The Health Care Delivery System
• Compare the various methods for financing health care.
• Explain the advantages and disadvantages of managed health care.
• Discuss the types of settings that provide various health care services.
• Discuss the role of nurses in different health care delivery settings.
• Differentiate primary care from primary health care.
• Explain the impact of quality and safety initiatives on delivery of health care.
• Discuss the implications that changes in the health care system have on nursing.
• Discuss opportunities for nursing within the changing health care delivery system.

http://evolve.elsevier.com/Potter/fundamentals/
The U.S. health care system is complex and constantly changing. A broad variety of services are available from different disciplines of health professionals, but gaining access to services is often very difficult for those with limited health care insurance. Uninsured patients present a challenge to health care and nursing because they are more likely to skip or delay treatment for acute and chronic illnesses and die prematurely (Thompson and Lee, 2007). The continuing development of new technologies and medications, which shortens length of stay (LOS), also causes health care costs to increase. Thus health care institutions are managing health care more as businesses than as service organizations. Challenges to health care leaders today include reducing health care costs while maintaining high-quality care for patients, improving access and coverage for more people, and encouraging healthy behaviors (Knickman and Kovner, 2009). Health care providers are discharging patients sooner from hospitals, resulting in more patients needing nursing homes or home care. Often families provide care for their loved ones in the home setting. Nurses face major challenges to prevent gaps in health care across health care settings so individuals remain healthy and well within their own homes and communities.
Nursing is a caring discipline. Values of the nursing profession are rooted in helping people to regain, maintain, or improve health; prevent illness; and find comfort and dignity. The health care system of the new millennium is less service oriented and more business oriented because of cost-saving initiatives, which often causes tension between the caring and business aspects of health care (Knickman and Kovner, 2009). The Institute of Medicine (IOM) (2001) calls for a health care delivery system that is safe, effective, patient centered, timely, efficient, and equitable. The National Priorities Partnership is a group of 28 organizations from a variety of health care disciplines that have joined together to work toward transforming health care (National Priorities Partnership, 2008). The group has set the following national priorities:
• Patient and Family Engagement—Providing patient-centered, effective care
• Population Health—Bringing increased focus on wellness and prevention
• Safety—Eliminating errors whenever and wherever possible
• Care Coordination—Providing patient-centered, high-value care
• Palliative Care—Providing appropriate and compassionate care for patients experiencing advanced illnesses
• Overuse—Reducing waste to achieve effective, affordable care
The Institute of Medicine and Robert Woods Johnson Foundation (2011) put forth a vision for a transformed health care delivery system. The health care system of the future makes quality care accessible to all populations, focuses on wellness and disease prevention, improves health outcomes, and provides compassionate care across the life span. Transformations in health care are changing the practice of nursing. Nursing continues to lead the way in change and retain values for patient care while meeting the challenges of new roles and responsibilities. These changes challenge the nurse to provide evidence-based, compassionate care and continue in the role as patient advocate (Singleton, 2010). According to the IOM (2011) report, nurses need to be transformed by:
• Practicing to the full extent of their education and training.
• Achieving higher levels of education and training through an improved education system that provides seamless progression.
• Becoming full partners, with physicians and other health care providers, in redesigning the health care system.
• Improving data collection and information infrastructure for effective workforce planning and policy making.
Health Care Regulation and Competition
Through most of the twentieth century, few incentives existed for controlling health care costs. Insurers or third-party payers paid for whatever the health care providers ordered for a patient’s care and treatment. As health care costs continued to rise out of control, regulatory and competitive approaches had to control health care spending. The federal government, the biggest consumer of health care, which paid for Medicare and Medicaid, created professional standards review organizations (PSROs) to review the quality, quantity, and cost of hospital care (Sultz and Young, 2006). Medicare-qualified hospitals had physician-supervised utilization review (UR) committees to review the admissions and to identify and eliminate overuse of diagnostic and treatment services ordered by physicians caring for patients on Medicare.
One of the most significant factors that influenced payment for health care was the prospective payment system (PPS). Established by Congress in 1983, the PPS eliminated cost-based reimbursement. Hospitals serving patients who received Medicare benefits were no longer able to charge whatever a patient’s care cost. Instead, the PPS grouped inpatient hospital services for Medicare patients into diagnosis-related groups (DRGs). Each group has a fixed reimbursement amount with adjustments based on case severity, rural/urban/regional costs, and teaching costs. Hospitals receive a set dollar amount for each patient based on the assigned DRG, regardless of the patient’s length of stay or use of services. Most health care providers (e.g., health care networks or managed care organizations) now receive capitated payments. Capitation means that the providers receive a fixed amount per patient or enrollee of a health care plan (Jonas et al., 2007). Capitation aims to build a payment plan for select diagnoses or surgical procedures that consists of the best standards of care at the lowest cost.
Capitation and prospective payment influences the way health care providers deliver care in all types of settings. Many now use DRGs in the rehabilitation setting, and resource utilization groups (RUGs) in long-term care. In all settings health care providers try to manage costs so the organizations remain profitable. For example, when patients are hospitalized for lengthy periods, hospitals have to absorb the portion of costs that are not reimbursed. This simply adds more pressure to ensure that patients are managed effectively and discharged as soon as is reasonably possible. Thus hospitals started to increase discharge planning activities, and hospital lengths of stay began to shorten. Because patients are discharged home as soon as possible, home care agencies now provide complex technological care, including mechanical ventilation and long-term parenteral nutrition.
Managed care describes health care systems in which the provider or health care system receives a predetermined capitated payment for each patient enrolled in the program. In this case the managed care organization assumes financial risk in addition to providing patient care. The focus of care of the organization shifts from individual illness care to prevention, early intervention, and outpatient care. If people stay healthy, the cost of medical care declines. Systems of managed care focus on containing or reducing costs, increasing patient satisfaction, and improving the health or functional status of individuals (Sultz and Young, 2006). Table 2-1 summarizes the most common types of health care insurance plans.
TABLE 2-1
| Type | Definition | Characteristics |
| Managed care organization (MCO) | Provides comprehensive preventive and treatment services to a specific group of voluntarily enrolled people. Structures include a variety of models: Staff model: Physicians are salaried employees of the MCO. Group model: MCO contracts with single group practice Network model: MCO contracts with multiple group practices and/or integrated organizations. Independent practice association (IPA): The MCO contracts with physicians who usually are not members of groups and whose practices include fee-for-service and capitated patients. |
Focus is on health maintenance, primary care. All care is provided by a primary care physician. Referral is needed for access to specialist and hospitalization. It may use capitated payments. |
| Preferred provider organization (PPO) | Type of managed care plan that limits an enrollee’s choice to a list of “preferred” hospitals, physicians, and providers. An enrollee pays more out-of-pocket expenses for using a provider not on the list. | Contractual agreement exists between a set of providers and one or more purchasers (self-insured employers or insurance plans). Comprehensive health services are at a discount to companies under contract. Focus is on health maintenance. |
| Medicare | A federally administrated program by the Commonwealth Fund or the Centers for Medicare and Medicaid Services (CMS); a funded national health insurance program in the United States for people 65 years and older. Part A provides basic protection for medical, surgical, and psychiatric care costs based on diagnosis-related groups (DRGs); also provides limited skilled nursing facility care, hospice, and home health care. Part B is a voluntary medical insurance; covers physician, certain other specified health professional services, and certain outpatient services. Part C is a managed care provision that provides a choice of three insurance plans. Part D is a voluntary Prescription Drug Improvement (Jonas et al, 2007). | Payment for plan is deducted from monthly individual Social Security check. It covers services of nurse practitioners. It does not pay full cost of certain services. Supplemental insurance is encouraged. |
| Medicaid | Federally funded, state-operated program that provides: (1) health insurance to low-income families; (2) health assistance to low-income people with long-term care (LTC) disabilities; and (3) supplemental coverage and LTC assistance to older adults and Medicare beneficiaries in nursing homes. Individual states determine eligibility and benefits. | It finances a large portion of care for poor children, their parents, pregnant women, and disabled very poor adults. It reimburses for nurse-midwifery and other advanced practice nurses (varies by state). It reimburses nursing home funding. |
| Private insurance | Traditional fee-for-service plan. Payment is computed after patient receives services on basis of number of services used. | Policies are typically expensive. Most policies have deductibles that patients have to meet before insurance pays. |
| LTC insurance | Supplemental insurance for coverage of LTC services. Policies provide a set amount of dollars for an unlimited time or for as little as 2 years. | It is very expensive. A good policy has a minimum waiting period for eligibility; payment for skilled nursing, intermediate, or custodial care and home care. |
| State Children’s Health Insurance Programs (SCHIP) | Federally funded, state-operated program to provide health coverage for uninsured children. Individual states determine participation eligibility and benefits. | It covers children not poor enough for Medicaid. |
In 2006 the National Quality Forum defined a list of 28 “Never Events” that are devastating and preventable. Examples of Never Events include patient death or serious injury related to a medication error or the administration of incompatible blood products. In 2007 Medicare ruled it would no longer pay for medical costs associated with these errors. Many states now require mandatory reporting of these events when they occur (Agency for Healthcare Research and Quality Patient Safety Network, n.d.).
