Chapter 49 Drugs in Sport
Competitors in sporting events often use drugs or other methods in attempts to enhance their performance; this is usually seen as unfair and potentially dangerous. Equally, competitors with medical conditions may require drugs to treat their condition and allow them to compete to their best ability. In this chapter, the use and abuse of drugs in sport is reviewed, and philosophical and ethical issues are considered. The pharmacology of the main groups of drugs prohibited or restricted by the World Anti-Doping Agency is reviewed: anabolic agents, β2 agonists, diuretics and masking agents, narcotic analgesics, hormones, antagonists and analogues, cannabinoids, alcohol, beta-blockers and stimulants. Banned blood doping and sample manipulation methods are described, and the clinical use and abuse in sport of erythropoietin (EPO) discussed.
The procedures for testing for drugs in athletes’ urine or blood samples are described briefly, and the use of ergogenic aids, dietary manipulation and complementary and alternative therapies as possible performance-enhancing methods is discussed. Medical use of some drugs is permitted provided the athlete has an approved Therapeutic Use Exemption. Ethical aspects related to drug use and abuse in sports are listed briefly for consideration.
(Note: For full details of drugs prohibited or restricted, and legal levels in bodily fluids, consult the latest WADA listing, available at: www.wada-ama.org/en/.)
Key abbreviations
AAS anabolic androgenic steroid
ASADA Australian Sports Anti-Doping Authority
ASDA Australian Sports Drug Agency
ESA erythropoiesis-stimulating agent
FEV1 forced expiratory volume in 1 second
IOC(MC) International Olympic Committee (Medical Commission)
Key background: history of drugs in sport
THE desire to excel in sport, and the pressure to win at all costs, may lead athletes to experiment with taking substances or using methods that are perceived to provide such advantages as improved strength, motor coordination, endurance or concentration. Doping is defined as the use in sport of substances and/or methods prohibited under that sport’s rules, to enhance performance or mask banned behaviours. Doping practices are prohibited in sport because it is generally agreed that doping may artificially enhance sports performance, contravenes the ethics of both sport and medical science and can be detrimental to the health of athletes.
History
It is not a recent phenomenon for athletes participating in sporting competitions to use drugs or magic potions in attempts to gain an advantage or improve performance. The ancient Egyptians used a drink made from ground and boiled hooves of asses (probably rich in gelatine and other proteins) and flavoured with roses, while in Roman times gladiators used stimulants to help recovery after injury. The Greek physician Galen, writing in the first century AD, reported athletes at the ancient Olympic Games using stimulants and special diets (including dried figs) to enhance performance.
In the 19th century, swimmers, cyclists and longdistance runners used stimulants, especially strychnine, caffeine, nitroglycerine and cocaine. Not surprisingly, many athletes died after taking such cocktails; this provided the impetus to control the abuse of drugs in sport. In early 20th century Tour de France cycling races, riders used alcohol and ether to dull the pain of competing in the endurance event. In the mid-20th century, the drugs most commonly abused were amphetamines, after their widespread use during World War II among military personnel to increase alertness and reduce fatigue. Cyclists on amphetamines died in the 1960 Olympic Games and the 1967 Tour de France (including the leader of the British team). Abuse of anabolic steroids came to prominence in the 1950s in America among bodybuilders, weightlifters and footballers. The International Olympic Committee (IOC) established a Medical Commission to design strategies to combat the misuse of drugs in Olympic sport. The World Anti-Doping Agency (WADA) was established in 1999. WADA-accredited laboratories now test more than 200,000 samples per year (Catlin et al 2008).
World records in most sports have improved consistently over time, with major improvements especially in strength events (lifts and throws) and in women’s events. Various factors have been credited with enhancing performances, including natural selection, improved training programs, implementation of findings from sports physiology, better nutrition and doping. In many sports the trend is approaching a plateau, and in some—notably women’s track and field strength events—the current best performances are significantly below those recorded in the infamous years when there was a systematic state-regulated doping program in some former Eastern bloc countries. It is feared that, as records asymptote towards a plateau, with less margin for honest physiological improvement, there is more pressure (from athletes, coaches, governments and the public) for resort to dishonest means to enhance performance (see later discussion under ‘Ethics in Sport’).
Amphetamines, cannabis and anabolic steroids are still widely abused despite bans and more sophisticated detection methods (see Clinical Interest Box 49-1 for some infamous cases).
Clinical Interest Box 49-1 Some doping-in-sport cases
Many cases of doping in sport have become infamous:
Evidence of efficacy?
There is in fact little hard scientific evidence of significant beneficial effects from many of the drugs or methods used. However, athletes and coaches often put great faith in the hoped-for efficacy of drugs while ignoring their proven adverse effects (see Clinical Interest Box 49-2). It is important that double-blind placebo-controlled clinical trials be run on the safety and efficacy of drugs in athletes, but there are major logistical and ethical problems—not least that athletes participating in trials of banned drugs would be liable to sanctions and prohibition from sporting competition.
Clinical Interest Box 49-2 Anabolic steroid use in sydney
Users (past, present and potential) of anabolic androgenic steroids (AASs) were invited to attend anonymously a clinic at an inner-city Sydney hospital, specifically to study their AAS use by questionnaire and physical examination. The 58 men reported:
The conclusions from the study were that the majority of AAS users experienced serious adverse effects; however, after discussion of the results, only 19% of the men reported that they would not use AASs in the future (O’Sullivan et al 2000).
Use and abuse of drugs in sport
The IOC and WADA codes
Recognising that—for safety and fairness—there needed to be regulation and testing of drug use in sport, the IOC over the years promulgated a medical code that listed classes of prohibited substances and methods of doping, as the basis of its doping policy. Recently, the World Anti-Doping Agency (WADA) assumed responsibility for doping control at the international level from the IOC. The national sporting organisations of most countries adopt WADA’s policies and classifications of ‘Prohibited Substances and Methods in Doping’.
