Skeletal System
1 Define and pronounce the key terms and anatomic terms in this chapter.
2 Locate and identify the bones of the head and neck and their landmarks on a diagram, skull, and patient.
3 Describe in detail the landmarks of the maxilla and mandible.
4 Discuss the skeletal system pathology associated with the head and neck.
5 Correctly complete the review questions and activities for this chapter.
6 Integrate an understanding of the skeletal system into the overall study of the head and neck anatomy and clinical dental practice.
Skeletal System Overview
The skeletal system consists of the bones, associated cartilage, and joints. The bones of the skeletal system are mineralized structures in the body. Bones protect the internal soft tissue (see Chapters 6, 8, and 10). Bones also serve as the biomechanic basis for movement of the body along with muscles, tendons, and ligaments (see Chapter 4). Bones are also a consideration in the spread of dental infection (see Chapter 12).
The prominences and depressions on the bony surface are landmarks for the attachments of associated muscles, tendons, and ligaments. The openings in the bone are also landmarks where various nerves and blood vessels enter or exit. An area of the bone that is neither a prominence nor depression, such as a plate, which is a flat, bony structure, can also be demarcated.
Bony Prominences
A general term for any prominence on a bony surface is a process. One specific type of prominence located on the bony surface is a condyle, an oval prominence usually involved in joints. An epicondyle is a small prominence that is located superior to or upon a condyle. A rounded surface projecting from a bone by a neck is a head. Another large, often rough prominence is a tuberosity. Tuberosities are usually attachment areas for muscles or tendons. An arch is shaped like a bridge with a bowlike outline. A cornu is a hornlike prominence.
Other prominences of the bone include the tubercles, crests, lines, and spines. These primarily serve as muscle and ligament attachments. A tubercle or eminence is a rounded elevation on a bony surface. A crest is a prominent, often roughened border or ridge. A line is a straight, small ridge. An abrupt prominence of the bone that may be a blunt or sharply pointed projection is a spine.
Bony Depressions
One type of depression on a bony surface is an incisura or notch, an indentation at the edge of the bone. Another depression(s) on a bony surface is a sulcus (plural, sulci), which is a shallow depression or groove that usually marks the course of arteries and nerves. A generally deeper depression(s) on a bony surface is a fossa (plural, fossae). Fossae can be parts of joints, attachment areas for muscles, or have other functions.
Bony Openings
The bone can have openings such as a foramen or canal. A foramen (plural, foramina) is a short windowlike opening(s) in the bone. A canal is a longer, narrow tubelike opening in the bone. A meatus is a type of canal. Another opening in a bone is a fissure, which is a narrow cleftlike opening. A small opening(s), especially as an entrance into a hollow organ or canal, is an ostium (plural, ostia). Another opening or orifice is an aperture.
Skeletal Articulations and Sutures
An articulation is an area of the skeleton where the bones are joined to each other. An articulation can be either a movable or immovable joint. A joint is a site of a junction or union between two or more bones. A suture is the union of bones joined by fibrous tissue and appears on the dry skull as jagged lines. Sutures are considered to be generally immovable but may provide biomechanic protection from the force of a blow by moving slightly to absorb the force. They are the most flexible in infants; much of the early growth of the skull occurs at the sutural edges of the cranial bones.
Bones Of Head And Neck
The bones of the head and neck serve as a base for palpation of the soft tissue in the area during both an intraoral and extraoral examination (see Appendix B). The bones also serve as markers when identifying the location of soft tissue pathology. A dental professional also examines these bones externally during a head and neck examination because a disease process may affect them. A dental professional must not only locate each of the head and neck bones but also recognize any abnormalities in the bony surface structure (discussed later).
In order to recognize any bony abnormalities, the dental professional must understand the normal anatomy of the bones of the head and neck. This includes locating the surface bony prominences, depressions, and articulations as well as the openings in these bones and the blood vessels and nerves that travel through those openings. For effective study of the bones of the head and neck, it is helpful to use photographs and illustrations of these bones as well as the skull model and palpation of peers and then later, patients, during both extraoral and intraoral examination.
Bones and their associated surface tissue also serve as landmarks when taking dental radiographs (see Chapter 2), before administering a local anesthetic injection (see Chapter 9), and in understanding the spread of dental infections (see Chapter 12).
Skull Bones
The bones of the skull or braincase can be divided into the cranium (kray-nee-um), which contains the brain with its cranial bones (kray-nee-al) and the face with its facial bones. The bones of the skull, whether facial or cranial, can be single or paired. These bones form the facial features, are involved in the temporomandibular joints, and participate with growth in the formation of dentition. Many anatomists use neurocranium for the cranial bones because they enclose the brain and viscerocranium for the facial bones. The skull has 22 bones, not including the six auditory ossicles of the middle ear (Table 3-1). Each ear contains one malleus, incus, and stapes. Their function is to transmit and amplify vibrations to inner ear and the tympanic membrane or eardrum.
TABLE 3-1
Cranial and Facial Bones*
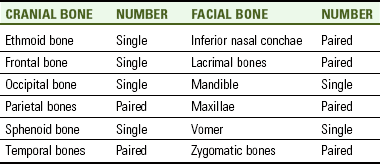
*Note that the palatine bones are paired bones of the skull that are not strictly considered facial bones.
Growth takes place in all bones of the skull during early youth. Growth of the upper face occurs at the sutures between the maxillae and other bones as well as at bony surfaces. Growth in the lower face takes place at the bony surfaces of the mandible and at the head of its condyle. Inadequate or disproportionate growth of the upper face and mandible may leave inadequate room for the developing dentition and cause other occlusal problems. This failure of growth can be addressed by orthodontic therapy as well as an endocrine workup and osseous surgery, if needed.
All skull bones are immovable, except the mandible with its temporomandibular joint. Instead, the articulation of many of the bones in the skull is by sutures (Table 3-2). In addition, the skull also has a movable articulation with the bony vertebral column in the neck area.
TABLE 3-2
Skull Sutures and Articulations
| SUTURE(S) | BONY ARTICULATIONS |
| Coronal sutures | Frontal bone and parietal bones |
| Frontonasal suture | Frontal bone and nasal bones |
| Intermaxillary suture | Maxillae |
| Lambdoidal suture | Occipital bone and parietal bones |
| Median palatine suture | Anterior part: Maxillae Posterior part: Palatine bones |
| Sagittal suture | Parietal bones |
| Squamosal sutures | Temporal bones and parietal bones |
| Temporozygomatic sutures | Zygomatic bones and temporal bones |
| Transverse palatine suture | Maxillae and palatine bones |
Many skull bones have openings for important nerves and blood vessels of the head and neck (Table 3-3). Skull bones also have many associated processes that are involved in important structures of the face and head (Table 3-4). For more effective study, this chapter may also be reviewed after reading the chapters on the vascular and nervous systems (see Chapters 6 and 8), the chapters on the muscles of the head and neck (see Chapter 4), as well as the chapter on the temporomandibular joint (see Chapter 5).
TABLE 3-3
Skull Bony Openings and Contents
| BONY OPENING(S) | LOCATION | CONTENTS FOR EACH OPENING |
| Carotid canals | Temporal bones | Internal carotid artery and nerve plexus |
| Cribriform plate with foramina | Ethmoid bone | Olfactory nerves |
| External acoustic meatus | Temporal bones | Opening to tympanic cavity |
| Foramina lacerum | Sphenoid, occipital, and temporal bones | Cartilage |
| Foramen magnum | Occipital bone | Spinal cord, vertebral arteries, and eleventh cranial nerve |
| Foramina ovale | Sphenoid bone | Mandibular nerve (or division) of fifth cranial or trigeminal nerve; lesser petrosal nerve |
| Foramina rotundum | Sphenoid bone | Maxillary nerve (or division) of fifth cranial or trigeminal nerve |
| Foramina spinosum | Sphenoid bone | Middle meningeal artery |
| Greater palatine foramina | Palatine bones | Greater palatine nerve and vessels |
| Hypoglossal canals | Occipital bone | Twelfth cranial or hypoglossal nerve and vessels |
| Incisive foramen | Maxillae | Right and left nasopalatine nerves and branches of the sphenopalatine artery |
| Inferior orbital fissures | Sphenoid bone and maxillae | Infraorbital and zygomatic nerves, infraorbital artery, and ophthalmic vein |
| Infraorbital foramina and canals | Maxillae | Infraorbital nerve and vessels |
| Internal acoustic meatus | Temporal bones | Seventh and eighth cranial nerves |
| Jugular foramina | Occipital and temporal bones | Internal jugular vein and ninth, tenth, and eleventh cranial nerves |
| Lesser palatine foramina | Palatine bones | Lesser palatine nerve and vessels |
| Mandibular foramina | Mandible | Inferior alveolar nerve and vessels |
| Mental foramina | Mandible | Mental nerve and vessels |
| Optic canals and foramina | Sphenoid bone | Optic nerve and ophthalmic artery |
| Petrotympanic fissures | Temporal bones | Chorda tympani nerve |
| Pterygoid canals | Sphenoid bone | Pterygoid nerve and vessels |
| Sphenopalatine foramen | Palatal bone and sphenoid bone | Pterygopalatine ganglion and sphenopalatine artery |
| Stylomastoid foramina | Temporal bones | Seventh cranial or facial nerve |
| Superior orbital fissures | Sphenoid bone | Third, fourth, and sixth cranial nerves and ophthalmic nerve (or division) of fifth cranial or trigeminal nerve and vein |
| Zygomaticofacial foramina | Zygomatic bones | Zygomaticofacial nerve and vessels |
| Zygomaticotemporal foramina | Zygomatic bones | Zygomaticotemporal nerve and vessels |
TABLE 3-4
| PROCESS OF SKULL | SKULL BONE | ASSOCIATED STRUCTURES |
| Alveolar process | Mandible | Contains roots of mandibular teeth |
| Alveolar process | Maxilla | Contains roots of maxillary teeth |
| Condyloid process | Mandible | Mandibular condyle and neck |
| Coronoid process | Mandible | Part of ramus |
| Frontal process | Maxilla | Forms medial infraorbital rim |
| Frontal process | Zygomatic bone | Forms anterior lateral orbital wall |
| Lesser wing | Sphenoid bone | Anterior process to sphenoid bone body |
| Greater wing | Sphenoid bone | Posterolateral process to sphenoid bone body |
| Mastoid process | Temporal bone | Composed of mastoid air cells |
| Maxillary process | Zygomatic bone | Forms infraorbital rim and part of anterior lateral orbital wall |
| Palatine processes | Maxillae | Forms anterior hard palate |
| Postglenoid process | Temporal bone | Posterior to temporomandibular joint |
| Pterygoid process | Sphenoid bone | Consists of medial and lateral pterygoid plates |
| Styloid process | Temporal bone | Serves as attachment for muscles and ligaments |
| Temporal process | Zygomatic bone | Part of zygomatic arch |
| Zygomatic process | Frontal bone | Lateral to orbit |
| Zygomatic process | Maxilla | Forms lateral part of infraorbital rim |
| Zygomatic process | Temporal bone | Part of zygomatic arch |
This chapter studies the skull by first looking at its various external views: superior, anterior, lateral, and inferior, and then secondly, by looking at its internal surface from both a superior and inferior view. This format of first visualizing the entire skull helps to obtain more general information about structures formed by several skull bones. Next the skull is studied by looking at its individual bones and their various features and landmarks, using the major categories of the cranial bones, facial bones, and neck bones. Finally, the more general features of the skull such as the fossae and paranasal sinuses are studied.
Superior View Of External Skull
To easily look at the superior view of the external skull, the cap can be removed from the entire model skull, if necessary, and studied. Certain bones and sutures are easily noted from this view.
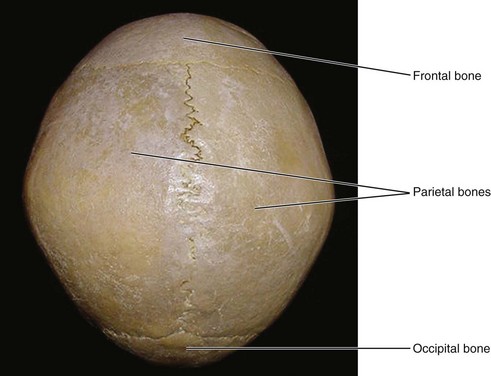
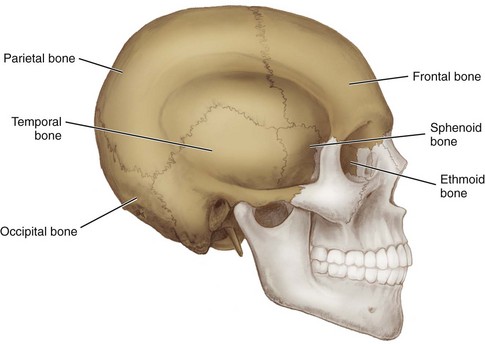
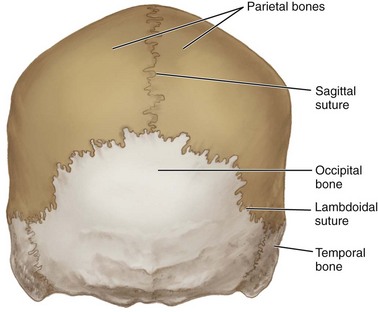
Cranial Bones from Superior View.: When the external skull is viewed from the superior aspect, four cranial bones are visible (Figure 3-1). At the front of the skull is the single frontal bone (frunt-il). At each side of the skull is the paired parietal bone (pah-ri-it-al). At the back of the skull is the single occipital bone (ok-sip-it-al). This main division of the cranial bones of the skull is discussed later.
Skull Sutures from Superior View.: Sutures among these four cranial bones are also visible from the superior aspect are the coronal, sagittal, and lambdoidal (Figure 3-2; see Table 3-2). The suture extending across the skull, between the frontal bone and parietal bone, is the paired coronal suture (kor-oh-nahl). This is the location of the diamond-shaped anterior fontanelle or “soft spot” in a newborn where the two frontal and two parietal bones join, which generally remains open until two years of age.
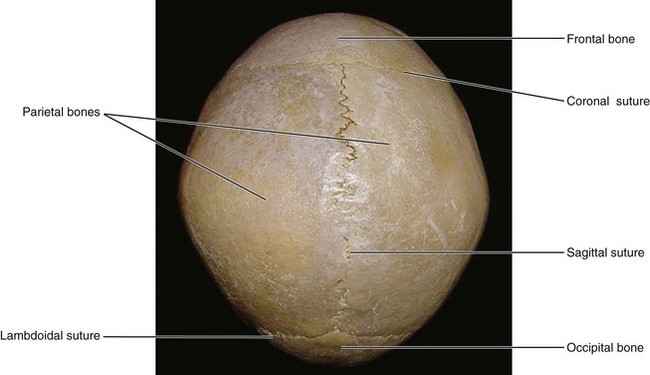
A single suture, the sagittal suture (saj-i-tel), extends from the front to the back of the skull at the midline between the parietal bones; the sagittal suture is parallel with the sagittal plane of the skull. The coronal sutures and sagittal suture generally form a right angle with each other. Another single suture located between the occipital bone and the parietal bone, is the lambdoidal suture (lam-doid-al), which is by far more serrated-looking than the others, resembling an upside down V.
Anterior View Of External Skull
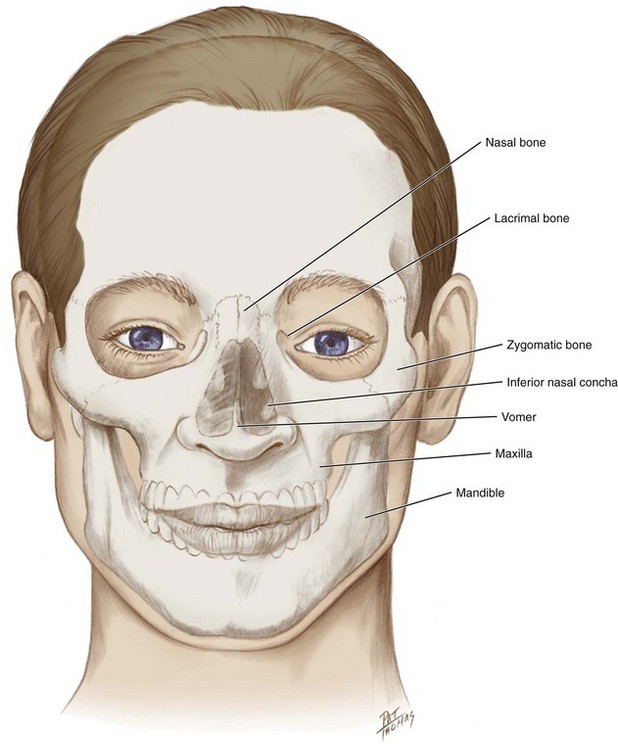
When the external skull is viewed from the anterior aspect, certain bones of the skull (or parts of these bones) are visible (Figure 3-3). These bones include: single frontal, ethmoid, vomer, sphenoid, mandible and also paired lacrimal, nasal, inferior nasal conchal, zygomatic, and maxillae. The facial bones as a group, orbit, and nasal cavity are easily noted from this view.
