affect the ankles; with increasing severity, it may progress up the body. In bedbound patients, it is important to check the sacrum.
Observation of the chest
When examining the chest it is important to remember the surface landmarks of the thoracic contents (Fig. 1.3). Some important points are:
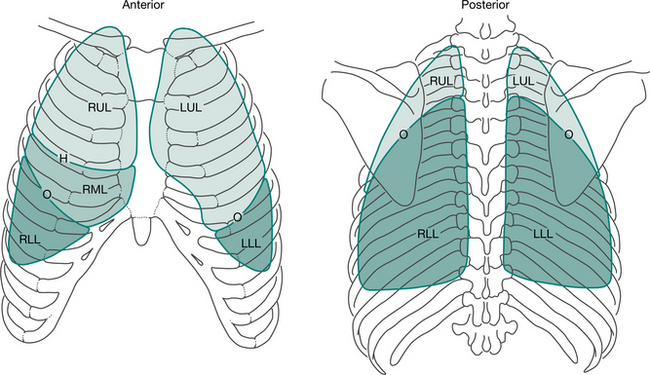
Figure 1.3 Surface markings of the lungs: H, horizontal fissure; O, oblique fissure; RUL, right upper lobe; LUL, left upper lobe; RML, right middle lobe; LLL, left lower lobe; RLL, right lower lobe.
The oblique fissure, dividing the upper and middle lobes from the lower lobes, runs underneath a line drawn from the spinous process of T2 around the chest to the sixth costochondral junction anteriorly. The horizontal fissure on the right, dividing the upper lobe from the middle lobe, runs from the fourth intercostal space at the right sternal edge horizontally to the midaxillary line, where it joins the oblique fissure. The diaphragm sits at approximately the sixth rib anteriorly, the eighth rib in the midaxillary line and the 10th rib posteriorly.Chest shape.
The chest should be symmetrical with the ribs, in adults, descending at approximately 45° from the spine. The transverse diameter should be greater than the anteroposterior (AP) diameter. The thoracic spine should have a slight kyphosis. Important common abnormalities include:
kyphoscoliosis, which comprises both lateral curvature of the spine with vertebral rotation (scoliosis) and an element of kyphosis. This causes a restrictive lung defect which, when severe, may cause respiratory failure pectus excavatum, or ‘funnel’ chest, is where part of the sternum is depressed inwards. This rarely causes significant changes in lung function but may be corrected surgically for cosmetic reasonsBreathing pattern.
Observation of the breathing pattern gives further information concerning the type and severity of respiratory disease.
Normal breathing should be regular with a rate of 12–16 breaths/min, as mentioned previously. Inspiration is active and expiration passive. The approximate ratio of inspiratory to expiratory time (I : E ratio) is 1 : 1.5 to 1 : 2.
Prolonged expiration may be seen in patients with obstructive lung disease, where expiratory airflow is severely limited by dynamic closure of the smaller airways. In severe obstruction the I : E ratio may increase to 1 : 3 or 1 : 4.
Pursed-lip breathing is often seen in patients with severe airways disease. By opposing the lips during expiration the airway pressure inside the chest is maintained, preventing the floppy airways from collapsing. Thus overall airflow is increased.
Tachypnoea refers to an increased respiratory rate, usually defined as >20 breaths/minute.
Bradypnoea, a rarely used term, refers to a respiratory rate of <10 breaths/minute.
Apnoea refers to a total cessation in breathing for >10 seconds.
Hypopnoea refers to shallow breathing (<50% of normal) for >10 seconds, usually recorded during the night as part of a sleep study.
Hypoventilation refers to reduced total ventilation (rate × volume) and usually increases arterial carbon dioxide. It is commonly seen with sedation or opiate analgesia. Severe obesity may also cause hypoventilation.
Hyperventilation refers to increased total ventilation (rate × volume) and usually lowers arterial carbon dioxide. It is commonly seen in anxiety/hyperventilation syndrome (Chapter 17).
Kussmaul’s respiration is rapid, deep breathing with a high minute ventilation. It is usually seen in patients with metabolic acidosis.