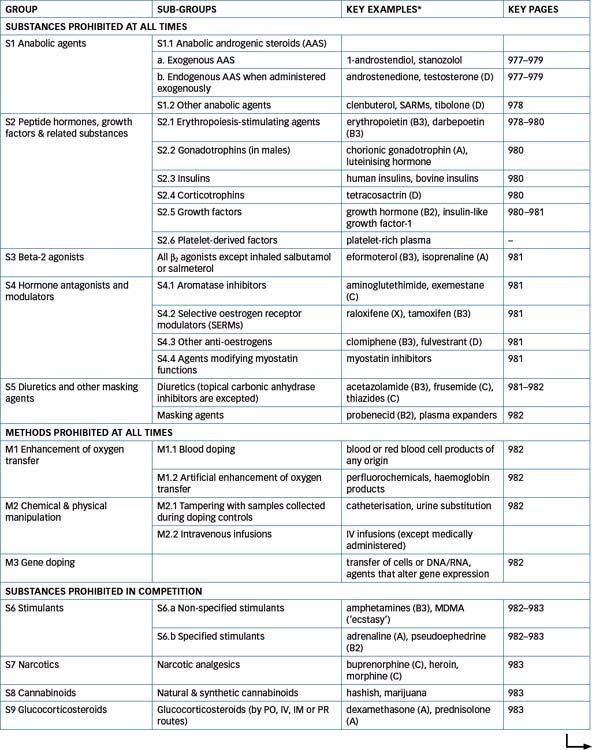
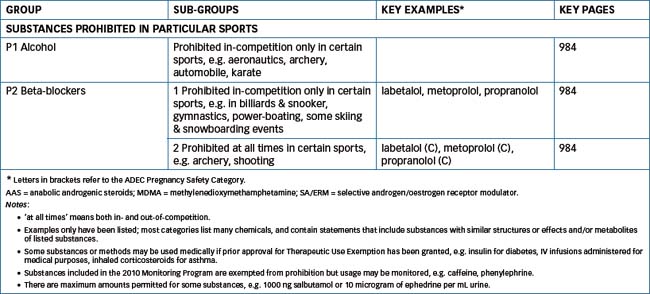
The WADA code classifies drugs and methods into four main groups: those banned at all times (in- and out-ofcompetition), those banned only in-competition, those called restricted (banned only in particular sports) and those which are not banned but are ‘specified’ as being particularly likely to lead to inadvertent violations and which may be monitored for abuse (see Table 49-1 for a summary of the 2010 Prohibited List; the list is updated annually). WADA also regulates the approval for therapeutic use in sport of drugs that would otherwise be banned. The onus is always on the athlete to ensure that any substance taken is approved for use in sport; ignorance is no excuse for a violation.
Table 49-1 Summary of the world anti-doping code 2010 prohibited list (see text and wada website for details)
WADA Prohibited List
The classes of drugs and methods that come under bans or restrictions include:
The presence of a prohibited substance or its metabolite or marker in a bodily specimen is a violation of the WADA rules, as are using, attempting to use, possessing or trafficking in a prohibited substance. Recommending, facilitating or authorising use of these doping drugs and methods are also prohibited. Refusing to submit to a test, unavailability for testing or interfering with testing procedures are also violations.
Exemptions for Therapeutic Use
It is recognised that in some cases there may be a medical requirement for an athlete to take particular drugs; for example, people with diabetes cannot stop using insulin, nor can those with asthma be expected to go without bronchodilators. In these situations, athletes are strongly advised to check with their national sporting association for approval procedures (such as applying for a Therapeutic Use Exemption), to take only medications prescribed by a doctor familiar with the WADA rules and to ensure that all preparations they take do not contain prohibited or restricted substances.2 When an athlete is required to provide a sample (urine or blood) for doping control, it is essential that all medications administered in the previous three days be declared on the official record.
Sanctions
The sanctions (penalties) applied to athletes testing positive to banned substances range from an initial warning to a 4-year ban for a first offence, and a possible life ban for subsequent offences. For example, in 2009 two young athletes in the Australian under-20 National Rugby League competition were penalised: a Gold Coast Titan banned for 2 years after testing positive to nandrolone, an anabolic androgenic steroid, and a New Zealand Warrior banned for 4 months after testing positive to cannabis.
The Australian Sports Anti-Doping Authority
Australia’s anti-doping program in relation to drugs in sport is administered by the Australian Sports Anti-Doping Authority (ASADA), which was established in 2006. ASADA is an integrated anti-doping organisation with functions outlined in the Australian Sports Anti-Doping Authority Act 2006 (Cth) and the Australian Sports Anti-Doping Authority Regulations 2006 (Cth). The ASADA website (http://www.asada.gov.au/) has much information about drugs in sport, and includes sites where athletes and others can check substances for restrictions, log their whereabouts or apply for exemption to allow medical use of a substance.
On its creation, ASADA assumed the drug testing, education and advocacy roles that were previously the mandate of the Australian Sports Drug Agency (ASDA) and also the functions of the Australian Sports Drug Medical Advisory Committee. ASADA has the power to investigate suspected violations of the Anti-Doping Rules, make recommendations on its findings and present cases against alleged offenders at sport tribunals. ASADA is also empowered to exchange sensitive information with the Australian Customs Service and the Australian Federal Police. Amendments were passed in 2009 in the ASADA Amendment Bill 2009 (Cth), reflecting recommendations from an independent review in 2008, implementing new structural and governance arrangements and establishing a panel to consider violations and sanctions.
Drugs and methods banned in sports
International lists of banned and restricted substances and methods are published (see for example in the early pages of MIMS Annual under ‘General medical and scientific information’). Because the lists cannot include every prohibited substance by every name used in every country, drugs are listed by class, and the term ‘and related substances’ or ‘includes but is not limited to’ is often added to embrace all substances having similar structures or actions. (The pharmacology of all these drugs is discussed in detail in earlier chapters; cross-references to appropriate Drug Monographs will be given to avoid repetition of information.) The WADA 2010 Prohibited List is summarised in Table 49-1; codes shown below refer to the WADA List groupings.
Substances prohibited at all times
Anabolic androgenic steroids (AAS; S1.1)
This group includes both exogenous (non-natural) steroids (S1.1a) such as stanozolol, nandrolone, fluoxymesterone and boldenone, and endogenous (natural) hormones (S1.1b) and their metabolites such as testosterone (T), androstenedione, dihydrotestosterone and dehydro epiandrosterone (DHEA). These are similar in effects to the natural androgenic hormone testosterone (see Drug Monograph 39-1). The male sex hormones have physiological actions in promoting tissue growth and repair (anabolic effects) and in main taining the male sex organs and characteristics (androgenic actions) (see review by Kicman [2008]).
It should be noted that androstenedione, formerly permitted, is now on the Prohibited List. Androstenedione is a natural precursor to the sex hormones and is produced endogenously in the adrenal glands and gonads, and in plants. It gained wide popularity as an ergogenic aid, assuming that it is converted to testosterone and will thus have anabolic effects. However, some studies have demon strated oestrogenic rather than androgenic effects in humans, and it is suggested that, if useful anabolic actions are possible, then adverse androgenic effects will also occur.
Abuse of AAS
Synthetic formulations are widely abused in conjunction with high-protein diets and intensive training, by both men and women hoping to increase muscle strength and body weight, to maximise the effects of training, to enhance appearance and to improve the chances of winning in sports. Use of AASs in the USA has been estimated to be as high as 80% in weightlifters and bodybuilders, while use overall by competitors in strength, power and endurance sports may be as high as 50%. Performance enhancement is particularly noticeable in women, as are the virilising effects; young adult males who abuse AASs are also associated with violent behaviours. Many users continue to abuse AASs despite knowing about and suffering from the adverse reactions (see Clinical Interest Box 49-2). Abuse of AAS has filtered into many sections of society; some recreational street drug users now use AAS to counteract the anorexic and muscle-wasting effects of illicit psychotropic agents such as cocaine and amphetamines.
