Social, Cultural, and Religious Influences on Child Health Promotion

http://evolve.elsevier.com/wong/ncic

Communicating with Families Through an Interpreter, Ch. 6
Family Influences on Child Health Promotion, Ch. 3
Lactose Intolerance, Ch. 13
Nutritional Assessment, Ch. 6
Sickle Cell Anemia, Ch. 35
Skin, Ch. 6
Toddler, Ch. 14; Preschooler, Ch. 15; School-Age Child, Ch. 17; Adolescent, Ch. 19
Vegetarian Diets, Ch. 13
Culture
Promoting the health of pediatric patients requires a nurse to understand social, cultural, and religious influences on children. This in turn depends on a purposeful awareness of the child’s sociocultural context. A holistic view of care was first described by Madeleine Leininger, the recognized founder of transcultural nursing, in her culture care diversity and universality theory (Leininger, 2001). The theory provides an intellectual framework and a research methodology for providing culturally congruent patient care. As the ethnic, racial, and cultural diversity in the U.S. population increases, it is imperative that nurses become competent in transcultural nursing (Munoz and Luckmann, 2005). They must remain aware that every family, child, and health care provider comes to a clinical encounter with a cultural lens through which they see and interpret the world.
Transcultural nursing care is important considering the ever-changing population. The demographic profile of the United States 2000 census includes 69% non-Hispanic white, 13% Hispanic/Latino, 12% Black/African-American, and 4% Asian (US Census Bureau, 2001).
Nurses can become culturally competent by learning about and developing an understanding of cultures other than their own, being sensitive to the effects of culture on the nursing care of patients, and understanding how their own culture affects their ability to provide care to others (Dunn, 2002).
Culture is a rich context through which people view and respond to their world (see Cultural Competence box). It also provides the lens through which all facets of human behavior can be interpreted (Spector, 2009). Culture is composed of individuals who share a set of values, beliefs, practices (e.g., language, dress, diet, health care), social relationships, laws, politics, economics, and norms of behavior that are learned, integrative, social, and satisfying. Culture is an ingrained orientation to life that serves as a frame of reference for individual perception and judgment. Culture is, essentially, the way of life of a group of people that incorporates experiences of the past, influences thought and action in the present, and transmits these traditions to future group members. Families pass their culture on to children, and the children perceive the world through this cultural lens. Culture adapts to the ever-changing world as group members abandon, modify, or assume new patterns of living and behavior to meet the group’s needs.
 CULTURAL COMPETENCE
CULTURAL COMPETENCE
Cultural Definitions
Culture characterizes a particular group with its values, beliefs, norms, patterns, and practices that are learned, shared, and transmitted from one generation to another (Leininger, 2001). Culture differs from both race and ethnicity. Race is a biologic term distinguishing variety in humans by physical traits. Ethnicity is the affiliation of a set of persons who share a unique cultural, social, and linguistic heritage. Socialization is the process by which society communicates its competencies, values, and expectations to children (Trawick-Smith, 2006). Culture is a complex whole in which each part is interrelated. It is an umbrella term that holds together many interrelated yet unique aspects of humanity like beliefs, tradition, life ways, and heritage. It is much more than a country of origin or a demographic designation such as African-American or Caucasian.
Material overt, or manifest, culture refers to the observable components of a culture, such as material objects (dress, art, utensils, and other artifacts) and actions. Nonmaterial covert culture refers to those aspects that cannot be observed directly, such as ideas, beliefs, customs, and feelings. Related to the large culture are many subcultures, each with an identity of its own. Children are socialized into a particular subculture rather than into the culture as a whole. Subcultural influences, such as ethnicity and social class, are discussed in more detail later in this chapter.
Cultures and subcultures contribute to the uniqueness of child members in such a subtle way and at such an early age that children grow up to think that their beliefs, attitudes, values, and practices are the “correct” or “normal” ones. By age 5 years, children can identify persons who belong to their own race or cultural background. During later primary years, children can identify those from different cultures (Trawick-Smith, 2006). A set of values learned in childhood is likely to characterize children’s attitudes and behavior for life, influencing their long-range goals and their short-range, impulsive inclinations. Thus every ongoing society socializes each succeeding generation to its cultural heritage.
The manner and sequence of the growth and development phenomenon are universal and fundamental features of all children; however, children’s varied behavioral responses to similar events are often determined by their culture. Culture plays a critical role in the parenting behaviors that facilitate children’s development (Melendez, 2005). Children acquire the skills, knowledge, beliefs, and values important to their own family and culture. Cultural backgrounds can influence the pace of acquisition of cognitive and motor skills as well as the child’s social and emotional development (Trawick-Smith, 2006).
Cultures may also differ in whether status in a group is based on age or on skill. Even children’s play and their types of games are culturally determined. In some cultures children play in groups composed of members of the same sex; in others they play in mixed-sex groups. In some cultures team games predominate; in others most play is limited to individual games.
Standards and norms vary from culture to culture and from location to location; a practice that is accepted in one area may meet with disapproval or create tension in another. The extent to which cultures tolerate divergence from the established norm also varies among cultures and subcultural groups. Although conforming to cultural norms provides a degree of security, it is a decided deterrent to change.
The Child and Family in North America
Context provides perspective for nursing care. The health and well-being of the child in the North American family is influenced by two distinct contexts: the context of family and the context of culture. Therefore understanding these layers of influence on pediatric health is integral to developing a family-centered and culturally competent nursing practice (Thibodeaux and Deatrick, 2007). America’s orientation toward homogenization—“the great melting pot”—is changing to an orientation of complex cultural diversity. Increased awareness of the growing proportion of ethnic minorities that make up the U.S. population, coupled with a new appreciation for ethnic diversity, has resulted in a renewed interest in cultural variation.
The frontier background of the American culture has contributed to the overall orientation to life and childrearing. Americans have always had a basic optimistic view of the world, a belief that things can be better and that the children can and will be better off than their parents. With this hopeful outlook, a general future orientation, and the possibility of upward social mobility, American culture typically encourages development of self-confidence and autonomy in children. Children are generally permitted a greater degree of freedom than in more tradition-oriented cultures.
Family life in North America is characterized by increasing geographic and economic mobility. Families are less reliant on tradition, are fragmented, and have limited opportunity to transmit and acquire the traditional and accepted customs of a culture. Consequently, young adults rely to a greater extent on the professed experts, peers, and the mass media for acquisition of acceptable patterns of behavior, including childrearing practices. Conflicting information can be a source of confusion and frustration as parents attempt to determine the comparatively stable, essential components of the culture and transmit these to their children.
Children in North America grow up with a number of adults who differ from one another but who all provide input as role models, teachers, and standards for behavior. Most children live in some form of nuclear family located in sharply differentiated neighborhoods determined by income and ethnic status within a highly technical, largely urban society. Class differences in childrearing persist, but they are becoming less divergent.
Early in life children in minority cultures become aware of their cultural context and the discriminatory attitudes of the majority culture toward their racial or ethnic group. The direct effects of discrimination are anger and low self-esteem, which manifest in a variety of behaviors. Attitudes are slowly changing in some groups and in some places. With a relatively recent emergence of racial and ethnic pride along with a growing awareness, interest, and understanding of the majority, children in minority groups are becoming more secure and confident in their racial or ethnic identity. Individuals vary in their reactions to membership in a minority group, and much of this variation can be attributed to familial factors. The most important influences on development of a positive self-image are warm, understanding parents who actively foster their children’s growth. Parents who accept their children and react positively and constructively rather than in a negative manner will help their children develop feelings of self-worth, self-esteem, and self-acceptance. The more adequate children feel, the more positive their attitudes toward peers in both the majority and minority groups and the greater their ability to withstand prejudice and intolerance and build lasting relationships.
Social Roles
Much of children’s self-concept comes from their ideas about their social roles. Roles are cultural creations; therefore the culture prescribes patterns of behavior for persons in a variety of social positions. All persons who hold similar social positions have an obligation to behave in a particular manner. A role prohibits some behaviors and allows others. Because culture outlines and clarifies roles, it is a significant influence on the development of children’s self-concept (i.e., attitudes and beliefs they have about themselves).
A social group consists of a system of roles carried out in both primary and secondary groups. A primary group has intimate, continued, face-to-face contact; mutual support of members; and the ability to order or constrain a considerable proportion of individual members’ behavior. Two such groups are the family and the peer group, both of which have a great deal of influence on the child.
Secondary groups are groups that have limited, intermittent contact and generally less concern for members’ behavior. These groups offer little in terms of support or pressure toward conformity except in rigidly limited areas. Examples of secondary groups are professional associations and social organizations such as church groups.
A concept of social role also depends largely on whether a child is reared in a primary- or secondary-group community. Children are subjected to perceptibly different forms of parental training in these two types of environments.
Primary- and Secondary-Group Influences
Children are raised within a primary-group environment and within a secondary-group environment. The influences, strengths, and limitations of both groups are significant. In a primary-group community (e.g., family; peer group; some contemporary rural, religious, or ethnic communities), all members know each other, most belong to the same subgroups, and all are concerned about each member’s behavior. Community members have a high degree of material and psychologic support and one traditional set of values that the entire group agrees on and supports; thus there is little conflict of values. In a stable community where the members remain within comparatively defined limits and relatives are likely to live close together, young members have ample opportunity to observe and absorb cultural practices and customs. Any member of the community feels justified in evaluating and censuring the conduct of another member.
Children reared in the relative isolation of secondary-group environmental influences tend to learn that there is only one acceptable way to respond to any given situation. The entire group agrees, and any tendency to deviate is met with collective disapproval. It is the parents’ duty to see that the children learn and follow social roles and modes of behavior defined and strengthened by the views of the community.
The childrearing orientation in a secondary-group environment, such as urban communities, can differ considerably from that of a primary-group environment. The interaction between primary and secondary groups may reinforce values when both groups endorse that value, or create confusion or conflict when one group rejects a value accepted by the other. An urban community is dynamic. Many of the traditional behaviors and values may not meet the needs of the changing society. Consequently, parents are often uncertain about what to teach their children. They may wish to rear their children with values consistent with their own, but the differences in experience between the generations are too great. As a result, they often grant their children autonomy in some areas of decision making early in the developmental process, and other secondary groups assume a greater influence. None of the groups is highly dominant in its influence; therefore the children are exposed to an eclectic set of values and expectations, some in agreement and some in conflict. From these they must ultimately select those that they determine to be best for them and adopt them to form a consistent set of roles and behaviors to incorporate into the self-concept.
Self-Esteem and Culture
Culture influences a child’s sense of self-esteem (Trawick-Smith, 2006). Some cultures are more collective in thought and action. A child from a collective culture will hold an inclusive view of self. Self-evaluation is related to the accomplishments or competencies of the entire family or community. School experiences that focus on personal achievement may promote positive self-esteem in some children but not in others who are more dependent on the success of a whole family or peer group. Their sense of control may not come from individual self-reliance but rather from a feeling of worth in their family or community (Trawick-Smith, 2006).
Families and culture also influence the criteria children use to evaluate their own abilities. Additionally cultures vary in whether they instill an internal locus of control (a belief in the ability to regulate one’s own life). Effects on self-esteem are minimal if these beliefs are directed by parents and are in accordance with cultural customs (Trawick-Smith, 2006). Ethnic pride can help children to maintain a positive self-image and counteract the effects of prejudice, which can have a negative impact on emotional health (Trawick-Smith, 2006).
Cultural Shock and Cultural Competence
Cultural shock is characterized by the inability to respond to or function within a new or strange situation. It can occur when the values and beliefs of a new cultural setting are radically different from those of the person’s native culture (Munoz and Luckmann, 2005). This state of shock or uneasiness can happen to a patient in a hospital or to a nurse caring for patients with different cultural backgrounds. Immigrants to a new country and persons from a subcultural group experience the same cultural shock when they must adjust to the ways of an unfamiliar subgroup or setting.
Numerous factors influence reactions to a new environment. Language barriers, including dialects and jargon specific to a subcultural group, inhibit effective communication. Habits and customs, such as different role behaviors or etiquette, and differences in attitudes and beliefs are puzzling to the newcomer in an unfamiliar environment. The child and family experiencing cultural shock can feel an intense sense of isolation, loneliness, and fear (Crom, 1995).