Major health care reform came in 2010 with the signing into law of the Patient Protection and Affordable Care Act (Public Law No. 111-148). Health care reform of this magnitude has not occurred in the United States since the 1960s when Medicare and Medicaid were signed into law. The Patient Protection and Affordable Care Act focuses on the major goals of increasing access to health care services for all, reducing health care costs, and improving health care quality. Provisions in the law include insurance industry reforms that increase insurance coverage and decrease costs, increased funding for community health centers, increased primary care services and providers, and improved coverage for children (Adashi et al., 2010; HealthReform.gov, 2010).
Emphasis on Population Wellness
The United States health care delivery system faces many issues such as rising costs, increased access to services, a growing population, and improved quality of outcomes. As a result, the emphasis of the health care industry today is shifting from managing illness to managing health of a community and the environment.
The Health Services Pyramid developed by the Core Functions Project serves as a model for improving the health care of U.S. citizens (Fig. 2-1). The pyramid shows that population-based health care services provide the basis for preventive services. These services include primary, secondary, and tertiary health care. Achievements in the lower tiers of the pyramid contribute to the improvement of health care delivered by the higher tiers. Health care in the United States is moving toward health care practices that emphasize managing health rather than managing illness. The premise is that in the long term, health promotion reduces health care costs. A wellness perspective focuses on the health of populations and the communities in which they live rather than just on finding a cure for an individual’s disease. Life expectancy for Americans is 77.9 years, which has shown a steady increase in the past century. Along with increased life expectancy, adult deaths related to coronary heart disease and stroke continue a long-term decreasing trend, and there is a decreasing trend in deaths of children since 1900 (Centers for Disease Control and Prevention, [CDC], 2007).The reduction in mortality rates has been credited to advancements in sanitation and prevention of infectious diseases (e.g., water, sewage, immunization, and crowded living conditions); patient teaching (e.g., dietary habits, decrease in tobacco use, and blood pressure control); and injury prevention programs (e.g., seat belt restraints, child seats, and helmet laws).
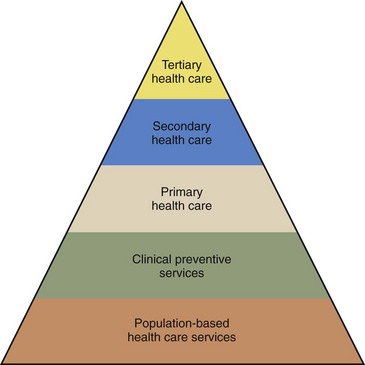
FIG. 2-1 Health services pyramid. (US Public Health Service: The core functions project, Washington, DC, 1994/update 2000, Office of Disease Prevention and Health Promotion. From Stanhope M, Lancaster J: Public health nursing: population-centered health care in the community, ed 7, St. Louis, 2008, Mosby.)
Health Care Settings and Services
Currently the U.S. health care system has five levels of care for which health care providers offer services: disease prevention; health promotion; and primary, secondary, and tertiary health care. The health care settings within which the levels of care are provided include preventive, primary, secondary, tertiary, restorative, and continuing care settings (Box 2-1). Larger health care systems have integrated delivery networks (IDNs) that include a set of providers and services organized to deliver a continuum of care to a population of patients at a capitated cost in a particular setting (Jonas et al., 2007). An integrated system reduces duplication of services across levels or settings of care to ensure that patients receive care in the most appropriate settings.
Changes unique to each setting of care have developed because of health care reform. For example, many health care providers now place greater emphasis on wellness, directing more resources toward primary and preventive care services. Nurses are especially important as patient advocates in maintaining continuity of care throughout the levels of care. They have the opportunity to provide leadership to communities and health care systems. The ability to find strategies that better address patient needs at all levels of care is critical to improving the health care delivery system.
Health care agencies seek accreditation and certification as a way to demonstrate quality and safety in the delivery of care and to evaluate the performance of the organization based on established standards. Accreditation is earned by the entire organization; specific programs or services within an organization earn certifications (The Joint Commission [TJC], 2011). The Joint Commission (formerly The Joint Commission on Accreditation of Healthcare Organizations) accredits health care organizations across the continuum of care, including hospitals and ambulatory care, long-term care, home care, and behavioral health agencies. Other accrediting agencies have a specific focus such as the Commission on Accreditation of Rehabilitation Facilities (CARF) and the Community Health Accrediting Program (CHAP). Disease-specific certifications are available in most all chronic diseases (TJC, 2011). Accreditation and certification survey processes help organizations identify problems and develop solutions to improve the safety and quality of delivered care and services.
Preventive and Primary Health Care
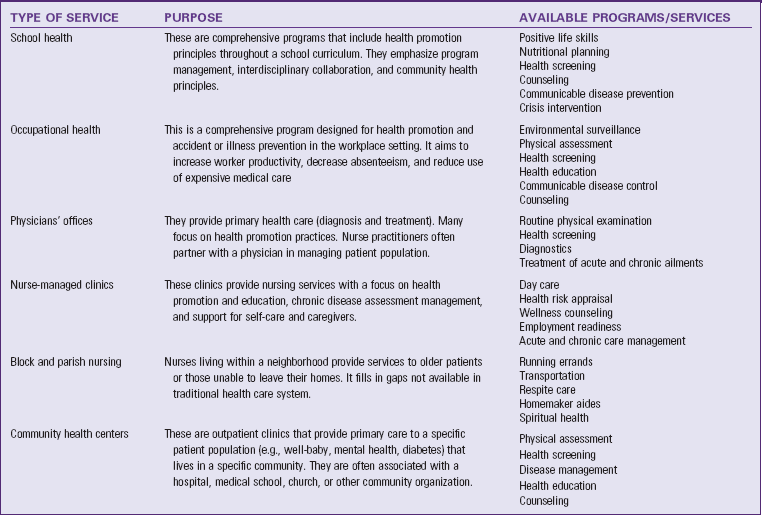
Primary health care focuses on improved health outcomes for an entire population. It includes primary care and health education, proper nutrition, maternal/child health care, family planning, immunizations, and control of diseases. Primary health care requires collaboration among health professionals, health care leaders, and community members. This collaboration needs to focus on improving health care equity, making health care systems person centered, developing reliable and accountable health care leaders, and promoting and protecting the health of communities (WHO, 2008). Successful community-based health programs take societal and environmental factors into consideration when addressing the health needs of communities (WHO, 2008). In settings in which patients receive preventive and primary care such as schools, physician’s offices, occupational health clinics, community health centers, and nursing centers, health promotion is a major theme (Table 2-2). Health promotion programs lower the overall costs of health care by reducing the incidence of disease, minimizing complications, and thus reducing the need to use more expensive health care resources. In contrast, preventive care is more disease oriented and focused on reducing and controlling risk factors for disease through activities such as immunization and occupational health programs. Chapter 3 provides a more comprehensive discussion of primary health care in the community.
Secondary and Tertiary Care
In secondary and tertiary care the diagnosis and treatment of illnesses are traditionally the most common services. With the arrival of managed care, many now deliver these services in primary care settings. Disease management is the most common and expensive service of the health care delivery system. The acutely and chronically ill represent about 20% of the people in the United States, who consume about 80% of health care spending (CDC, 2007). Over 80% of adults 65 years of age have at least one chronic health condition that causes multiple health problems (Missouri Families, 2008).
Uninsured individuals are an increasing problem in health care. The fastest growing age-group of uninsured citizens is young adults between the ages of 19 and 34 (Billings and Cantor, 2009). Young adults turning 19 years of age from low-income families are in danger of being uninsured because of the inability to attend college and find employment with health care benefits. Coverage for young adults is important for various reasons. This age-group has a high incidence of obesity, pregnancy, and human immunodeficiency virus (HIV). People in this age-group are also less likely to see a doctor on a regular basis and follow up on a problem if they do not have health insurance. Lack of insurance rates varies by race. Statistics show that 34% of Hispanics, 19% of African Americans, and 10% of the white or Caucasian population do not have health insurance (CDC, 2010).
People who do not have health care insurance often wait longer before presenting for treatment; thus they are usually sicker and need more health care. As a result, secondary and tertiary care (also called acute care) is more costly. With the arrival of more advanced technology and managed care, physicians now perform simple surgeries in office surgical suites instead of in the hospital. Cost to the patient is lower in the office because the general overhead cost of the facility is lower.
Hospitals
Hospital emergency departments, urgent care centers, critical care units, and inpatient medical-surgical units provide secondary and tertiary levels of care. Quality, safe care is the focus of most acute care organizations; satisfaction with health care services is important to them. Patient satisfaction becomes a priority in a busy, stressful location such as the inpatient nursing unit. Patients expect to receive courteous and respectful treatment, and they want to be involved in daily care decisions. As a nurse, you play a key role in bringing respect and dignity to the patient (Vlasses and Smeltzer, 2007). Acute care nurses need to be responsive to learning patient needs and expectations early to form effective partnerships that ultimately enhance the level of nursing care given.
Because of managed care, the number of days patients can expect to be hospitalized is limited based on their DRGs on admission. Therefore nurses need to use resources efficiently to help patients successfully recover and return home. To contain costs, many hospitals have redesigned nursing units. Because of work redesign, more services are available on nursing units, thus minimizing the need to transfer and transport patients across multiple diagnostic and treatment areas.
