Objectives, Questions, and Hypotheses
Researchers formulate objectives, questions, and hypotheses to bridge the gap between the more abstractly stated research purpose and the detailed plan for data collection and analysis. Objectives, questions, and hypotheses delineate the research variables, the relationships among the variables, and, often, the population to be studied.
Research variables are concepts at various levels of abstraction that are measured, manipulated, or controlled in a study. Concrete concepts, such as temperature, weight, and blood pressure, are referred to as variables in a study; abstract concepts, such as creativity, empathy, and social support, are sometimes referred to as research concepts. Research variables and concepts are conceptually defined, based on the study framework, and are operationally defined to direct their measurement, manipulation, or control in a study.
In this chapter, you will learn how to formulate research objectives, questions, and hypotheses, especially how to test different types of hypotheses through research. The chapter explores ways to select objectives, questions, or hypotheses to direct a study. It concludes with a discussion of variables and suggestions for conceptually and operationally defining variables for a study.
FORMULATING RESEARCH OBJECTIVES
Research objectives are clear, concise, declarative statements that are expressed in the present tense. For clarity, an objective usually focuses on one or two variables (or concepts) and indicates whether the variables are to be identified or described. Objectives can also identify relationships or associations among variables (relational), determine differences between groups or compare groups on selected variables (differences), and predict a dependent variable based on selected independent variables (prediction).
You might use the following formats for developing objectives to guide a study (the type of objective is identified in parentheses):
1. To identify the elements or characteristics of variable X in a specified population (Identification)
2. To describe the existence of variable X in a specified population (Description)
3. To determine the difference between group 1 and group 2 or to compare groups 1 and 2 on variable X in a specified population (Difference)
4. To determine or identify the relationship between variables X and Y in a specified population (Relational)
5. To determine whether certain independent variables are predictive of a dependent variable (Prediction)
Formulating Objectives in Quantitative Studies
In quantitative research, objectives are developed from the research problem and purpose to clarify the foci of the study, the variables, and population. The following excerpts, from a descriptive study of the education and support needs of younger and older cancer survivors, demonstrate the logical flow from research problem (including the problem significance, background, and statement) and purpose to research objectives (Narsavage & Romeo, 2003).
Cancer rates have continued to rise from the late 1970s to the 1990s, but improved treatments have resulted in increasing rates of survival [problem significance] (Gerlach, Gambosi, & Bowen, 1990).… For decades, regional cancer institutes have designed and implemented programs to educate and provide support to cancer patients and their families. A significant amount of research has focused on the effectiveness of cancer programs in improving knowledge and support but findings are conflicting [problem background] (Narsavage & Romeo, 2003, p. 103).
Cancer has been the second leading cause of death in Northeastern Pennsylvania (NEPA), an area with a large elderly population [problem significance] (Pennsylvania Department of Health, 1998). The Northeast Regional Cancer Institute (NRCI), a nonprofit cooperative network of six hospitals in NEPA, provided educational and support programs designed to help cancer patients and their families survive and manage their illness with improved quality of life [problem background].… As the number of survivors increased and program funding became increasingly limited, there was a need to target programs to the population served. Anecdotal accounts from cancer survivors in NEPA suggested that education and support services were limited [problem statement]. (Narsavage & Romeo, 2003, pp. 104–105)
“To address these concerns, this study examined the use, satisfaction with, and need for cancer education and support services in Northeastern Pennsylvania” by younger and older cancer survivors. (Narsavage & Romeo, 2003, p. 103)
“The study was designed to (1) identify what education and support services were being used, (2) measure satisfaction with current programs and services, and (3) identify what future programs and services were desired”. (Narsavage & Romeo, 2003, p. 105)
In this example, the problem provides a basis for the purpose, and the objectives evolve from the purpose and clearly indicate the foci or goals of the study. The first objective was identification of the variables education and support services used by younger and older cancer survivors (population) in Northeastern Pennsylvania (setting). The second objective was description of the survivors’ satisfaction (variable) with the current programs and services. The third objective was identification of the variables future programs and services that are needed in Northeastern Pennsylvania. The findings from this study identified the need for new types of education and support services, such as weekly radio talk shows and online Internet chat rooms for cancer survivors. In addition, future programs can be improved by tailoring them to the age of the cancer survivor. (Narsavage & Romeo, 2003)
Formulating Objectives in Qualitative Studies
The research objectives formulated for quantitative and qualitative studies have many similarities. However, the objectives directing qualitative studies commonly have a broader focus and include variables or concepts that are more complex and abstract than those of quantitative studies (Munhall, 2001). An ethnographic study by Happ, Swigart, Tate, Hoffman, and Arnold (2007) included objectives to direct their investigation of patients’ involvement in health-related decisions during prolonged critical illness.
Clinicians increasingly recognize the need to involve patients in decision making before, and, if possible, during prolonged critical illness, but have little guidance as to how and when to do this most effectively [problem significance].… Prior reports of studies containing the number of patients able to communicate treatment preferences or to participate in decisions during an acute or critical illness vary from none to as high as 48%.… Moreover, few reports of studies of treatment decision making indicate the criteria used to make decisional capacity assessments [problem background].… Consequently, empirical knowledge of practice in this important area of patient care is limited [problem statement]. (Happ et al., 2007, pp. 361–362).
The purpose of this study was to “describe patterns of communication of patients involved in health-related decision making during prolonged mechanical ventilation (PMV)”. (Happ et al., 2007, p. 362)
The objectives of this study were to “describe: (a) characteristics of patients who were involved in health-related decisions; (b) types of health-related decisions made with patient involvement; (c) how patient involvement occurred; and (d) the extent of patient involvement with health-related decisions during PMV”. (Happ et al., 2007, p. 361)
In this ethnographic study, the problem statement indicated that inadequate research had been conducted on patient involvement in health-related decisions during critical illness, which provided a basis for the study purpose. All four objectives focused on detailed descriptions of the study variables: (1) characteristics of the patients, (2) health-related decision making, and (3) patient involvement in a population of patients on prolonged mechanical ventilation. The findings from this study indicated that families, advanced practice nurses, and physicians were engaging critically ill patients in decision making whenever possible. However, most of the time the patients could not make independent decisions but were able to share decision making with their families and clinicians. These findings emphasize how important it is for families and clinicians to include critically ill patients in health-related decisions at whatever level possible. (Happ et al., 2007)
FORMULATING RESEARCH QUESTIONS
A research question is a concise, interrogative statement that is worded in the present tense and includes one or more variables (or concepts). The research questions focus on (1) the description of the variable(s), (2) a determination of differences between two or more groups regarding selected variables, (3) an examination of relationships among variables (relational), and (4) the use of independent variables to predict a dependent variable.
You might use the following formats for research questions developed for a study (the focus for each is shown in parentheses):
1. How is variable X described by a specified population? (Description)
2. Is there a difference between groups 1 and 2 regarding variable X? (Difference)
3. What is the relationship between variables X and Y in a specified population? (Relational)
4. Are independent variables W, X, and Y useful in predicting dependent variable Z? (Prediction)
Formulating Questions in Quantitative Studies
Cox, Teasley, Lacey, Carroll, and Sexton (2007) conducted a comparative descriptive study to examine environment perceptions of professional nurses working in pediatric and nonpediatric settings. The following excerpts from this study demonstrate the flow from research problem and purpose to research questions.
The professional practice of nursing within the pediatric environment can be both rewarding and challenging.… Although recruitment and retention may be less of a problem in some pediatric hospitals, ensuring a high-quality work environment of pediatric nurses continues to be a priority for nursing leadership [problem significance]. Efforts by multiple researchers have indicated that job satisfaction can be influenced by group cohesion, nurse-physician collaboration, nursing leadership behavior, job stress, pay, time to do nursing interventions in compliance with best practices, and confidence in one’s ability.… (Ernst et al., 2004) [problem background]… Although these preliminary investigations are important, such findings do not elucidate whether pediatric nurses are more or less satisfied than nurses working within nonpediatric environments.… This study will help fill the gaps in the literature related to the differences in support between nurses who work in pediatric facilities and those who work in general acute care sites [problem statement]. (Cox et al., 2007, pp. 9–10)
The purpose of this study was to determine “whether pediatric nurse perceptions of the work environment differed (1) from nurses employed in nonpediatric settings, (2) by the type of pediatric practice setting, or (3) by year of birth”. (Cox et al., 2007, p. 9)
1. Are there significant differences in perceptions of support (manager, unit, or peer), intent to stay, workload, and satisfaction between staff nurses who work in pediatric facilities and those who work in general acute care settings?