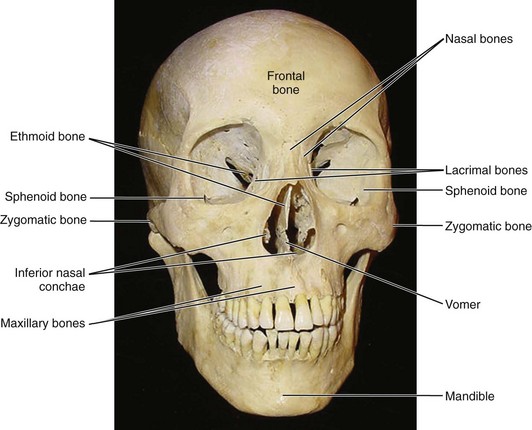
Facial Bones from Anterior View.: The facial bones on the anterior aspect of the skull include: lacrimal bone (lak-ri-mal), nasal bone (nay-zil), vomer (vo-mer), inferior nasal concha (kong-kah, plural, conchae [kong-kee]), zygomatic bone (zy-go-mat-ik), maxilla (mak-sil-ah), and mandible (man-di-bl) (Figure 3-4). The palatine bone (pal-ah-tine) is not visible on this view and is not strictly considered a facial bone by anatomists, but for ease of learning, it is included under the heading of facial bones. This main division of the facial bones of the skull is discussed later.
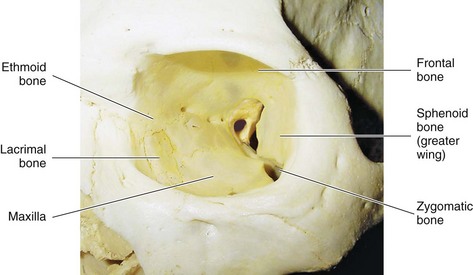
Orbit and Associated Structures from Anterior View.: The orbit (or-bit), which contains and protects the eyeball, is a prominent feature of the anterior part of the skull (Figure 3-5 and see Figure 2-6). Many skull bones form both the walls and apex of each of the orbits (Table 3-5). The larger orbital walls (or-bit-al) are composed of the orbital plates of the frontal bone (making the roof or superior wall), the ethmoid bone (forming the greatest part of the medial wall), the lacrimal bone (at the anterior medial corner of the orbit and orbital surfaces of the maxilla [the floor or inferior wall]), and the zygomatic bone (the anterior part of the lateral wall). The orbital surface of the greater wing of the sphenoid bone is also included (the posterior part of the lateral wall).
TABLE 3-5
| PART OF ORBIT | SKULL BONES |
| Roof or superior wall | Frontal bone |
| Medial wall | Ethmoid and lacrimal bones |
| Lateral wall | Zygomatic and sphenoid bones |
| Apex or base | Sphenoid and palatine bones* |
*Note that the maxilla, a facial bone, completes the base (front) of the orbit.
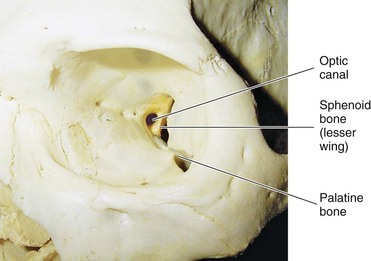
The orbital apex is the deepest part of the orbit and is composed of the lesser wing of the sphenoid bone (forming the base) and the palatine bone (a small inferior part) (Figure 3-6; see Table 3-5). The round opening in the orbital apex is the optic canal (op-tik), which lies between the two roots of the lesser wing of the sphenoid bone (see Table 3-3). The second cranial or optic nerve passes through the optic canal to reach the eyeball. The ophthalmic artery also extends through the canal to reach the eye.
Two orbital fissures are noted on the anterior aspect: the superior and inferior orbital fissures (Figure 3-7; see Table 3-3). Lateral to the optic canal is the curved and slitlike superior orbital fissure, between the greater and lesser wings of the sphenoid bone. Similar to the optic canal, the superior orbital fissure connects the orbit with the cranial cavity. The third cranial or oculomotor nerve, the fourth cranial or trochlear nerve, the sixth cranial or abducens nerve, and the ophthalmic nerve (or division from the fifth cranial or trigeminal nerve) and vein travel through this fissure (see Figures 8-8 and 8-9 ).
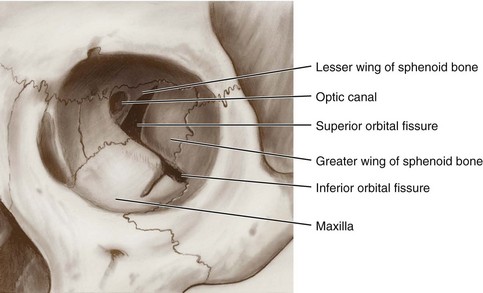
The inferior orbital fissure can also be seen between the greater wing of the sphenoid bone and the maxilla. The inferior orbital fissure connects the orbit with the infratemporal and pterygopalatine fossae (discussed later). The infraorbital and zygomatic nerves, branches of the maxillary nerve, and infraorbital artery enter the orbit through this fissure. The inferior ophthalmic vein travels through this fissure to join the pterygoid plexus of veins (see Figure 6-12).
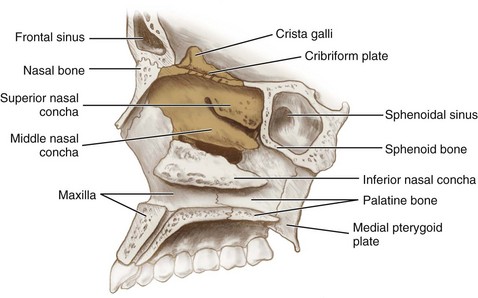
Nasal Cavity and Associated Structures from Anterior View.: The nasal cavity (nay-zil) or nasal fossa can also be viewed on the skull from the anterior (Figure 3-8; see Figure 3-56 and Figure 2-7). The nasal cavity is the upper part of the respiratory tract and is located between the orbits. It has lateral walls and a floor, with anterior and posterior openings, and is mainly composed of both bone and cartilage.
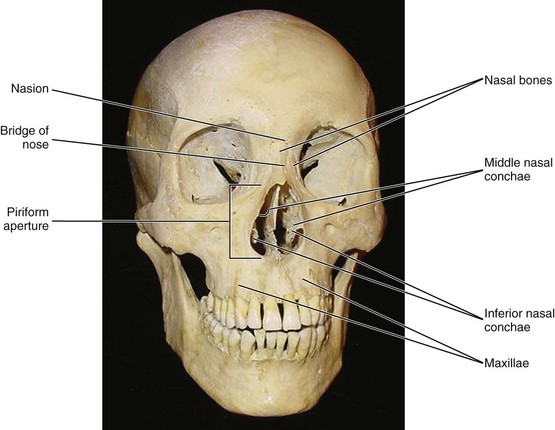
The bridge of the nose is formed from the paired nasal bones (see Figure 3-40). The nasion, a midpoint landmark, is located at the junction of the frontal and nasal bones. The anterior opening of the nasal cavity, the piriform aperture (pir-i-form), is large and triangular. The anterior openings to the nasal cavities are the nares, and the posterior openings are choanae (or posterior nasal apertures).
The floor of the nasal cavity is formed from the bones of the hard palate: palatine processes of the maxillae anteriorly and the horizontal plates of the palatine bones posteriorly (see Figure 3-16). The lateral boundaries of the nasal cavity are also formed by the maxillae. Each lateral wall of the nasal cavity has three projecting structures that extend inward from the maxilla, which are the nasal conchae or turbinates. These are the superior, middle, and inferior nasal conchae. Each extends like a scroll into the nasal cavity. The superior nasal concha and middle nasal concha are formed from the ethmoid bone; the inferior nasal concha is a separate facial bone. Protected by each nasal concha is a channel, the nasal meatus (me-ate-us). Each meatus has openings through which the paranasal sinuses or nasolacrimal duct communicates with the nasal cavity.
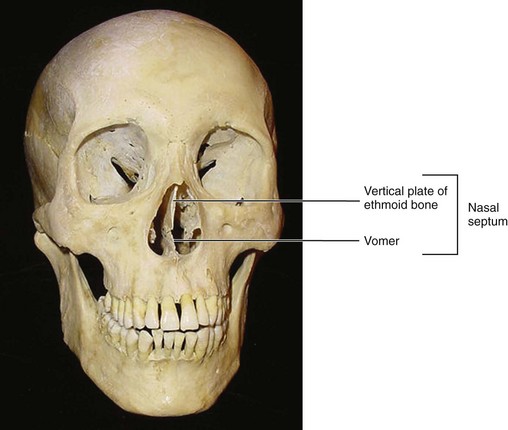
The vertical partition or fin, the nasal septum, divides the nasal cavity into two parts (Figure 3-9 and see Figure 2-17). Although it is frequently deflected slightly to the left or right, in general the septum is aligned perpendicularly. Anteriorly, the nasal septum is formed by both the perpendicular plate of the ethmoid bone superiorly and the nasal septal cartilage inferiorly. The posterior parts of the nasal septum are formed by the vomer.
Lateral View Of External Skull
When viewed from the lateral, the external skull shows both cranial bones and facial bones. A division between the cranial bones and facial bones can be reinforced by making an imaginary diagonal line that passes downward and backward from the supraorbital ridge of the frontal bone to the tip of the mastoid process of the temporal bone (Figure 3-10). These two main divisions of the bones of the skull are discussed in more detail later.
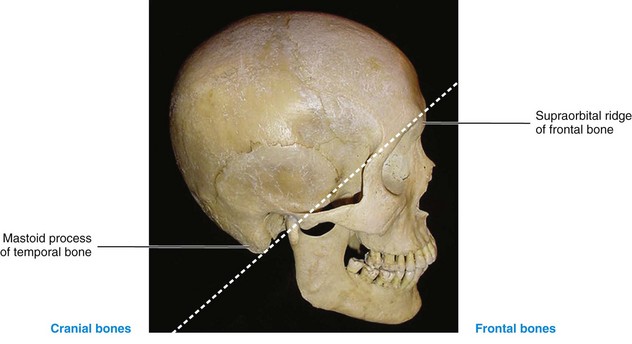
FIGURE 3-10 Lateral view of the external skull with an imaginary diagonal line (dashed) separating the cranial bones and facial bones.
Cranial Bones from Lateral View.: The cranium is easily noted on the lateral aspect, including the following cranial bones: the occipital, frontal, parietal, temporal, sphenoid bone (sfe-noid), and ethmoid bone (eth-moid) (Figure 3-11). This main division of the bones of the skull is discussed later.
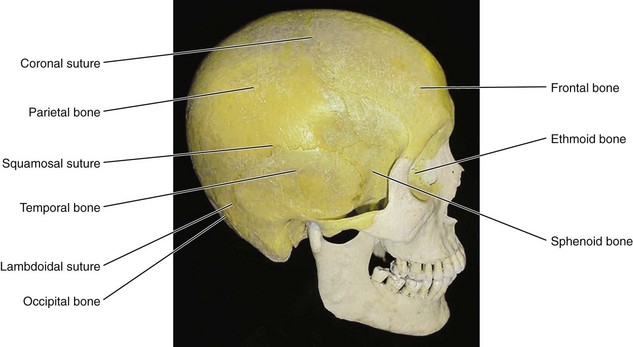
Skull Sutures from Lateral View.: Also noted on the lateral surface of the skull are the associated sutures of the cranial bones (see Figure 3-11 and Table 3-2). These sutures include the coronal suture, an articulation between the frontal bone and each parietal bone, and the lambdoidal suture, an articulation between the occipital bone and each parietal bone. Also present is the arched squamosal suture (skway-mus-al), between each temporal bone and parietal bone.
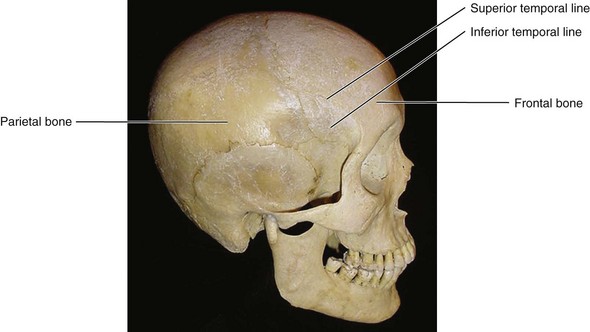
Skull Lines from Lateral View.: On the lateral surface of the skull are two separate parallel ridges or temporal lines (tem-poh-ral), crossing both the frontal and parietal bones (Figure 3-12). The superior ridge is the superior temporal line. The inferior ridge or inferior temporal line is the superior boundary of the temporal fossa where the fan-shaped temporalis muscle attaches (see Figure 4-22).
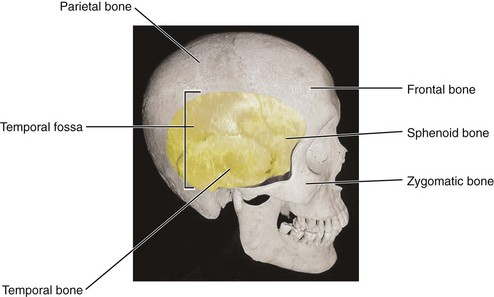
Skull Fossae from Lateral View.: The temporal fossa is easily seen on the lateral surface of the skull (Figure 3-13). The temporal fossa is formed by several bones of the skull and contains the body of the temporalis muscle. Inferior to the temporal fossa is the infratemporal fossa (in-frah-tem-poh-ral). Deep to the infratemporal fossa and more difficult to see is the pterygopalatine fossa (ter-i-go-pal-ah-tine). The temporal, infratemporal, and pterygopalatine fossae are discussed later and contain many important head and neck structures.
Zygomatic Arch and Temporomandibular Joint from Lateral View.: Farther inferior on the lateral aspect of the skull are many important bony landmarks (Figure 3-14). The zygomatic arch or cheekbone is visible, formed by the union of the broad temporal process of the zygomatic bone and the slender zygomatic process of the temporal bone (see Table 3-4 and see Figure 2-9). The suture between these two bones is the temporozygomatic suture (tem-por-oh-zi-go-mat-ik) (see Table 3-2). The zygomatic arch serves as the origin for the masseter muscle (see Figure 4-21).
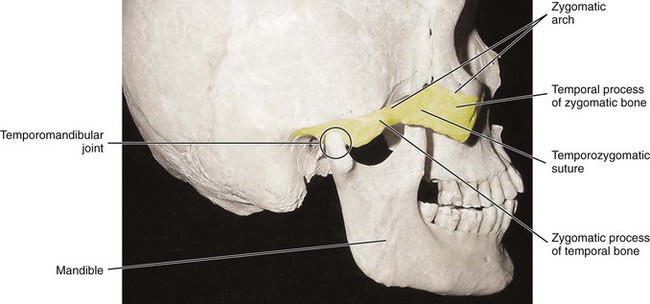
FIGURE 3-14 Lateral view of the external skull with the zygomatic arch highlighted and the temporomandibular joint noted (circle).
The temporomandibular joint (TMJ) is also noted, which is a movable articulation between the temporal bone and the mandible (see Chapter 5). More specific landmarks of these bones are discussed later.
Inferior View Of External Skull
Most of the structures of the inferior view of the external skull are more easily viewed on the skull model if the mandible is temporarily removed. The maxillary, zygomatic, vomer, temporal, sphenoid, occipital, and palatine bones are visible on this inferior view of the skull’s external surface (Figure 3-15).
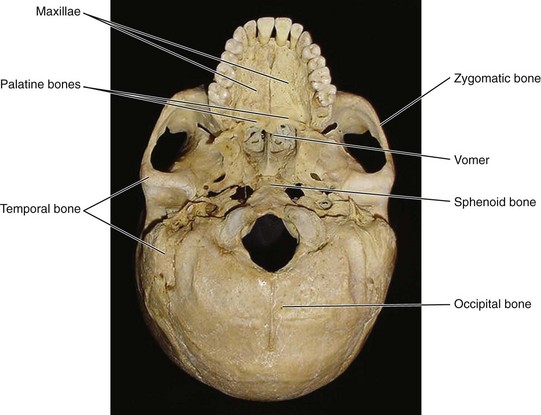
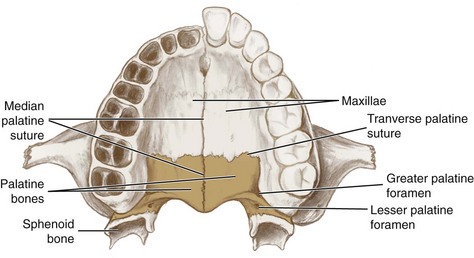
Hard Palate from Inferior View.: At the anterior part of the skull’s inferior surface is the hard palate, bordered by the alveolar process of the maxilla (al-vee-o-lar) with its maxillary teeth (Figure 3-16; see Figure 2-15 and Table 3-4). The hard palate is formed by the two palatine processes of the maxillae anteriorly and the two horizontal plates of the palatine bones posteriorly, an articulation which is noted by the prominent median palatine suture, which is noted clinically as the median palatine raphe (see Figure 2-15 and Table 3-2). The other suture is the transverse palatine suture, an articulation between the two palatine processes of the maxillae and the two horizontal plates of the palatine bones.
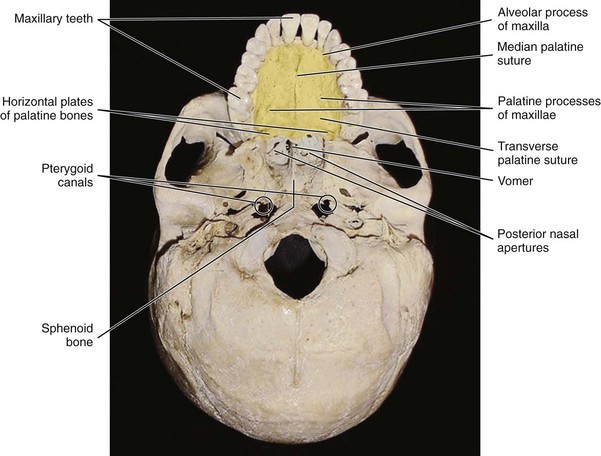
The hard palate forms the floor of the nasal cavity as well as the roof of the mouth. The posterior edge of the hard palate forms the inferior border of two funnel-shaped cavities, the posterior nasal apertures or choanae (ko-a-nay). The superior border of each aperture is formed by the vomer and the sphenoid bone. The posterior edge of the vomer forms the medial border of the posterior nasal apertures. The posterior nasal apertures are the posterior openings of the nasal cavity.