Hospitalized patients are acutely ill and need comprehensive and specialized tertiary health care. The services provided by hospitals vary considerably. Some small rural hospitals offer only limited emergency and diagnostic services and general inpatient services. In comparison, large urban medical centers offer comprehensive, up-to-date diagnostic services, trauma and emergency care, surgical intervention, intensive care units (ICUs), inpatient services, and rehabilitation facilities. Larger hospitals also offer professional staff from a variety of specialties such as social service, respiratory therapy, physical and occupational therapy, and speech therapy. The focus in hospitals is to provide the highest quality of care possible so patients are discharged early but safely to home or another health care facility that will adequately manage remaining health care needs.
Discharge planning begins the moment a patient is admitted to a health care facility. Nurses play an important role in discharge planning in the hospital, where continuity of care is important. To achieve continuity of care, nurses use critical thinking skills and apply the nursing process (see Unit 3). To anticipate and identify the patient’s needs, nurses work with all members of the interdisciplinary health care team. They take the lead to develop a plan of care that moves the patient from the hospital to another level of health care such as the patient’s home or a nursing home. Discharge planning is a centralized, coordinated, interdisciplinary process that ensures that the patient has a plan for continuing care after leaving a health care agency.
Because patients leave hospitals as soon as their physical conditions allow, they often have continuing health care needs when they go home or to another facility. For example, a surgical patient requires wound care at home after surgery. A patient who has had a stroke requires ambulation training. Patients and families worry about how they will care for unmet needs and manage over the long term. Nurses help by anticipating and identifying patients’ continuing needs before the actual time of discharge and by coordinating health care team members in achieving an appropriate discharge plan.
Some patients are more in need of discharge planning because of the risks they present (e.g., patients with limited financial resources, limited family support, and long-term disabilities or chronic illness). However, any patient who is being discharged from a health care facility with remaining functional limitations or who has to follow certain restrictions or therapies for recovery needs discharge planning. All caregivers who care for a patient with a specific health problem participate in discharge planning. The process is truly interdisciplinary. For example, patients with diabetes visiting a diabetes management center requires the group effort of a diabetes nurse educator, dietitian, and physician to ensure that they return home with the right information to manage their condition. A patient who has experienced a stroke will not be discharged from a hospital until the team has established plans with physical and occupational therapists to begin a program of rehabilitation.
Effective discharge planning often requires referrals to various health care disciplines. In many agencies a health care provider’s order is necessary for a referral, especially when planning specific therapies (e.g., physical therapy). It is best to have patients and families participate in referral processes so they are involved early in any necessary decision making. Some tips on making the referral process successful include the following:
• Make a referral as soon as possible.
• Give the care provider receiving the referral as much information about the patient as possible. This avoids duplication of effort and exclusion of important information.
• Involve the patient and family in the referral process, including selecting the necessary referral. Explain the service that the referral will provide, the reason for the referral, and what to expect from the services of the referral.
• Determine what the referral discipline recommends for the patient’s care and include this in the treatment plan as soon as possible.
The nurse provides resources to improve the long-term outcomes of patients with limitations. Discharge planning depends on comprehensive patient and family education (see Chapter 25). Patients need to know what to do when they get home, how to do it, and for what to observe when problems develop. Patients require the following instruction before they leave health care facilities:
• Safe and effective use of medications and medical equipment
• Instruction in potential food-drug interactions and counseling on nutrition and modified diets
• Rehabilitation techniques to support adaptation to and/or functional independence in the environment
• Access to available and appropriate community resources
• When and how to obtain further treatment
• The patient’s and family’s responsibilities in the patient’s ongoing health care needs and the knowledge and skills needed to carry out those responsibilities
• When to notify their health care provider for changes in functioning or new symptoms
Intensive Care
An ICU or critical care unit is a hospital unit in which patients receive close monitoring and intensive medical care. ICUs have advanced technologies such as computerized cardiac monitors and mechanical ventilators. Although many of these devices are on regular nursing units, the patients hospitalized within ICUs are monitored and maintained on multiple devices. Nursing and medical staff have special knowledge about critical care principles and techniques. An ICU is the most expensive health care delivery site because each nurse usually cares for only one or two patients at a time and because of all the treatments and procedures the patients in the ICU require.
Psychiatric Facilities
Patients who suffer emotional and behavioral problems such as depression, violent behavior, and eating disorders often require special counseling and treatment in psychiatric facilities. Located in hospitals, independent outpatient clinics, or private mental health hospitals, psychiatric facilities offer inpatient and outpatient services, depending on the seriousness of the problem. Patients enter these facilities voluntarily or involuntarily. Hospitalization involves relatively short stays with the purpose of stabilizing patients before transfer to outpatient treatment centers. Patients with psychiatric problems receive a comprehensive multidisciplinary treatment plan that involves them and their families. Medicine, nursing, social work, and activity therapy work together to develop a plan of care that enables patients to return to functional states within the community. At discharge from inpatient facilities, patients usually receive a referral for follow-up care at clinics or with counselors.
Rural Hospitals
Access to health care in rural areas has been a serious problem. Most rural hospitals have experienced a severe shortage of primary care providers. Many have closed because of economic failure. In 1989 the Omnibus Budget Reconciliation Act (OBRA) directed the U.S. Department of Health and Human Services (USDHHS) to create a new health care organization, the rural primary care hospital (RPCH). The Balanced Budget Act of 1997 changed the designation for rural hospitals to Critical Access Hospital (CAH) if certain criteria were met (American Medical Association, 2009). A CAH is located in a rural area and provides 24-hour emergency care, with no more than 25 inpatient beds for providing temporary care for 96 hours or less to patients needing stabilization before transfer to a larger hospital. Physicians, nurse practitioners, or physician assistants staff a CAH. The CAH provides inpatient care to acutely ill or injured people before transferring them to better-equipped facilities. Basic radiological and laboratory services are also available.
With health care reform, more big-city health care systems are branching out and establishing connections or mergers with rural hospitals. The rural hospitals provide a referral base to the larger tertiary care medical centers. With the development of advanced technologies such as telemedicine, rural hospitals have increased access to specialist consultations. Nurses who work in rural hospitals or clinics require competence in physical assessment, clinical decision making, and emergency care. Having a culture of evidence-based practice is important in rural hospitals so nurses practice using the best evidence to achieve optimal patient outcomes (Burns et al., 2009). Advanced practice nurses (e.g., nurse practitioners and clinical nurse specialists) use medical protocols and establish collaborative agreements with staff physicians.
Restorative Care
Patients recovering from an acute or chronic illness or disability often require additional services to return to their previous level of function or reach a new level of function limited by their illness or disability. The goals of restorative care are to help individuals regain maximal functional status and enhance quality of life through promotion of independence and self-care. With the emphasis on early discharge from hospitals, patients usually require some level of restorative care. For example, some patients require ongoing wound care and activity and exercise management until they have recovered enough following surgery to independently resume normal activities of daily living.
The intensity of care has increased in restorative care settings because patients leave hospitals earlier. The restorative health care team is an interdisciplinary group of health professionals and includes the patient and family or significant others. In restorative settings nurses recognize that success depends on effective and early collaboration with patients and their families. Patients and families require a clear understanding of goals for physical recovery, the rationale for any physical limitations, and the purpose and potential risks associated with therapies. Patients and families are more likely to follow treatment plans and achieve optimal functioning when they are involved in restorative care.
Home Health Care (Home Care)
Home care is the provision of medically related professional and paraprofessional services and equipment to patients and families in their homes for health maintenance, education, illness prevention, diagnosis and treatment of disease, palliation, and rehabilitation. Nursing is one service most patients use in home care. However, home care also includes medical and social services; physical, occupational, speech, and respiratory therapy; and nutritional therapy. These services usually occur once or twice a day for as long as 7 days a week. A home care service also coordinates the access to and delivery of home health equipment, or durable medical equipment, which is any medical product adapted for home use.
Health promotion and education are traditionally the primary objectives of home care, yet at present most patients receive home care because they need nursing or medical care. Examples of home nursing care include monitoring vital signs; assessment; administering parenteral or enteral nutrition, medications, and IV or blood therapy; and wound or respiratory care. The focus is on patient and family independence. Nurses address recovery and stabilization of illness in the home and identify problems related to lifestyle, safety, environment, family dynamics, and health care practices.
Approved home care agencies usually receive reimbursement for services from the government (such as Medicare and Medicaid in the United States), private insurance, and private pay. The government has strict regulations that govern reimbursement for home care services. An agency cannot simply charge whatever it wants for a service and expect to receive full reimbursement. Government programs set the cost of reimbursement for most professional services.
Nurses in home care provide individualized care. They have a caseload and assist patients in adapting to permanent or temporary physical limitations so they are able to assume a more normal daily home routine. Home care requires a strong knowledge base in many areas such as family dynamics (see Chapter 10), cultural practices (see Chapter 9), spiritual values (see Chapter 35), and communication principles (see Chapter 24).
Rehabilitation
Rehabilitation restores a person to the fullest physical, mental, social, vocational, and economic potential possible. Patients require rehabilitation after a physical or mental illness, injury, or chemical addiction. Specialized rehabilitation services such as cardiovascular, neurological, musculoskeletal, pulmonary, and mental health rehabilitation programs help patients and families adjust to necessary changes in lifestyle and learn to function with the limitations of their disease. Drug rehabilitation centers help patients become free from drug dependence and return to the community.
