The renal system
Renal examination
Anatomy
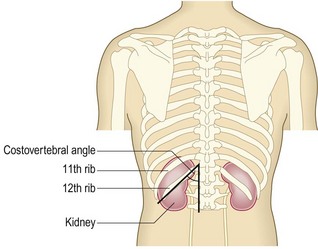
The kidneys lie posteriorly in the abdomen, retroperitoneally on either side of the spine at the T12–L3 level (Fig. 9.1) and are 11–14 cm long. The right kidney lies 1.5 cm lower than the left because of the liver. The liver and spleen lie anterior to the kidneys. The kidneys move downwards during inspiration as the lungs expand.
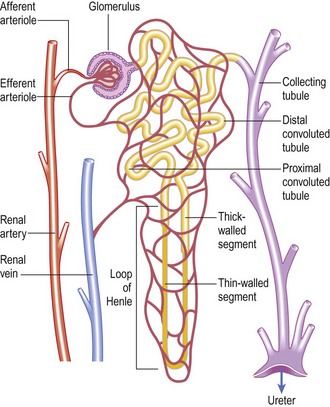
Together, the kidneys receive ~25% of cardiac output. Each kidney contains about one million nephrons, each comprising a glomerulus, proximal tubule, loop of Henle, distal tubule and collecting duct (Fig. 9.2). Urine is formed by glomerular filtration, modified by complex processes of secretion and reabsorption in the tubules, and then enters the calyces and the renal pelvis.
The primary functions of the kidneys are:
• excretion of waste products of metabolism such as urea and creatinine
• maintaining salt, water and electrolyte homeostasis
• regulating blood pressure via the renin–angiotensin system
• endocrine functions related to erythropoiesis and vitamin D metabolism.
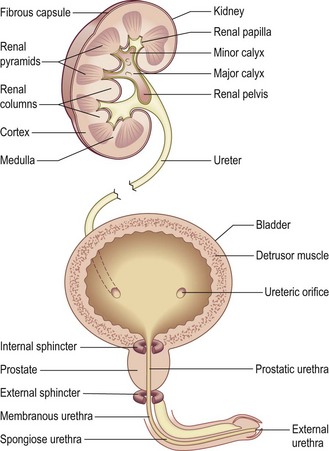
The renal capsule and ureter are innervated by T10–12/L1 nerve roots; pain from these structures is felt in these dermatomes (Fig. 11.28). The bladder acts as a reservoir. As it fills, it becomes ovoid, and rises out of the pelvis in the midline towards the umbilicus, behind the anterior abdominal wall. The bladder wall contains a layer of smooth muscle, the detrusor, which contracts under parasympathetic control, allowing urine to pass through the urethra (micturition). The conscious desire to micturate occurs when the bladder holds ~ 250–350 ml of urine. The male urethra runs from the bladder to the tip of the penis and has three parts: prostatic, membranous and spongiose (Fig. 9.3). The female urethra is much shorter, with the external meatus situated anterior to the vaginal orifice and behind the clitoris (Fig. 10.20). Two muscular rings acting as valves (sphincters) control micturition:
Symptoms and definitions
Severe renal disease may be asymptomatic, or have non-specific symptoms, such as tiredness or breathlessness from renal failure or associated anaemia. Detection often follows incidental testing of blood and urine. Ask about the following symptoms, but always test urine and blood to assess renal function.
Pain
Most kidney disease is painless. However, pain may arise from the kidney capsule (loin pain), the ureter (ureteric colic) or the bladder/urethra.
Renal angle (between the 12th rib and the spine) or loin pain is due to stretching of the renal capsule or renal pelvis. Causes include infection, inflammation or mechanical obstruction. Constant loin pain, with systemic upset, fever, rigors and pain on voiding, suggests infection of the upper urinary tract and kidney (acute pyelonephritis). Chronic dull, aching loin discomfort may occur with chronic renal infection and scarring from vesicoureteric reflux, adult polycystic kidney disease (APKD) or chronic urinary tract obstruction. Chronic obstruction may, however, be painfree. Dull loin pain also occurs in renal stone disease and some forms of glomerulonephritis, e.g. IgA nephropathy. It can be difficult to distinguish between renal pain and musculoskeletal conditions, e.g. osteoarthritis of the spine.
Ureteric colic (‘renal colic’) is caused by acute obstruction with distension of the renal pelvis and ureter by a stone, blood clot or, rarely, a necrotic renal papilla.