2. When looking at pediatric nursing alone, do nurses working in one clinical service area have better or worse work environment than nurses working in another?
3. Do pediatric nurses of different ages have different perceptions of the work environment? (Cox et al., 2007, p. 10)
Question 1 focused on examining differences in work environment perceptions between nurses in pediatric and nonpediatric settings. Questions 2 and 3 focused on examining differences among pediatric nurses based on type of setting and age. All of these questions include variables that were described in the study. The results of this comparative descriptive study indicate that “pediatric nurses had more positive perceptions of unit support, workload, and overall nurse satisfaction than their colleagues working in nonpediatric facilities. Specific to pediatrics, younger nurses and those working in critical care settings seemed to be the happiest with their work environment” (Cox et al., 2007, p. 9). The evidence from this study can help nurse managers to retain nurses in pediatric settings.
Formulating Questions in Qualitative Studies
The questions directing qualitative studies are often limited in number, have a broad focus, and include variables or concepts that are more complex and abstract than those included in quantitative studies. Marshall and Rossman (2006) have indicated that questions developed to direct qualitative research might be theoretical ones, which can be studied with different populations or in a variety of sites or the questions could be focused on a particular population or setting. Polzer (2007) conducted a qualitative study to describe African Americans with type 2 diabetes. The goal was to examine the participants’ perceptions of the spiritual role of health care providers (HCPs) and its effects on how the participants managed their diabetes. The problem, purpose, and research questions used to direct this study are presented in the following excerpts.
The establishment of quality patient/provider relationships is paramount in empowering patients to manage chronic illnesses.… Type 2 diabetes mellitus is a major health problem for African Americans, and is one of the primary causes of morbidity and mortality in this population (Center for Disease Control [CDC], 2005) [problem significance].… For many African Americans, spirituality is a source of support in managing diabetes.… Some, however, may also turn their self-management practices over to God in lieu of following health provider recommendations… In a recent grounded theory study (Polzer & Miles, 2007; parent study),… examined how spirituality affected self-management of diabetes in African Americans. The core construct identified in this study was self-management through a relationship with God. Based on their views, participates fell into one of three typologies: Relationship and Responsibility: God is in the Background; Relationship and Responsibility: God is in the Forefront; and Relationship and Relinquishing of Self-Management: God is Healer.… The three typologies shed light on how African Americans viewed their relationship with God, its impact on self-management, and how these perceptions affected their beliefs about HCPs helping them manage their diabetes [problem background]. Knowledge of these perceptions of spiritual care is important as there is little information related to spiritual interventions for African Americans [problem statement]. (Polzer, 2007, pp. 164–166)
Based on the grounded theory study [Polzer & Miles, 2007], a qualitative descriptive study was conducted to examine these perceptions of spiritual care, and further extend the three typologies (Polzer, 2007, p. 166)
The research questions addressed in this analysis were:
1. What are the perceptions of African Americans with diabetes regarding how, if, and when nurses and other HCPs should address spirituality in their care?
2. How do these perceptions differ by typology of self-management through a relationship with God? (Polzer, 2007, p. 166)
The first study question focused on developing a description of African Americans’ (population) perceptions of the complex concept of health care providers addressing spirituality in their care. The second question focused on examining differences in the African Americans’ perceptions based on their relationship with God. Based on her study findings, Polzer (2007) identified the following implications for practice: “The model of the three typologies may help health providers understand the importance of spiritual care for some African Americans, as well as how this care can affect self-management. This information also may assist in developing culturally sensitive interventions to improve self-management of diabetes among African Americans”. (p. 173)
FORMULATING HYPOTHESES
A hypothesis is the formal statement of the expected relationship or relationships between two or more variables in a specified population. The hypothesis translates the problem and purpose into a clear explanation or prediction of the expected results or outcomes of the study. This section describes the purpose, sources, and types of hypotheses and the process for developing and testing hypotheses in studies.
Purpose of Hypotheses
The purpose of a hypothesis is similar to that of research objectives and questions. A hypothesis (1) specifies the variables you will manipulate or measure, (2) identifies the population you will examine, (3) indicates the type of research, and (4) directs the conduct of your study. Hypotheses also influence the study design, sampling technique, data collection and analysis methods, and interpretation of findings. Hypotheses differ from objectives and questions by predicting the outcomes of a study, and the research findings indicate support for or rejection of each hypothesis.
Hypothesis testing allows us to generate knowledge by testing theoretical statements or relationships that were identified in previous research, proposed by theorists, or observed in practice. In addition, hypotheses direct the testing of new treatments and are often viewed as tools for uncovering ideas rather than as ends in themselves (Beveridge, 1950).
Sources of Hypotheses
We generate hypotheses by observing phenomena or problems in nursing practice, analyzing theory, and reviewing the literature. Many hypotheses originate from real-life experiences. Clinicians and researchers observe events in the world and identify relationships among these events (theorizing), which are the bases for formulating hypotheses. For example, you may notice that the hospitalized patient who complains the most receives the most pain medicine. The relationship identified is a prediction about events in clinical practice that has potential for empirical testing. You could use a literature review to identify a theory that supports this relationship.
Fagerhaugh and Strauss (1977) developed a theory of pain management and identified the following relationship or proposition: As expressions of pain increase, pain management increases. The researchers developed this proposition through the use of grounded theory research. Additional testing is necessary to determine its usefulness in describing how patients express pain and how that pain is managed in a variety of practice situations. On the basis of theory and clinical observation, the following hypothesis might be formulated: The more frequently a hospitalized patient complains of pain, the more often doses of analgesic medications are administered.
Some hypotheses are initially generated from relationships expressed in a theory, when the intent of the researcher is to test a theory (Chinn & Kramer, 2008). When a theory is being tested, the propositions (relationships) expressed in the theory are used to generate hypotheses. For example, Jennings-Dozier (1999) tested the theory of planned behavior (TPB) in predicting the intentions of African-American and Latina women to obtain a Pap smear. Figure 8-1 illustrates a model of the TPB developed by Ajzen (1985). This model includes direct and indirect relationships among the concepts, as indicated in the following propositions. These propositions provided the basis for the study hypotheses generated by Jennings-Dozier (1999):
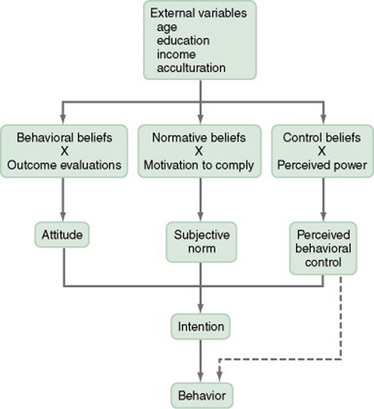
1. External variables (age, education, income, and acculturation) have a direct effect on behavioral beliefs, normative beliefs, and control beliefs.
2. Behavioral beliefs have a direct effect on attitude; normative beliefs have a direct effect on subjective norm; and control beliefs have a direct effect on perceived behavioral control.
3. Attitude, subjective norm, and perceived behavioral control have a direct effect on intention.
4. Intention has a direct effect on behavior.
5. External variables have an indirect effect on attitude, subjective norm, and perceived control.
6. External variables have an indirect effect on intention.
7. Behavioral beliefs, normative beliefs, and control beliefs have an indirect effect on intention.
Jennings-Dozier’s (1999) first hypothesis was as follows:
The seven propositions from the TPB, listed previously, can be linked to this study hypothesis in the following way:
Jennings-Dozier’s (1999) second hypothesis was as follows.
The seven propositions from TPB can be linked to the second study hypothesis in the following way:
These hypotheses were formulated to test the propositions from Ajzen’s theory of planned behavior (TPB). The study findings indicated that attitude and perceived behavior control were predictors of a patient’s intentions to obtain a Pap smear but that the subjective norms were not. Thus, the study supported some of the relationships in the TPB but not others (Jennings-Dozier, 1999). Further research is needed to determine the effectiveness of the TPB to explain the intentions of women of varying ages, cultures, and socioeconomic level to obtain a Pap smear. The evidence generated from these types of studies could be used to develop and test interventions to encourage and support women in getting Pap smears.
