Muscular System
1 Define and pronounce the key terms and anatomic terms in this chapter.
2 Locate and identify the muscles of the head and neck on a diagram, skull, and patient.
3 Describe the origin, insertion, action, and innervation of each muscle of the head and neck.
4 Discuss the processes of mastication, speech, and swallowing with regard to anatomic considerations involving the muscles.
5 Discuss the pathology associated with the muscles of the head and neck.
6 Correctly complete the review questions and activities for this chapter.
7 Integrate an understanding of the muscles of the head and neck into the clinical dental practice.
Muscular System Overview
The muscular system includes skeletal muscle tissue. A muscle in the muscular system shortens under neural control, causing soft tissue and bony structures of the body to move. Each muscle has two ends attached to these structures, and they are categorized according to their role in movement. The origin is the end of the muscle that is attached to the least movable structure. The insertion is the other end of the muscle and is attached to the more movable structure.
Generally, the insertion of the muscle moves toward the origin where the muscle arises when the muscle is contracted. The movement that is accomplished when the muscle fibers contract is the action of the muscle. The muscles have specific innervation that is discussed in this chapter, but a more thorough explanation of the nervous system can be found in Chapter 8. The blood supply to the muscular area is further discussed in Chapter 6. It is important to remember that unlike innervation to the muscles, which is a one-to-one relationship, arterial supply is regional. Arteries supply all structures in their vicinity, and muscles receive blood from all nearby arteries.
Muscles Of Head And Neck
The dental professional needs to determine the location and action of many skeletal muscles of the head and neck in order to perform a thorough patient examination (see Appendix B). This information is important because the placement of many other structures such as bones, blood vessels, nerves, and lymph nodes is related to the location of these skeletal muscles. These muscles may also malfunction and be involved in temporomandibular joint disorders (see Chapter 5), occlusal dysfunction, and certain nervous system diseases (discussed later). Muscles of the head and neck and their attachments are also a consideration in the spread of dental infections since they define many of the spaces in the face and neck (see Chapters 11 and 12).
The muscles of the head and neck are divided according to function into six main groups: cervical muscles, muscles of facial expression, muscles of mastication, hyoid muscles, muscles of the tongue, and muscles of the pharynx. Muscle groups of the ears, eyes, and nose are not included in this chapter and can be studied from reference materials (see Appendix A).
Cervical Muscles
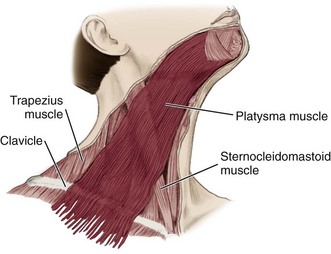
The cervical muscles considered in this chapter are both superficial and easily palpated on the neck. The two cervical muscles include: sternocleidomastoid and trapezius.
Sternocleidomastoid Muscle
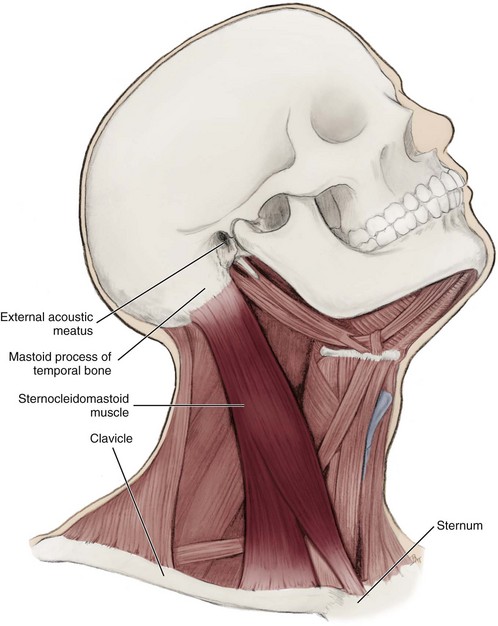
One of the largest and most superficial cervical muscles is the paired sternocleidomastoid muscle (SCM). It is thick and thus serves as a primary muscular landmark of the neck during an extraoral examination of a patient since it divides the neck region into anterior and posterior cervical triangles which helps define the location of structures, such as the lymph nodes for the head and neck (see Figures 2-23, 2-25, 2-26 and see Chapters 2 and 10).
Origin and Insertion.: The SCM originates from the medial part of the clavicle and the sternum’s superior and lateral surfaces and passes posteriorly and superiorly to insert on the mastoid process of the temporal bone (Figure 4-1). This insertion is just posterior and inferior to the external acoustic meatus of each ear.
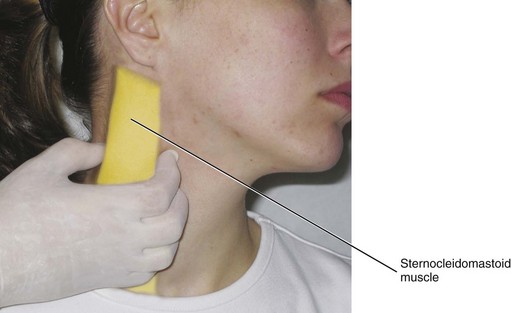
Action.: If one muscle contracts, the head and neck bend to the ipsilateral side, and the face and front of the neck rotate to the contralateral side. If both muscles contract, the head will flex at the neck and extend at the junction between the neck and skull. The SCM is effectively palpated on each side of the neck when the patient moves the head to the contralateral side (Figure 4-2).
Trapezius Muscle
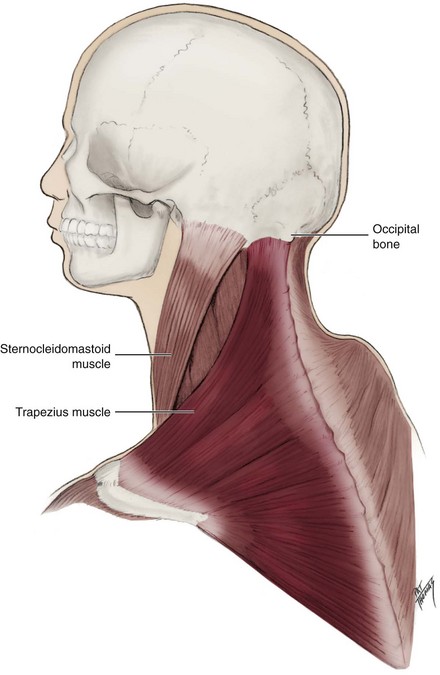
The other important superficial cervical muscle is the paired trapezius muscle (trah-pee-zee-us), which is superficial to both the lateral and posterior surfaces of the neck. It is a broad, flat, triangular muscle.
Origin and Insertion.: The trapezius muscle originates from the external surface of the occipital bone and the posterior midline of the cervical and thoracic regions. It then inserts on the lateral third of the clavicle and parts of the scapula (Figure 4-3).
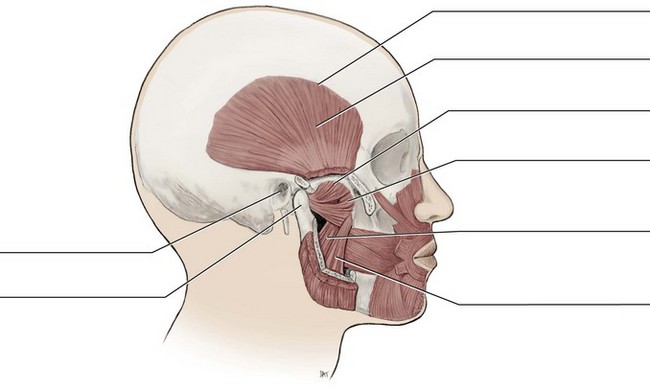
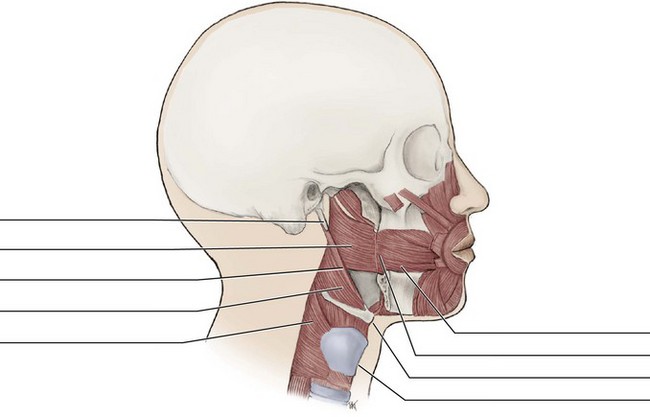
Muscles of Facial Expression
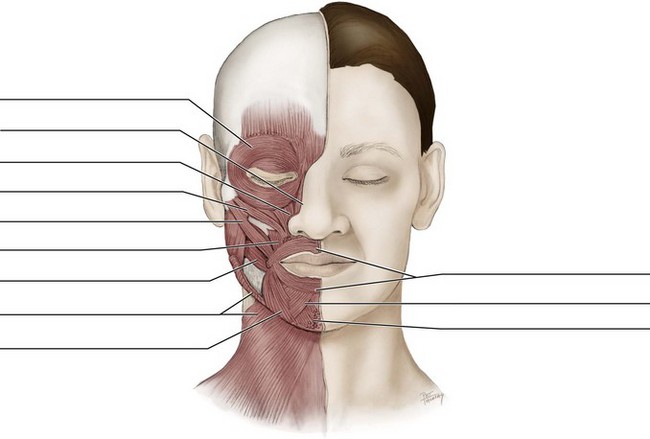
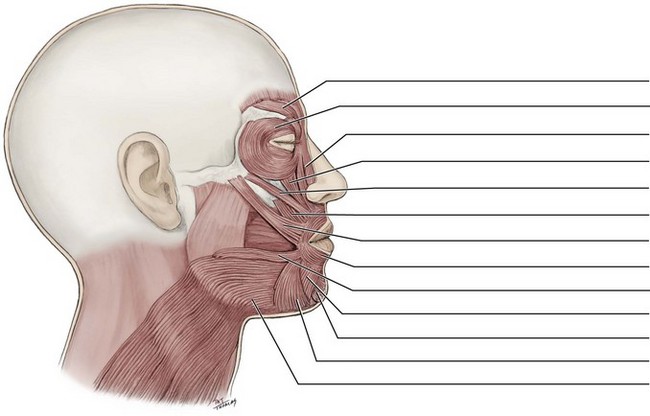
The muscles of facial expression are paired muscles in the superficial fascia of the facial tissue (Figures 4-4 and 4-5). All the muscles of facial expression originate from the surface of the skull bone (rarely the fascia) and insert on the dermis of skin. When they contract, the skin moves. These muscles also cause wrinkles at right angles to the muscles’ action line. Use of these muscles is noted during an extraoral examination, assuring function of the nerve to these muscles. Again, the use of a mirror as you perform various facial expressions is helpful in learning about these muscles. Interestingly, smiling really is easier than frowning, as the saying goes: it takes only a few muscles to smile (17), but many more to frown (43).
