Chapter 45The Crus
Anatomy
The crus is located between the stifle and hock joints. Anatomy of the hock and stifle are discussed in Chapters 44 and 46. The medial aspect of the tibia lacks muscle covering and is easily palpated, but muscles and tendons cover the cranial, lateral, and caudal aspects. The tibia has proximal and distal physes and a separate center of ossification for the tibial tuberosity.
The fibula is lateral, does not share axial load, and fuses with the tibia to form the lateral malleolus. The proximal aspect of the fibula may develop from two or more separate centers of ossification, and fibrous union may persist throughout life. The result of this union is transverse radiolucent lines that are evident radiologically and should not be mistaken for fractures (see discussion of rare fibular fractures later).1,2
Muscles and tendons of the crus are important in locomotion and support of the hindlimb. The long digital extensor muscle originates from a common tendon with the fibularis tertius from the extensor fossa of the femur and is located cranially and laterally in the crus. The fibularis tertius courses distally to divide into dorsal and dorsolateral tendons of attachment. Avulsion injury of the tendon of origin of the fibularis tertius and long digital extensor causes a classic disruption of the hindlimb reciprocal apparatus.  The tibialis cranialis muscle is deep to the long digital extensor muscle and distally splits into two parts, the medial of which is called the cunean tendon (jack tendon) and may play a minor role in distal hock joint pain. The lateral digital extensor muscle originates proximally, and its tendon courses laterally over the tarsus and joins the long digital extensor muscle in the proximal metatarsal region. Myotenectomy of the lateral digital extensor tendon and muscle is often performed for management of stringhalt.
The tibialis cranialis muscle is deep to the long digital extensor muscle and distally splits into two parts, the medial of which is called the cunean tendon (jack tendon) and may play a minor role in distal hock joint pain. The lateral digital extensor muscle originates proximally, and its tendon courses laterally over the tarsus and joins the long digital extensor muscle in the proximal metatarsal region. Myotenectomy of the lateral digital extensor tendon and muscle is often performed for management of stringhalt.
The paired gastrocnemius muscles originate from the distal, caudal aspect of the femur and share a single, strong tendon that courses distally and inserts on the calcaneus. The superficial digital flexor and deep digital flexor muscles and tendons arise caudally. The superficial digital flexor tendon (SDFT) begins medial to the gastrocnemius tendon and courses from medial to caudal to attach to the calcaneus before continuing distally. The deep digital flexor tendon (DDFT) is deep to both the SDFT and the gastrocnemius tendons and courses distally over the plantaromedial aspect of the calcaneus, the sustentaculum tali. The combined SDFT and gastrocnemius tendons form the common calcaneal tendon, the major extensor of the hock, and injuries can cause partial or complete loss of hock support. The tarsal sheath begins in the distal, caudal aspect of the crus and surrounds the DDFT.
The fibular (peroneal) nerve originates from the sciatic nerve and branches in the proximal aspect of the crus to become the superficial and deep fibular nerves that run between the long digital extensor and lateral digital extensor muscles and tendons. The tibial nerve is palpable in the distal, caudal aspect of the crus, cranial to the common calcaneal tendon.
Clinical Characteristics and Diagnosis of Lameness of the Crus
Degree of lameness can vary from a subtle, high-speed lameness seen in horses with early stress-related bone injury to an acute, non–weight-bearing lameness, swelling, and deformity seen in horses with complete tibial fractures. Horses with tearing of the gastrocnemius tendon, musculotendonous junction, origin, and insertion have varying degrees of hyperflexion of the tarsocrural joint and partial loss of the reciprocal apparatus. Because the hock drops during weight bearing, the degree of pelvic hike is less than expected and the degree of lameness may be underestimated. Foals with fibularis tertius and long digital extensor avulsion injury lose integrity of the reciprocal apparatus and have swelling on the lateral, proximal aspect of the crus. Rarely, foals can injure the fibularis tertius distally near the tarsus. Fibularis tertius injury in adult horses may cause swelling of the distal, cranial aspect of the crus near the tarsocrural joint, but lesions in the midcrus are not associated with swelling. In calcinosis circumscripta, round-to-oblong, nonpainful mineralized masses are attached to the distal aspect of the lateral patellar ligament and lateral femorotibial joint capsule or collateral ligament.