Reviewing the literature and synthesizing findings from different studies can also be used to generate hypotheses. For example, Anderson, Higgins, and Rozmus (1999) synthesized the findings from several studies focused on the outcomes of coronary artery bypass graft (CABG) surgery and formulated the following hypotheses to direct their study:
The results of this study supported the first hypothesis because patients who stayed 1 day in the ICU had significantly earlier ambulation than those staying 2 days in the ICU. The researchers rejected the second hypothesis because there was no significant difference in postoperative length of stay between patients who stayed 1 day and those who stayed 2 days in the ICU. These mixed findings indicate the need for this study to be replicated and for further research in this problem area.
Types of Hypotheses
Hypotheses identify different types of relationships and numbers of variables. Studies might have one, three, or more hypotheses, depending on the complexity and scope of the study. The type of hypothesis you develop will be based on the problem and purpose of your study. Hypotheses are described using the terms in the following four categories: (1) associative versus causal, (2) simple versus complex, (3) directional versus nondirectional, and (4) null versus research.
Associative versus Causal Hypotheses
The relationships in hypotheses are identified as associative or causal. An associative relationship identifies variables that occur or exist together in practice, and as one variable changes so does the other (Reynolds, 1971). For example, research indicates there is an associative relationship between anxiety and depression, and as a person’s depression changes so does the anxiety level. Thus, associative hypotheses are developed to examine relationships among variables in a study. The format used for expressing associative hypotheses follows:
1. Variable X is related to or associated with variable Y in a specified population. (Predicts a relationship between two variables but does not indicate the type of relationship.)
2. An increase in variable X is related to an increase in variable Y in a specified population. (Predicts a positive relationship.)
3. A decrease in variable X is related to a decrease in variable Y in a specified population. (Predicts a positive relationship.)
4. An increase in variable X is related to a decrease in variable Y in a specified population. (Predicts a negative or inverse relationship.)
5. Variables X and Y can be used to predict variable Z in a study. (The independent variables of X and Y are used to predict the dependent variable Z in a predictive correlational study.)
Associative hypotheses identify relationships among variables in a study but do not indicate that one variable causes an effect on another variable.
Reishtein (2005) conducted a predictive correlational study to examine the relationships between symptoms and functional performance in patients with chronic obstructed pulmonary disease (COPD). Reishtein used the following associative hypotheses to guide the study:
3. Dyspnea, fatigue, and sleep difficulty, taken together, will explain more of the variance in functional performance in people with COPD than any of these symptoms alone. (Reishtein, 2005, p. 40)
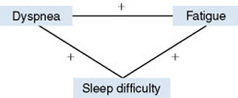
Hypothesis 1 predicts positive relationships or associations among the variables of dyspnea, fatigue, and sleep difficulty for patients with COPD. A positive relationship means that the variables change together; thus, they will all increase together in value or all decrease together. These relationships are depicted in the following diagram:
Hypothesis 2 predicts relationships between three variables—dyspnea, fatigue, and sleep difficulty—and the variable functional performance, but it does not identify the type of relationship. These relationships are shown in the following diagram:
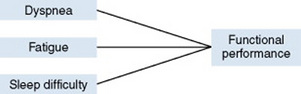
Hypothesis 3 uses the independent variables of dyspnea, fatigue, and sleep difficulty to predict the dependent or outcome variable functional performance in COPD patients. The predictive relationship is shown in the following diagram:

The results from Reishtein’s (2005) study partially supported hypothesis 1 in that dyspnea had positive, significant relationships with fatigue (r = 0.43, p < 0.001) and sleep difficulty (r = 0.39, p < 0.001), but fatigue and sleep difficulty were positively but not significantly related (r = 0.19). Hypothesis 2 was also partially supported in that dyspnea (r = −0.54, p < 0.001) and fatigue (r = −0.24, p < 0.01) were significantly, negatively related to functional performance, but sleep difficulty (r = −0.17) was not. Thus, in hypothesis 3, dyspnea was the most predictive of functional performance with fatigue and sleep difficulty providing limited prediction. Thus, managing dyspnea may be the best way to improve the symptoms and functional performance in patients with COPD. Additional research may distinguish other symptoms that might predict functional performance in COPD patients and thereby help them to manage this disease.
Causal relationships identify a cause-and-effect interaction between two or more variables, which are referred to as independent and dependent variables. The independent variable (intervention, treatment, or experimental variable) is manipulated or varied by the researcher to cause an effect on the dependent variable. The dependent variable (response or outcome variable) is measured to examine the effect created by the independent variable. A format for stating a causal hypothesis is as follows: The subjects in the experimental group who are exposed to the independent variable X demonstrate greater change, dependent variable Y, than do the subjects in the control or comparison group who are not exposed to the independent variable.
Artinian, Washington, and Templin (2001, p. 191) studied the “effects of the home telemonitoring and community-based monitoring on blood pressure control in urban African Americans.” The following causal hypothesis was used to direct their study:
The independent variables are the two types of nurse-managed BP monitoring, HT and CBM, and the dependent variable is BP (systolic and diastolic pressures). The population is clearly identified as African Americans with hypertension, who were recruited from a family community center in Detroit (setting). The findings from this study supported the hypothesis, indicating that the two monitoring interventions, HT and CBM, were significantly more effective than usual care in improving BP (systolic and diastolic pressures) in hypertensive African Americans. A causal arrow (α) is used to show the hypothesized relationships among the independent and dependent variables in the following diagram:

Simple versus Complex Hypotheses
A simple hypothesis predicts the relationship (associative or causal) between two variables. One format for stating a simple associative hypothesis is as follows: Variable X is related to variable Y. A simple causal hypothesis identifies the relationship between one independent variable and one dependent variable, for example, independent variable X causes a change in dependent variable Y. Vasan et al. (2003) studied the relationship of elevated plasma homocysteine levels with the risk for congestive heart failure (CHF) in adults without prior myocardial infarction (MI). A simple, associative hypothesis was developed to direct this study: “We hypothesized that elevated plasma homocysteine levels are associated with an increased risk for CHF” (Vasan et al., 2003, p. 1251). The following diagram demonstrates the positive relationship that was predicted between the two study variables of plasma homocysteine level and risk for CHF:

The results of this 8-year study indicated that elevated plasma homocysteine concentration was related positively and strongly to CHF risk in both men and women who did not have a prior history of an MI. The hypothesis was supported in this study, indicating that nurse practitioners and clinical nurse specialists might examine plasma homocysteine levels in individuals with a family history of CHF and treat those levels as needed.
A complex hypothesis predicts the relationship (associative or causal) among three or more variables. A complex associative hypothesis predicts the relationships among three or more variables, such as the relationships among the variables X, Y, and Z. Complex causal hypotheses also include three or more variables but predict the effects of one independent variable on two (or more) dependent variables or predicting the effects of two or more independent variables on one or more dependent variables. For example, Rawl et al. (2002) studied the effects of a computer-based nursing intervention on the psychological functioning of newly diagnosed cancer patients. The following complex, causal hypothesis was developed to direct their study: “Patients with cancer who received the intervention were hypothesized to have higher psychological functioning scores and lower depression and anxiety scores than those receiving standard care” (Rawl et al., 2002, p. 968).
This causal hypothesis has one independent variable (computer-based nursing intervention) and three dependent variables (psychological functioning, depression, and anxiety scores) and identifies the population of the study (cancer patients). A diagram of this hypothesis follows, with causal arrows (α) indicating the cause-and-effect relationship between the independent variable (IV) and dependent variables (DVs):
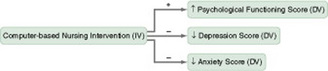
The findings from this study support part of this hypothesis, because the cancer patients exposed to the computer-based nursing intervention had significantly lower depression and anxiety scores but did not have a significant improvement in the psychological functioning score when compared to those subjects receiving standard care. This intervention offers potential benefits for nursing practice, but it requires additional investigation to determine its effectiveness in managing the emotional needs of cancer patients. Often, in practice situations, multiple variables cause an event, or an intervention results in multiple outcomes. Therefore, complex rather than simple causal hypotheses are often more representative of nursing practice.