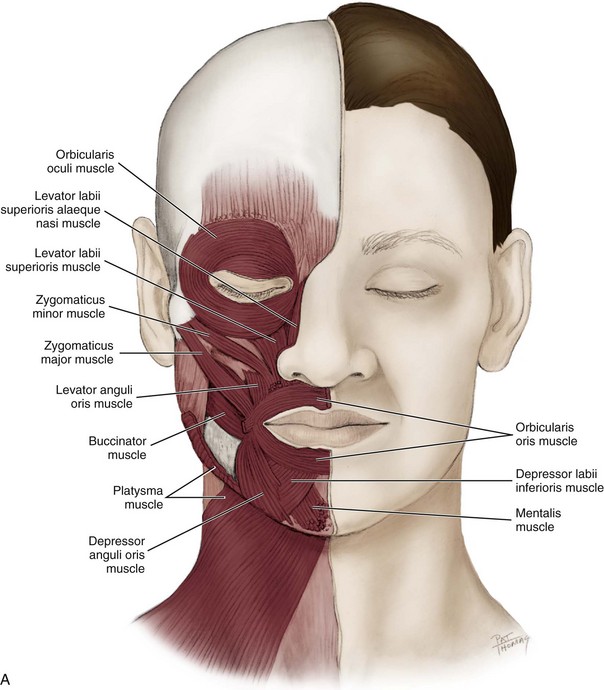
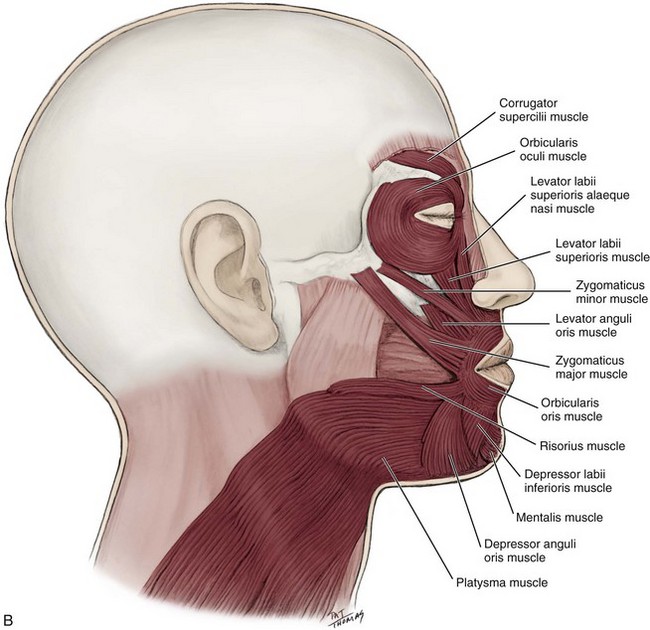
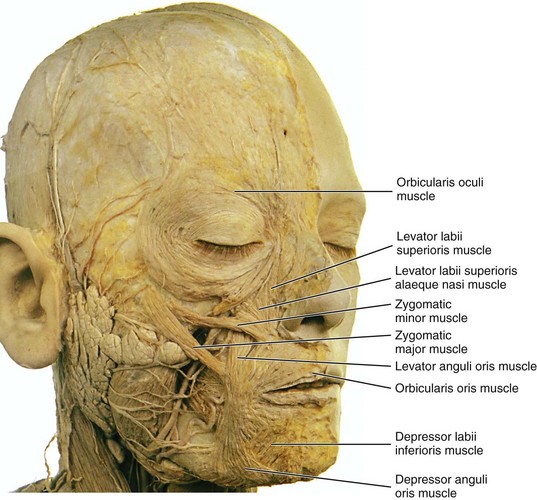
FIGURE 4-5 Superficial dissection of the face showing many of the muscles of facial expression. (From Reynolds PA, Abrahams PH: McMinn’s interactive clinical anatomy: head and neck, ed 2, London, 2001, Mosby Ltd.)
Origin and Insertion.
The locations of the muscles of facial expression vary; however, these muscles may be further grouped according to whether they are situated in the scalp, eye, or oral region (Table 4-1).
TABLE 4-1
| MUSCLE | ORIGIN | INSERTION |
| Epicranial | Frontal belly: epicranial aponeurosis Occipital belly: occipital and temporal bones |
Frontal belly: eyebrow and root of nose Occipital belly: epicranial aponeurosis |
| Orbicularis oculi | Orbital rim, frontal bone and maxilla | Lateral canthus area, some encircle eye |
| Orbicularis oris | Encircles mouth | Labial commissure |
| Buccinator | Maxilla, mandible, and pterygomandibular raphe | Labial commissure |
| Risorius | Fascia superficial to masseter muscle | Labial commissure |
| Levator labii superioris | Maxilla | Upper lip |
| Levator labii superioris alaeque nasi | Maxilla | Ala of nose and upper lip |
| Zygomaticus major | Zygomatic bone | Labial commissure |
| Zygomaticus minor | Zygomatic bone | Upper lip |
| Levator anguli oris | Maxilla | Labial commissure |
| Depressor anguli oris | Mandible | Labial commissure |
| Depressor labii inferioris | Mandible | Lower lip |
| Mentalis | Mandible | Chin |
| Platysma | Clavicle and shoulder | Mandible and muscles of mouth |
Action.
During facial expression, the muscles of the face act in various combinations, similar to the muscles of mastication discussed later (Table 4-2).
TABLE 4-2
Muscles of Facial Expression and Associated Facial Expressions
| MUSCLE | FACIAL EXPRESSION(S) |
| Epicranial | Surprise |
| Orbicularis oculi | Closing eyelid |
| Corrugator supercilii | Frowning |
| Orbicularis oris | Closing and pursing lips, as well as pouting and grimacing |
| Buccinator | Compresses the cheeks during chewing |
| Risorius | Stretching lips |
| Levator labii superioris | Raising upper lip |
| Levator labii superioris alaeque nasi | Raising upper lip and dilating nares in a sneer |
| Zygomaticus major | Smiling |
| Zygomaticus minor | Raising upper lip, assisting in smiling |
| Levator anguli oris | Smiling |
| Depressor anguli oris | Frowning |
| Depressor labii inferioris | Lowering lower lip |
| Mentalis | Raising chin and protruding lower lip |
| Platysma | Raising neck skin and grimacing |
Innervation.
All the muscles of facial expression are innervated by the seventh cranial or facial nerve, with each nerve serving one side of the face (see Figure 8-22).
Muscles of Facial Expression Pathology
An inability to form facial expressions on one side of the face may be the first sign of damage to the nerve of these muscles. Damage to the facial nerve results in facial paralysis of the muscles of facial expression on the involved side (Figure 4-6). Paralysis is the loss of voluntary muscle action; the facial nerve has become damaged permanently or temporarily. This damage can occur with a stroke (cerebrovascular accident), Bell palsy (as in this case), or parotid salivary gland cancer (malignant neoplasm) because the facial nerve travels through the gland (see Figure 8-22). The parotid gland can also be damaged permanently by surgery or temporarily by trauma, as with an incorrectly given inferior alveolar block (see Figure 9-37). These situations of paralysis not only inhibit facial expression but also seriously impair the patient’s ability to speak, either permanently or temporarily.

Muscles Of Facial Expression In Scalp Region
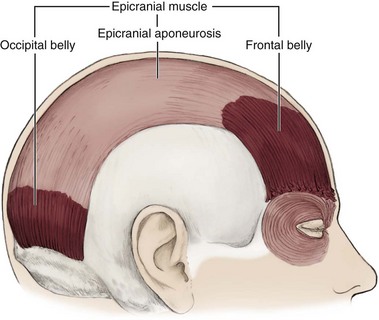
The epicranial muscle (ep-ee-kray-nee-al) or epicranius is a muscle of facial expression in the scalp region. This muscle and its tendon are one of the layers that form the scalp. This muscle has two bellies: frontal and occipital. The bellies are separated by a large, spread-out scalpal tendon, the epicranial aponeurosis (ap-o-new-row-sis) or galea aponeurotica.
