Skin cancer – Basal cell carcinoma
Malignant skin tumours are among the most common of all cancers. They are more frequent in light-skinned races, and ultraviolet (UV) radiation seems to be involved in their aetiology. The incidence of non-melanoma skin cancer in caucasoids in the USA was recently estimated at 230 per 100 000 per year, compared with 3 per 100 000 for African Americans. The majority of malignant skin tumours (Table 1) are epidermal in origin and are either basal cell or squamous cell carcinomas (p. 100) or malignant melanomas (p. 103). Premalignant epidermal conditions are common (p. 98), but dermal malignancies are comparatively rare.
Table 1 A classification of malignant skin tumours and premalignant conditions
| Cell origin | Premalignant condition | Malignant tumour |
|---|---|---|
| Keratinocyte | Actinic keratosis (p. 119), in situ squamous cell carcinoma (p. 100) | Basal cell carcinoma Squamous cell carcinoma |
| Melanocyte | Dysplastic naevus (p. 103) | Malignant melanoma (p. 103) |
| Fibroblast | Dermatofibrosarcoma (p. 98) | |
| Lymphocyte | Lymphoma (p. 98) | |
| Endothelium | Kaposi’s sarcoma (p. 56) | |
| Non-cutaneous | Secondary (p. 43) |
Basal cell carcinoma
Basal cell carcinomas (BCC, rodent ulcers) are the commonest form of skin cancer and are typically seen on the face in elderly or middle-aged subjects. Although there is strong epidemiological evidence for the role of UV radiation in the pathogenesis of BCCs, the tumours do not distribute to the most sun-exposed sites and BCCs of the dorsum of the hand, forearm and lip are uncommon. They arise from the basal keratinocytes of the epidermis, are locally invasive, but very rarely metastasize.
Aetiopathogenesis
Malignant transformation of basal cells may be induced by:
 prolonged UV exposure (and acute sunburn)
prolonged UV exposure (and acute sunburn)
immunosuppression (e.g. renal transplant recipients)
arsenic ingestion, e.g. in ‘tonics’ or drinking water
X-rays and other ionizing radiation
Basal cell carcinomas are most common in caucasoids with a fair ‘celtic’ skin who live near the equator, and are seen more in males than in females. In the UK, they mainly occur in those over the age of 40 years, although, in Australia, they may be seen in the third decade.
Pathology
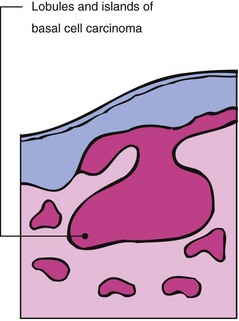
The tumour is classically composed of uniform basophilic cells, in well-defined islands, that invade the dermis from the epidermis as buds, lobules or strands (Fig. 1).
Clinical presentation
Basal cell carcinomas occur mainly on light-exposed sites, commonly around the nose, the inner canthus of the eyelids and the temple. They grow slowly but relentlessly, are locally invasive and may destroy cartilage, bone and soft tissue structures. A lesion has often been present for 2 years or more before the patient seeks advice. Often more than one tumour is evident. There are four main types of basal cell carcinoma, all of which may occasionally be pigmented:
1. Nodular. This is the commonest type of lesion and usually starts as a small, skin-coloured papule that shows fine telangiectasia and a glistening pearly edge (Fig. 2). Central necrosis often occurs and leaves a small ulcer with an adherent crust. The lesions are mostly less than 1 cm in diameter, but grow larger if present for several years. Clinically, they usually present as a thickened plaque rather than a tumour and, although firm to palpation, this may be difficult to establish in smaller lesions. Nodular BCCs often have slightly raised margins with a central depression. Superficial branching telangiectasia are characteristic and are seen on dermoscopy as ‘arborizing’ (Fig. 3). Stretching the skin between two fingers will often accentuate the margins giving them a pale white ‘pearly’ colour.
2. Cystic. These become tense and translucent and show cystic spaces on histology.
3. Multicentric. Superficial tumours, often multiple, plaque-like and several centimetres in diameter, are sometimes seen especially on the trunk (Fig. 4). They have a rim-like edge and are frequently lightly pigmented.
4. Morphoeic. This scarring (cicatricial) variant, most common on the face, often shows a white or yellow morphoea-like plaque that may be centrally depressed (Fig. 5).

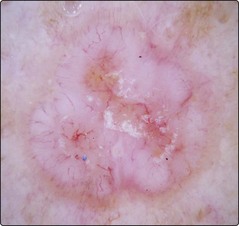

Fig. 4 Basal cell carcinoma of the superficial multifocal type.
This was located on the trunk. A biopsy (scar visible) confirmed the diagnosis.

Fig. 5 Basal cell carcinoma of the right cheek in an immunosuppressed patient.
This BCC has poorly defined clinical margins and is sited in a high-risk area. Discussion of planned management with a multidisciplinary team including a dermatological surgeon, plastic and maxillofacial surgeon and radiotherapist would be ideal.
Differential diagnosis
The differential diagnosis depends on the type, pigmentation and location of the basal cell carcinoma:
Nodular/cystic: intradermal naevus (p. 96), molluscum contagiosum (p. 53), keratoacanthoma (p. 100), squamous cell carcinoma, sebaceous hyperplasia (a benign proliferation of sebaceous glands).
Multicentric: discoid eczema (p. 38), psoriatic plaque (p. 29), in situ squamous cell carcinoma (p. 100).
Morphoeic: morphoea (p. 81), scar.
Pigmented: malignant melanoma (p. 103), seborrhoeic wart (p. 94), compound naevus (p. 96).
Management
The most appropriate treatment for any one tumour depends on its size, site, type and the patient’s age. If possible, complete excision is the best treatment, as this allows a histological check on the adequacy of removal. If excision is difficult or not possible, incisional biopsy (to confirm the diagnosis) and radiotherapy are suitable for those aged 60 years and over. Large tumours around the eye (Fig. 6) and the nasolabial fold, especially if of the morphoeic type, are best managed by surgical excision. Mohs’ micrographic surgery (p. 112) may be employed, as the margins of these tumours are often difficult to determine and may be extensive. Curettage and cautery is sometimes used for lesions on the trunk or upper extremities. Cryosurgery or topical imiquimod (p. 115) are acceptable modalities for multiple, superficial lesions, e.g. on the trunk.

Fig. 6 Basal cell carcinoma of the lower lid.
These lesions require careful surgical management to protect the lacrimal anatomy and prevent scar induced retraction of the eyelid margin.
The recurrence rate is about 5% at 5 years for most methods of treatment. Follow-up is particularly important if there is concern about the adequacy of treatment.
Basal cell carcinoma
Basal cell carcinoma (rodent ulcer) is a common tumour often seen on the face of elderly or middle-aged patients who may have had excessive sun exposure. It:
Basal cell carcinomas with a worse prognosis (high risk) include: