Cardiac and Vascular Care Plans
Acute Coronary Syndromes/Myocardial Infarction
 = Independent
= Independent  = Collaborative
= Collaborative For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
Unstable Angina; ST-Segment Elevation Myocardial Infarction; Non–ST-Segment Elevation Myocardial Infarction; Non–Q-Wave Myocardial Infarction; Q-Wave Myocardial Infarction
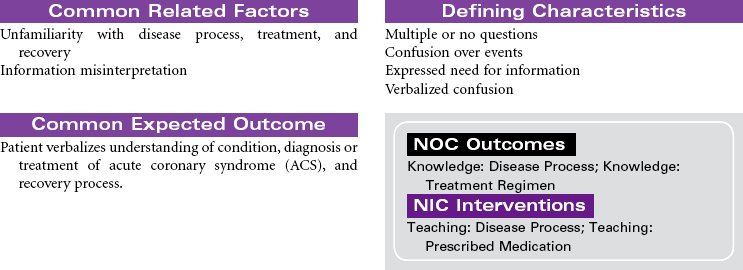
Acute coronary syndromes (ACSs) represent a spectrum of clinical conditions associated with acute myocardial ischemia. Most patients who experience ACS have atherosclerotic changes in the coronary arteries. Chronic inflammatory processes play a key role in the pathogenesis of atherosclerosis. The presence of atherosclerotic plaques narrows the lumen of the arteries, and disruption or rupture of those plaques exposes a thrombogenic surface on which platelets aggregate, contributing to thrombus formation that diminishes blood flow to the myocardium. The resulting imbalance between myocardial oxygen demand and supply is the primary cause of the clinical manifestation in ACS. Other causes of ACS include coronary artery spasm and arterial inflammation related to infection. Noncardiac conditions that increase myocardial oxygen demand can precipitate ACS in patients with preexisting coronary artery disease (CAD). These conditions include fever, tachycardia, and hyperthyroidism. Decreased myocardial oxygen supply can occur in noncardiac conditions such as hypotensive states, hypoxemia, and anemia.
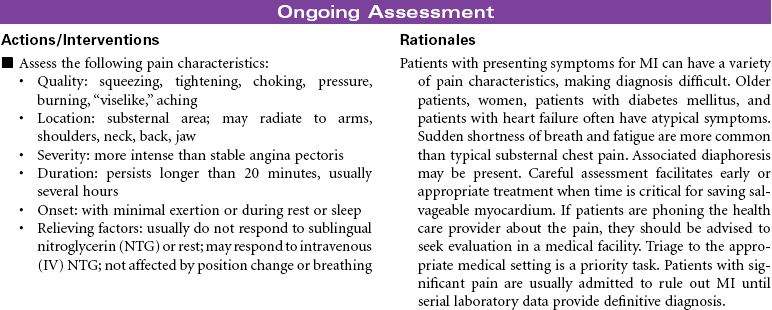
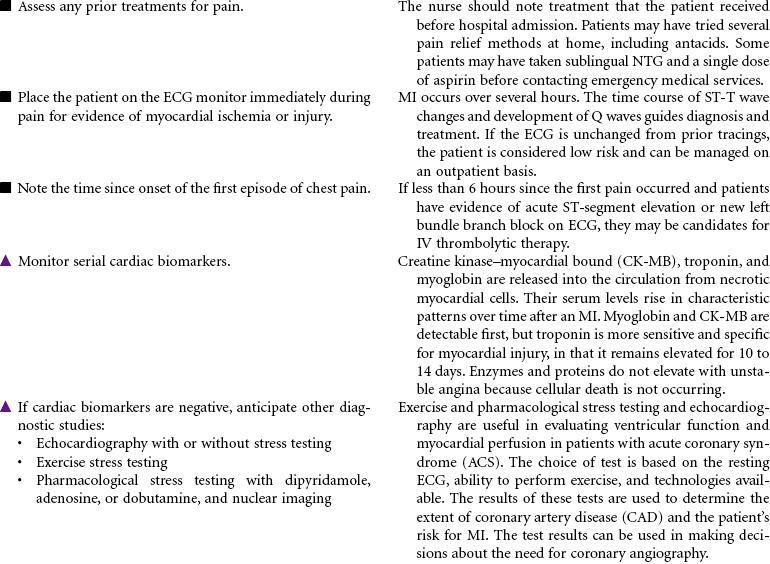
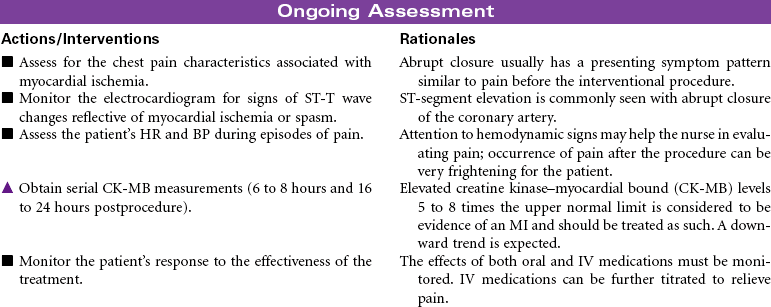
Clinical conditions included in ACS are unstable angina, variant angina, non–ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI). Evaluation of chest pain related to these disorders is a major cause of emergency department visits and hospitalizations in the United States. The term ACS is used prospectively to diagnose patients with chest pain or other clinical manifestations indicating the need to be triaged for treatment of unstable angina or acute MI. Although their pathogenesis and clinical presentation are similar, they differ primarily by whether ischemia is severe enough to cause sufficient myocardial damage to release detectable quantities of cardiac biomarkers (e.g., troponin, creatine kinase–myocardial bound [CK-MB], myoglobin) denoting acute MI. Early identification of ACS and intervention to improve myocardial perfusion reduces the risk for sudden cardiac death and acute MI in these patients.
Unstable angina is characterized by: (1) angina that occurs when the patient is at rest, (2) angina that significantly limits the patient’s activity, or (3) previously diagnosed angina that becomes more frequent, lasts longer, and increasingly limits the patient’s activity. Patients typically do not have ST-segment elevation and do not release cardiac biomarkers indicating myocardial necrosis. NSTEMI is distinguished from unstable angina by the presence of cardiac biomarkers, indicating myocardial necrosis. Most patients do not develop new Q waves on the electrocardiogram (ECG) and are diagnosed with non–Q-wave MI. STEMI is characterized by release of cardiac biomarkers and the presence of new Q waves on the ECG.
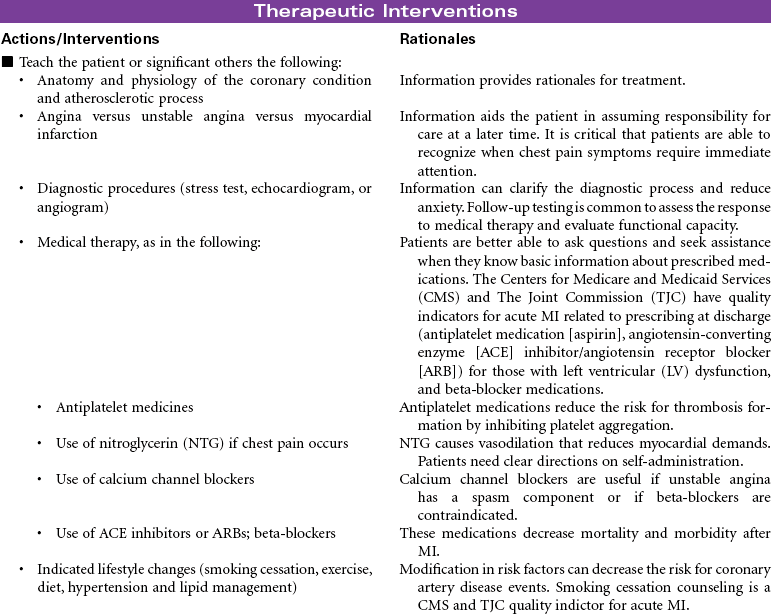
This care plan focuses on the assessment of and interventions for patients with all of these conditions. The American Heart Association and the American College of Cardiology have developed treatment guidelines for patients with unstable angina and NSTEMI, as well as for STEMI. Each guideline addresses initial and ongoing drug therapy, indications for fibrinolytic and percutaneous coronary interventions, and discharge considerations. For patients with MI, the therapeutic goals are to establish reperfusion, to minimize the infarct size, to prevent and treat complications, and to provide emotional support and education. The Centers for Medicare and Medicaid Services (CMS) and The Joint Commission (TJC) have developed core performance measures/quality indicators for acute MI treatment. This care plan focuses on acute management of ACS. The cardiac rehabilitation care plan presented later in this chapter addresses specific learning needs.
 Acute Pain
Acute Pain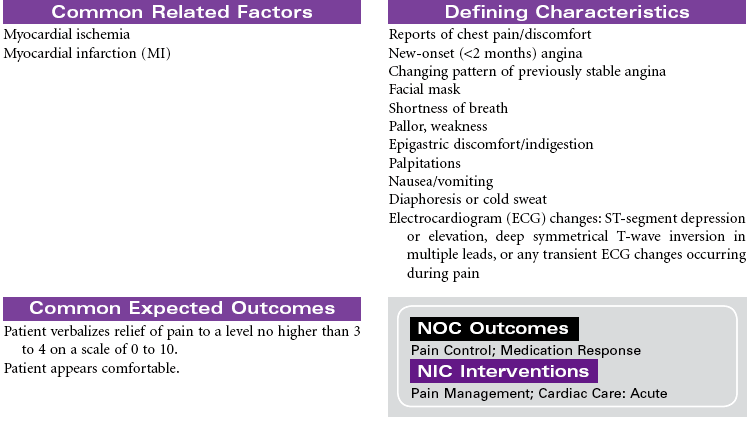





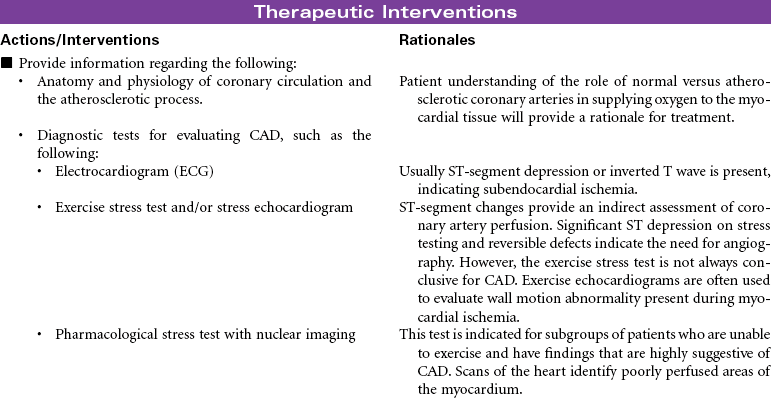
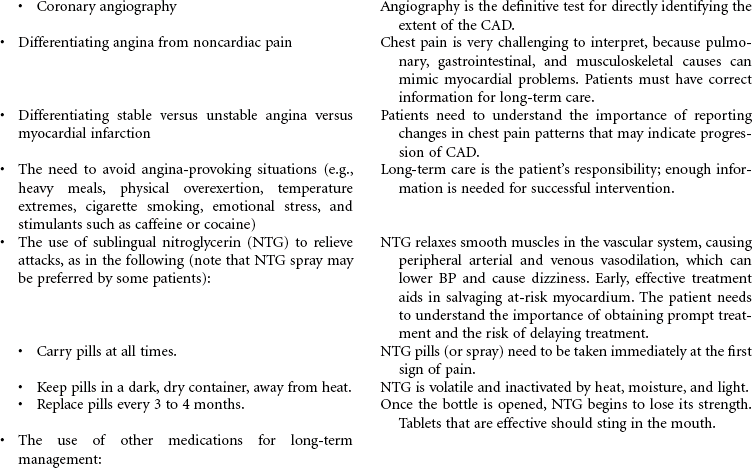
Angina Pectoris, Stable
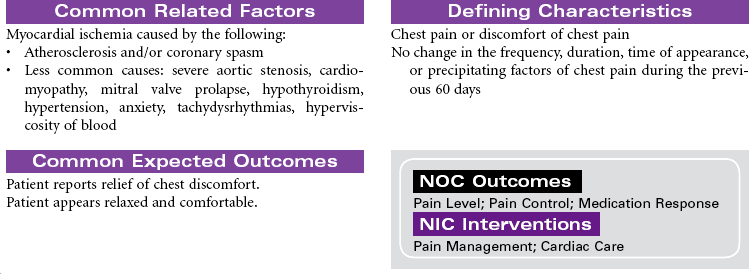
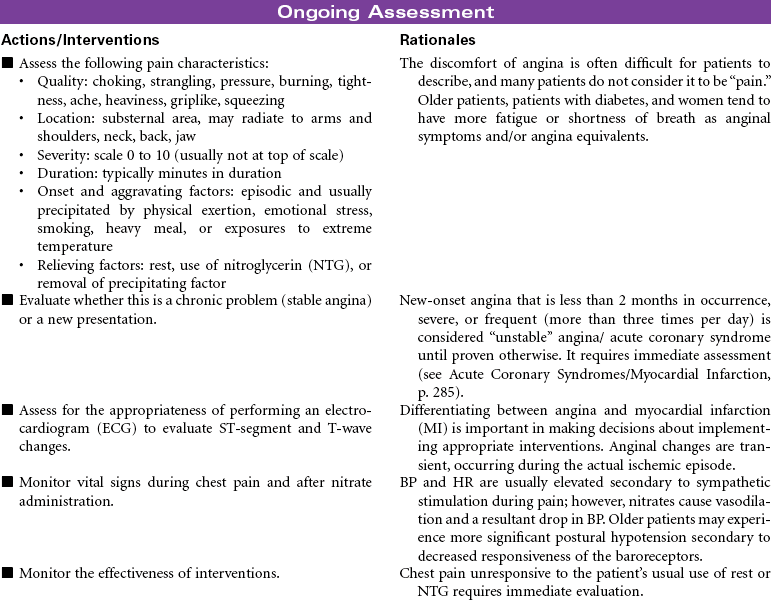
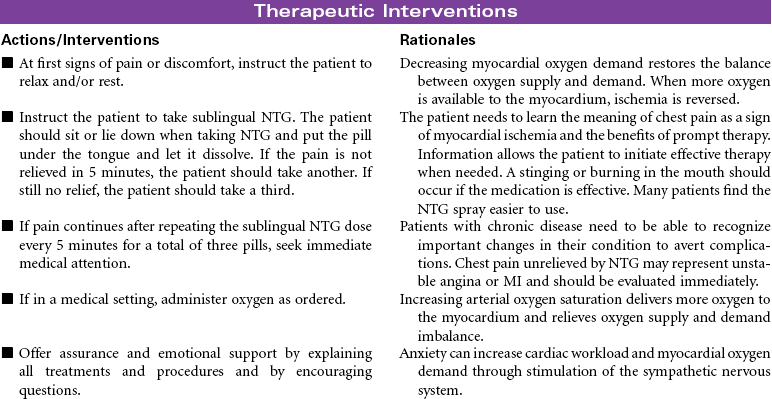
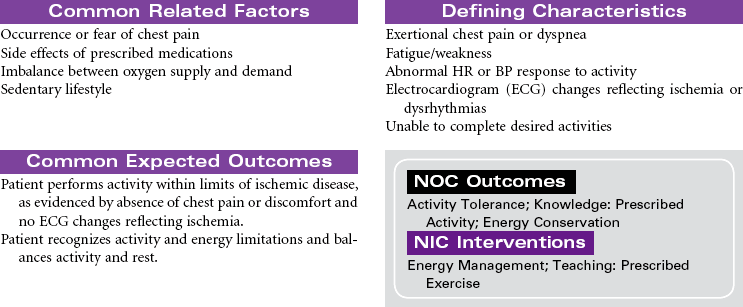
Stable angina pectoris is a clinical syndrome characterized by the abrupt or gradual onset of substernal discomfort (often with radiation to the neck, jaw, shoulder, back, or arm) caused by insufficient coronary blood flow and inadequate oxygen supply to the myocardial muscle. The patient with stable angina will have episodes of chest pain that are usually predictable. Chest pain will occur in response to hypoxia, or is aggravated by physical exertion or emotional stressors. Situations that increase myocardial oxygen demand or decrease oxygen supply include both cardiac and noncardiac causes. Stable angina usually persists for only a few minutes and subsides with cessation of the precipitating factor, rest, or use of nitroglycerin (NTG). Patients may present in ambulatory settings or during hospitalization for other medical problems. Stable angina usually can be controlled with medications on an outpatient basis. Stable angina can significantly affect one’s quality of life. A person may limit activities based on fear of precipitating episodes of chest pain.


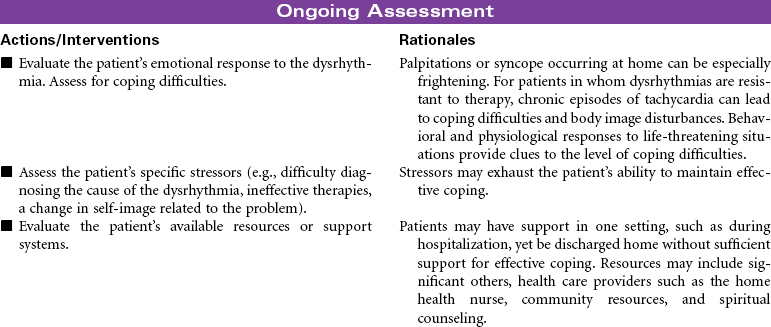
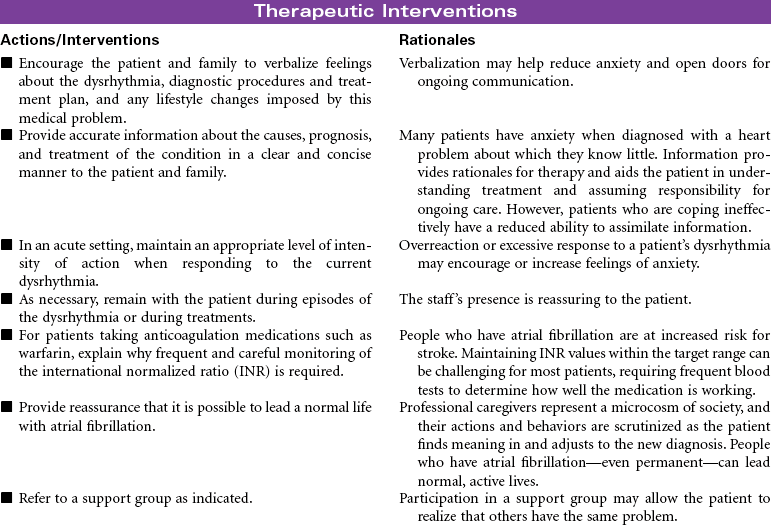
Atrial Fibrillation
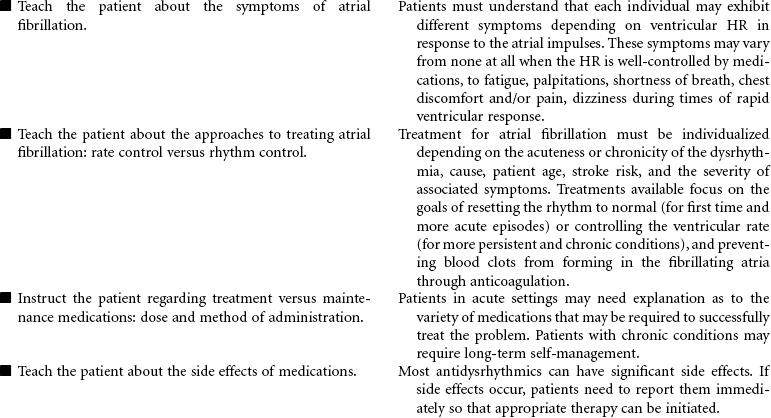
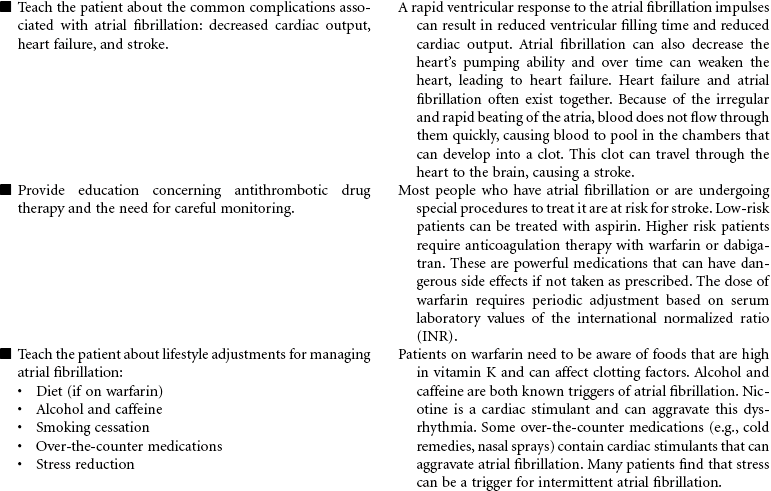
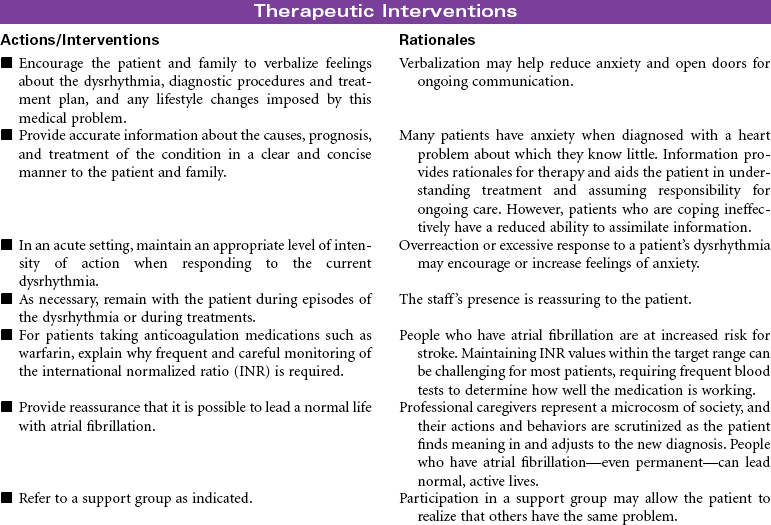
Atrial fibrillation is the most common sustained heart rhythm disturbance in the United States, affecting more than 2 million people. It is an abnormal heart rhythm characterized by an irregular or often rapid heart beat causing reduced cardiac output. In this dysrhythmia, the upper chambers of the heart (atria) fibrillate (quiver) rapidly and erratically, resulting in pooling of blood in the atrium and an irregular ventricular HR and pulse. Although atrial fibrillation itself is not life-threatening, if not adequately treated, it can cause significant side effects resulting in a decreased quality of life and can increase the risk for stroke and heart failure. Because the incidence of atrial fibrillation increases with age, this medical condition is projected to be a huge medical problem as the United States and world population ages. Atrial fibrillation is classified by how it terminates: paroxysmal atrial fibrillation, referring to occasional occurrences that start and stop on their own; persistent atrial fibrillation, a condition in which the abnormal rhythm continues for more than a week, does not self-terminate, but can be treated to a return to normal rhythm; and permanent atrial fibrillation, a condition in which the abnormal rhythm is chronic and unresponsive to treatment.
The most common causes and risk factors for atrial fibrillation include age older than 60 years, heart disease including valve disease, hypertension, heart failure, prior open heart surgery, thyroid disease, chronic lung disease, exposure to stimulants or excessive alcohol, viral infections, and sleep apnea. Some people develop atrial fibrillation for no apparent reason (termed “lone afib”).
Symptoms vary with each person depending on age, cause, and how much the atrial fibrillation affects the contractility of the heart. Symptoms can range from pulse rate that is faster than normal or changing between fast and slow with mild fatigue to shortness of breath, heart palpitations or fluttering, decreased BP, chest tightness or discomfort, dizziness, lightheadedness. Atrial fibrillation is diagnosed by an electrocardiogram (ECG) while the abnormal rhythm is occurring, but if the rhythm is intermittent, a portable Holter ECG monitor or an event recorder is used to document the dysrhythmia.
Management of atrial fibrillation can vary depending on the type, how long the person has had it, and factors such as age, underlying heart condition, stroke risk, and the severity of associated symptoms. A variety of treatments are available focused on the goals of resetting the rhythm to normal (for first time and more acute episodes) or controlling the ventricular rate (for more persistent and chronic conditions) and preventing blood clots from forming in the fibrillating atria through anticoagulation. Thus treatments may include antiarrhythmic medications, electrical cardioversion, catheter ablation, and a surgical maze procedure. Because atrial fibrillation increases the risk of development of blood clots in the atria, long-term anticoagulation is required for patients at increased risk for stroke.


