Androgens, anti-androgens and anabolic steroids
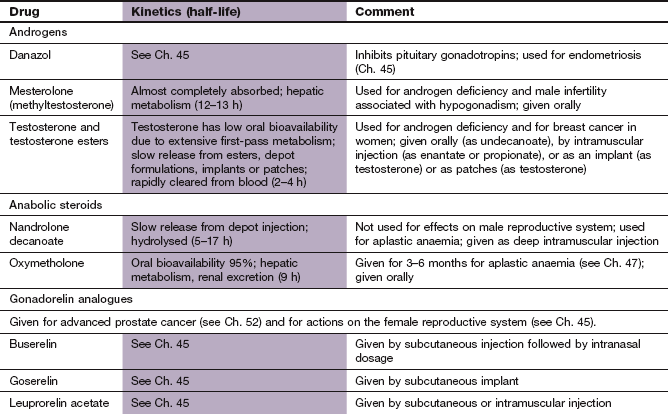
Androgens
Naturally occurring androgens are 19-carbon steroid hormones that are synthesised in the adrenal cortex and gonads (see Fig. 44.2). They have characteristic actions on the reproductive tract and other tissues as well as an anabolic effect on metabolism. A number of synthetic androgenic steroids have been developed. The term ‘anabolic steroid’ is used when the predominant action of the compound is anabolic rather than reproductive. There are a few medical uses for anabolic steroids, but they have achieved notoriety because of their abuse by athletes to enhance muscle development.
Testosterone is secreted by the Leydig cells of the testis, and its synthesis and release are stimulated by the gonadotropin luteinizing hormone (LH). In many tissues testosterone is aromatized to form oestradiol, which accelerates closure of bony epiphyses and contributes to brain development. It is oestradiol rather than testosterone that inhibits the release of gonadotropin-releasing hormone (GnRH) from the hypothalamus and LH via a negative-feedback loop (Ch. 43). Androgens are also released from the adrenal cortex, in response to stimulation by adrenocorticotropic hormone (ACTH; corticotropin); these are mainly dehydroepiandrosterone and androstenedione (see Fig. 44.2). Men produce large amounts of androgens and small amounts of oestrogens, while the reverse is the case in women.
The actions of testosterone are in part due to its metabolite dihydrotestosterone (DHT). This is produced from testosterone in the prostate, skin and reproductive tissues by the enzymatic action of 5α-reductase (Fig. 44.2). DHT has a higher affinity than testosterone for the androgen receptor, and is five times more potent as an androgen. DHT is mainly responsible for the development of secondary sexual characteristics in men.
The cellular mechanism of action of steroid hormones is discussed in Chapters 1 and 44. Androgens act mainly through genomic effects on protein synthesis via the cytoplasmic androgen receptor (AR), which is then translocated to the cell nucleus. The androgen receptor also produces rapid-onset, non-genomic actions in the cytoplasm by affecting signal transduction and ion transport. This is responsible for effects such as vasodilation (see also Ch. 44).
Circulating androgens are bound largely to a specific transport protein, sex hormone-binding globulin (SHBG), which has a greater affinity for androgens than for oestrogen.
Male sex hormones
Actions of testosterone
Actions of androgens include the following:
 sexual differentiation in the fetus,
sexual differentiation in the fetus,
sexual development of the male testis, penis, epididymis, seminal vesicles and prostate at puberty, and maintenance of these tissues in adults,
stimulation and maintenance of sexual function and behaviour,
metabolic actions. Testosterone is a powerful anabolic agent producing a positive nitrogen balance with an increase in the bulk of tissues such as muscle and bone. In the skin, sebum production is increased, which can provoke acne. Growth of axillary, pubic, facial and chest hair is stimulated. In the liver, testosterone increases the synthesis of several proteins, including clotting factors, but decreases high-density lipoprotein (HDL) synthesis (Ch. 48). Testosterone also induces several liver enzymes, including steroid hydroxylases,
haematological actions. Testosterone stimulates the production of erythropoietin by the kidneys, leading to higher haemoglobin concentrations in men than in women.
Pharmacokinetics
Oral preparations. Testosterone is well absorbed from the gut but is almost completely degraded by first-pass metabolism in the gut wall and liver. Oral absorption can be enhanced by esterification of testosterone to create hydrophobic compounds, such as testosterone undecanoate, which are absorbed via lacteals into the lymphatic system, thus avoiding hepatic metabolism. Mesterolone is a synthetic testosterone derivative that has a greater oral bioavailability than testosterone, but less androgenic activity.