No gait characteristics are pathognomonic for pain associated with the crus. Lameness of the crus is similar to that seen in horses with pain originating anywhere from the tarsus to the hind foot. Horses with tibial stress fractures have a shortened cranial phase of the stride and, most often, a stabbing type of hindlimb gait when viewed from behind. Injuries of the crus should be suspected when lameness is pronounced, but sites in the rest of the limb are eliminated by using diagnostic analgesia. In Thoroughbreds (TBs), in which the risk of tibial stress fractures is high, a tentative diagnosis of stress fracture is made when lameness is pronounced and recurrent after work.
Palpation of the crus should be done with the limb in both the standing and flexed positions, but this often yields no information. The medial side of the tibia is most easily felt, and occasionally in horses with tibial stress fractures, mild swelling is present and pain is elicited by deep compression (see Figure 6-27). Unfortunately, most tibial stress fractures involve the caudolateral cortex, and it is difficult to compress this area during palpation. Digital tibial percussion sometimes elicits a painful response in horses with tibial stress fractures, but there are many false-positive and false-negative responses. Forced tibial torsion with the limb in a flexed position may elicit pain in horses with tibial stress fractures (see Chapter 107), but I have found the results of this test to be inconsistent.
Diagnostic Analgesia
There is no practical method to use diagnostic analgesia in the entire crus. The distal portion is blocked when fibular and tibial nerve blocks are performed, and pain from injuries involving the distal aspect of the tibia and caudal soft tissues may be abolished, but this block is unreliable for abolition of crus-related pain. Lameness of the crus becomes more likely in horses in which perineural and intraarticular techniques for the rest of the limb have been exhausted. In at least three TB racehorses, pain associated with tibial stress fractures has been abolished or diminished by intraarticular analgesia of the femorotibial joint. An explanation is not readily apparent.
Imaging Considerations
Large cassettes or imaging plates (35 × 43 cm) should be used to obtain radiographs of the entire length of the tibia. There are normal areas of modeling involving the cranial proximal cortex of the tibia that appear as layers or a mound of bone, but stress fractures do not occur here. Occasionally, an obvious bony proliferation is seen involving the caudal or caudolateral tibial cortex, under the fibula in normal horses. Periosteal and endosteal proliferation of the caudal and lateral (medial is unusual) cortex and oblique linear radiolucency are changes that may be seen in horses with tibial stress fractures. Enostosis-like lesions appear as single or numerous medullary radiopacities. In some horses the fibula has one or more transverse radiolucent lines through the proximal third of the bone that should not be mistaken for fractures. Stress-related bone injury of the tibia is most easily imaged and diagnosed using scintigraphic examination. Without scintigraphy the diagnosis can be easily missed radiologically. Enostosis-like lesions may be associated with single to numerous areas of increased radiopharmaceutical uptake (IRU) in the medullary cavity and should be differentiated from the cortical uptake associated with tibial stress fractures. Numerous scintigraphic images are used to differentiate enostosis-like lesions, tibial stress fractures, and rare authentic lesions of the fibulae.
Ultrasonographic examination is useful in evaluating the gastrocnemius muscle and tendon. Patellar desmitis at the attachments can be diagnosed by using ultrasonographic and scintigraphic examinations. Ultrasonographic examination is useful in horses with fibularis tertius injury or thoroughpin or “false” thoroughpin and to evaluate the tarsal sheath.