Cheyne–Stokes respiration refers to irregular breathing with cycles consisting of a few relatively deep breaths, progressively shallower breaths (sometimes to the point of apnoea), and then slowly increasing depth of breaths. This is usually associated with heart failure, severe neurological disturbances or drugs (e.g. narcotics).
Ataxic breathing consists of haphazard, uncoordinated deep and shallow breaths. This may be found in patients with cerebellar disease.
Apneustic breathing is characterized by prolonged inspiration, and is usually the result of brain damage.
Chest movement.
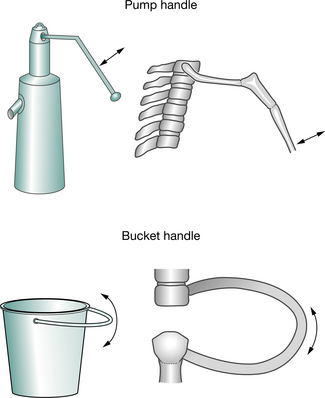
During normal inspiration, there are symmetrical increases in the anteroposterior, transverse and vertical diameters of the chest. The increase in vertical diameter is achieved by contraction of the diaphragm, causing the abdominal contents to descend. Sternal and rib movements are responsible for the increases in anteroposterior and transverse diameters of the chest. These movements can be divided into two components (Fig. 1.4). When elevated, the anterior ends of the ribs move forward and upwards with anterior movement of the sternum. This increase in anteroposterior diameter is likened to the movement of an old fashioned ‘pump handle’. At the same time, rotation of the ribs causes an increase in the transverse diameter, likened to the movement of a ‘bucket handle’.
During normal quiet breathing, the diaphragm is the main inspiratory muscle increasing the vertical diameter. There is also an increase in the lower thoracic transverse diameter due to external intercostal muscle contraction. Expiration is passive, caused by the elastic recoil of the lung and chest wall. When breathing is increased, all the accessory inspiratory muscles (sternomastoid, scalenes, trapezii) contract to increase the anteroposterior and transverse diameters, and the diaphragm activity increases, thus further increasing the vertical dimensions. Expiration may become active with contraction of the abdominal and internal intercostal muscles.
Intercostal indrawing occurs where the skin between the ribs is drawn inwards during inspiration. It may be seen in patients with severe inspiratory airflow resistance. Larger negative pressures during inspiration suck the soft tissues inwards. This is an important sign of respiratory distress in children, but is less often seen in adults.
Palpation of the chest
Trachea.
Firstly, the trachea is palpated to assess its position in relation to the sternal notch. Tracheal deviation indicates underlying mediastinal shift. The trachea may be pulled towards a collapsed or fibrosed upper lobe, or pushed away from a pneumothorax or large pleural effusion.
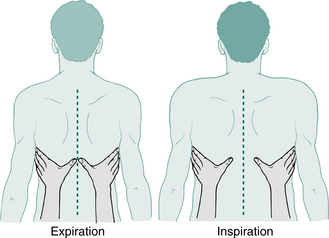
Chest expansion.
This can be assessed by observation, but palpation is more accurate. The patient is instructed to expire slowly to residual volume. At residual volume the examiner’s hands are placed spanning the posterolateral segments of both bases, with the thumbs touching in the midline posteriorly, as shown in Figure 1.5. In obese patients, it helps if the skin of the anterior chest wall is slightly retracted by the fingertips. The patient is then instructed to inspire slowly and the movement of both thumbs is observed. Both sides should move equally, with 3–5 cm being the normal displacement.
A similar technique may be used anteriorly, again to measure basal movements. Measurement of apical movement is more difficult. By placing the hand over the upper chest anteriorly, a qualitative comparison of the two sides can be made. In all cases, diminished movement is abnormal.
Paradoxical breathing is where some or all of the chest wall moves inwards on inspiration and outwards on expiration. It can involve anything from a localized area to the entire chest wall. Localized paradox occurs when the integrity of the chest wall is disrupted. Fractures of multiple ribs with two or more breaks in each rib will result in the central section losing the support usually provided by the rest of the thoracic cage. Thus, during inspiration, this loose segment (often called a ‘flail segment’) is drawn inwards as the rest of the chest wall moves out. In expiration the reverse occurs.