Origin and Insertion.: The frontal belly of the epicranial muscle arises from the epicranial aponeurosis (Figure 4-7). The epicranial aponeurosis is at the most superior part of the skull (see Figure 3-21). The frontal belly or frontalis then inserts into the skin of the eyebrow and root of the nose. The occipital belly or occipitalis originates from the occipital bone and mastoid process of the temporal bone and then inserts in the epicranial aponeurosis.
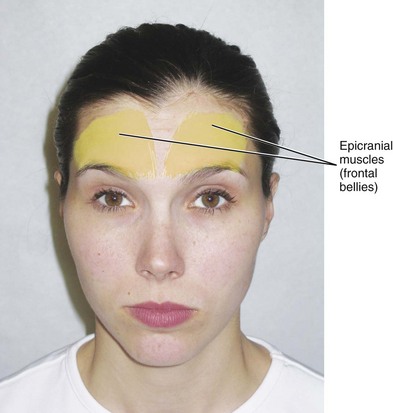
Action.: Both bellies of the epicranial muscle raise the eyebrows and scalp, as when a person shows surprise (Figure 4-8). However, the two bellies can also act independently of each other during certain facial expressions.
Muscles Of Facial Expression In Eye Region
The orbicularis oculi muscle (or-bik-you-laa-ris oc-yule-eye) is a muscle of facial expression that encircles the eye. This muscle has important functions in protecting and moistening the eye, as well as in facial expression. Thus loss of its use can cause damage to the eye(s) since they remain open.
Origin and Insertion.: This muscle originates on the orbital rim, the nasal process of the frontal bone, and the frontal process of the maxilla (Figure 4-9). Most of the fibers insert into the skin at the lateral canthus area, although some inner fibers completely encircle the eye.
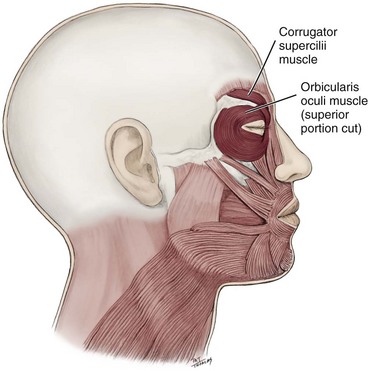
Corrugator Supercilii Muscle.
The corrugator supercilii muscle (cor-rew-gay-tor soo-per-sili-eye) is a muscle of facial expression in the eye region, deep to the superior part of the orbicularis oculi muscle.
Origin and Insertion.: This muscle originates on the frontal bone in the supraorbital region (see Figure 4-9). It then passes superiorly and laterally to insert into the skin of the eyebrow.
Action.: This muscle draws the skin of the eyebrow medially and inferiorly toward the nose, which causes vertical wrinkles in the glabella area of the forehead and horizontal wrinkles at the bridge of the nose, as when a person frowns (see Figure 4-14, B). It works in concert with the muscles of the nasal region.
Muscles Of Facial Expression In Oral Region
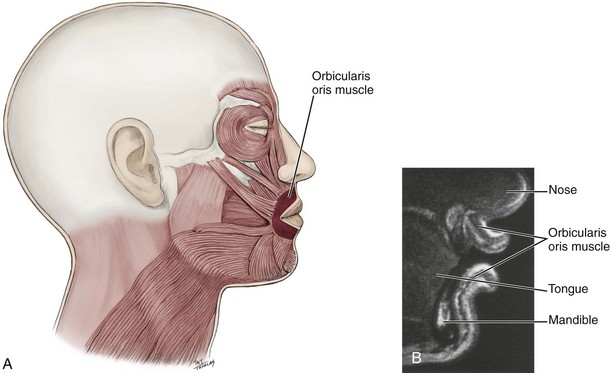
The orbicularis oris muscle (or-bik-you-laa-ris or-is) is an important muscle of facial expression in the oral region since it acts to shape and control the size of the mouth opening and is important for creating the lip positions and movements during speech. This muscle can show increased wrinkling with cigarette use or other prolonged oral habits.
Origin and Insertion.: This muscle encircles the mouth between the skin and labial mucosa of the lips, with no bony attachment. It then inserts in the skin of the lips at the labial commissures (Figure 4-10). In the upper lip, fibers also insert on the ridges of the philtrum.
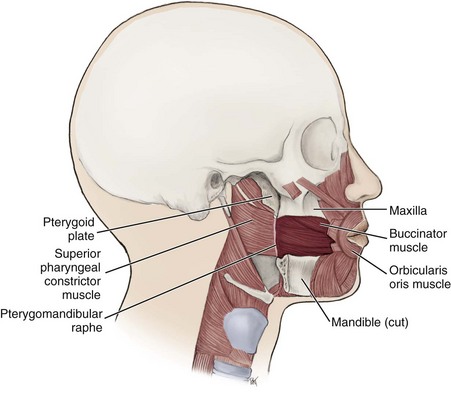
Buccinator Muscle.
The buccinator muscle (buck-sin-nay-tor) is a thin quadrilateral muscle of facial expression that forms the anterior part of the cheek or the lateral wall of the oral cavity.
Origin and Insertion.: This muscle originates from three areas: the alveolar processes of both the maxilla and mandible, as well as a fibrous structure, the pterygomandibular raphe (ter-i-go-man-dib-yule-lar ra-fe) (Figure 4-11). The pterygomandibular raphe extends from the hamulus and passes inferiorly to attach to the posterior end of the mandible’s mylohyoid line; it is noted in the oral cavity as the pterygomandibular fold (see Figure 2-21). The buccinator and superior pharyngeal constrictor muscles of the pharynx (discussed later) are attached to each other at the raphe. Many of the buccinator muscle fibers from the maxillary alveolar process and the superior part of the pterygomandibular raphe travel obliquely downward toward the lower lip, while many of those fibers from the mandibular alveolar process and inferior part of the pterygomandibular raphe travel obliquely upward toward the upper lip, creating an intersecting pattern at the labial commisures.
Action.: This muscle pulls each labial commisssure laterally and shortens the cheek both vertically and horizontally. This action causes the muscle to keep food pushed back on the occlusal surface of the posterior teeth, as when a person chews. By keeping the food in the correct position when chewing, the buccinator assists the muscles of mastication. In infants, the muscle provides suction for nursing. In addition, because of its importance in expelling air through pursed lips, blowpipes, or wind instruments, it has been called the “trumpet muscle.”
Risorius Muscle.
The risorius muscle (ri-soh-ree-us) is a thin muscle of facial expression in the oral region.
Origin and Insertion.: The risorius originates from fascia superficial to the masseter and then passes anteriorly to insert into the skin at the ipsilateral labial commissure (Figure 4-12).
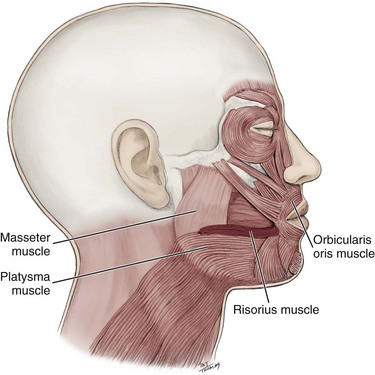
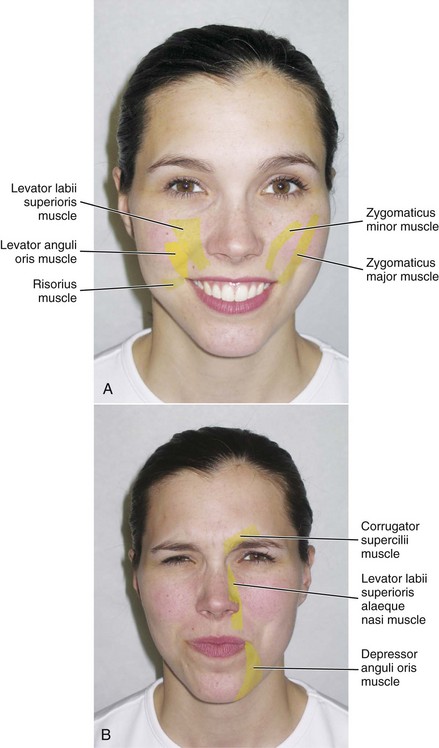
Action.: This muscle acts to stretch the lips laterally, retracting the labial commissure, and widening the mouth (see Figure 4-14, A). The muscle has been thought (erroneously) to produce “grinning” or “smiling” but really produces more of a grimace. The risorius has a connection with the platysma in that it often contracts with it.
Levator Labii Superioris Muscle.
A broad, flat muscle of facial expression in the oral region is the levator labii superioris muscle (le-vate-er lay-be-eye soo-per-ee-or-is) or quadratus labii superioris.
Origin and Insertion.: This muscle originates from the infraorbital rim of the maxilla. It then passes inferiorly to insert into the skin of the upper lip (Figure 4-13).
