Development of Childhood Occupations
1 Explain historical and current theories of child development.
2 Define how a child’s unique characteristics influence skill development
3 Using an occupational therapy perspective, explain how occupations develop.
4 Explain how individual biological systems and cultural, social, and physical contexts contribute to a child’s occupational performance in the first 10 years of life.
5 Describe the development of play and the variables that contribute to the development of play.
An understanding of child development is foundational knowledge for pediatric occupational therapists. Researchers from many disciplines, including medicine, psychology, anthropology, education, sociology, and occupational therapy, have contributed to the literature on human development, and the different perspectives they provide should be woven into a holistic and comprehensive understanding of how children become adults.
Occupational therapists want to know what developmental changes occur in children and how children develop their unique personhood. The answers to these questions provide essential knowledge for evaluating children and for determining the appropriate materials, activities, and environments to support children’s skill development and participation in their communities. They are also interested in how human occupations develop over the life span.
This chapter focuses on child development theories, with emphasis on concepts that have emerged in the past 2 decades. The first section discusses concepts that explain how children develop and what variables and interactions influence developmental outcomes. In the second part of the chapter, a model for the development of childhood occupations is applied to children’s development of play in the first 10 years of life. Chapter 4 describes the development of pre-adolescent and adolescent occupations in the second decade of life.
DEVELOPMENTAL THEORIES AND CONCEPTS
Researchers of the 1930s and 1940s identified a sequence of skill maturation that defined the steps of normal development. Gesell and Colleagues42–44 and McGraw74 assumed that normal development was revealed through a specific skill sequence that reflected maturation of the central nervous system (CNS). These workers believed that the sequence of motor, cognitive, socioemotional, and language skill development was relatively unaffected by the infant’s experiences. The work of these neuromaturational theorists in documenting this developmental sequence has been well respected and has allowed the creation of developmental assessment tools. The sequence of normal development is an important frame of reference for identifying children with disabilities. Gesell and coworkers believed that variations in the normal sequence of development indicate CNS dysfunction. Identifying children with developmental deficits or significant delays remains an important function of physicians, nurses, occupational therapists, and others who provide early intervention services.
Neuromaturation
Neuromaturational theory has been used frequently to explain motor development.34,76 According to neuromaturational theory, brainstem structures develop first, as evidenced by the reflexive responses of the newborn (e.g., automatic grasp, asymmetric tonic neck reflex), which are controlled by neural pathways originating in the brainstem. Cortical structures appear to develop later, as evidenced by the coordinated and planned actions of the child. The infant’s increasing control of action and movement indicates not only development and myelination of the midbrain and cortical structures, but also simultaneous inhibition of brainstem control of movement. Three primary principles of neuromaturational theory are recognized:
1. Movement progresses from primitive reflex patterns to voluntary, controlled movement. In newborn and young infants, motor reflexes provide the first methods of interaction with the environment (e.g., reflexive grasp) and are essential to life (e.g., the sucking and swallowing reflexes). Because early reflexive movements serve functional needs, the newborn appears surprisingly competent. These reflex patterns subside as balance, postural reactions, and voluntary motor control emerge (i.e., when the infant learns to roll, sit, creep, stand, and walk).
2. The sequence and rate of motor development are consistent among infants and children. The developmental scales of Gesell and Amatruda,43 Illingworth,60.61 Bayley,8,9 and others are based on a typical rate and sequence of development. By assuming that the sequence of milestones (i.e., major motor accomplishments) is constant and predictable, the normative developmental sequence can be used to diagnose neurological impairment and disability.9
3. Low-level skills are prerequisites for certain high-level skills. For example, infants develop motor control in a cephalocaudal direction, with head control maturing first, followed by trunk control sufficient for independent sitting, and, finally, pelvic control sufficient for standing and walking.
In assuming a hierarchy of CNS function, the neuromaturational theory limited the thinking on how a child learns to act in the environment. Using current research models,47,52,100,102 it has become apparent that multiple variables at different levels influence the child’s skill development. The child learns occupations through interaction with his or her environment rather than through the emergence of a predetermined scenario reflecting neuromaturational principles.57
Development as an Interplay of Intrinsic and Environmental Factors
Piaget expanded our understanding of a child’s maturation by emphasizing that development occurs through the interplay between the environment and the child’s innate abilities (see Chapter 2).83 Piaget emphasized the maturation of cognitive structures that enable the child to understand the environment, language, and social action. Infants develop an understanding of the world by interacting with the environment. The impact of environment on the child’s development changes as the child becomes increasingly able to assimilate the complexities of physical and social events. Piaget also believed the development is stagelike and discontinuous. The infant is an active learner who is motivated to learn about the world. Piaget documented the child’s maturation through stages to the acquisition of symbolic thought and formal cognitive operations. The developmental stages follow a predictable sequence but vary to the extent that they reflect genetic endowment and the child’s experiences. This interplay between the child’s abilities and his experience can be appreciated in the early development of tool use. Piaget observed that children at 8 to 10 months manipulate two objects and can move an obstacle to reach an interesting or novel object. By 12 months, infants can relate an object to other objects, in addition to relating the objects to themselves. At this stage, infants use a stick to rake in an object out of reach and place objects into containers. By 18 months, infants begin to use trial and error to solve problems. At 24 months of age, they no longer exclusively need physical manipulation to solve problems and begin to demonstrate use of mental manipulation.73,83
Research studies in the 1990s demonstrated that cognitive structures develop at earlier ages than Piaget assumed; they have also demonstrated that child development has more continuity and integration across the stages of development.13,37 Infants as young as 1 month demonstrate the ability to associate learning from one sensory system with another sensory system. For example, they recognize objects with their eyes that they previously felt in their mouths.70 Researchers have also found that 9-month-old infants can remember an event 1 week after it happened.75
Other research that has updated Piaget’s demonstrated that toddlers can manipulate and use tools and can solve problems such as how to grasp and use a spoon. McCarty and colleagues found that children 9 to 14 months of age picked up the spoon using an awkward grasp and then attempted to adjust the spoon’s orientation to get the food into the mouth.73 Children 19 months old planned how to grasp and orient the spoon to get the food before acting, avoiding the use of an awkward grasp that required adjusting. This study showed that children as young as 19 months can solve problems without physical manipulation and trial and error to handle a tool accurately. By this age, the child can scoop food, fill the spoon, and correctly angle it toward the mouth,56 signifying the early emergence of tool use.
Scholars have critiqued and expanded Piaget’s original theories to fully appreciate how the environment influences development. For example, Piaget’s theories lack appreciation of the influence of culture, society, and technology on children’s development. Current occupational therapy theories consider these variables to have important roles in a child’s development.10,116 In addition, Piaget’s theories did not address the development of emotions and did not have a coherent explanation for individual differences, individuality, or variability.37 The importance of variability has been highlighted in the work of other psychologists100,103 and by occupational therapy researchers.59
The Influence of Social Interaction
Following Piaget, another developmental theorist, Vygotsky, believed that children learn through social interaction.109 Vygotsky’s theories emphasized the importance of culture and shared participation in culturally valued activities to children’s development. He demonstrated that children learn when scaffolding, or support, is provided by caregivers and teachers. Parents and other family members intuitively provide environmental challenges that encourage the infant to exhibit a higher skill level and then support the infant’s efforts to reach that level. Parents and siblings naturally promote the infant’s development by modeling actions, assisting the infant’s first attempts to perform an action, and reinforcing his or her efforts with praise and expressions of delight.
Vygotsky explains the role of social interaction in children’s development by defining a “zone of proximal development” as “the distance between the actual development level as determined by [the child’s] independent problem solving and the level of potential development as determined through [his] problem solving under adult guidance or in collaboration with more capable peers” (p. 86).109 He believed that what children can do with the assistance of others was more indicative of their mental development than what they could do independently. When presented with a just right challenge, e.g., a task that is slightly more difficult than the tasks the child has currently mastered, the child generally attempts and succeeds in this challenge, thereby learning the next step in skill development.
Vygotsky and the many subsequent developmental theorists have examined how human development transpires through a dynamic interplay involving the child and the child’s cultural, social, and physical environments. Researchers of child development have documented differences in the rate of development in socioeconomic groups, regions, and individuals. For example, rates of development appear different in rural versus urban areas.106,108 Children’s rate of development also differs among cultural groups and generations, in part because of differences in nutrition and child care practices. In human development research, the emphasis currently is on the variations expressed by individual infants and on how human systems and environmental constraints contribute to these variations.
Studies that analyze the uniqueness of individual performance often use longitudinal and qualitative approaches to analyze the performance of children over time and in natural contexts.11,102 Because these longitudinal studies document the patterns of development over time, they uncover how individual systems are constructed and assembled. Longitudinal approaches make it possible to relate transitions of subsystems to each other and to other dynamic growth parameters.108 Understanding how children acquire qualitative differences in functional performance and how they become unique individuals can begin by focusing on the variables that influence a child’s developmental course. The following sections examine current theories of development that explain the relationships among a child’s biological functions, occupations, and environments.
Dynamical Systems Theory
Dynamical systems theory refers to performance or action patterns that emerge from the interaction and cooperation of many systems, both internal and external to the child.101 In the context of child development, performance patterns emerge from the interaction of an individual’s systems and performance contexts as the child strives to achieve a functional goal.71,72 The dynamical systems theory is useful in describing how specific motor and process skills develop.
In this model, a child’s behaviors and actions are initially highly variable, with many degrees of freedom. The first actions of the infant have been described as random and uncontrolled. Development of skill proceeds by means of constraint of these degrees of freedom as the child gains control of his or her actions. Behavior, therefore, is not prescribed by a hierarchical arrangement of the CNS, but rather emerges from external and internal constraints.97 These constraints provide information to the brain and body systems that set the boundaries or limits for the child’s behavior.22
Humans are complex biological systems comprising many subsystems (e.g., motor sensory, perceptual, skeletal, and psychologic subsystems). These subsystems are in constant flux, interacting according to the task at hand and conditions in the environment. The child’s actions during the performance of a task, therefore, are the result of the subsystems’ interaction with each other and with the environment. These individual systems come together and self-organize in a coordinated way to achieve the child’s goal.97 For example, initially a child is interested in exploring the sensory characteristics of a toy. As he or she reaches for the toy, grasps it, and brings it to midline in hand-to-hand play and then finally to the mouth, the child’s attention and cognitive focus are not on planning each of these actions. Instead, they are on assimilating the toy’s actions and perceptual features.
Longitudinal studies reveal that children demonstrate unique trajectories of development and that variations in functional performance among children persist into adulthood. Thelen and her colleagues demonstrated the uniqueness of motor development in a study of reaching in 4- and 5-month-old infants.102 Each 5-month-old infant was able to reach toward an object, but the patterns demonstrated were unique. Some infants demonstrated a slow, cautious first approach to the object, whereas others made ballistic arm movements in an attempt to reach it. Although all first reaches tended to be circuitous, the amount of correction made to obtain the object, the speed at which the attempt was made, and the angle at which arms were held were different. These investigators concluded that the development of reaching did not reflect changes in a single factor, but rather to reach and grasp an object, the infant needed to (1) be motivated, (2) localize the object in space, (3) understand that the object was reachable, (4) plan the trajectory of the reach, (5) correct the movement as the hand approached the toy, (6) lift and stabilize the arm, and (7) grasp the object. How a 5-month-old infant manages all of these components to reach and grasp a toy successfully varies among infants and for different reasons.
In a similar way, between 8 and 10 months, most infants acquire the motivation to be independently mobile. The need to self-initiate movement from place to place emerges as an important task, or goal, to accomplish. This goal reflects the infant’s curiosity about the environment, a desire to explore space, and a determination to reach a specific play object. Although mobility becomes a common goal for the infant toward the end of the first year, the method used to achieve that mobility varies greatly. Some infants roll to another space in the room, whereas others scoot on their buttocks in a sitting position. Some infants push backward while lying in a prone position, and others creep forward to explore their environment. How the infant achieves mobility is influenced by many contributing body systems (e.g., strength, coordination, and sense of balance and movement). Conditions in the environment also influence infant mobility (e.g., the surfaces on which the child plays, the encouragement provided by caregivers, and the way in which the task is presented). The child’s energy level, motivation, and curiosity about the environment also influence when independent mobility is achieved. In addition to the factors that influence the maturation of mobility skills, becoming mobile influences the development of skills in other performance domains. When an infant achieves mobility, he or she becomes more independent in initiating a social interaction or in seeking help. Therefore, independent mobility contributes to the acquisition of social skills, self-determination, problem solving, and motivation to explore (see Chapter 21). A child learns perceptual skills, spatial relations, form perception, and object relations by moving through the environment.
Perceptual Action Reciprocity
Perception and action are interdependent and inextricably linked. An individual’s perception of the environment informs action, and the individual’s actions provide feedback about movement, performance, and consequences in the environment. Initially, many of the child’s actions are exploratory in nature—that is, the child moves fingers over the surfaces of objects to learn their shape, texture, and consistency. The child waves an object in the air to hear the sounds it makes and feel its weight. These actions help the child perceive sensory and perceptual features (affordances) of objects. Affordance is the fit between the child and his or her environment.46,48,49 The environment and objects in it offer the child opportunities to explore and act. This action is based on what the environment affords, as well as the child’s perceptual capability to recognize affordances in that environment. For example, colorful noise-making toys afford manipulation because they have movable parts and rounded surfaces and fit easily into an infant’s hand. Learning about affordances entails exploratory activities. Individual finger movements, thumb opposition, hand-to-hand transfer, and eye-hand coordination are facilitated by the physical characteristics of the toy.