Nurses are challenged to overcome cultural shock and develop cultural sensitivity, an awareness of cultural similarities and differences. Doing so helps the nurse practice culturally competent care. This requires changing the way people think about, understand, and interact within the world around them (see Critical Thinking Exercise). The development of cultural competence is an ongoing, interactive process that involves six elements (Dunn, 2002):
1. Working on changing one’s world view by examining one’s own values and behaviors and working to reject racism and institutions that support it
2. Becoming familiar with core cultural issues by recognizing these issues and exploring them with patients
3. Becoming knowledgeable about the cultural groups one works with while learning about each individual patient’s unique history
4. Becoming familiar with core cultural issues related to health and illness and communicating in a way that encourages patients to explain what an illness means to them
5. Developing a relationship of trust with patients and creating a welcoming atmosphere in the health care setting
6. Negotiating for mutually acceptable and understandable interventions of care
 CRITICAL THINKING EXERCISE
CRITICAL THINKING EXERCISE
Reducing Cultural Shock
A woman from the Middle East is visiting her child who is hospitalized for a serious illness. Her husband left for home a short time ago to wash and change clothes. She speaks little English. You need to obtain her consent for an emergency procedure. She is hesitant and refuses to sign the consent form. What should you do?
When minority groups immigrate to another country, a certain degree of cultural and ethnic blending occurs through the involuntary process of acculturation, those gradual changes produced in a culture by the influence of another culture that cause one or both cultures to be more similar to each other. However, the changes occur to various degrees in different families and groups. Many groups continue to identify with their traditional heritage while adapting to the ill-defined concept of the “American way.” Acculturation may be referred to as assimilation, which is the process of developing a new cultural identity (Spector, 2009).
Subcultural Influences
Except in rare situations, children grow and develop in a blend of cultures and subcultures. In a large, complex society such as the United States, different groups have their own set of standards, values, and expectations within the collective ways of the large culture. Most subcultures were formed when groups of people clustered together by preference, by external pressures from the majority culture, or by geographic isolation. Although many cultural differences are related to geographic boundaries, subcultures are not always restricted by location. Some subcultures are even related to the stages of development and have traditions, games, loyalties, and rules. The behavior of school-age children and adolescents demonstrates age-related subcultures. The culture is handed down by word of mouth from one “generation” to the next, and its rituals and behavior standards are highly resistant to outside influence.
Children’s membership in a cultural subgroup is, for the most part, involuntary. They are born into a family with a specific ethnic or racial heritage, socioeconomic level, and religious beliefs. Although the complex American society has countless subcultures and considerable variation in the way of life, those subcultures that seem to have the greatest influence on childrearing are ethnicity, social class, and occupational role. In addition, schools and peer-group subcultures are strong influences in the socialization of the child.
 NURSING ALERT
NURSING ALERT
American cultures and subcultures can be so diverse, it is essential that nurses be aware of and knowledgeable about the predominant groups in their work community and apply this knowledge in their practice.
NURSING ALERT
Any generalization made about an ethnic group may not apply to certain groups or individuals.
Ethnicity
Ethnicity is the classification of or affiliation with any of the basic groups or divisions of humankind or any heterogeneous population differentiated by customs, characteristics, language, or similar distinguishing factors. Ethnic differences extend to many areas and include such manifestations as family structure, language, food preferences, moral codes, and expression of emotion. Some standards of behavior (e.g., the traditional role of the father) result from the cultural heritage of the specific ethnic group. Others reflect the interaction between subcultures, most notably between members of the majority culture and a minority subculture. The term ethnic has aroused strong negative feelings, and the general population often rejects this term (Spector, 2009).
To establish their place in the group, children learn to follow a mode of behavior that is in accordance with standards distinctive to the group and learn how they can expect others to behave toward them. They take their cues by observing and imitating those to whom they are exposed. For example, children of a racial minority form a perception of their role as a group member by observing how role models within the subgroup respond to treatment by people outside the subgroup. When they see group members display an attitude of inferiority, they assume this to be the appropriate behavior and incorporate these perceptions into their own self-concept.
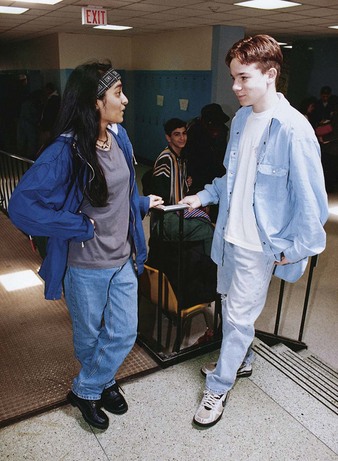
In the United States the cross-cultural lines are becoming blurred as subcultures are assimilated and blended into the larger culture (Fig. 2-1). Although ethnic differences in childrearing are probably diminishing, they remain important. It is particularly difficult for persons to attempt to maintain an identity within a subculture while living and conforming to the requirements of the larger culture.
Leavitt, Martinson, Liu, and colleagues (1999) found that immigrants from China who provided care for their children with cancer focused on dietary intake, whereas families that were of Caucasian descent focused on emotional support. The cultural framework directed the healing practices. Interestingly, the same study found that both groups shared the beliefs that mothers were the primary caregivers for the sick child. In this example one cultural behavior was unique to each cultural group while the other was similar. Consequently, children reared in this environment can become confused about roles and values of two or more cultures if they conflict. They usually adopt those of the more influential or higher-status culture. Youth, in particular, are influenced by the locally dominant group.
Ethnocentrism is the emotional attitude that one’s own ethnic group is superior to others; that one’s values, beliefs, and perceptions are the correct ones; and that the group’s ways of living and behaving are the best way (Spector, 2009). Ethnic stereotyping or labeling stems from ethnocentric views. Ethnocentrism implies that all other groups are inferior and that their ways are not in the best interests of the group. It is a common attitude among a dominant ethnic group and strongly influences a person’s ability to evaluate objectively the beliefs and behaviors of others. Nurses must overcome the natural tendency to have ethnocentric attitudes when caring for people from different cultures (Williams and Kruse, 1999). The culturally competent nurse has empathy for others, maintains an openness to feeling what the other feels, and remains curious and willing to ask questions to gain a better understanding. In addition, the nurse has a basic respect for self and others, and acknowledges the intrinsic value of all humans (Carrillo, Green, and Betancourt, 1999).
Minority-Group Membership
The United States has more racial, ethnic, and religious minority groups than any other country. Ethnic minority groups are becoming increasingly important because these groups are producing children at a faster rate than the majority Caucasian population. Consequently, the minority population is increasing. The rapidly emerging U.S. minority population will present special needs and require resources beyond what is currently available (Murdock, 2005).
The 2000 U.S. census revealed more than 280 million people in the United States, with 6.8 million reporting an ethnicity of more than two races. Blacks, or African-Americans, alone or in combination with another race, number more than 35 million, and Hispanics or Latinos of any race are more than 35 million. The Hispanic population increased 58%, or 13 million people, from 1990 to 2000 (US Census Bureau, 2001). Currently, Hispanics are the fastest growing minority in the United States and have many health needs that are not being met (Murdock, 2005; Warda, 2000). By the year 2010, Hispanics will surpass non-Hispanic blacks as the largest U.S. racial or ethnic group. In 2050 almost 30% of the U.S. population is expected to be Hispanic (Murdock, 2005) (see Cultural Competence box).
CULTURAL COMPETENCE
Overview of Race and Hispanic Origin in Census 2000
The federal government defines race and Hispanic origin as two separate and distinct concepts. In the 2000 U.S. Census, respondents were first asked if they are of Spanish/Hispanic/Latino origin. The second question asked respondents to report the race or races they considered themselves to be. The definitions of racial groups included (U.S. Census Bureau, 2001):
Whites—People having “origins in any of the original peoples of Europe, the Middle East, or North Africa”
African-Americans—Referred to as blacks and defined as “any persons whose lineage included ancestors who originated from any of the black racial groups of Africa”
Asians or Pacific Islanders—Any person with “origins in any of the original peoples of the Far East, Southeast Asia, the Indian subcontinent”
Native Hawaiian and Other Pacific Islanders—“People having origins in any of the original peoples of Hawaii, Guam, Samoa, or other Pacific Islands”
Native Americans—Referred to as American Indians and Alaskan Natives and defined as “persons having origins in the original peoples of North America and South America (including Central America), and who maintain cultural identification through tribal affiliations or community attachment”
Socioeconomic Class
Family relationships may be stronger in some ethnic or cultural groups than others. However, the influence of socioeconomic class cannot be overlooked. This relates to the family’s economic and educational levels. Strong family relationships exist among those of lower socioeconomic class who have few resources and must rely on the support of a family network to meet physical and emotional needs. Middle- and upper-class people often have resources that reach beyond the extended family. They are able to access physical and emotional support in the community (Giger and Davidhizar, 1999). Do not confuse the term socioeconomic class with cultural or ethnic diversity. Children of a specific race are not necessarily of low socioeconomic status. Additionally, children of poverty do not automatically have developmental delays (Trawick-Smith, 2006).
Communication Skills
Any concept that occurs to a person can be expressed in language. However, ease of communication and use of language codes vary among the social classes. Language is much more restricted in the lower classes, and grammar usage differs more than pronunciation. Persons in the middle classes use different grammar from those in the lower classes and are able to express more complicated ideas; persons in the lower classes use very simple grammar and are less likely to offer explanations.
These communication differences are highly significant in relation to school achievement. School is constructed around the elaborate language codes of the middle class; therefore children from the lower class who lack an understanding of these language skills are placed at a decided disadvantage. This is particularly true for bilingual children and children from ethnic groups that have developed a unique dialect.
Historically, schools have participated in devaluing Native American languages, cultures, and traditional ways of learning and knowing (Robinson-Zanartu, 1996). Unfortunately, Native American children have been deficient in their preparation for school (Dykeman, Nelson, and Appleton, 1995). Also, children of Native American nations have been at risk for low achievement, overrepresentation in special education, and dropping out (Robinson-Zanartu, 1996). Many regional dialects and variations in language usage must be considered when communicating with persons from these groups. English words that sound like another word in a foreign language can cause considerable misunderstanding.
Schools
When children enter school, their radius of relationships extends to include a wider variety of peers and a new focus of authority. Although parents continue to exert the major influence on children, in the school environment teachers have the most significant psychologic impact on their development and socialization. The teachers’ function is primarily limited to teaching, but, like parents, they are concerned about the children’s emotional welfare. Both parents and teachers must constrain behavior and enforce standards of conduct.
Socialization
Next to the family, the schools exert the major force in providing continuity between generations by conveying a vast amount of culture from the older members to the young. This prepares children to carry out the traditional social roles they are expected to assume as adults in society. School is the center of cultural diffusion wherein the cultural standards of the larger group are disseminated to the local community. It governs what is taught and, to a large extent, how it is taught. School rules and regulations regarding attendance, authority relationships, and the system of penalties and rewards based on achievement transmit to the child the behavioral expectations of the adult world of employment and relationships. School is often the only institution in which children systematically learn about the negative consequences of behaviors that depart from social expectations. In addition, the school provides an opportunity for some children to participate in the larger society in rewarding ways and often provides avenues for social mobility for both students and teachers. Individuals in the lower classes are offered the opportunity for further education and the capacity to move up in the social strata.
Teachers are responsible for transmitting the knowledge and values of the dominant culture (i.e., those values on which there is broad consensus). They are expected to stimulate and guide children’s intellectual development, sense of esthetics, and creative problem solving.
Traditionally the socialization process of school began when the child entered kindergarten or first grade. Today, with more than 60% of mothers of preschool children working outside the home, this socialization process begins much earlier for a significant number of children in a variety of childcare settings.
Children of some cultural groups fare less well in school. They come from underrepresented groups, including African-American, Mexican-American, Puerto-Rican, and Native-American children (Trawick-Smith, 2006). These cultural variations can be attributed to high rates of poverty, different cognitive styles, ineffective schools, and parents’ views of schools as oppressive to cultural and traditional values (Trawick-Smith, 2006).
Communities
Surveys of more than 1 million youth in the United States in grades 6 to 12 have shown that persons who experience a higher number of specific assets in their lives are more likely to make healthy choices and avoid high-risk behaviors. These assets offer a framework for positive child and adolescent development. The child or adolescent’s community is made up of family, school, neighborhood, youth organization, and other members.
Four categories of external assets that youth receive from the community are (Search Institute, 2007):
1. Support—Young people need to feel support, care, and love from their families, neighbors, and others. They also need organizations and institutions that offer positive, supportive environments.
2. Empowerment—Young people need to feel valued by their community and be able to contribute to others. They need to feel safe and secure.
3. Boundaries and expectations—Young people need to know what is expected of them and what activities and behaviors are within the community boundaries and what are outside of them.
4. Constructive use of time—Young people need opportunities for growth through constructive, enriching opportunities and through quality time at home.