Specific Conditions of the Crus
Tibial Stress Fractures
Tibial stress fractures are the most common lameness condition of the crus and occur most commonly in TB racehorses. In my experience, tibial stress fractures are rare in other sports horses, including the Standardbred (STB) racehorse. In an 8-year period, of 1020 STBs in which scintigraphic examination was performed, only three horses (two of which were trotters) had tibial stress fractures.3 Thirteen STB racehorses, 11 pacers, and two trotters with tibial stress fractures were reported in one study,4 but based on my experience this is a highly unusual clustering of horses. In that study pacers were overrepresented, and factors such as breeding, track size, training methods, and referral bias may have played a role. In my experience and practice area tibial stress fractures occur more commonly in trotters than in pacers. The caudal tibial cortex appears prone to stress-related bone injury because it is under compressive forces when loaded. The highest compressive forces were recorded in the middiaphysis at the walk, but loading at the gallop, pace, and trot was not determined.4-6
Tibial stress fractures usually occur in 2- and 3-year-old TB racehorses. In one study, tibial stress fractures occurred most commonly in 2-year-olds or unraced horses.7 In my experience tibial stress fractures occur later in training than stress fractures of the humerus, can occur when horses are racing, and also occur in older horses. Lameness in horses with humeral stress fractures often occurs within 4-8 weeks of returning to training in the early 3- or 4-year-old racing year. In horses with tibial stress fractures usually lameness is unilateral. Stress-related bone injury is more advanced in the lame limb, but scintigraphic evidence of stress-related bone injury can be bilateral. Typically TB racehorses with tibial stress fractures usually become acutely lame after training or racing, only to become reasonably sound within 3 to 5 days. Lameness recurs after another work session or race, but overt clinical signs other than lameness are subtle or lacking. Horses with pelvic stress fractures and those with stress-related bone injury of the distal aspect of the third metatarsal bone manifest similar clinical signs. Lameness may be severe initially, but within a few days horses can be trotted and show grade 2 to 4 lameness (of 5). Lameness may be worse in horses with caudal or caudomedial stress fractures than in those with caudolateral stress fractures. Horses with spiral tibial fractures involving the medial and lateral cortices and often the cranial cortex of the distal aspect of the tibia can be nearly non–weight bearing (see Figure 19-10).
Tibial stress fractures are seen as focal areas of IRU in the caudal or caudal lateral tibial cortex in the middiaphysis and are usually singular but can be multiple and bilateral (see Chapter 19). Tibial stress fractures must be differentiated from enostosis-like lesions, which can cause similar clinical signs but scintigraphically are located in the medullary cavity (see Figure 19-9). Caudomedial tibial stress fractures occur but are unusual. In horses in North America, tibial stress fractures are usually located from middiaphysis to the distal aspect of the tibia, but occasionally a fracture is seen in the proximal, caudal metaphyseal region. In TBs racing in Europe the proximal caudal site is affected more commonly than is seen in TBs from North America.8 Of 42 TB racehorses with tibial stress fractures examined in England, 52% had middiaphyseal fractures, 29% had distal tibial fractures, and 19% had proximal caudal fractures.9 In Australia fracture distribution mimics that seen in North America.7 Occasionally a spiral fracture of the distal tibial cortex is seen scintigraphically, but fractures are usually initially not detectable radiologically (see Figure 19-10). Horses with this configuration of fracture are at risk for catastrophic failure of the tibia, even while being stall rested. In general, intensity of IRU is inversely proportional to the amount of radiological change. In a U.K. study in Newmarket, no correlation was found between scintigraphic and radiological grades in TB racehorses.9 Curiously, there was no relationship between scintigraphic grade and degree of lameness, a finding that differs from my clinical experience.9 This may reflect the rapidity with which horses undergo scintigraphic examination in a first-opinion racehorse practice, compared with the delay before horses are referred to my second-opinion practice. In horses with stress-related bone injury a continuum of bone changes occurs; these bone changes precede and eventually lead to fracture. If radiographs show proliferative changes and an oblique fracture line, IRU is usually mild to moderate. In horses that develop sudden, severe lameness, focal or spiral intense IRU is seen, but radiological changes are equivocal or mild. Authentic tibial stress fractures do not occur in the cranial cortex (except distally in horses with spiral fractures), but IRU from a previous fibular nerve block can produce an artifact resembling fracture (see Figure 19-15).
