CHAPTER 23 Clinical Manifestations of the Pleural Cavity and Mediastinal Disease
GENERAL CONSIDERATIONS
Common abnormalities of the pleural cavity in the dog and cat include the accumulation of fluid (pleural effusion) or air (pneumothorax) in the pleural space. Mediastinal masses and pneumomediastinum are also discussed in this chapter. Respiratory signs caused by pleural disease result from interference with normal expansion of the lungs. Exercise intolerance is an early sign; overt respiratory distress ultimately occurs. Physical examination findings that assist in localizing the cause of respiratory compromise to the pleural space include increased respiratory rate and decreased lung sounds on auscultation (see Chapter 26). With increasing compromise, increased abdominal excursions during breathing may be seen. Breathing effort may be increased during inspiration relative to expiration, but this finding is not always obvious. In cats with mediastinal masses, decreased compressibility of the anterior thorax may be palpable. Thoracic radiography, thoracocentesis, or both are performed to confirm the presence of pleural space disease.
Pulmonary thromboembolism (PTE) can cause a pleural effusion. The effusion is generally mild and may be an exudate or a modified transudate. PTE should be considered as a diagnosis particularly in patients whose respiratory efforts seem in excess of the volume of effusion (see Chapter 22).
PLEURAL EFFUSION: FLUID CLASSIFICATION AND DIAGNOSTIC APPROACH
The presence of pleural effusion in a dog or cat is usually confirmed by thoracic radiography or thoracocentesis (see Chapter 24). In animals presented in respiratory distress with suspected pleural effusion, thoracocentesis is performed immediately to stabilize the animal’s condition before radiographs are taken. Although thoracocentesis is more invasive than radiography, the potential therapeutic benefit of the procedure far outweighs the small risk of complications. Animals in stable condition at presentation can be evaluated initially with thoracic radiographs to confirm the presence and location of fluid before thoracocentesis is performed.
Ultrasonography is a valuable tool for the evaluation of patients with pleural effusion. If equipment is available on site, animals in critical condition can be examined ultrasonographically with minimal stress to confirm both the presence of fluid and direct needle placement for thoracocentesis. Ultrasonography is also useful in evaluating the thorax for the presence of mass lesions, hernias, and primary cardiac or pericardial disease. Because sound waves cannot pass through aerated lungs, any masses must be adjacent to the chest wall, heart, or diaphragm to be detected by ultrasound. The presence of pleural fluid facilitates the ultrasonographic evaluation of the chest. If the patient is stable, it is preferable to evaluate the thorax ultrasonographically before removing the pleural fluid.
Thoracic radiographs should be taken again after as much fluid or air as possible has been removed from the pleural space and the lungs have had time to reexpand. Full expansion of the lungs is required for accurate evaluation of the pulmonary parenchyma. The presence of fluid also obscures visibility of heart size and shape and mass lesions.
Cytologic analysis of pleural fluid obtained by thoracocentesis is indicated for the diagnostic evaluation of all animals with pleural effusion. Measurement of the protein concentration and total nucleated cell count, as well as the qualitative assessment of individual cells, is essential for accurately classifying the fluid, formulating a diagnostic plan, and initiating appropriate therapy (Table 23-1).
 TABLE 23-1 Diagnostic Approach in Dogs and Cats with Pleural Effusion Based on Fluid Type
TABLE 23-1 Diagnostic Approach in Dogs and Cats with Pleural Effusion Based on Fluid Type
| FLUID TYPE | COMMON DISEASE | DIAGNOSTIC TESTS |
|---|---|---|
| Pure and modified transudates | ||
| Nonseptic exudates |
Pleural fluid cytology is generally sufficient. In questionable cases available tests are many, but none has shown good specificity for diagnosing FIP. Consider systemic evaluation, ophthalmoscopic examination, serum or fluid electrophoresis, coronavirus antibody titer, PCR of tissues or effusion (see Chapter 97)
|
|
| Septic exudates | Pyothorax | Gram staining, aerobic and anaerobic cultures, serial thor |
| Chylous effusion | Chylothorax | See Box 25-1 |
| Hemorrhagic effusion |
ACT, Activated, clotting time; CT, computed tomography; ECG, electrocardiography; echo, echocardiography; PCR, polymerase chain reaction; PT, prothrombin time; PTT, partial thromboplastin time; thor rad, thoracic radiography; US, ultrasonography.
