Chapter 1 Clinical examination and making a diagnosis
The focal point of any investigation of animal disease is the making of a diagnosis, and the critical part in making that decision is the clinical examination of the individual animal or group of animals. Therefore, it is appropriate that the first chapter of this book deals with this important subject.
However, before we begin that exercise, it is important that we be quite clear and agree upon what we mean by ‘disease’. Let us assume that disease can be defined as ‘inability to perform physiological functions at normal levels even though nutrition and other environmental requirements are provided at adequate levels’. When this definition is accepted, then not only does a clinically ill animal come into the area of examination but so also do those animals or herds that are not clinically ill but that do not perform as expected. As veterinarians working with food-producing animals and horses, we are required to recognize individual animals that are affected with a particular, recognizable pathological lesion, or biochemical or metabolic deficit, or nutritional deficiency, that results in recognizable clinical signs such as fever, dyspnea, convulsions or lameness. This is traditional veterinary medicine based on a transposition of attitudes and behavior from human medicine. However, it is also necessary for us to investigate disease that the owner recognizes simply as failure to perform or to reach predetermined objectives. This is not necessarily subclinical disease: it is recognizable clinically but perhaps only as poor performance, such as unthriftiness, without any specific system-oriented clinical signs. In other situations, the owner may not recognize any abnormality unless productivity is measured, e.g. milk production or growth rate per day.
There has been considerable emphasis on the clinical and laboratory examination of individual animals affected with clinical disease or that have not performed normally and the large body of information now available in laboratory medicine testifies to this preoccupation. Its greatest importance is in animals, such as companion and racing animals, that are kept as singles and, unless the diagnosis is simple and readily obvious, if a laboratory is available there may be a tendency to make one or more laboratory examinations. The more valuable the animal, the greater the tendency towards some laboratory work. Many biochemical, hematological and biophysical examinations of each body system can yield valuable clues about system or organ function, which usually lead to more accurate and detailed examination of that system or organ. In animals kept in herds or flocks these laboratory tests are also important but are equalled in importance overall by epidemiological investigations. There is little to be gained by this form of examination in animals kept as singles.
With a herd of animals affected with clinical disease, or which is failing to achieve expected objectives, an epidemiological investigation, in addition to the clinical examination of individual animals, may make a valuable contribution to the making of a diagnosis. This is not to suggest that clinical and laboratory examinations are de-emphasized in the examination of herd problems. In some instances, the clinical and laboratory examinations assume major importance to ensure that animals in a herd that is not performing normally are in fact not clinically ill. But when the presenting complaint is poor performance, it is necessary to collect all the pertinent epidemiological data, including accurate production measurements, and to decide whether or not an abnormality is present and, if so, its magnitude. It is at this point that veterinarians become the arbiters of what is ‘health’ and what is ‘illness’. In herd health programs this is a continuing and positive service provided by veterinarians to farmer clients.
In this chapter on clinical examination and making a diagnosis, we have described the standard procedure for the clinical examination of an individual animal followed by some guidelines for the examination of the herd. The level of the examination set out is sufficient to enable the clinician to determine the nature of the abnormality and the system involved. For more detailed examination it is recommended that subsequent chapters, which deal with individual systems, be consulted. Each of them sets out a method for a special examination of the particular system.
Clinical examination of the individual animal
A clinical examination has three parts:
Inadequate examination of any of these may lead to error. The examination of the affected animal represents only a part of the complete investigation. Careful questioning of the owner or attendant can yield information about the diet or the prior diet, about recent vaccinations or surgery or about the introduction of animals into the group, that will provide the clues to a successful diagnosis. However, in certain instances, for example in lead poisoning of cattle, the most detailed examination of the animal and the most careful questioning of the owner may fail to elicit the evidence necessary for a correct diagnosis. Only a careful physical search of the environment for a source of lead can provide this information. Thus neglect of one aspect of the clinical examination can render valueless a great deal of work on the other aspects and lead to an error in diagnosis.
HISTORY-TAKING
In veterinary medicine, history-taking is often the most important of the three aspects of a clinical examination. The significance of the results obtained by examination of the patient and the environment is liable to be modified by a number of factors. Animals are unable to describe their clinical symptoms; they vary widely in their reaction to handling and examination, and a wide range of normality must be permitted in the criteria used in a physical examination. These variations are much greater in some species than in others. Dairy cattle, horses, sheep and goats are usually easy to examine while beef cattle and pigs may be difficult to examine adequately under some conditions. A satisfactory examination of the environment may prove difficult because of lack of knowledge of the factors concerned or because of the examiner’s inability to assess their significance. Problems such as the measurement of the relative humidity of a barn and its importance as a predisposing factor in an outbreak of pneumonia or the determination of pH of the soil with reference to the spread of leptospirosis can present virtually insuperable difficulties to the veterinarian in the field. On the other hand, a search for a specific factor such as a known poison may be relatively simple.
Nevertheless, history-taking is an important key to accurate diagnosis in veterinary medicine, and to be worthwhile it must be accurate and complete. Admittedly, human fallibility must be taken into consideration; there may be insufficient time, the importance of particular factors may not be appreciated, and there may be misunderstanding. Although these are excusable up to a point, failure to recognize the importance of the history can lead only to error. To avoid being misled, it is essential that the veterinarian assesses the accuracy of the history by careful examination of what the owner relates about his or her animals.
The history should suggest not only the diagnostic possibilities but also the probabilities. A 1-year-old heifer is unlikely to have clinical Johne’s disease; an adult cow is more likely to have parturient paresis than a first-calf heifer, which in turn is more likely to have maternal obstetric paralysis than is the adult cow. The history may often indicate that special attention should be paid to the examination of a particular system in the animal, or a particular factor in the environment. For example, in hypovitaminosis-A in beef calves from 6–10 months of age, the animals may be seen when they are clinically normal and the only means of reaching a diagnosis may be a consideration of the history of the clinical findings and the nutritional status.
HISTORY-TAKING METHOD
Successful history-taking involves many veterinarian–client relationships, which must be learned by experience. Some suggestions are presented here as guidelines that may prove useful to the clinician.
The veterinarian should introduce himself or herself to the owner, and the usual greetings of the day will help to establish a veterinarian–client relationship. Asking the owner ‘How can I help you today?’ is an effective opening question, which provides the owner the opportunity to relate his or her concerns about the animals.
The owner or attendant must be handled with diplomacy and tact. The use of nontechnical terms is essential, since livestock owners are likely to be confused by technical expressions or reluctant to express themselves when confronted with terms they do not understand. Statements, particularly those concerned with time, should be tested for accuracy. Owners, and more especially herdsmen and agents, may attempt to disguise their neglect by condensing time or varying the chronology of events. If a detailed cross-examination of the owner seems likely to arouse some antagonism, it is advisable for the veterinarian to forego further questioning and be content with his or her own estimate of the dependability of the history. The clinician must try to separate owners’ observations from their interpretations. A statement that the horse had a bout of bladder trouble may, on closer examination, mean that the horse had an attack of abdominal pain in which it assumed a posture usually associated with urination. Often, however, it is impossible to avoid the use of leading questions – ‘Did the pigs scour?’, ‘Was there any vomiting?’ – but it is necessary to weigh the answers in accordance with the general veracity of the owner.
Absence of a sign can only be determined by inquiring whether or not it occurred. Simply to ask for a complete history of what has happened almost invariably results in an incomplete history. The clinician must, of course, know the right questions to ask; this knowledge comes with experience and familiarity with disease. Owners seldom describe clinical signs in their correct time sequence; part of the clinician’s task is to establish the chronology of events.
For completeness and accuracy in history-taking the clinician should conform to a set routine. The system outlined below includes patient data, disease history and management history. The order in which these parts of the history are taken will vary. In general it is best to take the disease history first. The psychological effect is good: the owner appreciates the desire to get down to the facts about his or her animal’s illness.
PATIENT DATA
If records are to be kept at all, even if only for financial purposes, accurate identification of the patient is essential. An animal’s previous history can be referred to, the disease status of a herd can be examined, specimens for laboratory examination can be dispatched with the knowledge that the results can be related to the correct patient. Accurate records are also necessary for the submission of accounts for veterinary services rendered and the details of the owner’s address and of the animals examined and treated must be accurate. These points may have no importance in establishing the diagnosis but they are of primary importance in the maintenance of a successful practice.
• Postal address and telephone number
• Species, type, breed (or estimate of parentage in a crossbred)
• Sex, age, name or number, body weight
• If necessary, a description, including color markings, polledness and other identifying marks, of the patient.
Such a list may appear formidable but many of the points, such as age, sex, breed, type (use made of animal, e.g. beef, dairy, mutton, wool), are often of importance in the diagnosis. A case history of a particular animal may suggest that further treatment is likely to be uneconomic because of age, or that a particular disease is assuming sufficient importance in a herd for different control measures to be warranted.
Computers are now being used extensively in veterinary practices for recording the details of farm calls, the animals examined and treated, the amounts charged for travel and professional services, the costs of laboratory services, the drugs used and dispensed, and the diseases that occur on a particular farm on an ongoing basis. It is now possible for veterinary practices to provide regular and annual health reports to herd owners so that planned health management programs can be assessed and evaluated. The ability to retrieve and summarize this information on an individual farm basis is a major step forward in providing optimal veterinary service to livestock herds regardless of their size and complexity.
DISEASE HISTORY
History-taking will vary considerably depending on whether one animal or a group of animals is involved in the disease problem under examination. As a general rule, in large animal work, all disease states should be considered as herd problems until proved to be otherwise. It is often rewarding to examine the remainder of a group and find animals that are in the early stages of the disease.
Present disease
Attempts should be made to elicit the details of the clinical abnormalities observed by the owner in the sequence in which they occurred. If more than one animal is affected, a typical case should be chosen and the variations in history in other cases should then be noted. Variations from the normal in the physiological functions such as intake of food or drink, milk production, growth, respiration, defecation, urination, sweating, activity, gait, posture, voice and odor should be noted in all cases. There are many specific questions that need to be asked in each case but they are too numerous to list here and for the most part they are variations on the questions already suggested.
If a number of animals are affected, information may be available from clinical pathological examinations carried out on living animals or necropsy examinations on fatal cases. The behavior of animals before death and the period of time elapsing between the first observable signs and death or recovery are important items of information. Prior surgical or medical procedures such as castration, docking, shearing, or vaccination may be important factors in the production of disease.
Morbidity, case fatality and population mortality rates
The morbidity rate is usually expressed as the percentage of animals that are clinically affected compared with the total number of animals exposed to the same risks. The case fatality rate is the percentage of affected animals that die. The population mortality rate is the percentage of all exposed animals that die. The estimates may be important in diagnosis because of the wide variations in morbidity, case fatality and population mortality rates that occur in different diseases. An equally important figure is the proportion of animals at risk that are clinically normal but show abnormality on the basis of laboratory or other tests.
Prior treatment
The owner may have treated animals before calling for assistance. Exact details of the preparations used and doses given may be of value in eliminating some diagnostic possibilities. They will certainly be of importance when assessing the probable efficiency of the treatment and the significance of clinical pathological tests, and in prescribing additional treatment. Drug withdrawal regulations now require that treated animals or their products, such as milk, be withheld from slaughter or market for varying lengths of time to allow drug residues to reach tolerable limits. This necessitates that owners reveal information about the drugs that they have used.
Prophylactic and control measures
It should be ascertained whether preventive or control procedures have already been attempted. There may have been clinical pathological tests, the introduction of artificial insemination to control venereal disease, vaccination, or changes in nutrition, management or hygiene. For example, in an outbreak of bovine mastitis careful questioning should be pursued regarding the method of disinfecting the cows’ teats after each milking, with particular reference to the type and concentration of the disinfectant used and whether or not back-flushing of teat cups is practiced. Spread of the disease may result from failure of the hygiene barrier at any one of a number of such points. When written reports are available they are more reliable than the memory of the owner.
Previous exposure
The history of the group relative to additions is of particular importance. Is the affected animal an established member of the group, or has it been introduced, and if so how long ago? If the affected animal has been in the group for some time, have there been recent additions? Is the herd a ‘closed herd’ or are animals introduced at frequent intervals? Not all herd additions are potential carriers of disease – they may have come from herds where control measures are adequate, they may have been tested before or after sale or kept in quarantine for an adequate period after arrival, or they may have received suitable biological or antibiotic prophylaxis. Herd additions may have come from areas where a particular disease does not occur, although a negative history of this type is less reliable than a positive history of derivation from an area where a particular disease is enzootic.
A reverse situation may occur where imported animals have no resistance to endemic infection in the home herd, or have not become adapted to environmental stressors such as high altitudes, high environmental temperatures and particular feeding methods, or are not accustomed to poisonous plants occurring in the environment.
Transit
The possibility of infection during transit is always a potential risk and pre-sale certificates of health may be of little value if an animal has passed through a sale barn, a show or communal trucking yards while in transit. Highly infectious diseases may be transmitted via trucks, railroad cars or other accommodation contaminated by previous inhabitants. Transient introductions, including animals brought in for work purposes, for mating or on temporary grazing, are often overlooked as possible vectors of disease. Other sources of infection are wild fauna that graze over the same area as domestic livestock and inanimate objects such as human footwear, car tires and feeding utensils.
Culling rate
There may be considerable significance in the reasons for culling, and the number of animals disposed of for health reasons. Failure to grow well, poor productivity and short productive life will suggest the possible occurrence of a number of chronic diseases, including some associated with infectious agents, by nutritional deficiencies or by poisons.
Previous disease
Information elicited by questioning on previous history of illness may be helpful. If there is a history of previous illness, inquiries should be made on the usual lines, including clinical observations, necropsy findings, morbidity, case fatality rates, the treatments and control measures used and the results obtained. If necessary, inquiries should be made about herds from which introduced animals have originated and also about herds to which other animals from the same source have been sent.
MANAGEMENT HISTORY
The management history includes nutrition, breeding policy and practice, housing, transport and general handling. It is most important to learn whether or not there has been any change in the prevailing practice prior to the appearance of disease. The fact that a disease has occurred when the affected animals have been receiving the same ration, deriving from the same source over a long period, suggests that the diet is not at fault, although errors in preparation of concentrate mixtures, particularly with the present-day practice of introducing additives to feeds, can cause variations that are not immediately apparent.
Nutrition
The major objective in the examination of the nutritional history is to determine how the quantity and quality of the diet which the animals have been receiving compares with the nutrient requirements that have been recommended for a similar class of animal. In some situations it may be necessary to submit feed and water samples for analyses to assess quality.
Livestock at pasture
Pastured livestock present a rather different problem from those being stall-fed in that they receive a diet that is less controlled and thus more difficult to assess. The risk of parasitic infestation and, in some cases, infectious disease is much greater in grazing animals. Inquiries should be made about the composition of the pasture, its probable nutritive value with particular reference to recent changes brought about by rain or drought, whether rotational grazing is practiced, the fertilizer program and whether or not minerals and trace elements are provided by top-dressing or mineral mixtures. The origin of mineral supplements, particularly phosphates, which may contain excess fluorine, and homemade mixtures, which may contain excessive quantities of other ingredients, should receive attention. Actual examination of the pasture area is usually more rewarding than a description of it.
Hand-fed/stall-fed animals
Hand-fed or stall-fed animals are subjected to a more or less controlled feed supply but, because of human error, they are frequently exposed to dietary mistakes. Types and amounts of feeds fed should be determined. Examples of disease caused by inadequate hand-fed diets include: osteodystrophia fibrosa in horses on diets containing excess grain; azoturia in the same species when heavy-carbohydrate diets are fed during periods of rest, and lactic acid indigestion in cattle introduced to high-level grain diets too rapidly. The sources of the dietary ingredients may also be of importance. Grains from some areas are often much heavier and contain a much greater proportion of starch to husk than grains from other areas so that when feed is measured, rather than weighed, overfeeding or underfeeding may occur.
Because the digestive enzyme capacity of newborn farm animals is most efficient in the digestion of whole milk, the use of non-milk sources of carbohydrates and proteins in the formulation of milk replacers may result in indigestion and nutritional diarrhea.
Exotic diseases may be imported in feed materials: anthrax, foot-and-mouth disease and hog cholera are well-known examples.
Variations in the preparation of ingredients of rations may produce variable diets. Overheating, as in pelleting or the cooking of feeds, can reduce their vitamin content; contamination with lubricating oil can result in poisoning by chlorinated naphthalene compounds; pressure extraction of linseed can leave considerable residues of hydrocyanic acid in the residual oil cake.
Feeding practices may in themselves contribute to the production of disease. Pigs fed in large numbers with inadequate trough space or calves fed from communal troughs are likely to be affected by overeating or inanition, depending on their size and vigor. High-level feeding and consequent rapid growth may create deficiency states by increasing the requirement for specific nutrients.
In both hand-fed and grazing animals changes in diet should be carefully noted. Movement of animals from one field to another, from pasture to cereal grazing, from unimproved to improved pasture may all precipitate the appearance of disease. Periods of sudden dietary deficiency can occur as a result of bad weather or transportation, or during change to unfamiliar feeds. Rapid changes are more important than gradual alterations, particularly in pregnant and lactating ruminants when metabolic diseases, including those caused by hypocalcemia, hypoglycemia and hypomagnesemia, are likely to occur.
The availability of drinking water must be determined: salt poisoning of swine occurs only when the supply of drinking water is inadequate.
Reproductive management and performance
In the examination of a single animal the breeding and parturition history may suggest or eliminate some diagnostic possibilities. For example, pregnancy toxemia occurs in sheep in late pregnancy while acetonemia in dairy cows occurs primarily 2–6 weeks after parturition. Acute septic metritis is a possibility within a few days after parturition in any species but unlikely several weeks later.
Breeding history
The breeding history may be of importance with regard to inherited disease. The existence of a relationship between sires and dams should be noted. Hybrid vigor in crossbred animals should be considered when there is apparent variation in resistance to disease between groups maintained under similar environmental conditions. A general relationship between selection for high productivity and susceptibility to certain diseases is apparent in many breeds of animal and even in certain families. The possibility of genetotrophic disease, i.e. the inheritance of a greater requirement than normal of a specific nutrient, should be considered.
Reproductive history
The examination of the herd reproductive history involves comparing past and present reproductive performance with certain optimum objectives. The mean length of the interval between parturition and conception, the mean number of services per conception and the percentage of young animals weaned relative to the number of females that were originally exposed for breeding (calf or lamb crop, pigs weaned) are general measures of reproductive performance and efficiency.
Using cattle as an example, certain other observations may assist in determining the cause of failure to reach reproductive performance objectives. These are:
• Percentage of females pregnant at specified times after the onset of breeding period
• Size and topography of breeding pastures
• Fertility status of the females and males at breeding time.
The percentage of females that need assistance at parturition and the percentage of calves that die at birth are also indices of reproductive performance that are indicative of the level of reproductive management provided.
Climate
Many diseases are influenced by climate. Foot rot in cattle and sheep reaches its peak incidence in warm, wet summers and is relatively rare in dry seasons. Diseases spread by insects are encouraged when climatic conditions favor the propagation of the vector. Internal parasites are similarly influenced by climate. Cool, wet seasons favor the development of hypomagnesemia in pastured cattle. Anhidrosis in horses is specifically a disease of hot, humid countries. The direction of prevailing winds is of importance in many disease outbreaks, particularly in relation to the contamination of pasture and drinking water by fumes from factories and mines and the spread of diseases carried by insects.
General management
There are so many items in the proper management of livestock that, if neglected, can lead to the occurrence of disease that they cannot be related here; animal management in the prevention of disease is a subject in its own right and is dealt with in all parts of this book. Some of the more important factors include:
• Hygiene, particularly in milking parlors and in parturition and rearing stalls
• Adequacy of housing in terms of space, ventilation, draining, situation and suitability of troughs
• Proper management of milking machines to avoid udder injury.
The class of livestock under consideration is also of importance; for example, enterotoxemia is most common in finishing lambs and pigs, parturient paresis in milking cows, obstructive urolithiasis in lambs and steers in feedlots and pregnancy toxemia in ewes used for fat lamb production.
EXAMINATION OF THE ENVIRONMENT
An examination of the environment is a necessary part of any clinical investigation because of the possible relationship between environmental factors and the incidence of disease. A satisfactory examination of the environment necessitates an adequate knowledge of animal husbandry and, with the development of species specialization, it will be desirable for the veterinarian to understand the environmental needs of a particular species or class of farm animal.
Depending on the region of the world, some animals are kept outside year round, some are housed for part of the year during the winter months, and some are kept under total confinement. For animals raised on pasture, the effects of topography, plants, soil type, ground surface and protection from extremes of weather assume major importance. For animals housed indoors, hygiene, ventilation and avoiding overcrowding are of major concern. Some of these items will be briefly presented here as guidelines. Each observation should be recorded in detail for preparation of reports for submission to the owners. Detailed records and even photographs of environmental characteristics assume major importance when poisonings are suspected and where litigation proceedings appear possible.
OUTDOOR ENVIRONMENT
Topography and soil type
The topography of grasslands, pastures and wooded areas can contribute to disease or inefficient production and reproduction. Flat, treeless plains offering no protection from wind predispose cattle to lactation tetany in inclement weather. Low, marshy areas facilitate the spread of insect-borne diseases and soil-borne infections requiring damp conditions, such as leptospirosis; Johne’s disease and diseases associated with liver fluke infestation and lungworm pneumonia are more prevalent in such areas. Rough grasslands with extensive wooded areas can have an adverse effect on reproductive performance in beef herds because of the difficulty the bulls have in getting to the females during peak periods of estrus activity.
The soil type of a district may provide important clues to the detection of nutritional deficiencies; copper and cobalt deficiencies are most common on littoral sands and the copper deficiency/molybdenum excess complex usually occurs on peat soils. The surface of the ground and its drainage characteristics are important in highly intensive beef feedlots and in large dairy herds where fattening cattle and dairy cows are kept and fed under total confinement. Ground surfaces that are relatively impermeable and/or not adequately sloped for drainage can become a sea of mud following a heavy rainfall or snowstorm. Constant wetting of the feet and udders commonly results in outbreaks of foot rot and mastitis. Dirty udders increase the time required for udder washing prior to milking and can seriously affect a mastitis control program.
In some regions of the world, beef cows are calved in outdoor paddocks in the spring when it is wet and cold with an excess of surface water; this increases the spread of infectious disease and results in a marked increase in neonatal mortality. A lack of sufficient protection from the prevailing winds, rain, snow or the heat of the sun can seriously affect production and can exacerbate an existing disease condition or precipitate an outbreak. Dusty feedlots during the hot summer months may contribute to an increase in the incidence of respiratory disease or delay the response to treatment of disease such as pneumonia.