• Site – unilateral, in the renal angle and flank area
• Character – usually very severe and sustained, may vary cyclically in intensity
• Radiation – may radiate to the iliac fossa, the groin and the genitalia, especially the testes
• Associated features – patient is usually restless and nauseated, and often vomits
• Timing – may last for several hours or even days, until the obstructing body reaches the bladder, when symptoms usually resolve
• Exacerbating/relieving factors – analgesia with non-steroidal anti-inflammatory drugs (NSAIDs) or opioids is required
• Severity – variable, but often very severe and incapacitating.
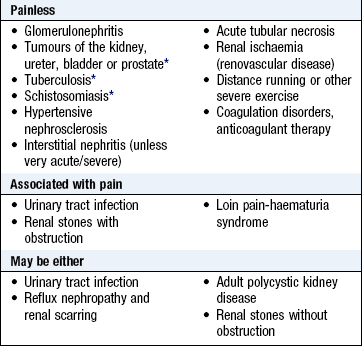
• Similar – distinguish from intestinal or biliary colic, appendicitis, torsion of an ovarian cyst, ruptured ectopic pregnancy. Test the urine for blood; haematuria (visible or non-visible) is usual and, if absent, casts doubt on the diagnosis (Box 9.1).
Patients with loin pain–haematuria syndrome complain of chronic unilateral or bilateral loin discomfort of varying severity. Characteristically they have non-visible haematuria and episodic visible haematuria.
Dysuria (voiding pain) is pain during or immediately after passing urine, often described as a ‘burning’ sensation felt at the urethral meatus or suprapubically.
Strangury describes slow and painful discharge of small volumes of urine related to involuntary bladder contractions.
Frequency is a desire to pass urine more often than usual.
The most common cause of the above symptoms is infection and/or inflammation of the bladder (cystitis). Prostatitis and urethritis produce similar symptoms. Prostatitis may cause perineal and rectal pain at the same time. Pain localised to the penis indicates local pathology, e.g. an inflammatory stricture, stone or, rarely, tumour.
Testicular and epididymal pain may be felt primarily in the groin and lower abdomen. Tenderness and swelling of the testis may be due to acute epididymo-orchitis; in pubertal boys and young men consider torsion of the testis, and be careful to distinguish these conditions from a strangulated inguinal hernia (p. 189).
Voiding symptoms
Lower urinary tract symptoms may be:
• Frequency – micturating more often with no increase in the total urine output.
• Urgency – a sudden strong need to pass urine. Urgency is due to either overactivity in the detrusor muscle or abnormal stretch receptor activity from the bladder (sensory urgency). Incontinence may occur.
Storage symptoms are usually associated with bladder, prostate or urethral problems, e.g. lower urinary tract infection, tumour, urinary stones or obstruction from prostatic enlargement, or are a consequence of neurological disease.
Voiding phase symptoms: Hesitancy is difficulty or delay in initiating urine flow. In men over 40 this is commonly due to bladder outlet obstruction by prostatic enlargement (Box 9.2). Assess the intrusiveness of this by the International Prostate Symptom Score (IPSS) (Box 9.3). In women these symptoms suggest urethral obstruction from stenosis or in association with genital prolapse (Boxes 9.4 and 9.5).
 9.2
9.2 9.3
9.3
The International Prostate Symptom Score
The International Prostate Symptom Score (IPSS) reliably assesses the severity of voiding phase symptoms in men >40 years.
Barry MJ, Fowler FJ, O’Leary MP et al. The American Urological Association symptom index for benign prostatic hyperplasia. J Urol 1992;148:1549–1557.
 9.4
9.4
International Prostate Symptom Score (IPSS)
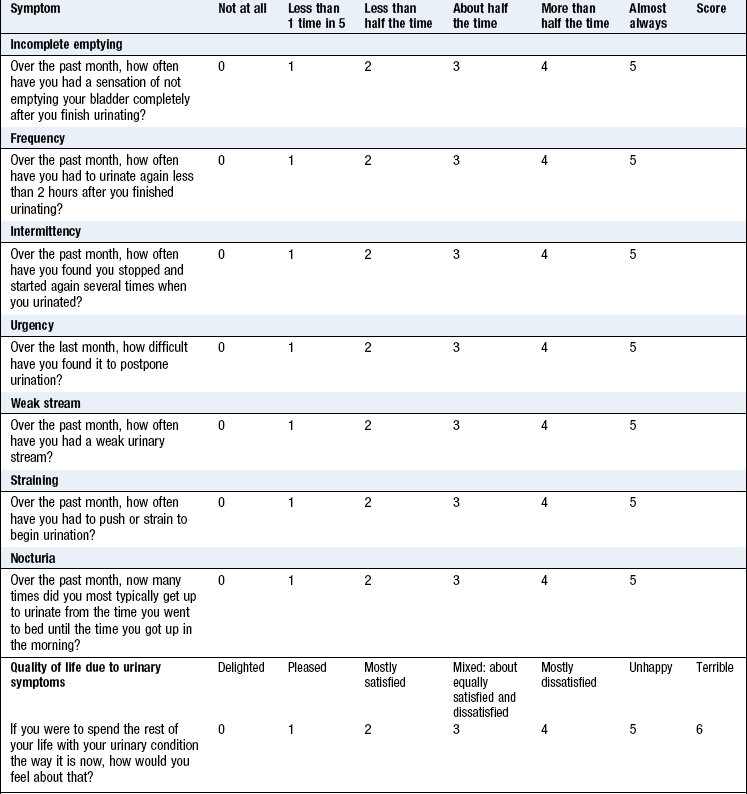
Total IPSS score: 0–7, mildly symptomatic; 8–19, moderately symptomatic; 20–35, severely symptomatic.
