The cardiovascular history
The following chapters deal with the history and the examination of the heart and blood vessels, as well as other parts of the body where symptoms and signs of heart disease may appear. Not only is this fundamental to the assessment of any patient, but the cardiovascular system is also one of the most commonly tested systems in OSCEs and viva voce examinations. It is believed by cardiologists to be the most important system in the body.
Presenting symptoms
CHEST PAIN
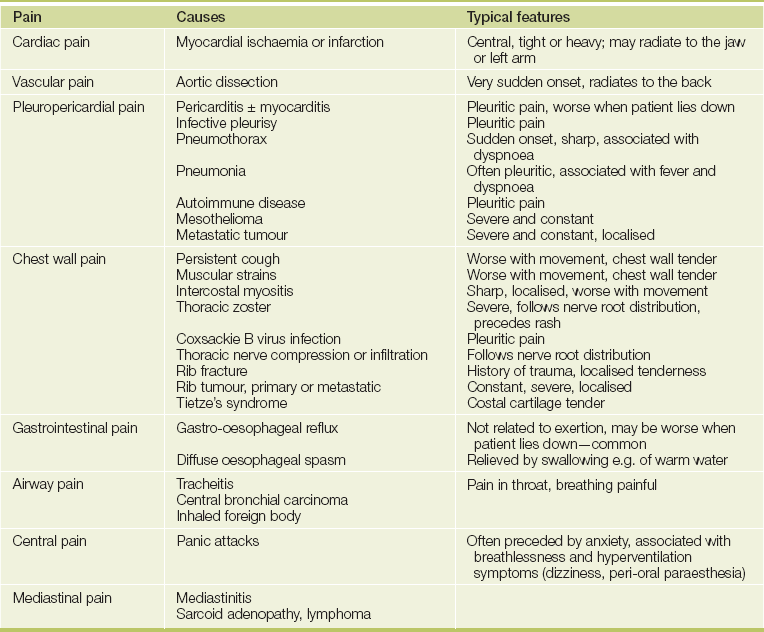
The mention of chest pain by a patient (see Table 4.1) tends to provoke more urgent attention than other symptoms. The surprised patient may find him- or herself whisked into an emergency ward with the rapid appearance of worried-looking doctors. This is because ischaemic heart disease, which may be a life-threatening condition, often presents in this manner (see List 4.1).
The pain of angina and myocardial infarction tends to be similar in character; both are due to the accumulation of metabolites from ischaemic muscle following complete or partial obstruction of a coronary artery which leads to stimulation of the cardiac sympathetic nerves.1,2 Patients with cardiac transplants who develop coronary disease in the transplanted heart may not feel angina, presumably because the heart is denervated. Similarly, patients with diabetes are more likely to be diagnosed with ‘silent infarcts’.
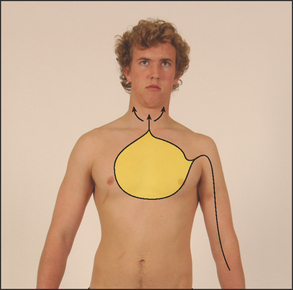
To help determine the cause of chest pain (see Tables 4.2A and B), it is important to ascertain the duration, location, quality and precipitating and aggravating factors (the four cardinal features), as well as means of relief and accompanying symptoms (the SOCRATES questions; see Chapter 1).3 The term anginaa was coined by Heberden from the Greek and Latin words meaning ‘choking’ or strangling; and the patient may complain of crushing pain, heaviness, discomfort or a choking sensation in the retrosternal area or in the throat. It is best to ask if the patient experiences chest ‘discomfort’ rather than ‘pain’, because angina is often dull and aching in character and may not be perceived as pain (see Figure 4.1).