Athletes often use the drugs in amounts far in excess (10–100-fold) of the recommended dosages. ‘Stacking’ of drugs (taking multiple anabolic steroids at one time) is a practice used by some. ‘Pyramiding’ refers to starting with a low dose, increasing gradually to high doses, then dropping back to lower doses to try to avoid detection by doping control tests during competition. AASs are readily detectable in urine but, as androgens are natural body hormones, their levels vary. If levels of endogenous AAS hormones exceed those likely to occur naturally, further testing is required. The concentration in a urine sample of a natural but inactive male steroid epitestosterone (E) is used to monitor abuse of AAS: if the T:E ratio is greater than 4, this is taken as evidence that T levels have been artificially increased by administration of exogenous hormone.
Adverse effects
As testosterone is convertible in the body to oestrogens (Figure 35-1), there may be adverse oestrogenic effects of T in men, including hypercalcaemia, infertility, gynaecomastia and decreased gonadotrophin production. Antioestrogens such as tamoxifen are sometimes taken in an attempt to reverse these effects; these are also banned (see below). The general public, and particularly those who work out at gymnasiums and are confronted with the abuse of steroids, should be informed of the potential serious health problems, especially for women and adolescent males, associated with short-term and long-term consumption of anabolic steroids (see Table 49-2).
Table 49-2 Major effects and adverse reactions of anabolic steroids
| Androgenic effects | Increased growth and development of the seminal vesicles and prostate gland |
| Increased body and facial hair | |
| Increased production of oil from the sebaceous glands | |
| Deepening of the voice | |
| Increased sexual interest and desire | |
| Anabolic effects | Increased organ and skeletal muscle mass |
| Increased calcium in bones | |
| Increased retention of total body nitrogen | |
| Increased haemoglobin concentration | |
| Increased protein synthesis | |
| Adverse reactions | |
| Both sexes | Hypercalcaemia, urinary calculi |
| Cardiovascular disease, oedema of feet or legs | |
| Jaundice, liver impairment; liver carcinoma (rare) | |
| Hypersensitivity | |
| Acne, tendon rupture | |
| Insomnia; mood swings: depression, paranoia, aggression (‘roid rage’) | |
| Iron-deficiency anaemia | |
| Nausea, vomiting, anorexia, stomach pains | |
| Increased risk of tumours | |
| Females | Oily skin, acne |
| Decrease in breast size, ovulation, lactation or menstruation | |
| Hoarse and deep voice tone (usually irreversible) | |
| Clitoral enlargement | |
| Unusual hair growth and/or male-type baldness (usually irreversible) | |
| If pregnant: fetal damage | |
| Males | Increased penis size, and enhanced secondary male characteristics |
| Baldness | |
| Priapism (continuing erections), difficult/increased urination | |
| Increase in breast size (gynaecomastia) | |
| Testicular atrophy, oligospermia, impotence, infertility | |
Advocates of steroid use claim that AASs boost muscle bulk and strength, while antidrug campaigners believe that the steroids merely engender feelings of aggression that encourage the person to train harder, and have serious adverse effects. There is little objective scientific evidence of positive effects of AASs on performance in athletes. The disqualification of Olympic athletes for using steroids, along with the many undesirable and harmful effects reported from their use, has led to an increase in regulation of this category of drugs.
Other anabolic agents (S1.2)
Included here are miscellaneous drugs such as selective androgen receptor modulators, tibolone (which has both male and female sex hormone activities) and the β-2 agonist clenbuterol (only approved in Australia for use in veterinary medicine). This classification previously included the main β-2 adrenoceptor agonists; however, these have now been moved into a separate group (S3).
Peptide hormones, growth factors and related substances (S2)
Many peptide hormones and related substances have been abused in sport for their growth-promoting or anabolic effects. Some are banned only in men. Where relevant, the appropriate hypothalamic-releasing factor or its analogues are also banned; thus growth hormone (GH; somatotrophin), various growth factors and ‘any other growth factor affecting muscle, tendon or ligament...’ are all banned. Glucocorticosteroids are classified by WADA as a separate group. The WADA rules stipulate that the detection in urine of an abnormal concentration of any of the banned hormones or their diagnostic markers constitutes an offence unless it can be conclusively proven to be solely due to a physiological or pathological condition (or, in the case of insulin, the person is registered as having insulindependent diabetes). Examples of banned hormones are shown in Table 49-1.
Erythropoiesis-stimulating agents (S2.1)
Erythropoietin (EPO; epoetin) is a glycoprotein hormone produced naturally in the kidney and liver when tissue hypoxia occurs. Its main physiological function is to bind to receptors on red blood cell (RBC) precursors in the bone marrow and increase production of RBCs (erythropoiesis) and oxygen-carrying capacity. EPO and a long-acting derivative, darbepoetin, are indicated for pharmacological treatment of renal failure and anaemias, and in AIDSrelated conditions (see Drug Monograph 49-1). Prolonged administration of EPO has been shown to raise haemoglobin levels and aerobic performance in healthy men, so it has been widely abused in endurance sports such as cycling and cross-country skiing.
Drug Monograph 49-1 Epoetin alfa
Epoetin alfa (EPO) is the approved name for a form of human erythropoietin produced by recombinant technology from Chinese hamster cell lines. It is a glycoprotein hormone, normally produced by the kidneys, that binds to EPO receptors in erythroid progenitor cells and acts as a colony-stimulating factor, stimulating erythropoiesis in anaemic patients with chronic renal failure in whom normal synthesis of EPO is impaired. The increase in number of mature RBCs takes several days to occur; the subsequent rise in haemoglobin levels may not be significant for 2–10 weeks. EPO improves energy levels and exercise performance, and reduces fatigue and the need for blood transfusions.
Indications
The cause of anaemia should be investigated and other possible treatments tried before EPO therapy is initiated. EPO is indicated in prevention and treatment of anaemia associated with chronic renal failure, anaemia following chemotherapy in patients with non-myeloid malignancies and anaemia in patients scheduled for elective surgery with an expected blood loss, to increase yield of autologous blood donations.
Pharmacokinetics
Because EPO is a protein, it cannot be administered orally. After IV injection, about 10% of the EPO dose is eliminated by the kidneys, with a half-life of 4–6 hours in normal volunteers and 6–9 hours in patients with renal failure. Patients with liver impairment may show increased effects due to decreased metabolism of EPO. Bioavailability after SC injection is only 20%–30% of that after IV administration.
Adverse drug reactions
Early in treatment, flu-like symptoms, bone pain and chills occur. Hypersensitivity reactions may induce rashes, urticaria, respiratory symptoms and hypotension; antibodies can cause red cell aplasia and severe anaemia. Later reactions due to increased RBC mass include hypertension, seizures and thrombotic events.
Drug interactions
The erythropoietic effects may be potentiated by other haematinic agents, including iron supplements. Blood levels of drugs that bind to RBCs, such as cyclosporin, may be altered and should be monitored.