Stocking rate (population density)
Overcrowding is a common predisposing cause of disease. There may be an excessive buildup of feces and urine, which increases the level of infection. The relative humidity is usually increased and more difficult to control. Fighting and cannibalism are also more common in overcrowded pens than when there is adequate space for animals to move around comfortably. The detection and identification of animals for whatever reason (illness, estrus) can be difficult and inaccurate under crowded conditions.
Feed and water supplies
Pasture and feed
On pastures the predominant plant types, both natural and introduced, should be observed as they are often associated with certain soil types and may be the cause of actual disease; the high estrogen content of some clovers, the occurrence of functional nervous diseases on pastures dominated by Phalaris aquatica (syn. P. tuberosa) and perennial rye grass and the presence of selective absorbing ‘converte’ plants on copper-rich and selenium-rich soils are all examples of the importance of the dominant vegetation. The presence of specific poisonous plants, evidence of overgrazing and the existence of a bone-chewing or bark-chewing habit can be determined by an examination of the environment.
Vital clues in the investigation of possible poisoning in a herd may be the existence of a garbage dump or ergotized grass or rye in the pasture, or the chewing of lead-based painted walls in the barn, or careless handling of poisons in the feed area. The possibility that the forage may have been contaminated by environmental pollution from nearby factories or highways should be examined. In some cases the physical nature of the pasture plants may be important; mature, bleached grass pasture can be seriously deficient in carotene, whereas lush young pasture can have rachitogenic potency because of its high carotene content or it may be capable of causing hypomagnesemia if it is dominated by grasses. Lush legume pasture or heavy concentrate feeding with insufficient roughage can cause a serious bloat problem.
The feed supplies for animals raised in confinement outdoors must be examined for evidence of moldy feed, contamination with feces and urine and excessive moisture due to lack of protection from rain and snow. Empty feed troughs may confirm a suspicion that the feeding system is faulty.
Water
The drinking water supply and its origin may be important in the production of disease. Water in ponds may be covered with algae containing neurotoxins or hepatotoxic agents and flowing streams may carry effluent from nearby industrial plants. In a feedlot, water may suddenly become unavailable because of frozen water lines or faulty water tank valves. This should not go unnoticed if one recognizes the anxiety of a group of cattle trying to obtain water from a dry tank.
Waste disposal
The disposal of feces and urine has become a major problem for large intensified livestock operations. Slurry is now spread on pastures and may be important in the spread of infectious disease. Lagoons can provide ideal conditions for the breeding of flies, which can be troublesome to a nearby livestock operation. The inadequate disposal of dead animals may be an important factor in the spread of certain diseases.
INDOOR ENVIRONMENT
There are few aspects of livestock production that have aroused more interest, development and controversy in the last few years than the housing and environmental needs of farm animals. Several textbooks on the subject have been written and only some of the important items will be mentioned here, with the aid of some examples. The effects of housing on animal health have not received the consideration they deserve, partly because of insufficient knowledge of animals’ environmental needs and partly because there has been a failure to apply what is already known.
As a general statement, it can be said that inadequate housing and ventilation, overcrowding and uncomfortable conditions are considered to have detrimental effects on housed animals that make them not only more susceptible to infectious disease but also less productive. Moreover, this reduction in productive efficiency may be a greater cause of economic loss than losses caused by infectious disease. For this reason, the veterinarian must learn to examine and assess all aspects of an indoor environment, which may be the primary cause of, or a predisposing factor to, disease. By way of illustration, the major causes of preweaning mortality of piglets are chilling and crushing of piglets in the first few days of life, and not infectious disease. These physical causes are commonly related to a combination of poorly designed farrowing crates, slippery floors, inadequate heating and perhaps overcrowding of the farrowing facilities.
Hygiene
One of the first things to observe is the level of sanitation and hygiene, which is usually a reliable indicator of the level of management; poor hygiene is often associated with a high level of infectious disease. For example, the incidence of diarrhea in piglets may be high because the farrowing crates are not suitably cleaned and disinfected before the pregnant sows are placed in them. A similar situation applies for lambing sheds, calving pens and foaling boxes. An excessive buildup of feces and urine with insufficient clean bedding will result in a high level of neonatal mortality. The methods used for cleaning and disinfection should be examined carefully. The removal of dried feces from animal pens that have been occupied for several months is a difficult and laborious task and often not done well. Undue reliance may be placed on the use of chemical disinfectants.
The total length of time that animals have occupied a pen without cleaning and disinfection (occupation time) should be noted. As the occupation time increases, there is a marked increase in the infection rate and the morbidity and mortality from infectious disease often increase.
Ventilation
Inadequate ventilation is considered to be a major risk factor contributing to the severity of swine enzootic pneumonia in finishing pigs. The primary infection has a minimal effect on the well-housed pig, but inadequate ventilation results in overheating of the barn in the summer months and chilling and dampness during the winter months, commonly resulting in subclinical and clinical pneumonia, which severely affects productive efficiency. Similarly, in young calves, which are raised indoors in most of the temperate zones of the world, protection from the cold during the winter is necessary. The effects of enzootic pneumonia of housed calves are much more severe when ventilation is inadequate than when the calves are comfortable and have clean, fresh air.
The evaluation of the adequacy of ventilation of a farm animal barn that is filled to economic capacity with animals is a difficult task and a major subject. Ventilation is assessed by a determination of the number of air changes per unit of time, the relative humidity during the day and night, the presence or absence of condensation on the hair coats of the animals or on the walls and ceilings, the presence of drafts, the building and insulation materials used, the positions and capacities of the fans and the size and location of the air inlets. The measurement of the concentration of noxious gases in animal barns, such as ammonia and hydrogen sulfide, may be a valuable aid in assessing the effectiveness of a ventilation system.
Animals raised indoors are frequently overcrowded, which may predispose to disease, and measurements of population density and observations of animal behavior in such conditions assume major importance. When pigs are raised indoors in crowded conditions with inadequate ventilation, their social habits may change drastically and they begin to defecate and urinate on the clean floor and on their pen-mates rather than over the slatted floor over the gutter. This can result in outbreaks of diseases that are transmitted by the fecal–oral route.
Flooring
The quality of the floor is often responsible for diseases of the musculoskeletal system and skin. Poorly finished concrete floors with an exposed aggregate can cause severe foot lesions and lameness in adult swine. Recently calved dairy cows are very susceptible to slipping on poor floors in dairy barns, a common cause of the downer cow syndrome. Loose-housing systems, particularly those with slatted floors, have resulted in a new spectrum of diseases of the feet of cattle because of the sharp edges of some of the slats. The quality and quantity of bedding used should be noted. Bedding is now rarely used in intensified swine operations. The use of sawdust or shavings in loose-housing systems for dairy cattle may be associated with outbreaks of coliform mastitis. Wet bedding, particularly during the winter months, is commonly associated with endemic pneumonia in calves.
Floor plan
The floor plan and general layout of an animal house must be examined for evidence that the routine movements of animal attendants, the movements of animals and feeding facilities may actually be spreading disease. Communal gutters running through adjacent pens may promote the spread of disease through fecal or urinary contamination. The nature of the partitions between pens, whether solid or open grid type, may assist the control or spread of infectious disease. The building materials used will influence the ease with which pens, such as farrowing crates and calf pens, can be cleaned and disinfected for a new batch of piglets or calves.
Lighting
The amount of light available in a barn should be noted. With insufficient light it may be difficult to maintain a sufficient level of sanitation and hygiene, sick animals may not be recognized early enough, and in general errors in management are likely to occur.
In the investigation of a herd problem of mastitis in dairy cattle the veterinarian should visit the farm at milking time and observe how the cows are prepared for milking, examine the teats and udders before and after they are washed, observe the use of the milking machine, and the level of sanitation and hygiene practiced. Several successive visits may be necessary to reveal possible weakness in a mastitis control program.
EXAMINATION OF THE PATIENT
A complete clinical examination of an animal patient includes, in addition to history-taking and an examination of the environment, physical and laboratory examinations. A complete clinical examination of every patient is unnecessary because of the simplicity of some diseases. However, a general clinical examination of every patient is necessary and the inexperienced clinician should spend as much time and effort as is practicable and economical in carrying it out. This will help to avoid the sort of embarrassing error in which a calf is operated on for umbilical hernia when it also has a congenital cardiac defect.
As learned experience develops, the clinician will know the extent to which a clinical examination is necessary. All the laboratory tests that are likely to be informative and that are practical and economical should be used. Because of the cost of laboratory tests, the clinician must be selective in the tests used. The most economical method is to examine the patient and then select those laboratory tests that will support or refute the tentative clinical diagnosis. In this section a system for the examination of a patient is outlined in a general way. There is a great deal of difference between species in the ease with which this examination is done and the amount of information that can be collected. Additional detailed examination techniques are described under the individual body systems.
The examination of a patient consists of a general inspection done from a distance (the distant examination, and the particular distant examination of body regions), followed by a close physical examination of all body regions and systems. Only the major body systems that are routinely examined are presented here as part of the general examination.
GENERAL INSPECTION (DISTANT EXAMINATION)
The importance of a distant examination of the animal cannot be overemphasized, and yet it is often overlooked. Apart from the general impression gained from observation at a distance, there are some signs that can best be assessed before the animal is disturbed. The proximity of the examiner is particularly disturbing to animals that are unaccustomed to frequent handling.
Behavior and general appearance
The general impression of the health of an animal obtained by an examination from a distance should be assessed according to the following.
Behavior
Separation of an animal from its group is often an indication of illness. The behavior is also a reflection of the animal’s health. If it responds normally to external stimuli, such as sound and movement, it is classified as bright. If the reactions are sluggish and the animal exhibits relative indifference to normal stimuli, it is said to be dull or apathetic. Cattle with carbohydrate engorgement are commonly reluctant to move unless coaxed. A pronounced state of indifference in which the animal remains standing and is able to move but does not respond at all to external stimuli is the ‘dummy’ syndrome. This occurs in subacute lead poisoning, listeriosis and some cases of acetonemia in cattle, and in encephalomyelitis and hepatic cirrhosis in horses. The terminal stage of apathy or depression is coma, in which the animal is unconscious and cannot be roused.
Excitation states
Excitation states vary in severity. A state of anxiety or apprehension is the mildest form: here the animal is alert and looks about constantly but is normal in its movements. Such behavior is usually expressive of moderate constant pain or other abnormal sensation, as in early parturient paresis or in recent blindness. A more severe manifestation is restlessness, in which the animal moves about a good deal, lies down and gets up and may go through other abnormal movements such as looking at its flanks, kicking at its belly and rolling and bellowing. Again, this demeanor is usually indicative of pain.
More extreme degrees of excited demeanor include mania and frenzy. In mania, the animal performs abnormal movements with vigor. Violent licking at its own body, licking or chewing inanimate objects and pressing forward with the head are typical examples. In frenzy, the actions are so wild and uncontrolled that the animals are a danger to anyone approaching them. In both mania and frenzy there is usually excitation of the brain, as in rabies, acute lead poisoning and some cases of nervous acetonemia.
Voice
Abnormality of the voice should be noted. It may be hoarse in rabies or weak in gut edema; there may be continuous lowing in nervous acetonemia or persistent bellowing indicative of acute pain. Soundless bellowing and yawning are commonly seen in rabid cattle and yawning is a common sign in animals affected with hepatic insufficiency.
Eating
The appetite of the animal can be assessed by observing its reaction to the offering of feed or by the amount of feed available that has not been eaten. It is important to determine the total amount of feed that the animal is eating per day. In a patient that has retained its appetite, there may be abnormality of prehension, mastication or swallowing and, in ruminants, of belching and regurgitation.
Prehension may be interfered with by inability to approach feed, paralysis of the tongue in cattle, in cerebellar ataxia, osteomyelitis of cervical vertebrae and other painful conditions of the neck. When there is pain in the mouth, prehension may be abnormal and affected animals may be able to take only certain types of feed. Mastication may be slow, one-sided or incomplete when mouth structures, particularly teeth, are affected. Periodic cessation of chewing when feed is still in the mouth occurs commonly in the ‘dummy’ syndrome, when there are space-occupying lesions of the cranium or an encephalomyelitis exists.
Swallowing may be painful because of inflammation of the pharynx or esophagus, as is found in strangles in the horse, in calf diphtheria, and where improper use of bailing and drenching guns or bottles has caused laceration of the pharyngeal mucosa. Attempts at swallowing followed by coughing up of feed or regurgitation through the nostrils can also be the result of painful conditions but are most likely to be due to physical obstructions such as esophageal diverticula or stenosis, a foreign body in the pharynx, or paralysis of the pharynx. It is important to differentiate between material that has reached the stomach and ingesta regurgitated from an esophageal site. Partial esophageal obstruction resulting in difficult swallowing is usually manifested by repeated swallowing movements, often with associated flexion of the neck and grunting.
In ruminants there may be abnormalities of rumination and eructation. Absence of cudding occurs in many diseases of cattle and sheep; violent efforts at regurgitation with grunting suggests esophageal or cardiac obstruction. There may be inability to control the cud – ‘cud-dropping’ – due to pharyngeal paralysis or painful conditions of the mouth. Failure to eructate is usually manifested by the appearance of bloat.
Defecation
In constipation and rectal paralysis or stenosis, the act of defecation may be difficult and be accompanied by straining or tenesmus. When there is abdominal pain or laceration of the mucocutaneous junction at the anus, defecation may cause obvious pain. Involuntary defecation occurs in severe diarrhea and when there is paralysis of the anal sphincter. Consideration of frequency, volume and character of feces is given later under the section on special examination of the digestive tract. Constipation must not be mistaken for scant feces, particularly in mature cattle with diseases of the forestomachs and failure of movement of ingesta in a caudad direction.
Urination
This may be difficult when there is partial obstruction of the urinary tract, and painful when there is inflammation of the bladder or urethra. In cystitis and urethritis, there is increased frequency with the passage of small amounts of fluid, and the animal remains in the urination posture for some time after the flow ceases. Incontinence, with constant dribbling of urine, is usually due to partial obstruction of the urethra or paralysis of its sphincter. If the animal urinates during the visual inspection, a sample of urine should be obtained, examined grossly and submitted for urinalysis.
Posture
Abnormal posture is not necessarily indicative of disease, but when associated with other signs it may indicate the site and severity of a disease process. One of the simplest examples is resting of a limb in painful conditions of the extremities; if a horse continually shifts its weight from limb to limb it may indicate the presence of laminitis or early osteodystrophia fibrosa. Arching of the back with the limbs tucked under the body usually indicates mild abdominal pain; downward arching of the back and ‘saw horse’ straddling of the legs is characteristic of severe abdominal pain, usually spasmodic in occurrence; a ‘dog-sitting’ posture in the horse associated with rolling and kicking at the belly is usually associated with abdominal pain and pressure on the diaphragm, such as occurs in acute gastric dilatation after engorgement on grain. This posture is commonly adopted by normal cattle but will occur in painful conditions of the pelvic limbs such as degenerative osteoarthritis in young cattle. Abduction of the elbows is usually synonymous with chest pain or difficulty in breathing. Elevation and rigidity of the tail, and rigidity of the ears and limbs, are good indications of tetanus in animals. The carriage of the tail in pigs is a useful barometer of their state of health. Sheep that are blind, as in early pregnancy toxemia, are immobile but stand with the head up and have an expression of extreme alertness.
When the animal is recumbent, there also may be abnormalities of posture. In cattle affected by dislocation of the hip or by sciatic nerve paralysis, the affected limb is not held flexed next to the abdomen but sticks straight out in an awkward position; unilateral pain in the chest may cause an animal to lie habitually on the other side; a weak hindleg may be kept under the animal. The head may be carried around towards the flank in parturient paresis in cows and in colic in horses. Sheep affected with hypocalcemia, and cattle with bilateral hip dislocation, often lie in sternal recumbency with the hindlegs extended behind in a frog-like attitude. Inability or lack of desire to rise are usually indicative of muscle weakness or of pain in the extremities as in enzootic muscular dystrophy or laminitis.
Gait
Movements of the limbs can be expressed in terms of rate, range, force and direction of movement. Abnormalities may occur in one or more of these categories. For example, in true cerebellar ataxia all qualities of limb movement are affected. In louping-ill in sheep it is the range and force that are excessive, giving a high-stepping gait and a bounding form of progression; in arthritis, because of pain in the joints, or in laminitis, because of pain in the feet, the range is diminished and the patient has a shuffling, stumbling walk. The direction of progress may be affected. Walking in circles is a common abnormality and is usually associated with rotation or deviation of the head; it may be a permanent state as in listeriosis or occur spasmodically as in acetonemia and pregnancy toxemia. Compulsive walking or walking directly ahead regardless of obstructions is part of the ‘dummy’ syndrome mentioned earlier and is characteristic of encephalomyelitis and hepatic insufficiency in the horse.
Body condition
The animal may be in normal bodily condition, or obese, thin or emaciated. The difference between thinness and emaciation is one of degree: the latter is more severe but there are additional signs that are usually taken into consideration. In an emaciated (cachectic) animal the coat is poor, the skin is dry and leathery and work performance is reduced. Thin animals, on the other hand, are physiologically normal. The difference between fatness and obesity is of the same order. Most beef cattle prepared for the show-ring are obese. In order to inject some degree of numerical assessment it is now customary in all farm animal species and in horses to use body condition on a scale of 1–5 or preferably 1–10.
Body conformation
The assessment of conformation or shape is based on the symmetry and the shape and size of the different body regions relative to other regions. An abdomen that is very large relative to the chest and hindquarters can be classified as an abnormality of conformation. To avoid repetition, points of conformation are included in the description of body regions.
Skin
Skin abnormalities can usually be seen at a distance. They include changes in the hair or wool, abnormal sweating, the presence of discrete or diffuse lesions, evidence of soiling by discharges and of itching. The normal luster of the coat may be absent: it may be dry as in most chronic debilitating diseases or excessively greasy as in seborrheic dermatitis. In debilitated animals the long winter coat may be retained past the normal time. Alopecia may be evident: in hyperkeratosis it is diffuse; in ringworm it may be diffuse but more commonly occurs in discrete areas. Sweating may be diminished, as in anhidrosis of horses; patchy as in peripheral nerve lesions; or excessive as in acute abdominal pain. Hypertrophy and folding of the skin may be evident, hyperkeratosis being the typical example. Discrete skin lesions range in type from urticarial plaques to the circumscribed scabs of ringworm, pox and impetigo. Diffuse lesions include the obvious enlargements due to subcutaneous edema, hemorrhage and emphysema. Enlargements of lymph nodes and lymphatics are also evident when examining an animal from a distance.
INSPECTION OF BODY REGIONS (PARTICULAR DISTANT EXAMINATION)
As a general rule, as much of a clinical examination as possible should be carried out before the animal is handled. This is partly to avoid unnecessary excitement of the patient but also because some abnormalities are better seen at a distance and in some cases cannot be discerned at close range. The general appearance of the animal should be noted and its behavior assessed. Some time should also be devoted to an inspection of the various body regions – a particular distant examination.
Head
The facial expression may be abnormal. The rigidity of tetanus, the cunning leer or maniacal expression of rabies and acute lead poisoning are cases in point. The symmetry and configuration of the bony structure should be examined. Doming of the forehead occurs in some cases of congenital hydrocephalus and in chondrodysplastic dwarfs, and in the latter there may be bilateral enlargement of the maxillae. Swelling of the maxillae and mandibles occurs in osteodystrophia fibrosa; in horses swelling of the facial bones is usually due to frontal sinusitis; in cattle enlargement of the maxilla or mandible is common in actinomycosis. Asymmetry of the soft structures may be evident and is most obvious in the carriage of the ears, degree of closure of the eyelids and situation of the muzzle and lower lip. Slackness of one side and drawing to the other are constant features in facial paralysis. Tetanus is accompanied by rigidity of the ears, prolapse of the third eyelid and dilatation of the nostrils.
The carriage of the head is most important: rotation is usually associated with defects of the vestibular apparatus on one side, deviation with unilateral involvement of the medulla and cervical cord; opisthotonos is an excitation phenomenon associated with tetanus, strychnine poisoning, acute lead poisoning, hypomagnesemic tetany, polioencephalomalacia and encephalitis.
The eyes merit attention. Visible discharge should be noted; protrusion of the eyeball, as occurs in orbital lymphomatosis, and retraction of the bulb, as occurs commonly in dehydration, are important findings; spasm of the eyelids and excessive blinking usually indicate pain or peripheral nerve involvement; prolapse of the nictitating membrane usually characterizes central nervous system derangement, generally tetanus.
Dilatation of the nostrils and nasal discharge suggest the advisability of closer examination of the nasal cavities at a later stage. Excessive salivation or frothing at the mouth denotes painful conditions of the mouth or pharynx or is associated with tremor of the jaw muscles due to nervous involvement. Swellings below the jaw may be inflammatory, as in actinobacillosis and strangles, or edematous, as in acute anemia, protein starvation or congestive heart failure. Unilateral or bilateral swelling of the cheeks in calves usually indicates necrotic stomatitis.
Neck
If there is enlargement of the throat this region should be more closely examined later to determine whether the cause is inflammatory and whether lymph nodes, salivary glands (or guttural pouches in the horse) or other soft tissues are involved. Goiter leads to local enlargement located further down the neck. A jugular pulse, jugular vein engorgement and edema should be looked for and local enlargement due to esophageal distension should be noted.
Thorax
The respiration should be examined from a distance, preferably with the animal in a standing position, as recumbency is likely to modify it considerably. Allowance should be made for the effects of exercise, excitement, high environmental temperatures and fatness of the subject: obese cattle may have respiratory rates two to three times that of normal animals. The rate, rhythm, depth and type of respiration should be noted.
Respiratory rate
In normal animals under average conditions the rate should fall within the following limits:
An increased respiratory rate is designated as polypnea, decreased rate as oligopnea and complete cessation as apnea. The rate may be counted by observation of rib or nostril movements, by feeling the nasal air movements or by auscultation of the thorax or trachea. A significant rise in environmental temperature or humidity may double the normal respiratory rate. Animals that are acclimatized to cold outdoor temperatures are susceptible to heat stress when exposed suddenly to warmer temperatures. When brought indoors the respiratory rate may increase to six or eight times the normal, and panting open-mouth breathing may be evident within 2 hours.