Manipulation is guided by visual, tactile, and kinesthetic input.86,94 Exploration of objects begins with visual exploration and mouthing.87 By 6 months, infants prefer exploring with their eyes and hands.86 Fingering and manipulation skills increase substantially between 6 and 12 months, enabling infants to gather more precise information about objects. By 12 months, infants detect object properties with increasing specificity and learn to adjust their exploratory action.1 For example, to perceive the consistency of a soft, squishy object, a child squeezes it, and to perceive the texture of velvet or corduroy, he or she runs the fingers back and forth over it.
Through object manipulation, the child develops haptic perception (i.e., an understanding of objects’ shape, texture, and mass). Bushnell and Boudreau propose that specific motor skills are required to develop haptic perception.12 They note that infants learn to identify an object’s sensory qualities (e.g., texture, consistency, temperature, contour) only when they develop the motor skills to explore each different sensory quality. For example, an infant does not accurately discriminate texture until he or she can explore texture by moving the fingers back and forth (at about 6 months). The child also cannot discriminate hardness until 6 months, when he or she can tighten and lessen the grip while holding an object.12 Because configural shape requires that two hands be involved in exploring an object’s surfaces, children typically cannot accurately perceive shape until 12 months. By 2½ years, children can identify common objects through their haptic sense, and by 5 years, children recognize common objects using active touch (without vision).16 By 5 years, the child has also fully developed in-hand manipulation skills,82 suggesting that haptic perception develops in association with the child’s development of manipulation skills. Maturation of haptic perception and manipulation underlies the child’s ability to use tools for written communication (e.g., handwriting and keyboarding) and activities of daily living.
Functional Performance: Flexible Synergies
As mentioned, the infant begins life with few constraints on performance, which permits the greatest variability in the system for the generation of spontaneous movements. This variability permits flexibility for exploration of the environment and rapid perceptual and cognitive learning. The infant quickly selects functional synergistic movement patterns. For example, from birth the infant demonstrates a pattern of hand-to-mouth movement (e.g., for self-calming by sucking on a fist) (Figure 3-1). Only minimal adaptive changes are made in this synergistic pattern (shoulder rotation and horizontal adduction, elbow flexion and forearm pronation, followed by supination and neutral wrist position) as the child learns to self-feed with various utensils (Figure 3-2).

FIGURE 3-1 Hand-to-mouth movement is observed throughout the first year, first for sensory exploration of the mouth and hand and then as a feeding behavior. From Henderson, A., & Pehoski, C. [2006]. Hand function in the child: Foundations for remediation [2nd ed.]. St. Louis: Mosby.

FIGURE 3-2 By 7 to 8 months, an infant finger-feeds, prehending small food pieces and bringing hand to mouth.
Because synergies that enable tool use are softly assembled around the goal of the task at hand, they are stable but flexible units. Synergies have specific consistent characteristics, such as the sequence of movements and the ratio of joint movement, which can be adjusted to accommodate each new situation. This adaptable stability is a hallmark of normal movement.21 Soft assembly is critical to allow the child to act in changing and variable environments. It also allows the child to explore and select a response to the environment, because his or her response patterns are variable and flexible.97
The functional synergies that characterize a child’s development of occupations are highly adaptable and reliable. The child self-organizes these synergies around tasks and goals, and his or her first goals are embedded in and organized around play (as described later in this chapter).
How Do Children Develop New Performance Skills?
How does a child learn new performance skills? Although learning new skills is not limitless and is constrained by biologic and contextual factors, human development is believed to have relative plasticity.66 This concept has obvious importance to occupational therapists, who provide intervention services designed to change and promote children’s performance. Gottlieb defines plasticity as a fusion of the organism (the child) and the environment (including its cultural, physical, and socioeconomic characteristics).52 Individual development involves the emergence of new structural (e.g., cellular) and functional components (e.g., body systems). The child’s experiences produce new neurologic connections (i.e., new associations) and structural changes (e.g., physical growth), and it is the relationships among components, not the components themselves, that are most important to development. Acknowledgment of the system’s plasticity places the focus on the child’s potential for change and on the contextual features that promote or limit the child’s performance.
How does competence develop during childhood? Children generally pass through three stages of learning to acquire a new skill.48,84,103 The first stage involves exploratory activity. The first year of life is primarily a period of sensorimotor exploration. Exploration occurs naturally in all human beings, generally when an individual is presented with a new object or task. Through exploration, a child learns about self and the environment. In this stage, the child experiments with objects and activities using different systems, new combinations of perception and movement, and new sequences of action. In this exploratory stage or when challenged by a new and difficult task, a child tends to demonstrate primitive movement. New challenges tend to elicit lower levels of skills, because these can be accessed more easily than the child’s highest-level skills, which demand more energy and effort.53 By using lower-level skills to address new problems, the child can focus on perceptual learning about the task before beginning to use higher-level skills, which ultimately allow more success in performing the task. Gilfoyle, Grady, and Moore noted that when children are first challenged with a new and difficult performance task (e.g., a first step), they use primitive movement patterns (e.g., balance by stiffening the legs and trunk) before progressing to integrated skill.50
In the second stage of learning, perceptual learning, the child begins to use the feedback and reinforcement received from his or her exploration. In this transitional stage, the child exhibits more consistency in the movement patterns used to accomplish tasks. Because this second stage is a phase of perceptual learning, certain actions that were tried initially are discarded as ineffective. Interest in the activity remains high as perceptual learning continues and is inherently motivating and meaningful to the child. In this stage, the child appears focused on learning and attempts activities multiple times. The child may fluctuate between higher and lower levels of skill. Connolly and Dalgleish found considerable variability when toddlers attempted to use a spoon.26 Greer and Lockman found similar variability when 3-year-olds attempted to use a writing tool.55 At times, the children grasped the tool using an adult gripping pattern, and at other times, they used a primitive, full-hand grasp. Mature patterns are selected more often as children enter the third stage of skill learning.
In the third stage of learning, skill achievement, the child selects the action pattern that works best for achieving a goal. The pattern selected is comfortable and efficient for the child. Selection of a single pattern indicates both perceptual learning and increased self-organization. During this end stage of learning, the child demonstrates flexible consistency in performance. He or she uses the same pattern and approach to the task but easily adapts the pattern according to task requirements. High adaptability is always characteristic of a well-learned task. Another attribute of learned performance is the use of action patterns that are orderly and economical. Children continue to practice performance when given opportunities in the environment. The third stage of learning leads to exploration of new and different activities; therefore, a child’s learning continues into new performance arenas, expanding his or her occupations.
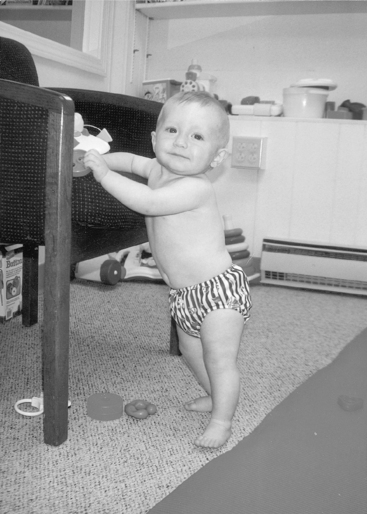
For most children, new experiences and new learning are sought and are a source of pleasure. Learning occurs when children seek opportunities for skill development; it also occurs when children adapt to the natural environment and daily activities in which they participate. Ayres explains that children make adaptive responses to the environment.3,4 An adaptive response is one in which the child responds to an environmental change in “a creative or useful way” (p. 14).4 These adaptive responses allow skill mastery and help to organize the child’s CNS. Therefore, an adaptive response helps to integrate the child’s sensory and perceptual systems to respond more skillfully to new challenges to the sensory system. For example, once the infants can pull themselves up to a standing position using a piece of furniture, they have acquired an adaptive skill that enables them to pull up to the mother’s lap to ask to be held or explore the objects on a coffee table. This organization of movement patterns was achieved because the vestibular, proprioceptive, and visual systems are innately organized toward achieving upright posture (Figure 3-3).
The Role of Motivation and Self-Efficacy
Children engage in the process of learning with innate motivation and apparent enjoyment. An infant’s inner drive motivates her to explore novel objects in the environment, learning their sensory characteristics, their relationships to each other, and their functions. A toddler or young child is motivated to solve problems and to attempt new skills, persevering until it is mastered. The concept of inner drive suggests that children attempt activities that will promote their development without specific teaching by adults. Occupational therapists view this innate drive as the child’s inner motivation to engage in occupations (task with meaning and purpose). Learning occurs when the match among child, task, and environment is optimal; hence, this match becomes the occupational therapist’s goal.58 When a child has a disability, motivation to learn and attempt new activities may be lower and the match among child, occupation, and environment may be less than optimal. In this case, a child may not learn independently and adult support may be needed to motivate, provide a just right challenge, support actions, and reinforce performance.
When a child’s inner drive leads to mastery of tasks, he or she develops a sense of self-efficacy.5–7 Bandura believes that children are inherently self-organizing and goal-directed; they typically have interest in new events and activities, initiate new tasks, and persevere in those tasks. When they succeed, positive self-efficacy is reinforced and they attempt other challenges. When they do not succeed, they are at risk for developing poor self-efficacy and eventually do not attempt new or challenging activities. Therefore, self-efficacy is highly linked to learning and occupational development because it influences levels of motivation, initiative, and perseverance.
Temperament and Emotional Development
The congruence, or goodness of fit, between the child and his or her social and physical context determines the quality of development, influencing which occupations are reinforced and which are hindered. Positive goodness of fit, meaning that the social and physical environment support the child’s skill development, can increase the child’s developmental trajectory. Lack of goodness of fit can create disruption of psychologic development and may put the child at risk for behavioral or academic problems.
Chess and Thomas asserted that if a child’s characteristics provide a good fit (or match) with the demands of a particular setting, adaptive outcomes result.19,20 The child’s temperament is an important determinant in how well a child matches the caregiving environment67 and is an important attribute in the child’s social interaction. According to Thomas and Chess, temperament refers to the child’s behavioral style, and it is believed to be innate and learned.104 Nine areas of temperament have been identified: (1) activity level, (2) approach or withdrawal, (3) distractibility, (4) intensity of response, (5) attention span and persistence, (6) quality of mood, (7) rhythmicity, (8) threshold of response, and (9) adaptability. Each of these areas contributes uniquely to the child’s ability to form social relationships and respond to the social environment.104
Taken together, these areas of temperament have their own continuum: extreme temperament levels are associated with problematic behaviors, and moderate levels are related to easy and appropriate behaviors. Children who exhibit extreme temperament characteristics (e.g., those who are highly active, moody, or irritable) have been identified as difficult. The difficult child may not fit with the expectations and schedules of caregivers. Others with happy moods and moderate intensity of response are considered easy. A child with an easy temperament may be rhythmic (exhibiting regular sleep/wake cycles) and have positive moods and may have a better fit with caregivers. A match of parent and infant temperament can facilitate strong attachment, just as a mismatch can create difficulties in attachment.
To illustrate how temperament affects goodness of fit, children with arrhythmic, poorly regulated sleep/wake cycles were reported to be difficult to manage by European American families in which the parents worked and needed a consistent routine of sleeping patterns. Puerto Rican parents did not have difficulty in accommodating children with poorly regulated sleep/wake cycles because they molded their schedules around them and allowed their children to sleep when they wanted. In the Puerto Rican families, the incidence of child behavior problems was very low, particularly before school age when a school schedule was imposed.66 These studies and many others suggest that the child’s temperament and behavior affect goodness of fit between the caregiver and the child, which in turn influences developmental outcomes.20
Emotions also play an important part in the child’s appraisal of his or her experience and in the child’s readiness for action in response to contextual change. Emotions relate to how a child evaluates the meaning of an experience in relation to his or her goals. Therefore, if a child engages in an activity with the goal of succeeding but does not, he or she may become disappointed or frustrated. If a child engages in an activity simply to participate and without expectation for success, he or she may experience pleasure irrespective of success. Emotions and temperament (see Chapter 13) influence the child’s interest in attempting new activities, the amount of effort demonstrated, and attempts to engage others. These variables influence how a child approaches an activity (e.g., joyfully, reluctantly) and influences its social nature (e.g., whether the child solicits the involvement of others).