Warnings and contraindications
EPO is contraindicated in patients with severe cardiovascular disease, including hypertension. Hypertension develops during the first 3 months in about 30% of patients treated with EPO. The growth factor activity of EPO may stimulate growth of tumour cells. Haemoglobin, iron, vitamin B12 and folate levels, platelet counts and blood pressure should be monitored regularly.
Dosage and administration
EPO is formulated in vials or prefilled syringes containing a range of strengths of solution, from 1000 IU/0.5 mL to 40,000 IU/mL. Dosage varies depending on indication and on response as monitored by RBC counts; for example, in chronic renal failure, during the correction phase, the dose is 50 IU/kg three times weekly for 1 month, increasing gradually until haemoglobin level is 10–11.5 g/dL.
Adverse effects can be life-threatening: raised levels of RBCs combined with dehydration during endurance sports are likely to raise the haematocrit, ‘thicken the blood’ and potentially cause hypertension, thrombosis and thromboembolic events such as strokes and myocardial infarctions; deaths have occurred in the Tour de France from abuse.3
Detection of abuse of EPO proved a difficult problem for many years, as the hormone is endogenous and has a short half-life (5–6 hours) but long duration of action. Safety guidelines were developed to prevent athletes competing if their haematocrit exceeded 50%. Just in time for the Sydney 2000 Olympic Games, scientists at the Australian Sports Drug Testing Laboratory in Sydney announced the successful development of a blood test for EPO that could detect EPO use up to 4 weeks earlier. The test was approved by the IOC and in use at the Games. It involves a battery of tests including EPO levels, haematocrit and various markers of iron deficiency and transport. New techniques are now available for detection of the new EPO isoforms.
A new EPO analogue with a longer half-life than epoietin is methoxy polyethylene glycol-epoietin beta. It is a chemically-synthesised erythropoiesis-stimulating agent (ESA) produced by recombinant DNA technology, and with large polyethylene glycol polymer inserted in the EPO molecule. It has lower affinity for the EPO receptor, and slower elimination, leading to the much longer half-life that allows dosage just once monthly. It is indicated for administration by SC injection or IV infusion, to treat anaemia associated with chronic kidney disease.
Hematide is another new entry in the prohibited substances list; it is a peptide EPO-mimetic agent that acts as a continuous erythropoiesis receptor activator. Many other erythropoiesis-stimulating agents are in the pipeline, so this group will no doubt be expanded in future Prohibited Lists (see review by Jelkmann [2009]).
Other peptide hormones and growth factors (S2.2-2.6)
Gonadotrophins, such as human chorionic gonadotrophin (hCG; Drug Monograph 38-1) and luteinising hormone, are banned in men because of their actions in increasing the production of endogenous androgenic steroids and reducing the testicular damage from anabolics.
Insulin (Drug Monograph 36-2) is the body’s fuelconserving hormone and so is likely to be abused for its anabolic actions, often in association with anabolic steroids. It is permitted in sport for use by those registered as having diabetes, after approval of a TUE.
Corticotrophin (ACTH, see Figure 35-2) and the analogue tetracosactrin, used to raise blood levels of glucocorticoids and hence improve mood and induce the gluconeogenic, lipolytic and anti-inflammatory effects, are prohibited.
Growth hormone is banned because its use in sport is considered unethical and dangerous (see discussion in Chapter 33 and Drug Monograph 33-2). It is abused because of perceptions that it has anabolic and lipolytic actions, despite absence of hard evidence of enhance ment of performance. The Atlanta Olympics in 1996 were nicknamed the ‘Growth Hormone Games’ because of suspicions of widespread abuse of GH there. At the time of the Sydney 2000 Olympic Games, there was no accepted test for GH abuse, despite many years and millions of dollars of research, and tall and large athletes had to defend themselves against innuendo.4 By the 2004 Athens Olympics, testing methods had been developed such that abuse of GH in the previous 84 days could be identified by alterations in levels of growth factors and other biomarkers of GH actions. Insulin-like growth factors (somatomedins, e.g. IGF-1) are stimulated by GH and mediate many of its anabolic actions, hence are considered likely to be abused and are prohibited.
Beta-2 adrenoceptor agonists (S3)
Beta-2 agonists such as salbutamol (see Drug Monograph 28-2) and eformoterol are usually administered by inhalation for their bronchodilator effects in asthma. They also, however, have anabolic actions through stimulation of β-receptors, including increased glycogenolysis, hyperglycaemia, lipolysis and heat production. They have therefore been abused in sport to increase lean body mass and decrease body fat. There is no evidence that β2 agonists such as clenbuterol alter athletic performance or strength in healthy people; there are, however, reports of sudden deaths in bodybuilders taking the drugs.
These drugs are unusual in that they are classified as both stimulants and anabolics. The ‘stimulant’ effects are those due to stimulation of β1-adrenoceptors in the heart, i.e. increased rate and force of contraction; there may also be effects in skeletal muscle, such as increased rate of contraction, but muscle tremor and cramps are unhelpful in many sports. Systemic β2-agonists are prohibited in sports when administered by oral or parenteral routes.
It is recognised that β2-agonists are essential therapy for asthma. Some (currently two: salbutamol and salmeterol) are therefore permitted for use by inhalation for registered asthmatics, after declaration of use or approval of a TUE.5 It has been shown that about 90% of a dose of inhaled aerosol is actually swallowed, then absorbed from the gastrointestinal tract, so the distinction here between inhaled and oral agents is probably very tenuous.
With respect to doping control testing, a urinary salbutamol concentration higher than 1000 ng/mL counts as a positive result for a β2-agonist agent even if the athlete has flagged therapeutic use, unless the athlete proves by a pharmacokinetic study that it occurred through therapeutic use of an inhaled dose. A standard ‘puffer’ delivers a 100-mcg dose of salbutamol; it can be calculated from salbutamol pharmacokinetic data that, to record a positive test result for salbutamol from an inhaler, an athlete would have to administer about 12–14 puffs within a short space of time. This would certainly cause significant systemic adverse effects such as palpitations, tremor and hypokalaemia.
Hormone antagonists and modulators (S4)
Female hormone antagonists (S4.1–3)
Anti-oestrogens such as clomiphene, selective oestrogen receptor modulators (SERMs; tamoxifen [Drug Monograph 42-3] and raloxifene) and aromatase inhibitors (anastrozole and exemestane) are used clinically in treatment of breast cancers. They may be abused in sport in attempts to overcome some of the adverse feminising effects of AAS, such as gynaecomastia. Previously banned only in men, they are now banned in both sexes. (The pharmacology of these drugs is discussed in Chapters 39, 40 and 42.)