Most horses are given 4 weeks of stall rest, followed by 4 weeks of stall rest with handwalking, then 8 weeks of turnout in a small paddock before returning to race training. In North America it is difficult to enforce a 16-week rest period, but earlier return to race training predisposes to recurrence of stress-related bone injury and fracture. Trainers are often content with a 45- to 60-day period of rest but balk at giving longer rest periods; however, fractures heal neither clinically nor scintigraphically in 60 days. Because stress fractures occur as a result of accumulated bone stress from race training, early return to training on the very surface on which the horse was training when the fracture occurred and in the same training regimen predisposes to reinjury. Fracture of the contralateral limb the next racing year is possible, but recurrence of ipsilateral fracture is unusual, unlike recurrence seen early in training in horses with humeral stress fractures. Horses with severe lameness may have difficulty rising in the stall and should be bedded on good footing or kept in the standing position for several weeks by the use of crossties or other suitable restraints. Clients should be warned that even while horses are resting, spiral tibial fractures can become comminuted.
Tibial Diaphyseal Fractures in Adult Horses
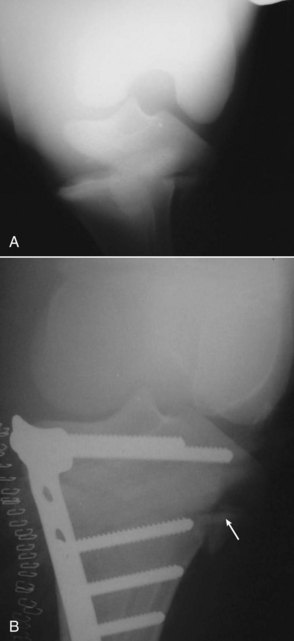
Tibial fractures in adult horses occur from trauma from falling, from spills (falls) sustained while performing, from being kicked, or during attempts to rise after general anesthesia. Horses with tibial stress fractures, usually those with severe initial lameness or spiral fracture, can develop comminuted fractures if turnout exercise is given too soon or if a horse struggles to rise in a stall. One of the only reported successful repairs of an adult horse with a displaced tibial fracture was performed after the horse had been anesthetized for radiographs of the pelvis and coxofemoral joint only to develop a displaced, closed tibial fracture as a result of displacement from a tibial stress fracture. The injury was repaired using two dynamic compression plates and bone screws.10 In general, however, prognosis is grave for adult horses with displaced, comminuted tibial fractures, because comminution is severe, additional fracture lines often propagate proximal and distal from the fracture site, fractures are often open, and implant failures are common (Figure 45-1). Prognosis for horses with comminuted fractures involving the distal aspect of the tibia and tarsocrural joint is hopeless. A horse with a closed, simple, or mildly comminuted midshaft oblique or transverse fracture may be a candidate for an attempt at internal fixation. With newly developed implants such as the locking compression plate, and with the use of sling assistance to protect the contralateral limb from the development of laminitis and to add stress protection of the repaired limb, it may be possible to successfully repair simple, mildly comminuted or oblique midshaft tibial fractures in adult horses. However, prognosis is poor to grave, because even with double-plating or triple-plating techniques, implant or bone failure is common and fixation usually fails during anesthetic recovery even with a pool recovery system. Given the extremely poor prognosis, transportation of a horse with a flail leg should be avoided. Most horses should be immediately destroyed.

Tibial Fractures in Foals
Suckling and weanling foals with displaced, comminuted tibial fractures have a reasonable prognosis for salvage, and some become performance horses and racehorses. The size of the foal is critical, and complications in those heavier than 225 to 325 kg may be similar to those in adult horses. Most foals with tibial fractures sustain kick trauma from mares or have other accidents.
Proximal Physeal Tibial Fractures
Salter-Harris type II fractures occur in sucklings, weanlings, and rarely in yearlings. These fractures result in acute-onset lameness and swelling of the proximal, medial aspect of the crus and stifle. Within 1 to 3 days, foals are often weight bearing and may be surprisingly comfortable. Radiographs reveal a simple Salter-Harris type II fracture with a lateral metaphyseal component (Figure 45-2). Occasionally, mild comminution exists laterally. Foals with minimal displacement can be managed conservatively, but progressive displacement, as evidenced by valgus deformity, usually occurs. Foals should be treated surgically. Many methods have been used, but the most stable repair is a medial approach in which either a T plate or two short dynamic compression plates are applied by using 5.5-mm cortex bone screws in the epiphyseal component. A long metaphyseal component can be engaged using screws placed in lag fashion. The tension side of the proximal aspect of the tibia is medial, and the T plate should be applied in this location. Because the soft tissue covering is minimal, chronic drainage from the wound is common until the plate(s) is removed. Prognosis for life is good to excellent and for soundness is fair to good. Prognosis for racing is not established, and sequelae from differences in limb length are unknown, but racing is not out of the question.