Respiratory rhythm
The normal respiratory cycle consists of three phases of equal length: inspiration, expiration and pause; variation in the length of one or all phases constitutes an abnormality of rhythm. The breathing pattern of the neonatal foal is markedly different from that of the adult horse, and similar to that of other neonates. It has a higher respiratory rate, a higher airflow rate, and a higher minute ventilation on a body weight basis. In addition, in the standing neonatal foal, both the inspiratory and expiratory airflow patterns are essentially monophasic, whereas the adult horse typically has a biphasic inspiratory and expiratory airflow pattern. The transition from monophasic to biphasic flow patterns occurs within the first year of life.
Prolongation of phases
Prolongation of inspiration is usually due to obstruction of the upper respiratory tract; prolongation of the expiration is often due to failure of normal lung collapse, as in emphysema. In most diseases of the lungs there is no pause and the rhythm consists of two beats instead of three. There may be variation between cycles: Cheyne– Stokes respiration, characteristic of advanced renal and cardiac disease, is a gradual increase and then a gradual decrease in the depth of respiration; Biot’s breathing, which occurs in meningitis affecting the medullary region, is characterized by alternating periods of hyperpnea and apnea, the periods often being of unequal length. Periodic breathing also occurs commonly in animals with electrolyte and acid–base imbalances – there are periods of apnea followed by short bursts of hyperventilation.
Respiratory depth
The amplitude or depth of respiratory movements may be reduced in painful conditions of the chest or diaphragm and increased in any form of anoxia. Moderate increase in depth is referred to as hyperpnea and labored breathing as dyspnea. In dyspnea, the accessory respiratory movements become more prominent: there is extension of the head and neck, dilatation of the nostrils, abduction of the elbows and breathing through the mouth plus increased movement of the thoracic and abdominal walls. Loud respiratory sounds, especially grunting, may also be heard.
Type of respiration
In normal respiration there is movement of the thorax and abdomen. In painful conditions of the thorax, e.g. acute pleurisy, and in paralysis of the intercostal muscles, there is relative fixation of the thoracic wall and a marked increase in the movements of the abdominal wall; there also may be an associated pleuritic ridge caused by thoracic immobility with the thorax expanded. This syndrome is usually referred to as an abdominal-type respiration. The reverse situation is thoracic-type respiration, in which the movements are largely confined to the thoracic wall, as in peritonitis, particularly when there is diaphragmatic involvement.
Thorax symmetry
This can also be evaluated by inspection. Collapse or consolidation of one lung may lead to restriction of movements of the thoracic wall on the affected side. The ‘rachitic rosary’ of enlarged costochondral junctions is typical of rickets.
Respiratory noises or stridors
• Coughing – due to irritation of the pharynx, trachea and bronchi
• Sneezing – due to nasal irritation
• Wheezing – due to stenosis of the nasal passages
• Snoring – when there is pharyngeal obstruction, as in tuberculous adenitis of the pharyngeal lymph nodes
• Roaring – in paralysis of the vocal cords
• Grunting – a forced expiration against a closed glottis, which happens in many types of painful and labored breathing.
An important part of the clinical examination of a horse that produces an externally audible noise, usually a grunt, while working is to determine when the noise occurs in the respiratory cycle. This can be related to limb movements, expiration occurring as the leading foot hits the ground at the canter or gallop. Flexion of the head by the rider will exacerbate the noise.
Abdomen
Variations in abdominal size are usually appreciated during the general inspection of the animal. An increase in size may be due to the presence of excessive feed, fluid, feces, flatus or fat, the presence of a fetus or a neoplasm. Further differentiation is usually possible only on close examination. In advanced pregnancy, fetal movements may be visible over the right flank of cattle. In severe distension of the intestines with gas, the loops of intestine may be visible in the flank, especially in calves. Intestinal tympany usually results in uniform distension of the abdomen whereas fluid tends to result in increased distension ventrally.
The term ‘gaunt’ is used to describe an obvious decrease in the size of the abdomen. It occurs most commonly in starvation, in severe diarrhea and in many chronic diseases where appetite is reduced. An umbilical hernia, omphalophlebitis, or dribbling of urine from a previous urachus may be apparent on visual inspection of the ventral abdominal wall. Ventral edema is commonly associated with approaching parturition, gangrenous mastitis, congestive heart failure, infectious equine anemia, and rupture of the urethra due to obstructive urolithiasis. A grossly enlarged asymmetrical swelling of the flank may suggest herniation of the abdominal wall. Ruminal movements can be seen in the left paralumbar fossa and flank of cattle but a complete examination of the rumen requires auscultation, palpation and percussion, which are described later.
External genitalia
Gross enlargements of the preputial sheath or scrotum are usually inflammatory in origin but varicocele or tumors can also be responsible. Degenerative changes in the testicles may result in a small scrotum. Discharges of pus and blood from the vagina indicate infection of the genitourinary tract.
Mammary glands
Disproportionate size of the udder suggests acute inflammation, atrophy or hypertrophy of the gland. These conditions can be differentiated only by further palpation and examination of the milk or secretions.
Limbs
General abnormalities of posture and gait have been described. Symmetry is important and comparison of the various aspects of pairs of limbs should be used when there is doubt about the significance of an apparent abnormality. Enlargement or distortion of bones, joints, tendons, sheaths and bursae should be noted and so should any enlargement of peripheral lymph nodes and lymphatic vessels.
CLOSE PHYSICAL EXAMINATION
Some of the techniques used in making a close physical examination are set out below.
Palpation
Direct palpation with the fingers or indirect palpation with a probe is aimed at determining the size, consistency, temperature and sensitivity of a lesion or organ. Terms used to describe palpation findings include the following:
• Doughy – when the structure pits on pressure, as in edema
• Firm – when the structure has the consistency of normal liver
• Hard – when the consistency is bone-like
• Fluctuating – when the structure is soft, elastic and undulates on pressure but does not retain the imprint of the fingers
• Tense – when the structure feels like a viscus distended with gas or fluid under some considerable pressure
• Emphysematous – when the structure is puffy and swollen, and moves and crackles under pressure because of the presence of gas in the tissue.
Percussion
In percussion, the body surface is struck so as to set deep parts in vibration and cause them to emit audible sounds. The sounds vary with the density of the parts set in vibration and may be classified as follows:
• Resonant – the sound emitted by organs containing air, e.g. normal lung
• Tympanitic – a drum-like note emitted by an organ containing gas under pressure such as a tympanitic rumen or cecum
• Dull – the sound emitted by solid organs such as heart and liver.
Percussion can be performed with the fingers using one hand as a plexor and one as a pleximeter. In large animals a pleximeter hammer on a pleximeter disk is recommended for consistency.
The quality of the sound elicited is governed by a number of factors. The strength of the percussion blow must be kept constant as the sound volume increases with stronger percussion. Allowances must be made for the thickness and consistency of overlying tissues. For example, the thinner the thoracic wall, the more resonant the lung. Percussion on a rib must not be compared with percussion on an intercostal space. The size and body condition score of the animal are also important considerations. The technique may be relatively ineffective in a fat animal. Pigs and sheep are of a suitable size but the fatness of the pig and the wool coat of the sheep plus the uncooperative nature of both species make percussion impracticable. In mature cattle and horses the abdominal organs are too large and the overlying tissue too thick for satisfactory outlining of organs or abnormal areas, unless the observer is highly skilled. The lungs of cattle and horses can be satisfactorily examined by percussion but this requires practice and experience to become skillful and accurate.
Percussion is a valuable aid in the diagnosis of diseases of the lungs and abdominal viscera of all large animals. Increased dullness over the thorax indicates consolidation of the lung, a pleural effusion, or space-occupying lesion such as tumor or abscess. Increased resonance over the thorax suggests emphysema or pneumothorax.
Ballottement
Ballottement is a technique used to detect floating viscera or masses in the abdominal cavity. Using the extended fingers or the clenched fist the abdominal wall is palpated vigorously with a firm push to move the organ or mass away and then allow it to rebound on to the fingertips. Ballottement of a fetus is a typical example; the fetal prominences can be easily felt by pushing the gravid uterus through the abdominal wall over the right flank in pregnant cattle. Impaction of the abomasum, large tumors and abscesses of the abdominal cavity may also be detected by ballottement. Ballottement and auscultation of the flanks of cattle is also useful to detect fluid-splashing sounds. Their presence on the left side suggests carbohydrate engorgement and excessive quantities of fluid in the rumen, or left-side displacement of the abomasum. Over the right flank, fluid-splashing sounds may indicate intestinal obstruction, abomasal volvulus, cecal dilatation and torsion, and paralytic ileus.
Ballottement and auscultation of the abdomen of the horse with colic may elicit fluid-splashing sounds indicative of intestines filled with fluid, as in intestinal obstruction or paralytic ileus. A modification of the method is tactile percussion, when a cavity containing fluid is percussed sharply on one side and the fluid wave thus set up is palpated on the other. The sensation created by the fluid wave is called a fluid thrill. It is felt most acutely by the palm of the hand at the base of the fingers. Diseases that cause ascites and accumulation of fluid in the peritoneal cavity are examples where this technique is useful.
Auscultation
Direct listening to the sounds produced by organ movement is performed by placing the ear to the body surface over the organ. Indirect auscultation by a stethoscope is the preferred technique. A considerable amount of work has been done to determine the most effective stethoscopic equipment, including investigation of such things as the shape and proportions of bell chest pieces, the thickness of rubber tubes and the diameter and depth of phonendoscope chest pieces. A comparatively expensive unit from a reputable instrument firm is a wise investment. For large animal work, a stethoscope with interchangeable 5 cm diameter phonendoscope and rubber (to reduce hair friction sounds) bell chest pieces is all that is required. The details of the sounds heard on auscultations of the various organs are described in their respective sections. Auscultation is used routinely to assess heart sounds, lung sounds and gastrointestinal sounds.
Percussion and simultaneous auscultation of abdomen
Percussion and simultaneous auscultation of the left and right sides of the abdomen is a useful technique for examination of the abdomen of large animals. The stethoscope is placed over the area to be examined and the areas around the stethoscope and radiating out from it are percussed. This is a valuable diagnostic aid for the detection and localization of a gas-filled viscus in the abdomen of cattle with left-side displacement of the abomasum, right-side dilatation and volvulus of the abomasum, cecal dilatation and torsion, intestinal tympany associated with acute obstruction or paralytic ileus, or pneumoperitoneum.
Simultaneous percussion and auscultation of the abdomen of the horse with colic is useful to detect pings indicative of intestinal tympany associated with intestinal obstruction or paralytic ileus. In diaphragmatic hernia the presence of gas-filled intestines in the thorax may be determined by this method. To elicit the diagnostic ‘ping’, it is necessary to percuss and auscultate side by side and to percuss with a quick, sharp, light and localized force. The obvious method is a quick tap with a percussion hammer or similar object. Another favored method is a ‘flick’ with the back of a forefinger suddenly released from behind the thumb. A gas-filled viscus gives a characteristic clear, sharp, high-pitched ‘ping’ which is distinctly different from the full, low-pitched note of solid or fluid-filled viscera. The difference between the two is so dramatic that it is comparatively easy to define the borders of the gas-filled viscus.
The factors that determine whether a ‘ping’ will be audible are the force of the percussion, the size of the gas-filled viscus and its proximity to the abdominal wall. The musical quality of the ping is dependent on the thickness of the wall of the viscus (e.g. rumen, abomasum, small or large intestines) and the amount and nature of the fluid and gas in the intestines or viscus.
Succussion
This technique, which involves moving the body from side to side to detect the presence of fluid, is an adaptation of the above method. By careful auscultation while the body is moved, free fluid in the intestines or stomach will result in fluid-splashing or tinkling sounds.
Other techniques
Special physical techniques including biopsy and paracentesis are described under special examination of the various systems to which they apply. With suitable equipment and technique, one of the most valuable adjuncts to a physical examination is a radiographic examination. The size, location and shape of soft tissue organs are often demonstrable in animals of up to moderate size. Radiology, other than of limbs and neonates, is not commonly practiced in larger animals. Ultrasound appears to have much more general application but will require its own textbook.
SEQUENCE USED IN THE CLOSE PHYSICAL EXAMINATION
The close physical examination should be performed as quietly and gently as possible to avoid disturbing the patient and thus increasing the resting heart and respiratory rates. At a later stage it may be necessary to examine certain body systems after exercise, but resting measurements should be carried out first. If possible the animal should be standing, as recumbency is likely to cause variation in heart and pulse rates, respiration and other functions.
The sequence used in the close physical examination will vary with the species being examined, the results of the distant examinations, the history obtained, and the diagnostic hypotheses that the clinician has generated. The various parts of the close physical examination that are described here can be modified according to individual circumstances but it is important to do a thorough clinical examination based on the circumstances.
Following the distant examination, and the particular distant examination, it is recommended that the vital signs be determined before the animal is handled for examination of body regions such as the oral cavity.
In general, an appropriate sequence for the close physical examination would be as follows:
• Vital signs: temperature, heart and pulse rates, respirations, state of hydration
• Thorax: heart sounds (rate, rhythm, intensity); lung sounds
• Abdomen: nasogastric intubation
• Head and neck: including eyes, oral cavity, facial structures, and the jugular veins
The important principle is to determine the vital signs before handling and examining other body systems, which may distort the vital signs. The sequence that follows taking the vital signs can vary, based on individual circumstances, the urgency of the case, if any, and the ease of doing the particular examinations. For example, it may be very important to pass a nasogastric tube as one of the first diagnostic techniques in a horse with severe colic associated with gastric distension. When presented with a lactating dairy cow with peracute mastitis, the sequence will be recording the temperature, heart rate and sounds, respirations and status of the lungs, status of the rumen, followed by careful examination of the mammary gland. The close physical examination of each body region or body systems is outlined below.
Vital signs
Temperature
Normally the temperature is taken per rectum. When this is impossible the thermometer should be inserted into the vagina. Ensure that the mercury column is shaken down, moisten the bulb to facilitate entry and, if the anus is flaccid or the rectum full of hard feces, insert a finger also to ensure that the thermometer bulb is held against the mucosa. When the temperature is read immediately after defecation, or if the thermometer is stuck into a ball of feces or is left in the rectum for insufficient time, a false, low reading will result.
As a general rule the thermometer should be left in place for 2 minutes. If there is doubt as to the accuracy of the reading, the temperature should be taken again. The normal average temperature range for the various species at average environmental temperature is as shown in Table 1.1.
Table 1.1 Normal average temperatures with critical points
| Species | Normal temperature | Critical point |
|---|---|---|
| Horse | 38.0°C (100.5°F) | 39.0°C (102.0°F) |
| Cattle | 38.5°C (101.5°F) | 39.5°C (103.0°F) |
| Pig | 39.0°C (102.0°F) | 40.0°C (103.5°F) |
| Sheep | 39.0°C (102.0°F) | 40.0°C (104.0°F) |
| Goat | 39.5°C (103.0°F) | 40.5°C (105.0°F) |
Temperature conversions are approximate.
The reference values in Table 1.1 indicate the average resting temperature for the species and the critical temperature above which hyperthermia can be said to be present. Normal physiological variations occur in body temperature and are not an indication of disease: a diurnal variation of up to 1°C (2°F) may occur, with the low point in the morning and the peak in the late afternoon. There may be a mild rise of about 0.6°C (1°F) in late pregnancy, but a precipitate although insignificant decline just before calving is not uncommon in cows and ewes and lower temperatures than normal occur just before estrus and at ovulation – the degree of change (about 0.3°C; 0.6°F) is unlikely to attract clinical attention.
In sows the body temperature is subnormal before farrowing and there is a significant rise in body temperature coinciding with parturition. This rise is commonly high enough to exceed the critical temperature of 40°C and may be considered erroneously as evidence of disease. The elevation of temperature that occurs in sows at the time of parturition, of the order of 1°C, is maintained through lactation and disappears at weaning.
High environmental humidity and temperature and exercise will cause elevation of the temperature; the deviation may be as much as 1.6°C (3°F) in the case of high environmental temperatures and as much as 2.5–3°C (4.5°F) after severe exercise; in horses, after racing, 2 hours may be required before the temperature returns to normal.
If animals that have been acclimatized to cold outside temperatures are brought indoors to a warmer temperature their body temperatures may exceed the critical temperature within 2–4 hours. Marked temperature variations are an indication of a pathological process:
• Hyperthermia is simple elevation of the temperature past the critical point, as in heat stroke
• Fever or pyrexia is the state where hyperthermia is combined with toxemia, as in most infectious diseases
• Hypothermia, a subnormal body temperature, occurs in shock, circulatory collapse (as in parturient paresis and acute rumen impaction of cattle), hypothyroidism and just before death in most diseases.
Pulse
The pulse should be taken at the middle coccygeal or facial arteries in cattle, the facial artery in the horse and the femoral artery in sheep and goats. With careful palpation a number of characters may be determined, including rate, rhythm, amplitude, tone, maximum and minimum pulse pressures and the form of the arterial pulse. Some of these characters are more properly included in special examination of the circulatory system and are dealt with under that heading.
Rate
The pulse rate is dependent on the heart alone and is not directly affected by changes in the peripheral vascular system. The pulse rate may or may not represent the heart rate; in cases with a pulse deficit, where some heartbeats do not produce a pulse wave, the rates will differ. Normal resting rates (per minute) for the various species are shown in Table 1.2.
| Species | Pulse rate per minute |
|---|---|
| Adult horses | 30–40 |
| Foals up to 1 year | 70–80 |
| Adult cattle | 60–80 |
| Young calves | 100–120 |
| Sheep and goats | 70–90 |
Although there are significant differences in rate between breeds of dairy cow, and between high- and low-producing cows, the differences would not be noticeable to a clinician performing a routine examination. In newborn thoroughbred foals the pulse rate is 30–90 in the first 5 minutes, then 60–200 during the first hour, and then 70–130 during the first 48 hours after birth. Draught horses have heart rates slightly higher than those quoted, which are based on a light horse population. The pulse is not readily palpable in the pig but the comparable heart rate is 60–100 per minute. The same techniques are used in intensive clinical examinations for horses afflicted with the poor performance syndrome.
Bradycardia, or marked slowing of the heartbeat, is unusual unless there is partial or complete heart block, but it does occur in cases of space-occupying lesions of the cranium, in cases of diaphragmatic adhesions after traumatic reticulitis in cattle, or when the rumen is much emptier than normal.
Tachycardia, or increased pulse rate, is common and occurs in most cases of septicemia, toxemia, circulatory failure and in animals affected by pain and excitement. Counting should be carried out over a period of at least 30 seconds.
Rhythm
The rhythm may be regular or irregular. All irregularities must be considered as abnormal except sinus arrhythmia, the phasic irregularity coinciding with the respiratory cycle. There are two components of the rhythm, namely the time between peaks of pulse waves and the amplitude of the waves. These are usually both irregular at the one time, variations in diastolic filling of the heart causing variation in the subsequent stroke volume. Regular irregularities occur with constant periodicity and are usually associated with partial heart block. Irregular irregularities are due to ventricular extrasystoles or atrial fibrillation. Most of these irregularities, except that due to atrial fibrillation, disappear with exercise. Their significance lies chiefly in indicating the presence of myocardial disease.
Amplitude
The amplitude of the pulse is determined by the amount of digital pressure required to obliterate the pulse wave. It is largely a measure of cardiac stroke volume and may be considerably increased, as in the ‘water hammer’ pulse of aortic semilunar valve incompetence, or decreased, as in most cases of myocardial weakness.
State of hydration
The state of hydration is assessed by inspection of the eyes for evidence of dehydration and evaluating the elasticity of the skin. Dehydration is characterized by sunken eyes of varying degrees, and the skin will ‘tent’ when lifted with the fingers and remain tented for varying lengths of time.
EXAMINATION OF BODY REGIONS
After the examination of the temperature, pulse and respirations the physical examination proceeds with an examination of the various body regions.
Thorax
Examination of the thorax includes palpation, auscultation and percussion of the cardiac area (precordium) and the lung area. The wide variations between species in the thickness of the thoracic wall, the size of the animal and the respiratory rate require careful and methodical examination. For example, in the adult horse the thick thoracic wall and the normally slow respiratory rate contribute to an almost soundless respiration on auscultation of the thorax. There is, too, the need to detect minor pulmonary lesions, which may reduce the work performance of the horse only slightly but, because of the importance of perfect fitness in a racing animal, may have major significance. Another important factor that emphasizes the care that must be taken with the examination of the respiratory system of the horse is the ability of racing animals to compensate for even major pulmonary lesions from their immense functional reserve. Because of this, one is likely to encounter horses with massive pulmonary involvement and yet with little obvious impairment of respiratory function.
Cardiac area
Auscultation of the heart is aimed at determining the character of normal heart sounds and detecting the presence of abnormal sounds. Optimum auscultation sites are the fourth and fifth intercostal spaces and, because of the heavy shoulder muscles that cover the anterior border of the heart, the use of a flat phonendoscope chest piece pushed under the triceps muscles is necessary. Extension of the forelimb may facilitate auscultation if the animal is quiet. Areas where the various sounds are heard with maximum intensity are not directly over the anatomical sites of the cardiac orifices, because conduction of the sound through the fluid in the chamber gives optimum auscultation at the point where the fluid is closest to the chest wall.
The first (systolic) sound is heard best over the cardiac apex, the tricuspid closure being most audible over the right apex and mitral closure over the left apex. The second (diastolic) sound is heard best over the base of the heart, the aortic semilunar closure posteriorly and the pulmonary semilunar anteriorly, both on the left side.
In auscultation of the heart, the points to be noted are the rate, rhythm, intensity and quality of sounds and whether abnormal sounds are present. Comparison of the heart and pulse rates will determine whether there is a pulse deficit due to weak heart contractions failing to cause palpable pulse waves; this is most likely to occur in irregular hearts. Normally the rhythm is in three time and can be described as
the first sound being dull, deep, long and loud and the second sound sharper and shorter. As the heart rate increases the cycle becomes shortened, mainly at the expense of diastole and the rhythm assumes a two-time quality. More than two sounds per cycle is classified as a ‘gallop’ rhythm and may be due to reduplication of either the first or second sounds. Reduplication of the first sound is common in normal cattle and its significance in other species is discussed under diseases of the circulatory system.
The rhythm between successive cycles should be regular except in the normal sinus arrhythmia associated with respiration. With irregularity, there is usually variation in the time intervals between cycles and in the intensity of the sounds – louder sounds coming directly after prolonged pauses and being softer than normal sounds after shortened intervals, as in extrasystolic contractions. The intensity of the heart sounds may vary in two ways, absolutely or relatively: absolutely when the two sounds are louder than normal, and relatively when one sound is increased compared to the other in the cycle. For example, there is increased absolute intensity in anemia and in cardiac hypertrophy.
