28 DYSPNOEA: WHAT TO LOOK FOR
| Dyspnoea: | Difficult, laboured or uncomfortable breathing…the sense of not getting enough air. A symptom, not a sign. |
| Acute dyspnoea: | Dyspnoea arising over the preceding 24–48 hours1. |
| Chronic dyspnoea: | Dyspnoea lasting more than one month2. |
| Golden Rule 1: | The usefulness of the CXR findings — positive or negative — depends on the input derived from the clinical history and the physical examination. |
| Golden Rule 2: | Always tailor your inspection of the CXR to the individual patient…asking the CXR a specific question. |
| Golden Rule 3: | You only see what you look for — you only look for what you know. |
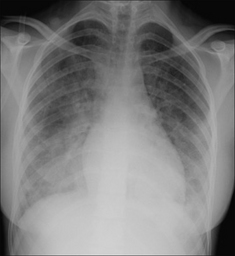
Figure 28.1 Chronic dyspnoea. Extensive alveolar shadowing. Wide differential diagnosis. Apply Golden Rule 1—clinical details are crucial. Known renal failure with fluid retention. CXR conclusion—alveolar pulmonary oedema.
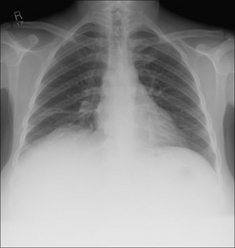
Figure 28.2 Acute dyspnoea. Lungs clear. Both domes of the diaphragm are high. Apply Golden Rule 1—clinical details are crucial. Abdomen is distended with a succussion splash when shaken. CXR conclusion—ascites displacing the diaphragm upwards.

Figure 28.3 Chronic dyspnoea. Shadowing in the right lower zone. Apply Golden Rule 3—you only look for what you know. CXR conclusion—collapse of the right lower lobe.
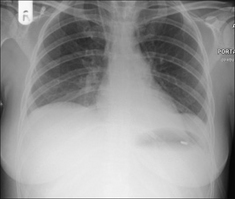
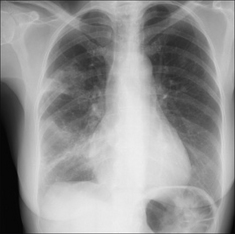
Figure 28.4 Acute dyspnoea. Left dome of the diaphragm appears to be high. Apply Golden Rule 3—you only look for what you know. Note the inferior displacement of the stomach air bubble. CXR conclusion—large subpulmonary effusion, not an elevated dome of the diaphragm (See p. 82).
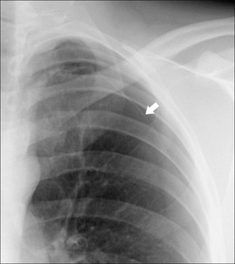
Figure 28.5 Acute dyspnoea. No obvious CXR abnormality. Apply Golden Rule 1—clinical details are crucial. History of left sided pleuritic pain. Apply Golden Rule 2—ask the CXR a specific question…and Golden Rule 3—you only look for what you know. CXR conclusion—careful inspection of the left apex reveals a shallow pneumothorax. The arrow indicates the visceral pleura.
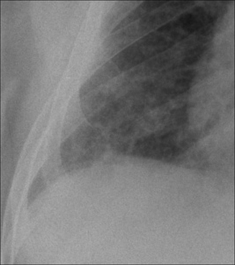
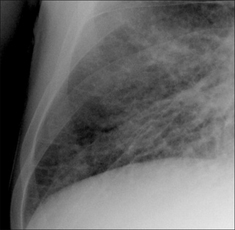
Figure 28.6 Chronic dyspnoea. Apply Golden Rule 3—you only look for what you know. Fine interstitial lines and nodules in the right lower zone. The same appearance was evident in the left lower zone. CXR conclusion—interstitial fibrosis. Subsequently confirmed.
DYSPNOEA—POSSIBLE CAUSES
The clinical history and examination will predict the precise diagnosis in 70–80% of patients presenting with dyspnoea1,3-6. In many instances the CXR findings—normal or abnormal—will confirm or support the pre-test clinical diagnosis (see Chapter 17). On the other hand, the pre-test clinical diagnosis may be uncertain. The physician will know whether the dyspnoea is acute or chronic, and based on this and the clinical findings she needs to compose the question that she wishes the CXR to answer.
 Chronic dyspnoea: are there any features to suggest bronchiectasis? Any evidence of elevated pulmonary venous pressure? Is there any subtle shadowing that would suggest interstitial fibrosis?
Chronic dyspnoea: are there any features to suggest bronchiectasis? Any evidence of elevated pulmonary venous pressure? Is there any subtle shadowing that would suggest interstitial fibrosis?Table 28.1 Acute dyspnoea: pulmonary and cardiac causes.
| Pulmonary disease | ||
| Cardiac disease |
Table 28.2 Acute dyspnoea: other causes.
Table 28.3 Chronic dyspnoea: pulmonary and cardiac causes.
| Pulmonary disease | |
| Cardiac disease |
Table 28.4 Chronic dyspnoea: other causes.
| Anaemia | |
| Neuromuscular… | Weakness of respiratory muscles |
| Thyroid disease… | Hyperthyroidism |
| Deconditioning… | Poor physical condition |
CXR EVALUATION
It is important that the CXR is analysed in a systematic manner in order not to overlook subtle evidence of disease (see p. 10). If you think that the CXR is normal, then take a few more seconds to re-examine or exclude:
DYSPNOEA—CXR IMPACT ON DIAGNOSIS
Sometimes the CXR will provide the precise diagnosis, sometimes it will suggest a possible diagnosis…and a normal CXR will often exclude several diagnoses.
CXR ABNORMAL—DIAGNOSIS CONFIRMED OR DISCLOSED

