ALTERATIONS OF MUSCULOSKELETAL FUNCTION



Musculoskeletal injuries include fractures, dislocations, sprains, and strains. Fractures are the most serious. Alterations in bones, joints, and muscles may be caused by metabolic disorders, infections, inflammatory or noninflammatory diseases, or tumors. Trauma is the leading cause of death of people ages 1 to 44 years of all races and socioeconomic levels.
MUSCULOSKELETAL INJURIES
Skeletal muscles can withstand many penetrating injuries without permanent loss of function. For example, studies of soldiers with severe combat injuries showed that muscle function was preserved after the removal of large portions of muscle tissue. Successful regeneration of skeletal muscle fibers depends primarily on the extent of injury, preservation of vascular supply (and source of nutrition), and the availability of terminal axons for reinnervation.
Skeletal Trauma
A fracture is a break in the continuity of a bone. A break occurs when force is applied that exceeds the tensile or compressive strength of the bone. The incidence of fractures varies for individual bones according to age and gender. The highest incidence of fractures occurs in young males (between ages 15 and 24 years) and in adults 65 years of age and older. Fractures of healthy bones, particularly the tibia, clavicle, and lower humerus, tend to occur in young persons and tend to be the result of trauma. Fractures of the hands and feet are usually caused by accidents in the workplace. The incidence of fractures of the upper femur, upper humerus, vertebrae, and pelvis is highest in older or older adults and is often associated with osteoporosis (see p. 1576). In 1990, an estimated 1.66 million hip fractures occurred worldwide; that number is expected to increase to 6.3 million by the year 2050.1
Classification: Fractures can be classified as complete or incomplete and open or closed (Figure 42-1). In a complete fracture the bone is broken all the way through, whereas in an incomplete fracture the bone is damaged but still in one piece. Complete or incomplete fractures also can be classified as open (formerly referred to as compound) if the skin is broken or as closed (formerly called simple) if it is not. A fracture in which a bone breaks into more than two fragments is termed a comminuted fracture. Fractures are classified also according to the direction of the fracture line. A linear fracture runs parallel to the long axis of the bone. An oblique fracture is a slanted fracture of the shaft of the bone. A spiral fracture encircles the bone, and a transverse fracture occurs straight across the bone.
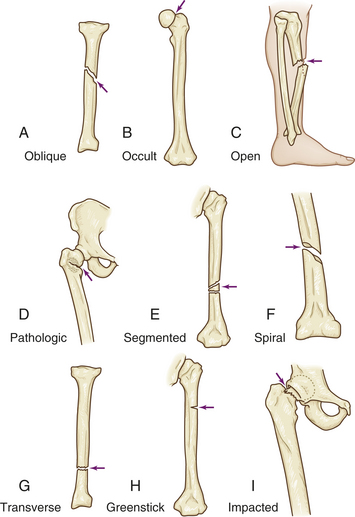
Figure 42-1 Examples of types of bone fractures A, Oblique: fracture at oblique angle across both cortices. Cause: direct or indirect energy, with angulation and some compression. B, Occult: fracture that is hidden or not readily discernible. Cause: minor force or energy. C, Open: skin broken over fracture; possible soft tissue trauma. Cause: moderate to severe energy that is continuous and exceeds tissue tolerances. D, Pathologic: transverse, oblique, or spiral fracture of bone weakened by tumor pressure or presence. Cause: minor energy or force, which may be direct or indirect. E, Segmented: fracture with two or more pieces or segments. Cause: direct or indirect moderate to severe force. F, Spiral: fracture that curves around cortices and may become displaced by twist. Cause: direct or indirect twisting energy or force with distal part held or unable to move. G, Transverse: horizontal break through bone. Cause: direct or indirect energy toward bone. H, Greenstick: break in only one cortex of bone. Cause: minor direct or indirect energy. I, Impacted: fracture with one end wedged into opposite end of inside fractured fragment. Cause: compressive axial energy or force directly to distal fragment. (Redrawn from Mourad L: Musculoskeletal system. In Thompson JM et al, editors: Mosby’s clinical nursing, ed 7, St Louis, 2002, Mosby.)
Incomplete fractures tend to occur in the more flexible, growing bones of children. The three main types of incomplete fractures are greenstick, torus, and bowing. A greenstick fracture perforates one cortex and splinters the spongy bone. The name is derived from the damage sustained by a young tree branch (a green stick) when it is bent sharply. The outer surface is disrupted, but the inner surface remains intact. Greenstick fractures typically occur in the metaphysis or diaphysis of the tibia, radius, and ulna. In a torus fracture the cortex buckles but does not break. Bowing fractures usually occur when longitudinal force is applied to bone. This type of fracture is common in children and usually involves the paired radius-ulna or fibula-tibia. A complete diaphyseal fracture occurs in one of the bones of the pair, which disperses the stress sufficiently to prevent a complete fracture of the second bone, which bows. A bowing fracture resists correction (reduction) because the force necessary to reduce it must be equal to the force that bowed it. Treatment of bowing fractures is difficult also because the bowed bone interferes with reduction of the fractured bone. A fracture that results from a low-level trauma (one that would not normally cause a fracture) is called a fragility fracture, which is often seen in osteoporosis. Types of fractures are summarized in Table 42-1.
Table 42-1
| Type | Definition |
| Typical Complete Fractures | |
| Closed fracture | The skin overlying the bone is intact |
| Open fracture | Communicating wound between bone and skin |
| Comminuted fracture | Multiple bone fragments |
| Linear fracture | Fracture line parallel to long axis of bone |
| Oblique fracture | Fracture line at an angle to long axis of bone |
| Spiral fracture | Fracture line encircling bone (as a spiral staircase) |
| Transverse fracture | Fracture line perpendicular to long axis of bone |
| Impacted | Fracture fragments are pushed into each other |
| Pathologic | Fracture occurs at a point in the bone weakened by disease (for example, bones with tumors or osteoporosis) |
| Avulsion | A fragment of bone connected to a ligament or tendon breaks off from the main bone |
| Compression | Fracture is wedged or squeezed together on one side of bone |
| Displaced | Fracture with one, both, or all fragments out of normal alignment |
| Extracapsular | Fragment is close to the joint but remains outside the joint capsule |
| Intracapsular | Fragment extends into or is within the joint capsule |
| Fragility | Fracture caused by low-level trauma |
| Typical Incomplete Fractures | |
| Greenstick fracture | Break on one cortex of bone with splintering of inner bone surface (commonly occurs in children and older adults) |
| Torus fracture | Buckling of cortex |
| Bowing fracture | Bending of the bone |
| Stress fracture | Microfracture |
| Transchondral fracture | Separation of cartilaginous joint surface (articular cartilage) from main shaft of bone |
Fractures may be further classified by cause as pathologic, stress, or transchondral. A pathologic fracture is a break at the site of a preexisting abnormality, usually by force that would not fracture a normal bone. Any disease process that weakens a bone (especially the cortex) predisposes the bone to pathologic fracture, commonly associated with tumors, osteoporosis, infections, and metabolic bone disorders.
Stress fractures occur in normal or abnormal bone that is subjected to repeated stress, such as occurs during athletics. The stress is less than the stress that usually causes a fracture. Two types of stress fractures are fatigue fractures, caused by abnormal stress or torque applied to a bone with normal ability to deform and recover (e.g., joggers, dancers, military recruits), and insufficiency fractures, stress fractures that occur in bones lacking normal ability to deform and recover (i.e., normal weight bearing or activity fractures the bone).
A transchondral fracture consists of fragmentation and separation of a portion of the articular cartilage that covers the end of a bone at a joint. (Joint structures are defined in Chapter 41.) The fragments may consist of cartilage alone or cartilage and bone. Typical sites of transchondral fracture are the distal femur, the ankle, the kneecap, the elbow, and the wrist. Transchondral fractures are most prevalent in adolescents.
PATHOPHYSIOLOGY When a bone is broken the periosteum and blood vessels in the cortex, marrow, and surrounding soft tissues are disrupted. Bleeding occurs from the damaged ends of the bone and from the neighboring soft tissue. A clot (hematoma) forms within the medullary canal, between the fractured ends of the bone, and beneath the periosteum. Bone tissue immediately adjacent to the fracture dies. This necrotic tissue (along with any debris in the fracture area) stimulates an intense inflammatory response characterized by vasodilation, exudation of plasma and leukocytes, and infiltration by inflammatory leukocytes and mast cells. Within 48 hours after the injury, vascular tissue invades the fracture area from surrounding soft tissue and the marrow cavity, and blood flow to the entire bone is increased. Bone-forming cells in the periosteum, endosteum, and marrow are activated to produce subperiosteal procallus along the outer surface of the shaft and over the broken ends of the bone (Figure 42-2). Osteoblasts within the procallus synthesize collagen and matrix, which becomes mineralized to form callus. As the repair process continues, remodeling occurs, during which unnecessary callus is resorbed and trabeculae are formed along lines of stress. Except for the liver, bone is unique among all body tissues in that it will form new bone, not scar tissue, when it heals after a fracture.

Figure 42-2 Exuberant callus formation following fracture. (From Rosai J: Ackerman’s surgical pathology, ed 8, St Louis, 1996, Mosby.)
CLINICAL MANIFESTATIONS The clinical manifestations of a fracture vary according to the type of fracture, site of the fracture, and associated soft tissue injury. In general, the signs and symptoms of a fracture include impaired function, unnatural alignment (deformity), swelling, muscle spasm, tenderness, pain, and impaired sensation. The position of the bone segments is determined by the pull of attached muscles, gravity, and the direction and magnitude of the force that caused the fracture. One or both segments may be rotated inward or outward on the bone’s long axis (rotation), be misaligned at an angle (angulation), slide over the other segment (overriding), or be out of normal position (displaced).
The immediate pain of a fracture is severe and usually caused by trauma. Subsequent pain may be produced by muscle spasm, overriding of the fracture segments, or damage to adjacent soft tissues. Numbness is common and is caused by swelling, by the pinching or severing of a nerve, by the trauma, or by bone fragments. Pathologic fractures usually cause angular deformity, painless swelling, or generalized bone pain. Pathologic fractures are not usually associated with trauma or trauma-related pain. Stress fractures are painful, not because of trauma, but because of accelerated remodeling. The pain occurs during activity and is usually relieved by rest. Stress fractures also cause local tenderness and soft tissue swelling. Transchondral fractures may be entirely asymptomatic or painful during movement. Range of motion in the joint is limited, and movement may evoke audible clicking sounds (crepitus).
EVALUATION AND TREATMENT Treatment of a displaced fracture involves realigning the bone fragments (reduction) close to their normal or anatomic position and holding the fragments in place (immobilization) so that bone union can occur. Several methods are available to reduce a fracture: closed manipulation, traction, and open reduction. Many fractures heal without manipulation—they require only adequate immobilization. A fracture that is malaligned, however, requires more aggressive treatment.
Many fractures can be reduced by closed manipulation: the skin is not opened, and the bone is moved or manipulated into place. Closed manipulation is used when the contour of the bone is in fair alignment and can be maintained well with immobilization.
Traction is used to accomplish or maintain reduction. When bone fragments are displaced (not in their anatomic position), weights are used to apply firm, steady traction (pull) and countertraction to the long axis of the bone. Traction stretches and fatigues muscles that pull the bone fragments out of place, allowing the distal fragment to align with the proximal fragment. Traction can be applied to the skin (skin traction), directly to the involved bone, or distal to the involved bone (skeletal traction). Skin traction is used when only a few pounds of pulling force are needed to realign the fragments or when the traction will be used for brief times only, such as before surgery or, for children with femoral fractures, for 3 to 7 days before applying a cast. In skeletal traction, a pin or wire is drilled through the bone below the fracture site, and a traction bow, rope, and weights are attached to the pin or wire to apply tension and to provide the pulling force needed to overcome the muscle spasm and help realign the fracture fragments.
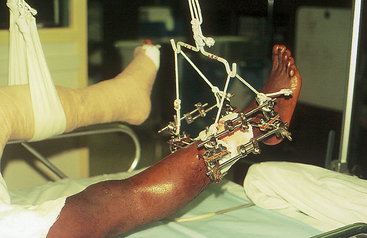
External fixation is used to reduce and immobilize significantly displaced open fractures. Pins are placed in the bone proximal and distal to the break and then stabilized by an external frame of clamps and rods (Figure 42-3).