The intensity of the first sound depends on the force of ventricular contraction and is thus increased in ventricular hypertrophy and decreased in myocardial asthenia. The intensity of the second sound depends upon the semilunar closure, i.e. on the arterial blood pressure, and is therefore increased when the blood pressure is high and decreased when the pressure is low.
Abnormal sounds may replace one or both of the normal sounds or may accompany them. The heart sounds are muffled when the pericardial sac is distended with fluid. Sounds that are related to events in the cardiac cycle are murmurs or bruits and are caused mainly by endocardial lesions such as valvular vegetations or adhesions, by insufficiency of closure of valves and by abnormal orifices such as a patent interventricular septum or ductus arteriosus. Interference with normal blood flow causes the development of turbulence with resultant eddying and the creation of murmurs. In attempting to determine the site and type of the lesion it is necessary to identify its time of occurrence in the cardiac cycle: it may be presystolic, systolic or diastolic and it is usually necessary to palpate the arterial pulse and auscultate the heart simultaneously to determine accurately the time of occurrence. The site of maximum audibility may indicate the probable site of the lesion, but other observations, including abnormalities of the arterial pulse wave, should be taken into account. In many cases of advanced debility, anemia and toxemia, soft murmurs can be heard that wax and wane with respiration (hemic murmurs) and are probably due to myocardial asthenia. In cases of local pressure on the heart by other organs, for example in diaphragmatic hernia in cattle, loud systolic murmurs may be heard, probably due to distortion of the valvular orifices.
Abnormal sounds not related to the cardiac cycle include pericardial friction rubs, which occur with each heart cycle but are not specifically related to either systolic or diastolic sounds. They are more superficial, more distinctly heard than murmurs and have a to-and-fro character. Local pleuritic friction rubs may be confused with pericardial sounds, especially if respiratory and cardiac rates are equal.
Palpation of the heart beat has real value: the size of the cardiac impulses can be assessed and palpable thrills may on occasion be of more value than auscultation of murmurs. It is best carried out with the palm of the hand and should be performed on both sides. An increased cardiac impulse, the movements of the heart against the chest wall during systole, may be easily seen on close inspection of the left precordium and can be felt on both sides. It may be due to cardiac hypertrophy or dilatation associated with cardiac insufficiency or anemia or to distension of the pericardial sac with edema or inflammatory fluid. Care should be taken not to confuse a readily palpable cardiac impulse due to cardiac enlargement with one due to contraction of lung tissue and increased exposure of the heart to the chest wall.
Normally, the heart movements can be felt as distinct systolic and diastolic thumps. These thumps are replaced by thrills when valvular insufficiencies or stenoses or congenital defects are present. When the defects are large the murmur heard on auscultation may not be very loud but the thrill is readily palpable. Early pericarditis may also produce a friction thrill. The cardiac impulse should be much stronger on the left than the right side and reversal of this situation indicates displacement of the heart to the right side. Caudal or anterior displacement can also occur.
Percussion to determine the boundaries of the heart is of little value in large animal work because of the relatively large size of the heart and lungs and the depth of tissue involved. The area of cardiac dullness is increased in cardiac hypertrophy and dilatation and decreased when the heart is covered by more than the usual amount of lung, as in pulmonary emphysema. More detailed examination of the heart by electrocardiography, radiographic examination, test puncture and blood pressure are described under diseases of the heart.
Lung area
Auscultation, percussion and palpation are the major methods used for examination of the lungs.
The lung area available for satisfactory auscultation is slightly larger than that available for percussion. The normal breath sounds are heard over most of the lungs, particularly in the middle third anteriorly over the base of the lung, and consist of a soft, sipping VEE–EFF, the latter, softer sound occurring at expiration. The sounds are heard with variable ease depending on the thickness of the chest wall and the amplitude of the respiratory excursion. In well-fleshed horses and fat beef cattle the sounds may not be discernible at rest. The amplitude or loudness of the breath sounds is increased in dyspnea and in early pulmonary congestion and inflammation. The amplitude of the breath sounds is decreased or totally inaudible when there is pleural effusion, and in space-occupying lesions in the lung or pleural cavity. Abnormal lung sounds include crackles, wheezes and pleuritic friction rubs. They are the result of interference with the free movement of air in and out of the lungs, and of the presence of lesions that interfere with the normal movement of the lung and thus create additional respiratory sounds, which are an indication of disease. The descriptions and interpretations of the normal and abnormal lung sounds, and other respiratory noises are described in Chapter 10.
The intensity of abnormal lung sounds may be increased and their clarity improved by measuring the rate and depth of respirations with forced mild exercise such as walking for a few minutes followed by immediate auscultation. If exercise is undesirable the occlusion of both nostrils for 30–45 seconds will be followed by some deep inspirations and accentuation of abnormal lungs. An alternative maneuver which is effective in both horses and cattle is to pull a plastic bag over the muzzle and lower face. When respiratory movements become exaggerated the bag is removed and the lungs auscultated immediately.
Sounds of peristalsis are normally heard over the lung area on the left side in cattle and in horses. In cattle, these sounds are due to reticular movement and in horses to movements of the colon. Their presence is not of much significance in these species unless there are other signs. In cattle, too, sounds of swallowing, eructation and regurgitation may be confused with peristaltic sounds; ruminal movements and the esophagus should be observed for the passage of gas or a bolus to identify these sounds. Other techniques for examination of the thorax are described under diseases of the respiratory system (Ch. 10).
Palpation of the thoracic wall may reveal the presence of a pleuritic thrill, bulging of the intercostal spaces when fluid is present in the thoracic cavity, or narrowed intercostal spaces and decreased rib movement over areas of collapsed lung.
Percussion may be by the usual direct means, or indirectly by tracheal percussion when the trachea is tapped gently and the sound is listened for over the lung area. By direct percussion within the intercostal spaces the area of normal lung resonance can be defined and abnormal dullness or resonance detected. Increased dullness may indicate the presence of a space-occupying mass, consolidated lung, edematous lung or an accumulation of fluid. In a pleural effusion the upper limit of the area of dullness can be determined by percussion and the fluid line can be delineated and identified and used to assess the progress of therapy.
An overloud normal percussion note is obtained over tissue containing more air than usual, e.g. emphysematous lung. A definite tympanitic note can be elicited over pneumothorax or a gas-filled viscus penetrating through a diaphragmatic hernia. For percussion to be a satisfactory diagnostic aid, affected areas need to be large with maximum abnormality, and the chest wall must be thin.
Abdomen
Clinical examination of the abdomen includes:
• Visual inspection of the abdominal contour for evidence of distension or gauntness
• Auscultation of the gastrointestinal sounds
• Palpation and percussion through the abdominal wall
Auscultation
Auscultation of the abdomen is an essential part of the clinical examination of cattle, horses and sheep. It is of limited value in pigs. The intestinal or stomach sounds will indicate the nature of the intraluminal contents and the frequency and amplitude of gastrointestinal movements, which are valuable aids in clinical diagnosis. The intensity, duration and frequency of the sounds should be noted. All these characteristics will be increased in animals that have just eaten or immediately following excitement.
Auscultation of the rumen of cattle and sheep
This is a very useful part of the clinical examination. In normal animals there are 1–2 primary contractions per minute, involving the reticulum and the dorsal and ventral sacs of the rumen; the frequency depends on the amount of time that has elapsed since feeding and the type of food consumed. Secondary contractions of the dorsal and ventral sacs of the rumen occur at about 1 per minute and are commonly associated with eructation. The examination is made in the left paralumbar fossa and a normal sequence of sounds consists of a lift of the flank with a fluid gurgling sound, followed by a second more pronounced lift accompanied by a booming, gassy sound. Auscultation over the lower left ribs will reveal the fainter fluid sounds of reticular contractions just prior to the contractions of the dorsal and ventral ruminal sacs described above. The reticular and ruminal sounds are the predominant abdominal sounds in the normal ruminant.
A grunt, detectable by auscultation over the trachea, may occur during the reticular contraction phase of a primary contraction in cattle with traumatic reticuloperitonitis. The factors that result in a decrease in the intensity and frequency of ruminal sounds are discussed in detail in Chapter 6.
The intestinal sounds that are audible on auscultation of the right flank of cattle and sheep consist of frequent faint gurgling sounds, which are usually difficult to interpret. The contraction of the abomasum and the intestines result in a mixture of sounds that are difficult to distinguish.
Intestinal sounds of the horse
These sounds are clearly audible and their assessment is one of the most vital parts of the clinical examination and surveillance of the horse with suspected abdominal disease. Over the right and ventral abdomen there are the loud, booming sounds (borborygmi) of the colon and cecum, which are at peak intensity about every 15–20 seconds. Over the left abdomen there are the much fainter rushing fluid sounds of the small intestines. An increase in the intensity and frequency of sounds with a distinct fluid quality are heard in enteritis and loud, almost crackling, sounds in spasmodic colic. In impaction of the large intestine there is a decrease in the intensity and frequency of the borborygmi, and in thromboembolic colic due to verminous aneurysm and infarction of the colon there may be complete absence of sounds. In intestinal obstruction the intestinal sounds due to peristalsis are markedly decreased and usually absent and fluid tinkling sounds occur infrequently. In intestinal stasis in the horse, auscultation in the right flank often detects the tinkling sound of fluid dropping from the ileocecal valve through gas into the dorsal sac of the cecum.
Palpation and percussion through the abdominal wall
Because of the thickness and weight of the abdominal wall in mature cattle and horses, deep palpation of viscera and organs through the abdominal wall has limited value in these species compared to its usefulness in small animals. No viscera or organ, with the exception of the fetus, can be palpated with certainty through the abdominal wall in the horse. In cattle, the rumen and its contents can usually be palpated in the left paralumbar fossa. Ruminal distension is usually obvious while an inability to palpate the rumen may be due to a small, relatively empty rumen or to medial displacement, as in left-side displacement of the abomasum.
Percussion and simultaneous auscultation
In left-side displacement of the abomasum, percussion and simultaneous auscultation over the upper third of the costal arch between the 9 th and 12 th ribs of the left side will elicit the typical high-pitched musical-quality sounds or ping. These may be mistaken for similar sounds present in ruminal atony. A markedly enlarged liver in a cow may be palpable by ballottement immediately behind the right costal arch. Using a combination of palpation, percussion and simultaneous auscultation over the right paralumbar fossa and caudal to the entire length of the right costal arch it may be possible to detect any of the following in cattle:
• Dilatation and torsion of the abomasum
• Cecal dilatation and torsion
• Impaction of the abomasum and omasum
• Intestinal obstructions, including torsion of the coiled colon.
Percussion and auscultation over viscera that are distended with fluid and gas may be undertaken and the size and location of the tympanitic area will provide some indication of the viscera likely to be involved.
Tactile percussion of the abdomen
This technique aids detection of an excessive quantity of fluid in the peritoneal cavity: ascites due to a ruptured bladder, transudate in congestive heart failure and exudate in diffuse peritonitis. A sharp blow is struck on one side of the abdomen and a fluid wave, a ‘blip’ or undulation of the abdominal wall, can be seen and felt on the opposite side of the abdomen. The peritoneal cavity must be about one-third full of fluid before a fluid wave can be elicited.
Abdominal pain
The location of abdominal pain may be located by deep external palpation of the abdominal wall in cattle. Deep palpation with a firm uniform lift of the closed hand or with the aid of a horizontal bar held by two people under the animal immediately caudal to the xiphoid sternum is a useful aid for the detection of a grunt associated with traumatic reticuloperitonitis in cattle. Superficial pain may be elicited by a firm poke of the hand or extended finger in cattle or horses. In cattle, pain may be elicited over the right costal arch when there are liver lesions or generally over the abdomen in diffuse peritonitis.
The response to palpation of a focus of abdominal pain in cattle is a ‘grunt’ which may be clearly audible without the aid of a stethoscope. However, if there is doubt about the audibility of the grunt, the simultaneous auscultation of the trachea will detect a perceptible grunt when the affected area is reached. In calves with abomasal ulceration, a focus of abdominal pain may be present on deep palpation over the area of the abomasum.
In cases of severe abdominal distension (ruminal tympany in cattle, torsion of the large intestine) it is usually impossible to determine, by palpation and percussion, the viscera that are distended. Pneumoperitoneum is rare and thus gross distension of the abdomen is usually due to distension of viscera with gas, fluid or ingesta. A combination of rectal examination, passage of a stomach tube, paracentesis and exploratory laparotomy may be necessary to determine the cause.
The abdomen of pigs is difficult to examine by palpation because pigs are seldom sufficiently quiet or relaxed and the thickness of the abdominal wall limits the extent of deep palpation. In late pregnancy in sows the gravid uterus may be ballotted but it is usually not possible to palpate fetal prominences.
In sheep, the rumen, impacted abomasum and the gravid uterus are usually palpable through the abdominal wall. Positioning the sheep on its hindquarters will shift the viscera to a more easily palpable position.
Nasogastric intubation
An important part of the examination of the abdomen and gastrointestinal tract of large animals, especially cattle and horses, is the passage of the nasogastric tube into the rumen of cattle and into the stomach of horses. Gastric reflux occurs commonly in the horse with colic and it is important to determine if the stomach is distended with fluid and to relieve it as necessary. This topic is presented in detail in the chapter dealing with equine colic. In cattle, when disease of the rumen is suspected, the nasogastric tube is passed into the rumen to relieve any distension and to obtain a sample of rumen juice for determination of rumen pH and the presence or absence of rumen protozoa.
Head and neck
Eyes
Any discharge from the eyes should be noted: it may be watery in obstruction of the lacrimal duct, serous in the early stages of inflammation and purulent in the later stages. Whether the discharge is unilateral or bilateral is of considerable importance; a unilateral discharge may be due to local inflammation, a bilateral discharge may denote a systemic disease. Abnormalities of the eyelids include abnormal movement, position and thickness. Movement may be excessive in painful eye conditions or in cases of nervous irritability including hypomagnesemia, lead poisoning and encephalitis. The lids may be kept permanently closed when there is pain in the eye or when the eyelids are swollen, as for instance in local edema due to photosensitization or allergy. The membrana nictitans may be carried across the eye when there is pain in the orbit or in tetanus or encephalitis. There may be tumors on the eyelids.
Examination of the conjunctiva
This examination is important because it is a good indicator of the state of the peripheral vascular system. The pallor of anemia and the yellow coloration of jaundice may be visible, although they are more readily observed on the oral or vaginal mucosa. Engorgement of the scleral vessels, petechial hemorrhages, edema of the conjunctiva as in gut edema of pigs or congestive heart failure, and dryness due to acute pain or high fever are all readily observable abnormalities.
Corneal abnormalities
These include opacity, varying from the faint cloudiness of early keratitis to the solid white of advanced keratitis, often with associated vascularization, ulceration and scarring. Increased convexity of the cornea is usually due to increased pressure within the eyeball and may be due to glaucoma or hypopyon.
Size of the eyeball
Eyeball size does not usually vary but protrusion is relatively common and when unilateral is due in most cases to pressure from behind the orbit. Periorbital lymphoma in cattle, dislocation of the mandible and periorbital hemorrhage are common causes. Retraction of the eyeballs is a common manifestation of reduction in volume of periorbital tissues, e.g. in starvation when there is disappearance of fat and in dehydration when there is loss of fluids.
Abnormal eyeball movements
Abnormal movements occur in nystagmus due to anoxia or to lesions of the cerebellum or vestibular tracts. In nystagmus there is periodic, involuntary movement with a slow component in one direction and a quick return to the original position. The movement may be horizontal, vertical or rotatory. In paralysis of the motor nerves to the orbital muscles there is restriction of movement and abnormal position of the eyeball at rest.
Examination of the deep structures
Assessment of the deep structures of the eye necessitates an ophthalmoscope but gross abnormalities may be observed by direct vision. Pus in the anterior chamber, hypopyon, is usually manifested by yellow to white opacity often with a horizontal upper border obscuring the iris. The pupil may be of abnormal shape or abnormal in position due to adhesions to the cornea or other structures. An abnormal degree of dilatation is an important sign, unilateral abnormality usually suggesting a lesion of the orbit.
Bilateral excessive dilatation (mydriasis) occurs in local lesions of the central nervous system affecting the oculomotor nucleus, or in diffuse lesions including encephalopathies, or in functional disorders such as botulism and anoxia. Peripheral blindness due to bilateral lesions of the orbits may have a similar effect. Excessive constriction of the pupils (miosis) is unusual unless there has been overdose with organic phosphatic insecticides or parasympathomimetic drugs. Opacity of the lens is readily visible, especially in advanced cases.
Vision tests
Several tests of vision and of ocular reflexes are easily carried out, and when warranted should be done at this stage of the examination. Tests for blindness include the menace reflex and an obstacle test. In the former a blow at the eye is simulated, care being taken not to cause air currents. The objective is to elicit the eye preservation reflex manifested by reflex closure of the eyelids. This does not occur in peripheral or central blindness and in facial nerve paralysis there may be withdrawal of the head but no eyelid closure. An obstacle test in unfamiliar surroundings should be arranged and the animal’s ability to avoid obstacles assessed. The results are often difficult to interpret if the animal is nervous. A similar test for night-blindness (nyctalopia) should be arranged in subdued light, either at dusk or on a moonlit night. Nyctalopia is one of the earliest indications of avitaminosis-A. Total blindness is called amaurosis, partial blindness is called amblyopia. The pupillary light reflex – closure and dilatation of the iris in response to lightness and darkness – is best tested with a strong flashlight.
Nostrils
Particular attention should be paid to the odor of the nasal breath. There may be a sweet sickly smell of ketosis in cattle or a fetid odor, which may originate from any of a number of sources including gangrenous pneumonia, necrosis in the nasal cavities or the accumulation of nasal exudate. Odors originating in the respiratory tract are usually constant with each breath and may be unilateral. The sour smell of alimentary tract disturbance is detectable only periodically, coinciding with eructation. Odors originating in the mouth from bad teeth or from necrotic ulcers associated with Fusobacterium necrophorum in calves may be smelled on the nasal breath but are stronger on the oral breath.
In certain circumstances it may be important to note the volume of the breath expelled through the nostrils: it may be the only way of determining whether the animal is breathing and, in some cases, of counting the respiratory rate. Variation in volume between nostrils, as felt on the hands, may indicate obstruction or stenosis of one nasal cavity. This can be examined further by closing off the nostrils one at a time; if obstruction is present in one nostril, closure of the other causes severe respiratory embarrassment.
Any nasal discharge that is present should receive special attention and its examination should be carried out at the same time as an inspection of the nasal mucosa. Discharges may be restricted to one nostril in a local infection or be bilateral in systemic infection. The color and consistency of the exudate will indicate its source. In the early stages of inflammation the discharge will be a clear, colorless fluid, which later turns to a white to yellow exudate as leukocytes accumulate in it. In Channel Island cattle the color may be a deep orange, especially in allergic rhinitis. A rust or prune juice color indicates blood originating from the lower respiratory tract, as in pneumonia and in equine infectious anemia in the horse. Blood clots derived from the upper respiratory tract or pharynx may be present in large quantities, or appear as small flecks. In general, blood from the upper respiratory tract is unevenly mixed with any discharge, whereas that from the lower tract comes through as an even color.
The consistency of the nasal discharge will vary from watery in the early stages of inflammation, through thick, to cheesy in longstanding cases. Bubbles or foam may be present. When the bubbles are coarse it signifies that the discharge originates in the pharynx or nasal cavities; fine bubbles originate in the lower respiratory tract. In all species, vomiting or regurgitation caused by pharyngitis or esophageal obstruction may be accompanied by the discharge of food material from the nose or the presence of food particles in the nostrils. In some cases the volume of nasal discharge varies from time to time, often increasing when the animal is feeding from the ground, leading to infection of cranial sinuses.
Inflammation of the nasal mucosa varies from simple hyperemia, as in allergic rhinitis, to diffuse necrosis, as in bovine malignant catarrh and mucosal disease, to deep ulceration as in glanders. In hemorrhagic diseases variations in mucosal color can be observed and petechial hemorrhages may be present.
Mouth
Excessive salivation, with ropes of saliva hanging from the mouth and usually accompanied by chewing movements, occurs when a foreign body is present in the mouth and also in many forms of inflammation of the oral mucosa or of the tongue. Actinobacillosis of the tongue, foot-and-mouth disease and mucosal disease are typical examples. Excessive salivation may also occur in diseases of the central nervous system, as in acute lead poisoning in young cattle. Hypersalivation is a characteristic sign in epidermic hyperthermia associated with the mycotoxins of Acremonium coenophialum and Claviceps purpurea and by the fungus Rhizoctonia leguminicola sometimes found on red clover. Dryness of the mouth occurs in dehydration and poisoning with belladonna alkaloids, or when high levels of urea are fed.
Abnormalities of the buccal mucosa include local lesions, hemorrhages in purpuric diseases, the discolorations of jaundice and cyanosis and the pallor of anemia. Care must be taken to define the exact nature of lesions in the mouth, especially in cattle; differentiation between vesicles, erosive and ulcerative lesions is of diagnostic significance in the mucosal diseases of this species.
Teeth
Examination of the teeth for individual defects is a surgical subject but a general examination of the dentition can yield useful medical information. Delayed eruption and uneven wear may signify mineral deficiency, especially calcium deficiency in sheep; excessive wear with mottling and pitting of the enamel is suggestive of chronic fluorosis.
Tongue
The tongue may be swollen by local edema or by inflammation as in actinobacillosis of cattle, or shrunken and atrophied in post-inflammatory or nervous atrophy. Lesions of the lingual mucosa are part of the general buccal mucosal response to injury.
Pharynx
Examination of the pharyngeal region in large animals requires some dexterity and the use of a speculum of appropriate size. The oral cavity and pharynx of calves, lambs and goat kids is examined by holding the mouth open, depressing the base of the tongue with the fingers or a tongue depressor and viewing the pharynx, the glottis and the proximal part of the larynx and arytenoid cartilages. In adult cattle, a metal or Plexiglass cylindrical speculum, 45 cm in length and 4 cm in diameter, placed in the oral cavity and over the base of the tongue will allow viewing of the pharynx and the larynx. Foreign bodies, diffuse cellulitis and pharyngeal lymph node enlargement can also be detected by this means. The use of a speculum wedged between the upper and lower molar teeth in cattle allows manual exploration and evaluation of lesions of the pharynx and proximal part of the larynx. In the horse, the pharynx cannot be viewed from the oral cavity and manual exploration of the pharynx requires general anesthesia. Endoscopy is a useful method of examination in this species, and the modern fiberoptiscope has made it possible to visualize lesions in the posterior nares and pharynx–esophagus, larynx–trachea in the standing, conscious horse or ox.