International Prostate Symptom Score © (I-PSS©) Michael J Barry, 1992. All rights reserved.
 9.5 Functional assessment of the lower urinary tract
9.5 Functional assessment of the lower urinary tract
• Invasive tests, necessitating insertion of bladder and rectal catheters to measure total bladder pressure and abdominal pressure and to allow bladder filling
• Filling studies determine detrusor activity and compliance
• Low detrusor pressures with low urine flow suggest detrusor function problems
• High detrusor pressures with a low flow suggest bladder outlet obstruction
After micturition: Dribbling and incomplete emptying are caused by bladder neck obstruction, but if they are associated with storage symptoms, may indicate abnormal detrusor function.
Incontinence: Involuntary release of urine may occur with a need to void (urge incontinence), result from an increase in intra-abdominal pressure (stress incontinence) or be a combination of both (mixed incontinence) (Box 9.6). Urge incontinence occurs when the detrusor is overactive. Stress incontinence occurs in women due to weakness of the pelvic floor, usually following childbirth. Continual incontinence implies a fistula between the bladder and either the urethra or the vagina due to complications of obstetric delivery, pelvic surgery, radiotherapy, tumour or trauma. Such fistulas are a major public health problem for women in many underdeveloped countries due to inadequate obstetric care and a high incidence of impacted labour. Enuresis is incontinence during sleep, and common in childhood. In adults it suggests bladder outlet obstruction or abnormalities of the wakening mechanism.
Abnormalities in urine volume and composition: Healthy adults produce 2–3 litres of urine per day, equivalent to their fluid intake minus insensible fluid losses through the skin and respiratory tract (500–800 ml/day).
Polyuria: Polyuria is an abnormally large volume of urine, and is most commonly due to excessive fluid intake. Rarely, this is a manifestation of psychiatric disease (psychogenic polydipsia). Polyuria also occurs when the kidneys cannot concentrate urine. Causes may be extrarenal, e.g. diuretic drugs; hyperglycaemia with glycosuria causing an osmotic diuresis; lack of arginine vasopressin (AVP) from the pituitary gland in cranial diabetes insipidus, or failure of aldosterone secretion by the adrenal gland in Addison’s disease. Renal causes occur when the kidney tubules fail to reabsorb water appropriately in response to AVP. This occurs in nephrogenic diabetes insipidus, usually due to genetic mutation in the tubular AVP receptor. It may also reflect chronic tubulointerstitial damage, reflux nephropathy, analgesic nephropathy and drugs, e.g. lithium.
Oliguria: Oliguria is a reduction in urine volume to <800 ml/day. It may be appropriate with a very low fluid intake, but may also indicate loss of kidney function. The minimum urine volume needed to excrete the daily solute load varies with diet, physical activity and metabolic rate, but is at least 400 ml/day. Acute renal failure is usually associated with oliguria, although 20% of patients have non-oliguric acute renal failure.
Anuria: Anuria is the total absence of urine production. Exclude urinary tract obstruction, which may be lower (bladder neck or urethral obstruction causing acute urinary retention) or upper, e.g. a ureteric stone in a patient with a single functioning kidney.
Pneumaturia: Pneumaturia, passing gas bubbles in the urine, is rare. It may be associated with faecuria, when faeces are voided. It suggests a fistula between the bladder and the colon, from a diverticular abscess, cancer or Crohn’s disease.
Haematuria: Haematuria is red blood cells in the urine arising from the kidneys or urinary tract. This may be visible (to the naked eye) or non-visible (detected on urinalysis or microscopy). Non-visible haematuria occurs in renal or urinary tract disease, especially if associated with proteinuria, hypertension, raised serum creatinine or reduced estimated glomerular filtration rate. Visible haematuria may be due to urinary tract infection with its associated symptoms but should be investigated, if painless, by upper urinary tract imaging and cystoscopy, as it may be due to cancer of the kidney, bladder or prostate. Investigate all patients >40 years with haematuria (visible or non-visible), because the incidence of these conditions increases with age.