Nondirectional versus Directional Hypotheses
A nondirectional hypothesis states that a relationship exists but does not predict the nature of the relationship. If the direction of the relationship being studied is not clear in clinical practice or the theoretical or empirical literature, the researcher has no clear indication of the nature of the relationship and states a nondirectional hypothesis. For example, Reishtein’s (2005, p. 4) second hypothesis (introduced earlier in this chapter) is nondirectional: “Dyspnea, fatigue, and sleep difficulty are related to functional performance.” This hypothesis indicates that dyspnea, fatigue, and sleep difficulty are related to functional performance, but it does not indicate the direction or nature (positive or negative) of the relationship. This hypothesis is nondirectional, complex (four variables), and associative (indicating a relationship exists).
A directional hypothesis states the nature or direction of the relationship between two or more variables. These hypotheses are developed from theoretical statements, findings of previous studies, and clinical experience. As the knowledge on which a study is based increases, the researcher is able to predict the direction of a relationship between the variables being studied. Terms such as less, more, increase, decrease, greater, and smaller indicate the directions of relationships in hypotheses. Directional hypotheses can be associative or causal and simple or complex.
McDonald, Frakes, Apostolidis, Armstrong, Goldblatt, and Bernardo (2003, p. 226) hypothesized that nurses providing care for patients with a psychiatric diagnosis “(a) estimate a lower probability that the patient was experiencing a myocardial infraction, (b) plan less time for nursing care, (c) delegate more patient care activities to ancillary staff, and (d) do not identify additional ambiguous symptoms as possible evidence of an evolving myocardial infarction.” This complex, associative, directional hypothesis was supported by the findings, indicating that nurses provided lower quality of care for acute medical conditions when the patients had a psychiatric diagnosis than when they did not. Evidence from this study indicates that patients with a psychiatric diagnosis are vulnerable when experiencing acute medical problems. It is important for nurses to avoid stereotyping patients with psychiatric diagnoses and to focus on identifying and managing the patient’s medical problem.
A causal hypothesis predicts the effect of an independent variable on a dependent variable, specifying the direction of the relationship. Thus, all causal hypotheses are directional. Efe and Özer (2007) examined the pain-relieving effect of breast-feeding during immunization injections in healthy neonates and used a causal hypothesis to direct their study. “The hypothesis tested was that breast-feeding would decrease the length of crying time, prevent an increase in heart rate, and prevent a decrease in oxygen saturation during vaccination as compared with the control condition (i.e., no breast-feeding)” (Efe & Özer, 2007, p. 11). This causal hypothesis predicted the effect of an intervention or independent variable of breast-feeding during immunization injections on the dependent variables of length of crying time, heart rate, and oxygen saturation. Thus, this is a complex (four variables), directional (decrease crying time and prevent increased heart rate and decreased oxygen saturation), causal hypothesis. The breast-feeding significantly decreased crying time but did not significantly affect the neonates’ heart rate or oxygen saturation. Because breast-feeding did decrease neonate crying time during immunizations, nurses might encourage mothers to implement this safe, easy, effective intervention.
Null versus Research Hypotheses
The null hypothesis (H0), also referred to as a statistical hypothesis, is used for statistical testing and interpretation of statistical outcomes. Even if the null hypothesis is not stated, it is implied, because it is the converse of the research hypothesis (Kerlinger & Lee, 2000). A null hypothesis can be simple or complex and associative or causal. An associative null hypothesis states that there is no relationship between the variables studied. A causal null hypothesis might be stated in one of the following formats:
1. The independent variable has no effect on the dependent variable.
2. The experimental group, who received the independent variable, is no different than the control group for the dependent variable.
Schultz, Drew, and Hewitt (2002) conducted a quasi-experimental study to determine the effectiveness of heparinized and normal saline flushes in maintaining the patency of 24-gauge (G) intermittent peripheral intravenous (IV) catheters in neonates in intensive care. “The hypothesis stated that there would be no significant difference in the duration of patency of a 24 G IV lock in a neonatal patient when flushed with 0.5 mL [millimeters] of heparinized saline (2U/mL), our standard practice, compared with 0.5 mL of 0.9% normal saline” (Schultz et al., 2002, p. 30).
This is a simple, null hypothesis with one independent variable (0.9% normal saline flush) and one dependent variable (patency of 24 G IV catheter). The comparison group received standard care of heparinized saline flush, and the population was neonates in an intensive care setting. The findings of the study did not support the null hypothesis because the catheters flushed with heparinized saline were patent significantly longer than the catheters flushed with normal saline. Thus, the researchers recommended continuing the use of heparinized saline as the standard for flushing 24 G catheters in infants.
A research hypothesis is the alternative hypothesis (H1 or Ha) to the null. The research hypothesis states that there is a relationship between two or more variables, and it can be simple or complex, nondirectional or directional, and associative or causal. The prediction in a research hypothesis must be based on theoretical statements, previous research findings, or clinical experience. All the previous examples of hypotheses presented in this chapter were research hypotheses except for the one null hypothesis. Researchers have different beliefs about when to state a research hypothesis versus a null hypothesis. Some researchers state the null hypothesis because it is more easily interpreted on the basis of the results of statistical analyses. A researcher will also use the null hypothesis when she or he believes there is no relationship between two or more variables and when there is inadequate theoretical or empirical information to state a research hypothesis. Otherwise it is best to state a research hypothesis that clearly predicts the outcome of a study (Kerlinger & Lee, 2000).
Cheng, Studdiford, Chambers, Diamond, and Paynter (2002) developed both a null hypothesis and a research hypothesis to direct their study of the consistency of patient self-reported blood pressures (BPs) and stored monitor BPs. They developed a simple, associate, null hypothesis: “Patient-reported blood pressures would not consistently match electronically stored pressures” (Cheng et al., 2002, p. 260). They also stated a simple, directional, research hypothesis: “Electronically stored pressures unreported by patients would be higher, on average, than reported pressures” (Cheng et al., 2002, p. 260). The findings from this study encouraged the researchers to reject both the null and research hypotheses and to make the following recommendation for practice: “The reliability of self-reporting of blood pressures for many patients supports the potential usefulness of self-monitoring of blood pressure in hypertension management” (Cheng et al., 2002, p. 259).
Developing Hypotheses
Developing hypotheses requires inductive and deductive thinking. Most people have a predominant way of thinking and will use that thinking pattern in developing hypotheses. Inductive thinkers have a tendency to focus on the relationships they observe in clinical practice, and they synthesize these observations to formulate a general statement about the relationships (Chinn & Kramer, 2008). For example, inductive thinkers might note that elderly patients who are not instructed about the reasons for early postoperative ambulation make no effort to get out of bed. Deductive thinkers examine more abstract statements from theories or previous research and then formulate a hypothesis for study. Deductive thinkers might translate a statement or proposition, such as “people who receive education about self-care are more capable in caring for themselves,” from Orem’s (2001) theory into a hypothesis.
The inductive thinker must link the relational statement or hypothesis that was developed from clinical observations with a theoretical framework. Making this connection with the framework requires deductive thinking and improves the usefulness of the study findings. The deductive thinker must use inductive thinking to determine whether the proposition from a theory accurately predicts the relationship of events in clinical practice. Without this real-world experience, the selection of subjects and the identification of ways to measure the variables would be unclear. An example hypothesis is, “Elderly patients who receive an educational program and handout about activity following surgery ambulate earlier and have a shorter hospital stay after surgery than elderly patients who receive standard care.”
In formulating a hypothesis, you as a researcher will have several decisions to make. These decisions are directed by the problem studied and by your own expertise and preference. You must decide whether the problem is best investigated with the use of simple or complex hypotheses. Complex hypotheses frequently require complex methodology, and the outcomes may be difficult to interpret. Some beginning researchers prefer the clarity of simple hypotheses.
The research problem and purpose determine whether you will study an associative or a causal relationship. Testing a hypothesis that states a causal relationship requires expertise in implementing a treatment and controlling extraneous variables. Another decision you must make involves the formulation of a research or a null hypothesis. You must make this decision according to what you believe is the most accurate prediction of the relationship between the study variables.