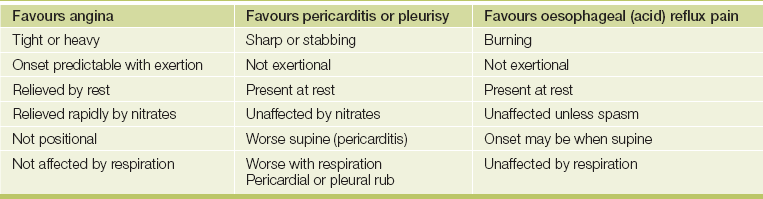
TABLE 4.2B
Differential diagnosis of chest pain
| Favours myocardial infarction (acute coronary syndrome) | Favours angina |
| Onset at rest | Onset with exertion |
| Severe pain | Moderate pain or discomfort |
| Sweating | No sweating |
| Anxiety (angor) | Mild or no anxiety |
| No relief with nitrates | Rapid relief with nitrates |
| Associated symptoms (nausea and vomiting) | Associated symptoms absent |
| Favours myocardial infarction | Favours aortic dissection* |
| Central chest pain | Radiates to back |
| Subacute onset (minutes) | Instantaneous onset |
| Severe pain | Very severe pain, tearing quality |
| Favours myocardial ischaemia | Favours chest wall pain |
| Exertional | Positional |
| Occurs with exertion | Often worse at rest |
| Brief episodes | Prolonged |
| Diffuse | Localised |
| No chest wall tenderness (only discriminates between infarction and chest wall pain) | Chest wall tenderness |
*LR of dissection of 66 if all three characteristics or two plus history of hypertension.
(Adapted from Simel DL, Rennie D. The rational clinical examination: evidence-based diagnosis. New York: McGraw-Hill, 2009.)
Questions box 4.1
Questions to ask the patient with suspected angina
 denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. Can you tell me what the pain or discomfort is like? Is it sharp or dull, heavy or tight?
2. When do you get the pain? Does it come out of the blue, or does it come on when you do physical things? Is it worse if you exercise after eating?
5. Does it make you stop or slow down?
6. Does it go away quickly when you stop exercising?
7. Is it coming on with less effort or at rest? (Unstable symptoms)
The pain or discomfort is usually central rather than left-sided. The patient may dismiss the pain as non-cardiac because it is not felt over the heart on the left side. It may radiate to the jaw or to the arms, but very rarely travels below the umbilicus. The severity of the pain or discomfort is variable.
Angina characteristically occurs with exertion, with rapid relief once the patient rests or slows down. The amount of exertion necessary to produce the pain may be predictable to the patient. A change in the pattern of onset of previously stable angina must be taken very seriously.
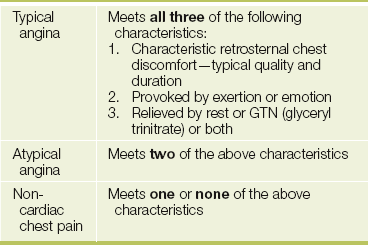
These features constitute typical angina (see Table 4.3).3,4 Although angina typically occurs on exertion, it may also occur at rest or wake a patient from sleep. Ischaemic chest pain is usually unaffected by respiration. The use of sublingual nitrates characteristically brings relief within a couple of minutes, but this is not specific as nitrates may also relieve oesophageal spasm and have a pronounced placebo effect.
The pain associated with an acute coronary syndrome (myocardial infarction or unstable angina) often comes on at rest, is usually more severe and lasts much longer. Acute coronary syndromes are usually caused by the rupture of a coronary artery plaque, which leads to the formation of thrombus in the arterial lumen. Stable exertional angina is a result of a fixed coronary narrowing. Pain present for more than half an hour is more likely to be due to an acute coronary syndrome than to stable angina, but pain present continuously for many days is unlikely to be either. Associated symptoms of myocardial infarction include dyspnoea, sweating, anxiety, nausea and faintness.
Other causes of retrosternal pain are listed in Tables 4.1 and 4.2A. Chest pain made worse by inspiration is called pleuritic pain. This may be due to pleurisy or pericarditis (page 249). Pleurisy may occur because of inflammation of the pleura as a primary problem (usually due to viral infection), or secondary to pneumonia or pulmonary embolism. Pleuritic pain is not usually brought on by exertion and is often relieved by sitting up and leaning forwards. It is caused by the movement of inflamed pleural or pericardial surfaces on one another.
Chest wall pain is usually localised to a small area of the chest wall, is sharp and is associated with respiration or movement of the shoulders rather than with exertion. It may last only a few seconds or be present for prolonged periods. Disease of the cervical or upper thoracic spine may also cause pain associated with movement. This pain tends to radiate around from the back towards the front of the chest.