Risk and Resiliency
As suggested in the previous section, developmental outcomes have been attributed to the child’s personality. Research has shown that certain children attain positive developmental outcomes despite a poor caregiving environment. Resiliency refers to a child’s internal characteristics that enable him or her to thrive and develop despite high-risk factors in the environment. The concept of resiliency emerged from studies of child development in which the context included risk factors known to have negative effects (e.g., child abuse, parental mental illness or substance abuse, socioeconomic hardship).107,110 A resilient child has protective factors that enable him or her to develop positive interpersonal skills and general competence despite stressful or traumatic experiences or social environments known to limit developmental potential (e.g., that of an adolescent, single parent). Both child protective factors (e.g., intelligence, prosocial behavior, and social competence) and family protective factors (e.g., material resources, love, nurturance and sense of safety and security, quality of parent-child relationship) are important to positive child outcomes. Researchers have demonstrated that a high-quality relationship with at least one parent, characterized by high levels of warmth and openness and low levels of conflict, is associated with positive outcomes across levels of risk and stages of development.111
A child’s resiliency versus vulnerability also seems to relate to basic physiologic and regulatory characteristics. Children with low cardiovascular reactivity and high immune competence cope better with stressful situations and are less vulnerable to illness when stressed.110 In middle childhood, well-developed problem solving and communication skills are important to a child’s ability to deal with stress. Resilient boys and girls tend to be reflective rather than impulsive, demonstrate an internal locus of control, and use flexible coping strategies in overcoming adversity.110 Therefore, not only are intelligence and competence important to positive outcomes, but so is emotional regulation, that is, being able to monitor, evaluate, and modify the intensity and duration of emotional reactions.107
These concepts suggest that in the interpretation of the influence of environmental factors on a child’s development, variables internal to the child can overcome negative contextual variables, including those believed to have a profound influence (e.g., poor caregiving). Although the evidence suggests that children with strong resilience can overcome a high-risk environment (e.g., abusive situations, poverty), a recent research synthesis of risk and resilience studies found that both internal (e.g., child’s intelligence, positive affect, emotional regulation) and contextual (e.g., supportive family relationships) protective factors are needed for positive outcomes (e.g., school success, positive relationships).107 Taken together, the theories that explain how children grow and develop into competent adults and full participants in the community suggest that a child’s development of occupations must always be understood as an interaction between the child’s biological being and his or her cultural, social, and physical contexts.
AN OCCUPATIONAL THERAPY PERSPECTIVE
Occupations can be defined as the “patterns of action that emerge through transaction between the child and environment and are the things the child wants to do or is expected to do” (p. 22).58 Although most children accomplish certain occupations and their corresponding tasks in a known sequence, the way these tasks are accomplished is unique for each child. A child learns new occupations based on the facility that she or he brings to the activity. Motor and praxis, sensory-perceptual, emotional regulation, cognitive, and communication and social skills contribute to occupational performance.2 These skill areas are interdependent; that is, they work together in such a way that the strengths of one system (e.g., visual) can support limitations in others (e.g., kinesthetic). Which systems are recruited for a task varies according to the novelty of the activity and the degree to which the task has become automatic. For example, research has shown that self-feeding using a spoon involves visual-perceptual, kinesthetic, visual-motor, and cognitive systems.25,45,56 As previously described, grasp of the spoon initially is guided by vision, and the child uses trial and error to hold the spoon so that he or she can scoop the food. With practice and maturation, grasp of the spoon is guided primarily by the kinesthetic system, and correct grasp becomes automatic; vision plays a lesser role. Once food is in the mouth, chewing skills require primarily oral motor skill and somatosensory perception of food texture and food location within the mouth. The skills involved in occupational performance vary not only according to the learning phase but also according to the child’s learning preferences and styles.
Development of Occupations
Humphry proposes that three broad mechanisms enable children to develop occupations.58 These mechanisms, society’s investment in children and their participation in the community, interpersonal influences including caregiving adults and peers, and the dynamics of the child’s occupational performance, are briefly described next.
The broadest influence on children’s occupations is the community in which the child is raised. Communities and society in general have invested in children’s occupations by providing playgrounds, preschools, child-oriented music, child-oriented restaurants, and soccer fields. A community’s orientation toward children determines available opportunities to play organized sports, learn about art and music, safely play in neighborhoods, and gain friendships with diverse peers. Communities that value organized sports and outdoor activity may have soccer or baseball teams, horseback riding, and swimming specifically designed for children with disabilities (e.g., Special Olympics, Miracle League Baseball, therapeutic horseback riding). Characteristics of the community become barriers or opportunities for the child and family and their desired occupations. As advocates for children with disabilities, occupational therapists can influence the development of programs that are accessible and appropriate for children with a wide range of ability. They can emphasize the importance of supporting the participation of all children in community activities, recognizing the different levels of support and accommodation needed.
Humphry suggests that children learn through both direct and indirect social participation.58 A young child’s first learning about an occupation is often through observing his parents, siblings, and other adults or peers. The first representational pretend play is typically imitation of the mother’s actions when cleaning and cooking. Children imitate their parents’ gestures and speech without being explicitly taught to do so. They also learn the consequences of actions by observing how their parents respond to each other or to their siblings. They can learn that an action is wrong by observing punishment of a peer for that action. Vicarious learning appears to be particularly important to a child’s assuming cultural beliefs and values. Children learn the traditions and rituals of a culture by observing their family’s participation in these. Inclusive models of education are believed to be effective learning environments for children with disabilities based on the known benefit of observing and interacting with typical peer models.31,32 When in a child’s presence, therapists should always be conscious that their actions and words influence children’s learning and of whether these actions are directed toward the child.
Learning is generally more vigorous when the child actively participates in an occupation. Children’s play with each other is an integrated learning experience in which the child acts, observes, and interacts. Play involves most or all performance areas, including affective, sensory, motor, communicative, social, and cognitive. When children play together, they learn from, model for, challenge, and reinforce each other. This flow of interactions occurs in meaningful activities that generally bring pleasure and intrinsic reinforcement and enable learning.
To learn a specific skill, the child must actively practice it. Specific scaffolding, guidance, cueing, prompting, and reinforcement by an occupational therapist can assist the child in learning to perform a skill. This direct support from the therapist (or other adult) can facilitate performance at a higher level or at a more appropriate level so that the fit between the child and desired occupations and context becomes optimal. In the case of a child with disabilities, a more intensive level of direct support and scaffolding may be necessary for learning new skills. Adult guidance and support of the child during play can facilitate a successful strategy, help the child evaluate his or her performance, and encourage and reinforce continued practice. Therapists can also optimize the environment to support and reinforce the child’s performance. Participation in play occupations in a natural environment results in integrated learning across performance areas (e.g., including sensory, motor, cognitive, and affective learning).
The child’s play and actions are always within a social, cultural, and physical context. To understand the development of occupational performance, the occupational therapist must understand the child’s play and actions as coherent occupations within specific contexts.
Contexts for Development
Children develop occupations through participation in family activities and cultural practices. As a child participates in the family’s cultural practices, he or she learns occupations and performance skills that enable him or her to become a full participant in the community. Rogoff explains: “People develop as participants in cultural communities. Their development can be understood only in light of the cultural practices and circumstances of their communities” (pp. 3–4).88 Variations in the child’s play activities (e.g., how he or she builds with wooden blocks, draws a picture of himself or herself, or sings a song) reflect the child’s biological abilities and the influence of cultural, social, and physical contexts.
A child’s cultural, social, and physical contexts change through the course of development and tend to expand as the child matures. The environment surrounds and supports the child’s action; it also forces the child to adapt and assists or accommodates that adaptation. As a child perceives the affordances of the environment, he or she learns to act on those affordances, expanding a repertoire of actions. At the same time, the child’s understanding of how the world responds to his or her actions increases. Rogoff argued that culture affects every aspect of the child’s development, which cannot be understood outside this context.88 The child is nested in his or her family, culture, and community, which have influenced the child’s genetic makeup and continue to provide the learning environment. By recognizing this influence, occupational therapists view each child in his or her cultural context and work as change agents within that context.
Cultural practices are the routine activities common to a people of a culture and may reflect religion, traditions, economic survival, community organization, and regional ideology. The child learns motor and process skills through his or her participation in these cultural practices. Reciprocally, a child’s motor and process skills enable participation in the occupations and cultural practices of the child’s family and community.
Cultural Contexts
To fully understand how children develop through participation in cultural practices, Rogoff and her colleagues have studied child development in various cultures, including the European American culture. Their findings, as well as the findings of occupational therapists,10,30 have expanded our understanding of how children develop and have broadened the definition of typical child development.
Cultures vary in many aspects, such as the roles of women and children, values and beliefs about family and religion, family traditions, and the importance of health care and education. The continuum of interdependence versus autonomy of individuals varies in cultural groups and is a significant determinant of childhood occupations. The value a people or community places on interdependence among its members versus individual autonomy creates differences in child-rearing practices and different experiences for developing children.
Most middle-class European Americans value independence as a primary important goal for their children. U.S. parents encourage individuality, self-expression, and independence in their children’s actions and thoughts. To foster early independence in children, U.S. parents do not sleep with their infants; instead infants sleep in their own crib and/or room. Yet this practice is unusual within other societies in the world, such as Asia, Africa, and South America, where infants sleep in their parents’ bed or room.77 For example, Japanese parents report that co-sleeping facilitates infants’ transformation from separate individuals to persons able to engage in interdependent relationships. Japanese parents are interested in promoting continued reciprocity with their children, encouraging the primacy of family relationships.88
One consequence of the early separation of infants from their parents for sleeping is that middle-class U.S. parents often engage in elaborate and time-consuming bedtime routines. In contrast, Mayan parents reported that they do not use bedtime routines (e.g., stories or lullabies) to coax babies to sleep.89 To encourage interdependence, Mayan parents hold their infants continuously, and they often hold them so that they can orient to the group (i.e., facing other members of the group rather than their mothers). By observing others more than their mother, infants become aware of their adult community. In the Latino culture, which also encourages interdependence, parents are permissive and indulgent with young children. Latino parents do not push developmental skills, in part because they value interdependence with the family as opposed to autonomy of the individual.117
In general, cultures that value independence over interdependence also value competition over cooperation. Korean American children have been found to be more cooperative in play than European American children. Mexican children also are more likely to cooperate than European American children.88 These examples briefly illustrate how cultural beliefs influence the ways parents raise their children and communities support and challenge children.
Social Contexts
Culture influences the social relationships that envelop the child, yet certain aspects of the child’s social context appear to be independent of cultural influences and are consistent across cultures. This section defines elements of the social context particularly important to a child’s development. The most important relationships formed during infancy are those with parents and/or primary caregivers. When caregivers are sensitive and responsive to the infant, healthy socioemotional development results.33,68 Infants’ interactions with parents serve to enhance the infants’ basic physiologic and regulatory systems. When parents attune to the infant’s sensory modulation and arousal needs and support these needs, the infant develops secure attachment. Mothers who modulate their behaviors to match their infants’ needs for stimulation and comfort also promote the infants’ abilities to self-regulate. The child’s interaction with a caregiver gives him or her essential information about how self and other are related, which becomes important to engaging in future relationships. Attachment patterns seem to influence the child’s style of interaction and engagement in later years. Sensitive responding consolidates the infant’s sense of efficacy and provides a foundation of security for confident exploration of the environment.33
Csikszentmihalyi and Rathunde describe parenting as a dance between supporting and challenging the child.29 Supporting the child enables him or her to assimilate or explore the environment—that is, to play. Parental challenge requires a child to accommodate and conform. Parenting provides a combination of these supports and challenges. Rogoff defines the support-challenge combination of guided participation as adults’ challenging, constraining, and supporting children in solving problems.88 All parents use some measure of support to bolster children’s attempts to master skills and some degree of challenge to move children toward higher levels of mastery. These elements are subtly provided by parents in the ways they present tasks and select when and how they instruct or intervene. Effective guidance relies on careful observation of the child’s cues. Sensitivity and responsivity to the child’s needs appear to be among the most important variables in the promotion of child development.66 The concept of guided participation is similar to Vygotsky’s notion of the zone of proximal development. In guided participation, emphasis is placed on parents’ sensitivity to the child’s skills to determine the level of support or challenge needed.
In typical situations, infants receive care from multiple care providers, including child care providers, grandparents, and other adults. The infant may or may not attach to caregivers other than the parents or primary caregivers; however, these social relationships are important to the infant’s emotional development and provide opportunities for the development of social skills. At least 60% of children under 5 years of age participate in non-parent child care, including center-based and family child care.78 A study for the National Institute of Child Health and Human Development revealed that positive caregiving occurred when children were in smaller groups, child-to-adult ratios were low, caregivers did not use an authoritarian style, and the physical environment was safe, clean, and stimulating.79 Family factors predicted child outcomes even for children who spent many hours in child care. The family environment appears to have a significantly greater effect on a child’s development than the child care environment.38
Physical Contexts
The physical environment surrounds and supports the child’s action; it forces the child to adapt his or her actions to meet the demands and constraints of the physical surroundings. As a child perceives the affordances of the environment, he or she learns to act on those affordances, thus expanding a repertoire of actions. At the same time, the child’s understanding of how the world responds to his or her actions increases. Gibson explained how a child’s exploration of physical surfaces and objects allows him or her to develop and practice mobility and manipulation skills.47 Examples of the interactions of a child and his or her physical environments and the developmental consequences are presented next.
CHILDREN’S OCCUPATIONS, PERFORMANCE SKILLS, AND CONTEXTS
This section describes the child’s development of play occupations as enabled by his or her performance skills and cultural, physical, and social contexts. For three age groups—infancy, early childhood, and middle childhood—typical play occupations and activities are described. The contribution of motor, sensory, emotional, cognitive, and social abilities and contexts to the development of play occupations is described. Although children’s occupations are similar within a particular age level, the contexts, individual abilities, and activities are varied and diverse, resulting in a unique occupational performance for each child. Recognition of the uniqueness of a child’s development and of how these components contribute to performance within individuals is key to analysis of occupational performance.