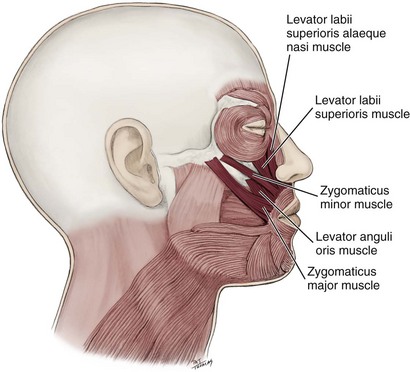
Action.: It elevates the upper lip (Figure 4-14, A).
Levator Labii Superioris Alaeque Nasi Muscle.
The levator labii superioris alaeque nasi muscle (le-vate-er lay-be-eye soo-per-ee-or-is a-lah-cue naz-eye) is a muscle of facial expression in the oral region.
Origin and Insertion.: This muscle originates from the frontal process of the maxilla. It then passes inferiorly to insert into two areas: the skin of the ala of the nose and upper lip (see Figure 4-13).
Action.: This muscle elevates the upper lip and ala of the nose, thus also dilating each nares, as in a sneering expression (Figure 4-14, B).
Zygomaticus Major Muscle.
A muscle of facial expression in the oral region is the zygomaticus major muscle (zy-go-mat-i-kus), lateral to the zygomaticus minor muscle.
Origin and Insertion.: This muscle originates from the zygomatic bone, lateral to the zygomaticus minor. It then passes anteriorly and inferiorly to insert into the skin at the ipsilateral labial commissure, in and around the obicularis oris (see Figure 4-13).
Action.: This muscle elevates the labial commissure of the upper lip and pulls it laterally, as when a person smiles (see Figure 4-14, A). Some research suggests that the difference between a genuine smile and a perfunctory (or faux) smile is that when a person truly feels happy, the zygomatic major muscle contracts together with the orbicularis oculi.
Zygomaticus Minor Muscle.
The zygomaticus minor muscle is a small muscle of facial expression in the oral region, medial to the zygomaticus major muscle.
Origin and Insertion.: This muscle originates on the body of the zygomatic bone. It then inserts in the skin of the upper lip adjacent to the insertion of the levator labii superioris (see Figure 4-13).
Action.: It elevates the upper lip, assisting in smiling (see Figure 4-14, A).
Levator Anguli Oris Muscle.
Deep to both the zygomaticus major and zygomaticus minor muscles of facial expression in the oral region is the levator anguli oris muscle (le-vate-er an-gu-lie) or caninusa.
Origin and Insertion.: This muscle originates in the canine fossa of the maxilla, usually superior to the root of the maxillary canine (see Figure 3-47). It then passes inferiorly to insert into the skin at the ipsilateral labial commissure, intermingling with those of the zygomaticus major, depressor anguli oris, and orbicularis oris (see Figure 4-13).
Action.: It elevates the labial commissure, as when a person smiles (see Figure 4-14, A).
Depressor Anguli Oris Muscle.
The depressor anguli oris muscle (de-pres-er an-gu-lie) or triangularis is a triangular muscle of facial expression in the oral region.
Origin and Insertion.: This muscle originates on the inferior border of the mandible and then passes superiorly to insert into the skin at the ipsilateral labial commissure (Figure 4-15).
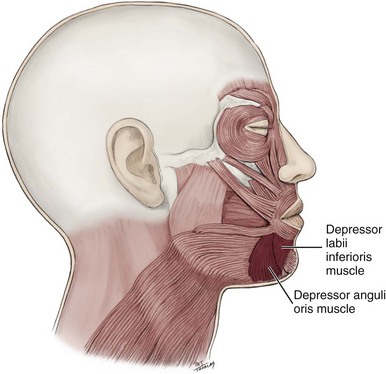
Action.: It depresses the labial commissure, as when a person frowns (see Figure 4-14, B).
Depressor Labii Inferioris Muscle.
Deep to the depressor anguli oris muscle is the depressor labii inferioris muscle (de-pres-er lay-be-eye in-fere-ee-o-ris) or quadratus labii inferioris, a small quadrilateral muscle of facial expression in the oral region.
Origin and Insertion.: This muscle originates from the inferior border of the mandible and passes superiorly to then insert into the skin of the lower lip (see Figure 4-15).
Mentalis Muscle.
The mentalis muscle (men-ta-lis) or levator menti is a short, thick muscle of facial expression superior and medial to the mental nerve in the oral region.
Origin and Insertion.: This muscle originates on the mandible near the midline and then inserts in the skin of the chin (Figure 4-16).
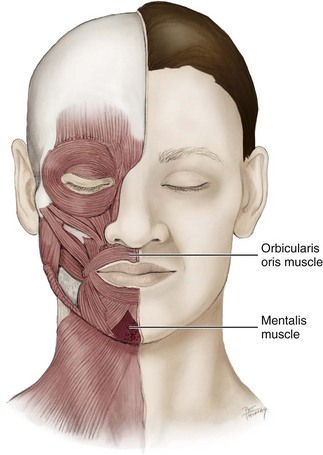
Action.: It raises the chin, wrinkling the skin, causing the displaced lower lip to protrude, narrowing the oral vestibule. Thus when active, these fibers may dislodge a complete denture in an edentulous patient who has lost alveolar ridge height. The mentalis is so named because its actions are associated with thinking or concentration; however, it also has been said to express doubt.
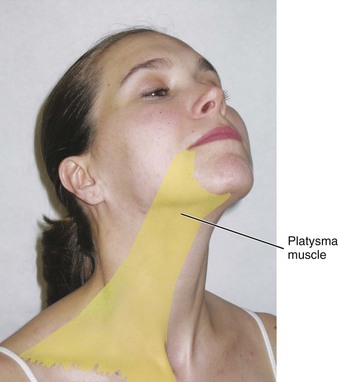
Platysma Muscle.
The platysma muscle (plah-tiz-mah) is a muscle of facial expression that runs from the neck all the way to the mouth, superficial to the anterior cervical triangle (see Figure 2-23).
Origin and Insertion.: This muscle originates in the skin superficial to the clavicle and shoulder. It then passes anteriorly to insert on the inferior border of the mandible and the muscles surrounding the mouth (see earlier discussion and Figure 4-17).
Action.: This muscle raises the skin of the neck to form noticeable vertical and horizontal ridges and depressions. It can also pull the labial commissures down, as when a person grimaces (Figure 4-18).
Muscles of Mastication
The muscles of mastication (mass-ti-kay-shun) are four pairs of muscles attached to the mandible: the masseter, temporalis, medial pterygoid, and lateral pterygoid muscles. These muscles of mastication work with the temporomandibular joint to accomplish movements of the mandible (see Figure 5-6). These muscles may also be involved in pathology associated with the temporomandibular joint (see Chapter 5).
Origin and Insertion.
The origin and insertion of each muscle of mastication varies (Table 4-3).
TABLE 4-3
| MUSCLE | ORIGIN | INSERTION |
| Masseter | Superficial head: zygomatic process of maxilla and anterior two thirds of inferior border of zygomatic arch Deep head: posterior one third and medial surface of zygomatic arch |
Superficial head: angle of mandible Deep head: ramus of mandible |
| Temporalis | Temporal fossa on temporal bone | Coronoid process and ramus of mandible |
| Medial pterygoid | Deep head: lateral pterygoid plate of sphenoid bone Superficial head: pyramidal process of palatine bone and maxillary tuberosity of maxilla |
Both heads: medial surface of ramus and angle of mandible |
| Lateral pterygoid | Superior head: greater wing of sphenoid bone Inferior head: lateral pterygoid plate of sphenoid bone |
Superior head: pterygoid fovea of mandible Inferior head: Temporomandibular joint disc and capsule |
Action.
The muscles of mastication are responsible for closing the jaws, moving the lower jaw forward or backward, and shifting the lower jaw to one side. These jaw movements involve the movement of the mandible, while the rest of the skull remains relatively stable. The dental professional needs to understand the association of the muscles of mastication with the movements of the mandible: depression, elevation, protrusion, retraction, and lateral deviation (Table 4-4).
TABLE 4-4
Muscles of Mastication and Associated Mandibular Movements
| MUSCLE | MANDIBULAR MOVEMENT(S) |
| Masseter | Elevation of mandible (during jaw closing) |
| Temporalis | Elevation of mandible (during jaw closing) Retraction of mandible (lower jaw backward) |
| Medial pterygoid | Elevation of mandible (during jaw closing) |
| Lateral pterygoid | Inferior heads: slight depression of mandible (during jaw opening) One muscle: lateral deviation of mandible (shift lower jaw to contralateral side) Both muscles: mainly protrusion of mandible (lower jaw forward), slight depression of mandible (during jaw opening) |
Masseter Muscle
The most obvious muscle of mastication is the masseter muscle since it is the most superficial and one of the strongest (see Figure 2-9). The muscle is a broad, thick, flat rectangular muscle (almost quadrilateral) on each side of the face, anterior to the parotid salivary gland. This muscle has two heads that differ in depth: superficial and deep.
Origin and Insertion.
Both heads originate from the zygomatic arch but from differing areas (Figure 4-19). The superficial head originates from the zygomatic process of the maxilla, and from the anterior two thirds of the inferior border of the zygomatic arch. The deep head originates from the posterior one third and the entire medial surface of the zygomatic arch. The deep part is partly concealed by the superficial part.