Near the superior border of each posterior nasal aperture is a small canal, the pterygoid canal (ter-i-goid) (see Table 3-3). The pterygoid canal extends to open into the pterygopalatine fossa and carries the pterygoid nerve and blood vessels (further discussion later).
Middle Part of Skull from Inferior View.: The middle part of the skull from the inferior view has many important surface prominences and depressions (Figure 3-17). The lateral borders of the posterior nasal apertures are formed on each side by the pterygoid process of the sphenoid bone (see Table 3-4).
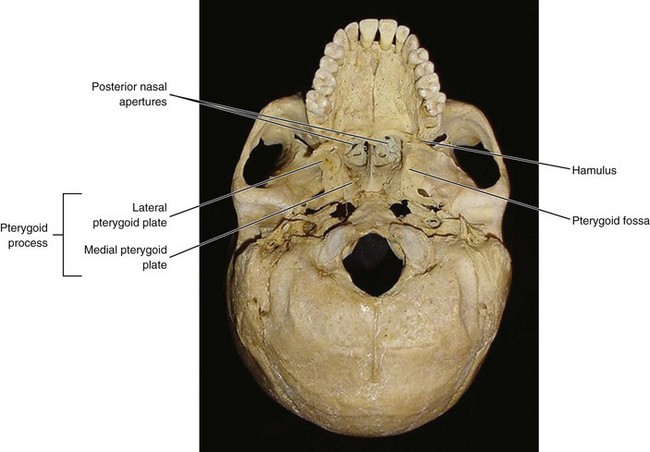
Each pterygoid process consists of a thin medial pterygoid plate and a flattened lateral pterygoid plate. The depression between the medial and lateral plates is the pterygoid fossa. At the inferior part of the medial plate of the pterygoid process is a thin curved process, the hamulus (ham-u-lis). The sphenoid bone and its landmarks are discussed later.
External Skull Foramina from Inferior View.: The inferior surface of the external skull has a large number of foramina (Figure 3-18; see Table 3-3). These openings provide entrances and exits for the arteries and veins that supply the brain and facial tissue (see Chapter 6). They also allow the cranial nerves to pass to and from the brain (see Figure 8-5).
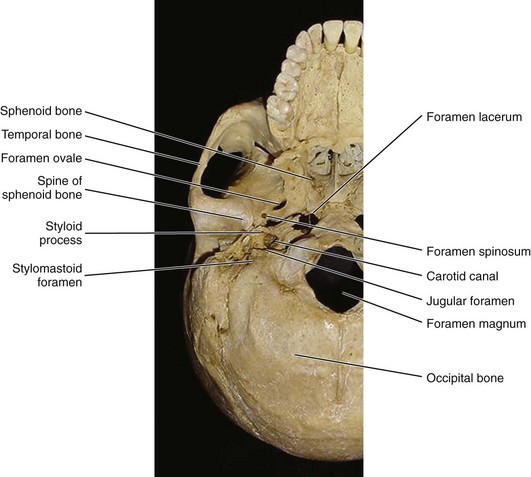
The larger anterior oval opening on the sphenoid bone is the foramen ovale (o-va-lee) for the mandibular nerve (or division) of the fifth cranial or trigeminal nerve (see Figure 8-7). The adjacent smaller and more posterior opening is the foramen spinosum (spine-o-sum), which carries the middle meningeal artery into the cranial cavity. The foramen spinosum receives its name from the nearby (angular) spine of the sphenoid bone, which is at the posterior extremity of the sphenoid bone.
Also on the external surface of the skull is the large, irregularly shaped foramen lacerum (lah-ser-um), which in life is filled with cartilage. Posterolateral to the foramen lacerum is a round opening in the petrous part of the temporal bone, the carotid canal (kah-rot-id). The carotid canal carries the internal carotid artery and sympathetic carotid plexus. A pointed bony projection, the styloid process (sty-loid), is visible lateral and posterior to the carotid canal (see Table 3-4). Immediately posterior to the styloid process is the stylomastoid foramen (sty-lo-mas-toid), an opening through which the seventh cranial or facial nerve exits from the skull to the face.
The jugular foramen (jug-you-lar), just medial to the styloid process, is more easily seen if the skull model is tilted to one side. The jugular foramen is the opening through which pass the internal jugular vein and three cranial nerves: the ninth cranial or glossopharyngeal nerve, the tenth cranial or vagus nerve, and the eleventh cranial or accessory nerve.
The largest opening on the inferior view is the foramen magnum (mag-num) of the occipital bone, through which the spinal cord, vertebral arteries, and eleventh cranial or accessory nerve pass.
Superior View Of Internal Skull
To have a superior view of the internal skull, remove the cap again of the skull model. The frontal, ethmoid, sphenoid, temporal, occipital, and parietal bones are visible from this view of the internal surface of the skull (Figure 3-19).
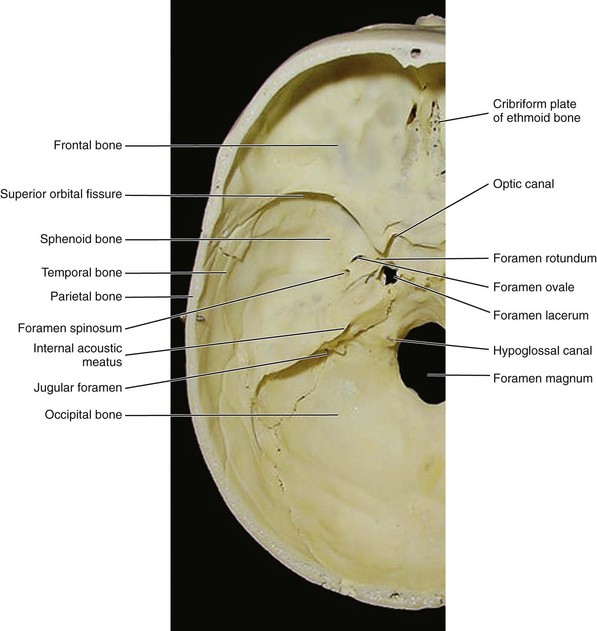
FIGURE 3-19 Superior view of the internal surface of the skull with its foramina and associated structures noted.
Internal Skull Foramina from Superior View.: Also present on the superior surface of the internal skull are the inside openings of the optic canal, superior orbital fissure, foramen ovale, foramen spinosum, foramen lacerum, jugular foramen, and foramen magnum, as discussed before when viewing the external skull surface (see Figure 3-19; see Table 3-3). Additionally, many other foramina are present on the internal surface of the skull. The perforated cribriform plate (krib-ri-form), with foramina for the first cranial or olfactory nerve, and the foramen rotundum (row-tun-dum) for the maxillary nerve (or division) of the fifth cranial or trigeminal nerve are also seen from this view (see Figure 8-7).
Finally, also present are the hypoglossal canal (hi-poh-gloss-al) for the twelfth cranial or hypoglossal nerve and the internal acoustic meatus (ah-koos-tik) for the seventh cranial or facial nerve and the eighth cranial or vestibulocochlear nerve.
Cranial Bones
The cranium is formed from the eight cranial bones. The cranial bones include the single occipital, frontal, sphenoid, and ethmoid as well as the paired parietal and temporal (Figure 3-20).
Occipital Bone
The occipital bone is a single cranial bone that forms the posterior part of the skull and the base of the cranium (Figure 3-21). It is an irregular, four-sided bone that is somewhat curved upon itself. The occipital bone articulates with the parietal, temporal, and sphenoid of the skull. The occipital bone also articulates with the first cervical vertebra or atlas (see Figure 3-62). The occipital bone can also be studied from an inferior view of its external surface.
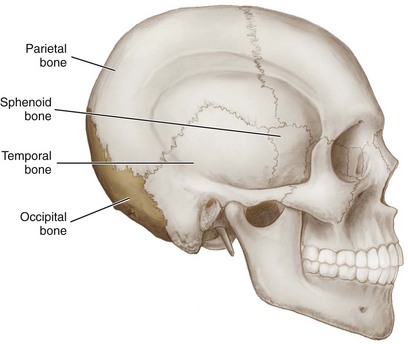
FIGURE 3-21 Lateral view of the external skull with the occipital bone highlighted and its bony articulations noted.
Occipital Bone from Inferior View.: On the external surface of the occipital bone from an inferior view, it can be seen that the foramen magnum is completely formed by this bone (Figure 3-22; see Table 3-3). Lateral and anterior to the foramen magnum are the paired occipital condyles, curved and smooth projections. The occipital condyles have a movable articulation with the atlas, the first cervical vertebra of the vertebral column (discussed later). On the stout basilar part (bas-i-lar), a four-sided plate anterior to the foramen magnum, is a midline projection, the pharyngeal tubercle (fah-rin-je-al).
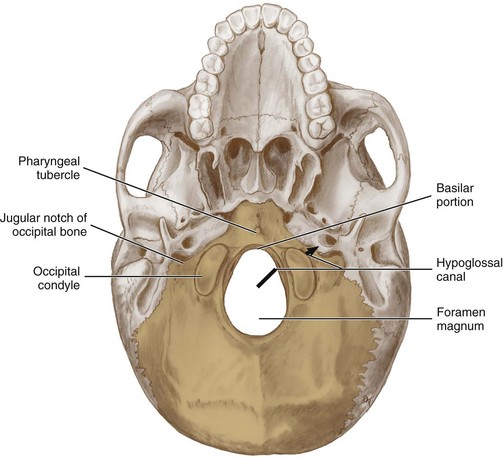
FIGURE 3-22 Inferior view of the external surface of the skull with the occipital bone highlighted and its features noted.
When tilting the skull model, the openings anterior and lateral to the foramen magnum are visible on the inferior view of the occipital bone (see Table 3-3). These openings are the paired hypoglossal canals (see Figure 3-22). The twelfth cranial or hypoglossal nerve is transmitted through the hypoglossal canal. Also present is the jugular notch of the occipital bone, the medial part that forms the jugular foramen (the lateral part is from the temporal bone).
Frontal Bone
The frontal bone is a single fused cranial bone that forms the anterior part of the skull superior to the eyes in the frontal region, and includes the forehead and the roof of the orbits (Figure 3-23 and see Figures 2-2 and 2-6 ). It develops as two bones, which are usually fused together by age 5 or 6.
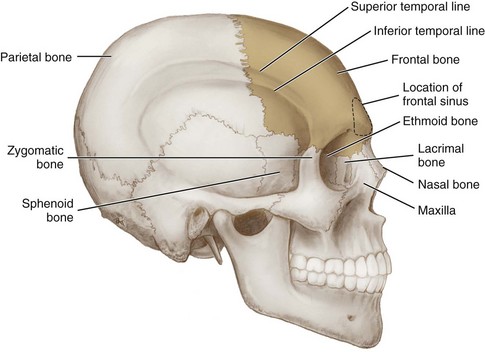
FIGURE 3-23 Lateral view of the skull with the frontal bone highlighted and its bony articulations noted.
The frontal bone articulates with the parietal bones, sphenoid bone, lacrimal bones, nasal bones, ethmoid bone, zygomatic bones, and maxillae. The frontal bone’s part of the superior temporal line and inferior temporal line is visible when the bone is viewed from the lateral aspect as discussed earlier. Internally, the frontal bone contains the paired paranasal sinuses, the frontal sinuses (discussed later). The frontal bone can also be studied from both anterior and inferior views.
Frontal Bone from Anterior View.: On the anterior aspect, certain landmarks are visible on the frontal bone (Figure 3-24, see Figures 2-2 and 2-6 ). The orbital plate of the frontal bone forms the superior wall or orbital roof. The curved elevations over the superior part of the orbit are the supraorbital ridges, subjacent to the eyebrows, which are more prominent in adult males. The supraorbital notch (soo-prah-or-bit-al) is located on the medial part of the supraorbital ridge and is where the supraorbital artery and nerve travel from the orbit to the forehead. The supraorbital notch is located about 1 inch from the midline and can produce soreness when palpated.
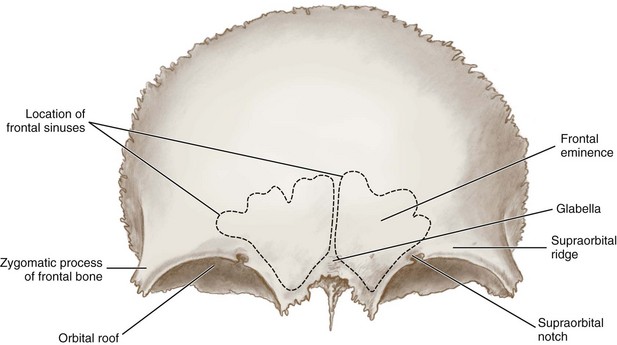
Between the supraorbital ridges is the glabella, the smooth elevated area between the eyebrows, which tends to be flat in children and adult females, but forms a rounded prominence in adult males. The prominence of the forehead, the frontal eminence, is also evident. In contrast, the frontal eminence is usually more pronounced in children and adult females. Lateral to the orbit is a projection, the orbital surface of the zygomatic process of the frontal bone (see Table 3-4).
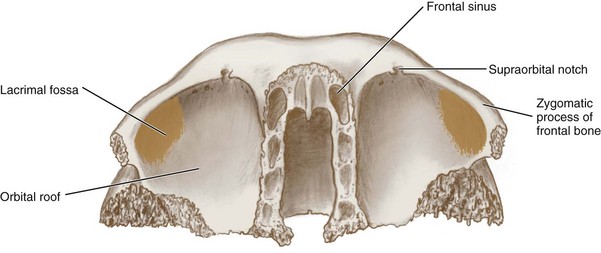
Frontal Bone from Inferior View.: From the inferior view of the frontal bone, each lacrimal fossa (lak-ri-mal) is visible (Figure 3-25 and see Figure 2-6). The lacrimal fossa is located just inside the lateral part of the supraorbital ridge. This fossa contains the lacrimal gland, which produces lacrimal fluid or tears (see Chapter 7). After lubricating the eye, the lacrimal fluid empties into the nasal cavity through the nasolacrimal duct.
Parietal Bones
The parietal bones are paired cranial bones that articulate with each other at the sagittal suture (see Figure 3-26; see Table 3-2). The parietal bones also articulate with the occipital, frontal, temporal, and sphenoid bones; they articulate with the occipital bone at the lambdoidal suture. They are located posterior to the frontal bone, forming the greater part of the right and left lateral walls and the roof of the skull. They each have four borders and are shaped like a curved plate.
Temporal Bones
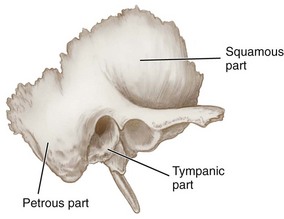
The temporal bones are paired cranial bones that form the lateral walls of the skull in the temporal region and part of the base of the skull in the auricular region. The bone is deep to the temple as well as part of the sphenoid bone (Figure 3-27). Each temporal bone articulates with one zygomatic and one parietal bone, the occipital and sphenoid bones, and the mandible. Each temporal bone is composed of three parts: the squamous, tympanic, and petrous.
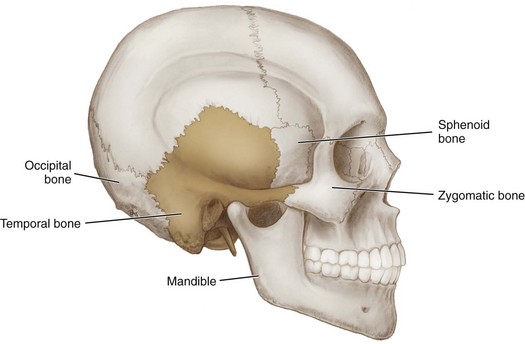
FIGURE 3-27 Lateral view of the skull with the temporal bone highlighted and its bony articulations noted.
The parts of the temporal bone can be viewed from the lateral aspect of the skull (Figure 3-28). The large, fan-shaped, flat part on each of the temporal bones is the squamous part of the temporal bone (skwa-mus). The second part is the small, irregularly shaped tympanic part of the temporal bone (tim-pan-ik), which is associated with the ear canal. The third part is the petrous part of the temporal bone (pet-rus), which is inferiorly located and helps form the cranial floor.
Squamous Part of Temporal Bone.: In addition to helping form the braincase, the squamous part of the temporal bone forms the zygomatic process of the temporal bone, which forms a part of the zygomatic arch (Figure 3-29; see Table 3-4). This part of the temporal bone also forms the cranial part of the temporomandibular joint (see Chapter 5). On the inferior surface of the zygomatic process of the temporal bone is the articular fossa (ar-tik-you-ler) (see Figures 5-2 and 5-4 ).
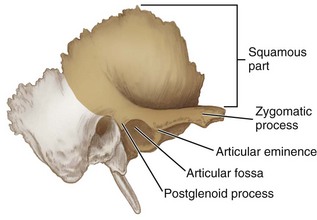
Anterior to the articular fossa is the articular eminence, and posterior is the postglenoid process (post-gle-noid) (see Table 3-4). The articular fossa and eminence are parts of the temporal bone that articulate with the mandible at the temporomandibular joint, which is an important consideration for dental professionals.