A hypothesis that is clearly and concisely stated gives the greatest direction for conducting a study. For clarity, hypotheses are expressed as declarative statements written in the present tense. Thus, hypotheses must be written without the phrase “There will be no relationship…,” because the future tense refers to the sample being studied. Hypotheses are statements of relationships about populations, not about study samples. According to mathematical theory regarding generalization, one cannot generalize to the future (Kerlinger & Lee, 2000).
Hypotheses are clearer without the phrase “There is no significant difference…,” because the level of significance is only a statistical technique applied to sample data (Armstrong, 1981). In addition, hypotheses should not identify methodological points, such as techniques of sampling, measurement, and data analysis (Kerlinger & Lee, 2000). Therefore, statements such as “measured by,” “in a random sample of,” or “using ANOVA (analysis of variance)” are not appropriate. These phrases limit hypotheses to measurement methods, sampling methods, or data analysis techniques in a single study. Hypotheses must reflect the variables and population outlined in the research problem and should not be limited to a single study. A well-formulated hypothesis clearly identifies the relationship between the variables. There is no set number for how many hypotheses are needed to direct a study, but the number formulated usually reflects the researcher’s expertise and the complexity of the problem and purpose. However, most studies contain one to three hypotheses, and the relationships identified in these hypotheses set the limits for a study.
Testing Hypotheses
A hypothesis’s value is ultimately derived from whether or not it can be tested in the real world. A testable hypothesis contains variables that can be measured or manipulated in practice. For example, Efe and Özer (2007) manipulated the breast-feeding intervention in their study using set protocol so that the treatment was consistently manipulated for each study situation. They measured crying time in seconds and measured the heart rate and oxygen saturation with a pulse oximeter (Nellcor N180).
Hypotheses are evaluated with statistical analyses. If the hypothesis states an associative relationship, correlational analyses are usually conducted on the data. The Spearman rank order correlation coefficient is often used to analyze ordinal level data, and the Pearson’s product-moment correlation coefficient is used for interval and ratio level data (see Chapter 20). These correlational analyses determine the existence, type, and degree of the relationship between the variables studied.
A hypothesis that states a causal relationship is analyzed through the use of statistics that examine differences, such as Mann-Whitney U,t-test, and analysis of variance (ANOVA) (see Chapter 22). It is the null hypothesis (stated or implied) that is tested. The intent is to determine whether the independent variable had a significant effect on the dependent variable. The level of significance, alpha (αα) = 0.05, 0.01, 0.001, is set after the generation of causal hypotheses and before the conduct of the study. To learn more about selecting statistical tests and a level of significance for testing hypotheses, see Chapter 18.
The results obtained from testing a hypothesis are described with the use of certain terminology. Research findings do not prove hypotheses true or false; instead, hypotheses are statements of relationships or differences in populations. Even after a series of studies, the word proven is not used in scientific language because of the tentative nature of science. Research hypotheses are described as being supported or not supported in a study. When a null hypothesis is tested, it is either rejected or accepted. Accepting the null hypothesis indicates that no relationship or effect was found among the variables. Rejecting the null hypothesis indicates the possibility that a relationship or difference exists. A study might partially support a complex hypothesis. Efe and Özer’s (2007, p. 11) hypothesis stated that “breast-feeding decreases the length of crying time, prevents an increase in heart rate, and prevents a decrease in oxygen saturation during vaccination as compared with the control condition (i.e., no breast feeding).” Their study supported the decreased crying time part of the hypothesis, but it did not support the part of the hypothesis that focused on the prevention of increased heart rate and decreased oxygen saturation. However, the study did provide valuable evidence about the effectiveness of breast-feeding in reducing the pain of immunization injections in infants. In addition, this study provides direction for future research.
SELECTING OBJECTIVES, QUESTIONS, OR HYPOTHESES FOR QUANTITATIVE OR QUALITATIVE RESEARCH
Selecting objectives, questions, or hypotheses for a study is often based on (1) the number and quality of relevant studies conducted on a selected problem (existing knowledge base), (2) the framework of the study, (3) the expertise and preference of the researcher, and (4) the type of study to be conducted (quantitative or qualitative). Commonly, if minimal or no research has been conducted on a problem, investigators state objectives or questions because they do not have the knowledge necessary to formulate hypotheses. The framework for a study indicates whether the intent is to develop or to test theory. Objectives and questions are usually stated to guide theory development, and the focus of a hypothesis is to test theory.
Researcher expertise and preference can also influence the selection of objectives, questions, or hypotheses to direct a study. Moody, Wilson, Smyth, Schwartz, Tittle, and Van Cott (1988) analyzed the focus of nursing practice research from 1977 to 1986 and found that 16% of the studies had research questions and 31% contained hypotheses. The number of nursing studies containing hypotheses continues to grow, and there appears to be a “trend away from descriptive and fact-finding studies toward efforts to establish relationships between variables and to test hypotheses” (Brown, Tanner, & Padrick, 1984, p. 31). The greater use of hypotheses to direct research could indicate the growth of knowledge in selected problem areas and the increasing sophistication of nurse researchers. However, Brown et al. (1984) noted that only 51% of the studies they reviewed contained explicitly stated hypotheses; the other studies had implicit or implied hypotheses. An explicit statement of hypotheses is important to provide clear direction for both the conduct of a study and the use of the findings in practice.
The objectives, questions, or hypotheses designated for study frequently indicate a pattern that the researcher uses in conducting investigations. Problems can be investigated in a variety of ways. Some researchers start at the core of a problem and work their way outward. Other investigators study a problem from the outside edge and work to the core (Kaplan, 1964). Each study must logically build on the other, as the researcher establishes a pattern for studying a problem area that will affect the quality and quantity of the knowledge generated in that area.
Researchers select objectives, questions, or hypotheses according to the type of study they plan to conduct. Objectives and questions are typically stated when the intent of the study is to identify or describe characteristics of variables, to examine relationships among variables, or both. Thus, objectives or questions are often formulated to direct qualitative and selected quantitative (descriptive and correlational) studies (Table 8-1). However, some experienced researchers can clearly focus and develop a study without using objectives or questions. In these studies, a research purpose directs the research process.
TABLE 8-1
Selecting Objectives, Questions, or Hypotheses for Different Types of Research
| Type of Research | Use of Objectives, Questions, or Hypotheses? |
| Qualitative research | Objectives, questions, or none |
| Quantitative research | |
| Descriptive studies | Objectives, questions, or none |
| Correlational studies | Objectives, questions, hypotheses, or none |
| Quasi-experimental studies | Usually hypotheses |
| Experimental studies | Hypotheses |
In some qualitative research, the investigator uses only a problem and purpose to direct the study. The specification of objectives or questions might limit the scope of the study and the methods of data collection and analysis (Munhall, 2001). Discovery is important in qualitative research, and sometimes the “research questions may be unclear, the objectives ambiguous, and the final outcome uncertain. Hypotheses and detailed accounts of precise research strategies are neither necessary nor desirable in a well constructed qualitative design” (Aamodt, 1983, p. 399).
Researchers often develop hypotheses when the relationships or results of a study can be anticipated or predicted. Hypotheses are typically used in quantitative research to direct predictive correlational, quasi-experimental, and experimental studies.
IDENTIFYING AND DEFINING STUDY VARIABLES
The research purpose and objectives, questions, and hypotheses identify the variables or concepts to be examined in a study. Variables are qualities, properties, or characteristics of persons, things, or situations that change or vary in a study. Variables are characterized by degrees, amounts, and differences within a study. Variables are also concepts of various levels of abstraction that are concisely defined so that they can be measured or manipulated within a study (Kaplan, 1964; Moody, 1990).
The concepts examined in research can be concrete and directly measurable in practice, such as heart rate, hemoglobin value, and tidal volume of the lung. These concrete concepts are usually referred to as variables in a study. Other concepts, such as anxiety, coping, and pain, are more abstract and are indirectly observable in the real world (Chinn & Cramer, 2008). Thus, the properties of these concepts are inferred from a combination of measurements. For example, one can infer the properties of anxiety by combining information obtained from (1) observing the signs and symptoms of anxiety (frequent movements, sweating, lack of eye contact, and verbalization of anxiety), (2) examining completed questionnaires or scales (A-state and trait anxiety scales), and (3) measuring physiological responses (galvanic skin response). The concept of anxiety might be represented by the variables “reported anxiety” or “perceived level of anxiety.”