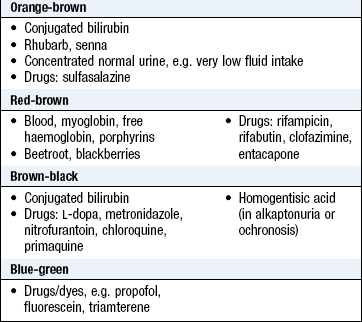
Distinguish haematuria from contamination of the urine by blood from the female genital tract during menstruation. Free haemoglobin in the urine due to haemolysis, myoglobin in rhabdomyolysis and other abnormalities of urine colour may mimic haematuria (Box 9.7) but can be differentiated by urinalysis and urine microscopy (Fig. 9.4 and Box 9.8).
Proteinuria: Proteinuria is excess protein in urine and indicates kidney disease (Boxes 9.9 and 9.10). It is usually asymptomatic and detected by urinalysis. Albumin (from plasma) is the main component, although in certain conditions, e.g. myeloma, chronic lymphatic leukaemia or amyloidosis, globulins and immunoglobulin light chains (Bence Jones protein) may predominate. Suspect these conditions if the urine dipstick test is negative but other tests suggest proteinuria, since the stick reagents are albumin-specific.
 9.9 Causes of proteinuria
9.9 Causes of proteinuria
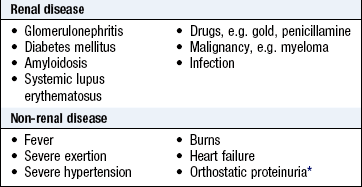
*Occurs when a patient is upright but not lying down; the first morning sample will not show proteinuria.

Proteinuria up to 2 g/24 h is non-specific. Values greater than this indicate a glomerular abnormality, most commonly glomerulonephritis or diabetic nephropathy. Radioimmunoassay techniques can detect albumin excretion rates as low as 30 mg/day. Microalbuminuria (30–300 mg/day) occurs early in diabetic nephropathy, and is a risk factor for myocardial infarction, stroke and venous thromboembolism.
Proteinuria may occur in normal patients with febrile illness. Orthostatic proteinuria is proteinuria <1 g/l which disappears when lying down and is occasionally found in healthy young subjects; protein is not detected in the first urine passed after sleeping recumbent overnight, but is present during the day.
Severe proteinuria may produce frothy urine. If it lowers the plasma albumin concentration enough to reduce the plasma oncotic pressure, the patient develops generalised oedema: the nephrotic syndrome.
Pruritus (itch) is a prominent symptom of advanced chronic kidney disease (CKD stage 4–5).
The history
Ask about the reason(s) for seeking medical attention. then ask about the key symptoms above, including pain, symptoms related to micturition, any change in urine volume or appearance (Box 9.11).
Other symptoms include tiredness, breathlessness, poor appetite, sleep disturbance, restless legs, particularly at night, muscle twitching due to hypocalcaemia and, in end-stage renal disease, vomiting, diarrhoea, confusion and altered consciousness.
Past history
Ask about any previous history of renal system disease. Also ask about:
• hypertension (which may cause or result from renal disease)
• diabetes mellitus (associated with diabetic nephropathy and renovascular disease)
• vascular disease at other sites (which makes renovascular disease more likely)
• past history of urinary tract stones or surgery
• recurrent infections (particularly urinary infections which may be associated with renal scarring, and upper respiratory infections which may be associated with glomerulonephritis and/or vasculitis)
Drug history
Renal failure affects drug metabolism and pharmacokinetics, and drugs may adversely affect renal function.
Take a full drug history, paying particular attention to drugs which accumulate in renal failure, such as digoxin, lithium, aminoglycosides, opioids and water-soluble beta-blockers, e.g. atenolol. Drugs which may affect renal function include angiotensin-converting enzyme inhibitors, angiotensin receptor antagonists and NSAIDs. These drugs do not impair the function of normal kidneys, but further reduce glomerular filtration when the kidneys are underperfused. Ask about over-the-counter NSAIDs, which can dramatically reduce renal function in the context of systemic infection or hypovolaemia. Aminoglycosides, amphotericin, lithium, ciclosporin, tacrolimus and, in overdose, paracetamol are toxic to normal kidneys. Some drugs cause kidney failure indirectly: for example, cocaine and ecstasy can cause rhabdomyolysis and myoglobinuria leading to acute renal failure.