Depot injection. The most popular form of therapy for hypogonadism in men is an intramuscular injection of a testosterone ester, usually in oily solution, given at intervals from 2–3 weeks up to 10–14 weeks depending on the formulation. Testosterone is absorbed gradually after ester hydrolysis at the site of injection. Examples are testosterone enantate, propionate and undecanoate.
Transdermal delivery. A transdermal delivery patch containing testosterone can be applied to the back, abdomen, upper arm or thigh, rotating the site daily to avoid skin irritation. Testosterone gel is an alternative way to deliver the drug transdermally.
Buccal delivery. Testosterone can be delivered via a buccal tablet which softens to a gel and adheres to the mucosa. This provides sustained release of testosterone, and avoids hepatic first-pass metabolism.
Subcutaneous implant. A pellet of pure crystalline testosterone provides a reservoir for gradual absorption into the systemic circulation for 4–5 months. A minor surgical procedure is necessary, and therefore this method of delivery is rarely used.
Testosterone is metabolised in the liver to androstenedione, and then to inactive compounds. Some testosterone undergoes conversion in specific organs to dihydrotestosterone, and a small amount undergoes aromatisation to oestradiol (see above). Mesterolone is not metabolised to oestrogenic compounds.
Unwanted effects
In hypogonadal adolescents, initial nitrogen retention and a spurt in linear growth is followed by premature epiphyseal closure and short stature. A short course of testosterone can be used for the treatment of delayed puberty without inducing epiphyseal closure.
Nausea, vomiting, gastrointestinal bleeding.
Sodium retention with oedema and hypertension.
Hirsutism, male-pattern baldness, acne. Virilisation occurs in women given testosterone.
Conversion to oestrogens by aromatase can produce gynaecomastia (see Fig. 44.2). This is less likely to occur with mesterolone.
Suppression of gonadotropin release with diminished testicular size and reduced spermatogenesis. Hypogonadal men will not regain fertility while taking androgens.
Cholestatic jaundice. Liver tumours are a rare complication.
Clinical uses of testosterone
The main clinical use is as hormone-replacement therapy for primary hypogonadism in adult males. Late-onset hypogonadism may present with erectile dysfunction, fatigue, depression, hot flushes, muscle weakness and reduced body hair. Testosterone replacement can improve quality of life in this situation.
It can be used briefly in constitutionally delayed puberty, even in the absence of hypogonadism.
Androgens are occasionally beneficial for promoting erythropoiesis in some forms of aplastic anaemia.
Danazol
Danazol is an androgen derivative described as an ‘impeded’ androgen, which is weakly androgenic on peripheral tissues. It has no oestrogenic activity as, unlike testosterone, it is not converted into an oestrogen by aromatases. Its main action is feedback inhibition of gonadotropin and gonadotropin-releasing hormone (GnRH) secretion. It therefore has anti-oestrogenic and anti-progestogenic actions.
Pharmacokinetics
Danazol is well absorbed orally, metabolised in the liver and has a short half-life (3 h).
Anabolic steroids
Anabolic steroids are most frequently encountered as drugs of abuse to improve athletic performance (doping). In medical practice there are few indications for these compounds and there is little evidence for efficacy in many conditions where their use has been advocated.
Pharmacokinetics
Nandrolone is given as a decanoate ester depot formulation by intramuscular injection every 3 weeks. Oxymetholone is available as an oral formulation from specialist suppliers.
Abuse of anabolic steroids
The ability of androgens to promote an increase in muscle mass has led to their abuse to improve physical performance by athletes, weightlifters and bodybuilders. Often, several different androgens are used for prolonged periods, perhaps with a brief ‘drug-free’ period. Abused compounds include testosterone, nandrolone and oxymetholone and many others that are licensed only for veterinary use. The consequences of abuse include:
weight gain from muscle hypertrophy and fluid retention,
acne in adolescent and young men,
decreased testicular size and reduced sperm count,
hepatotoxicity with cholestasis, hepatitis or, occasionally, hepatocellular tumours,
atherogenic changes in the plasma lipids with a rise in plasma LDL cholesterol and a fall in HDL cholesterol (Ch. 48); these changes may predispose to premature vascular disease,
psychological disturbance, including changes in libido, increased aggression and psychotic symptoms.