Pleural fluid is classified as a transudate, modified transudate, or exudate on the basis of protein concentration and nucleated cell count. Further classification of fluid may be possible on the basis of other cytologic or biochemical features. Clinically useful fluid categories include septic exudate, chylous effusion, hemorrhagic effusion, and effusion caused by neoplasia. Although various types of fluid have typical gross appearances (Fig. 23-1), reliance on gross appearance alone will lead to the misclassification of fluid and missed diagnoses (through the failure to identify organisms or abnormal cell populations) in some cases. In addition to the inflammatory cell types in each cytologic category described in the subsequent sections, mesothelial cells are generally present and are often reactive.
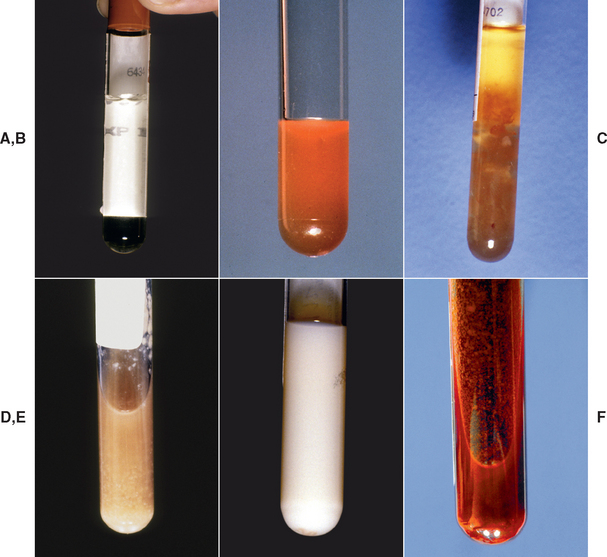
FIG 23-1 Characteristic gross appearance of the various types of pleural effusion. Note that cytologic analysis should always be performed to ensure accurate classification of fluid and to avoid missing diagnostic organisms or neoplastic cells. A, Transudate. Fluid is nearly clear. B, Modified transudate. Fluid is slightly opaque and, in this example, red-tinged. C, Nonseptic exudate. Fluid is more opaque. The fluid shown is from a cat with feline infectious peritonitis (FIP). FIP fluid is characteristically straw colored with grossly visible fibrin clots. D, Septic exudate. Fluid has a purulent appearance, with cellular debris gravitating toward the bottom of the tube. E, Chylous effusion. Fluid is milky white. F, Hemorrhagic effusion. Hemorrhagic effusions are bright to dark red. In this case, cytologic examination revealed filamentous organisms demonstrating the importance of cytologic analysis.
TRANSUDATES AND MODIFIED TRANSUDATES
Pure transudates are fluids with low protein concentrations of less than 2.5 to 3 g/dl and low nucleated cell counts of less than 500 to 1000/μl. The primary cell types are mononuclear cells, composed of macrophages, lymphocytes, and mesothelial cells. Modified transudates have a slightly higher protein concentration of up to 3.5 g/dl and nucleated cell counts of up to 5000/μl. The primary cell types include neutrophils as well as mononuclear cells.
Transudates and modified transudates form as a result of increased hydrostatic pressure, decreased plasma oncotic pressure, or a lymphatic obstruction. Increased hydrostatic pressure occurs in association with right-sided congestive heart failure or pericardial disease. Physical examination findings such as abnormal jugular pulses, gallop rhythms, arrhythmias, or murmurs support a diagnosis of heart disease. Heart sounds may be muffled in animals with pericardial effusions. Thoracic radiography (after fluid removal), electrocardiography, and echocardiography are indicated for cardiac evaluation (see Chapter 2).