Paradoxical movement of one hemithorax may be remarkably difficult to observe. It may be caused by unilateral diaphragm paralysis. Paradox of the entire chest wall occurs in bilateral diaphragm weakness or paralysis. It is most apparent when the patient is supine.
Paradoxical movement of the lower chest can occur in patients with severe chronic airflow limitation who are extremely hyperinflated. As the dome of the diaphragm cannot descend any further, diaphragm contraction during inspiration pulls the lower ribs inwards. This is called ‘Hoover’s sign’.
Surgical emphysema.
Air in the subcutaneous tissues of the chest, neck or face should also be noted. On palpation there is a characteristic crackling in the skin. This occurs when a pneumomediastinum (air in the mediastinum) has tracked outwards. A chest radiograph must be performed immediately, as a pneumomediastinum may be associated with a pneumothorax.
Vocal fremitus.
Vocal fremitus is the measure of speech vibrations transmitted through the chest wall to the examiner’s hands. It is measured by asking the patient to repeatedly say ‘ninety-nine’ while the examiner’s hands are placed flat on both sides of the chest. The hands are moved from apices to bases, anteriorly and posteriorly, comparing the vibration felt. Vocal fremitus is increased when the lung underneath is relatively solid (consolidated), as this transmits sound better. As sound transmission is decreased through any interface between lung and air or fluid, vocal fremitus is decreased in patients with a pneumothorax or a pleural effusion.
Percussion
Percussion of the chest provides further information that can help in the assessment and localization of lung disease. It is performed by placing the left hand firmly on the chest wall so that the fingers have good contact with the skin. The middle finger of the left hand is struck over the distal interphalangeal joint with the middle finger of the right hand. The right wrist should be relaxed so that the weight of the entire right hand is transmitted through the middle finger. Both sides of the chest from top to bottom should be percussed alternately, paying particular attention to the comparison between sides.
Resonance is generated by the chest wall vibrating over the underlying tissues. Normal resonance is heard over aerated lung, while consolidated lung sounds dull, and a pleural effusion sounds ‘stony dull’. Increased resonance is heard when the chest wall is free to vibrate over an air-filled space, such as a pneumothorax or bulla. In situations where the chest wall is unable to move freely, as may occur in obese patients, the percussion note may sound dull, even if the underlying lung is normal.
Auscultation
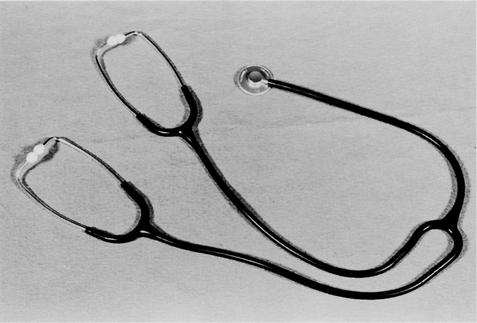
Chest auscultation is the process of listening to and interpreting the sounds produced within the thorax. A stethoscope simplifies auscultation and facilitates localization of any abnormalities. It consists of a diaphragm and bell connected by tubing to two earpieces. The diaphragm is generally used for listening to breath sounds, while the bell is best for the very low frequencies generated by the heart (especially the third and fourth heart sounds). The diaphragm and bell must be intact for a sound to be heard properly, and the tubing relatively short to minimize absorption of the sound. The earpieces, made of plastic or rubber, should fit snugly within the ears, pointing slightly forward in order to maximize sound transmission into the auditory canal.
A teaching stethoscope (Fig. 1.6) is a useful tool to allow both the experienced and inexperienced physiotherapist to hear the same sounds simultaneously (Ellis 1985). More recently, a number of electronic stethoscopes have been produced, allowing teacher and students to listen together.
Chest auscultation should ideally be performed in a quiet room, with the chest exposed. The patient is instructed to take deep breaths through an open mouth, as turbulence within the nose can interfere with the breath sounds. There is a wide variation in the intensity of breath sounds depending on chest wall thickness. The terms used are described below.