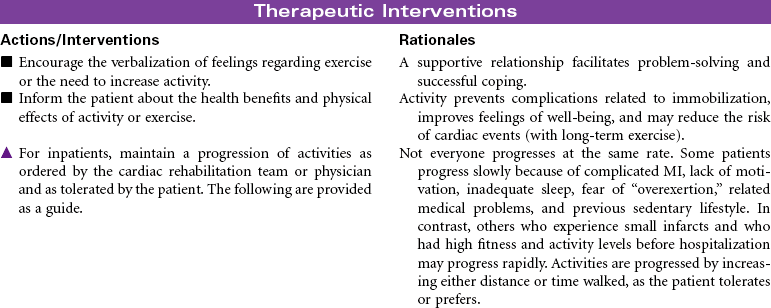
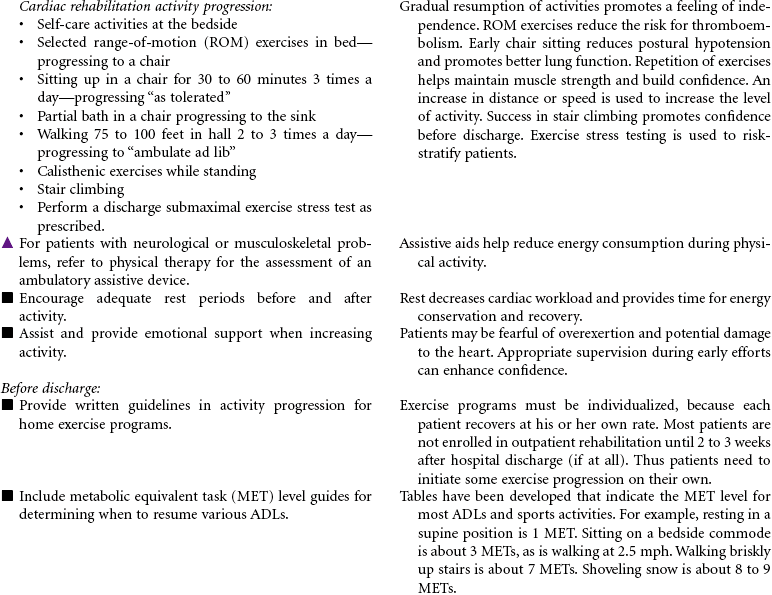
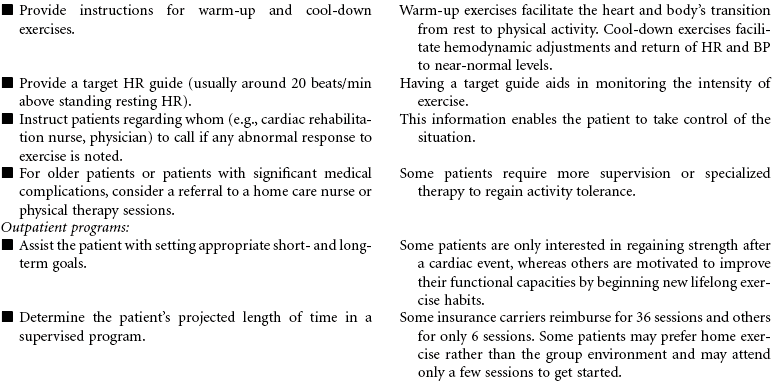
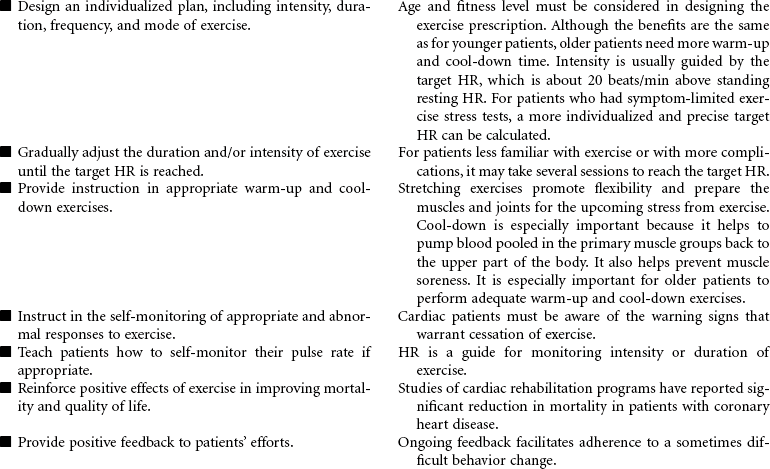
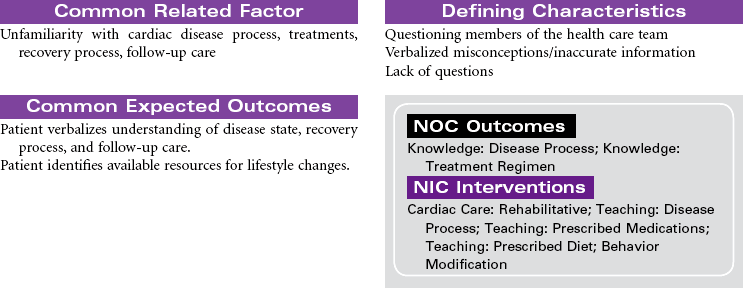
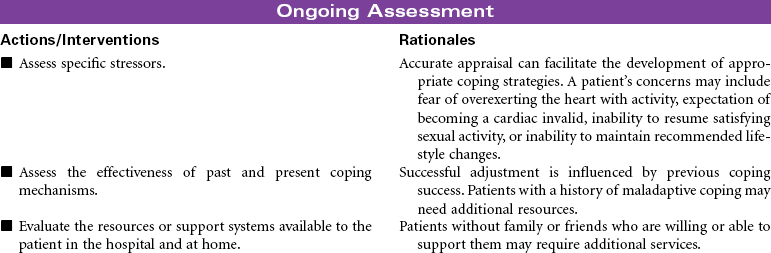
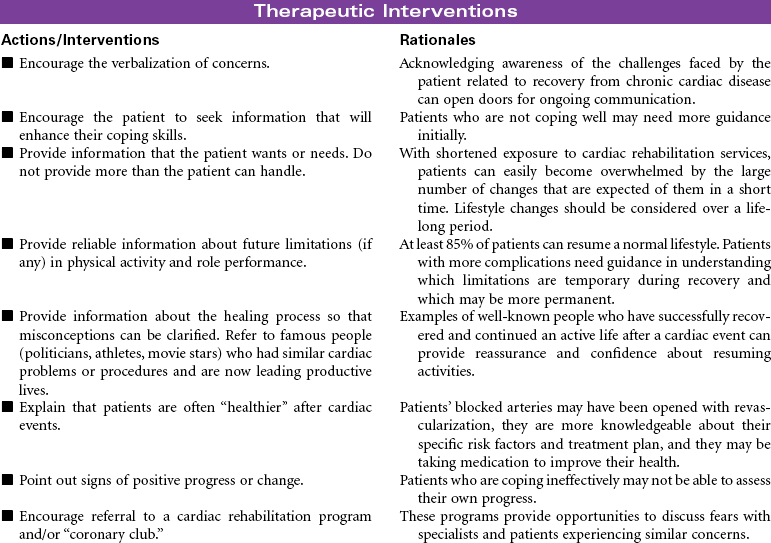
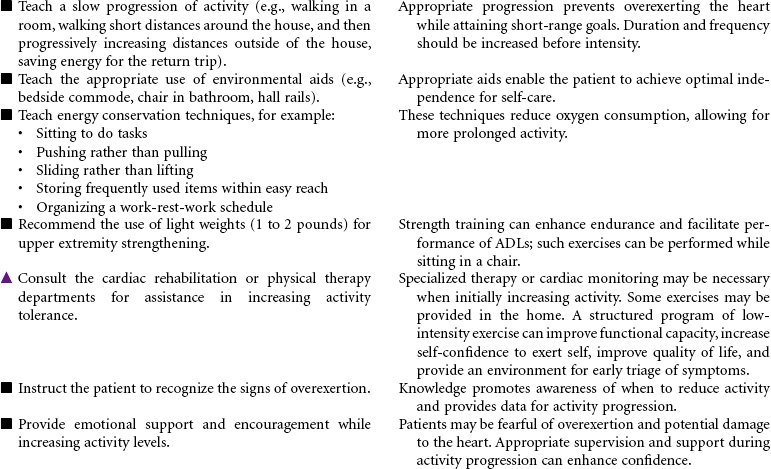
Cardiac Rehabilitation
Post–Myocardial Infarction; Post–Cardiac Surgery; Post–Percutaneous Transluminal Coronary Angioplasty; Chronic Heart Failure; Stable Angina; Activity Progression; Cardiac Education
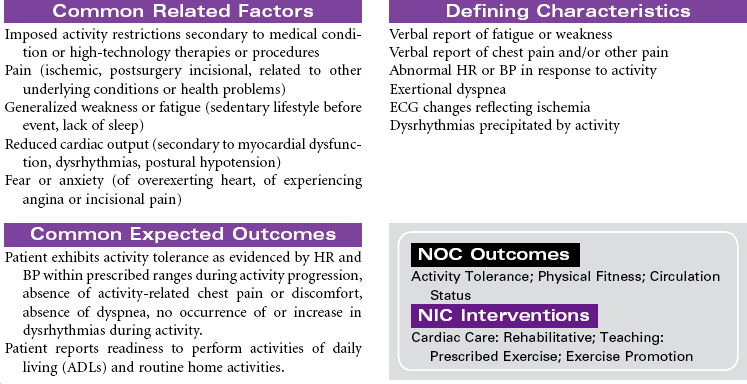
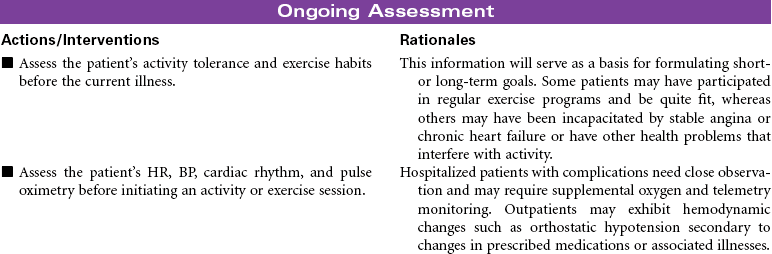
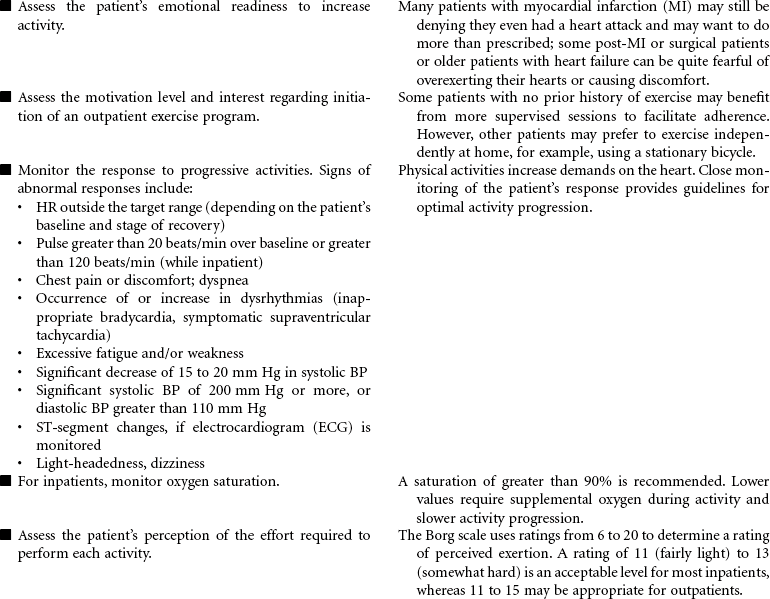
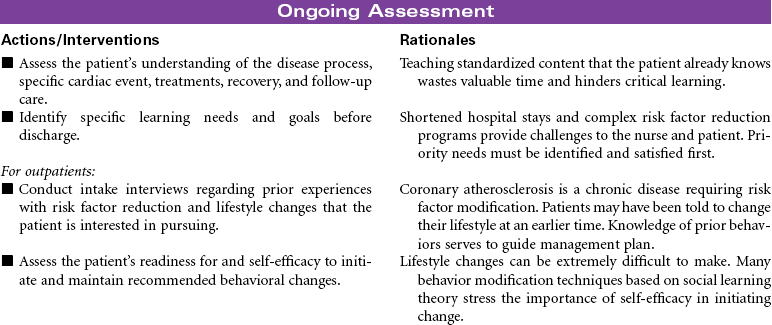
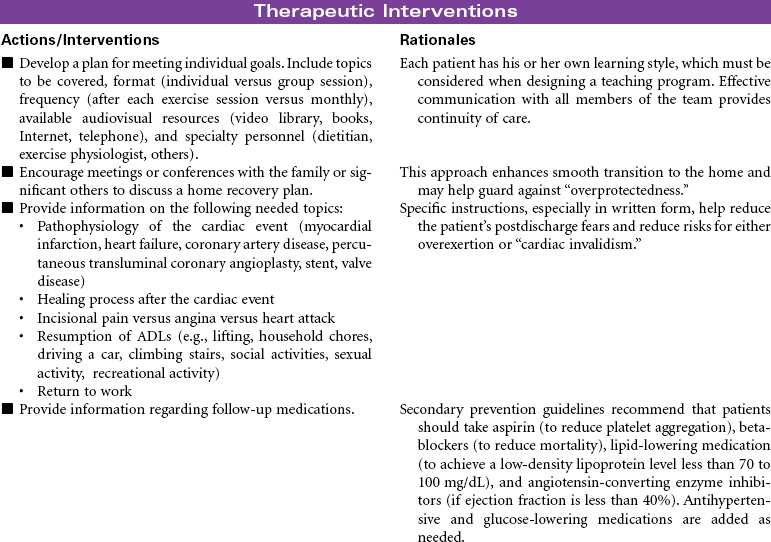
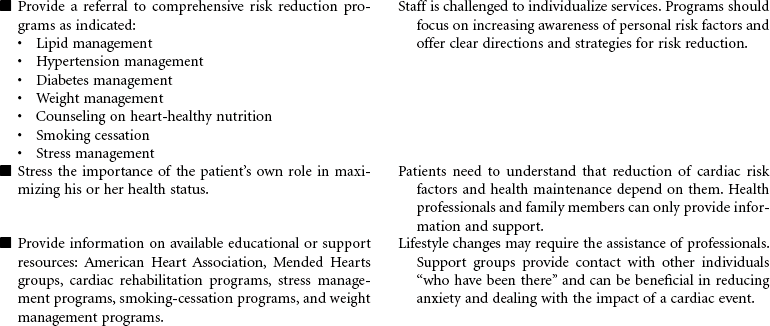
Cardiac rehabilitation is the process of actively assisting patients with known heart disease to achieve and maintain optimal physical and emotional health and wellness. It has undergone significant evolution, redesigning itself from a primarily exercise-focused intervention into a comprehensive disease management program. Core components of these programs include baseline and follow-up patient assessments; aggressive strategies for reducing modifiable risk factors for cardiovascular disease (CVD; e.g., dyslipidemia, hypertension, diabetes, obesity); counseling on heart-healthy nutrition, smoking cessation, and stress management; assistance in adhering to prescribed medications; promotion of lifestyle physical activity; exercise training; and psychosocial and vocational counseling. These integrated services are best provided by a multidisciplinary team composed of physicians, nurses, health educators, exercise physiologists, dietitians, and behavioral medicine specialists. More recently, the nurse has changed from team member to case manager. Cardiac rehabilitation programs typically begin in the hospital setting and progress to supervised (and often electrocardiogram [ECG]-monitored) outpatient programs. However, with shorter hospital stays, little time may be available for adequate instruction regarding lifestyle management and activity progression. Key to providing cost-effective care is an interdisciplinary team and the provision of interventions based on each patient’s unique needs, interests, and skills.
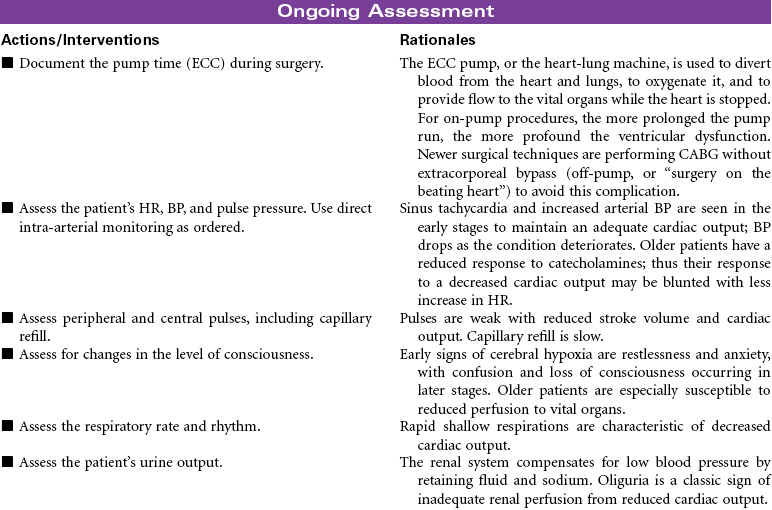
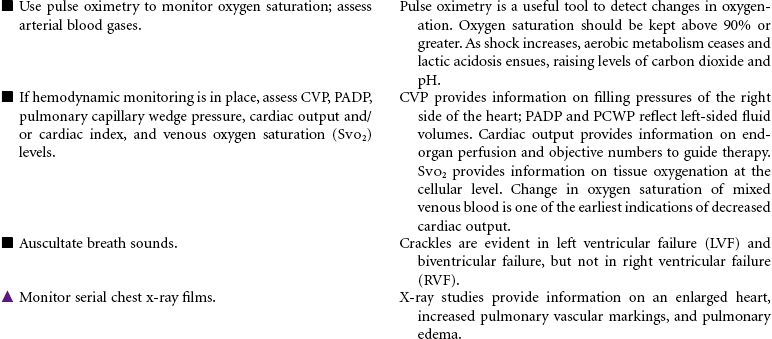
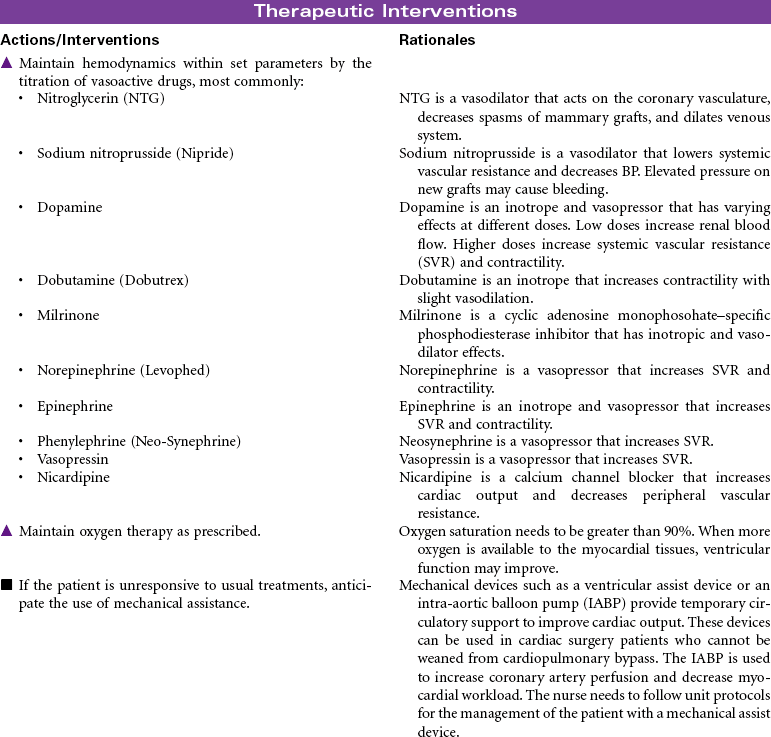
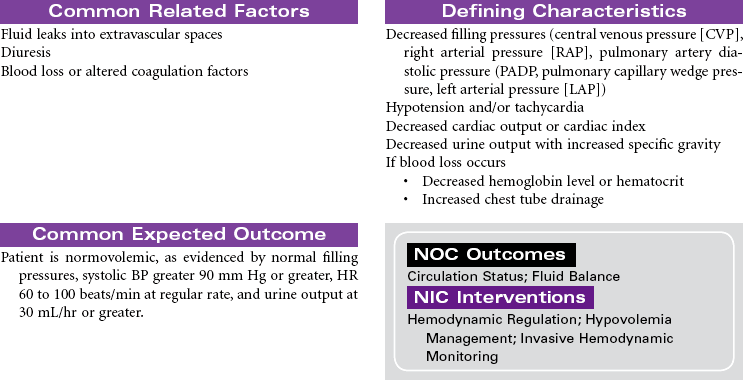
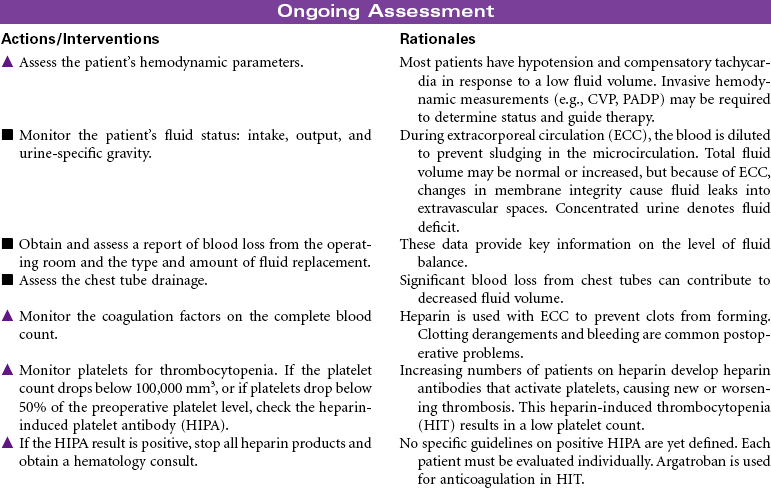
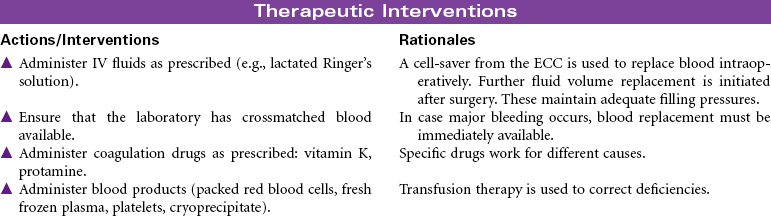
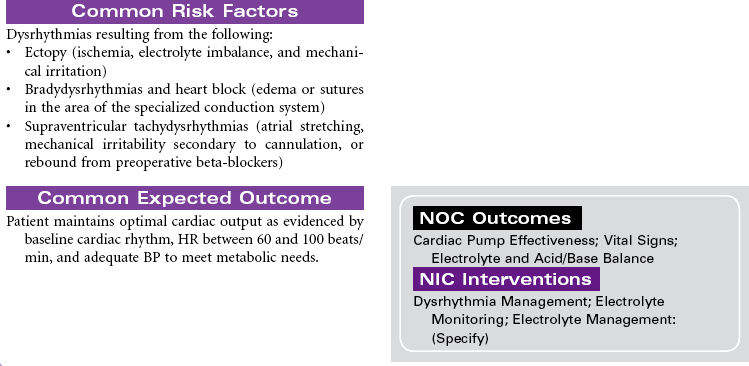
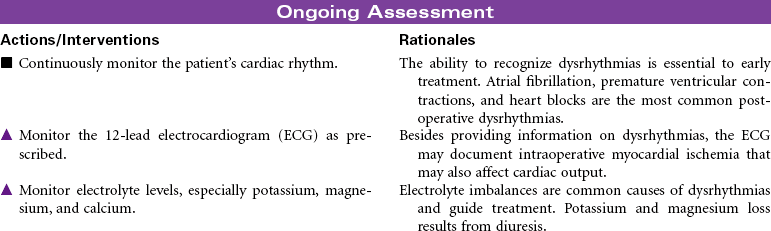
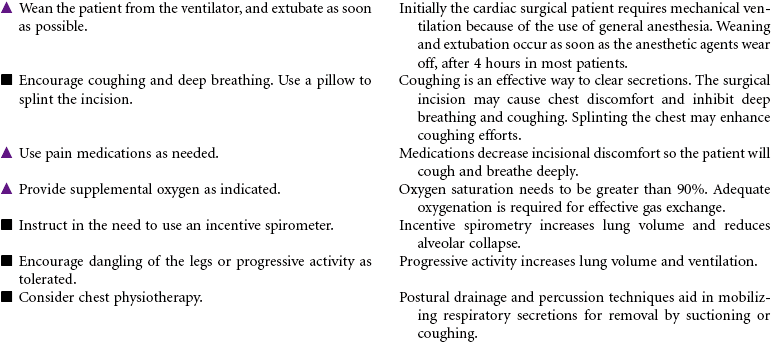
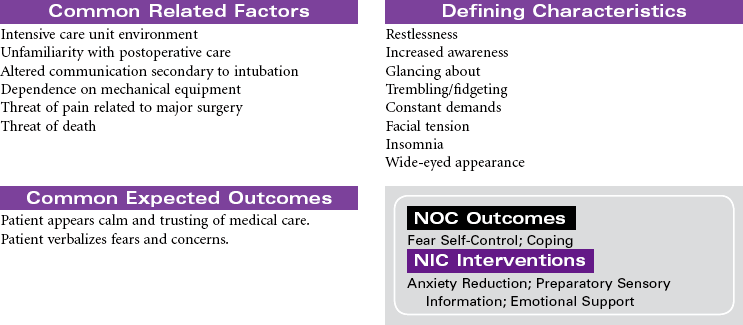
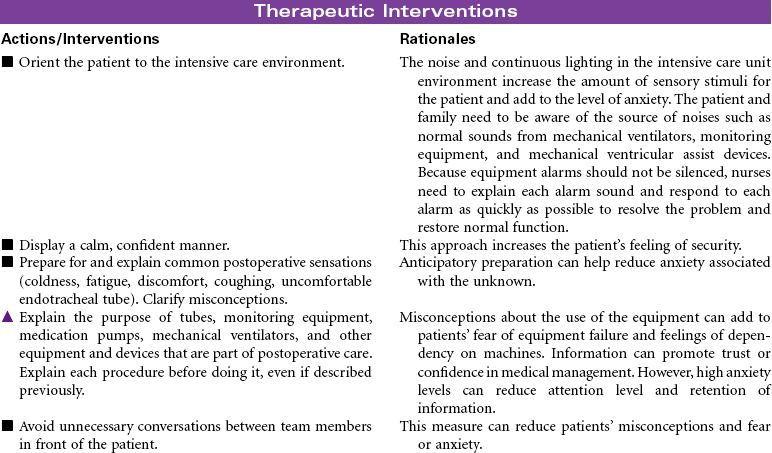
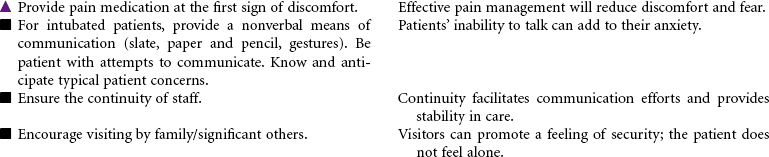
Coronary Bypass/Valve Surgery: Postoperative Care
Coronary Artery Bypass Graft (CABG); Valve Replacement; Minimally Invasive Surgery; Off-Pump CABG (OPCAB)
Coronary Bypass Surgery
The surgical approach to myocardial revascularization for coronary artery disease is bypass grafting. An artery from the chest wall (internal mammary) or a vein from the leg (saphenous) is used to supply blood distal to the area of stenosis. Internal mammary arteries have a higher patency rate. Today’s coronary artery bypass graft (CABG) patients are older (even octogenarians unresponsive to medical therapy or with failed coronary angioplasties or stents), have poorer left ventricular function, and may have undergone prior sternotomies. Older patients are at higher risk for complications and have a higher mortality rate. Women tend to have CABG surgery performed later in life. They have more complicated recovery courses than men because of the smaller diameter of women’s vessels and their associated comorbidity. Women have also been noted to have less favorable outcomes, with more recurrent angina and less return to work. Newer techniques for revascularization are available, such as transmyocardial revascularization with laser and video-assisted thoracoscopy. These techniques use limited incision and reduce the need for cardiopulmonary bypass and related perioperative complications. Surgical procedures for CABG without cardiopulmonary bypass or cardioplegia (off-pump) hold promise for reductions in postoperative morbidity.
Valve Replacement Surgery
Rheumatic fever, infection, calcification, or degeneration can cause the valve to become stenotic (incomplete opening) or regurgitant (incomplete closure), leading to valvular heart surgery. Whenever possible, the native valve is repaired. If the valve is beyond repair, it is replaced. Replacement valves can be tissue or mechanical. Tissue valves have a short life span; mechanical valves can last a lifetime but require long-term anticoagulation. Valve surgery involves intracardiac suture lines; therefore these patients are at high risk for conduction defects and postoperative bleeding. This care plan focuses only on acute care. See Cardiac Rehabilitation care plan presented earlier in this chapter for patient education information.
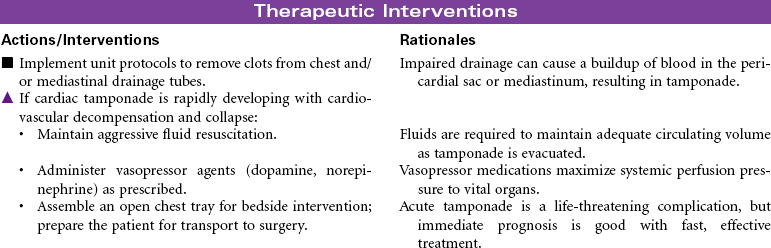
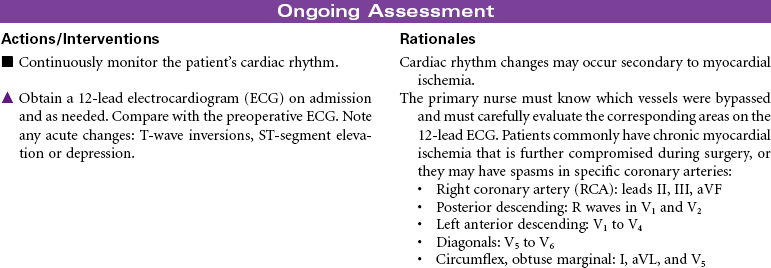
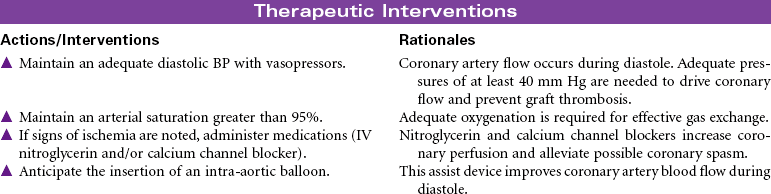
 Risk for Ineffective Myocardial Tissue Perfusion
Risk for Ineffective Myocardial Tissue Perfusion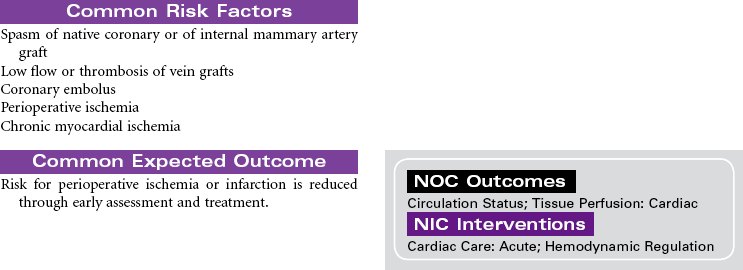