Internal assets must also be nurtured in the community’s young members. These internal qualities guide choices and create a sense of centeredness, purpose, and focus. The four categories of internal assets are (Search Institute, 2007):
1. Commitment to learning—Young people need to develop a commitment to education and life-long learning.
2. Positive values—Youth need to have a strong sense of values that direct their choices.
3. Social competencies—Young people need competencies that help them make positive choices and build relationships.
4. Positive identity—Young people need a sense of their own power, purpose, worth, and promise.
Social Capital
Social capital is a health-related concept that provides a way for pediatric nurses to include a social context in their assessments. It considers where and how the children and families they care for live. Social capital is defined as the total sum of the social relationships within the family and the family’s relationship with peers, with institutions (schools, clubs, faith-based organizations), and with communities that affect the health and well-being of children (Looman and Lindeke, 2005). It is the way people mobilize resources and allows them to turn relationships into resources. Families develop a sense of belonging and find strength in knowing others in the same situation (Looman, 2004). The focus is on the interaction rather than specific supports. Research shows that social capital is related to positive health outcomes (Looman and Lindeke, 2005). Pediatric nurses can include social capital in their practice by bringing families, community members, and professionals together for a common purpose. Nurses can also include social capital in practice by encouraging repeated contacts over time, encouraging storytelling, and advocating for community experiences that enhance health-promoting behaviors (Looman and Lindeke, 2005).
Peer Cultures
Peer groups also have an impact on the socialization of children (Fig. 2-2). Peer relationships become increasingly important and influential as children proceed through school. In school, children have what can be regarded as a culture of their own. This is even more apparent in an unsupervised playgroup, since in school the culture is partly produced by adults.
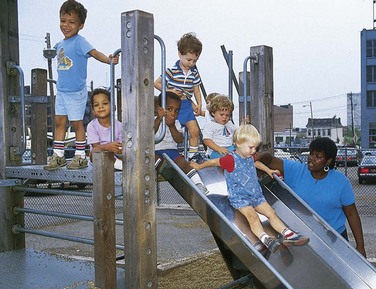
Fig. 2-2 Children from a variety of cultural and ethnic backgrounds begin to socialize in the child care setting.
During their lives children are exposed to value systems such as those of the family, ethnic group, and social class. In peer-group interaction they confront a variety of these sets of values. The values imposed by the peer group are especially compelling because children must accept and conform to them to be accepted as members of the group. When the peer values are not too different from those of family and teachers, the mild conflict created by these small differences serves to separate children from the adults in their lives and to strengthen the feeling of belonging to the peer group.
The kind of socialization provided by the peer group depends on the subculture that develops from its members’ background, interests, and capabilities. Some groups support school achievement, others focus on athletic prowess, and still others are decidedly against educative goals. Scholastic achievement is strongly related to the peer group’s value system. Many conflicts between teachers and students and between parents and students can be attributed to fear of rejection by peers. What is expected from parents regarding academic achievement and what is expected from the peer culture often conflict, especially during high school. Chapter 19 discusses this in further detail.
Although the peer group has neither the traditional authority of the parents nor the legal authority of the schools for teaching information, it manages to convey a substantial amount of information to its members, especially on taboo subjects such as sex and drugs. Children’s need for the friendship of their peers brings them into an increasingly complex social system. Through peer relationships, children learn to deal with dominance and hostility and to relate with persons in positions of leadership and authority. Other functions of the peer subculture are to relieve boredom and to provide recognition that individual members do not receive from teachers and other authority figures.
The peer-group culture has secrets, mores, and codes of ethics that promote group solidarity and detachment from adults. They have traditions and folkways, including age-related games and other activities, that are transferred from “generation to generation” of schoolchildren and that have a great influence over the behavior of all group members. As children move from one level to the next, they discard folkways of the younger group as they adopt those of the new group. For example, a school-age child rides a bicycle to school; the high school student prefers a car. As they advance, children are forward oriented only—they look forward with anticipation but may look backward with contempt.
Biculture
Some children are exposed to the values, role relationships, and lifestyles of two or more cultures. The virtual “straddling” of two cultures is referred to as biculturation and involves the ability to efficiently bridge the gap between an individual’s culture of origin and the dominant culture (Rogers, 1995). This may occur because the child’s parents are from two or more different cultures. In Hawaii, for example, it is common for children to be from four or more cultures. Other children straddle cultures as members of a minority culture within the dominant culture. This biculture is sometimes observed in the playgroup but usually is not a significant factor until children enter school. Then they must unlearn some of the established practices of one culture to become socialized in the other, especially in role relationships. For example, children from Hispanic and Asian cultures are taught to look away when scolded; in U.S. schools the teacher expects direct eye contact—“Look at me when I speak to you.” Children learn new roles and social behavior more rapidly than their adult counterparts.
This biculture is particularly marked in language differences. The bilingual child is said to be at a disadvantage in school situations of the dominant culture, in which there is controversy over bilingual education. Those supporting bilingual education adhere to the principle that children will understand more readily and perform more realistically (especially in testing situations) if learning is directed in their own language; others contend that children living in a dominant culture should adopt the ways of that culture, including language. The child faces less conflict when the school supports his or her language and culture, even if the dominant language is used.
Mass Media
The media provide children with a means for extending their knowledge about the world in which they live and have helped narrow the differences between social classes. However, many people are concerned about the enormous influence the media can have on the developing child and on health promotion behaviors (see Research Focus box). Children and adolescents in the United States spend more than 6 hours per day utilizing entertainment media (Council on Communications and Media, 2009). Increased use of entertainment media has been associated with the epidemic of obesity in children and adolescents and increased aggression in children (Jordan, 2004; Council on Communications and Media, 2009).
 RESEARCH FOCUS
RESEARCH FOCUS
Entertainment Media and High-Risk Behaviors
Researchers have established links between mass media and an increase in the use of tobacco, alcohol, and violent behavior in adolescents (Council on Communications and Media, 2009; American Academy of Pediatrics, 2001; Strasburger and Donnerstein, 1999). The images of risky behavior presented by the media may serve to establish or reinforce teenagers’ perceptions of their social environment. Also, media content may directly influence risk perception; media protagonists seldom suffer adverse consequences of their behaviors despite their grossly distorted experiences with violence, illness, or crime.
Children may identify closely with people or characters portrayed in reading materials, movies, videos, and television programs and commercials. Pediatric nurses can educate and support parents on the effects of mass media on their children through the following recommendations (Jordan, 2004):
• Be aware of the content of the child’s media and amount of time spent looking at a screen.
• Help young children watching television to find educational programs.
• Remove television, Internet-accessible computers, and videogame systems from the bedroom to decrease the amount of time spent using these activities.
• Limit television viewing to 2 hours a day or less.
• Watch age-appropriate programs and play age-appropriate games with children.
Reading Materials
The oldest form of mass media—books, newspapers, and magazines—contributes to children’s competence in almost every direction and provides enjoyment. Recognition of the impact that reading matter in schools has on value systems and the socialization process has prompted reevaluation of textbook content in several areas, such as stereotyped male and female role models, the sugar-coated view of life situations, and the biased history of minority groups.
Reading aloud to children is a vital activity in promoting success in reading. It provides cognitive and language stimulation, is a forum for quality parent-child interaction, and may reduce parent stress (Klass, Needlman, and Zuckerman, 2002).
Movies
Movies that are not closely bound to reality and often portray an assortment of socially approved behaviors perhaps make a contribution to children’s value systems and do provide opportunities for desirable social learning. On the other hand, children, especially adolescents, flock to “macho” movies and those whose heroes resort to violent resolution of problems, such as karate and wild automobile chases. The carryover of these influences into daily life and relationships may account in part for the increase in violent behavior of young persons.
A recent concern is the violent and R-rated movies available to children and teenagers in theaters and through cable television and DVDs. The content of movies has changed markedly over the past few years, with mutilation being a major theme. To children who are unable to distinguish between reality and fantasy, these films play on their deepest fears and result in bedtime fears, nightmares, and a fearful view of the world.
Television
The medium that has the most impact on children in the United States today is television; it has become one of the most significant socializing agents in the lives of young children. The programs and commercials provide multiple sources for acquiring information, modeling behaviors, and observing value orientations. Besides producing a leveling effect on class differences in general information and vocabulary, TV exposes children to a wider variety of topics and events than they encounter in day-to-day life. Television always has time to talk to children and is a form of access to the adult world. Positive results occur only when viewing is relatively light, yet the average child in the United States over the age of 8 spends more time watching television or using a computer and video games (>6 hours/day) than in any other activity except sleeping (Fig. 2-3) (Council on Communications and Media, 2009).
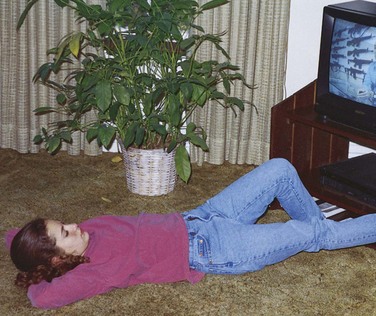
Fig. 2-3 The average child in the United States spends more time watching television than in any other activity except sleeping.
Television can offer some beneficial effects on the growing child. In their follow-up study of adolescents who had participated as preschoolers in an investigation of television use, researchers found that children who viewed educational programs as preschoolers had higher grades, read more books, valued achievement, had greater creativity, and were less aggressive (Anderson, Huston, Schmitt, et al, 2001).
Most researchers have concluded, however, that protracted television viewing can have negative effects on children. Increased verbal and physical aggressiveness, reduced persistence at problem solving, greater sex-role stereotyping, and reduced creativity have been reported repeatedly. In fairness, no one has yet defined the long-term effects of other electronic factors such as stereo headphones versus conversation, computer games or drills versus active social play, or DVDs versus books. However, clearly children in the modern electronic environment are constantly stimulated from the outside, which allows them little time to reflect and develop the inner speech that feeds brain development.
Most programs are designed to attract attention by visual jolts; the child establishes the habit of ignoring language in favor of hectic visual and auditory gimmicks. Like movies, television programs and commercials contain many implicit and explicit messages that promote alcohol consumption, smoking, violence, and promiscuous or unsafe sexual activity. An area of particular concern is unmonitored use of the Internet with videos sensationalizing violence, sex, suicide, and other destructive behaviors.
Socioeconomic Influences
A subcultural influence closely related to but different from social class is the condition known as poverty. It is a relative concept and is usually associated with the general standards of a population. The term poverty implies both visible and invisible impoverishment. It is a condition in which families live without adequate resources (Trawick-Smith, 2006). Visible poverty refers to lack of money or material resources, which includes poor nutrition, insufficient clothing, poor sanitation, and deteriorating housing. Invisible poverty refers to social and cultural deprivation such as limited employment opportunities, inferior educational opportunities, lack of or inferior medical services and health care facilities, and an absence of public services.
An absolute standard of poverty attempts to delimit a basic set of resources needed for adequate existence; a relative standard reflects the median standard of living in a society and is the term used in referring to childhood poverty in the United States; that is, what appears to be deprivation in one area may be a standard or norm in another.
An important development affecting the American family since the end of World War II is the widening disparity in income status among generations. Children from families with a single mother compose the largest group of children in poverty in the country (Wertheimer, 2005).
Growth in the number of poor children over the past decade has not been due to an increase in the number of welfare-dependent families, but to growth in the ranks of the working poor. Between 1994 and 2000, the poverty rate fell approximately 30%, but the trend has recently reversed, and the poverty rate rose 6% between 2000 and 2007. Approximately 18% of children in the United States live below the national poverty threshold, which is currently estimated at $21,027 for two adults and two children (Annie E Casey Foundation, 2009). In addition, approximately 20% of children live in neighborhoods where more than 20% of the population currently lives below the federal poverty threshold.
Such factors illustrate the growing inability of the American family to provide economic essentials for their children. Approximately 11.6% (about 8.5 million) of all children in the United States were uninsured in 2002 (Szilagyi, 2005). Uninsured children are more likely to miss school, jeopardizing their education as well as their health.
A high correlation between poverty and illness has long been observed. Impoverished families suffer from poor nutrition; without medical insurance, they have little if any preventive health care, inadequate health maintenance, and limited access to health services. One of the most significant health problems related to poverty is a high infant mortality rate. Although the rate of infant mortality has decreased in the United States, it still remains higher than that of most industrialized nations (Annie E Casey Foundation, 2009). Day-to-day needs of food, clothing, and lodging take precedence over health care as long as the ailing person feels able to perform activities of daily living.
Poor families may be denied access to some institutions for emergency or other hospital care. Frequently they must travel long distances to service centers that are willing to assume their care. In an emergency they must find money for taxi fare, borrow an automobile, or seek other means of transportation. They must find care for dependents, such as other infants and small children, or take them along when taking the ill child for care. Families tend to delay preventive care indefinitely unless health services are relatively accessible. They are more likely to consult folk practitioners or other persons within their community.