Open reduction is a surgical procedure that exposes the fracture site; the fragments are brought into alignment under direct visualization. Some form of prosthesis, screw, plate, nail, or wire usually is used to maintain the reduction (internal fixation).
Splints and casts are used to immobilize and hold a reduction in place. Improper reduction or immobilization of a fractured bone may result in nonunion, delayed union, or malunion. Nonunion is failure of the bone ends to grow together (Figure 42-4). The gap between the broken ends of the bone fills with dense fibrous and fibrocartilaginous tissue instead of new bone. Occasionally the fibrous tissue contains a fluid-filled space that resembles a joint and is termed a false joint, or pseudoarthrosis. Delayed union is union that does not occur until approximately 8 to 9 months after a fracture. Malunion is the healing of a bone in a nonanatomic position. Treatment of delayed union and nonunion includes use of various modalities designed to stimulate new bone formation. Physical modalities, such as implantable or external electric current devices, electromagnetic field generations, and low-density ultrasound, have been effective in stimulating bone formation. Gene therapy also shows promise in promoting formation of new bone. Large defects in bone can be filled with bone graft or synthetic materials, such as calcium phosphate cement.2

Dislocation and Subluxation
Dislocation and subluxation are usually caused by trauma. Dislocation is the temporary displacement of a bone from its normal position in a joint. If the contact between the two surfaces is only partially lost, the injury is called a subluxation.
Dislocation and subluxation are most common in persons younger than 20 years and are generally associated with fractures. Dislocation and subluxation, however, may result from congenital or acquired disorders that cause (1) muscular imbalance, as occurs with congenital dislocation of the hip or neurologic disorders; (2) incongruities in the articulating surfaces of the bones, as occurs with rheumatoid arthritis (see p. 1596); or (3) joint instability.
Most often dislocated or subluxated are the joints of the shoulder, elbow, wrist, finger, hip, and knee (Figure 42-5). The shoulder’s glenohumeral joint is a relatively unstable joint because the articular surface of the glenoid cavity is only one third as large as the surface of the humeral head. As a result, the glenohumeral joint is often injured. Physical trauma to the shoulder can cause anterior, posterior, superior, or inferior dislocation. Anterior dislocation is the most common and is usually the result of an indirect force that places the shoulder in extreme external rotation. Posterior dislocations usually occur as a result of trauma. A superior dislocation is rare and usually the result of an extreme forward and upward force on an adducted arm. Inferior displacement is often seen in persons with neurologic injuries of the brachial plexus and is believed to be caused by stretching of the supporting muscles or by joint effusion.

Figure 42-5 Displaced fracture. X-ray showing a displaced fracture of the base of the first metacarpal, also known as a Bennett fracture.
Traumatic dislocation of the elbow joint is common in the immature skeleton. In adults an elbow dislocation is usually associated with a fracture of the ulna or head of the radius. Posterior dislocations occur when the individual falls on an outstretched hand with the elbow extended. Anterior dislocations are usually the result of a direct blow to the flexed elbow.
Traumatic dislocation of the wrist usually involves the distal ulna and carpal bones. Any one of the eight carpal bones can be dislocated after an injury. The most common cause is a fall on the hyperextended hand.
Dislocation in the hand usually involves the metacarpophalangeal and interphalangeal joints. Dislocation of the metacarpophalangeal joint is often the result of a fall on the outstretched hand that forces the joint into hyperextension. Dislocation of the interphalangeal joint occurs as a result of injury to the fingers in a hyperextended position.
Considerable trauma is needed to dislocate the hip. Anterior hip dislocation is rather rare and is caused by forced abduction, for example, when an individual lands on the feet from a high fall. Posterior dislocation of the hip can occur in an automobile accident in which the flexed knee strikes the dashboard.
The knee is an unstable joint that depends heavily on the soft tissue structures around it for support. Because the knee is an unstable weight-bearing joint exposed to many different types of motion (flexion, extension, rotation), it is one of the most commonly injured joints. A knee dislocation can be anterior, posterior, lateral, medial, or rotary. It is usually the result of a hyperextension injury that occurs during sports activities.
PATHOPHYSIOLOGY Dislocations and subluxations are often accompanied by fracture because stress is placed on areas of bone not normally subjected to stress. In addition, as the bone separates from the joint, it may bruise or tear adjacent nerves, blood vessels, ligaments, supporting structures, and soft tissue. Dislocation of the shoulder may damage the shoulder capsule and the axillary nerve. Damage to the axillary nerve causes anesthesia in the sensory distribution of the nerve and paralysis of the deltoid muscle. Elbow dislocations are accompanied by torn periosteum, ligaments, and muscle. Bleeding from the damaged periosteum and muscle puts pressure on adjacent arteries that shuts off circulation to and from the forearm and hand. If the pressure is not promptly relieved, ischemic paralysis develops. Dislocations of the hand often result in permanent disability because of damage to the tendons and intricate mechanisms that allow smooth gliding in the joints. Avascular necrosis of the femoral head is a complication seen in hip dislocations. Knee dislocation usually tears both the collateral and cruciate ligaments.
CLINICAL MANIFESTATIONS Signs and symptoms of dislocations or subluxations include pain, swelling, limitation of motion, and joint deformity. Pain may be caused by effusion of inflammatory exudate into the joint or associated tension and ligament injury. Joint deformity is usually caused by muscle contractions that exert pull on the dislocated or subluxated joint or fluid within the joint. Limitation of motion may be a result of effusion into the joint or the displacement of bones.
Tenderness and deformity are prominent in dislocations of the fingers. Unusual muscle pull and pain often result in abnormal posturing of the fingers; for example, the fingers or thumb may be abnormally flexed. A dislocated elbow is often held in a flexed position, and the joint resists active or passive movement. Pain is the key symptom of shoulder injuries. Attempts to lift the arm aggravate the pain. In most shoulder dislocations, the ability to elevate the arm is minimal and the individual supports the injured arm with the opposite hand. Pain and an abnormal gait or limp or inability to bear full weight usually accompany traumatic dislocation of the hip. The pain is constant and severe and is often felt in the inguinal region or thigh. The thigh and leg may assume a position of inward rotation, adduction, or flexion and appear shortened. In a rare anterior dislocation, the limb is not shortened and the joint is fixed in abduction, outward rotation, and flexion.
EVALUATION AND TREATMENT Evaluation of dislocations and subluxations is based on clinical manifestations and roentgenograms. Treatment consists of reduction and immobilization for 2 to 6 weeks and exercises to maintain normal range of motion in the joint. Depending on the joint, healing is usually complete within months to years.
Support Structures
Sprains and Strains of Tendons and Ligaments
Tendon and ligament injuries can accompany fractures and dislocations. A tendon is fibrous connective tissue that attaches skeletal muscle to bone. A ligament is a band of fibrous connective tissue that connects bones where they meet at a joint. Tendons and ligaments support the bones and joints and either facilitate or limit motion. Tendons and ligaments can be torn, ruptured, or completely separated from bone at their points of attachment.
A tear in a tendon is commonly known as a strain. Major trauma can tear or rupture a tendon at any site in the body. Most often injured are the tendons of the hands and feet, the knee (patellar), the upper arm (biceps and triceps), the thigh (quadriceps), the ankle, and the heel (Achilles). Lifting excessive weight with the arms can cause traumatic rupture of the biceps tendon. Rupture of the Achilles tendon occurs when forced dorsiflexion is applied to the foot when it is in plantar flexion. Spontaneous tendon ruptures can occur in individuals receiving local corticosteroid injections, fluoroquinolones, and persons with rheumatoid arthritis or systemic lupus erythematosus.
Ligament tears are commonly known as sprains. Ligament tears and ruptures can occur at any joint but are most common in the wrist, ankle, elbow, and knee joints. A complete separation of a tendon or ligament from its bony attachment site is known as an avulsion. An avulsion is the result of abnormal stress on the ligament or tendon and is commonly seen in young athletes, especially sprinters, hurdlers, and runners.
Strains and sprains are classified as first degree (least severe), second degree, and third degree (most severe).
PATHOPHYSIOLOGY When a tendon or ligament is torn, an extensive cascade of inflammatory processes begins. An inflammatory exudate develops between the torn ends. Later, granulation tissue containing macrophages, fibroblasts, and capillary buds grows inward from the surrounding soft tissue and cartilage to begin the repair process. Within 4 to 5 days after the injury, collagen formation begins. At first, collagen formation is random and disorganized. As the collagen fibers interweave and connect with preexisting tendon fibers, they become organized parallel to the lines of stress. Eventually vascular fibrous tissue fuses the new and surrounding tissues into a single mass. As reorganization takes place, the healing tendon or ligament separates from the surrounding soft tissue. Usually a healing tendon or ligament lacks sufficient strength to withstand strong pull for 4 to 5 weeks after the injury. If strong muscle pull does occur during this time, the tendon or ligament ends may separate again, which causes the tendon or ligament to heal in a lengthened shape with an excessive amount of scar tissue that renders the tendon or ligament functionless. Scar remodeling may take months to years before it is complete.3
CLINICAL MANIFESTATIONS Tendon and ligament injuries are painful and are usually accompanied by soft tissue swelling, changes in tendon or ligament contour, and dislocation or subluxation of bones. The pain is generally sharp and localized, and tenderness persists over the distribution of the tendon or ligament. Painful joint swelling usually can be seen in finger and elbow sprains. Flexion deformities of the fingers and thumb occur in injuries to the extensor tendons. Crepitus may accompany tendon injury in the wrist. Pain in the elbow may be accentuated by flexion, supination, and extension of the elbow or by extension of the wrist. Lifting small objects requires extension of the wrist and therefore aggravates the pain. Tendon injuries in the upper arm cause weakness when the individual tries to flex the forearm. Pain is often the key symptom of shoulder injuries. It may be referred to the deltoid muscle or extend down the arm. The pain is usually aggravated by attempts to lift the arms. Depending on the ligament or tendon involved, tendon and ligament injuries in the knee may produce pronounced immobility, lost lateral movement, instability when walking down stairs, semiflexion, crepitus, or an upward or downward shift of the patella.
EVALUATION AND TREATMENT Evaluation is based on clinical manifestations, stress radiography, arthroscopy, or arthrography. When possible, treatment consists of protecting the involved structures (splinting), early motion, and rehabilitation. Suturing the tendon or ligament ends in close approximation may be necessary to treat complete rupture. If this is not possible because of the extent of damage, tendon or ligament grafting may be necessary. Prolonged rehabilitation exercises help ensure that the patient regains nearly normal functions.
Tendinopathy and Bursitis
Trauma and repetitive stress can cause painful degradation of collagen fibers (tendinosis), inflammation of tendons (tendinitis), or inflammation in bursal sacs (bursitis). The term tendinopathy includes tendinitis, tendinosis, and paratendinitis.4 Other causes of tendinopathy include crystal deposits, postural misalignment, and hypermobility in a joint. Table 42-2 summarizes classes of tendinopathies.
Table 42-2
Histopathologic Classification of Tendon Disorders
| Pathologic Diagnosis | Macroscopic Pathology | Histopathologic Findings |
| Tendinosis | Intratendinous degeneration (commonly due to aging, microtrauma, muscular compromise) | Collagen disorientation, disorganization and fiber separation by an increase in mucoid ground substance, increased preponderance of cells and vascular spaces with or without neovascularization and focal necrosis or calcification |
| Tendinitis | Symptomatic degeneration of the tendon with vascular disruption and inflammatory repair response | Degenerative changes as noted above with superimposed evidence of tear, including fibroblastic and myofibroblastic proliferation, hemorrhage, and organizing granulation tissue |
| Paratenonitis | “Inflammation” of the outer layer of the tendon (paratenon) alone, whether or not the paratenon is lined by synovium | Mucoid degeneration if the areolar tissue is seen. A scattered mild mononuclear infiltrate with or without focal fibrin deposition and fibrinous exudate |
| Paratenonitis with tendinosis | Paratenonitis associated with intratendinous degeneration | Degenerative changes as noted in tendinosis with mucoid degeneration with or without fibrous and scattered inflammatory cells in the paratenon alveolar tissue |
From Maffulli N, Wong J, Almekinders LC: Clin Sports Med 22(4):675-692, 2003.