Submaxillary region
Abnormalities of the submaxillary region that should be noted include enlargement of lymph nodes due to local foci of infection, subcutaneous edema as part of a general edema, local cellulitis with swelling and pain, enlargement of salivary glands or guttural pouch distension in the horse. Thyroid gland enlargement is often missed or mistaken for other lesions, but its site, pulsation and surrounding edema are characteristic.
Neck
The most important part of the examination of the neck of cattle and horses is to determine the state of the jugular veins. Bilateral engorgement of the jugular veins may be due to obstruction of the veins by compression or constriction, or to right-side congestive heart failure. A jugular pulse of small magnitude moving up the jugular vein about one-third of the way up the neck is normal in most animals but it must be differentiated from a transmitted carotid pulse, which is not obliterated by compression of the jugular vein at a lower level. Variations in size of the vein may occur synchronously with deep respiratory movements but bear no relation to the cardiac cycles. When the jugular pulse is associated with each cardiac movement it should be determined whether it is physiological or pathological. The physiological pulse is presystolic and due to atrial systole, and is normal. The pathological pulse is systolic and occurs simultaneously with the arterial pulse and the first heart sound; it is characteristic of an insufficient tricuspid valve.
Local or general enlargement of the esophagus associated with vomiting or dysphagia occurs in esophageal diverticulum, stenosis and paralysis, and in cardial obstructions. Passage of a stomach tube or probang can assist in the examination of esophageal abnormalities.
Tracheal auscultation is a useful diagnostic aid. Normally, the sounds that are audible are louder and more distinct than breath sounds audible over the lung. In upper respiratory tract disease such as laryngitis and tracheitis, the sounds are louder and harsher and may be whistling in the presence of stenosis. Very loud stenotic tracheal sounds are characteristic of calves with tracheal collapse. Abnormal tracheal sounds, regardless of their cause, are usually transferred down the major bronchi and are audible on auscultation over the thorax, primarily during inspiration. They are commonly confused with abnormal lung sounds due to pneumonia, but in pneumonia the abnormal sounds are usually present both on inspiration and on expiration.
Rectal examination
Rectal exploration of the abdomen is a vital part of the complete examination of the abdomen of large animals, especially cattle and horses. Abnormalities that are completely unexpected may be present and may be the cause of illness in animals in which no other significant clinical abnormalities were detected on clinical examination. Special care is necessary to avoid injuring the patient and causing it to strain. Suitable lubrication and avoidance of force are the two most important factors. Rectal examination enables observations to be made on the alimentary, urinary and genital tracts and on the vessels, peritoneum and pelvic structures. The amount and nature of the feces in the rectum should be determined.
Palpable abnormalities of the digestive tract include paralysis and ballooning of the rectum, distension of the loops of the intestine with fluid or gas, the presence of hard masses of ingesta as in cecal and colonic impactions in the horse, and intestinal obstruction due to volvulus, intussusception or strangulation. The detection of tight bands of mesentery leading to displacement segments may be a valuable guide. In cattle, the caudal sacs of the rumen are readily palpable. When the rumen is distended as in bloat or vagus indigestion they may push well into the pelvis or be only just within reach when the rumen is empty. A distended abomasum may be felt in the right half of the abdomen in cases of abomasal torsion and occasionally in vagus indigestion. In healthy animals there is little to feel because of the space occupied by normal intestines. Palpable objects should be carefully examined.
The left kidney in the cow can be felt in the midline and distinct lobulations are evident. In the horse, the caudal pole of the left kidney is easily palpable, but the right kidney is not. There may be abnormalities of size in pyelonephritis, hydronephrosis and amyloidosis, and pain on pressure in pyelonephritis. The ureters are not normally palpable nor is the empty bladder. A distended bladder or chronic cystitis with thickening of the wall can be felt in the midline at the anterior end of the pelvic cavity. Abnormalities of the bladder and ureters in cattle are also palpable through the ventral aspects of the vagina. Large calculi have a stone-like hardness and are occasionally observed in horses in the same position. Pain with spasmodic jerking of the penis on palpation of the urethra occurs in urinary obstruction due to small calculi, cystitis and urethritis. Enlarged, thickened ureters such as occur in pyelonephritis can be felt between the kidney and the bladder.
On the peritoneum and mesentery one may feel the small, grape-like lesions of tuberculosis, the large, irregular, hard masses of fat necrosis and the enlarged lymph nodes of lymphomatosis. The abdominal aorta is palpable, and in horses the anterior mesenteric artery and some of its branches can be felt. This may be an important examination if a verminous aneurysm is suspected, in which case the vessels are thickened but still pulsate, have an uneven rough surface and may be painful. In horses the caudal edge of the spleen is usually palpable in the left abdomen. During a rectal examination in a horse it is advantageous in some cases to palpate the inguinal ring from inside the abdomen and, by pushing the other hand between the horse’s thighs, to palpate the external ring simultaneously. It is then easier to decide whether any abnormal structures are passing through the ring.
Feces and defecation
Examination of the feces may provide valuable information on the digestive and motor functions of the tract. They should be examined for volume, consistency, form, color, covering, odor and composition. Note should be made of the frequency and the time taken for material to pass through the tract. Laboratory examinations may be advisable to detect the presence of helminth eggs, occult blood, bile pigments, pathogenic bacteria or protozoa.
The volume of feces is usually described scant, normal or copious but, in certain circumstances, it may be advisable to weigh or measure the daily output. The normal output for each species is as follows:
There is an increased bulk when much fiber is fed or during attacks of diarrhea. The consistency and form of the feces varies with each species and varies widely within a normal range, depending particularly on the nature of the food. Variations in consistency not explainable by changes in the character of the feed may indicate abnormalities of any of the functions of the tract. The consistency is more fluid in diarrhea and less fluid than normal in constipation. The consistency and form of the feces may provide some indication of the location of the dysfunction of the gastrointestinal tract. In general, large quantities of liquid feces suggest a dysfunction of the small intestine where normally most of the fluid is absorbed. If the feces contain large quantities of undigested feed this suggests overfeeding, incomplete mastication, a digestive enzyme deficiency or an acute disorder of the small intestine or stomachs. Large quantities of soft feces that contain well-digested ingesta suggest a dysfunction of the large intestine. However, these are only guidelines and are subject to error.
Color of the feces
This also varies widely with the color of the food, but feces of a lighter color than normal may be caused by an insufficient secretion of bile or by simple dilution of the pigments, as occurs in diarrhea. The effect of blood on the appearance of feces has already been described. Discoloration by drugs should be considered when the animal is undergoing treatment.
Fecal odor
This depends largely on the nature of the food eaten but in severe enteritis the odor is characteristically one of putrefaction.
Composition
The composition of the feces should be noted. In herbivorous animals, there is always a proportion of undigested fiber but excessive amounts suggest incomplete digestion due to, for example, bad teeth and faulty mastication. Excessively pasty feces are usually associated with a prolonged sojourn in the tract such as occurs in vagal indigestion or abomasal displacement in cattle. Foreign material of diagnostic significance includes sand or gravel, wool, and shreds of mucosa. Mucus is a normal constituent but, in excessive amounts, indicates either chronic inflammation, when it is associated with fluid, copious feces, or constipation when the feces are small in volume and hard. Mucosal shreds or casts always indicate inflammation.
Frequency of defecation
Frequency and the length of sojourn in the gastrointestinal tract are usually closely allied, increased frequency and decreased sojourn occurring in diarrhea and the reverse in constipation. Most animals defecate eight to 12 times a day but the sojourn varies widely with the species. Omnivores and carnivores with simple stomachs have an alimentary sojourn of 12–35 hours. In ruminants it is 2–4 days and in horses 1–4 days, depending on the type of feed.
Other observations
Observation of other acts associated with the functions of the alimentary tract may provide information of diagnostic value. Prehension, mastication, swallowing, vomiting and defecation should be observed and an attempt made to analyze the behavior of the animal when there is evidence of abdominal pain.
Paracentesis of the abdomen
Paracentesis of the abdomen includes obtaining a sample of peritoneal fluid when peritonitis or inflammation of the serosae of the intestines or other viscera of the abdomen is suspected. Aspiration of fluid from a distended abdominal viscus is also possible and may aid in the diagnosis.
Urinary system
Examination of the urinary tract consists of observations of the act of urination, evidence of difficult and painful urination, abnormal urine, collection of urine and urinalysis, and, depending on the species, palpation of the kidneys, bladder and urethra. Details of the examination of the urinary tract are presented in Chapter 11.
Reproductive tract
Examination of the reproductive tract is usually carried out at this stage but is not discussed here because it is dealt with adequately in texts on diseases of the genital system. In the immediate postpartum period, the vagina, cervix and uterus should be examined thoroughly for evidence of gross abnormalities such as metritis, retained placenta and ruptured uterus, which may be the cause of illness not obvious on examination of other body systems.
Mammary gland
The mammary gland(s) of all species is examined by inspection and palpation of the udder and teats, and gross examination of the milk or abnormal secretions of the glands. Details of this examination are presented in Chapter 15.
Musculoskeletal system and feet
Examination of the musculoskeletal system and feet is necessary when there is lameness, weakness, or recumbency. Inspection of the gait during the walk and trot is used to determine the origin of the lameness. The muscles, joints, ligaments, tendons, and bones are inspected and palpated to determine abnormalities associated with lameness, weakness or recumbency. The feet are examined by inspection, palpation and the trimming of hooves in farm animals to identify lesions associated with lameness. Medical imaging is commonly used to define lesions not readily recognizable by routine clinical examination. Details of examination of the musculoskeletal system and feet are presented in Chapter 13.
Nervous system
In routine veterinary practice, veterinarians will commonly include several components of a neurological examination in a complete clinical examination. Most often a diagnosis and differential diagnosis can be made from consideration of the history and the clinical findings. However, if the diagnosis is uncertain it may be necessary to conduct a complete neurological examination, which may uncover additional clinical findings necessary to make a diagnosis and give a prognosis.
A complete neurological examination includes examination of the mental status, head and posture, cranial nerve function, gait and posture, function of the neck and forelimbs, function of the trunk and hindlimbs, palpation of the bony encasement of the central nervous system, examination of cerebrospinal fluid, medical imaging of the bony skeleton of the head and vertebral column. The details of the neurological examination are presented in Chapter 12.
Skin including ears, hooves and horns
A systematic method for the examination of the skin is necessary to avoid misinterpretation of the lesions. Inspection of the behavior of the animal and of the skin and hair, and palpation and smelling of the skin are the most common physical methods used for clinical examination of the skin. The important prerequisites for an adequate examination of the skin are good lighting such as natural light or day-type lamps, clipping the animal’s hair when necessary to adequately visualize lesions, magnification of the lesions with a hand lens to improve visualization of the changes, and adequate restraint and positioning of the animal. Palpation can be used to assess the consistency of lesions, the thickness and elasticity of skin, and to determine the presence of pain associated with diseases of the skin.
Close inspection and palpation of the skin and hair coat are necessary to identify and characterize lesions. Magnifying spectacles or an illuminated magnifying glass may prove useful. The dorsal aspect of the body is inspected by viewing it from the rear, as elevated hairs and patchy alopecia may be more obvious from that angle. All parts of the head including the nose, muzzle and ears are examined. The lateral trunk and the extremities are then examined. The feet of large animals need to be picked up to examine the interdigital clefts and parts of the coronary bands. The skin of the udder and teats of cattle, sheep and goats, and horses must be observed. The ventral aspect of the body is carefully examined using a source of light to illuminate the underside of adult cattle and horses. The external and internal aspects of the ears, and the hooves and horns must be examined by inspection and palpation.
Every centimeter of the skin needs to be examined for the presence of lesions in different stages of development. The visual, tactile and olfactory senses are used to see, feel and smell the lesions. The presence or absence of some ectoparasites can be determined by direct inspection. For example, lice and ticks of cattle are usually easily visible. The odor of the skin in some diseases may be abnormal; dermatophilosis in cattle is characterized by a foul and musty odor. Parting the hairs with the fingers or by gently blowing them is necessary to evaluate the length of the hair shafts. Broken hairs, changes in hair color and the accumulation of exudative material on hair shafts are noted. The texture and elasticity of the skin must be assessed by rolling the skin between the fingers. Careful digital palpation of the hair coat which appears normal on visual inspection may reveal underlying lesions such as pustules which may be covered by the hair coat. In some cases, tufts of hairs may be seen protruding through an accumulation of exudate. A combination of visual inspection of the wool coat of sheep is done carefully and systematically by parting the wool coat and evaluating the condition of the wool fibers and the underlying skin. The hair coat should not be clipped, groomed or washed before the lesions have been identified and characterized.
DIAGNOSTIC ULTRASONOGRAPHY
Diagnostic ultrasonography in animals is the continuation of the clinical examination
Ultrasonography has developed into a valuable imaging technique in almost all animal species because of the rapid development of technically improved portable units and their potential use at any given location, which is important in farm animals not being examined in a veterinary clinic. It is indeed a continuation of the clinical examination.1
The ultrasonographic examination is unique in its patient application because it is a dynamic examination technique with no risk to the patient or the sonographer. It is a continuation of the clinical examination. Ultrasonography is noninvasive, and well tolerated in unsedated animals. It enables serial examinations to monitor the progression of an abnormality or response to treatment. Ultrasonography requires considerable skill and experience to make a diagnosis. Some practitioners may hesitate before investing considerable resources in an ultrasound machine if they feel it will not be used regularly and if they believe they do not have enough time for the examination. Continuing education courses and workshops are becoming more common and they provide excellent training and the latest concepts. When employed correctly, ultrasonography is of great benefit to every veterinary clinician and practitioner in continuing the clinical examination. Ultrasonography can be valuable in examining the contents of cavitary lesions, synovial cavities, cysts or other fluid-filled lesions for the presence of liquid, semisolid or solid contents and/or effusion. Centesis of synovial cavities or body cavities, and biopsy of organs such as liver or kidney are now frequently done as part of the clinical examination. Ultrasonography enables accurate needle placement following ultrasonographic examination of the designated structure, assisting with the measurement of the distance from the skin surface to the structure when, for example, a freehand biopsy technique is to be performed.
The literature on the history of the development, advances and application of ultrasound in animals has been reviewed.2
When a pulse of ultrasound is directed into a substance, varying amounts are reflected back to the source according to the material encountered and the returning signal conveys information regarding the structures it has penetrated. Real-time brightness or ‘B’ mode imaging is currently the form of ultrasound most commonly used. Examination of moving structures such as the heart required a technique known as time motion or ‘M’ mode ultrasound.
During a routine ultrasound examination, real-time B mode provides information regarding the physical form and structure of tissues, allows subjective assessment of movement such as peristaltic contractions within the intestine and provides an overview that guides the application of other ultrasound modes. M mode is now an integral part of echocardiographic examinations and all modern ultrasound machines are equipped with this capability.
The benefits of ultrasound as a veterinary diagnostic imaging procedure are numerous.2 Routine examinations have no harmful biological effects. It is a safe procedure for the animal, the operator and nearby personnel, allowing it to be done in any location without the need for specific safety precautions.
The ability of ultrasound to distinguish fluid from soft tissue and differentiate between soft tissues on the basis of their composition makes it more suited than radiography for examining soft tissue structures. Ultrasonography can often provide information that was previously only available through exploratory laparotomy. Ultrasound is limited by its inability to penetrate gas-filled or bony structures; therefore ‘acoustic windows’ must be found that avoid the interposition of bone or gas between the transducer and the region of interest, although this can often be achieved by judicious positioning of the patient. Transcutaneous examinations in animals require removal of the hair overlying the region of interest by clipping, as the beam cannot penetrate the air trapped between the hairs.
Examples of the use of ultrasonography in bovine practice include the diagnosis of gastrointestinal disease,3 diseases of the mammary gland,4 thoracic disease,5 splenic disease,6 ruptured gall bladder in cows7 and the blood flow patterns in the common carotid artery and external jugular vein for cardiac and blood vessel disease.8
The use of ultrasonography as a reproductive management aid in dairy cattle practice represents a major advance in understanding reproductive biology in cattle.9 The literature on the veterinary ultrasound equipment, imaging the bovine ovary (ovarian follicles, corpora lutea, ovarian cysts), the bovine uterus (early pregnancy diagnosis, early embryonic loss, identification of cows carrying twins, determination of fetal sex) and the diagnostic limitations of ultrasonic imaging has been reviewed.9 Because nonpregnancy can be established 7–14 days earlier after artificial insemination (AI) using ultrasound compared with rectal palpation, nonpregnant cows can be detected earlier and returned to AI service, thereby improving the pregnancy rate through an increased AI service rate.
The use of ultrasonography to examine various body systems is described briefly in their respective chapters in the General Medicine part of the textbook. Readers are encouraged to consult the publications listed under Review Literature and References, and textbooks dealing with ultrasonography. Short courses and laboratory workshops are now commonplace and readily available and highly recommended. The development of extension education programs to train bovine practitioners is a critical step toward rapid implementation of this technology into the dairy industry.
Braun U. Fluckiger M, Kahn W, et al, editors. Atlas und Lehrbuch der Ultraschalldiagnostik beim Rind. Berlin: Parey Buchverlag im Blackwell Wisseshafts-Verlag, 1997.
Radostits OM, Mayhew IG, Houston DM. Veterinary clinical examination and diagnosis. London: WB Saunders, 2000.
Braun U. Ultrasonography in gastrointestinal disease in cattle. Vet J. 2003;166:112-124.
King AM. Development, advances and applications of diagnostic ultrasound in animals. Vet J. 2006;171:408-420.
Kofler J. Diagnostic ultrasonography in animals — Continuation of the clinical examination? Vet J 2006; In press.
Making a diagnosis
The practice of clinical veterinary medicine consists of two major facets: the making of a diagnosis and the provision of treatment and control measures. For treatment and control to be of optimum value the diagnosis must be as accurate as possible, so that diagnosis is the crux of all medical problems.
A diagnosis is the identification of the disease affecting the patient, and to be complete should include three parts:
• The abnormality of structure or function produced by the causative agent, and which is inimical to normal body processes
• The clinical manifestation of that abnormality produced by the causative agent.
For recording purposes the animal species should also be included, for example, ‘equine Rhodococcus equi pneumonia and lung abscess’. Many diagnoses fall short of this objective because of lack of confirmatory laboratory assistance. So clinical signs (such as bovine chronic diarrhea) or necropsy lesions (such as bovine polioencephalomalacia) are often used.
DIAGNOSTIC METHODS
At least five distinctly recognizable methods are used and they are presented here in order of increasing complexity. As a general rule the experienced clinician uses more of the simpler strategies, the novice clinician more of the complex ones. This is because the simple method omits several steps in the clinical reasoning process – the sort of appropriate and safe ‘cutting of corners’ that it is possible to carry out with confidence only after gaining wide experience and after paying a good deal of attention to assessing one’s own personal competence as a clinician and especially as a diagnostician.
METHOD 1: THE SYNDROME OR PATTERN RECOGNITION
In the first few moments of viewing the patient, e.g. the pain-generated behavior of a horse with abdominal pain or the skin lesions of ecthyma in a sheep or papillomatosis in a cow, the diagnosis is made instantaneously and reflexly. The same experience may occur while taking the history: one may have to rely entirely on the history in the case of a cow having an epileptic seizure to be able to diagnose it. This recognition is based on the comparison of the subject case and previous cases in the clinician’s memory and the one is recognized as a replica of the other. There is no need to seek further supporting advice and the definitive diagnosis is made then and there. In the hands of the wise and experienced clinician the method is quick and accurate.
METHOD 2: HYPOTHETICO-DEDUCTIVE REASONING
As soon as the client begins to relate the presenting signs, usually commencing with the key clinical sign, the clinician begins to draw up a short list of diagnostic possibilities, usually three or four. This is the process of generating multiple plausible hypotheses from initial cues. The clinician then begins to ask questions and conduct clinical examinations that test the hypotheses. The questions and examinations may be directed at supporting or discounting the tentative diagnoses (the confirm/exclude technique) but they may lead to the addition of more hypotheses and the deletion of some others. (The questions used here are search ones, aimed at supporting a hypothesis, and are distinctly different from scanning questions, which are ‘fishing’ expeditions looking for more key signs about which to ask search questions.) This process of hypothesis and deduction is continued until one diagnosis is preferred to the others. The original list of hypotheses may be expanded but not usually to more than seven, and in the final stages is usually reduced to two or three. These are then arranged in order of preference and become the list of diagnostic possibilities.
In farm animal medicine there is usually a general absence of both hard primary data and ancillary data such as clinical pathology, so that the clinician may be in the position of having to provide treatment for two or three possible illnesses. An example is the parturition syndrome of recently calved dairy cows in which the treatment of subacute mastitis, metritis and acetonemia is standard procedure because the clinician is uncertain about which disease is most accountable for the illness. In the more resourceful arena of a veterinary teaching hospital it may still be necessary to proceed in this way in the first instance but then to narrow down the list of hypotheses when additional information is received from the laboratory. This polypharmacy approach has a number of disadvantages, among which are included the additional expense and the increased possibility of contamination of food products of animal origin by medications, especially antibiotics and sulfonamides, and with resistant strains of bacteria.
One of the important characteristics of this strategy is the dependence on the selection of a critical or key clinical sign or cue on which to base the original hypotheses. The selection of the key sign and additional supporting clinical findings is done instinctively by experienced clinicians on the basis of prior experience in similar situations. For novice clinicians it may be necessary to examine two or more key signs.
METHOD 3: THE ARBORIZATION OR ALGORITHM METHOD
This is really an extension of method 2 but the hypothetico-deductive reasoning method is formalized and carried out according to a preplanned program. The hypothetico-deductive reasoning method depends on the clinician remembering and being aware of an all-inclusive list of diagnostic possibilities in the case under consideration. Because memory is unreliable and impressionistic the method is subject to error by omission. The arborization or algorithmic method similarly approaches a listed series of diagnoses and examines each one in turn with supporting or disproving questions; if they pass the proving test they stay in, if they fail it they are deleted. For example, a key sign of red urine in a cow promotes the question: Has the cow had access to plant substances that color the urine red? If the answer is no, the next question is: Is the red color caused by hemoglobinuria or hematuria? If the answer is hemoglobinuria, all the diagnoses on the hematuria branch of the algorithm are deleted and the questioner proceeds to the next question, which will attempt to determine whether the cow has postparturient hemoglobinuria or any one of a number of diseases characterized by intravascular hemolysis.