Pain due to a dissecting aneurysm of the aorta is usually very severe and may be described as tearing. This pain is often greatest at the moment of onset and radiates to the back. These three features—quality, rapid onset and radiation—are very specific for aortic dissection. A proximal dissection causes anterior chest pain and involvement of the descending aorta causes interscapular pain. A history of hypertension or of a connective tissue disorder such as Marfan’s syndrome or Ehlers-Danlos syndrome puts the patient at increased risk of this condition.
Massive pulmonary embolism causes pain of very sudden onset which may be retrosternal and associated with collapse, dyspnoea and cyanosis (page 159). It is often pleuritic, but can be identical to anginal pain, especially if associated with right ventricular ischaemia.
Spontaneous pneumothorax may result in pain and severe dyspnoea (page 155). The pain is sharp and localised to one part of the chest.
Gastro-oesophageal reflux commonly causes angina-like pain without heartburn. It is important to remember that these two relatively common conditions may coexist. Oesophageal spasm may cause retrosternal chest pain or discomfort and can be quite difficult to distinguish from angina but is uncommon; the pain may radiate to the jaw and is often relieved by swallowing warm water or by the use of nitrates.
Cholecystitis can cause chest pain and be confused with myocardial infarction. Right upper quadrant abdominal tenderness is usually present (page 200).
The cause of severe, usually unilateral, chest pain may not be apparent until the typical vesicular rash of herpes zoster appears in a thoracic nerve root distribution.
DYSPNOEA
Shortness of breath may be due to cardiac disease. Dyspnoea (from the Greek dys ‘bad’, pnoia ‘breathing’) is often defined as an unexpected awareness of breathing. It occurs whenever the work of breathing is excessive, but the mechanism is uncertain. It is probably due to a sensation of increased force required of the respiratory muscles to produce a volume change in the lungs, because of a reduction in compliance of the lungs or increased resistance to air flow.
Cardiac dyspnoea is typically chronic and occurs with exertion because of failure of the left ventricular output to rise with exercise; this in turn leads to an acute rise in left ventricular end-diastolic pressure, raised pulmonary venous pressure, interstitial fluid leakage and thus reduced lung compliance. However, the dyspnoea of chronic cardiac failure does not correlate well with measurements of pulmonary artery pressures, and clearly the origin of the symptom of cardiac dyspnoea is complicated.5 Left ventricular function may be impaired because of ischaemia (temporary or permanent reduction in myocardial blood supply), previous infarction (damage) or hypertrophy (often related to hypertension). As it becomes more severe, cardiac dyspnoea occurs at rest.
Orthopnoea (from the Greek ortho ‘straight’; see List 4.2), or dyspnoea that develops when a patient is supine, occurs because in an upright position the patient’s interstitial oedema is redistributed; the lower zones of the lungs become worse and the upper zones better. This allows improved overall blood oxygenation. Patients with severe orthopnoea spend the night sitting up in a chair or propped up on numerous pillows in bed. The absence of orthopnoea suggests that left ventricular failure is unlikely to be the cause of a patient’s dyspnoea (negative likelihood ratio [LR] = 0.046).
Paroxysmalb nocturnal dyspnoea (PND) is severe dyspnoea that wakes the patient from sleep so that he or she is forced to get up gasping for breath. This occurs because of a sudden failure of left ventricular output with an acute rise in pulmonary venous and capillary pressures; this leads to transudation of fluid into the interstitial tissues, which increases the work of breathing. The sequence may be precipitated by resorption of peripheral oedema at night while supine. Acute cardiac dyspnoea may also occur with acute pulmonary oedema or a pulmonary embolus.
Cardiac dyspnoea can be difficult to distinguish from that due to lung disease or other causes (page 131).7 One should enquire particularly about a history of any cardiac disease that could be responsible for the onset of cardiac failure. For example, a patient with a number of known previous myocardial infarctions who develops dyspnoea is more likely to have decreased left ventricular contractility. A patient with a history of hypertension or a very heavy alcohol intake may have hypertensive heart disease or an alcoholic cardiomyopathy. The presence of orthopnoea or paroxysmal nocturnal dyspnoea is more suggestive of cardiac failure than of lung disease.
Dyspnoea is also a common symptom of anxiety. These patients often describe an inability to take a big enough breath to fill the lungs in a satisfying way. Their breathing may be deep and punctuated with sighs.