Epicondylitis is inflammation of a tendon where it attaches to a bone (at its origin). Most tendon pathology, however, is caused by tissue degeneration rather than inflammation. Epicondylar areas of the humerus, radius, or ulna and the area around the knee are most often involved. Lateral epicondylopathy, commonly called tennis elbow, is the result of tissue degeneration or irritation of the extensor carpi radialis brevis tendon at its origin. Medial epicondylopathy, referred to as golfer’s elbow, is a degenerative process of the pronator teres, flexor carpi radialis, and palmaris longus tendons at the medial humeral condyle5 (Figure 42-6). Epicondylopathy is also related to smoking, obesity, and work activities that involve forceful or repetitive cyclic flexion and extension of the elbow, or cyclic pronation, supination, extension, and flexion of the wrist that generates loads to the elbow and forearm region.6
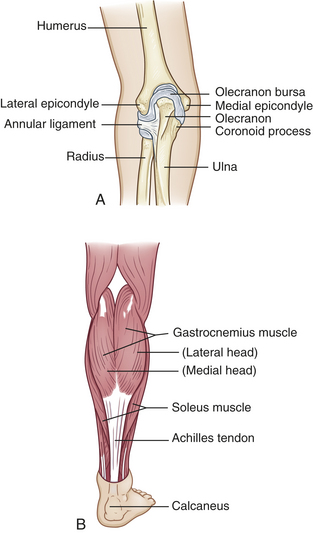
Figure 42-6 Tendinitis and epicondylitis A, Medial or lateral epicondyles of humerus, site of epicondylitis. B, Achilles tendon, site of commonly occurring tendinitis.
Bursae are small sacs lined with synovial membrane and filled with synovial fluid; they are located between tendons, muscles, and bony prominences. Their primary function is to separate, lubricate, and cushion these structures. Acute bursitis occurs primarily in the middle years and is caused by trauma. Chronic bursitis can result from repeated trauma. Septic bursitis is caused by wound infection or bacterial infection of the skin overlying the bursae. Bursitis commonly occurs in the shoulder, hip, knee, and elbow.
PATHOPHYSIOLOGY In tendinitis, fluid from inflammation accumulates, causing swelling of the tendon and its enclosing sheath. Inflammatory changes cause thickening of the sheath, which limits movements and causes pain. Microtears cause bleeding, edema, and pain in the involved tendons or surrounding structures. At times, after repeated inflammations, calcium may be deposited in the tendon origin area, causing a calcific tendinitis.
The usual bursitis is an inflammation that is reactive to overuse or excessive pressure. The inflamed bursal sac becomes engorged, and the inflammation can spread to adjacent tissues (Figure 42-7). The inflammation may decrease with rest, heat, and aspiration of the fluid. (Inflammation is discussed in Chapter 6.)

Figure 42-7 Olecranon bursa. A case of olecranon bursitis in a patient with rheumatoid arthritis. A rheumatoid nodule is also shown. (From Klippel JH, Deippe PA, editors: Rheumatology, ed 2, London, 1998, Mosby-Wolfe.)
CLINICAL MANIFESTATIONS Tendinopathy may be asymptomatic, but generally there is localized pain that worsens with active more than passive motion. With symptomatic tendinopathy, the pain is localized over the involved tendon and movement in the affected joint is limited. In bursitis, onset of pain may be gradual or sudden, and movement in the joint is, itself, normal. Shoulder bursitis impairs arm abduction because of pain and swelling of the bursa. Bursitis in the knee produces pain when climbing stairs, and crossing the legs is painful in bursitis of the hip. Lying on the side of the inflamed trochanteric bursa is also very painful. Table 42-3 summarizes common sites of bursitis. Signs of infectious bursitis may include the presence of a puncture site, prior corticosteroid injection, severe inflammation, or an adjacent source of infection.
Table 42-3
Common Sites and Causes of Bursitis
| Site | Common Causes |
| Shoulder (subacromial) | Repetitive overhead activities |
| Elbow (olecranon) | Rheumatoid arthritis (RA), gout, tuberculosis, leaning on elbow |
| Hip (greater trochanter) | Acute trauma, chronic stress |
| Ischial (weaver’s bottom) | Overuse (runner, ballet dancers), lumbosacral disease, RA, osteoarthritis (OA) |
| Knee | |
| Prepatellar (housemaid’s knee) | Trauma, frequent kneeling, infection |
| Pes anserine (medial knee) | Obesity, long-distance runner, OA, type 2 diabetes |
| Heel (calcaneal) | Poorly fitting footwear, Achilles tendinitis |
EVALUATION AND TREATMENT Evaluation of tendinopathy, epicondylopathy, and bursitis is based on clinical manifestations, physical examination, arthroscopy, arthrography, ultrasound, and possibly magnetic resonance imaging (MRI). Treatment includes systemic analgesics, ice or heat applications, or local injection of an anesthetic and a corticosteroid to reduce inflammation. Physical therapy to prevent loss of function begins after acute symptoms subside.
Muscle Strains
Mild injury such as muscle strain is usually seen after traumatic or sports injuries. Muscle strain is a general term for local muscle damage. It is often the result of sudden, forced motion causing the muscle to become stretched beyond normal capacity. Strains often involve the tendon as well. Muscles are ruptured more often than tendons in young people; the opposite is true in older adults. Muscle strain may be chronic when the muscle is repeatedly stretched beyond its usual capacity. There is evidence of tissue disruption with subsequent signs of muscle regeneration and connective tissue repair when a biopsy is performed. Hemorrhage into the surrounding tissue and signs of inflammation also may be present. Knife and gunshot wounds also cause traumatic rupture. Regardless of the cause of trauma, muscle cells usually can regenerate. Regeneration may take up to 6 weeks, and the affected muscle should be protected during this time. Types of muscle strain, together with their manifestations and treatment, are summarized in Table 42-4.
Table 42-4
| Type | Manifestations | Treatment |
| First degree (e.g., bench press in untrained athlete) | Muscle overstretched, painful | Ice should be applied 5 or 6 times in the first 24-48 hours; complete rest for up to 2 weeks, followed by weightbearing 3 times per week and range of motion daily |
| Second degree (e.g., any muscle strain with bruising and pain) | Muscle intact with some tearing pain, mild bruising; fascia is intact | Treatment similar to that for first-degree strains, with added mild analgesia; cryokinetics (a treatment system of alternating applications of cold with progressive exercise) |
| Third degree (e.g., traumatic injury) | Caused by tearing of fascia; muscle rupture palpable, bleeding present | Surgery to approximate ruptured edges; immobilization and rest for 6 weeks, followed by an individualized rehabilitation regimen of strengthening exercises |
A late complication of localized muscle injury is myositis ossificans. Its true etiology is usually unknown.7 This condition is thought to be caused by scar tissue calcification and subsequent ossification. Examples include “rider’s bone,” in which the adductor muscle of the thigh of equestrians becomes calcified, as well as in football players after muscle injury to thigh muscles; and “drill bone,” in which the same complication is seen in the deltoid and pectoral muscles of fencers and infantry soldiers.
Rhabdomyolysis
Rhabdomyolysis, or myoglobinuria, can be a life-threatening complication of severe muscle trauma with muscle cell loss. Myoglobinuria is named for the principal manifestation of the condition—an excess of myoglobin (an intracellular muscle protein) in the urine. Muscle cell damage releases the myoglobin. The most severe form is often called crush syndrome. Less severe and more localized forms of muscle damage are called compartment syndromes, which can lead to Volkmann ischemic contracture in the forearm or leg. Crush syndrome first gained notoriety in the reports of injuries seen after the London air raids in World War II. More recently it has been reported in individuals found unresponsive and immobile for long periods, often after a drug or alcohol overdose. Other causes of rhabdomyolysis include malignant hyperthermia, infection, herbal medicines, snakebite, cowfish ingestion, cocaine inhalation, hypernatremia, fire ant bites, and venlafaxine.8–10 Rhabdomyolysis also can be seen after viral infections, administration of certain anesthetic agents, or some cholesterol-lowering agents known as “statins,” strychnine poisoning, tetanus, heat stroke, electrolyte disturbances, and fractures. Strains themselves may or may not lead to rhabdomyolysis, but drug interactions involving statins have been implicated.11–12 Excessive muscular activity also has been implicated in reports of myoglobinuria in athletes, such as long-distance runners, ice skaters, skiers, military recruits, and those subjected to fraternity hazing. Status epilepticus, electroconvulsive therapy, and high-voltage electrical shock are also associated with severe and sometimes fatal myoglobinuria. Box 42-1 summarizes some of these risk factors for rhabdomyolysis.
If the myoglobinuria is caused by fulminant malignant hyperthermia, severe muscle spasm and rhabdomyolysis can lead to renal failure. Other complications include intraoperative rigidity, tachycardia, cardiac dysrhythmias, metabolic and respiratory acidosis, and temperature elevations up to 43° C (109.4° F), which can occur very rapidly. Cerebral edema, cardiogenic and hypovolemic shock, pulmonary edema, and disseminated intravascular clotting can contribute to the death of an individual with malignant hyperthermia.
PATHOPHYSIOLOGY The weight of a limp extremity can generate enough pressure to produce muscle ischemia (Figure 42-8). This causes edema, rising compartment pressure, and tamponade that leads to muscle infarction and neural injury and, finally, results in cell loss. Physical interruptions in the sarcolemmal membrane, called holes or delta lesions, suggest that the sarcolemmal membrane may be the route by which muscle constituents are released. (The sarcolemmal membrane, the plasma membrane [including creatine kinase, myoglobin, and phosphate] of the muscle cell, is described in Chapter 41.)
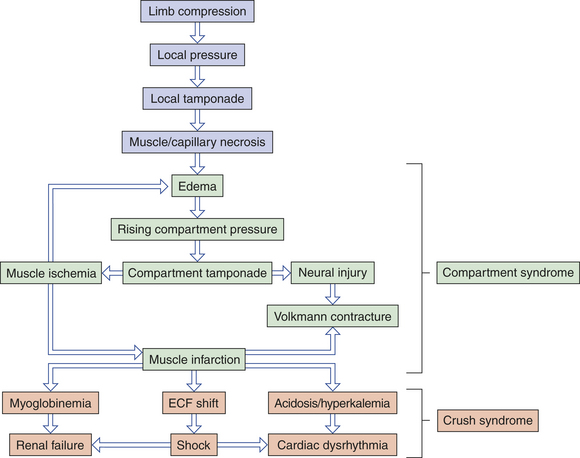
Figure 42-8 Pathogenesis of compartment syndrome and crush syndrome caused by prolonged muscle compression. ECF, Extracellular fluid.
CLINICAL MANIFESTATIONS When myoglobin is released from the muscle cells into the circulation, it can cause a visible, dark reddish brown pigmentation of the urine. The renal threshold for myoglobin is low, approximately 0.5 mg/dl of urine, so that only 200 g of muscle need be damaged to cause visible changes in the urine. Along with the release of myoglobin, creatine kinase (CK) and other serum enzymes are released in massive quantities. The CK level is often 100 times greater than normal (5 to 25 units/ml for women and 5 to 35 units/ml for men). The efflux of proteins and enzymes also includes loss of potassium, phosphate, nucleotides, creatinine, and creatine. Serum hypocalcemia is seen early in the course of myoglobinuria and is followed by late hypercalcemia.
EVALUATION AND TREATMENT Careful and thorough preoperative assessment should alert the anesthesiologist to the possibility of a susceptible individual. A family history of anesthetic problems and previous untoward anesthetic experiences (muscle cramping, unexplained fevers, dark urine) are criteria that require further clarification before administration of a volatile anesthetic.
Priorities in treatment of myoglobinuria include identifying and treating the underlying disorder and preventing life-threatening renal failure. Malignant hyperthermia and myoglobinuria caused by succinylcholine or volatile anesthetic agents can be treated by halting the anesthetic administration and infusing dantrolene sodium (Dantrium). Diluting myoglobin using intravenous fluids and administration of diuretics to “flush” the kidney have been advocated to prevent renal failure. Correction of any electrolyte imbalance also is important. Other secondary problems include electrolyte imbalance, volume depletion, acidosis, hyperuricemia, hyperkalemia, and calcium imbalance. These require specific treatment. Short-term dialysis also may be necessary.