Although the child learns occupations other than play (e.g., those related to school function), occupational therapists most often use play activities to engage the child in the therapeutic process. Play activities serve as the means to improve performance because they are self-motivating and offer goals around which the child can self-organize.81 Play also serves as the end or goal of therapy services. Children put effort and energy into play activities because they are inherently interesting and fun. (A more detailed description of play as a goal and modality of therapy can be found in Chapter 18.) Descriptions of a child’s development of feeding, self-care, and school function are presented in other chapters (Chapters 15,16 and 24). The contribution of communication abilities is also important to the development of play and other childhood occupations, but it is not discussed in this chapter because language and communication are not primary concerns for occupational therapists.
Infants: Birth to 2 Years
The play occupations of infants in the first 12 months are exploratory and social—that is, they are related to bonding with caregivers (Boxes 3-1 and 3-2). As in every stage, these occupations overlap (e.g., bonding occurs during exploratory play with the parent’s hair and face, and the parent’s holding supports the infant’s play with objects). Much of the infant’s awake and alert time is spent in exploratory play, often play that occurs in the caregiver’s arms or with the caregiver nearby.
Exploratory play is also called sensorimotor play. Rubin defined exploratory play as an activity performed simply for the enjoyment of the physical sensation it creates.92 It includes repetitive movements to create actions in toys for the sensory experiences of hearing, seeing, and feeling. The infant places toys in the mouth, waves them in the air, and explores their surfaces with the hands. These actions allow for intense perceptual learning and bring delight to the infant (without any more complex purpose).
In the second year of life, the infant engages in functional, or relational, play; that is, an object’s function is understood, and that function determines the action (Boxes 3-3 and 3-4). Initially, children use objects on themselves (e.g., pretending to drink from a cup or to comb the hair). These self-directed actions signal the beginning of pretend play.83 The child knows cause and effect and repeatedly makes the toy telephone ring or the battery-powered doll squeal to enjoy the effect of the initial action.
By the end of the second year, play has expanded in two important ways. First, the child begins to combine actions into play sequences (e.g., he or she relates objects to each other by stacking one on the other or by lining up toys beside each other). These combined actions show a play purpose that matches the function of the toy. Second, 2-year-old children now direct actions away from themselves. The objects used in play generally resemble real-life objects.67 The child places the doll in a toy bed and then covers it. The child pretends to feed a stuffed animal or drives toy cars through a toy garage. At 2 years of age, play remains a very central occupation of the child, who now has an increased attention span and the ability to combine multiple actions in play. The emergence of symbolic, or imaginary, play with toys and objects offers the first opportunities for the child to practice the skills of living.
The child also engages in gross motor play throughout the day. As he or she becomes mobile, exploration of space, surfaces, and large action toys becomes a primary occupation. Movement is also enjoyed simply as movement; the child delights in swinging and running or attempting to run and moving in water or sand. Deep proprioceptive pressure and touch are craved and requested. As in exploratory play, the child’s exploration of space involves simple, repeated actions in which the goal appears to be sensation. Often, extremes in sensation seem to be enjoyed and are frequently requested. Repetition of these full-body kinesthetic, vestibular, and tactile experiences appears to be organizing to the CNS. In addition, this repetition is important to the child’s development of balance, coordination, and motor planning. Hence, the occupational goal of movement and exploration becomes the means for development of multiple performance areas.
In the first year, the goal of an infant’s social play is attachment, or bonding, to the parents). As described by Greenspan, this is a period in which the infant falls in love with the parents and learns to trust the environment because of the care and attention provided by the parents or caregivers.54 These occupations are critical foundations to later occupations that involve social relating and demonstration of emotions. At 1 year of age, infants play social games with parents and others to elicit responses. Although infants at this age engage readily with individuals other than family, they require their parents’ presence as an emotional base and return to them for occasional emotional refueling before returning to play.105
By the second year, children exhibit social play in which they imitate adults and peers. Imitation of others is a first way to interact and socially relate. Both immediate and deferred imitation of others are important to social play as children enter preschool environments and begin to relate to their peers.
Performance Skills
Sensory and Motor Skills: The newborn can interpret body sensations and respond reflexively. He enjoys and needs a consistent caregiver’s physical contact and tactile stimulation. The neonate turns his head when touched on the cheek, relaxes in his mother’s arms, and expresses discomfort from a wet diaper. Self-regulation of sleep-wake cycles, feeding, and display of emotions and arousal emerge in early infancy. The infant molds himself to the parents’s embrace, clinging to the parent’s arms and chest. The newborn’s vestibular system is also quite mature as he calms from rocking and enjoys the motion of a parent walking him about the room. The neonate demonstrates orientation and attention to visual, auditory, and tactile stimuli. An important fact is that the newborn also exhibits habituation, or the ability to extinguish incoming sensory information (e.g., ability to sleep by blocking out sound in a noisy nursery).
Gross motor activity begins prenatally in response to vestibular and tactile input inside the womb. The first movements of newborns appear to be reflexive; however, on closer examination, they reveal the ability to process and integrate sensory information. The neonate’s motor responses contribute to perceptual development and organization. In the first month of life, the infant moves the head side to side when in a prone position and rights the head when supported in sitting. By 4 months, the prone infant lifts the head to visualize activities in the room. This ability to lift and sustain an erect-head position appears to relate to the infant’s interest in watching the activities of others, as well as improved trunk strength and stability. As the infant reaches 6 months, he or she demonstrates increased ability to lift the head and trunk when in a prone position to visualize the environment when prone. The infant can also move side to side on the forearms, then the hands, and can lift an arm to grasp a toy (Figure 3-4). When supine, the child actively kicks and brings the feet to the mouth. Over the next 6 months, this dynamic, postural stability prepares the infant to become mobile.

FIGURE 3-4 Inprone position, the infant shifts his weight from side to side when playing with toys; later he learns to pivot while prone to expand where he can reach and what he can visualize.
Rolling is normally the infant’s first method of becoming mobile and exploring the environment. Initially, rolling is an automatic reaction of body righting; usually the infant first rolls from the stomach to the side and then from the stomach to the back. By 6 months, the infant rolls sequentially to move across the room. Heavy or large babies may initiate rolling several months later, and infants with hypersensitivity of the vestibular system (i.e., overreactivity to rotary movement) may avoid rolling entirely.
Most infants enjoy supported sitting at a very early age. As their vision improves in the first 4 months, they become more eager to view their environment from a supported sitting position. The newborn sits with a rounded back; the head is erect only momentarily. Head control emerges quickly. By 4 months, the infant can hold the head upright with control for long periods, moving it side to side with ease. Most 6-month-old infants sit alone by propping forward on the arms, using a wide base of support with the legs flexed. However, this position is precarious, and the infant easily topples when tilted. Many 7-month-old infants sit independently. Often their hands are freed for play with toys, but they struggle to reach beyond arm’s length.
By 8 to 9 months, the infant sits erect and unsupported for several minutes. At that time, or within the next couple of months, the infant may rise from a prone posture by rotating (from a side-lying position) into a sitting position. This important skill gives the infant the ability to progress by creeping to a toy and then, after arriving at the toy, to sit and play. By 12 months, the infant can rise to sitting from a supine position, rotate and pivot when sitting, and easily move in between positions of sitting and creeping (Figure 3-5).


FIGURE 3-5 A, In dynamic sitting, the infant has sufficient postural stability to reach in all directions. B, By 10 months, the infant easily moves into and out of sitting positions.
After experimenting with pivoting and backward crawling in a prone position, the 7-month-old infant crawls forward. He or she may first attempt belly crawling using both sides of the body together. However, reciprocal arm and leg movements quickly emerge as the most successful method of forward progression. Crawling in a hands-and-knees posture (sometimes called creeping) requires more strength and coordination than belly crawling. The two sides of the body move reciprocally. In addition, shoulder and pelvic stability are needed for the infant to hold the body weight over the hands and knees. Mature, reciprocal hands-and-knees crawling also requires slight trunk rotation (Figure 3-6). Through the practice of crawling in the second 6 months of life, the child develops trunk flexibility and rotation. Most 10- to 12-month-old infants crawl rapidly across the room, over various surfaces, and even up and down inclines.
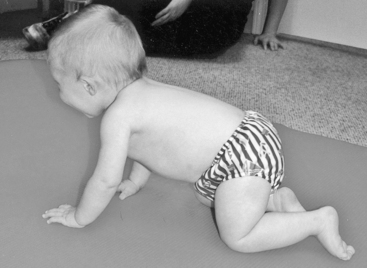
FIGURE 3-6 Crawling on all fours allows the infant to explore new spaces. This form of mobility increases shoulder and pelvic stability for upright stance and promote the rotational patterns needed for ambulation. From Henderson, A., & Pehoski, C. [2006]. Hand function in the child: Foundations for remediation [2nd ed.]. St. Louis: Mosby.
Infants at 5 and 6 months delight in standing, and they gleefully bounce up and down while supported by their parents’ arms. The strong vestibular input and practice of patterns of hip and knee flexion and extension are important to the development of full upright posture after 1 year. The young infant also prepares for a full upright posture by standing against furniture or the parent’s lap. A 10-month-old infant practices rising and lowering in upright postures while holding onto the furniture. By pulling up on furniture to standing, the infant can reach objects previously unavailable. This new level of exploration and increase in potential play objects motivates infants to practice standing and motivates parents to place breakable objects on higher shelves (Figure 3-7). At 12 months the infant learns to shift the body weight onto one leg and to step to the side with the other leg. The infant soon takes small steps forward while holding onto furniture or the parent’s finger.

The infant’s first efforts toward unsupported forward movement through walking are often seen in short, erratic steps, a wide-based gait, and arms held in high guard. All these postural and mobility skills contribute to the infant’s ability to explore space and obtain desired play objects. By 18 months, the infant prefers walking to other forms of mobility, but balance remains immature, and the infant falls frequently. He or she continues to use a wide-based gait and has difficulty with stopping and turning. Infants remain highly motivated to practice this new skill, however, because walking brings new avenues of exploration and a sense of autonomy, and the parent must now protect the infant from objects that previously could not be reached and from spaces that have not yet been explored.
The newborn moves the arms in wide ranges, mostly to the side of the body. In the first 3 months, the infant contacts objects with the eyes more than with the hands. By 3 months, he follows his mother’s face in a smooth arc, crossing midline. As early as 1 to 2 months, an infant learns to swipe at objects placed at his or her side. This first pattern of reaching is inaccurate, but by 5 months, the accuracy of reaching towards objects increases greatly.91 The infant struggles to combine grasp with reach and may make several efforts to grasp an object held at a distance. As postural stability increases, the infant also learns to control arm and hand movements as a means of exploring objects and materials in the environment. By the time an infant is 6 months old, direct unilateral and bilateral reaches are observed, and the infant smoothly and accurately extends the arm toward a desired object.108
Grasp changes dramatically in the first 6 months (Figure 3-8, A and B). Initially, grasping occurs automatically (when anything is placed in the hand) and involves mass flexion of the fingers as a unit. The object is held in the palm rather than distally in the fingers or fingertips. Three- to 4-month-old infants, therefore, squeeze objects within their hands, and the thumb does not appear to be involved in this grasp. At 4 to 5 months, the infant exhibits a palmar grasp in which flexed fingers and an adducted thumb press the object against the palm (Figure 3-8, C). At 6 months, the infant uses a radial palmar grasping pattern in which the first two fingers hold the object against the thumb. This grasp enables the infant to orient the object so that it can be easily seen or brought to the mouth (Figure 3-8, D). The infant secures small objects using a raking motion of the fingers, with the forearm stabilized on the surface.
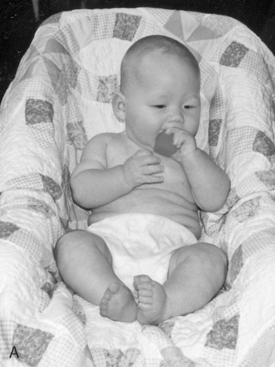

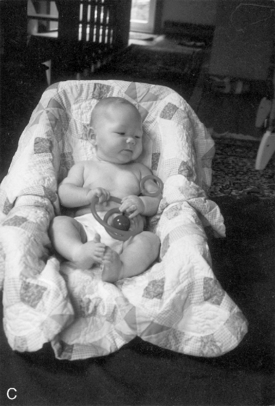
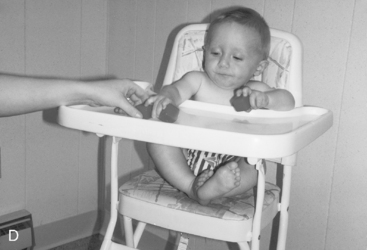
FIGURE 3-8 A, Grasping patterns evolve from palmar grasps without active thumb use to radial digital grasps as in B. C, At 4 months, the infant holds the object tight against the palm, with all fingers flexing as a unit. D, At 8 months, the infant holds objects in the radial digits. A and B from Henderson, A., & Pehoski, C. [2006]. Hand function in the child: Foundations for remediation [2nd ed.]. St. Louis: Mosby.
Grasp continues to change rapidly between 7 and 12 months.14,27 A radial digital grasp emerges in which the thumb opposes the index and middle finger pads. At approximately 9 months, wrist stability in extension increases, and the infant is better able to use the fingertips in grasping (e.g., the infant can use fingertips to grasp a small object, such as a cube or cracker). By holding objects distally in the fingers, the infant can move the object while it is in the hand; movement of objects within the hands allows the infant to explore them and use objects for functional purposes. A pincer grasp, with which the infant holds small objects between the thumb and finger pads, develops by 10 to 11 months. The 12-month-old infant uses a variety of grasping patterns, often holding an object in the radial fingers and thumb. The infant may also grasp a raisin or piece of cereal with a mature pincer grasp (i.e., one in which the thumb opposes the index finger).