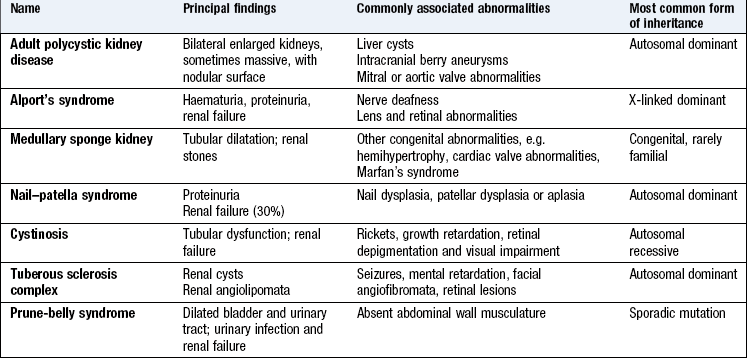
Family history
The most common inherited conditions are APKD (autosomal dominant) and Alport’s syndrome (X-linked dominant) (Box 9.12). APKD is associated with subarachnoid haemorrhage from intracranial berry aneurysms; Alport’s syndrome is associated with high-tone sensorineural deafness. Some patients with type 1 diabetes mellitus have a genetically increased susceptibility to diabetic nephropathy which may be revealed by the family history.
Social history
Find out about your patients’ ideas, concerns and expectation (ICE: p. 8). End-stage renal disease requiring dialysis and/or transplantation has major implications for lifestyle, employment and relationships. Similarly, incontinence has major implications for daily living.
Smoking is a risk factor for atheromatous renal vascular disease, for nephropathy in diabetic patients and for urothelial cancers. Excess alcohol consumption is associated with hypertensive renal damage and increased incidence of IgA nephropathy.
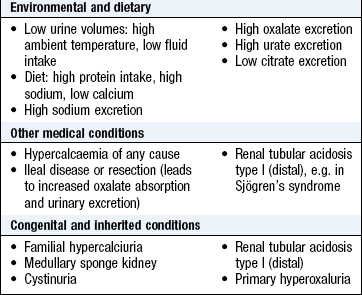
Take a dietary history in patients with renal stones: include intake of water, calcium, e.g. milk and dairy products, and oxalate, e.g. chocolate, rhubarb, spinach and soya. Assess dietary protein intake in patients with CKD to make sure it is not excessive. Ask about salt (sodium) intake in patients with hypertension and CKD.
Some renal conditions are found in particular ethnic groups: for example, Balkan nephropathy (interstitial nephritis and urinary tract tumours, probably caused by fungal toxins in grain), systemic lupus erythematosus (SLE) with nephritis in the Far East, and severe hypertension or diabetes mellitus with renal failure in patients of African origin.
Occupational history
Living and working in hot conditions with more concentrated urine may predispose to renal stone formation (Box 9.13). Exposure to organic solvents may cause glomerulonephritis. Aniline dye and rubber workers have an increased incidence of urothelial cancer. Long-term exposure to lead and cadmium may cause renal damage.
The physical examination
Physical examination may be normal, even with significant kidney disease.
Examination sequence
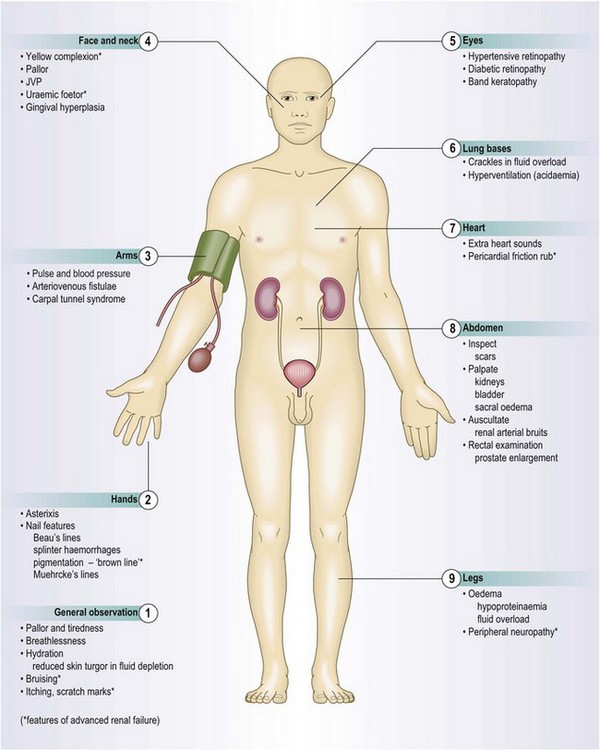
Assess the patient’s general appearance and conscious level. Is he well or ill?
 Look for fatigue, pallor, breathlessness, uraemic complexion, cushingoid appearance and hirsutism.
Look for fatigue, pallor, breathlessness, uraemic complexion, cushingoid appearance and hirsutism.