Poor nutrition accounts for many health problems in the lower classes. Lack of funds, education, and readily available healthy foods results in a diet that may be seriously lacking in essential food substances, especially protein, vitamins, and iron. This inadequate diet often leads to nutritional deficiency disorders and growth retardation in children. On the other hand, these issues may contribute to pediatric overweight and type 2 diabetes because nonnourishing foods are less expensive and are easier to access in some neighborhoods.
Dental problems are more prevalent because of deficient preventive care. Lack of standard immunizations together with reduced resistance from poor nutrition renders children in poor segments of the population vulnerable to communicable diseases. Poor sanitation and crowded living conditions also contribute to the higher incidence and perpetuation of illness. In general, poor people become ill more frequently and remain ill for longer periods than those in the general population.
Homelessness
One of the most pressing problems in the United States is the growing number of homeless families. Homeless individuals are those persons who lack resources and community ties necessary to provide for their own adequate shelter. In the past the homeless population traditionally included single adults, mostly men. Families with children make up 40% of the homeless population, compared with single men, who make up about 41% of the group (Redlener, 2005). Homeless children have increased in numbers as poverty has become feminized, minorities have become poorer, and low-income housing has become less accessible. Estimates of the number of homeless children in the United States may be as high as 1 million; about 10% of the children living in poverty were homeless (Redlener, 2005). Many homeless children are younger than 5 years and are from minority groups.
Most homelessness is a direct result of increasing number of people in poverty combined with a lack of decent, affordable housing. Other reasons include job layoffs, low incomes, parental mental illness, domestic conflict, and unexpected family or economic crises.
Another group of homeless children are the “runaway” and “throwaway” adolescents. Approximately 12% of the homeless population consists of adolescents (National Coalition to End Homelessness, 2009). Many runaways are victims of physical and sexual abuse and leave home because of long-term family or school problems. Poor parent-child relationships, extreme family conflict, feelings of alienation from parents, inconsistent supervision, and unpredictability in discipline are other factors often cited. These adolescents and young adults are at risk for violence, exploitation, substance abuse, and sexually transmitted infections (including HIV and AIDS).
Lack of a permanent housing deprives children of the most basic necessities for proper growth and development. Homelessness disrupts a child’s friendships and schooling (Strehlow and Amos-Jones, 1999). Homeless children suffer from physical and mental disorders more often than do poor children who have a permanent residence. Homeless children lack basic health care, including routine immunization and screening for routine problems, and they suffer high rates of acute and chronic illnesses (Redlener, 2005).
Migrant Families
Children in migrant farm worker families are medically underserved. Their numbers are staggering; of the 2 million migrant farm workers who labor in the United States, 63% are accompanied by minor children (Gentry, Quandt, Davis, et al, 2007). These children face both acute and chronic health care issues as a result of poverty, parental occupation, and assimilation into American culture. They are often exposed to risks similar to those facing their parents, since they may accompany them into the fields. These children frequently live in substandard housing conditions, which are subject to overcrowding and transmission of communicable diseases.
Migrant farm worker families face many obstacles when attempting to interface with the U.S. health care system. Three of every five families live below the federally designated poverty line and may lack insurance. The family’s use of health care may be affected by parental work schedules and access to transportation. Their own limited English proficiency is further exacerbated by a health care encounter that lacks cultural sensitivity, translation services, and language capability. Cultural expectations of the health care system may differ between the farm worker families and health care providers. This may ultimately have a negative effect on families’ utilization of the health care system. In fact, many families living on the U.S.-Mexico border seek the majority of care for their children in Mexico, regardless of their insurance status. In addition, less than 20% of migrant farm worker families use the primary care and health promotion centers that are federally funded through the 1962 Migrant Health Act (Gentry, Quandt, Davis, et al, 2007).  These two statistics demonstrate the need for culturally sensitive care that is consistent with the perceived needs and expectations of the recipients of such care.
These two statistics demonstrate the need for culturally sensitive care that is consistent with the perceived needs and expectations of the recipients of such care.
 Skill—Providing Culturally Sensitive Care
Skill—Providing Culturally Sensitive Care
Nurses and other health care providers should be mindful of the persistence of various forms of child labor in the United States (Hindman, 2006). Approximately 50% of 12- to 15-year-olds participate in some sort of paid activity each year, and half of this population have jobs in which they are considered employees. Children, adolescents, and young adults may work in a variety of areas, including agriculture, construction, retail, or even street trades or scams. Youth who work on family farms often face the greatest risk of injury and death from handling dangerous or heavy machinery. Youth who work in street trades and scams or traveling sales crews may be subject to physical or verbal abuse or victimization (Hindman, 2006).
Cultural Influences
Nurses need to consider clients’ cultural differences when providing health care. An understanding of the various beliefs regarding the causation of illness and disease, as well as traditional health practices, is essential to successful intervention. The more nurses know about the values, beliefs, and customs of other ethnic groups and how to elicit this information from families, the better they are able to meet the needs of these families and to gain their cooperation and compliance.
Case Study—Cultural Considerations
Cultural Relativity
Although clinical characteristics of a disease or condition are essentially the same across cultures, how a child or family interprets or experiences the disease or condition varies. Culture as an influence is one obvious explanation for variance. Cultural relativity is the concept that any behavior must be judged first in the context of the culture in which it occurs. Cultural factors such as belief systems and view of the world influence the patient’s and family’s response to health care. These cultural beliefs and behaviors influence adherence to a treatment plan (Munoz and Luckmann, 2005). Some cultures, for example, may view a chronic illness or disability as affecting only particular aspects of a child’s life, and the child as a whole is viewed as normal. In contrast, other families may describe the illness as having global effects on many aspects of the child’s present and future life (Martinson, Armstrong, and Qiao, 1997). These contrasting views may result in parents having different goals and expectations for their children.
Culture influences the assignment of gender roles, perception of disease, and perception of the side effects of the disease and the treatment the child should receive. For example, the family may expect the mother to be the primary caregiver. This places her at risk for caregiver strain when she is caring for a sick child.
Nurses can often recognize a family’s health-related cultural perceptions and interpretations through discussion and observation. They should explore and consider implications of these perceptions when planning culturally appropriate interventions. Nurses must be comfortable having discussions with families about their cultural beliefs and practices. The conversations can begin easily as, “I want to take the best care of your child and family as possible. Is there anything in particular about your beliefs [cultural, religious, family] that you think I should know?”
Relationships with Health Care Providers
The manner of relating with health care providers differs considerably among cultural groups. For some nurses, one area of conflict is the attitude toward time and waiting that is part of some cultures. The time orientation of Hispanic and African-American ethnic groups is in the present. For example, African-Americans are flexible in their time orientation; an African-American family may be late for or miss appointments because other issues take precedence, and they may not communicate this to the health agency. Hispanics, too, have a relaxed view of time. Whereas the dominant culture in the United States says that “time flies,” the Hispanic says that “time walks.”
The Japanese, on the other hand, consider time to be valuable and to be used wisely. They tend to be punctual for medical appointments and persistent in following prescribed regimens. A Vietnamese family will subordinate time to values considered to be more significant, such as propriety. They may be late for an appointment because of an overextended visit by a friend in their home. In general, Asian-Americans view the American focus on time as offensive. They spend hours getting to know people and view predetermined, abrupt endings as rude. Introductory small talk is considered good manners.
Navajo Indians view time on a continuum with no beginning and no end. The present-time orientation may cause a Navajo to eat two meals a day today, four meals tomorrow, no meals the next day, and three meals the day after. This becomes an important nursing consideration if a Navajo is told to take medication with meals to ensure three doses per day.
In many cultural groups the mother assumes the responsibility for health care; in others both parents are involved equally in relationships with health workers. A somewhat different approach is apparent in some of the Asian cultures. For example, a Vietnamese or Filipino father, as unquestioned head of the family, is traditionally the one who interacts with persons, including health care providers, outside the family unit. In the Hispanic family the father, as head of the house, makes decisions regarding illness and treatment of adult family members, but the grandmother in the extended family is consulted regarding child care. Usually the family confers with other members before reaching a decision regarding treatment or hospitalization of a child. The Arab family also relies on others to give advice and guidance in a time of crisis. A Japanese father may appear to be passive and uninvolved but actually is involved according to his own cultural standards.
NURSING ALERT
In working with families, it is essential for nurses to identify key members and decision makers; failure to include these significant individuals in teaching can seriously hinder adherence to the care plan.
Nurses should learn about any specific attitudes regarding the manner of approach to a child in a given culture. Navajo Indians do not like a stranger near their infants. They fear that the stranger may “witch” the child and cause the child harm. On the other hand, if a stranger, particularly a woman, lavishes attention on a Hispanic infant but fails to touch the child, some Hispanics believe the infant will develop symptoms of the “evil eye” (see p. 33). Vietnamese and Korean families may become upset if a newborn is admired at length for fear the evil spirits will overhear and desire the infant.
Some groups, such as the Amish, consider a child’s admission to the hospital a family affair, with all members gathering to support and console the child and parents. In other groups the family is willing to relinquish the care of the child to the hospital authority without interference. Their visits with the child are short, although intense, but hospital staff may misinterpret this behavior as disinterest or abandonment.
All ethnic groups are entitled to be treated with dignity and respect. Family members should be addressed by their last names; many groups consider it an affront to be called by their first names. Stereotyping is to be condemned. People are individuals who are evaluated in relation to their cultural standards, needs, and preferences. For example, believing that fathers are never involved in the direct care of their child can result in wrong assumptions about a culture (Fig. 2-4).

Fig. 2-4 Many fathers assume an active parenting role. (Courtesy E. Jacob, Texas Children’s Hospital, Houston.)
Nurses who are members of a majority culture may encounter tension and distrust in a child from a minority culture as a result of the child’s learned conceptions or relationships with other persons in the majority group. Based on these perceptions, minority children may suspect that nurses have hostile feelings toward them and fear ill treatment. When such children are hospitalized, this suspicion increases the feelings of loneliness and helplessness that accompany fearful events and separation from families. The reverse situation may be encountered by a nurse from a minority culture attempting to meet the needs of a child who has been conditioned to view the nurse’s cultural or ethnic group as inferior. Either situation is more likely to occur if the nurse or the child has had little or no personal contact with the other’s culture. For example, a child from a minority culture from the inner city who lives in a neighborhood and attends school only with children from his or her minority culture may be more suspicious of a nurse from a different culture than would a child from the same minority group who lives in a culturally diverse neighborhood or attends an integrated school. Becoming familiar with cultures different from one’s own and making an effort to know each other as individuals can shatter myths and, with time, build the trust needed to establish rewarding relationships between children, their families, and the nurse.
Communication
Communication is basic to all human relationships, but it may be a source of distress and misunderstanding between persons from different ethnic groups, especially if the languages are different. Prejudice is one of the biggest barriers to cross-cultural communication. The Office of Minority Health and Health Disparities of the U.S. Department of Health and Human Services has established national standards on culturally and linguistically appropriate services in health care. Health care organizations must ensure the competence of language assistance provided to person with limited English proficiency by interpreters and bilingual staff. Family and friends should not be used for interpretation services except on the patient’s request (Shaw-Taylor, 2002). (See Communicating with Families Through an Interpreter, Chapter 6.)
Part of culturally sensitive communication is taking time to assess beliefs and values. In a study on childhood asthma, management researchers discovered that parents who believed asthma to be intermittent rather than a chronic condition provided suboptimal treatment to their child (Yoos, Kitzman, Henderson, et al, 2007). It is vital that the family members fully understand all implications of a child’s care and management before they consent for special procedures or assume responsibility for the child’s medication administration. Some persons with poor or limited language comprehension may simply smile and nod in agreement if they do not understand the questions or directives. It is not uncommon for an Asian family to indicate “yes” when in fact they mean “no” in order to avoid social disharmony. They tend to address issues indirectly rather than through confrontation and may become evasive when direct questioning makes them uncomfortable.
Nonverbal communication is a practiced art in many Native American tribes, and the members are highly sensitive to body language. They emphasize periods of silence to formulate thoughts in preparation for speech and often remain silent after listening to others to properly assimilate what has been said. Interruption, interjection, or haste to arrive at a conclusion is perceived as immature behavior.
Different cultures view eye contact differently. Although Caucasians are advised to look people straight in the eye, persons in some ethnic groups avoid eye contact and become uncomfortable when conversing with health care workers. In non-Western cultures a patient may not look directly into the nurse’s eyes as a sign of respect. Some Native Americans make eye contact during the initial greeting, but consider continued, unwavering eye contact insulting and disrespectful. Asians may consider eye contact a sign of hostility or impoliteness.