Breath sounds
Normal breath sounds are generated by turbulent airflow in the trachea and large airways. These sounds, which can be heard directly over the trachea, comprise high, medium and low frequencies. The higher frequencies are attenuated by normal lung tissue so that breath sounds heard over the periphery are softer and lower pitched. Originally it was thought that the higher-pitched sounds were generated by the bronchi (bronchial breath sounds) and the lower ones by airflow into the alveoli (vesicular breath sounds). It is now known that normal breath sounds (previously called ‘vesicular’) simply represent filtering of the ‘bronchial’ breath sounds generated in the large airways. Although technically incorrect, normal breath sounds are still sometimes referred to as ‘vesicular’ or ‘bronchovesicular’. Normal breath sounds are heard all over the chest wall throughout inspiration and for a short period during expiration.
Bronchial breath sounds are the normal tracheal and large airway sounds, transmitted through airless lung, which does not attenuate the higher frequencies. Thus, the sounds heard over an area of consolidated lung are similar to those heard over the trachea itself. Bronchial breath sounds are loud and high-pitched, with a harsh quality. They are heard equally throughout inspiration and expiration, with a short pause between the two. In all three respects, bronchial breath sounds differ from normal breath sounds which are faint, lower-pitched and absent during the latter half of expiration.
If the bronchus supplying an area of consolidated lung is obstructed (e.g. carcinoma, large sputum plug) bronchial breath sounds may not be heard as the obstruction blocks sound transmission.
Diminished sounds occur when there is a reduction in the initial generation of the sound or when there is an increase in sound attenuation. As the breath sounds are generated by flow-related turbulence, reduced flow causes less sound. Thus patients who will not (e.g. due to pain) or cannot (e.g. due to muscle weakness) breathe deeply will have globally diminished breath sounds. Similarly, diminished breath sounds are heard in some patients with emphysema where the combination of parenchymal destruction and hyperinflation causes greater attenuation of the normal breath sounds. In obese patients, breath sounds are diminished by attenuation through the fat over the chest wall.
Locally diminished breath sounds may represent obstruction of a bronchus by tumour or large sputum plugs. Localized accumulation of air or fluid in the pleural space will block sound transmission so that breath sounds are absent.
Added sounds
Wheezes, previously called ‘rhonchi’, are musical tones produced by airflow vibrating a narrowed or compressed airway. A fixed, monophonic wheeze is caused by a single obstructed airway, while polyphonic wheezes are due to widespread disease. Any cause of narrowing, for example, bronchospasm, mucosal oedema, sputum or foreign bodies, may cause wheezes. As the airways are normally compressed during expiration, wheezes are first heard at this time. When airway narrowing is more severe, wheezes may also be heard during inspiration. The pitch of the wheeze is directly related to the degree of narrowing, with high-pitched wheezes indicating near total obstruction. However, the volume of the wheeze may be misleading as the moderate asthmatic may have loud wheezes while the very severe asthmatic may have a ‘quiet chest’ because he is not generating sufficient airflow to cause wheezes.
Low-pitched, localized wheezes are caused by sputum retention and can change or clear after coughing.
Crackles, previously called ‘crepitations’ or ‘râles’, are clicking sounds heard during inspiration. They are caused by the opening of previously closed alveoli and small airways during inspiration. Crackles are described as ‘early’ or ‘late’, ‘fine’ or ‘coarse’, and ‘localized’ or ‘widespread’. Coarse, early inspiratory crackles occur when bronchioles open (often heard in bronchiectasis and bronchitis), while fine, late inspiratory crackles occur when alveoli and respiratory bronchioles open (often heard in pulmonary oedema and pulmonary fibrosis). When severe, the late inspiratory crackles of pulmonary oedema and pulmonary fibrosis may become coarser and start earlier in inspiration.