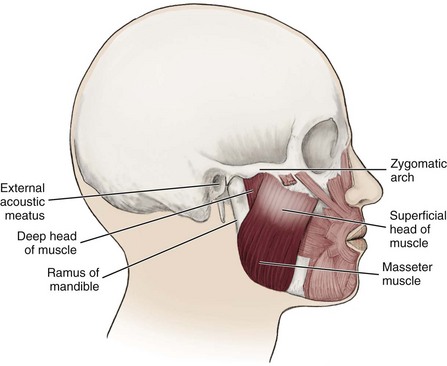
Both these heads then pass inferiorly to insert on different parts of the external surface of the mandible: the superficial head on the lateral surface of the angle, and the deep head on the ramus superior to the angle.
Action.
The action of the muscle during bilateral contraction of the entire muscle is to elevate the mandible, raising the lower jaw. Elevation of the mandible occurs during the closing of the jaws. The masseter parallels the medial pterygoid, but it is stronger. During an extraoral examination, stand near the patient and visually inspect and bilaterally palpate the muscle. Place the fingers of each hand over the muscle and ask the patient to clench his or her teeth several times (Figure 4-20).

FIGURE 4-20 Palpation of the masseter muscle when the patient clenches his or her teeth during an extraoral examination.
Masseter Muscle Pathology
This muscle can become enlarged in patients who habitually clench or grind (with bruxism) their teeth and even in those who constantly chew gum. This masseteric hypertrophy is asymptomatic and soft; it is usually bilateral but can be unilateral. Even if the hypertrophy is bilateral, there still may be asymmetry of the face due to unequal enlargement of the muscles (Figure 4-21).

This extraoral enlargement may be confused with parotid salivary gland disease, dental infections, and maxillofacial neoplasms. However, no other signs are present except those involved in changes in occlusion intraorally such as pain, and the enlargement corresponds with the outline of the muscle. Most patients seek medical attention because of comments about facial appearance and this situation may be associated with further pathology of the temporomandibular joint (see Chapter 5).
Temporalis Muscle.
The temporalis muscle (tem-poh-ral-is) is a broad, fan-shaped muscle of mastication on each side of the head that fills the temporal fossa, superior to the zygomatic arch (see Figure 3-59).
Origin and Insertion.: This muscle originates from the entire temporal fossa on the temporal bone that is bound superiorly by the inferior temporal line and inferiorly by the infratemporal crest. It then passes inferiorly to insert onto the medial surface, apex, and anterior border of the coronoid process of the mandible at the anteriomedial border of the ramus (Figure 4-22).
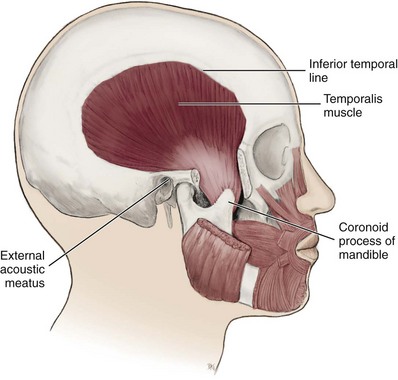
Action.: If the entire muscle contracts, the main action is to elevate the mandible, raising the lower jaw. Elevation of the mandible occurs during the closing of the jaws. If only the posterior part contracts, the muscle moves the lower jaw backward. Moving the lower jaw backward causes retraction of the mandible. Retraction of the jaw often accompanies the closing of the jaws.
Medial Pterygoid Muscle.
Deeper, yet similar in form to the more superficial masseter (rectangular, but more quadrilateral, in this case), is another muscle of mastication, the medial pterygoid muscle (ter-i-goid) or internal pterygoid muscle. This muscle also has two heads due to their differing depth: deep and superficial, similar to the masseter.
Origin and Insertion.: The larger deep head originates from the pterygoid fossa on the medial surface of the lateral pterygoid plate of the sphenoid bone. The smaller superficial head originates from the lateral surfaces of the pyramidal process of the palatine bone and maxillary tuberosity of the maxilla (see Figure 3-32). Both heads then pass inferiorly, posteriorly, and laterally to insert on the medial surface of the ramus and angle of the mandible, as far superior as the mandibular foramen (Figure 4-23).
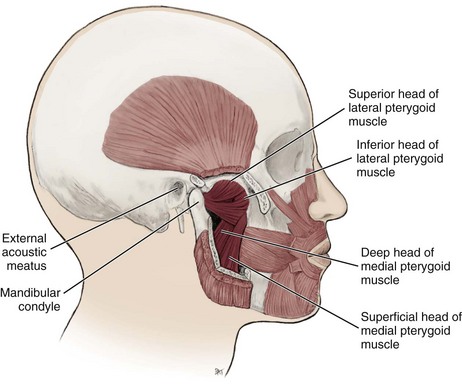
Lateral Pterygoid Muscle.
The lateral pterygoid muscle or external pterygoid muscle is a short, thick, almost conical muscle of mastication superior to the medial pterygoid. This muscle has two separate heads of origin: superior and inferior. The two heads are separated anteriorly by a slight interval but fuse together posteriorly. The entire muscle lies within the infratemporal fossa, deep to the temporalis muscle (see Figure 3-60).
Origin and Insertion.: The superior head originates from the infratemporal surface and infratemporal crest of the greater wing of the sphenoid bone and passes inferiorly to insert on the anterior margin of the temporomandibular joint disc and capsule (see Figures 4-23 and 3-52). The inferior head originates from the lateral surface of the lateral pterygoid plate of the sphenoid bone and inserts on the anterior surface of the neck of the mandible at the pterygoid fovea.
Action.: Unlike the other three muscles of mastication, the lateral pterygoid is the only muscle of mastication that assists in depressing the mandible, lowering the lower jaw. Depression of the mandible occurs during the opening of the jaws. However, the main action when both muscles contract is to bring the lower jaw forward, thus causing the protrusion of the mandible. Protrusion of the mandible often occurs during opening of the jaws. If only one muscle is contracted, the lower jaw shifts to the contralateral side, causing lateral deviation of the mandible.
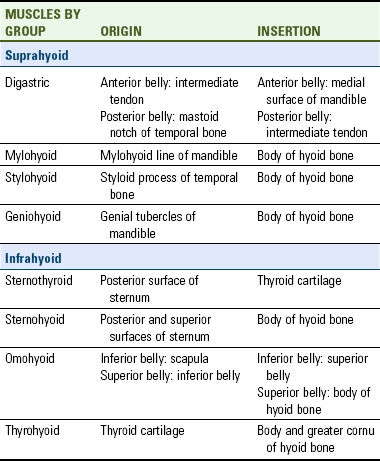
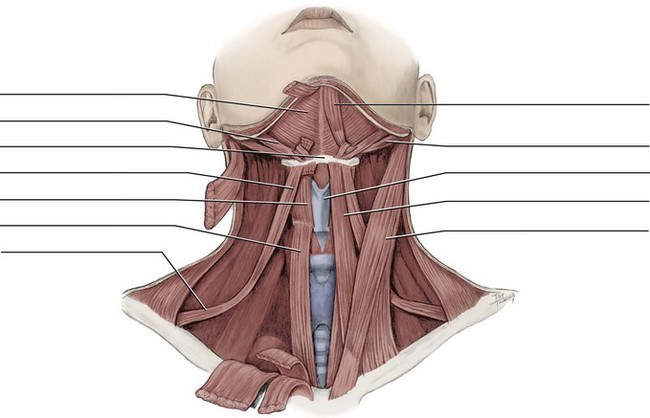
Hyoid Muscles
The hyoid muscles (hi-oid) assist in the actions of mastication and swallowing through their attachment to the hyoid bone. The hyoid bone is a horseshoe-shaped bone suspended inferior to the mandible; it does not articulate with any other bone and has only muscular and ligamentary attachments (see Figure 3-65). The muscles can be further grouped based on their vertical position in relationship to the hyoid bone: suprahyoid or infrahyoid (Box 4-1).
Origin and Insertion.
Most of these muscles are in a superficial position in the neck tissue. Both groups of the hyoid muscles are attached to the hyoid bone (Figure 4-24). The specific origin and insertion of each muscle are discussed in Table 4-5.
Suprahyoid Muscles
The suprahyoid muscles (soo-prah-hi-oid) are superior to the hyoid bone as well as its inferior hyoid muscles (Figures 4-25 and 4-26; see Figure 4-24). These superior muscles may be further divided according to their horizontal position in relationship to the hyoid bone: anterior or posterior. The anterior suprahyoid muscle group includes: the anterior belly of the digastric, the mylohyoid, and the geniohyoid. The posterior suprahyoid muscle group includes: the posterior belly of the digastric and stylohyoid.
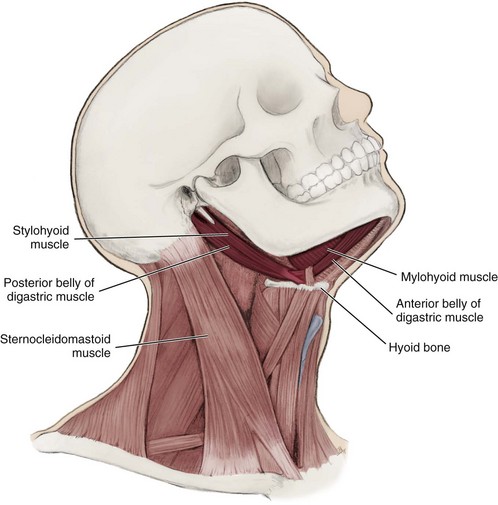
FIGURE 4-25 Lateral view of the hyoid bone with the suprahyoid muscles highlighted (except the geniohyoid muscle).