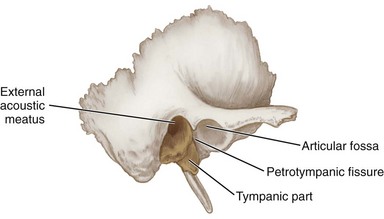
Tympanic Part of Temporal Bone.: The tympanic part of the temporal bone forms most of the external acoustic meatus (ah-koos-tik), a short canal leading to the tympanic cavity, located posterior to the articular fossa (Figure 3-30; see Figure 2-4 and Table 3-3). Also, posterior to the articular fossa, the tympanic part is separated from the petrosal part by a fissure, the petrotympanic fissure (pe-troh-tim-pan-ik), through which the chorda tympani nerve emerges.
Petrous Part of Temporal Bone.: On the inferior aspect of the petrous part of the temporal bone and posterior to the external acoustic meatus is a large roughened projection, the mastoid process (mass-toid) (Figure 3-31; see Table 3-4). The mastoid process is composed of air spaces or mastoid air cells that communicate with the middle ear cavity and also serves as the site for attachment of the large muscles of the neck such as the sternocleidomastoid muscle (see Figure 4-1).
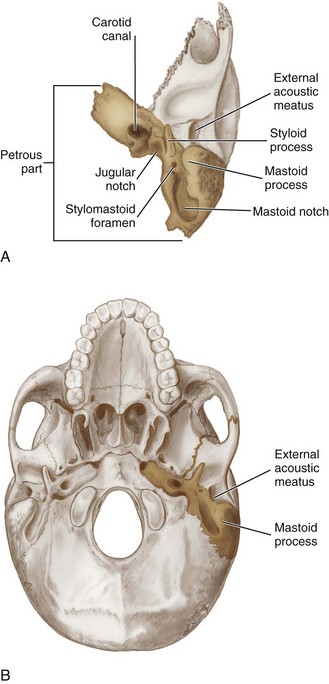
FIGURE 3-31 A, Inferior view of the temporal bone with the petrous part highlighted. B, Inferior view of the external skull surface with the petrous part of the temporal bone noted.
Medial to the mastoid process is the mastoid notch (see Figure 3-31). Inferior and medial to the external acoustic meatus is a long, pointed bony projection, the styloid process, a structure that serves for the attachment of tongue and pharyngeal muscles and ligaments (see Table 3-4). The stylomastoid foramen carries the seventh cranial or facial nerve and is named for its location between the styloid process and mastoid process (see Table 3-3).
The large circular aperture of the carotid canal is also noted, which ascends at first vertically, and then, making a bend, runs horizontally forward and medialward; it transmits into the cranium the internal carotid artery, and the carotid plexus of nerves. When the skull model is tilted, the jugular notch of the temporal bone is visible (see Table 3-3), which is the lateral part that forms the jugular foramen (the medial part is from the occipital bone).
On the intracranial surface of the petrous part of the temporal bone is the internal acoustic meatus, which carries the eighth cranial or vestibulocochlear nerve and the seventh cranial or facial nerve (see Figure 3-19; see Table 3-3). The size of the internal acoustic meatus varies considerably; its margins are smooth and rounded, and it leads into a short canal, about 1 cm in length, which runs lateralward. Both of these cranial nerves enter the skull at the internal acoustic meatus from the brain. The vestibulocochlear nerve remains inside the petrous part of the temporal bone, which contains the inner ear. In contrast, the facial nerve takes a convoluted path through the bone, eventually emerging at the stylomastoid foramen.
Sphenoid Bone
The single sphenoid bone is a cranial bone that somewhat resembles a bat with its wings extended; others see a butterfly taking wing (Figures 3-32 and 3-33). The sphenoid is a midline bone since it runs through the midsagittal section and thus is internally wedged between several other bones in the anterior part of the cranium. The sphenoid articulates with the frontal, parietal, ethmoid, temporal, zygomatic, maxillae, palatine, vomer, and occipital bones and helps to connect the cranial skeleton to the facial skeleton. This bone assists with the formation of the base of the cranium, the sides of the skull, and the floors and walls of each of the orbits.
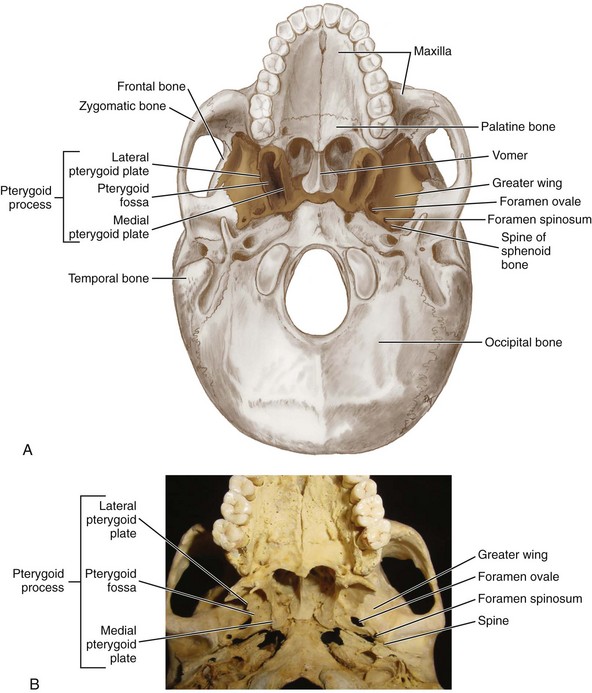
FIGURE 3-32 Inferior view of the external surface of the skull with the sphenoid bone highlighted (A) and close-up of sphenoid bone with its features noted (B).
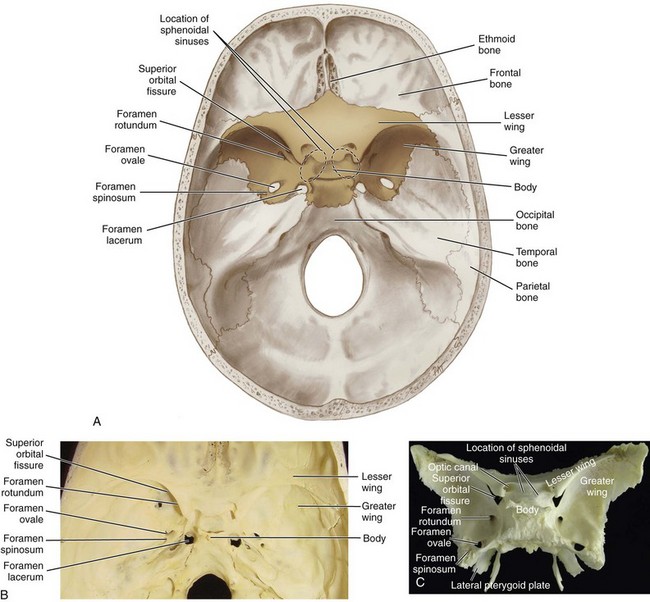
FIGURE 3-33 Superior view of the internal surface of the skull with the sphenoid bone highlighted (A) and close-up of sphenoid bone (B) and disarticulated bone (C).
This bone is complex, with some parts of the sphenoid encountered in almost every significant area of the skull. It consists of a body and its processes, as well as having a number of features, projections, and important foramina. This allows it to be seen from various views of the skull. Thus it is one of the more difficult bones to describe and visualize. The sphenoid is also important to dental professionals since it is the site for attachment for most of the muscles of mastication as well as providing passage by way of foramina for the branches of the trigeminal nerve or fifth cranial nerve that serves the oral cavity.
Body of Sphenoid Bone.: The middle part is the body of the sphenoid bone, which articulates on its anterior surface with the ethmoid bone and posteriorly with the basilar part of the occipital bone (see Figures 3-32 and 3-33). The body contains the paired paranasal sinuses, the sphenoidal sinuses (discussed later).
Sphenoid Bone Processes.: The body of the sphenoid bone has three paired processes projecting from it: the lesser wing, the greater wing, and the pterygoid process (Figure 3-34; see Figures 3-32 and 3-33 and Table 3-4). The projections include an anterior process, the lesser wing of the sphenoid bone, which forms the base of the orbital apex, and a posterolateral process, the greater wing of the sphenoid bone (see Figures 3-5 and 3-6).
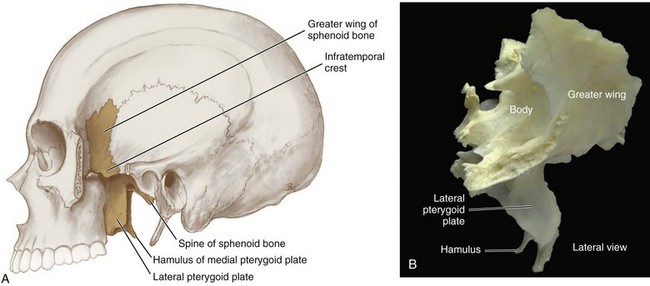
FIGURE 3-34 Lateral aspect of the sphenoid bone with cutaway view of the upper part of the skull with bone highlighted (A) and disarticulated bone (B).
Inferior to the greater wing of the sphenoid bone is the pterygoid process, an area of attachment for some of the muscles of mastication. The pterygoid process consists of two plates that project inferiorly, the flattened lateral pterygoid plate and thinner medial pterygoid plate, with the pterygoid fossa between them (see Figure 3-17). The hamulus, a thin curved process, is the inferior termination of the medial pterygoid plate. The pterygomaxillary fissure is between the pterygoid process of the sphenoid bone and the maxillary tuberosity of the maxilla (see Figure 3-61).
A sharp, pointed area, the (angular) spine of the sphenoid bone, is located at the posterior corner of each greater wing of the sphenoid bone. Each greater wing is divided into two smaller surfaces by the infratemporal crest: the temporal and infratemporal surfaces. The infratemporal fossa is lateral to the lateral pterygoid plate.
Sphenoid Bone Foramina.: Many foramina and fissures are located in the sphenoid which carry nerves and blood vessels of the head and neck that are significant to dental professionals, such as the superior orbital fissure (with ophthalmic nerve), foramen rotundum (with maxillary nerve) and foramen ovale (with mandibular nerve) (see Figures 3-32 and 3-33; see Table 3-3).
Ethmoid Bone
The ethmoid bone is a single midline cranial bone of the skull that runs through the midsagittal plane and helps connect the cranial skeleton to the facial skeleton similarly to the sphenoid bone (Figure 3-35). The ethmoid is located anterior to the sphenoid in the anterior part of the cranium. The ethmoid articulates with the frontal, sphenoid, lacrimal, and maxilla and adjoins the vomer at its inferior and posterior borders. If the sphenoid is the most difficult cranial bone to describe and visualize, the ethmoid is the second most difficult. It has a number of features and projections, but unlike the sphenoid the ethmoid cannot be seen from various views of the skull.
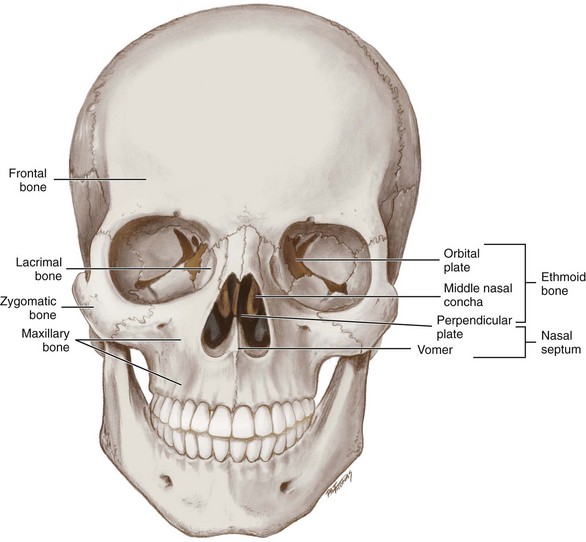
FIGURE 3-35 Anterior view of the skull with the ethmoid bone highlighted and its bony articulations and features noted.
Ethmoid Bone Plates and Associated Structures.: First to consider are the two unpaired plates that form the ethmoid bone: the midline vertical perpendicular plate (per-pen-dik-you-lar) and the horizontal cribriform plate, which it crosses. The perpendicular plate is easily seen in the nasal cavity and aids the nasal septal cartilage and vomer in forming the nasal septum (see Figure 3-35). A vertical midline continuation of the perpendicular plate superiorly into the cranial cavity is the wedge-shaped crista galli (kris-tah gal-lee), which serves as an attachment for layers covering the brain.
The cribriform plate, visible from the inside of the cranial cavity and present on the superior aspect of the bone and surrounding the cristal galli, is perforated by foramina to allow the passage of olfactory nerves for the sense of smell (Figures 3-36 and 3-37).
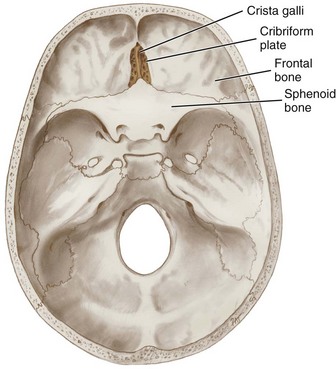
FIGURE 3-36 Superior view of the internal surface of the skull with the ethmoid bone highlighted and its bony articulations noted.
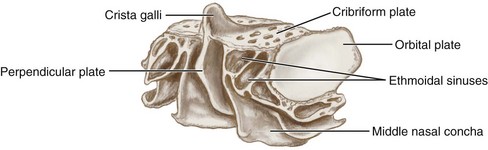
The lateral parts of the ethmoid bone form the superior nasal conchae (kong-kee) and middle nasal conchae in the nasal cavity and the paired orbital plates (Figure 3-38; see Figure 3-37). The orbital plate of the ethmoid bone forms the medial orbital wall. Between the orbital plate and the conchae are the ethmoidal sinuses or ethmoid air cells, which are a variable number of small cavities in the lateral mass of the ethmoid (discussed later).
Facial Bones
The facial bones form the facial features and serve as a base for dentition. The facial bones include the single vomer and mandible as well as the paired lacrimal, nasal, inferior nasal conchal, zygomatic bones, and maxillae (see Figure 3-4). For ease of learning, the paired palatine bones are considered under the heading of facial bones, but they are not strictly considered facial bones.
Many bones of the face are shared by two or more soft tissue structures of the face. For example, the frontal bone forms both the forehead and the areas around the eyes. This is important to remember because an abnormality in one facial bone often involves many soft tissue structures (discussed later).
Vomer
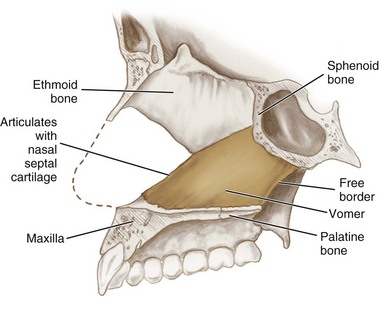
The vomer is a thin, flat single midline facial bone almost trapezoid in shape. The vomer forms the posterior part of the nasal septum, with the anterior part formed by the ethmoid. It is located in the midsagittal plane inside the nasal cavity and its articulations are easily seen on a lateral view of the bone (Figure 3-39). The vomer articulates with the ethmoid bone on its anterosuperior border, the nasal cartilage anteriorly, the palatine bones and maxillae inferiorly, and the sphenoid bone on its posterosuperior border. The posteroinferior border is free of bony articulation and has no muscle attachments.
Lacrimal Bones, Nasal Bones, And Inferior Nasal Conchae
Each paired lacrimal bone is an irregular, thin plate of bone that forms a small part of the anterior medial wall of the orbit (Figure 3-40; see Figure 3-5). The lacrimal bones are the smallest and most fragile of the facial bones and are each located posterior to the frontal process of the maxilla. Each lacrimal bone articulates with the ethmoid and frontal bones as well as the maxilla. The nasolacrimal duct (nay-so-lak-rim-al) is formed at the junction of the lacrimal and maxilla. Lacrimal fluid or tears from the lacrimal gland are drained through this duct into the inferior nasal meatus (see Chapter 7).
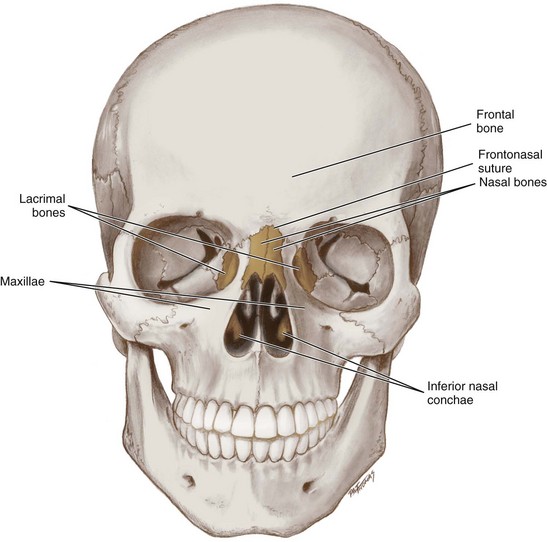
FIGURE 3-40 Anterior view of the skull with the nasal bones, inferior nasal conchae, and lacrimal bones.
The nasal bones are small oblong paired facial bones that lie side by side, fused to each other to form the bridge of the nose in the midline superior to the piriform aperture (see Figure 2-7). The nasal bones fit between the frontal processes of the maxillae and thus articulate with the frontal bone superiorly at the frontonasal suture (frunt-o-nay-zil) and the maxillae laterally (see Figure 3-40 and Table 3-2).