ANKLE SWELLING
The presence of oedema alone is poorly correlated with heart failure (there are many more common causes), but some heart failure patients present with bilateral ankle swelling due to oedema. Unlike the swelling that occurs with inflammatory conditions, the area is not painful or red. Patients with the recent onset of oedema and who take a serious interest in their weight may have noticed a weight gain of 3 kg or more.
Ankle oedema of cardiac origin is usually symmetrical and worse in the evenings, with improvement during the night. It may be a symptom of biventricular failure or right ventricular failure secondary to a number of possible underlying aetiologies. As failure progresses, oedema ascends to involve the legs, thighs, genitalia and abdomen. There are usually other symptoms or signs of heart disease.
It is important to find out whether the patient is taking a vasodilating drug (e.g. a calcium channel blocker), which can cause peripheral oedema. There are other (more) common causes of ankle oedema than heart failure that also need to be considered; see List 6.2 on page 88). Oedema that affects the face is more likely to be related to kidney disease, from the nephrotic syndrome (page 260).
PALPITATIONS
This is not a very precise term (see Table 4.4). It is usually taken to mean an unexpected awareness of the heartbeat.8 Ask the patient to describe exactly what he or she notices and whether the palpitations are slow or fast, regular or irregular, and how long they last (see Questions box 4.2).
Questions box 4.2
Questions to ask the patient with palpitations
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. Is the sensation one of the heart beating abnormally, or something else?
2. Does the heart seem fast or slow? Have you counted how fast? Is it faster than it ever goes at any other time, e.g. with exercise?
3. Does the heart seem regular or irregular: stopping and starting? If it is irregular, is this the feeling of normal heart beats interrupted by missed or strong beats—ectopic beats; or is it completely irregular? (Atrial fibrillation)
4. How long do the episodes last?
5. Do the episodes start and stop very suddenly? (Supraventricular tachycardia (SVT))
6. Can you terminate the episodes by deep breathing or holding your breath? (SVT)
7. Is there a sensation of pounding in the neck? (Some types of SVT9)
8. Has an episode ever been recorded on an ECG?
9. Have you lost consciousness during an episode? (Ventricular arrhythmias)
10. Have you had other heart problems such as heart failure or a heart attack in the past? (Ventricular arrhythmias?)
11. Is there heart trouble of this sort or of people dying suddenly in the family? (Sudden death syndromes e.g. Brugada syndrome or a long QT interval syndrome)
TABLE 4.4
Palpitations: differential diagnosis
| Feature | Suggests |
| Heart misses and thumps | Ectopic beats |
| Worse at rest | Ectopic beats |
| Very fast, regular | SVT(VT) |
| Instantaneous onset | SVT(VT) |
| Offset with vagal manoeuvres | SVT |
| Fast and irregular | AF |
| Forceful and regular—not fast | Awareness of sinus rhythm (anxiety) |
| Severe dizziness or syncope | VT |
| Pre-existing heart failure | VT |
SVT = supraventricular tachycardia; VT = ventricular tachycardia; AF = atrial fibrillation.
There may be the sensation of a missed beat followed by a particularly heavy beat; this can be due to an atrial or ventricular ectopic beat (which produces little cardiac output) followed by a compensating pause and then a normally conducted beat (which is more forceful than usual because there has been a longer diastolic filling period for the ventricle).
If the patient complains of a rapid heartbeat, it is important to find out whether the palpitations are of sudden or gradual onset and offset. Cardiac arrhythmias are usually instantaneous in onset and offset, whereas the onset and offset of sinus tachycardia is more gradual. A completely irregular rhythm is suggestive of atrial fibrillation, particularly if it is rapid.
It may be helpful to ask the patient to tap the rate and rhythm of the palpitations with his or her finger. Associated features including pain, dyspnoea or faintness must be inquired about. The awareness of rapid palpitations followed by syncope suggests ventricular tachycardia. These patients usually have a past history of significant heart disease. Any rapid rhythm may precipitate angina in a patient with ischaemic heart disease.
Patients may have learned manoeuvres that will return the rhythm to normal. Attacks of supraventricular tachycardia (SVT) may be suddenly terminated by increasing vagal tone with the Valsalva manoeuvre (page 82), by carotid massage, coughing or swallowing cold water or ice cubes.c
SYNCOPE, PRESYNCOPE AND DIZZINESS
Syncope is a transient loss of consciousness resulting from cerebral anoxia, usually due to inadequate blood flow (see List 4.3). Presyncope is a transient sensation of weakness without loss of consciousness. (See Questions box 31.4 on page 396.)