Decreased plasma oncotic pressure is a result of hypoalbuminemia. Effusions secondary to hypoalbuminemia alone are pure transudates, having very low protein concentrations. Subcutaneous edema may be detected in dependent areas of the body. A decreased production of albumin causes hypoalbuminemia in patients with liver disease, and an increased loss of albumin causes it in patients with glomerulopathies or protein-losing enteropathies. The total plasma protein concentration shown by refractometry during the initial evaluation of the dog or cat can provide an early indication of hypoalbuminemia. Serum biochemical analysis provides an exact measurement of the albumin concentration. In general, albumin concentrations must be lower than 1 g/dl before transudation occurs caused only because of hypoalbuminemia.
Lymphatic obstruction can be caused by neoplasia and diaphragmatic hernias. Diaphragmatic hernias should be suspected in any animal with a history of trauma. The trauma may have been recent or may have occurred years ago. Although a modified transudate usually forms as a result of chronic diaphragmatic hernia, an exudative fluid can also be found. Diaphragmatic hernias are identified by radiography or ultrasonography. Occasionally, it is necessary to administer barium orally and perform an upper gastrointestinal series or to intraperitoneally administer water-soluble iodinated contrast media and perform peritoneography to confirm the presence of a diaphragmatic hernia. Normal imaging findings do not entirely rule out the existence of a tear in the diaphragm, however.
Neoplasia must be considered as a differential diagnosis for patients with any type of effusion, although it is rare for a pure transudate to develop. (See the section on effusions caused by neoplasia for further discussion.)
SEPTIC AND NONSEPTIC EXUDATES
Exudates have a high protein concentration (greater than 3 g/dl) compared with that in transudates. Nucleated cell counts are also high (greater than 5000/μl). Cell types in nonseptic exudates include neutrophils, macrophages, eosinophils, and lymphocytes. The macrophages and lymphocytes may be activated, and typically the neutrophils are nonde generative. There is no evidence of organisms. Differential diagnoses in animals with nonseptic exudates include feline infectious peritonitis (FIP), neoplasia, chronic diaphragmatic hernia, lung lobe torsion, and resolving septic exudates. Prior treatment with antibiotics in animals with a septic effusion can alter the characteristics of the neutrophil population in the fluid, making them appear nondegenerative, and decrease the number of organisms present in the fluid to an undetectable level. Therefore pleural fluid analysis should be performed before treatment is initiated so that bacterial infection is not overlooked.
Cats with FIP can present with fever or chorioretinitis in addition to respiratory signs (see Chapter 97). The pleural fluid protein concentration is often very high in such animals, approaching serum concentrations. It is common to see fibrin strands or clots in the fluid. Careful cytologic evaluation of the fluid is essential to differentiate FIP fluid from exudates caused by pyothorax or malignant lymphoma. The evaluation of animals for diaphragmatic hernia was described in the previous section and is described for neoplasia in a following section (i.e., Effusion Caused by Neoplasia).
Spontaneous lung lobe torsions are most common in dogs with deep, narrow thoracic cavities. In addition to causing an effusion, torsions can be seen in dogs and cats secondary to pleural effusion. Underlying pulmonary disease resulting in lobe atelectasis can also contribute to the development of torsion. Torsion should be considered in animals with a preexisting effusion or pulmonary disease if their condition suddenly deteriorates. The effusion is often a nonseptic exudate, but it may be chylous or hemorrhagic. Signs of lung lobe torsion may be identified through thoracic radiography or ultrasonography (see Chapter 20). Bronchoscopy or thoracotomy is required to verify the condition in some animals.
