Environmental and Occupational Medicine
INTRODUCTION
Environmental medicine is a broad term that encompasses industrial and occupational medicine and environmentally induced illnesses and conditions. It is used throughout this chapter to refer to all three branches of study. Environmental medicine and a separate branch of medicine called clinical ecology both study the results of interaction between humans and the environment. Occupational medicine is a specialty involving the health of workers and workplaces and can be considered a special form of environmental medicine.
Clinical ecology encompasses little-understood health disorders and chronically fluctuating illnesses mainly attributed by clinical medicine to psychosomatic complaints. Considerable polarization occurs over the issues of environment-related illnesses. People affected by environment-related illnesses consider themselves victims of medical ignorance, and the medical community is skeptical of the physiologic basis for the often numerous and vague symptoms described.
The environment is defined as all agents outside the body, including infectious organisms, toxins, and food. Intrinsic factors include the genetic makeup of the host and the individual’s underlying state of health and history of past illnesses. Cell injury and resultant disease result from interplay of the environment and these intrinsic factors when the host defenses are overcome. Whether at home, in the workplace, or in the community at large, chemical, physical, biologic, psychosocial-spiritual, and traumatic hazards exist.
Usually the focus of environmental medicine is on chemical and physical hazards in the environment. Many diseases, disorders, and defects (contact dermatitis, obstructive lung disease, nephropathy, neuropathy, autoimmune disorders, various cancers, and birth defects are a few examples) occur when the body is exposed to some agent or stressor in the environment.
Industrial, occupational, and environmental illnesses, injuries, and diseases widely affect the population. Hazardous waste sites, nuclear energy leaks, contaminated drinking water, low-level exposures to untested chemical compounds, and repeated exposure to electromagnetic waves and secondhand smoke are examples of problems the American public continues to face. However, it should be noted that in comparison to all the possible hazards listed, morbidity and mortality from the voluntary intake of tobacco smoke, alcohol, and illicit psychoactive drugs far exceed effects from all other environmental hazards combined.
Many consumers are critical of the lack of an adequate, integrated, or holistic approach to health care, including the consideration of biopsychosocial-spiritual aspects. The challenge in the new millennium is to develop effective consumer protection against environmental illnesses for the general population and to bring evidence-based medical practice to the treatment of these illnesses for those people already affected.45
Molecular Epidemiology
A new area of research called molecular epidemiology is specifically aimed at measuring biologic effects and the influence of individual susceptibility to carcinogens and mutagens. With the development of the Human Genome Project, increased genetic and population-based association studies are focusing on identifying underlying susceptibility genes and contributions from geneenvironment interaction to common complex diseases.
Exposure to environmental contaminants can now be measured using biomarkers such as metabolites in urine, chromosomal aberrations, mutations in specific genes, or deoxyribonucleic acid (DNA) measure of exposure to hydrocarbons or tobacco smoke. Biomonitoring involves looking for “pollution in people” by testing bodily substances, usually blood and urine, for the presence of harmful substances such as dioxins, polychlorinated biphenyls (PCBs), and DDT.
Epidemiologic studies support the use of chromosomal breakage as a relevant biomarker of cancer risk. New ways of analyzing oxidative damage to DNA are now available.152
Regulation of Environmental Health Care
Multiple agencies exist for the investigation and regulation of environmental health care. The National Institute for Occupational Safety and Health (NIOSH) is the federal research agency that conducts studies to develop safety and health standards. It does not have legal authority to adopt or enforce regulations.
The Occupational Safety and Health Administration (OSHA) is the primary regulatory agency that determines which of the standards proposed by NIOSH are adopted and enforced. Its standards are law throughout the United States, and its compliance officers can inspect the workplace at any time to determine the status of health and safety. Many other government and private agencies and organizations are concerned with these regulatory issues.
Risk assessment used by the Environmental Protection Agency (EPA) in regulating new chemicals determines how much harm is acceptable to human health, animals, or the environment. Risk assessment determines how much hormone or pesticide residue is allowed in food, how much of a toxic substance can be discharged into a river, how much pollutant can be released as automobile exhaust, or how clean a Superfund site has to be before it is deemed “safe.” Some scientists are advocating an alternative to this type of risk assessment by asking whether this toxin is necessary instead of how much is safe.110
Applying a precautionary principle and questioning whether a new substance is needed requires the industry to find alternatives when there is evidence of damage to the environment. For example, the industry did find an alternative to chlorofluorocarbons (CFCs) when damage to the ozone was identified. Many countries around the world have already established this approach by offering financial incentives for organic farming, resisting importation of beef treated with growth hormones, and seeking alternatives to new chemicals.
ENVIRONMENTAL MEDICINE
The rapid proliferation of new industrial materials, production methods, and commercial products in the twentieth century (particularly since World War II) has progressed with little known about their effects on the environment and human health. Only about 10,000 of the estimated 85,000 chemicals used commercially today have been tested for toxicity in animals. Although toxicity testing lags far behind the rate of new developments, the incidence of work-and environment-related illnesses in humans increases.
Each year in the United States, more than 2 million people experience permanent or temporary disability from various causes, including occupational illness and injury. Although the number of people with disabilities resulting from occupational illness is not known, it has been estimated that at least 390,000 new cases of disabling occupational illness and as many as 100,000 deaths from occupational diseases occur each year.
It is likely that because of the difficulty of diagnosis and the likelihood that occupational illness claims will be disputed by employers, these figures are most likely gross underestimates of the true incidence of environmentally induced illnesses. An estimated 25% of preventable illnesses worldwide can be attributed to poor environmental quality. In the United States, air pollution alone is estimated to be associated with 50,000 premature deaths and an estimated $40 to $50 billion in health-related costs annually (preterm birth, infant mortality, lung disorders, or asthma).
The National Academy of Sciences estimates that 15% of the population experiences some degree of chemical sensitivity, and chemical-related injury and illness are dramatically on the rise. The Social Security Administration recognized chemical sensitivity as an environmental illness and disability in 1988.
The Clean Air Act, which was last amended in 1990, requires the EPA to set National Ambient Air Quality Standards for pollutants considered harmful to public health and the environment. The Clean Air Act established two types of national air quality standards. Primary standards set limits to protect public health, including the health of sensitive subgroups such as children, older adults, and anyone with conditions such as asthma or chronic obstructive pulmonary disease. Secondary standards set limits to protect public welfare, crops, vegetation, and buildings.165
The federal government now has proposed stricter standards for particulates, which are pollutants that come from road dust, boilers, wood stoves, diesel fuel, traffic, and other sources. These standards, referred to as National Ambient Air Quality Standards, govern pollutants such as carbon monoxide, lead, nitrogen dioxide, particulate matter, ozone, and sulfur oxides.165
Children are especially more likely to be adversely affected by environmental contaminants. From fetal development to early childhood, a greater risk of damage and impairment from exposure to environmental hazards is likely. Children are born with immature nervous, respiratory, reproductive, and immune systems. They absorb a greater proportion of substances through their intestinal tract and lungs and detoxify and excrete toxins differently than adults. Children are outdoors more often, engage in hand-to-mouth activity, and often play in the dirt or on the floor or carpet that places them closer to the source of many pollutants. Air pollution affects children more significantly because of the narrow airways and rapid rate of respiration, allowing inhalation of more pollutants per pound of body weight.
The EPA has established an Office of Child Care Protection to increase its studies on the welfare of children in its environment. Researchers are investigating the possible causal relationship between environmental exposure and the increased incidence of childhood onset of asthma, childhood cancers, autism, and learning disabilities or attention deficit disorders.
Of great concern is the recent finding of polybrominated diphenyl ethers (PBDEs) in human breast milk. PBDEs are flame retardants added to a multitude of products to reduce flammability. PBDEs have also been used in U.S. plastics for the last 30 years. Common consumer products that often include PBDEs are computers, electronics, clothes, and mattresses that are treated to be flame resistant. PBDEs have been found in breast milk samples from around the world and in both the northern and the southern hemispheres, indicating that PBDEs have become a major persistent organic pollutant.76,141,161,173
The EPA is now conducting a biomonitoring study of breast milk. Many chemicals accumulate in the fat cells, making the breasts a prime target for these substances. Concerns about high levels of breast cancer in some areas of the United States have raised the suspicion of synthetic chemicals as an environmental risk factor for this disease. In 1940, a woman’s lifetime risk of developing breast cancer was 1 in 22. Today that figure has jumped to 1 in 8. The increase cannot be explained simply by the fact that women live longer now.