Localized crackles may occur in dependent alveoli, which are gradually closed by compression from the lung above. This early feature of subsegmental lung collapse resolves when the patient breathes deeply or coughs. The crackles of pulmonary oedema are also more marked basally, but only clear transiently after coughing. The differentiation between subsegmental lung collapse and pulmonary oedema may be difficult, and sometimes auscultation will not clarify the situation. Elevation of the jugular venous pressure and peripheral oedema suggest pulmonary oedema, whereas ineffective cough, recent anaesthesia and pyrexia suggest sputum retention, which could lead to subsegmental lung collapse (Table 1.3). Postoperative and intensive care patients may have a combination of both pulmonary oedema and sputum retention.
Table 1.3 Differentiation between pulmonary oedema and sputum retention
| Chest sign | Pulmonary oedema | Sputum retention |
|---|---|---|
| Auscultation | Fine crackles, especially at bases, with or without wheezes | Scattered or localized crackles, with or without wheezes, may move with coughing |
| Sputum | Frothy white or pink | Thicker, more viscid, any colour |
JVP, jugular venous pressure
Pleural rub is the creaking or rubbing sound that occurs with each breath when the pleural surfaces are roughened by inflammation, infection or neoplasm. Normally the visceral and parietal pleura slide silently. Pleural rubs range from being localized and soft to being loud and generalized, sometimes even palpable. In certain instances, they may be difficult to differentiate from crackles. An important distinguishing feature is that pleural rubs are heard equally during inspiration and expiration, with the sounds often recurring in reverse order during expiration.
Vocal resonance.
Vocal resonance is the transmission of voice through the airways and lung tissue to the chest wall where it is heard through a stethoscope. It is usually tested by instructing the patient to say ‘ninety-nine’ repeatedly (like vocal fremitus which is felt with the hands). As mentioned previously, normal lung attenuates the higher frequencies so that the lower frequencies dominate. Thus, speech normally becomes a low-pitched mumble. Consolidated lung transmits all sounds better, especially the high frequencies, so the transmitted sound is louder and higher pitched. In this situation speech can actually be understood. Whispered speech lacks the lower frequencies and is normally not transmitted to the chest wall. However, over areas of consolidation the whisper is clearly heard and intelligible – this is called ‘whispering pectoriloquy’.
As with auscultation of breath sounds, vocal resonance is decreased when the transmission of sound through the lung or from the lung to chest wall is impeded. This occurs with emphysema, pneumothorax, pleural thickening or pleural effusion.
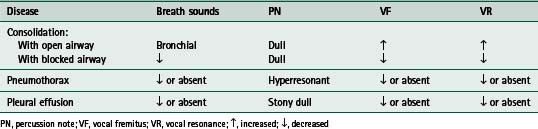
A summary of the chest examination in selected chest problems is given in Table 1.4.
Heart sounds.
The normal heart sounds represent the closure of the four heart valves. The first heart sound is caused by closure of the mitral and tricuspid valves, while the second heart sound is due to closure of the aortic and pulmonary valves. A third heart sound indicates cardiac failure in adults, but may be normal in children. It is attributed to vibration of the ventricular walls caused by rapid filling in early diastole. The fourth heart sound is caused by vibration of the ventricular walls in late diastole as the atria contract. It may be heard in heart failure, hypertension and aortic valve disease.
A murmur is the sound generated by turbulent flow through a valve. The murmur of valvular incompetence is caused by back flow across the valve, while stenotic valves generate murmurs by turbulent forward flow.
Sputum
At the end of the respiratory examination, it is often worthwhile to instruct the patient to huff to a low lung volume to assess the presence of retained secretions. Any sputum produced should be examined for colour, consistency and quantity as previously described.
Physiotherapy techniques
In patients who have previously been taught physiotherapy, it is important to ascertain which techniques are used, how well they are performed, and their effectiveness. For example, patients who use huffing to clear retained secretions should have its effectiveness assessed. Suboptimal techniques need to be identified and their correction included in the treatment plan.
