Foundations for Occupational Therapy Practice with Children
1 Explain the history and evolution of theories pertaining to child development.
2 Define the term occupation and describe the study of occupation with emphasis placed on the occupations of children.
3 Explain what is meant by person–environment congruence.
4 Articulate the concepts and principles that define family-centered services.
5 Explain the developmental and learning theories of the early and middle 1900s, which provided the foundation for occupational therapy theories.
6 Explain and apply cognitive models of practice.
7 Use a dynamic systems approach to explain how children develop motor skills.
8 Explain how the person-environment-occupation model is used with other specific models of practice in occupational therapy intervention with children.
9 Describe and apply learning theories and approaches.
10 Define and explain the appropriate use of and evidence for neurodevelopmental and sensory integration therapy approaches.
11 Describe strategies that exemplify each practice model using client examples.
12 Compare and contrast intervention activities derived from different theoretical approaches and practice models.
Occupational therapists have developed and used theory as the basis for professional practice for many years. Early developers of occupational therapy focused on the theories of occupation and the use of time.124,172 As stated by Meyer,
Our conception of man is that of an organism that maintains and balances itself in the world of reality and actuality by being in active life and active use, i.e., using and living and acting its time in harmony with its own nature and the nature about it. It is the use that we make of ourselves that gives the ultimate stamp to our [being] (p. 64).124
Meyer posited that humans maintain rhythms of work, play, rest, and sleep that need to be balanced and that “the only way to attain balance in all this is actual doing, actual practice” (p. 64).124 Current practices build on many of the original concepts of the profession’s founders. Meyer’s words are echoed by those of Mandich and Rodger, who explain that through “doing and participation in everyday occupations, children learn and master new skills” (p. 115).117 Furthermore, social engagement (doing with family and friends) enables children to develop a sense of belonging and self-esteem that contributes to health and well-being. Since the time of Meyer, occupational therapists have continued to develop models of practice based on an understanding of humans as occupational beings. They have also integrated the theories and science of psychologists, neuroscientists, and other disciplines into their practices. This chapter describes current occupational theories, models of practice that reflect those theories, and concepts from other disciplines that support occupational therapy practices.
This chapter begins with a brief overview of the historical and current perspectives on the theories that underlie current service provision: development, occupation, and environment. Foundational theories for occupational therapy practice are discussed next. Then, an overall framework for occupational therapy practice with children, based on a person-environment-occupation (PEO) perspective, is presented, followed by descriptions of current models of practice and the interventions that exemplify those models. Finally, these models of practice are applied to specific practice scenarios, demonstrating the interconnection of theories, models of practice, assessment, and interventions.
OCCUPATIONAL THERAPY PRACTICE WITH CHILDREN
In one version of an ideal childhood, summer is remembered as a time when friends spent the entire day playing outside. Children moved from activity to activity as a group, enjoying one another’s company and participating in a variety of play activities. Life was about running with the dog, playing tag in the woods, climbing trees, playing ball in the alley, and pretending to be a superhero or a princess. Adults often have fond memories of their childhood days. As children, however, they did not think about the reasons they engaged in play activities or why particular activities were enjoyable—it was just fun! Occupational therapists, however, have a different perspective on play.
Play is considered a primary occupation of childhood. Multiple, interrelated factors within the child, family, and environment influence a child’s ability to engage in play, and a child’s play actions become a window for understanding how the child interacts with his environment. Occupational therapists understand that play is essential for development, and they study the concepts and assumptions that underlie the theories of play. It is through play that children learn to adapt to their environments and to develop competencies.155 By playing, children develop skills that they will later employ in work settings. Children with disabilities face challenges to play. Children with disabilities may exhibit less playfulness (see Chapter 18), demonstrate lower levels of physical play,151 and require more support to play.22,175 Play is also a means to the development of other functions (e.g., motor, social, cognitive, and self-care skills).142 Play activities are generally central to an occupational therapy session because these activities engage and motivate the child, elevating his or her focus and performance.
Parham explains that play “is an active ingredient of a healthy lifestyle” and prepares a person for work.147,154 As a child undergoes transition to adolescence and adulthood, this primary occupation of play evolves into the occupations of adulthood—work, activities of daily living, and leisure.
Play theories are but one set of theories applied by occupational therapists, who use theories in a variety of ways as a foundation to their reasoning. Therapists make decisions and select strategies using their synthesized knowledge of practice theories, including evidence for those theories, their own experiences, and their perceptions of the client’s priorities. Through the use of theory, assessment, and professional reasoning, occupational therapists hypothesize and then develop interventions to improve the occupational performance of children.
For purposes of this chapter, a theory is defined as a set of facts, concepts, and assumptions that together are used to describe, explain, or predict phenomena. Using theory, occupational therapists organize knowledge, understand observations, and explain or predict occupational function and dysfunction. Theories, therefore, provide a guide or rationale for occupational therapy intervention. Theories form the foundation for models of practice that guide the day-to-day delivery of occupational therapy services. A model of practice (also called a frame of reference) is the practical expression of theory and provides therapists with specific methods and guidelines for occupational therapy intervention. Models of practice draw from one or more theories and use concepts and assumptions to delineate the specific details of an occupational therapy practice, including who receives intervention, what intervention strategies are used, and when and where intervention is provided. The model of practice a practitioner applies can define the evaluations used, the intervention focus and strategies, and expected outcomes. It is the responsibility of the profession to research the theories and models of practice that are core to its practice; this chapter also explains the role of evidence-based practice in the development and application of theory-based models of practice.
Concepts Influencing Occupational Therapy Practice with Children
Perspectives on development and occupation have changed over the past century with changes in our knowledge about children, the factors affecting their development, and their basic need for engagement in purposeful tasks and activities. Developmental theories focus on explaining the processes by which infants mature and gain skills to become fully functioning adults. At the core of developmental theories is an explanation of the relationship between human biologic capacity and maturation and the influence of the environment on the behavior and performance of the individual. In fact, developmental theories tend to be distinguished from each other by the relative weight given to these two factors, nature or nurture, or by the emphasis on a particular aspect of human biologic function or environment. The theories of Gesell emphasized the genetic and biologic determinants of development; however, more recent theories (e.g., Piagetian theories) focus on interaction of biologic and environmental determinants of behavior.70 In current times, developmental theorists generally agree that human development is both the process and the product of biologic maturation and environmental experiences.
Development may be defined as the sequential changes in function that occur with maturation of the individual or species. These sequential changes should be differentiated from the concept of growth, which refers to maturational changes that are physically measurable. In the past, different dimensions of development have been emphasized. For example, longitudinal development focuses on the stages of development, whereas hierarchical development focuses on the prerequisite skills needed for higher-level skills. Evolving views and theories of development place less emphasis on the stages and components of development and more on the person as a whole and his or her development in relation to environment, roles, and occupations.84 The emerging theories of person–environment relations and complex systems have influenced these changes. Developmental theories are further explained later in the chapter.
Participation in Occupations
Throughout the 1920s and into the 1930s, the focus of occupational therapy was the development of the idea of occupation as a cure for disease and disability. The occupations best suited to cure specific medical problems were identified. Dunton led an effort to analyze occupations systematically.60 Occupational therapists used the principles of graded, purposeful activity and a balance of work, rest, and play as the basis for treatment methods.122,172
In the 1940s, changes in the medical arena (e.g., the discovery of antibiotics and the advancement of specific medical and surgical techniques) had a tremendous influence on the way in which occupational therapists used occupation in treatment. The development of specific techniques increased, and more focus was placed on programs addressing activities of daily living. Occupational therapy treatment focused on the prescription of activities with specific aims.87 For example, the flexion-extension-pronation-supination (FEPS) loom was developed to ensure that targeted ranges of movement were achieved. As a result of these changes, treatment became “medicalized.” In other words, the focus of occupational therapy became a series of technical activities rather than purposeful occupation. The influence of the medical model on the profession dominated for three decades and remains a predominant influence today.
As the 1960s ended, occupational therapists were increasingly uncomfortable with the technical focus of their profession. There was a call for more emphasis on the development of theory and a renewed interest in the roots of the profession: occupation.203 During this time, Reilly described a theory of occupational behavior in which the individual strives to develop skills and competencies directed toward mastery and achievement.153,156 Work and play were viewed as the contexts in which these skills and competencies developed. Fidler and Fidler focused on the importance of purposeful activity, or doing, in the development of self and the prevention of dysfunction.65 Kielhofner and Burke, building on Reilly’s work, described a model of human occupation that incorporated a systems theoretical view of the nature of occupation.91 This model expanded the understanding of life roles and the powerful influence they have on daily life and health.
In the past 20 years, a specific academic discipline called occupational science became a basis of occupational therapy.204 Study of the human as an occupational being is essential to an understanding of the complexity of engagement in occupation and the relationship between occupation and human health. As noted by Parham, “A full understanding of occupation requires the integration of knowledge from many disciplines, such as philosophy, biology, psychology, sociology, and anthropology” (p. 25).142 Wilcock emphasized occupation as purposeful activity and explained that humans need to use time in a purposeful way in order to develop and flourish.195
As the study of occupation has developed, occupational therapy scholars have proposed definitions of occupation. Clark and colleagues defined occupations as “chunks of daily activity that can be named in the lexicon of the culture” (p. 301).36 Christiansen, Clark, Kielhofner, and Rogers defined occupation as the “ordinary and familiar things that people do every day” (p. 1015).34 The definition adopted by the Canadian Association of Occupational Therapists (CAOT) states that “occupation refers to a group of activities and tasks of everyday life, named, organized, and given value and meaning by individuals and a culture” (p. 34).30
Each definition refers to daily activities or “chunks” of activity. Because occupation references daily activity, it is often thought of as simple; that is, the basic activities that people perform each day to look after themselves, to be productive, and to enjoy life. The definition of occupation becomes more complex with the inclusion of its meaning or purpose. The meaning of an occupation for an individual or the value of an occupation determined by a culture begins to show the many layers of occupation and the central relationship of occupation to the human experience.
Participation in occupations meets a basic human need.30 Dunton expressed his belief that occupation is as necessary to life as food and drink.60 Occupation also is an important determinant of health. Health can be strongly influenced by a person’s engagement in meaningful occupations, and conversely, the absence of meaningful occupation can have dire health consequences.196 Occupation serves as a means of organizing time, space, and materials. Patterns, habits, and roles evolve through the organization of occupation.90 Occupations change over the lifespan (as do patterns of time use), representing occupational development.
Play is a key area of occupational focus in practice with children. Chapter 18 describes occupational therapy perspectives on play. Most of the focus in the occupational therapy literature has been on play as a means and an end: as a therapeutic medium (a means to developmental change) and as an indication of developmental level (an outcome of intervention).142 Therefore, play elicits more than enjoyment; it is also a catalyst to the development of motor or cognitive skills. In their survey of pediatric occupational therapists, Couch, Deitz, and Kanny found that pediatric occupational therapists most often use play in therapy as a medium for developing both the skills underlying function (e.g., understanding cause-and-effect relationships, exploring an object by manipulating it) and an understanding of the rules that guide behavior (e.g., taking turns).42 Occupational therapists often observe children’s play and play with them to determine their level of performance and to analyze their performance (Figure 2-1).104 Less often, but probably more importantly, therapists view play as a priority outcome of interest, the end rather than the means. Parham suggested that therapists must understand that “play is a legitimate end in itself because it is a critical element of the human experience” (p. 24).142 Play is therefore a quality-of-life issue that promotes health and well-being.

In a similar way, occupation has a dual role in the profession, as both the focus of intervention and the medium through which occupational therapists often intervene. For example, a child may be struggling at school to successfully fulfill his role as a student because he has Asperger’s syndrome. The student struggles with his academic occupations because he is anxious and overaroused. His social participation is limited because he has limited ability to read the social cues of his peers. The occupational therapist evaluates the school activities in which this child is expected to participate and determines the personal and environmental factors that are influencing the child’s performance. These occupations become the focus of intervention; for example, the occupational therapist helps the teacher make accommodations to the classroom environment to decrease the student’s overarousal and improve his concentration in class. The occupational therapist also helps the student interpret social cues and gestures. The therapist models and instructs the student in appropriate social responses and creates opportunities for him to interact with peers with therapist support. Scaffolding the child’s participation in social activities with peers at school is likely to develop skills that generalize to other opportunities for social participation. This brief example illustrates intervention principles that enable children’s participation in everyday occupations (Box 2-1).96
The goal of an occupation-based model of practice is the child’s achievement of optimal occupational performance. What do professionals know about the occupational performance of children with special needs? According to the National Health Interview Survey of 1992 to 1994, 6.5% of children in the United States with disabilities are limited to some degree in their participation in daily activities.135 The study investigators reported that children with physical disabilities are “two to three times more likely to be unable to perform their usual activities than children with other conditions (e.g., asthma)” (p. 612).135 Children with special needs also have lower rates of participation in ordinary daily activities.173 Researchers have documented that children with disabilities are more restricted in active recreation and community socialization activities.16 Specifically, Bedell and Dumas found that children with acquired brain injury were most restricted in participating in structured community events, managing daily routines, and socializing with peers and they were least restricted in physical mobility.17
Australian studies113 and Canadian studies101 have found an inverse relationship in children with disabilities between amount of physical activity and age, with a significant decline in active leisure participation from childhood to adolescence. Although healthy children are less physically active as adolescents, they continue to participate in a wide range of leisure activities. In contrast, adolescents with disabilities engage in fewer leisure and social activities, and their activities tend to be more often home-based than community-based.168 See Chapter 4 for a discussion of adolescent participation.
In their systematic review of studies of leisure activities in children and youth with physical disabilities, Shikako-Thomas et al. found that children with disabilities participate more in informal activities (e.g., those activities that require little or no planning and are often self-initiated [reading, playing with toys]) than in formal activities (e.g., those with a formally designated coach or instructor [music or art lessons, organized sports]).168
Both intrinsic (personal) and environmental (family and community) factors influence the diversity of activities and the intensity of participation. The intrinsic factors include motor function,140 personality, social skills, age, and gender. Girls tend to participate more in arts and social activities, and boys participate more in group activities involving physical activity and sports.61,168 Family support can have a positive or negative effect. Children’s activities may be restricted by family time constraints, financial burden, and lack of supportive mechanisms (e.g., babysitting).101 Participation for children with disabilities is positively influenced by high levels of family cohesion, high incomes, strong family coping skills, and low levels of stress.101,168 Community barriers to children’s participation include barriers to physical access, lack of programming, and negative attitudes. Clearly, encouraging participation in the typical activities of childhood needs to be the major focus of pediatric occupational therapy.
Environment
Human ecology is the study of human beings and their relationships with their environments. Environments are the contexts and situations that occur outside individuals and elicit responses from them, including personal, social, institutional, and physical factors. Environmental factors can facilitate or limit engagement in occupation. A concept prevalent in the human development literature and more recently in health care is person–environment congruence, or environmental fit, which is described as the congruence between individuals and their environments.176
Over the past two decades, occupational therapists have stressed the importance of the interaction between individual and environment. Specific models of practice have been developed with a focus on environment.57,99 Systems theory, emphasizing the interdependent relationship between individual and environment, forms the basis for concepts that define occupational therapy and models of practice. Primary models of practice address the environment in terms of its cultural, social, institutional, and physical dimensions and the transactional relationship between people and the environments in which they live, work, and play.158,204
Psychologists who created theories and models about the relationship between humans and their environments that have influenced occupational therapy include Bronfenbrenner,25 E. Gibson,71 and J. Gibson.72 Bronfenbrenner, with a background in developmental psychology, studied how the child’s social and cultural environments influenced development.25 He believed that an interdependent relationship exists between a person and his or her social and cultural environments. Different levels of social support and social interactions surround the individual, including informal (e.g., family and friends) and formal (e.g., occupational therapists and teachers). Levels of the environment are defined by their proximity to the individual; that is, family is most important, then friends and extended family, and then the community and society. Children interact with and are influenced by all levels of the social environment. Changes at any level of the environment influence a person’s behavior. Throughout his or her life, a person constantly adapts to and influences changes in his or her social environments.
According to Bronfenbrenner’s theories of social development, occupational therapists are part of a person’s social environment.25 These theories help the therapist understand lifespan changes in clients in the context of their social settings. The interdependence between a person and the social environment helps therapists to expand intervention strategies to include families and communities.
Ecologic psychologists E. Gibson and J. Gibson considered the interdependence of a person with his or her environment to be an explanation of perceptual development. E. Gibson understood that manipulative play had a key role in the infant’s cognitive development.71 She believed that the child’s intrinsically motivated exploratory actions lead to perceptual, motor, and cognitive development through the concept of affordance. An affordance is a quality of an object or an environment that allows an individual to perform an action. Action and perception are tightly linked: the child’s first actions are to gather new information about the environment and those actions form the basis for perceptual development (the child’s understanding of the environment). “As new action systems mature, new affordances open up and new experiments on the world can be undertaken” (p. 7).71 As explained by E. Gibson:
The young organism grows up in the environment (both physical and social) in which his species evolved, one that imposes demands on his actions for his individual survival. To accommodate to his world, he must detect the information for these actions—that is, perceive the affordances it holds. How does the infant creature manage this accomplishment? … I think evolution has provided him with action systems and sensory systems that equip him to discover what the world is all about. He is “programmed” or motivated to use these systems, first by exploring the accessible surround, then acting on it … extending his explorations further. The exploratory systems emerge in an orderly way that permits an ever-spiraling path of discovery. The observations made possible via both exploratory and performatory actions provide the material for his knowledge of the world—a knowledge that does not cease expanding, whose end (if there is an end) is understanding (p. 37).71
Successful adaptation to the environment occurs when a person matches his or her activities to the affordances of the environment or when the person modifies the environment to ensure successful completion of an activity.
The Gibsons’ theories emphasize the importance of understanding a child’s development in the context of daily surroundings and activities. Occupational therapists are encouraged to provide activities (based on their understanding of the activity’s inherent affordances) that allow a child to explore and learn about the environment, enabling achievement of the child’s goals. Figure 2-2 demonstrates an infant’s motivation to explore.