Septic exudates often have extremely high nucleated cell counts (e.g., 50,000 to more than 100,000/μl), and degenerate neutrophils are the predominant cells. Bacteria can often be observed within neutrophils and macrophages as well as extracellularly (see Fig. 25-1). The fluid may have a foul odor. Septic exudates are diagnostic for pyothorax. Pyothorax can occur spontaneously, secondary to wounds that penetrate into the thoracic cavity through the chest wall or esophagus, secondary to migrating grass awns or other foreign bodies, or as an extension of bacterial pneumonia. Sterile technique should be used during thoracocentesis and chest tube placement in all animals with pleural effusion or pneumothorax to prevent iatrogenic infection.
Gram staining and both aerobic and anaerobic bacterial cultures with antibiotic sensitivity testing should be performed on the fluid. Culture and sensitivity testing provide valuable information that can be used for selecting appropriate antibiotics and monitoring therapy. Mixed bacterial infections are common. However, bacteria do not grow from cultures of all septic exudates, and results are not available for several days. Gram staining provides immediate information that can be used to help select antibiotics and is helpful in cases in which bacteria cannot be grown from the fluid.
CHYLOUS EFFUSIONS
Chylous effusion (chylothroax) results from the leakage of fluid from the thoracic duct, which carries lipid-rich lymph from the body. Such leakage can be idiopathic, congenital, or secondary to trauma, neoplasia, cardiac disease, pericardial disease, dirofilariasis, lung lobe torsion, or diaphragmatic hernia. Chyle is usually milky white and turbid (see Fig 23-1, E), largely as a result of chylomicrons that carry fats from the intestines. The fluid is occasionally blood tinged, although this finding may also be an artifact from prior thoracocentesis. It is also possible to obtain clear and colorless fluids, particularly in anorectic animals, but this is uncommon.
Chyle has the cytologic characteristics of a modified transudate or nonseptic exudate with moderate concentrations of protein, usually greater than 2.5 g/dl. The nucleated cell count is low to moderate, ranging from 400 to 10,000/μl. Early in the disease the predominant cell type is the small lymphocyte. A few neutrophils may also be present. With time, nondegenerative neutrophils become more predominant and there are fewer lymphocytes. Macrophages also increase in number with time, and plasma cells may be present.
A diagnosis of chylothorax is confirmed by measuring the concentrations of triglycerides in the pleural fluid and serum. Each specimen should be well mixed by the laboratory before a portion is analyzed because of the tendency for the lipid portion to rise to the surface. The triglyceride content in chyle is high compared with that in serum. Rarely, the test will need to be repeated after a meal in anorectic animals.
Most cases of chylothorax are idiopathic, but this diagnosis can be made only after the other disorders have been ruled out. Treatment is most likely to be successful if an underlying problem is identified and treated directly. (See Chapter 25 for a complete discussion of chylothorax.)
HEMORRHAGIC EFFUSIONS
Hemorrhagic effusions are grossly red as a result of the large red blood cell content. Hemorrhagic effusions have greater than 3 g/dl of protein and more than 1000 nucleated cells/μl, with a distribution similar to that of peripheral blood. Over time the numbers of neutrophils and macrophages increase. Hemorrhagic effusions (except those obtained immediately after bleeding into the thorax) are readily distinguished from the recovery of peripheral blood through traumatic thoracocentesis by several features: hemorrhagic effusions have erythrophagocytosis and an inflammatory response on cytologic evaluation, hemorrhagic effusions do not clot, and the packed cell volume (PCV) of hemorrhagic effusions is lower than that of peripheral blood.
Hypovolemia and anemia may contribute to the clinical signs of patients with hemothorax (see Chapter 26). Hemothorax can result from trauma, systemic bleeding disorders, neoplasia, and lung lobe torsion. Rarely, septic exudates are grossly hemorrhagic (see Fig 23-1, F) and are distinguished cytologically. Respiratory distress caused by hemothorax may be the only clinical sign in animals with some bleeding disorders, including rodenticide intoxication. An activated clotting time and platelet count should be performed early in the evaluation of these animals, followed by more specific clotting tests (i.e., prothrombin time and partial thromboplastin time). Hemangiosarcoma of the heart or lungs is a common neoplastic cause of a hemorrhagic effusion, but malignant cells are rarely identified cytologically. Neoplastic effusions are discussed further in the next section.