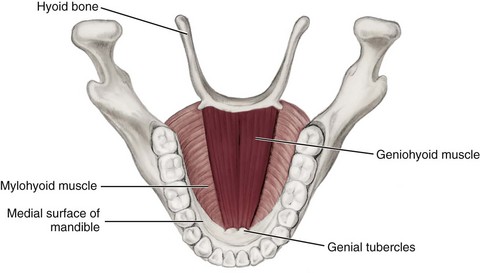
FIGURE 4-26 Superior view of the floor of the oral cavity showing the origin and insertion of the highlighted geniohyoid muscle.
Action.
Two actions associated with mastication result from muscle contraction. One action of both the anterior and posterior suprahyoid muscles is to cause the elevation of the hyoid bone and larynx if the mandible is stabilized by contraction of the muscles of mastication. This action occurs during swallowing.
The other action associated with mastication results from the contraction of the anterior suprahyoid muscles, which causes the mandible to depress and the jaws to open. Thus normal jaw opening involves the lateral pterygoid muscles, which protrude the mandible, and the anterior suprahyoid muscles, which lower the mandible. Some of the suprahyoid muscles have additional specific actions that are also discussed.
Digastric Muscle.
The digastric muscle (di-gas-trik) is a suprahyoid muscle that has two separate bellies: anterior and posterior (see Figure 4-25). The anterior belly is a part of the anterior suprahyoid muscle group, and the posterior belly is a part of the posterior suprahyoid muscle group. Each digastric muscle demarcates the superior part of the anterior cervical triangle, forming (with the mandible) a submandibular triangle on each side of the neck; the right and left anterior bellies of the muscle also form a midline submental triangle (see Figure 2-25).
Origin and Insertion.: The anterior belly originates on the intermediate tendon, which is loosely attached to the body and the greater cornu of the hyoid bone, and then passes superiorly and anteriorly to insert close to the symphysis on the medial surface of the mandible. The posterior belly arises from the mastoid notch, medial to the mastoid process of the temporal bone, and then passes anteriorly and inferiorly to insert on the intermediate tendon.
Mylohyoid Muscle.
The mylohyoid muscle (my-lo-hi-oid) is an anterior suprahyoid muscle deep to the digastric muscle with fibers running transversely between the rami of the mandible (see Figure 4-25).
Origin and Insertion.: This muscle originates from the mylohyoid line on the medial surface of the mandible (see Figure 3-54). The right and left muscles then pass inferiorly to unite medially, forming the floor of the mouth. The most posterior fibers of the muscle then insert on the body of the hyoid bone.
Stylohyoid Muscle.
The stylohyoid muscle (sty-lo-hi-oid) is a thin posterior suprahyoid muscle that has two slips, superficial and deep, on either side of the intermediate tendon of the digastric muscle (see Figure 4-25).
Geniohyoid Muscle.
The geniohyoid muscle (ji-nee-o-hi-oid) is an anterior suprahyoid muscle superior to the medial border of the mylohyoid (see Figure 4-26).
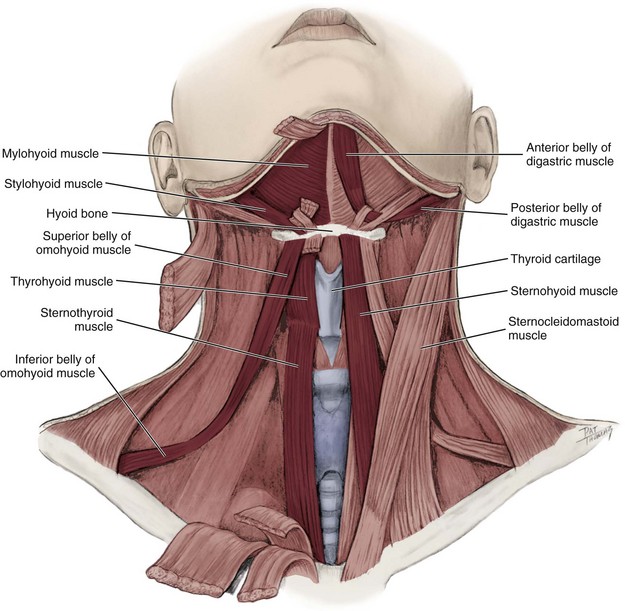
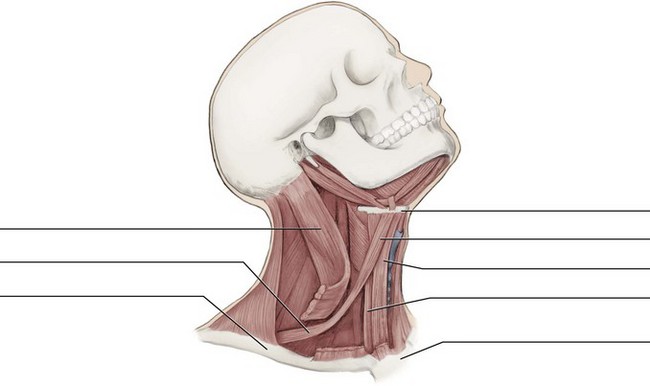
Infrahyoid Muscles
The infrahyoid muscles (in-frah-hi-oid) are four pairs of hyoid muscles inferior to the hyoid bone (Figure 4-27; see Figure 4-24). The infrahyoid muscles include the sternohyoid, sternothyroid, thyrohyoid, and omohyoid muscles.
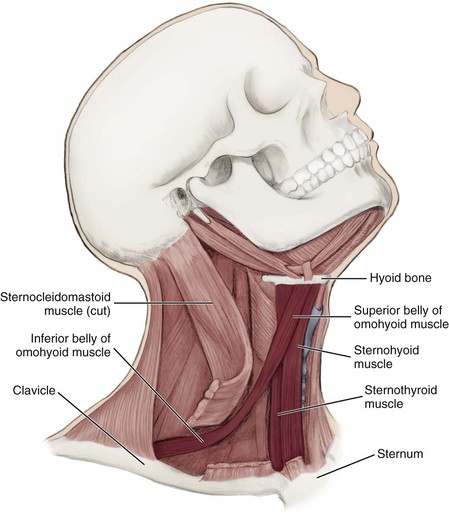
FIGURE 4-27 Lateral view of the hyoid bone and the highlighted infrahyoid muscles (see Figure 4-24 for thyrohyoid muscle).
Action.
Most of the infrahyoid muscles depress the hyoid bone; some have additional specific actions that are also discussed.
Sternothyroid Muscle.
The sternothyroid muscle (ster-no-thy-roid) is an infrahyoid muscle superficial to the thyroid gland.
Sternohyoid Muscle.
The sternohyoid muscle (ster-no-hi-oid) is an infrahyoid muscle superficial to the sternothyroid as well as the thyroid cartilage and thyroid gland.
Omohyoid Muscle.
The omohyoid muscle (o-mo-hi-oid) is an infrahyoid muscle lateral to both the sternothyroid and thyrohyoid muscles. This muscle has two separate bellies: superior and inferior. The superior belly divides the inferior part of the anterior cervical triangle into the carotid and muscular triangles. In the posterior cervical triangle, the inferior belly serves to demarcate the subclavian triangle inferiorly from the occipital triangle superiorly (see Figures 2-25 and 2-26).
Origin and Insertion.: The inferior belly originates from the scapula. The inferior belly then passes anteriorly and superiorly, crossing the internal jugular vein deep to the SCM, where it then attaches by a short tendon to the superior belly. The superior belly originates from the short tendon attached to the inferior belly and then inserts on the lateral border of the body of the hyoid bone.
Thyrohyoid Muscle.
The thyrohyoid muscle (thy-ro-hi-oid) is deep to the omohyoid and sternohyoid.
Origin and Insertion.: The thyrohyoid originates on the thyroid cartilage and inserts on the body and greater cornu of the hyoid bone; it appears as a continuation of the sternothyroid (see Figure 4-24).
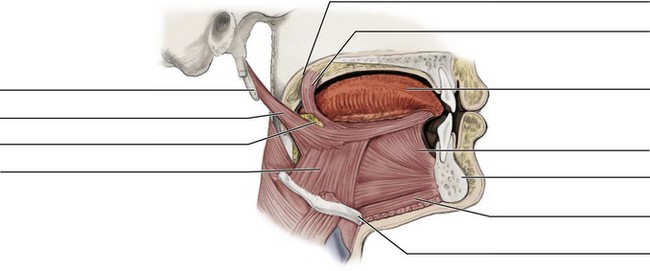
Muscles of Tongue
The tongue is a thick vascular mass of voluntary muscle surrounded by a mucous membrane that is anchored to the floor of the mouth by the lingual frenum. The tongue has complex movements during mastication, speaking, and swallowing; these movements are a result of the combined action of muscles of the tongue. The tongue consists of symmetric halves divided from each other by the median septum (sep-tum), a deep fibrous structure in the midline. The median septum corresponds with the median lingual sulcus, a midline depression on the tongue’s dorsal surface (see Figure 2-17). The tongue is further divided into the base, the body, the dorsal/lateral/ventral surfaces, and the apex.
The muscles of the tongue can be grouped according to their location: intrinsic and extrinsic, with the intrinsic and extrinsic tongue muscles intertwining (Figure 4-28). Each half of the tongue has muscular groups within these two main groups, separated by the median septum.