Risk and Resilience
Several theories and research programs have been developed to explain the ways the environment influences the developmental outcomes of children and adolescents. Most of this work focuses on the participation of children and youth in everyday activities and on factors that either place children and adolescents at risk for poor outcomes or help them achieve optimal outcomes. For example, psychologist Emmy Werner studied the people of Kauai for more than 40 years. Her research indicated that participation in extracurricular activities plays an important role in the lives of resilient adolescents, especially when they participate in cooperative activities.192
Resilience can be defined as the characteristic of an individual who achieves a positive outcome in the context of risk, or factors known to be associated with negative outcomes. Research on risk and resilience has attempted to explain why some children have better outcomes than others who were raised in similar circumstances. The study of resilience has implications for increasing understanding of child development and for developing new interventions to improve outcomes for children at risk. When the concept of resilience was first studied, it was believed to be a stable personality characteristic, such as temperament or IQ. If resilience were an internal, stable characteristic, it would explain why one child did better than another in a particular environment. Currently, researchers understand resilience to be a dynamic process that is refined over time through ongoing transactions between a child and the environment.110
What are the risk factors for children who receive occupational therapy? Often the disability is not a primary risk; however, it can add to cumulative risk when the family has socioeconomic disadvantage, negative parental relationships, parental mental illness or physical illness, and lack of extended family support. Emerging evidence indicates that it is the total number of risk factors to which a child is exposed and the resources available to promote resilience for that child that ultimately are predictive of the child’s vulnerability to future adverse events and developmental outcomes.62,163
Protective factors are defined as characteristics of the child, family, and wider environment that reduce the negative effect of adversity on the child.120 These protective factors may be specific to the risk factor; for example, having warm and loving parents is a protective factor in early childhood, but may not serve as a protective factor when the child become an adolescent and is more influenced by peers and the teen culture. Researchers such as Rutter162 and Garmezy68 have identified general protective factors related to the child, the family milieu, and the social environment. Understanding these general protective factors may be helpful in designing interventions for at-risk children. Child protective factors include strong self-esteem and positive communication skills.68,192,193 Other child attributes that are associated with positive outcomes include intelligence, emotion regulation, temperament, coping strategies, and attention.184 Children who can effectively process information and problem-solve can use these abilities in adverse situations. Children who can regulate their emotions can monitor and modify the intensity and duration of their emotional reactions, enabling them to better function at school and in social relationships. An easygoing temperament is also a protective factor because it may evoke more positive attention from adults. Coping skills are also important because children with strong coping skills can moderate the impact of a difficult situation.
Essential resources that lead to resilience in the child are family resources such as love, nurturance, and a sense of safety and security. These must be accompanied by material resources such as nutrition and shelter.184 Attributes of the family that influence positive outcomes include family cohesion and harmony.68 Researchers have shown that a high-quality relationship with at least one parent, characterized by high levels of warmth and openness and low levels of conflict, is associated with positive outcomes across level of risk and stages of development.109
Protective factors in the community also contribute to the child’s development. Neighborhood quality, youth community organizations, quality of school programs and after-school activities can all influence a child’s ability to cope with risk factors and overcome adversity.184 Attributes of the social environment that promote resilience include extended social support and availability of external resources.68 Environmental factors, such as family-centered service delivery, acceptance of community attitudes, supportive home environments, and mentoring relationships with adults, have been shown to have a positive influence on child development.157,189,193
Family-Centered Service
During the past 20 years, families of children with disabilities have increased their role in determining and implementing services for their children. Families have been leaders in promoting family-centered service, a philosophy of service provision that emphasizes the central role of families in making decisions about the care their children receive. Challenged by the changes in the health services field and an increased demand by consumers for involvement in the services they receive, health care providers have made great strides in implementing family-centered service.
The term family-centered service arose from early intervention programs. Three important concepts define family-centered service: (1) parents know their children best and want the best for their children; (2) families are different and unique; and (3) optimal child functioning occurs in a supportive family and community context. Chapter 5 explains the rationale for and application of family-centered practice.
In family-centered service the family’s right to make autonomous decisions is honored. The relationship between the family and professionals is a partnership in which the family defines the priorities for intervention and, with the service providers, helps direct the intervention process.59 In working with families, service providers emphasize education to enable parents to make informed choices about the therapeutic needs of their child. Comprehensive education about services and community resources can help families understand the disability, acquire tools to manage behavior, and develop strategies for obtaining community resources. In family-centered practice intervention is based on the family’s visions and values; service providers recognize their own values and do not impose them on the family. The family’s roles and interests, the environments in which the family members live, and the family’s culture make up the context for service provision. Individualization of both the assessment and intervention processes is essential to family centeredness. Intervention is viewed as a dynamic process in which clients and parents work together as partners to define the therapeutic needs of the child with a disability. Services are designed to fit the needs of the family, rather than to force the family to fit the needs of the service providers or the intervention policies already in place. DeGrace explains that occupational therapy intervention needs to fit into a family daily routine because how a family participates in daily routines “defines who that family is and plays a key role in determining its health” (p. 348).50 Because each family is unique, practitioners need to ask about and learn how each family defines their routines, habits, and values, and to adapt their services to this family-constructed definition.
Research has demonstrated that parents feel more positive about their roles when service providers solicit and value parental participation. Increasing evidence in the literature indicates that interdisciplinary, family-centered service for children with disabilities leads to increased family satisfaction and may lead to greater functional improvement in children with disabilities.114,161 Parents are less likely to act on behalf of their child when practitioners are unresponsive to the family’s needs, are paternalistic, or fail to recognize and accept family decisions.58
Family-centered practice is characterized by appreciation and valuing of the family’s concerns and priorities, family support, and family education. Therapists who practice family-centered care seek information about how the disability impacts family occupations and what occupations are important to the family.51 Other examples of family-centered practice include helping families find social supports and network with other families19 and supporting families in gathering needed resources.77
The findings of a recent survey completed by 494 parents and 324 service providers from children’s rehabilitation centers indicate that parental satisfaction with service is primarily determined by the family-centered culture of the organization and by parental perceptions of family-centered service.100 Families’ satisfaction with services also decreases feelings of distress and depression and improves feeling of wellbeing.92 Occupational therapists who work with children enhance the effectiveness of their services when they practice from a family-centered perspective.
World Health Organization International Classification of Functioning, Disability, and Health
The World Health Organization (WHO) International Classification system, which is used in the broad rehabilitation and disability arena, influenced the structure of the Occupational Therapy Practice Framework2 and has been used to guide the structure of occupational therapy evaluation. The International Classification of Impairments, Disabilities, and Handicaps (ICIDH) was first developed and published in 1980.201 The revised classification system is titled the International Classification of Functioning, Disability, and Health (ICF).202 The ICF views human functioning at three levels: the body (structure and function), the person (activities), and society (participation). It also includes the domain of environmental factors, which can have a significant influence on a person’s functioning and health. The ICF model of functioning, disability, and health depicts the dynamic interaction between a person and his or her environment at all levels of functioning. A recent extension of the ICF, the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) has been developed to address the unique concerns of developing children.107 Recently developed measures align with the ICF and enable practitioners to assess children at multiple levels. The School Function Assessment is an example of scale that rates function at two levels, activities and participation.41 The American Occupational Therapy Association (AOTA) has acknowledged the strong connection between its practice framework and the ICF by establishing the domain of the profession as “supporting health and participation in life through engagement in occupation” (pp. 626-627).2
FOUNDATIONAL THEORIES
Foundational theories form the basis of occupational therapy intervention approaches. These theories come from many fields of study, ranging from the biologic sciences to social sciences to humanities. Occupational therapists draw from a wide range of foundational theories to explain occupational performance. Most theories used by occupational therapists who work in pediatrics are concerned with change. Such theoretical perspectives complement the therapist’s view of human development as growth that occurs over time in the function of an individual or a species. Considering the complex nature of the PEO perspective and the transactions involved in occupational performance, a number of foundational theories are relevant. This section reviews the theories most commonly used by occupational therapists who work with children and adolescents with disabilities.
Developmental Theories
Developmental theories explain and describe the components of a person as they relate to occupational performance. Different theorists have focused on particular components of the individual in an effort to explain developmental function and dysfunction. The most common theories used by occupational therapists are presented.
Piaget and Cognitive Development
Jean Piaget was concerned with the developmental adaptation of the individual in response to ongoing environmental experiences.145 He defined adaptation as the child’s ability to adjust to change to fit into his or her environment, and he examined adaptation through the child’s relationships with human and nonhuman objects and through time and space. Piaget144 introduced the idea that children are intrinsically motivated to learn from their surroundings and that they act on, rather than simply react to, their environment.95 Piaget used the terms cognitive structures, or schema, to describe the way in which children represent objects, events, and relationships in their minds. Piaget viewed every interaction as an opportunity either to assimilate new knowledge into existing structures or to adapt existing structures to accommodate new information. Accommodation is new learning, and it is believed to be the way that the cognitive progress is made. Piaget’s developmental stages have been the focus of research and critique; however, his descriptions of the gradual accumulation of knowledge in specific content areas remain valid concepts in child development.
Piaget believed the child organizes his experiences into mental schemes (concepts) through mental operations. Operations may be defined as the cognitive methods used by the child to organize his or her schemes and experiences to direct his or her actions. The totality of operational schemes available to the child at any given time constitutes the adapted intelligence, or cognitive competence, of the child.
Piaget believed that an invariant, hierarchical development of cognition proceeded from the simple to the complex, from the concrete to the abstract, and from personal to worldly concerns. He specified four maturational levels or periods of cognitive function: sensorimotor, preoperational, concrete operational, and formal operational.37,67 He believed that this sequence of development leads to the cognitive maturity of adulthood. The culmination of these levels is a person with values, goals, and plans and an understanding of his or her purpose in society. In current times, most child researchers agree that the child is an active learner, but do not view development in discrete stages.
An understanding of Piaget’s theory is important to occupational therapists who plan programs for children. Regardless of the therapeutic approach used in treatment, the therapist interacts with a thinking child who is continually learning from his environment. It is essential that the selection and structure of an activity be in accordance with the operational skills and concepts of the child.
The primary focus of Piaget’s concept is an explanation of cognitive learning, but Schmidt developed the idea further in the area of motor learning.167 He proposed that motor schemas are formed as combinations of (1) the initial conditions of the movement, (2) the specific parameters used to create it, (3) the knowledge of the results in the environment, and (4) the sensory consequences of the movement. Through repeated experiences, the child abstracts relationships among these four features and is considered to have learned a new movement.
Vygotsky and the Zone of Proximal Development
Vygotsky viewed human development as historically situated and culturally determined.194 The child develops by internalizing the social interactions that he experiences. Vygotsky was primarily interested in speech and language development; however, his concepts have important applications to child development across domains. Like his predecessors (e.g., Gesell and Piaget) Vygotsky understood that genetics has unequivocal influence on psychological development. However, he recognized that psychological function could only be explained by considering the role of social interaction. Social interaction has a fundamental influence on the child’s development of high mental functions. Vygotsky explained that a child’s cognitive processing first requires the assistance of another being within a social interaction before the child can mentally process on his own. Therefore, cognitive processing is a social process before it is an internal process and a child’s development and learning are critically dependent on social interaction. Vygotsky defined a “zone of proximal development” to explain how learning occurs through social interaction. The zone of proximal development is “the distance between the actual developmental level as determined by independent problem solving and the level of potential development as determined through problem solving under adult guidance or collaboration with more capable peers” (p. 86).188 What a child can achieve and learn with the assistance of another is the zone of proximal development and defines the area in which adults can work with the child to promote his development and independence in a particular skill.
When an adult and a child experience an activity together, they interpret the objects and events differently. Adults use language to help the child redefine the situation so that adult and child have a shared definition. When a learning opportunity is created that provides an optimal balance between the child’s existing skills and the challenge of the task, the adult can model language and behavior that will help the child progress. Vygotsky’s emphasis on the interactions among a child’s learning, his environment, the type of instruction provided, and his culture was a precursor to many of the dynamic systems models that influence learning theory today.
Vygotsky’s concepts about social learning within the zone of proximal development led to a therapeutic principle called scaffolding. Scaffolding is the process by which therapists or adults support or guide a child’s actions to improve his or her competence. Appropriate guidance is the just right amount of support that enables the child to perform at a higher level. When using scaffolding to facilitate the child’s learning, the adult gradually decreases the amount of support provided such that the child performs more independently. Through this process, actions that are externally supported become internalized. Wertsch makes the point that the child’s help-seeking in an activity can be as important to his learning as receiving that assistance.194 By asking questions and help-seeking, the child becomes more self-directed in his learning; he also develops an understanding about his own learning and how to direct social interactions that can lead to his learning. When the occupational therapist understands a child’s zone of proximal development and perceives methods for scaffolding his learning, she or he can design an optimal activity to promote the child’s learning. Case Study 2-1 presents an example of applying Vygotsky’s theories.
Maslow and the Hierarchy of Basic Needs
Abraham Maslow is generally considered the father of humanistic psychology in the United States.76 He outlined a hierarchy of basic human needs that is believed to follow a longitudinal sequence.118,119 An individual’s most basic needs, those at the base of this hierarchy, are physiologic needs, such as food, water, rest, air, and warmth, that are necessary to basic survival. The next level is characterized by the need for safety, broadly defined as the need for both physical and physiologic security. The need for love and belonging promotes the individual’s search for affection, emotional support, and group affiliation. The need for a sense of self-esteem, which is defined as the ability to regard the self as competent and of value to society, is evidenced as an individual grows. The need for self-actualization, which represents the highest level, is attained through achievement of personal goals.
Maslow proposed that each of these needs serves as a motivator to achieve a higher level of human potential. Throughout development, individuals must satisfy their most basic needs before they are motivated by or interested in other life goals. Foundational biologic and egocentric needs must be satisfied before an individual has social interests and can fully participate in social relationships. With important social relationships established, an individual becomes interested in the broader community and has a broader sense of commitment and responsibility to others within the community. If the lower level needs are not met, the individual is not able to direct his or her energies toward higher levels. For example, a child who comes to school hungry finds it difficult to concentrate on the classroom learning activities. Recognition of a child’s needs and the hierarchy of development of these basic needs helps the occupational therapist understand behaviors that indicate that basic needs are not met and identify needs that should become the focus of goals and interventions.
Learning and Systems Theories
Most important to occupational therapy are theories that integrate concepts about people, their environments, and their occupations. Development has been defined as an “evolution of predictable sequences of interactions between a child and the objects in his or her environment” (p. 446).111 Developmental theories emphasize maturation of the central nervous system as it interacts with the social and physical environment. In addition to maturation, the primary process that results in developmental change is learning.
Learning is the acquisition of knowledge, skills, and occupations through experience that leads to a permanent change in behavior and performance. The basis by which humans are able to learn is neuroplasticity (i.e., the ability of the central nervous system to adapt to and assimilate novel information or tasks). Learning theories foundational to occupational therapy practice models include behavioral theories and social cognitive learning. Dynamic system theory provides a comprehensive framework for understanding a child’s development in context. Learning principles and system theories foundational to occupational therapy are discussed in the following section.
Behavioral Theories
The past 60 years have witnessed tremendous progress in the field of learning theories. Early learning theorists, such as Thorndike, emphasized the association between a behavior and the resulting reward or punishment as a simple explanation of behavioral change. Skinner described perhaps the best known learning theory from this era. He believed that the environment shapes all human behaviors and that behaviors may be randomly emitted in response to an environmental stimulus.170 In other words, a person tries a behavior that worked in a previous situation, or an involuntary, reflexive response is elicited by an environmental stimulus. The behavior is then reinforced by the environmental consequences that follow. This sequence—stimulus situation, behavioral response, and environmental consequence—constitutes a contingency of behavior, the mechanism by which the environment shapes behavior.
Skinner stated that through natural occurrences in the environment, a child’s adaptive behaviors are reinforced, and behaviors that are not adaptive are ignored or punished.171 The Skinnerian concept that became fundamental to interventions for children is instrumental or operant learning or the use of reinforcement to modify behavior. Behavior is strengthened and maintained when it results in positive reinforcement (rather than punishment). If reinforcement is absent (i.e., not given) and therefore is negative, positive behaviors may be extinguished.
Skinner believed that all behavior is a result of the environmental control of the individual, culture, and species. He specified that humans, species, and culture are all part of the environment; therefore, they control as much as they are controlled. Problems arise when an environment changes and becomes inconsistent with prior contingency patterns. For example, children use one set of behaviors with their families and another set with friends. Behaviors that are reinforced by friends may bring complaints from or may be ignored by parents. Critics of this theory cite its failure to explain personality traits (e.g., motivation) and cognitive abilities (e.g., imagination and creativity) and its tendency to generalize across age and gender spectrums with no recognition of developmental differences. Chapter 14 provides further explanation of behavioral interventions.
Extensive research has confirmed that when particular behaviors result in specific, consistent consequences, these behaviors can be modified.40 Therapists using a behavioral approach can help a child achieve a higher level of performance through a process called shaping. Shaping involves breaking down a complex behavior into components and reinforcing each behavior individually and systematically until it approximates the desired behavior (Box 2-2).
 CASE STUDY 2-1 Example of Vygotsky: Scaffolding and the Zone of Proximal Development
CASE STUDY 2-1 Example of Vygotsky: Scaffolding and the Zone of Proximal Development
Sarah is a 4-year-old with an autism spectrum disorder. She demonstrates age-appropriate development in her motor skills; however, she has difficulty with motor planning and sequencing a series of movements. However, her communication, play, and activities of daily living skills appear to be at a 2-year level. She also has difficulty with perceptual skills and often confuses concepts such as up–down, right–left, and spatial awareness. Teresa, an occupational therapist, selected a dress-up activity to promote Sarah’s development of visual perception and motor planning in a dressing occupation. Teresa, who has collaborated with the speech language pathologist, also tries to elicit simple questions and use of action verbs in this play scenario.