Exercise capacity
For a complete assessment of the respiratory system, exercise capacity should also be measured. Depending on the situation, this may vary from a full exercise test for measuring maximum oxygen uptake, to a simple assessment of breathlessness during normal activities. An exercise test provides the best measure of functional limitation, which may differ from that suggested by a patient’s lung function. Two of the most common methods used to assess patients with respiratory disease are the 6-minute walking test (Butland et al 1982) and the shuttle walking tests (Bradley et al 1999, Revill et al 1999, Singh et al 1992).
Test results
The final stage of assessment of a respiratory or cardiac patient involves the use of tests, in particular spirometry, arterial blood gases and chest radiography. The following is a brief summary of the application of these tests. A full discussion is given in Chapters 2 and 3.
Spirometry
The forced expiratory volume in 1 second (FEV1), the forced vital capacity (FVC) and peak expiratory flow (PEF) are important measures of ventilatory function. Normal values, based on population studies, depend on age, height, sex and race. Weight is not an important determinant of lung function, except in the markedly obese or malnourished.
Although often expressed as absolute values, lung function should always be compared with predicted values and previous recordings for that patient. For example a 21-year-old, 6-foot-tall male asthmatic changing his spirometry (FEV1/FVC) from 4.0/5.0 litres to 1.5/3.0 litres should cause concern, while a normal 81-year-old, 5-foot female may never manage to blow more than 1.3/1.8 litres!
Arterial blood gases
Arterial blood gases (ABGs) provide an accurate measure of oxygen uptake and carbon dioxide removal by the respiratory system as a whole. The arterial blood is usually sampled from the radial artery at the wrist, but arterialized capillary samples may be taken from the earlobe. Arterial blood gases are best used as a mea-sure of steady-state gas exchange; thus it is imperative that the patient is resting quietly with a constant inspired oxygen level (FiO2) and mode of ventilation for at least 30 minutes before sampling. When analysing the results, consideration must be given to all these factors. Normal values for arterial blood gases are given in Box 1.4.
Thoracic imaging
Chest radiographs and other imaging techniques (Chapter 2) are an important aid to physical examination as they provide a clear picture of the extent and severity of disease at that time. In some instances, chest radiographs or computed tomography (CT) may show more extensive disease than expected, while in others they may underestimate the pathology present. Comparison with previous images provides an excellent measure of improvement or deterioration over time, and an objective assessment of the response to treatment. It should be noted that chest radiograph may sometimes lag 1–2 days behind the clinical findings.
Electrocardiogram and echocardiograms
The electrocardiogram (ECG) and echocardiogram provide important information regarding cardiac electrical and mechanical function. An understanding of these is essential as abnormalities may alter the treatment plan. More detailed information about their measurement and implications are covered in Chapter 3.
PROBLEM LIST
The second part of the problem-oriented medical record (POMR) is the problem list (see Fig. 1.1). The information in the database, together with the subjective and objective assessment, are analysed as a whole, and integrated with the physiotherapist’s knowledge of disease processes.
The problem list is then compiled. It consists of a simple, functional and specific list of the patient’s problems at that time, not always listed in order of priority. Each problem is numbered and dated at the time of assessment. The problem list should not only include those problems amenable to physiotherapy (e.g. breathlessness on exertion) but should also include other problems for consideration when designing and implementing a treatment plan (e.g. anaemia). The problem list should not be a list of signs and symptoms, as this would provide the wrong emphasis for treatment. In the past, disease-based treatment tended to result in standardized treatment, ignoring the patient’s individual problems. This meant that all chronic airflow limitation patients were given treatment for impaired airway clearance. All intubated patients also received standard treatment, irrespective of the presence or absence of excess secretions and the patient’s ability to clear them. The best system is one that is individualized to each patient.
Problems once resolved should be signed off and dated. Any subsequent problems are added and dated appropriately.
INITIAL PLANS
For each of the physiotherapy problems listed, long- and short-term goals are formulated. These should be Specific, Measurable, Achievable, Realistic and Timed (SMART). Prioritizing the problem list and developing the goals for each problem should be performed, where possible, in consultation with the patient. The importance of involving the patient himself cannot be overstressed, as cooperation is fundamental to nearly all physiotherapy treatment. The patient assessment will have identified important factors that must be considered when developing a plan and goals. Such factors may include coexisting conditions or disease (e.g. diabetes mellitus) or other factors such as age, motivation, cultural or social factors.