Look at the eyes for the conjunctival pallor of anaemia and across the cornea – for band keratopathy, and at the edge of the cornea – limbic calcification.
Note any bruising or excoriation.
Examine the hands for nail changes.
Ask the patient to hold out the arms and fully extend the hands. Look for a coarse flapping tremor (asterixis) developing after a few seconds (Fig. 7.10).
Smell the patient’s breath for uraemic fetor.
Assess hydration by checking skin turgor, eyeball tone, JVP and presence of oedema (p. 61).
Abnormal findings: CKD may be associated with a lemon-yellow coloration of the skin (uraemic complexion; Fig. 9.5), and bruising and excoriation secondary to pruritus (Fig. 9.6). These patients are often anaemic and have a urine-like smell on the breath (uraemic fetor). Nail changes include a brownish discoloration of the distal nail bed (Fig. 9.7), leukonychia (white nails), Muehrcke’s nails (leukonychia striata; band-like pale discolorations) and Beau’s lines (transverse grooves or furrows on the nail plate) in chronic hypoalbuminaemia (Fig. 4.15C).
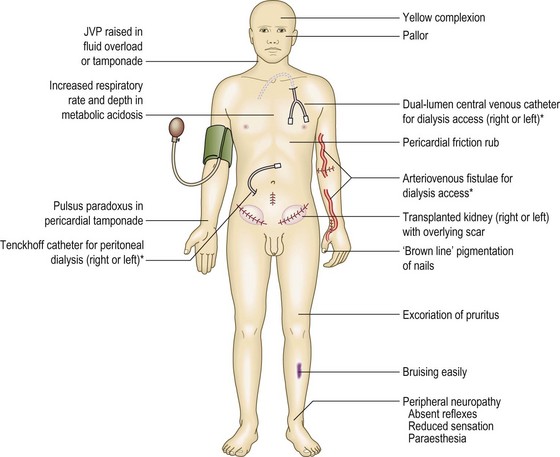
Fig. 9.5 Physical signs in chronic kidney disease.
*Features of renal replacement therapy. JVP, jugular venous pressure.


In untreated end-stage renal disease there may be altered consciousness and asterixis (p. 151).
Note any surgically created arteriovenous (AV) fistula at the wrist or elbow which allows vascular access for haemodialysis.
Drug treatment may cause abnormalities: for example, cushingoid features with steroid therapy, hirsutism and gum hypertrophy related to ciclosporin, and warts and skin cancers due to immunosuppression in patients with a renal transplant.
Abdominal examination
 Examination sequence
Examination sequence
Ask the patient to lie flat with his head on a pillow with his arms by his side to relax the abdominal muscles. Expose the abdomen fully.
Look for distension (from the enlarged kidneys of APKD, or occasionally in obstructive uropathy) and suprapubically from bladder distension.
Look in the loins for scars of renal tract surgery and in the iliac fossae for those of transplant surgery. You may see a catheter for peritoneal dialysis or small scars left by one in the midline and hypochondrium.
Use the fingers of your right hand. Start in the right lower quadrant and palpate each area systematically (Fig. 8.3).
To detect lesser degrees of kidney enlargement; place your left hand behind the patient’s back below the lower ribs and your right hand anteriorly over the upper quadrant just lateral to the rectus muscle (Fig. 9.8).
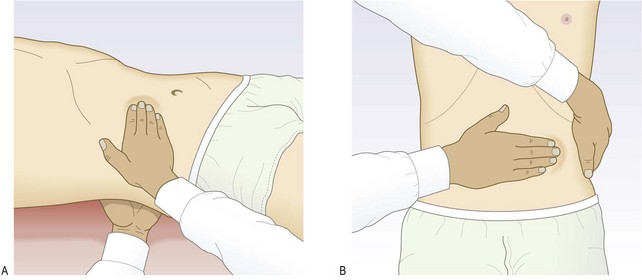
Firmly, but gently, push your hands together as the patient breathes out. Ask the patient to breathe in deeply; feel for the lower pole of the kidney moving down between your hands. If this happens, gently push the kidney back and forwards between your two hands to demonstrate its mobility. This is ballotting, and confirms that this structure is the kidney.
If the kidney is palpable, assess its size, surface and consistency.
Ask the patient to sit up. Palpate the renal angle (between the spine and 12th rib posteriorly) firmly but gently. If this does not cause the patient discomfort, firmly (but with moderate force only) strike the renal angle once with the ulnar aspect of your closed fist after warning the patient what to expect (Fig. 9.9) and note any discomfort.