Rehabilitation services include physical, occupational, and speech therapy and social services. Ideally rehabilitation begins the moment a patient enters a health care setting for treatment. For example, some orthopedic programs now have patients perform physical therapy exercises before major joint repair to enhance their recovery after surgery. Initially rehabilitation usually focuses on the prevention of complications related to the illness or injury. As the condition stabilizes, rehabilitation helps to maximize the patient’s functioning and level of independence.
Rehabilitation occurs in many health care settings, including special rehabilitation agencies, outpatient settings, and the home. Frequently patients needing long-term rehabilitation (e.g., patients who have had strokes and spinal cord injuries) have severe disabilities affecting their ability to carry out the activities of daily living. When rehabilitation services occur in outpatient settings, patients receive treatment at specified times during the week but live at home the rest of the time. Health care providers apply specific rehabilitation strategies to the home environment. Nurses and other members of the health care team visit homes and help patients and families learn to adapt to illness or injury.
Extended Care Facilities
An extended care facility provides intermediate medical, nursing, or custodial care for patients recovering from acute illness or those with chronic illnesses or disabilities. Extended care facilities include intermediate care and skilled nursing facilities. Some include long-term care and assisted living facilities. At one point extended care facilities primarily cared for older adults. However, because hospitals discharge their patients sooner, there is a greater need for intermediate care settings for patients of all ages. For example, health care providers transfer a young patient who has experienced a traumatic brain injury resulting from a car accident to an extended care facility for rehabilitative or supportive care until discharge to the home becomes a safe option.
An intermediate care or skilled nursing facility offers skilled care from a licensed nursing staff. This often includes administration of IV fluids, wound care, long-term ventilator management, and physical rehabilitation. Patients receive extensive supportive care until they are able to move back into the community or into residential care. Extended care facilities provide around-the-clock nursing coverage. Nurses who work in a skilled nursing facility need nursing expertise similar to that of nurses working in acute care inpatient settings, along with a background in gerontological nursing principles (see Chapter 14).
Continuing Care
Continuing care describes a variety of health, personal, and social services provided over a prolonged period. These services are for people who are disabled, who were never functionally independent, or who suffer a terminal disease. The need for continuing health care services is growing in the United States. People are living longer, and many of those with continuing health care needs have no immediate family members to care for them. A decline in the number of children families choose to have, the aging of care providers, and the increasing rates of divorce and remarriage complicate this problem. Continuing care is available within institutional settings (e.g., nursing centers or nursing homes, group homes, and retirement communities), communities (e.g., adult day care and senior centers), or the home (e.g., home care, home-delivered meals, and hospice) (Meiner, 2011).
Nursing Centers or Facilities
The language of long-term care is confusing and constantly changing. The nursing home has been the dominant setting for long-term care (Meiner, 2011). With the 1987 OBRA, the term nursing facility became the term for nursing homes and other facilities that provided long-term care. Now nursing center is the most appropriate term. A nursing center typically provides 24-hour intermediate and custodial care such as nursing, rehabilitation, dietary, recreational, social, and religious services for residents of any age with chronic or debilitating illnesses. In some cases patients stay in nursing centers for room, food, and laundry services only. Most persons living in nursing centers are older adults. A nursing center is a resident’s temporary or permanent home, with surroundings made as homelike as possible (Sorrentino, 2007). The philosophy of care is to provide a planned, systematic, and interdisciplinary approach to nursing care to help residents reach and maintain their highest level of function (Resnick and Fleishell, 2002).
According to the U.S. Bureau of the Census, just over 5% of people 65 years of age and older live in nursing centers and other facilities (Missouri Families, 2008). The nursing center industry is one of the most highly regulated industries in the United States. These regulations have raised the standard of services provided (Box 2-2). One regulatory area that deserves special mention is that of resident rights. Nursing facilities have to recognize residents as active participants and decision makers in their care and life in institutional settings (Meiner, 2011). This also means that family members are active partners in the planning of residents’ care.
Box 2-2
Major Regulatory Requirements Defined by the 1987 Omnibus Budget Reconciliation Act
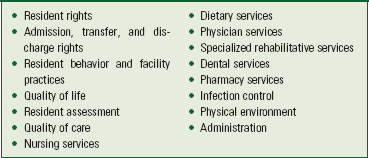
From Health Care Financing Administration, Department of Health and Human Services: Requirements for states and long-term care facilities, 42 CFR 483 Subpart B (483.1-75), October 1, 2004. http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&tpl=/ecfrbrowse/Title42/42cfr483_main_02.tpl. Accessed June 18, 2011.
Interdisciplinary functional assessment of residents is the cornerstone of clinical practice within nursing centers (Meiner, 2011). Government regulations require that staff comprehensively assess each resident and make care planning decisions within a prescribed period. A resident’s functional ability (e.g., ability to perform activities of daily living) and long-term physical and psychosocial well-being are the focus. Staff must complete the Resident Assessment Instrument (RAI) on all residents. The RAI consists of the Minimum Data Set (MDS) (Box 2-3), Resident Assessment Protocols, and utilization guidelines of each state. The RAI provides a national database for nursing facilities so policy makers will better understand the health care needs of the long-term care population. The MDS is a rich resource for nurses in determining the best interventions to support the health care needs of this growing population.
Assisted Living
Assisted living is one of the fastest growing industries within the United States. There are approximately 38,000 assisted living facilities that house more than 975,000 people in the United States (National Center for Assisted Living [NCLA], 2010). Assisted living offers an attractive long-term care setting with an environment more like home and greater resident autonomy. Residents require some assistance with activities of daily living but remain relatively independent within a partially protective setting. A group of residents live together, but each resident has his or her own room and shares dining and social activity areas. Usually people keep all of their personal possessions in their residences. Facilities range from hotel-like buildings with hundreds of units to modest group homes that house a handful of seniors. Assisted living provides independence, security, and privacy all at the same time (Ebersole et al., 2008). These facilities promote physical and psychosocial health (Fig. 2-2). Services in an assisted living facility include laundry, assistance with meals and personal care, 24-hour oversight, and housekeeping (NCAL, 2010). Some facilities provide assistance with medication administration. Nursing care services are not always directly available, although home care nurses can visit patients in assisted living facilities. Unfortunately most residents of assisted living facilities pay privately. The average monthly fee is $3022 for a private unit (NCAL, 2010). With no government fee caps and little regulation, assisted living is not always an option for individuals with limited financial resources.

Respite Care
The need to care for family members within the home creates great physical and emotional problems for family caregivers, especially if the people for whom they care have either physical or cognitive limitations. The family caregiver usually not only has the responsibility for providing care to a loved one but often has to maintain a full-time job, raise a family, and manage the routines of daily living as well. Respite care is a service that provides short-term relief or “time off” for people providing home care to an ill, disabled, or frail older adult (Meiner, 2011). Respite care is offered in the home, a day care setting, or a health care institution that provides overnight care. The family caregiver is able to leave the home for errands or some social time while a responsible person stays in the home to care for the loved one. There are few formal respite care programs in the United States because of cost. Currently Medicare does not cover respite care, and Medicaid has strict requirements for services and eligibility (Sultz and Young, 2006).
Adult Day Care Centers
Adult day care centers provide a variety of health and social services to specific patient populations who live alone or with family in the community. Services offered during the day allow family members to maintain their lifestyles and employment and still provide home care for their relatives (Meiner, 2011). Day care centers are associated with a hospital or nursing home or exist as independent centers. Frequently the patients need continuous health care services (e.g., physical therapy or counseling) while their families or support persons work. The centers usually operate 5 days per week during typical business hours and usually charge on a daily basis. Adult day care centers allow patients to retain more independence by living at home, thus potentially reducing the costs of health care by avoiding or delaying an older adult’s admission to a nursing center. Nurses working in day care centers provide continuity between care delivered in the home and the center. For example, nurses ensure that patients continue to take prescribed medication and administer specific treatments. Knowledge of community needs and resources is essential in providing adequate patient support (Ebersole et al., 2008).
Hospice
A hospice is a system of family-centered care that allows patients to live and remain at home with comfort, independence, and dignity while easing the pains of terminal illness. The focus of hospice care is palliative care, not curative treatment (see Chapter 43). The interdisciplinary team in the hospice works continuously with the patient’s health care provider to develop and maintain a patient-directed individualized plan of care. Many hospice programs provide respite care, which is important in maintaining the health of the primary caregiver and family.
Issues in Health Care Delivery
The climate in health care today influences both health care professionals and consumers. Because those who provide patient care are the most qualified to make changes in the health care delivery system, nurses need to participate fully and effectively within all aspects of health care. As nursing faces issues of how to maintain health care quality while reducing costs, nurses need to acquire the knowledge, skills, and values necessary to practice competently and effectively. It will also become more important than ever before to collaborate with other health care professionals to design new approaches for patient care delivery.