Middiaphyseal Tibial Fractures
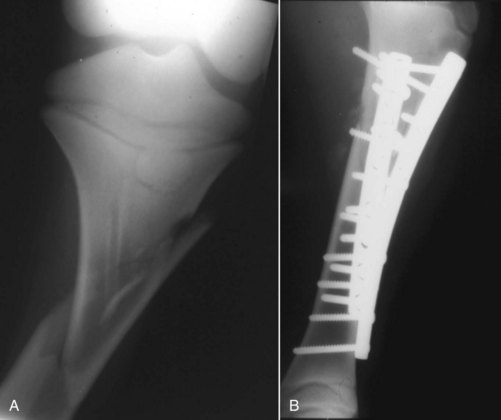
Similar considerations for degree of comminution, location of fracture, and whether the site is open or closed apply to foals and adult horses, but in foals prognosis associated with repair is considerably better than in adults. Foals with closed, midshaft, transverse, or oblique fractures with minimal comminution are the best surgical candidates, but successful repair of those with comminution has been achieved (Figure 45-3). Foals with open fractures that are associated with a small wound and minimal contamination are also surgical candidates. A cranial approach is used to place two dynamic or locking compression plates on the craniolateral and craniomedial aspects, and additional screws are used to repair loose fragments. In a retrospective study of nine foals whose injuries were repaired in this manner, results were considered excellent in six and good or fair in two.11 Additional stability can be achieved using locking compression plates, but success was reasonable with older style of implants. If fractures heal, implants should be removed, and if contralateral angular deformity does not develop, prognosis for racing should be fair to good.
Distal Physeal Fractures of the Tibia
Distal physeal fractures of the tibia do occur but are rare. Acute severe lameness, swelling, and angular and rotational deformity of the limb are present. Salter-Harris type II fractures are most common, but the small size of the epiphysis complicates surgical repair. Substantial tibial shortening can be expected, and prognosis is poor.
Tibial Malleolar Fractures
Medial malleolar fractures are rare but occasionally occur from trauma and may be associated with substantial collateral ligament injury. When collateral ligament injury is minimal, fragments can be removed arthroscopically, but visibility can be difficult without proper instrumentation. After fragments are removed, the arthroscope can usually be advanced to the plantar pouch. Prognosis is good in horses without substantial collateral ligament damage and tarsocrural instability. However, if there are additional loose fragments within the joint, this may indicate further damage of the tarsocrural joint.
See Chapter 44 for a discussion of lateral malleolar fractures.
Tibial Tuberosity Fractures
Direct trauma causes tibial tuberosity fractures, which occur most often in field hunters and jumpers. Fractures are usually nonarticular and can vary in length, width, and depth. In most horses with injuries that are managed conservatively, fractures heal functionally but without radiological evidence of union. In a retrospective study surgical repair of nonarticular fractures in six horses resulted in a successful outcome.12 Large fractures involving the femorotibial joint surfaces can be repaired, but surgical repair is not necessary in most horses and can be associated with catastrophic fracture of the tibia if occult fracture lines are not recognized and implant failure occurs13 (see Figure 46-12). In one study, 10 of 14 horses with nonarticular tibial tuberosity fractures that were managed conservatively were sound, and horses performed at the expected level14 (Figure 45-4). If fractures are repaired rather than simply having screws placed across the fracture line, a tension band technique such as a short plate and screws or a combination of screws and wire should be used.

Enostosis-like Lesions of the Tibia
Enostosis-like lesions of the tibia are diagnosed by scintigraphic and radiological examinations. These lesions can be a cause of chronic, mild hindlimb lameness, or in the TB (rarely STB) racehorse they occasionally cause acute pronounced lameness mimicking that seen with a tibial stress fracture.