Syncope may represent a simple faint or be a symptom of cardiac or neurological disease. One must establish whether the patient actually loses consciousness and under what circumstances the syncope occurs—for example, on standing for prolonged periods or standing up suddenly (postural syncope), while passing urine (micturition syncope), on coughing (tussive syncope) or with sudden emotional stress (vasovagal syncope). Find out whether there is any warning, such as dizziness or palpitations, and how long the episodes last. Recovery may be spontaneous or the patient may require attention from bystanders.
If the patient’s symptoms appear to be postural, enquire about the use of antihypertensive or anti-anginal drugs and other medications that may induce postural hypotension. If the episode is vasovagal, it may be precipitated by something unpleasant like the sight of blood or occur in a crowded, hot room; patients often sigh and yawn and feel nauseated and sweaty before fainting and may have previously had similar episodes, especially during adolescence and young adulthood.
If syncope is due to an arrhythmia, there is a sudden loss of consciousness regardless of the patient’s posture; chest pain may also occur if the patient has ischaemic heart disease or aortic stenosis.10 Recovery is equally quick. Exertional syncope may occur with obstruction to left ventricular outflow by aortic stenosis or hypertrophic cardiomyopathy. Profound and sudden slowing of the pulse (bradycardia), usually a result of complete heart block, causes sudden and recurrent syncope (Stokes-Adamsd attackse). These patients may have a history of atrial fibrillation. Typically they have periods of tachycardia (fast heart rate) as well as periods of bradycardia (slow heart rate). This condition is called the sick sinus syndrome. The patient must be asked about drug treatment that could cause bradycardia (e.g. beta-blockers, digoxin, calcium channel blockers).
It is important to ask about a family history of sudden death. An increasing number of ion channelopathies are being identified as a cause of syncope and sudden death. These rare inherited conditions include the long and short QT syndromes and the Brugada syndrome.f,11 They are often diagnosed from typical ECG changes. In addition, certain drugs can cause the acquired long QT syndrome (see List 4.4 overleaf).
Neurological causes of syncope are associated with a slow recovery and often residual neurological symptoms or signs. Bystanders may also have noticed abnormal movements if the patient has epilepsy, although cerebral hypoxia caused by a cardiac arrhythmia can also cause tonic and clonic movements. Dizziness that occurs even when the patient is lying down or that is made worse by movements of the head is more likely to be of neurological origin, although recurrent tachyarrhythmias may occasionally cause dizziness in any position. One should attempt to decide whether the dizziness is really vertiginous (where the world seems to be turning around) or is a presyncopal (impending loss of consciousness) feeling.
FATIGUE
Fatigue is a common symptom of cardiac failure. It may be associated with a reduced cardiac output and poor blood supply to the skeletal muscles. There are many other causes of fatigue, including lack of sleep, anaemia and depression.
INTERMITTENT CLAUDICATION AND PERIPHERAL VASCULAR DISEASE
The word claudicationg comes from the Latin meaning to limp. Patients with claudication notice pain in one or both calves, thighs or buttocks when they walk more than a certain distance. This distance is called the claudication distance. The claudication distance may be shorter when patients walk up hills. A history of claudication suggests peripheral vascular disease with a poor blood supply to the affected muscles. The most important risk factors are smoking, diabetes, hypertension and a history of vascular disease elsewhere in the body, including cerebrovascular disease and ischaemic heart disease (see Questions box 4.). More severe disease causes the feet or legs to feel cold, numb and finally painful at rest. Rest pain is a symptom of severely compromised arterial supply. Remember the six Ps of peripheral vascular disease:
Questions box 4.3
Questions to ask the patient with suspected peripheral vascular disease
denotes symptoms for the possible diagnosis of an urgent or dangerous problem.