Provided that the list of possible diagnoses is complete and is frequently updated as new diagnoses become available – and, just as importantly, as new ways of supporting or discounting each hypothesis are added as soon as they are published – the method works well. These algorithms are eminently suited to computerization and can be made available by the supply of floppy disks or by access to a central database via a modem, the online database, or dial-up information system.
The arborization method is well suited to the clinician who has not had the necessary experience for the memorization of long lists of potential diagnoses and the critical tests that confirm or exclude each of them. Because the algorithms are likely to include all the recorded diagnoses that have that particular key sign, error by omission is not a risk. Thus they are also valuable to the specialist, who is less able to afford an omission than the general practitioner and certainly cannot really afford to miss even the most obscure and unlikely diagnosis. Another major advantage is that they provide a system of tests that should be performed and clinical findings that should be searched for – which is really a form of clinical protocol, acting as a reminder of the sequential diagnostic steps to be taken. The arrangement of the algorithm represents the clinical reasoning of the person who designed it and it should have considerable merit, assuming that the designer was an expert. This characteristic does arouse the comment that the method does away with the need for the clinicians to do their own clinical reasoning. That may be so, but the interests of optimum clinical care of patients are probably better served by having first-year interns apply the clinical reasoning of a specialist and as a consequence achieve significantly better results.
METHOD 4: THE KEY ABNORMALITY METHOD
This is a more time-consuming method than the previous ones and requires that clinicians rely on their knowledge of normal structure and function to select the key abnormality or clinical cue. The method consists of five steps and is summarized in Figure 1.1.
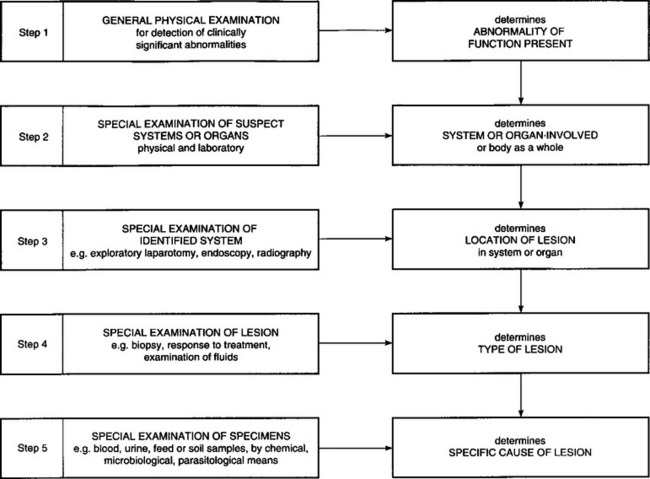
Determination of the abnormality of function present
Disease is abnormality of function which is harmful to the animal. The first step is to decide what abnormality of function is present. There may of course be more than one and some clinically insignificant abnormalities may be present, e.g. a physiological cardiac murmur in a newborn foal. Definition of the abnormality is usually in general terms such as paralysis, state of the alimentary tract, hypoxia, respiratory insufficiency, nervous shock and so on. These terms are largely clinical, referring to abnormalities of normal physiological function, and their use requires a foreknowledge of normal physiology. It is at this point that the preclinical study of physiology merges into the clinical study of medicine.
The necessary familiarity with the normal, combined with observation of the case in hand, makes it possible to determine the physiological abnormality that may be, e.g. hypoxia. The next step is to determine the body system or body as a whole or organ involved in the production of the hypoxia.
Determination of the system or body as a whole or organ affected
Having made a careful physical examination and noted any abnormalities, it is then possible to consider which body system or organ is the cause of the abnormality. In some cases the body as a whole may be involved. This may not be difficult with some systems: for example, hypoxia may be due to failure of the respiratory or circulatory systems and examination of these is not difficult. However, special problems arise when attempting to examine the nervous system, the liver, kidney, endocrine glands, spleen and hemopoietic systems. Here, routine physical examination by palpation, auscultation and percussion is not very rewarding: special ancillary examination techniques with the aid of a laboratory are usually necessary. These are described under special examination methods for the various systems. As a guiding principle, all functions of the organ under examination should be observed and any abnormalities noted. For example, if the integrity of the central nervous system is to be examined, the clinician would look for abnormalities of mental state, gait, posture, muscle and sphincter tone and involuntary movements, abnormal posture and paralysis. Knowing the normal physiological functions of systems, one looks for aberrations of them.
When only simple physical examination is available it may be extremely difficult to choose between two or more systems as the possible location of the abnormality. For example, in an animal that is unable to rise from the recumbent position it may be difficult to decide whether the nervous system or the musculoskeletal system or generalized weakness from a systemic illness is the origin of the clinical recumbency. If special diagnostic techniques and laboratory evaluations are inconclusive or not available, it may be necessary to resort to probability as a guide. For example, paresis due to diseases of the muscles is most common in young calves, lambs and foals and generally uncommon in mature farm animals, with the exception of the myopathy associated with the downer cow syndrome in dairy cattle. However, paresis is common in mature cows affected with parturient hypocalcemia, peracute coliform mastitis and acute diffuse peritonitis.
Determination of the location of the lesion within the system or organ affected
The location of the lesion within the body system involved is not always obvious and may require special physical and laboratory examination techniques. For example, a detailed neurological examination may be necessary to localize the lesion in an animal with manifestation of disease of the nervous system. This may be combined with radiographic techniques such as myelography. An exploratory laparotomy with or without biopsy techniques may be necessary to determine the location of an intestinal lesion thought to be the cause of chronic diarrhea. Endoscopy is rapidly becoming standard practice for the localization of lesions of the respiratory tract of the horse. Radiography is often necessary to localize lesions of the musculoskeletal system and diseases of the feet of horses and cattle.
Determination of the type of lesion
The abnormality observed may be produced by lesions of different types. In general, lesions can be divided into anatomical or physical lesions and functional disturbances. The physical lesions can be further subdivided into inflammatory, degenerative or space-occupying. These classifications are not mutually exclusive, as a lesion may be both inflammatory and space-occupying: abscesses in the spinal cord or lung are typical examples. In these circumstances it is necessary to modify the diagnosis and say that such and such a lesion is space-occupying and may or may not be inflammatory.
The differentiation between functional disturbances and physical lesions is often extremely difficult because the abnormalities produced may be identical. For example, in a case of hypomagnesemia in a cow there is no physical lesion but differentiation from the encephalitis of furious rabies may be impossible. As a rule, functional disturbances are transient, often recurrent or fluctuating and are readily reversible by treatment, whereas structural lesions cause changes that are relatively static or at least change slowly and are affected only gradually by treatment. This is by no means a regular rule: the acute abdominal pain of intestinal obstruction usually fluctuates but the lesion is a physical one, whereas the paralysis of parturient paresis in cattle is static but the disturbance is functional only.
Differentiation between inflammatory, degenerative and space-occupying lesions is usually simpler. The latter produce signs characteristic of pressure on surrounding organs and can often be detected by physical means. Inflammatory lesions are characterized by heat, pain, swelling and a local or general leukocytosis and, in severe cases, a systemic toxemia. A total white blood cell count and differential is a sensitive but nonspecific test for the presence of an infection. A leukopenia, neutropenia and a degenerative left shift suggests a severe infection. A neutrophilia and regenerative shift suggests an active chronic infection. The most common infections of cattle, which are often not readily obvious, are in the thoracic and abdominal cavities (pleuritis, pulmonary abscesses, pericarditis and peritonitis). Degenerative lesions produce the same loss or abnormality of function as lesions of the other types but are not usually accompanied by evidence of inflammation unless they are extensive. If the lesion is accessible, biopsy should be considered as a means of determining its nature.
Determination of the specific cause of the lesion
If in the system involved, the nature of the abnormality and the type of lesion can be satisfactorily determined, it then remains to decide on the specific causative agent. If, for example, it could be said that a particular case of paralysis in a calf was caused by a degenerative lesion of the musculature, only a few specific etiological agents would have to be considered to make a final diagnosis. In many, if not most cases it is impossible to go beyond this stage without additional techniques of examination, particularly laboratory examinations, and it is a general practice to make a diagnosis without this confirmatory evidence because of limitations of time or facilities.
It is at this stage that a careful history-taking and examination of the environment show their real value. It is only by a detailed knowledge of specific disease entities, the conditions under which they occur, the epidemiology and the clinical characteristics of each disease that an informed judgment can be made with any degree of accuracy. If the diagnostic possibilities can be reduced to a small number, confirmation of the diagnosis by laboratory methods becomes so much easier because there are fewer examinations to be made and confirmation by response to treatment is easier to assess. If it is necessary to treat with a great many drugs serially or in combination to achieve a cure, the expense is greater and the satisfaction of both the client and the veterinarian is diluted in proportion to the range of treatments. Accuracy in diagnosis means increased efficiency, and this is the final criterion of veterinary practice.
METHOD 5: THE DATABASE METHOD
The basis of this method (also called the Weed or problem-oriented method, is to conduct a complete clinical and clinicopathological examination of the patient in order to acquire a comprehensive patient database. The problems (key signs) in this database are then matched with the diagnostic database, in which collections of signs or syndromes are labeled with diagnoses, to select the best fit with the patient’s data.
This method also uses the problem-oriented veterinary medical record system, which is an excellent system for the daily recording of clinical and laboratory data in an orderly, systematic and consistent manner that can be easily followed by clinicians and their colleagues. This system is now used widely by veterinary teaching hospitals. The system has four components based on the four phases of veterinary medical action:
The progress notes are created daily and divided into four parts known collectively by the acronym SOAP to designate:
The method requires that clinicians be very painstaking in their examination and recording. It places great demands on the time spent by clinicians and clinical pathologists, on laboratory resources and on clinical record storage. Much of the data has no diagnostic significance because the diagnostic decisions are made largely on the presence or absence of relatively few key signs. It also has the disadvantage that there is a tendency to make the patient fit a category. It is the opposite of the key abnormality method, in which only the signs and other indicants relevant to the proposed diagnosis are sought and recorded. Because of its requirement of time and data recording and storage this method is not suitable for use in food animal medicine, where speed is a vital component of the diagnostic process. As mentioned earlier, however, it is an excellent system for the teaching of clinical veterinary medicine.
The method is really an expanded version of the hypothetico-deductive method, where the hypotheses are made sequentially as further information becomes available. In the database method all the hypotheses are pursued in parallel because all the possible data have been collected into the patient’s database. The source of error in the method is the possibility of undue importance being attached to a chance abnormality in, say, the clinical biochemistry. If the abnormality cannot be matched to a clinical sign, it should be weighted downwards in value or marked for comment only. The same error may result from inclusion of a sign that is important, e.g. diarrhea, but that happens to be present at low intensity.
INTERPRETATION OF LABORATORY DATA
WHEN TO COLLECT LABORATORY DATA
Collection of a full history and performance of a purposeful physical examination are the most powerful tools available to the veterinarian in determining the nature of an animal’s disease and its likely cause. However, laboratory data, including results of clinical, biochemical, hematologic, serologic, radiographic, electrocardiographic, ultrasonographic and other examinations, are often obtained from individual animals or groups of animals. The reasons for collecting laboratory data can be summarized as:
• To confirm the presence or cause of a disease
• To assess the severity of a disease
• To predict the clinical course of a disease or to determine a prognosis
• To estimate the likely response to therapy
• To determine the response to therapy or monitor progression of a disease
• To satisfy regulatory requirements
• To determine the disease or immune status of an animal, herd or flock.
Collection of laboratory data should not be viewed as a fishing expedition performed in the hope that ‘something will turn up’. The decision to collect laboratory data should always be made with one or more of the above aims, with the intention that the data collected will answer a particular, clearly stated question. It is very easy, when faced with a sick animal with clinical signs that are not clearly diagnostic or indicative of the organ system involved, to request a ‘serum biochemical profile’ and complete blood count without having a clear idea of the usefulness of the information provided by the results of these tests. While the usefulness of these tests in most cases is very clear, the results of the tests are most informative when used to address a particular question, for instance: does the animal have evidence of kidney disease?
A test should never be performed unless one can anticipate all the likely results and provide a meaningful interpretation for each. Collecting laboratory data for the sake of running a test or as an act of diagnostic desperation is wasteful of resources and will not, in all likelihood, contribute to management of the animal or group of animals. It is more likely that the results of the test will be uninterpretable and will muddy the diagnostic picture.
PROPERTIES OF DIAGNOSTIC TESTS
The following properties of a test, and of the population to which it is applied, should be known before it is considered to be reliable:
• The test should be developed and validated in the population of interest. Tests developed in one population might not be valid in an animal from another population. For instance, tests developed for use in one species might not be reliable if used in another species
• You should know how accurate the test is in the situation in which you intend to use it
• The specificity of the test, i.e. the ability of a positive result of the test to rule in the disease of interest, should be known. While this is a property of the test that is usually independent of the prevalence of the disease in the population being tested, this might not always be the case
• The sensitivity of the test, i.e. the ability of a negative result of the test to rule out the disease of interest, should be known. While this is a property of the test that is usually independent of the prevalence of the disease in the population being tested, this might not always be the case
• The pre-test likelihood of the disease in the population should be known. This permits calculation of post-test odds of the animal having (positive predictive value) or not having (negative predictive value) the disease for which it is being tested
• The likelihood ratios of the various test results should be known for the population of animals being tested
• The reliability of the laboratory performing the test should be known. There should be considerable confidence in the quality control of the laboratory such that test results are repeatable and reliable
• Are the references ranges (values in animals without the disease or condition of interest) known and with what certainty are they known? The meaning of an abnormal test result should be clear
• The test should allow you to rule in or rule out one of the differential diagnoses, in the instance in which a test is being used for diagnostic, as opposed to monitoring or other purposes
• All test results should be interpretable. In other words, all results should provide information that will be of use in diagnosis or monitoring.
Utility
To be useful, a diagnostic test must be accurate. An accurate test reliably differentiates between normal and diseased animals, thereby contributing to effective management of the animal or its disease. Inaccurate diagnostic tests provide unreliable data, which in the best scenario are useless and in the worst scenario cause mismanagement of the animal or its disease. The diagnostic accuracy of a test should be known before it is used extensively and a test of unknown diagnostic accuracy should be assumed to be inaccurate until proven otherwise.
The usefulness of a test to a veterinarian depends on a number of factors. Firstly, the test must be accurate, as discussed above. Secondly, it should be technically feasible and reliable, i.e. the test must be readily performed and its characteristics (listed above) must be known. A test that cannot be readily performed has minimal usefulness and unreliable tests are inaccurate. For testing of analytes, such as serum biochemical analysis or serology, it is important that the analysis yields results that are accurate and precise. Laboratory tests that are accurate yield results that are the same (or very close to) the true value of the variable being measured. Precise tests yield results that have very little variability around the expected value. Note that a test can be precise without being accurate, i.e. it has little variability but yields a value that is different from the actual value. Tests that are inaccurate or are highly variable (have poor precision) are not useful because the results are unreliable.
Thirdly, the test must have diagnostic utility in that the results of the test should enable the veterinarian to make a decision that will affect the subsequent management of the animal or its disease. If the results of the test will not alter the animal’s management or treatment of its disease nor improve its production or prognosis, then the test has no diagnostic utility and should not be performed. The diagnostic utility depends on the characteristics of the test in the population of animals being tested. The important characteristics, which should be known before the test is widely used, are the sensitivity and specificity of the test and the likelihood ratios associated with the possible results, in the population in which it will be used. That a test has sensitivity and specificity implies that there is a range of values expected in normal animals, the so-called ‘reference range’.
Reference range (Interval)
An important aspect of evaluating laboratory data is to decide whether or not the result of a test is consistent with the animal being healthy or diseased. Healthy animals are assumed to have values within a certain range, whereas diseased animals may have values that differ from that expected in a healthy animal. The range of values in healthy animals is often referred to as being the ‘normal range’ although, because of the statistical connotation of this term, ‘reference range’ or ‘reference interval’ is preferred.
The reference range represents the range of values of a test that are expected in a group of healthy animals. Animals with values outside the reference range are at increased risk of having the disease, compared to animals with values within the reference range. The actual increase in risk of being diseased depends on the way in which the reference range was determined, the sensitivity and specificity of the test and the prevalence of the disease in the population from which the animal was selected. Calculation of likelihood ratios, both positive and negative, is a useful means of quantitatively assessing the results of a test.
The reference range for a particular test is usually developed by collecting values from a large number of healthy or ‘normal’ animals and performing a statistical analysis of the values. For variables that have a range of possible values (e.g. serum urea nitrogen concentration), as opposed to being either present or absent (e.g. seropositive or seronegative for antibodies to a disease), the range of values in normal animals will have a characteristic spread. For the range of values of the variable in normal animals, an upper and a lower value are chosen that represent the upper and lower limits of the reference range. These values are usually chosen to include 95% of the values from normal animals, calculated as the mean value for the population of normal animals plus or minus 2 standard deviations, or as the 2.5–97.5 percentile range.
Problems with reference ranges
There are problems with using the reference range of normal animals to diagnose diseased animals. Firstly, 5% of normal animals will have values for the test that are outside the reference range and may be incorrectly diagnosed as being diseased (false positive). Although a 5% false-positive rate is very low, the error is compounded when batteries of tests are run at the same time. This is a potentially serious problem when interpreting data from a serum biochemical profile analysis, in which 20 or more analytes may be measured simultaneously from one animal. The risk of the value of any one analyte being outside the normal range is only 5%, but when 20 analytes are measured simultaneously the chance of finding one analyte of the 20 with a value outside the reference range is almost 66% (100(1–0.9520)).
This problem can be mitigated in several ways. Firstly, serum biochemical profiles often contain more than one variable that is indicative of a particular disorder. If disease affecting a particular organ system is present, then there should be appropriate changes in all variables indicative of disease in this system. For instance, most serum biochemical profiles measure both serum creatinine and urea nitrogen concentrations. An elevation in the serum urea nitrogen concentration may be indicative of renal disease, but if the serum creatinine concentration is not also increased, then the likelihood of important renal dysfunction is much less than if both analytes were above the reference range. Secondly, disease may be associated only with marked increases in value of the variable such that unusually low values could be disregarded. For example, a serum creatinine concentration below the reference range is very unlikely to indicate the presence of renal disease, and a serum creatine kinase activity below the reference range has almost no diagnostic value. Thirdly, the extent to which the variable is outside the reference range should be considered. A small difference from the reference range is much less likely to indicate the presence of disease than is a much larger difference – calculation of likelihood ratios is one way of expressing this effect of variables that are markedly abnormal.
Another problem with using the reference range to detect disease is that not all diseased animals will have a value for the variable of interest that is outside the normal range. Some diseased animals will have values of useful variables that are within the reference range and these animals may be falsely diagnosed as not having the disease (false negative). This problem can be mitigated by reducing the size of the reference range, although this will increase the false-positive rate, or by measuring other variables that are also useful in detecting the suspected disease. For instance, an animal with liver disease may have a value of the serum activity of a hepatic enzyme that is within the reference range suggesting the lack of liver disease (a false-negative result). However, the same animal may have marked increases in serum bilirubin and bile acid concentrations, findings strongly suggestive of liver disease.
Sensitivity and specificity
The sensitivity of a test is a measure of the test’s ability to detect animals that are diseased and its numerical value represents the proportion of animals with the disease that are detected by the test (Table 1.3). A test with high sensitivity will detect most diseased animals within a population.
Table 1.3 Method for determining sensitivity, specificity, likelihood ratio for positive and negative tests, positive predictive value and negative predictive value of a test
| True disease status Disease present | Disease absent | |
|---|---|---|
| Test positive | True positive (TP) | False positive (FP) |
| Test negative | False negative (FN) | True negative (TN) |
Sensitivity = (TP/[TP + FN]) ×100
Specificity = (TN/[FP + TN]) × 100
Likelihood ratio positive test = Sensitivity/(1 – Specificity)
Likelihood ratio negative test = Specificity/(1 – Sensitivity)
Positive predictive value = TP/(TP + FP)
Negative predictive value = TN/(TN + FN)
The specificity of a test is a measure of the test’s ability to detect animals that are not diseased and its numerical value represents the proportion of normal animals detected by the test. A highly specific test will rule out the disease in most normal animals. Stated another way, a negative result for a test with high sensitivity effectively rules out the disease being tested for, whereas a positive test result for a test of high specificity effectively rules in the disease for which the animal is being tested.
Sensitivity and specificity are intrinsic properties of the test and their values are not influenced by the likelihood before the animal is tested that it has the disease for which it is being tested. The ability of a test to detect whether an animal has a particular disease depends on the likelihood that the animal has the disease at the time it is tested (the prevalence of disease in the population from which the animal being tested is drawn) as well as on the sensitivity and specificity of the test. The sensitivity and specificity can be combined to produce a single number, the likelihood ratio.
Likelihood ratio
The likelihood ratio is an overall measure of the efficiency of the diagnostic test, combining both sensitivity and specificity (Table 1.3) and permitting the calculation of post-test odds of the disease from the pre-test odds of disease. The likelihood ratio is a quality of the test and is not influenced in most instances by the prevalence of the disease in the population. The likelihood ratio is useful for quantifying the post-test odds of an animal having the disease. For instance, in hospitalized neonatal foals, a positive stall-side test for failure of transfer of passive immunity has a likelihood ratio of 4.86. A foal with pretest probability of having the disease of 50% that has a positive test (i.e. indicative of lack of passive immunity) therefore has a post-test probability of having the disease of 81%.1
Positive and negative predictive value
The combined effects on the ability of the test to correctly detect diseased or healthy animals of (a) the prevalence of the disease and (b) the sensitivity and specificity of the test can be calculated and are called the positive predictive value (PPV) and negative predictive value (NPV) respectively. These are important values because they determine the usefulness of the test in detecting diseased, or normal, animals. The positive predictive value is the likelihood that a positive test is from an animal with the disease. The negative predictive value is the likelihood that a negative test is from an animal that does not have the disease.
Both the PPV and NPV are inextricably linked to the prevalence of the disease in the population being tested. Reports of the PPV and NPV are therefore only useful for populations of animals similar to those in which the values of these variables was determined, especially with regard to the prevalence of the disease in the population. The prevalence of the disease can also be viewed as the probability that an animal selected at random from the population has the disease – it is the pretest probability of disease in the animal. For a test of given sensitivity and specificity, the likelihood that a positive test correctly predicts the presence of disease (the PPV) increases as the proportion of diseased animals in the population increases (the disease has higher prevalence). Conversely, the NPV increases as the prevalence of the disease decreases.