The inferior nasal conchae are paired facial bones that project from the maxillae to form a part of the lateral walls of the nasal cavity (see Figure 3-40). Unlike the superior and middle nasal conchae that also project from the maxillae, the inferior nasal conchae are separate facial bones. Each inferior nasal concha is composed of fragile, thin, spongy bone curved onto itself like a scroll. By projecting into the nasal cavity, the medial surface of these bones assists in increasing the surface area and, by directing and deflecting airflow propels the inspired air. These bones articulate with the ethmoid, lacrimal, and palatine bones as well as the maxillae. The inferior nasal conchae do not have any muscle attachments.
Zygomatic Bones
Each zygomatic bone or zygoma is a paired facial bone of the skull that forms the cheekbones or malar surfaces, and helps to form the walls and floor of the orbits (Figures 3-41 and 3-42). The zygomatic bones articulate with the frontal, temporal, sphenoid bones as well as the maxillae. Each zygomatic bone is diamond-shaped and composed of three processes with similarly named associated bony articulations: frontal, temporal, and maxillary.
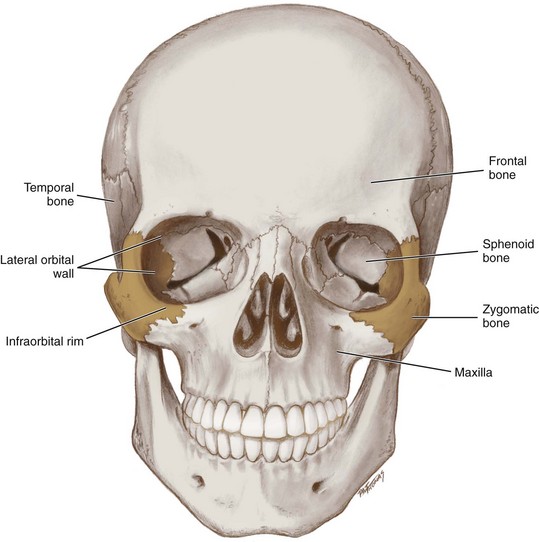
FIGURE 3-41 Anterior view of the skull with the zygomatic bones highlighted and their articulations and features noted.
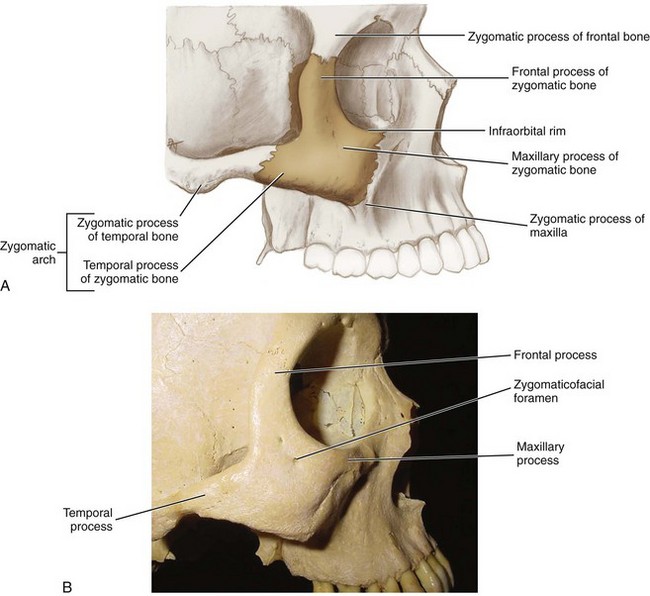
FIGURE 3-42 Lateral view of the middle part of the skull with the zygomatic bone highlighted with its bony articulations and features noted such as the zygomatic arch (A) and close-up of zygomatic bone and its processes (B).
Zygomatic Bone Processes.: Each process of the zygomatic bone forms important structures of the skull (see Figures 3-41 and 3-42 and Table 3-4). The orbital surface of the frontal process of the zygomatic bone forms the anterior lateral orbital wall, with usually a small paired foramen, the zygomaticofacial foramen (zy-go-mat-i-ko-fay-shal) opening on its lateral surface (see Table 3-3). The temporal process of the zygomatic bone forms the zygomatic arch along with the zygomatic process of the temporal bone, with a paired zygomaticotemporal foramen (zy-go-mat-i-ko-tem-poh-ral) present on the surface of the bone (see Table 3-3). The orbital surface of the maxillary process of the zygomatic bone forms a part of the infraorbital rim (in-frah-or-bit-al) and a small part of the anterior part of the lateral orbital wall.
Palatine Bones
The palatine bones are paired bones of the skull that are not strictly facial bones, but are considered under this heading for ease of learning. Each palatine bone is somewhat L-shaped and thus consists of two plates: horizontal and vertical. They form the posterior part of the hard palate and the floor of the nasal cavity; anteriorly, they join with the maxillae.
Plates and Sutures of Palatine Bones.: Both the horizontal and vertical plates can be seen from a posterior view of a palatine bone (Figure 3-43). The horizontal plates of the palatine bone form the lesser or posterior part of the hard palate. The vertical plates of the palatine bone form a part of the lateral walls of the nasal cavity, and each plate contributes a small lip of bone to the orbital apex.
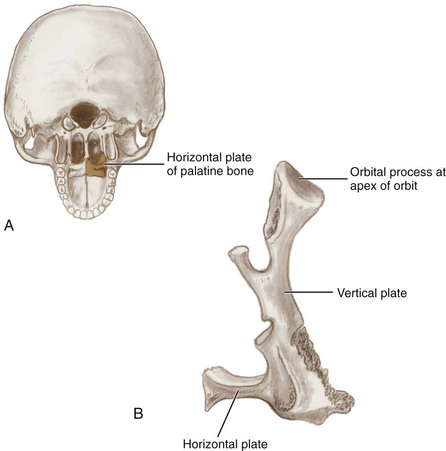
FIGURE 3-43 Posterior view of the right palatine bone with its location highlighted on a posterior-inferior view of the skull (A) and lateral view of the disarticulated bone with its features noted (B).
The palatine bones serve as a link between the maxillae and the sphenoid bone with which they articulate, as well as with each other. The two horizontal plates articulate with each other at the posterior part of the median palatine suture and more anteriorly with the maxillae at the transverse palatine suture (Figure 3-44; see Table 3-2 and Figure 2-15).
Foramina of Palatine Bones.: There are two important foramina in the palatine bones that transmit nerves and blood vessels to this region: the greater and lesser palatine (see Figure 3-44 and Table 3-3). The larger greater palatine foramen is located in the posterolateral region of each of the palatine bones, usually at the apex of the maxillary third molar. The greater palatine foramen transmits the greater palatine nerve and blood vessels and is a landmark for the administration of the greater palatine block (see Figure 9-19).
A smaller opening nearby, the lesser palatine foramen, transmits the lesser palatine nerve and blood vessels to the soft palate and tonsils. Both foramina are openings of the pterygopalatine canal that carries the descending palatine nerves and blood vessels from the pterygopalatine fossa to the palate.
The sphenopalatine foramen (sfe-no-pal-ah-tine) is the opening between the sphenoid bone and orbital processes of the palatine bone; it opens into the nasal cavity and gives passage to branches from the pterygopalatine ganglion and the sphenopalatine artery from the maxillary artery.
Maxillae
The maxillae (mak-sil-lay) consist of paired maxillary bones or maxilla that are fused together at the intermaxillary suture (Figure 3-45 and see Table 3-2). These bones are the largest bones of the face and together form the upper jaw. Each maxilla articulates with the frontal, lacrimal, nasal, inferior nasal conchal, vomer, sphenoid, ethmoid, palatine, and zygomatic bones. Each maxilla includes a body and four processes: frontal, zygomatic, palatine, and alveolar.
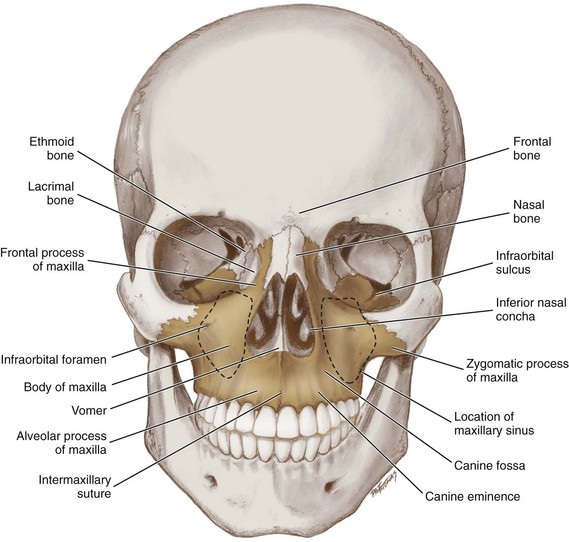
FIGURE 3-45 Anterior view of the skull with the maxillae highlighted and its bony articulations noted (articulation of maxillae with pterygoid process of the sphenoid bone and palatine bones cannot be seen in this view).
The body of the maxilla has orbital, nasal, infratemporal, and facial surfaces. The bodies contain air-filled spaces or paranasal sinuses, the maxillary sinuses (discussed later). Each maxilla can be studied from three views: anterior, lateral, and inferior.
Maxillae from Anterior View.: From the anterior view, each frontal process of the maxilla articulates with the frontal bone and forms the medial orbital rim with the lacrimal bone on its anterior surface (Figures 3-46 and 3-47; see Figure 3-45 and Table 3-4). Each maxilla’s orbital surface is separated from the sphenoid bone by the inferior orbital fissure (see Figure 3-7 and Table 3-3). The inferior orbital fissure carries the infraorbital and zygomatic nerves, infraorbital artery, and inferior ophthalmic vein. The groove in the floor of the orbital surface is the infraorbital sulcus.
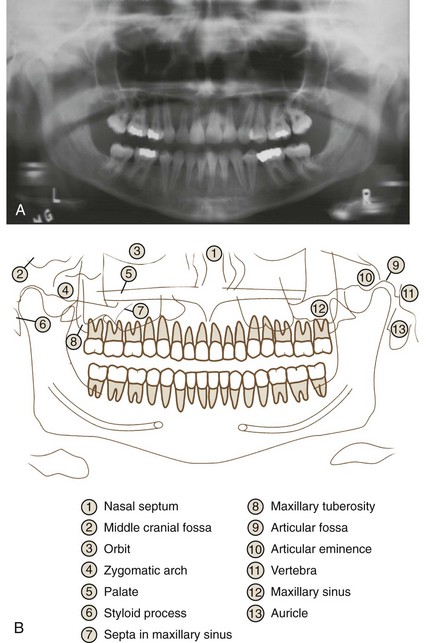
FIGURE 3-46 A, Panoramic radiograph. B, Panoramic anatomy of the midface. (A from Bath-Balogh M, Fehrenbach MJ: Illustrated dental embryology, histology, and anatomy, ed 3, St. Louis, 2011, Saunders. B modified from Olson SS: Dental radiography laboratory manual, Philadelphia, 1995, WB Saunders.)
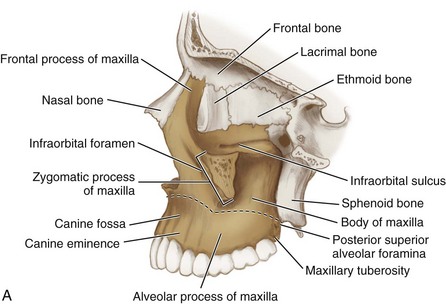
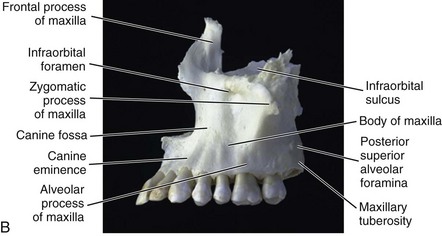
FIGURE 3-47 Cutaway view of the lateral aspect of the skull with the maxilla highlighted with features noted (A) and disarticulated bone (B). Note also the approximate junction between the alveolar process and the body of the maxilla (dashed lines).
The infraorbital sulcus becomes the infraorbital canal and then terminates on the facial surface of each maxilla as the infraorbital foramen (see Table 3-3). It is located approximately 2 cm inferior to the midpoint of the inferior margin of the orbit, in a vertical line with the supraorbital notch, which is superior to it. This foramen transmits the infraorbital nerve and blood vessels. The infraorbital foramen is a landmark for the administration of the infraorbital block (see Figure 9-15). Palpation of the infraorbital foramen during an extraoral examination or an administration of a local anesthetic agent will cause soreness to the area. Inferior to the infraorbital foramen is an elongated depression, the canine fossa (kay-nine). The canine fossa is just posterosuperior to the roots of each of the maxillary canine teeth.
Each tooth of the maxillary arch is covered by a prominent facial ridge of bone, a part of the alveolar process of the maxilla (see Table 3-4). The facial ridge over each of the maxillary canines, the canine eminence, is especially prominent, making it a landmark for the administration of the anterior superior alveolar block (see Figure 9-12). The maxillary bone over the facial surface of the maxillary teeth is less dense than the mandibular bone over similar teeth as can be viewed on a panoramic radiograph (see Figures 3-46 and 3-50). This allows a greater incidence of clinically adequate local anesthesia for the maxillary teeth when the agent is administered as a local infiltration than would occur with similar teeth on the mandibular arch (see Chapter 9).
Maxilla from Lateral View.: From the lateral view, each zygomatic process of the maxilla articulates with the zygomatic bone laterally, completing the infraorbital rim (see Figures 3-46 and 3-47 and Table 3-4). Some of the landmarks noted from the anterior view of the maxilla are also present.
On the posterior part of the body of the maxilla is a rounded, roughened elevation, the maxillary tuberosity, just posterior to the most distal molar of the maxillary arch of the dentition, which is a landmark for mounting radiographs as well serving as the one of the boundaries of the fossae of the skull (see Figures 3-46 to 3-48, 3-61 and 2-21). The superolateral part of the maxillary tuberosity is perforated by the posterior superior alveolar foramina, where the posterior superior alveolar nerve and blood vessel branches enter the bone from the posterior. The maxillary tuberosity and posterior superior alveolar foramina are also landmarks for the administration of the posterior superior alveolar block (see Figure 9-2).
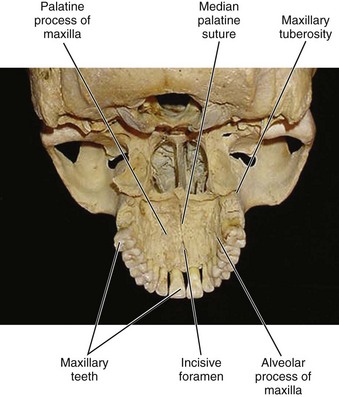
Maxillae from Inferior View.: On the inferior aspect, each palatine process of the maxilla articulates with the other to form the major or anterior part of the hard palate (Figure 3-48; see Figure 3-46 and Table 3-4). There are a number of small pores in the maxillary bone of the anterior hard palate. The suture between these two palatine processes of the maxilla is the anterior part of the median palatine suture (see Table 3-2). This is covered by the median palatine raphe, a midline fibrous band of tissue, which is a landmark along with the hard palate pores for the administration of the anterior middle superior alveolar block (see Figures 2-15 and 9-28 ). On the posterior part of the body of the maxilla, the maxillary tuberosity is again viewed.
In the anterior midline between the articulating palatine processes of the maxillae, just posterior to the maxillary central incisors, is the incisive foramen (in-sy-ziv) (see Table 3-3). This foramen carries the branches of both the right and left nasopalatine nerves and blood vessels from the nasal cavity to the anterior hard palate. The soft tissue that bulges over the incisive foramen is the incisive papilla (see Figure 2-15). The incisive foramen and incisive papilla are landmarks for the administration of the nasopalatine block (see Figure 9-23).
The alveolar process of the maxilla usually contains the roots of the maxillary teeth (see Figures 3-46, 48, and 2-13 and Table 3-4). The alveolar process of the maxilla can become resorbed when completely edentulous in the maxillary arch (resorption occurs to a lesser extent in partially edentulous cases), possibly leading to problems with the maxillary sinuses (discussed later). However, the more superior body of the maxilla is not resorbed with tooth loss, but its walls may become thinner in this case.
The density of the maxillary bone in an area determines the route that a dental infection takes with abscess and fistula formation (see Chapter 12). In addition, the differences in alveolar process density determine the easiest and most convenient areas of bony fracture used if needed during tooth extraction. Thus the maxillary teeth are easier to remove by fracturing the thinner facial surface rather than the thicker lingual surface.
Mandible
The mandible is a single fused facial bone that forms the lower jaw and is the only freely movable bone of the skull. This bone is also the largest and strongest facial bone, almost horseshoe-shaped with an upward sloping part at each end. The mandible has a movable articulation with the temporal bones at each temporomandibular joint (Figure 3-49, see Figure 5-1). The mandible also articulates with each of the maxilla by way of their contained respective mandibular and maxillary arches of the dentition. The mandible is more effectively studied when it is temporarily removed from the skull model and can be studied from three views: anterior, lateral, and medial.
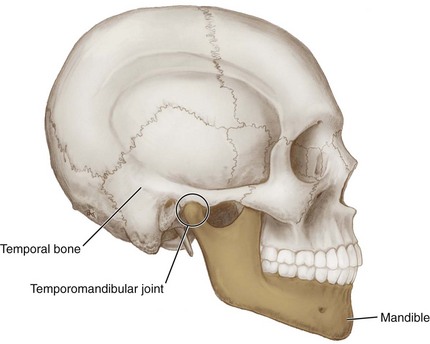
FIGURE 3-49 Lateral view of the skull showing the mandible highlighted and the temporomandibular joint noted (circled).