1. Have you had problems with walking because of pains in the legs?
2. Where do you feel the pain?
3. How far can you walk before it occurs?
5. Does it go away when you stop walking?
6. Does the pain ever occur at rest? (Severe ischaemia may threaten the limb)
7. Have there been changes in the colour of the skin over your feet or ankles?
8. Have you had any sores or ulcers on your feet or legs that have not healed?
9. Have you needed treatment of the arteries of your legs in the past?
10. Have you had diabetes, high blood pressure or problems with stroke or heart attacks in the past?
Popliteal artery entrapment can occur, especially in young men with intermittent claudication on walking but not running. Also, lumbar spinal stenosis causes pseudo-claudication: unlike vascular claudication, the pain in the calves is not relieved by standing still, but is relieved by sitting (flexing the spine) and may be exacerbated by extending the spine (e.g. walking downhill).
Risk factors for coronary artery disease
An essential part of the cardiac history involves obtaining detailed information about a patient’s risk factors—the patient’s cardiovascular risk factor profile (see Questions box 4.4).
Previous ischaemic heart disease is the most important risk factor for further ischaemia. The patient may know of previous infarcts or have had a diagnosis of angina in the past.
Hypercholesterolaemia is the next most important risk factor for ischaemic heart disease. Many patients now know their serum cholesterol levels because widespread testing has become fashionable. The total serum cholesterol is a useful screening test, and levels above 5.2 mmol/L are considered undesirable. Cholesterol measurements (unlike triglyceride measurements) are accurate even when a patient has not been fasting. Patients with established coronary artery disease benefit from lowering of total cholesterol to below 4 mmol/L. An elevated total cholesterol level is even more significant if the high-density lipoprotein (HDL) level is low (less than 1.0 mmol/L). Significant elevation of the triglyceride level is a coronary risk factor in its own right and also adds further to the risk if the total cholesterol is high. If a patient already has coronary disease, hyperlipidaemia is even more important. Control of risk factors for these patients is called secondary prevention. Patients who have multiple risk factors for ischaemic heart disease (e.g. diabetes and hypertension) should have their cholesterol controlled aggressively. If the patient’s cholesterol is known to be high, it is worth obtaining a dietary history. This can be very trying. It is important to remember that not only foods containing cholesterol but also those containing saturated fats contribute to the serum cholesterol level. High alcohol consumption and obesity are associated with hypertriglyceridaemia.
Smoking is probably the next most important risk factor for cardiovascular disease and peripheral vascular disease. Some patients describe themselves as non-smokers even though they stopped smoking only a few hours ago. The number of years the patient has smoked and the number of cigarettes smoked per day are both very important (and are recorded as packet-years; page 11). The significance of a history of smoking for a patient who has not smoked for many years is controversial. The risk of symptomatic ischaemic heart disease falls gradually over the years after smoking has been stopped. After about 2 years the risk of myocardial infarction falls to the same level as for those who have never smoked. After 10 years the risk of developing angina falls close to that of non-smokers.
Hypertension is another important risk factor for coronary artery disease. Find out when hypertension was first diagnosed and what treatment, if any, has been instituted (see Questions box 4.4). Treatment of hypertension reduces the risk of ischaemic heart disease, hypertensive heart disease, cardiac failure and cerebrovascular disease (stroke). Treatment of hypertension has also been shown to reverse left ventricular hypertrophy.
A family history of coronary artery disease increases a patient’s risk, particularly if it has been present in first-degree relatives (parents or siblings) and if it has affected these people before the age of 60. Not all heart disease, however, is ischaemic; a patient whose relatives suffered from rheumatic heart disease is at no greater risk of ischaemic heart disease than anybody else.
A history of diabetes mellitus increases the risk of ischaemic heart disease very substantially. A diabetic without a history of ischaemic heart disease has the same risk of myocardial infarction as a non-diabetic who has had an infarct. It is important to find out how long a patient has been diabetic and whether insulin treatment has been required. Good control of the blood sugar level of diabetics reduces this risk. An attempt should therefore be made to find out how well a patient’s diabetes has been controlled.
Chronic kidney disease is associated with a very high risk of vascular disease. This is possibly related to high calcium-×-phosphate product. The risk may be reduced by dietary intervention, ‘phosphate binders’, efficient dialysis or renal transplant. Ischaemic heart disease is the most common cause of death in patients with kidney disease on dialysis.
Chronic inflammatory diseases such as rheumatoid arthritis significantly increase the risk of vascular disease too.
Erectile dysfunction is a sensitive indicator of arterial endothelial abnormality and is a risk factor or indicator of vascular disease.
The presence of multiple risk factors makes control of each one more important. Aggressive control of risk factors is often indicated in these patients.