Nursing Shortage
There are more than 3.1 million nurses in the United States, making nursing the largest health care profession in the country (American Association of Colleges of Nursing [AACN], 2011). Although nearly 57% of the nurses work in medical-surgical hospitals, they are involved in delivering health care at all levels, including primary and preventive care (AACN, 2011). In spite of the large number of practicing nurses, a critical shortage of nurses is projected in the United States. It is expected that this shortage will worsen with increased need for health care services by the aging baby-boomer generation (AACN, 2010). It is estimated that over 500,000 new nursing positions will be created by 2018, resulting in a 22% increase in the size of the nursing workforce (U.S. Department of Labor, 2009). The economic climate and recession had brought about an easing of the nursing shortage (Buerhaus et al., 2009). This easing is not expected to last, mainly because of the aging nursing workforce and potential retirements. The average age of nurses is projected to be 44.5 years by 2012 (AACN, 2010). One other factor contributing to the shortage is the slow growth in nursing school enrollments, often because of nursing faculty shortages, space limitations, and clinical site availability (AACN, 2010; Buerhaus et al., 2009). Buerhaus et al. (2009) estimate that by 2025 the shortage will grow to 260,000 nurses.
Competency
The Pew Health Professions Commission, a national and interdisciplinary group of health care leaders, recommended 21 competencies for health care professionals in the twenty-first century (Pew Health Professions Commission, 1998). The competencies emphasize the importance of public service, caring for the health of communities, and developing ethically responsible behaviors. In addressing the continued challenge facing the health care system, the IOM (2001) identified five interrelated competencies that are essential for all health care workers in the twenty-first century (Box 2-4). Shifts to an emphasis on prevention and management place increased importance on the competencies of care management and coordination, patient education, public health, and transitional care (IOM, 2011). The IOM also identified 10 important rules of performance for a health care system to follow to better meet patient needs (Box 2-5) (IOM, 2003).
The health care practitioner competencies are an excellent tool for measuring how well a nurse practices nursing and serve as a guide for the development of a professional nursing career. A consumer of health care expects that the standards of nursing care and practice in any health care setting are appropriate, safe, and efficacious. Health care organizations ensure quality care by establishing policies, procedures, and protocols that are evidence based and follow national accrediting standards. A nurse’s responsibility is to follow policies and procedures and know the most current practice standards. Ongoing competency is a nurse’s responsibility. It is also the nurse’s responsibility to obtain necessary continuing education, follow an established code of ethics, and earn certifications in specialty areas (Jordan et al., 2008). Development of a professional practice portfolio that shows learning activities and professional accomplishments is one way to show competency in nursing (Scott-Tilley, 2008).
Evidence-Based Practice
As professionals, nurses are challenged to stay familiar with new information to provide the highest quality of patient care. Nursing practice is dynamic and always changing because of new information coming from research studies, practice trends, technological development, and social issues affecting patients. Nurses need to analyze new knowledge to make sound and informed decisions about patient care (Kotzer and Arellana, 2008). Evidence-based practice is a problem-solving approach to clinical practice that involves the conscientious use of current best evidence, along with clinical expertise and patient preferences and values in making decisions about patient care (Melnyk and Fineout-Overholt, 2010). Evidence-based practice, research-based practice, and best practice are terms that are often used interchangeably. However, research-based practice refers to the use of knowledge based on the results of research studies; whereas evidence-based practice adds a nurse’s clinical experience, practice trends, and patient preferences (Melnyk and Fineout-Overholt, 2010). Chapter 5 offers a thorough review of evidence-based practice.
Quality and Safety in Health Care
Nursing plays an important role in quality and safety in health care (Box 2-6). Quality health care is the “degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge” (IOM, 2001). Safety is a critical part of quality health care (Tzeng and Yin, 2007). The National Quality Forum (NQF) (2010) identified 34 health care practices, organized in seven functional areas that improve patient safety by decreasing the occurrence of adverse events. Examples of NQF practices include hand hygiene, teamwork, training, influenza prevention, catheter-associated urinary tract infection prevention, fall prevention, and medication reconciliation (NQF, 2010). Health care providers define the quality of their services by measuring health care outcomes that show how a patient’s health status has changed. Examples of outcomes that are monitored are readmission rates for patients who have had surgery, functional health status of patients after discharge (e.g., ability and time frame for returning to work), and the rate of infection after surgery. Nurses play an important role in gathering and analyzing quality outcome data. Within a rural hospital setting, knowledge of the rural culture and connectedness to the community are unique features related to quality care (Baernholdt et al., 2010).
Pay for performance programs and public reporting of hospital quality data are designed to promote quality, effective, and safe patient care by physicians and health care organizations. These programs are quality improvement strategies that reward excellence through financial incentives to motivate change to achieve measurable improvements (Lindenauer et al., 2007). Nurses play an important role in helping hospitals meet the measure for quality, efficiency, and patient satisfaction (Lutz and Root, 2007). They are often the health care provider who ensures that performance measures occur. For example, one performance measure is the standard that any patient admitted with a possible myocardial infarction receives an aspirin. In an acute care setting a nurse is the one who obtains an order for the aspirin and ensures that the patient receives it in a timely manner (Bodrock and Mion, 2008). Research shows that financial incentives modestly increase quality improvement efforts in hospitals that do public reporting (Lindenauer et al., 2007). Some health care organizations use balanced scorecards to report data on their key performance indicators. These scorecards are reported publicly so health care consumers can use the information when choosing health care services.
More and more health care institutions are focused on improving processes as a way to improve quality and safety. Many use strategies such as Six Sigma, Lean Six Sigma, or Value Stream Analysis. Six Sigma is a data-driven approach to process improvement that reduces variation in process. It is a measure of quality (isixsigma, 2010). For example, a nursing unit sets up a project to collect data on the process of administering the first dose of an ordered chemotherapy. The audit reveals delays in getting the drug from the pharmacy to the nursing unit. Using Six Sigma, the collected data are analyzed, and unnecessary steps in the process are identified. On the basis of this analysis the process is streamlined to decrease time from ordering to administration. Lean Six Sigma and value stream analysis are two other methods that focus on improvement of processes through studying each step of a process to determine if the step adds value and reduces the health care organization’s time, costs, and resources (Burger, 2008; Carey, 2010). The aim of both is to eliminate unnecessary, nonvalue-added costly steps to reduce waste.
Health plans throughout the United States rely on the Healthcare Effectiveness Data and Information Set (HEDIS) as a quality measure. The National Committee for Quality Assurance (NCQA) created HEDIS to collect various data to measure the quality of care and services provided by different health plans. It is the database of choice for the Centers for Medicare and Medicaid Services (CMS). HEDIS compares how well health plans perform on 71 measures across eight domains of care in the key areas of quality and effectiveness of care, access to care, and patient satisfaction with the health plan and doctors (NCQA, 2010). For accreditation purposes The Joint Commission requires health care organizations to determine how well an organization meets patient needs and expectations. Organizations are using outcomes such as patient satisfaction to redesign how they manage and deliver care in hopes of improving quality in the long term.
Patient Satisfaction
Every major health care organization measures certain aspects of patient satisfaction. The Hospital Consumer of Assessment of Healthcare Providers and Systems (HCAHPS) is a standardized survey developed to measure patient perceptions of their hospital experience (HCAHPS, 2010). HCAHPS was developed by the CMS and the Agency for Healthcare Research and Quality as a way for hospitals to collect and report data publicly for comparison purposes. The survey is administered to a randomly selected sample of adults who were discharged from a hospital between 48 hours and 6 weeks ago. The survey has 27 questions that ask patients to respond about communication with nurses and physicians, responsiveness of hospital staff, pain management, communication about medications, discharge planning, cleanliness and quietness of the environment, overall satisfaction, and willingness to recommend the hospital (HCAHPS, 2010). Nursing environments affect HCAHPS scores. Research found that hospitals that improved the nursing work environment and lowered nurse-patient ratios by one patient had higher patient satisfaction levels and patients who were more likely to recommend the hospital to others (Kutney-Lee et al., 2009).
The Picker Institute identified eight dimensions of patient-centered care (Box 2-7) that most affect patients’ experiences with health care. The eight dimensions cover most of the scope of nursing practice. This is not a surprise because nurses are involved in almost every aspect of a patient’s care in a hospital. A close look shows that many of the aspects reflected in patient satisfaction apply to almost any health care setting.
The survey tool from The Picker Institute measures patient satisfaction along the eight dimensions. The survey looks globally at patient perceptions of care in an attempt to understand how all hospital departments influence patient satisfaction. The program mails surveys to patients after they leave a health care setting. Many other companies have developed similar patient satisfaction surveys that are distributed in the mail to patients. Staff involved in patient care receive the satisfaction scores as feedback regarding their success in meeting patient expectations. The nursing staff is responsible for identifying unique issues that influence patient satisfaction on their unit. For example, nurses working on an oncology unit have different patient satisfaction issues around physical comfort than nurses caring for new mothers. Patient satisfaction findings become the basis for many quality improvement studies.
It is important for nurses to recognize the need to provide patient- and family-centered care. Identifying patient and family expectations, knowledge, preferences, cultural beliefs, and values is an important part of patient-centered care (Cronenwett et al., 2007; Institute for Patient- and Family-Centered Care [IPFCC], 2010). Concepts of patient-centered care include respect and dignity, sharing of information, participation in care and care decisions, and collaboration (IPFCC, 2010). By learning early what a patient expects with regard to information, comfort, and availability of family and friends, nurses are able to better plan patient care. They should ask about the patient’s expectations when the patient first enters a health care setting, while care continues, and when a patient is discharged. Patient expectations are an important measure of the evaluation of nursing care. A Patient and Family Advisory Council is one strategy that is effective in obtaining patient and family feedback to develop patient- and family-centered care (Zarubi et al., 2008).