Mandible from Anterior View.: From the anterior view, there are many important landmarks such as the mental protuberance, the bony prominence of the chin, located inferior to the roots of the mandibular incisors (Figure 3-50; see Figure 2-22). The mental protuberance is more pronounced in males but can be visualized and palpated in females. In the midline on the anterior surface of the mandible is a faint ridge, an indication of the mandibular symphysis (sim-fi-sis), where the bone is formed by the fusion of right and left processes during mandibular development. Like other symphyses in the body, this is a midline articulation where the bones are joined by fibrocartilage, but this articulation fuses together in early childhood.
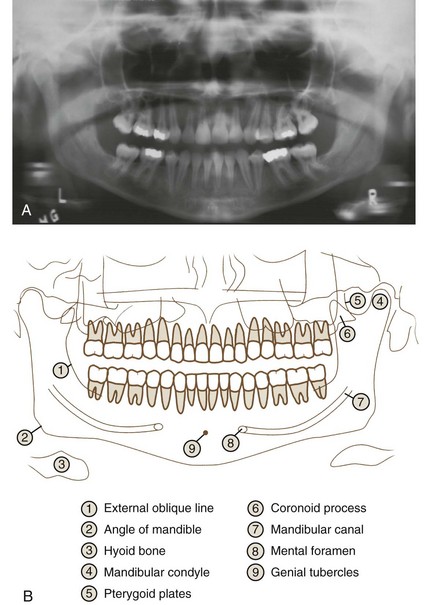
FIGURE 3-50 A, Panoramic radiograph. B, Panoramic anatomy of the lower face. (A from Bath-Balogh M, Fehrenbach MJ: Illustrated dental embryology, histology, and anatomy, ed 3, St. Louis, 2011, Saunders/Elsevier. B modified from Olson SS: Dental radiography laboratory manual, Philadelphia, 1995, WB Saunders.)
Farther posteriorly on the lateral surface of the mandible, usually inferior to the apices of the mandibular first and second premolars, is an opening, the mental foramen (see Figures 3-50 to 3-52 and Table 3-3). As mandibular growth proceeds in young children, the mental foramen alters in direction of its opening from anterior to posterosuperior. The mental foramen allows the entrance of the mental nerve and blood vessels into the mandibular canal (discussed later).
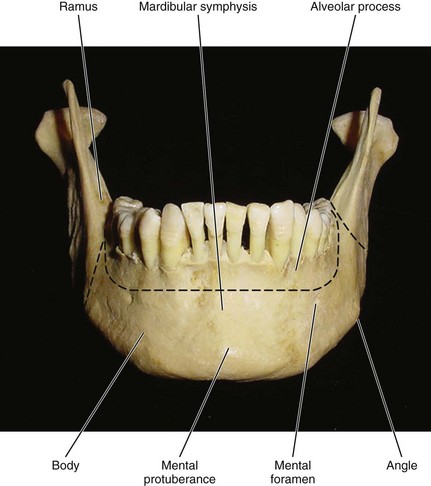
FIGURE 3-51 Anterior view of the mandible and its associated features. Note also the approximate junction between the alveolar process and the body of the mandible (dashed lines).
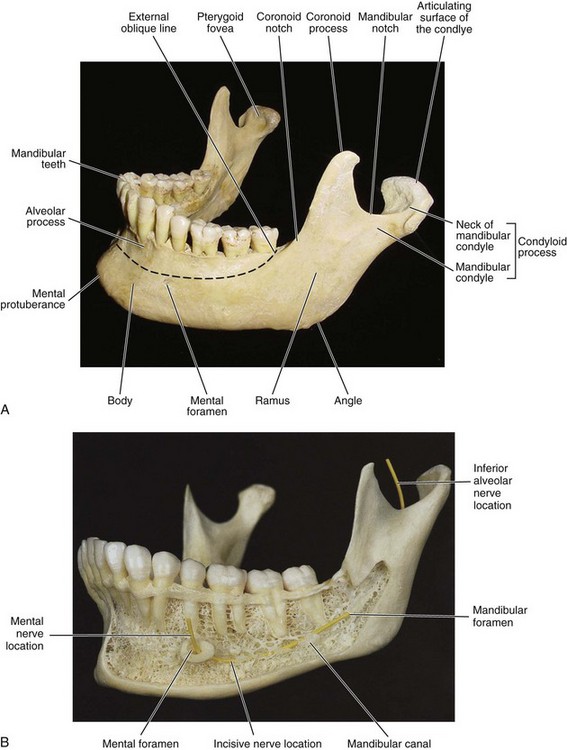
FIGURE 3-52 Slightly oblique lateral view of the mandible and its associated features (A) and with cutaway view that has a yellow marker for the pathway of the inferior alveolar nerve, which enters the mandibular foramen as the incisive nerve and exits the mental foramen as the mental nerve (B). Note also the approximate junction between the alveolar process and the body of the mandible (dashed lines [A]). (B from Logan BM, Reynold PA, Hutching RT: McMinn’s color atlas of head and neck anatomy, ed 4, London, 2010, Mosby Ltd.)
The mental foramen’s posterosuperior opening in adults signifies the changed direction of the emerging mental nerve. This is an important landmark to note intraorally and on a radiograph before administration of both mental and incisive blocks (see Figures 9-42 and 9-46). Not confusing the circular radiolucent mental foramen on a radiograph with a periapical lesion related to the teeth or any other oral radiolucent lesions is also important.
The heavy horizontal part of the lower jaw inferior to the mental foramen is the body of the mandible or base (see Figure 3-51). Superior to this, the part of the lower jaw that usually contains the roots of the mandibular teeth is the alveolar process of the mandible (see Figures 2-13 and 3-52 and Table 3-4). The body of the mandible, along with the alveolar process, elongates to provide space for additional teeth as the child nears adulthood.
The mandibular alveolar process can become resorbed when completely edentulous in the mandibular arch (occasionally noted also in partially edentulous cases). This resorption can occur to such an extent that the mental foramen is virtually on the superior border of the mandible, instead of opening on the anterior surface, changing its relative position. However, the more inferior body of the mandible is not affected and remains thick and rounded.
The alveolar process of the mandibular incisors is less dense than the body of the mandible and even less dense than the alveolar process of the mandibular posterior teeth as can be viewed on a panoramic radiograph (see Figures 3-46 and 3-50). This allows a local infiltration of local anesthetic agent for the mandibular anterior teeth to have a higher degree of success than the mandibular posterior teeth but always less success than all the maxillary teeth (see Chapter 9).
The density of the mandibular bone in an area also determines the route that a dental infection takes with abscess and fistula formation (see Chapter 12). In addition, the differences in alveolar process density determine the easiest and most convenient areas of bony fracture used during tooth extraction. Thus the mandibular third molar is easier to remove by fracturing the thinner lingual surface (being careful of nearby lingual nerve) rather than the thicker buccal surface, if needed.
Mandible from Lateral View.: On the lateral aspect of the mandible, the stout, flat plate(s) of the ramus (plural, rami) (ray-mus, ray-me) extends superiorly and posteriorly from the body of the mandible on each side (see Figure 3-52). During growth of the body, both the body of the mandible and alveolar process elongate posterior to the mental foramen, providing space for three additional permanent teeth. Each ramus, which serves as the primary area for the attachment of the muscles of mastication, grows superiorly and posteriorly, displacing the mental protuberance of the chin inferiorly and anteriorly nearing adulthood.
The anterior border of the ramus is a thin, sharp margin that terminates in the coronoid process (kor-ah-noid) (see Table 3-4). The main part of the anterior border of the ramus forms a concave forward curve, the coronoid notch. This notch is the greatest depression on the anterior border of the ramus. The coronoid notch is a landmark for the administration of the inferior alveolar block (see Figures 9-35 and 9-37). Inferior to the coronoid notch, the anterior border of the ramus becomes the external oblique line (ob-leek), a crest where the ramus joins the body of the mandible. The line is noted as a radiopaque line on a radiograph superior to the mylohyoid line; clinicians may use this line intraorally to help locate the coronoid notch (see Figure 3-50).
The posterior border of the ramus is thicker and extends from the angle of the mandible, which is the juncture between the ramus and the body of the mandible, to a large more posterior projection, the condyloid process (kon-di-loid), which consists of two parts: the mandibular condyle, and the constricted part which supports it, the neck (see Figures 3-50 to 3-53 and Table 3-4). The anteromedial border of the mandibular condylar neck is a landmark for the Gow-Gates mandibular block (see Figure 9-48). The articulating surface of the condyle (ar-tik-you-late-ing) is an oval head of the condyle involved in the temporomandibular joint (see Figure 5-3). Between the coronoid process and the condyle is a depression, the mandibular notch or sigmoid notch.
Mandible from Medial View.: Visible on the medial view of the mandible are the body of the mandible, the alveolar process of the mandible (see Table 3-4), and the ramus (Figure 3-54). In addition, near the midline of the mandible are the genial tubercles (ji-ni-il) or mental spines, a cluster of small projections that serve as a muscle attachment area.
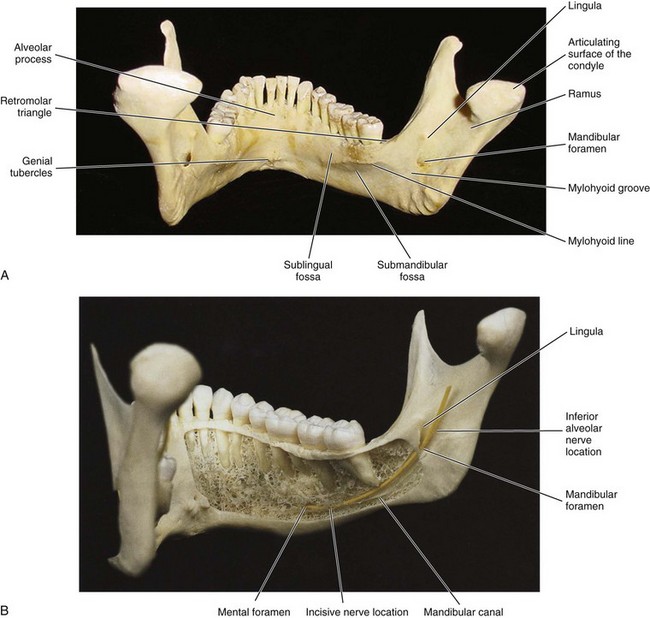
FIGURE 3-54 Medial view of the mandible and its associated features (A) and cutaway view that has a yellow marker for the pathway of the inferior alveolar nerve, which enters the mandibular foramen as the incisive nerve and exits the mental foramen as the mental nerve (B). (B from Logan BM, Reynold PA, Hutching RT: McMinn’s color atlas of head and neck anatomy, ed 4, London, 2010, Mosby Ltd.)
At the lateral edge of each mandibular alveolar process is a rounded, roughened area, the retromolar triangle (re-tro-moh-lar), just posterior to the most distal molar of the mandibular arch of the dentition. The retromolar triangle is a bony landmark that, when covered with soft tissue, is the retromolar pad (see Figure 2-21).
Along each medial surface of the body of the mandible is the internal oblique ridge or mylohyoid line (my-lo-hi-oid) that extends posteriorly and superiorly, becoming more prominent as it ascends each body. The mylohyoid line is the point of attachment of the mylohyoid muscle that forms the floor of the mouth (see Figure 4-24). The roots of the mandibular posterior teeth often extend internally inferior to the mylohyoid line. The line can be noted on a radiograph as the radiopaque line inferior to the external oblique line (see Figure 3-50).
A shallow depression, the sublingual fossa (sub-ling-gwal), which contains the sublingual salivary gland, is located superior to the anterior part of the mylohyoid line (see Figure 7-7). Inferior to the posterior part of the mylohyoid line and inferior to the mandibular posterior teeth is a deeper depression, the submandibular fossa (sub-man-dib-you-lar), which contains the submandibular salivary gland (see Figure 7-5).
On the medial surface of the ramus is the mandibular foramen (man-dib-you-lar), which is the opening of the mandibular canal (see Figure 3-54 and Table 3-3). The mandibular foramen is three fourths the distance from the coronoid notch to the posterior border of the ramus (see Figure 9-35). The inferior alveolar nerve and blood vessels exit the mandible through the mandibular foramen after traveling in the mandibular canal. With age and tooth loss, the alveolar process is absorbed so that the mandibular canal becomes nearer the superior border. Sometimes with excessive alveolar process absorption, the mandibular canal disappears entirely and leaves the inferior alveolar nerve without its bony protection, although it is still covered by soft tissue.
Rarely, a bifid inferior alveolar nerve may be present, in which case a second mandibular foramen, more inferiorly placed, exists and can be detected by noting a doubled mandibular canal on a radiograph (see Chapter 8). Keeping this anatomic variant concerning the mandibular foramen, as well as its usual location, in mind is important when administering an inferior alveolar block (see Chapter 9).
Overhanging the mandibular foramen is a bony spine, the lingula (lin-gu-lah), which serves as an attachment for the sphenomandibular ligament associated with the temporomandibular joint (see Figure 5-5, A). A small groove, the mylohyoid groove, passes anteriorly to and inferiorly from the mandibular foramen. The mylohyoid nerve and blood vessels travel in the mylohyoid groove.
The articulating surface of the condyle can also be seen in this medial view. This is where the mandible articulates with the temporal bone at the temporomandibular joint (see Chapter 5). Inferior to the articular surface of the condyle on the anterior surface of the neck is a triangular depression, the pterygoid fovea (fo-vee-ah), which serves for the attachment of the lateral pterygoid muscle (see Figures 3-52 and 4-23).
Paranasal Sinuses
The paranasal sinuses (pare-ah-nay-zil) are paired, air-filled cavities in bone, which project laterally, superiorly, and posteriorly into surrounding bones (Figures 3-55 and 3-56). These sinuses are lined with mucous membranes and are continuous with the nasal cavities. The paranasal sinuses include: the frontal, sphenoidal, ethmoidal, and maxillary sinuses. The sinuses communicate with the nasal cavity through small ostia or openings in the lateral nasal wall. The sinuses serve to lighten the skull bones, act as sound resonators, and provide mucus for the nasal cavity.
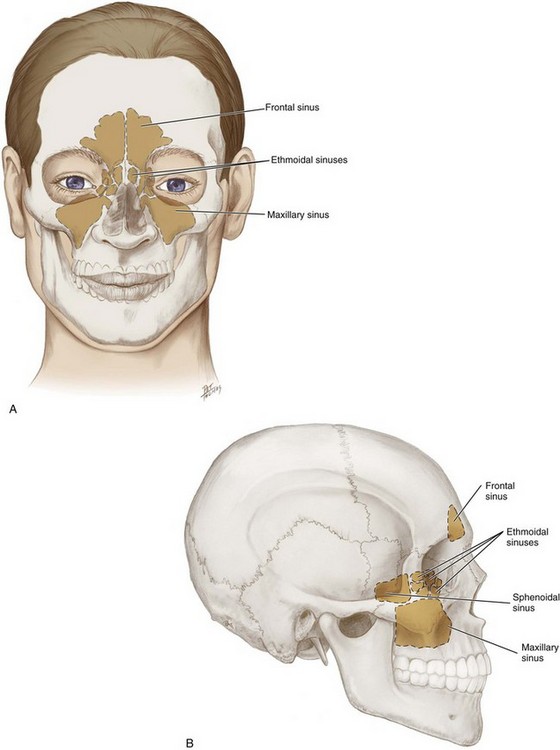
FIGURE 3-55 Anterior view of the skull with the location of the paranasal sinuses highlighted (see dashed lines) and with the superimposition of facial structures (A) and lateral view (B).
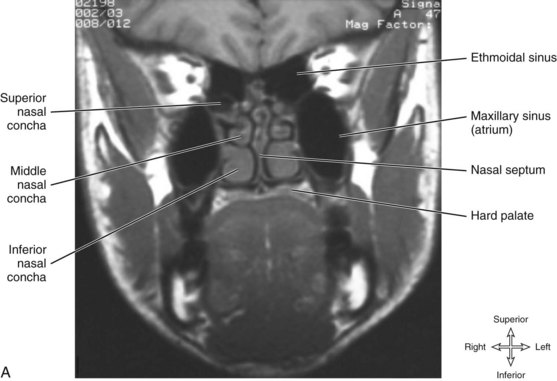

FIGURE 3-56 A, Coronal magnetic resonance imaging (MRI) of the nasopharynx and oropharynx showing the ethmoidal sinus and maxillary sinus. B, Waters view (occipitomental sinus) radiograph showing the opacification (or cloudiness) of the infected left maxillary sinus (arrow) due to retained mucus as compared to the translucent normal right sinus. (From Reynolds PA, Abrahams PH: McMinn’s interactive clinical anatomy: head and neck, ed 2, London, 2001, Mosby Ltd.)
Frontal Sinuses
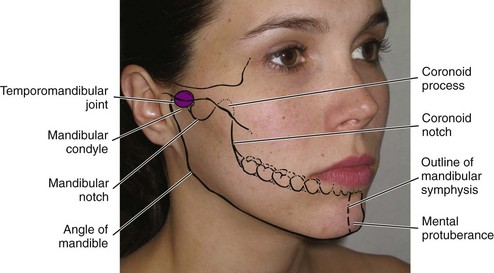
The paired frontal sinuses are located in the frontal bone just superior to the nasal cavity (see Figures 3-23 and 3-25). These two paranasal sinuses are asymmetric (approximately 2 to 3 cm in diameter), but the left and right sinuses are always separated by a septum. Each frontal sinus communicates with and drains into the nasal cavity by a constricted canal to the middle nasal meatus, the frontonasal duct (frunt-o-nay-zil). Stand near the patient during an extraoral examination and visually inspect and bilaterally palpate the frontal sinuses (Figure 3-57).