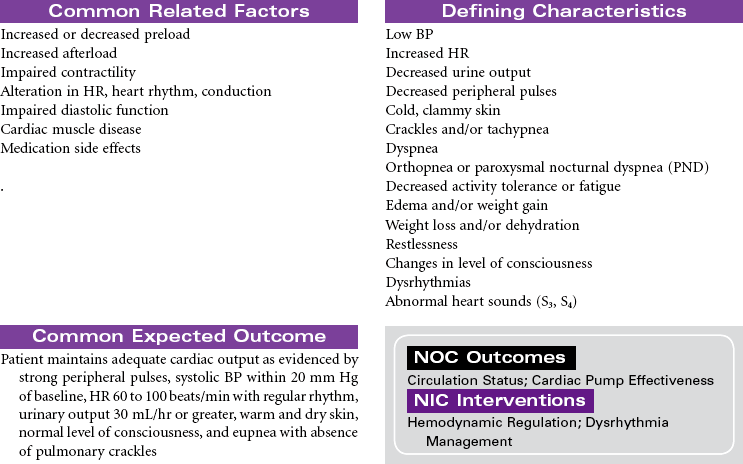
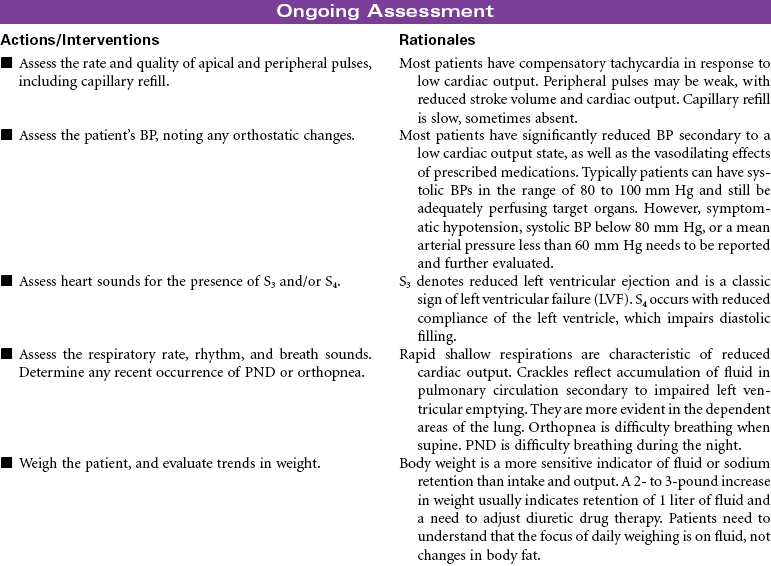
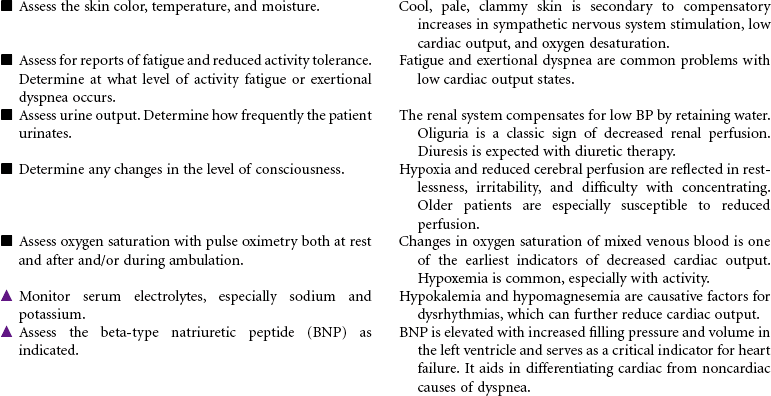
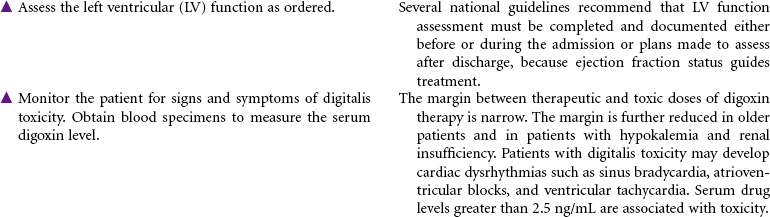
Heart Failure, Chronic
Congestive Heart Failure; Cardiomyopathy; Left-Sided Failure; Right-Sided Failure; Pump Failure; Systolic Dysfunction; Diastolic Dysfunction
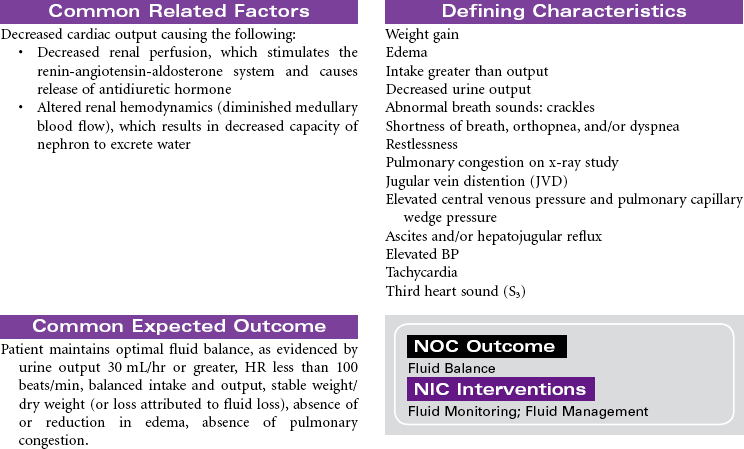
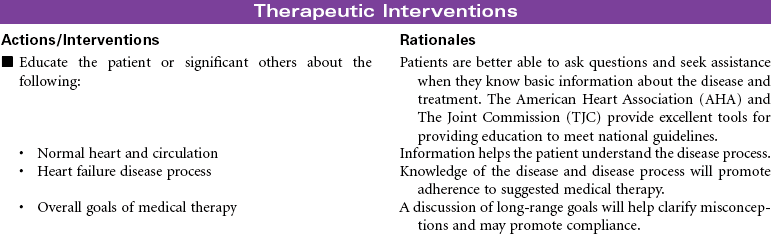
Heart failure is described as a common clinical syndrome resulting in the inability of the heart to meet the hemodynamic and metabolic demands of the body, producing a variety of biochemical and neurohormonal changes and manifesting in a variety of ways. With more than 5 million people in the United States having heart failure, it is a major health problem associated with high mortality rates, major morbidity, and rehospitalization. There is an increased prevalence with age, especially with women, making this a key geriatric concern. Heart failure remains one of the most disabling conditions, carrying a high economic burden related to the frequency of hospital readmissions.
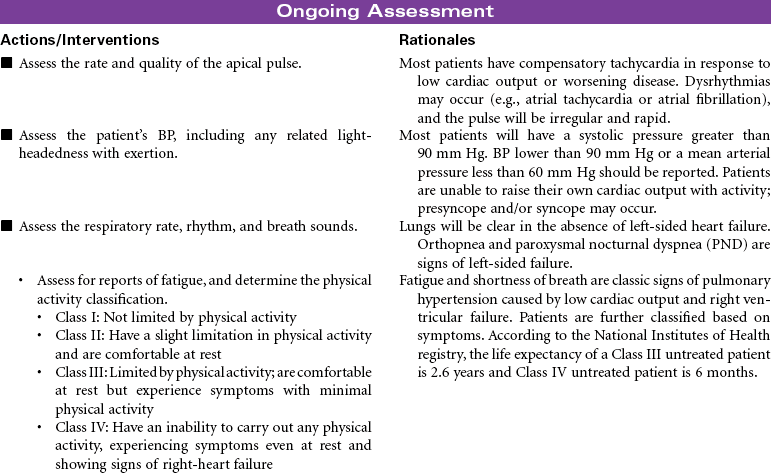
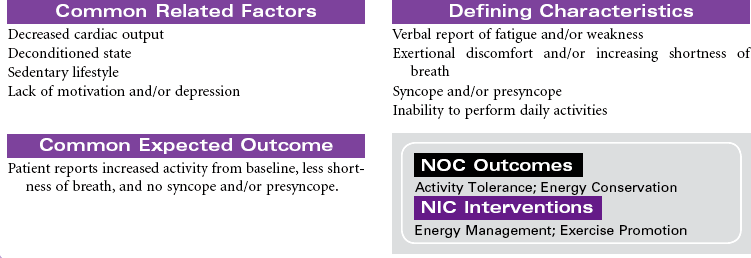
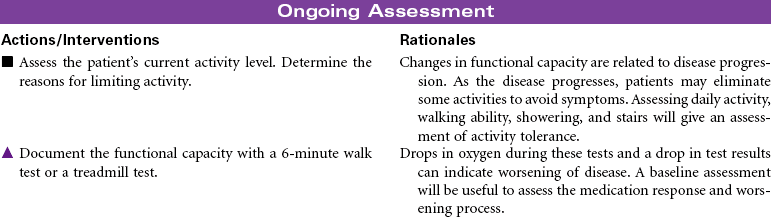
Heart failure is the final syndrome of a wide spectrum of endothelial and myocardial injuries that produce ventricular systolic dysfunction (poor pumping function) and/or diastolic dysfunction (poor relaxation and filling function). Hypertension and coronary artery disease are the most common contributing factors to heart failure, though the list of causative factors is quite extensive. These causes are often described as resulting from myocardial ischemia and chamber enlargement from a variety of causes, volume-related factors, pressure-loading conditions, and restrictive causes. Because of the health consequences of heart failure, attention is being directed to identifying and treating earlier those at risk for heart failure. A lettered classification system has been developed with characteristics defined for stages A, B, C, and D, with A being high risk but without structural problems or heart failure symptoms to D being refractory heart failure requiring specialized interventions. This somewhat parallels the classic New York Heart Association functional classification system based on severity of symptoms. Class I patients have no symptoms or physical limitations. Class II patients have slight limitations in their physical activity, whereby ordinary physical activities can cause symptoms such as fatigue, palpitations, dyspnea, or angina. Class III patients have marked physical limitations, with less than ordinary level of activities causing symptoms. Class IV patients experience dyspnea even at rest; activity is severely restricted.
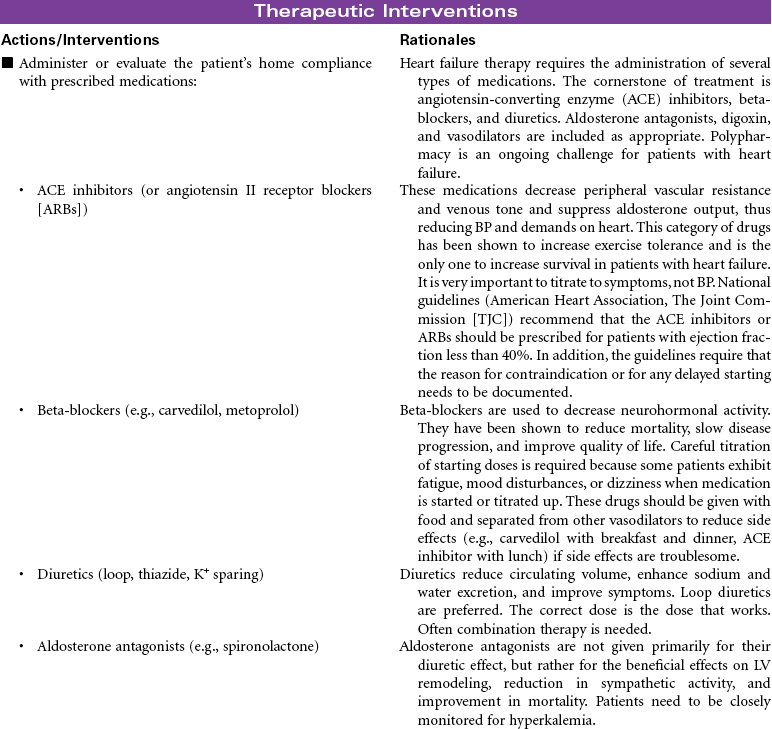
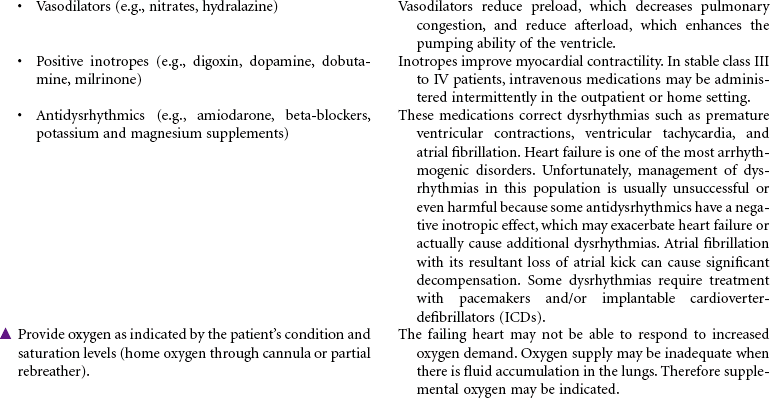
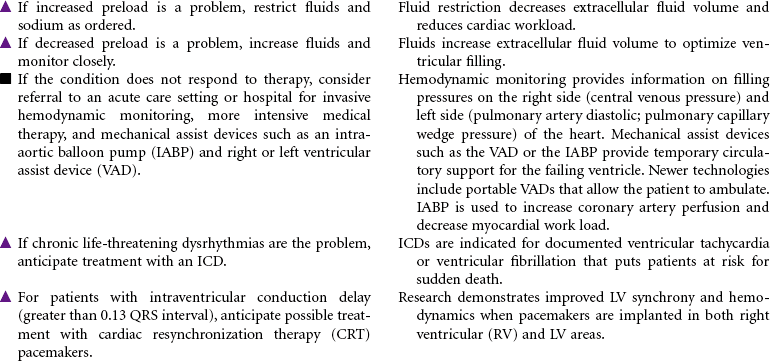
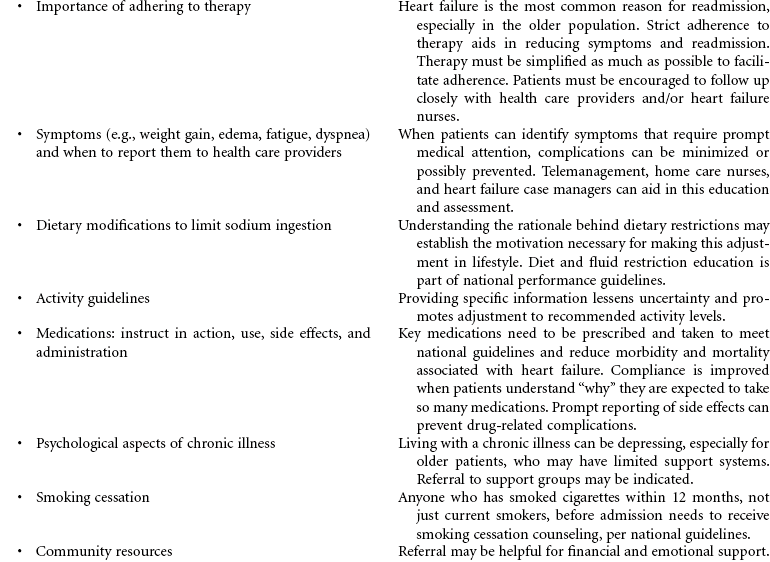
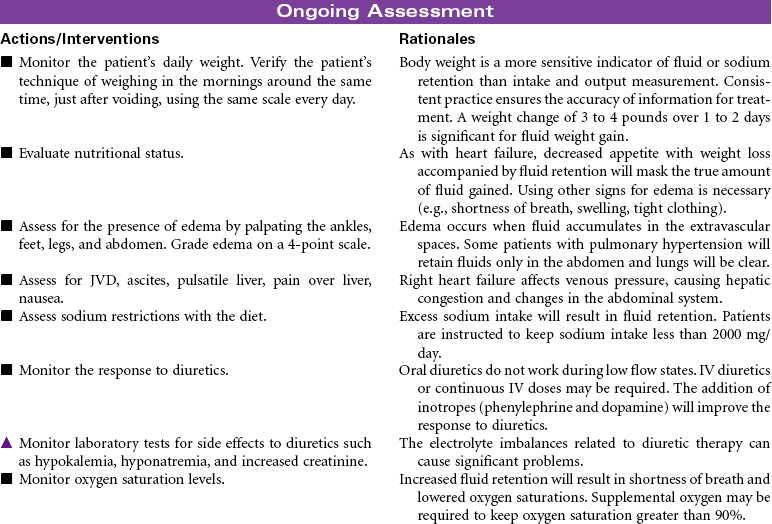
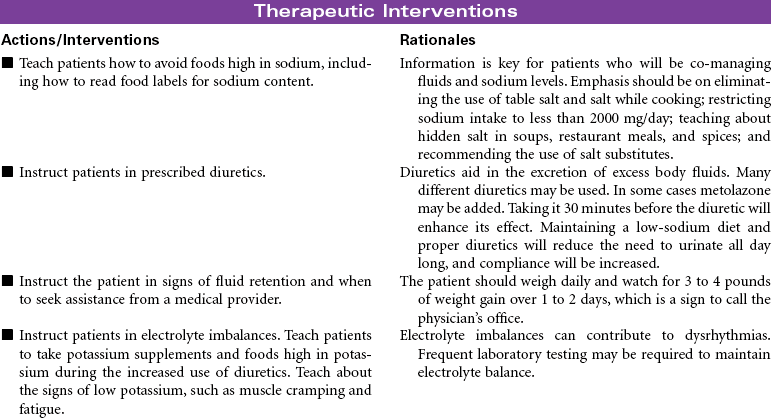
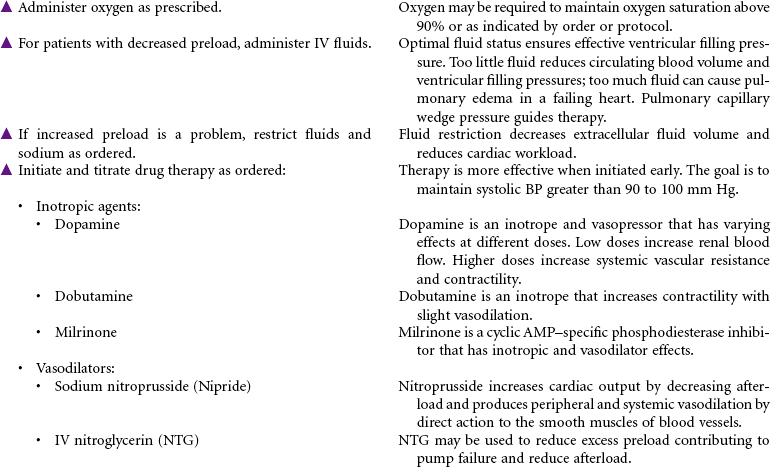
The goals of treatment are to prevent progression of heart failure, reduce exacerbations, recognize early signs of decompensation, control symptoms, assist patient in co-managing the disease, and improve quality of life. The basis of medical therapy is neurohormonal inhibition. Angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, beta-blockers (e.g., carvedilol), and aldosterone antagonists vasodilate, prevent decompensation, and reduce mortality. These drugs are used in combination with diuretics that reduce fluid overload. Digoxin is sometimes used in appropriate patients but does not reduce mortality. As patients deteriorate and experience acute decompensation, additional therapies of IV vasodilators and inotropes are indicated. Additional device therapies are available for patients with more complicated conditions. These include ultrafiltration to remove excess fluids and sodium, cardiac resynchronization therapy pacemakers to optimize cardiac output, implantable defibrillators to reduce risk for sudden cardiac death, and ventricular assist devices to extend life.
Innovative programs such as cardiac case-managed home care, community-based heart failure case management, telemanagement, and heart failure cardiac rehabilitation programs are being developed to reduce the need for acute care or hospital services for this growing population. Because the goal of therapy is to manage patients outside the hospital, this care plan focuses on treatment in an ambulatory setting for patients with heart failure symptoms (Stage C, Functional Class II-III). Note: Several national organizations have performance outcome goals related to heart failure: the American Heart Association’s Get With the Guidelines—Heart Failure initiative and The Joint Commission’s National Patient Safety Goals and National Quality Improvement Goals.
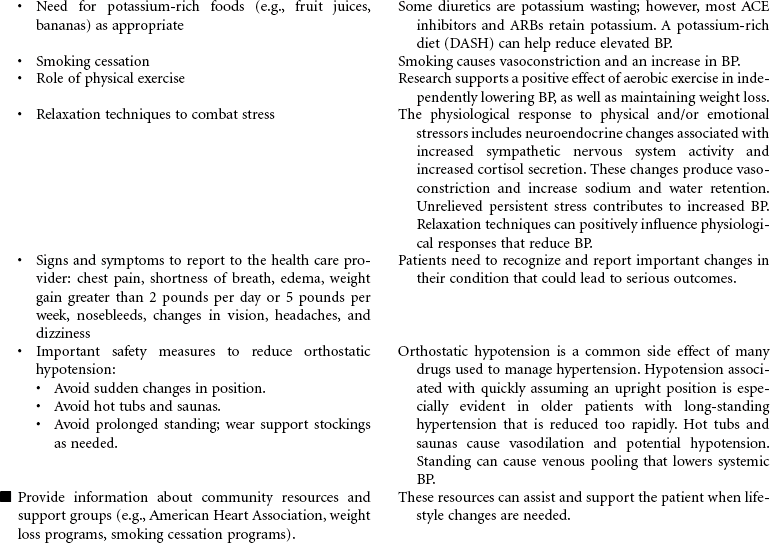
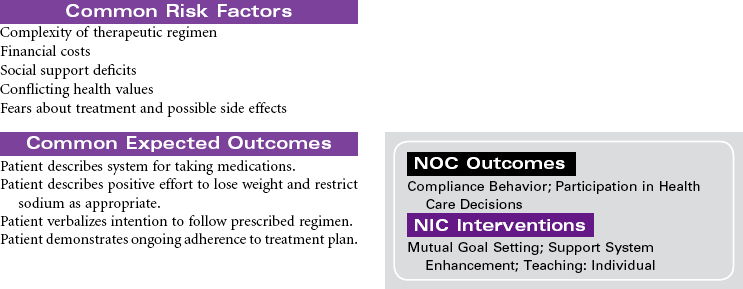
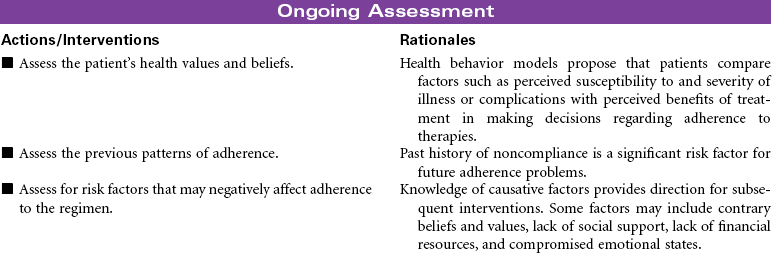
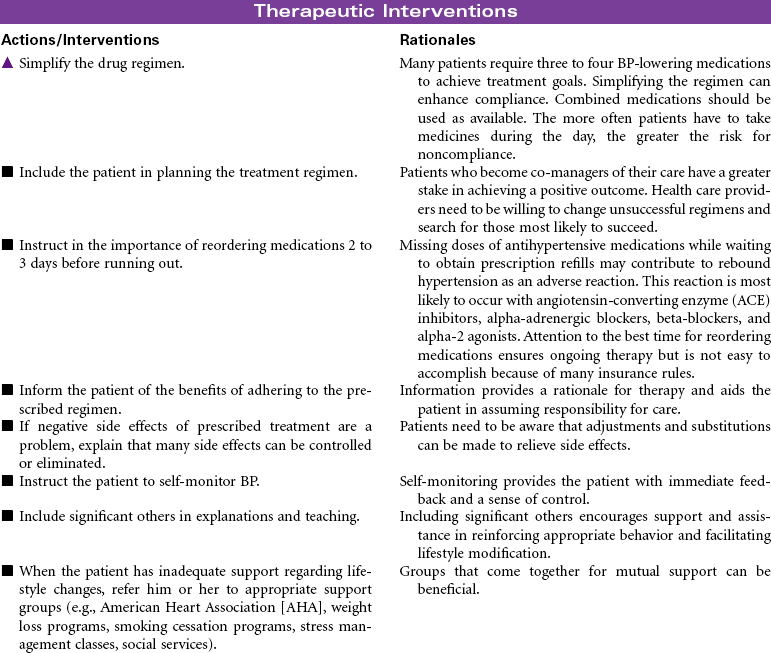
Hypertension
High Blood Pressure; Isolated Systolic Hypertension
High BP is classified according to the level of severity. The following table is from the Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC).