EFFUSIONS CAUSED BY NEOPLASIA
Neoplasia within the thoracic cavity can result in most types of effusion (modified transudates, exudates, chylous effusion, or hemorrhagic effusion). Neoplasms may involve any of the intrathoracic structures, including the lungs, mediastinal tissues, pleura, heart, and lymph nodes. In some cases, neoplastic cells exfoliate from the tumor into the effusion, and an early diagnosis can be made through fluid cytology. This is often possible in patients with mediastinal lymphoma. Unfortunately, other than in cases of lymphoma, it can be difficult or impossible to establish a definitive diagnosis of neoplasia on the basis of cytologic findings in the pleural fluid alone. Inflammation can result in considerable hyperplastic changes of mesothelial cells that are easily confused with neoplastic cells. A cytologic diagnosis of neoplasia other than lymphoma should be made with extreme caution.
In the majority of cases, neoplastic cells are not present in the fluid or a cytologic diagnosis cannot be made. Thoracic radiography and ultrasonography should be performed to evaluate the thorax for evidence of neoplasia (see Chapter 24). Ultrasonography can be used to differentiate localized accumulations of fluid from soft tissue masses. If soft tissue masses are detected, aspirates or biopsy specimens are obtained for cytologic or histopathologic evaluation. A definitive diagnosis cannot be made on the basis of the radiograph findings or ultrasound images alone.
Diffuse neoplastic infiltration of the pleura and some masses cannot be seen with these imaging techniques. Repeated thoracic radiography, computed tomography, thoracoscopy, or surgical exploration may be necessary in such cases.
PNEUMOTHORAX
Pneumothorax is the accumulation of air in the pleural space. The diagnosis is confirmed by means of thoracic radiography. The pleural cavity is normally under negative pressure, which keeps the lungs expanded in health. However, if an opening forms between the pleural cavity and the atmosphere or the airways of the lungs, air is transferred into the pleural space because of this negative pressure. A tension pneumothorax occurs if a one-way valve is created by tissue at the site of leakage, such that air can enter into the pleural space during inspiration but cannot return to the airways or atmosphere during expiration. Increased intrapleural pressure and resultant respiratory distress occur quickly.
Leaks through the thoracic wall can occur after a traumatic injury or as a result of a faulty pleural drainage system. Air can also enter the thorax during abdominal surgery through a previously undetected diaphragmatic hernia. These causes are readily identified.
Pneumothorax resulting from pulmonary air can occur after blunt trauma to the chest (i.e., traumatic pneumothorax) or as a result of existing pulmonary lesions (i.e., spontaneous pneumothorax). Traumatic pneumothorax occurs frequently, and the history and physical examination findings allow this to be diagnosed. Pulmonary contusions are often present in these animals.
Spontaneous pneumothorax occurs when preexisting pulmonary lesions rupture. Cavitary lung diseases include blebs, bullae, and cysts, which can be congenital or idiopathic or result from prior trauma, chronic airway disease, or Paragonimus infection. Necrotic centers can develop in neoplasms, thromboembolized regions, abscesses, and granulomas involving the airways, and these can rupture, allowing air to escape into the pleural space. (See Chapter 20 for further discussion of cavitary lesions, and Chapter 25 for further discussion of spontaneous pneumothorax.)
Dogs and cats with pneumothorax and a recent history of trauma are managed conservatively. Cage rest, the removal of accumulating air by periodic thoracocentesis or by chest tube, and radiographic monitoring are indicated. If abnormal radiographic opacities persist without improvement for more than several days in trauma patients, further diagnostic tests should be performed, as described in the section on spontaneous pneumothorax (see Chapter 25).