Teresa sets up the activity by inviting Sarah to come explore the large bin of dress-up clothes in the preschool classroom. As Teresa holds up a fireman’s jacket and a doctor’s coat, she asks Sarah to identify the top and bottom and to state what part of the body it fits. When Teresa asks Sarah what she wants to be (would you like to be a princess, a nurse, a superhero?), Sarah’s pretend skills are not sufficiently developed to choose. Teresa suggests that she be a princess, wearing a gown, princess shoes, and a crown. Teresa asks, “How will you get on your gown?” Sarah is hesitant so Teresa points to the top and bottom, shows the zipper, and indicates that she can step into the gown. Sarah hesitates and Teresa holds her hand to encourage her to step into the gown. She verbally cues her to slide her arms through the sleeves and models the action with an imaginary dress. Physical assistance is not necessary as Sarah dons the gown with this cueing.
Throughout the activity, Teresa helps Sarah learn and integrate body awareness, saying, “Where are your toes? Let me see your hands and fingers.” When Sarah has her gown, shoes, and crown on, Teresa suggests that she dance in front of a mirror to see how the gown flows and to imagine being a princess. They parade through the preschool classroom so that the other children can see her gown. When it is time to go outside and Sarah must take off the gown, Teresa decides to allow Sarah to sequence the undressing activity without verbal or physical cueing. She kneels by Sarah, prepared to help or give guidance, but knowing that undressing is easier, she hopes that Sarah can accomplish it on her own. Although Teresa begins the zipper, Sarah removes her princess clothing independently. Teresa reminds her of top and bottom, right and left during the undressing to reinforce those concepts.
Although this is a simple play scenario, common in preschool classroom, Teresa has applied principles of Vygotsky’s theories. She selected an activity within Sarah’s proximal zone of development that she could achieve with a minimal amount of support. Teresa was prepared at each step to provide assistance (e.g., physical assistance in donning), but she first observed what support was needed to give the just right amount of support. She reinforced Sarah’s learning by making short descriptive comments about the task and by asking about body parts and basic perceptual concepts.
In recent years, learning and behavioral theories used with young children have evolved into approaches that can be applied broadly across settings. Applied behavioral interventions primarily use operant conditioning in highly controlled environments in which a therapist or teacher gives the child an instruction and then rewards the child for an appropriate response (reinforcement). Applied behavioral interventions are successful in developing skill; however, skills learned in an isolated setting, as in discrete trial training, do not always generalize into new or higher level behaviors across all settings. Educators have developed behavioral approaches that also use Skinner’s framework of instrumental (operant) learning and can be implemented in the child’s natural environment to teach children adaptive behaviors that generalize across environments.94 Educators in early childhood programs have advocated for naturalistic teaching procedures that can be implemented in minimally structured sessions, in a variety of locations and contexts, with a variety of stimuli. Although educators who used naturalistic teaching procedures hold the same developmental goals for children as those who use classical behavioral theory, their procedures are much less structured, incorporate peers, and use naturalistic conditions and reinforcers.43 Two types of these naturalistic learning procedures, incidental teaching and pivotal response training, are frequently used with young children in early childhood programs.
In incidental teaching, a play environment is created to stimulate the young child’s interest and curiosity. It is important that toys used be developmentally appropriate, with both novel and familiar toys. The goal is for the child to select an activity and spontaneously begin to play. The therapist builds on the child’s play selection by expanding the play scenario so that it becomes more challenging or creates a problem for the child to solve. The therapist may cue the child to perform a different action and reward the child for attempting more challenging actions. These teaching sessions take a different approach than do behavioral interventions, which use discrete trial training in which the child is given specific directives and rewarded for a specific response. Table 2-1 compares incidental teaching and discrete trial training.
TABLE 2-1
Comparison of Discrete Trial Training and Incidental Teaching in Early Childhood Programs
| Discrete Trial Training | Incidental Teaching |
| The therapist plans highly structured sessions with planned stimulus and reward. | The therapist plans a loosely structured session with environment designed to elicit specific responses, but directives are not used. |
| The therapist gives instructions to direct the child’s actions. | The child initiates and paces the activity. |
| The training session is generally one-on-one in a clinic or the home. | The session generally takes place in the classroom, child care center, or home, in the child’s natural environment. |
| The same stimuli are used repeatedly. | A variety of stimuli are used. These stimuli are selected from the natural environment. |
| The therapist uses artificial reinforcers and often the same reinforcers. | A variety of reinforcers are used and these are selected from the natural environment. The goal is that these reinforcers be available to the child without the presence of the therapist. |
Adapted from Cowan, R. J., & Allen, K. D. (2007). Using naturalistic procedures to enhance learning in individuals with autism: A focus on generalized teaching within the school setting. Psychology in the Schools, 44, 701-715.
Pivotal response training is also a naturalistic teaching and learning approach used with young children.93 The goal of pivotal response training is to teach children a set of pivotal behaviors believed to be central to learning. The desired outcomes of pivotal response training include increasing (1) the child’s motivation to learn, (2) attention to learning tasks, (3) persistence in tasks, (4) initiation of interactions, and (5) positive affect.115 Procedures that are used in pivotal behavioral training are similar to those used in incidental teaching with emphasis on methods to promote generalization of learning. When applying pivotal response training, the therapist gives the child a choice in play materials, uses natural reinforcers, intersperses mastered tasks with learned tasks, and reinforces attempts at new learning (Figure 2-3).43 These theories are further explained in Chapter 23 on early intervention programs.

Social Cognitive Theories
In general, social cognitive theory explains learning that occurs in a social context. The initial acquisition of highly complex and abstract behaviors was difficult for learning theorists to explain until the advent of the social cognitive theory proposed by Bandura.11 Bandura11 and Piaget144 introduced the idea that children can learn by observing the behavior of others. This learning may not be immediately observed in behavior but becomes part of the child’s general understanding of the world. In contrast with the behavioralists, who believe that all learning produces behavioral change, social cognitive theorists believe that learning can occur without observable behavioral changes. A child can learn by observing the behavior of others, such as subtle nonverbal gestures that are used in conversation. These are observed and stored in memory and may not be demonstrated by the child until a much later time, when the child may exhibit similar gestures but with his or her own unique style.
In social cognitive theory, people determine their own learning by seeking certain experiences and focusing on their own goals. Therefore, children do not simply learn random elements from the environment, but they direct their own learning and are goal oriented in what they learn. Social cognitive theorists also believe that children learn indirectly by observing how their peers’ behaviors are rewarded or punished. Direct reinforcement is not always needed when learning new behaviors.138
Social cognitive learning is often indirect, as when the child learns by observing the consequences of behaviors of those around him or her. Learning that occurs when observing the behaviors of others also depends on the child’s goals, interests, and relationship to those observed. Children’s learning increases when they are given an incentive to learning (i.e., an anticipated valued outcome or reward). Learning is also promoted when the child establishes his or her own goals, is given opportunities to work on those goals, and evaluates whether the goal was accomplished. When children set their own goals, they direct their behavior in a specific way, they are more likely to persist in the behavior to achieve the goal, and they are often more satisfied with the outcome.
In this theory, children learn social skills through group experiences. When children have delayed social skills, they can gain an understanding of social gestures and peer interaction by becoming involved in a group where these behaviors are modeled and rewarded. Bandura believed that critical factors in the child influence the learning process, including the child’s perception of his or her competencies (i.e., self-efficacy). The ways in which a strong sense of efficacy can enhance personal accomplishment are described next.
The Influence of Motivation and Self-Efficacy on Learning
A number of factors in the child are believed to influence learning, such as cognition, motivation, attitude, and self-perception. The relationship between learning and other affective components is complex. It is widely accepted that children’s motivation to perform occupations is influenced by their perceptions of their efficacy, regardless of whether these perceptions are correct.11 If children experience success in learning situations, it is assumed that they increase their perceived competence and internal control, gain support from significant others, and show pleasure at mastering the task. The assumption is made that children are more likely to seek out optimal challenges if they have experienced success.13 The corollary of this theory is that children who experience repeated failure begin to avoid challenges and are less likely to seek out new learning situations.79
Motivation to learn and to achieve is developed through (1) casual attributions, (2) outcome expectancy, and (3) personal goals. When children feel self-efficacious, they attribute any failure to lack of effort. When children feel inefficacious, they attribute their failure to low ability. The efficacious child remains motivated to try harder and to improve performance; the inefficacious child believes that there is no point in trying harder because he or she is destined to fail. A child self-motivates by setting a personal goal higher than his or her current skill levels. Then the child mobilizes the energy to achieve that goal. With success the child sets a higher goal and become motivated to achieve a higher-level task.
Self-efficacy beliefs contribute to motivation in several ways. They determine the goals people set for themselves, how much effort they expend, how long they persevere in the face of difficulties, and how they respond to failure.11 All of these decisions contribute to success in a particular goal and contribute to learning. Perceived self-efficacy also contributes to a child’s coping ability, which is discussed later in this chapter.
Therapists need to be aware of the importance of providing successful learning opportunities and optimal challenge situations. It is also important to note, however, that when children are young, they may not have the metacognitive awareness required to compare their own performance accurately against that of others. This lack of awareness may actually have an adaptive purpose in childhood. The fact that young children do not evaluate their own performance increases the likelihood that they will put energy and effort into practicing skills in a wide variety of environments with little concern about their actual competency.21 As children develop, however, their expectation of competence becomes more specific to the type of task and is influenced by their prior experiences with that task, their observations of typically developing peers performing it, and the evaluative feedback provided by credible adults.12
Dynamic Systems Theory
Emerging theoretical ideas from systems theory influence today’s thinking in many areas of development in children, and these ideas are beginning to lead to creation of alternative models of practice for therapy intervention. In contrast with a hierarchical model of neural organization, systems theory (also called dynamic systems theory) proposes a flexible model of neural organization in which the functions of control and coordination are distributed among many elements of the system rather than vested in a single hierarchical level.186 Work that led to the development of dynamic systems theory includes research by Bernstein,20 who used concepts from physics related to movement and applied these ideas to motor development. Bernstein proposed that the central nervous system (CNS) controls groups of muscles (not individual muscles) and that these groups can change motor behavior on their own without CNS control. He believed that motor control could emerge spontaneously from relationships among kinematics (muscles) and biomechanics (joints and bones) that naturally limit the degrees of freedom of movement. Therefore the motor system is self-organizing.169
Systems theory has its roots in geometric concepts, and at the most basic level, a dynamic system is simply something that changes over time. Dynamic systems theorists emphasize that learning does not occur just in the brain and that the body and environment are all constantly changing and simultaneously influencing each other.185 In this theoretical approach, instead of viewing behavior (e.g., motor skills) as predetermined in the CNS, systems theory views motor behavior as emerging from the dynamic cooperation of the many subsystems in a task-specific context. It implies that all factors contributing to the motor behavior are important and exert an influence on the outcome by either facilitating performance or constraining it.
In this approach, the therapist looks for periods of stability in learning and watches for signs that a child is ready to shift to a qualitatively different type of behavior. Identification of the system variables that drive the transition from one level to another facilitates learning.27 These variables can be related to the child, the task, or the environment. Thelen suggested that variables such as physical growth and biomechanics may be more important for motor learning in infancy, whereas factors such as experience, practice, and motivation may be more influential in the learning of motor activities in an older child.180
Dynamic systems theory is an ecologic approach that assumes that a child’s functional performance depends on the interactions of the child’s inherent and emerging skills, the characteristics of the desired task or activity, and the environment in which the activity is performed. Self-organization is optimal in a functional task that has a goal and outcome. Most functional tasks (e.g., eating and drinking) elicit a predictable pattern of movement; therefore, the task itself can organize the movements attempted. These features suggest that dynamic systems theory aligns well with occupational therapy.
Research in dynamic systems theory has focused on explaining the ways new skills are learned.64,133,181,182 The learning of new movements or ways of completing an activity requires that previously stable movements be broken down or become unstable. New movements and skills emerge when a critical change occurs in any of the components that contribute to motor behavior. These periods of change are called transitions. Motor change in young children is envisioned as a series of events during which destabilization and stabilization of movement take place before the transitional phase movement becomes stable and functional.147
The period of instability that occurs in a transitional phase is seen as the optimal time to effect changes in movement behavior. Three characteristic situations mark the transitional stage:
1. Variability in motor performance increases. The child experiments with different movement patterns.
2. Through these exploratory movements, the child determines which pattern is the most adaptive.
3. The child selects the movement that is most adaptive, the movement that meets his or her goals given environmental demands and constraints (e.g. which pattern makes it easiest to rise from sit to stand given the effects of gravity and available supports). During this phase, the child repeatedly practices the same movement pattern.
In children with impairments such as cerebral palsy, constraints hinder the emergence of motor functions. Such constraints are limitations imposed on motor behaviors by the child’s physical, social, cognitive, and neurologic characteristics. The constraint that traditionally has received most attention is the integrity of the CNS; less frequently, other biomechanical constraints are considered, such as biomechanical forces, muscle strength, or a disproportionate trunk-to-limb ratio. Environmental constraints include physical, social, and cultural factors not related to a specific task. One example of a physical constraint is a suboptimal surface for the child’s activity (e.g., a slippery or inclined surface); a social constraint could be a parent’s lack of reinforcement of the acquisition of motor behaviors. Task constraints are restrictions on motor behavior imposed by the nature of the task. Established motor behaviors may be altered by specific task requirements. For example, when faced with the task of crawling on rough terrain, infants may alter motor behavior by straightening the knees and “bear walking.” When a child reaches for a ball, the ball’s size influences the shape of the child’s hand and the approach taken (e.g., one hand versus two). The unique features of these tasks have shaped the child’s motor behavior. See Table 2-2 for a list of dynamic systems theory principles. Dynamic systems theory has many similarities to the emerging occupational therapy theories that focus on person, environment, and occupation relationships. This theory is further explained in Chapters 3 and 9.
TABLE 2-2
Principles of Dynamic Systems Theory Applied to Motor Development
| Dynamic System Theory Principle | Application to Motor Development |
| Sensory perception and motor systems are coupled. These systems continually interact in learning new motor skills. The infant’s perceptions guide his or her movements, which in turn create the infant’s perception of the world. | Haptic sense, discrimination of the physical properties of objects through touch, is acquired through object manipulation. Sensory information is gained as the infant’s fingers move over the object’s surfaces. |
| Functional synergies are the basis of motor behavior. Movement synergies are based on kinematic (e.g., muscles) and biomechanic (e.g., joints) constraints and are the basic units that control movement. Therefore, the basic units of motor behavior are functional synergies or coordinated structures rather than specific muscle actions. These functional synergies are “soft”—assembled (i.e., they are highly adaptable and highly reliable). | Similar synergies are used for eating and drinking that involve shoulder internal rotation and adduction, elbow extension followed by flexion, forearm pronation followed by slight supination, and a neutral wrist position. This functional synergy is also used, with slight modification in combing one’s hair and cleansing face and teeth. This is a stable but flexible synergy. |
| Transition to new movement patterns involves exploration, selection, and practice phases. The infant or child first explores many different patterns and exhibits high variability in movement. Then the infant selects an optimal pattern to achieve his goal. This pattern is practiced and becomes more adaptable to a variety of environmental demands. | When first learning to eat with a spoon, the infant exhibits a variety of patterns with the spoon, including banging, stabbing, and waving. Then the infant selects a functional pattern that successfully meets the environmental demand (e.g., the toddler learns to supinate the forearm when bringing the spoon to mouth so that the food reaches the mouth rather than spilling down the chest). This adaptive pattern is repeatedly practiced as the toddler insists on always self-feeding. |
| The infant’s unique motor patterns are the result of input from multiple systems that interact in dynamic ways to both facilitate and constrain movement. Behavior is multiply determined and children develop in context. Behavior is determined by an integrated system of perception, action, and cognition. These elements are integrated over time to form a child’s unique developmental trajectory. | The pattern an infant uses to reach for an object is determined by many variables. Variables that may influence reaching include biomechanic and kinematic factors such as weight of his or her arm, stiffness of joints, strength, and eye-hand coordination. However, the reaching pattern is also influenced by how successful the child was in previous reach and grasp (did the object move before the child could obtain it?), how motivated the child is to attain the object, general energy level, and curiosity. |
Adapted from Case-Smith, J. (1996). Analysis of current motor development theory and recently published infant motor assessments. Infants and Young Children, 9(1), 29-41; Spencer, J. P., Corbetta, D., Buchanan, P., Clearfield, M., Ulrich, B., & Schoner, G. (2006). Moving toward a grand theory of development: A memory of Esther Thelen. Society for Research in Child Development, 77, 1521-1538.
MODELS OF PRACTICE USED BY OCCUPATIONAL THERAPISTS
Occupational therapy practitioners recognize that health is supported and maintained when clients are able to engage in occupations and activities that allow desired or needed participation in home, school, workplace, and community life.2 Thus, occupational therapy practitioners are concerned not only with the child’s performance in everyday activities but also the environmental influences that enable a child’s engagement and participation in those activities.197
This section of the chapter focuses on models of practice developed specifically for occupational therapy assessment and intervention with children. An example of a theoretical framework that focuses on occupation and performance is presented first. Discussion of this overall framework is followed by overviews of specific models of practice used with children and youth. These models of practice are used in conjunction with an overall focus on occupation and occupational performance.
Most occupational therapy practice models explain the interaction of person, occupation, and environment. They recognize the premise that human performance cannot be understood outside of context.57 In earlier models (e.g., person-environment-performance,32 person-task-environment81), the focus of primary intervention is on the person, with relatively less emphasis on changing environments. Law and colleagues developed the person-environment-occupation (PEO) model, which focuses equally on facilitating change in the person, occupation, and/or environment.99
The PEO model was developed using theoretical foundations from the Canadian Guidelines for Occupational Therapy, environmental-behavioral theory, and work by Csikszentmihalyi & Csikszentmihalyi45 on the theory of optimal experience. The PEO model outlines the concepts of person, environment, and occupation as follows99:
• Person: A unique being who, across time and space, participates in a variety of roles important to him or her.