In many qualitative studies and in some quantitative studies (descriptive and correlational), the focus is abstract concepts, such as grieving, caring, and promoting health (Marshall & Rossman, 2006; Munhall, 2001). Researchers identify the elements of the study as concepts, not variables. In the ethnographic study previously described, Happ et al. (2007) investigated the concept of health-related decision making by critically ill patients during prolonged mechanical ventilations (PMV). The concept health-related decision making was defined as “choices about initiating, continuing, or discontinuing treatment, diagnostics, or therapeutic care activities” (p. 363). In this study, health-related decision making was operationalized to include the following:
choices about mechanical ventilation and other therapies, such as invasive diagnostic procedures and placement of central lines and nutritional access devices that may or may not require written informed consent, and about discharge placement. Financial or legal decisions, such as appointment of a power of attorney or signing financial documents to enable insurance payment for health care, were considered health-related in the context of prolonged critical illness. (Happ et al., 2007, p. 363)
Types of Variables
Variables have been classified into a variety of types to explain their use in research. Some variables are manipulated; others are controlled. Some variables are identified but not measured; others are measured with refined measurement devices. The types of variables presented in this section are independent, dependent, research, extraneous, demographic, moderator, and mediator.
Independent and Dependent Variables
The relationship between independent variables and dependent variables is the basis for formulating hypotheses for correlational, quasi-experimental, and experimental studies. An independent variable is a stimulus or activity that the researcher manipulates or varies to create an effect on the dependent variable. The independent variable is also called an intervention, treatment, or experimental variable.
A dependent variable is the response, behavior, or outcome that the researcher wants to predict or explain. Changes in the dependent variable are presumed to be caused by the independent variable. The dependent variable can also be called an effect or outcome variable or a criterion measure (Kerlinger & Lee, 2000).
The null hypothesis developed by Schultz et al. (2002, p. 30), introduced earlier in the chapter, “stated that there would be no significant difference in the duration of patency of a 24 G IV lock in a neonatal patient when flushed with 0.5 mL [millimeters] of heparinized saline (2U/mL), our standard practice, compared with 0.5 mL of 0.9% normal saline.” The independent variable that was manipulated in this study was the 0.5 mL of 0.9% normal saline flush and the dependent variable that was measured was the patency of the 24 G IV. The 0.5 mL of heparinized saline was the standard care for flushing the 24 G IVs of the neonates in the comparison group.
Research Variables or Concepts
Qualitative studies and some quantitative (descriptive and correlational) studies involve the investigation of research variables or concepts. Research variables or concepts are the qualities, properties, or characteristics identified in the research purpose and objectives or questions that are observed or measured in a study. They are used when the intent of the study is to observe or measure variables as they exist in a natural setting without the implementation of a treatment. Thus, no independent variables are manipulated, and no cause-and-effect relationships are examined.
Qualitative studies often focus on abstract concepts. For example, Orne et al. (2000, p. 205) conducted a qualitative phenomenological study of the “experience of being medically uninsured from the perspective of American workers who have lived it.” The study was directed by the following research question: “What is the lived experience of being employed but medically uninsured?” (Orne, Fishman, Manka, & Pagnozzi, 2000, p. 205). This study focused on describing the research concept of the experience of medically uninsured in a population of employed adults. We will define this research concept, conceptually and operationally, later in this chapter.
Extraneous Variables
Extraneous variables exist in all studies and can affect the measurement of study variables and the relationships among them. Extraneous variables are of primary concern in quantitative studies, because they can obscure one’s understanding of the relational or causal dynamics within the studies. Extraneous variables are classified as (1) recognized or unrecognized and (2) controlled or uncontrolled.
The extraneous variables that are not recognized until the study is in process or are recognized before the study is initiated but cannot be controlled are referred to as confounding variables. Sometimes these variables can be measured during the study and controlled statistically during analysis. In other cases, it is not possible to measure a confounding variable, and the variable thus hinders the interpretation of findings. Such extraneous variables must be identified as limitations or areas of study weakness in the discussion section of a research report. As control decreases in quasi-experimental and experimental studies, the potential influence of confounding variables increases.
Researchers attempt to recognize and control as many extraneous variables as possible in quasi-experimental and experimental studies, and specific designs have been developed to control the influence of such variables (see Chapter 11). Schultz et al. (2002) controlled some of the extraneous variables in their study, previously described, by implementing a double-blind experimental design, using specific inclusion and exclusion criteria for sample selection, training the nursing staff participating in the study, and randomizing the subjects to groups. The following excerpt identifies the controls the researchers used in their study to decrease the effect of extraneous variables and bias and to increase the likelihood that the findings are an accurate reflection of reality and not due to error.
Inclusion criteria were all neonates younger than 30 days with a new 24 G IV lock 3/4 inch in length. Exclusion criteria were neonates with central catheters, recent surgery, a diagnosis of disseminated intravascular coagulopathy or idiopathic thrombocytopenia, or current or previous treatment of a patent ductus arteriosis with indomethacin.…
… Competency was established for the flushing procedure by having each nurse pass a quiz on IV lock flush protocol with a score of 90% or higher and show proper IV lock flush technique. All staff nurses completed the requirements to participate in the study.…
… Only the first IV lock per infant was included in the study.… Randomization of subjects occurred in the pharmacy on receipt of an order for the study solution and a copy of the informed consent.… Study solutions were prepared, coded, and labeled in the pharmacy and delivered to the NICU [neonatal intensive care unit]. All staff members, including the study investigators, were blinded to the study group. Only the pharmacist knew the results of the randomization. (p. 30)
Environmental variables are a type of extraneous variable that make up the setting in which the study is conducted. Examples are climate, home, health care system, community setting, and governmental organizations. If a researcher is studying humans in an uncontrolled or natural setting, it is impossible and undesirable to control all the environmental variables. In qualitative and some quantitative (descriptive and correlational) studies, researchers make little or no attempt to control environmental variables. Their intent is to study subjects in their natural environment without controlling or altering it. The environmental variables in quasi-experimental and experimental research can be controlled through the use of a study protocol and a laboratory setting or a specially constructed research unit in a hospital.
In intervention effectiveness research, the extraneous variables are referred to as contextual variables. Contextual variables are those factors that could influence the implementation of an intervention and thus the outcomes of the study (Sidani & Braden, 1998). These contextual or extraneous factors include social and environmental setting and individual variables that can influence the intervention and study outcomes.
For a study to yield the best understanding of an intervention and its usefulness to practice, the study design must provide for the examination of relevant contextual variables and link them to the study interventions and outcomes. Thus, rather than controlling or preventing the influence of extraneous variables as do quasi-experimental and experimental research, intervention effectiveness research focuses on studying them. Identifying and studying the effects of contextual (extraneous) variables greatly increases the complexity of a study, but it also improves the accuracy of the findings for practice. Intervention effectiveness research is the focus of Chapter 13.
Demographic Variables
Demographic variables are attributes of the subjects that are measured during the study and used to describe the sample. Some common demographic variables examined in nursing research are age, gender, ethnicity, educational level, income, job classification, length of hospital stay, and medical diagnosis. Researchers select demographic variables based on the focus of their study, the demographic variables included in previous studies, and clinical experience. However, age, gender, and ethnicity are essential demographic variables to examine in all types of research. These demographics describe the sample and determine the population for generalization of the findings. More research is needed to improve health care for elderly, women, children, and minorities, and funding agencies often give priority to studies that focus on these individuals.
To obtain data on demographic variables, subjects are asked to complete a demographic or information sheet. When the study is completed, the demographic information is analyzed to provide a picture of the sample, which is called the sample characteristics. Sample characteristics are presented in a table or discussed in the narrative of the research report (or both). As previously discussed, Schultz et al. (2002) studied the effects of heparinized saline versus normal saline in promoting patency of IV catheters in neonates. They summarized their sample characteristics in a table (Table 8-2) and discussed them in the narrative of their article:
TABLE 8-2
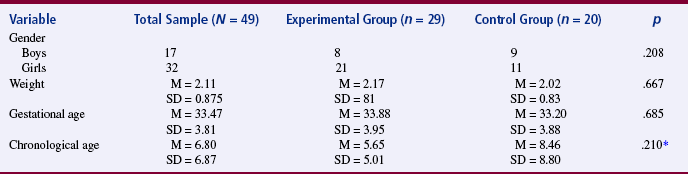
*Significance based on unequal variances.