In the second year of life, grasping patterns continue to be refined. The child holds objects distally in the fingers, where holding is more dynamic. By the end of the second year, a tripod grasp on utensils and other tools may be observed. Other grasping patterns may also be used, depending on the size, shape, and weight of the object held. For example, tools are held in the hand using first a palmar grasp and then a digital grasp. Blended grasping patterns develop toward the end of the second year, allowing the child to hold a tool securely in the ulnar digits while the radial digits guide its use.
Voluntary release of objects develops around 7 and 8 months. The first release is awkward and is characterized by full extension of all fingers. The infant becomes interested in dropping objects and practices release by flinging them from the high chair. By 10 months, objects are purposefully released into a container, one of the first ways the infant relates separate objects. As the infant combines objects in play, release becomes important for stacking and accurate placement. For example, the play of 1-year-old children includes placing objects in containers, dumping them out, and then beginning the activity again.
Between 15 and 18 months, the infant demonstrates release of a raisin into a small bottle and the ability to stack two cubes. Stacking blocks is part of relational play, because the infant now has the needed control of the arm in space, precision grasp without support, controlled release, spatial relations, and depth perception. The infant can also place large, simple puzzle pieces and pegs in the proper areas. At the same time, the infant acquires the ability to discriminate simple forms and shapes. Therefore, the infant’s learning of perceptual skills is supported by improved manipulative abilities, and increased perceptual discrimination promotes the infant’s practice of manipulation.82 Perception of force increases, enabling the infant to hold an object with the just-right amount of pressure (e.g., so cookies are not crushed before eaten).
The complementary use of both hands to play with objects develops between 12 months and 2 years. During this time, one hand is used to hold the object while the other hand manipulates or moves the object. It is not until the third year that children consistently demonstrate use of two hands in simultaneous, coordinated actions (e.g., using both hands to string beads or button a shirt).36
Cognitive Skills: In the first 6 months, the infant learns about the body and the effects of its actions. Interests are focused on the actions with objects and the sensory input these actions provide. The infant’s learning occurs through the primary senses: looking, tasting, touching, smelling, hearing, and moving. The infant enjoys repeating actions for their own sake, and play is focused on the action that can be performed with an object (e.g., mouthing, banging, shaking), rather than the object itself.67 By 8 to 9 months, the infant has an attention span of 2 to 3 minutes and combines objects when playing (e.g., placing favorite toy in a container). At this age, children begin to understand object permanence; that is, they know that an object continues to exist even though it is hidden and cannot be seen.23 They can also find a hidden sound and actively try to locate new sounds.
By 12 months, the infant’s understanding of the functional purpose of objects increases. Play behaviors are increasingly determined by the purpose of the toy, and toys are used according to their function. The infant also demonstrates more goal-directed behaviors, performing a particular action with the intent of obtaining a specific result or goal. Tools become important at this time, because the infant uses play tools (e.g., hammers, spoons, shovels) to gain further understanding of how objects work. At the same time, the infant begins to understand how objects work (e.g., how to activate a switch or open a door).
In the second year, the child can put together a sequence of several actions, such as placing small “people” in a toy bus and pushing it across the floor. The sequencing of actions indicates increasing memory and attention span. Some of the first sequential behaviors illustrate the child’s imitation of parent or sibling actions; therefore, increased ability to imitate and increased play sequences appear to develop concurrently (Figure 3-9).
Social Skills: The infant’s emotional transition from the protective, warm womb to the moment of birth is a dramatic change. The primary purpose of the newborn’s system is to maintain body functions (i.e., the cardiovascular, respiratory, and gastrointestinal systems). However, as the infant matures, the focus shifts to increasing competence in interaction with the environment. The sense of basic trust or mistrust becomes a main theme in the infant’s affective development and is highly dependent on the relationship with the primary caregivers. According to Erikson, the first demonstration of an infant’s social trust is observed in the ease with which he or she feeds and sleeps.35
The basic trust relationship has varying degrees of involvement. Parent-infant bonding is not endowed but is developed from experiences shared between parent and child over time. These feelings are seen in the progression of physical contact between parent and infant. The infant shows a differentiated response to the parent’s voice, usually quieting and calming. Although infants are capable of crying from birth, they begin to express other emotions by 2 months, such as smiling and laughing.
By 5 to 6 months, the infant becomes very interested in a mirror, indicating a beginning recognition of self. By 4 to 5 months, he or she vocalizes in tones that indicate pleasure and displeasure. In the second year of life, the parents (or caregivers) remain the most important people in the child’s life. The 2-year-old infant likes to be in constant sight of the parents and expresses emotions by hugging and kissing them.
Although toddlers practice their autonomy around parents, they have no intention of giving up reliance on them and may become upset or frightened when the parents leave. Two-year-old children are interested in other children, but they tend to watch them rather than verbally or physically interacting with them. In a room of open spaces, these children are likely to play next to each other. Their side-by-side play often involves imitation, with few verbal acknowledgments of each other.
Contexts of Infancy
Cultural Contexts: The family’s cultural beliefs and values influence caregiving practices and determine many of the child’s earliest experiences. For example, feeding and co-sleeping practices both influence the infant’s development. Breast feeding and bottle feeding practices vary in different cultures and ethnic groups. Although practices vary in the United States, European American mothers tend to breast-feed for the first 6 months. Mothers often establish a feeding schedule, separating feedings by longer intervals as the infant matures. African American families expect the infant to make the transition to table food quickly, and infants generally eat only table food by 1 year.113 In contrast, Chinese and Filipino infants are often breast-fed on demand until 2 to 2½ years of age.17,18 These parents are often very attentive, carrying and holding their infants throughout the day, even during naps. When the infants are not held, they are kept nearby and picked up immediately if they cry.18 In many countries, children are fed certain foods as medicine, that is, to improve health or prevent illness. For example, in the Middle East, infants are given tea and herbal mixtures to prevent or cure illness, and a dietary balance of hot and cold foods is believed to be essential to good health.95
Children around the world are encouraged to self-feed at different ages using different utensils and methods. In India, toddlers learn to use only the right hand to eat. The left hand is dirty and is used only to clean oneself after defecation. As children learn to self-feed, parents often restrain the left hand.88 As a result, the right hand develops early advanced skills to manipulate and prehend food without the assistance of the left. These self-feeding practices can contribute to children’s rapid maturation of right-hand dexterity. Studies of Japanese child have shown higher-level fine motor skills than those in American children. The greater fine motor skills of Chinese children have been attributed, in part, to their early use of chopsticks as feeding utensils.114
In most middle-class U.S. homes, children sleep separated from their parents. For the earliest ages, children are placed in a separate crib and generally a separate room. The parents believe that infants and toddlers need to learn to sleep independently and become independent in self-care skills as soon as possible. In most societies outside the United States, infants sleep with their mothers.88 Mayan infants and toddlers sleep in the same room with their parents, often in the mother’s bed.77 Asian and Middle Eastern parents tend to sleep with their infants, because they believe that these sleeping arrangements are important to nurturing and bonding. In some African American and Appalachian families, parents sleep with their infants. Close physical contact at night and then into the day can foster interdependence within families, in contrast with the independence that most U.S. parents often foster in their children.
Physical Contexts: Although many infants have a supplemental play area in a child care center, the home provides the infant’s first play environment. The crib is often a play environment, providing a place for comforting toys (e.g., music boxes, colorful mobiles). Other early play spaces include the playpen, infant seat, and swing. The infant also spends time playing on the floor’s carpeted surface or on a blanket. Because the infant is not yet mobile, safety is not as much of a concern as it will be in the next 2 years of life. Early play also occurs in the parent’s or caregiver’s arms. Exploratory play and attachment occupations are pursued on the parent’s lap, and the infant is fascinated by the parent’s face and clothing. At the same time, the infant feels safe and comforted by the parent’s presence.
In the second 6 months, the infant requires less support to play, and a major role of the parent becomes one of protector from harm. As the infant becomes more mobile, spaces are closed and objects now within reach are removed. Exploration of all accessible spaces becomes an infant’s primary goal.
In the second year of life, the child’s environment may expand to the yard, to neighbors’ homes and yards, and to previously unexplored spaces in the home. Most children have opportunities for play in their home’s yard or in the fenced-in areas of their child care centers. Although the child’s increasing interest in visiting outdoor spaces provides important opportunities for sensory exploration, it also creates certain safety concerns. Parents therefore invest in gates and other methods of restricting the child’s mobility to safe areas.
Early Childhood: Ages 2 to 5 Years
The three types of play that predominate in early childhood are (1) pretend, or symbolic, play, (2) constructive play, and (3) rough-and-tumble, or physical, play (Boxes 3-5 and 3-6). Similar changes are observed in each type of play. First, the child’s play becomes more elaborate—that is, the child now combines multiple steps and multiple schema. Short play sequences become long scripts involving several characters or actors in a story.64,67 Second, play becomes more social. The preschool-age child orients play toward peers, involving one or two peers in the story and taking turns playing various roles. When preschool-age children play with peers, the interaction appears to be as important as the activity’s goal. As the child approaches 5 years of age, all play becomes increasingly social, generally involving a small group of peers.64,99
Beginning at 2 years of age and continuing through the early childhood years, the child’s play is symbolic and imaginative. The child pretends that dolls, figurines, and stuffed animals are real. He or she may also imitate the actions of parents, teachers, and peers. At ages 3 and 4, pretend play becomes more abstract, and objects, such as a block, can be used to represent something else. Pretend play now involves many steps that relate to each other. Children develop scripts as a basis for their play (e.g., one child is the father and one is the mother). They base these scripts on real-life events and play their roles with enthusiasm and imagination, creating their own stories and enjoying the power of their imaginary roles. Their dramatic play is quite complex at this time. However, when they are in small groups, their interaction with their peers seems to be more important than the play goal, and they can easily turn to new activities suggested by one of the group.
By 5 years of age, this imaginary play is predominantly social, as small groups of two and three join in cooperative play. About one-third of the time, a 5-year-old child engages in pretend play.93 However, this pretend play is based on imitation of real life and dressing up to play certain roles (e.g., firefighter, police officer, ballerina). Although children of this age demonstrate some understanding of adult roles, they erroneously assume that roles are one-dimensional (e.g., a firefighter has one role, that of putting out fires). Through pretending, children develop creativity, problem solving, and an understanding of another person’s point of view (Boxes 3-7 and 3-8).96
Play that involves building and construction also teaches the child a variety of skills during early childhood. At first, these skills are demonstrated in the completion of puzzles and toys with fit-together pieces (Figure 3-10). However, with mastery of simple pegs and puzzles, the child becomes more creative in construction. For example, the 4-year-old child can develop a plan to build a structure with blocks and then carry out the steps to complete the project. With instructions and a model, the 5-year-old child can make a simple art project or create a three-dimensional design. A 5-year-old child can also put together a 10-piece puzzle. The final product has become more important, and the child is motivated to complete it and show others the final result. The planning and designing involved in building and construction play helps the child acquire an understanding of spatial perception and object relationships. This activity also appears to be foundational to academic performance in school.

FIGURE 3-10 Four-year-old children complete puzzles and enjoy construction activities in small groups.
Children from 2 to 5 years of age are extremely active and almost always readily engage in rough-and-tumble play. They continue to delight in movement experiences that provide strong sensory input. Activities such as running, hopping, skipping, and tumbling are performed as play without any particular goal. Although rough-and-tumble play generally involves other children, it is generally noncompetitive and rarely organized. Children enjoy this activity for the simple, simultaneous pleasure of movement as they play together.15
In associative physical play, children are generally more interested in being with other children than in the goal of the activity. However, it is important to note that some children enjoy primarily social play, whereas others enjoy solitary play. These differences do not relate to ability as much as they relate to preferences and temperament.105
Performance Skills
Sensory and Motor Skills: Young children are amazingly competent individuals, and their repertoire of motor function leaps forward during the preschool years (see Performance Skills in Boxes 3-6, 3-7 and 3-8). By age 2 years, the child walks with an increased length of stride and an efficient, well-coordinated, and well-balanced gait. Although children begin to run by 2 years, they do not exhibit true running (characterized by trunk rotation and arm swing) until 3 to 4 years of age. The 4-year-old child demonstrates a walking pattern similar to that of an adult. By 5 to 6 years of age, the mature running pattern has developed, and children test their speed by challenging each other to races.
As mobility develops, children gain access to spaces previously unavailable to them. By 2 years of age, a child walks up stairs without holding onto a parent’s hand, and at 2½ years the child can walk down stairs without support. The 3½-year-old child walks up and down stairs by alternating the feet and without needing to hold onto a rail.
Running and stair climbing become possible, in part, because the child’s balance and strength increase. Emerging balance can be observed as the 2-year-old child briefly stands on one foot to kick a ball. By 5 years of age, the child can balance on one foot for several seconds and walk on a curb without falling.40 Between 3 and 5 years, the child may successfully attempt to use skates or roller blades.
Jumping is first observed in the 2-year-old child. This skill requires strength, coordination, and balance. By 3 years of age the child can jump easily from a step. Hopping requires greater strength and balance than jumping and is first observed at 3½ years. Skipping is the more difficult gross motor pattern, because it requires sequencing of a rhythmic pattern that includes a step and a hop. A coordinated skipping pattern is not observed until 5 years of age.63
Two-year-old children begin to pedal tricycles and move small riding toys. By 3 years of age they can pedal a tricycle but may run into objects. The 4-year-old child can steer and maneuver the tricycle around obstacles.