Long-term goals are generally directed at returning the patient to his maximum functional capacity. Specifically, goals may be simplified to functions that are important to the patient, e.g. to be able to walk home from the shops carrying one bag of shopping. When setting goals for an inpatient, consideration must be given to his discharge. If the home situation includes two flights of stairs to the bedroom then the goal of exercise ability should reflect this. If physiotherapy is to be continued at home after discharge, one of the goals must be to teach the patient or a relative how to perform the treatment effectively.
Short-term goals are the steps taken to achieve the long-term goals. In general these are small, simple activities that are more easily achieved. All goals, both short- and long-term, should state expected outcomes and time frames. The goals, especially the short-term goals, should be reviewed regularly as some patients may improve faster than others. If goals are not met within the agreed time frame, then revision is necessary. The time frame may have been too short, the goal inappropriate, or other problems need attention before this goal can be met.
The treatment plan includes the specifics of treatment, together with its frequency and equipment requirements. Patient education must not be omitted from the treatment plan, as it is an important component of physiotherapy.
A summary, as a reminder of the key points of assessment, is given in Box 1.5.
PROGRESS NOTES
These are written on a daily basis using the ‘subjective, objective, analysis, plan’ (SOAP) format:
Entries should be made for each physiotherapy problem, signed and dated. If there have been no changes, nothing further needs to be written.
Progress notes may also include a graph or flow chart. Graphs are particularly useful in displaying the change in a parameter with time, for example an asthmatic’s peak expiratory flow rates. Flow chart displays are useful if multiple factors are changing over a period of time, as may occur in the intensive care patient.
Outcomes
The short- and long-term goals provide a basis for evaluating the effectiveness of treatment for each problem. One of the best indicators of outcome is the change in objective findings after treatment. Although changes that occur immediately after a single treatment are related to physiotherapy intervention alone, changes over longer periods of time reflect treatment by the entire health team. Chest auscultation before and after a treatment may provide a simple indication of the effectiveness of that treatment. Similarly, the chest radiograph can demonstrate the effectiveness of physiotherapy treatment by showing diminution in the area of collapsed/consolidated lung. On a long-term basis, changes in lung function or exercise tolerance provide the most valuable measures of treatment outcome. If there are discrepancies between the actual and expected outcomes, the plan (P) documents the changes to the goals and/or treatment, as required.
The selection and use of appropriate outcome measures is fundamental to the evaluation of any therapy. Demonstrating the effects of physiotherapy intervention, using instruments that have high reliability and validity, is increasingly being required by healthcare providers and physiotherapists themselves. Other people who may require outcome data include the patient, caregivers, community and patient support groups.
To standardize the measurement of outcomes, the World Health Organization (WHO) has developed a scale of functioning and disability, the International Classification of Functioning, Disability and Health (ICIDH-2) (WHO 2001). This scale focuses on human functioning at the level of body, the whole person and the person within the social/environmental context. It classifies functioning of the affected body part, and the whole person in terms of impairment to bodily function and structure, limitation of activity and restriction to participation. It is designed to measure the effectiveness of an intervention using a patient-focused measure rather than the more traditional medical focus. For example, a patient with bronchiectasis who has had three admissions to hospital for chest infections over the last year is taught an airway clearance technique to assist sputum clearance. Over the next 12 months the outcome measure important to the patient is the ability to maintain a full-time job; while the outcome measure important to the Area Health Service is the cost saving achieved by a reduction in hospital admissions. Thus when selecting an outcome measure it is important to take into account for whom the data is needed.
DISCHARGE SUMMARY
Upon discharge or transfer elsewhere, a summary should be written of the patient’s initial problems, treatment and outcomes. Instruction for home programmes and any other relevant information should also be included. Discharge summaries are helpful to other physiotherapists who may treat the patient in the future. The summary should always contain adequate information for future audit and studies of patient care.
AUDIT
‘Audit’ refers to the systematic and critical analysis of the quality of care. There are three main forms of audit: structure, process and outcome.