The Environmental Working Group (EWG) also conducted a study of 10 umbilical cord samples from babies born in U.S. hospitals and found 287 industrial chemicals and pollutants. The blood harbored pesticides, chemicals from nonstick cooking pans and plastic wrap, long-banned PCBs, and wastes from burning coal, gasoline, and garbage. Each baby was exposed to an average of 200 chemicals. The blood sample with the lowest readings contained 154 chemicals. This study confirms that the placenta does not shield cord blood and the baby from chemicals and pollutants.73
This was the first time a baby’s “body burden” was identified and measured. The term body burden is used to describe the amount of pollutants buried in the bloodstream, organ tissues, and fat cells. Exposure to chemicals is a bigger concern with infants because the blood-brain barrier that keeps the contaminants from reaching the central nervous system (CNS) is not yet developed, putting the infants at risk for greater neurologic impairment. In addition, females are born with eggs that could become their own babies, meaning later generations may also be exposed.73
As a result of this study, there has been a call for more publicly funded studies of the impact of chemical exposure to children and biomonitoring of exposure to environmental contaminants throughout the lifespan. The National Children’s Study established in 2000 is examining the effects of environmental influences on the health and development of more than 100,000 children across the United States, following them from before birth until age 21. The goal of the study is to improve the health and well-being of children. It is anticipated that the preliminary results from the first years of the study will be available in 2009-2010.11,105
Etiologic Factors
Chemical (organic and inorganic), physical, and biologic agents that can be considered environmental hazards are numerous (Box 4-1). Despite the many restrictions on industries placed by the EPA, according to the Toxic Release Inventory (TRI), the increased number of polluters in the United States (and worldwide) and underreporting practices have resulted in the release of more toxic chemicals into the environment each year. The TRI is a publicly available EPA database that contains information on toxic chemical releases and other waste management activities reported annually by some industry groups, as well as federal facilities.48
These agents, combined with psychosocial factors, can lower the body’s resistance, making a person more susceptible to infectious diseases. Only chemical and physi- cal agents are discussed here; biologic agents are discussed in Chapter 7; behavioral, social, and lifestyle factors are presented in Chapter 2; and psychosocial-spiritual factors are discussed in Chapter 3.
Chemical Agents
Chemical agents can be classified by use (e.g., agricultural chemicals, automotive products, pharmaceutical agents, cleaning agents, paints, dyes, or explosives); mechanism of action (e.g., enzyme disruption, metabolic poison, irritants, or free radical formation); and target organ(s) (e.g., neurotoxins, hepatotoxins, or cardiotoxins). Although many toxic effects can occur, they can be broken down into three main categories: local acute effects, systemic effects, and idiosyncratic (unpredictable) effects.
Air Pollution
Many investigations of home and workplace environments have clearly documented the role of air pollutants in causing health complaints and disease. For example, construction and architectural modifications introduced in the 1970s as a result of the worldwide energy crisis have resulted in better insulated and tighter buildings with reduced ventilation. Illnesses that develop from indoor air pollution in tight, energy-efficient homes and buildings with poor ventilation and reduced air-exchange rates are known as sick building syndrome or building-related illness.
Although exposure to air pollution is classified separately as indoor and outdoor, the concept of total personal exposure, whether exposure occurs in the home, office, outdoors, at home or at work, in a car or movie theater, and so on, is relevant to every individual. Anecdotal evidence and statistical studies have made a correlation between pollution and a variety of diseases, particularly asthma, heart disease, respiratory disorders, and cancer.
People considered especially susceptible to air pollution include cigarette smokers (or those exposed to secondhand smoke), older adults, infants and young children, and people with chronic obstructive pulmonary disease (COPD) or coronary heart disease (CHD). Increased rates of heart attacks and other cardiovascular events are reported with increased exposure to air pollution for individuals with known heart and blood vessel disease. Fine particulate matter that travels directly into the bloodstream, constricting arteries, is considered to be the mechanism for this effect.24,25
Indoor Air Pollution.: Other sources of indoor air pollution include tobacco smoke; fireplaces; space heaters; stoves; pilot lights; gas ranges; mothballs; cleaning fluids; glues; photocopiers; formaldehyde in foam, glues, plywood, particleboard, carpet backing, and fabrics; and infectious and allergic agents such as dust mites, cockroaches, bacteria, fungi, viruses, and pollen. Toxic chemicals found in every home, from drain cleaners to furniture polish, are three times more likely to cause respiratory distress than airborne pollutants.
The National Pollution Control Center estimates that the average home has approximately 62 different chemicals and that more than 2 million poisonings involving children age 6 and younger occur every year in the United States. Older children and adults account for another 900,000 poisonings.
Radon, a product of the breakdown of radium, poses an environmental risk because of its carcinogenic, especially lung cancer, properties. Exposure is predominantly naturally occurring rather than generated by human polluters and is present in poorly ventilated homes in the form of an odorless gas. Other sources include radioactive waste and underground mines; exposure to tobacco smoke multiplies the risk of concurrent exposure to radon.84,100
Outdoor Air Pollution.: As part of the Clean Air Act of 1990, the EPA set air quality standards to protect sensitive population groups from outdoor air pollutants. The Clean Air Act regulates oxide emissions, making these particles less available to react with volatile organic compounds that form ozone. Healthy People 2010 set goals to reduce the proportion of people exposed to air that does not meet the EPA’s standards for ozone and to reduce the proportion of nonsmokers exposed to environmental tobacco smoke. Preliminary research on pollutants indicates that biofiltration technology used to clean up airborne waste stream removes 94% of total hazardous air pollutants. Scientists are working to identify microbes that will clean up more difficult-to-remove pollutants.54
Carbon monoxide (CO), an odorless, tasteless, and colorless gas, is a common environmental pollutant from automobile exhaust emissions; the use of liquefied petroleum gas (LPG)-powered forklifts in inadequately ventilated warehouses and production facilities; fires; and in some areas, home heating systems (e.g., the incidence of CO poisoning in homes with faulty furnaces has become an increasing problem, especially in the Midwest). Inexpensive CO-monitoring devices have helped identify many previously undetected cases of high levels of CO in private homes.
CO is commonly recognized for its toxicologic characteristics, especially CNS and cardiovascular effects. CO combines 240 times more quickly with hemoglobin (or myoglobin affecting muscles) than oxygen, so when carbon dioxide is bound to hemoglobin, its oxygen-carrying capacity is decreased. In the presence of CO, oxygen is not released normally by the blood, resulting in tissue hypoxia.
Tissue hypoxia has serious functional consequences for organ systems that require a continuous supply of oxygen such as the brain and the heart. Exposure to CO also causes impaired visual acuity, headache, nausea, vomiting, fatigue, seizures, behavioral change, and ataxia. In addition, when tissue partial pressure of oxygen is low, CO binds to intracellular hemoproteins, such as myoglobin, inhibiting their function and thereby affecting muscle function.
More severe CO poisoning can produce metabolic acidosis, pulmonary edema, coma, and death. The classic clinical findings of cherry-red lips and nail bed cyanosis caused by the bright-red color of carboxyhemoglobin (COHb) may occur if the COHb concentration is above 40%, but this is rarely observed.
Other air pollutants include smog, a combination of smoke and fog that develops when vehicle emissions and exhaust fumes containing nitrous oxides and hydrocarbons are photochemically oxidized. Ozone and nitrogen, the components of smog, result from the action of sunlight on the products of vehicular internal combustion engines. Automobiles and trucks emit unburnt hydrocarbons and nitrogen dioxide. Ultraviolet irradiation of these compounds leads to complex chemical reactions that produce ozone, various nitrates, and other organic and inorganic compounds constituting smog.