CXR ABNORMAL—A POSSIBLE DIAGNOSIS IS SUGGESTED
A CXR finding may not be definitive—in terms of diagnosis—but will assist by directing the physician towards a likely possibility.
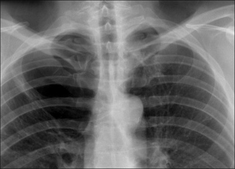
Figure 28.10 Chronic dyspnoea. Large bulla in the right upper zone. COPD suggested as a cause for the dyspnoea.
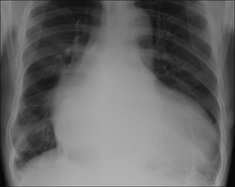
Figure 28.11 Chronic dyspnoea. The heart is enlarged. Cardiac disease suggested as a cause for the dyspnoea.

Figure 28.12 Chronic dyspnoea. The proximal pulmonary arteries are large and the arteries in the mid zones of both lungs are disproportionately smaller. Pulmonary arterial hypertension suggested as the cause for the dyspnoea (see pp. 162–163).
CXR NORMAL…BUT HELPFUL8
An important reminder. A normal CXR does not exclude:
 Pulmonary thromboembolic disease…in many patients pulmonary embolism will be the default diagnosis and this must be excluded or confirmed by utilising other tests (pp. 291–292).
Pulmonary thromboembolic disease…in many patients pulmonary embolism will be the default diagnosis and this must be excluded or confirmed by utilising other tests (pp. 291–292).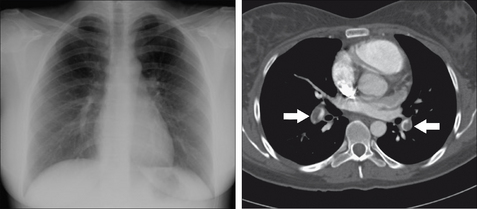
Figure 28.13 Female. Age 24. Acute dyspnoea. Normal CXR. The CT pulmonary angiogram reveals large thrombi in the pulmonary arteries (arrows). Acute pulmonary embolism.
1. Boyars MC, Karnath BM, Mercado AC. Acute dyspnea: a sign of underlying disease. Hosp Physician. 2004;7:23-27.
2. American Thoracic Society. Dyspnea. Mechanisms, assessment, and management: a consensus statement. Am J Respir Crit Care Med. 1999;159:321-340.
3. Mulrow CD, Lucey CR, Farnett LE. Discriminating causes of dyspnea through clinical examination. J Gen Intern Med. 1993;8:383-392.
4. Schmitt BP, Kushner MS, Weiner SL. The diagnostic usefulness of the history of the patient with dyspnea. J Gen Intern Med. 1986;1:386-393.
5. Michelson E, Hollrah S. Evaluation of the patient with shortness of breath: an evidence based approach. Emerg Med Clin North Am. 1999;17:221-237.
6. Wang CS, Fitzgerald JM, Schulzer M, et al. Does this dyspneic patient in the emergency department have congestive heart failure? JAMA. 2005;294:1944-1956.
7. American Thoracic Society. Idiopathic pulmonary fibrosis: diagnosis and treatment. International consensus statement. American Thoracic Society (ATS) and the European Respiratory Society (ERS). Am J Respir Crit Care Med. 2000;161:646-664.
8. Gorry GA, Pauker SG, Schwartz WB. The diagnostic importance of the normal finding. N Engl J Med. 1978;298:486-489.
9. Gudbjerg CE. Roentgenologic diagnosis of bronchiectasis. An analysis of 112 cases. Acta Radiol. 1955;43:210-226.
10. Johnston ID, Prescott RJ, Chalmers JC, et al. British Thoracic Society study of cryptogenic fibrosing alveolitis: current presentation and initial management. Thorax. 1997;52:38-44.