Compartment syndromes may require emergency treatment when blood flow to the affected extremity is compromised because of increased venous pressure, leading to decreased arterial inflow, ischemia, and edema. When clinical evaluation is inconclusive, the rising compartment pressure can be directly measured by inserting a wick catheter, needle, or slit catheter into the muscle. Immediate fasciotomy and débridement have been advocated for elevated intracompartmental pressures.13 Compartments frequently affected are the compartments of the leg, the volar compartment of the hand, and the gluteal compartments.
DISORDERS OF BONES
Metabolic bone disease is characterized by abnormal bone structure that is caused by altered or inadequate biochemical reactions. The altered or inadequate biochemical reactions may be attributable to genetics, diet, or hormones.
Osteoporosis
Osteoporosis, or porous bone, is a disease in which bone tissue is normally mineralized but the mass—density of bone—is decreased and the structural integrity of trabecular bone is impaired. There are two types of osteoporosis. Type 1, or primary osteoporosis, can be further subdivided into postmenopausal or senile types. Senile osteoporosis occurs after age 70. Type 2, or secondary osteoporosis, is caused by other etiologies, such as disease or drugs. Cortical bone becomes more porous and thinner, making bone weaker and prone to fractures (Figure 42-9). The World Health Organization (WHO) has defined osteoporosis based on bone density:

Figure 42-9 Vertebral body. Osteoporotic vertebra (right) shortened by compression fractures compared with normal vertebral body (left). Note that the osteoporotic vertebra has characteristic loss of horizontal trabeculae and thickened vertebral trabeculae. (From Kumar et al: Robbins & Cotran pathologic basis of disease, ed 7, Philadelphia, 2005, Saunders.)
1. Normal bone is greater than 833 mg/cm2
Severe or established osteoporosis is identified when there has been a fragility fracture. The disease can be (1) generalized, involving major portions of the axial skeleton, or (2) regional, involving one segment of the appendicular skeleton.
Throughout a lifetime, old bone is removed (resorption) and new bone is added (formation) to the skeleton. During childhood and teenage years, new bone is added faster than old bone is removed. Consequently, bones become larger, heavier, and denser. Bone formation continues at a pace faster than resorption until peak bone mass, or maximum bone density and strength, is reached, around age 30, after which bone resorption slowly exceeds bone formation. In women, bone loss is most rapid in the first years after menopause but persists throughout the postmenopausal years. Bone loss in women begins before menopause. The WHO recently redefined the approach to evaluating, treating, and preventing fractures associated with low bone density. Rather than diagnosing osteoporosis solely on low bone mass, worldwide efforts are being directed toward individualized assessment of a 10-year fracture risk.14 An estimated 10 million Americans older than age 50 have osteoporosis, and 34 million are at risk.15 The major risks for persons with osteoporosis are fractures. Men lose bone density with aging but because they begin with a higher bone density, they reach osteoporotic levels at an older age than do women. Osteoporotic fractures affect 1 in 2 women and 1 in 5 men older than the age of 50.16
Vertebral fractures are the most common osteoporotic fracture but may be asymptomatic.17 Even if the fracture does not cause pain, vertebral fractures can cause deformity, reduced pulmonary function, and loss of height. The degree of compression necessary to define a vertebral fracture has not been standardized. Thus the true prevalence is unknown, but fractures do increase in frequency by the sixth and seventh decades. Vertebral fracture prevalence in men is close to that in women.18
Osteoporosis is most common in white and Asian women, but affects all races. Whites are more susceptible than other races to osteoporosis caused by loss of bone density with age. Blacks have only about half the fracture of whites, probably related to their higher peak bone mass.19,20 The cause of generalized osteoporosis remains uncertain but is probably multifactorial (see following).
Bone quality is not just bone mass (as measured by bone density) but also the microarchitecture of the bone. Thus other variables include crystal size and shape, brittleness, vitality of the bone cells, structure of the bone proteins, integrity of the trabecular network, and the ability to repair tiny cracks.18 Because bone density relates to quantity of bone, quality of the bone is not accurately identified by bone density testing. Therefore, bone density testing may or may not accurately identify those who will go on to develop a fracture.
Osteoporosis is a complex, multifactorial chronic disease that often progresses silently for decades until fractures occur. It is the most common disease that affects bone. It is not necessarily a consequence of the aging process because some older adults retain strong, relatively dense bones.21 In osteoporosis, the old bone is being reabsorbed faster than new bone is being made, causing the bones to lose density, becoming thinner and more porous. A progressive loss of bone mass may continue until the skeleton is no longer strong enough to support itself. Eventually, bones can fracture spontaneously. As bone becomes more fragile, falls or bumps that would not have caused fracture previously at that point do cause a fracture.
Postmenopausal osteoporosis—which occurs in middle-aged and older women is probably caused by changes in osteoprotegerin, (see Pathophysiology) insulin-like growth factor (IGF), a combination of inadequate dietary calcium intake and lack of vitamin D, possibly decreased magnesium, lack of exercise, decreased levels of estrogen, and family history. IGF is known to help in fracture healing and collagen synthesis and improves conditions for bone mineralization. IGF levels significantly decline by age 60. Excessive phosphorus intake, chiefly through the intake of sodas and junk foods interferes with the calcium-phosphorus balance, resulting in an increased risk of brittle bones.
Sex hormones, especially estrogen and testosterone, are significant in premenopausal bone maintenance; however, when estrogen levels drop after menopause, it appears that circulating androgens become significant effectors on bone metabolism. In clinical studies of women, data have suggested that serum androgens influence bone density in pre-, peri-, and postmenopausal women.22,23 Androgens (i.e., testosterone and dihydrotestosterone) have long been recognized to stimulate bone formation. Testosterone is converted to estradiol by the enzyme aromatase. Increasing age in men and women is associated with declining levels of estrogen. In addition, progesterone deficiency may be related to osteoporosis. Decreases in weight-bearing exercise are associated with osteoporosis. Other risk factors are identified in Box 42-2.
Poor nutrition and insufficient intake or malabsorption of dietary minerals, particularly calcium, are factors in the development of osteoporosis.24 Calcium absorption from the intestine decreases with age, and studies of individuals with osteoporosis show that their calcium intake is lower than that of age-matched controls. Deficiencies of vitamins, particularly vitamins C and D, also contribute to bone loss.
Skeletal homeostasis depends on a very narrow range of plasma calcium and phosphate concentrations, which are maintained by the endocrine system. Therefore, endocrine dysfunction ultimately can cause metabolic bone disease. In addition to declining levels of sex steroids, the hormones most commonly associated with osteoporosis are parathyroid hormone, cortisol, thyroid hormone, and growth hormone. Excessive intakes of caffeine, alcohol, and nicotine along with
low body fat have been considered risk factors. In addition, significant differences in the trace elements (zinc, copper, manganese) were noted in the bones and hair of unaffected individuals compared with those with osteoporosis25 (see Nutrition & Disease: Trace Elements and Their Effects on Skeletal Tissue). Development of selective androgen receptor modulators (SARMs) promises novel treatment for osteoporosis through increasing bone formation and building more muscle mass. By selectively affecting bone, muscle mass, and other desired sites while not affecting lipid or estrogen levels or blood pressure, side effects can be controlled.26
Secondary osteoporosis sometimes develops temporarily in individuals receiving large doses of heparin, perhaps because heparin promotes bone resorption by decreasing collagen synthesis or by increasing collagen breakdown. Osteoporosis caused by heparin therapy usually resolves when therapy ceases. Treatment with other medications may lead to development of osteoporosis, such as the use of glucocorticoid treatment for rheumatoid arthritis. Other medications increasing risk of osteoporosis include lithium, methotrexate, anticonvulsants, cyclophosphamide, and cyclosporine.
One form, transient osteoporosis of the hip, is associated with the third trimester of pregnancy or the immediate postpartum period. However, most transient osteoporosis is a typically self-limiting syndrome affecting the lower extremity joints of middle-aged men. The etiology is unknown and although most cases spontaneously resolve, some occurrences of bone demineralization may be related to osteonecrosis.27–29
Regional osteoporosis—osteoporosis confined to a region or segment of the appendicular skeleton—usually has a known cause. Classic regional osteoporosis is associated with disuse or immobilization of a limb because of fractures, motor paralysis, or bone or joint inflammation (see Figure 42-13). A negative calcium balance develops early and continues throughout the period of immobilization. After 8 weeks of immobilization, significant osteoporosis is present, although it may develop earlier in persons younger than 20 years or older than 50 years. A uniform distribution of osteoporosis also has been observed in astronauts and in individuals treated with air suspension therapy as a result of weightlessness and lack of mechanical strain.
PATHOPHYSIOLOGY Whatever the cause, osteoporosis develops when the remodeling cycle—the process of bone resorption and bone formation—is disrupted, leading to an imbalance in the coupling process. Osteoclasts are differentiated cells that function to resorb bone. The explosion of new information in the field of bone biology has led to new understanding of osteoclast biology and bone pathophysiology. The osteoclast differentiation pathway is directed by a series of processes that include proliferation, differentiation, fusion, and activation.30 These processes are controlled by hormones and cytokines and paracrine stromal-cell microenvironment interactions. Thus the intercellular communication in bone and the key molecular regulators are necessary for bone homeostasis. Interleukins (IL-1, IL-4, IL-6, IL-7, IL-11, IL-17), tumor necrosis factor (TNF), transforming growth factor-beta (TGF-β), prostaglandin E2, and hormones interact to control osteoclasts30 (Figure 42-10). Staggering in its importance is the recent identification of the cytokine receptor activator of nuclear factor kβ ligand (RANKL), its receptor RANK, and its decoy receptor osteoprotegerin (OPG); this has led to a tremendously increased understanding of osteoclast biology and pathogenesis of bone diseases.
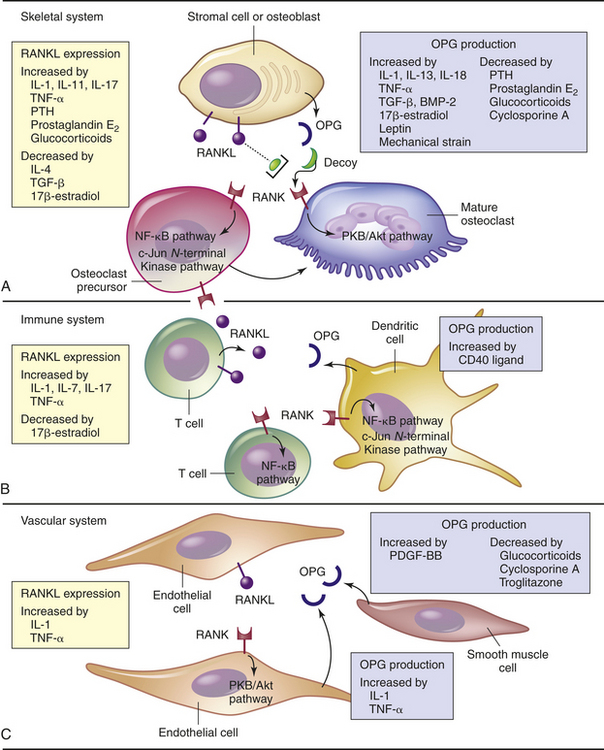
Figure 42-10 OPG/RANKL/RANK system. Receptor activator of nuclear factor кβ ligand (RANKL), a cytokine and part of the tumor necrosis factor (TNF) family, expression and osteoprotegerin (OPG), a glycoprotein receptor antagonist, are modulated by various cytokines, hormones, drugs, and mechanical strains (see inserts). A, In bone, RANKL is expressed by both stromal cells and osteoblasts. RANKL stimulates the receptor RANK on osteoclast precursor cells and mature osteoclasts, activates intracellular signaling pathways to promote osteoclast differentiation and activation and cytoskeletal reorganization and survival (PKB/Akt pathway) that increases resorption and bone loss. OPG, secreted by stromal cells and osteoblasts, acts as a “decoy” receptor and blocks RANKL binding to and activating RANK. B, In the immune system, RANKL is expressed and secreted by T cells. T-cell–derived RANKL also can activate RANK on osteoclasts, T cells, and dendritic cells (antigen-presenting cells), which enhances bone loss that occurs in inflammatory bone diseases such as rheumatoid arthritis. Dendritic cells may regulate these processes by secreting OPG. C, In the vascular system, endothelial cells express RANKL and the RANK receptor. RANKL/RANK interactions contribute to endothelial and smooth muscle cells and can block RANKL binding. The physiologic significance of the OPG/RANKL/RANK system in endothelial and smooth muscle cells is being studied. BMP-2, Bone morphogenic protein 2; IL, interleukin, PDGF-BB, platelet-derived growth factor beta polypeptide; PTH, parathyroid hormone; TGF-β transforming growth factor-beta. (Adapted from Hofbauer LC, Schoppet M: JAMA 292[4]:490-495, 2004.)