• Environment: Cultural, socioeconomic, institutional, physical, and social factors outside a person that affect his or her experiences.
• Occupation: Any self-directed, functional task or activity in which a person engages over the life span.
The PEO model suggests that occupational performance is the result of the dynamic, transactive relationship involving person, environment, and occupation (Figure 2-4, A). Across the lifespan and in different environments, the three major components—person, environment, and occupation—interact continually to determine occupational performance. Increased congruence, or fit, among these components represents more optimal occupational performance (Figure 2-4, B).

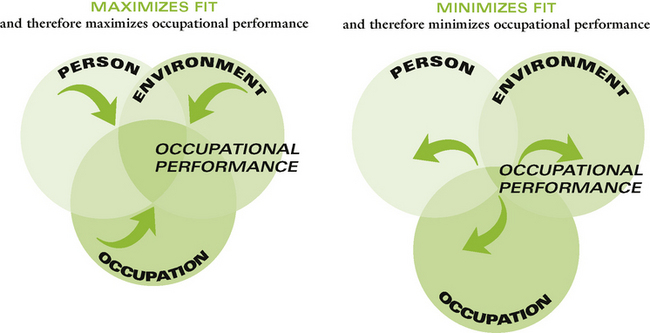
FIGURE 2-4 A, Person-environment-occupation model. B, Person-environment-occupation analysis. (From Law, M., Cooper, B., Strong, S., Stewart, D., Rigby, P., & Letts, L. [1996]. The person-environment-occupation model: A transactive approach to occupational performance. Canadian Journal of Occupational Therapy, 63[1], 9-23.)
The PEO model is used as an analytic tool to identify factors in the person, environment, or occupation that facilitate or hinder the performance of occupations chosen by the person. Occupational therapy intervention can then focus on facilitating change in any of these three dimensions to improve occupational performance. Specific models of practice, as outlined next, can be used in conjunction with the PEO model to address specific performance limitations or environmental conditions that impede occupational performance.
Specific Models of Practice
The models of practice or frames of reference currently used in occupational therapy operate within systems theory, as each considers the interaction of person, environment, and activity or occupation. A discussion of systems theory as it influences occupational therapy interventions is presented first; then specific practice models used by occupational therapists in their work with children are explained.
A Systems Approach
Occupational therapists approach intervention with a child by first gaining an understanding of the environmental, family, and child factors that influence the performance of specific activities. From the literature that discusses the application of systems theory or dynamic systems theory to occupational therapy intervention, the following principles emerge:
• Assessment and intervention strategies must recognize the inherent complexity of task performance. The most useful assessment strategy is to develop a “picture” or “profile” of the ways performance components and environmental and task factors affect performance of the tasks the child wants to accomplish. Assessment of only one or a few components (e.g., balance, mood, strength) is not likely to lead to the most effective identification of constraints.
• The focus of assessment and intervention is on the interaction of the person, the environment, and the occupation. Therapy begins and ends with a focus on the occupational performance tasks a child or youth wants to, needs to, or is expected to perform. When a child shows readiness and motivation to attempt a task or activity, the focus of intervention on that particular activity can effect changes in his or her performance.97
• The therapy process focuses on identification and change of child, task, or environmental constraints that prevent the achievement of the desired activity. Some of these factors may be manipulated to enhance the functional motor task or goal; others may be managed by providing the missing component during the execution of the task. Parts of activities can be changed (e.g., different toy sizes, different position for child or activity). Activities should be practiced in a variety of environments that can facilitate completion of the task and promote the flexibility of movement patterns. Activities incorporated into the child’s daily routine provide opportunities for finding solutions for functional motor challenges (Figure 2-5).
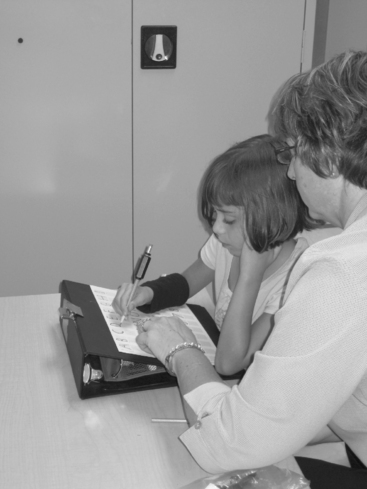
FIGURE 2-5 In this functional activity, a slant board is used to promote improved posture and grasp of the pencil. A weight on the pencil provides added proprioceptive input.
• When preparing therapeutic activities, the therapist identifies playful activities that would motivate the child, are developmentally appropriate, match the child and family’s goals, provide a challenge to current skills levels, and match an expected or hoped for outcome.
• With intervention through the systems approach, the focus on changing environments and occupations is at least as great as the focus on changing the inherent skills of the child or adolescent. Intervention is best accomplished in natural, realistic environments. The accomplishment of whole occupations, not parts of them, is emphasized. The goal in therapy is to enable a child to accomplish an identified activity, rather than promote change in a developmental sequence or improve the quality of the movement.
• Therapeutic effect and positive outcomes are determined by the child’s engagement in the activity, the match between the intervention activities and the child’s skill levels, the meaningfulness of the activity, the amount of practice, and the opportunities to transfer and generalize the newly learned skill to a variety of contexts. Positive effects relate to how well the interventions enable the child to perform well across his or her natural environments given age and role expectations.
Models of practice for therapy assessment and intervention, based on dynamic systems theory, are beginning to emerge, although challenges to implementation remain.31,46 Common among these models is the focus on successful achievement of functional goals rather than on the development of typical patterns of movement.26,47,169 Ketelaar et al.,89 in a study of 55 children receiving either functional therapy based on dynamic systems theory or therapy aimed at developing “typical” movement patterns, found that children in the functional therapy group demonstrated significantly more functional skills (mobility and self-care) as measured by the Pediatric Evaluation of Disability Inventory.89
Cognitive Approaches
Cognitive approaches are “top down” or occupation-based approaches because the emphasis in therapy is on assisting the child to identify, develop, and use cognitive strategies to perform daily occupations effectively. These models build on Bandura’s research11 supporting the importance of self-efficacy and establishing goals to motivate individual achievement.
In cognitive approaches, the occupational therapist designs interventions to increase a child’s repertoire of cognitive strategies and improve the child’s ability to select, monitor, and evaluate his or her use of these strategies during the performance of a task. The inherent assumption is that improved performance results from the dynamic interaction of the child’s skills with the parameters of the task in the context in which it needs to be performed. Therefore, the child discovers, applies, and evaluates cognitive strategies during task performance in his or her typical environments.131
The cognitive model of practice requires that the therapist identify and use a global problem-solving strategy, which provides a consistent framework within which the child discovers specific strategies applicable to tasks that he or she either needs or wants to perform. This global strategy is based on the five-stage problem-solving structure first outlined by Luria.108 Using occupational therapy terminology, these steps include (1) task analysis, (2) anticipation of the child’s difficulties, (3) exploration and selection of task-specific strategies, (4) application of a strategy to the task, and (5) evaluation of the strategy’s effectiveness.130 The child is guided to develop his or her own cognitive strategies based on the problems encountered during tasks. The task-specific strategies a child discovers are unique to him or her.
Using cognitive skills to assess his performance, identifying successful and unsuccessful actions, the child learns to become more efficient in functional activities. The occupational therapist supports the child’s goals and self-evaluation. The therapist can also cue, prompt, or model the task, aligning these supports to the child’s goals. The atmosphere in the therapy session is one of acceptance and support for taking risks. Although the child guides the selection of activities, the therapist is always aware of the generalization and task-specific strategies that the child needs to learn and creates opportunities for the child to discover these.131,150
Because the selection of tasks is critical to the approach, a client-centered tool must be used that allows the child to identify goals for intervention. An appropriate goal-setting instrument for use with children older than 9 years of age is the Canadian Occupational Performance Measure (COPM)97; for children 5 to 9 years of age, the Perceived Efficacy and Goal Setting (PEGS) system can be used.132 The cognitive approach is probably not a suitable model of practice for children under 5 years of age because of its emphasis on the development of metacognitive skill and knowledge.
One of the key features of a cognitive model of practice is the way in which the therapist helps the child explore strategies, make decisions, apply strategies, and evaluate their use. The therapist does not give instructions. Rather, he or she uses questions to help children (1) discover the relevant aspects of the task, (2) examine how they are currently performing the task, (3) identify where they are getting “stuck,” (4) creatively think about alternative solutions, and (5) try out these solutions and evaluate them in a supportive environment. Once a strategy is found to be helpful, the therapist uses questions to help the child “bridge” or generalize the strategy, eliciting from the child other times and situations in which that strategy may apply.150
In recent years a particular cognitive approach, the cognitive orientation to daily occupational performance (CO-OP),149 has been researched systematically to determine whether it is an effective model to use with children with developmental coordination disorder. Evidence is accumulating that CO-OP is effective at enabling skill acquisition and that it also results in generalization and transfer of learned skills.150 A randomized clinical trial comparing CO-OP with an equivalent number of sessions of direct skill training found that, although children in both groups improved and achieved motor goals, the gains in the CO-OP group were greater; long-term maintenance both of the motor goals and of the cognitive strategies was significantly stronger in the CO-OP group, which led parents to report greater satisfaction with this treatment approach.127 Studies on CO-OP have shown its effectiveness with children with developmental coordination disorder,127,179 cerebral palsy or acquired brain injury, and Asperger’s syndrome.159,160
Through research such as this, a variety of cognitive strategies have been identified that seem to be helpful to many different children experiencing occupational performance difficulties. Videotape analysis has been used to systematically identify and describe some of these strategies.116 It appears that children need to be able to state and apply a global executive strategy, such as “Goal, Plan, Do, Check,”123 to guide their problem solving. In addition, specific strategies seem to be useful for improving their performance, including verbal self-guidance (child talks himself or herself through the motor sequence); feeling the movement (drawing attention to an aspect of the sensation of movement as it is performed); motor mnemonic (labeling a body position or motor sequence); body position (verbalizing or directing attention to the body position or body parts relative to the task); and task specification (discussing specific parts of the task or actions to change the task).116
In summary, occupational therapists who use a cognitive model of practice (1) focus on the occupations a child wishes to perform rather than on foundational skill building; (2) use a general problem-solving framework that guides the child to discover, select, apply, and evaluate the use of specific cognitive strategies; (3) use process questions to increase the child’s awareness of the use of strategy during the performance of daily tasks; and (4) plan for transfer and generalization of the strategies that the child has learned.130,150
Adaptation and Compensation Interventions
Occupational performance is successful when the demands of the task, the skills of the child, and the features of the environment are congruent. When the skills of the person do not meet the demands of the task in the environment, occupational performance becomes less successful. Most of the models of practice in occupational therapy, particularly with children who are still developing, focus on increasing the child’s skills. The adaptation model of practice involves adapting the demands of the task or modifying the environment so that they are congruent with the child’s ability level. Adaptations may involve modifying the occupation so that it is easier to perform, using assistive technology devices, or changing the physical or social environment.44 Often when children have significant impairments, task modification is needed to maximize the child’s participation. For example, a child with cerebral palsy may require an adapted spoon and cup to eat dinner with his family. A child with autism may require a picture exchange card system to communicate his need to use the bathroom.
When skills are insufficient to enable performance, task adaptation is used to modify the demands of a task to bring it to the competence level of the child. Task demands are analyzed and functional limitations are identified, and difficulties then are creatively circumvented. An example in school-based practice would be adapting the writing surface by using a slant board so that the child’s written work is more easily visualized and the child’s hand and arm posture are supported in a posture that promotes writing skill. A child with a learning disability may be able to complete a page of arithmetic problems when the font is enlarged and the paper has a color tint.
Often adaptive equipment or assistive technology (AT) is used to modify or adapt the task. Campbell, Milbourne, and Wilcox view assistive technology as a bridge or mediator between the skills that a child can currently perform and the requirements of the task.29 Assistive technology may be as simple as adaptive brushes or crayons that allow a preschool child to participate in art activities. A wide variety of assistive technology devices can enable children with significant motor impairments to better access their environment. For example, AT devices can help position the child to perform an activity (e.g., a prone stander) or provide postural support (e.g., wheelchair straps). “High-tech” technology is also available to provide a method for written communication (e.g., a laptop computer) or augmentative communication (e.g., a device for synthesized speech). Chapters 16, 20, and 21 describe assistive technology devices that use this approach to increase children’s participation in their natural environments.
With children, the compensatory approach often complements other approaches that focus on skill building. Methods for adapting tasks are selected not only so that the child succeeds at a particular task, but also to promote skills in similar tasks and in other environments. For example, a boy with poor drawing skills can create a picture using peel-off stickers of animals. Although this adaptation allows the boy to create a picture more easily than drawing with markers, peeling off and placing the stickers provide practice of fine motor skills—specifically, bilateral coordination, isolated finger movements, spatial relations, and use of force. Practice in these skills may generalize to other art activities, and the easy success the child achieves when using colorful animal stickers may encourage him to attempt other art activities.
Psychosocial Approaches
Occupational therapists use a variety of psychosocial approaches when working with children and adolescents experiencing problems in occupational performance because of social, emotional, or behavioral issues or difficulties with relationships. Several of these approaches, such as a cognitive approach or the compensatory and environmental approach, are discussed elsewhere in this chapter. These approaches are grounded in theories that focus on the development of self, on family and peer relationships, and on the aspects of the social and cultural environment that influence each of these. Although the number of occupational therapists who work with children with chronic mental health issues is relatively small, all occupational therapists who work in pediatrics use the concepts of psychologic and social development implicitly, because developing the ability to maintain relationships with peers and significant others is an essential part of the occupational performance of childhood and adolescence.
Chapter 13 describes the models of practice that focus on social behavior and the development of self. Personal attributes, such as temperament, self-esteem and self-efficacy, problem-solving ability, and social skills, are considered important determinants of healthy functioning. Environmental influences on behavior and social development suggest the need to consider the expectations and social elements of the home, school, and community environments and to recognize the importance of friends in a young person’s life. For the occupational therapist, the critical consideration is the impact of the person’s attributes and environmental influences on ability to participate in daily occupations.
Given the complex nature of behavior and social relationships, occupational therapists often draw on a number of intervention approaches in this model of practice. The therapist’s knowledge of normal behavior, vulnerabilities associated with particular disabilities, attachment, coping skills, and compatibility of temperaments may guide intervention with a parent–child dyad. Cognitive behavioral strategies may be used by occupational therapists to help young people who are depressed or socially withdrawn develop strategies that encourage participation in social situations (see Chapter 13).
Coping Model
The coping model addresses psychosocial function, uses cognitive behavioral strategies, and is congruent with the PEO model.199,205 Therapists who use this model emphasize the use of coping resources that enable the child to meet challenges posed by the environment. The goal is to improve the child’s ability to cope with stress in personal, social, and other occupational performance areas. When children are successful in coping with their own personal needs and the demands of the environment, they feel good about themselves and their place in the world. Coping strategies are learned, and children build on previous successful experiences in coping with environmental expectations.205
All children experience stress when faced with physical, cognitive, and emotional challenges. When these challenges are successfully met by the child’s inner resources and caregiving supports, the result is a sense of motivation, learning, and mastery. Stress can evoke negative feelings when the child’s resources are poorly matched to the environment’s demands. Both internal and external resources assist in the process of coping. Internal coping resources include coping style, beliefs and values, physical and affective states, and developmental skills. External coping resources include human supports and materials and environmental supports.
Internal and External Coping Resources: Children have unique patterns of sensorimotor organization, reactivity, and self-initiation.206Coping style is the way the child reacts to social interactions and responds to environmental events. Intrinsically motivated and self-initiated behaviors are part of a child’s coping style. Examples of these behaviors are the child’s exploration of objects and space, initiation of interaction, and persistence in activities. Self-initiated behaviors are particularly important to occupational therapists, because many children with disabilities show limited spontaneous behaviors when exploring the environment, initiating play, and persisting in activity. Physical and affective states influence the child’s ability to cope with environmental stress. Energy, endurance, moods, and emotions define the child’s ability to respond to, engage in, and persist in activity. Chronic illness, emotional instability, and depression may impair the child’s ability to handle the demands of the environment effectively.148
Developmental skills and competence are the internal resources a child brings to a task. Often a child with disabilities is placed in situations that match the chronologic age (e.g., a preschooler play group) but not necessarily the developmental age. When expected behaviors do not match developmental skills (e.g., to sit quietly and attend), children experience stress and generally seek external coping supports.
Human supports are people in the child’s environment who support the child’s coping efforts. Parents and other primary caregivers are the most significant external resources for coping in the child’s early years.199 Parents buffer the child’s exposure to stress, make demands, model coping behaviors, encourage and assist the child in coping efforts, and give contingent feedback. They provide material supports and resources, including food, clothing, and shelter. Environmental supports are the spaces and materials available to the child and may include adapted equipment and technology associated with comfort and functional support.
Effective Coping: The child successfully copes with new challenges when (1) he or she has underlying resources that enable a successful response to an environmental demand or new situation; (2) human supports are provided to facilitate his or her performance (e.g., the therapist gives the child a visual or verbal cue); and (3) environmental supports are provided that enable the child to feel safe and comfortable, be attentive and engaged, and feel calm and organized (e.g., a classroom that is quiet and well organized and that has a comfortable lighting level and temperature). The therapist continually evaluates whether the child’s skills (internal resources) and environmental supports (external resources) are adequate to meet the demands of the activity. When the child exhibits ineffective coping strategies, the therapist adjusts the task demands and provides more human or environmental support to enable the child to succeed in his or her coping efforts.
To facilitate effective coping, Williamson and Szczepanski defined three postulates199:
1. The occupational therapist can grade or modify the environmental demands to ensure that they are congruent with the child’s adaptive capabilities. For example, the environment of a child with attention deficit–hyperactivity disorder (ADHD) can be adapted by reorganizing materials to reduce visual demands and enhance visual attention. To enhance the social skills of children with behavioral disorders, a tabletop of materials for an art activity can be provided in insufficient quantity for the number of children, to encourage sharing.