The level of comfort with body space or distance from others varies among cultures. Caucasians are generally comfortable at arm’s length, Hispanics tend to get closer, and some Asians prefer a greater distance. Also, gestures may have different meanings. For example, some Asians consider pointing with a finger or foot disrespectful. Some Native Americans consider vigorous handshaking a sign of aggression, whereas to Caucasians the gesture is a sign of goodwill and strong character.
Families may be reluctant to question or otherwise initiate contact with health professionals. In Asian cultures, for example, it is considered a sign of disrespect to question persons of authority. A Japanese family may wait silently rather than ask or question. They believe the health professionals know best and will meet their needs without being asked. They also think it is important to avoid criticism. Criticism can cause the Japanese-American to “lose face,” to feel ashamed, which is highly undesirable.
Language has been considered the biggest barrier to the use of health care services by many families, especially Southeast Asians (Mattson, 1995). Often, families may have poor language comprehension, so it is necessary to speak slowly and carefully, not loudly, when conversing with them. Many persons are able to read and write English better than they can speak or understand it. Also, people usually revert to their dominant language in anxiety-provoking situations, even if they are able to communicate satisfactorily under ordinary circumstances.
Terms of address and use of first and last names vary among cultures and can create confusion in institutions. For example, in Asian cultures, the family name is given first in respect for the family and the given names follow. Therefore all siblings in a family have the same first name (or, in some families, the same middle name). The Mennonites refer to children as sons and daughters of a particular parent, such as “Josiah’s son,” rather than by the children’s names.
Although all people share the basic emotions, there are decided ethnic variations in the ways emotions are expressed. People in some cultures (e.g., Italian, Latin, or Jewish background) express emotions openly and are accustomed to sharing their sorrows and joys with family and friends. Conversely, Nordic and Asian groups are more restrained in expressing emotion.
Health care providers generally ask questions and use handouts, booklets, and—particularly with children—dolls and pictures as communication aids. This is uncommon in some cultures. For example, Native American healers ask few questions and do not use forms. Nurses need to consider both verbal and nonverbal communication techniques to interact effectively with children and their families from different cultures (see Nursing Care Guidelines box).
 NURSING CARE GUIDELINES
NURSING CARE GUIDELINES
Culturally Sensitive Interactions
Invite family members to choose where they would like to sit or stand, allowing them to select a comfortable distance.
Observe interactions with others to determine which body gestures (e.g., shaking hands) are acceptable and appropriate. Ask when in doubt. Know when physical contact is prohibited.
Observe for cues regarding appropriate eye contact. Avoiding eye contact may be a sign of respect.
Learn appropriate use of pauses or interruptions for different cultures.
Ask for clarification if nonverbal meaning is unclear.
Learn if smiling indicates friendliness or if it is taboo (Spector, 2009).
Learn proper terms of address.
Use a positive tone of voice to convey interest.
Speak concisely and thoughtfully, not loudly, when families have poor language comprehension.
Learn basic words and sentences of family’s language, if possible.
When asking questions, tell family why the questions are being asked, the way in which the information they provide will be used, and how it might benefit their child.
Repeat important information more than once.
Always give the reason for a treatment or prescription.
Use information written in the family’s language.
Arrange for the services of an interpreter when necessary (see Chapter 6).
Learn from families and representatives of their culture methods of communicating information without creating discomfort.
Address intergenerational needs (e.g., family’s need to consult with others).
Food Customs
Food customs and symbolism of various cultural, ethnic, and religious groups are an integral part of their lives. Although in a large country such as the United States most people have adopted the eclectic food habits that have evolved over generations, many still retain ethnic and geographic food traditions and preferences. Special holidays, ceremonies, and life experiences such as births, birthdays, weddings, and death are often marked by special food items or feasts. In many cultures specific food practices are followed during pregnancy in the belief that certain foods damage or benefit the developing fetus. The distinctive food customs of ethnic groups are a product of their native environment, determined by availability.
A number of restrictions are related to food items. Some have a physiologic origin, such as lack of dairy foods in the diets of some persons of African or Asian ancestry with lactose intolerance. Others are religious restrictions, such as kosher foods and food preparation of the Orthodox Jewish faith and the vegetarian diet of Seventh Day Adventists. (See Vegetarian Diets, Chapter 13.)
Children in a strange environment, such as the hospital, feel much more comfortable when they are served familiar foods. Hospital food often tastes strange and bland, especially to children who enjoy the highly seasoned foods of their culture. Also, the family may be concerned that the child is not receiving foods appropriate to their culture and beliefs. When possible, provide the children’s ethnic foods or allow families to bring favorite foods that are not on the hospital menu. Concern for differences in food habits and patterns projects an attitude of respect for the family’s ethnic or religious heritage (Ohio State University Extension, 2005).
It is also important for nurses and other health care providers to be mindful of the meaning of food and eating within a family or community. Feeding and food preparation are ways in which families nurture and care for one another. This is especially true in the parent-child relationship. Parents and other family members may struggle with this desire to feed and nurture their child in circumstances when the child does not want to eat or cannot tolerate oral intake (i.e., a child receiving chemotherapy). Nurses can encourage families to nurture the sick child in other ways, such as touch, reading, or other enjoyable activities.
Health Beliefs and Practices
The nurse encounters people of many different racial and ethnic origins in the process of meeting the health needs of children and families. Some of these families have become so enculturated to the majority culture that their health beliefs and practices are consistent with those of the health care system. For many families, however, traditional practices and beliefs are an integral part of their daily lives. Health care workers should be aware that other people might live by different rules and priorities, which decisively influence health-related behavior.
A model for learning about health traditions that differ from the Western, or modern, health care system is based on three dimensions:
1. What are the physical aspects of caring for the body (e.g., are there special clothes, foods, medicines)?
2. What are the mental parts of caring for health (e.g., feelings, attitudes, rituals, actions)?
3. What are the spiritual aspects of health (who I am, spiritual customs, prayers, healers)?
For each of these dimensions, one must consider the cultural traditions used to maintain health, protect health, and restore health (Spector, 2009).
Health Beliefs
The beliefs related to the cause of illness and the maintenance of health are an integral part of a family’s cultural heritage. Often inseparable from religious beliefs, they influence the way families cope with health problems and respond to health care providers. Predominant among most cultures are beliefs related to natural forces, supernatural forces, and imbalance between forces.
Natural Forces
The most common natural forces held responsible for ill health if the body is not adequately protected include cold air entering the body and impurities in the air. For example, a Chinese parent may overdress the infant in an effort to keep cold wind from entering the child’s body. The Chinese believe that cold weather, rain, or wind is responsible for “cold” conditions. They also believe that an innate energy called chi enters and leaves the body through the mouth, nose, and ears and flows through the body in definite pathways, or meridians, at specific times and locations. The Chinese believe that a lack of chi and blood causes fatigue, low energy, and a variety of ailments.
In the African-American culture, some individuals believe natural phenomena such as phases of the moon, seasons of the year, and planet positions affect the body and its processes; therefore health maintenance is strongly associated with the ability to read “the signs.” Some cultures consider behaviors such as overeating, overwork, anxiety, and inadequate food and sleep to be natural causes of illness. Most Native Americans consider health to be a state of harmony with nature and the universe.
Supernatural Forces
High on the list of causes of illness are forces beyond comprehension and logical explanation. Some cultures view evil influences such as voodoo, witchcraft, or evil spirits as causes of illness, especially those illnesses that cannot be explained by other means.
A health belief that is common among people from Latin American, Mediterranean, some Asian, and some African societies is the concept of the “evil eye” (Spector, 2009). It is part of the concept of health as a state of balance and illness as a state of imbalance (see following section). Strength and power are associated with the evil eye; therefore, as long as an individual’s strength and weakness remain in balance, he or she is unlikely to become a victim of the evil eye. Weaknesses are not necessarily physical. For example, an excess of some emotion, such as envy, can create weakness. Infants and small children, because of immature development of their internal strength-weakness states, are especially vulnerable to the gaze of the evil eye. Consequently, the evil eye serves to rationalize an inexplicable onset of illness in children who display symptoms such as restlessness, crying, diarrhea, vomiting, and fever.
Health Protection
Cultural traditions used in the protection of health may include protective objects, which may be worn, carried, or hung in the home or room. For example, amulets are objects or charms that are worn on a string or chain to protect the wearer from the evil eye or evil spirits. It is important to allow people to wear these objects in the health care setting. Another cultural practice is the inclusion of substances in the diet that protect health. For example, the ginseng root is used to “build the blood” in the Chinese culture. Religious practices, such as burning candles or prayer, are also traditions used to protect health (Spector, 2009).
Imbalance of Forces
The concept of balance or equilibrium is widespread throughout the world. One of the most common imbalances supported by the Hispanic, Filipino, Chinese, and Arab cultures is that which exists between “hot” and “cold.” This belief is reputedly derived from the Hippocratic theory of humoral pathology, which states that illness is caused by an imbalance of the four humors: phlegm, blood, black bile, and yellow bile (Sekhon, 1996). “Hot” and “cold” describe certain properties and conditions completely unrelated to temperature. Diseases, areas of the body, foods, and illnesses are classified as either “hot” or “cold.” In Chinese health belief the forces are termed yin (cold) and yang (hot) (Wang and Martinson, 1996). To maintain health and prevent illness, these forces must be kept in balance.
Illness is treated by restoring normal balance through the application of appropriate “hot” or “cold” remedies. A “cold” condition such as a respiratory disease is believed to be caused by exposure to cold weather, rain, or cold wind entering the body; it is treated by administration of “hot” foods, herbs, or drugs. Menstruation is considered a “hot” condition; therefore women are cautioned against ingesting “hot” foods, which might increase menstrual flow or produce cramping. Ingesting too much of either “hot” or “cold” foods can also be interpreted as a cause of illness.
Health care workers who are aware of this belief are better able to understand why some persons refuse to eat certain foods. It is often useful to discuss the diet with the family to determine their beliefs regarding food choices. It is possible to help families devise a diet that contains the necessary balance of basic food groups prescribed by the medical subculture while conforming to the beliefs of the ethnic subculture.
The “hot-cold” food classification may have adverse effects. For example, in some cultures newborn infants are often started on evaporated milk formulas. Evaporated milk is considered a “hot” food, whereas whole milk is viewed as a “cold” food. Infants tend to develop rashes, which are believed to be caused by “hot” foods; in such cases parents may decide to switch to whole milk. However, parents fear that it is dangerous to change too rapidly, so they often feed the child some type of neutralizing substance, which may create additional health problems. The nurse can help avoid such a problem by determining the family’s preference before discharge from the hospital and prescribing a formula that is agreeable to both the family and the practitioner.
Health Practices
Cultures have numerous similarities regarding prevention and treatment of illness. All cultures have some types of home remedies that they apply before seeking help from other persons. Within the ethnic community, folk healers who are endowed with the ability to “cure” maladies are sought for special situations and when home remedies are unsuccessful. The curandero (male) or curandera (female) of the Mexican-American community is believed to have healing powers that are a gift from God. The Asian consults an herbalist, knowledgeable in medicines, or perhaps an ethnic practitioner in Asian therapies, including acupuncture (insertion of needles), acupressure (application of pressure), and moxibustion (application of heat). Native Americans consult a variety of healers with specific skills and knowledge. Specialized medicine persons diagnose illness, provide nonsacred treatments (usually by way of massage and herbs), and care for souls. Other specialists perform services or effect cures through the use of spiritual means. Native Hawaiians consult kahunas and practice ho’oponopono to heal family imbalance or disputes.
The folk healers are powerful persons in their community and can acquire information about an illness without resorting to probing questions. They “speak the language” of the family who seeks help and often combine their rituals and potions with prayer and entreaties to God. They also are able to create an atmosphere conducive to successful management. Furthermore, they exhibit a sincere interest in the family and their problem.
Some folk remedies are compatible with the medical regimen and are useful to reinforce the treatment plan. For example, aspirin (a “hot” medication) is an appropriate therapy for “cold” diseases such as the common cold and arthritis. It is not uncommon to discover that a folk prescription has a scientific basis. In any case, respect practices that do no harm patients.
In cultures that believe in the concept, overcoming the effect of the evil eye usually requires specialized rituals conducted by the appropriate practitioner. For example, the Chicano curandero ascertains that the condition is truly the result of the evil eye by performing an assessment ritual and then performs a curative ritual. Sometimes faith in the folk practitioner delays obtaining needed medical treatment, although the practitioner usually suggests medical care if his or her ministrations are unsuccessful.
Health practices of different cultures may also present problems of assessment and interpretation. For example, certain cultural practices or remedies can be misdiagnosed as evidence of child abuse by uninformed professionals (Box 2-1). It is important to explain why some of these and other familiar remedies may now be considered harmful. Families need to understand how such practices can place them in jeopardy with child protective services, and they need to explore alternative measures that are more acceptable to the dominant culture (Hayes and Dreher, 1991).