Epidemiological studies report that 1 in 3 U.S. adults have hypertension, with 65 million people in the United States having BPs 140/90 mm Hg or higher or taking antihypertensive medications. Age, gender, and ethnic differences are evident. African Americans in the United States develop hypertension earlier, have more significantly elevated BP, and have more target organ disease than Caucasians. Likewise, African American women have a higher incidence of hypertension than white women.
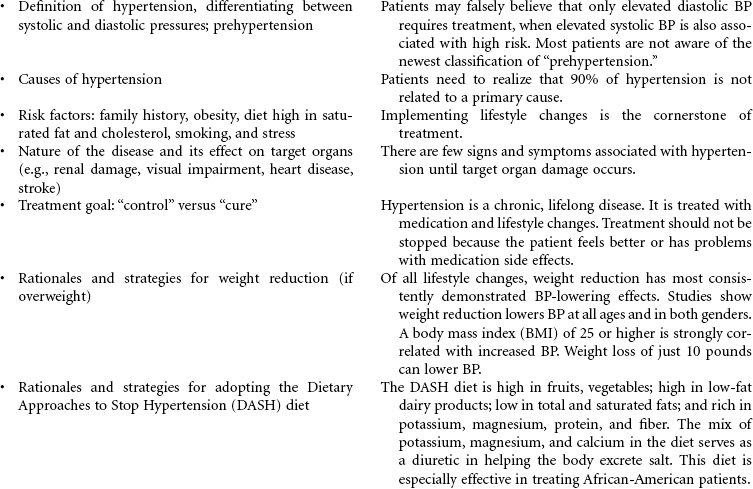
Although hypertension can be initiated in childhood, it is most evident in middle life. As the population ages, the prevalence of hypertension will increase unless effective prevention measures are implemented. The category of prehypertension identifies a significant segment of the population who are at twice the risk for developing hypertension than people in the normal category. Preventive efforts in this population are aimed at reducing risk factors through therapeutic lifestyle changes, which are detailed in the JNC guidelines.
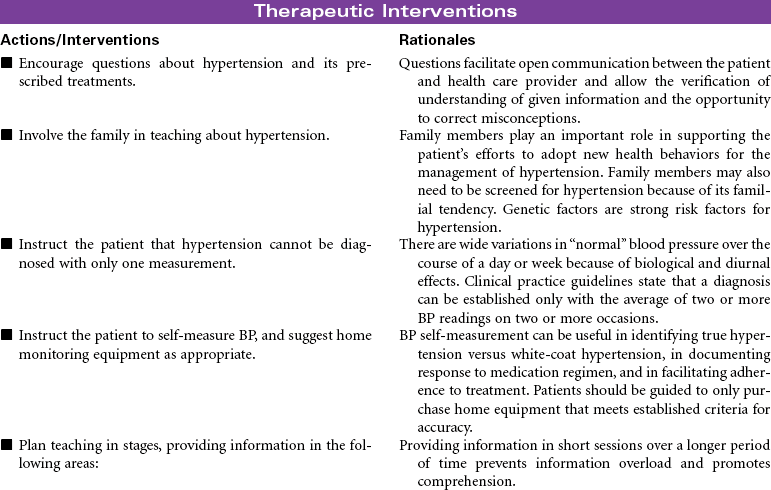
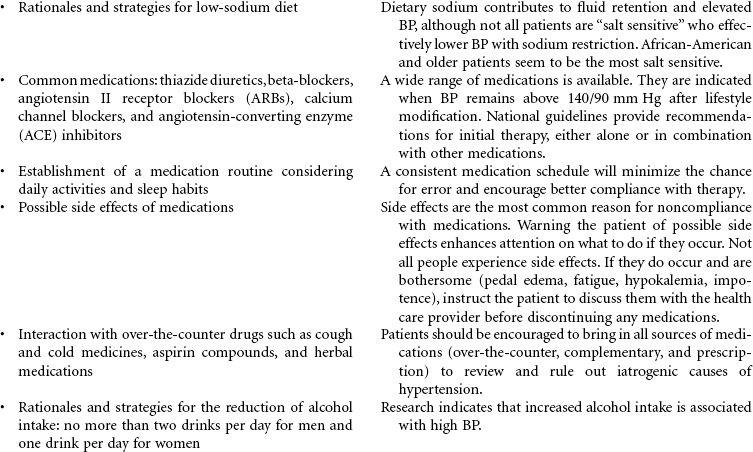
Blood pressure self-management is key to successful treatment. Ambulatory BP monitoring may be indicated to document changes in BP throughout the day (circadian pattern) and provide information for treating drug-resistant patients and those experiencing hypotension secondary to medication. Several classes of drugs are available for treatment. Usually two or more antihypertensive medications are needed to achieve optimal BP control. This care plan focuses on patients with hypertension in an ambulatory care setting.



Percutaneous Coronary Intervention: Percutaneous Transluminal Coronary Angioplasty, Atherectomy, Stents
Intracoronary Stenting; Drug-Eluting Stents; Directional Atherectomy (DCA); Intracoronary Radiation; Brachytherapy
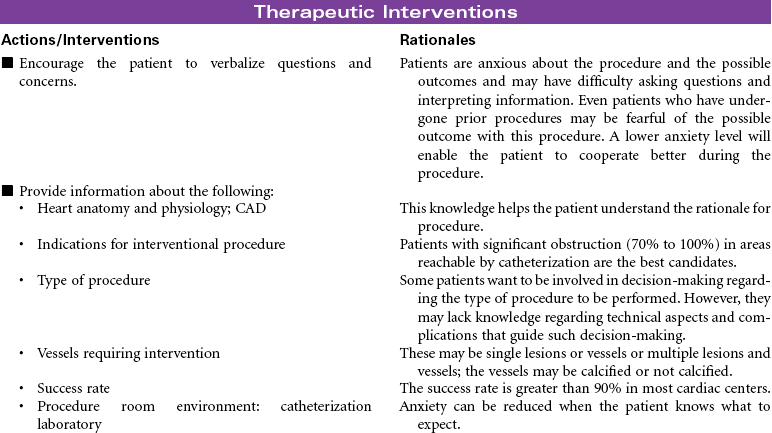
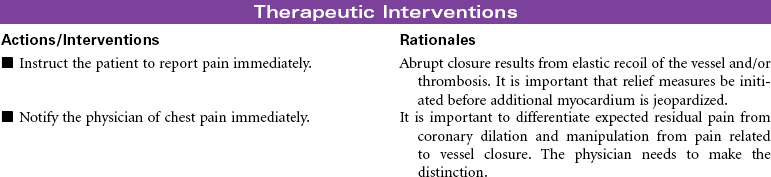
These interventions provide a means to nonsurgically improve coronary blood flow and revascularize the myocardium. A variety of procedures have been developed, although percutaneous transluminal coronary angioplasty (PTCA) remains the mainstay. Unfortunately, restenosis remains a critical problem with all techniques. Interventional procedures may be performed in combination with the diagnostic coronary angiogram, electively after diagnostic evaluation, or urgently if there is suspicion of coronary artery blockage in the setting of unstable angina or acute myocardial infarction (MI).
PTCA: This procedure uses a balloon-tipped catheter that is positioned at the site of the lesion. Multiple balloon inflations are performed until the artery is satisfactorily dilated to restore blood flow. The number of PTCA procedures performed annually continues to rise, especially among the older population, particularly older women, because of the risks associated with coronary artery bypass graft surgery for these patients.
Coronary Atherectomy: This term refers to removal of plaque material by excision. It may be performed in conjunction with PTCA or stenting and continues to be applied to a wider patient domain that includes patients with multivessel disease and complex coronary anatomy. Atherectomy may be more effective than PTCA for more calcified lesions. Two types of devices have been developed:
1. Directional: Has a rotating cutter blade that shaves the plaque. The tissue obtained is collected in a cone for removal. It is indicated for lesions with calcification or thrombus and for those at the ostium of a vessel.
2. Rotational: Uses a burr at the tip of the catheter, which rotates at high speeds to grind up hard plaque. The removed pulverized microparticles are released into the distal circulation rather than collected as in directional atherectomy.
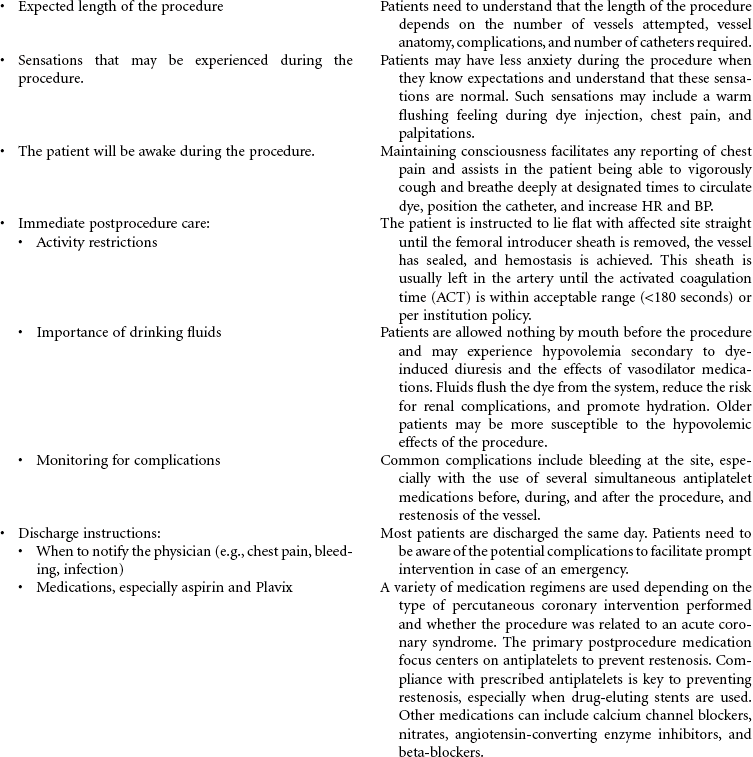
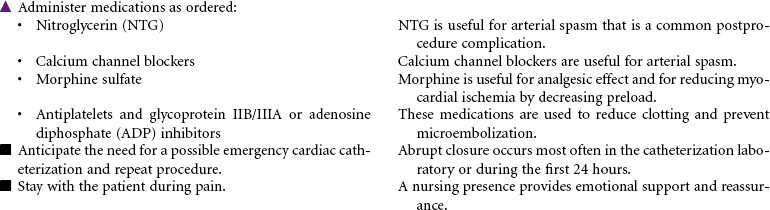
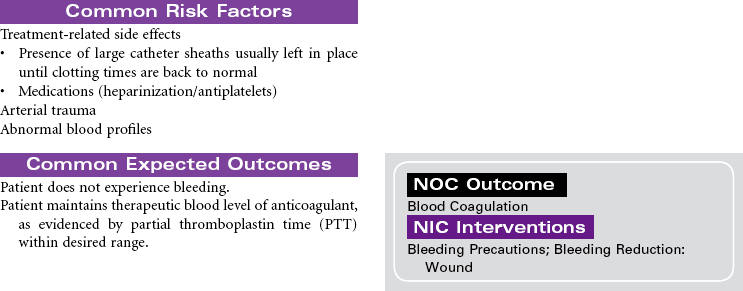
Intracoronary Stents: These metallic coils are inserted after balloon dilation or atherectomy, or they are used alone, to provide structural support (“internal scaffolding”) to the vessel. The stent remains in place as the catheter is removed. Because of the thrombogenic nature of the stent, anticoagulation and antiplatelet therapy are indicated for an indefinite period. These stents have reduced restenosis rates significantly. The newest models are “drug-eluding” stents that have an imbedded amount of medication, sometimes in a thin polymer for timed release, that inhibits new cell and tissue growth and prevents neointimal hyperplasia and restenosis. They have reduced typical restenosis rates to single digits. Additional antiplatelet therapy is needed for a year or more.
Brachytherapy: This technique uses intracoronary radiation to treat in-stent stenosis. It uses either gamma or beta radiation isotopes. The use of drug-eluting stents has reduced the need for this therapy.
Coronary Laser Angioplasty: This technique uses laser energy to treat in-stent stenosis.

Peripheral Arterial Revascularization
Femoral Popliteal Bypass; Percutaneous Transluminal Angioplasty (PTA)
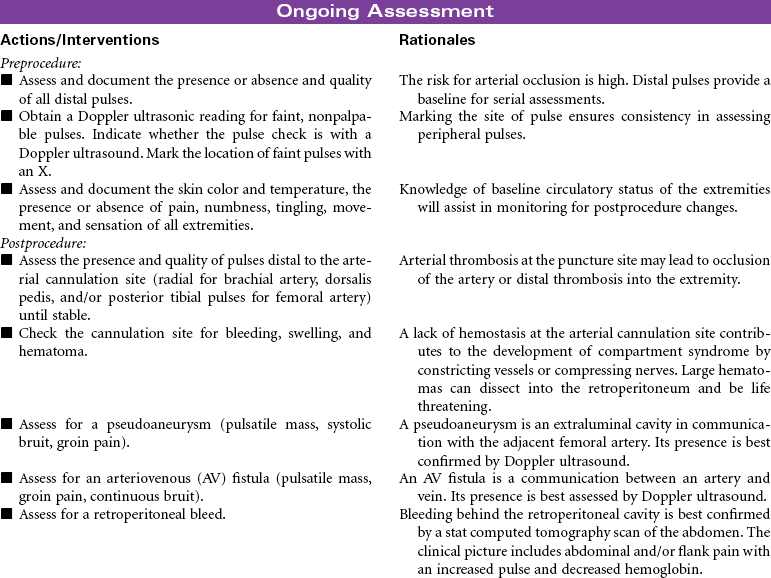
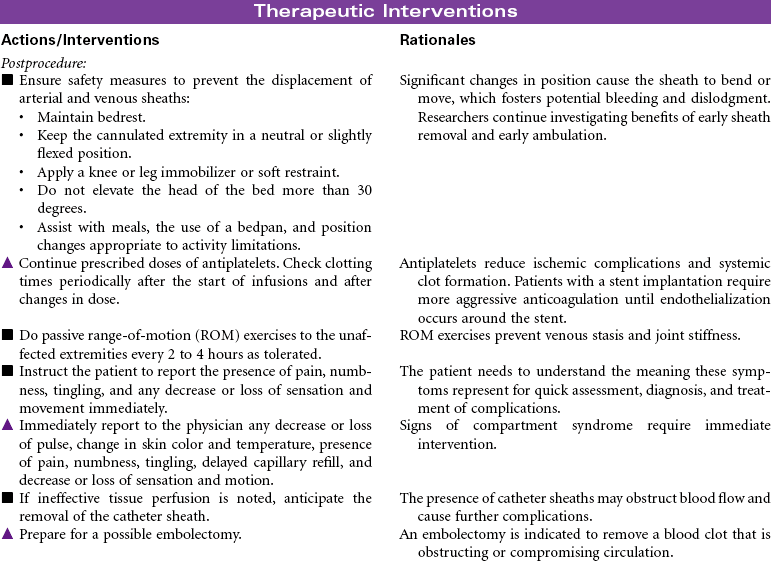
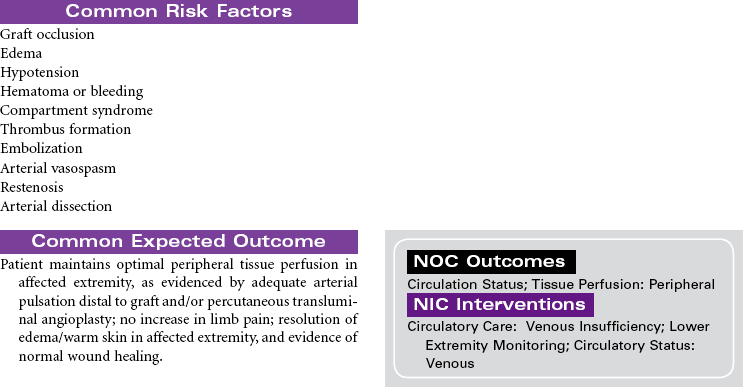
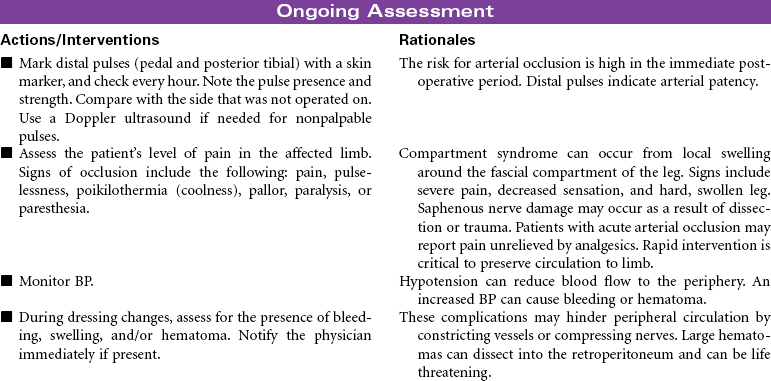
Chronic peripheral arterial occlusive disease (PAD) is most commonly caused by atherosclerosis resulting in reduced arterial blood flow to peripheral tissues. Complications associated with arterial insufficiency include pain in the leg(s), ulcers or wounds that do not heal, and progressive amputation of the affected extremity. Revascularization is indicated when medical management is ineffective. Revascularization procedures are available to treat PAD of the femoral arteries with the goals of improving tissue perfusion, preventing tissue necrosis, reducing pain, and limb salvage. This care plan focuses on preoperative teaching and postprocedure care.
Femoral Popliteal Bypass Surgery: This procedure involves a surgical opening of the upper leg to directly visualize the femoral artery. It is performed to bypass the occluded arterial segment in the femoral artery using another blood vessel such as the saphenous vein or a synthetic material such as Dacron or Gore-Tex that is attached to the popliteal artery either above or below the knee. This allows rerouting the blood flow around the obstruction to optimize peripheral circulation. The distal vessel must be at least 50% patent for the grafts to remain patent. Additional locations along the arterial system can be bypassed. An aortoiliac endarterectomy can also be performed whereby the atheromatous plaque is removed and the vessel is sutured to restore circulation.
Percutaneous transluminal angioplasty (PTA): This minimally invasive endovascular procedure uses balloon-tipped catheters that are positioned at the site of the lesion or blockage. Multiple balloon inflations are performed until the atherosclerotic plaque is compressed and the artery is satisfactorily dilated. A stent (tiny, expandable metal coil) may be inserted into the newly opened area to provide structural support to the vessel. The stent remains in place as the deflated balloon catheter is removed. These stents can reduce restenosis rates.




Peripheral Arterial Occlusive Disease, Chronic
Intermittent Claudication; Arterial Insufficiency; Arteriosclerosis Obliterans; Percutaneous Transluminal Angioplasty (PTA)
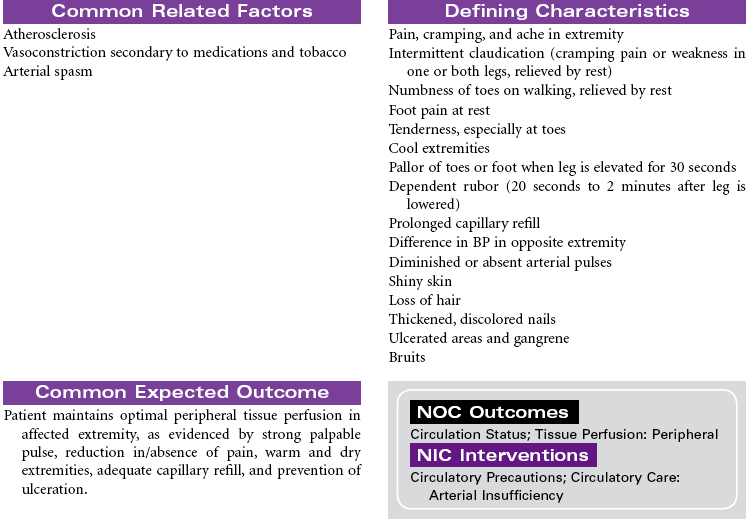
Chronic peripheral arterial occlusive disease is most commonly caused by atherosclerosis resulting in reduced arterial blood flow to peripheral tissues, causing decreased nutrition and oxygenation at the cellular level. It can be characterized by four stages: asymptomatic, claudication, rest pain, and necrosis. Management is directed at removing vasoconstricting factors, improving peripheral blood flow, and reducing metabolic demands on the body. Because atherosclerosis is a progressive disease, older patients experience an increased incidence of this disease. Diabetes mellitus and tobacco use are significant risk factors in the development of chronic arterial insufficiency. Complications associated with arterial insufficiency include necrotic skin ulcers and progressive amputation of the affected extremity. Peripheral arterial disease is a major cause of disability, significantly affecting quality of life. It is also a significant predictor of future cardiac and cerebrovascular events and is considered a cardiovascular disease risk equivalent.


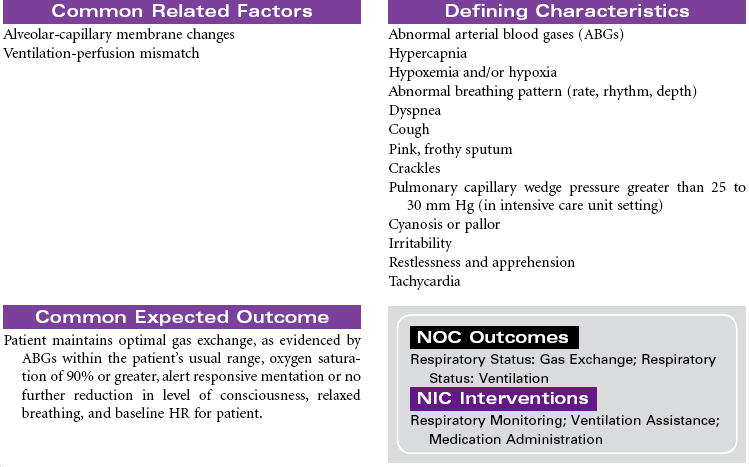
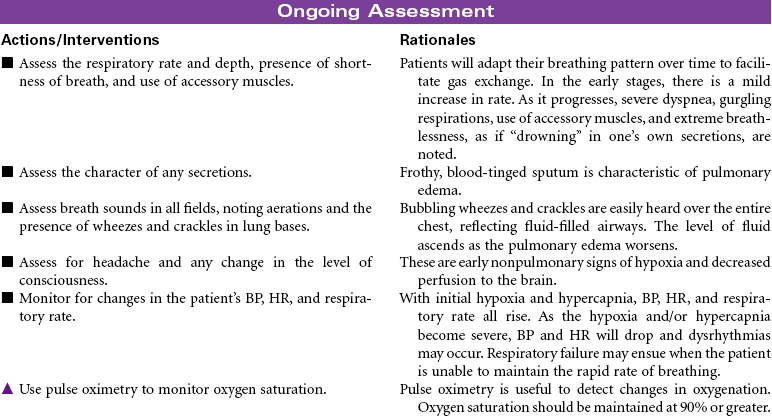
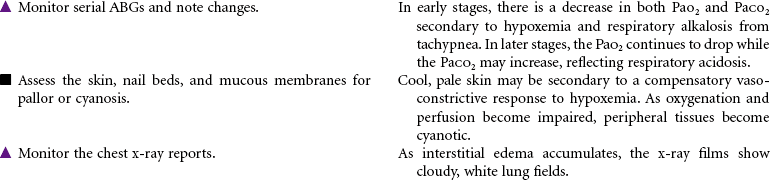
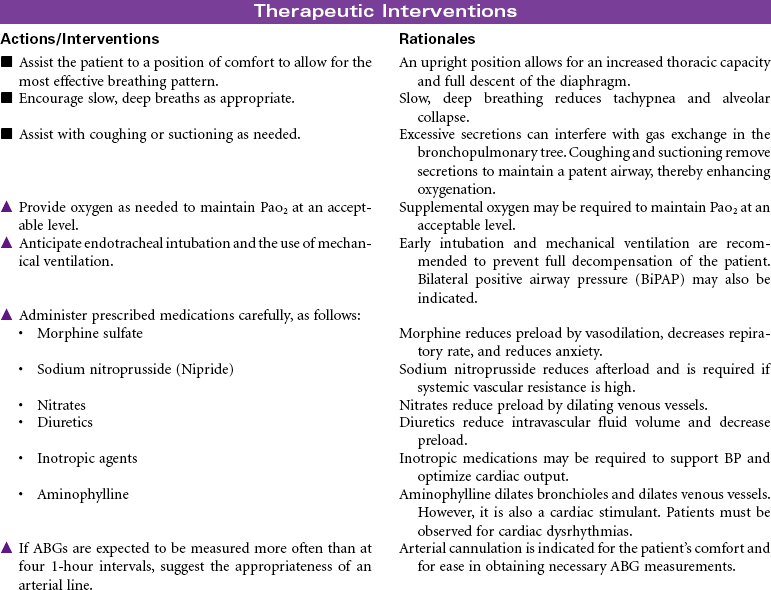
Pulmonary Edema, Acute
Pulmonary Congestion; Cardiogenic Pulmonary Edema; Acute Heart Failure
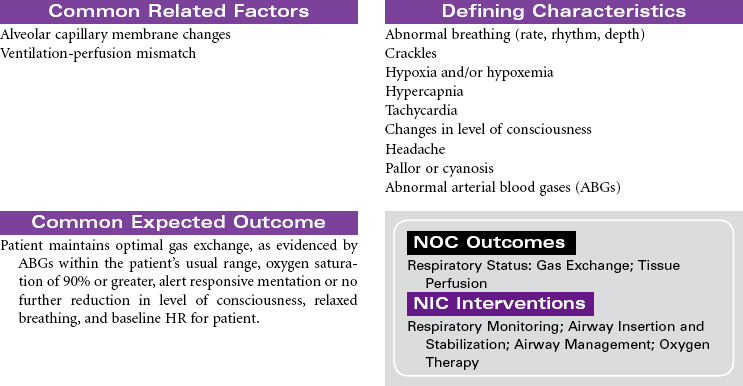
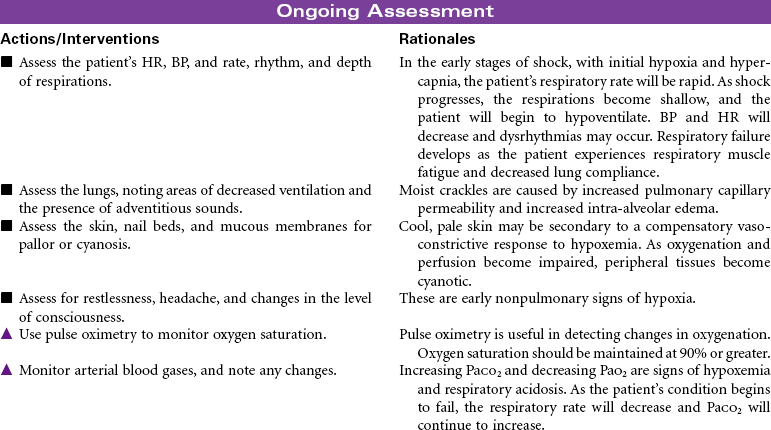
Pulmonary edema is a pathological state in which there is an abnormal and/or excessive, diffuse accumulation of fluid in the alveoli and interstitial spaces of the lung. This fluid causes impaired gas exchange by interfering with diffusion between the pulmonary capillaries and the alveoli. It is commonly caused by left ventricular failure, altered capillary permeability of the lungs, acute respiratory distress syndrome, neoplasms, overhydration, and hypoalbuminemia. Acute pulmonary edema is considered a medical emergency.
Pulmonary Arterial Hypertension
Right Ventricular Dilation, Right Atrial Dilation; Right-Sided Failure
The World Health Organization classified pulmonary hypertension into five categories as discussed below. Distinguishing the group is important, because treatment is different for each.
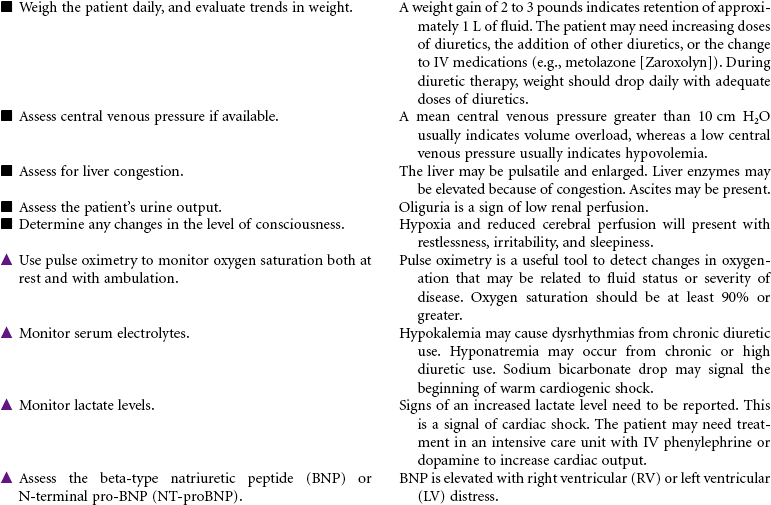
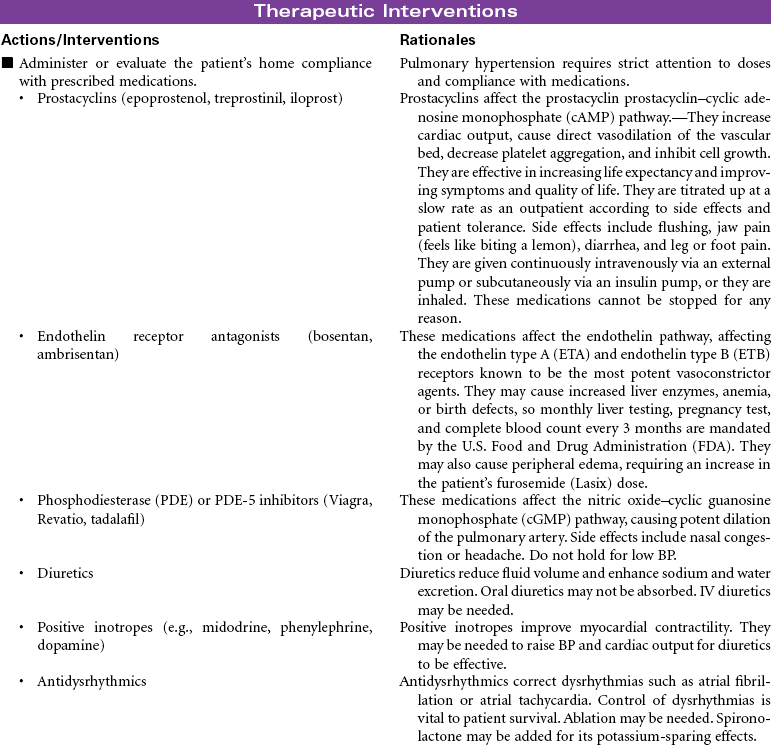
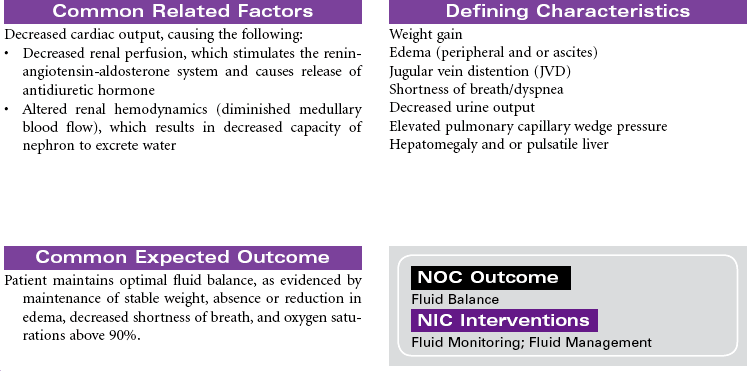
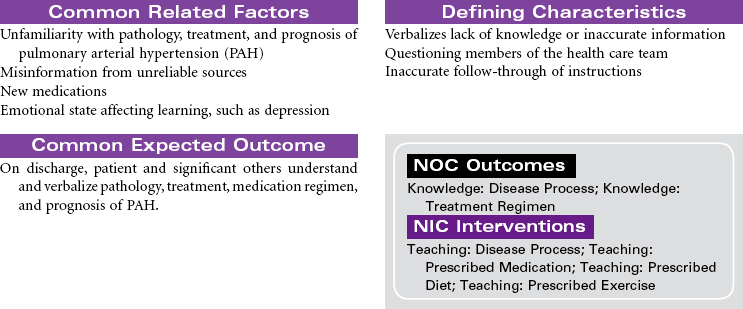
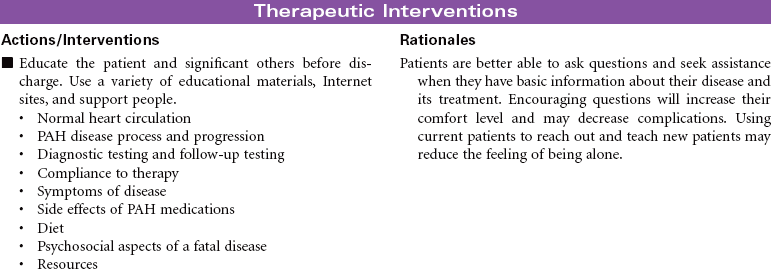
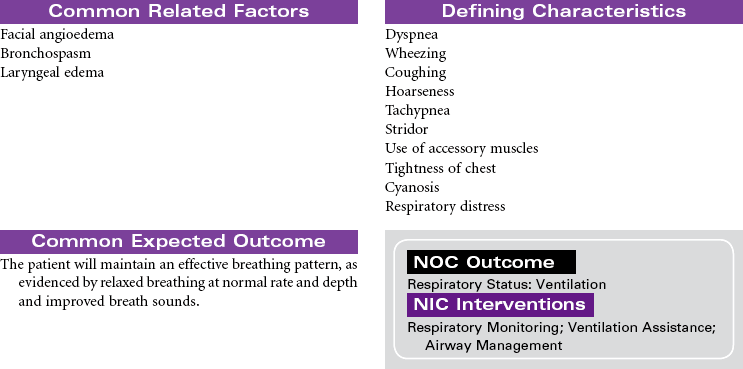
Group 1 pulmonary arterial hypertension (PAH) is the inability of the right ventricle to pump adequate blood into the lungs for oxygenation. PAH is characterized by progressive elevation of the pulmonary artery pressure and vascular resistance. Injury to the vascular bed impairs the function in the endothelium, vascular smooth muscle, and potassium channel, causing vasoconstriction. As the disease progresses, plexiform lesions, in situ thrombosis, and cell proliferation result in irreversible disease. Patients are limited by shortness of breath, dyspnea on exertion, presyncope and/or syncope, chest pain, edema, and ascites. PAH often leads to right ventricular failure and death. The cause is broken down into two categories: idiopathic (primary) pulmonary hypertension, either sporadic or familial, and secondary PAH, which is related to collagen-vascular disease, congenital systemic-to-pulmonary shunts, portal hypertension, human immunodeficiency virus (HIV) infection, appetite supressants, and persistent pulmonary hypertension of the newborn. Diagnosis is made by an echocardiogram, electrocardiogram (ECG), physical examination, and heart catheterization. The right heart pressures during heart catheterization will show a mean pulmonary artery pressure of greater than 25 mm Hg at rest and greater than 35 mm Hg with exercise, with a normal wedge pressure. The echocardiogram will show a dilated right ventricle and right atrium with a normal left ventricular function and size; the left ventricle will, however, be underfilled. Right axis deviation and right ventricular hypertrophy will be documented on ECG. On physical examination, jugular venous distention, reduced carotid volume, right ventricular heave, right-sided fourth heart sound, loud pulmonic valve closure (P2), and tricuspid regurgitation murmur will be present. Peripheral edema and/or ascites may be present. Treatment goals are to increase cardiac output, dilate the pulmonary artery, decrease complications, manage symptoms, recognize early signs of right ventricular failure, reduce hospitalizations through teaching, increase life expectancy, and improve quality of life. The basis of current treatment is to affect one or more of the three molecular vascular pathways (prostacyclin–cyclic adenosine monophosphate [cAMP] pathway, the nitric oxide–cyclic guanosine monophosphate [cGMP] pathway, or the endothelin pathway) by medications that reduce vessel tone and inhibit proliferation of cells. Additional medications are prescribed in conjunction with the PAH medications to decrease symptoms, reduce side effects, and improve quality of life. In a very select few patients with advanced PAH, atrial septostomy may result in significant improvement in symptoms. The shunt created in this procedure may decompress the heart and alleviate right ventricular failure. Long-term survival after atrial septostomy has not been determined. Some pulmonary hypertension centers may use it as a bridge to lung transplant. Lung transplantation is considered based on the patient’s stage of PAH, comorbidities, and underlying disease. To qualify, there must be symptomatic progression of disease despite optimal treatment with a prostacyclin, cardiac index less than 2 L/min/m2, right atrial pressure greater than 15 mm Hg, and a mean pulmonary pressure greater than 55 mm Hg. The lung allocation score is calculated using the waiting-list urgency measure and post-transplant survival measure. Survival for patients with PAH at 1, 3, and 5 years is reported as 75%, 60%, and 48%, respectively. Right ventricular function and size has been shown to return to normal by 3 months after lung transplantation.
Group 2 pulmonary venous hypertension is the result of left ventricular diastolic dysfunction. The left ventricle cannot relax, causing a rise in pressures on the right side. Treatment is focused on the underlying cause (e.g., obesity, hypertension, diabetes, diet [salt intake]). Treating with PAH medications may cause pulmonary edema and a worsening of patients’ symptoms.
Group 3 pulmonary hypertension is associated with disorders of the respiratory system and/or hypoxemia. Patients may respond to phosphodiesterase (PDE)-5 inhibitors (e.g., sildenafil [Revatio]) or an endothelin antagonist (bosentan, ambrisentan); however, a ventilation-perfusion ( ) mismatch may occur, causing a worsening of patients’ hypoxemia.
) mismatch may occur, causing a worsening of patients’ hypoxemia.
Group 4 pulmonary hypertension caused by chronic thrombotic and/or embolic disease (chronic thromboembolic pulmonary hypertension) may respond to PDE-5 inhibitors or low-dose prostacyclins.  scans and computed tomography (CT) scans of the chest are required to determine if the patient is a surgical candidate for pulmonary endarterectomy. A successful surgery can improve hemodynamics, functional class, quality of life, and survival.
scans and computed tomography (CT) scans of the chest are required to determine if the patient is a surgical candidate for pulmonary endarterectomy. A successful surgery can improve hemodynamics, functional class, quality of life, and survival.
Group 5 pulmonary hypertension caused by disorders directly affecting the pulmonary vasculature (e.g., pulmonary venoocclusive disease) rarely responds to any treatment. Lung transplant may be the only treatment choice.