The effect of changes in prevalence on the PPV and NPV of two tests with differing sensitivities and specificities is illustrated in Table 1.4. The probability that either test will detect the presence of disease in an animal with a high pretest likelihood of having the disease is very high. Similarly, the probability that a negative result is indicative of the absence of disease in an animal from a population with very low prevalence of disease is also very high. Importantly, the ability of a very good test (sensitivity and specificity both 95%) to correctly predict the presence of disease in an animal with a positive test from a population with a low prevalence (1% of animals affected) of the disease is very poor. Applied to an individual animal, this means that even a very good test is likely to yield an incorrect result in an animal that is unlikely to have the disease.
Table 1.4 Effect of changes in prevalence (pretest probability of disease) on the positive predictive value (PPV) and negative predictive value (NPV) of tests with 95% sensitivity and specificity (Test A) and 60% sensitivity and specificity (Test B)
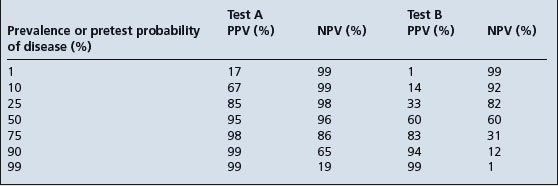
Conversely, although the test result is very unlikely to be incorrect, a positive result in an animal with a very high pretest probability of having the disease yields little further information. The test result does not increase the likelihood of the animal having the disease by very much. The diagnostic test has its greatest utility when the pretest probability of disease is approximately 50% and the increase in PPV and NPV is much greater for a test with higher sensitivity and specificity.
The pre-test probability of disease, and thus the positive predictive value of the test, can be increased by selecting animals to be tested through careful physical examination and collection of an appropriate history. The PPV of a test in an animal that has signs of the disease being tested for is much higher than the PPV of a test in an animal without signs of the disease. Testing clinically normal animals is more likely to yield false-positive than true-positive results and such indiscriminate testing is not wise.
COMPUTER-ASSISTED DIAGNOSIS
In the 1980s there was considerable interest in computer-assisted diagnosis. The entry of the clinical and laboratory data from a patient into a computer program could yield a differential diagnosis list of diseases in order of highest to lowest probability. However, despite over 20 years of activity and interest in the use of computers for diagnosis, the impact of computer-assisted diagnosis in medical practice has been slight. Computerized programs have been useful in circumscribed areas such as the differential diagnosis of abdominal pain in humans and the diagnosis and treatment of meningitis. However, no program developed for use in a specific localized area of the body has been successfully adapted for generalized use. Theoretically, the computer could be expected to be useful to aid the clinician with the workup in order to make multiple and complex diagnoses.
Research on clinical decision-making has confirmed the importance of creating the list of differential diagnoses or diagnostic hypotheses. A clinician faced with a diagnostic problem must use clinical findings to develop a list of possible diagnoses. With a knowledge of the epidemiological and clinical characteristics of each disease, the veterinarian can confirm or exclude certain diagnostic possibilities. Diagnostic acumen depends on the ability to recognize the most important clinical abnormalities and to generate a list of differential diagnoses – a task that becomes more efficient with experience.
Specialists can generate many differential diagnoses in a narrow area of expertise, but the breadth of knowledge required in general practice makes it difficult for generalists to keep current on rare or unusual conditions. If a disease is not considered by the clinician faced with a presenting problem, it is frequently overlooked as a possibility and may not be ‘stumbled-on’ during the diagnostic process. This problem is complicated in veterinary education by the common practice of teaching according to disease entity. All the nosology of a disease is presented in a standard format but the information must then be used in reverse order in clinical practice: the clinician generates a list of diseases based on the history and clinical findings. Textbooks that feature lists of differential diagnoses for animals with similar clinical findings assist in this task, but rapidly become outdated because of the many major and minor clinical findings that can be associated with a disease. The large storage capacity of computer databases and the ease of access to stored data makes the computer useful for handling this sort of information.
The success of a computer-assisted diagnosis will depend first on the clinician determining the important finding or forceful feature or pivot of the case, which can be useful in separating possible look-alike diseases. The second most important requirement is to know the propensity for a certain clinical finding to occur in a disease syndrome. The algorithm is the center of a computer-aided diagnostic system. Statistical algorithms calculate the most likely diagnosis from explicit statistical analysis of disease probabilities and the frequency of clinical findings in a particular disease.1 A statistical algorithm is based on the Bayes theorem. The posterior probability that an animal has a given disease can be calculated if one has access to:
• The incidence (prior probability) of the disease
• The probability of a given clinical finding if the animal has the disease
• The probability of the same clinical finding occurring if the animal has the disease.
After receiving the data, the computer uses this theory to calculate the likelihood of various diseases. However, a major problem of a Bayesian system is the nonavailability of an order of probabilities of the incidence of diseases and clinical findings associated with them. There is a need in veterinary medicine to generate comprehensive databases from which the probabilities of incidence and clinical finding for each disease can be determined from actual clinical practice.
In spite of these limitations, some progress is being made in the development of computer-assisted diagnosis in veterinary medicine. One computer-assisted diagnostic system for veterinary medicine was developed at the College of Veterinary Medicine, Cornell University, Ithaca, NY. The CONSULTANT program designed by M. E. White and J. Lewkowicz2 is available on the Internet at: http://www.vet.cornell.edu. The Web version of the CONSULTANT program is based on the 1996 database. Direct access to the most current database of CONSULTANT at the College is possible using dial-in or telnet.
The data bank contains a description of several thousand diseases of dogs, cats, horses, cattle, sheep, pigs and goats. For each disease, there is a short description, including information on diagnostic testing, a list of current references, and a list of the clinical findings that might be present in the disease. The clinician enters one or more of the clinical findings present in a patient. The computer supplies a list of the diseases in which that clinical finding or combination of clinical findings are present. The complete description can be retrieved for any disease in the list of differential diagnoses. The program is available by long-distance telephone and a modem. A major limitation of the program to date is that the list of differential diagnoses is not in order of probability from highest to lowest. This is because the program does not include the probability of incidence and clinical findings for each disease, information that, as mentioned earlier, is not yet available.
Experience with the Cornell CONSULTANT program has shown that computer-assisted diagnosis is not used in day-to-day management of routine cases but is used primarily when faced with an unusual problem, to provide assurance that a diagnosis was not overlooked. Computerized databases also offer a mechanism for the generalist to search through a complete list of differential diagnoses compiled from the recorded experience of many specialists and kept current as new information is published. Practitioners feel that having access to CONSULTANT is also a significant part of continuing education and a source of references. Experience with a computer-assisted diagnostic system has also confirmed the importance of an accurate history and an adequate clinical examination. If an important clinical finding is not detected, or not adequately recognized – for example, mistaking weakness of a limb for lameness due to musculoskeletal pain – the computer program will be ineffective. Disagreement between observers about the meaning of a clinical finding will also continue to be a problem as computer-assisted diagnosis becomes more widely used.
At the present time, the most important service the computer can provide in making a diagnosis is the generation of a hypothesis through the generation of a list of differential diagnoses, and access to further information. Computers will probably not be able to make a definitive etiological diagnosis but they are able to remind the user of diagnoses that should be considered and to suggest the collection of additional data that might have diagnostic value.
Prognosis and therapeutic decision-making
The dilemma of whether or not to administer a certain drug or perform a certain operation in an animal patient with or without an established diagnosis, or when the outcome is uncertain, is familiar to veterinarians. Owners of animals with a disease, or merely a minor lesion, expect to receive a reasonably accurate prediction of the outcome and the cost of treatment, but often considerable uncertainty exists about the presence or absence of a certain disease, or its severity, because confirmatory diagnostic information is not available.
The information required for a reasonably accurate prognosis includes:
• The expected morbidity and case fatality rates for the disease
• Whether or not a specific treatment or surgical operation is available or possible
If success is dependent on prolonged and intensive therapy, the high cost may be prohibitive to the owner, who then may select euthanasia of the animal as the optimal choice. Veterinarians have an obligation to keep their clients informed about all the possible outcomes and the treatment that is deemed necessary, and should not hesitate to make strong recommendations regarding the treatment or disposal of a case. There are also different levels of outcome, which may affect the prognosis and therapeutic decision-making. In the case of breeding animals, mere survival from a disease is insufficient and treatment is often not undertaken if it is unlikely that it will result in complete recovery and return to full breeding capacity. Slaughter for salvage may be the most economical choice. In other cases, e.g. a pleasure horse, the return of sufficient health to permit light work may satisfy the owner.
DECISION ANALYSIS
Veterinarians must routinely make decisions that have economic consequences for the client and the veterinarian. Questions such as whether to vaccinate or not, whether to treat an animal or recommend slaughter for salvage value, whether or not to perform surgery, or even which surgical procedure to use to correct a case of left-side displacement of the abomasum, are common.3 Many of these questions are complex, requiring several successive decisions, and each decision may have more than one outcome. Clinical decisions are not only unavoidable but also must be made under conditions of uncertainty. This uncertainty arises from several sources and include the following:
• Errors in clinical and laboratory data
• Ambiguity of clinical data and variations in interpretations
• Uncertainty about the relationships between clinical information and presence of disease
• Uncertainty about the effects and costs of treatment
• Uncertainty about the efficacy of control procedures such as vaccination or the medication of feed and water supplies in an attempt to control an infectious disease.
The process of selecting a management plan from a range of options involves a mental assessment of the available options and their probable outcomes. Decision analysis provides a framework for handling complex decisions so that they can be more objectively evaluated. Decision analysis is a systematic approach to decision-making under conditions of uncertainty. Because the technique can be so useful in sorting out complex questions associated with the treatment and control of disease in individual animals and in herds, it is almost certain to become more commonly used by large-animal practitioners.
Decision analysis involves identifying all available choices and the potential outcomes of each, and structuring a model of the decision, usually in the form of a decision tree. Such a tree consists figuratively of nodes, which describe choices and chances, and outcomes. The tree is used to represent the strategies available to the veterinarian and to calculate the likelihood that each outcome will occur if a particular strategy is employed. A probability value must be assigned to each possible outcome, and the sum of the probabilities assigned to the branches must equal 1.0. Objective estimates of these probabilities may be available from research studies or from a veterinarian’s own personal records or it may be necessary to use subjective estimates. The monetary value associated with each possible outcome is then assigned, followed by calculation of the expected value at each node in the tree. At each decision node the value of the branch with the best expected value is chosen and that becomes the expected value for that node. The expected value establishes a basis for the decision. An example of a decision tree without probability values assigned is shown in Figure 1.24
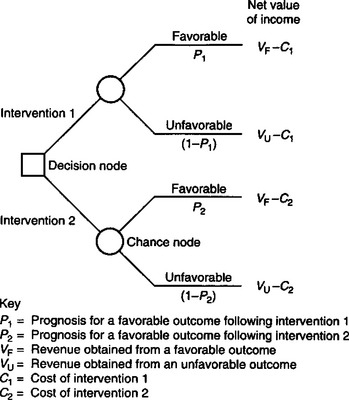
Fig. 1.2 A decision tree for choosing between two interventions.
(With permission from Fetrow J et al. J Am Vet Med Assoc 1985; 186:792–797.)
In the decision tree, choices such as the decision to use intervention no. 1 or intervention no. 2 are represented by squares, called decision nodes. Chance events, such as favorable or unfavorable outcomes, are represented by circles called chance nodes. When several decisions are made in sequence, the decision nodes must be placed from left to right in the same order in which the decisions would have to be made, based on information available at that time. The tree may become very complicated, but the basic units of choice and chance events represented by squares and circles remain the same. Lines, or branches, follow each node and lead to the next event. The branches following each decision node must be exhaustive; for example, they must include all possible outcomes, and the outcomes must be mutually exclusive.3 After each chance node there is a probability that an event occurs. The probabilities following a chance node must add up to 1.0. The probabilities are placed on the tree following the chance node. The expected outcomes (VF and VU in Fig. 1.2) are entered at the far right of the tree. The outcomes represent the value that would result if the events preceding them on the tree were to take place, and must include the costs of the intervention.
When a complete tree accurately representing the problem has been constructed, the next step is to solve it for the best decision to follow. This is done by starting at the right of the tree, where outcome values are multiplied by the probabilities of outcome at the preceding chance node. The figures derived from this procedure are added together to obtain the equivalent of a weighted average value at the chance node, known as the expected value, which by convention is circled with an oval. This procedure is repeated from right to left on the tree at each chance node. When a decision node is reached when moving from right to left, the most profitable path is chosen and a double bar is drawn across the branches leading to the lesser cost-effective decisions. When the first decision node at the left of the tree is reached, a single path will remain that leads from left to right and has not been blocked by double bars. This path represents the best way to handle the problem according to the available information, including the outcome at the end of that path.
An example of the construction and use of a decision tree to assist in deciding at what day postpartum an ovarian cyst should be treated, as opposed to waiting for spontaneous recovery, is illustrated in Figure 1.3.4 In structuring the problem, over time, the clinician knows that the cyst can be treated or left to be treated later. Retreatment is possible if the first treatment is ineffective. The structure must include all alternatives. The other information needed to solve the problem includes:
• The incidence or chances of spontaneous recovery
• The response to treatment, both initially and following repeated treatments
• The cost of treatment and the cost of the disease.4
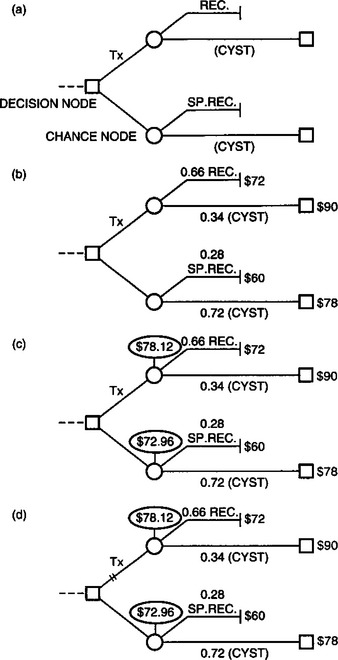
Fig. 1.3 Example of the construction and use of a decision tree. The sources of probabilities and dollar values are discussed in the text. (a) The skeleton of the decision tree with a decision (treat Tx versus do not treat) and chance outcomes (recovery (REC) or spontaneous recovery (SPREC) versus continued cyst (CYST)). (b) Probabilities and previously calculated outcome values are placed on the tree. (c) Expected costs of decision alternatives have been calculated and written in balloons above the chance nodes. (d) At this decision node, the correct choice is no treatment because it is cheaper ($72.96 v $78.12). Double bars mark the pathway that is not chosen (treatment). The value $72.96 is then the outcome cost for this decision node. The value is used in the calculation of the best alternative to the previous decision node, as the process is repeated from right to left (not shown).
(With permission from White ME, Erb HN. Comp Cont Educ Pract Vet 1982; 4:S426–S430.)
The critical factor in each tree is the probability value for each possible outcome. The monetary value of each outcome can be estimated on a daily basis but, unless the probability of the outcome can be assessed as accurately as possible, the decision analysis will be unreliable. Decision analysis has been used to determine the cost-effectiveness of heat mount detectors, the time at which to treat bovine ovarian cysts, the effectiveness of three alternative approaches to the control of Haemophilus meningoencephalitis in feedlot cattle, the economically optimal control strategy among several alternatives for the control of infection with Brucella ovis in a sheep flock5 and the relative merits of testing or not testing calves entering a feedlot with a metabolic and cellular profile test as predictors of performance in the feedlot. Decision analysis can now be done on microcomputers which makes the process highly suitable for assisting the veterinarian in daily decision-making.
The details of the steps used in decision analysis of several different problems in food-animal practice have been described and the reader is referred to the publications for further information.4 There are some limitations to using decision analysis in animal health programs:6 the technique requires time and effort, which practitioners are reluctant to provide unless the benefits are obvious. The estimates of the probabilities associated with the respective branches of the tree are seldom readily available.
A number of techniques that can be used to derive these probabilities and incorporate them in decision-making have been recorded. The rapidly developing use of analytical veterinary clinical epidemiology can now provide the tools to generate the numerical data necessary to make reliable decisions. There is a need to apply epidemiological principles to prospective clinical studies to determine the most effective therapy or the efficacy of control procedures for the commonly occurring economically important diseases of food-producing animals. The inputs and outputs of a given strategy may not have a market value, or the market value may not be an appropriate measure, or they may not be tangible or measurable in the usual monetary units. For example, the market value of a dairy cow may not represent the true or real value of the cow to the farmer. The farmer may consider the value of the cow in relation to cattle replacement determinants such as herd size, the availability of replacements and the genetic potential of the animal. The final selection of one option or the other is usually a complex process that will also vary from individual to individual depending on the decision criterion used.
In summary, decision analysis provides a systematic framework for making rational decisions about major questions in animal health and it is hoped that some veterinarians will adopt the technique for field use.
Sackett DL, et al. Clinical epidemiology. In: A basic science for clinical medicine. Boston: Little, Brown & Co.; 1991:3-170.
Wilson J. Physical examination. Vet Clin North Am Food Anim Pract. 1992;8:1-433.
Farver TB. Concepts of normality in clinical biochemistry. In: Kaneko JJ, Harvey JW, Bruss M, editors. Clinical biochemistry of domestic animals. 5th ed. San Diego, CA: Academic Press; 1997:1-19.
1 Sackett DL, et al. Clinical epidemiology. In A basic science for clinical medicine. Toronto: Little, Brown & Co.; 1985.
2 White ME. J Am Vet Med Assoc. 1985;187:475.
3 Fetrow J, et al. J Am Vet Med Assoc. 1985;186:792.
4 White ME, Erb HN. Compend Contin Educ Pract Vet. 1982;4:S426.
Examination of the herd
The examination of the herd assumes importance where there are outbreaks of disease or problems of herd productivity due to subclinical disease. The purpose of a herd examination is to define the exact nature of the problem and to identify those dysfunctions within the herd environment that are associated with its occurrence. The ultimate objective in the examination of a herd is to establish strategies for the treatment, correction and control of the disease problem at the herd level. This may involve strategies to increase the resistance of the animals or strategies that change adverse factors in the herd environment.
There are a number of ways in which these objectives can be achieved and they are not mutually exclusive. The methods for examination of the herd include:
• Initial definition of the problem to be examined
• Clinical examination of individual animals in the herd
• Analysis of records of performance and disease
• Examinations of the environment of the herd
• Laboratory examination of animal; nutritional and environmental sampling
Methods for correction of the problem include:
• Treatment of individual sick animals
• Selective or strategic prophylactic medication of the impacted group
• Alterations to the nutrition, the environment or the management of the herd or of selected groups within it.
One, or several, of these methodologies may be used in dealing with herd problems depending upon the nature of the disease under consideration.
Herd examinations can be expensive and in clinical settings the depth of investigation must be justified by the degree of economic importance of the problem. Some diseases are well defined, they are easily and definitively recognized by clinical or postmortem examination, their determinants are well established, and there are established effective methods for their control. In these instances a herd examination in a clinical setting would be limited to the initial examinations that establish the diagnosis and to the implementation of corrective strategies.
Other diseases are less well defined. There may be several determinants of their occurrence and consequently all facets of the examination methods may be needed to determine the most appropriate method for control. It is for this type of disease that epidemiological investigations are of particular importance and, where there is an economic justification, an in-depth epidemiological investigation should be considered in order to determine the appropriate method of intervention.
APPROACH TO HERD EXAMINATION
The previous sections have discussed the approach to clinical examination of the individual animal and the methods for determining the presence of system dysfunction and of reaching a diagnosis as to cause. Basically, these consist of a physical examination to assess the function of each body system coupled with laboratory or other ancillary diagnostic methods and information that can assist in this assessment and in the establishment of cause. In the individual animal, disease is usually diagnosed and classified by the system involved and the inciting agent as, for example, pneumonia associated with Histophilus somni, myopathy caused by a deficiency of selenium. Subsequent treatment is based on this knowledge and usually consists of therapy directed against the cause and therapy aimed at correcting the system dysfunction.
The approach to the examination of the herd has a similar logical and systematic approach but it is obviously expanded beyond the examination of individual animals and involves different systems. It also involves different approaches to the cause of disease. Herd examinations are conducted because there is an outbreak of disease or a problem of production inefficiency. By definition this involves a group or a population of animals. Most outbreaks of disease and problems of production inefficiency in groups of animals result from faults or dysfunctions in the complex of interactions that occur within groups of animals and between the groups of animals and their management, environment and nutrition. The characteristics of the group of animals that are affected thus become a focus of the examination and the management, environment and nutrition are the broad systems that are examined in relation to this group of animals. In the examination of the herd one is asking the following questions:
• What is the disease problem that is present?
• What are the characteristics of the animals that are involved?
• Why has this group of animals developed the disease?
• Why are they at increased risk in relation to others within the herd?
• What are the factors in their management, nutrition or other environment that have led to this increased risk?
• What intervention strategies can be used to correct the problem?
A major objective of the examination is to establish a diagnosis of cause. In particular, the objective is to establish a diagnosis of cause that can be altered by an intervention. The diagnosis of cause in a herd disease problem is often different from the diagnosis of cause established in the examination of an individual. Disease occurrence in groups of animals is often multifactorial in cause and the result of the interaction of several risk factors, which may be characteristics of the animals, their environment or of an inciting agent. In the context of the herd the cause or ‘etiology’ of a disease can be a management fault. In making a diagnosis of cause, the clinician establishes and ranks the major determinants of the problem from among the various risk factors.
Examples of multifactorial etiology of a disease
The examination of an individual animal that is representative of a group of young calves with respiratory disease may lead to a diagnosis of pneumonia associated with Histophilus somni. The diagnosis of the cause of the same problem following a herd examination that evaluates the numerous risk factors for pneumonia in calves might be:
In making a diagnosis of cause, the clinician establishes and ranks the major determinants of the problem from among the various risk factors.
With many diseases one progresses to an examination of cause in the herd using knowledge of recognized risk factors for the disease. These risk factors usually have a logical relation to the disease being examined, as with the example of calf pneumonia. With other diseases the logic of these relationships may be less apparent. This occurs particularly with newly developing or recently recognized diseases, where the pathogenesis of the disease is poorly understood but epidemiological examinations have established certain relationships that have a causal association. The definition of circumstances of occurrence for a disease can lead to a method of control even though the cause of the disease, in the traditional sense, is not known and the relationship between the inciting or associated circumstance and the disease is obscure. A current example would be the developing recognition of an association between dry cow nutrition in dairy cattle and metabolic and infectious diseases that occur early in lactation.
Example of the control of a disease without knowledge of its etiological cause
It is now known that facial eczema in sheep is a toxicosis from fungal toxins produced on pastures. However, long before the toxic nature of this disease was fully understood, the epidemiological circumstances of its occurrence were defined and it was prevented by removing sheep from pastures that had risk for the disease during predicted risk periods factors.