It is interesting to note that in the diagnosis of angina the patient’s description of typical symptoms is more discriminating than is the presence of risk factors, which only marginally increase the likelihood that chest pain is ischaemic.4 Previous ischaemic heart disease is an exception. Certainly a patient who has had angina before and says he or she has it again is usually right.
A history of dental decay or infection is important for patients with valvular heart disease, since it puts them at risk of infective endocarditis. Dental caries may also be associated with an increased risk of ischaemic heart disease. Ask about the regularity of visits to the dentist and the patient’s awareness of the need for antibiotic prophylaxish before dental (and some surgical) procedures. Cardiac surgeons will not replace heart valves for people with infected teeth or gums for fear of infection on the artificial valve.
Drug and treatment history
The medications a patient is taking often give a good clue to the diagnosis. Find out about any ill-effects from current or previous medications. The surgical history must also be elicited. The patient may have had a previous angioplasty or coronary artery bypass grafting, and may know how many arteries were dilated or bypassed. If the patient is unable to provide a history, a midline sternotomy scar and leg scars (consistent with previous saphenous vein harvesting) support this diagnosis.
Patients with heart failure may have been advised to restrict their total daily fluid intake. Ask what volume has been recommended (often 1500 mL). They may also have been advised to weigh themselves daily and to increase their diuretic drug dose if their weight has increased. Ask what advice has been given about this.
Street drug use is relevant. The use of cocaine or amphetamines is an important cause of myocardial infarction in young people.
Past history
Patients with a history of definite previous angina or myocardial infarction remain at high risk of further ischaemic events. It is very useful at this stage to find out how a diagnosis of ischaemic heart disease was made and in particular what investigations were undertaken. The patient may well remember exercise testing or a coronary angiogram, and some patients can even remember how many coronary arteries were narrowed, how many coronary bypasses were performed (having more than three grafts often leads to a certain amount of boasting). The angioplasty patient may know how many arteries were dilated and whether stents (often called coronary stunts by patients and cardiac surgeons) were inserted. Acute coronary syndromes are now usually treated with early coronary angioplasty.
Patients may recall a diagnosis of rheumatic fever in their childhood, but many were labelled as having ‘growing pains’.12 A patient who was put to bed for a long period as a child may well have had rheumatic fever. A history of chorea (quick abnormal involuntary movements; page 478) is strongly associated with rheumatic fever in girls. A history of rheumatic fever places patients at risk of rheumatic valvular disease.
Hypertension may be caused or exacerbated by aspects of the patient’s activities and diet (see Questions box 4.5). A high salt intake, moderate or greater alcohol use, lack of exercise, obesity and kidney disease may all be factors contributing to high blood pressure. Non-steroidal anti-inflammatory drugs (NSAIDs) cause salt and fluid retention and may also worsen blood pressure. Ask about these, about previous advice to modify these factors and about any drug treatment of hypertension when interviewing any patient with high blood pressure.
Social history
Both ischaemic heart disease and rheumatic heart disease are chronic conditions that may affect a patient’s ability to function normally. It is therefore important to find out whether the patient’s condition has prevented him or her from working and over what period. Patients with severe cardiac failure, for example, may need to make adjustments to their living arrangements so that they are not required to walk up and down stairs at home.
Most hospitals run cardiac rehabilitation programs for patients with ischaemic heart disease or chronic heart failure. They provide exercise classes that help patients to regain their confidence and physical fitness, along with information classes about diet and drug treatment, and can help with psychological problems. Find out if the patient has been enrolled in one of these and whether it has been helpful. Is this service used as a point of contact for the patient if he or she has concerns about new symptoms or the management of medications?
The return of confidence and self-esteem are very important issues for patients and for their families after a life-threatening illness.
Family history
Certain heart diseases are genetic. Onset of heart disease at a young age (e.g. as a result of familial hypercholesterolaemia) or sudden death in the family (e.g. hypertrophic cardiomyopathy, Brugada syndrome) should raise the spectre of genetic disease.
References
1. Albert, JS. The patient with angina: the importance of careful listening. J Am Col Cardiol. 1988; 11:27. [The history further distinguishes cardiac events even if a coronary angiogram is available.].