Magnet Recognition Program
The American Nurses Credentialing Center (ANCC) established the Magnet Recognition Program to recognize health care organizations that achieve excellence in nursing practice (ANCC, 2010c). In the United States approximately 6.4% of health care organizations have achieved Magnet status (ANCC, 2010b). Health care organizations that apply for Magnet status must demonstrate quality patient care, nursing excellence, and innovations in professional practice. The professional work environment must allow nurses to practice with a sense of empowerment and autonomy to deliver quality nursing care. The revised Magnet model has five components that are affected by global issues that are challenging nursing today (ANCC, 2010a) (Box 2-8). The five components are Transformational Leadership; Structural Empowerment; Exemplary Professional Practice; New Knowledge, Innovation, and Improvements; and Empirical Quality Results. Institutions achieve Magnet status through an appraisal process that requires them to present evidence showing achievement of the 14 forces of magnetism (see Box 2-8). Magnet status requires nurses to collect data on specific nursing-sensitive quality indicators or outcomes and compare their outcomes against a national, state, or regional database to demonstrate quality of care.
Box 2-8
Magnet Model and Forces of Magnetism
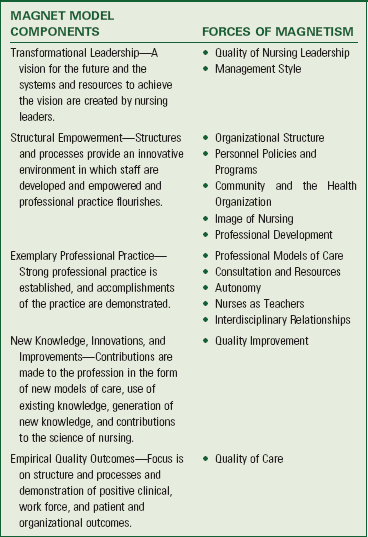
Adapted from American Nurses Credentialing Center: A new model for ANCC’s Magnet Recognition Program, 2010a, http://www.nursecredentialing.org/Magnet/ProgramOverview/NewMagnetModel.aspx.
Nursing-Sensitive Outcomes
Nursing-sensitive outcomes are patient outcomes and select nursing workforce characteristics that are directly related to nursing care such as changes in patients’ symptom experiences, functional status, safety, psychological distress, registered nurse (RN) job satisfaction, total nursing hours per patient day, and costs. Nurses assume accountability and responsibility for achieving and accepting the consequences of these outcomes. The National Database of Nursing Quality Indicators (NDNQI) was developed by the American Nurses Association to measure and evaluate nursing-sensitive outcomes with the purpose of improving patient safety and quality care (NDNQI, 2010) (Box 2-9). The NDNQI reports quarterly results on nursing outcomes at the nursing unit level. This provides a database for individual hospitals to compare their performance against nursing performance nationally (Kurtzman and Jennings, 2008). The evaluation of patient outcomes and nursing workforce characteristics remains important to nursing and the health care delivery system. Chapter 5 describes approaches for measuring outcomes.
Because of the importance of nursing-sensitive outcomes, the Agency for Healthcare Research Quality funded several nursing research studies that looked at the relationship of nurse staffing levels to adverse patient outcomes. These studies found a connection between higher levels of staffing by registered nurses (RNs) in hospitals and fewer negative patient outcomes. For example, the incidence of hospital-acquired pneumonia was highly sensitive to RN staffing levels. Adding just 30 minutes of RN staffing per patient day greatly reduced the incidence of pneumonia in patients following surgery. These studies also found that increased levels of nurse staffing positively impacted nurse satisfaction. Future studies will examine how nurses’ workloads affect patient safety and how their working conditions affect medication safety. Measuring and monitoring nursing-sensitive outcomes reveal the interventions that improve patients’ outcomes. Nurses and health care facilities use nursing-sensitive outcomes to improve nurses’ workloads, enhance patient safety, and develop sound policies related to nursing practice and health care.
Nursing Informatics and Technological Advancements
Quality and Safety Education for Nurses (QSEN) identified informatics as a competency for nurses (Cronenwett et al., 2007). Nursing informatics “uses information and technology to communicate, manage knowledge, mitigate error, and support decision-making” (Cronenwett et al., 2007). Data are individually distinct pieces of reality. Examples of data nurses collect and use to deliver safe patient care include a patient’s blood pressure or the measurement of a patient’s wound. Nurses gain or use information when they organize, structure, or interpret data. A nurse uses information when looking at trends in a patient’s blood pressure readings over the past 24 hours or when evaluating the changes in the size of a wound over the past 3 weeks. Knowledge develops when nurses combine and identify relationships between different pieces of information. For example, nurses know that diet plays an important role in blood pressure control and wound healing. They use this knowledge to teach patients at risk for developing high blood pressure to limit their salt intake and to teach patients who have wounds the importance of eating a well-rounded diet that includes adequate protein, vitamins, and minerals. Knowledge and skills in informatics also provides the nurse ability to access quality electronic sources of health care information to plan and coordinate patient care (Cronenwett et al., 2007). The focus of nursing informatics is not on the technology or the computer; rather, its focus is on the organization, analysis, and dissemination of information (American Nurses Association, 2008). Chapter 26 provides a thorough review of how nursing informatics improves the way nurses provide health care through use of the electronic health record.
Advances in technology are constantly evolving. People work, play, and view the world much differently because of these advances. Technological advancements also influence where and how nurses provide care to patients. Technological advances help nurses improve direct care processes, patient outcomes, and work environments (Zuzelo et al., 2008). Sophisticated equipment such as electronic IV infusion devices, cardiac telemetry (a device that monitors a patient’s heart rate wherever the patient is on a nursing unit), and computerized medication dispensation systems (see Chapter 31) are just a few examples that have changed health care. In many ways, technology makes the nurse’s work easier, but it does not replace nursing judgment. For example, it is the nurse’s responsibility when managing a patient’s IV therapy to monitor the infusion to be sure that it infuses on time and without complications. An electronic infusion device provides a constant rate of infusion, but nurses need to be sure that they calculate the rate correctly. The device sets off an alarm if the infusion slows, making it important for the nurse to respond to the alarm and troubleshoot the problem. Technology does not replace a nurse’s critical eye and clinical judgment. Challenges arise for nurses when technologies create inefficient delivery systems or uses or need repairs. These problems increase the nurses’ workload (Zuzelo et al., 2008).
Technology also affects the way we communicate with others. Personal computers, cell phones, and personal digital assistants (PDAs) allow us to communicate and share information or data with others in a variety of formats around the world. People expect accurate information to be delivered to them as it develops. Managing communication, information, and data is challenging in health care. Health care agencies use data to measure their outcomes and improve patient care. Accrediting bodies, insurance companies, and Medicare/Medicaid all require collection and reporting of accurate data. Furthermore, nurses need accurate, up-to-date information to make the best decisions about patient care. Therefore it is crucial that nurses help health care agencies develop an effective way to manage the collection, interpretation, and distribution of information.
Nurses need to play a role in evaluating and implementing new technological advances. They use technology and informatics to improve the effectiveness of nursing care, enhance safety, and improve patient outcomes. Most important, it is essential for nurses to remember that the focus of nursing care is not the machine or the technology; it is the patient. Therefore nurses need to constantly attend to and connect with their patients and ensure that their dignity and rights are preserved at all levels of care.
Globalization of Health Care
Globalization, the increasing connectedness of the world’s economy, culture, and technology, is one of the forces reshaping the health care delivery system (Oulton, 2012). Advances in communication, primarily through the Internet, allow nurses, patients, and other health care providers to talk with others worldwide about health care issues. Improved communication, easier air travel, and easing of trade restrictions are making it easier for people to engage in “health tourism.” Health tourism is the travel to other nations to seek out health care.
Many problems affect the health status of people around the world. For example, poverty is still deadlier than any disease and is the most frequent reason for death in the world today. Poverty increases the disparities in health care services among vulnerable populations (Crigger, 2008). Nations and communities that experience poverty have limited access to vaccines, clean water, and standard medical care. The growth of urbanization also currently is affecting global health. As cities become more densely populated, problems with pollution, noise, crowding, inadequate water, improper waste disposal, and other environmental hazards become more apparent. Children, women, and older adults are vulnerable populations most threatened by urbanization. Nurses work toward improving the health of all populations (Crigger, 2008). Although globalization of trade, travel, and culture improves the availability of health care services, the spread of communicable diseases such as tuberculosis and severe acute respiratory syndrome has become more common. Finally, the results of global environmental changes and disasters affect health. Changes in climate and natural disasters threaten food supplies and often allow infectious diseases to spread more rapidly.