By 2½ years, most children can catch a 10-inch ball. This pattern of maturity enables the 4-year-old child to catch a much smaller ball successfully, such as a tennis ball.40 The first pattern of throwing involves a pushing motion, with the elbow providing the force for the throw. The 4-year-old child demonstrates more forward weight shift with throwing, thereby increasing the force of the ball and the distance thrown. Kicking emerges in the 2- to 3-year-old child, with accurate kicking to a target exhibited by 6 years of age. Ball skills become increasingly important as the child begins participating in organized sports during the primary grades.
Early childhood is a time of rapid improvement in fine motor and manipulation performance. By 4 years of age, children learn to move small objects efficiently within one hand (i.e., in-hand manipulation). The 4-year-old child can hold several small objects in the palm of the hand while moving individual pieces with the radial fingers.82 In-hand manipulation indicates that isolated finger movement is well controlled and that the thumb easily moves into opposition for pad-o-pad prehension. These skills also indicate that the child can modulate force and that he or she has an accurate perception of the gentle force needed to handle small objects with the fingertips.82
With efficient in-hand manipulation, the preschool child also learns the functional use of drawing and cutting tools. Most 3-year-old children hold a pencil with a static tripod grasp (i.e., with the pencil resting between the thumb and first two fingers) and use forearm and wrist movement to draw; however, by 5 years, a child demonstrates a mature, dynamic tripod. In this grasp pattern, the pencil is held in the tips of the radial fingers and is moved using finger movement. By controlling the pencil using individual finger movements, the child can make letters and small forms.
Drawing skills progress from drawing circles to lines that intersect and cross in a diagonal (e.g., an X). The 5-year-old child can draw a person with multiple and recognizable parts. Drawing is often a strong interest at this age and therefore contributes to the child’s imaginative play. He or she can also draw detailed figures created in the imagination (i.e., monsters, fairies, and other fanciful creatures).
The development of scissors skills follows the development of controlled pencil use. The first cutting skill, observed at 3 years, is snipping with alternating full-finger extension and flexion. Between 4 and 6 years, bilateral hand coordination, dexterity, and eye-hand coordination improve, enabling the child to cut out simple shapes. Mature use of scissors is not achieved until 5 to 6 years, because it requires isolated finger movements, simultaneous hand control, and well-developed eye-hand coordination for cutting accuracy.40
Other fine motor skills acquired during the preschool years are important to the child’s constructive and dramatic play. Activities such as putting puzzles together, building towers, stringing small beads, using keys, and cutting out complex designs usually require dexterity, bilateral coordination, and motor planning.
Cognitive Skills: Preschool-age children create symbolic representations of real-life objects and events during play. In addition, they begin to plan pretend scenarios in advance, organizing who and what are needed to complete the activity. Play becomes an elaborate sequence of events that is remembered, acted out, and later described for others. For example, the child may act out the role of an adult, imitating action remembered from an earlier experience. This form of role play demonstrates the child’s understanding of how roles relate to actions and how actions relate to each other (e.g., the child may role play a grocery store clerk, displaying items for sale, taking money from the customer, and placing the money in a toy cash register).
Abstract thinking begins in the preschool years as the child pretends that an object is something else. For example, the child may pretend a block is a doll bed; later the same block may become a telephone receiver or a train car.
The motor skills noted in early childhood also reflect cognitive skills. To construct a three-dimensional building, the child must have the ability to discriminate size and shape. Building in three dimensions also requires spatial understanding and problem-solving skills. When building from a set of blocks, the child usually must first categorize and organize the blocks. Next, the child must solve the problem of how to fit them together to replicate a model or create the imagined structure.
In a similar way, the emergence of drawing skills reflects both cognitive abilities and fine motor skills. The 3-year-old child makes crude attempts to represent people and objects in drawings. By 4 years of age, a child can draw a recognizable person, demonstrating the ability to select salient features and represent them on a two-dimensional surface. The 4-year-old child not only identifies the parts of a person but also relates them correctly, although the size of the parts is rarely proportional to real life. At 5 years, the child’s drawing is more refined, more realistic, and better proportioned. By this age, pictures begin to tell stories and reflect the child’s emotions.67
Social Skills: In early childhood, interaction and play with peers take on increasing importance. Children become social beings and identify themselves as individuals (i.e., separate from parents). Autonomy dominates the psychosocial development from 2 to 4 years, as the toddler shows his independence by moving away from the parent. The child is adamant about making personal decisions. The development of trust in the environment and improvements in language bring forth control over self, strengthening the child’s autonomous nature.
The discovery of the body and how to control it promotes independence in self-care. Success in acting independently instills a sense of confidence and self-control. The child also begins to perceive that now all of his independent actions meet the approval of adults.
Children need to achieve a balance between initiative to act independently and the responsibility they feel for their own actions. Children 4 to 5 years old explore beyond the environment, discovering new activities. They seek new experiences for the pleasure of learning about the environment and for the opportunities they offer for exploration. If the child’s learning experiences are successful and effective and his or her actions meet parental approval, a sense of initiative is developed. Through these activities, the child learns to question, reason, and find solutions to problems.
Adult-child relationships and early home experiences also influence later peer relations. According to research, children whose attachments to their mothers are rated as secure tend to be more responsive to other children in child care settings. They are also more curious and competent.62,115 Peer play becomes an important avenue for the child’s development of social and cognitive abilities. With their peers, they practice social roles, engage in dramatic play, and enjoy rough and tumble play.
The development of autonomy provides a foundation for the child’s imagination. Now the young child explores the world not only through the use of his or her senses but also by thinking and reasoning. Although play can be reality based, it usually includes fantasy, wishes, and role play. Words, rhymes, and songs also complement this type of play.
Contexts
Cultural and Social Contexts: The social roles of young children vary across cultures. The following discussion of cultural differences highlights how culture contributes to a child’s development. In the United States, the importance of interaction with peers is stressed at young ages. Most American children begin to interact with their peers (same age group) at about 3 years of age. Same-age peers become increasingly important through elementary school and dominate the social life of a teenager. In the United States and much of the world, children are grouped exclusively by age. These age groupings may provide more opportunities for play, but they also diminish opportunities for older children to teach and nurture younger children. Younger children have fewer opportunities to imitate older children.
Children in other parts of the world play and socialize with people of different ages. For example, in Mayan communities, children spend almost all of their time with siblings and other young relatives of a wide range of ages.10 In Polynesia, children remain with family members, including extended family. They socially participate in mixed-age groups, playing “on the edge” and watching intently until they can join in the play. In Mexican families, toddlers play with children of various ages. Often they play with older siblings. This “enduring social network” remains in place over time to care for, teach, and discipline children to adulthood.88
When children spend their days with a variety of ages, they have many opportunities to imitate and learn from older children and adults. Interaction with children of varying ages provides older children the opportunity to practice teaching and nurturance with young children and provides young children with the opportunity to imitate older children.112
At very young ages, Mayan children play within their parents’ work activities.10 For example, children engage in play activities while helping their mothers wash clothes. The children’s play in the Mayan culture is tolerated during daily work activities but is not specifically encouraged.10 Bazyk and her colleagues10 found that children’s work was playful, blurring the European American distinction between work and play. When children play in work activities, they are learning skills that will serve them well in adulthood. In contrast, the age-based groupings used in U.S. child care centers and preschools provide children with opportunities to play with same-age peers but reduce their opportunities to play within adult work activities.
Families in the United States specifically design and encourage their children’s play and at times become playmates with children. Although play is emphasized as the primary occupation for young children, children demonstrate interest in helping parents accomplish their work. Parents may encourage young children (e.g., 5-6 years) to participate in household tasks, such as picking up their own toys. When children begin school, parents usually expect them to participate more in household tasks such as cleaning and meal preparation.65
Physical Contexts: By the age of 5, a child’s outdoor environment has expanded beyond the areas around the home and child care center. A variety of outdoor environments offer space for rough-and-tumble play, and expanded social and physical environments give the child new opportunities for learning (and generalizing) the skills he or she has achieved. Although adult supervision remains essential, the entire neighborhood may become the child’s playground.
The availability of new indoor environments is also to be expected. Preschool classrooms usually have centers for different types of activities (e.g., creating art, listening to stories, playing games). In addition, community groups often sponsor a variety of indoor activities (e.g., preschool gymnastics, organized play programs) in which the child can take part.
Expanded environments offer children the opportunity to adapt play skills learned at home to the constraints of new spaces. For example, the child who climbs and slides down the stairs at home learns to climb a 6-foot ladder and slide down the slide in the neighborhood park. Parks and playgrounds also provide the child with new surfaces that challenge balance and equipment that offers intense vestibular experiences.
Cultural and socioeconomic differences can influence a child’s physical environment. Inner city parents frequently confine their children to the immediate household and forbid them to go outside after school, particularly to play. These protective strategies limit children’s exposure to dangerous neighborhood influences, but they also severely restrict the physical context available for play.41
Most preschool-aged children also enjoy spending time in quiet spaces. Children, especially those who demonstrate overreactivity to sensory input, may feel drawn to quiet, enclosed spaces (e.g., a space behind the couch, the safe haven of their bedrooms, a small tent in the corner of the playroom) (Figure 3-11). Quiet spaces can be organizing and calming after a day in a child care center. Other children who may have under-reacting sensory systems may seek stimulating environments that are full of activity, or they may create their own high activity in an otherwise quiet space.
When placed in new environments, children often respond by instinctively exploring the new spaces (e.g., hallways, cupboards, corners, furniture). Exploring the features of an environment can help orient children to the spaces that surround them, promote perceptual learning, and provide an understanding of the play possibilities in that environment.
Middle Childhood: Ages 6 to 10 Years
Although 6-year-old children continue to enjoy imaginative play, they begin increasingly to structure and organize their play. By the time a child is 7 or 8 years of age, structured games and organized play predominate (Box 3-9). Games with rules are the primary mode for physical and social play. Groups of children organize themselves, assign roles, and explain (or create) rules to guide the game they plan to play. The goal of the game now competes with the reward of interacting with peers, and children become fascinated with the rules that govern the games they play.
At 7 and 8 years of age, children do not understand that rules apply equally to everyone involved in the game, and they are often unable to place the rules of the game above the personal need to win.39 However, breaking the rules may incur the criticism of peers, who also acknowledge the importance of rules at this time. By 9 and 10 years of age, children are more conscientious about obeying rules. They also learn to negotiate the rules of a game and construct their own rules.
By 8 and 9 years, children become interested in sports, and parents are generally supportive of sports activities. Although a form of play, organized sports can assume a serious nature (i.e., intrinsic motivation and the internal sense of control are overridden by the external demands of practice and serious competition with peers). In addition to organized sports, physical play is a favorite interest, including climbing, rollerblading, skipping rope, and skateboarding (Figure 3-12).

FIGURE 3-12 Children seek opportunities to challenge their balance. By 9 and 10 years, postural stability and strength are sufficiently developed to maintain standing balance on a porch railing.
Interest in creating craft and art projects continues into middle childhood. During this time, the child shows an increased ability to organize, solve problems, and create from abstract materials. However, the completion of craft and art projects continues to require the support of adults to organize materials and identify steps. The final product, which is relatively unimportant to younger children, is now valued.
In middle childhood, children play in cooperative groups and value interaction with their peers. When friends come together, almost all activity is play and fun. Simply talking and joking become playful and entertaining. Children spend more than 40% of their waking hours with peers.24 In these peer groups, children learn to cooperate but also to compete.39 They are now interested in achievement through play; they recognize and accept an outside standard for success or failure and criteria for winning or losing. With competition in play comes risk taking and strategic thinking. Children who compete in sports and other activities exhibit courage to perform against an outside standard.85
Performance Skills
Sensory and Motor Skills: During the elementary school years, motor development continues to focus on the refining of previously acquired skills. With this refinement, hours of repetition of activities to attain mastery of common interests are observed. Children ride bicycles, scale fences, swim, skate, and jump rope (Figure 3-13). Although motor capabilities are highly varied for this age group, balance and coordination improve throughout the middle childhood years, providing children with the agility to dance and play sports with proficiency. Research indicates that children who struggle in physical skills have lower self-esteem and are very socially marginalized.69 Not only does self-esteem improve as children master physical skills, but peer acceptance improves as well.

FIGURE 3-13 Favorite play activities for all children include swimming, ball play, and outdoor sports.
Fine motor skills in middle childhood include efficient tool use (e.g., scissors, tweezers) and precise drawing skills. Children handle and manipulate materials (fold, sort, adhere, cut) with competency. The drawing skills of 8- and 9-year-old children demonstrate appropriate proportions and accuracy, and handwriting skills improve in speed and accuracy as children learn manuscript and then cursive writing. These improvements provide evidence of increased dexterity and coordination. Construction skills, manipulation, and abilities to use tools continue to generalize across performance areas, with increases in speed, strength, and precision.
Cognitive Skills: In middle childhood, concepts and relationships in the physical world are understood and applied. The child relates past events to future plans and comprehends how situations change over time. Thinking has become more flexible and abstract. The child has become a reasoning individual who can solve problems by understanding variables and weighing pertinent factors before making decisions. They now have a clear understanding of the difference between fantasy and reality and they choose to move from one to the other.