MEDIASTINAL MASSES
Mediastinal masses can cause inspiratory distress as a result of displacement of lung tissue by the mass itself or by the secondary pleural effusion that may develop. Additional clinical signs such as coughing, regurgitation, and facial edema may also be present. Neoplasia is the primary differential diagnosis. Lymphoma involving the mediastinum is common, particularly in cats. Other types of neoplasms include thymoma and rarely thyroid carcinoma, parathyroid carcinoma, and chemodectoma. Nonneoplastic mass lesions such as abscesses, granulomas, hematomas, and cysts are other possibilities.
Mediastinal masses in cats can often be palpated during gentle compression of the anterior thorax. Radiographically, mediastinal masses appear as soft tissue opacities in the anterior mediastinum (Fig. 23-2). However, it can be difficult to accurately identify a mediastinal mass if pleural fluid is present. Pleural fluid can both mimic the appearance of a mass and obscure its borders. Ultrasonography done before removal of the pleural fluid is helpful in identifying a mass and determining the extent to which surrounding structures are involved.

FIG 23-2 Ventrodorsal view of the thorax of a cat with an anterior mediastinal mass. Soft tissue opacity fills the anterior mediastinum and obscures the border of the heart.
Thoracocentesis and fluid analysis should be performed in animals with pleural effusion. Lymphoma can frequently be diagnosed through the identification of malignant cells in the effusion. Transthoracic fine-needle aspiration or biopsy can be performed to obtain specimens for microscopic evaluation of the mass itself. Aspiration cytology is generally performed initially, followed by biopsy if a cytologic diagnosis is not obtained. Transthoracic biopsy specimens can be obtained relatively safely, particularly if the lesion is solid rather than cystic. Ultrasonography can be helpful in determining the consistency of the mass and can also be used to guide biopsy. Alternatively, sites for sampling can be determined from two radiographic views of the thorax. The dorsal mediastinal area and heart should be avoided when obtaining biopsy samples. A study by Lana et al. (2006) demonstrated the usefulness of flow cytometry of mediastinal mass aspirates in differentiating lymphoma from thymoma in dogs.
Surgical exploration or thoracoscopy may be necessary to biopsy small lesions, cavitary lesions, and lesions adjacent to the heart or main blood vessels. Complete excision of the mass should be attempted at that time, unless lymphoma is diagnosed. (Specific recommendations for the management of dogs and cats with mediastinal neoplasia are given in Chapter 79)
PNEUMOMEDIASTINUM
Pneumomediastinum is identified radiographically. Subcutaneous emphysema or pneumothorax can occur concurrently or secondarily. Respiratory compromise most often results from pneumothorax. Mediastinal air commonly originates from rupture or tears in the trachea, bronchi, or alveoli. These leaks can occur as a result of bite wounds of the neck or sudden changes in intrathoracic pressure resulting from coughing, blunt trauma, or excessive respiratory efforts against obstructed airways. Potential iatrogenic causes include tracheal washing, tracheostomy, and endotracheal tube placement (usually caused by excessive endotracheal tube cuff pressure). Air can also enter the mediastinum through esophageal tears, generally resulting from foreign bodies.
Strict cage rest is indicated for animals with pneumomediastinum to facilitate natural sealing of the tear. If air continues to accumulate, causing respiratory compromise, bronchoscopy should be performed to identify tracheal or bronchial lacerations that may require surgical repair.
Hardie EM, et al. Tracheal rupture in cats: 16 cases (1983–1998). J Am Vet Med Assoc. 1999;214:508.
Lana S, et al. Diagnosis of mediastinal masses in dogs by flow cytometry. J Vet Intern Med. 2006;20:1161.
Scott JA, et al. Canine pyothorax: pleural anatomy and pathophysiology. Compend Contin Educ Pract Vet. 2003;25:172.