Nurses need to understand how worldwide communication and globalization of health care influence nursing practice. Health care consumers demand quality and service and have become more knowledgeable. They often have searched the Internet about their health concerns and medical conditions. They also use the Internet to select their health care providers. As a result of globalization, health care providers have to make their services more accessible. Because of advances in communication, nurses and other health care providers practice across state and national boundaries. In response to the nursing shortage in the early 2000s, health care institutions recruited nurses from around the world to work in the United States. This was an effort to continue to provide quality, safe patient care. This trend is expected to continue to fill vacant nursing positions (Buerhaus et al., 2009). The hiring of nurses from other nations has required American hospitals to better understand and work with nurses from different cultures and with different needs.
As a leader in health care, remain aware of what is happening in the community, nation, and around the world. The International Council of Nurses (ICN), based in Switzerland, represents nursing worldwide. The purpose of the ICN is to advance the nursing profession worldwide and influence health policy (ICN, 2010). The goals of ICN are to bring nursing together, advance the nursing profession, and influence health policy worldwide (ICN, 2010). The unique focus of nursing on caring helps nurses address the issues presented by globalization. Nurses and the nursing profession are able to help overcome these issues by working together to improve nursing education throughout the world, retaining nurses and recruiting people to be nurses, and being advocates for changes that will improve the delivery of health care. Be prepared for future health care issues. Globalization has influenced many other industries. As a leader, nursing has to take control and be proactive in developing solutions before someone outside of nursing takes control.
The Future of Health Care
This discussion of the health care delivery system began with the issue of change. Change is often threatening, but it also opens up opportunities for improvement. The ultimate issue in designing and delivering health care is ensuring the health and welfare of the population. Health care in the United States and around the world is not perfect. Patients do not receive continuity of care when they see multiple health care providers. Often patients are uninsured or underinsured and do not have access to necessary services. However, health care organizations are trying to become better prepared to deal with the challenges in health care. Increasingly, health care organizations are changing how they provide their services, reducing unnecessary costs, improving access to care, and trying to provide high-quality patient care. Professional nursing is an important player in the future of health care delivery. The solutions necessary to improve the quality of health care depend largely on the active participation of nurses.
Key Points
• Increasing costs and decreasing reimbursement are forcing health care institutions to deliver care more efficiently without sacrificing quality.
• In a managed care system the provider of care receives a predetermined capitated payment regardless of the services a patient uses.
• The Medicare prospective reimbursement system is based on payment calculated on the basis of DRG assignment.
• Levels of health care describe the range of services and settings in which health care is available to patients in all stages of health and illness.
• Health promotion occurs in home, work, and community settings.
• Nurses are facing the challenge of keeping populations healthy and well within their own homes and communities.
• Successful community-based health programs involve building relationships with the community and incorporating cultural and environmental factors.
• Hospitalized patients are acutely ill, requiring better coordination of services before discharge.
• Rehabilitation allows an individual to return to a level of normal or near-normal function after a physical or mental illness, injury, or chemical dependency.
• Home care agencies provide a wide variety of health care services with an emphasis on patient and family independence.
• Discharge planning begins at admission to a health care facility and helps in the transition of a patient’s care from one environment to another.
• Health care organizations are being evaluated on the basis of outcomes such as prevention of complications, patients’ functional outcomes, and patient satisfaction.
• Nurses need to remain knowledgeable and proactive about issues in the health care delivery system to provide quality patient care and positively affect health.
Clinical Application Questions
Preparing for clinical practice
Community Hospital is a 400-bed urban hospital, one of six hospitals in a health care system. The system also operates a local community clinic that primarily serves a poor multicultural population. The nursing department of the hospital is considering making application to the American Nurses Credentialing Center for Magnet status. Nursing units are working on a number of projects to prepare for the Magnet application process.
1. You are a staff nurse on a medical-surgical floor at the hospital. The unit is trying to improve its culture in patient safety. How would you go about helping to improve the culture of safety on the unit?
2. Discuss three strategies that the community clinic can use to deliver patient- and family-centered care.
3. You are asked by a nurse at another hospital what it means to be a “Magnet hospital.” Describe the Magnet model of nursing to answer the nurse’s question.
 Answers to Clinical Application Questions can be found on the Evolve website.
Answers to Clinical Application Questions can be found on the Evolve website.
Are you ready to test your nursing knowledge?
1. Which of the following is an example of the principle of patient-centered care focused on continuity and transition?
1. The nurse asks the patient who in the family should have access to patient information
2. The nurse is teaching the patient how to change the wound dressing at home
3. The nurse responds promptly to the patient’s request for pain medication
4. The nurse schedules the patient’s diagnostic scan following the physical therapy session
2. Which activity performed by the nurse is related to maintaining competency in nursing practice?
1. Asking another nurse about how to change the settings on a medication pump
2. Regularly attending unit staff meetings
3. Participating as a member of the professional nursing council
4. Attending a review course in preparation for the certification examination
3. The patient tells the nurse that she is enrolled in a preferred provider organization (PPO) but does not understand what this is. What is the nurse’s best explanation of a PPO?
1. This health plan is for people who cannot afford their own health insurance
2. This health plan is operated by the government to provide health care to older adults
3. This health plan provides you with a preferred list of physicians, hospitals, and providers from which you can choose
4. This is a fee-for-service plan in which you can choose any physician or hospital
4. Which of the following is an example of the nurse participating in primary care activities?
1. Providing prenatal teaching on nutrition to a pregnant woman during the first trimester
2. Working with patients in a cardiac rehabilitation program
5. Nurses on a nursing unit are discussing the processes that led up to a near-miss error on the clinical unit. They are outlining strategies that will prevent this in the future. This is an example of nurses working on what issue in the health care system?
6. Which of the following statements is true regarding Magnet status recognition for a hospital?
1. Nursing is run by a Magnet manager who makes decisions for the nursing units
2. Nurses in Magnet hospitals make all of the decisions on the clinical units
3. Magnet is a term that is used to describe hospitals that are able to hire the nurses they need
4. Magnet is a special designation for hospitals that achieve excellence in nursing practice
7. Which statement made by the nurse is an example of applying the principle of patient-centered care while focusing on alleviation of a patient’s fear and anxiety?
1. “Let’s talk about the concerns that you have about going home.”
2. “I’ll get the medication prescriptions for you before discharge”
8. Which of the following is/are characteristics of managed care systems? (Select all that apply.)
1. Provider receives a predetermined payment for each patient in the program.
2. Payment is based on a set fee for each service provided.
3. System includes a voluntary prescription drug program for an additional cost.
4. System tries to reduce costs while keeping patients healthy.
9. Which of the following nursing activities is found in a tertiary health care environment?
1. Administering influenza immunizations at the senior independent living facility
2. Providing well-baby care in the clinic run by the local community health department
3. Admitting a patient following open heart surgery to the cardiovascular intensive care unit
10. Which of the following activities performed by the nurse is/are focused on the patient-centered care principle of physical comfort? (Select all that apply.)
1. Asking the patient what a tolerable level of pain is for him or her following surgery
2. Providing a back rub at bedtime
3. Offering the patient a warm washcloth for his or her hands before eating
4. Teaching the patient about the new antihypertensive medication ordered
5. Scheduling the patient’s follow-up appointments on discharge
6. Changing the bed linens for a patient who is experiencing diaphoresis
11. The nursing staff is developing a quality program for the floor. Which of the following are nursing-sensitive indicators from the National Database of Nursing Quality Indicators that the nurses can use to measure patient safety and quality for the unit? (Select all that apply.)
1. Number of medication errors committed by registered nurses (RNs)
12. The nurse is providing restorative care to a patient following an extended hospitalization for an acute illness. Which of the following is an appropriate goal for restorative care?
1. Patient will be able to walk 200 feet without shortness of breath
2. Wound will heal without signs of infection
13. A nurse is presenting information to a management class of nursing students on the topic of groups of inpatient hospital services that have a fixed reimbursement amount, with adjustments made on the basis of case severity and regional costs. The nurse is presenting information to the class on which topic?
14. When a nurse uses information and technology to communicate, locate and use knowledge, reduce and eliminate errors, and help make decisions, the nurse is working in which area?
15. Which of the following are examples of the principle of patient-centered care that is focused on respect, values, preferences, and expressed needs? (Select all that apply.)
1. Administer antihypertensive medications to patient daily.
2. Pulling the curtain around the patient bed before changing the wound dressing on the patient’s leg
3. Allowing the patient to ask questions and express his or her concern about surgery
4. Explaining a colonoscopy procedure to the patient
5. Working with the family to bring in ethnic foods that the patient prefers
Answers: 1. 2; 2. 4; 3. 3; 4. 1; 5. 1; 6. 4; 7. 1; 8. 1, 4, 5; 9. 3; 10. 1, 2, 3, 6; 11. 2, 3, 4; 12. 1; 13. 4; 14. 3; 15. 2, 3, 5.
References
Adashi, EY, et al. Health care reform and primary care—the growing importance of the community health center. N Engl J Med. 2010;362(22):2047.
Agency for Healthcare Research and Quality Patient Safety Network (AHRQ PSNet). Patient safety primer: Never events. n.d. http://psnet.ahrq.gov/printviewPrimer.aspx?primerID=3. [Accessed September 5, 2011].
American Association of Colleges of Nursing. Nursing fact sheet. http://www.aacn.nche/edu/Media/FactSheets/nursfact.htm, 2011. [Accessed June 20, 2011].