Nitrogen dioxide and ozone are toxic byproducts of this reaction. Ozone is also produced in the welding process when oxygen is ionized. Both of these byproducts are toxic to the respiratory tract, damaging ciliated endothelial cells lining bronchioles and impairing the mucociliary clearance mechanism. Outdoor air pollution has long been associated with clinically significant adverse health effects. The very young, very old, heavy smokers, or those with preexisting lung disease are at increased risk in the presence of these toxins. Although it is unclear whether outdoor air pollution contributes to the development of asthma, it does trigger asthma episodes.1
Growing evidence from around the world shows that the harmful effects of smog extend even to the unborn in utero. More than a dozen peer reviewed studies in the United States, Brazil, Europe, Mexico, South Korea, and Taiwan have linked smog to low birth weight, premature births, stillbirths, and infant deaths. In the United States, research has documented ill effects on infants even in cities with modern pollution controls. Although this research shows a correlation between air quality and infant illnesses, it does not establish a conclusive cause-effect connection.125
Acid rain caused by the interaction of sulfur dioxide and nitrogen oxides in the atmosphere forms fine sulfate and nitrate particles transported by wind currents over long distances through the air. Outdoor sulfate and nitrate particles penetrate indoors and can be inhaled deep into the lungs. The northeastern United States experiences the greatest levels of acid and sulfate aerosols (up to 25% of the breathable particles) during the spring and summer months.64,151 No known correlation exists between elevated levels of these fine particles and bronchoconstrictive disorders such as asthma, emphysema, and bronchitis.
Water Pollution
Water pollution in the form of contamination of drinking water by toxic chemicals has become widely recognized as a public health issue since the late 1970s. Increased monitoring since then has shown that many pesticides and industrial chemicals can be detected in drinking water. The EPA, in conjunction with public health officials and the drinking water industry (e.g., Partnership for Safe Water), has worked diligently to survey and reduce waterborne-disease outbreaks, chemical contamination from leached industrial waste chemicals, and toxins released into recreational and drinking water.12
In 1996, the Safe Drinking Water Act was amended to require all community water systems to deliver an annual water quality report to their customers, including levels of any detected contaminants. The EPA has placed limits on the amount of certain contaminants in water provided by public water systems. Anyone with a private source of water (e.g., cistern or well water) does not come under this type of protection. Water that travels over the surface of the land or through the ground can pick up radioactive substances, naturally occurring minerals, or substances resulting from the presence of animals or human activity.
Contaminants that may be present in source water include microbial contaminants, such as viruses and bacteria, that come from sewage treatment plants, septic systems, agricultural livestock operations, and wildlife. Inorganic contaminants, such as salts and metals, may be present from urban stormwater runoff, industrial or domestic wastewater discharges, oil and gas production, mining, or farming.
Pesticides and herbicides from a variety of sources (e.g., agriculture, urban stormwater runoff, or residential uses) and organic chemical contaminants from by-products of industrial processes and petroleum production (including from gas stations) are additional source-water contaminants.
Some subgroups of people may be more vulnerable to contaminants in drinking water than the general population. Immunocompromised individuals, such as those with cancer who are undergoing treatment; organ transplant recipients; people with human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) or other immune system disorders; some older adults; and infants are at increased risk from infections.
Disinfection with chlorine is the most common method to ensure drinking water safety in the United States. A dramatic decline in waterborne diseases, such as cholera and typhoid fever, occurs when water systems are disinfected this way. One potential downside of this disinfectant treatment is the increased genotoxicity that occurs with water treatment. Ways to evaluate the toxicity and genotoxicity of disinfected drinking water are under investigation.
A different form of water pollution has also raised concerns. Billions of gallons of treated sewage are released offshore into deep waters via long undersea pipelines called outfalls. Wastewater is filtered and processed, but many contaminants (especially estrogenic compounds) remain and settle into ocean sediment, where they are consumed by bottom-feeding organisms that become food for other ocean life. Evidence of abnormalities in animals and fish exposed to sewage and industrial contaminants has been reported, but the effect on overall health and abundance of fish populations and the rest of the marine ecosystem remains unknown.132
In other areas of the United States, past abuses from mining thousands of tons of arsenic, copper, manganese, and other metals harmful to humans and aquatic life polluted the soil and groundwater, leaving areas barren and unable to support vegetation. Acid-generating deposits called slickens scattered throughout the floodplain continue to send toxic metals directly into rivers through runoff. Not all areas have undergone cleanup and restoration. The effect on health and potential for higher incidences of cancer and other diseases remains underdetermined at this time.
Food
Food as a pollutant is one of the major environmental agents to which people are exposed. In many documented cases, reversible and irreversible human and ecologic damage has occurred as a result of pollution-induced food contamination. As scientific and epidemiologic information accumulates, society is questioning to what degree these technologies and by-products contribute to the steadily rising incidence of certain cancers, autoimmune and other chronic diseases, birth defects, autism, learning disorders, and other health problems for which the cause is not well understood.
Pesticides, Insecticides, and Herbicides.: Pesticide, insecticide, and herbicide residues in food; hormone residues; food irradiation (a method of preservation and protection from microbial contamination); genetically modified foods; and food additives and preservatives are major consumer concerns. Pesticide and herbicide exposure can cause many different health effects, from acute problems, such as dermatitis and asthma exacerbation, to chronic problems, such as COPD and cancer.130 Acute pesticide poisoning has been reported among food handlers (e.g., clerks, baggers, stockers, or shipping/receiving handlers) and janitors in retail establishments that sell food products, especially fruits and vegetables.31
Among the people most in danger from pesticide exposure are farmers and agricultural workers. Many studies of these groups have shown an increase in soft tissue sarcomas, presumably from herbicide exposure.56 Children, especially very young children, are also at greater risk from exposures to pesticides and other environmental toxins compared to adults because, pound for pound of body weight, children drink more water, eat more food, and breathe more air than adults.
Childhood leukemia has also been linked with the use of home insecticides and garden fungicides during pregnancy and early childhood. The treatment of pediculosis (lice) with an insecticidal shampoo also may be associated with an increased risk of childhood leukemia.94 School-aged children are also at increased risk for acute illnesses from repellants and pesticides applied within school grounds, pesticide drift exposure from farmland, and pesticide use at parks.3
In the United States, environmental exposure to chlorophenoxy herbicides used in wheat production has been linked to musculoskeletal and respiratory-circulatory birth defects, cancer, type 2 diabetes, and heart disease.135,136 Counties in which wheat is produced have a high rate of defects among infant boys conceived during April or June when herbicide application takes place. Boys conceived during other times of the year and born in counties with low wheat production have far fewer birth defects.134
Pesticides that are not registered or are restricted for use in the United States can be imported in fruits, vegetables, and seafood produced abroad. Environmental quality is a global concern as increasing numbers of people and products cross national borders, transferring health risks such as infectious diseases and chemical hazards.
Contaminated Soil
Contaminated soil is often the main source of chemical exposure for humans, and an active interchange of chemicals occurs between soil and water, air, and food. Direct contact and ingestion of soil are important exposure pathways, and inhalation of volatile compounds or dust must also be considered. The movement of contaminants through soil is very complex, some moving rapidly and others slowly, eventually reaching and contaminating surface or ground water on which people rely for drinking and other purposes.
Asbestos
Asbestos continues to be a significant occupational hazard. It was not until the late 1960s and early 1970s that the public was made aware that asbestos used in products ranging from automotive brake linings to building insulation caused chronic respiratory illnesses, cancer, and other illnesses. Since then, commercial use of asbestos has decreased dramatically.
Abatement workers employed to remove asbestos in buildings wear protective clothing to decrease exposure but still are considered at risk. Long latency (exposure occurring 30 or more years ago continues to affect former workers) and long-term, low-level exposure to the presence of indoor asbestos remain risk factors. It is not just asbestos but other long, thin mineral fibers in the workplace or in the environment that can have similar effects. See Chapter 15 for a discussion of asbestosis.
Manmade vitreous fibers containing mineral wool, glass wool or fiber, and ceramic fiber have replaced asbestos in the workplace. The nonoccupational exposure to manmade minerals does not put consumers at substantial risk; health issues related to these materials mainly occur among workers with long duration of exposure. Clinical consequences are similar to those of asbestos, including pulmonary fibrosis, bronchogenic carcinoma, mesothelioma, and possibly other types of cancers.