The audit process is cyclical. Firstly, a standard of care is defined. The actual practice is then audited in comparison with the agreed standard. Discrepancies provoke further discussion. Changes are then made to eliminate these discrepancies. After an appropriate length of time the cycle begins again.
EDUCATIONAL PROGRAMME
By using a structured system of problem-oriented medical records and audit, the problem-oriented medical system allows identification of areas where goals are not being met within an appropriate time frame. Audit may also reveal situations where the agreed standards are not met. In both instances staff education programmes will improve patient care.
CONCLUSION
Accurate assessment should reveal the exact nature of the patient’s problems and identify those amenable to physiotherapy. Only then can the best treatment be chosen for that patient. Subsequent reassessment is essential to ensure that treatment is specific, effective and efficient. This process ensures high-quality patient care.
Aaronson NK. Quality of life assessment in clinical trials: methodological issues. Controlled Clinical Trials. 1989;10:195S-208S.
Borg GA. Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise. 1982;14(5):377-381.
Bradley J, Howard J, Wallace E, et al. Validity of a modified shuttle test in adult cystic fibrosis. Thorax. 1999;54:437-439.
Butland RJA, Pang J, Gross ER, et al. Two-, six-, and 12-minute walking tests in respiratory disease. British Medical Journal. 1982;284:1607-1608.
Criteria Committee of the New York Heart Association, 1994 Nomenclature and criteria for diagnosis of diseases of the heart and great vessels (www.americanheart.org/presenter.jhtml?identifier=1712) (Accessed 25 July 2007)
Ellis E. Making a teaching stethoscope. Australian Journal of Physiotherapy. 1985;31:244.
Juniper EF, Guyatt GH, Cox FM, et al. Development and validation of the mini asthma quality of life questionnaire. European Respiratory Journal. 1999;14(1):32-38.
Kinney MR, Burfitt SN, Stullenbarger E, et al. Quality of life in cardiac patient research: a meta-analysis. Nursing Research. 1996;45(3):173-180.
Mahler DA. How should health-related quality of life be assessed in patients with COPD? Chest. 2000;117(2):54S-57S. Suppl
Manthous CA, Hall JB, Olson D, et al. Effect of cooling on oxygen consumption in febrile critically ill patients. American Journal of Respiratory and Critical Care Medicine. 1995;151:10-14.
Miller DL. A study of techniques for the examination of sputum in a field survey of chronic bronchitis. American Review of Respiratory Disease. 1963;88:473-483.
Orr A, McVean RJ, Webb AK, et al. Urinary incontinence in women with cystic firosis is a marginalized and undertreated problem: questionnaire survey. British Medical Journal. 2001;322:1521.
Pashkow P, Ades PA, Emery CF, et al. Outcome measurement in cardiac and pulmonary rehabilitation. Journal of Cardiopulmonary Rehabilitation. 1995;15(6):394-405.
Revill SM, Morgan MDL, Singh SJ, et al. The endurance shuttle walk: a new field test for the assessment of endurance capacity in chronic obstructive pulmonary disease. Thorax. 1999;54:213-222.
Rubinstein I, Zamel N, DuBarry L, et al. Airflow limitation in morbidly obese, non-smoking men. Annals of Internal Medicine. 1990;112(11):828-832.
Scottish Intercollegiate Guidelines Network, 2004 Management of urinary incontinence in primary care (www.sign.ac.uk)
Singh SJ, Morgan MDL, Scott S, et al. The development of the shuttle walking test of disability in patients with chronic airways obstruction. Thorax. 1992;47(12):1019-1024.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2(7872):81-84.
Thakar R, Stanton S. Management of urinary incontinence in women. British Medical Journal. 2000;321:1326-1331.
Ware JE, Sherbourne CD. The MOS-short-form health survey (SF-36). Medical Care. 1992;30:473-483.
Weed LL. Medical records that guide and teach. New England Journal of Medicine. 1968;278:593-600. 652-657
World Health Organization, 2001 International Classification of Functioning, Disability and Health (www.who.int/icidh)