Osteochondroma of the Tibia
Osteochondroma of the tibia is a rare radiological finding in the distal, caudal aspect of the tibia and may be incidental or may cause tarsal tenosynovitis. I have seen one adult horse with osteochondroma that as a foal had repair of a tibial fracture. The condition has rarely been reported.15
Osseous Cystlike Lesions of the Proximal Aspect of the Tibia
Osseous cystlike lesions of the proximal aspect of the tibia are unusual, may be the result of osteochondrosis, and frequently communicate with the lateral femorotibial joint (see Figure 23-3) (Figure 45-5). There may be concomitant osteochondrosis lesions involving the distal aspect of the lateral femoral condyle. Some adult horses develop radiolucent changes caused by osteoarthritis, but in these horses osseous cystlike lesions are acquired, not developmental. Some adult horses develop sudden-onset lameness associated with a well-established osseous cystlike lesion that was previously asymptomatic with no evidence of primary osteoarthritis. Clinical signs are similar to those in horses with other subchondral bone cysts or osseous cystlike lesions of the femorotibial joint, but lameness is often pronounced in adult horses with osteoarthritis. In most horses with osseous cystlike lesions involving the lateral femorotibial joint, curettage is difficult without elevating or severing the lateral meniscus. Some of these horses respond to conservative management and intraarticular injections of hyaluronan and corticosteroids. Intralesional injection with corticosteroids has also been reported. In horses with acquired osseous cystlike lesions related to osteoarthritis, the lesion is usually medial and prognosis is poor because cartilage damage of the proximal tibial condyle and distal medial femoral condyle is usually severe. One study described 12 horses with osseous cystlike lesions. In six the lesions were believed to be the result of osteochondrosis, and three of the six horses that received surgical debridement became athletes. Only two of six horses in which osseous cystlike lesions were caused by osteoarthritis returned to work after surgery.16 Often, location precludes complete surgical debridement because cysts most commonly occur in the midportion of the proximal aspect of the tibia under the lateral meniscus. Prognosis worsens when the cyst cannot be completely debrided, there is concomitant involvement of the distal aspect of the femur, there is deterioration or tearing of the lateral meniscus, or there is substantial osteoarthritis.
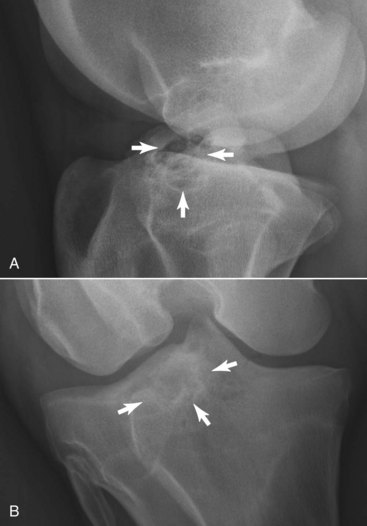
Fig. 45-5 Lateromedial (A) and caudocranial (B, lateral is to the left) digital radiographic images of a 3-year-old Standardbred gelding with a multiloculated osseous cystlike lesion and increased radiopacity of the proximal lateral tibial epiphysis (arrows). Intraarticular photographs are shown in Figure 23-3. This horse underwent arthroscopic surgical debridement using a cranial approach through the femoropatellar joint and septectomy.
Osseous Cystlike Lesions of the Distal Aspect of the Tibia
Osseous cystlike lesions of the distal aspect of the tibia are rare injuries and appear to be acquired as the result of trauma or stress-related bone injury. I have seen osseous cystlike lesions in this location in a jumper and a STB racehorse. In both horses, there was acute-onset lameness and tarsocrural effusion. However, such lesions can be present in the absence of effusion. Scintigraphic examination revealed focal, moderate-to-intense IRU of the distal aspect of the tibia. Horses were rested and later performed at a level similar to preinjury level. Computed tomography was useful in elucidating the lesion in other horses (see Chapter 20).