Other Chemical Compounds
Polyvinyl chloride (PVC), a type of plastic made flexible through the addition of a chemical, is used in a variety of products, including medical solutions stored in PVC medical devices such as saline bags. Vinyl chloride production has doubled in the last 20 years, with current production of 27 million tons per year worldwide. Concern exists over the possibility of chemical plasticizers leaching into the solutions used long-term by certain populations, including people on dialysis, individuals with hemophilia, or neonates exposed at critical points in development.
Additionally, measured changes in the acidity of intravenous (IV) solutions in PVC packaging have been reported.155 Dioxin, a byproduct of PVC plastics manufacturing, was declared a carcinogen by the EPA in June 2000. Dioxin accumulates in fatty tissues of mammals and fish. The observed toxicities of these chemicals have been linked to birth defects and immune system disorders, resulting in the request for PVC-free medical devices and reduction of environmental contamination with these compounds to the lowest level possible.82,160 High levels of dioxin exposure are associated with chloracne, a distinctive form of acne (Fig. 4-1), and with porphyria cutanea tarda (Fig. 4-2).
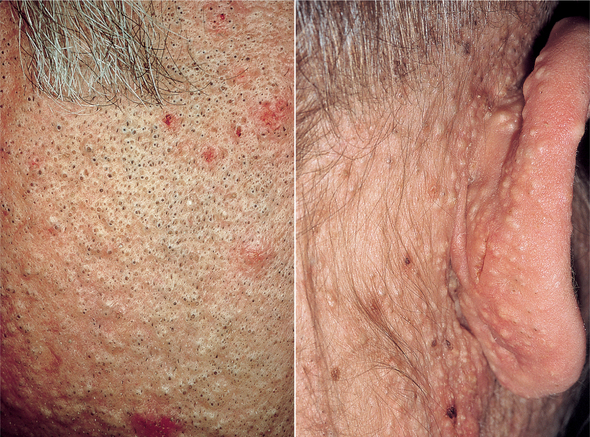
Figure 4-1 Chloracne. (From Bolognia JL, Jorizzo JL, Rapini RP: Dermatology, St Louis, 2003, Mosby.)

Figure 4-2 Porphyria cutanea tarda. Erosion, crusting, and vesicles on the dorsum of the hand in an individual with porphyria cutanea tarda. (From Goldman L: Cecil textbook of medicine, ed 22, Philadelphia, 2004, WB Saunders.)
Most adults tested also show the chemical perfluorooctanoic acid (PFOA), a chemical compound widely used in Teflon-coated cookware, water-and stain-resistant clothing, cosmetics, and many other products. There has been growing concern about the effects of this compound. Extensive scientific assessment of the perfluorochemical family is underway to determine whether the substances cause sexual reproductive and developmental damage to females. PFOA has also been linked to testicular, liver, and pancreatic cancer in animals.30,115
Fire and Pyrolysis
Fire and pyrolysis directly affect 2 million people annually who are treated for burns, including civilians and firefighters. Pyrolysis, or incomplete combustion, of wood releases many highly toxic compounds that can react with other organic substances to produce new toxic and irritant chemicals. Incomplete combustion and fire-fighting water also produce highly acidic aerosols. Smoldering or partially controlled fires release many toxic products.
The most common type of injuries is in the category of smoke inhalation and respiratory problems followed by lacerations, contusions, and falls. Death can occur as a result of smoke inhalation and myocardial infarction. See the section on Occupational Burns in this chapter.
Waste
Waste from solid, hazardous, and incinerator by-products is not likely to be encountered directly in a therapy practice. However, the effects of exposure to medical/infectious waste may be more problematic. Standard precautions for handling all medical/infectious waste are available (see Chapter 8 and Appendix A).
Heavy Metals
Heavy metals, such as lead, arsenic, and mercury, actually fall under the chemical agents category but are mentioned separately because of their former prevalence and uniqueness as classic occupational and environmental hazards. In the early 1990s, environmental concerns shifted attention away from lead, mercury, arsenic, and asbestos exposure despite continued high production volume chemical development, toxicology testing, and issues centered around environmental justice.85
However, new findings from the TRI have resulted in a resurgence of interest and research in this area. The TRI is a publicly available EPA database that contains information on toxic chemical releases and other waste management activities reported annually by some industry groups, as well as federal facilities. The 2006 TRI findings report 4.24 billion pounds of on-site and off-site disposal or other releases of toxic chemicals. Total disposal or other releases of mercury and mercury compounds amounted to 4.8 million lbs in 2004.
Lead Poisoning
A normal blood lead level is 0. Apparent toxicity is not usually demonstrated until the blood serum lead levels exceed 24 mg/dl in adults and 10 mg/dl in children. Lower levels (5 mg/dl) have been identified for pregnant women. Any levels above these marks require intervention. OSHA prohibits workers with levels greater than 40 mg/dl from returning to the workplace where lead is present.32
Lead poisoning is on the decline in the United States as a result of federal initiatives to end the use of lead in gasoline, lead solder in the seams of food cans (beware of foods in cans manufactured outside the United States), lead-based paints, and plumbing in homes. Consumers should also be aware that the porcelain glaze of old bathtubs and the glaze on imported dishware (ceramics, china, or porcelain) often contain lead and are a potential source of lead exposure. Internet purchases of dishware and ceramics on-line present a particular threat. Lead can leach out of dishware when the glaze is improperly fired or when the glaze has broken down because of wear from daily usage, especially after repeated use in a microwave or dishwasher. Chips and cracks in ceramic ware also allow leaching of lead. Children’s risk for such exposures is increased with frequent consumption of acidic juices that promote lead leaching from ceramics.99
Ingestion of lead paints found in older residential neighborhoods and exposure to lead dust particles during home renovation projects remain continuing problems among the pediatric population. Likewise, dust and soil containing lead particles too small to see expose children, who are more likely to be on the ground or outside and who engage in more hand-to-mouth activities.
Children.: Lead is particularly toxic to infants and children for several reasons, including (1) the blood-brain barrier is immature before the age of 3, allowing lead to enter the brain more readily; (2) ingested lead has a 40% bioavailability in children, compared with 10% in adults; and (3) the behavioral hand-to-mouth habits previously mentioned. Lead is stored in the body predominantly in bone but may adversely affect many organ systems, including the CNS and the gastrointestinal, hemopoietic, reproductive, and renal systems.
Health effects in infants born to women with moderately elevated blood lead levels include preterm birth, decreased gestational maturity, lower birth weight, reduced postnatal growth, increased incidence of minor congenital anomalies, and early neurologic or neurobehavioral deficits. It remains unclear how long these neurologic effects persist, but some evidence suggests a link between prenatal elevated lead levels and decreased intelligence in children up to age 7 years.32
Serum levels once thought to be safe have been shown to be associated with intelligence quotient (IQ) deficits, behavioral disorders, slowed growth, decreased competency in verbal performance and auditory processing, and impaired hearing. The impairment of cognitive function begins to occur at levels greater than 10 μg/100 ml, even though clinical symptoms may not be apparent; serum levels are required for diagnosis. Other studies show cognitive and delayed puberty at levels below 10 μg.33,126,140 Lead exposure has also been linked with reproductive dysfunction and toxicity to the kidneys, blood, and endocrine system.
Other risk factors for children include age under 6 years, low income, and urban dwelling. Adults are more likely to be exposed to lead in the manufacture of brass, batteries, bullets, solder, or glass; furniture refinishing; home renovations; stained-glass or pottery making; and prolonged exposure to the burning of metallic wick candles (e.g., home use, restaurant, religious, or ceremonial).109,149
Arsenic
Arsenic is used in the manufacture of glass, pesticides, and wood preservatives and has been found to contaminate water, beer, and seafood. Arsenic binds to tissue proteins and is concentrated in the liver, skin, kidney, nervous system, and bone, with bone being affected to a lesser extent than with lead. The symptoms of acute inorganic arsenic poisoning may include severe burning of the mouth and throat, abdominal pain, nausea, vomiting, diarrhea, hypotension, and muscle spasms.