Sphenoidal Sinuses
The paired sphenoidal sinuses are located in the body of the sphenoid bone and cannot be palpated during an extraoral examination (see Figure 3-33). These two paranasal sinuses are frequently asymmetric (approximately 1.5 to 2.5 cm in diameter) due to the lateral displacement of the intervening septum. The sphenoidal sinuses communicate with and drain into the nasal cavity through an opening superior to each superior nasal concha.
Ethmoidal Sinuses
The ethmoidal sinuses or ethmoid air cells are a variable number of small cavities in the lateral mass of each of the ethmoid bones and cannot be palpated during an extraoral examination (see Figures 3-37 and 3-56). These paranasal sinuses are roughly divided into the anterior, middle, and posterior ethmoid air cells. The posterior ethmoid air cells open into the superior meatus of the nasal cavity, and the middle and anterior ethmoid air cells open into the middle meatus.
Maxillary Sinuses
The maxillary sinuses are paired paranasal sinuses located in each body of the maxillae, just posterior to the maxillary canine and premolars (see Figures 3-45, 3-46, 3-56). The size varies according to individuals and their ages. However, these pyramid-shaped sinuses are the largest of the paranasal sinuses, and each one has an apex, three walls, a roof, and a floor.
The apex of the pyramid of the maxillary sinus points into the zygomatic arch, with the medial wall formed by the lateral wall of the nasal cavity. The anterior wall corresponds with the anterior or facial wall of the maxillae, and the posterior wall is the infratemporal surface of the maxilla, the maxillary tuberosity. The roof of the maxillary sinus is the orbital floor, and the floor is the alveolar process of each maxillae. Each maxillary sinus is further divided into communicating compartments by bony walls or septa.
The maxillary sinus drains into the middle meatus on each side. Drainage of the maxillary sinus is complicated and may promote a prolonged or chronic sinusitis because the ostium of each sinus is higher than the floor of the sinus cavity (see next discussion). Surgery may be possibly required in the case of chronic maxillary sinusitis.
Stand near the patient during an extraoral examination to visually inspect and bilaterally palpate the maxillary sinuses (Figure 3-58). A part of the sinuses can be seen on radiographs of the maxillary posterior teeth. Due to the proximity of the maxillary sinus to the alveolar process containing the roots of the maxillary posterior teeth, the periodontal tissue of these teeth may be in direct contact with the mucosa of the maxillary sinus (see Figure 3-46). The discomfort associated with primary maxillary sinus infection can also mimic the discomfort of endodontic or periodontal infection of the maxillary posterior teeth.

With age, the enlarging maxillary sinus may even begin to surround the roots of the maxillary posterior teeth and extend its margins into the body of the zygomatic bone. If the maxillary posterior teeth are lost, the maxillary sinus may expand even more, thinning the bony floor of the alveolar process so that only a thin shell of bone is present. These instances of proximity can cause serious clinical problems such as secondary sinusitis and perforation during infection (see Chapter 12), extraction, or trauma related to the maxillary posterior teeth.
Skull Fossae
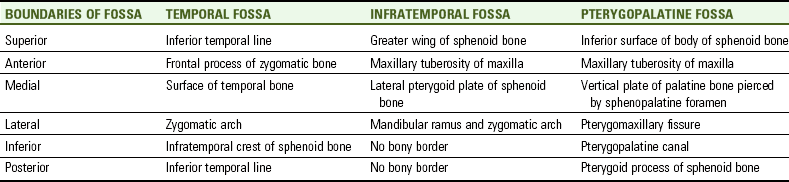
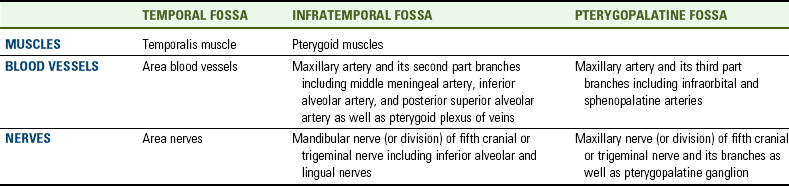
Three depressions or fossae are present on the external surface of the skull: temporal, infratemporal, and pterygopalatine. The bony boundaries for these paired fossae should be located on both the skull model and skull diagrams as well as on peers and patients (Table 3-6). These fossae are important landmarks of the skull for locating muscles, blood vessels, and nerves (Table 3-7).
Temporal Fossa
The temporal fossa is a flat, fan-shaped paired depression on the lateral surface of the skull (Figure 3-59; see Figures 3-12 and 3-13). The temporal fossa is formed by parts of five bones: zygomatic, frontal, greater wing of the sphenoid, temporal, and parietal.
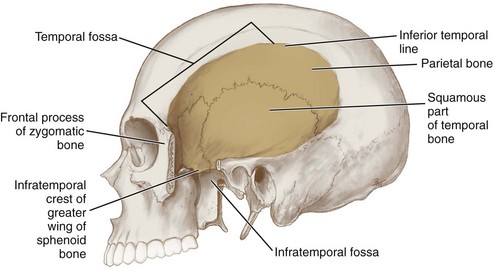
FIGURE 3-59 Lateral view of the skull and the temporal fossa highlighted and its boundaries noted (with parts of zygomatic and temporal bones removed).
The boundaries of the temporal fossa include: superiorly and posteriorly, the inferior temporal line; anteriorly, the frontal process of the zygomatic bone; medially, the surface of the temporal bone; and laterally, the zygomatic arch. Inferiorly, the boundary between the temporal fossa and the infratemporal fossa is the infratemporal crest on the greater wing of the sphenoid bone.
The temporal fossa includes a narrow strip of the parietal bone, the squamous part of the temporal bone, the temporal surface of the frontal bone, and the temporal surface of the greater wing of the sphenoid bone. The temporal fossa contains the body of the temporalis muscle and area blood vessels and nerves (see Figure 4-22).
Infratemporal Fossa
The infratemporal fossa is a paired depression that is inferior to the anterior part of the temporal fossa (see Figure 3-59). The infratemporal crest on the greater wing of the sphenoid bone contributes to the adjoining temporal fossa and infratemporal fossa. The infratemporal fossa can also be viewed from the inferior aspect of the skull model after temporarily removing the mandible (Figure 3-60).
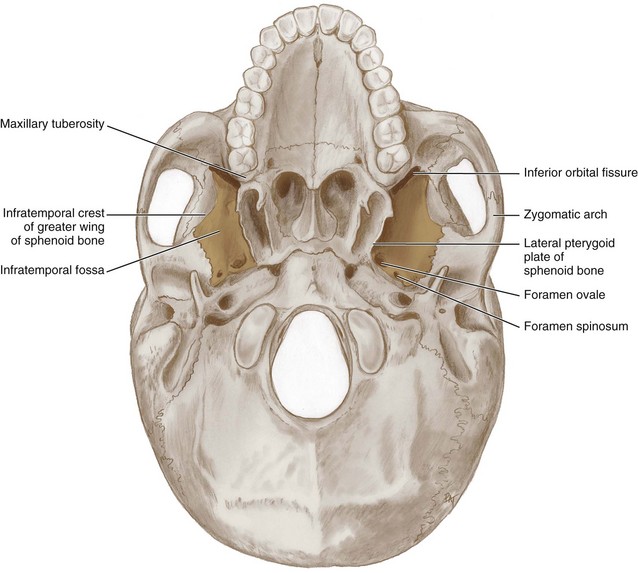
FIGURE 3-60 Inferior view of the skull (with the mandible removed) and the infratemporal fossae highlighted with boundaries and features noted.
The boundaries of the infratemporal fossa include: superiorly, the greater wing of the sphenoid bone; anteriorly, the maxillary tuberosity of the maxilla; medially, the lateral pterygoid plate of the sphenoid bone; and laterally, the ramus of the mandible and zygomatic arch. No bony inferior or posterior boundary exists; so it is bounded by both bone and soft tissue.
Many structures pass from the infratemporal fossa into the orbit through the inferior orbital fissure, which is located at the anterior and superior end of the fossa. Other structures pass into the infratemporal fossa from the cranial cavity (see Figures 9-3 and 9-31).
The infratemporal fossa contains the maxillary artery and its second part branches which arise here, including the middle meningeal artery, which goes into the cranial cavity through the foramen spinosum; the inferior alveolar artery, which enters the mandible through the mandibular foramen; and the posterior alveolar artery, which enters the maxilla through the posterior superior alveolar foramina on the maxillary tuberosity (see Table 3-3). The fossa also contains the pterygoid plexus of veins and the pterygoid muscles (see Figure 6-12).
The infratemporal fossa contains the mandibular nerve (or division) of the fifth cranial or trigeminal nerve (including the inferior alveolar and lingual nerves), which enters by way of the foramen ovale, passing between the cranial and oral cavities (see Table 3-3).
Pterygopalatine Fossa
The pterygopalatine fossa is a cone-shaped paired depression deep to the infratemporal fossa and posterior to the maxilla on each side of the skull (Figure 3-61). This smaller but still important fossa is located between the pterygoid process and the maxillary tuberosity, close to the apex of the orbit. The fossa communicates via fissures and foramina in its walls with the following: the cranial cavity, the infratemporal fossa, the orbit, the nasal cavity, and the oral cavity.
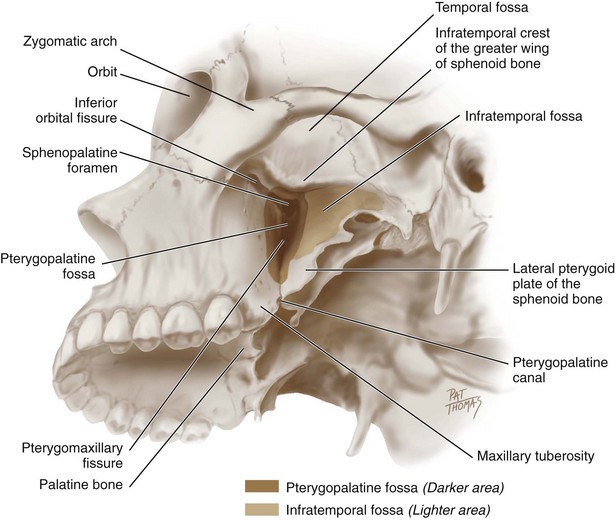
FIGURE 3-61 Oblique lateral view of the base of the skull and the roof of the infratemporal fossa (lighter area) and pterygopalatine fossa (darker area) highlighted with their boundaries and features noted.
The boundaries of the pterygopalatine fossa include: superiorly, the inferior surface of the body of the sphenoid bone; anteriorly, the maxillary tuberosity of the maxilla; medially, the vertical plate of the palatine bone; laterally, the pterygomaxillary fissure; inferiorly, the pterygopalatine canal; and posteriorly, the pterygoid process of the sphenoid bone.
The pterygopalatine fossa contains the maxillary artery and its third part branches which arise here, including the infraorbital and sphenopalatine arteries, and the maxillary nerve (or division) of the fifth cranial or trigeminal nerve and its branches, as well as the pterygopalatine ganglion (see Table 3-3). The foramen rotundum is the entrance route for the maxillary nerve; a second foramen in the pterygoid process, the pterygoid canal, transmits autonomic fibers to the pterygopalatine ganglion. The pterygopalatine canal also connects with the greater and lesser palatine foramina of the palatine bones of the posterior hard palate.
Bones of Neck
The cervical vertebrae (ver-teh-bray) are located in the vertebral column between the skull and the thoracic vertebrae. All seven cervical vertebrae have a central vertebral foramen (ver-teh-brahl) for the spinal cord and associated tissue. In contrast to most other vertebrae, the cervical vertebrae are characterized by the presence of a transverse foramen in the transverse process on each side of the vertebral foramen. The vertebral artery runs through these transverse foramina.
Only the first two cervical vertebrae are described because their anatomy is unusual and they are located near the skull. However, damage to any of the vertebrae can affect dental treatment as the patient may experience a range of problems, from difficulty in movement to paralysis.
First Cervical Vertebra.: The first cervical vertebra or atlas (at-lis) articulates with the skull at the occipital condyles of the occipital bone (Figure 3-62). The atlas has the form of an irregular ring consisting of two lateral masses connected by a short anterior arch and a longer posterior arch (Figure 3-63). This cervical bone lacks a body and a spine.
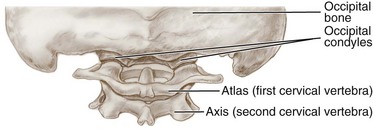
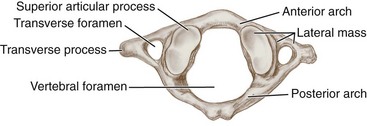
The lateral masses can be effectively palpated by placing fingers between the two mastoid processes and the angles of the mandible. More medially, the lateral masses present large concave superior articular processes for the corresponding occipital condyles of the skull. The lateral masses also have circular inferior articular processes for articulation with the second cervical vertebra.
Second Cervical Vertebra.: The second cervical vertebra or axis (ak-sis) is characterized by the dens (denz) or odontoid process (Figure 3-64). The dens articulates anteriorly with the anterior arch of the first cervical vertebra (Figure 3-65). The body of the axis is inferior to the dens. The spine of the axis is located posterior to the body. The body and the adjoining transverse process present superior articular processes for an additional articulation with the inferior articulating surfaces of the atlas. The inferior aspect of the axis presents inferior articular processes for articulating with the articular processes of the third cervical vertebra.
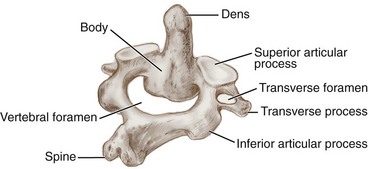
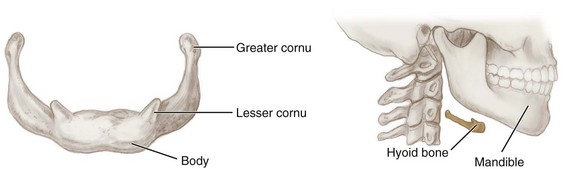
Hyoid Bone
The hyoid bone (hi-oid) is suspended in the neck from the styloid process of the temporal bone by the two stylohyoid ligaments. With its orientation in a horizontal plane, it forms the base of the tongue and larynx. Thus the hyoid bone does not articulate with any other bones, giving it its characteristic mobility, which is necessary for mastication, swallowing, and speech. Instead, many muscles attach to the hyoid bone (see Chapter 4).
The hyoid bone can be effectively palpated inferior to and medial to the angles of the mandible. Do not confuse the hyoid bone with the inferiorly placed thyroid cartilage (the “Adam’s apple”) (see Figure 2-24). The hyoid bone is superior and anterior to the thyroid cartilage of the larynx; it is usually at the level of the third cervical vertebra but raises during swallowing and other activities. It is lowered by the broad thyrohyoid membrane, which connects it to the thyroid cartilage.
The U-shaped hyoid bone consists of five parts as seen from an anterior view (see Figure 3-65 and Figure 3-66). The anterior part is the midline body of the hyoid bone. There is also a pair of projections on each side of the hyoid bone, the greater cornu and lesser cornu. These horns serve as attachments for muscles and ligaments (see Figure 4-24).
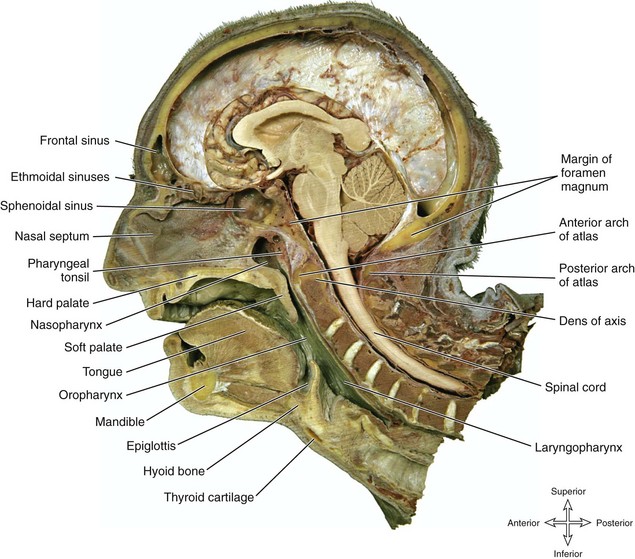
FIGURE 3-66 Dissection showing a sagittal section of the internal skull and associated bony and soft tissue structures (for further identification of section, see Figure 8-4, B). (From Reynolds PA, Abrahams PH: McMinn’s interactive clinical anatomy: head and neck, ed 2, London, 2001, Mosby Ltd.)
Internal Skull from Sagittal View
Now that the external and internal parts of the skull have been viewed, as well as the individual bones of the skull, it is useful to consider also an internal view of the skull on a sagittal section in order to understand the overall placement of bony structures as well as associated soft tissue (see Figure 3-66, for further identification of section, see also Figure 8-4, B).
Skeletal System Pathology
The skeletal system pathology associated with the head and neck can include fractures that may heal with abnormal contours or bony enlargements. Bone can fracture with severe blows to the face. Fractures of the facial skeleton tend to occur at its points of buttress with the cranium. These buttress points include the medial aspect of the orbit, the articulation of the zygomatic bone with both the frontal and temporal bones, the articulation of the pterygoid plates, the palatine bones, and each maxilla.
The fracture of the bone may be detected by gentle palpation during an extraoral examination after radiographic analysis. If the fracture is bilateral, the entire facial skeleton can be pushed posteriorly, resulting in upper respiratory tract obstruction. These fractures may heal poorly and result in abnormal bony contours. The dental professional needs to record any abnormal areas of bone and make any appropriate referrals.