2. The therapist can design intervention activities to enhance the child’s internal and external coping resources. Intervention focuses on the child’s resources, including coping style, physical and affective states, developmental skills, human supports, and material and environmental supports. The therapist can foster a positive sense of self and can involve the child in activities that promote self-efficacy. For older children, the therapist can facilitate group discussions of personal goals and plans for reaching these goals. Personal social skills may be emphasized by practice of social skills in the context of games with peers. Activities that emphasize group skills, such as problem solving, sharing, and communication, can help older children develop improved personal social skills that can be generalized to school and extracurricular activities.
3. The therapist can provide appropriate, contingent responses to the child’s coping efforts. Timely, positive, and explicit feedback to coping efforts helps the child experience a sense of mastery. Feedback that effectively enhances coping efforts emphasizes self-directed, purposeful behaviors. Therefore, the therapist supports child-initiated activity and provides feedback that encourages the extension and elaboration of emerging skills. Because research suggests that children with disabilities tend to assume passive, dependent roles, highly structured and therapist-directed activities should be replaced with child-initiated activities that are specifically and appropriately reinforced and then generalized to other situations (Figure 2-6).

Social Skills Training
Interventions that develop positive coping strategies in children and adolescents with psychosocial dysfunctions can be essential for promoting the ability to participate in social interactions and relationships. Occupational therapists working with older children and adolescents with mental health problems often use social skills groups to promote coping effectiveness and occupational performance. A group milieu allows young people to master developing skills in a safe and supportive environment. Social skills training groups have shown positive effect with adolescents with autism.80 Monthly group meetings focused on social skill development resulted in adolescents improving in maintaining and initiating conversation. Broderick, Caswell, Gregory, Marzolini and Wilson evaluated the effect of a social skill group of adolescents with autism spectrum disorder and found that they improved in self esteem and confidence.24 See Table 2-3 for examples of venues for social skills training.
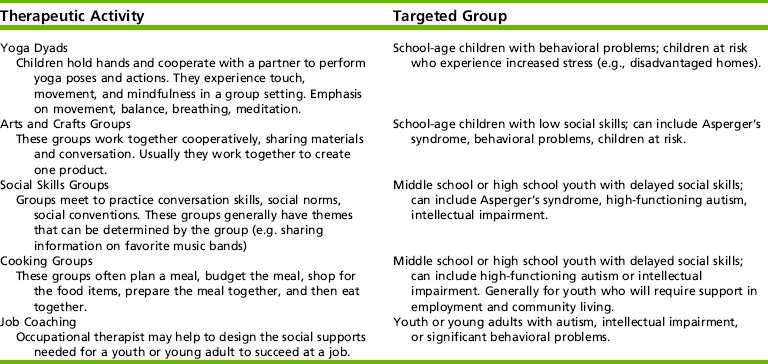
Social networks have been shown to help a person establish positive attitudes and role behavior, maintain and improve self-esteem, and develop moral and social values.35,78 Other studies have identified the interactive, protective factors in child, family, and social environment that enable a child to be resilient to the effects of disability. Bedell, Cohn, and Dumas described a “Building Friendship Approach” in which collaborative student-centered school teams (student, school personnel, family, and friends) identify strategies for improving the social opportunities of the student with brain injury.16 The team helps the student generate his or her own solutions and set goals to improve his or her social opportunities. This approach appears to be effective but the outcomes need to be monitored to ensure that they are maintained.
Research on psychosocial approaches is difficult to review because of its scope and because of the variety of types of practice and their implementation across different disciplines. Evidence in the literature supporting the use of specific approaches is minimal. Studies on the effectiveness of social skills training have been conducted with school-age children with brain injury,74 depression,66,152 schizophrenia,80 and autism.24,83 Although many of these studies have methodologic limitations, the results seem to offer support for social skills interventions in improving self-esteem, positive affect, problem-solving, and social behaviors.
Motor Learning and Skill Acquisition
Motor learning as a model of practice focuses on helping the child achieve goal-directed functional actions. It may initially appear to be a skill-building approach, because the focus is on the acquisition of skills involved in movement and balance. However, motor learning is actually an occupation-based approach, because it is directed toward the search for a motor solution that emerges from an interaction of the child with the task and the environment.
When a child is learning a new functional task, a general movement structure is brought into place that takes into consideration the relationship involving the child’s movement capabilities, the environmental conditions, and the action goal. When the task is performed repeatedly, these correspondences become more refined, and the goal is achieved more successfully. Specific processes, such as muscle contraction patterns, stabilization and positioning of joints, and response to gravity and other forces, are only crudely organized at first. However, with continued practice, these become more organized and finely tuned.69 These patterns are called movement synergies, or coordinative structures, and they represent the child’s preferred strategy for solving a task in the most energy-efficient way.180
Children with motor programming and motor control deficits often have difficulty establishing the timing and sequencing of functional synergies. Task and activity demands may vary, and each of these dimensions is relevant to the way in which tasks are learned. These characteristics of a task determine what motor learning strategies are used to improve performance.
1. Simple-complex. Simple tasks, such as reaching for an object, require a decision followed by a sequenced response. Complex tasks, such as handwriting, require the integration of information from a variety of sources and the application of underlying rules that guide performance.
2. Open loop–closed loop. In an open-loop task, a motor program is put into place before the action begins and is not modified during the performance of a task. An example of an open-loop task is throwing a ball. In a closed-loop task, the child continues to monitor and respond to feedback that he or she receives intrinsically from the body and extrinsically from the environment. An example of a closed-loop task is cutting out a shape using scissors.1
3. Environment changing–environment stationary. The difficulty of learning a task is tremendously influenced by the extent to which the task is predictable. When the environment is changeable or variable, the child has to learn the movement and learn to monitor the environment to adapt to change. Running on rough terrain and playing soccer are examples of tasks in which the environment is constantly changing. This concept is not to be confused with the open- and closed-loop features of the task previously described. Brushing the teeth and playing the piano are tasks during which the child must monitor sensory feedback (closed loop), but the environment remains stationary.177
4. Task characteristics. The ease or difficulty of learning a task depends on the match between the way the task is presented and the preferred learning style of the child. Some children learn best through auditory or visual methods; others prefer movement and touch.
Different types of feedback contribute to the motor learning process. Feedback is intrinsic when it is produced by the child’s sensory systems and is inherent in a task. An example of intrinsic feedback is information available to the child through vision, proprioception, sensation, or kinesthesia. Extrinsic feedback is provided to the child by an external source, such as the therapist, or by observing the results of one’s actions.136,169Knowledge of results is a type of extrinsic feedback in which the therapist provides information to the child about the relationship between the actions and the goal, but only after the fact. For example, a child who is throwing a basketball toward the hoop may be told that the ball is not going high enough and therefore is missing the hoop. Knowledge of performance is a type of extrinsic feedback that emphasizes the pattern of movement and its relationship to achievement of the task. In the same example, the child may be told that he is not extending his arms far enough before releasing the ball. In both cases, the therapist’s feedback focuses on the outcome of the action, not on the child’s effort. These terms are further explained in Chapter 9.
Research on the scheduling, frequency, and amount of feedback that best promote learning has been published.102,178 Studies have shown that immediate extrinsic feedback may prevent the learner from paying attention to the intrinsic sources of feedback that are always available, such as vision and proprioception. This lack of attention to intrinsic feedback may make the learner dependent on information from the person providing instruction.167
Very little research has focused on the effect of different types of feedback on task performance with children experiencing occupational performance difficulties. However, research investigating motor learning principles with children with movement difficulties has suggested that these children may not solve movement problems in a typical way. The research suggests that extrinsic sources of feedback that focus a child’s attention on specific aspects of the task and on important sensory cues may be important.103
Another important concept in motor learning is the influence of different types of practice on learning and performance. There is no question that practice of a task is beneficial to learning. The difficulty confronting most therapists is the dilemma of whether to practice the whole task or only parts or components of the task. Study results indicate that the benefits of practicing either the whole task or parts of the task depend on the inherent goals of the task.169 If coordination or timing of the parts is important to the task, whole-task practice is more effective for learning. Examples of these continuous types of tasks are walking, swinging at a ball, and bicycling. If a task contains distinct parts that can be performed in a serial manner, these can be practiced as parts of the task. A child learning to don his jacket can be taught how to zip it as a first step. Most occupations involving movement are actually a combination of continuous and discrete tasks (Figure 2-7). Consequently, doing the whole task must follow learning its parts. In learning to ride a tricycle, for example, the child can focus on learning to pedal separately from steering, but he or she must then combine them.

FIGURE 2-7 This activity of threading a string through hooks to create a design involves eye-hand coordination, dexterity, and control of arm in space (strength). It requires multiple steps to achieve a completed product.
Another important consideration in planning practice sessions is the use of random versus blocked practice. During random practice, the environmental conditions vary slightly each time; blocked practice involves drilling the task over and over in the same way. In most cases, random practice produces better learning, because the variable practice allows the child to solve a slightly different movement “problem” every time.102
Some of the key techniques that therapists use in this model of practice are giving verbal instructions and demonstrating movement strategies. Verbal instructions focus on the relationship between the child and the objects in the environment and emphasize key movement features directly related to achievement of the functional goal.69 Physical or manual guidance can be helpful during the initial teaching of a movement because it may clarify the goal, guide selective attention, and help the child organize and plan the movement (Figure 2-8). Researchers stress that guidance or facilitation of movement should be removed as soon as possible, arguing that the therapist rapidly becomes part of the environment, which alters the performance context and the intrinsic feedback available to the child.69
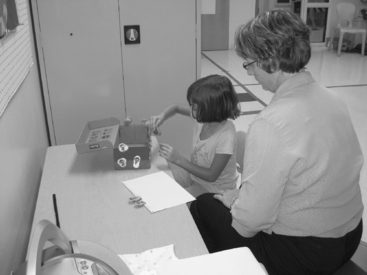
FIGURE 2-8 In this task emphasizing bilateral coordination and hand strength, the therapist suggests an outcome but the child decides what she wants to create.
Motor learning researchers137,178,200 recognize that learning takes place only when there is evidence of a relatively permanent change in the child’s ability to respond to a movement problem or to achieve a movement goal. The learning of a new motor skill needs to be evaluated through tests of retention and transfer, not just immediate changes in performance.112 Therefore, therapists who use a motor learning model of practice must create opportunities for the child to demonstrate their learning during a subsequent therapy session (retention), on a closely related task (transfer), or in a different setting (generalization). Table 2-4 summarizes motor learning concepts, with examples of application in occupational therapy intervention.
TABLE 2-4
Application of Motor Learning Concepts
| Concept | Definition | Application |
| Specificity of learning | Practice experiences that result in the fastest learning and best skill retention are those that most closely approximate the entire task in the child’s natural context. It is the task, not preexisting practice of components, that assembles the emerging skill. | Child who are learning dressing skills should practice in the context of natural dressing opportunities (e.g., after toileting, when going outside to the playground) rather than practicing components such as a buttoning using a button strip on a table. |
| Implicit learning | Improvement in performance results from experiences with a task without specific attention to or awareness of a change in performance. Therefore, success is not always necessary for learning. | Children can learn from participating in tasks without explicit reinforcement for their performance and without explicit recognition of the change in their performance. Success in every intervention task is not necessary. |
| Maximizing opportunity for practice | Repetition is essential for acquisition of motor skills. The most important variable in a training program has been found to be the amount of practice. | Children require guidance and reinforcement to practice a motor skill. It is difficult to dedicate large portions of an intervention session to practice; therefore, it is critical to identify opportunities for the child to practice a new skill across his daily routine. |
| Blocked and random practice | Blocked practice is repeated practice of the same action many times (e.g., a drill). Random practice is a practice sequence in which the related tasks of a skill are performed in no particular order. Blocked practice may be useful in initial learning, but random practice results in better learning. | When teaching a new skill such as in-hand manipulation, the therapist designs intervention activities so that the child has intermittent but frequent opportunities to rotate or translate objects within the hand (e.g., rotate pencil to erase, game with small pieces, resistive lacing). |
| Distribution of practice | Learning increases in distributed practice (practice with rest periods) when compared to massed practice. | Competence in a new skill is reached when it is practiced each week for 5-10 minutes rather than spending a 30-minute session practicing a single skill. |
| Extrinsic feedback | Extrinsic feedback is the information about performance that the therapist gives the child. Extrinsic feedback has been found to improve motivation and to reduce error. Extrinsic feedback is useful to beginners, who may not yet be able to interpret their performance. More frequent feedback is helpful in early learning, and intermittent feedback is better in later learning. | Extrinsic feedback that has been found to improve performance includes information about the adequacy of the child’s performance, how long the child will have to persist in the task before the activity ends, and the therapist’s pleasure in the child’s performance. |
| Transfer of learning | New learning must be applied consistently in a variety of environments. | Learning transfers optimally to a variety of environments when it is learned and practiced in the child natural routines and environments. |
Adapted from Sheppard, J. J. (2008). Using motor learning approaches for treating swallowing and feeding disorders: A review. Language, Speech, and Hearing Services in Schools, 39, 227-236.
Occupational therapists use theories about motor learning to promote development in areas of function that involve learning complex skills and behaviors. Self-care and handwriting are examples of areas of occupational performance to which occupational therapists have applied a motor learning approach. Handwriting is an area of occupational performance in which a motor learning or acquisitional approach has been advocated (see Chapter 19). Although few studies of the effectiveness of this approach to handwriting have been published, many remedial or practice-based handwriting programs are commercially available. A few published studies have demonstrated that the use of acquisitional principles by therapists and educators in a positive, interesting, and dynamic learning environment promotes the development of handwriting.15,129 Some handwriting studies provide therapists and educators with strategies for remediation that use some of the concepts previously listed.18,52 Further research is needed to determine the effectiveness of this approach with different populations of children across a broad range of skills and areas of occupational performance.
To summarize, a therapist using a motor learning model of practice:
1. Analyzes the movement synergies the child uses to achieve the functional action goal
2. Considers the child’s stage of learning and determines how best to facilitate the provision of both extrinsic and intrinsic feedback to improve the efficiency of the movement
3. Provides opportunities for optimal practice of the goal and encourages practice in the natural environment
4. Promotes independent performance and decision making as soon as possible and evaluates whether the motor learning has been acquired, transferred, and generalized
Neurodevelopmental Theory
Historically, the primary concept underpinning a neurodevelopmental therapy (NDT) approach to practice was that normal postural reactions are necessary for normal movement and that these postural reactions are for the most part automatic.23 Although this intervention approach continues to focus on problems in postural control and motor coordination, as seen in cerebral palsy, the principles underlying the treatment approach have expanded to include motor learning and dynamic systems theories. In addition, NDT principles have shifted to recognize the importance of the environment and to place more emphasis on activities that are clearly functional and meaningful to the child.82
When using this approach to evaluate a child, the therapist analyzes the child’s movements to identify missing or atypical muscular-skeletal elements that create functional limitations. These missing elements become one focus of intervention and are used to select the developmental level of therapeutic activities. Therapeutic handling is integral to the NDT approach and is used to facilitate postural control and movement synergies and to inhibit or constrain motor patterns that, if practiced, would lead to secondary deformities and dysfunction.82 A therapist applying NDT strategies focuses on changing movement patterns to achieve the most energy-efficient performance for the individual in the context of age-appropriate tasks.
As the therapist manually guides and handles the child in the context of an activity, these elements are always combined with the child’s active participation. With the therapist’s guidance, the child practices sequences of movements in slightly different ways to reinforce learning of the task. This practice is important for making a movement strategy functional and automatic. Therapists emphasize quality of movement (e.g., accuracy, quickness, adaptability, and fluency). Although therapeutic handling remains an integral part of NDT, practitioners use many treatment methods, “manipulating the individual task or the environment in order to positively influence function” (p. 63).82
Acknowledging that NDT principles have changed over the years to incorporate theories of motor learning and dynamic systems theory, clinical evaluation studies of the neurodevelopmental therapy approach (many of which were completed more than 10 years ago) have raised questions about its efficacy. Comparison studies of this approach for children with cerebral palsy have been conducted over the past 30 years. In these studies, the NDT approach has been compared with functional therapy,166,174 with infant stimulation,141 with Vojta therapy,48 and with differing intensities of therapy.98,121 The results of these trials have been mixed, with two demonstrating no difference,99,174 two supporting NDT,121,166 and two supporting alternate treatments.48,141 The more rigorous randomized clinical trials have generally produced results that do not support the efficacy of the neurodevelopmental approach.146
A recent systematic review of NDT concluded that “the preponderance of results….do not confer any advantage to NDT over alternatives to which it was compared” (p. 789).28 The only consistent effect of NDT that was statistically significant was an immediate effect on range of motion. In contrast with NDT methods, the motor-based interventions that produce meaningful improvements in functional outcomes for children with disabilities incorporate three essential elements: (1) intensive task repetition, (2) progressive challenges to the learner with increasing difficulty, and (3) the presence of motivators and rewards.137,165 Despite lack of evidence on efficacy,165 NDT remains a widely used approach with children who have cerebral palsy and CNS dysfunction affecting motor performance. Because the conceptual basis of NDT has evolved over the past decade, a first step in additional research on its efficacy would be to operationalize the new concepts into treatment protocols that can be measured and replicated for research purposes.
Sensory Integration
The theory of sensory integration, together with the treatment approach derived from that theory, grew from the work of Jean Ayres.3–5 Ayres developed her theory in an effort to explain behaviors observed in children with learning difficulties based on neural functioning. Specifically, she hypothesized that some children with learning difficulties experience problems in “organizing sensory information for use.”4 She named this neural process sensory integration.