RANKL, a member of the TNF family, is expressed by osteoblasts and their immature precursors and is necessary for osteoclast development. RANKL activates the receptor RANK, which is expressed on osteoclasts and their precursors and suppresses apoptosis, which leads to activation and prolongation of osteoclast survival.31 The effects of RANKL are blocked by OPG, which is a glycoprotein that acts as a decoy or soluble receptor antagonist for RANKL that prevents it from binding and activating RANK (see Figure 42-10). The balance between RANKL and OPG is regulated by cytokines and hormones, and alterations of the RANKL/RANK/OPG system can lead to dysregulation and pathologic conditions including osteoporosis, immune-mediated bone diseases, malignant bone disorders, and inherited skeletal diseases (see Figure 42-10).
Postmenopausal osteoporosis is characterized by increased bone resorption relative to the rate of bone formation, leading to sustained bone loss resulting from estrogen deficiency. Bone loss resulting from estrogen deficiency also contributes to osteoporosis in men.32 The increase in bone resorption results from increased development of osteoclasts and decreased osteoclast apoptosis. Evidence involving the OPG/RANKL/RANK system is emerging (see Figure 42-10). OPG production is stimulated by estrogens and the drug referred to as a selective estrogen receptor modulator (SERM), raloxifene.30 Unlike normal bone remodeling whereby osteoblast development is stimulated by factors released from bone marrow stromal cells during osteoclastic resorption, estrogen deficiency unleashes signals capable of stimulating osteoblast progenitor cells that are different from those needed to stimulate bone resorption and thus are pathologic. Postmenopausal women express higher levels of RANKL on bone marrow stromal cells, T cells, and B cells than premenopausal women. Importantly, RANKL expression is inversely correlated with serum level of 17 β-estradiol, that is, with estradiol deficiency, RANKL is increased. Despite numerous studies, it is still unclear which paracrine mediators of the increased osteoclastogenic activity are induced by estrogen deficiency.
Recently, data revealed that sex steroids (e.g., estrogens) exert antiapoptotic effects on osteoblasts but exert proapoptotic effects on osteoclasts; in both scenarios this is accomplished by activating the extracellular signal regulated kinases (ERKs). Estrogen activates ERKs outside the nucleus; ERKs then accumulate in the nucleus and activate downstream transcription factors.33 This confusing and complicated data eventually revealed that the important determinant of whether proapoptosis or antiapoptosis was exhibited was the length of time that the phosphorylated ERKs remained in the nucleus. Prolonged nuclear accumulation of activated ERKs converted the antiapoptotic effect of estradiol to proapoptotic. In addition to ERKs, RANKL is required for the antiapoptotic and thus longer life span of osteoclasts.34 These effects increase the life span of osteoclasts (i.e., longer bone resorbing) and shorten the life span of the bone-forming cells, or osteoblasts. Wnt signaling induces a biochemical series of events that increases osteoblast and bone formation.31 These alterations account for critical pathophysiologic changes in most acquired metabolic bone diseases including postmenopausal osteoporosis, aging effects, and glucocorticoid (i.e., cortisone) excess. In addition agents such as parathyroid hormone and bisphosphonates, used for treatment of bone loss, exert their positive effects by altering the rate of birth of new osteoblasts or osteoclasts or osteoclast apoptosis.
Glucocorticoid (e.g., cortisone)-induced osteoporosis is characterized by increased bone resorption and decreased bone formation. Glucocorticoids increase RANKL expression and inhibit OPG production by osteoblasts (see Figure 42-10). The use of immunosuppressive drugs (i.e., cyclosporine A) to reduce rejection of transplanted organs also alters the OPG/RANKL/RANK system and can lead to posttransplantation osteoporosis. Other conditions affected by OPG/RANKL/RANK include rheumatoid arthritis, myeloma, and skeletal metastases from neoplastic disorders, vascular diseases, and others.
Age-related bone loss begins in the fourth decade. The cause remains unclear, but it is known that decreased serum growth hormone (GH) and IGF levels along with increased binding of RANKL and decreased OPG affect osteoblast and osteoclast function. Loss of trabecular bone in men proceeds in a linear fashion, with thinning of trabecular bone rather than complete loss as is noted in women (Figure 42-11). Men have approximately 30% more bone mass than women, which may be a factor in their later involvement with osteoporosis (Figure 42-12). Androgens promote osteoprotegerin production, thus inhibiting the osteoclastic effect of RANKL.35 Reduction in physical activity in older persons also may be a major factor in the degree of bone loss because preservation of bone mass depends on skeletal stress (mechanical) through muscle contraction and weightbearing.36
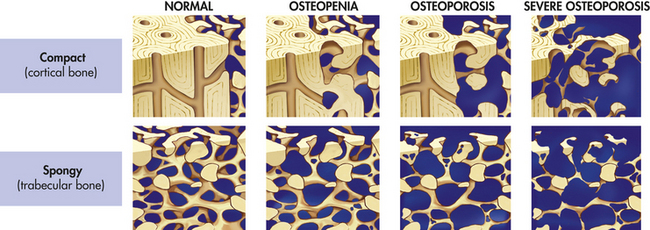
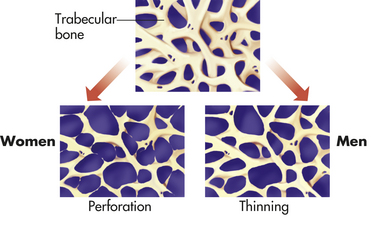
Figure 42-12 Mechanism of loss of trabecular bone in women and trabecular thinning in men. Bone thinning predominates in men because of reduced bone formation. Loss of connectivity and complete trabecular loss predominates in women.
CLINICAL MANIFESTATIONS The specific clinical manifestations of osteoporosis depend on the bones involved. The most common manifestation, however, is bone deformity. Pain tends to occur only when there is a fragility fracture. Fractures are likely to occur because the trabeculae of spongy bone become thin and sparse and compact bone becomes porous. As the bones lose volume, they become brittle and weak and may collapse or become misshapen. Vertebral collapse causes kyphosis (hunchback) and diminished height (Figure 42-13). Fractures of the long bones (particularly the femur and humerus), distal radius, ribs, and vertebrae are most common. Fracture of the neck of the femur—the so-called broken hip—tends to occur in older or older adult women with osteoporosis. Fatal complications of fractures include fat or pulmonary embolism, hemorrhage, and shock. Approximately 20% of persons with a hip fracture may die as a result of surgical complications.
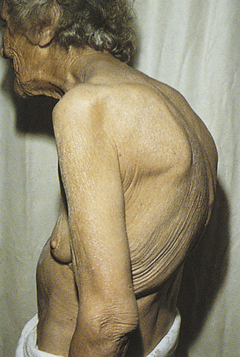
Figure 42-13 Kyphosis. This older adult woman’s condition was caused by a combination of spinal osteoporotic vertebral collapse and chronic degenerative changes in the vertebral column. (From Kamal A, Brocklehurst JC: Color atlas of geriatric medicine, ed 2, St Louis, 1992, Mosby.)
EVALUATION AND TREATMENT Generally, osteoporosis is detected radiographically as increased radiolucency of bone. By the time abnormalities are detected by x-ray examination, as much as 25% to 30% of bone tissue may have been lost.
Types of radiologic examinations include single- or dual-photon absorptiometry (SXA, DXA) and computed tomography (CT) scans (Figure 42-14). Because osteoporosis is asymptomatic unless a fracture occurs, diagnosis is often delayed. At present, DXA is the current examination of choice for diagnosis. Unfortunately, DXA does not provide information about bone strength or fracture risk.37
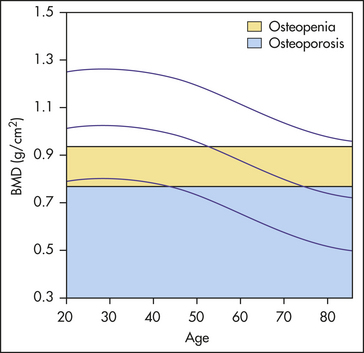
Figure 42-14 Lumbar spine bone mass density (BMD). The normal female reference curves for lumbar spine BMD are plotted in this graph to include the World Health Organization definitions of osteopenia and osteoporosis. (Redrawn from Collier BD, Fogelman I, Rosenthall L: Skeletal nuclear medicine, St Louis, 1996, Mosby.)
Because fractures are the problem with osteoporosis, the WHO has developed an assessment tool to estimate an individual’s 10-year risk of fracture. The WHO’s Fracture Risk Assessment (FRAX) is a downloadable computer-drive questionnaire that has been developed for use in Europe, North America, Asia, and Australia. Once completed, the imbedded algorithms predict the 10-year probability of hip, spine, forearm, or shoulder fractures. This tool can be downloaded from www.shef.ac.uk/FRAX. Other evaluation procedures include tests for levels of serum calcium, phosphorus, and alkaline phosphatase and protein electrophoresis. Body calcium levels also can be measured by neuron activation analysis, a procedure involving use of radioactive calcium-49, whose gamma activity can be measured with a whole-body counter.
The goals of osteoporosis treatment are to slow down the rate of calcium and bone loss and to stop the disease before it progresses too far. Controversial is the role of calcium intake to prevent and treat osteoporosis. It is well accepted that oral calcium intake sufficient to maintain normal calcium balance is necessary during adolescence to ensure development of peak bone mass, and that calcium-deficient diets can aggravate bone loss associated with menopause and aging. Although recommendations have been established for young women of 1000 mg of calcium daily and for postmenopausal women of 1500 mg daily (with vitamin D) if receiving sex hormone replacement therapy, it has been difficult to translate these recommendations into clear-cut clinical outcomes. A significant relationship has been observed between an individual’s lifetime history of calcium intake and peak bone mineral density. Clinical trials must be done to test the effects of dietary calcium or supplements on bone loss that accounts for potential confounding factors, such as menopausal status, estrogen levels, vitamin D levels (see Nutrition and Disease: Vitamin D and Fracture Risk), magnesium levels, smoking, contraceptive use, usual calcium intake, and level of physical activity.
Magnesium (Mg++), another mineral important for skeletal development, is an essential mineral in many biochemical and physiologic functions, including activation of enzymes, involvement in adenosine triphosphate (ATP) synthesis, protein synthesis, regulation of membrane channels, and muscle contraction. New evidence suggests that large fluxes of magnesium can cross the cell plasma membrane in either direction following a variety of stimuli, resulting in a modification of activity for several cellular enzymes. Mg++ is important to bone quality because it controls hydroxyapatite crystal growth and thereby prevents formation of brittle bones. It seems reasonable that Mg++ is required for normal calcium (Ca++) absorption because severe Mg++ deficiency results in hypocalcemia. Elevation of plasma Mg++ or Ca++ concentration inhibits Mg++ and Ca++ resorption, leading to hypermagnesiuria and hypercalciuria. An extracellular Ca++/Mg++ sensing receptor has been found located on distal tubule
cells. Also data have shown a relationship between Mg++ and Ca++ signaling in pancreatic and other secretory epithelia. Significant extrusion of Mg++ from these cells is related to mobilization of intracellular Ca++.38
Regular, moderate weight-bearing exercise can slow down the bone loss and, in some cases, reverse demineralization because the mechanical stress of exercise stimulates bone formation. Vitamin D and Mg++ also may be recommended. It is important to reduce the risk of falls and enhance bone quality. Therefore, an exercise program to enhance muscle strength is advised. Important new findings suggest that estrogen may prevent excessive bone loss before and after menopause by limiting osteoclast life span through promotion of apoptosis. Hormone replacement therapy helps maintain bone density but it is not routinely recommended because of the increased risk of stroke and breast cancer and no significant cardioprotective effects.