Other cultural health remedies that are harmful include eating clay or excessive amounts of salt. A mercury compound, azogue (the Spanish name for quicksilver), is commonly used in Mexico and sometimes sold illegally to low-income Hispanic families in the United States as a remedy for diarrhea. Alert health care workers know that the drug can cause permanent central nervous system damage. A careful history can reveal these practices, but it may require the collaboration of a folk healer to convince a user to stop.
Faith healing and religious rituals are closely allied with many folk-healing practices. Wearing of amulets, medals, and other religious relics believed by the culture to protect the individual and facilitate healing is a common practice. It is important for health workers to recognize the value of this practice and keep the items where the family has placed them or nearby. It offers comfort and support and rarely impedes medical and nursing care. If an item must be removed during a procedure, it should be replaced, if possible, when the procedure is completed. The nurse should explain the reason for its temporary removal to the family to reassure them their wishes will be respected (see Family-Centered Care box).
 FAMILY-CENTERED CARE
FAMILY-CENTERED CARE
Cultural Awareness
I am a pediatric emergency nurse with a high regard for cultural diversity and a respect for healing practices and beliefs. I even made a manual for my emergency department that contains some of the information needed to help us understand and communicate with subcultures in the urban community we serve. Although I learned a great deal putting this manual together, it doesn’t come close to the lesson I learned with the following experience.
A 15-month-old Bosnian girl in status epilepticus was carried in by her parents. They were frightened and spoke little English. I learned that the child had received a measles, mumps, and rubella (MMR) immunization the day before. As I proceeded to unwrap her from the blanket she was in, I quickly assessed the ABCs (airway, breathing, and circulation). I noticed that she was warm (probably a febrile seizure) and that a rag soaked in alcohol was tied around each thigh. Focusing on her potential airway compromise and trying to calm the parents, I proceeded to put an oxygen mask on her, undress her for a full assessment, and remove the alcohol rags. I spoke to the parents all the while in a calm, soothing voice. Once I had established an intravenous line and given her lorazepam (Ativan), the seizures stopped. So did the communication between her parents and me. I noticed that they would no longer give me eye contact, and the mother would not even speak to me after the seizures stopped. It wasn’t until I was returning to the department from admitting her that I realized why they might have stopped communicating with me—I had removed the rags! Had I only thought to replace the rags or asked their permission to remove the rags, things may have been different.
Laura L. Kuensting, MSN(R), RN
Nurses can be most effective when operating from a multicultural perspective, which means using appropriate aspects of the culture in question to develop culturally acceptable health care interventions. When the folk practices do not interfere with the patient’s welfare, they need not be discouraged. Often a compromise can be reached that accomplishes the nurse’s goal while maintaining the patient’s dignity and self-esteem.
NURSING ALERT
Avoid attacking traditional health cultural beliefs and practices as wrong or harmful, or implying that biomedical measures are uniformly correct and effective and the only way to prevent illness or treat sickness. Such attacks usually result in rejection of biomedical health care practitioners and health teaching based on biomedicine or scientific facts.
Importance of Cultural Competence to Nurses
A consensus exists among nurses that cultural competence of professional nursing practice should be raised (Lester, 1998). The challenge for nurses is to gain knowledge about cultural care values, beliefs, and practices and to use this knowledge in the care they provide (Leininger, 2001). To understand and deal effectively with families in a multicultural community, nurses must be aware of their own attitudes and values. Nurses, too, are a product of their own cultural background and education. They are part of the “nursing culture.” Nurses function within the framework of a professional culture with its own values and traditions and, as such, become socialized into that culture by educational programs and later by the work environment and professional associations.
Frequently nurses and other health care workers are not aware of their own cultural values and how those values influence their thoughts and actions. A model for self-examination on cultural competence is the ASKED model (Box 2-2). Recognizing that a behavior may be characteristic of a culture rather than being an “abnormal” behavior places nurses at an advantage in their relationships with families. Ethnocentric approaches to nursing care are ineffective in meeting health and nursing needs of diverse cultural groups of patients (American Nurses Association, 1991). When nurses respect the cultural differences of a family, they are better able to determine whether the behavior is distinctive to the individual or a characteristic of the culture. What appears to be puzzling behavior may simply be the customary response in the culture (e.g., expression of emotion).
Cultural standards and values, the family structure and function, and past experiences with health care influence a family’s feelings and attitudes toward health, their children, and health care delivery systems. It is often difficult for nurses to be nonjudgmental and objective in working with families whose behaviors and attitudes differ from or conflict with their own. The nurse needs to understand how his or her own cultural background influences the way care is delivered (American Nurses Association, 1991).
Relying only on one’s own values and experiences for guidance can result in frustration and disappointment. It is one thing to know what is needed to deal with a health problem; it is often more difficult to implement a fruitful course of action unless nurses work within the cultural and socioeconomic framework of the family (see Critical Thinking Exercise, p. 23).
It is essential to make an effort to adapt ethnic practices to the family’s health needs rather than attempt to change longstanding beliefs. To aid their efforts to understand and respect the cultural beliefs of families, nurses should have a readily available resource file containing pertinent information about the cultural and subcultural characteristics of the community in which they practice (e.g., traditional practices related to infant feeding practices and the time and manner of weaning and toilet training). Cultural competence is a process that is facilitated by recognizing cultural differences, integrating cultural knowledge, and acting in a culturally appropriate manner (Munoz and Luckmann, 2005) (see Cultural Competence box).
CULTURAL COMPETENCE
Five Components of Cultural Competence
Cultural competence includes following five components (Munoz and Luckmann, 2005):
1. Cultural awareness—A cognitive process through which the nurse appreciates and is sensitive to the cultural values of the patient and family
2. Cultural knowledge—The foundation the nurse builds through formal and informal education that includes world views of different cultures, values, beliefs, and perceptions about health and illness
3. Cultural skill—The ability to include cultural data in the nursing assessment through the collection of cultural data in the health interview and observations
4. Cultural encounter—The process through which the nurse seeks opportunities to engage in cross-cultural interactions directly or indirectly
5. Cultural desire—The genuine and sincere motivation to work effectively with minority clients; can only be achieved if the individual wants to engage in the process of acquiring cultural competence
Cultural Awareness
Cultural and religious rituals are important practices among families from various cultures. An example is the Jewish upsherenish ceremony, which celebrates a boy’s first haircut when he reaches 3 years of age. Any procedure requiring haircutting, such as placement of an intravenous line in a scalp vein, must be discussed with parents to obtain their permission.
Table 2-1 outlines some characteristics of selected cultures. Nurses must assess the cultural and religious practices of families to identify how these practices are similar to and different from those of their own cultural and religious backgrounds. Guidelines for culturally sensitive interactions are described on p. 33.
TABLE 2-1
BROAD CULTURAL CHARACTERISTICS RELATED TO HEALTH CARE OF CHILDREN AND FAMILIES
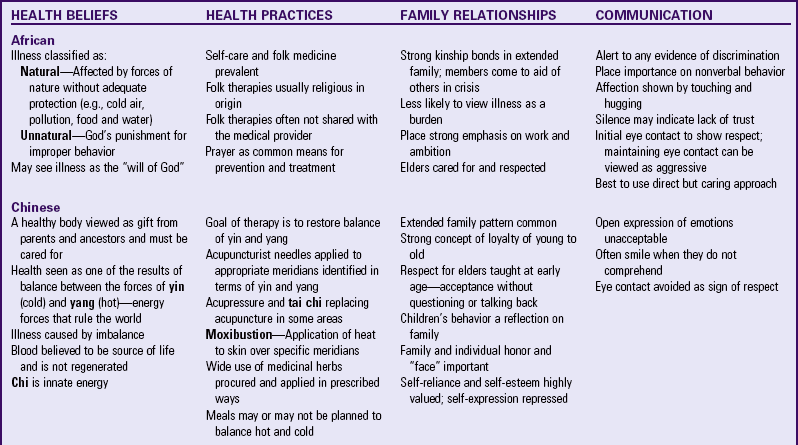
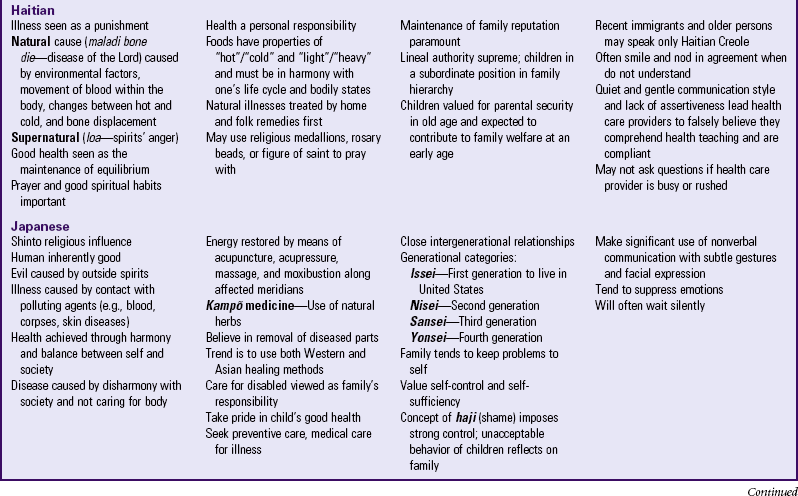
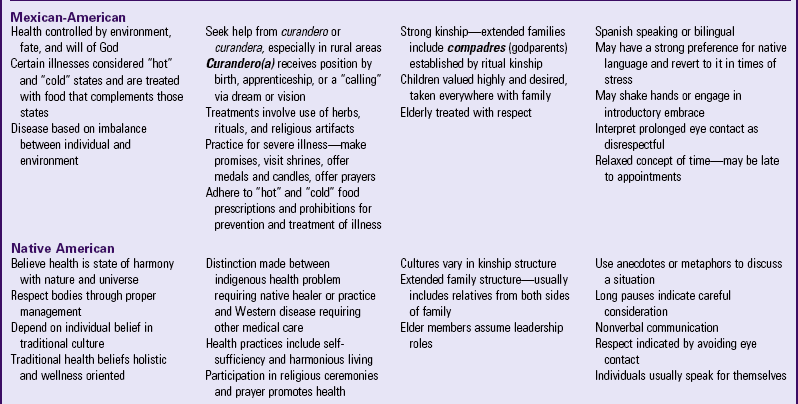
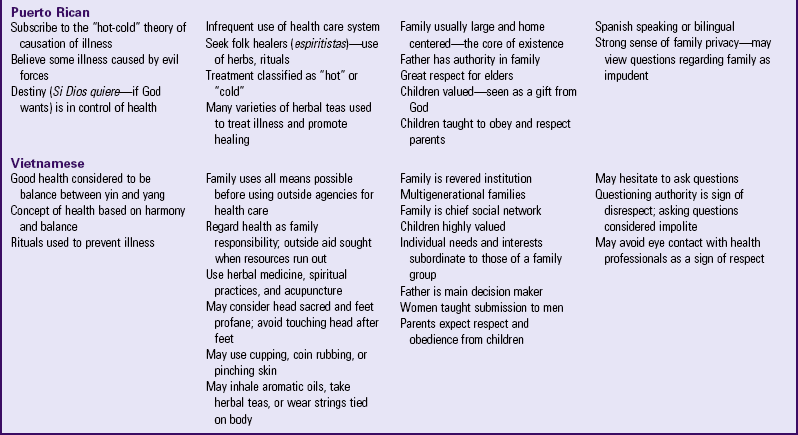
Data from Galanti G: Caring for patients from different cultures, ed 3, Philadelphia, 2004, University of Pennsylvania Press; Lipson JG, Dibble SL, Minarik PA: Culture and clinical care: a pocket guide, San Francisco, 2005, UCSF Nursing Press; Purnell LD, Paulanka BJ: Transcultural health care: a culturally competent approach, Philadelphia, 2003, Davis; and Spector RE: Cultural diversity in health and illness, ed 6, Upper Saddle River, NJ, 2004, Pearson Prentice Hall.
NURSING ALERT
These generalizations are presented to help nurses learn the unique beliefs and practices of various groups and are not meant to be stereotypes of any group. It is critical to remember that no cultural group is homogeneous, every racial and ethnic group contains great diversity, and knowledge of a culture may not reflect an individual member’s beliefs (Nance, 1995; Kleinman and Benson, 2006).
Concepts that come from medical anthropology can provide a framework for addressing health care issues. These concepts can have a direct impact on patient care. It leads the nurse away from an ethnocentric or medicocentric view of the health care encounter into the health care reality as constructed by the patient and family. This is relevant for addressing many of the problems that plague the American health care system: patient dissatisfaction with the health care they receive, unequal distribution of high-quality health care, and excessive cost (Kleinman, Eisenberg, and Good, 1978; Kleinman and Benson, 2006).