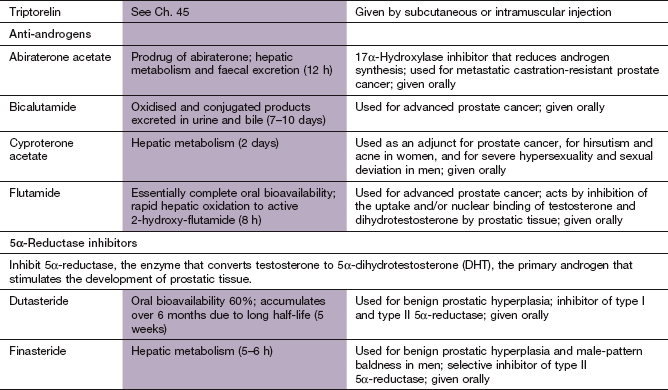
Anti-androgens
Mechanism of action
Bicalutamide and flutamide are non-steroidal, relatively pure anti-androgens. They bind to androgen receptors in the cell cytoplasm, either to the hormone binding site or to an adjacent site producing distortion of the co-activator binding site, so that the receptor cannot initiate gene transcription.
Cyproterone acetate
Cyproterone acetate, a 21-carbon steroid, is a progestogen and a weak glucocorticoid (Ch. 44). Its progestational activity produces feedback inhibition of gonadotrophin (LH) secretion (Ch. 45). At high doses cyproterone inhibits androgen binding to its receptors.
Clinical uses of anti-androgens
The main use of anti-androgens is in the treatment of carcinoma of the prostate (Ch. 52), usually in conjunction with a gonadorelin analogue (Ch. 43).
Cyproterone acetate is used in male sexual offenders as ‘chemical castration’.
Cyproterone acetate can be given for manifestations of hyper-androgenisation in females, such as acne and hirsutism, in conjunction with ethinylestradiol in an oral combined hormonal contraceptive (Ch. 45).
5α-Reductase inhibitors
Mechanism of action and effects
Dutasteride and finasteride reduce the formation of dihydrotestosterone by inhibiting 5α-reductase, rather than acting as an antagonist at androgen receptors. In the adult male finasteride and dutasteride can produce regression of benign prostatic hypertrophy and improve the symptoms of prostatism. More details are found in Ch. 15.
True/false questions
1. Androgen deficiency in adult men may cause decreased libido.
2. Testosterone cannot be given orally.
3. Testosterone alone is used to stimulate spermatogenesis.
4. Nandrolone causes less virilisation in women than testosterone.
5. Cyproterone acetate is used as an adjunct to the treatment of prostate cancer.
1. True. Androgen deficiency may also cause impotence, reduced muscle mass, loss of body hair and other effects.
2. True. Testosterone is ineffective when given orally as it undergoes very extensive first-pass metabolism; it is given as testosterone ester formulations or in transdermal patches.
3. False. Other treatments are required, including human chorionic gonadotropin (HCG) and other gonadotropins.
4. True. Nandrolone has fewer androgenic effects than testosterone, but has many other unwanted effects.
5. True. Cyproterone acetate is an anti-androgen used with a gonadorelin analogue in prostate cancer.
6. True. Anti-androgens can cause gynaecomastia, inhibition of spermatogenesis and other unwanted effects.
OBA answer
A Incorrect. 5α-Reductase converts testosterone to active dihydrotestosterone.
B Incorrect. Cyproterone is an anti-androgen; it inhibits spermatogenesis.
C Incorrect. Nandrolone is an androgen and causes an increase in muscle mass.
D Correct. Danazol has anti-androgen, anti-oestrogen and anti-progesterone activity and is used in the treatment of endometriosis.
E Incorrect. Testosterone is markedly anabolic, increasing turnover and growth in many tissues and cells.
Di Luigi, L, Romanelli, F, Lenzi, A. Androgenic-anabolic steroids abuse in males. J Endocrinol Invest. 2005;28(suppl 3):81–84.
Kazi, M, Geraci, SA, Koch, CA. Considerations for the diagnosis and treatment of testosterone deficiency in elderly men. Am J Med. 2007;120:835–840.
Rhoden, EL, Morgentaler, A. Risks of testosterone-replacement therapy and recommendations for monitoring. N Engl J Med. 2004;350:482–492.
Schneider, HPG. Androgens and antiandrogens. Ann NY Acad Sci. 2003;997:292–306.
Traish, AM, Miner, MM, Morgentaler, A, et al. Testosterone deficiency. Am J Med. 2011;124:578–587.