Myostatin antagonists (S4.4)
This is a very new grouping in the Prohibited List, and an indication that WADA has to run fast to keep up with the drug cheats! The gene encoding myostatin was only discovered in 1997, as a member of the transforming growth factor β superfamily of proteins that control growth and differentiation; it is an inhibitor of muscle growth. Mutations in the myostatin gene are associated with gross hypertrophy of skeletal muscle in animals and humans, hence it could be expected that inhibitors of myostatin would enhance muscle growth and thus potentially be useful in treating muscle wasting diseases and muscle dystrophies (as well as enhancing sporting performance). Monoclonal antibodies against myostatin do increase muscle mass in wild-type mice and mice with a mutation in the dystrophin gene, and in monkeys with a muscular dystrophy condition. No small-molecule myostatin inhibitors had gone into clinical use by 2009; however fake ‘anti-myostatins’ are apparently being sold on the internet to athletes keen to get ahead of their competitors and ahead of WADA testing techniques (see review by Fedoruk and Rupert [2008]).
Diuretics and other masking agents (S5)
Diuretics
Diuretics such as the thiazide (Drug Monograph 25-2), potassium-sparing and loop diuretics have been abused in sport to reduce body weight quickly in sports with strict weight classifications, to dilute urine in an attempt to mask the presence of banned substances or to relieve oedema from AAS abuse. Potential adverse drug reactions include dehydration, muscle cramps and cardiovascular impairment. Topical carbonic anhydrase inhibitors such as dorzolamide and brinzolamide used in eyedrops to control glaucoma are not prohibited.
Masking agents
Other masking agents are those used to impair the excretion of prohibited substances or to conceal their presence in bodily samples, whether urine or blood. Examples include probenecid (an antigout drug), to impair excretion of other drugs, or plasma expanders such as glycerol, mannitol or albumin to dilute the banned drug in the bloodstream or to replace volume after dehydration.
Methods of doping prohibited at all times
Enhancement of oxygen transfer (M1)
Formerly called blood doping, these are techniques to enhance oxygen transfer, by the administration of blood, RBCs or blood products to an athlete. It usually involves transfusion of extra blood, either the athlete’s own (autologous) or a compatible donor’s (homologous), into the circulatory system to increase red cell mass to provide extra oxygen-carrying capacity and enhance aerobic performance. It creates a similar effect as training at high altitude (shown to be important in the Mexico Olympics) and so is useful in endurance events such as marathonrunning, cycling and cross-country skiing. The risks involved are those of infections, mismatching of blood, blood or iron overload, increased viscosity (hence thrombosis or embolism) and cardiovascular problems such as heart attack, heart failure or stroke. The ready availability of EPO has now essentially made blood doping by transfusion obsolete.
Another type of blood doping is the administration of artificial oxygen carriers such as perfluorocarbons and artificial haemoglobins. However, use of supplemental oxygen is not prohibited.
Manipulation of samples (M2)
Sample manipulation is the use of pharmacological, chemical or physical means to alter or substitute the body fluid sample, usually urine or blood, taken in a doping control test. Whether or not the attempt at manipulation succeeds is immaterial; attempts are prohibited at all times.
Examples of such techniques include:
Intravenous infusions are prohibited unless prescribed as medical treatment.
Gene doping (M3)
Gene doping, i.e. non-therapeutic use or modification of genes or genetic material (DNA, RNA) to enhance performance, is considered a potential method, and as such has already been prohibited. A likely target for this type of abuse is considered to be the myostatin gene; studies in laboratory and farm animals have shown that deletion of this gene causes massive increase in muscle volume and strength. Another target is the EPO gene; as described in an earlier footnote, mutation in this gene can cause increased RBC production without a prior increase in EPO levels. Other candidate targets are over-expression of splice variants of insulin-like growth factor-1 to induce muscle hypertrophy, enhancement of vascular endothelial growth factors to induce extra angiogenesis, deletion of the angiotensin-converting enzyme gene for increased strength or insertion of it for greater endurance, and expression of peroxisome-proliferator-activated receptor-delta to change muscle phenotype (see reviews by Wells [2008] and Sharp [2008]).
The potential risks are serious, especially the risk that it may prove impossible to ‘turn off’ the new gene or gene product, and the risk of inducing uncontrolled growth and cancers.
Substances banned in-competition only
Stimulants (S6)
Various types of drugs that enhance alertness and aggressiveness and reduce fatigue are classified by WADA as stimulants. Such drugs are often abused as recreational drugs and are likely to be used during competition to reduce fatigue and stimulate the cardiovascular and respiratory systems; they may cause impairment of judgement, hyperthermia and cardiovascular collapse and heighten risk of accidents. Stimulants are most likely to be abused in sports in which intense exercise is required, such as cycling, ice hockey, skiing, football and baseball.
In some previous IOC lists, sympathomimetic amines such as ephedrine, pseudoephedrine and phenylpropanolamine (Drug Monograph 28-6) were prohibited or monitored; these substances may be present in ‘cold cures’, and are taken as decongestants or appetite suppressants or to ‘burn fat’. Many cases have occurred of athletes being banned (and medals removed) after testing positive to these substances taken in ‘cold cures’. In the 2010 WADA code, these substances are ‘specified’ in the Monitoring Program, and maximum urine levels may be specified. After some years of monitoring, it was found that abuse of pseudoephedrine is on the increase, so it is again prohibited above stated levels. Pseudoephedrine has been reported from studies in laboratory test conditions to improve performance of male runners over 1500 metre races by about 2.1%.
Amphetamines are the drugs of choice in treatment of children with attention deficit hyperactivity disorder (ADHD, see Chapter 19); the jury is still out on how long into adulthood these drugs should be prescribed. The number of American baseball players claiming to have ADHD, and getting a TUE for stimulants, has risen dramatically over the last few years.
The 2010 Monitoring Program also includes the stimulants phenylephrine, caffeine (Drug Monograph 19-2), pipradol and bupropion. Caffeine, being the most commonly taken psychoactive drug worldwide, is no longer prohibited or monitored; even very young athletes sometimes abuse caffeine to seek performance advantages from cardiovascular and CNS stimulation. Some studies have shown performance benefits, especially in endurance sports, from moderate amounts of caffeine (e.g. 3–6 mg/kg body weight), an amount that might be consumed in 1–10 cups of coffee, depending on method of brewing (see Clinical Interest Box 21-12; and review by Ganio et al [2009]).
Adrenaline is permitted for local administration or with local anaesthetics.
Narcotic analgesics (S7)
Strong narcotic analgesics such as morphine (Drug Monograph 15-1), buprenorphine, pethidine and methadone (Drug Monograph 21-2) are prohibited in-competition; heroin is not a legal drug in Australia at any time. They are sometimes abused in sport to mask pain or for their euphoriant actions. Adverse effects include tissue damage from ignoring pain signals, sedation, constipation, nausea and vomiting, respiratory depression and addiction. Mild narcotic analgesics, including codeine and pholcodine (Drug Monograph 28-5), and dextropropoxyphene, are permitted.