From Schultz, A. A., Drew, D, & Hewitt, H. (2002). Comparison of normal saline and heparinized saline for patency of IV Locks in neonates. Applied Nursing Research, 15(1): 31.
Gestational age for the sample ranged from 26 to 42 weeks, with a mean of 33.5 weeks (SD = 3.8). Chronological age ranged from 1 to 30 days, with a mean of 6.8 days (SD = 6.9). Mean birth weight was 2.11 kg (SD = 0.875), with a range from 0.52 to 3.89 kg. There were no statistically significant differences in sex determined by chi-square analysis. There were no statistically significant differences in birth weight, gestational age, or chronological age of subjects between the two groups [experimental and control] based on Student’s t-test [see Table 8-2]. (Schultz et al., 2002, p. 31)
The demographic variables in this study were gender, weight, gestational age, and chronological age. The experimental and control groups were compared on these demographic variables to ensure that they were similar before the treatment was implemented. Because the results indicated that the catheters flushed with heparinized saline, which was the standard practice of this agency, were patent significantly longer than the catheters flushed with normal saline, it can be assume that the decreased patency results in the experimental group were due to the effect of the treatment (normal saline flush) rather than demographic or extraneous variables.
Moderator and Mediator Variables
Moderator and mediator variables are examined in intervention effectiveness research to improve our understanding of the effect of the intervention on practice-related outcomes. A moderator variable occurs with the intervention (independent variable) and alters the causal relationship between the intervention and the outcomes. Moderator variables include characteristics of the subjects and of the person implementing the intervention. Mediator variables bring about the effects of the intervention after it has occurred and thus influence the outcomes of the study (Sidani & Braden, 1998).
The theoretical model that provides the framework for the study usually identifies the relevant moderator and mediator variables to be examined in the study. The design is developed to examine not only the independent (intervention) and dependent (outcomes) variables but also the moderator, mediator, and contextual variables (see Chapter 13 for a detailed discussion and examples of these types of variables).
OPERATIONALIZING VARIABLES OR CONCEPTS FOR A STUDY
Operationalizing a variable or concept involves developing conceptual and operational definitions. A conceptual definition provides the theoretical meaning of a concept or variable and is derived from a theorist’s definition of that concept or is developed through concept analysis. The study framework, which includes concepts and their definitions, provides a basis for conceptually defining the variables. Artinian et al. (2001) studied the effects of two independent variables (home telemonitoring and community-based monitoring) on one dependent variable (blood pressure). The framework for this study was the health belief model, and the proposition studied was that a cue to action is implemented to activate a readiness to change health behaviors (Strecher & Rosenstock, 1997).
 INDEPENDENT VARIABLE—HOME TELEMONITORING
INDEPENDENT VARIABLE—HOME TELEMONITORING
Home telemonitoring (HT) is a cue to action or a strategy to increase a person’s awareness of the need to change behavior. (Strecher & Rosenstock, 1997)
HT intervention included providing instructions on how to monitor BP in the home three times a week over 12 weeks. In addition, telephone counseling about lifestyle modification was provided once a week for 12 weeks by a specially trained registered nurse. (Artinian et al., 2001)
INDEPENDENT VARIABLE—COMMUNITY-BASED MONITORING
Community-based monitoring (CBM) is a cue to action or a strategy to increase a person’s awareness of the need to change behavior. (Strecher & Rosenstock, 1997)
CBM intervention required participants to “visit the community center three times a week in the morning to have their BP measured. Participants also received feedback about their BP and weekly education counseling about lifestyle modification and adherence to their medication regimen”. (Artinian et al., 2001, p. 193)
DEPENDENT VARIABLE—BLOOD PRESSURE
BP control requires a change in lifestyle and health behavior that is triggered by educational cues to action. (Strecher & Rosenstock, 1997)
Both systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured three times a week. For the HT group, the SBP and DBP “were measured with an electronic home BPLink monitor (model A & D UA 767PC)” and BP monitoring services provided by LifeLink Monitoring, Inc., located in Bearsville, New York. For the CBM, the SBP and DBP were “measured with the BP equipment at the community center” and recorded by a nurse trained by the researcher. (Artinian et al., 2001, p. 194)
Figure 8-2 presents the significant changes in the SBP and DBP for both treatment groups (HT and CBM). The HT and CBM treatment groups had significantly lower SBP and DBP than the usual care group. These monitoring interventions promoted blood pressure control among African Americans, who often have difficultly managing hypertension.
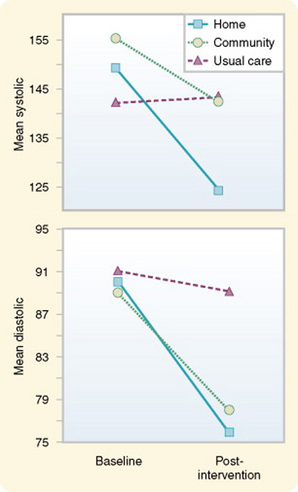
Figure 8-2 Change in SBP and DBP during 3 months for the home telemonitoring, community-based monitoring, and usual care groups. (Home telemonitoring, n = 6; community-based monitoring, n = 6; usual care only, n = 9.)
The variables in quasi-experimental and experimental research are narrow and specific in focus and are capable of being quantified (converted to numbers) or manipulated through the use of specified steps. In addition, the variables are objectively defined to reduce researcher bias. The concepts or variables in descriptive and correlational quantitative studies and qualitative studies are usually more abstract and broadly defined than the variables in quasi-experimental studies.
Some researchers believe that the concepts in qualitative studies do not require operational definitions because sensitizing or experiencing the real situation rather than operationalizing the concepts is most important. Operational definitions are thought to limit the investigation so that a phenomenon, such as pain, or a characteristic of a culture, such as health practices, is not completely experienced or understood. In other qualitative studies, the phenomena being examined are not named until the data analysis step (Marshall & Ross, 2006; Munhall, 2001). Thus, some concepts may not be identified or defined until late in the study. For example, Orne et al. (2000, p. 205) conducted their study “with the goal of constructing a vivid depiction of the lived experience of being employed but medically uninsured.” The conceptual definition for the experience of being medically uninsured was identified in the analysis section of the research report in a table format.
RESEARCH CONCEPT—EXPERIENCE OF BEING MEDICALLY UNINSURED
Table 8-3 illustrates this definition, including the theme clusters and themes for the experience of being medically uninsured.
TABLE 8-3
| Theme Clusters | Themes |
| A Marginalized Life | Vulnerable on all fronts |
| Limits, loss, and hard times | |
| Up against Rocks and Hard Places | The paradox of middle ground |
| Entangled in power and politics | |
| Making Choices— Chancing It | Setting priorities—weighing the odds |
| Living with compromise | |
| A game of Russian roulette | |
| Getting By—More or Less | Lucky so far |
| Resilience | |
| Resigned to adversity | |
| The emotional price tag |
From Orne, R. M., Fishman, S. J., Manka, M., & Pagnozzi, M. E. (2000). Living on the edge: A phenomenological study of medically uninsured working Americans. Research in Nursing & Health, 23(3): 207.
The research concept of the experience of being medically uninsured while working was investigated using audiotaped, face-to-face interviews that were conducted with an unstructured format.
Participants initially were asked to respond to the statement, “Please describe to me as thoroughly as you can, what it is like to be working and without medical insurance.” Additional questioning, for clarification, requests for specific examples, and reflective statements were used to encourage the participants to describe their experience in detail. (Orne et al., 2000, p. 206)
Thus, the focus of the study by Orne et al. (2000) was to conceptually define and describe the concept of the experience of being medically uninsured while being employed. The findings from this study could become the basis for additional research to expand our understanding and ability to manage the problems of the medically uninsured population.
SUMMARY
• Research objectives, questions, and hypotheses are formulated to bridge the gap between the more abstractly stated research problem and purpose and the detailed design and plan for data collection and analysis.
• Research objectives are clear, concise, declarative statements that are expressed in the present tense.