Because many facial bones are shared by two or more soft tissue components of the face, it is important to remember that an abnormality of one facial bone often also involves many soft tissue components. Thus a fracture of the frontal bone may involve both the facial features of the forehead and the eyes.
Bony enlargements can lead to facial asymmetry as well as nodular intraoral areas, if due to traumatic injury or other pathologies (Figures 3-67 and 3-68). Some, such as palatal or mandibular tori, are normal variations, but others can be due to endocrine diseases causing abnormal bone growth. Bone can also enlarge with neoplastic growth of bone or other tissue such as hard dental tissue (enamel), as in the case of an ameloblastoma. Pathology associated with the temporomandibular joint is discussed in Chapter 5.

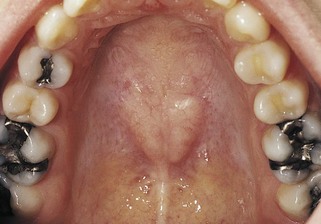
Identification Exercises
Identify the structures on the following diagrams by filling in each blank with the correct anatomic term. You can check your answers by looking back at the figure indicated in parentheses for each identification diagram.
1. (Figure 3-4)
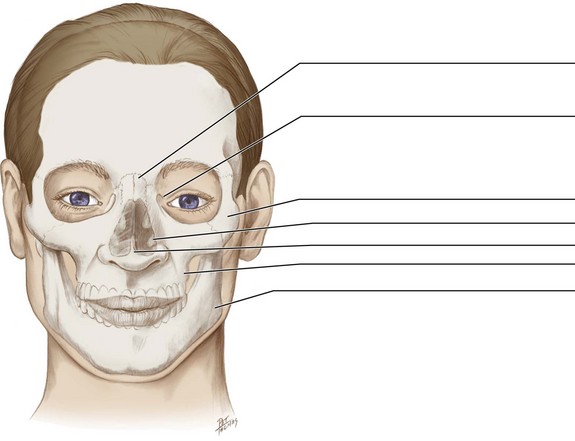
2. (Figures 3-5, 3-6 and 3-7)
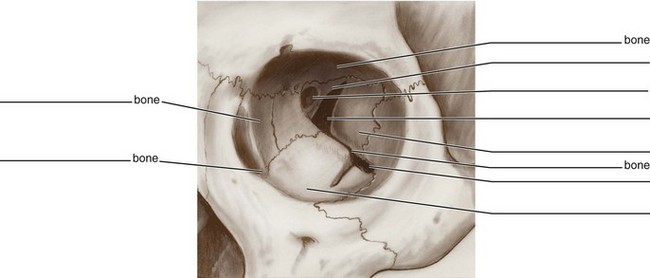
3. (Figures 3-20, 3-23, and 3-27)
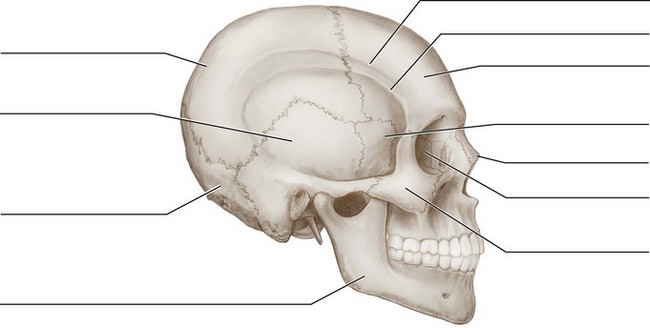
4. (Figure 3-22)
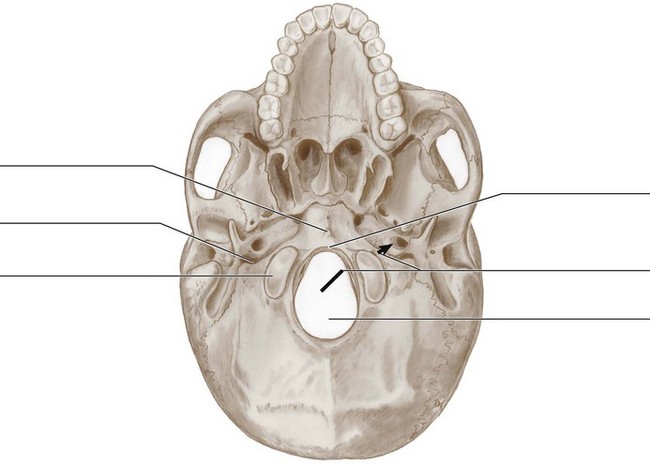
5. (Figures 3-28, 3-29 and 3-30)
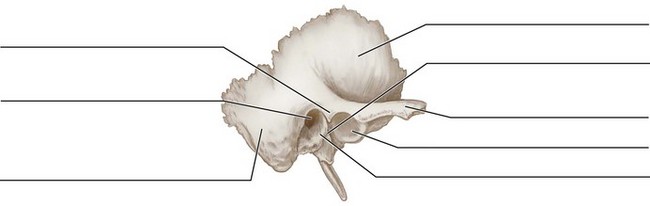
6. (Figures 3-31 and 3-32, A)
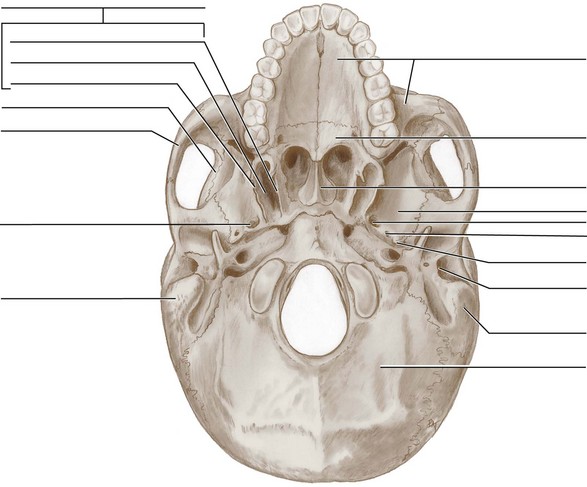
7. (Figure 3-33, A)
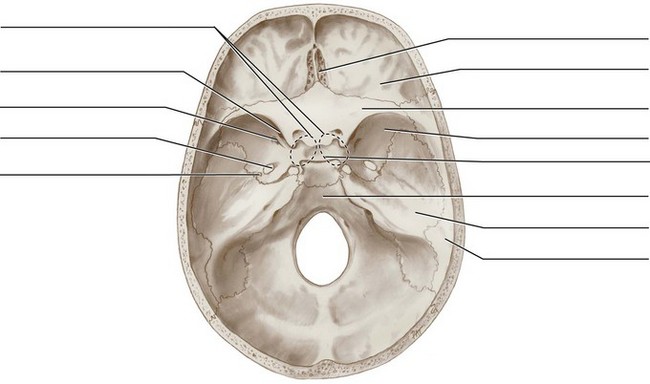
8. (Figure 3-35)
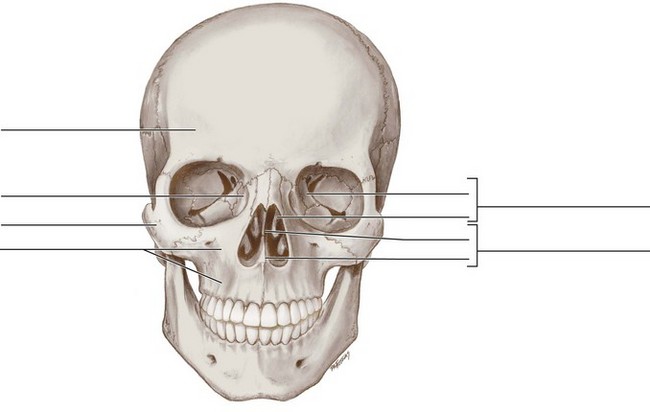
9. (Figure 3-38)
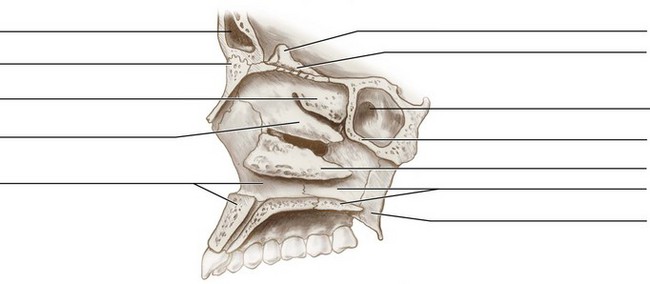
10. (Figures 3-40 and 3-41)
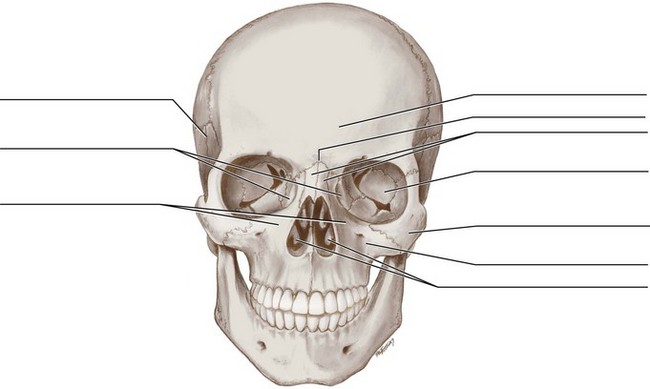
11. (Figure 3-42)
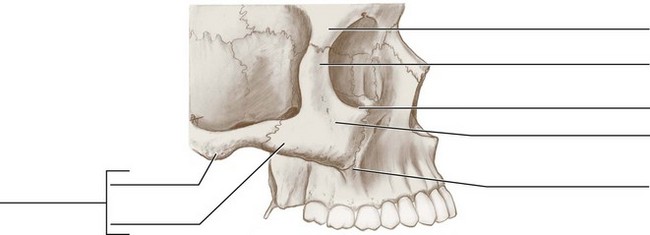
12. (Figure 3-44)
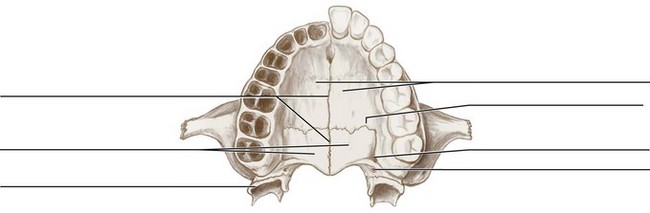
13. (Figure 3-45)
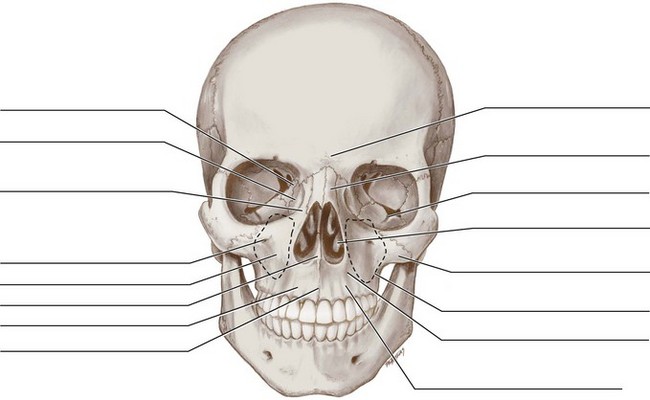
14. (Figure 3-47, A)
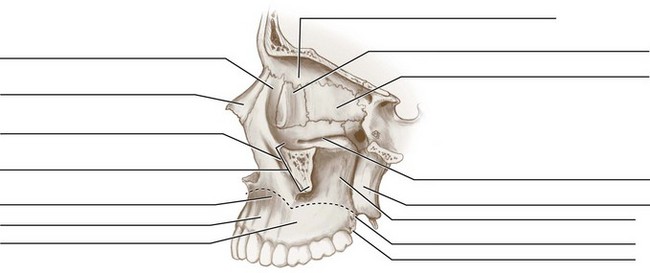
15. (Figures 3-52 and 3-55, B)
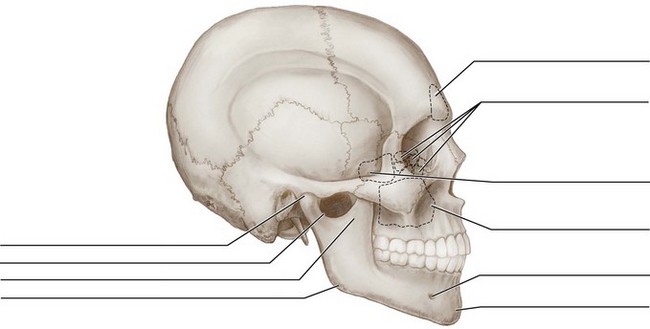
16. (Figure 3-60)
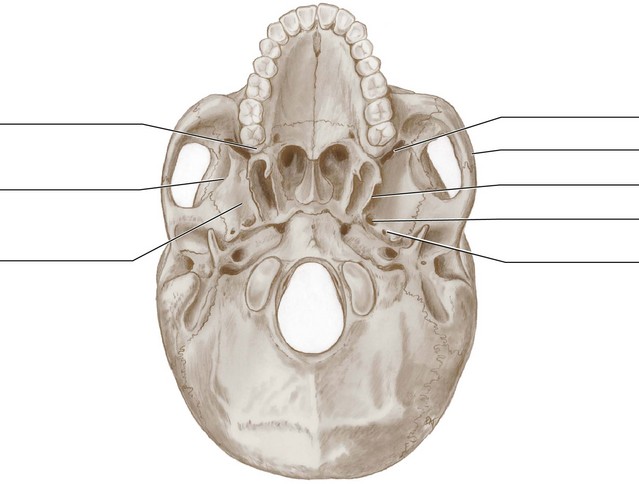
17. (Figure 3-61)
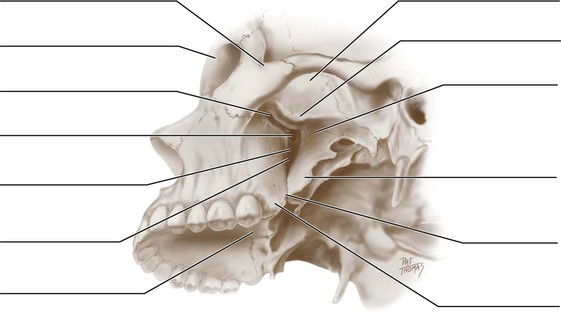
18. (Figure 3-62)
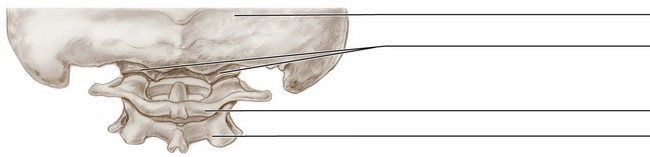
19. (Figure 3-65)
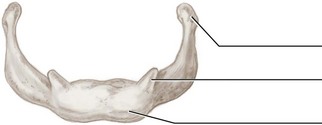
20. (Figure 3-65)
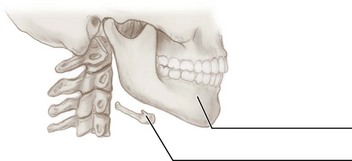
1. Which of the following features is located on the temporal bone?
2. Which area is immediately posterior to the most distal tooth in the upper arch of the dentition?
3. In addition to the zygomatic bone, which of the following bones has a process that forms the other part of the zygomatic arch?
4. Which of the following is the location of the articulation of the parietal bones and the occipital bone?
5. Which of the following bony landmarks form an articulation with each other?
A Occipital condyles with atlas
B Occipital condyles with axis
6. Which of the following features is located on the lateral surface of the mandible?
7. The orbital apex is composed of the lesser wing of the sphenoid bone and the
8. Which of the following landmarks is formed by the maxillae?
9. Which of the following structures is located or travels within the infratemporal fossa?
10. The concavity noted on the anterior border of the coronoid process of the ramus is the
11. Which of the following landmarks serves to locate the hyoid bone?
A Level of the first cervical vertebra
B Superior and anterior to the thyroid cartilage
12. Which of the following structures forms the floor of each maxillary sinus?
13. Which of the following processes is located just inferior and medial to the external acoustic meatus?
14. The spaces under the three conchae of the lateral walls of the nasal cavity are the
15. Which of the following bones and their processes form the hard palate?
A Maxillary processes of the maxillae and horizontal plates of the palatine bones
B Palatal processes of the maxillae and maxillary plates of the palatine bones
C Horizontal plates of the palatine bones and palatine processes of the maxillae
D Maxillary plates of the palatine bones and horizontal processes of the maxillae
16. Which of the following cranial nerves is associated with the stylomastoid foramen?
17. Which of the following bones of the skull is paired?
18. Which of the following bony plates is perforated to allow the passage of the olfactory nerves for the sense of smell?
A Medial plate of sphenoid bone
B Lateral plate of sphenoid bone
19. Which of the following bones of the skull is considered a cranial bone?
20. In which part of the temporal bone is the temporomandibular joint located?
21. Which is a single bone located at the midline of the skull?
22. Which of the following structures is a short, windowlike opening normally found in bone?
23. Which of the following bones forms the jugular foramen along with the jugular notch of the temporal bone?
24. Which of the following is a faint ridge noted where the right and left mandibular processes fused together in early childhood?
25. In which bone are both the infraorbital foramen and canal located?
26. Which of the following structures is a large, roughened projection on the petrous part of the temporal bone?
27. Which of the following landmarks is an anterior process located on the sphenoid bone?
28. The lacrimal gland is located just inside the lateral part of the
29. The occipital condyles are located ________________ and ________________ to the foramen magnum.
30. Which bone forms both the superior and middle nasal conchae?