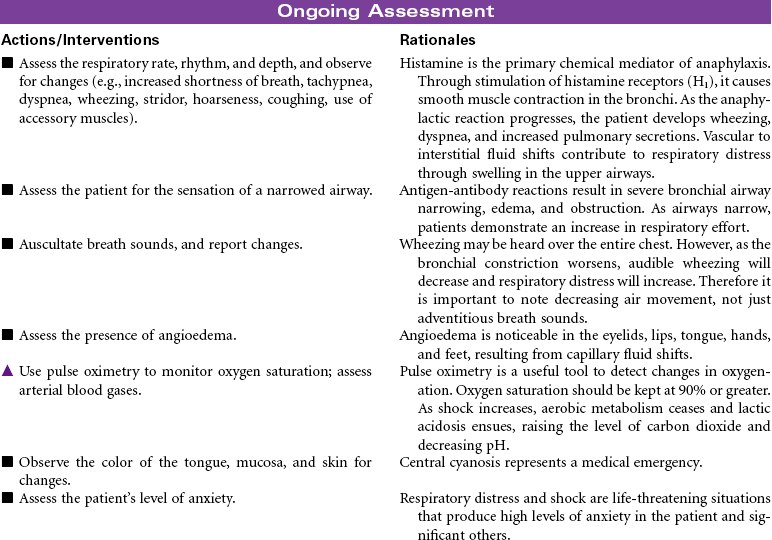
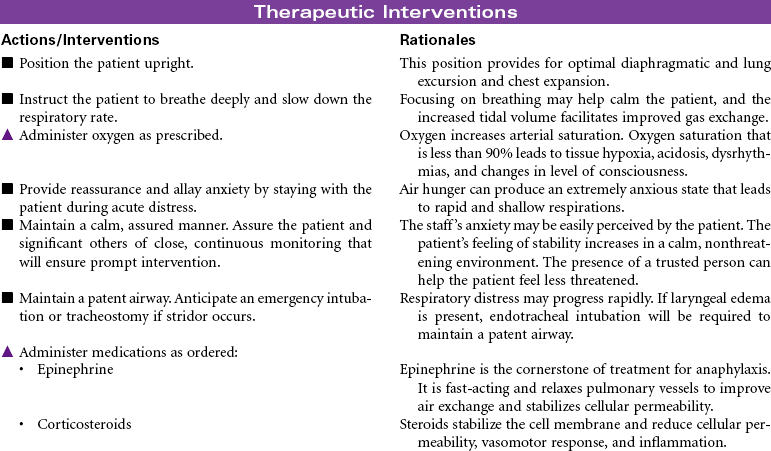
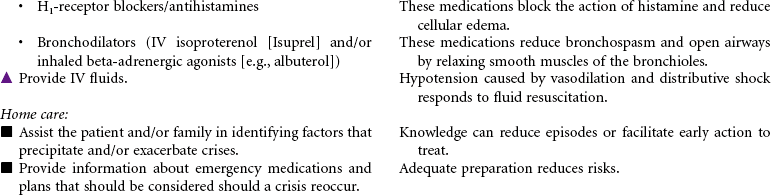
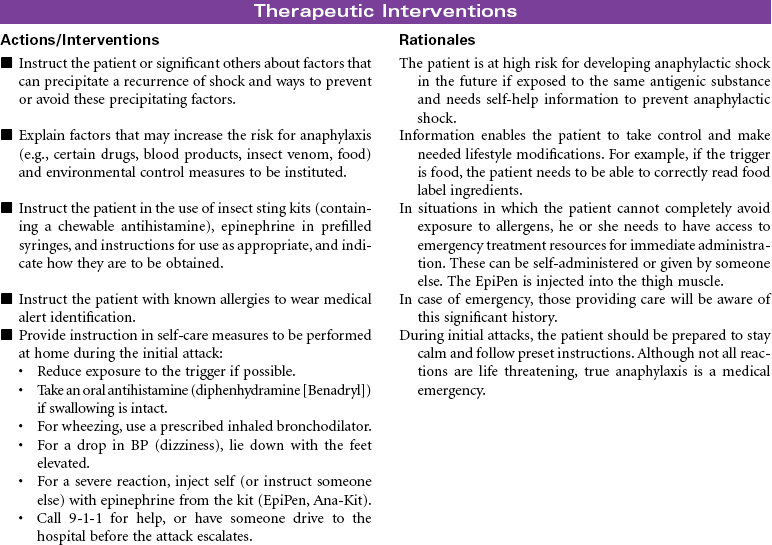
Shock, Anaphylactic
Allergic Reaction; Distributive Shock; Vasogenic Shock
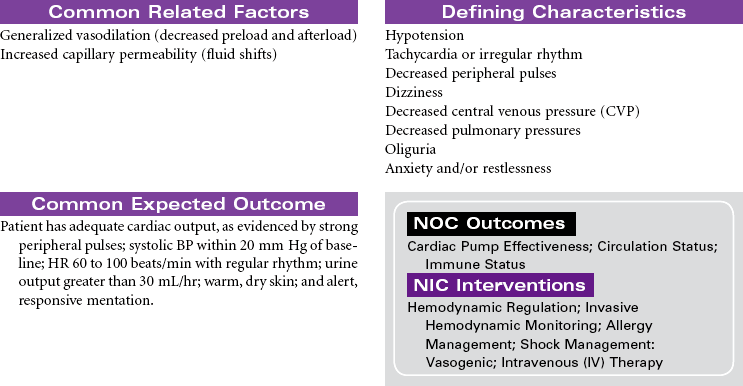
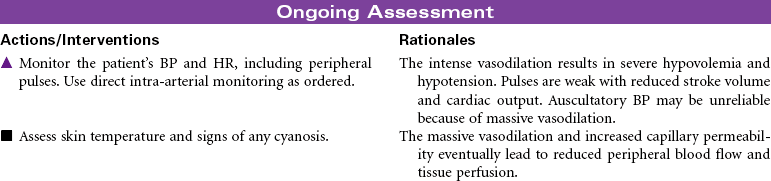
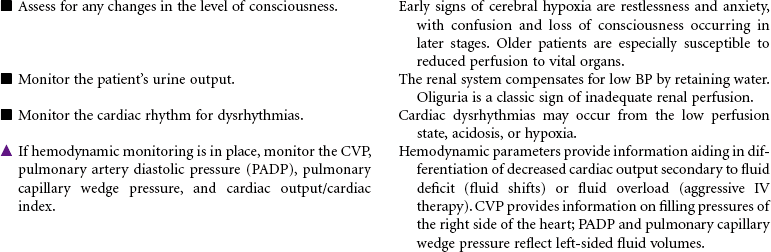
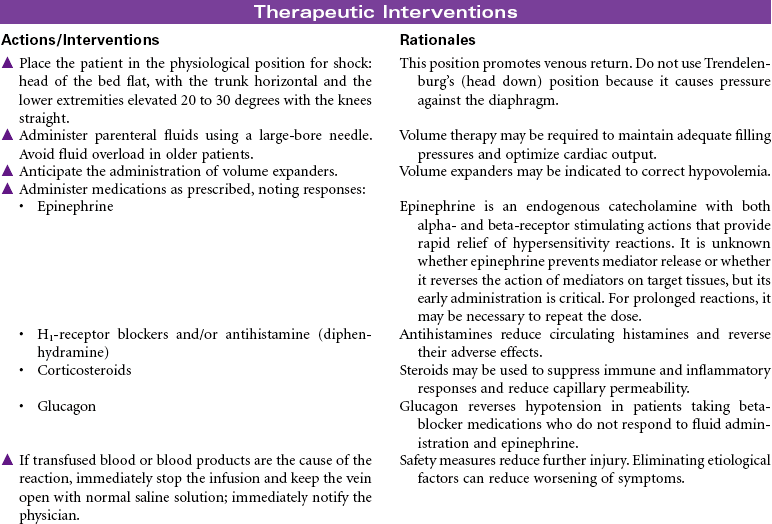
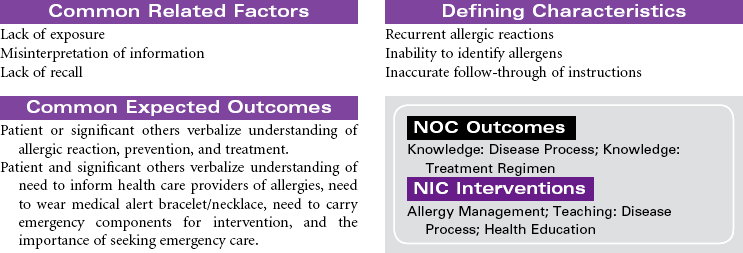
Anaphylactic shock is a potentially life-threatening situation characterized by massive vasodilation and increased capillary permeability triggered by a release of histamine. It is the most severe systemic form of hypersensitivity (antigen-antibody interaction); it occurs within seconds to minutes after contact with an antigenic substance and progresses rapidly to respiratory distress, vascular collapse, systemic shock, and possibly death if emergency treatment is not initiated. Causative agents include severe reactions to a sensitive substance such as a drug, vaccine, food (e.g., eggs, peanuts, shellfish), insect venom, dyes or contrast media, or transfused blood or blood products.


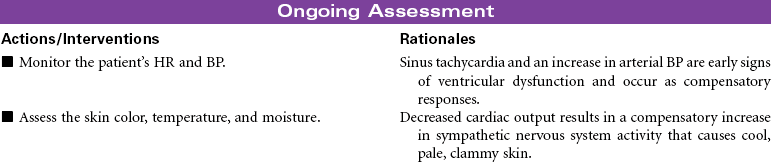
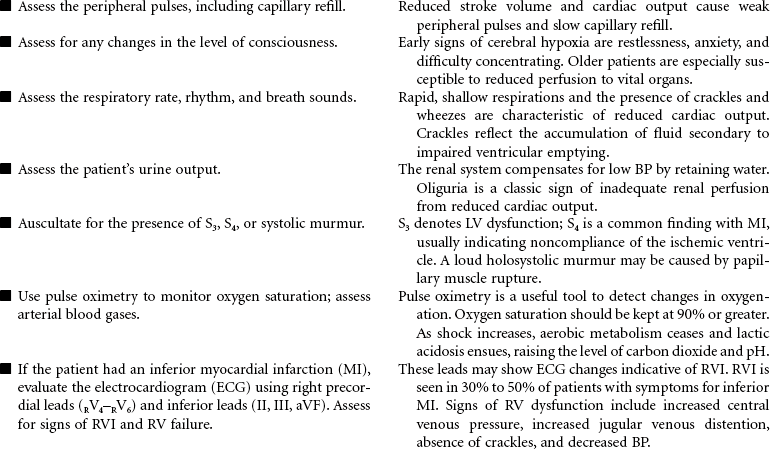
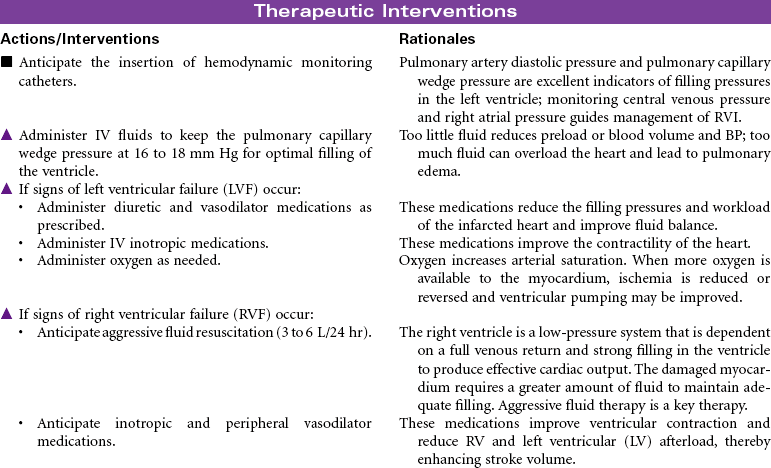
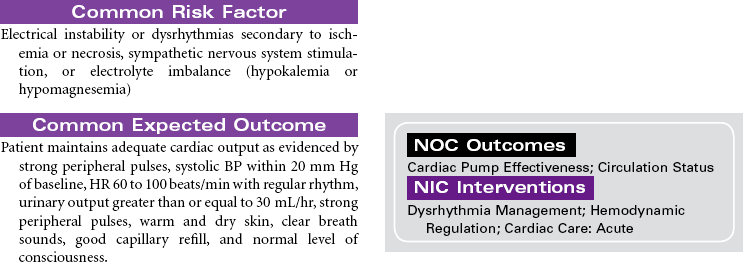
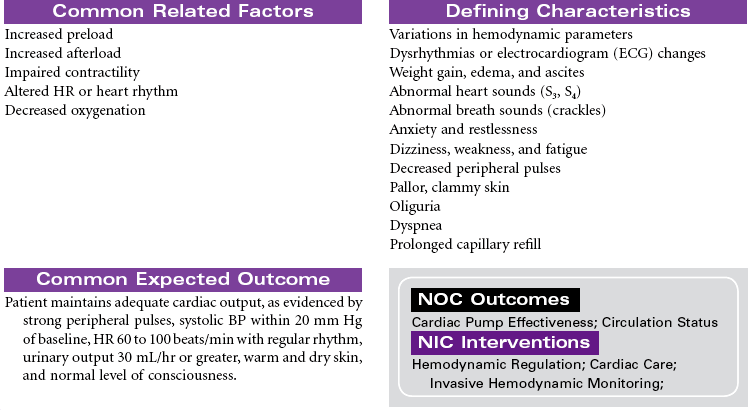
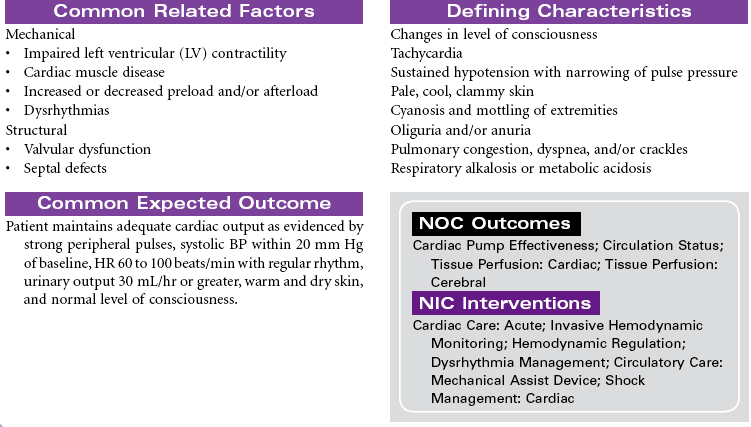
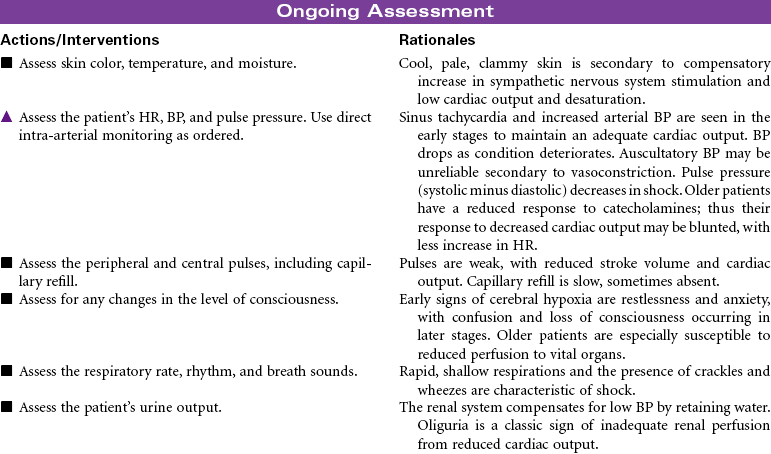
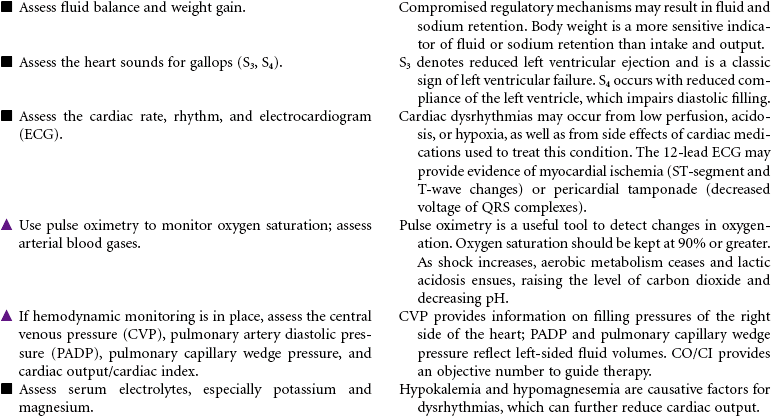
Shock, Cardiogenic
Pump Failure; Acute Pulmonary Edema
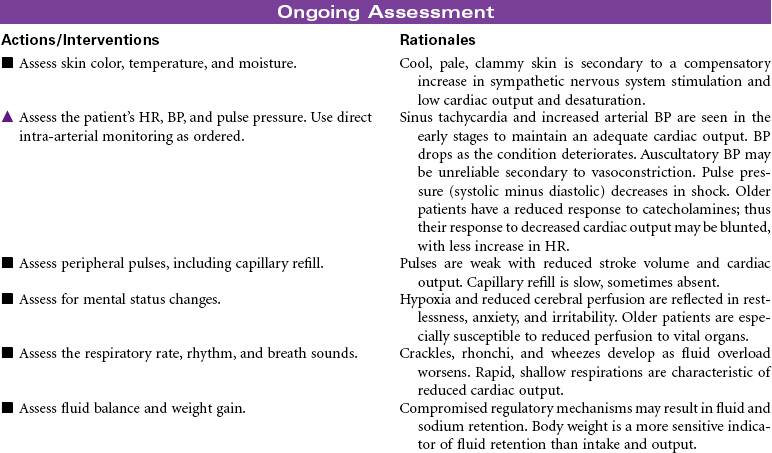
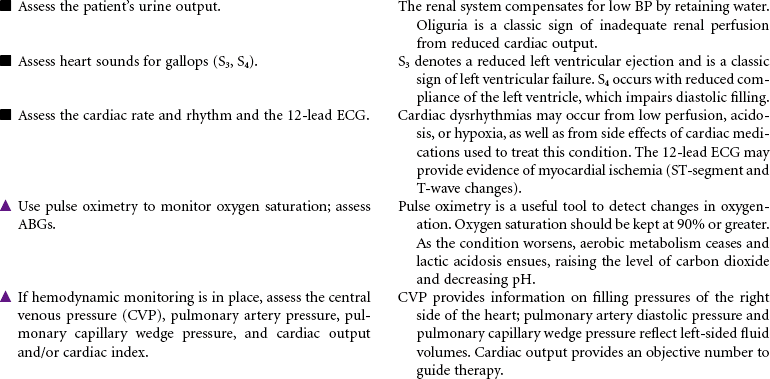
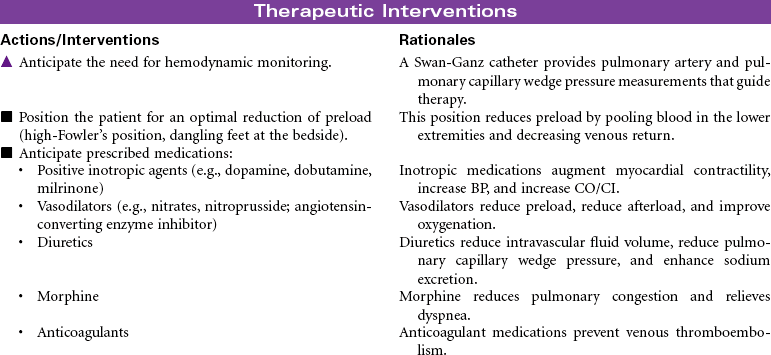
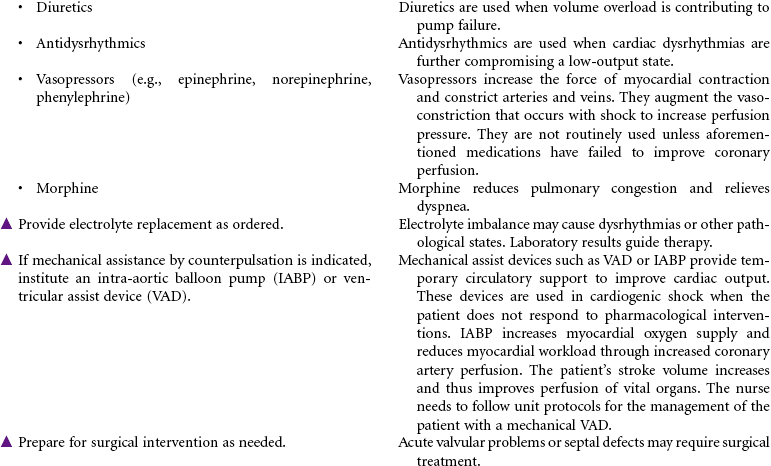
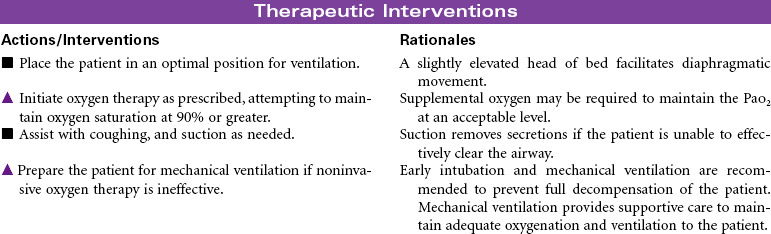
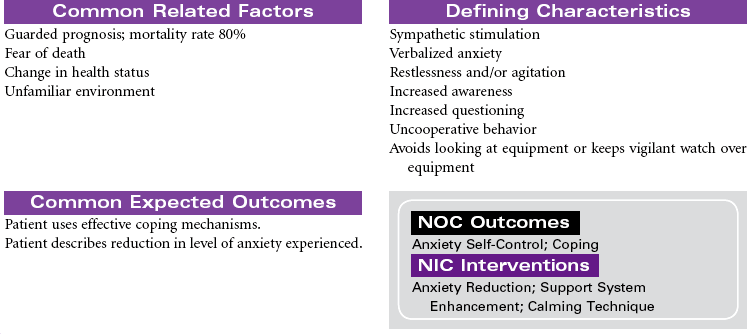
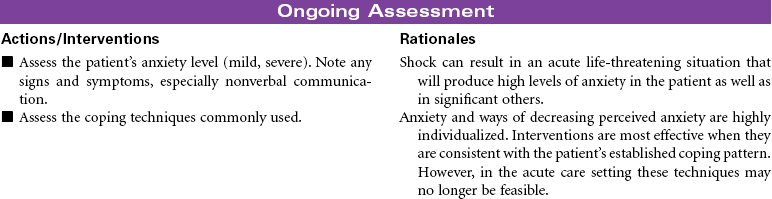
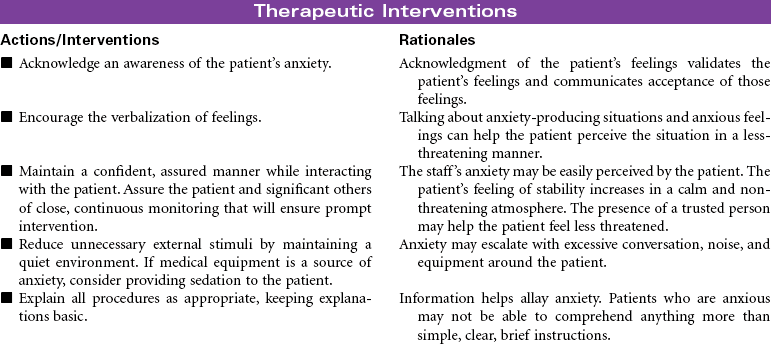
Cardiogenic shock is an acute state of sustained decreased tissue perfusion caused by the impaired contractility of the heart. It is usually associated with myocardial infarction (MI), cardiomyopathies, dysrhythmias, valvular stenosis, massive pulmonary embolism, cardiac surgery, or cardiac tamponade. It is a self-perpetuating condition because coronary blood flow to the myocardium is compromised, causing further ischemia and ventricular dysfunction. Patients with massive MIs involving 40% or more of the left ventricular (LV) muscle mass are at highest risk for developing cardiogenic shock. The mortality rate for cardiogenic shock often exceeds 80%. This care plan focuses on the care of an unstable patient in a shock state.