Epidemiologic studies have demonstrated a correlation between environmental or occupational arsenic exposure and a risk of vascular diseases related to atherosclerosis. It appears that arsenic induces endothelial dysfunction as a result of impaired nitric oxide (NO) balance, and inflammatory and coagulating activity. Arsenic may accelerate atherosclerosis, but the mechanism for this event remains under investigation.145
In severe cases, cardiomyopathy, jaundice, renal impairment, red cell hemolysis, ventricular arrhythmias, coma, seizures, and intestinal hemorrhage are seen. Chronic arsenic poisoning is characterized by an irregular dusky pigmentation and hyperkeratosis of the skin that looks like raindrops on a dusty road. Painful dysesthesia in the hands and feet, bone marrow depression, transverse white striae of the nails, altered mentation, and occasionally garlicky perspiration odor may occur.
Cancers of the skin, kidney, bladder, and lungs have been associated with arsenic poisoning, but the mechanisms responsible for arsenic carcinogenesis have not been established. Increasing evidence indicates that arsenic acts at the level of tumor promotion by modulating the signaling pathways responsible for cell growth.146,170 The risk of arsenic-induced cancer is associated with 20 or 30 years of drinking polluted water, not from a brief or occupational exposure. The current standard in the United States is 10 parts per billion. Any water supply that has much higher arsenic levels is not considered safe for human consumption.
Mercury
Mercury is widespread and persistent in the environment and can be dangerous when ingested, inhaled, or absorbed through the skin. Most people have some amount of mercury in their bodies, but random testing of individuals has revealed higher than the acceptable, safe limit of 1 part per million set jointly by the EPA and the Food and Drug Administration (FDA).
Exposures to women of childbearing age, pregnant and nursing women, and children younger than age 15 are of great concern because of the susceptibility of these groups and resultant adverse effects. According to analysis of data gathered by the National Health and Nutrition Examination Survey, between 200,000 and 400,000 children born in the United States each year have been exposed to mercury levels in their mothers’ wombs high enough to impair neurologic development.106
Sources of Mercury.: Harmful mercury vapors can be transferred to water and soil where they can be introduced into the food chain, causing renal and neurologic disorders. Although eating contaminated fish is the leading cause of mercury accumulation in humans, elevated levels of emissions from coal-burning power plants and petroleum refineries, mining-related wastes, and the improper disposal of mercury products have resulted in increased mercury in the environment, with the trickle down effects on fish. The larger the fish, the higher the concentrations of mercury found in the fish.
Elemental or inorganic mercury is released into the air or water where it accumulates in animal tissues and increases in concentration through the food chain. The U.S. population is primarily exposed by eating fish, but mercury is also used in electrical products and as a fungicide. Industrial sources, such as coal-fired power plants, cement kilns, and refineries, also emit mercury into landfills and into the air and water. In water, mercury becomes methylmercury, a toxic substance that is consumed by fish.
American hospitals dispose of 17 tons of waste each year containing mercury found in medical supplies. In 1998 the American Hospital Association (AHA) and the EPA enacted a new initiative called Hospitals for a Healthy Environment (H2E), which outlined 10 steps for environment-friendly healthcare. Some of the top priorities are to reduce the total volume of hospital waste to 0% by 2010, with the total elimination of mercury products.67,72
There is considerable controversy as to whether dental amalgams (“silver fillings”) may cause significant health effects in humans. Dental amalgams still contain mercury as other materials have not been developed that are as strong or as long lasting. Amalgam restorations contain mercury, silver, tin, copper, and a trace amount of zinc. There is some evidence that a sustained release of mercury and other metals occurs from the amalgam into the body. Researchers have measured a daily release of mercury on the order of 10 μg from the amalgam into the body. Mercury is a toxic metal; the smallest amount damages cells.
In response to a need for a greater concentration of research in this area, a group of concerned dentists formed the International Academy of Oral Medicine and Toxicology (IAOMT) in 1984. One of their objectives was to scientifically explore the safety of amalgam restorations. Since that time, scientists at universities around the world have begun to research possible pathophysiologic effects associated with mercury leaking from amalgam restorations.
Consequently, there are a growing number of scientific studies that document pathophysiologic effects associated with amalgam mercury. In the interest of protecting their citizens’ health, Sweden, Norway, Germany, Denmark, Austria, Finland, and Canada have recently taken steps to limit and phase out the use of amalgam restorations. About one-third of the dentists in the United States no longer use mercury-containing products. Resin composite fillings, which match the tooth color, are used instead.
Despite consumer concerns about mercury exposure from dental fillings, clients and dental personnel are at greatest risk when amalgams are removed. The aerolization during removal creates greater mercury exposure than the hardened and intact filling in the mouth. It is advised by some that amalgams should only be removed when the filling (or tooth) is no longer intact, rather than to eliminate mercury exposure. Dental personnel are at greatest risk for this type of repeated exposure.
Clinical Manifestations (Mercury Exposure).: The EPA reports that about 5 million women had at least 5.8 parts per billion of mercury in their blood as of 2000. They also noted that children born to women with blood concentrations of mercury above 5.8 parts per billion are at some risk of adverse health effects, especially decreased IQ and problems with motor skills.47
Exposure to hazardous levels of mercury can cause permanent neurologic heart and kidney impairment. Neurologic or neurodegenerative diseases, mental retardation, cerebral palsy, seizures, memory loss, learning disabilities, developmental delays, autoimmune disorders, mental health disorders, and birth defects are among the many conditions blamed on mercury exposure.
Vaccines commonly given to children before 2001 contained a preservative (Thimerosal) that contained mercury. There were concerns raised over the total number of vaccinations given to children during the first 6 months of life that could lead to toxic levels of mercury. There was some suspicion that increased rates of autism could be the result of mercury poisoning from vaccines, but this has not been proved conclusively.
Although mercury is poorly absorbed from the gastrointestinal tract, mercury vapor is well absorbed through the lungs and from the gut. Mercury poisoning causes irritation of the mouth and pharynx and is accompanied by vomiting, dehydration, abdominal cramps, and bloody diarrhea. Death can occur from acute renal failure.
Chronic exposure to mercury may cause additional symptoms of gingivitis, speech defects, tremor, and a chronic personality disorder called the Mad Hatter syndrome, characterized by unusual shyness, labile affect, and decline in intellect. Mercury poison affects the nervous system, resulting in dysarthria, ataxia, paresthesias, and constricted visual fields.
Mercury Regulation.: In 2005, the EPA took its first step toward reducing mercury pollution from coal-fired power plants with the Clear Air Mercury Rule designed to reduce mercury emissions by 70% over the next 20 years. The long-term strategy for reducing exposure to mercury is to cap mercury emissions from coal-burning power plants nationwide, thereby lowering mercury releases into the atmosphere and lowering mercury concentrations in fish. Phasing out mercury-containing products, such as thermometers and thermostats, has already become a national trend.
The new rule does not require all plants to reduce emissions by the same amount. Some may be allowed to pollute more than others by buying “pollution credits” from other plants. This practice is called cap and trade. It is based on the assumption that mercury pollution disperses evenly in the environment, but in fact, mercury emitted by coal-fired power plants tends to remain near those plants. This creates what are referred to as geographical “hot spots” of mercury.
EPA regulations for waste incineration have resulted in decreased air emissions of mercury in the last two decades, and this trend is expected to continue. The FDA advises that children, nursing mothers, pregnant women, and those who may become pregnant should not eat fresh tuna, canned white (albacore) tuna, shark, swordfish, king mackerel, and tile fish known to contain elevated levels of mercury.98
Xenoestrogens/Xenobiotics
Xenoestrogens are also part of chemical environmental exposure but are discussed separately because of their unique place as a hazardous agent. In the early 1970s, scientists from around the world met together to discuss the cumulative efforts of researchers investigating various endangered species. Together they identified that exposure to petrochemicals (previously called xenoestrogens but now referred to as xenobiotics, meaning “foreign to life”) is the underlying cause of dwindling births in these species.
Petrochemicals, such as pesticides and insecticides, are the primary xenobiotics and constitute substances totally foreign to nature—that is, they are not found in the natural world but rather are synthesized chemicals. Other petrochemicals are present in commonly used items or products such as emollients in lotions and creams, spreaders in salad dressing, carpet glues, paints, solvents, automobile gasoline, plastics, and a multitude of other common household objects. Researchers concluded that the effect of these residues is selective to the reproductive systems of the developing fetuses so that exposure in the developing fetuses resulted in infertility or sterility. Since that time, it has been recognized that these chemicals can affect other systems, including the thyroid, immune function, and nervous system.