SERMs and SARMs have been developed to provide the positive effects of estrogen on bone but minimize estrogen’s negative effect on breast and endometrial tissues. Raloxifene and tamoxifen are examples of SERMs.
The bisphosphonates alendronate and risedronate have been effective in reducing hip and vertebral fractures in glucocorticoid-induced osteoporosis and in women with osteoporosis by inhibiting bone resorption. Recent evidence reveals the bisphosphonates activate a previously unknown signaling pathway that is triggered by the opening of connexin 43, a protein that forms a gap junction important for intercellular communication. After opening of connexin 43, activation of ERKs (see p. 1582) occurs, which mediates osteocyte survival. Osteocyte viability possibly maintains the effectiveness of bisphosphonates as well as other agents (e.g., estrogen, and daily parathyroid injections) by preventing apoptosis of osteocytes and osteoblasts.33 Two recombinant bone morphogenic proteins (BMPs), BMP-2 and BMP-7, have been used to improve fracture healing and spinal fusions.39 Teriparatide, a biosynthetic form of parathormone, is injected subcutaneously. However, use is limited to a period of 24 months because of the risk of developing osteosarcoma. Men with osteoporosis are treated with bisphosphonates and testosterone. Controversial is testosterone treatment for women. Restoration of a balanced RANKL/OPG ratio (see p. 1580) or inhibiting RANK responsiveness is known to prevent osteoclast activation and bone resorption. Anti-RANKL therapy significantly reduces bone resorption. Denosumab, a monoclonal antibody, is the first of these compounds.34,40
Osteomalacia
Osteomalacia is a metabolic disease characterized by inadequate and delayed mineralization of osteoid in mature compact and spongy bone. In osteomalacia the remodeling cycle proceeds normally through osteoid formation, but mineral calcification and deposition do not occur. Bone volume remains unchanged, but the replaced bone consists of soft osteoid instead of rigid bone. The result is abnormal bone matrix mineralization. Rickets is similar to osteomalacia in pathogenesis, but it occurs in the growing bones of children, whereas osteomalacia occurs in adult bone. Chronically low-serum phosphate level is a major cause of osteomalacia. Fibroblast growth factor-23 (FGF-23) plays a significant role in maintaining normal serum phosphate.41 Primarily produced by osteocytes, FGF-23 functions to inhibit reabsorption of phosphate in the renal proximal tubule.42 (Rickets is described in Chapter 43.)
Osteomalacia and rickets are rare in the United States and Western Europe but are significant health problems in Great Britain, Ethiopia, Pakistan, Iran, and India. In the United States these diseases occur in older adults, in premature infants of very low birth weight, and in individuals adhering to rigid macrobiotic vegetarian diets.
Certain forms of osteomalacia are caused by genetic abnormalities; other forms can be caused by tumors. Many factors contribute to the development of osteomalacia, but the most important is a deficiency of vitamin D. The major risk factors in vitamin D deficiency are diets deficient in vitamin D, decreased endogenous production of vitamin D, intestinal malabsorption of vitamin D, renal tubular diseases, and anticonvulsant therapy. Classic vitamin D deficiency is rare in the United States because of the addition of synthetic vitamin D to dairy products and bread.
However, disorders of the small bowel, hepatobiliary system, and pancreas are common causes of vitamin D deficiency in the United States. In malabsorptive disease of the small bowel, vitamin D and calcium absorption are decreased, so vitamin D is lost in feces. Liver disease interferes with the metabolism of vitamin D to its more active form, and diseases of the pancreas and biliary system cause a deficiency of bile salts, which are necessary for normal intestinal absorption of vitamin D.
The mechanism by which anticonvulsant drug therapy results in vitamin D deficiency is not completely understood, but researchers think that the anticonvulsants phenobarbital and phenytoin interfere with calcium absorption and increase degradation of vitamin D metabolism in the liver.
PATHOPHYSIOLOGY Crystallization of minerals in osteoid requires adequate concentrations of calcium and phosphate. When the concentrations are too low, crystallization (and hence ossification) does not proceed normally.
Vitamin D deficiency disrupts mineralization because vitamin D normally regulates and enhances the absorption of calcium ions from the intestine. A lack of vitamin D causes the plasma calcium concentrations to fall. Low plasma calcium levels stimulate increased synthesis and secretion of parathyroid hormone (PTH). Although the increase in circulating PTH raises the plasma calcium concentration, it also stimulates increased renal clearance of phosphate. When the concentration of phosphate in the bone decreases below a critical level, mineralization cannot proceed normally.
Abnormalities occur in spongy as well as compact bone. Trabeculae in spongy bone become thinner and fewer, whereas haversian systems in compact bone develop large channels and become irregular. Because osteoid continues to be produced but not mineralized, abnormal quantities of osteoid build up, coating the trabeculae and the linings of the haversian canals. Excessive osteoid also can accumulate in areas beneath the periosteum. The excess of osteoid leads to gross deformities of the long bones, spine, pelvis, and skull.
CLINICAL MANIFESTATIONS Osteomalacia causes varying degrees of diffuse skeletal pain and tenderness. Pain is noted particularly in the hips, and the individual may be hesitant to walk. Muscular weakness is common and may contribute to a waddling gait. Bone fractures and vertebral collapse occur with minimal trauma. Low back pain may be an early complaint, but pain also may involve ribs, feet, other areas of the vertebral column, and other sites. Uremia may be present in renal osteodystrophy.
EVALUATION AND TREATMENT Laboratory data may include elevated blood urea nitrogen (BUN) and creatinine levels, normal or low serum calcium levels, and a serum inorganic phosphate level that is usually higher than 5.5 mg. Alkaline phosphatase and PTH levels are usually elevated. Radiographic findings show pseudofractures and radiolucent bands perpendicular to the surface of involved bones. Diagnosis of certain types of osteomalacia is becoming easier because of the ability to measure an individual’s serum FGF-23. Elevated FGF-23 levels are common in X-linked hypophosphatemic and tumor-induced osteomalacia.43,44
Paget Disease
Paget disease (osteitis deformans) is a state of increased metabolic activity in bone characterized by abnormal and excessive bone remodeling, both resorption and formation. Genetic manipulations involving the RANK-NF-Kβ signaling pathway are significant in the development of Paget disease.45 Chronic accelerated remodeling eventually enlarges and softens the affected bones.
Paget disease most often affects the axial skeleton, especially the vertebrae, skull, sacrum, sternum, pelvis, and femur. The disease process may occur in one or more bones without causing significant clinical manifestations.
The disease is seldom found before age 40 years, but its incidence almost doubles each decade from age 50. It affects men more than women in a proportion of 1.8:1.46 Because it is often symptomless and can be diagnosed only by invasive procedures, few epidemiologic data are available. Autopsy data from England and Germany indicate that approximately 3% to 4% of persons older than 40 years have Paget disease. It is most prevalent in Australia, Great Britain, New Zealand, and the United States.
The cause of Paget disease is unknown, but there appears to be a strong genetic component. A viral connection (slow virus infection) to Paget disease also has been proposed.45 Classic Paget disease arises as a consequence of disorderly bone resorption and formation.
PATHOPHYSIOLOGY Paget disease begins with excessive resorption of spongy bone. The trabeculae diminish, and bone marrow is replaced by extremely vascular fibrous tissue.
The resorption phase of Paget disease is followed by the formation of abnormal new bone at an accelerated rate. The collagen fibers are disorganized, and glycoprotein levels in the matrix decrease. Mineralization may extend into the bone marrow. Bone formation is excessive around partially resorbed trabeculae, causing them to thicken and enlarge. Eventually, Paget disease progresses to an inactive phase, in which abnormal remodeling is minimal or absent. Osteoclasts of individuals with Paget disease have increased responses to RANKL.45
CLINICAL MANIFESTATIONS In the skull, abnormal remodeling is first evident in the frontal or occipital regions, then encroaches on the outer and inner surfaces of the entire skull. The skull thickens and assumes an asymmetric shape (Figure 42-15). Thickened segments of the skull may compress areas of the brain, producing altered mentality and dementia. Impingement of new bone on cranial nerves causes sensory abnormalities, impaired motor function, deafness, atrophy of the optic nerve, and obstruction of the lacrimal duct. Headache is commonly noted.
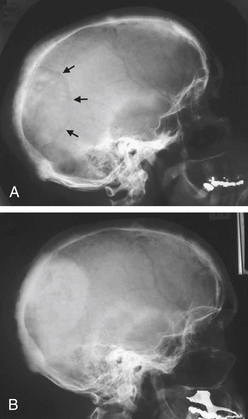
Figure 42-15 Paget disease of the skull A, Active Paget disease of the skull, with marked cortical thickening and an area of osteoporosis circumscripta (arrows). B, The same individual some years later (after bisphosphonate treatment), with the lytic lesion largely replaced by sclerotic bone. (From Walsh JP: Med J Aust 181[5]:263, 2004.)
Extensive alterations of the facial bones are rare except in the jaw, where sclerosis and thickening of the maxilla and mandible displace teeth and produce malocclusion. In long bones, resorption begins in the subchondral regions of the epiphysis and extends into the metaphysis and diaphysis. Warmth over the affected area, bone and joint pain, and bone deformity may occur. Occasionally, Paget disease affects both ends of a tubular bone. In the femur, Paget disease produces an exaggerated lateral curvature. In the tibia, anterior curvature is also exaggerated. Stress fractures are common in the lower extremities.
Clinical manifestations of Paget disease in the vertebral column depend on the level of involvement and are caused by compression of adjacent structures. In the cervical spine, cord compression can lead to spastic quadriplegia. Approximately 1% of persons with Paget disease develop osteogenic sarcoma. Paget-related sarcoma has a poor prognosis.
EVALUATION AND TREATMENT Evaluation of Paget disease is made on the basis of radiographic findings of irregular bone trabeculae with a thickened and disorganized pattern. Early disease is detected by bone scanning that shows increased uptake of bone radionuclides. Alkaline phosphatase and urinary hydroxyproline are elevated.
Most individuals require no treatment because the disease is localized and does not cause symptoms. Treatment during active disease is for pain relief, prevention of deformity, or fracture. Bisphosphonates (alendronate, risedronate, and pamidronate) and calcitonin (salmon and human) are the mainstays of treatment. Surgery is indicated if there are neurologic complications or severe bony deformities.
Infectious Bone Disease: Osteomyelitis
Infectious bone disease is expensive and difficult to treat and often culminates in extensive physical disability. The following factors contribute to the difficulty in treating bone infection:
1. Bone contains multiple microscopic channels that are impermeable to the cells and biochemicals of the body’s natural defenses. Once bacteria gain access to these channels, they are able to proliferate unimpeded.
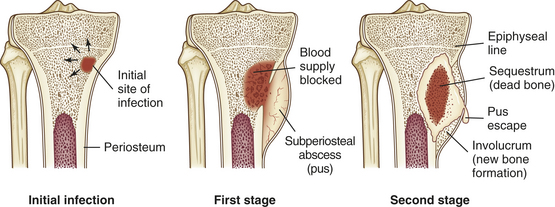
2. The microcirculation of bone is highly vulnerable to damage and destruction by bacterial toxins. Vessel damage causes local thrombosis (blockage) of the small vessels, which leads to ischemic necrosis (death) of bone.
3. Bone cells have a limited capacity to replace bone destroyed by infections. Initially, osteoclasts are stimulated by infection to resorb bone, which opens up isolated bone channels so that cells of the inflammatory and immune system can gain access to the infected bone. At the same time, however, resorption weakens the structural integrity of the bone. New bone formation usually lags behind resorption, and the haversian systems in the new bone are incomplete.