It is also important for nurses to recognize that disease and illness are distinct entities. Clinicians diagnose and treat diseases, “abnormalities in the structure and function of body organs and systems” (Kleinman, Eisenberg, and Good, 1978). Patients suffer from and deal with illnesses, “the human experience of sickness” (Kleinman, Eisenberg, and Good, 1978). Illness and disease are not interchangeable; illness may occur even when disease is not present, and the course of a disease may vary substantially from the experience of illness.
Illness is culturally constructed; an individual’s culture influences how a sickness is perceived, labeled, and explained. Culture also influences the meaning assigned to the illness, the role the individual with the sickness adopts, and the response of the family and community to the sickness.
Tension may arise when the perception of the illness and disease varies widely among the patient, family, and health care team. Failure of health care providers to recognize these disparities may be partially to blame in cases of noncompliance, delivery of inadequate care, and patient or family dissatisfaction. To begin addressing these issues, it is important for nurses to understand the various domains of health care in which individuals operate in American society: professional (health care providers and institutions), popular (family, community, and lay literature), and folk (nonprofessional healers) (Kleinman, Eisenberg, and Good, 1978). Each domain possesses a method for defining and explaining the sickness and what should be done to address it. The challenge for nurses and other health care providers is to address this disconnect with families and develop mutually agreed on goals. Nurses are in a prime position to assume this role, since understanding the human response to disease is central to their role. In addition, collaboration with the child and family is central to the role of the pediatric nurse.
Not all health care providers feel adequately prepared to care for culturally diverse populations. A study of 1700 resident physicians by Betancourt (2007) revealed that 25% to 30% of them did not feel prepared to deal with families who are mistrustful of the health care system, those with limited English proficiency, those whose health perspective differs from a Western-based model, those adults who incorporate other family into the decision-making process, or those who bring their spirituality into the health care environment. Unfortunately, the numbers may not be too different for nursing and other health care professionals. Such statistics are a wake-up call for anyone who strives for high-quality patient care.
One method of addressing this disconnect with families and beginning collaboration is by understanding the family’s explanatory model of illness. The questions in Box 2-3, developed by Arthur Kleinman, a physician and anthropologist, aim to elicit an individual’s beliefs about the disease or illness, the meaning attached to it, goals, and expectations of the outcome and role of the health care provider. The wording may need to be adapted depending on the child, family, setting, and clinical issue to be addressed. Nurses can then point out areas of discrepancy for further dialogue, negotiation, and collaboration. This discussion, when conducted with a genuine interest in the family and child’s perspective, is a significant step in building trusting relationships, promoting adherence, decreasing disparities, and increasing health care satisfaction.
Hereditary Factors
Some groups of people are more susceptible or more resistant to certain illnesses than other groups. An innate susceptibility is acquired through generations of evolutionary changes that take place within constrained or segregated populations. The proximity to disease, environmental factors, and general physical status are significant factors associated with health problems.
Historically, the increased health risks associated with ethnicity have been explained in terms of genetic differences or related factors such as socioeconomic status (Scribner, 1996). The genetic constitution of individuals in groups is known to influence the degree to which they are susceptible to a specific disorder. It may be a result of an inherent lack of resistance to a disease organism; a trait that is an advantage in one environment but places the possessor at a disadvantage in another; or intermarriage within a relatively narrow range of geographic, ethnic, or religious restrictions.
A classic example of a geographic constraint is the common communicable disease rubeola. The rubeola virus, or the populations that were continually exposed to it, became altered in such a way that the disease was considered to be a universal disease of childhood from which the majority of children suffered without ill effects. When other populations (e.g., the inhabitants of the Hawaiian Islands) were exposed to the virus by explorers and missionaries, they experienced a violent response that resulted in high mortality.
Another communicable disease, tuberculosis, appears to be more prevalent in certain ethnic groups such as the Native Americans of the Southwest, Vietnamese immigrants, and Mexican-Americans. In many populations it is difficult to determine how much the increased incidence can be attributed to ethnic factors and how much is related to lifestyles in the lower social strata.
A number of diseases show ethnic or racial differences (Box 2-4). For example, Tay-Sachs disease, characterized by early neurologic deterioration and mental retardation, primarily affects Ashkenazi Jewish families, particularly those of northeastern European origin, whereas Sephardic Jewish families appear to be no more at risk for the disease than other populations. The incidence of cystic fibrosis is highest in Caucasians and almost nonexistent in Asians, and the rare affected African-Americans are usually in areas where there is likely to be mixed ancestry. A classic disorder of African-Americans is sickle cell disease (see Chapter 35); however, the incidence of cardiovascular disease, pneumonia, and diabetes is also high in this group. Native Americans have particularly high rates of diabetes, tuberculosis, diarrhea, alcoholism, and suicide. Consider racial and ethnic differences in relation to diseases and defects as they are discussed throughout the book.
Common food items and drugs may cause health problems in certain ethnic groups. For example, people of Mediterranean, African, and Asian origin frequently have glucose-6-phosphate dehydrogenase (G6PD) deficiency. They may develop acute hemolytic anemia after they ingest fava (horse or broad) beans or certain drugs such as aspirin preparations, sulfonamides, or primaquine. Other groups, especially southern Europeans, Jews, Arabs, African-Americans, Asians, and Native Americans, have a deficiency of lactase, the enzyme needed to metabolize lactose. Ingestion of lactose can cause abdominal distention, flatus, and diarrhea. Unknowing but well-meaning health care workers may be responsible for these symptoms in their patients when they prescribe foods or food supplements containing lactose as sources of nutrients.
Physical Characteristics
Members of different racial groups have observable differences in physical appearance. The most obvious are skin and hair coloring and texture. Skin color is determined by the amount of melanin in the skin. People from countries located near the equator have darkly pigmented skin, which protects the skin from the year-round exposure to the sun’s rays; those from northern countries have light skin, which provides for maximum exposure to the sun’s rays (necessary for vitamin D metabolism) during the short daylight hours. Skin color can show wide variations between these two extremes because of geographic origin or intermixing of persons with dark and light skin color.
As a consequence of the dark pigmentation, the detection of skin color changes can be difficult and requires modification of assessment techniques. For example, vasomotor alterations, cyanosis, and jaundice are not easily recognized in very dark skin. Variations in skin color can alter the appearance of the skin in a given circumstance (see Table 6-8).
In the newborn, variations are often related to racial or ethnic origin. For example, newborn infants of Asian and African-American parents are smaller than infants of Caucasian parents, and bluish pigmented areas (mongolian spots) on the sacral region are a common observation in Asian, African-American, Native American, and Mexican infants. It is important that health care providers be familiar with these birthmarks. They should be documented at newborn examinations and subsequent visits so they are not suddenly interpreted as bruises (Garwick and Auger, 2000).
Evaluation of stature and body build reveals some racial tendencies. Children from Asian countries are commonly smaller, falling below the 10th percentile on weight and height charts used for children in the United States. This difference in stature can lead to misinterpretation of health status and capabilities. A small child may appear intelligent for body size but be of average mental ability for age.
Religious Influences
Probably the most influential factor shaping the U.S. culture is the Judeo-Christian faith. Many immigrants came to the United States for religious freedom and established a religious and moral atmosphere that persists today. However, individual differences are part of the general culture.
The family’s religious orientation dictates a code of morality and influences the family’s attitudes toward education, male and female role identity, and their ultimate destiny. It may also determine the school that the children attend, their companions, and often their mate selection. Religious beliefs are such an integral part of many cultures that it is difficult to distinguish the culture from the religion. In a few instances, such as in the Mennonite and Amish communities, religion is the basis for a common way of life that determines where the children are raised and their lifestyle.
Religious Beliefs
Religious and spiritual dimensions are among the most important influences in many people’s lives (Fig. 2-5). The terms religion and spirituality are often used interchangeably; however, spirituality includes religion. Both religion and spirituality lend meaning in life and provide a source of love and relatedness between individuals and their God (Lukoff, Lu, and Turner, 1995). Nurses promote holistic nursing care through an integration of spiritual and psychosocial care. The care focuses on activities that support a person’s system of beliefs and worship, such as praying, reading religious materials, and performing religious rituals. Meeting the spiritual needs of the child and family can provide strength, whereas unmet spiritual needs can result in spiritual distress and debilitation (Fulton and Moore, 1995). In practice, application of the nursing process for spiritual care (Box 2-5) can enhance the spiritual well-being of the child and family.

Religion influences the lifestyles of most cultures. Among many groups, illness, injury, or death is believed to be sent by God as a punishment for sin. Some may believe that health workers will be unable to help a person whom God is punishing and may express a fatalistic attitude toward treatment, stating that the illness is “the will of God.” Others view it as a test of strength, like the testing of Job in the Bible, and strive to remain faithful and overcome the conflicts.
The nurse clarifies dietary restrictions with the family, especially in denominations with many variations. Except when specific religious practices (such as fasting) interfere with the child’s health or therapy, the family’s wishes are respected. The nurse should ask family members whether they want a clergy member present and whether they prefer hospital staff to call or prefer to do this on their own.
It is important to determine the family’s wishes regarding baptism, rites or practices related to death, and other religious rituals (such as circumcision, communion, or use of amulets or icons). Many religions have special clothing requirements, such as a cap (kippah) for the head (Orthodox Jews) or underclothes (Mormons). Respecting these rituals is especially important during a physical examination or preparation for surgery. An important role of the nurse is to be aware of families’ spiritual needs and convey an attitude of concern for this important element of the child’s care. Religion, which offers families understanding and spiritual support, is a valuable asset to health care. Table 2-2 outlines characteristics of selected religions with beliefs that affect health care.
TABLE 2-2
RELIGIOUS BELIEFS THAT MAY AFFECT NURSING CARE
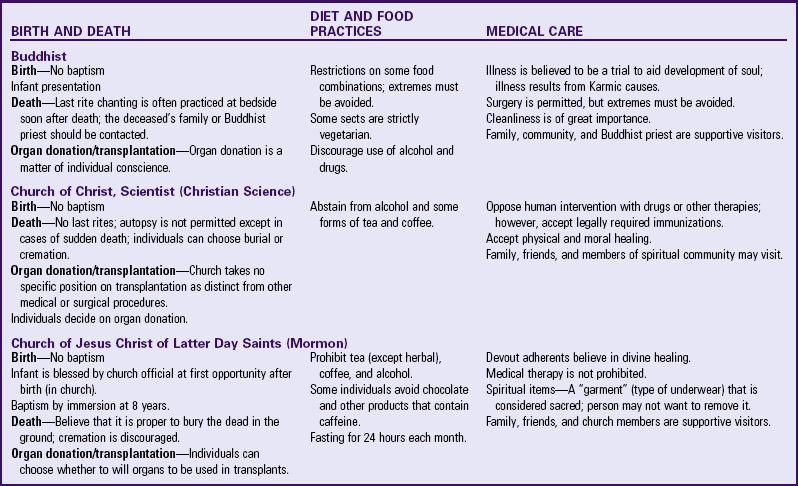
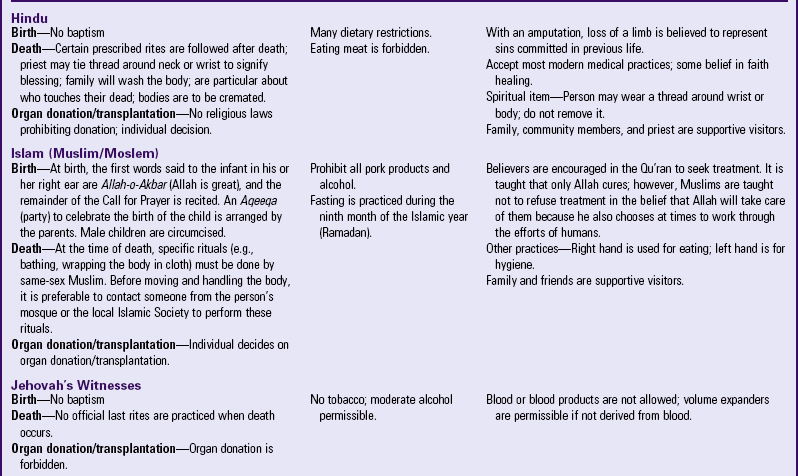
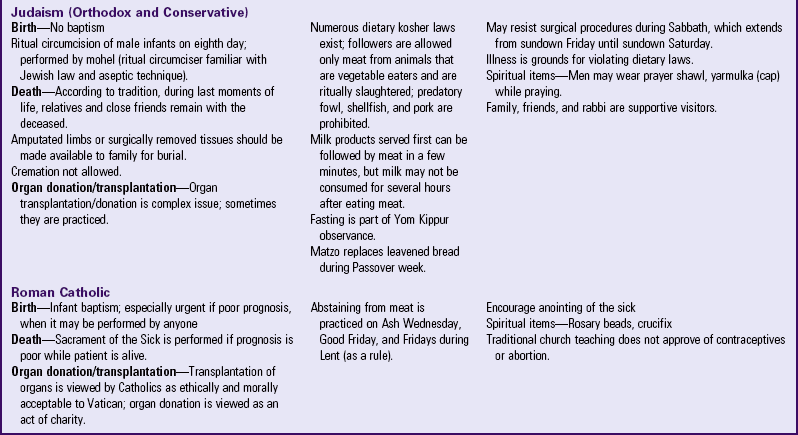
Data from Galanti G: Caring for patients from different cultures, ed 3, Philadelphia, 2004, University of Pennsylvania Press; Lipson JG, Dibble SL, Minarik PA: Culture and clinical care: a pocket guide, San Francisco, 2005, UCSF Nursing Press; Purnell LD, Paulanka BJ: Transcultural health care: a culturally competent approach, Philadelphia, 2003, Davis; Spector RE: Cultural diversity in health and illness, ed 6, Upper Saddle River, NJ, 2004, Pearson Prentice Hall.