Cannabinoids (S8)
The popularity of cannabis as a social drug puts it at the top of the list of drugs detected by anti-doping authorities worldwide. All forms of ingested or inhaled cannabinoids (see Chapter 21), such as marijuana, THC and hashish, are prohibited during competition; it is considered that dermatological administration of cannabis is unlikely to lead to significant absorption. Due to its very long half-life, there are problems with interpretation of results of drug testing for cannabis, both in sport and in the context of effects on driving. Adverse effects are impaired coordination, slowing of responses and increased appetite; long-term effects include higher incidence of psychosis and impairment of respiration from smoking ‘joints’ (see review by Saugy et al [2006]).
Glucocorticosteroids (S9)
Glucocorticosteroids (also often referred to as glucocorticoids or corticosteroids) are powerful antiinflammatory and immunosuppressant agents (see Chapters 35 and 47); they may be natural hormones secreted by the adrenal gland, such as hydrocortisone (Drug Monograph 35-1) or synthetic compounds with similar actions. They are likely to be abused in sport for their anti-inflammatory and euphoriant effects or to mask injury. Adverse reactions that limit the usefulness of corticosteroids in athletes include osteoporosis, mood changes, fluid retention and impaired healing.
The status of glucocorticosteroids in sport depends critically on the route by which they are administered. Dermatological administration, e.g. in creams, ointments or sprays applied to the skin, or ear- or eye-drops, is permitted at all times. Systemic administration of corticosteroids, including via the oral, intravenous, intramuscular and rectal routes, is universally banned, and medical use requires an abbreviated Therapeutic Use Exemption (TUE). Glucocorticoids administered by other non-systemic routes, such as by inhalation for asthma, and by intraarticular, intradermal or epidural routes when medically necessary are permitted after approval of a full TUE.
Drugs prohibited in certain sports
Some drugs are prohibited in some sports in-competition and are permitted in other cases. As described above, two β2-agonists are permitted for inhalation by registered asthmatics, but systemic administration is prohibited. In some previous WADA codes, drugs with sedative actions were banned in some sports; however this prohibition has now been relaxed (except for alcohol).
Alcohol (P1)
Alcohol use would be detrimental to most sports, as it can cause impaired motor coordination, prolonged reaction time, sedation and mental confusion, and can become a safety hazard (see Drug Monograph 21-3, and Table 21-4). Athletes are warned that blood alcohol levels may be tested in doping controls in some sports (e.g. modern pentathlon, archery, karate and motor sports). Alcohol use by referees and umpires is prohibited by some sporting organisations.
Beta-blockers (P2)
Beta-blockers, such as propranolol, metoprolol and labetalol, are banned in some sports, as they reduce excitability of the cardiovascular system, thereby reducing blood pressure, cardiac output, heart rate and, importantly, muscle tremor. In some sports, a steady action and reduced response to stress can be beneficial, so β-blockers are restricted in-competition in sports such as gymnastics, shooting, archery, ski-jumping, wrestling and also bridge (the card game). In strenuous and endurance physical sports, however, reduced cardiovascular response to stress would be detrimental. Whether or not β-blockers are prohibited, and when, is determined by the international bodies regulating specific sports.
Substances permitted in sports
Permitted drugs and other substances
It is important for athletes to know not only what drugs are prohibited or restricted in their sports but also what drugs and substances are permitted. Athletes are advised to double-check that medications are permitted before taking them, including over-the-counter, complementary and alternative preparations and drugs from overseas. Some drugs are permitted only in women (e.g. hCG, luteinising hormone) or only in people registered as having particular diseases (e.g. asthma or diabetes). Local anaesthetics (except cocaine) are permitted if medically justified; local anaesthetics mask pain, thus putting the person at risk of tissue damage.
Permitted drugs
Lists of permitted drugs are available from ASADA, particularly drugs used to treat common conditions such as allergies and hay fever, diarrhoea, pain and inflammation, nausea and vomiting, and coughs and colds. For example, aspirin is allowed as a pain-reliever (whereas morphine is not), NSAIDs are allowed as anti-inflammatory agents whereas corticosteroids are tightly controlled, angiotensin-converting enzyme (ACE) inhibitors are being used to enhance oxygen uptake and response to training and sildenafil (aka Viagra, the anti-impotence drug) is being abused so commonly as a vasodilator to enhance cardiovascular capacity that it has been referred to as ‘vitamin V’. Interested persons are always advised to check on the WADA or ASADA website for the approval status of any questioned drug.
Ergogenic aids and nutrients
In attempts to enhance performance without contravening WADA prohibitions, athletes have tried to find other substances that improve energy utilisation (i.e. are ergogenic); nutritional supplements are often taken. Such substances, unlike drugs, do not have to go through extensive clinical trials of safety and efficacy before being marketed, and claims made as to their usefulness are rarely scientifically validated. Sports drinks, energy bars and protein–carbohydrate shakes are all popular with athletes. Thus far, WADA has not banned any ergogenic aids, which in itself suggests that they do not significantly or unfairly enhance performance. However, there is a strong placebo effect encouraging use of supposed ergogenic aids (see review by McClung and Collins [2007]).
There have been many cases of athletes testing positive to banned drugs but claiming only to have taken nutritional supplements; the most infamous cases were of several tennis players all testing positive to AAS but claiming they had taken supplements provided by the Association of Tennis Professionals—they were all exonerated on the basis of strange results from laboratory tests. Substances that have been found in commercial nutritional supplements include testosterone, stanozolol, DHEA, many androstenedione look-alikes and metabolites, caffeine, ephedrine and sibutramine, an anti-obesity drug (see review by de Hon and Coumans [2007]).
Antioxidants
Antioxidants such as carotenes (vitamin A, see Clinical Interest Box 48-4) and vitamins C and E may enhance performance indirectly by detoxifying free radicals (lipid peroxides) formed, thus enhancing recovery. It is accepted that nutritional supplementation with these vitamins may protect athletes from oxidative stress.
Creatine
The amino acid creatine is an important constituent of muscle and is involved in energy utilisation and phosphate exchange. Short-term creatine loading may improve performance during high-intensity exercise such as sprinting, by overcoming creatine depletion (see also Clinical Interest Box 49-3).
Clinical Interest Box 49-3 Does substance use predict steroid abuse?
An interesting study was carried out in 214 Sydney men (mean age: 30 years) who regularly exercised, to determine their level of substance use and intentions to use steroids. Current users of anabolic androgenic steroids (AAS) were excluded from participation; 80% of the subjects reported current use of substances including ‘sports supplements’ with vitamins and proteins, and 36% had used creatine in the previous 6 months. More than half had used illicit drugs (commonly amphetamines and cannabis) recently.
The men were asked why they did not currently use AAS; reasons most commonly given were that steroids are unsafe, not worth risking the side effects, not needed, unnatural, unfair, expensive and illegal. Only 7% said that their sports program tested their urine and they did not want to risk being caught.
Approximately 16% of the men indicated that they would use steroids in the future, hoping to increase their muscle size and strength and improve their appearance. Significant predictors of future abuse of AAS were recent use of creatine, and knowing someone who already used AAS (see Dunn et al [2009]).