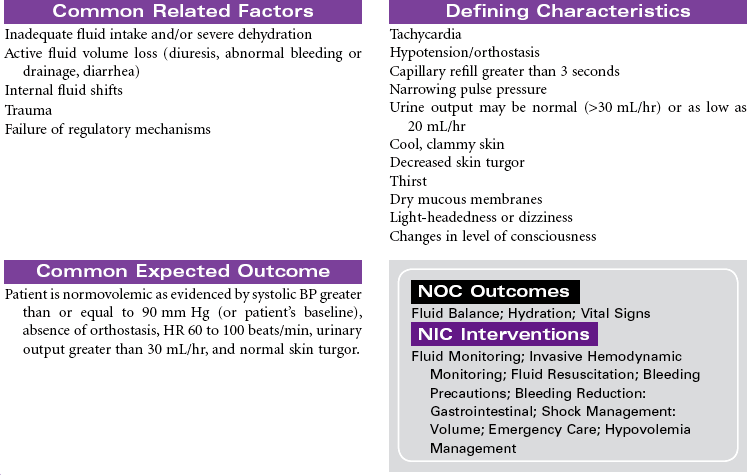
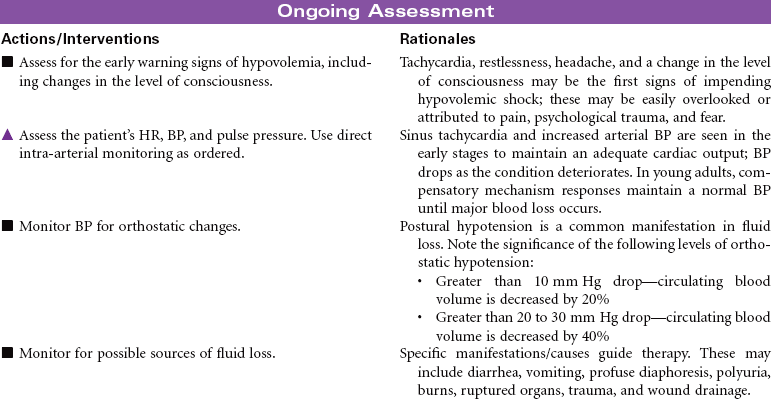
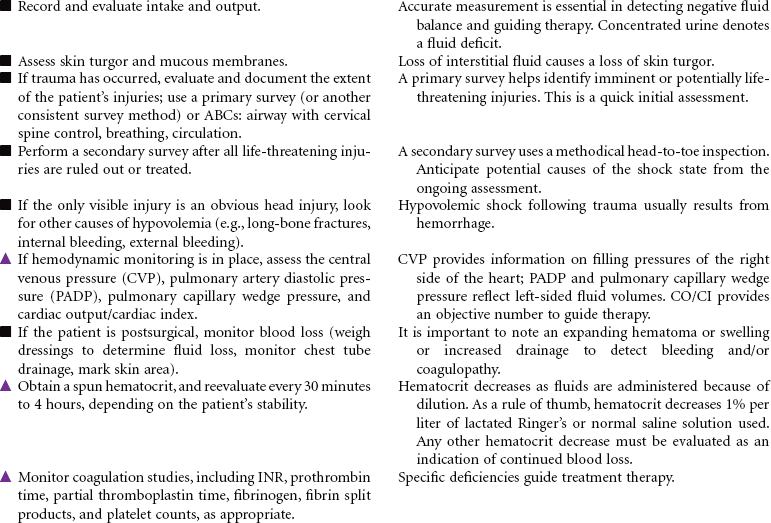
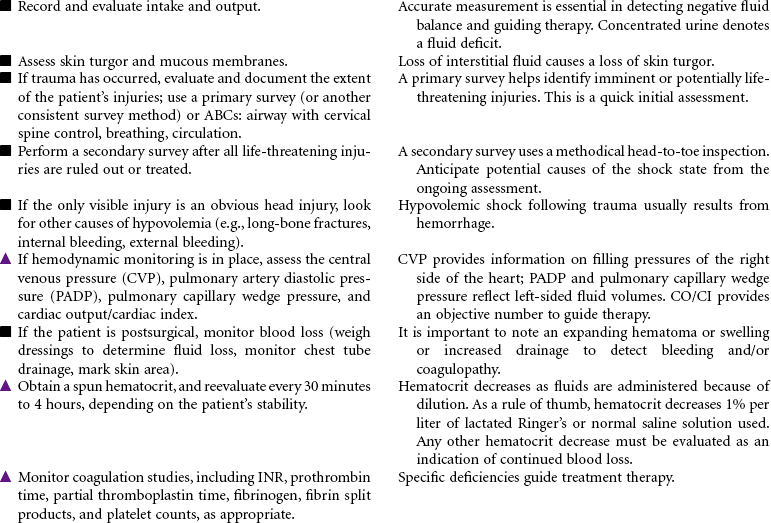
Shock, Hypovolemic
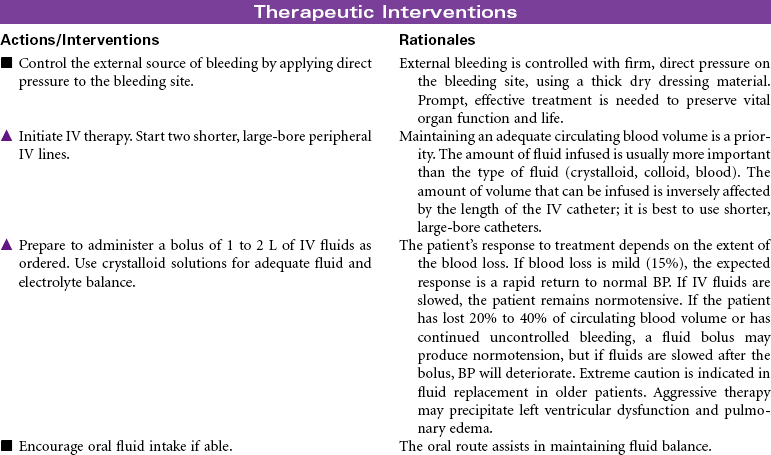
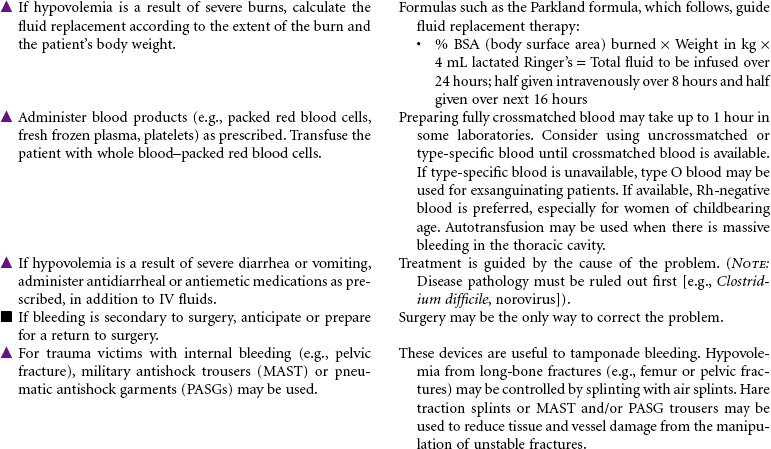
Hypovolemic shock is an emergency situation that occurs from decreased intravascular fluid volume, resulting from either internal fluid shifts or external fluid loss. This fluid can be whole blood, plasma, or water and electrolytes. Losing about one fifth of total blood volume can produce this condition, resulting in circulatory dysfunction and inadequate tissue perfusion. Common causes include hemorrhage (external or internal), severe burns, vomiting, and diarrhea. Hemorrhagic shock often occurs after trauma, gastrointestinal bleeding, or rupture of organs or aneurysms. Internal fluid losses occur in clinical conditions associated with increased capillary permeability and resulting shifts in fluid from the vascular compartment to interstitial spaces or other closed fluid compartments (e.g., peritoneal cavity). This third-spacing of fluids in the body is seen in patients with extensive burns or with ascites and leads to hypovolemic shock.
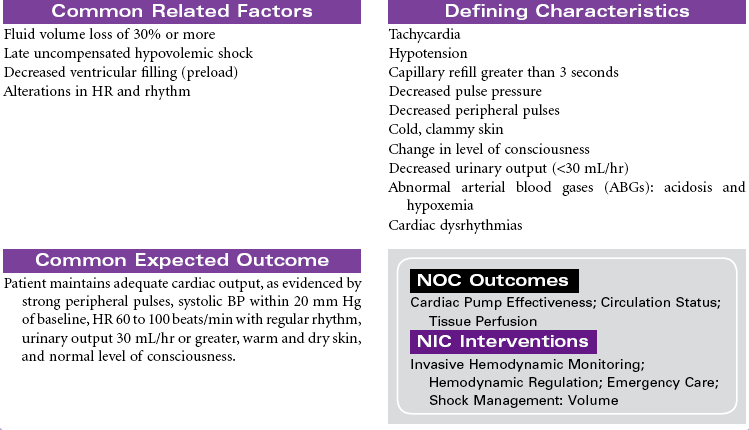
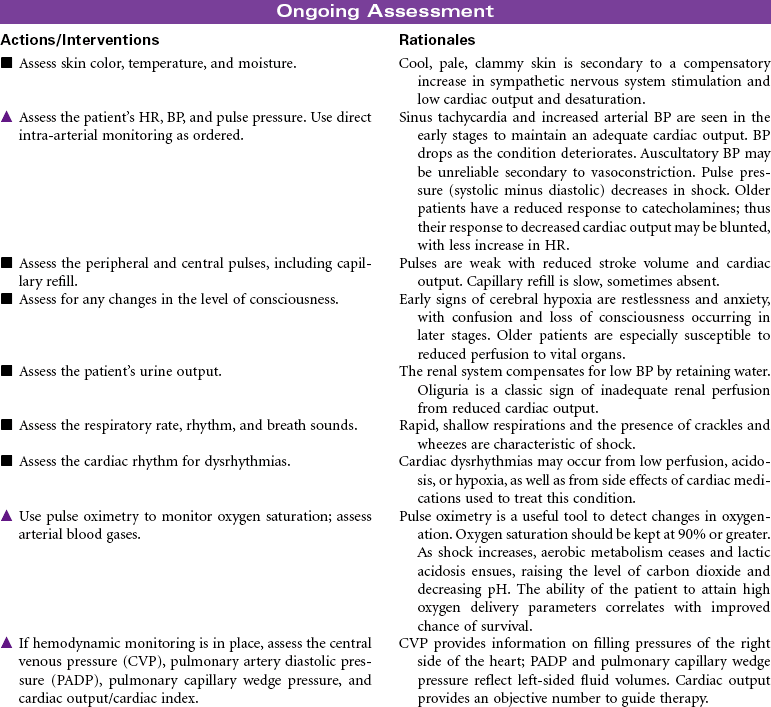
Hypovolemic shock can be classified according to the percentage of fluid loss. Mild shock (stage 1) is up to 15% blood volume loss, moderate shock (stage 2) is 15% to 30% blood volume loss, stage 3 is 30% to 40% blood volume loss, and severe shock is a greater than 40% loss. Older patients may exhibit signs of shock with smaller losses of fluid volume because of their compromised ability to compensate for fluid changes. Treatment focuses on prompt fluid and/or blood replacement, identification of causative factors and/or bleeding sites, control of bleeding, and prevention of complications. If aggressive treatment is not prompt, further collapse can cause irreversible brain and kidney damage and eventual cardiac arrest and death.
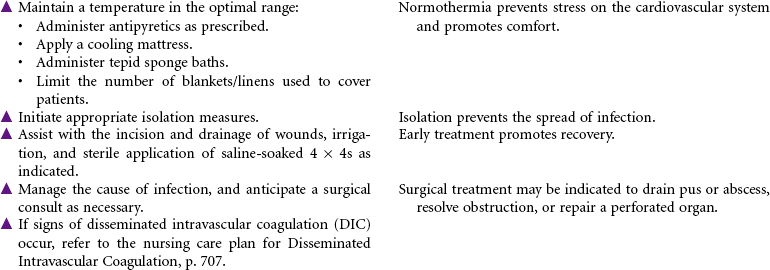
Shock, Septic
Distributive Shock; Sepsis; Bacteremia; Endotoxic Shock; Disseminated Intravascular Coagulation (DIC); Multiple Organ Failure
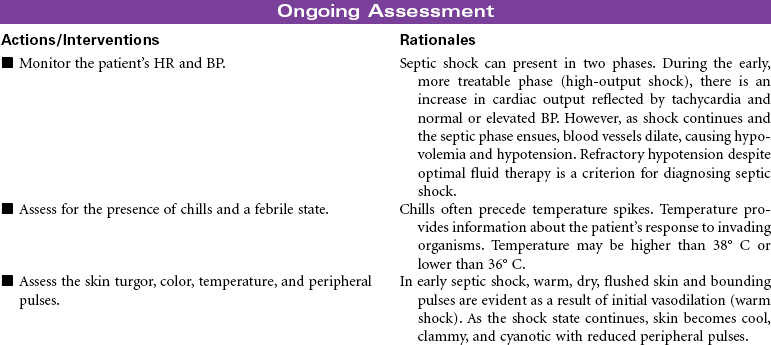
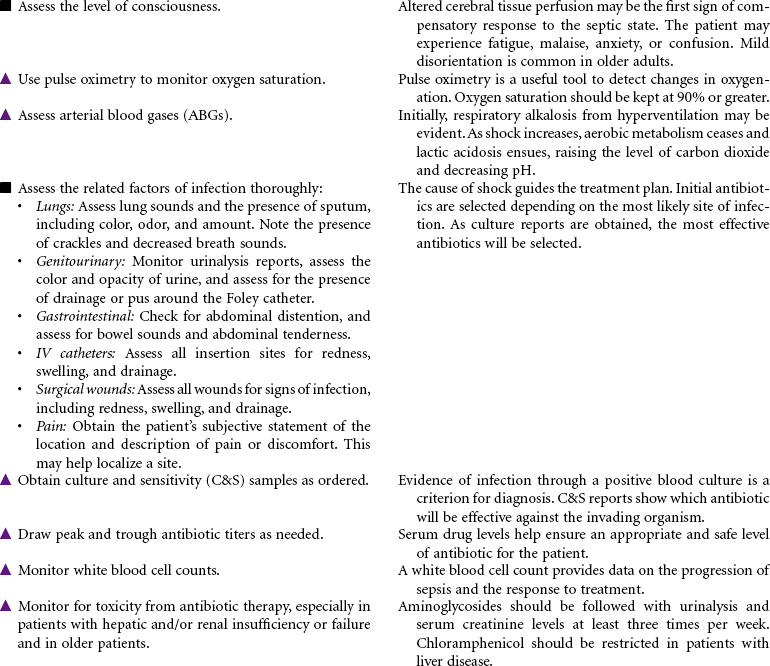
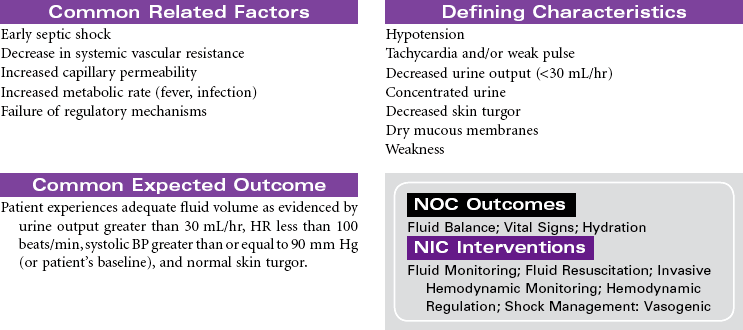
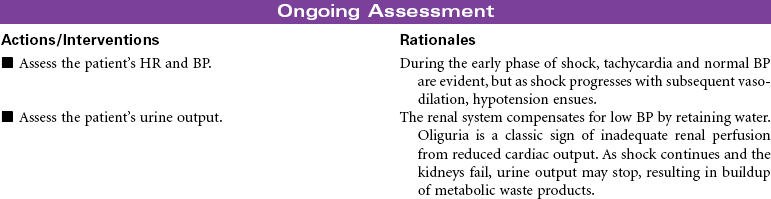
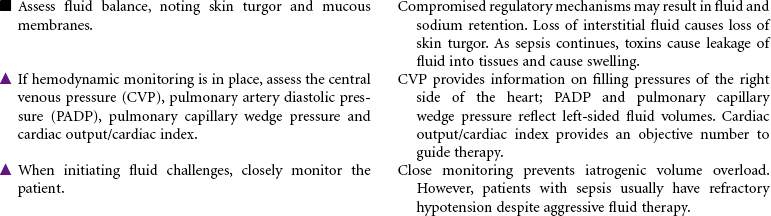
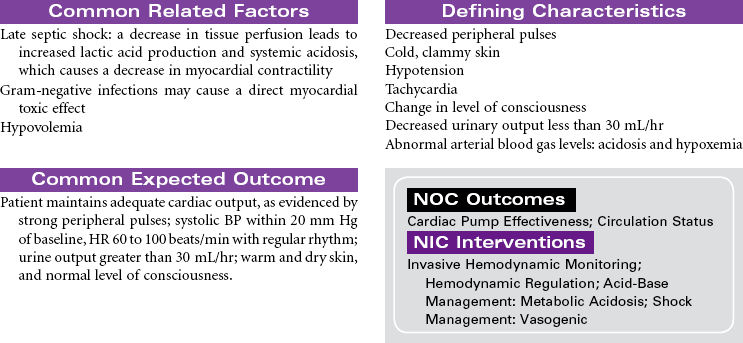
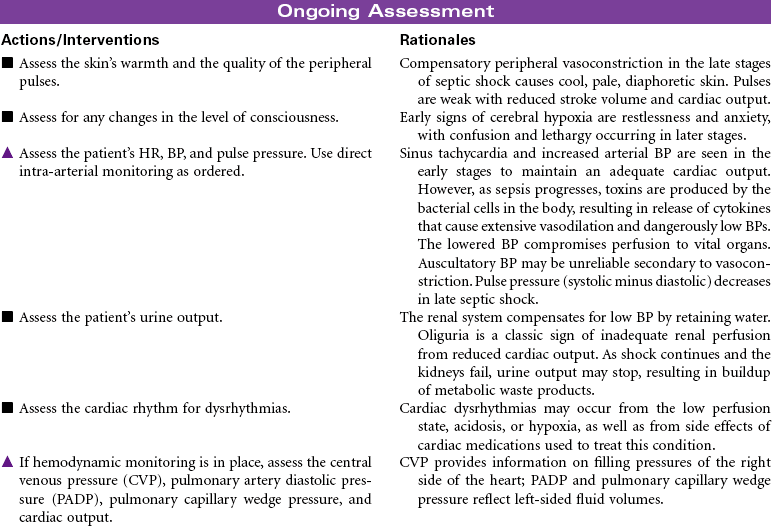
Septic shock is associated with severe infection and occurs after bacteremia of gram-negative bacilli (most common) or gram-positive cocci. Septic shock is mediated by a complex interaction of hormonal and chemical substances through an immune system response to bacterial endotoxins. In the early stages of sepsis, the body responds to infection by the normal inflammatory response. As the infection progresses, sepsis becomes more severe and leads to decreased tissue perfusion and oxygen delivery and multiple-organ dysfunction. Septic shock occurs as an exaggerated inflammatory response that leads to hypotension even with adequate fluid resuscitation. The primary effects of septic shock are massive vasodilation, maldistribution of blood volume, and myocardial depression. The maldistribution of circulatory volume results in some tissues receiving more than adequate blood flow and other tissues receiving less than adequate blood flow. As shock progresses, disseminated intravascular coagulation may occur, resulting in a serious imbalance between clotting and bleeding.
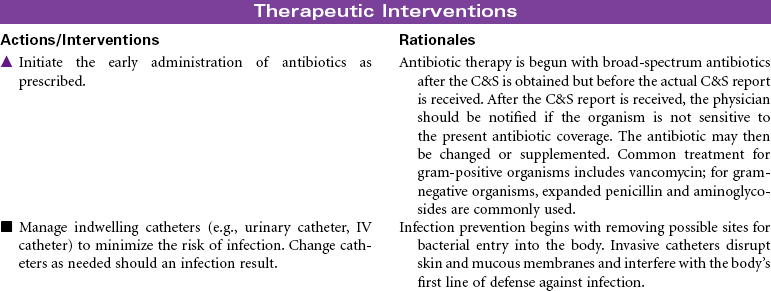
Older patients are at increased risk for septic shock because of factors such as impaired immune response, impaired organ function, chronic debilitating illnesses, impaired mobility that can lead to pneumonia, decubitus ulcers, and loss of bladder control requiring indwelling catheters. The mortality rate from septic shock is high (from 30% to approximately 50%), especially in older patients. Immunocompromised patients and those with chronic diseases are also at increased risk. Patients are usually treated in an intensive care unit. Treatment is focused on providing fluid volume resuscitation and antibiotic therapy based on causative bacteria and/or cocci and supporting major organ dysfunction.

Thrombosis, Deep Vein
Venous Thromboembolic Disease; Phlebitis; Phlebothrombosis
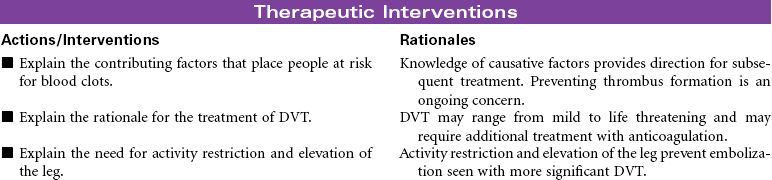
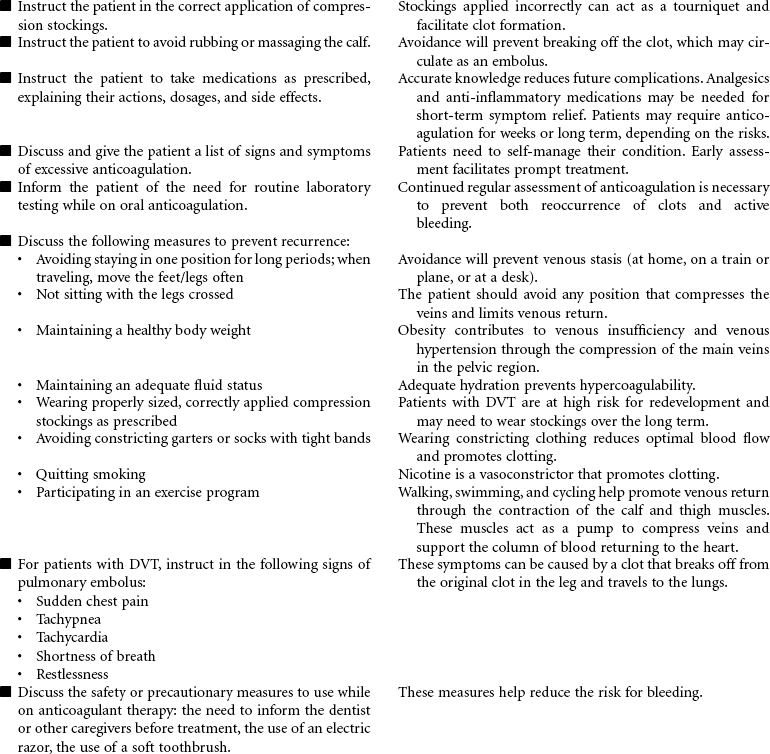
Thrombophlebitis is the inflammation of the wall of a vein, usually resulting in the formation of a blood clot (thrombosis) that may partially or completely block the flow of blood through the vessel. Venous thrombophlebitis usually occurs in the lower extremities. It may occur in superficial veins, which, although painful, is not life threatening and does not require hospitalization, or it may occur in a deep vein, which can be life threatening because clots may break free (embolize) and cause a pulmonary embolism. Three factors contribute to the development of deep vein thrombosis (DVT): venous stasis, hypercoagulability, and endothelial damage to the vein. Prolonged immobility is the primary cause of venous stasis. Hypercoagulability is seen in patients with deficient fluid volume, oral contraceptive use, smoking, and certain malignancies. Venous wall damage may occur secondary to IV infusions, certain medications, fractures, and contrast x-ray studies. DVT most commonly occurs in lower extremities, where it is often asymptomatic and resolves in a few days. More proximal DVTs are associated with greater symptomatology and carry a higher risk for dislodgment and migration. Treatment is supportive, usually with anticoagulant therapy. Goals are to reduce risk for complications and prevent reoccurrence.