Auscultate for bruits arising from the renal arteries. Listen carefully over both loins posteriorly and in the epigastrium, using the stethoscope diaphragm. Renal artery bruits cannot be distinguished from those in adjacent vessels, e.g. the mesenteric arteries, but any abdominal bruits, diminished or absent femoral artery pulses and bruits increase the probability of coexistent atheromatous renal artery disease.
Test for ascites (p. 186), which may be found in nephrotic syndrome or in patients having peritoneal dialysis.
In men examine the external genitalia and perform a rectal examination (pp. 238 and 189) to assess the prostate for benign or malignant change.
In women, perform a vaginal examination to exclude pelvic malignancy and to assess prolapse and the integrity of the pelvic floor (p. 225).
Abnormal findings: The kidneys are normally mobile and move as much as 3 cm inferiorly during inspiration. It is usually easier to feel the right kidney, as it is lower than the left. Minor degrees of kidney enlargement are difficult to assess. In very thin subjects the lower pole of a normal right kidney may be palpable, but even very large kidneys may be impossible to feel in obese subjects. A markedly enlarged liver is difficult to differentiate from the right kidney, especially if APKD is associated with cystic disease of the liver.
Enlargement of one kidney may result from compensatory hypertrophy due to renal agenesis, hypoplasia or atrophy, or surgical removal of the other kidney. It may also be due to a renal tumour or hydronephrosis. Enlargement of both kidneys occurs in APKD, amyloidosis and in acute glomerulonephritis. A transplanted kidney is palpable as a smooth mass in either iliac fossa with an overlying scar.
Polycystic kidneys have a distinctive irregular nodular surface and vary in size from moderately enlarged to filling the whole of one side of the abdomen. Kidneys containing tumours are usually firm and irregular, and sometimes tethered to surrounding structures. Enlarged obstructed or hypertrophic kidneys have a smooth surface. Tenderness over the kidneys is most often due to acute pyelonephritis or acute urinary obstruction. A distended bladder is a smooth firm mass arising from the pelvis, which disappears after urethral catheterisation (Box 9.14).
9.14
Renal artery stenosis
Hearing an abdominal bruit (especially if systolic and diastolic) in a patient with severe, or difficult to control, hypertension strongly suggests renal artery stenosis.
Krijnen P, van Jaarsveld BC, Steyerberg EW et al. A clinical prediction rule for renal artery stenosis. Ann Intern Med 1998;129:705–711.
Cardiovascular examination
Examination sequence


Abnormal findings: Blood pressure is often elevated in renal disease, but may be low with a postural drop in patients with tubulointerstitial disease who lose sodium and water inappropriately because of impaired tubular reabsorption. Pulsus paradoxus (p. 111) may be present with pericardial tamponade due to uraemic pericarditis, along with a raised JVP and low blood pressure. In the nephrotic syndrome, although oedema is present, the JVP is not usually raised and there are no added heart sounds, as the intravascular volume is often normal or reduced.
The apex beat may be displaced in fluid overload and heart failure, or heaving in patients with left ventricular hypertrophy or secondary to hypertension. ‘Flow’ murmurs are common in patients with ‘renal’ anaemia, particularly if the cardiac output is increased because of an AV fistula. Added heart sounds occur in fluid overload and/or heart failure, and a pericardial friction rub may be present due to uraemic pericarditis.
Peripheral oedema usually signifies fluid retention and expanded extracellular fluid volume; the exceptions are in hypoalbuminaemia (decreased capillary oncotic pressure) and the use of vasodilator drugs, e.g. calcium channel blockers (increased capillary hydrostatic pressure).
Respiratory examination
• Measure the respiratory rate (p. 145).
• Percuss the chest to detect pleural effusions.
• Auscultate for bilateral basal lung crackles indicating fluid overload or heart failure.
Abnormal findings: In CKD, respiratory compensation for the associated metabolic acidosis may lead to an increased respiratory rate and deep sighing respirations (Küssmaul respiration; p. 146). Pleural effusions may be present due to fluid overload or hypoalbuminaemia.
Putting it all together
In renal disease, blood-and urine tests and appropriate imaging are essential for definitive diagnosis. Although some kidney conditions are primary, e.g. many forms of glomerulonephritis, others are secondary to systemic conditions, e.g. diabetes, autoimmune disorders and systemic vasculitis, adverse drug reactions, malignancies such as lymphoma, and infections including septicaemia.