Much of Ayres’ work, and that of her colleagues, was devoted to the development of evaluation tools that could clearly identify individuals with sensory integrative problems. The Sensory Integration and Praxis Tests (SIPT) are the result of this work.8 Included in this area of identification and evaluation are a number of studies aimed at describing different subtypes of sensory integrative problems (see Chapter 11 for a summary). Based on current confirmatory studies, these identified subtypes that can be identified by the SIPT include (1) visual and tactile perception with praxis, (2) vestibular and proprioceptive processing with bilateral functions, (3) attention and tactile defensiveness, and (4) visual and tactile discrimination.134
In recent years, scholars in sensory integration have further described sensory integration processes55 and categorized sensory integration disorders.125 Miller and colleagues proposed three patterns of sensory processing disorder, described in Table 2-5.
TABLE 2-5
Sensory Processing Disorder Categories
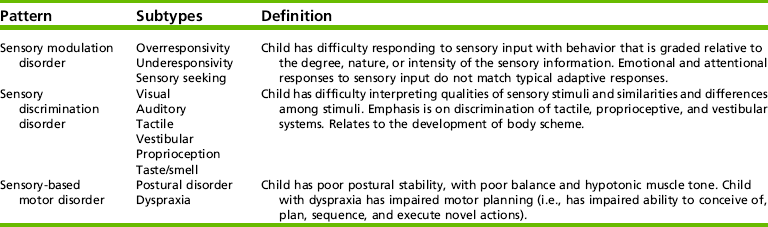
Adapted from Miller, L., Anzalone, M., Lane, S., Cermak, S., & Osten, B. (2007). Typology and terminology of sensory integration. American Journal of Occupational Therapy, 61(2), 135-140.
Although there is some overlap in these disorders, each suggests a specific type of intervention. Dunn’s work identifying children with a sensory modulation disorder has shown that they have patterns of poor registration of sensation, are hypersensitive to stimuli, avoid certain sensations, or seek particular inputs.53 These sensory processing patterns may be present in children with a variety of developmental disorders, and they are often described in children with pervasive developmental disorders or autism.14,88,183,191 Dunn and colleagues have developed evaluation tools for identifying sensory processing problems in children and adults.54,56,63 A number of authors have proposed intervention programs to address sensory modulation disorders.128,164,198 Although there is significant intuitive appeal for sensory modulation disorders as explanatory models for children’s observed behaviors, more research is required to validate these theories and to investigate appropriate interventions.
Ayres also developed interventions that she believed would help to resolve sensory integration problems. She proposed an intervention approach based on assumptions drawn from neuromaturation theory and systems theory.4,7 Neuromaturation concepts, such as hierarchical organization of cortical and subcortical areas, developmental sequence of learning and skill acquisition, and neural plasticity, are essential to an understanding of the mechanisms of sensory integration. Systems theory also underlies sensory integration because the focus is on the child seeking sensory input and using adaptive behavior as an organizer of the input. Figure 2-9 shows a child’s choice of activity. Based on these assumptions, a sensory integration approach seeks to provide the child with enhanced opportunities for controlled sensory input, with a particular emphasis on vestibular, proprioceptive, and tactile input, in the context of meaningful activity. In intervention the therapist facilitates an adaptive response, which requires the child to integrate the sensory information (Figure 2-10). Sensory integration is hypothesized to improve through this process.

FIGURE 2-9 The child’s selection of jumping on an inner tube helps to meet his need for vestibular and proprioceptive input.

Ayres5,9,10 and Miller126 have conducted research aimed at evaluating the process of sensory integration and determining the efficacy of sensory integration intervention (see Chapter 11). In a recent study, a group of scholars examined the research literature on sensory integration to develop a fidelity measure for sensory integration intervention.143 This study involved a comprehensive review of the research literature and produced a definition of the core elements of sensory integration intervention that will be useful to future trials (see Table 2-6).
TABLE 2-6
Core Elements of Sensory Integration Intervention
| Core Element | Explanation |
| Provide sensory opportunities | The therapist provides opportunities for the child to experience intense sensory experiences, including tactile, vestibular, and/or proprioceptive input, generally in combination. |
| Provide “just right” challenges | Activities are developmentally appropriate and challenge the child to exhibit a higher level skill than typical performance. The challenge presented evokes an adaptive response for the child. |
| Collaborate on activity choice and guide self-organization | Child is an active collaborator in the therapy session. The child selects activities and is encouraged to initiate activities. The therapist supports and guides the child in organizing his or her behavior, making choices, and planning activities. |
| Support optimal arousal and arrange room to engage child | During the session, the therapist supports the child’s optimal arousal and attention, engagement, and comfort. The room is arranged to engage the child’s attention and help him or her modulate sensory responses. |
| Create play context | The therapist creates a play context, building on the child’s intrinsic motivation using activities that the child enjoys. |
| Maximize child’s success | The therapist presents and modifies activities so that the child’s adaptive response is successful. |
| Ensure physical safety | The therapist ensures that the child is physically safe by using protective equipment and by maintaining physical proximity to the child. |
| Foster therapeutic alliance | The therapist conveys positive regard toward the child and makes efforts to build the child’s trust. |
Adapted from Parham, L. D., Cohn, E. S., Spitzer, S., Koomar, J. A., Miller, L. M., et al. (2007). Fidelity in sensory integration intervention research. American Journal of Occupational Therapy, 61, 216-227.
Early work by Ayres5,6 and others9,139 had reported positive changes resulting from sensory integration intervention in such outcomes as motor, academic, and language performance. Studies in the late 1980s and the 1990s evaluated the efficacy of sensory integration intervention using more rigorous methods, including randomized controlled trials. Using meta-analysis techniques, Vargas and Camilli found that early efficacy studies of sensory integration produced large positive effects, but studies conducted after 1982 did not yield significant positive effects.187 The more recent studies of sensory integration intervention have demonstrated effects equal to those of alternative treatments in the participants’ psychoeducational and motor performance areas, with no improvement noted in sensory perceptual areas.187
Recent studies using rigorous methods have shown positive effects of sensory integration interventions. In a randomized trial comparing sensory integration intervention to an activity protocol or no treatment, Miller, Coll, and Schoen assigned 24 children with sensory modulation disorders to one of three groups.126 The children in the sensory integration group and the activity group received intervention twice a week for 10 weeks, and the control group children were placed on a wait list for intervention. Those in the sensory integration intervention group made significant gains on goal attainment scaling and in attention, cognition, and social performance as measured by the Leiter International Performance Scale. Other measures of child behavior, sensory processing, and electrodermal reactivity improved in the sensory integration group but did not differ when the sensory integration group was compared with the activity and control groups. Miller et al. suggested that a larger sample was needed to detect significant differences in these measures.126
Although sensory integration research typically has demonstrated only small positive effects, sensory integration intervention is widely practiced by occupational therapists and is a powerful force in clinical reasoning in the field of pediatrics. In a survey of occupational therapists working with children with autism, fully 99% of the therapists reported using sensory integration techniques with their clients.190 More recent research has also included parents’ perceptions of change in their children and in themselves as a result of occupational therapy that used sensory integration intervention.38,39 Parents reported positive changes in their children’s social participation, perceived competence, and self-regulation. The parents valued the new understanding of the child’s behavior and used this perspective to support and advocate for the child more effectively. Ayres’ work has had a significant impact on occupational therapy practice with children, and its controversial nature has led to an increased sophistication and rigor in the scholarly work accomplished in the field of occupational therapy.
Developmental Approaches
During the 1960s and 1970s, occupational therapists working with children had a strong developmental perspective. These theories attempted to explain the functioning and growth of children and adolescents from an occupational therapy perspective. Perhaps the best-known occupational therapy theorist of this time was Lela Llorens. She identified a developmental frame of reference that focused on the physical, social, and psychologic aspects of life tasks and relationships.105,106 Llorens viewed the role of the occupational therapist to be one of facilitating development and assisting in the mastery of life tasks and the ability to cope with life expectations. Chapter 3 explains developmental theories used in occupational therapy.
The section on developmental theories presented earlier in this chapter provides a broad basis for occupational therapy evaluation and intervention. Specifically, the theories of Piaget145 form a foundation for the spatiotemporal adaptation model of practice.73 Piaget explained that the adaptation process has four components: assimilation, accommodation, association, and differentiation. Assimilation is the reception of sensory stimuli from internal and external environments. Accommodation is the motor response to these stimuli. Association is the organized process of relating current sensory information with the current motor response and then relating this relationship to past responses. Differentiation is the process of identifying the specific elements in a child’s situation that are useful and relevant to another situation to refine the responsive pattern. Based on prior experience, the child develops a sense of what is useful and what is not useful to motor activity in the current situation. In this view of development, the child is continually modifying older, more primitive behaviors for effective motor responses, rather than continually acquiring new skills. The spatiotemporal adaptation model of practice73 views development as a spiraling process, moving from simple to complex. Adaptation is a continuous process of interaction involving the individual, time, and space. This model became central to occupational therapists’ view of child development and fostered the development of intervention models.
Recent theories and models of development in the occupational therapy literature incorporate new concepts of PEO relationships, dynamic systems theories, and lifespan changes. Instead of focusing on different components of functioning, such as motor, social, or cognitive development, occupational therapy theorists are addressing the development of occupation across the lifespan.49,84,86
Two emerging occupational perspectives on development remain in the conceptual and exploratory stages of theory development and require further research and validation. In one of these proposals, Humphry suggests a dynamic system perspective in a model of developmental processes.84,85 A child’s occupational development is based on complex, reciprocal, and nonlinear relationships involving the child’s innate characteristics and environmental factors. Humphry proposes that children learn through three broad mechanisms. First, communities invest in children by developing programs, places, and opportunities for social engagement that enable them to participate in community life. Examples of community investment in child development include (1) child care centers that allow children with disabilities to attend their programming, (2) play spaces that use universal design allowing all children to use them, and (3) educational programs that encourage the participation of families with young children. Communities that are invested in child development support human resources, child-care centers, educational programs, and spaces that encourage healthy development and learning in children of all abilities. A second mechanism of child development are interpersonal influences (i.e., the social opportunities for children to interact with others). Children learn by observing others perform activity, through play with other children and adults, and through adults teaching and modeling for them. These social mechanisms are the catalyst for much of a child’s learning. Humphry noted that vicarious learning through observation of others can be as important as direct teaching.85 Children also learn through shared occupations such as circle time or group activities in preschool. Occupational therapists need to recognize the complexity of children’s learning across domains when children participate in groups.
Although vicarious learning in social situations is important to development, a third mechanism, doing, is equally important. When engaging in a novel activity, the child reorganizes learned skills, adapts skills on the basis of trial and error, and tries new actions to accomplish the activity. Fully engaging in an activity is an important catalyst to learning. To completely engage, the child must find the activity to be meaningful, fun, and challenging. These concepts about development of performance imply that children learn in social contexts and that engagement in activity results in learning. A variety of adult roles are implied by these concepts, including designing group activities, creating learning environments, modeling, encouraging, supporting, and guiding.
Occupational therapy approaches have logically evolved from theories and concepts of psychology, education, neuroscience, and other fields. These practice models guide interventions that consider the child, his or occupations, the environment, and the interactions of these elements. Practitioners recognize that theories are overlapping and complementary. To meet the individual needs of the children they serve, they use theoretical concepts specific to certain problems but also in combination. Occupational therapists seek evidence regarding each practice model’s effectiveness in making decisions about which model to implement.
CLINICAL APPLICATION EXAMPLES
In this section, three case studies are used to outline the different assessment and intervention strategies and expected outcomes for the models of practice discussed in the preceding section. The examples include a young child with cerebral palsy (Case Study 2-2), a school-aged child with DCD (Case Study 2-3), and an adolescent with sensory modulation and behavioral problems (Case Study 2-4). For each example, the most commonly used approaches are selected for the clinical situation. These choices do not mean that other approaches cannot be used, but they are applied less often.
Stacey is a 4-year-old girl who has cerebral palsy with moderate quadriplegia. She is able to walk short distances using a walker. She has difficulty controlling the movement of her arms and hands. Her parents have set current goals for Stacey that include participation in dressing tasks, drawing and cutting skills in preparation for kindergarten activities, and increased participation with peers in play. In this example, the focus is on the goal of participation in dressing and improved drawing and cutting skills (Table 2-7).
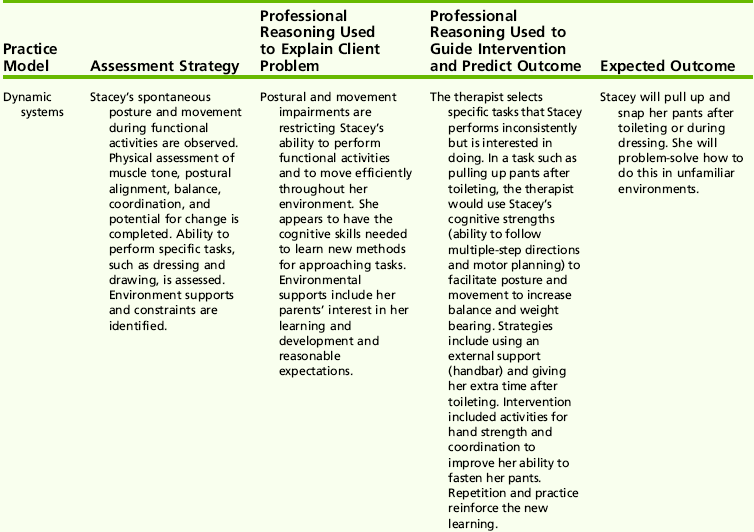
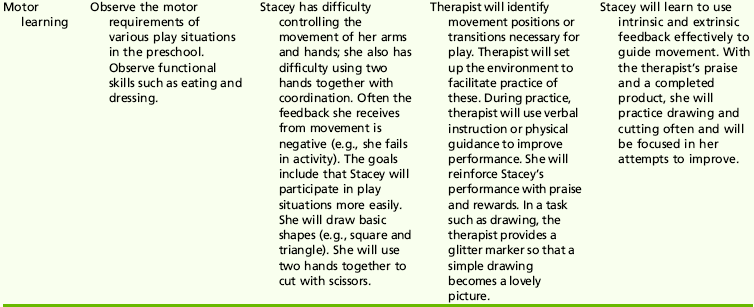
Brian is a 9-year-old boy with DCD. He is isolated from his peers at school, is clumsy, has difficulty performing any tasks requiring handwriting, is poorly organized, and has trouble staying on task (Table 2-8). A COPM was completed with Brian, and he identified the following occupational performance issues:
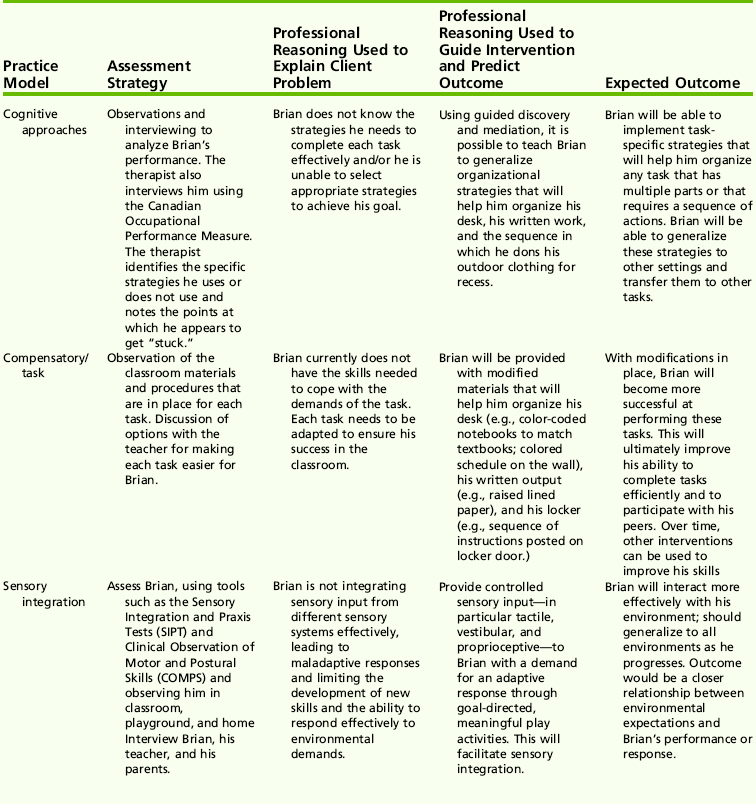
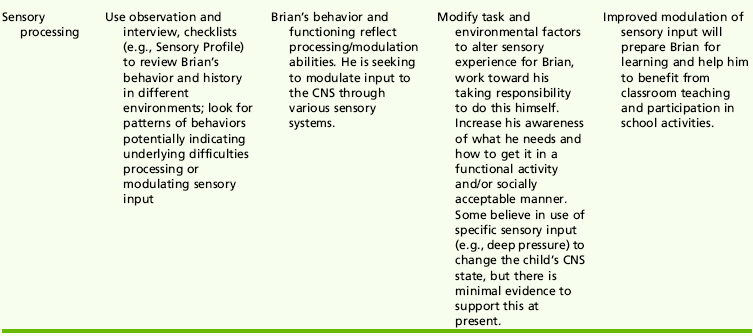
Chris is a 15-year-old high school student who is currently struggling to complete grade 10. He has dropped one subject in the current year and has been labeled an underachiever. He has difficulty taking notes in class and reorganizing his work. He has been referred to a community psychiatric service because of problems with low mood, lack of motivation in his academic and social life, poor social adjustment, and disturbed family relations.
His parents complain that Chris regularly lies to them about petty thefts from the home and that hours of confrontation and badgering by them are required to get the truth. They report various other instances of misbehavior. He presents himself as a somewhat disheveled youth who denies any knowledge or insight into his difficulties. His parents are eager in seeking intervention to improve his success in school and his behavior at home (Table 2-9).