2. Panju, AA, Hemmegan, BR, Guyatt, GH, Simel, DL. Is this patient having a myocardial infarction. JAMA. 1995; 273:1211–1218. [A focused history and examination (and an ECG) can aid subdivision of patients into those highly likely and those highly unlikely to be having a myocardial infarction.].
3. Evan, AT. Sensitivity and specificity of the history and physical examination for coronary artery disease. Ann Intern Med. 1994; 120:344–345.
4. Chun, AA, McGee, SR. Bedside diagnosis of coronary artery disease: a systematic review. Am J Med. 2004; 117:334–343.
5. Poole-Wilson, P. The origin of symptoms in patients with chronic heart failure. Eur Heart J. 1998; 9(supplement H):49–53. [This article discusses the lack of correlation between symptoms of heart failure and haemodynamic measurements.].
6. McGee, S. Evidence-based physical diagnosis, 3rd edn. St Louis: Saunders, 2012.
7. Wang, CS, FitzGerald, JS, Schulzer, M, et al. Does this dyspneic patient in the emergency department have congestive heart failure. JAMA. 2005; 294(15):1944–1956.
8. Brugada, P, Gursoy, S, Brugada, J, Ardries, E. Investigation of palpitations. Lancet. 1993; 341:1254–1258. [Emphasises the role of history taking and examination as well as the ECG in sorting out the patient presenting with palpitations.].
9. Gursoy, S, Steurer, G, Brugada, J, et al. The hemodynamic mechanism of pounding in the neck in atrioventricular nodal reentrant tachycardia. N Engl J Med. 1992; 327:772–774.
10. Calkins, H, Shyr, Y, Frumin, H, Schork, A, Morady, F. The value of the clinical history in the differentiation of syncope due to ventricular tachycardia, atrioventricular block, and neurocardiogenic syncope. Am J Med. 1995; 98:365–373. [Describes useful historical features in differential diagnosis.].
11. Brugada, J, Brugada, P, Brugada, R. The syndrome of right bundle branch block ST segment elevation in V1 to V3 and sudden death: the Brugada syndrome. Europace. 1999; 1(3):156–166.
12. Special Writing Group of the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease of the Council on Cardiovascular Disease in the Young of the American Heart Association. Guidelines for the diagnosis of rheumatic fever. Jones Criteria, 1992 Update. JAMA. 1992; 268:2069–2073.
aWilliam Heberden’s (1710–1801) description of angina (1768) is difficult to improve upon: ‘They who are afflicted with it, are seized while they are walking (more especially if it be up hill and soon after eating) with a painful and most disagreeable sensation in the breast, which seems as if it would extinguish life, if it were to increase or continue; but the moment they stand still, all this uneasiness vanishes.’ Heberden did not realise that angina was a result of coronary artery narrowing.
bParoxysmal symptoms or signs occur suddenly and intermittently.
cTesticular traction is a potent vagal manoeuvre but not in common use. Carotid massage (whereby the carotid artery is compressed below the angle of the jaw for several seconds) can be dangerous for people with carotid disease because of the risk of precipitating a stroke.
dWilliam Stokes (1804–1878) succeeded his father as Regius professor of physic in 1840. He was a member of the ‘Dublin School’ of medicine along with famous physicians like Graves, Cheyne, Adams and Corrigan. He was an art lover, and insisted his students have an arts degree before studying medicine.
Robert Adams (1791–1875) was Regius professor of surgery in Dublin, and became Queen Victoria’s surgeon. He was affected by gout, and wrote a famous paper on it.
eStokes-Adams attacks were probably described first by Gerbezius in 1691 and then by Morgagni in 1761; the latter was a pupil of Valsalva and also described Turner’s syndrome 170 years before Turner.
fJoseph, Philip and Raoul Brugada are three brothers who are contemporary Spanish electrophysiologists.
gThe Roman Emperor Tiberius Claudius Drusus Nero Germanicus (10 BC–54 AD) limped owing to some form of paralysis. ‘Claudication’ and ‘Claudius’, however, are etymologically unrelated, which seems rather a cruel coincidence for Claudius. ‘Claudicant’ first appeared in English in 1624.
hThis means the use of 1 or 2 doses of antibiotics given before and after a procedure which may lead to bacteraemia (circulation of microorganisms in the blood) and potential infection of a heart valve (endocarditis). Having a level of antibiotics present in the blood at the time of such procedures is thought (but not proven) to prevent endocarditis.