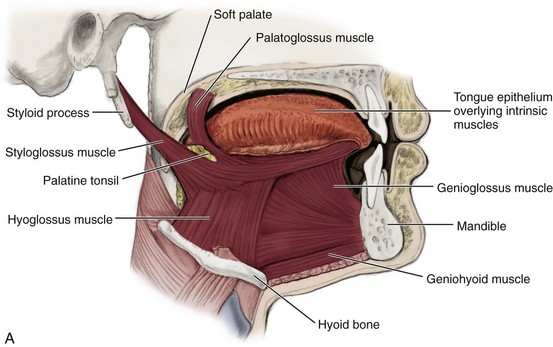
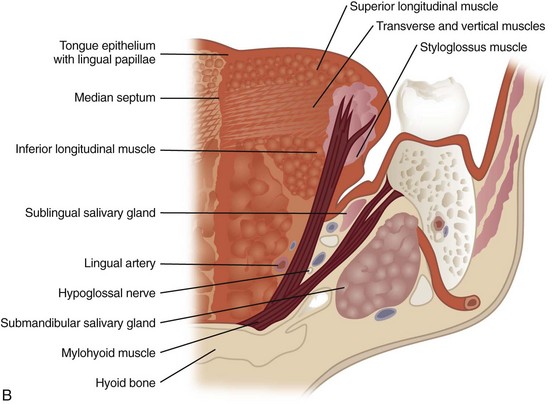
FIGURE 4-28 Tongue with its intrinsic and extrinsic muscles highlighted: A, sagittal section; B, coronal section from a posterior view (note the palatoglossus muscle is not strictly considered an extrinsic muscle but a muscle of the soft palate that is easily viewed within this section).
Origin and Insertion.
Intrinsic muscles are located inside the tongue. Extrinsic muscles have their origin outside the tongue yet have their insertion inside the tongue.
Action.
The intrinsic muscles change the shape of the tongue. The muscles also move the tongue while suspending and anchoring the tongue to bony structures: the mandible, the styloid process, and the hyoid bone. Extrinsic tongue muscles have a more complex involvement. The extrinsic muscles also move the tongue while suspending and anchoring the tongue to bony structures: the mandible, the styloid process, and the hyoid bone. Extrinsic tongue muscles have a more complex involvement (discussed later)
Intrinsic Tongue Muscles
The four pairs of intrinsic tongue muscles (in-trin-sik) are located entirely inside the tongue (see Figure 4-28). These muscles are named by their orientation: superior longitudinal, transverse, vertical, and inferior longitudinal.
Origin and Insertion.
The superior longitudinal muscle is the most superficial of the intrinsic muscles and runs in an oblique and longitudinal direction in the dorsal surface from the base to the apex. Deep to the superior longitudinal muscle is the transverse muscle, which runs in a transverse direction from the median septum to pass outward toward the lateral surface. The vertical muscle runs in a vertical direction from the dorsal surface to the ventral surface in the body. The inferior longitudinal muscle is in the ventral surface of the tongue and runs in a longitudinal direction from the base to the apex.
Extrinsic Tongue Muscles
The three pairs of extrinsic tongue muscles (eks-trin-sik) have different origins outside the tongue but all their insertions are inside the tongue (Table 4-6; see Figure 4-28). These muscles have names ending in “glossus,” the Greek word for tongue, and include: styloglossus, genioglossus, and hyoglossus with each name indicating its location. Some anatomists also include the palatoglossus muscle in this category because it is involved in tongue movement; however, it is discussed with the muscles of the soft palate in this chapter.
TABLE 4-6
Extrinsic Tongue Muscles*
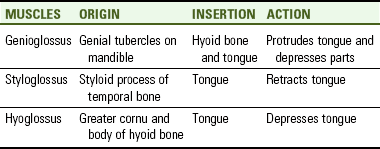
*The palatoglossus muscle is noted under the muscles of the soft palate.
Innervation.
All the extrinsic tongue muscles are innervated by the twelfth cranial or hypoglossal nerve.
Styloglossus Muscle.
The styloglossus muscle (sty-lo-gloss-us) is an extrinsic tongue muscle.
Genioglossus Muscle.
The genioglossus muscle (ji-nee-o-gloss-us) is a fan-shaped extrinsic tongue muscle superior to the geniohyoid.
Origin and Insertion.: It arises from the genial tubercles on the medial surface of the mandible. A few of the most inferior fibers insert on the hyoid bone, but most of the fibers insert into the tongue from its base almost to the apex. The right and left muscles are separated by the tongue’s median septum.
Action.: Different parts of the muscle can protrude the tongue out of the oral cavity or depress parts of the tongue surface. The protrusive activity of the muscle helps to prevent the tongue from sinking back and obstructing respiration; therefore during general anesthesia, the mandible is sometimes pulled forward to achieve the same effect to ensure complete respiration.
Muscles of Pharynx
The muscles of the pharynx are involved in speaking, swallowing, and middle ear function. These muscles are responsible for initiating the swallowing process. The pharynx is part of both the respiratory and digestive tracts and is connected to both the nasal and oral cavities. The pharynx consists of three parts: the nasopharynx, oropharynx, and laryngopharynx (see Figure 2-20). The muscles of the pharynx include the stylopharyngeus, the pharyngeal constrictor, and the soft palate muscles.
Stylopharyngeus Muscle
The stylopharyngeus muscle (sty-lo-fah-rin-je-us) is a paired longitudinal muscle of the pharynx.
Origin and Insertion.
This muscle originates from the styloid process of the temporal bone. It then inserts into the lateral and posterior pharyngeal walls (Figure 4-29).
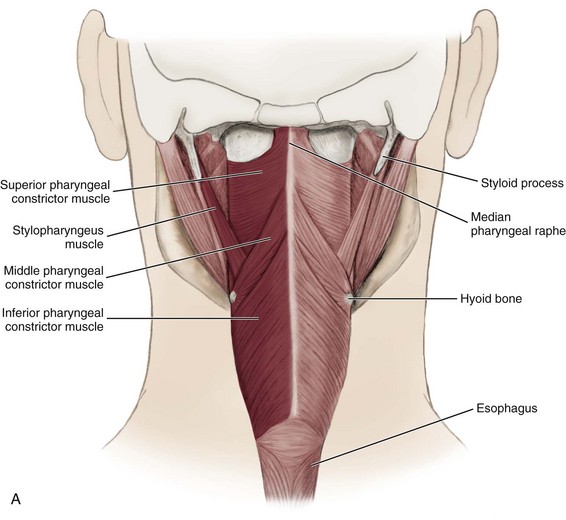
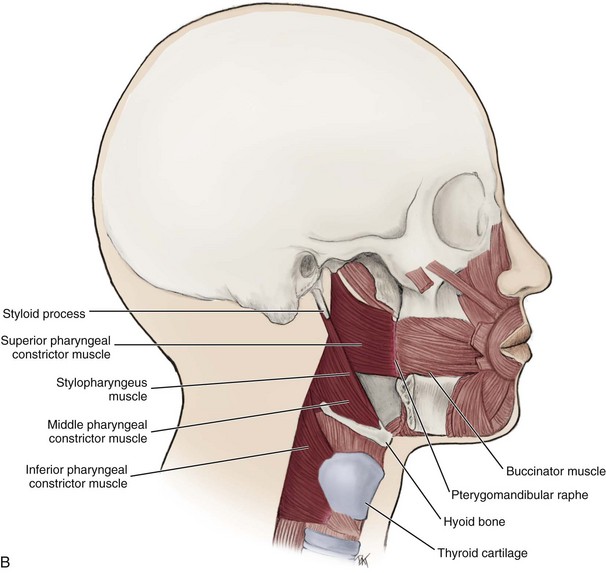
Pharyngeal Constrictor Muscles
The pharyngeal constrictor muscles (fah-rin-je-il kon-strik-tor) form the lateral and posterior walls of the pharynx. They consist of three paired muscles based on their vertical relationship to the pharynx: superior, middle, and inferior.
Origin and Insertion.
The origin of each muscle is different, although the muscles overlap each other and have similar insertions (see Figure 4-29). The superior pharyngeal constrictor originates from the pterygoid hamulus, mandible, and pterygomandibular raphe. The middle pharyngeal constrictor originates on the hyoid bone and stylohyoid ligament. The inferior pharyngeal constrictor originates from both the thyroid and cricoid cartilage of the larynx. When these three muscles overlap, the inferior is most superficial. These muscles then all insert into the median pharyngeal raphe, a midline fibrous band of the posterior wall of the pharynx that is itself attached to the base of the skull.
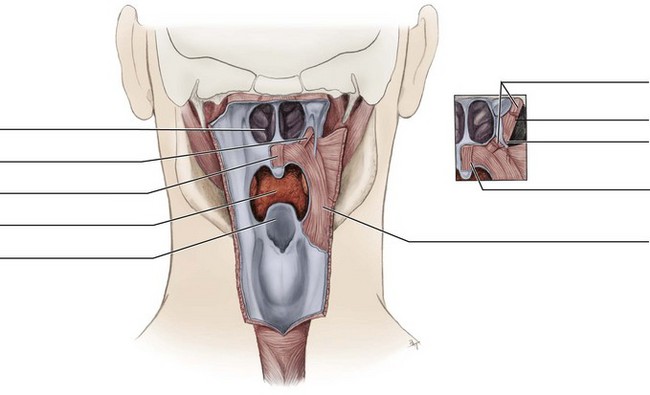
Muscles Of The Soft Palate
The five paired muscles of the soft palate are all involved in speaking and swallowing. The soft palate forms the nonbony posterior part of the roof of the mouth or the oropharynx and connects laterally with the tongue (see Figure 2-20). The muscles of the soft palate include the palatoglossus, the palatopharyngeus, the levator veli palatini, the tensor veli palatini, and the muscle of the uvula (Figures 4-30 and 4-31, Table 4-7). Some anatomists consider the palatoglossus muscle to be an extrinsic muscle of the tongue because it is involved in tongue movement, but it will be considered only a muscle of the soft palate in this chapter.