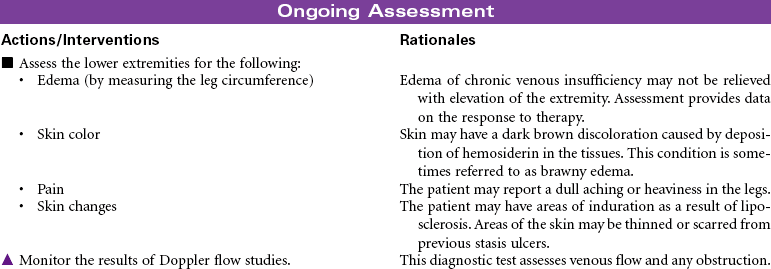
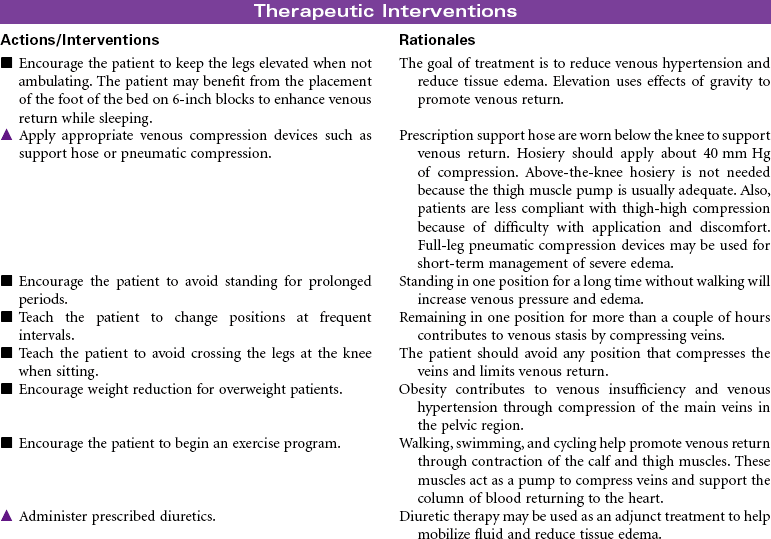
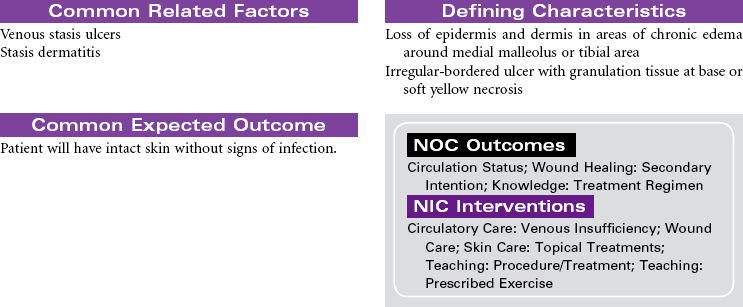
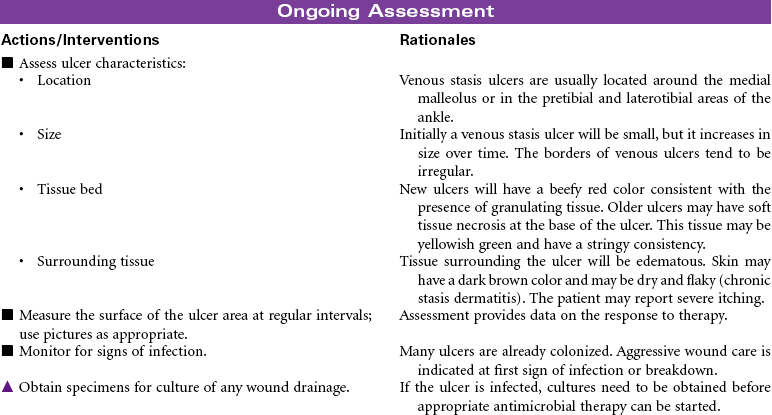
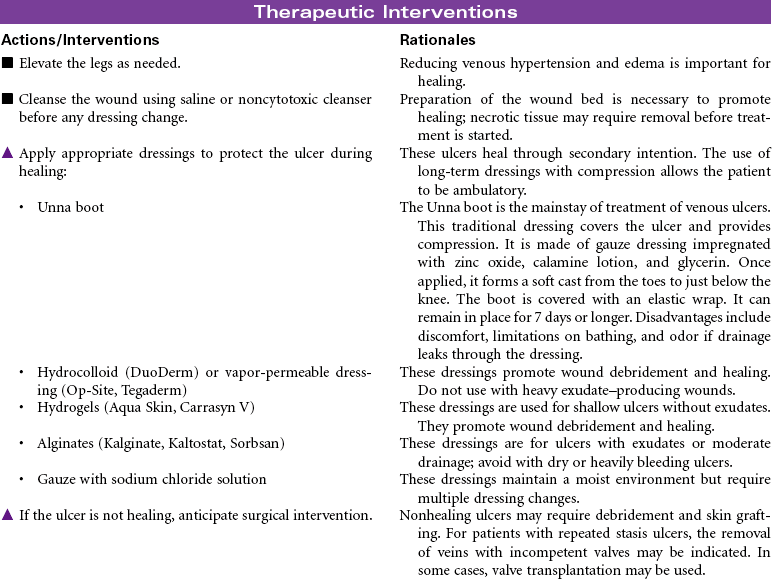
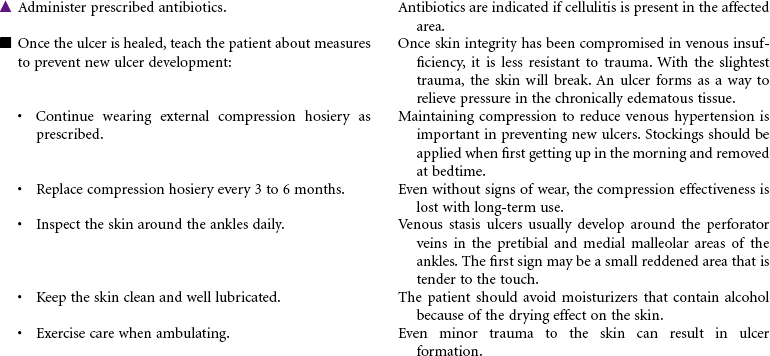
Venous Insufficiency, Chronic
Postphlebitic Syndrome; Peripheral Venous Hypertension; Venous Stasis Ulcer
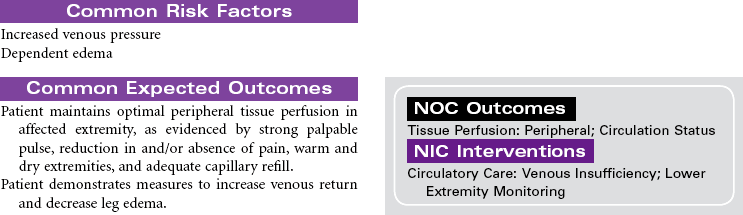
Chronic venous insufficiency occurs from a disruption in the venous system that results in the pressure from the venous blood column no longer being supported toward the heart. This pressure is directed as backflow to the ankle area. The most common causes are congenital venous valve insufficiency, acquired valve incompetence from venous valve prolapse (often from history of deep vein thrombosis [DVT] or varicose veins), venous obstruction from tumor or fibrosis, or calf muscle pump malfunction from sedentary lifestyle or muscle wasting disease. The increased backflow and pressure cause dilation of the venules of the skin, primarily in the ankle area, with resulting movement of fluid from the vascular bed to the tissue bed. Because the endothelium of the venules is subjected to higher than normal pressures, red blood cells move across the vessel wall into the interstitial spaces. When these red blood cells break down, they deposit hemosiderin in the tissues. The presence of hemosiderin in the tissues produces the characteristic skin color changes in venous insufficiency. The clinical manifestations of chronic venous insufficiency include dull aching, tenderness, pain in leg; leg pain getting worse when standing or when legs are raised; edema; skin color changes; dermatitis; and venous stasis ulcers. Once skin ulceration occurs, it is difficult to heal. Ulcers may recur with minimal skin trauma.
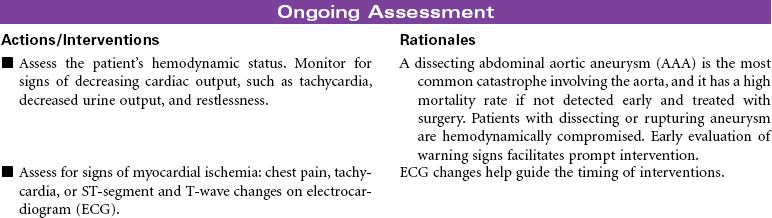
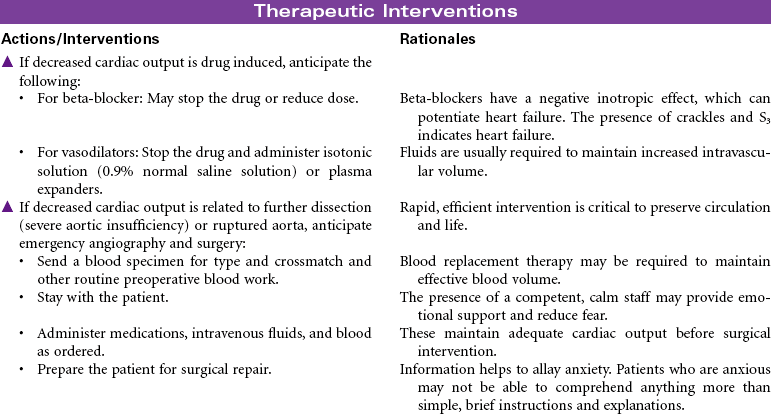
Aortic Aneurysm
Dissecting Aneurysm; Thoracic Aneurysm; Abdominal Aneurysm
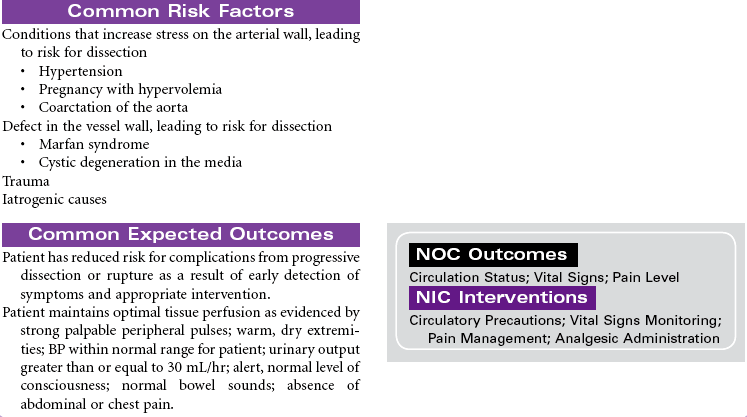
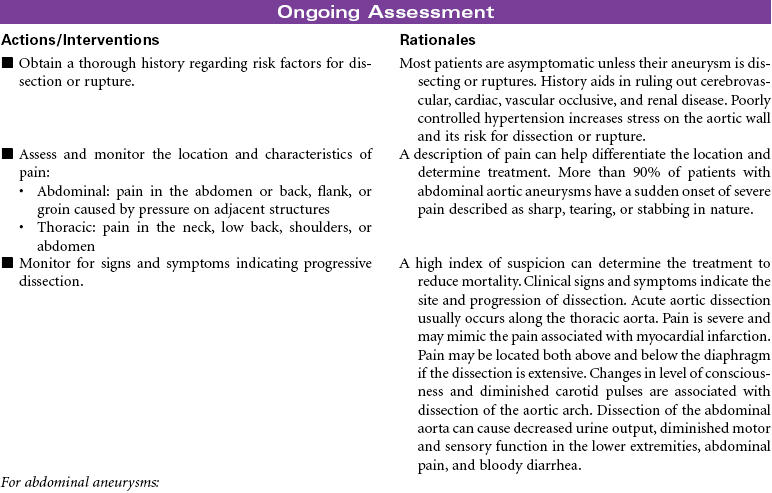
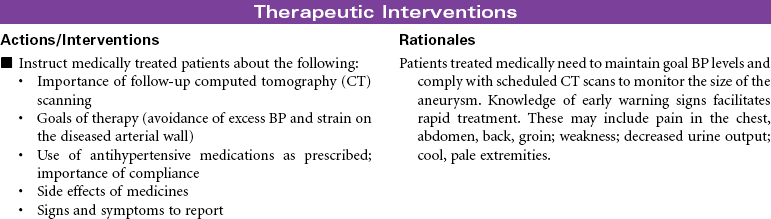
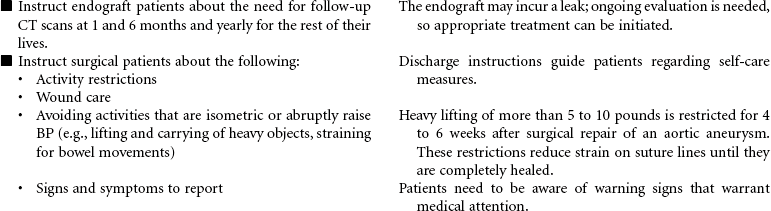
An aneurysm is a localized, circumscribed, blood-filled abnormal dilation of an artery caused by disease or weakening of the vessel wall. True aneurysms involve dilation of all layers of the vessel wall. The two types of true aneurysms are: (1) saccular, which is characterized by a bulbous out-pouching of one side of the artery resulting in localized stretching of the artery wall, and (2) fusiform, which is characterized by a uniformly shaped dilation of the entire circumference of the artery. True aneurysms are asymptomatic and are typically diagnosed by physical examination or a diagnostic ultrasound or computed tomography scan. The natural history of an aneurysm is enlargement; as a rule, the larger it is, the greater the chance of rupture. Aneurysms are most commonly seen in the abdominal aorta. Abdominal aortic aneurysms (AAAs) account for about 75% and thoracic aneurysms for about 25% of all cases. They occur more often in men than in women. Risk factors include smoking and having a family history of aneurysms. When an aneurysm becomes large enough for risk for rupture, it can be repaired by open surgical repair or a less-invasive endograft-covered stent repair.
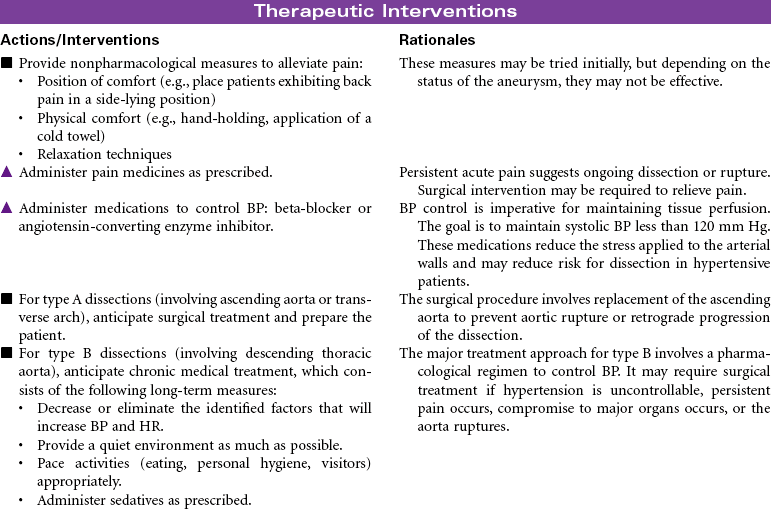
Dissecting aneurysms occur when the inner layer of the blood vessel wall tears and splits, creating a false channel and cavity of blood between the intimal and adventitial layers. They are typically classified according to the location. According to the Stanford Classification, type A involves the ascending aorta and its transverse arch and type B involves the descending aorta. A dissecting AAA is the most common catastrophe involving the aorta, and it has a high mortality rate if not detected early and treated with surgery. More than 90% of patients present with sudden onset of severe pain, which is usually described as sharp, tearing, or stabbing in nature. Symptoms depend on the size and location of the dissection or rupture. Risk factors for dissection include hypertension, pregnancy, trauma, and Marfan syndrome.


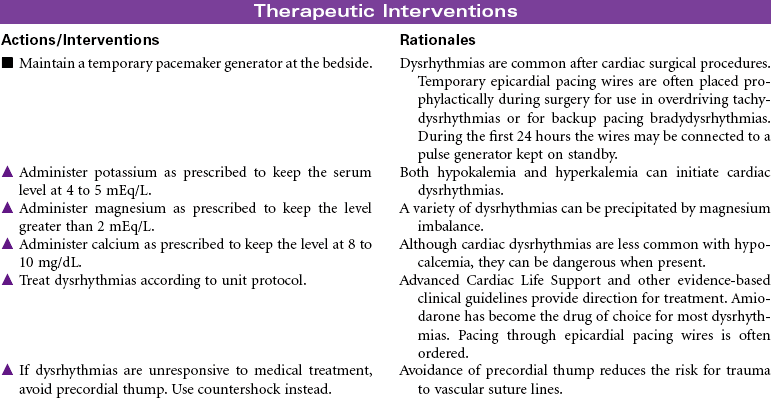
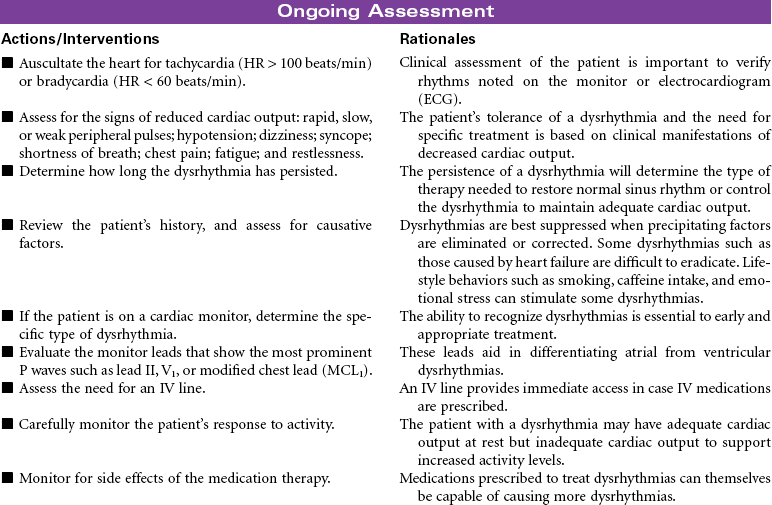
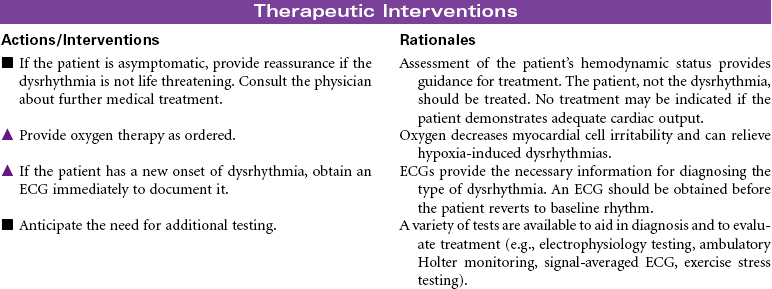
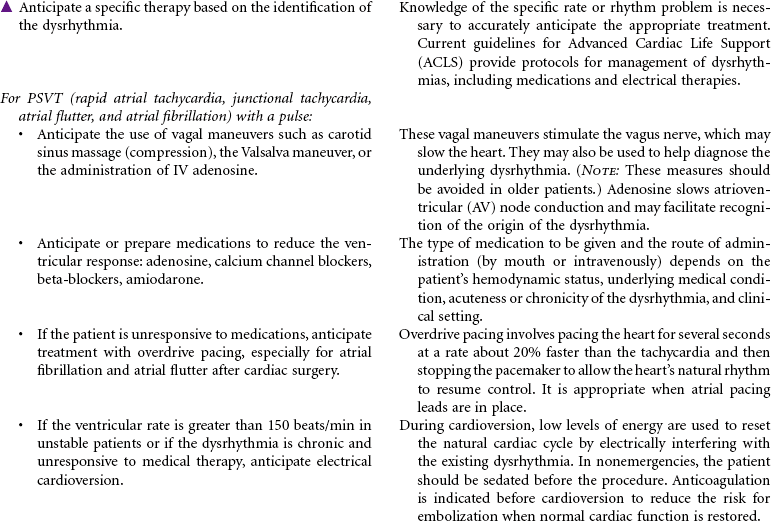
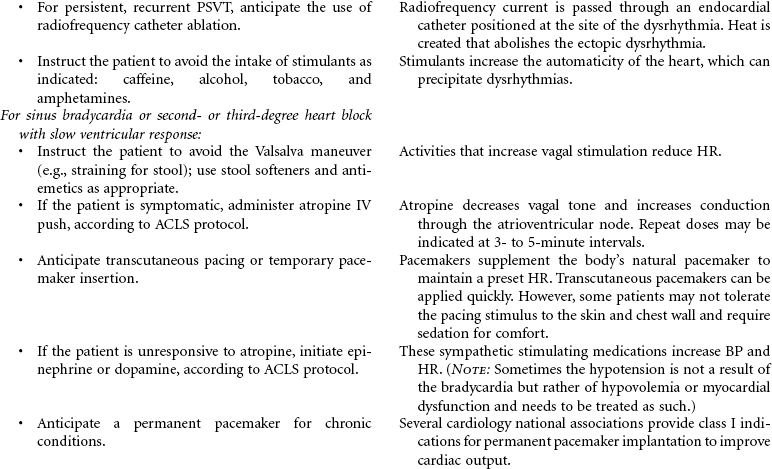
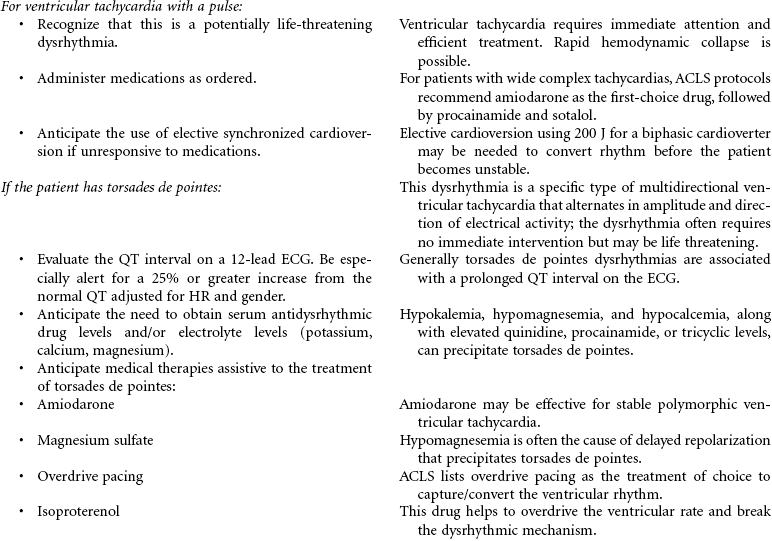
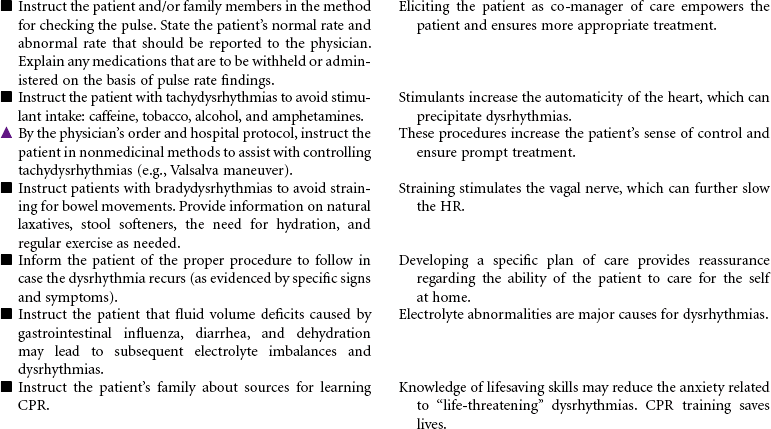
Dysrhythmias
Tachycardia; Bradycardia; Atrial Flutter; Atrial Fibrillation; Paroxysmal Supraventricular Tachycardia (PSVT); Heart Block; Pacemakers
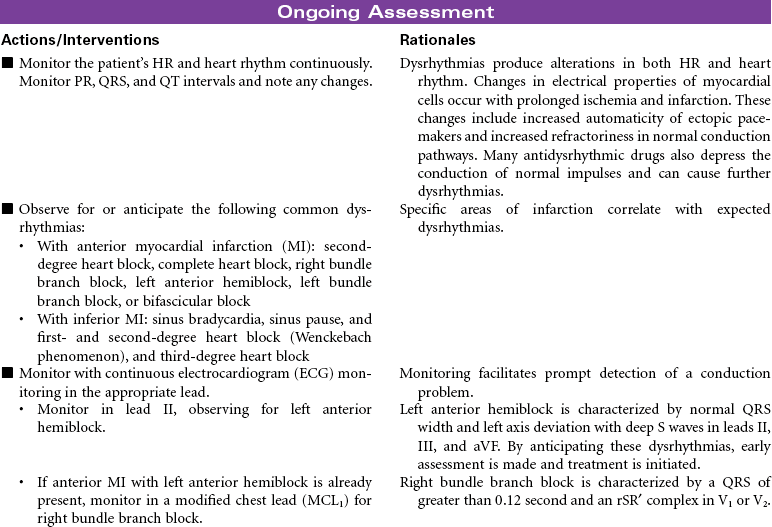
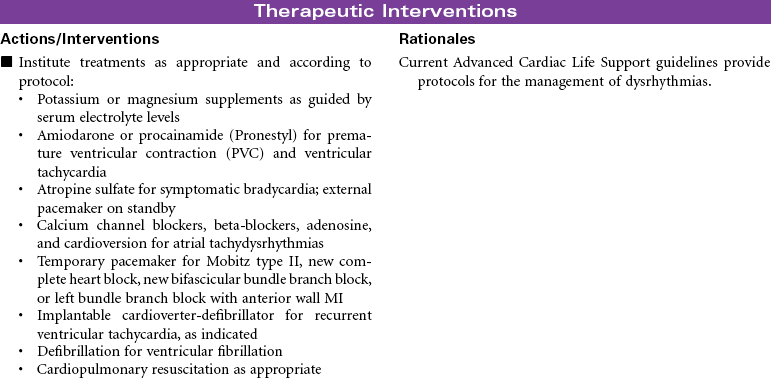
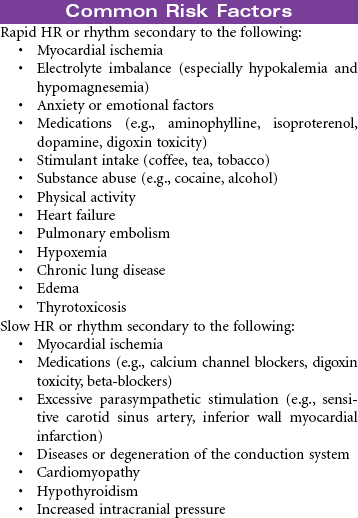
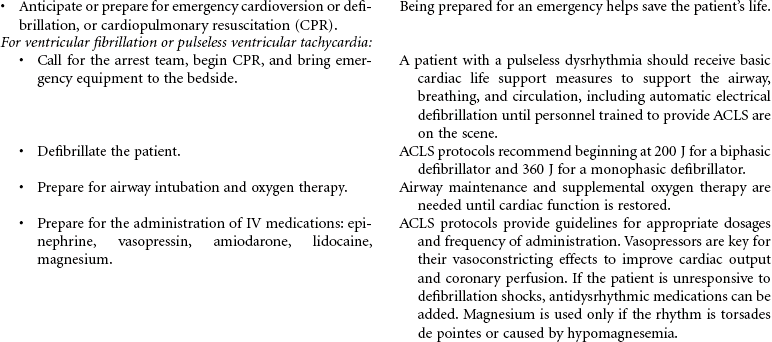
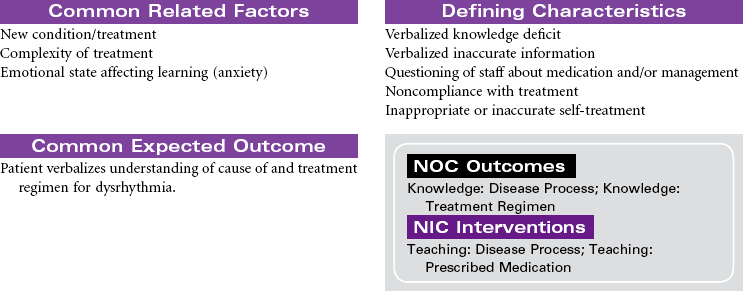
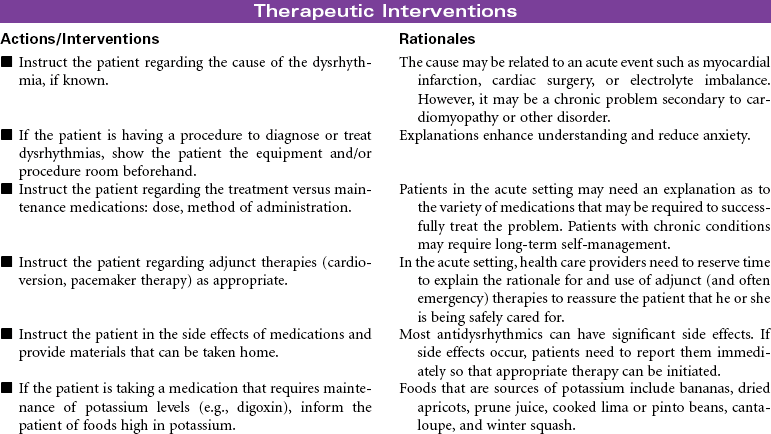
Dysrhythmias involve any disturbance in the rhythm, rate, or conduction in the cardiac electrical system. They can occur for a variety of reasons. Dysrhythmias can develop as a result of myocardial ischemia, electrolyte imbalances, acid-base imbalances, and adverse reactions to drugs. Even the aging process causes changes in the electrical properties of myocardial cells. Changes in electrical events in the heart have a direct effect on contraction and relaxation of the myocardium. The end result is hemodynamic alterations that may lead to decreased cardiac output. The clinical significance of dysrhythmias can range from benign occurrences not requiring treatment to life-threatening situations. For some patients, syncope or even sudden cardiac death is the first occurrence of the dysrhythmia. Evaluation of the causative factors for and the clinical significance of the dysrhythmia guide the therapeutic management. Treatment usually consists of drug therapy but may also include pacemaker support, electrical cardioversion, radiofrequency catheter ablation, an implantable defibrillator, or cardiopulmonary resuscitation. The American Heart Association (AHA) Guidelines for Advanced Cardiac Life Support provide treatment protocols for the management of patients experiencing dysrhythmias. This care plan focuses on acute management in a medical setting.