At younger ages, children could apply only one solution, and they often were stuck when the solution of choice did not work. By 8 and 9 years of age, however, they recognize that different solutions can be tried, and they arrive at answers through abstract reasoning rather than through concrete trial and error. At this age, children can also pay attention to more than one physical characteristic at a time and can systematically put elements together.
In play, children order objects by size or shape, demonstrating the ability to discriminate perceptual aspects of objects and to order them accurately. They also understand the relationship of the whole to the parts, and they imagine pieces as parts of a whole. With this understanding, they become more competent in organizing tasks and organizing time. Children 9 and 10 years of age can give instructions to others and tell stories in detail.
By middle childhood, children learn to combine tasks and routines into complex games and competitive sports. Because a number of rules are needed to play sports, such as baseball or hockey, the child understands the need to combine the rules into a complete game. To participate in the activity successfully, he or she also understands when rules apply and when rules can be negotiated.
Social Skills: Children 6 to 10 years of age form close friendships and “belong” to one or more peer groups that greatly influence their decisions, how they spend their time, and what they value. Florey and Greene explain, “In the beginning of middle childhood, friendships are characterized by sharing of interests. Toward the end of this period, children tend to organize around common values, commitment, loyalty, and mutual support” (p. 282).39
Children in middle childhood focus on meeting challenges in themselves as well as challenges presented by others. Children appreciate the recognition that comes with successful completion of assignments or projects. Comparison with peers is increasingly important during this time. If a child’s schoolwork is compared with the work of a more successful student, a negative evaluation can reduce his or her sense of mastery and may produce feelings of inferiority.
School-aged children seek independence of identity. They are not as egocentric as young children and demonstrate a more objective view of themselves. Children at this age have a definite subculture, or clique, that includes only certain friends. At this age, children are quick to criticize those who do not conform to the group esthetic. Therefore rejection by the child’s peers may result from a lack of conformity in dress or physical appearance. Children who have difficulty communicating or who do not know how to initiate relationships are less likely to have close friendships. Children who are socially able and positive are more accepted and have more close friendships.
During middle childhood, children become disinterested in adults, including their parents. The values of peers become significantly more important than those of adults. Data indicate that children between 7 and 10 years of age are highly compliant with and easily shift in the direction of their peers.28,39
The child’s progression from games with some structure and flexible rules to highly competitive games demonstrates progression in moral development. Early in the child’s thinking (before 7 years of age), rules are viewed as absolute, sacred, and unchangeable. Children 7 to 10 years old recognize that rules come from someone in authority, and they accept what this authority says. However, late in the elementary school years, children cast aside their beliefs in the absolute infallibility of rules, because they have gained the knowledge that people are the creators of rules. Questioning of the rules and the authority that makes them begins at this age.39
Contexts
Cultural Contexts: Expectations for children to work appear to vary across cultures. These expectations determine the timing and type of occupations children develop and the balance between work and play. In countries other than the United States and those of Europe, the typical age for children to assume work responsibilities is 5 to 7 years. In a study of 50 communities, children at 5 to 7 years are given responsibility for caring for younger children, for tending animals, and for carrying out household chores.90 In the United States, chores are rarely given to children younger than 8 or 9 years of age. Many American families do not expect children to take responsibility for chores until the age of 10 or 11. In contrast, Polynesian children develop household skills by 3 or 4 years, at which time they gather wood, sweep, or run errands to the store. In West Africa, children have duties and run errands when they are 3 years old. In Kenya, 8-year-old girls perform most of the housework.88
Mayan children are continuously at their parents’ side during work days. At early ages, they participate in work tasks, such as running errands and helping with cleanup. Bazyk et al. found that although Mayan children began work activities at a very early age, they embedded play in these chores.10 Children in Central Africa acquire work experience from toddler age, and by age 12 they can trap animals, kill game, make medicines, and garden.88 Ogunnaike and Houser examined the effects of participation in work activities and errands on cognitive performance in young Yoruban children.80 In Yoruba, young children are taught to be helpful, responsible, and respectful. Before age 5, Yoruban girls are taught to perform household chores such as washing, sweeping, cooking, and caring for their younger siblings. By middle childhood, the girls take full responsibility for these work roles. The number of errands a child was required to run and cognitive performance were significantly related, indicating that having children participate in work tasks at an early age may enhance cognitive competence.80
In the United States, most children and youth have very few opportunities to work with adults. Goldscheider and Waite estimated that children contribute about 15% of all labor in households.51 Rogoff believes that American children are missing valuable opportunities for learning and gaining self-satisfaction.88 In comparison with practices in societies outside the United States, the lack of work opportunities for American children limits their practice of skills important to their future and may delay their entry into adult work roles. Through experiences in school and guided participation in household work, children may develop work skills and also learn social rules and cultural values.65
Physical Contexts: In middle childhood, the child’s play environment is now large and complex; more activities take place in the neighborhood and at school. The school’s playground supports both social and physical play of small groups (or pairs) of children. Play occurs on ball fields and in community centers, amusement parks, and sports arenas. Organized activities are often sponsored by churches or by groups such as the Young Men’s Christian Association (YMCA). By middle childhood, children have the mobility skills to maneuver through all environments (e.g., rough terrain, busy city streets). The society of school-aged children dominates neighborhood streets and backyards, with bicycle races and spontaneous street hockey games. These children explore the woods and go on adventures in nearby parks to find areas unexplored by others. Although supervision by adults is still needed at times, intermittent supervision usually suffices.
Children spend many of their waking hours in school. Schools offer complex environments (e.g., playgrounds, computer rooms, libraries, classrooms, lunchrooms) with many social and learning opportunities.
SUMMARY
The development of occupational performance is influenced by many systems and variables in the individual child and in the environment. The various patterns observed in children provide insight into how and why a child follows a certain developmental trajectory. Sensory, motor, cognitive, and social skills support the child’s performance in play occupations. At the same time, a child’s activities are highly influenced by his or her cultural, social, and physical contexts. As an essential occupation of childhood, play provides a means of understanding and appreciating children’s performance and a means for enhancing functional performance when development is delayed. The ability to play is also an important outcome of occupational therapy, one that reflects the being of childhood.
REFERENCES
1. Adolf, K.E., Eppler, M.A., Gibson, E.J., Development of perception of affordances. Rovee-Collier, C., Lipsitt, L.P., eds. Advances in infancy research, Norwood, NJ, Ablex, 1993;Vol. 8:51–98.
2. American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process. 2nd ed. American Journal of Occupational Therapy. 2008;62:625–683.
3. Ayres, A.J. Sensory integration and the child. Los Angeles: Western Psychological Services, 1979.
4. Ayres, A.J. Sensory integration and the child: Understanding hidden sensory challenges. 25th anniversary edition. Los Angeles: Western Psychological Services, 2005.
5. Bandura, A. The self system in reciprocal determinism. American Psychologist. 1978;33:344–358.
6. Bandura, A. Perceived self-efficacy in cognitive development and functioning. Educational Psychologist. 1993;28:117–148.
7. Bandura, A. A social cognitive theory of personality. In: Pervin L., John O., eds. Handbook of personality. 2nd ed. New York: Guilford Press; 1999:154–197.
8. Bayley, N. Bayley Scales of Infant Development, 2nd ed. San Antonio: Psychological Corporation, 1993.
9. Bayley, N. Bayley Scales of Infant Development, 3rd ed. San Antonio: Psychological Corporation, 2005.
10. Bazyk, S., Stalnaker, D., Llerena, M., Ekelman, B., Bazyk, J. Play in Mayan children. American Journal of Occupational Therapy. 2003;57:273–283.
11. Bruner. Organization of early skilled action. Child Development. 1973;44:1–11.
12. Bushnell, E.W., Boudreau, J.P. Motor development and the mind: the potential role of motor abilities as a determinant of aspects of perceptual development. Child Development. 1993;64:1005–1021.
13. Case, R. Conceptual development in the child and the field: A personal view of the Piagetian legacy. In: Scholnick E., Nelson K., Gelman S., Miller P., eds. Conceptual development: Piaget’s legacy. Mahwah, NJ: Lawrence Erlbaum; 1999:23–51.
14. Case-Smith, J. Hand skill development in the context of infants’ play: Birth to 2 years. In: Hendersen A., Pehoski P., eds. Hand function in the child: Foundations for remediation. St. Louis: Mosby; 2006:117–142.
15. Case-Smith, J., Kuhaneck, H. Play preferences of typically developing children and children with developmental delays between ages 3 and 7 years. OTJR: Occupation, Participation and Health. 2008;28:19–29.
16. Cermak, S. Perceptual functions of the hand. In: Hendersen A., Pehoski P., eds. Hand function in the child: Foundations for remediation. St. Louis: Mosby; 2006:63–88.
17. Chan, S. Families with Asian roots. In: Lynch E.W., Hanson M.J., eds. Developing cross-cultural competence. 2nd ed. Baltimore: Brookes; 1998:251–354.
18. Chan, S. Families with Filipino roots. In: Lynch E.W., Hanson M.J., eds. Developing cross-cultural competence. 2nd ed. Baltimore: Brookes; 1998:355–408.
19. Chess, S., Thomas, A. The origins and evolution of behavior disorders: Infancy to early adult life. New York: Brunner/Mazel, 1984.
20. Chess, S., Thomas, A. Goodness of fit: Clinical applications from infancy through adult life. New York: Brunner/Mazel, 1999.
21. Cioni, G., Ferrari, F., Einspieler, C., Paolicelli, P., Barbiani, T., Prechtl, H.F. Comparison between the observation of spontaneous movements and neurologic examination in preterm infants. Journal of Pediatrics. 1997;130:704–711.
22. Clark, J. A dynamical systems perspective on the development of complex adaptive skill. In: Dent-Read C., Zukow-Goldring P., eds. Evolving explanations of development: Ecological approaches to organisms-environment systems. Washington, DC: American Psychological Association, 1997.
23. Cohen, L.B., Cashon, C.H. Infant perception and cognition. In: Lerner R.M., Easterbrooks M.A., Mistry J., eds. Handbook of psychology: Vol. 6. Developmental psychology. New York: John Wiley & Sons; 2003:65–90.
24. Cole, M., Cole, S. The development of children. New York: Scientific American Books, 1989.
25. Connolly, K., Dalgleish, M. The emergence of a tool-using skill in infancy. Developmental Psychology. 1989;25:894–912.
26. Connolly, K.J., Dalgleish, M. Individual patterns of tool use by infants. In: Kalverboer A.F., Hopkins B., Geuze R., eds. Motor development in early and later childhood: Longitudinal approaches. Cambridge: Cambridge University Press; 1993:174–204.
27. Corbetta, D., Mounoud, P. Early development of grasping and manipulation. In: Bard C., Fleury M., Hay L., eds. Development of eye-hand coordination across the life span. Columbia, SC: University of South Carolina Press, 1990.
28. Costanzo, P.R., Shaw, M.E. Conformity as a function of age level. Child Development. 1966;37:967–975.
29. Csikszentmihalyi, M., Rathunde, K. The development of the person: An experiential perspective on the ontogenesis of psychological complexity. In: Damon W., Lerner R.M., eds. Handbook of child psychology: Vol 1. Theoretical models of human development. 5th ed. New York: John Wiley & Sons; 1998:635–684.
30. Daunhauer, L.A., Coster, W.J., Tickle-Degen, L., Cermak, S.A. Effects of caregiver-child interactions on play occupations among young children institutionalized in Eastern Europe. American Journal of Occupational Therapy. 2007;61:429–440.
31. Dunst, C.J. Participation of young children with disabilities in community learning activities. In: Guralnick M.J., ed. Early childhood inclusion: Focus on change. Baltimore: Paul H. Brookes; 2001:307–333.
32. Dunst, C.J., Bruder, M.B., Trivette, C.M., Raab, M., McLean, M. Natural learning opportunities for infants, toddlers and preschoolers. Young Exceptional Children. 2001;4:18–25.
33. Easterbrooks, M.A., Biringen, Z. Mapping the terrain of emotional availability and attachment. Attachment and Human Development. 2000;2:123–129.
34. Ellison, P.H. The INFANIB: A reliable method for the neuromotor assessment of infants. Tucson, AZ: Therapy Skill Builders, 1994.
35. Erikson, E.H. Childhood and society, 2nd ed. New York: W.W. Norton, 1963.
36. Fagaard, J. The development of bimanual coordination. In: Bard C., Fleury M., Hay L., eds. Development of eye-hand coordination across the life span. Columbia, SC: University of South Carolina Press, 1990.
37. Feldman, D.H. Cognitive development in childhood. In: Lerner R.M., Easterbrooks M.A., Mistry J., eds. Handbook of psychology, Vol. 6. Developmental psychology. Hoboken, NJ: John Wiley & Sons, Inc; 2003:195–210.
38. Fitzgerald, H., Munn, T., Cabrera, N., Wong, M.M. Diversity in caregiving contexts. In: Lerner R.M., Easterbrooks M.A., Mistry J., eds. Handbook of psychology: Vol. 6. Developmental psychology. New York: John Wiley & Sons; 2003:135–169.
39. Florey, L.L., Greene, S. Play in middle childhood. In: Parham L.D., Fazio L., eds. Play in occupational therapy for children. 2nd ed. St. Louis: Mosby; 2008:279–300.