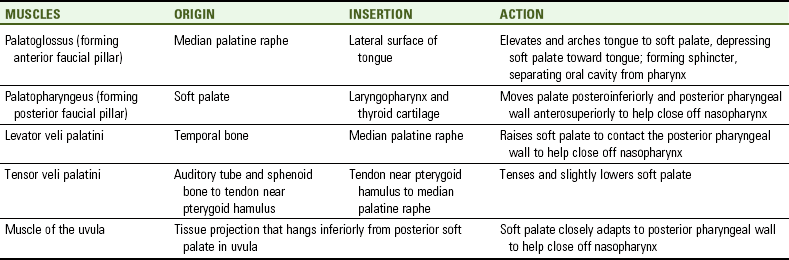
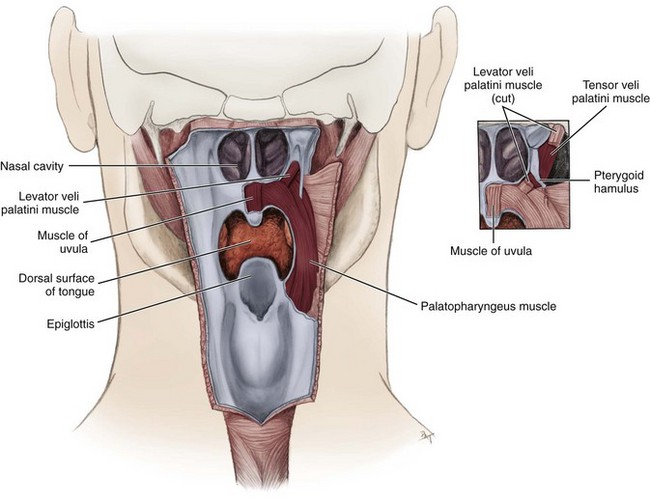
FIGURE 4-30 Posterior view of the muscles of the soft palate highlighted (pharyngeal constrictor muscles have been cut and mucous membranes partially removed) with close-up view (see inset).
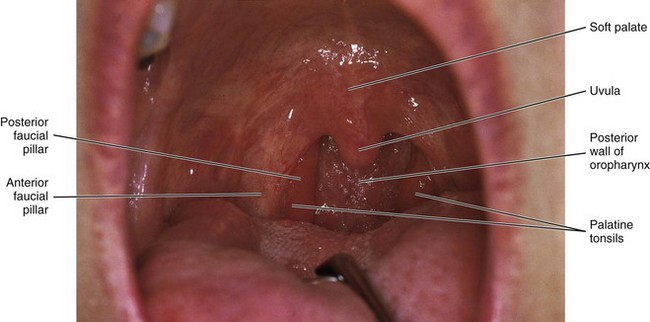
FIGURE 4-31 Intraoral view of the soft palate, uvula, and anterior and posterior faucial pillars with palatine tonsils, which are all oral cavity structures related to underlying muscles; see Figure 2-21 for more detail.
Action.
When the muscles of the soft palate are relaxed, the soft palate extends posteriorly superficial to the anterior oropharynx. The combined actions of several muscles of the soft palate move the soft palate superiorly and posteriorly to contact the posterior pharyngeal wall that is being moved anteriorly. This movement of both the soft palate and pharyngeal wall brings a separation between the nasopharynx and oral cavity during swallowing to prevent food from entering the nasal cavity while eating. Specific actions of each muscle of the soft palate will also be discussed.
Innervation.
All of the muscles except the tensor veli palatini muscle are innervated by the pharyngeal plexus; this muscle is supplied by the mandibular nerve (or division) of the fifth cranial or trigeminal nerve.
Palatoglossus Muscle.
The palatoglossus muscle (pal-ah-to-gloss-us) forms the anterior faucial pillar in the oral cavity, a vertical fold anterior to each palatine tonsil (see Figures 2-21, 4-28, 4-31, and 10-19).
Palatopharyngeus Muscle.
The palatopharyngeus muscle (pal-ah-to-fah-rin-je-us) forms the posterior faucial pillar in the oral cavity, a vertical fold posterior to each palatine tonsil (see Figures 2-21, 4-30, 4-31, and 10-19).
Levator Veli Palatini Muscle.
The levator veli palatini muscle (le-vate-er vee-lie pal-ah-teen-ee) is a muscle mainly superior to the soft palate (see Figure 4-30).
Origin and Insertion.: This muscle originates from the inferior surface of the temporal bone. It then inserts into the median palatine raphe, a midline fibrous band of the palate (see Figure 2-15).
Tensor Veli Palatini Muscle.
The tensor veli palatini muscle (ten-ser vee-lie pal-ah-teen-ee) is a special muscle that stiffens the soft palate (see Figure 4-30). This muscle is probably active during all palatal movements; some of its fibers are also responsible for opening the auditory tube to allow air to flow between the pharynx and middle ear cavity.
Origin and Insertion.: This muscle originates from the auditory tube area and the inferior surface of the sphenoid bone. It then passes inferiorly between the medial pterygoid muscle and medial pterygoid plate, forming a tendon near the pterygoid hamulus. The tendon winds around the hamulus, using it as a pulley, then spreads out to insert into the median palatine raphe.
Muscle of the Uvula.
The muscle of the uvula (u-vu-lah) is a muscle of the soft palate.
Origin and Insertion.: The muscle lies entirely within the uvula of the palate, which is a midline tissue structure that hangs inferiorly from the posterior margin of the soft palate and can be noted during an intraoral examination (see Figure 2-21 and Figures 4-30, 4-31).
Action.: This muscle shortens and broadens the uvula, changing the contour of the posterior part of the soft palate. This change in contour allows the soft palate to adapt closely to the posterior pharyngeal wall to help close off the nasopharynx during swallowing.
Identification Exercises: Identify the structures on the following diagrams by filling in each blank with the correct anatomic term. You can check your answers by looking back at the figure indicated in parentheses for each identification diagram.
1. (Figure 4-4, A)
2. (Figure 4-4, B)
3. (Figures 4-22 and 4-23)
4. (Figure 4-24)
5. (Figure 4-27)
6. (Figure 4-28)
7. (Figure 4-29, B)
8. (Figure 4-30)
1. Both the origin of the frontal belly of the epicranial muscle and the insertion of its occipital belly are at the
2. Which of the following muscles is considered a muscle of mastication?
3. The origin of a muscle is considered to be
A the starting point of a muscle.
B where the muscle fibers join the bone tendon.
4. Which of the following muscle pairs is divided by a median septum?
5. Which of the following paired muscles unite medially, forming the floor of the mouth?
6. Which of the following muscle groups listed below serve to depress the hyoid bone?
7. Which of the following muscles has two bellies, giving the muscle two different origins?
8. Which of the following is the MOST commonly used muscle when the patient’s lips close around the saliva ejector?
9. Which of the following muscle groups is involved in both elevating the hyoid bone and depressing the mandible?
10. Which of the following muscle groups listed below is innervated by the cervical nerves?
11. Which muscle can make the patient’s oral vestibule more shallow, thereby making dental work sometimes difficult?
12. Which of the following muscle groups is innervated by the facial nerve?
13. Which of the following muscle groups inserts directly on the hyoid bone?
A Geniohyoid, stylohyoid, and omohyoid muscles
B Masseter, stylohyoid, and digastric muscles
C Masseter, buccinator, and omohyoid muscles
D Palatopharyngeus and palatoglossus muscles and muscle of the uvula
14. Which of the following muscles is used when a patient grimaces?
15. Which of the following muscles is an extrinsic muscle of the tongue?
16. Which muscle of facial expression compresses the cheeks during chewing, assisting the muscles of mastication?
17. The superior pharyngeal constrictor muscle is noted to
18. Which of the following statements concerning the masseter muscle is CORRECT?
A Most superficial muscle of facial expression
B Originates from the zygomatic arch
19. Which of the following muscles forms the anterior faucial pillar in the oral cavity?
20. Which of the following situations occurs when BOTH sternocleidomastoid muscles are used by the patient?
21. Which muscle does NOT aid in smiling with the lips when it contracts?
22. Which muscle is located just deep to the skin of the neck?
23. Which muscle listed is considered MOST superior on the head and neck?
24. Which muscle listed below, when contracted, causes a frown?
25. Which muscle listed below is MOST superficial in regards to location?
26. Which of the following muscle pairs are considered to be intrinsic tongue muscles?
27. All the muscles of the pharynx are known to be involved in
28. The posterior belly of the digastric muscle is also considered a(n)
29. Which of the following nerves innervates the temporalis muscle?
A First cervical nerve by way of the hypoglossal nerve
B Ninth cranial nerve or glossopharyngeal nerve
C Maxillary branch of the trigeminal nerve
30. Which muscle’s activity helps to prevent the tongue from sinking back and obstructing respiration?