The effect of these chemicals has been to create what is referred to as an estrogen-dominant environment because the chemicals have estrogenic activity. Estrogen dominance on humans (both men and women, although women are more susceptible) is the subject of intense scrutiny by scientists and researchers.
Studies from around the world continue to report broad human exposure to what are now called estrogenic endocrine-disrupting chemicals (EDCs) from environmental media such as food and water contaminated by dioxin and bisphenol A (BPA) widely used for the production of plastic products. BPA has been found in fetal serum and full-term amniotic fluid, confirming passage through the placenta.164 This biologic phenomenon may be linked to autoimmune dysfunction, increased body fat, decreased sex drive and sperm production, altered blood clotting, early menarche, zinc deficiency associated with prostate dysfunction, endometriosis, and headaches associated with fluid retention.
Researchers are in agreement that such compounds in high doses may cause developmental, reproductive, and tumorigenic effects, but controversy remains regarding the risks associated with xenoestrogens under low exposure that are considered more realistic and how to assess the interaction of exogenous compounds with the endocrine system and its complex regulation.41
Physical Agents
The long-term effects of exposure to electromagnetic radiation or electromagnetic fields (EMF), including radiofrequency and microwave, ultraviolet light, x-ray, and gamma rays, remain under intense scrutiny (Fig. 4-3). Ionizing radiation is the result of electromagnetic waves entering the body and acting on neutral atoms or molecules with sufficient force to remove electrons, creating an ion. The most common sources of ionizing radiation exposure in humans are accidental environmental exposure and medical, therapeutic, or diagnostic irradiation.
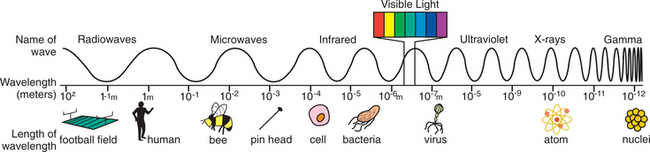
Figure 4-3 Electromagnetic (EM) spectrum. Different types of electromagnetic radiation have different frequency or wavelengths. Radio waves, television waves, and microwaves are all types of electromagnetic waves. The electromagnetic spectrum includes, from longest wavelength to shortest: radio waves, microwaves, infrared, optical, ultraviolet, x-rays, and gamma rays. Waves in the electromagnetic spectrum vary in size from very long radio waves the size of buildings, to very short gamma rays smaller than the size of the nucleus of an atom. The frequency is the rate at which the electromagnetic field goes through one complete oscillation (cycle) and is usually given in Hertz (Hz), where 1 Hz is one cycle per second. As the frequency rises, the wavelength gets shorter.
All living material is vulnerable to ionization by high-energy radiation because the disruption of atoms joined into molecules producing ions and free radicals (see Chapter 6 and Fig. 6-2) can result in further biochemical damage, including somatic effects, such as cell death, and genetic effects, including reproductive effects and cancer. Radiation-induced changes can cause genetic mutations and structural rearrangements in chromosomes that can be transmitted from generation to generation.16,163
A wide range of other adverse health effects have been attributed to ionizing radiation, including visual, thermal, behavioral, CNS, and auditory effects; effects on the blood-brain barrier; and immunologic, endocrinologic (including effects on biorhythm), hematologic, developmental, and cardiovascular effects.
Exposure to nonionizing radiation (i.e., the electromagnetic wave does not have enough energy to strip an atom of its electron) occurs most commonly as a result of the use of a wide variety of industrial and electronic devices (e.g., microwave ovens, scanning lasers in stores, high-intensity lamps, video display terminals [VDTs], scanning radars, or electronic antitheft surveillance).
Chemical compounds from plastic wrap surrounding food or covering dishes used in a microwave can leach into the foods and affect the body. Packaging and plastic wraps that contain polyethylene are preferred for use in the microwave, since these do not have plasticizers (materials that make the wrap more pliable). Containers meant for cold foods, such as margarine or whipped topping, should also be avoided for microwave use, since these containers can melt, dispersing some of their components into the food.
Considerable speculation has gone on around the world that long-term exposure to EMFs is correlated with the development of breast cancer, leukemia, miscarriage, and neurodegenerative diseases such as Alzheimer’s disease, Parkinson’s disease, and amyotrophic lateral sclerosis (ALS).63
The unexplained high incidence of breast cancer in industrialized nations is suspected as being linked to electric power generation and consumption. The proposed biologic mechanism is the inhibition of melatonin caused by the products of electric power generation, EMFs, and light at night, but this has not been proved and further investigation is warranted.40,93,114
Most exposures to electromagnetic interference are transient and pose no threat to people with pacemakers and implantable cardioverter defibrillators; however, magnetic resonance imaging (MRI) and prolonged exposure to EMFs are contraindicated in anyone who is pacemaker-dependent.118
Concerns that cellular telephone radiation is linked to brain tumors or causes a variety of serious problems (e.g., genetic damage, pacemaker or implantable cardioverter defibrillator disruption, interference with heart/lung monitors, or compromise to the blood-brain barrier) have not been substantiated or proven clinically important.162 Long-term studies of longer induction periods, especially for slow-growing tumors with neuronal features, conclude that the data do not support the hypothesis that mobile phone use is related to an increased risk of brain tumors.86,127,138
The lack of ionizing radiation and the low energy level emitted from cell phones and absorbed by human tissues make it unlikely that these devices cause cancer. The only health hazard of cell phones that has been confirmed is the increased risk of having an accident while driving and using a cell phone.36 Likewise, a previous concern that living in close proximity to power lines was correlated to cancer has not been proved21,148 nor have reports linking VDTs to miscarriages been substantiated.87
However, considerable evidence suggests that EMFs affect sleep and therefore affect mood, behavior, and cognitive abilities.144 Exposure to EMFs has been suggested as the cause of a condition referred to as electrosupersensitivity/screen dermatitis in susceptible people using VDTs or artificial light. Cutaneous problems (e.g., itch, heat sensation, pain, erythema, papules, or pustules) and symptoms from internal organs (e.g., the heart) have been reported in association with EMFs.
From the results of recent studies, it is clear that EMFs affect mast cells releasing inflammatory substances, such as histamines, that result in these symptoms. Mast cells are also present in the heart tissue, and data from studies made on interactions of EMFs with cardiac function have demonstrated changes present in the heart after exposure to EMFs. However, the exact significance or cause of these changes remains unknown.57
Vibration
Vibration is divided into two types: whole-body vibration (WBV) and hand-arm vibration (HAV). Truck, bus, and boat drivers; helicopter pilots; heavy equipment operators; miners; and others are at increased risk for WBV. Major clinical concerns of WBV exposure are chronic back pain and degenerative disk diseases, visual and vestibular changes, and circulatory and digestive system disorders.18,62,96 The risk for increased spinal loading and physiologic changes associated with WBV can be reduced by vibration damping, good ergonomic design, reducing exposure, and reducing other risks such as lifting.119
Vibration-induced white finger disease is the most common example of an occupational injury caused by vibration of the hands. This condition occurs secondary to the use of hand tools, such as power saws, grinders, sanders, pneumatic drills, and jackhammers, and other equipment used in construction, foundry work, machining, and mining. Interestingly, WBV is being used in a new neuromuscular training method for athletes called vibration exercise (VE) to increase the mechanical power output of muscles and improve neuromuscular efficiency; VE is also being investigated for the prevention and treatment of osteoporosis.23,95,124
Heat Stress
Heat stress exceeding human tolerance can result in heat-related disorders (e.g., exertional heat stroke, exhaustion, cramps, dehydration, or prickly heat) and heat illnesses (e.g., chronic heat exhaustion, reduced heat tolerance, anhidrotic heat exhaustion, or exertional hyponatremia), some of which are fatal. Heat illness is more likely in hot, humid weather but can occur in the absence of hot and humid conditions.
More than 300 people die every year of heat-related illnesses, and many others require medical attention.34 In a therapy setting, the groups of people most likely to experience heat stress include older adults during temperature extremes, industrial workers, construction workers, firefighters, outdoor sports participants, agricultural workers, pregnant women, and people taking mood-altering drugs (i.e., they lose touch with their environment).