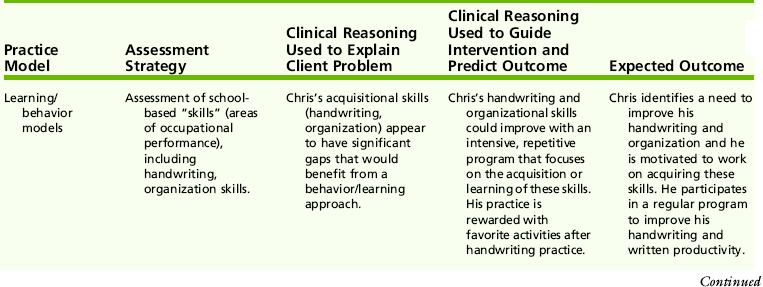
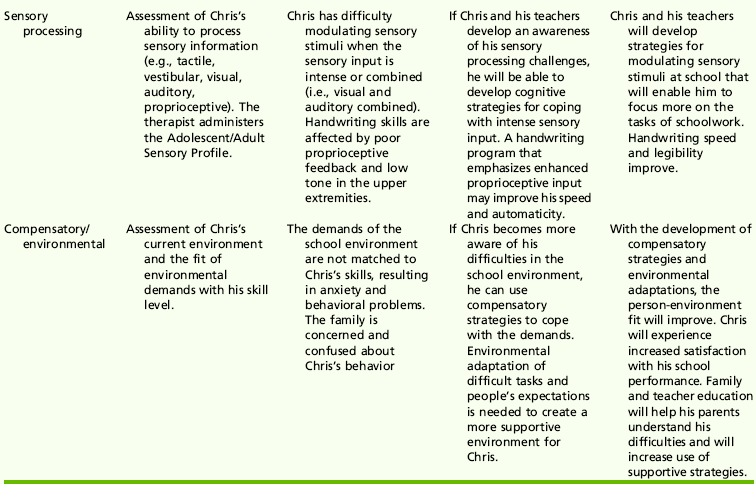
REFERENCES
1. Adams, J.A. A closed-loop theory of motor learning. Journal of Motor Behavior. 1971;3:111–149.
2. American Occupational Therapy Association, Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy, 2008;62:625–683.
3. Ayres, A.J. Deficits in sensory integration in educationally handicapped children. Journal of Learning Disabilities. 1969;2:160–168.
4. Ayres, A.J. Sensory integration and learning disorders. Los Angeles: Western Psychological Services, 1972.
5. Ayres, A.J. Improving academic scores through sensory integration. Journal of Learning Disabilities. 1972;5:338–343.
6. Ayres, A.J. Learning disabilities and the vestibular system. Journal of Learning Disabilities. 1978;11:18–29.
7. Ayres, A.J. Sensory integration and the child. Los Angeles: Western Psychological Services, 1979.
8. Ayres, A.J. Sensory Integration and Praxis Tests. Los Angeles: Western Psychological Services, 1989.
9. Ayres, A.J., Mailloux, Z.K. Influence of sensory integrative procedures on language development. American Journal of Occupational Therapy. 1981;35:383–390.
10. Ayres, A.J., Tickle, L. Hyperresponsivity to touch and vestibular stimuli as a predictor of positive response to sensory integration procedures in autistic children. American Journal of Occupational Therapy. 1980;34:375–381.
11. Bandura, A. Perceived self-efficacy in cognitive development and functioning. Educational Psychologist. 1993;28:117–148.
12. Bandura, A. Self-efficacy: The exercise of control. New York: Freeman, 1997.
13. Bandura, A., Barbaranelli, C., Caprara, G.V., Pasatorelli, C. Multifaceted impact of self-efficacy beliefs on academic functioning. Child Development. 1996;67:1206–1222.
14. Baranek, G.T., Foster, L.G., Berkson, G. Sensory defensiveness in persons with developmental disabilities. Journal of Autism and Developmental Disorders. 1997;29:213–224.
15. Barchers, S.I. Teaching language arts: An integrated approach. Minneapolis: West Publishing, 1994.
16. Bedell, G.M., Cohn, E.S., Dumas, H.M. Exploring parents’ use of strategies to promote social participation of school-age children with acquired brain injuries. American Journal of Occupational Therapy. 2005;59:65–75.
17. Bedell, G.M., Dumas, H.M. Social participation of children and youth with acquired brain injuries discharged from inpatient rehabilitation: A follow-up study. Brian Injury. 2004;18:65–82.
18. Bergman, K.E., McLaughlin, T.F. Remediating handwriting difficulties with learning disabled students: A review. Journal of Special Education. 1988;12:101–120.
19. Bernheimer, L.P., Weisner, T.S. Let me just tell you what I do all day…”: The family story at the center of intervention research and practice. Infants & Young Children. 2007;20(3):192–201.
20. Bernstein, N. Coordination and regulation of movements. New York: John Wiley & Sons, 1967.
21. Bjorklund, D.F., Green, B.L. The adaptive nature of cognitive immaturity. American Psychologist. 1992;47:46–54.
22. Blanche, E.I. Play in children with cerebral palsy: Doing with—not doing to. In: Parham D.L., Fazio L., eds. Play and occupational therapy. 2nd ed. St. Louis: Mosby; 2008:375–394.
23. Bobath, K. A neurophysiological basis for the treatment of cerebral palsy. London: Heinemann Books, 1980.
24. Broderick, C., Caswell, R., Gregory, S., Marzolini, S., Wilson, O. Can I join the club”: A social integration scheme for adolescents with Asperger syndrome. Autism. 2002;5:427–431.
25. Bronfenbrenner, U. Toward an experimental ecology of human development. American Psychologist. 1977;32:513–531.
26. Burton, A.W., Davis, W.E. Ecological task analysis: Utilizing intrinsic measures in research and practice. Human Movement Science. 1996;15:285–314.
27. Burton, A.W., Miller, D.E. Movement skill assessment. Champaign, IL: Human Kinetics, 1998.
28. Butler, C., Darrah, J. Effects of neurodevelopmental treatment (NDT) for cerebral palsy: An AACPDM evidence report. Developmental Medicine and Child Neurology. 2001;43(11):778–790.
29. Campbell, P.H., Milbourne, S., Wilcox, M.J. Adaptation interventions to promote participation in natural settings. Infants & Young Children. 2008;21:94–106.
30. Canadian Association of Occupational Therapists (CAOT). Enabling occupation: An occupational therapy perspective. Ottawa, ON: Canadian Association of Occupational Therapists (CAOT), 1997.
31. Case-Smith, J. Analysis of current motor development theory and recently published infant motor assessments. Infants and Young Children. 1996;9(1):29–41.
33. Christiansen, C., Baum, C. Occupational therapy: Enabling function and well-being. Thorofare, NJ: Slack, 1997.
34. Christiansen, C.H., Clark, F., Kielhofner, G., Rogers, J. Position paper: Occupation. American Journal of Occupational Therapy. 1995;49:1015–1018.
35. Christopher, J.S., Nangle, D.W., Hansen, D.J. Social skills interventions with adolescents. Behavior Modification. 1993;17:314–338.
36. Clark, F.A., Parham, D., Carlson, M.E., Frank, G., Jackson, J., Pierce, D., et al. Occupational science: Academic innovation in the service of occupational therapy’s future. American Journal of Occupational Therapy. 1991;45:300–310.
37. Cohen, L.B., Cashon, C.H., Infant perception and cognition. Lerner, R.M., Easterbrooks, M.A., Mistry, J., eds. Handbook of psychology: Developmental psychology, Hoboken, NJ, John Wiley & Sons, Inc, 2003;Vol. 6:65–90.
38. Cohn, E.S. Parent perspectives of occupational therapy using a sensory integration approach. American Journal of Occupational Therapy. 2001;55:285–294.
39. Cohn, E., Miller, L.J., Tickle-Degnen, L. Parental hopes for therapy outcomes: Children with sensory modulation disorders. American Journal of Occupational Therapy. 2000;54:36–43.
40. Cooper, J.O., Heron, T.E., Heward, W.L. Applied behavior analysis. Upper Saddle River, NJ: Pearson Merrill Prentice Hall, 2007.
41. Coster, W., Deeny, T., Haltiwanger, J., Haley, S. School Function Assessment. San Antonio, TX: Psychological Corporation, 1998.
42. Couch, K.J., Deitz, J.C., Kanny, E.M. The role of play in pediatric occupational therapy. American Journal of Occupational Therapy. 1998;52:111–117.
43. Cowan, R.J., Allen, K.D. Using naturalistic procedures to enhance learning in individuals with autism: A focus on generalized teaching within the school setting. Psychology in the Schools. 2007;44:701–715.
44. Crepeau, E.B., Schell, B.A.B. Analyzing occupations and activity. In: Crepeau E.B., Cohn E.S., Schell B.A.B., eds. Willard & Spackman’s occupational therapy. 11th ed. Philadelphia: Lippincott Williams & Wilkins; 2008:359–374.
45. Csikszentmihalyi, M., Csikszentmihalyi, I.S. Optimal experience: Psychological studies in flow in consciousness. Cambridge, UK: Cambridge University Press, 1988.
46. Darrah, J., Barlett, D. Dynamic systems theory and management of children with cerebral palsy: unresolved issues. Infants and Young Children. 1995;8:52–59.
47. Darrah, J., Law, M., Pollock, N. Innovations in practice: Family-centered functional therapy—a choice for children with motor dysfunction. Infants and Young Children. 2001;13(4):79–87.
48. D’Avignon, M. Early physiotherapy ad modum Vojta or Bobath in infants with suspected neuromotor disturbance. Neuropediatrics. 1981;12:232–241.
49. Davis, J., Polatajko, H. The occupational development of children. In: Rodger S., Ziviani J., eds. Occupational therapy with children: Understanding children’s occupations and enabling participation. Oxford, UK: Blackwell Publishing; 2006:136–156.
50. DeGrace, B.W. Occupation-based and family centered care: A challenge for current practice. American Journal of Occupational Therapy. 2003;57:347–350.
51. DeGrace, B.W. The everyday occupation of families with children with autism. American Journal of Occupational Therapy. 2004;58:543–550.
52. Denton, P., Cope, S., Moser, C. Effects of sensorimotor-based intervention versus therapeutic practice on improving handwriting performance in 6-to-11-year-old children. American Journal of Occupational Therapy. 2006;60:16–27.
53. Dunn, W. The impact of sensory processing abilities on the daily lives of young children and their families: A conceptual model. Infants and Young Children. 1997;9:23–35.
54. Dunn, W. The Sensory Profile User’s Manual. San Antonio, TX: Psychological Corporation, 1999.
55. Dunn, W. The sensations of everyday life: Empirical, theoretical, and pragmatic considerations. American Journal of Occupational Therapy. 2001;66:608–620.
56. Dunn, W., Brown, C. Factor analysis on the sensory profile from a national sample of children without disabilities. American Journal of Occupational Therapy. 1997;51:490–495.
57. Dunn, W., Brown, C., McGuigan, A. The ecology of human performance: A framework for considering the effect of context. American Journal of Occupational Therapy. 1994;48:595–607.
58. Dunst, C.J., Trivette, C.M., Davis, M., Cornwall, J. Enabling and empowering families of children with health impairments. Child Health Care. 1988;17:71–81.
59. Dunst, C., Trivette, C., Deal, A. Supporting and strengthening families: Methods, strategies and practices. Cambridge, MA: Brookline Books, 1994.
60. Dunton, W.R. Reconstruction therapy. Philadelphia: W.B. Saunders, 1919.
61. Engel-Yeger, B., Jarus, T., Anaby, D., Law, M. Differences in patterns of participation between youths with cerebral palsy and typically developing peer. American Journal of Occupational Therapy. 2009;63:96–104.
62. Engle, P.L., Castle, S., Meno, P. Child development: Vulnerability and resilience. Social Science and Medicine. 1996;43(5):621–635.
63. Ermer, J., Dunn, W. The Sensory Profile: A discriminant analysis of children with and without disabilities. American Journal of Occupational Therapy. 1997;51:283–290.
64. Evans, J.L. Variability in comprehension strategy use in children with SLI: A dynamical systems account. International Journal of Language and Communication Disorders. 2002;37(2):95–116.
65. Fidler, G.S., Fidler, J.W. Doing and becoming: Purposeful action and self-actualization. American Journal of Occupational Therapy. 1978;32:305–310.
66. Fine, S., Forth, A., Gilbert, M., Haley, G. Group therapy for adolescent depressive disorder: A comparison of social skills and therapeutic support. Journal of the American Academy of Child and Adolescent Psychiatry. 1991;30:79–85.
67. Flavell, J. Cognitive development. Englewood Cliffs, NJ: Prentice-Hall, 1985.
68. Garmezy, N. Stress-resistant children: The search for protective factors. In: Stevenson J.E., ed. Recent research in developmental psychopathology. Journal of Child Psychology and Psychiatry Book. Oxford, UK: Pergamon Press; 1985:213–233. [Suppl. 4].
69. Gentile, A.M. Implicit and explicit processes during acquisition of functional skills. Scandinavian Journal of Occupational Therapy. 1998;5:7–16.
70. Gesell. The embryology of behavior: the beginnings of the human mind. New York: Harper & Brothers, 1945.
71. Gibson, E. Exploratory behavior in the development of perceiving, acting and acquiring of knowledge. Annual Review of Psychology. 1988;39:1–41.
72. Gibson, J. The ecological approach to visual perception. Boston: Houghton-Mifflin, 1979.
73. Gilfoyle, E.M., Grady, A.P., Moore, J.C. Children adapt, 2nd ed. Thorofare, NJ: Slack, 1990.
74. Glang, A., Todis, B., Cooley, E., Wells, J., Voss, J. Building social networks for children and adolescents with traumatic brain injury: A school-based intervention. Journal of Head Trauma Rehabilitation. 1997;12:32–47.
75. Haley, S.M., Coster, W.J., Ludlow, L.H., Haltiwanger, J., Andrellos, P. Administrative manual for the Pediatric Evaluation of Disability Inventory. San Antonio, TX: Psychological Corporation, 1992.
76. Hall, C.S., Lindzey, G. Theories of personality, 3rd ed. New York: John Wiley & Sons, 1978.
77. Hanft, B.E., Rush, D.D., Shelden, M.L. Coaching families and colleagues in early intervention. Baltimore, MD: Brookes Publishing, 2004.
78. Hansen, D.J., Watson-Perczel, M., Christopher, J.S. Clinical issues in social skills training with adolescents. Clinical Psychology Review. 1989;9:365–391.
79. Harter, S. Effectance motivation reconsidered: Toward a developmental model. Human Development. 1978;21:34–64.
80. Hayes, R.L., Halford, W.K., Varghese, F.N. Generalization of the effects of activity therapy and social skills training on the social behavior of low functioning schizophrenic patients. Occupational Therapy in Mental Health. 1991;11:3–20.
81. Rogers, J.C., Holm, M.B. The occupational therapy process. In: Crepeau E.B., Cohn E.S., Schell B.A.B., eds. Willard & Spackman’s occupational therapy. Philadelphia: Lippincott Williams & Wilkins; 2009:22–32.
82. Howle, J.M. Neurodevelopmental treatment approach: Theoretical foundations and principles of clinical practice. Laguna Beach, CA: Neuro-Developmental Treatment Association, 2002.
83. Howlin, P., Yates, P. The potential effectiveness of social skills group for adults with autism. Autism. 1999;3:299–307.
84. Humphry, R. Young children’s occupations: Explicating the dynamics of developmental processes. American Journal of Occupational Therapy. 2002;56:171–179.
85. Humphry, R. Occupation and development: A contextual perspective. In: Crepeau E.B., Cohn E.S., Schell B.A.B., eds. Willard & Spackman’s occupational therapy. Philadelphia: Lippincott Williams & Wilkins; 2009:22–32.
86. Humphry, R., Wakeford, L. An occupation-centered discussion of development and implications for practice. American Journal of Occupational Therapy. 2006;60:258–267.
87. Hyatt, G.B. Occupational therapy: Can doses be exact? Occupational Therapy and Rehabilitation. 1946;25:57–61.
88. Keintz, M.A., Dunn, W. A comparison of the performance of children with and without autism on the Sensory Profile. American Journal of Occupational Therapy. 1997;51:530–537.
89. Ketelaar, M., Vermeer, A., Hart, H., van, E., Helders, P. Effects of a functional therapy program on motor abilities of children with cerebral palsy. Physical Therapy. 2001;81:1534–1545.
90. Kielhofner, G. A model of human occupation: Theory and application, 4th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2006.
91. Kielhofner, G., Burke, J. A model of human occupation. Part 1. Conceptual framework and content. American Journal of Occupational Therapy. 1980;34:572–581.
92. King, G., King, S., Rosenbaum, P., Goffin, R. Family-centred care-giving and wellbeing of parents of children with disabilities: Linking process with outcome. Journal of Pediatric Psychology. 1999;24:41–53.
93. Koegel, R.L., Koegel, L.K. Pivotal response treatment for autism: Communication, social, and academic development. Baltimore, MD: Brookes, 2006.
94. Koegel, R.L., Koegel, L.K., Carter, C.M. Pivotal teaching interactions for children with autism. School Psychology Review. 1999;28:576–594.
95. Krantz, M. Child development: Risk and opportunity. Belmont, CA: Wadsworth, 1994.
96. Law, M. Participation in the occupations of everyday life. American Journal of Occupational Therapy. 2002;56:640–649.
98. Law, M., Cadman, D., Rosenbaum, P., DeMatteo, C., Walter, S., Russell, D. Neurodevelopmental therapy and upper extremity casting: Results of a clinical trial. Developmental Medicine and Child Neurology. 1991;33:334–340.
99. Law, M., Cooper, B., Strong, S., Stewart, D., Rigby, P., Letts, L. The person-environment-occupation model: A transactive approach to occupational performance. Canadian Journal of Occupational Therapy. 1996;63(1):9–23.
100. Law, M., Hanna, S., King, G., Hurley, P., King, S., Kertoy, M., et al. Factors affecting family-centred service delivery for children with disabilities. Child Care Health and Development. 2003;29:41–53.
101. Law, M., King, G., Kind, S., Kertoy, M., Hurley, P., Rosenbaum, P., et al. Patterns of participation in recreation and leisure activities among children with complex physical disabilities. Development Medicine and Child Neurology. 2006;48:337–342.