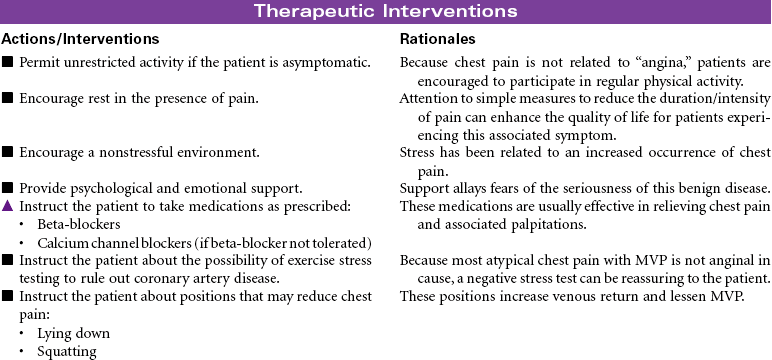
Mitral Valve Prolapse
Barlow’s Disease; Floppy Valve, Click-Murmur Syndrome
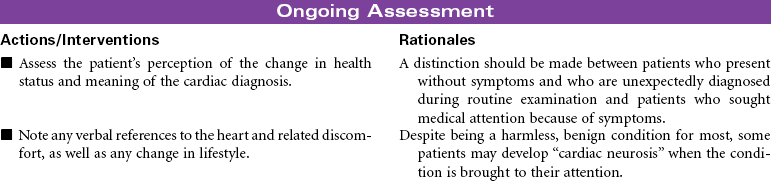
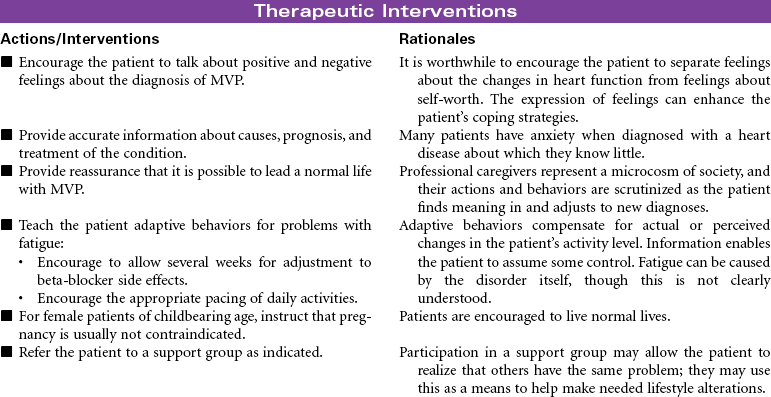
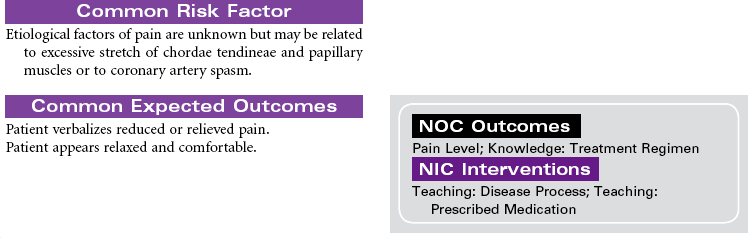
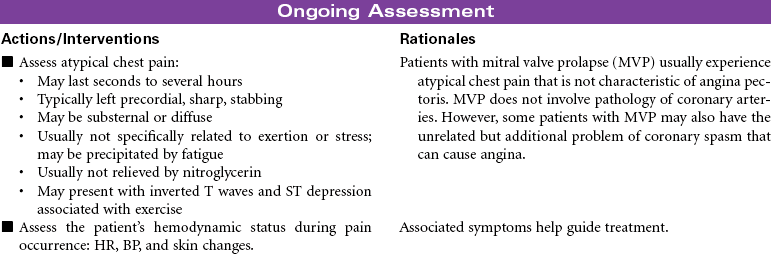
Mitral valve prolapse (MVP) is the most common abnormality of the heart valves. The mitral valve lies between the left atrium and ventricle. Prolapse of this valve refers to the upward movement of the mitral leaflets back into the left atrium during systole. MVP usually results from abnormality in the connective tissue of the leaflets, annulus, or chordae tendineae and occurs in about 2% to 3% of the general population, usually in people ages 20 to 40 years. It is seen in both men and women. MVP can be inherited, especially if associated with connective tissue disorders such as Marfan’s syndrome. Most people with MVP are asymptomatic and do not require treatment, except reassurance that this is a benign condition. Others may experience symptoms associated with mitral regurgitation, atypical chest pain related to tension the prolapsed valve exerts on the papillary muscle, harmless palpitations as the result of an autonomic nervous system imbalance, and fatigue. Diagnostic findings include midsystolic click, late systolic murmur, echocardiogram abnormalities, and angiographic findings.

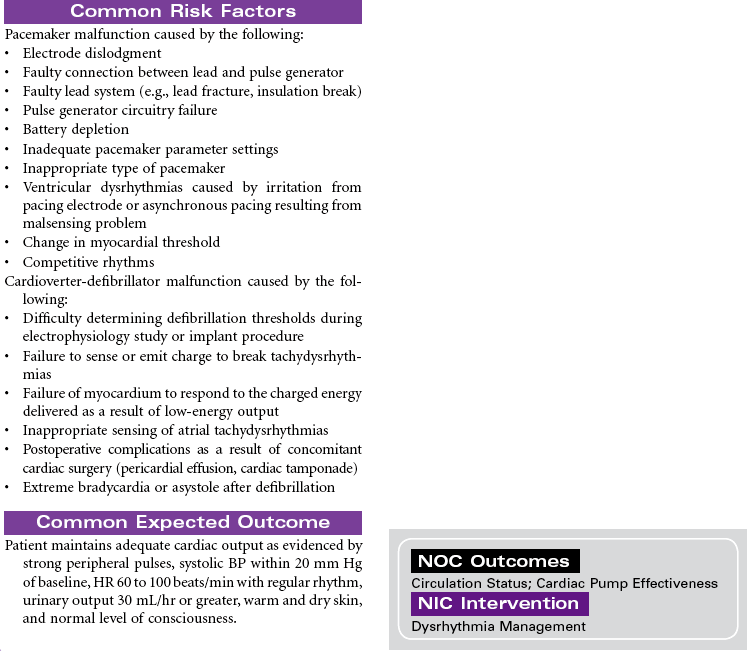
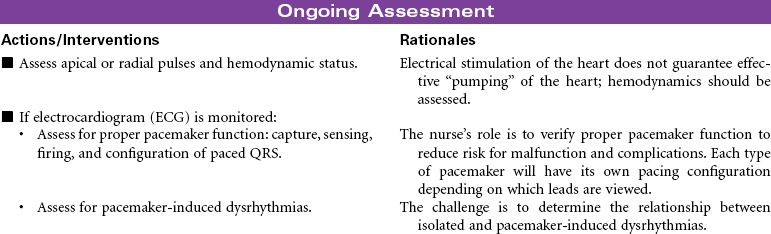
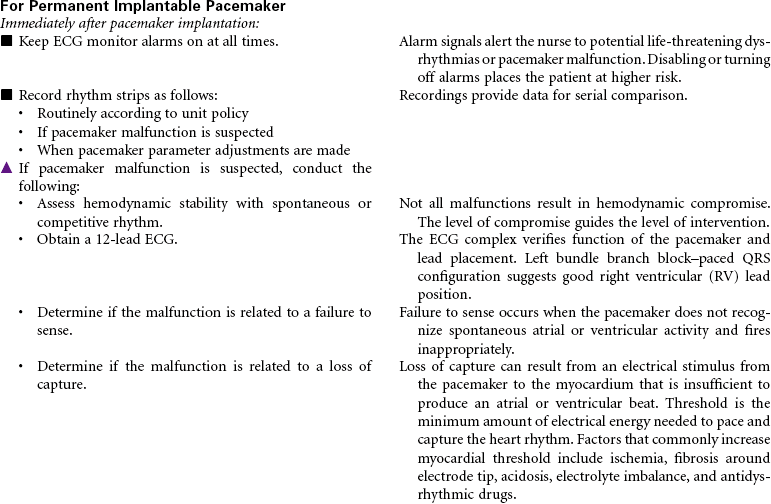
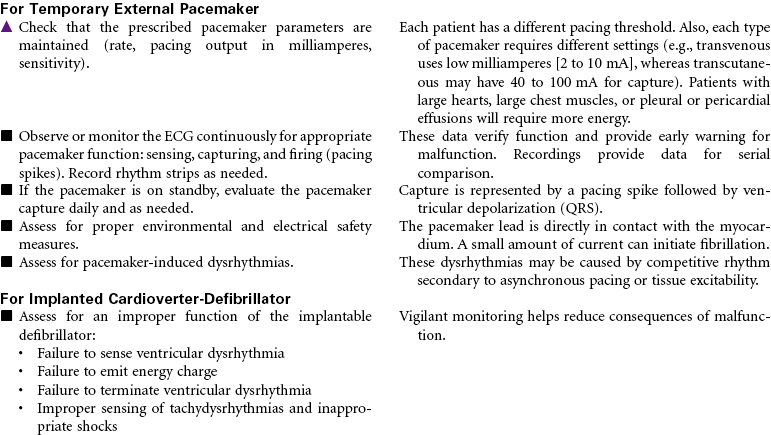
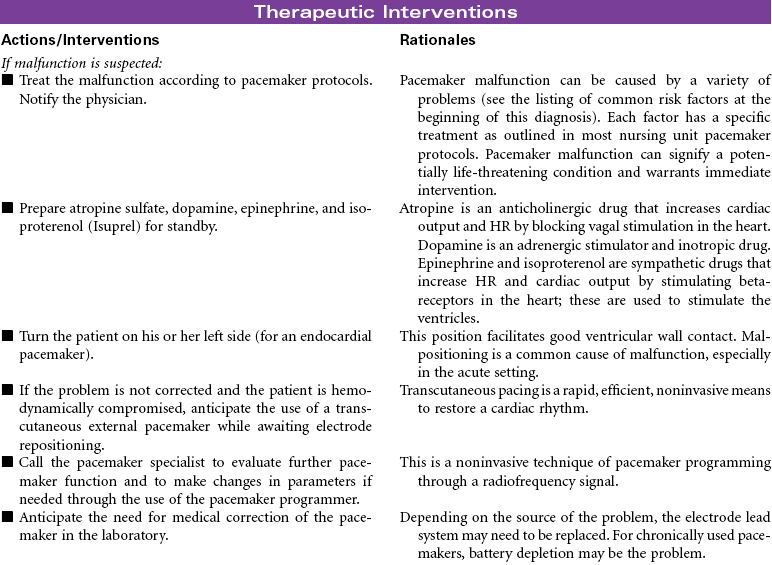
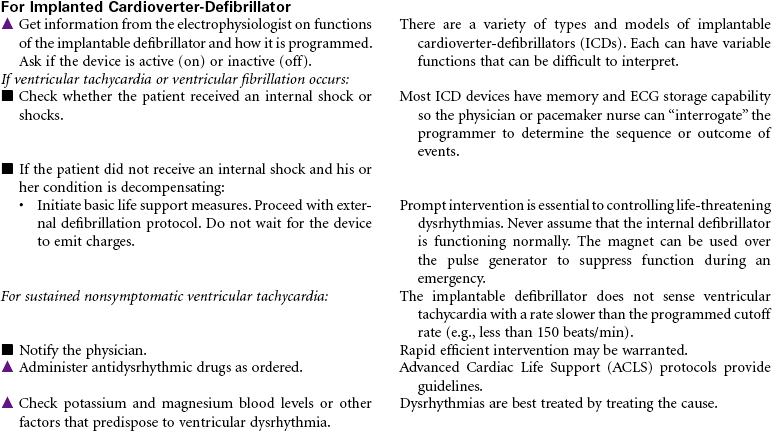
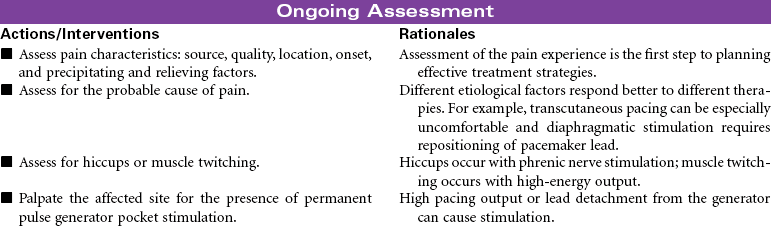
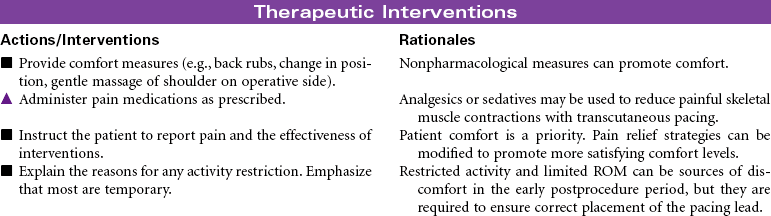
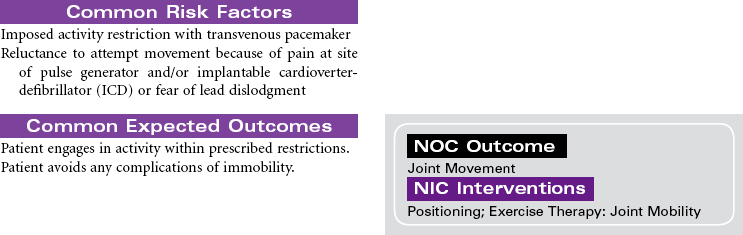
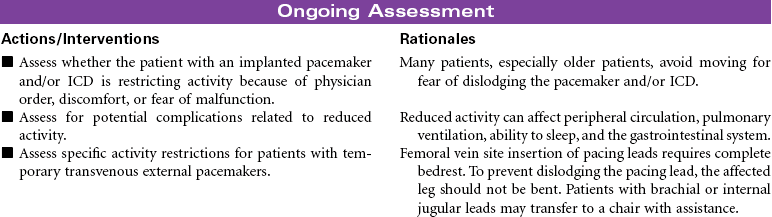
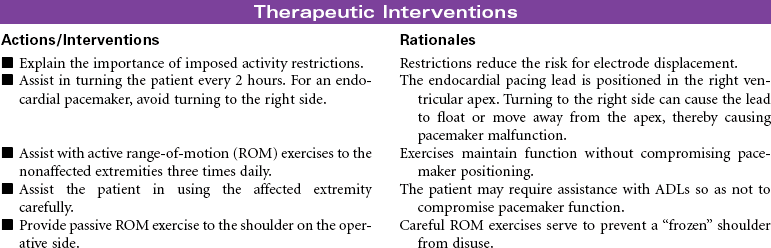
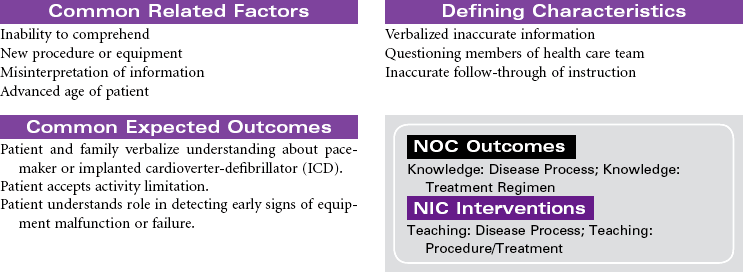
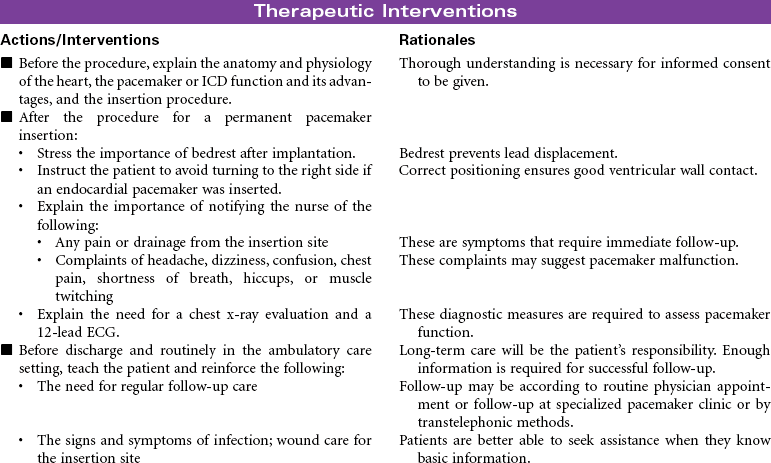
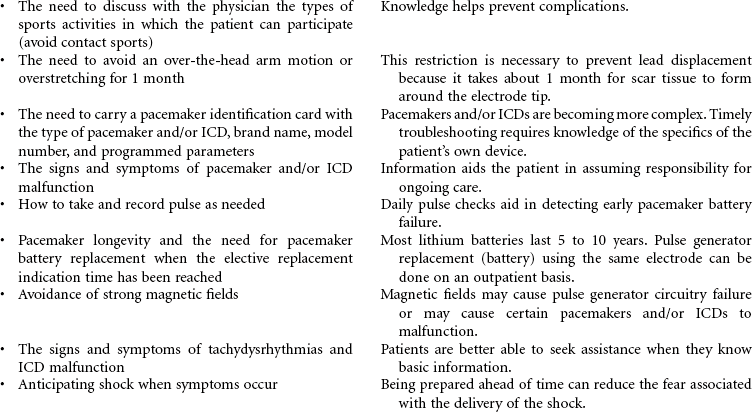
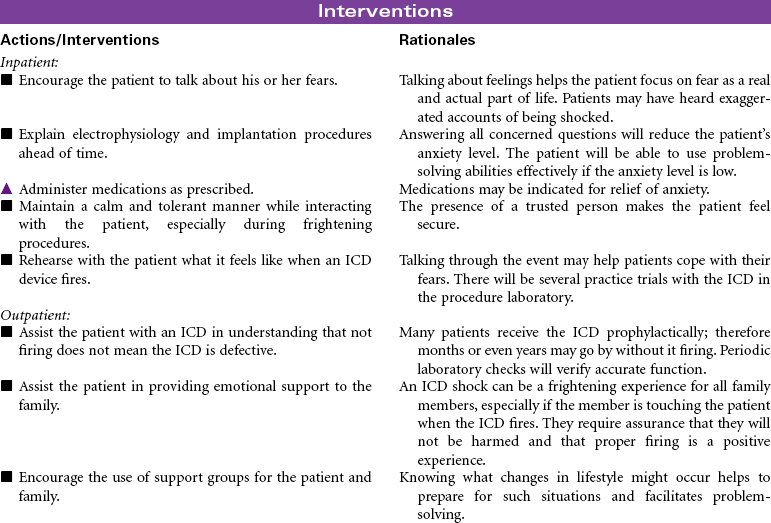
Pacemaker/Cardioverter-Defibrillator
Implantable (Permanent); External Pacemaker (Temporary); Cardioverter-Defibrillator (ICD)
Cardiac rhythm management (CRM) devices is a new term to encompass the spectrum of pacemaker and defibrillation systems now available to treat symptomatic bradydysrhythmias and tachydysrhythmias, terminate lethal dysrhythmias, and improve conduction system abnormalities. The types of pacemakers currently available are as follows:
Bradycardia pacemaker: Its mode of response is inhibited, triggered, or asynchronous. It is indicated for chronic symptomatic bradydysrhythmias or for second- or third-degree atrioventricular (AV) block. A dual-chamber pacemaker is indicated for bradycardia with competent sinus node to provide AV synchrony and rate variability.
Rate-modulated pacemaker: This is indicated for patients who can benefit from an increase in pacing rate, either atrial or ventricular, in response to their body’s metabolic (physiological) needs or to activity (nonphysiological) for increased cardiac output.
Antitachycardia pacemaker: This is indicated for pace-terminable conditions: recurrent supraventricular tachycardia (e.g., AV reciprocating tachydysrhythmias [as in Wolff-Parkinson-White], atrial flutter, and other AV tachydysrhythmias).
Cardiac resynchronization pacemaker: This biventricular pacing system is indicated for severe heart failure and patients with cardiomyopathy with intraventricular conduction delays who can benefit from synchronized septal wall motion and improved left ventricular (LV) contraction.
Seveal options exist for placement of pacemaker leads and generators, depending on whether they are to be used on a permanent or temporary basis. An implantable, permanent pacemaker delivers an electrical stimulus to the heart muscle when needed. Epicardial pacing stimulates the myocardium through one or two pacing electrodes sutured loosely through the epicardial surface of the heart. It is most commonly used after open heart surgery for temporary relief of bradyarrhythmias or for overdrive pacing for tachyarrhythmias. An external pacemaker delivers an electrical stimulus to the heart for the acute management of bradydysrhythmias and certain types of tachydysrhythmias and for use in provocative diagnostic cardiac procedures. One example is the transvenous endocardial pacemaker that directly stimulates the myocardial tissue with electrical current pulses through an electrode catheter inserted through a vein into the right atrium or right ventricle; the pacemaker generator is external to the body. Another example is transcutaneous cardiac pacing (noninvasive) that delivers an electrical current from an external power source through large electrodes applied to the patient’s chest. It is an alternative method to transvenous pacing for the initial management of bradysystolic arrest situations until definitive treatment can be instituted or to overdrive tachydysrhythmias in emergency situations. Cardiac resynchronization pacemakers use transvenous pacing electrodes positioned in the right ventricle and in the coronary sinus (to pace the left ventricle).
An implanted cardioverter-defibrillator (ICD) delivers one or more countershocks (depending on device model) directly to the heart after it recognizes a dysrhythmia through rate-detection criteria. It is a life-prolonging therapy for patients with serious ventricular dysrhythmias. Ongoing randomized controlled trials continue to identify patients most likely to benefit from ICDs. Some of the national recommendations for implantation include: (1) secondary prevention for those who have survived sudden cardiac death caused by the tachydysrhythmias not due to transient or reversible cause and (2) primary prevention in patients with and without ischemic heart disease or cardiomyopathy with an ejection fraction of less than 30%, with New York Heart Association Functional Class II or III symptoms while undergoing optimal medical therapy. After a preset sensing period in which the system detects a lethal dysrhythmia, the defibrillator mechanism delivers a shock (usually 25 J) to the heart muscle. If needed, repeat shocks are delivered. The shock delivered is often described as a hard thump or as a kick to the chest. Most ICDs also contain antitachycardia (overdrive) and antibradycardia (backup pacing) pacemakers.




Percutaneous Balloon Valvuloplasty
Percutaneous balloon valvuloplasty is a procedure that uses a balloon-tipped catheter to dilate the opening of a narrowed valve and split the valve leaflets apart. Valves become stenotic from either congenital defects or acquired diseases. Balloon valvuloplasty is most commonly used to repair mitral and aortic valves in adults. It is indicated for symptomatic patients who no longer respond to medical therapy and for those who are not candidates for valve replacement surgery. It is often used for older patients when surgery poses too great a risk. Successful balloon valvuloplasty may improve the patient’s hemodynamic state sufficiently to reduce the risks associated with valve replacement surgery. This procedure can be performed in a catheterization laboratory under fluoroscopy and without the use of general anesthesia. A percutaneous retrograde approach through the femoral artery is most commonly used for aortic valves. The femoral vein is used in the antegrade approach across the atrial septum to the left atrium for the mitral valve.