Bicarbonate
During long intense exercise, adenosine triphosphate (ATP) is formed from anaerobic glycolysis, and lactic acid accumulates. In an attempt to overcome this acidosis, bicarbonate loading has been tried, with a dose of 300 mg/kg sodium bicarbonate (baking soda) taken 1–2 hours before high-intensity exercise. In some studies, performance has been enhanced by up to 30%. Adverse reactions such as gastrointestinal bloating and diarrhoea can occur, especially if overdoses or insufficient water are taken.
Dietary manipulation
Carbohydrates consumed immediately before or after performance boost glycogen stores and delay fatigue, thus enhancing performance; many athletes ‘carb load’ the night before competition. Protein and amino acid supplementation has anabolic effects, increasing protein synthesis. Some other complementary and alternative medicine therapies used in sport are described in Clinical Interest Box 49-4.
Clinical Interest Box 49-4 Complementary and alternative therapies in sport
Complementary and alternative therapies are increasingly popular and marketed as sport performance enhancers, both as ‘natural’ aids and to circumvent WADA testing. As well as the ergogenic aids described in the text, various food supplements and natural compounds have been tried, including:
As with all herbal and natural products, there are potential problems with respect to knowing all the actual constituents, the strengths of any active ingredients and the presence of any contaminants. Cases are documented of ‘natural’ anti-asthma products being proven to contain synthetic β2-agonists, ‘natural’ antidiabetic remedies containing oral hypoglycaemic agents and ‘natural’ remedies for inflammation containing synthetic glucocorticoids.
ASADA cannot provide information as to the status of complementary and alternative products, as such products are not subject to government regulation, and information about the ingredients is usually sparse. ASADA warns athletes that ‘natural remedies’ may contain banned substances and/or may be toxic. As always, the onus is on the athlete to ensure that a product is safe and not prohibited.
The American College of Sports Medicine (see American Dietetic Association et al [2009]) has published their position stand on nutrition and athletic performance, spelling out optimal nutrition for physical activity, athletic performance and recovery. In summary, provided an athlete has adequate fluid and nutrition from a varied diet, the most important extra requirements are fluid, glucose and salt (sodium chloride), and other supplements are usually not needed.
Drug testing
Drug testing policies
The IOC, international sports federations and some national authorities have regulations to require athletes to undergo drug testing procedures to enforce anti-doping policies. Testing is intended to be a deterrent rather than sufficiently extensive to catch all incidences of use of banned drugs or methods. The first Olympic Games at which testing was carried out were the Mexico Games in 1968; the Australian runner Ron Clarke was the first athlete to be tested.
Testing is carried out not only at competitions, but also now out-of-competition in order to detect drugs taken long-term during training. Many drugs (especially anabolics and blood-doping drugs and methods) are abused chronically for their long-term effects, but if stopped before competition may not show up in samples taken immediately after events. Out-of-competition testing is logistically more difficult to implement. Athletes in a ‘Registered Testing Pool’ are required to provide information as to their daily whereabouts to enable effective no-notice testing.7 For the Sydney Olympic Games, for the first time, many athletes were subjected to testing before competition and out-of-competition, as well as after their events. Summary statistics relating to testing over the period 1988–2008 are shown in Table 49-3.
Table 49-3 Statistics for drug testing by some ioc-accredited laboratories
| Year | Total number of a-samples analysed | % Samples positive for stimulants |
| 1988 | 47,069 | 0.89 |
| 1993 | 89,166 | 0.37 |
| 1998 | 105,250 | 0.39 |
The drug testing process
The doping control procedures carried out at Olympic Games competitions are under the control of the Organizing Committee of those Games. Both urine samples and blood samples may be collected, and breath-testing for alcohol is also implemented. Doping controls are carried out in all sports, and all competitors must agree to comply with the IOC Anti-Doping Code and provide samples as requested. Generally, the first four or five competitors or teams in a final are tested, plus other competitors selected randomly. Competitors are warned that they could be selected more than once and could be tested out-of-competition.
Important stages of the doping control procedures for urine samples include:
The presence of a banned substance is sufficient to count as a positive test: the testing authority does not have to prove how the substance was taken. Positive results are further tested by the IOC, and the duplicate, sample B, may be tested in the presence of the competitor or a representative.
Rights and responsibilities
Health professionals’ rights and responsibilities
Health professionals, especially doctors, physiotherapists and podiatrists, are often consulted by athletes to treat medical conditions, including those arising from participation in sport; to advise on therapeutic and adverse effects from drug use; or to prescribe or provide drugs that may enhance performance. The main responsibility of such health professionals is the health of the athlete; they must also avoid prescribing any drugs banned in the particular sport.
The Royal Australasian College of Physicians (1997) prepared a position paper on drugs in sport and discussed the ethical aspects of prescribing drugs such as anabolic steroids. The College opposes prescribing of drugs for performance enhancement or bodybuilding. In a more recent paper (Orchard et al 2006), the essentials for the practice of sports medicine in Australia were summarised as: ‘Doctors need to know if a patient is an athlete subject to drug testing, and to be aware of the legal situation surrounding drugs they prescribe such patients’.
Athletes’ rights and responsibilities
Athletes have specified rights with respect to the testing procedures, including the right to have a representative and interpreter present and the right to information; for in-competition testing, their rights include performing in a warm-down, victory ceremony or media commitment; obtaining necessary medical treatment or competing in further competitions. Athletes have the responsibility to report immediately for a test when notified, to remain within direct observation of the chaperone at all times after notification of testing until completion of sample collection, to produce appropriate identification and to comply with sample collection procedures.
Ethical aspects of drugs in sport
There are many philosophical and ethical issues related to the use and abuse of drugs in the sporting arena. Some of these issues and controversial questions are summarised below:
As they are ethical and philosophical questions rather than scientific hypotheses, these issues cannot readily be resolved; however, it is important that they be debated and not ignored. Meanwhile, the testing authorities continue to refine techniques to assay more drugs down to lower blood levels, and some competitors still manage to circumvent the anti-doping policies of sporting authorities (see reviews by Kayser et al [2007]; emps Lardon [2008]; and Spedding and Spedding [2008]).
Note: To avoid repetition, the earlier Table 49-1, the WADA 2010 Prohibited List, has been modified to double as a ‘DRUGS AT A GLANCE’ table; note that the pharmacological mechanisms and therapeutic uses of these drugs are all covered in earlier chapters and are cross-referenced wherever possible. Many substances abused in sport have no medical uses, so have not been classified with respect to pregnancy safety.
Key points
Review exercises
Note: References marked with an asterisk, Note: References marked with an asterisk (*) come from an issue of the British Journal of Pharmacology (volume 154, issue 3) published in June 2008 to coincide with the Beijing Olympic Games and devoted to Drugs in Sport, with 11 articles related to the actions and detection of the major drug groups involved, written by experts in the field. The paper by Spedding and Spedding is unique in that it is by two brothers, both runners, of whom one won the Olympic marathon bronze medal in 1984 and the other is a Professor of Pharmacology. The articles can be downloaded from http://www.brjpharmacol.org/details/issue/143218/volume_154_issue_3_june_2008.html.