40. Folio, M.R., Fewell, R.R. Peabody Developmental Motor Scales, rev. ed. Austin, TX: Pro-Ed, 2000.
41. Garcia Coll, C., Magnuson, K. Cultural differences as sources of developmental vulnerabilities and resources. In: Shonkoff J.P., Meisels S.J., eds. Handbook of early childhood intervention. 2nd ed. Cambridge: Cambridge University Press; 2000:94–114.
42. Gesell, A. The embryology of behavior: The beginnings of the human mind. New York: Harper & Brothers, 1945.
43. Gesell, A., Amatruda, G. Developmental diagnosis, 2nd ed. New York: Harper & Row, 1947.
44. Gesell, A., Halverson, H.M., Thompson, H., Ilg, F.L., Castner, B.M., Ames, L.B., et al. The first five years of life. New York: Harper & Row, 1940.
45. Gesell, A., Ilg, F. Feeding behavior of infants. Philadelphia: Lippincott, 1937.
46. Gibson, E.J. Exploratory behavior in the development of perceiving, acting, and the acquiring of knowledge. Annual Reviews Psychology. 1988;39:1–42.
47. Gibson, E.J. Exploratory behavior in the development of perceiving, acting, and the acquiring of knowledge. In: Lipsitt L.P., Rovee-Collier C., eds. Advances in infancy. Norwood, NJ: Ablex; 1995:xxi–lxi.
48. Gibson, E.J. An ecological psychologist’s prolegomena for perceptual development: A functional approach. In: Dent-Read C., Zukow-Goldring P., eds. Evolving explanations of development: Ecological approaches to organisms-environment systems. Washington, DC: American Psychological Association, 1997.
49. Gibson, J.J. The ecological approach to visual perception. Boston: Houghton-Mifflin, 1979.
50. Gilfolye, E., Grady, A., Moore, J. Children adapt, 2nd ed. Thorofare, NJ: Slack, 1990.
51. Gottlieb, G. Synthesizing nature-nurture: Prenatal roots of instinctive behavior. Lawrence Erlbaum: Hillsdale, NJ, 1997.
52. Goldscheider, F., Waite, L. New families, no families? Los Angeles: University of California Press, 1991.
53. Granott, N. How microdevelopment creates macrodevelopment: Reiterated sequences, backward transitions, and the zone of current development. In: Granott N., Parziale J., eds. Microdevelopment: Transition processes in development and learning. Cambridge: Cambridge University Press; 2002:213–242.
54. Greenspan, G. Infancy and early childhood: The practice of clinical assessment and intervention with emotional and developmental challenges. New York: International Universities Press, 1990.
55. Greer, T., Lockman, J.J. Using writing instruments: Invariances in young children and adults. Child Development. 1998;69:888–902.
56. Henderson, A. Self care and hand skill. In Henderson A., Pehoski C., eds.: Hand function in the child, 2nd ed., St. Louis: Mosby, 2006.
57. Humphry, R. Young children’s occupations: Explicating the dynamics of developmental processes. American Journal of Occupational Therapy. 2002;56:172–179.
58. Humphry, R. Occupation and development: A contextual perspective. In: Crepeau E.B., Cohn E.S., Schell B.A.B., eds. Willard & Spackman’s occupational therapy. Philadelphia: Lippincott Williams & Wilkins; 2009:22–32.
59. Humphry, R., Wakeford, L. An occupation-centered discussion of development and implications for practice. American Journal of Occupational Therapy. 2006;60:258–268.
60. Illingworth, R.S. The diagnosis of cerebral palsy in the first year of life. Developmental Medicine and Child Neurology. 1966;8:178–194.
61. Illingworth, R.S. The development of the infant and young child. Edinburgh: Churchill Livingstone, 1984.
62. Jacobson, S.L., Wille, D.E. The influence of attachment pattern on developmental changes in peer interaction from the child to the preschool period. Child Development. 1986;57:338–347.
63. Knobloch, H., Pasamanick, B. Gesell & Amatruda’s developmental diagnosis, 3rd ed. New York: Harper & Row, 1974.
64. Knox, S. Development and current use of the Knox Preschool Play Scale. In: Parham L.D., Fazio L., eds. Play in occupational therapy for children. 2nd ed. St. Louis: Mosby; 2008:55–70.
65. Larson, E.A. Children’s work: The less-considered childhood occupation. American Journal of Occupational Therapy. 2004;58:369–379.
66. Lerner, R.M., Anderson, P.M., Balsano, A.B., Dowling, E.M., Bobek, D.L. Lerner R.M., Easterbrooks M.A., Mistry J., eds. Handbook of psychology, Vol. 6. Developmental psychology. John Wiley & Sons: New York, 2003:535–558.
67. Linder, T. Transdisciplinary play-based assessment, rev. ed. Baltimore: Brookes, 2008.
68. Luthar, S.S., Latendresse, S.J. Comparable “risks” at the socioeconomic status extremes: Preadoleescents’ perceptions of parenting. Development and Psychopathology. 2005;17:207–230.
69. Mandich, A., Polatajko, H., Rodger, S. Rites of passage: Understanding participation of children with developmental coordination disorder. Human Movement Science. 2003;22:583–595.
70. Mandler, J.M. A new perspective on cognitive development in infancy. American Scientist. 1990;78:236–243.
71. Mathiowetz, V., Haugen, J. Motor behavior research: Implications for therapeutic approaches to central nervous system dysfunction. American Journal of Occupational Therapy. 1994;48:733–745.
72. Mathiowetz, V., Haugen, J. Evaluation of motor behavior: Traditional and contemporary views. In: Trombly C.A., ed. Occupational therapy for physical dysfunction. 4th ed. Baltimore: Williams & Wilkins; 1995:157–186.
73. McCarty, M.E., Clifton, R.K., Collard, R.R. The beginnings of tool use by infants and toddlers. Infancy. 2001;2:233–256.
74. McGraw, M. The neuromuscular maturation of the human infant. New York: Macmillan, 1945.
75. Metzoff, A.N., Moore, M.K. Early imitation within a functional framework: The importance of person identity, movement, and development. Infant Behavior and Development. 1992;15:470–505.
76. Milani-Comparetti, A., Gidoni, E.A. Pattern analysis of motor development and its disorders. Developmental Medicine and Child Neurology. 1967;9:625–630.
77. Morelli, G.A., Rogoff, B., Oppenheim, D., Goldsmith, D. Cultural variation in infants’ sleeping arrangements: Questions of independence. Developmental Psychology. 1992;28:604–613.
78. Morrissey, T.W., Banghart, P. Family child care in the United States. Child Care & Early Education Research Connections, 2007. Retrieved June 2009 at, http://www.childcareresearch.org/location/12036.
79. National Institute of Child Health and Human Development (NICHD), Early Child Care Research Network. Characteristics and quality of child care for toddlers and preschoolers. Applied Development Science. 2000;4:116–135.
80. Ogunnaike, O.A., Houser, R.F. Yoruba toddlers’ engagement in errands and cognitive performance on the Yoruba Mental Subscale. International Journal of Behavioral Development. 2002;26:145–153.
81. Parham, L.D. Play and occupational therapy. In: Parham L.D., Fazio L., eds. Play in occupational therapy for children. St. Louis: Mosby; 2008:2–22.
82. Pehoski, C. Object manipulation in infants and children. In: Henderson A., Pehoski C., eds. Hand function in the child. St. Louis: Mosby; 2006:143–160.
83. Piaget, J. The origins of intelligence in children. New York: International Universities Press, 1952. [M. Cook, Trans.].
84. Piper, M.C., Darrah, J. Motor assessment of the developing infant. Philadelphia: W.B. Saunders, 1994.
85. Reilly M., ed. Play as exploratory learning. Beverly Hills, CA: Sage Publications, 1974.
86. Rochat, P. Object manipulation and exploration in 2- to 5-month-old infants. Developmental Psychology. 1989;25:871–884.
87. Rochat, P., Gibson, E.J. Early mouthing and grasping: Development and cross-modal responsiveness to soft and rigid objects in young infants. Canadian Psychology. 1985;26:452.
88. Rogoff, B. The cultural nature of human development. New York: Oxford University Press, 2003.
89. Rogoff, B., Mosier, C., Mistry, J., Goncu, A. Guided participation in cultural activity by toddlers and caregivers. Monographs of the Society for Research in Child Development. 1993;58:1–179.
90. Rogoff, B., Selless, M.J., Pinotta, S., Fox, N., White, S.H. Age of assignment of roles and responsibilities to children: A cross-cultural survey. Human Development. 1975;18:353–369.
91. Rosblad, B. Reaching and eye-hand coordination. In: Henderson A., Pehoski C., eds. Hand function in the child. St. Louis: Mosby; 2006:89–100.
92. Rubin, K. The Play Observation Scale. Ontario, Canada: University of Waterloo Press, 1984.
93. Rubin, K., Maioni, T.L., Hornung, M. Free play behaviors in middle-class and lower-class children: Parten and Piaget revisited. Child Development. 1976;47:414–419.
94. Ruff, H.A. The infant’s use of visual and haptic information in the perception and recognition of objects. Canadian Journal of Psychology. 1989;43:302–319.
95. Sharifzadeh, V.S. Families with Middle Eastern roots. In: Lynch E.W., Hanson M.J., eds. Developing cross-cultural competence. 2nd ed. Baltimore: Brookes; 1998:409–440.
96. Singer, D.G., Singer, J.L. The house of make-believe: Play and the developing imagination. Cambridge, MA: Harvard University Press, 1990.
97. Spencer, J.P., Corbetta, D., Buchanan, P., Clearfield, M., Ulrich, B., Schoner, G. Moving toward a grand theory of development: In memory of Esther Thelen. Child Development. 2006;77:1521–1538.
98. Stone, J.L., Church, J. Childhood and adolescence: A psychology of the growing person, 3rd ed. New York: Random House, 1973.
99. Takata, N. Play as a prescription. In: Reilly M., ed. Play as exploratory learning. Beverly Hills, CA: Sage Publications; 1974:209–246.
100. Thelen, E. Motor development: A new synthesis. American Psychologist. 1995;50:79–95.
101. Thelen, E. Self-organization in developmental processes: Can systems approaches work? In: Johnson M., Munakata Y., eds. Brain development and cognition: A reader. 2nd ed. Malden, MA: Blackwell Publishers; 2002:544–557.
102. Thelen, E., Corbetta, D., Kamm, K., Spencer, J., Schneider, K., Zernicke, R.F. The transition to reaching: Mapping intention and intrinsic dynamics. Child Development. 1993;64:1058–1098.
103. Thelen, E., Corbetta, D., Spencer, J.P. The development of reaching during the first year. The role of movement speed. Journal of Experimental Psychology: Human Perception and Performance. 1996;22:1059–1076.
104. Thomas, A., Chess, S. Temperament and development. New York: Brunner/Mazel, 1977.
105. Thompson, R.A., Easterbrooks, M.A., Padilla-Walker, L.M. Social and emotional development in infancy. In: Lerner R.M., Easterbrooks M.A., Mistry J., eds. Handbook of psychology: Vol. 6. Developmental psychology. New York: John Wiley & Sons; 2003:91–112.
106. Touwen, B.C.L. Examination of the child with minor neurological dysfunction: Clinics in Development Medicine 71, 1979.
107. Vanderbilt-Adriance, E., Shaw, D.S. Conceptualizing and re-evaluating resilience across levels of risk, time, and domains of competence. Clinical Child and Family Psychology Review. 2008;11:30–58.
108. von Hofsten, C. Studying the development of goal-directed behaviour. In: Kalverboer A.F., Hopkins B., Geuze R., eds. Motor development in early and later childhood: Longitudinal approaches. New York: Cambridge Press, 1993.
109. Vygotsky, L.S. Mind in society: The development of higher psychological processes. Cambridge, MA: Harvard University Press, 1978.
110. Werner, E.E. Protective factors and individual resilience. In: Shonkoff J.P., Meisels S.J., eds. Handbook of early childhood intervention. Cambridge: Cambridge University Press; 2000:115–134.
111. Werner, E.E., Smith, R.S. Overcoming the odds: High risk children from birth to adulthood. Ithaca, NY: Cornell University Press, 1992.
112. Whiting, B., Edwards, C.P. A cross-cultural analysis of sex differences in the behavior of children aged 3 through 11. In: Handel G., ed. Childhood socialization. Cambridge, MA: Harvard University Press; 1988:281–297.
113. Willis, W. Families with African American roots. In: Lynch E.W., Hanson M.J., eds. Developing cross-cultural competence. 2nd ed. Baltimore: Brookes; 1998:165–208.
114. Wong, S., Chan, K., Wong, V., Wong, W. Use of chopsticks in Chinese children. Child: Care, Health, and Development. 2002;28:157–163.
115. Youngblade, L.M., Belsky, J. Parent-child antecedents of 5-year-olds’ close friendships: A longitudinal analysis. Development Psychology. 1992;28:700–713.
116. Ziviani, J., Rodger, S. Environmental influences on children’s participation. In: Rodger S., Ziviani J., eds. Occupational therapy with children: Understanding children’s occupations and enabling participation. Oxford, UK: Blackwell Publishing, Inc; 2006:41–66.
117. Zuniga, M.E. Families with Latino roots. In: Lynch E.W., Hanson M.J., eds. Developing cross-cultural competence. 2nd ed. Baltimore: Brookes; 1998:209–250.