• A research question is a concise, interrogative statement that is worded in the present tense and consists of one or more variables (or concepts).
• A hypothesis is the formal statement of the expected relationships between two or more variables in a specified population.
• Hypotheses can be described in terms of four categories: (1) associative versus causal, (2) simple versus complex, (3) nondirectional versus directional, and (4) null versus research.
• Selecting objectives, questions, or hypotheses for a study is based on (1) the number and quality of relevant studies conducted on a selected problem (existing knowledge base), (2) the framework of the study, (3) the expertise and preference of the researcher, and (4) the type of study to be conducted (quantitative, qualitative, outcomes, and intervention).
• Variables are qualities, properties, or characteristics of persons, things, or situations that change or vary in a study.
• The types of variables discussed in this chapter are independent, dependent, research, extraneous, demographic, moderator, and mediator.
• An independent variable is a stimulus or intervention that the researcher manipulates or varies to create an effect on the dependent variable.
• A dependent variable is the response, behavior, or outcome that the researcher wants to predict or explain.
• Research variables or concepts are the qualities, properties, or characteristics that are observed or measured in a study.
• Demographic variables are attributes of the subjects that are measured in a study to describe the sample.
• The variables require conceptual and operational definitions, and a conceptual definition provides the theoretical meaning of a concept or variable and is derived from a theorist’s definition of the concept or is developed through concept analysis.
• An operational definition is derived from a set of procedures or progressive acts that a researcher performs either to manipulate an independent variable or to measure the existence or degree of existence of the dependent variable.
REFERENCES
Aamodt, A.M. Problems in doing nursing research: Developing criteria for evaluating qualitative research. Western Journal of Nursing Research. 1983;5(4):398–402.
Ajzen, I. From intention to action: A theory of planned behavior. In. In: Kuhl J., Beckmann J., eds. Action control: From cognition to behavior. New York: Springer; 1985:11–39.
Anderson, B., Higgins, L., Rozmus, C. Critical pathways: Application to selected patient outcomes following coronary artery bypass graft. Applied Nursing Research. 1999;12(4):168–174.
Armstrong, R.L. Hypothesis formulation. In. In: Krampitz S.D., Pavlovich N., eds. Readings for nursing research. St. Louis: Mosby; 1981:29–39.
Artinian, N.T., Washington, O.G., Templin, T.N. Effects of home telemonitoring and community-based monitoring on blood pressure control in urban African Americans: A pilot study. Heart & Lung. 2001;30(3):191–199.
Beveridge, W.B. The art of scientific investigation. New York: Vintage Books, 1950.
Brown, J.S., Tanner, C.A., Padrick, K.P. Nursing’s search for scientific knowledge. Nursing Research. 1984;33(1):26–32.
Center for Disease Control and Prevention Diabetes surveillance report. Department of Health and Human Services, 2005. Retrieved November 26, 2005, from http://www.cdc.gov/diabetes/statistics/prevalence_national.htm.
Cheng, C., Studdiford, J.S., Chambers, C.V., Diamond, J.J., Paynter, N. The reliability of patient self-reported blood pressures. Journal of Clinical Hypertension. 2002;4(4):259–264. [273].
Chinn, P.L., Kramer, M.K. Integrated theory and knowledge development in nursing, (7th ed.). St. Louis: Mosby, 2008.
Cox, K.S., Teasley, S.L., Lacey, S.R., Carroll, C.A., Sexton, K.A. Work environment perceptions of pediatric nurses. Journal of Pediatric Nursing. 2007;22(1):9–14.
Efe, E., Özer, Z.C. The use of breast-feeding for pain relief during neonatal immunization injections. Applied Nursing Research. 2007;20(1):10–16.
Ernst, M.E., Messmer, P.R., Franco, M., Gonzalez, J.L. Nurses’ job satisfaction, stress, and recognition in pediatric setting. Pediatric Nursing. 2004;30(3):219–227.
Fagerhaugh, S.Y., Strauss, A. Politics of pain management. Menlo Park, CA: Addison-Wesley, 1977.
Gerlach, R.W., Gambosi, J.R., Bowen, R.H. Cancer survivors’ needs reported by survivors and their families. Journal of Cancer Education. 1990;5(1):63–70.
Happ, M.B., Swigart, V.A., Tate, J.A., Hoffman, L.A., Arnold, R.M. Patient involvement in health-related decisions during prolonged critical illness. Research in Nursing & Health. 2007;30(4):361–372.
Jennings-Dozier, K. Predicting intentions to obtain a Pap smear among African American and Latina women: Testing the theory of planned behavior. Nursing Research. 1999;48(4):198–205.
Kaplan, A. The conduct of inquiry: Methodology for behavioral science. New York: Harper & Row, 1964.
Kerlinger, F.N., Lee, H.B. Foundations of behavioral research, (4th ed.). Fort Worth, TX: Harcourt College Publishers, 2000.
Marshall, C., Rossman, G.B. Designing qualitative research, (4th ed.). Thousand Oaks: CA: Sage, 2006.
McDonald, D.D., Frakes, M., Apostolidis, B., Armstrong, B., Goldblatt, S., Bernardo, D. Effect of a psychiatric diagnosis on nursing care for nonpsychiatric problems. Research in Nursing & Health. 2003;26(3):225–232.
Moody, L.E., Advancing nursing science through research, Vol. 1. Newbury Park, CA: Sage, 1990.
Moody, L.E., Wilson, M.E., Smyth, K., Schwartz, R., Tittle, M., Van Cott, M.L. Analysis of a decade of nursing practice research: 1977–1986. Nursing Research. 1988;37(6):374–379.
Munhall, P.L. Nursing research: A qualitative perspective, (3rd ed.). Sudbury, MA: Jones & Bartlett and National League for Nursing, 2001.
Narsavage, G., Romeo, E. Education and support needs of younger and older cancer survivors. Applied Nursing Research. 2003;16(2):103–109.
Orem, D.E. Nursing concepts of practice. St. Louis: Mosby, 2001.
Orne, R.M., Fishman, S.J., Manka, M., Pagnozzi, M.E. Living on the edge: A phenomenological study of medically uninsured working Americans. Research in Nursing & Health. 2000;23(3):204–212.
Pennsylvania Department of Health, Number of observed and expected cancer cases by sex and primary site, 1994–1998. Lackawanna County Health Profile 1998. Retrieved May 29, 2002, from http://www.health.state.pa.us/pdf/hpa/ststs/profile98/lacka.pdf. http://webserver.health.state.pa.us/health/lib/health/Pennsylvania_cancer.pdf.
Polzer, R.L. African Americans and diabetes: Spiritual role of the health care provider in self-management. Research in Nursing & Health. 2007;30(2):164–174.
Polzer, R.L., Miles, M.S. Spirituality in African Americans with diabetes: Self-management through a relationship with God. Qualitative Health Research. 2007;17(2):176–188.
Rawl, S.M., Given, B.A., Given, C.W., Champion, V.L., Kozachik, S.L., Barton, D., et al. Intervention to improve psychological functioning for newly diagnosed patients with cancer. Oncology Nursing Forum. 2002;29(6):967–975.
Reishtein, J.L. Relationship between symptoms and functional performance in COPD. Research in Nursing & Health. 2005;28(1):39–47.
Reynolds, P.D. A primer in theory construction. Indianapolis: Bobbs-Merrill, 1971.
Schultz, A.A., Drew, D., Hewitt, H. Comparison of normal saline and heparinized saline for patency of IV locks in neonates. Applied Nursing Research. 2002;15(1):28–34.
Sidani, S., Braden, C.J. Evaluating nursing interventions: A theory-driven approach. Thousand Oaks, CA: Sage, 1998.
Strecher, V.J., Rosenstock, I.M. The health belief model. In. In: Glanz K., Lewis F.M., Rimer B.K., eds. Health behavior and health education: Theory, research and practice. 2nd ed. San Francisco: Jossey-Bass; 1997:41–59.
Vasan, R.S., Beiser, A., D’Agostino, R.B., Levy, D., Selhub, J., Jacques, P.F., et al. Plasma homocysteine and risk for congestive heart failure in adults without prior myocardial infarction. Journal of the American Medical Association. 2003;289(10):1251–1257.