Osteomyelitis is a bone infection most often caused by bacteria; however, fungi, parasites, and viruses also can cause bone infection (Figure 42-16). Exogenous osteomyelitis is an infection that enters from outside the body, for example, through open fractures, penetrating wounds, or surgical procedures. In exogenous osteomyelitis, the infection spreads from soft tissues into adjacent bone. Endogenous (hematogenous) osteomyelitis is caused by pathogens carried in the blood from sites of infection elsewhere in the body. In hematogenous osteomyelitis, the infection spreads from bone to adjacent soft tissues. Hematogenous osteomyelitis is commonly found in infants, children, and older adults. (Osteomyelitis in children is discussed in Chapter 43.) In infants, incidence rates among males and females are approximately equal. In children and older adults, however, males are most commonly affected. Osteomyelitis is a common complication of sickle cell anemia and low oxygen tension.
Staphylococcus aureus is the usual cause of hematogenous osteomyelitis. Other microorganisms include group B streptococci, Haemophilus influenzae, Salmonella, and gram-negative bacteria. Group B streptococci and H. influenzae tend to infect young children; Salmonella infection is associated with sickle cell anemia; and gram-negative infections are most common in older adults and individuals with impaired immunity. Mycobacterial and fungal infections occur in immunocompromised individuals.
Cutaneous, sinus, ear, and dental infections are the primary sources of bacteria in hematogenous bone infections. Soft tissue infections, disorders of the gastrointestinal tract, infections of the genitourinary system, and respiratory infections are also sources of bacterial contamination. In addition, infections contracted after total joint replacements can be causes of osteomyelitis. The vulnerability of specific bone depends on the anatomy of its vascular supply.
In adults, hematogenous osteomyelitis is more common in the spine, pelvis, and small bones. Microorganisms reach the vertebrae through arteries, veins, or lymphatic vessels. The spread of infection from pelvic organs to the vertebrae is well documented. Vaginal, uterine, ovarian, bladder, and intestinal infections can lead to iliac or sacral osteomyelitis.
Exogenous osteomyelitis can be caused by human bites or fist blows to the mouth. Superficial animal or human bites inoculate local soft tissue with bacteria that later spread to underlying bone. Deep bites can introduce microorganisms directly onto bone. The most common infecting organism in human bites is S. aureus. In animal bites the most common infecting organism is Pasteurella multocida, which is part of the normal mouth flora of cats and dogs.
Direct contamination of bones with bacteria also can occur in open fractures or dislocations with an overlying skin wound. Intervertebral disk surgery and operative procedures involving implantation of large foreign objects, such as metallic plates or artificial joints, are associated with exogenous osteomyelitis. Local injections and venous punctures are significant causes of exogenous osteomyelitis. Exogenous osteomyelitis of the arm and hand bones tends to occur in drug abusers. S. aureus is the most common pathogen. In general, persons who are chronically ill, have diabetes or alcoholism, or are receiving large doses of steroids or immunosuppressive drugs are particularly susceptible to exogenous osteomyelitis or recurring episodes of this disease.
PATHOPHYSIOLOGY Regardless of the source of the pathogen, the pathologic features of bone infection are similar to those in any other body tissue (see Chapter 9). First, the invading pathogen provokes an intense inflammatory response. Inflammation in bone is characterized by vascular engorgement, edema, leukocyte activity, and abscess formation. Once inflammation is initiated, the small terminal vessels thrombose and exudate seals the bone’s canaliculi. Inflammatory exudate extends into the metaphysis and the marrow cavity and through small metaphyseal openings into the cortex. In children, exudate that reaches the outer surface of the cortex forms abscesses that lift the periosteum off underlying bone. Lifting of the periosteum disrupts blood vessels that enter bone through the periosteum, which deprives underlying bone of its blood supply; this leads to necrosis and death of the area of bone infected, producing sequestrum, an area of devitalized bone (see Figure 42-16). Lifting of the periosteum also stimulates an intense osteoblastic response. Osteoblasts lay down new bone that can partially or completely surround the infected bone. This layer of new bone surrounding the infected bone is called an involucrum. Openings in the involucrum allow the exudate to escape into surrounding soft tissue and ultimately through the skin by way of sinus tracts.
In adults this complication is rare because the periosteum is firmly attached to the cortex and resists displacement. Instead, infection disrupts and weakens the cortex, which predisposes the bone to pathologic fracture.
CLINICAL MANIFESTATIONS Clinical manifestations of osteomyelitis vary with the age of the individual, the site of involvement, the initiating event, the infecting organism, and whether the infection is acute, subacute, or chronic. Acute osteomyelitis causes an abrupt onset of inflammation. If an acute infection is not completely eliminated, the disease may become subacute or chronic. In subacute osteomyelitis, signs and symptoms are usually vague. In the chronic stage, infection is indolent or silent between exacerbations. The microorganisms persist in small abscesses or fragments of necrotic bone and produce occasional flare-ups of acute osteomyelitis. The progression from acute to subacute osteomyelitis may be the result of inadequate or inappropriate therapy or the development of drug-resistant microorganisms.
In the adult, hematogenous osteomyelitis has an insidious onset. The symptoms are usually vague and include fever, malaise, anorexia, and weight loss. Recent infection (urinary, respiratory, skin) or instrumentation (catheterization, cystoscopy, myelography, diskography) usually precedes onset of symptoms.
The primary symptom of acute osteomyelitis in the spine is back pain.47 The pain may be intermittent or constant, aggravated by motion, and throbbing at rest. It may radiate in a radicular distribution and is commonly accompanied by spinal tenderness and rigidity. Hip contracture can occur in the presence of soft tissue inflammation as a result of irritation of the psoas muscle.
The signs and symptoms of sacroiliac osteomyelitis are generally severe and include local pain, tenderness, and a limp. The pain may radiate to the buttock or the abdomen.
Single or multiple abscesses (Brodie abscesses) characterize subacute or chronic osteomyelitis. Brodie abscesses are circumscribed lesions 1 to 4 cm in diameter, usually in the ends of long bones and surrounded by dense ossified bone matrix. The abscesses are thought to develop when the infectious microorganism has become less virulent or the individual’s immune system is resisting the infection somewhat successfully.
In exogenous osteomyelitis, signs and symptoms of soft tissue infection predominate. Inflammatory exudate in the soft tissues disrupts muscles and supporting structures and forms abscesses. Low-grade fever, lymphadenopathy, local pain, and swelling usually occur within days of contamination by a puncture wound. Osteomyelitis in the hand causes exquisite tenderness over the course of tendon sheaths. The fingers are usually in a semiflexed position, and extension usually causes severe pain. Palmar swelling or symmetric swelling of the fingers may be present.
EVALUATION AND TREATMENT Laboratory data show an elevated white cell count. Radiographic studies include radionuclide bone scanning, CT, and MRI. MRI is especially useful in detecting early bone changes associated with infection.48 Treatment of osteomyelitis includes antibiotics and débridement with bone biopsy and culture. Initial antibiotic therapy should be intravenous. Chronic conditions may require surgical removal of the inflammatory exudate followed by continuous wound irrigation with antibiotic solutions in addition to systemic treatment with antibiotics. Hyperbaric oxygen therapy of 100% oxygen, given at 2 atmospheres of pressure for 2 hours’ duration per day for 30 treatments, is also beneficial for chronic refractory osteomyelitis. Implants for total joint replacements may be removed to treat the infected joint more thoroughly.
Bone Tumors
Many different types of tumors involve the skeleton. Bone tumors may originate from bone cells, cartilage, fibrous tissue, marrow, or vascular tissue. Based on the tissue of origin, bone tumors are classified as osteogenic, chondrogenic, collagenic, and myelogenic. Each of the four types arises from one of the four stem cells that are ultimately derived from the primitive mesoderm (Figure 42-17). In addition, bone tumors may be classified as being of histiocytic, notochordal, lipogenic, and neurogenic origins.
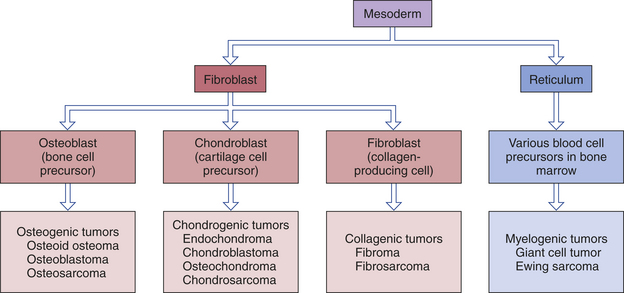
The mesoderm contributes the primitive fibroblast and reticulum cells. The fibroblast is the progenitor of the osteoblast and the chondroblast. Each cell synthesizes a specific type of intercellular ground substance, and the tumor derived from the cell is generally characterized by the type of ground substance produced by the cell. For example, osteogenic tumors usually contain cells that have the appearance of osteoblasts and produce an intercellular substance that can be recognized as osteoid. Chondrogenic tumors contain chondroblasts and produce an intercellular substance similar to chondroid (cartilage). Collagenic tumors contain fibrous tissue cells and produce an intercellular substance similar to the type of collagen found in fibrous connective tissue.
Tumors are also classified as benign or malignant. The criteria used to identify tumor cells as malignant are (1) an increased nuclear/cytoplasmic ratio, (2) an irregular nuclear border, (3) excess chromatin, (4) a prominent nucleolus, and (5) an increase in the number of cells undergoing mitosis. However, many young, rapidly growing, normal cells and cells subjected to inflammation and change in their blood supply also exhibit many of these same characteristics. (Tumor characteristics in general are described in Chapter 11.)
Epidemiology
The incidence of bone tumors varies with age. In children younger than 15 years, the rate of bone tumors is relatively low, constituting approximately 3% of all malignancies. Adolescents have the highest incidence of bone tumors, and adults between 30 and 35 years of age have the lowest incidence. After age 35, the incidence slowly increases until, at age 60, it equals the incidence in adolescents, primarily related to metastatic tumors.
Patterns of Bone Destruction
The general pathologic features of bone tumors include bone destruction, erosion or expansion of the cortex, and periosteal response to changes in underlying bone. The least amount of pathologic damage occurs with benign bone tumors that push against neighboring tissue. Because they usually have a symmetric, controlled growth pattern, benign bone tumors tend to compress and displace neighboring normal bone tissue, which weakens the bone’s structure until it is incapable of withstanding the stress of ordinary use, leading to pathologic fracture. Other tumors invade and destroy adjacent normal bone tissue by producing substances that promote resorption by increasing osteoclast activity or by interfering with a bone’s blood supply.
Three patterns of bone destruction by bone tumors have been identified: (1) the geographic pattern, (2) the moth-eaten pattern, and (3) the permeative pattern (Table 42-5).
Table 42-5
Patterns of Bone Destruction by Bone Tumors
| Type of Destruction | Pattern Seen |
| Geographic | Well-defined margins separated from surrounding normal bone; well-defined lytic area in affected bone |
| Moth-eaten | Less-defined margin not easily separated from normal bone; areas of partially destroyed bone adjacent to completely lytic areas |
| Permeative | Poorly demarcated margins; abnormal lytic bone merges imperceptibly with surrounding normal bone |
Tumors that erode the cortex of the bone usually stimulate a periosteal response, that is, new bone formation at the interface between the surface of the bone and the periosteum. Slow erosion of the cortex usually stimulates a uniform periosteal response. Additional layers of bone are added to the exterior surface of the bone to buttress the cortex. Eventually the additional layers expand the bone’s contour. Aggressive penetration of the cortex usually elevates the periosteum and stimulates erratic patterns of new bone formation. Examples of erratic patterns include concentric layers of new bone; a sunburst pattern, in which delicate rays of new bone radiate toward the periosteum from a single focus on the underlying surface; and rays of new bone that grow perpendicularly, creating a brush or bristle pattern.
Diagnosis
Malignant bone tumors account for less than 0.2% of all cancers. A tumor must be identified early to allow survival of the individual and the preservation of the affected limb. However, individuals often have only vague symptoms that may be attributed to minor trauma, degenerative changes, or inflammatory conditions. In addition, other conditions may obscure the diagnosis.
Thorough diagnostic studies are needed to determine the exact type and extent of bone tumor present, which also helps determine the optimal treatment regimen. Staging of any bone tumor is critical to determine future treatment and results. The Enneking staging system is the most commonly used arrangement (Table 42-6). This system classifies tumors as to grade (G), tumor site (T), and metastasis (M). Benign tumors are given a numeric value of zero, whereas malignant tumors are low grade (G1) or high grade (G2).