Individuals receiving medications that interfere with salt and water balance are at increased risk for heat-related illness and death. Watch for diuretics, anticholinergic agents, and tranquilizers that impair sweating, as well as antidepressants, such as tricyclic antidepressants, that affect the body’s ability to respond to temperature changes.
Other risk factors include obesity, age, mental illness, heart disease, poor circulation, prescription drug use, and alcohol and other drug use. People 65 years of age and older may not compensate for heat stress efficiently and are less likely to sense and respond to changes in temperature. Although older adults, the very young, and individuals with chronic diseases or mental health disorders are at greatest risk, anyone involved in strenuous physical activity during hot weather can be affected. Sudden change in temperature is an additional risk factor to consider.
The signs and symptoms of exertional heat illnesses may vary from person to person but often include thirst, sweating, transient muscle cramps, fatigue, dizziness or lightheadedness, and dehydration (Table 4-1). Headache, nausea, loss of appetite, decreased urine output, chills, weakness, pallor, or cool and clammy skin may also occur, especially with exercise (heat) exhaustion.
Table 4-1
Clinical Manifestations of Exertional Heat Illnesses
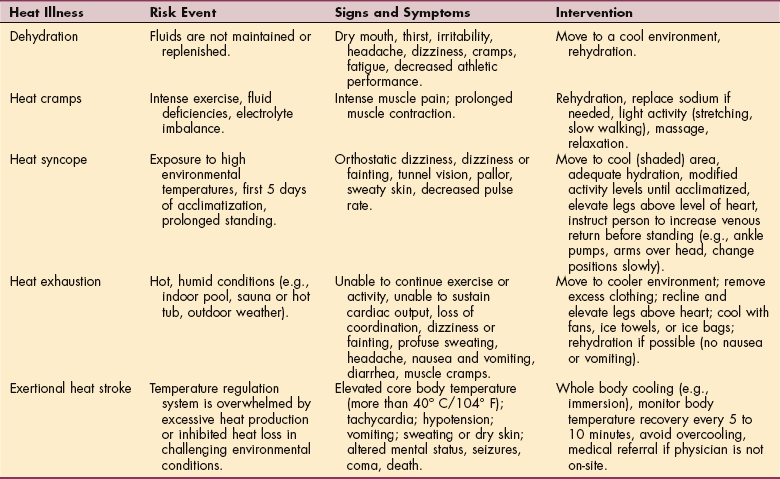
Data from Centers for Disease Control and Prevention (CDC): Extreme heat: a prevention guide to promote your personal health and safety. Available at www.bt.cdc.gov/disasters/extremeheat/heat_guide.asp. Accessed April 21, 2007.
Disorientation, staggering, seizures, loss of consciousness (coma), or emotional instability (even hysteria) occur with exertional heat stroke. Exertional hyponatremia is characterized by increased body-core temperature, low blood-sodium level, progressive headache, confusion, lethargy, significant mental compromise, seizures, swelling of the hands and feet, and even coma.19
High-Altitude
High-altitude environment (8000 to 14,000 feet) is characterized by atmosphere with decreasing partial pressure of oxygen and decreasing temperature. Hypoxia (reduced availability of oxygen to the body) appears to be the underlying cause of most of the physiologic changes of elevated altitude.
Acute altitude sickness includes acute mountain sickness, high-altitude pulmonary edema, and high-altitude cerebral edema. These three probably represent a continuum of disease, but each has different symptom complexes, pathogenesis, and slightly different treatment interventions. With high-altitude pulmonary edema, fluid accumulates in the lungs when the arteries become constricted because of a lack of oxygen and the decrease in air pressure. Symptoms include fatigue; breathlessness at rest; fast, shallow breathing; cough that produces pink, frothy sputum; blue or gray lips or fingernails (cyanosis); chest tightness; and drowsiness.
High-altitude cerebral edema is brain swelling severe enough to interfere with brain function. The affected individual may experience confusion, inability to think or concentrate, confusion, and loss of physical coordination. Vision can become blurred if bleeding occurs from blood vessels at the back of the eye.
Not everyone gets sick at higher altitudes, but health risks increase the higher and faster one climbs, especially if early warning signs are ignored (e.g., headache, fatigue, dizziness or lightheadedness, nausea, or vomiting). People with cardiopulmonary and other diseases (e.g., sickle cell disease) are at increased risk for worsening of the medical disorder and possibly at increased risk for acute altitude illnesses with ascent to high altitudes. Aviation and aerospace illnesses are rarely encountered by the therapist and are beyond the scope of this book.
Risk Factors
Environmental pathogenesis requires an understanding of latency, the concept that a hazardous or toxic agent may initiate a series of internal reactions that do not manifest as overt disease for many years or even decades as the body strives to maintain a state of optimal health or homeostasis. Exposures to any of the agents discussed in the previous section on etiology are in fact risk factors. Many additional factors, such as route of exposure (e.g., inhalation, ingestion, or absorption through the skin); magnitude or concentration (dose) of exposure; duration (e.g., minutes, hours, days, lifetime); and frequency (e.g., seasonal, daily, weekly, or monthly), play into the development of progressive and overt disease.
Likewise, personal factors that vary from one person to another may affect pathogenesis and must be considered. These include age, gender, ethnicity, nutritional status, personal habits and lifestyle, genetic makeup and host susceptibility, and the strength of individual defense mechanisms. The host-agent-environment interactions are immensely complex and poorly understood at this time.
Pathogenesis
Once a hazardous substance is released into the environment, it may be transported and transformed in a variety of complex ways. For example, a chemical may be modified by the environment before entering the body; transformed by chemical or biochemical processes; or undergo vaporization, diffusion, dilution, or concentration by physical or biologic processes. Plants and animals may accumulate small doses of a chemical agent and bioconcentrate them to the degree that they become hazardous when consumed by humans.
All cells respond to a variety of different adverse environmental stimuli with a cellular defense response now commonly referred to as the stress response. Molecules released by the cells in response to stress (e.g., hyperthermic shock, radiation, toxins, or viral infections) are called heat shock or stress proteins. Increased levels of these proteins after a cellular injury from any of the environmental hazardous agents seem to act as molecular chaperones that facilitate the synthesis and assembly of new reparative proteins.
Cells that produce high levels of stress proteins seem better able to survive ischemic damage; stress proteins may be influential in certain immunologic responses and may also be a requirement for cells to recover from a metabolic insult. This finding may lead to further research investigating the role of pharmacology in raising the levels of stress proteins to provide additional protection to injured tissues and organs. This therapeutic approach could have other applications outside environmental medicine such as to reduce tissue damage from surgery-induced ischemia or to help protect isolated organs used for transplantation, which often experience ischemia and reperfusion injury.49
Once some people are sensitized to chemicals, they develop increasingly severe reactions to more and more chemicals at smaller and smaller concentrations. The allergic response that occurs does not appear to be a typical response, perhaps suggesting altered immune system modulation. Immunologists have also discovered a possible connection between stress proteins and autoimmune disease, which may lead to preparations of specific protective vaccines.35,171
Chronic exposure to air particulate matter leads to inflammation and oxidative stress, precursors to pulmonary and cardiovascular diseases and cancer.123 Exposure to environmental pollutants has been linked with oxidative DNA damage in humans.147 Exposures are genotoxic and interfere with DNA repair and inhibit the cellular apoptosis needed to prevent cancer. Biomonitoring studies show that DNA damage is influenced by a variety of lifestyle and environmental exposures, including exercise, air pollution, sunlight, diet, and the chemical and physical agents discussed in this chapter.17,97,156
Clinical Manifestations
An environmental illness may manifest in a variety of ways. The illness may present as a newly developed clinical syndrome or an aggravation or change in a preexisting condition. The EPA identifies the following seven categories of human health effects from hazardous exposures46:
• Carcinogenicity: can cause cancer.
• Heritable genetic and chromosomal mutations: can cause mutations in genes and chromosomes that will be passed on to the next generation, such as caused by ionizing radiation.
• Developmental toxicity: can cause birth defects or miscarriages.
• Reproductive toxicity: can damage the ability of men and women to reproduce.
• Acute toxicity: can cause death from even short-term exposure to the lungs, through the mouth, or the skin.
• Chronic toxicity: can cause long-term damage other than cancer, such as liver, kidney, or lung damage.