102. Lee, T.D., Swinnen, S.P., Serrien, D.J. Cognitive effort and motor learning. Quest. 1994;46:328–344.
103. Lefebvre, C., Reid, G. Prediction in ball catching by children with and without a developmental coordination disorder. Adapted Physical Activity Quarterly. 1998;15:299–315.
104. Linder, T.W. Transdisciplinary play-based assessment, 2nd ed. Baltimore, MD: Brookes, 2008.
105. Llorens, L.A. Application of developmental theory for health and rehabilitation. Rockville, MD: American Occupational Therapy Association, 1976.
106. Llorens, L.A. Performance tasks and roles throughout the life span. In: Christiansen C., Baum C., eds. Occupational therapy: Overcoming human performance deficits. Thorofare, NJ: Slack; 1991:45–68.
107. Lollar, D.J., Simeonsson, R.J. Diagnosis to function: Classification for children and youths. Developmental and Behavioral Pediatrics. 2005;26:323–330.
108. Luria, A. The role of speech in the regulation of normal and abnormal behaviors. New York: Liveright, 1961.
109. Luthar, S.S., Resilience in development: A synthesis of research across five decades. Cicchetti, D., Cohen, D., eds. Developmental psychopathology: Risk, disorder, and adaptation, 2nd ed., Vol. 3. Hoboken, NJ: John Wiley & Sons, Inc, 2006;739–795.
110. Luthar, S.S., Zelazo, L.M. Research on resilience: An integrative review. In: Luthar S.S., ed. Resilience and vulnerability: Adaptation in the context of childhood adversities. New York: Cambridge University Press; 2003:510–549.
111. Lyons, B.G. Defining a child’s zone of proximal development: Evaluation process for treatment planning. American Journal of Occupational Therapy. 1984;38:446–451.
112. Ma, H., Trombly, C.A., Robinson-Podolski, C. The effect of context on skill acquisition and transfer. American Journal of Occupational Therapy. 1999;53:138–144.
113. Maher, C.A., Williams, M.T., Olds, T., Lane, A.E. Physical and sedentary activity in adolescents with cerebral palsy. Developmental Medicine & Child Neurology. 2007;29:450–457.
114. Mahoney, G., O’Sullivan, P. Early intervention practices with families of children with handicaps. Mental Retardation. 1990;28:169–176.
115. Mahoney, G., Perales, F. Relationship-focused early intervention with children with pervasive developmental disorders and other disabilities: A comparative study. Developmental and Behavioral Pediatrics. 2005;26:77–85.
116. Mandich, A., Polatajko, H., Missiuna, C., Miller, L. Cognitive strategies and motor performance in children with developmental coordination disorder. Physical and Occupational Therapy in Pediatrics. 2001;20(2/3):125–143.
117. Mandich, A., Roger. Doing, being and becoming: Their importance for children. In: Rodger S., Ziviani J., eds. Occupational therapy with children: Understanding children’s occupations and enabling participation. Oxford, UK: Blackwell Publishing Ltd; 2006:115–135.
118. Maslow, A.H. Toward a psychology of being. Princeton, NJ: Van Nostrand, 1968.
119. Maslow, A.H. Motivation and personality. New York: Harper & Row, 1970.
120. Masten, A.S., Reed, M.G.J. Resilience in development. In: Snyder C.R., Lopez S.J., eds. Handbook of positive psychology. New York: Oxford University Press; 2002:74–88.
121. Mayo, N.E. The effect of physical therapy for children with motor delay and cerebral palsy. American Journal of Physical Medicine and Rehabilitation. 1991;70:258–267.
122. McColl, M., Law, M., Stewart, D., Doubt, L., Pollock, N., Krupa, T. Theoretical basis of occupational therapy, 2nd ed. Thorofare, NJ: Slack, 2003.
123. Meichenbaum, D. Cognitive-behavior modification: An integrative approach. New York: Plenum Press, 1977.
124. Meyer, A. The philosophy of occupational therapy. Archives of Occupational Therapy. 1922;1:1–10.
125. Miller, L., Anzalone, M., Lane, S., Cermak, S., Osten, B. Typology and terminology of sensory integration. American Journal of Occupational Therapy. 2007;61(2):135–140.
126. Miller, L.J., Coll, J.R., Schoen, S.A. A randomized controlled pilot study of the effectiveness of occupational therapy for children with sensory modulation disorder. American Journal of Occupational Therapy. 2007;61:228–238.
127. Miller, L., Polatajko, H., Missiuna, C., Mandich, A., Macnab, J., Malloy-Miller, T. A pilot trial of a cognitive treatment for children with developmental coordination disorder. Human Movement Science. 2001;20:183–210.
128. Miller, L.J., Wilbarger, J., Stackhouse, T., Trunnell, S. Clinical reasoning in occupational therapy: The STEP-SI model of intervention of sensory modulation dysfunction. In: Bundy A., Lane S., Murray E., eds. Sensory integration therapy and practice. 2nd ed. Philadelphia: F.A. Davis; 2002:435–451.
129. Milone, M.N., Jr., Waslyk, T.M. Handwriting in special education. Teaching Exceptional Children. 1981;14:58–61.
130. Missiuna, C., Malloy-Miller, T., Mandich, A. Mediational techniques: Origins and application to occupational therapy in pediatrics. Canadian Journal of Occupational Therapy. 1998;65:202–209.
131. Missiuna, C., Mandich, A., Polatajko, P., Malloy-Miller, T. Cognitive orientation to daily occupational performance (CO-OP). Part 1. Theoretical foundations. Physical and Occupational Therapy in Pediatrics. 2001;20(2/3):69–81.
132. Missiuna, C., Pollock, N. Perceived efficacy and goal setting in young children. Canadian Journal of Occupational Therapy. 2000;67:101–109.
133. Mitchell, P.R. A dynamic interactive developmental view of early speech and language production: Application to clinical practice in motor speech disorders. Seminars in Speech & Language. 1995;16:100–109.
134. Mulligan, S. Patterns of sensory integration dysfunction: A confirmatory factor analysis. American Journal of Occupational Therapy. 1998;52:819–828.
135. Newacheck, P., Halfon, N. Prevalence and impact of disabling chronic conditions in childhood. American Journal of Public Health. 1998;88(4):610–617.
136. Nicholson, D.E. Motor learning. In: Fredericks C.M., Saladin L.K., eds. Pathophysiology of the motor systems: Principles and clinical presentations. Philadelphia: F.A. Davis; 1996:238–254.
137. Nudo, R.J. Plasticity. NeuroRx. 2006;3:420–427.
138. Ormrod, J.E. Educational psychology: Developing learners, 5th ed. Upper Saddle River, NJ: Prentice Hall, 2006.
139. Ottenbacher, K., Short, M.A., Watson, P.J. Nystagmus duration changes in learning disabled children during sensory integrative therapy. Perceptual and Motor Skills. 1979;48:1159–1164.
140. Palisano, R.J., Copeland, W.P., Galuppi, B.E. Performance of physical activities by adolescents with cerebral palsy. Physical Therapy. 2007;87:77–87.
141. Palmer, F.B., Shapiro, B.K., Wachtal, R.C., Allen, M.C., Hiller, J.E., Harryman, S.E., et al. The effects of physical therapy on cerebral palsy: A controlled trial in infants with spastic diplegia. New England Journal of Medicine. 1988;318:903–908.
142. Parham, L.D. Play and occupational therapy. In: Parham L.D., Fazio L., eds. Play in occupational therapy for children. 2nd ed. St. Louis: Elsevier; 2008:3–42.
143. Parham, L.D., Cohn, E.S., Spitzer, S., Koomar, J.A., Miller, L.M., et al. Fidelity in sensory integration intervention research. American Journal of Occupational Therapy. 2007;61:216–227.
144. Piaget, J. The origins of intelligence in children. New York: International Universities, 1952.
145. Piaget, J. Psychology and epistemology: Towards a theory of knowledge. New York: Viking Press, 1971.
146. Piper, M.C. Efficacy of physical therapy: Rate of motor development in children with cerebral palsy. Pediatric Physical Therapy. 1990;2:126–130.
147. Piper, M.C., Darrah, J. Motor assessment of the developing infant. Philadelphia: W.B. Saunders, 1994.
148. Pless, I.B., Cripps, H.A., Davies, J.M.C., Wadsworth, M.E.J. Chronic physical illness in childhood: Psychological and social effects in adolescence and adult life. Developmental Medicine and Child Neurology. 1989;31:746–755.
149. Polatajko, H.J., Mandich, A.D., Miller, L.T., Macnab, J.J. Cognitive orientation to daily occupational performance (CO-OP). Part 2. The evidence. Physical and Occupational Therapy in Pediatrics. 2001;20(2/3):83–106.
150. Polatajko, H.J., Mandich, A.D., Missiuna, C., Miller, L.T., Macnab, J., Malloy-Miller, T. Cognitive orientation to daily occupational performance (CO-OP). Part 3. The protocol in brief. Physical and Occupational Therapy in Pediatrics. 2001;20(2/3):107–123.
151. Poulson, A., Ziviani, J. Can I play too? Physical activity engagement patterns of children with developmental coordination disorders. Canadian Journal of Occupational Therapy. 2004;71:100–107.
152. Reed, M.K. Social skills training to reduce depression in adolescents. Adolescence. 1994;29:293–302.
153. Reilly. A psychiatric occupational therapy program as a teaching model. American Journal of Occupational Therapy. 1966;20:62–67.
154. Reilly. The educational process. American Journal of Occupational Therapy. 1969;23:299–307.
155. Reilly. Play as exploratory learning. Beverly Hills, CA: Sage Publications, 1974.
156. Reilly. Occupational behavior: A perspective on work and play. American Journal of Occupational Therapy. 1974;25:291–296.
157. Richmond, J.B., Beardslee, W.R. Resiliency: Research and practical implications for pediatricians. Journal of Developmental and Behavioral Pediatrics. 1988;9:157–163.
158. Rigby, P., Letts, L. Environment and occupational performance: Theoretical considerations. In: Letts L., Rigby P., Stewart D., eds. Using environments to enable occupational performance. Thorofare, NJ: Slack; 2003:17–32.
159. Rodger, S., Brandenburg, J. Cognitive Orientation to (daily) Occupational Performance (CO-OP) with children with Asperger’s syndrome who have motor-based occupational performance goals. Australian Occupational Therapy Journal. 2009;56:41–50.
160. Rodger, S., Springfield, E., Polatajko, H. Cognitive orientation for daily occupational performance approach for children with Asperger’s syndrome: A case report. Physical and Occupational Therapy in Pediatrics. 2007;27:7–22.
161. Rosenbaum, P., King, S., Law, M., King, G., Evans, J. Family-centred service: A conceptual framework and research review. Physical and Occupational Therapy in Pediatrics. 1998;18:1–20.
162. Rutter, M. Psychosocial resilience and protective mechanisms. In: Rolf J., Masten A.S., Cicchetti D., Nuechterlein K., Weintraub S., eds. Risk and protective factors in the development of psychopathology. Cambridge, UK: Cambridge University Press; 1990:181–214.
163. Sandler, I. Quality and ecology of adversity as common mechanisms of risk and resilience. American Journal of Community Psychology. 2001;29(1):19–61.
164. Schaaf, R.C., Nightlinger, K.M. Occupational therapy using a sensory integrative approach: A case study of effectiveness. American Journal of Occupational Therapy. 2007;61:239–246.
165. Schertz, M., Gordon, A.M. Changing the model: A call for a re-examination of intervention approaches and translational research in children with developmental disabilities. Developmental Medicine & Child Neurology. 2009;51:6–7.
166. Scherzer, A.L., Mike, V., Ilson, J. Physical therapy as a determinant of change in the cerebral palsied infant. Pediatrics. 1976;53:47–52.
167. Schmidt, R.A. Motor control and learning: A behavioral emphasis. Champaign, IL: Human Kinetics, 1988.
168. Shikako-Thomas, K., Majnemer, A., Law, M., Lach, L. Determinants of participation in leisure activities in children and youth with cerebral palsy: Systematic review. Physical and Occupational Therapy in Pediatrics. 2008;28:155–170.
169. Shumway-Cook, A., Woollacott, M.H. Motor control: Translating research into clinical practice. Baltimore, MD: Lippincott Williams & Wilkins, 2006.
170. Skinner, B.F. Science and human behavior. New York: Free Press, 1953.
171. Skinner, B.F. Walden two. New York: Macmillan, 1976.
172. Slagle, E.C. Training aides for mental patients. Archives of Occupational Therapy. 1922;1:11–17.
173. Sloper, P., Turner, S., Knussen, C., Cunningham, C. Social life of school children with Down’s syndrome. Child: Care. Health and Development. 1990;16(4):235–251.
174. Sommerfeld, D., Fraser, B.A., Hensinger, R.N., Beresford, C.V. Evaluation of physical therapy service for severely mentally impaired students with cerebral palsy. Physical Therapy. 1981;61:338–344.
175. Spitzer, S.L. Play in children with autism: Structure and experience. In Parham L.D., Fazio L., eds.: Play in occupational therapy for children, 2nd ed., St. Louis: Elsevier, 2008.
176. Stewart, D., Law, M. The environment: Paradigms and practice in health, occupational therapy and inquiry. In: Letts L., Rigby P., Stewart D., eds. Using environments to enable occupational performance. Thorofare, NJ: Slack; 2003:3–15.
177. Sugden, D.A., Sugden, L. The assessment and management of movement skill problems. Leeds, UK: School of Education, 1990.
178. Sullivan, K.J., Kantak, S.S., Burtner, P.A. Motor learning in children: Feedback effects on skills acquisition. Physical Therapy. 2008;88:720–732.
179. Taylor, S., Fayed, N., Mandrich, A. CO-OP intervention for young children with developmental coordination disorder. OTJR: Occupation, Participation and Health. 2007;27:124–130.
180. Thelen, E. Motor development: A new synthesis. American Psychologist. 1995;50(2):79–95.
181. Thelen, E., Schoner, G., Scheier, C., Smith, L. The dynamics of embodiment: A field theory of infant preservative reaching. Behavioral and Brain Sciences. 2001;24:1–86.
182. Thelen, E., Spencer, J.P. Postural control during reaching in young infants: A dynamic systems approach. Neuroscience and Behavioral Reviews. 1998;22:507–514.
183. Tomchek, S.D., Dunn, W. Sensory processing in children with and without autism: A comparative study using the Short Sensory Profile. American Journal of Occupational Therapy. 2007;61:190–200.
184. Vanderbilt-Adriance, E., Shaw, D.S. Conceptualizing and re-evaluating resilience across levels of risk, time, and domains of competence. Clinical Child and Family Psychology Review. 2008;11:30–58.
185. Van Gelder, T. What might cognition be, if not computation? Journal of Philosophy. 1995;91:345–381.
186. VanSant, A.F. Neurodevelopmental treatment and pediatric physical therapy: A commentary. Pediatric Physical Therapy. 1991;3:137–141.
187. Vargas, S., Camilli, G. A meta-analysis of research on sensory integration treatment. American Journal of Occupational Therapy. 1999;53:180–198.
188. Vygotsky, L.S. Mind in society: The development of higher mental processes. Mind in society: The development of higher mental processes. Cambridge, MA: Harvard University Press, 1978.
189. Wallander, J., Varni, J. Social support and adjustment in chronically ill and handicapped children. American Journal of Community Psychology. 1989;17(2):185–201.
190. Watling, R., Deitz, J., Kanny, E.M., McLaughlin, J.F. Current practice of occupational therapy for children with autism. American Journal of Occupational Therapy. 1999;53:498–505.
191. Watling, R., Deitz, J., White, O. Comparison of sensory profile scores of young children with and without autism spectrum disorders. American Journal of Occupational Therapy. 2001;55:416–423.
192. Werner, E.E. High-risk children in young adulthood: A longitudinal study from birth to 32 years. American Journal of Orthopsychiatry. 1989;59:72–81.
193. Werner, E.E. Overcoming the odds. Developmental and Behavioral Pediatrics. 1994;15:131–136.
194. Wertsch, J.V. From social interaction to higher psychological processes: A clarification and application of Vygotsky’s theory. Human Development. 2008;51:66–79.
195. Wilcock, A. A theory of human need for occupation. Occupational Science: Australia. 1993;1:17–24.
196. Wilcock, A. Reflections on doing, being, becoming. Canadian Journal of Occupational Therapy. 1998;65:248–256.
197. Wilcock, A., Townshend, E. Occupational justice. In: Crepeau E.B., Cohn W.S., Schell B.B., eds. Willard & Spackman’s occupational therapy. 11th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2008:192–199.
198. Williams, M.S., Shellenberger, S. How does your engine run? A leader’s guide to the alert program for self-regulation. Albuquerque, NM: Therapy Works, 1994.
199. Williamson, G., Szczepanski, M. Coping frame of reference. In: Kramer P., Hinojosa J., eds. Frames of reference in pediatric occupational therapy. Baltimore, MD: Williams & Wilkins; 1999:431–465.
200. Winstein, C.J., Merians, A.S., Sullivan, K.J. Motor learning after unilateral brain damage. Neuropsychologia. 1999;37:975–987.
201. World Health Organization. International classification of impairments, disability and handicap. Geneva, Switzerland: World Health Organization, 1980.
202. World Health Organization. International classification of disability, functioning and health. Geneva, Switzerland: World Health Organization, 2001.
203. Yerxa, E.J. Authentic occupational therapy. American Journal of Occupational Therapy. 1967;21:1–9.
204. Yerxa, E.J., Clark, F., Frank, G., Jackson, J., Parham, D., Pierce, D., et al. Occupational science: The foundation for new models of practice. Occupational Therapy in Health Care. 1989;6:1–17.
205. Zeitlin, S., Williamson, G.G. Coping in young children: Early intervention practices to enhance adaptive behavior and resilience. Baltimore, MD: Brookes, 1994.
206. Zeitlin, S., Williamson, G.G., Szczepanski, M. Early coping inventory. Bensenville, IL: Scholastic Testing Service, 1988.