Problems of disease and production inefficiency encountered in herds can present a considerable challenge in diagnosis and correction. In part this is because disease in groups or herds is commonly multifactorial in cause and, for this reason, in an examination of the herd, all the factors that influence the behavior of a disease in that herd assume importance. The obvious approach is a quantitative definition of the disease and a quantitative examination of the relative importance of these risk factors. However, this approach can be difficult in practice.
In clinical settings there is usually no difficulty in achieving a quantitative definition of the animals affected and their characteristics. In large, well-recorded herds it is usually possible to conduct a quantitative examination of risk factors if the records contain information that relates to them. In small herds, a quantitative examination of the relative importance of risk factors may be limited by low numbers of animals. Knowledge of risk factors and their relative importance in disease causation is improving with epidemiological research studies that involve large numbers of animals and several herds. The role of the clinician in the approach to a herd disease problem is to know and to be able to detect these established influences, to be able to quantify them where possible, and to be able to choose from among them those that are most subject to correction by intervention from both a practical and an economic standpoint.
EXAMINATION STEPS
There is no single protocol that can be used for the examination of the herd as this will depend both upon the type of disease problem and the type of herd. For example the methods of examination that would be used in the examination and definition of a problem of ill-thrift in a flock of weaned lambs would be different from those used for a problem of lameness in dairy cattle. Most herd investigations will follow certain broad principles and steps, and these are outlined in Figure 1.4. A given herd examination would not necessarily follow all the steps in this illustration nor would it necessarily proceed in the exact order given. However, the general principles apply to most investigations.
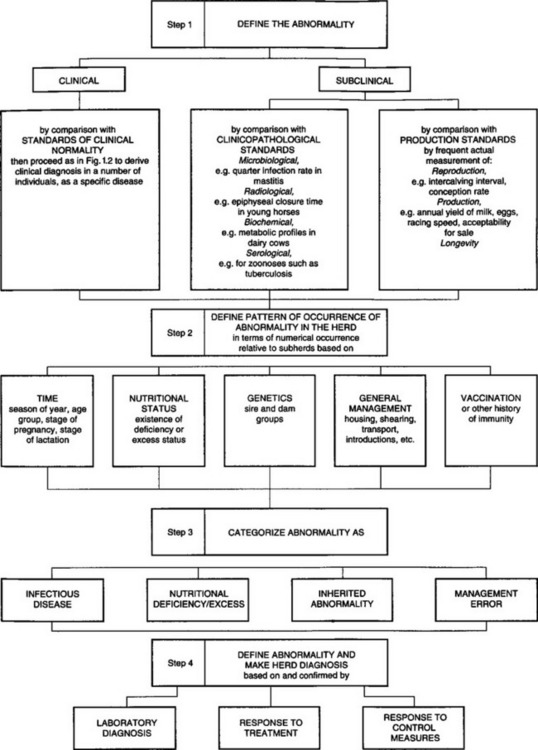
Step 1: Defining the abnormality
It is essential first to define the abnormality in either clinical or subclinical terms. This definition must be accurate, as this step of the examination determines the focus of the examination and the types of cases that will be included in the examination and analytical procedures. A case is defined as an animal or a group of animals that have the characteristics of the disease or a defined deviation from targets of production. With some investigations the problem will have obvious clinical manifestations and the primary definition of cases will be made by clinical examination of affected individuals. With others the primary complaint may be lowered production in the absence of clinical disease. An apparent problem in production efficiency can be focused by the examination of records. In many herds this will prove to be an immediate major limitation to the investigation because of a lack of sufficient records on reproduction, production and associated management to define the complaint. In these circumstances the criteria of the production inefficiency that will be considered in the examination will need to be determined and some form of measurement established.
Step 2: Defining the pattern of occurrence and risk factors
This step of the examination is often conducted in conjunction with step 1 above. It has the purpose of defining the characteristics of the animals that are affected in the disease problem and that have been established as cases, and of determining differences between them, as individuals or as a group, and the nonaffected animals within the herd. These differences may be attributes of the animals themselves or of environmental influences that affect them.
The initial examination is usually directed towards the determination of the characteristics of the animals involved and the temporal (when) and spatial (where) patterns of the disease. In general, the information that allows these examinations is collected at the same time and consists of such factors as:
• A listing of the cases that have occurred
• The date when disease was first observed in each case
• The age, breed and other individual information for each case, which may include such information as source, family association, vaccination history, previous medication
• Management group membership, which may be pen membership, milking string, pastoral group, etc.
• Type of ration and nutritional data
• Management and other environmental information that is relevant to the problem.
In order to compute risk group analysis the number of animals present in both sick and well groupings must be recorded, as must be any similarities and differences in their management and environment. After the identity of the abnormality has been established, all the available clinical, production and laboratory data are examined according to the affected subgroups in the herd and according to time occurrence, management differences, nutritional and environmental influences and factors such as vaccination history.
In most herd examinations the analysis of these data is restricted to a cross-sectional study. Prevalence rates within the various groups are calculated and the population at risk can be determined. Animals or groups can be examined as those with and without disease and those with and without hypothesized risk factors, using a 2 × 2 contingency table generated for each variable. Relative risk, odds ratios or rate ratios can be calculated as a measure of association of the variable with chi-square and Mantel–Haenszel procedures used for evaluation of the significance of the risk. This attempts to determine if any associations exist between certain groups of animals and those factors that can influence the behavior of disease.
In some herds, where there has been extensive historical recording, it may be possible to examine the nature of the problem on the basis of a case-control study. However, in most herds this will not be possible because of the paucity of recording of factors of importance to the definition of the disease problem. With problems that are of obvious continuing importance to the economic viability of the herd it may be necessary to establish recording systems that allow a prospective examination of the problem.
Temporal pattern
The temporal pattern of distribution of a disease in a population can be of importance in suggesting the type of disease that is occurring and its possible causes. Temporal recording and graphing of cases is of value in indicating possible portals of entry of an infectious agent or sources of a toxic influence. For this analysis the temporal occurrence of the disease is determined by the collection and graphing of the time of onset of clinical cases (hours, days, weeks) and by relating this information to management or environmental changes.
Generally two types of epidemic curve are graphed. A point source epidemic curve is characterized by a rapid increase in the number of cases over a short period of time. This type of epidemic curve occurs when all the animals in a population are exposed at the one time to a common agent. Generally this will be a poison or a highly infectious agent, with many animals becoming affected at approximately the same time and, depending on the variation in the incubation period, a sharply rising or a bell-shaped curve of short time duration. The graphing of a sporadic outbreak suggests the occasional introduction of a disease agent into a susceptible population or the sporadic occurrence of factors suitable to the clinical manifestation of an endemic agent, as opposed to the relatively continual occurrence of an endemic disease.
When the infection has to be transferred from animal to animal after undergoing multiplication in each, delay results and the epidemic curve develops a flatter bell-shaped occurrence of much longer duration and with varying peaks depending upon temporal differences in, and opportunities for, transmission. This is known as a propagative epidemic. Whereas the occurrence and identification of an index case has considerable value in epidemiological examinations of this nature, it commonly cannot be identified in veterinary clinical settings.
Spatial examination
The spatial examination of a disease problem requires the gathering of information on affected and nonaffected animals in relation to areas of the housing environment, or pastures, or animal movements. A cluster of cases associated with a specific area may indicate the source of the problem. This is best analyzed by plotting the frequency of cases on maps of the environment that include possible risk factors such as pen locations within buildings, buildings themselves, water sources, pastures, rubbish dumps, roads, implement storage areas, etc. When spatial associations are established, further detailed examination of the location is indicated.
Step 3: Defining the etiological group
Following characterization of the abnormality according to groups within the herd, and having made comparisons of the prevalence rates between groups, it may be possible to discern to which etiological category the abnormality most logically belongs. In many instances considerable difficulty may be encountered in deciding in which of the general areas of etiology the major determinant is located. In so many cases herd problems are not the result of a single error but are multifactorial, with several determinants contributing to a greater or lesser degree, and the problem may fall in several categories.
An example might be a problem of mortality in calves where examinations have determined that population mortality rates are highest in the winter period, that most mortality occurs between 4 days and 1 month of age, that calves that die early in this period have septicemia, or have scours associated with rotavirus and cryptosporidial infections, that the body condition scores of the calves fall during the third and fourth weeks of life and that calves that die later in the time period appear to die of starvation. Probable causes include improper feeding of colostrum, a poor environment leading to a high infection pressure and possibly also to excess cold exposure, malnutrition resulting either from the residual effects of enteric disease on intestinal absorption of nutrients or from an inadequate caloric intake or both. This complex could be placed in the categories of infectious disease, nutritional disease and also in the category of management error; further definition is the next step.
The use of path models that summarize current knowledge of the causality of the disease under consideration can help in this aspect of the herd examination. Path models specific to the problem at hand can be constructed and can show the interrelationships between various risk factors and give some indication of the dependence of any one factor on the occurrence of another. This information can be used to estimate the relative contributions of the various etiological categories and to give guidance as to the area where intervention is most likely to be effective.
Step 4: Defining the specific etiology
The final step is to select the probable most important determinant or combination of determinants from within one or more of the general areas and to make corrective interventions based on this diagnosis. In many instances the primary cause may be clear and the correction, be it alterations in nutrition, alterations in management, vaccination, etc., can be made at this stage. In other cases further prospective examinations may be conducted for a better definition before an intervention is attempted. In the example above, failure of passive transfer of colostral immunoglobulins and inadequate caloric intake would have been suspect or even identified as underlying determinants of the problem. However, with most farm recording systems there is likely to be no available data that would help delineate the specific reasons, and the specific management deficiencies that require correction, and so a prospective study to establish these would need to be established.
It can be very difficult to obtain a clearly defined diagnosis of cause of disease in a herd, because of its complexity, but the known important relationships are given for the individual diseases in the special medicine section. Methods for practical clinical quantitative assessment of the level of management expertise or, more importantly, the intensity with which it is applied, are not available. Consequently this must be assessed qualitatively for most management practices. Surrogates such as the percentage of cows presented for pregnancy diagnosis but not pregnant, bulk tank somatic count, rates of failure of passive transfer of colostral immunoglobulins, etc., can give some indication.
TECHNIQUES IN EXAMINATION OF THE HERD OR FLOCK
Set out below are some of the techniques used in examining a group or herd of animals. Any one or combination of the techniques may be used at the one time, depending on the nature of the problem, the availability of support facilities such as diagnostic laboratories and data analysis laboratories, and their cost.
CLINICAL EXAMINATION
A clinical examination is essential if clinical illness is a feature of the disease; a representative sample of animals should be examined. The importance of this component of the examination cannot be overemphasized. Where there is clinical disease an accurate definition by clinical examination may lead to a diagnosis of a disease with known and specific determinants and further examination of the herd can focus specifically on these factors. Where clinical examination does not lead to a finite definition of the cause of the disease but gives a diagnosis of a disease of multifactorial determinants, the examination will still lead to the identification of risk factors that need to be included in the herd examination.
Recording the findings is important and is greatly assisted by a structured report form so that the same clinical features are recorded for each animal. Commonly, clinically affected animals are enrolled as cases in an investigation on the basis of the presence of certain defined signs or clinical abnormalities and a recording form aids in this selection. This is especially important where several veterinarians in a practice may be involved in the herd examination over time.
Selection of the animals to be examined is vital. This should not be left to the farmer because that selection may be biased to include the sickest, the thinnest and the oldest, and not necessarily the animals that are representative of the disease under examination. This is particularly important if a group of animals is to be brought from the farm to a central site for detailed clinical examination as part of the workup of the problem. Strict instructions should be given to the owner to select 10–12 animals as a minimum. The groups should include eight sick animals, if possible four advanced and four early cases, and four normal animals as controls. If the situation permits it, the inclusion of animals that can be sacrificed for necropsy examination is an advantage. Ideally, unless facilities will not allow it, the clinical examinations should be on the farm and the veterinarian should select the animals for examination.
In outbreaks of disease where there is mortality, necropsy examination and associated sampling is an extremely valuable investigative and diagnostic tool. Necropsy examination should not be ignored as the primary method of establishing a diagnosis of problems of disease or production inefficiency in larger herds and flocks. With many diseases in swine herds and larger sheep flocks the costs associated with the sacrifice of a few animals for this purpose are by far outweighed by the benefits of an early and accurate diagnosis and the ability to intervene quickly with corrective strategies. Even in cattle herds, owners are willing to sacrifice affected cattle if by so doing they can facilitate a more accurate definition of their problem. It must also be recognized that some diseases cannot be accurately defined on the basis of their clinical manifestation and epidemiology and a necropsy is required as part of the examination system.
SAMPLING AND LABORATORY TESTING
Laboratory examination is conducted for a number of legitimate reasons. It may be conducted to aid in the establishment of a diagnosis or it may be conducted following the establishment of a diagnosis to aid in the definition of risk factors or in the evaluation or the efficacy of treatment and control strategies.
The validity of laboratory testing in the investigation of disease is only as good as the quality and relevance of the samples that are submitted. The samples submitted must be appropriate to the question that is being asked of them. Frequently samples that can be most conveniently obtained are not the best for this purpose and a sampling strategy specifically directed to the question may need to be established.
Laboratory analysis of samples is expensive and should not be undertaken unless there is a specific objective. Before submitting samples for examination the following questions should be asked:
• Is the sampling strategy structured to answer specific questions or is it a random ‘fishing expedition’?
• Have you established a sampling strategy that will allow a comparison of animals in your ‘at risk’ category with those believed not at risk for the disease or the exposure factor?
• Is there a ‘gold standard’ for the analysis and its interpretation?
• What information will be gained from the results of the laboratory examination that could not be gained by other examinations or logically inferred without these examinations?
• What are the specific steps to be taken that depend upon the results of these examinations, or will the steps be taken regardless of the results?
This type of questioning of sampling for laboratory examination may limit it to situations where it is cost-effective.
Laboratory examination of samples taken in association with clinical examination is usually conducted to help establish the presence and severity of organ dysfunction – which generally cannot establish cause. The value and use of laboratory examinations in the assessment of organ function is discussed in the sections in this text that deal with system diseases. Similarly the nature and value of sampling to establish the etiological association of toxic or infectious agents with disease is discussed under specific disease headings.
Laboratory testing can also be conducted to determine risk and exposure factors. When used for this purpose the sampling strategy must be directed and should be conducted after the preliminary diagnosis has been made. It must be aimed at answering the specific questions above, otherwise it will be inordinately expensive. An example would be the examination of specific feeds that have been implicated as potential sources for a toxin following the epidemiological examination and risk factor analysis in a herd where a specific toxicity was established as the cause of mortality. Without this prior epidemiological examination a mass sampling of the herd and its environment for the presence of the toxin would be extremely expensive and of limited value.
At the time of the initial farm visit, it is advisable to collect samples that are pertinent to the problem and its differential diagnosis but are not of primary analytical significance in the initial definition of the problem. These can be stored and, depending upon the results of initial laboratory examinations, may be discarded or used to further define the problem. Duplicates of some samples with storage is often desirable so that second thoughts on tests can be accommodated. This is particularly important in serological work where the hindsight may be at a long time interval and a serum bank is most profitable when one is attempting a retrospective examination of prevalence.
In many outbreaks it is usually wise to collect samples from ‘controls’ that are established specifically to evaluate the problem under investigation. These may be clinically normal animals that have not experienced the suspect exposure factor, animals that are clinically normal but that have been exposed and are possibly in an incubation or subclinical stage, and from a third group of clinically affected animals. This system approximates the protocol for the Compton Metabolic Profile, which is described in detail in Chapter 28.
The other consideration is the number of animals to be included in each sampling group. The sample size required for the detection of an attribute varies with the confidence of detection that is desired, with the size of the population and the prevalence or frequency of the attribute in that population. Obviously there can be no set recommendation even for one disease. For example, the sample size required to confirm a diagnosis of copper deficiency in a group of animals with overt clinical deficiency disease will be much smaller than that which is required to establish a developing deficiency state or the risk for clinical disease in the face of deficient intakes on pasture. Unfortunately, cost severely limits the size of the sample that can be tested in most circumstances and the small size that is common can place severe restrictions on any meaningful interpretation. The commonly recommended 10 animals or 10% of the group would appear to have little validity in most examinations.
Numerical assessment of performance
Productivity indexes can be used as indicators of health; they can also be used to measure response to treatment or control measures. More and more they are being used as guides to husbandry and management questions to meet the present-day farmer’s concerns with costs and returns. If recording systems are present on the farm they can be invaluable data sources in the investigation of herd problems with disease. Monitors of production efficiency are used extensively in performance or production management veterinary practice and are detailed in texts on that subject in the reference literature section.
Intervention strategies and response trials
As the result of a herd examination, a clinician formulates a hypothesis concerning the disease. This may include hypotheses on the population of animals at risk, the determinants of the disease, the source of the problem and its methods of transmission or propagation. There may be sufficient confidence in these hypotheses that they may result in intervention strategies to correct the problem without further analysis. In other outbreaks the hypotheses may be less secure and may require further examination of response trials.
Response trials are often used in an approach to herd disease problems and problems of production inefficiency. They have several purposes: they may be used to establish or confirm a diagnosis, and when used for this purpose it is usually because of the difficulty in confirming the diagnosis by other methods. This may result from the lack of a suitable laboratory test or because the result of the test is supportive for the diagnosis but not confirmatory. Response trials can also be used to determine the degree of intervention that is required and the efficacy of the level of intervention that has been used.
Example of reason for response trials
The finding of hypocupremia in a group of poorly growing calves would support a diagnosis of growth retardation due to copper deficiency but does not confirm it, as calves with normal growth can also be hypocupremic. The only way to confirm the association and the diagnosis is to conduct a response trial with copper treatment as the variable.
An example of monitoring efficacy of interventions
Response trials can be used to determine the degree of intervention that is required and the efficacy of the level of intervention that has been used. Copper deficiency in grazing calves may occur as a simple deficiency or as a conditioned deficiency. Simple copper deficiency can usually be prevented by a single subcutaneous treatment of copper glycinate and this may protect for several months. On the other hand, a conditioned copper deficiency may require treatment every 4–6 weeks.
Some prediction as to the required treatment frequency can be made by pasture element analysis but a response trial with 6-week-interval monitoring of blood copper concentrations and weight gain can monitor the efficacy of the treatment that has been decided upon and also allow a corrective intervention, if indicated. In the absence of a treatment response trial, a nonresponse due to an incorrect decision on treatment frequency could result in the discarding of the correct diagnosis.
There are many limitations to conducting response trials in clinical situations in private herds and their structure may not always meet the strict requirements of those conducted in research. It is not always possible to establish a controlled response trial in clinical practice but the efficacy of intervention strategies should still be monitored. The ultimate interest is in whether the disease or production problem is corrected; however, the efficacy of the individual strategies should be specifically monitored where possible. In the earlier example of calf mortality a decision might have been made to change the method of feeding colostrum and to improve the caloric intake of the calves. There can be various ways that either of these changes could be achieved. The overall efficacy of these changes will be determined by improved survival of the calves. However, the efficacy of the colostrum management change in improving passive transfer should be determined specifically by measurements of serum immunoglobulin concentrations in the serum of a proportion of calves and the efficacy of caloric improvement by weight measurements. Should calf mortality drop, these latter measures are of limited value but if it does not, then there are measures of whether the failure was due to misdiagnosis of the problem or due to poor efficacy of the suggested corrective strategies in correcting their respective target areas.
A diagnosis made on the basis of a response trial is often presumptive and it has become customary to couch the diagnosis in terms of response to a treatment, for instance, ‘selenium-responsive infertility’ in sheep. This is not a diagnosis in terms of satisfying the original concepts of Koch’s postulates, although it does satisfy the subsequent modifications of these postulates that are now generally accepted and have been based on a broader interpretation of disease causation. In populations of animals, diseases are largely the result of a number of interacting factors of different genres, including management, nutrition and environmental factors, interacting with traditional agent-causes of disease, including microbiological and toxic agents. The answer for the practical problem may be most economically derived by finding the cure rather than the cause. This is especially desirable if that course is cost-effective and finding the cause is more expensive than the wastage caused by the disease.
A simple example would be mortality in a group of cattle that followed a change of feed to a more concentrated ration. An epidemiological examination, including a temporal examination of cause or determinants, might closely link the mortality to the change in ration. This should be sufficient to indicate that the ration should be withdrawn or its method of feeding modified. The alternative approach would be to defer any decision for correction of the problem until the exact problem with the ration was established. This could involve a ration analysis and an examination for unknown toxic components. These examinations would take considerable time, would involve considerable costs, and could well give no additional information that would modify the immediate initial intervention strategy.
The role of the planned animal health and production program
Properly conducted herd health programs and planned animal health and production programs maintain accurate records on all matters of production and health. These are maintained against a background of epidemiological data, including number of animals in the herd, numbers of animals in the reproductive cycle segment group or age group that are therefore at risk. In many instances all the data required to effectively diagnose a disease or monitor its prevalence are already at hand in the records of these herds. It does put the veterinarian and the farmer in the position of almost being able to do a herd examination simply by consulting the records. This approach is detailed in texts on herd health and production medicine.
Kahrs RF. Techniques for investigating outbreaks of livestock disease. J Am Vet Med Assoc. 1978;73:101-103.
Blood, DC. The clinical examination of cattle. Part 2: Examination of the herd. In: Proceedings of the 14th Annual Convention of the AABP, 1981;14–21.
Cannon AR, Roe RT. Livestock disease surveys. In A field manual for veterinarians. Canberra: Australian Government Publishing Co.; 1982.
Dohoo IR, Waltner-Toews D. Observational studies and interpretation of results. Comp Cont Educ Pract Vet. 1985;7:S605-S613.
Thrushfield MV, Aitken CGG. An introduction to veterinary observational studies. Edinburgh: University of Edinburgh Press, 1985;35.
Thrushfield MV. Veterinary epidemiology. London: Butterworths, 1986;165.
Martin SW, Meek AH, Welleberg P. Veterinary epidemiology. In: Principles and methods. Ames, IA: Iowa State University Press; 1987:343.
Lessard PR, Perry BD. Investigation of disease outbreaks and impaired productivity. Vet Clin North Am, Food Anim Pract. 1988;4:1-212.
Smith RD. Veterinary clinical epidemiology. In: A problem oriented approach. Boston, MA: Butterworth-Heinemann; 1991:234.
Radostits OM. Herd health. Food animal production medicine, 3rd ed. 2001. Philadelphia, PA: WB Saunders.