Table 42-6
The Ennenking Surgical Staging System for Malignant Bone Tumors

Data from Rosen G et al: Bone tumors. In Bast RC et al, editors: Cancer medicine, ed 5, Hamilton, Ontario, 2000, B.D. Decker.
Serum alkaline phosphatase levels are elevated in bone lytic tumors, and they are significantly elevated in osteosarcoma and Ewing sarcoma. Radiologic studies include plain radiologic films, technetium-99 bone scan, CT scan, and MRI, which has become the examination of choice for the local staging of bone tumors, especially the staging of peripheral osteosarcomas (see Table 42-5). MRI is also used to monitor the response of osteosarcomas to radiation or chemotherapy and to detect recurrent disease. A CT scan can evaluate involvement of osteosarcoma in flat bones when the tumor is not well defined on a plain film, can assist in differentiating the tumor, and can locate pulmonary metastases. Radionucleotide bone scans show an increased uptake at the tumor site.
Additional diagnostic studies performed for specific bone tumors include a complete blood count and erythrocyte sedimentation rate (to rule out infection, myeloma, or Ewing sarcoma) and serum levels of calcium and phosphorus to detect hypercalcemia. Serum glucose levels may be elevated in chondrosarcoma. Acid phosphatase may show moderate elevations in bone metastases, multiple myeloma, and advanced Paget disease. Serum protein electrophoresis and immunoelectrophoresis are done to rule out multiple myeloma. Fine-needle biopsy is done, usually at the time of surgery, to determine the exact tumor type.
Types
A very large number of lesions are classified as bone tumors. The bone tumors most representative of the four derivative types (see Figure 42-17)—osteogenic, chondrogenic, collagenic, and myelogenic tumors—are described here.
Osteogenic Tumors: Osteosarcoma: Osteogenic (bone-forming) tumors are characterized by the formation of bone or osteoid tissue with a sarcomatous tissue. The tissue can have the appearance of compact or spongy bone. The most common malignant primary bone tumor is osteosarcoma. Osteosarcomas account for 38% of bone tumors. The male/female ratio is 3:2, and osteosarcoma occurs predominantly in adolescents and young adults; 60% of osteosarcomas occur in persons younger than 20 years. A secondary peak incidence for osteosarcoma occurs in the 50- to 60-year-old age group, primarily in individuals with a history of radiation therapy several years previously for pelvic or other malignancies (Figure 42-18).
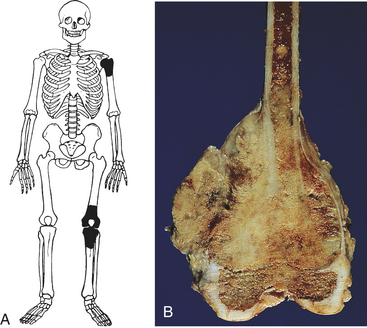
Figure 42-18 Osteosarcoma A, Common locations of osteosarcoma. B, Femur has a large mass involving the metaphysis of the bone; the tumor has destroyed the cortex, forming a soft tissue component. (From Damjanov I, Linder J, editors: Anderson’s pathology, ed 10, St Louis, 1996, Mosby.)
An osteosarcoma is a malignant bone-forming tumor. It is aggressive and most often found in bone marrow; it has a moth-eaten pattern of bone destruction. The borders of the tumor are indistinct and merge into adjacent normal bone. Osteosarcomas always contain osteoid and callus (osteoblastic sarcoma), produced by anaplastic stromal cells, which are atypical, abnormal cells not seen in normal developing bone; they are neither normal nor embryonal. The osteosarcoma also may contain chondroid (cartilage) (chondroblastic sarcoma) and fibrinoid tissue (fibroblastic sarcoma) that may form the bulk of the tumor. The osteoid is deposited in thick masses or “streamers” between the trabeculae of callus, which infiltrate the normal compact bone, destroy it, and replace it with dense callus and masses of osteoid. Demonstrating the presence of osteoid aids in the diagnosis of osteosarcoma. Bone tissue produced by osteosarcomas never matures to compact bone.
Ninety percent of osteosarcomas are located in the metaphyses of long bones, especially the distal femur and proximal tibia, with 50% around the knee area.49 The tumor typically breaks through the cortex, lifts the periosteum, and forms a soft tissue mass that is not covered by a smooth shell of new bone. Lifting of the periosteum stimulates bizarre patterns of new bone formation called a periosteal reaction. Distinct osteosarcomas occur on the surface of long bones, called parosteal, periosteal, or high-grade surface osteosarcomas; dedifferentiated parosteal and central osteosarcomas also occur.
The most common initial symptoms are pain and swelling. Initially the pain is slight and intermittent, but within a short time it increases in severity and duration. Pain is usually worse at night and gradually requires medication. Systemic symptoms are uncommon. Usually a coincidental history of trauma is noted. Occasionally the individual may have a pathologic fracture.
Systemic chemotherapy and surgery are the treatments of choice, with the location of the tumor, its size, malignancy grade, and evidence of metastasis dictating the type and extent of surgery. Preoperative chemotherapy has greatly increased the number of individuals qualifying for limb salvage surgery. Limb salvaging procedures have been made possible by advances in reconstructive techniques and endoprosthetics. Limb salvage ultimately may be successful in as many as 80% of persons. Individuals must have achieved most of their bone growth to be candidates for limb salvage procedures, which are preferred to amputation. Skeletally immature individuals may have a limb salvage operation, referred to as a rotationplasty, in which the major portions of the thigh, the tumor, and contaminated knee are resected while preserving the nerve supply (sciatic) to the leg and foot. The proximal tibia is internally fixed to the stump of the proximal femur after it has been rotated 180 degrees. The foot is positioned at a desired spot or direction, allowing the ankle joint to function as a knee joint with the foot supplying the traditional role of the tibial stump in a below-knee amputation.
If an amputation is done, individuals are monitored closely with chest roentgenograms and CT. Pulmonary metastases are surgically resected, and chemotherapy is now a common therapy given both before and after operation, using combinations of chemotherapeutic agents. Promising agents under investigation include monoclonal antibodies, hormone antagonists, gene therapy, and other biologic agents that may dramatically improve survival.49
Chondrogenic Tumors: Chondrosarcoma: Chondrogenic (cartilage-forming) tumors produce cartilage or chondroid, a primitive cartilage or cartilage-like substance. The most common chondrogenic tumor is chondrosarcoma, accounting for 20% of bone tumors.
Chondrosarcoma, the second most common primary malignant bone tumor, is a tumor of middle-age and older adults. Most cases of primary chondrosarcoma are found in persons between 50 and 70 years of age. Secondary chondrosarcoma (a chondrosarcoma derived from an endochondroma) occurs most often in young adults between 20 and 30 years of age. The tumor is found more commonly in men than in women.
A chondrosarcoma is a large ill-defined malignant tumor that infiltrates trabeculae in spongy bone. It occurs most often in the metaphysis or diaphysis of long bones, especially the femur, and in the bones of the pelvis (Figure 42-19). The tumor contains large lobules of hyaline cartilage that are separated by bands of fibrous tissue and anaplastic cells. Chondrosarcomas typically implant in surrounding tissue (“seeding”).
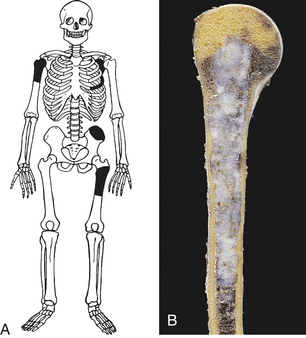
Figure 42-19 Chondrosarcoma A, Common locations of chondrosarcoma. B, Chondrosarcoma of humerus. (From Damjanov I, Linder J, editors: Anderson’s pathology, ed 10, St Louis, 1996, Mosby.)
Symptoms associated with chondrosarcoma have an insidious onset. Local swelling and pain are the usual symptoms that cause a person to seek treatment. At first the pain is dull and intermittent, then gradually intensifies and becomes constant. It may waken the person at night.
Diagnostic studies include radiographs, which must be reviewed carefully for an accurate diagnosis. Biopsy is done at the time of surgery. (If biopsy is done before scheduled surgical incision, seeding of tumor cells could occur.) Sufficient tumor material must be obtained to facilitate an accurate diagnosis.
Surgical excision is generally regarded as the treatment of choice because chemotherapy and radiation seem to have little effect. Many surgically treated individuals demonstrate recurrences, however, so amputation is becoming one treatment of choice. Therefore, individuals with tumors located in the limbs have a better prognosis than those with pelvic lesions.
Collagenic Tumors: Fibrosarcoma: Collagenic (collagen-forming) tumors produce fibrous connective tissue. The most typical collagenic tumor is the fibrosarcoma.
Fibrosarcomas represent 4% of primary malignant bone tumors, with a broad age distribution. They may occur at any age but are most common in adults between 30 and 50 years of age. The incidence is slightly greater in females. Fibrosarcoma also may be a secondary complication of radiation therapy, Paget disease, and long-standing osteomyelitis.
Fibrosarcoma is a solitary tumor that most often affects the metaphyseal region of the femur or tibia. The tumor is composed of a firm fibrous mass of tissue that contains collagen, malignant fibroblasts, and occasional osteoclast-like giant cells.
The tumor begins in the marrow cavity of the bone and infiltrates the trabeculae. It demonstrates a permeative growth pattern, destroys the cortex, and extends into the soft tissue. Metastasis to the lung is common.
Symptoms associated with the tumor have an insidious onset, which delays diagnosis. Pain and swelling, the usual symptoms that cause the individual to seek treatment, usually indicate that the tumor has broken through the cortex. Local tenderness, a palpable mass, and limitation of motion also may be present. A pathologic fracture in the affected bone is often the reason for seeking medical help. Diagnostic studies include radiographs and MRI.
Radical surgery and amputation are the treatments of choice for fibrosarcoma. Radiation therapy is generally considered ineffective treatment for this tumor.
Myelogenic Tumors: Myelogenic tumors originate from various bone marrow cells. Two types of myelogenic tumors are giant cell tumor and myeloma.
Giant Cell Tumor: Giant cell tumor is the sixth most common of the primary bone tumors, accounting for 4% to 5% of bone tumors. Giant cell tumors have a wide age distribution; however, they are rare in persons younger than 10 years or older than 70 years. Most giant cell tumors are found in persons between 20 and 40 years of age. Unlike most other bone tumors, giant cell tumors affect females more often than males.
The giant cell tumor is generally a benign, solitary, circumscribed tumor that causes extensive bone resorption because of its osteoclastic origin (Figure 42-20). Giant cell tumor has a high rate of recurrence but rarely metastasizes. The tumor is rich in osteoclast-like giant cells and anaplastic stromal cells. It also may contain osteoid, callus, and collagen. Overexpression of several genes, including osteoprotegerin ligand (OPGL), occurs in giant cell tumors. The giant cell tumor is typically located in the center of the epiphysis in the femur, tibia, radius, or humerus. The tumor has a slow, relentless growth rate and is usually contained within the original contour of the affected bone. Tumors are often associated with pathologic fractures. It may, however, extend into the articular cartilage. When the tumor extends, it is usually covered by periosteum or periosteal bone growth.
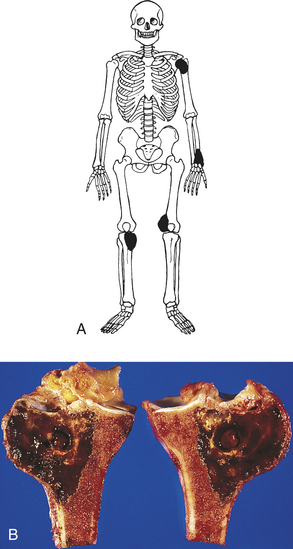
Figure 42-20 Giant cell tumor of bone A, Common skeletal locations. B, Gross picture of cell tumor of bone (epimetaphysis). (From Damjanov I, Linder J, editors: Anderson’s pathology, ed 10, St Louis, 1996, Mosby.)
The most common symptoms associated with giant cell tumor are pain, local swelling, and limitation of movement. Diagnostic studies include radiographs, CT, and MRI. Cryosurgery and resection of the tumor with the use of adjuvant polymethyl methacrylate (PMMA) for bone grafts decrease recurrence and are more successful treatments than curettage and radiation.50 Amputation may be necessary but is not common.