American Association of Colleges of Nursing. Nursing shortage. http://www.aacn.nche.edu/Media/FactSheets/NursingShortage.htm, 2010. [Accessed June 18, 2011].
American Medical Association. Critical access hospital fact sheet. http://www.aacvpr.org/Portals/0/policy/resources/CAH_factsheet_june2009.pdf, 2009. [Accessed June 20, 2011].
American Nurses Association. Nursing informatics scope and standards of practice. Silver Springs, Md: The Association; 2008.
American Nurses Credentialing Center. A new model for ANCC’s Magnet Recognition Program. http://www.nursecredentialing.org/Magnet/ProgramOverview/NewMagnetModel.aspx, 2010. [Accessed May 5, 2010].
American Nurses Credentialing Center. Growth of the program. http://www.nursecredentialing.org/Magnet/ProgramOverview/GrowthoftheProgram.aspx, 2010. [Accessed June 18, 2011].
American Nurses Credentialing Center. Magnet program overview. http://www.nursecredentialing.org/Magnet/ProgramOverview.aspx, 2010. [Accessed June 18, 2011].
Billings, J, Cantor, JC. Access to care. In Kovner AR, Knickman JR, eds.: Health care delivery in the United States, ed 9, New York: Springer, 2009.
Bodrock, JA, Mion, LC. Pay for performance in hospitals: implications for nurses and nursing care. Qual Manage Health Care. 2008;17(2):102.
Burger, G. The 5 Whys: A Simple Tool in Value Stream Analysis. http://www.isixigma.com/library/content/c070910a.asp, 2008. [Accessed June 18, 2011].
Carey, G. Comparing and blending ISO9000 and lean six sigma. http://www.isixsigma.com/index.php?option=comk2&view=item&id=67&Itemid=1&Itemid=1, 2010. [Accessed January 10, 2012].
Centers for Disease Control and Prevention. Fast facts: life expectancy. Deaths: final data for 2007. http://www.cdc.gov/nchs/fastats/lifexpec.htm, 2007. [Accessed June 18, 2011].
Centers for Disease Control and Prevention. Health risks in the United States: behavioral risk factor surveillance system at a glance. http://www.cdc.gov/chronicdisease/resources/publications/AAG/brfss.htm, 2010. [Accessed June 18, 2011].
Crigger, NJ. Towards a viable and just global nursing ethics. Nurs Ethics. 2008;15(1):17.
Cronenwett, L, et al. Quality and safety education for nurses. Nurs Outlook. 2007;55:122.
Ebersole, P, et al. Toward healthy aging: human needs and nursing response, ed 7. St Louis: Mosby; 2008.
HCAHPS. Fact sheet (CAHPS hospital survey, July 2010). http://www.hcahpsonline.org/facts.aspx, 2010. [Accessed June 18, 2011].
HealthReform.gov. Key provisions that take effect immediately. http://www.healthreform.gov/reports/keyprovisions.html, 2010. [Accessed June 18, 2011].
Institute for Patient and Family Centered Care [IPFCC]. FAQ. http://www.ipfcc.org/faq.html, 2010. [Accessed June 18, 2011].
Institute of Medicine (IOM). Crossing the quality chasm: a new health system for the 21st century. Washington DC: National Academies Press; 2001.
Institute of Medicine. Health professions education: a bridge to quality. Washington, DC: National Academies Press; 2003.
Institute of Medicine (IOM). The future of nursing: leading change, advancing health. Washington DC: National Academies Press; 2011.
International Council of Nurses [ICN]. Our mission. http://www.icn.ch/about-icn/icns-mission/, 2010.
isixsigma. Statistical Six Sigma definition. http://www.isixsigma.com/index/php?option=com_k2&view=item&layout=item&id=1254&Itemid=110, 2010. [Accessed June 18, 2011].
Jonas, S, et al. An introduction to the US health care system, ed 6. New York: Springer; 2007.
Jordan, C, et al. Public policy on competency: how will nursing address this complex issue? J Cont Educ Nurs. 2008;39(2):86.
Knickman, JR, Kovner, AR. Overview: the state of health care delivery in the United States. In Kovner AR, Knickman JR, eds.: Health care delivery in the United States, ed 9, New York: Springer, 2009.
Kotzer, AM, Arellana, K. Defining an evidenced-based work environment for nursing in the USA. J Clin Nurs. 2008;17(12):1652.
Kurtzman, ET, Jennings, BM. Trends in transparency: nursing performance measurement and reporting. J Nurs Admin. 2008;38(7):349.
Lutz, SL, Root, D. Nurses, consumer satisfaction, and pay for performance. Healthcare Finance Manage. 2007;61(10):57.
Meiner, SE. Gerontologic nursing, ed 4. St. Louis: Mosby; 2011.
Melnyk, BM, Fineout-Overholt, E. Evidence-based practice in nursing and health care: a guide to best practice, ed 2. Philadelphia: Lippincott, Williams & Wilkins; 2010.
Missouri Families. Aging. http://missourifamilies.org/quick/agingqa/agingqa30.htm, 2008. [Accessed June 18, 2011].
National Center for Assisted Living [NCAL]. Assisted living facility profile. http://www.ahcancal.org/ncal/resources/Pages/ALFacilityProfile.aspx, 2010. [Accessed June 18, 2011].
National Committee for Quality Assurance [NCQA]. HEDIS and quality compass. http://www.ncqa.org/tabid/187/Default.aspx, 2010. [Accessed June 18, 2011].
National Database of Nursing Quality Indicators (NDNQI). NDNQI: transforming data into quality care. http://www.nursingquality.org, 2010. [Accessed June 18, 2011].
National Priorities Partnership. National priorities and goals: aligning our efforts to transform America’s healthcare. Washington, DC: National Quality Forum; 2008.
National Quality Forum [NQF]. Safe practices for better healthcare—2010 update: a consensus report. Washington, DC: National Quality Forum; 2010.
Oulton, J. Nursing in the international community: a broader view of nursing issues. In Mason DJ, et al, eds.: Policy and politics in nursing and health care, ed 6, St Louis: Saunders, 2012.
Pew Health Professions Commission, The Fourth Report of the Pew Health Professions Commission: Recreating health professional practice for a new century, 1998, The Commission.
Resnick, B, Fleishell, A. Developing a restorative care program: a five step approach that involves the resident. Am J Nurs. 2002;102(7):95.
Scott-Tilley, DD. Competency in nursing: a concept analysis. J Cont Educ Nurs. 2008;39(2):58.
Singleton, KA. Lead, follow, and get in the way: the medical-surgical nurse’s role in health care reform. Medsurg Nurs. 2010;19(1):5.
Sorrentino, S. Mosby’s textbook for nursing assistants, ed 7. St Louis: Mosby; 2007.
Sultz, HA, Young, KM. Health care USA: understanding its organization and delivery, ed 5. Sudbury: Jones & Bartlett; 2006.
The Joint Commission. Accreditation Process Overview. http://www.jointcommission.org/accreditation_process_overview/, 2011. [Accessed June 20, 2011].
Thompson, JA, Lee, V. The effect of health insurance disparities on the health care system. AORN J. 2007;86(5):745.
US Department of Labor. Bureau of Labor Statistics: Employment projections: occupations with the largest job growth. http://www.bls.gov/emp/ep_table_104.htm, 2009. [Accessed June 20, 2011].
Vlasses, FR, Smeltzer, CH. Toward a new future for healthcare and nursing practice. J Nurs Admin. 2007;37(9):375.
World Health Organization [WHO]. The WHO report 2008: primary health care now more than ever. Geneva, Switzerland: WHO; 2008.
Research References
Baernholdt, M, et al. What does quality care mean to nurses in rural hospitals? J Adv Nurs. 2010;66(6):1346.
Buerhaus, PI, et al. The recent surge in nurse employment: causes and implications. Health Affairs. 2009;28(4):w657. [published online 12 June 2009, doi:10.1377/hlthaff.28.4.w657].
Burns, HK, et al. Building an evidence-based practice infrastructure and culture: a model for rural and community hospitals. J Nurs Admin. 2009;39(7/8):321.
Hughes, LC, et al. Quality and strength of patient safety climate on medical-surgical units. Health Care Manage Rev. 2009;34(1):28.
Kendall-Gallagher, D, Blegen, MA. Competence and certification of registered nurses and safety of patients in intensive care units. Am J Crit Care. 2009;18(2):106.
Kutney-Lee, A, et al. Nursing: a key to patient satisfaction. Health Affairs. 2009;28(4):w669. [published online 12 June 2009, doi:10.1377/hlthaff.28.4.w669].
Lindenauer, PK, et al. Public reporting and pay for performance in hospital quality improvement. New Engl J Med. 2007;356(5):486.
Spence Laschinger, HK. Effect of empowerment on professional practice environments, work satisfaction, and patient care quality: further testing the nursing work life mode. J Nurs Care Qual. 2008;23(4):322.
Tzeng, H, Yin, C. No safety, no quality: synthesis of research on hospital and patient safety (1996-2007). J Nurs Care Qual. 2007;22(4):229.
Zarubi, KL, et al. Putting patients and families at the center of care. J Nurs Admin. 2008;38(6):278.
Zuzelo, PR, et al. Describing the influence of technologies on registered nurses’ work. Clin Nurse Spec. 2008;22(3):132.