Fibular Fractures
Authentic fibular fractures occur rarely and are often fortuitously diagnosed scintigraphically or radiologically when images are obtained in horses with undiagnosed hindlimb lameness or in those with suspected tibial stress fractures. Fractures occur either proximally or in the middiaphyseal region and can appear as a chronic nonunion fracture with bulbous proliferation on each side of the fracture. There can be numerous apparent fibular fractures, and the condition can occur bilaterally. Proliferation likely existed before onset of clinical signs. Horses with midshaft fibular fractures have a large, nearly intact fibula that may predispose to fracture, but a causal relationship between this anatomical finding and fracture has not been established. Often, scintigraphic examination reveals focal IRU at the fracture site and sometimes diffuse IRU in the fibula peripheral to the fracture (Figure 45-6). The entire limb should be evaluated carefully to exclude another site of pain causing lameness. In a Warmblood jumper I observed a focal area of intense IRU of the midfibula that appeared radiologically like a large, chronic nonunion, but moderate hindlimb lameness abated after high plantar analgesia, and suspensory desmitis was the bona fide source of pain. Occasionally there is focal IRU involving both the most proximal aspect of the fibula and the immediately adjacent tibia that may reflect trauma to their articulation. Verification of this as a cause of pain and lameness is difficult. I have seen horses—three TB racehorses and one STB racehorse—with authentic fibular fractures that were discovered during scintigraphic examination. Horses were examined for poor racing or training performance or undiagnosed or high-speed hindlimb lameness and were sound with rest (see Figure 45-6).17 Four months’ rest is recommended, but in horses in which lameness persists, segmental fibular ostectomy remains a potential surgical approach. The entire limb should be evaluated carefully to exclude another site of pain causing lameness. Six horses with proximal fibular fractures made complete functional recoveries; horses were sound within 3 months, but a fracture line persisted radiologically until 4 to 6 months after the injury.8
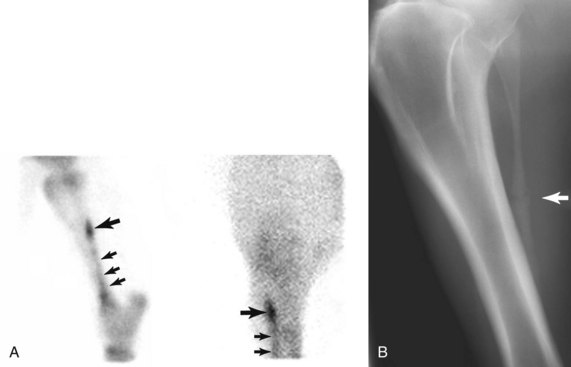
Fig. 45-6 A, Lateral (left) and caudal (lateral is to the left) delayed phase scintigraphic images of a 4-year-old Standardbred racehorse that underwent bone scintigraphy for undiagnosed left hindlimb lameness. Focal, intense increased radiopharmaceutical uptake (IRU) of the left fibula (large arrows) is diagnostic of fracture. In the lateral image, focal IRU could easily be confused with a tibial stress fracture, but in the caudal image IRU is clearly in the fistula. There is diffuse mild-to-moderate IRU in the fibula distal to the fracture site (small arrows), indicating that abnormal bone modeling exists peripheral to the fracture site. B, Craniolateral-caudomedial oblique plain radiographic image showing a midshaft fibular fracture (arrow) and bony enlargement of the fibula proximal and distal to the fracture site. A large, nearly intact fibula is present.
Nonossifying Fibromas of the Proximal Tibia
A yearling TB filly with rare, nonossifying fibromas of both tibias was examined because of kyphosis of the lumbar spine and a stilted hindlimb gait.18 Radiographs revealing radiolucent defects and sclerosis of the proximal tibial epiphyses and scintigraphic images published in the case report18 look similar to those of horses I have seen with multiloculated proximal tibial osseous cystlike lesions thought to be a form of osteochondrosis (see Figure 45-5).
Tumors
Hemangiosarcoma occurs rarely in the proximal aspect of the crus. Firm, slow-growing, subcutaneous, soft tissue masses without bone involvement are composed of multiloculated areas of hemorrhage and can be excised without recurrence. It was reported that a fibrosarcoma of the distal, caudomedial aspect of the crus just above the tarsus was resected and recurrence was not seen at  years after surgery.19
years after surgery.19
Soft Tissue Injuries of the Crus
Fibularis tertius injury in foals and adult horses is discussed in Chapter 80, and gastrocnemius tendonitis is discussed in Chapter 80. Stringhalt is discussed in Chapter 48.