Investigations
Examine the urine in all patients (Boxes 9.15 and 9.16). Urine abnormalities may reflect:
9.15 Uses of urinalysis
| Use | Indication | Of value in: |
| Screening | Random | Diabetes mellitus |
| Asymptomatic bacteriuria | ||
| Selective | Antenatal care | |
| Hypertensive patients | ||
| Diagnosis | Primary renal disease | Glomerulonephritis |
| Secondary renal disease | Bacterial endocarditis | |
| Non-renal disorders | Diabetes mellitus | |
| Monitoring | Disease progression | Diabetic nephropathy |
| Drug toxicity | Gold therapy | |
| Drug compliance | Rifampicin therapy | |
| Illicit drug use | Opioids, benzodiazepines |
9.16 Urine dipstick test*
| Investigation | Comment |
| Specific gravity | Reflects urine solute concentration. Varies between 1.002 and 1.035; ↑ when kidneys actively reabsorb water, e.g. fluid depletion or renal failure due to ↓ perfusion. Abnormally low values indicate failure to concentrate urine |
| pH | Normally 4.5–8.0. In renal tubular acidosis pH never falls <5.3 despite acidaemia |
| Glucose | Small amounts may be excreted by normal kidneys |
| Ketones | Test is specific for acetoacetate and does not detect other ketones, e.g. β-OH butyrate, acetone. Ketonuria occurs in diabetic ketoacidosis, starvation, alcohol use and very-low-carbohydrate diets |
| Protein | Readings > ‘trace’ (300 mg/L) indicate significant proteinuria. Proteinuria >2 g/day suggests glomerular disease |
| Blood | The test does not differentiate between haemoglobin and myoglobin. If you suspect rhabdomyolysis, measure myoglobin with specific laboratory test |
| Bilirubin and urobilinogen | Bilirubin not normally present. Urobilinogen may be up to 33 µmol/L in health. Abnormalities of bilirubin and urobilinogen require investigation for possible haemolysis or hepatobiliary disease |
| Leukocyte esterase | Indicates presence of leukocytes in urine. Seen in urinary tract infection or inflammation, stone disease and urothelial cancers |
| Nitrite | Most Gram-ve bacteria convert urinary nitrate to nitrite. A positive result indicates bacteriuria, but a negative result does not exclude its presence |
• abnormally high levels of a substance in the blood exceeding the capacity for normal tubular reabsorption, e.g. glucose, ketones, conjugated bilirubin and urobilinogen (Fig. 9.12)

• altered kidney function, e.g. proteinuria, failure to concentrate urine
• abnormal contents, e.g. blood entering at any point from the kidney to the urethra.
Normal fresh urine is clear but varies in colour. Phosphates and urates may precipitate out of normal clear urine left to stand and make it cloudy. Cloudy fresh urine is usually due to the presence of leukocytes (pyuria), often with bacteria. An unusually strong fishy smell suggests urinary infection. Some foods, e.g. asparagus, impart a characteristic smell to the urine (Box 9.17).
9.17
Urinary tract infection in women
In a woman with one or more relevant symptoms (dysuria, frequency, haematuria, back pain), the probability of (culture-positive) urinary tract infection is ~50%. This increases to ~80% with a positive dipstick urinalysis for nitrite and leukocyte esterase.
Bent S, Nallamothu BK, Simel DL et al. Does this woman have an acute uncomplicated urinary tract infection? In: Simel D, Rinne D (eds) The rational clinical examination. New York: JAMA and Archives Journals/McGraw-Hill Professional, 2008, pp. 675–685.
Other investigations: Measure the 24-hour urine volume to confirm oliguria or polyuria. In critically ill patients, hourly urine flow is a good dynamic indicator of organ perfusion (Box 9.4; Boxes 9.18 and 9.19).
9.19 Imaging and biopsy investigations
| Investigation | Indication/Comment |
| Plain abdominal X-ray | Assesses renal outline/size, stones (>90% are radio-opaque), gas in the urinary collecting system |
| Ultrasound scan | Assesses kidney size/shape/position; evidence of obstruction; renal cysts or solid lesions; stones; ureteric urine flow; gross abnormality of bladder, post-micturition residual volume Used to guide kidney biopsy |
| Doppler ultrasound of renal vessels | Assesses renovascular disease, renal vein thrombosis Arterial resistive index may indicate obstruction |
| IV urography | Haematuria; renal colic; renal mass; renal, ureteric or bladder stones; cysts; tumours; hydronephrosis NB In many hospitals IVU has been replaced by CT and other imaging forms |
| CT urogram | Stone disease; renal mass; ureteric obstruction; tumour staging; renal, retroperitoneal or other tumour masses or fibrosis |
| Angiography/CT or MR angiography | Hypertension ± renal failure, renal artery stenosis; angioplasty and/or stenting |
| Isotope scan | Suspected renal scarring, e.g. reflux nephropathy; diagnosis of obstruction Assessment of GFR in each kidney - measures renal uptake and excretion of radio-labelled chemicals |
| Renal biopsy | Used to diagnose parenchymal renal disease |