In some instances the rights of the family and the responsibility of the state may be in conflict. For example, Jehovah’s Witnesses refuse blood transfusions for themselves and for their children. Parents, by law, have the primary obligation to care for and make decisions about their minor children. However, the legal principle of parens patriae says that the state has an overriding interest in the health and welfare of its citizens. Parents’ refusal of medical treatment for their child that is deemed essential can be interpreted as neglect. In addition to advocating for the child and family, the nurse’s role may include assuming the role of consultant to the staff and family regarding new, alternative methods of transfusion and, if necessary, coordinating with officials to petition juvenile or family court for temporary guardianship of the child.
Key Points
• Culture is the pattern of assumptions, beliefs, and practices, encompassing other products of human work and thoughts specific to members of an intergenerational group, community, or population.
• Nurses have a responsibility to understand the influence of culture, race, and ethnicity on the development of social and emotional relationships, childrearing practices, and attitudes toward health.
• A child’s self-concept evolves from ideas about his or her social roles.
• Primary groups are characterized by intimate contact, mutual support, and behavior constraint among members.
• Secondary groups have limited, intermittent contact; little mutual support; and no pressure for conformity.
• Culture influences a child’s self-esteem.
• Important subcultural influences on children include ethnicity, social class, occupation, schools, peers, biculture, and mass media.
• A trend that has significantly influenced the American family is increasing geographic and economic mobility.
• The minority group population is increasing in the United States, whereas the percentage of the Caucasian population is decreasing.
• Socioeconomic influences play a major role in opportunities for health promotion and wellness.
• Religious practices greatly influence health promotion beliefs in families.
• A child’s physical characteristics and susceptibility to health problems are related to ethnic and cultural variations of hereditary and socioeconomic forces.
• Groups of children suffering from greater physical and mental health problems are those living in poverty, those who are homeless, or those who have migrant families.
• Drug response, food sensitivity, disease resistance, physical characteristics, and disease states may demonstrate ethnic or cultural variations.
• Because verbal and nonverbal communication is an important cultural consideration, nurses need to acknowledge and respect their patient’s practices for productive interaction to occur.
• Cultural beliefs related to cause of illness and maintenance of health may focus on natural forces, supernatural forces, or imbalance of forces.
• The development of cultural competence is continual and an important concept in the nursing process. Nurses can facilitate this process by recognizing cultural differences, integrating cultural knowledge, and acting in a culturally appropriate manner.
• No cultural group is homogeneous; every racial and ethnic group contains great diversity.
Answers to Critical Thinking Exercise
1. An understanding of the Arab culture provides insight into the woman’s hesitancy to make decisions in her husband’s absence.
2. a.Typically in the Arab culture men make the decisions and women are expected to support these decisions.
b. The need for an interpreter is evident to make certain the mother understands the seriousness of the situation.
c. Knowledge of the process for obtaining approval for emergency procedures without informed consent will facilitate the best care for the child.
d. Appropriate documentation of how approval was obtained without parental consent is essential.
3. The first priority is to make certain the child is receiving the best care possible and that the necessary procedure is performed as soon as possible. The next priority is to ensure the mother understands the urgency of the situation by using an interpreter.
4. The child’s health status is most important at this time.
References
American Academy of Pediatrics, Committee on Public Education. Children, adolescents, and television. Pediatrics. 2001;107(2):423–426.
American Nurses Association. Position statement: cultural diversity in nursing practice. available at www.nursingworld.org/EthicsHumanRights, 1991. [(accessed December 2, 2009)].
Anderson, DR, Huston, AC, Schmitt, KL, et al. Early childhood television viewing and adolescent behavior: the recontact study. Monogr Soc Res Child Dev. 2001;66(1):I–VIII. [1-147].
Annie E Casey Foundation. 2009 Kids count data book: state profiles of child well-being. Baltimore: The Foundation; 2009.
Betancourt, J. Commentary on “Current approaches to integrating elements of cultural competence in nursing education. J Transcult Nurs. 2007;18(25s):25s–27s.
Carrillo, JE, Green, AR, Betancourt, JR. Cross-cultural primary care: a patient-based approach. Ann Intern Med. 1999;130(10):829–834.
Council on Communications and Media. Media violence—policy statement. Pediatrics. 2009;124(5):1495–1503.
Crom, DB. The experience of South American mothers who have a child being treated for malignancy in the United States. J Pediatr Oncol Nurs. 1995;12(3):104–112.
Dunn, AM. Culture competence and the primary care provider. J Pediatr Health Care. 2002;16(3):105–111.
Dykeman, C, Nelson, JR, Appleton, V. Building strong working alliances with American Indian families. Soc Work Educ. 1995;17(3):148–157.
Fulton, RA, Moore, CM. Spiritual care of the school-age child with a chronic condition. J Pediatr Nurs. 1995;10(4):224–231.
Garwick, A, Auger, S. What do providers need to know about American Indian culture? Recommendations from urban Indian family caregivers. Fam Systems Health. 2000;18:177–189.
Gentry, K, Quandt, SA, Davis, SW, et al. Child healthcare in two farmworker populations. J Commun Health. 2007;32(6):419–431.
Giger, JN, Davidhizar, RE. Transcultural nursing: assessment and intervention, ed 3. St Louis: Mosby; 1999.
Hayes, J, Dreher, C. Providing culturally sensitive care. In: Smith D, ed. Comprehensive child and family nursing skills. St Louis: Mosby, 1991.
Hindman, HD. Unfinished business: the persistence of child labor in the US. Employee Responsibilities Rights J. 2006;18(2):125–131.
Jordan, A. The role of media in children’s development: an ecological perspective. J Dev Behav Pediatr. 2004;25(3):196–206.
Klass, P, Needlman, R, Zuckerman, B. Reach out and get your patients to read. Contemp Pediatr. 2002;19(1):51–58.
Kleinman, A, Benson, P. Anthropology in the clinic: the problem of cultural competency and how to fix it. PLoS Medicine. 2006;3(10):1673–1676.
Kleinman, A, Eisenberg, L, Good, B. Culture, illness, and care: clinical lessons from anthropologic and cross-cultural research. Ann Intern Med. 1978;88:251–258.
Leavitt, M, Martinson, ID, Liu, C, et al. Common themes and ethnic differences in family caregiving the first year after diagnosis of childhood cancer, part II. J Pediatr Nurs. 1999;14(2):110–122.
Leininger, MM. The theory of culture care diversity and universality. In: Leininger MM, ed. Culture care diversity and universality: a theory of nursing. Sudbury, Mass: Jones & Bartlett, 2001.
Lester, N. Cultural competence: a nursing dialogue 2. Am J Nurs. 1998;98(9):36–42. [quiz 43].
Looman, WS. Defining social capital for nursing: experiences of family caregivers of children with chronic conditions. J Fam Nurs. 2004;10:412–428.
Looman, WS, Lindeke, LL. Health and social context: social capital’s utility as a construct for nursing and health promotion. J Pediatr Health Care. 2005;19(2):90–94.
Lukoff, D, Lu, FG, Turner, R. Cultural considerations in the assessment and treatment of religious and spiritual problems. Psychiatr Clin North Am. 1995;18(3):467–485.
Martinson, IM, Armstrong, V, Qiao, J. The experience of the family of children with chronic illness at home in China. Pediatr Nurs. 1997;23(4):371–375.
Mattson, S. Culturally sensitive perinatal care for Southeast Asians. J Obstet Gynecol Neonat Nurs. 1995;24(4):335–341.
Melendez, L. Parental beliefs and practices around early self-regulation: the impact of culture and immigration. Infants Young Child. 2005;18(2):136–146.
Munoz, CC, Luckmann, J. Transcultural communication in nursing. Clifton Park, NY: Thomson Delmar Learning; 2005.
Murdock, SH. Minority child population growth. In: Cosby AG, Greenberg RE, Southward LH, et al, eds. About children: an authoritative resource on the state of childhood today. Elk Grove Village, Ill: American Academy of Pediatrics, 2005.
Nance, TA. Intercultural communication: finding common ground. J Obstet Gynecol Neonat Nurs. 1995;24(3):249–255.
National Coalition to End Homelessness. Youth. available at www.endhomelessness.org/section/policy/focusareas/youth, 2009. [(accessed March 28, 2009)].
Ohio State University Extension. Cultural diversity: eating in America. available at www.nal.usda.gov/fnic/etext/000010.html, 2005. [(accessed April 20, 2005)].
Redlener, I. Homelessness and its consequences. In: Cosby AG, Greenberg RE, Southward LH, et al, eds. About children: an authoritative resource on the state of childhood today. Elk Grove Village, Ill: American Academy of Pediatrics, 2005.
Robinson-Zanartu, C. Serving Native American children and families: considering cultural variables. Lang Speech Hearing Serv Schools. 1996;27:373–384.
Rogers, G. Educating case managers for culturally competent practice. J Case Manage. 1995;4(2):60–65.
Scribner, R. Paradox as paradigm: the health outcomes of Mexican Americans. Am J Pub Health. 1996;86(3):303–304.
Search Institute. Developmental assets lists. available at www.search-institute.org/developmental-assets/lists, 2007. [(accessed December 2, 2009)].
Sekhon, SK. Insights into South Asian culture: food and nutritional values, Topics. Clin Nutr. 1996;11(4):47–56.
Shaw-Taylor, Y. Culturally and linguistically appropriate health care for racial or ethnic minorities: analysis of the US Office of Minority Health’s recommended standards. Health Policy. 2002;62:211–221.
Spector, RE. Cultural diversity in health and illness, ed 7. Upper Saddle River, NJ: Prentice-Hall; 2009.
Strasburger, VC, Donnerstein, E. Children, adolescents, and the media: issues and solutions. Pediatrics. 1999;103(1):129–139.
Strehlow, AJ, Amos-Jones, T. The homeless as a vulnerable population. Nurs Clin North Am. 1999;34(2):261–274.
Szilagyi, PG. Health insurance. In: Cosby AG, Greenberg RE, Southward LH, et al, eds. About children: an authoritative resource on the state of childhood today. Elk Grove Village, Ill: American Academy of Pediatrics, 2005.
Trawick-Smith, J. Early childhood development: a multicultural perspective, ed 4. Upper Saddle River, NJ: Prentice-Hall; 2006.
Thibodeaux, AG, Deatrick, JA. Cultural influence on family management of children with cancer. J Pediatr Oncol Nurs. 2007;24(4):227–233.
US Census Bureau. Overview of race and Hispanic origin: census 2000 brief. available at www.census.gov/prod/2001pubs/c2kbr01-1.pdf, 2001. [(accessed December 2, 2009)].
Wang, R, Martinson, IM. Behavioral responses of healthy Chinese siblings to the stress of childhood cancer in the family. J Pediatr Nurs. 1996;11(6):383–391.
Warda, MR. Mexican Americans’ perceptions of culturally competent care. West J Nurs Res. 2000;22(2):203–224.
Wertheimer, R. Poverty. In: Cosby AG, Greenberg RE, Southward LH, et al, eds. About children: an authoritative resource on the state of childhood today. Elk Grove Village, Ill: American Academy of Pediatrics, 2005.
Williams, LA, Kruse, L. A culture fair: a creative, fun, and informative method of cultural awareness education. J Staff Dev. 1999;15(2):71–74.
Yoos, HL, Kitzman, H, Henderson, C, et al. The impact of parental illness representation on disease management in childhood asthma. Nurs Res. 2007;56(3):167–174.