Alaranta et al., Alaranta A, Alaranta H, Helenius I. Use of prescription drugs in athletes. Sports Medicine 38(6): 449-463.
American Dietetic Association et al. American College of Sports Medicine position stand: Nutrition and athletic performance. Medicine & Science in Sport & Exercise. 2009;41(3):709-731.
Anderson S.D., Sue-Chu M., Perry C.P., et al. Bronchial challenges in athletes applying to inhale a beta-2 agonist at the 2004 Summer Olympics. Journal of Allergy and Clinical Immunology. 2006;117(4):767-773.
Australian Sports Anti-Doping and Authority., Australian Sports Anti-Doping Authority. 2007/08 Annual Report. ASADA, Canberra.
Bains A. EPO to finish last, in Aussie first. Today’s Life Science 2000; Sept/Oct: 18.
Catlin D.H., Fitch K.D., Ljungqvist A. Medicine and science in the fight against doping in sport. Journal of Internal Medicine. 2008;264(2):99-114.
Corrigan B., Kazlauskas R. Drug testing at the Sydney Olympics. Medical Journal of Australia. 2000;173:312-313.
Davis E., Loiacono R., Summers R.J. The rush to adrenaline: drugs in sport acting on the beta-adrenergic system. British Journal of Pharmacology. 2008;154(3):584-597.
Dawson R.T. Drugs in sport: the role of the physician. Journal of Endocrinology. 2001;170(1):55-61.
de Hon O., Coumans B. The continuing story of nutritional supplements and doping infractions. British Journal of Sports Medicine. 2007;41:800-805.
Dillon P., Cox G., O’Connor M. What’s the score? The Facts on Alcohol, Drugs and Sport. Canberra: Australian Sports Commission; 2004.
Docherty J.R. Pharmacology of stimulants prohibited by the World Anti-Doping Agency (WADA). British Journal of Pharmacology. 2008;154(3):606-622.
Dunn M., Mazanov J., Sitharthan G. Predicting future anabolicandrogenic steroid use intentions with current substance use: findings from an internet-based survey. Clinical Journal of Sport Medicine. 2009;19(3):222-227.
Fedoruk M.N., Rupert J.L. Myostatin inhibition: a potential performance enhancement strategy? Scandinavian Journal of Medicine and Science in Sports. 2008;18(2):123-131.
Fricker P. The anti-doping code in sport: update for 2004. Australian Prescriber. 2004;27(4):84-87.
Ganio M.S., Klau J.F., Casa D.J., et al. Effect of caffeine on sportspecific endurance performance: a systematic review. Journal of Strength and Conditioning Research. 2009;23(1):315-324.
Holt R.I. Growth hormone, IGF-1 and insulin and their abuse in sport. British Journal of Pharmacology. 2008;154(3):542-556.
Jelkmann W. Erythropoiesis stimulating agents and techniques: a challenge for doping analysts. Current Medicinal Chemistry. 2009;16(10):1236-1247.
Kayser B., Mauron A., Miah A. Current anti-doping policy: a critical appraisal. BMC Medical Ethics. 2007;8:2.
Kennedy M.C.S. Drugs, sport and the Olympics 2000-2004. Medical Journal of Australia. 2004;181(4):227.
Kennedy M.C., Kennedy J.R. Ethics of prescribing drugs to enhance sporting performance. Medical Journal of Australia. 1999;171:204-205.
Kicman A.T. Pharmacology of anabolic steroids. British Journal of Pharmacology. 2008;154(3):502-521.
Kron J. Staying clear of steroids. Australian Doctor. 2000;6:51-52. Oct
Lainscak M., Osredkar J. Doping and the Olympic games: the good, the bad and the ugly. Wiener Klinische Wochenschrift. 2009;121:13-14.
Lardon M.T. Performance-enhancing drugs: where should the line be drawn and by whom? Psychiatry. 2008;5(7):58-61.
Mason C. Gold medals, vitamin V and miscreant sports. Canadian Medical Association Journal. 2008;179(3):219-222.
McClung M., Collins D. “Because I know it will”: placebo effects of an ergogenic aid on athletic performance. Journal of Sport and Exercise Psychology. 2007;29(3):382-394.
Mullis P.E. Doping in sport. Clinical Endocrinology & Metabolism. 14(1), 2000. [Special issue devoted to drugs in sport; including papers on anabolic steroids, growth hormone, CNS stimulants, blood boosting, EPO, and analytical testing.]
Orchard J.W., Fricker P.A., White S.L., Burke L.M., Healey D.J. The use and misuse of performance-enhancing substances in sport. Medical Journal of Australia. 2006;184(3):132-136.
O’Sullivan A.J., Kennedy M.C., Casey J.H., et al. Anabolicandrogenic steroids: medical assessment of present, past and potential users. Medical Journal of Australia. 2000;173:323-327.
Royal Australasian College of and Physicians. Drugs in sport: a position paper. RACP Fellowship Affairs; 1997.
Saugy M., Avois L., Saudan C., et al. Cannabis and sport. British Journal of Sports Medicine. 2006;40(Suppl 1):i13-i15.
Sharp N.C.C. The human genome and sport, including epigenetics and athleticogenomics: a brief look at a rapidly changing field. Journal of Sports Sciences. 2008;26(11):1127-1133.
Sinclair C.J., Geiger J.D. Caffeine use in sports: a pharmacological review. Journal of Sports Medicine & Physical Fitness. 2000;40(1):71-79.
Sonksen P.H. Insulin, growth hormone and sport. Journal of Endocrinology. 2001;170(1):13-25.
Spedding M., Spedding C. Drugs in sport: a scientist–athlete’s perspective: from ambition to neurochemistry. British Journal of Pharmacology. 2008;154(3):496-501.
Stuart M. The war on drugs in sport: a perspective from the Athens Olympics. Pharmaceutical Journal. 2004;273(7315):320-321.
Sydney Organising Committee for the Olympic Games (SOCOG). Doping Control Guide, Sydney 2000. Sydney: SOCOG; 2000.
Warren M.P., Shantha S. The female athlete. Clinical Endocrinology & Metabolism. 2000;14(1):37-53.
Wells D.J. Gene doping: the hype and the reality. British Journal of Pharmacology. 2008;154(3):623-631.
Australian Sports Anti-Doping Authority: www.asada.gov.au/
Australian Sports Anti-Doping Authority publications available at: www.asada.gov.au/resources/publications.html
New Zealand Medicines and Medical Devices Safety Authority: www.medsafe.govt.nz
World Anti-Doping Agency: www.wada-ama.org/en/
WADA publications and reports available at: www.wada-ama.org/en/Resources1/Publications/
More weblinks at: http://evolve.elsevier.com/AU/Bryant/pharmacology