• Neurotoxicity: can harm the nervous system by affecting the brain, spinal cord, or nerves.
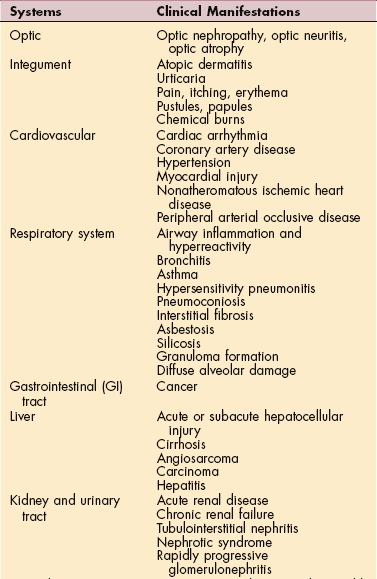
Local toxicities from exposure to environmental agents, such as ocular damage, mucous membrane complaints (eye, nose, and throat irritation), chemical burns to skin, noise-induced hearing loss, and vestibular disorders, can occur. Systemic toxicities can involve any organ system (Table 4-2). The clinical syndrome may mimic a wide range of psychiatric, metabolic, nutritional, inflammatory, and degenerative diseases.
Over the last 15 years, a new syndrome of environmental symptoms associated with chemicals, called multiple chemical sensitivity (MCS), has been observed both in the United States and in European countries. MCS is characterized by a chronic condition with symptoms that recur reproducibly in response to low levels of exposure to a wide variety of chemicals found in everyday substances, such as household cleaning agents, pesticides, fresh paint, new carpeting, synthetic building materials, newsprint, and perfume, and many other petrochemical products.
Symptoms occur in multiple organ systems and improve or resolve when irritants are removed.37 Two to four times as many cases of MCS exist among Gulf War veterans compared with undeployed controls121,157 (see the section on Gulf War Syndrome in this chapter). Objective physical findings and consistent laboratory abnormalities or biomarkers associated with MCS are typically nonexistent, leading some of the medical community to call this condition idiopathic environmental intolerance (IEI), a psychosomatic or neuropsychiatric disorder. Reported symptoms range from runny nose to difficulty breathing and heart palpitations but also include fatigue, headaches, weakness, malaise, decreased attention/concentration, memory loss, disorientation, confusion, and mood changes.
The treatment focus of this philosophy is to overcome the affected individual’s belief in a toxicogenic explanation for the symptoms,154 whereas other health care professionals are calling for accurate diagnostic assessment, agreement on the use of specific questionnaires, clinical and technical diagnostic procedures, and prospective clinical studies of people with MCS, comparative groups, and experimental approaches.5 All in all, the concept of MCS has ignited considerable controversy in the fields of medicine, toxicology, immunology, allergy, psychology, and neuropsychology.81
Neurotoxicity
Of particular interest to the therapist may be the effects of hazardous or toxic agents on the nervous system. Neurologic symptoms are common presenting symptoms in people seen by occupational and environmental health professionals. Cognitive difficulties, headaches, fatigue, dizziness, and limb paresthesias are often experienced, but these are nonspecific and seldom point to a single disease or cause.
Many toxins manifest as a nonspecific syndrome of distal sensorimotor impairment that is indistinguishable from the neuropathy caused by common systemic diseases (e.g., diabetes mellitus, vitamin B6 deficiency, alcoholism, or uremia). Toxins, such as lead, have a striking predilection for motor fibers and usually produce minimal sensory symptoms.
Neurologic symptoms that appear immediately after acute exposure are usually a result of the physiologic effects of the specific (usually chemical) agent. These symptoms subside with cessation of exposure and elimination of the compound from the body. By contrast, delayed neurologic disorders are generally a result of pathologic alterations of the nervous system.
Symptoms appear in a subacute manner over days or weeks after short-term exposure. In the case of long-term exposure, symptoms may appear insidiously and progress over many weeks or months. Recovery can be expected after cessation of exposure, but recovery is slow and depends on the extent of neuronal damage, the half-life of the chemical (i.e., continued exposure until the drug is out of the system), and the adverse effects of chelates used in the chemotherapy of metal poisoning.
Neurotoxicants do not cause focal (asymmetric) neurologic syndrome. Neurotoxins reach the nervous system by the systemic route and cause neurologic symptoms and deficits in a diffuse and symmetric manner, resulting in polyneuropathy. Any significant asymmetry in the presentation, such as weakness or numbness affecting one limb or one side of the body, is not likely to be attributed to neurotoxicity. Multiple neurologic syndromes are possible from a single toxin. Although the effects of neurotoxins are symmetric, neurons from different parts of the nervous system react differently to the agent.
Toxic polyneuropathy affects the distal limbs first, reflecting the greater vulnerability of the longest nerve axons. Sensory disturbances are usually reported as a tingling or burning sensation distributed in a stocking-and-glove pattern (see Fig. 39-5). The toes and the feet are affected first; hand symptoms are seldom present during the early stage. Involvement of the motor nerve fibers, if present, manifests first as atrophy and weakness of the intrinsic foot and hand muscles, bilaterally. More severe cases may present with footdrop or wristdrop, reflecting degeneration of motor axons to the lower leg and forearm muscles.
Neuropathic pain is commonly encountered in people with peripheral neuropathies regardless of the cause. In other words, pain patterns associated with chemically induced peripheral neuropathies do not differ significantly from the clinical picture of pain associated with neuropathy of other causes. Often this pain bears little relationship to the severity of neuropathy and may intensify during a period of recovery, or it may remit paradoxically as the neuropathy progresses, often with further loss of sensation. Pain is not a reliable indicator of neurologic progression or recovery.
MEDICAL MANAGEMENT
Clinical assessment may include assessing the details of exposure and correlating them with the medical condition. Various testing procedures may be developed on the basis of the historical information provided by the client. The clinical presentation, environmental history, and results of laboratory tests assist the physician in demonstrating a correlation between exposure and the clinical manifestations. Nerve conduction velocity (NCV) studies and electromyography (EMG) are the primary tools for the laboratory evaluation of neuromuscular disorders. A toxic polyneuropathy is characterized by a diffuse and relatively symmetric pattern of NCV abnormalities.
Removal from exposure and decontamination of the exposed victim are essential in the treatment of exposure-linked toxicity. Specific intervention protocols depend on the agent involved (e.g., pesticide poisoning requires symptom-specific therapy such as IV anticonvulsants to halt a seizure; antihistamines are used for allergic reactions), the particular organ system involved, and the presenting pathologic condition.
OCCUPATIONAL INJURIES AND DISEASES
Each year, millions of the estimated 140 million U.S. workers are injured on the job or become ill from exposure to hazards at work. These work-related injuries and illnesses result in substantial human and economic costs for workers, employers, and society; estimated direct and indirect costs of work-related injuries and illnesses are approximately $170 billion each year.159
Data collected through a National Electronic Injury Surveillance System (NEISS) report an estimated 3.4 million nonfatal injuries and illnesses among workers of all ages. More than three-fourths of all nonfatal workplace injuries/illnesses were attributed to contact with objects or equipment (e.g., being struck by a falling tool or caught in machinery), sprain or strain, and falls. Male workers under the age of 25 have the highest rate of workplace injuries.42
Approximately half of all injuries are sprains, strains, lacerations, amputations, punctures, and avulsions. Most sprains and strains affect the trunk (shoulder, back, chest, or abdomen) and lower extremities. The majority of lacerations, punctures, amputations, and avulsions affect the upper extremities. Dislocations and fractures account for approximately 7% of injuries and were attributed most often to falls.42
The lifetime cost of all injuries (including occupational and others) occurring in a single year in the U.S. totals an estimated $406 billion in medical expenses and productivity losses, including wages, fringe benefits, and the ability to perform normal household duties. The actual cost of these injuries is likely much higher when other related costs not included in the analysis are considered (e.g., police services, caregiver time, pain and suffering, decreased quality of life, or nonmedical expenditures such as wheelchair ramps or hand controls for vehicles).51
Computers and other time-saving devices have resulted in less physically demanding jobs, but new physical challenges and risk of impairments occur from incorrect ergonomics and prolonged (static) postures and positions, as well as repetitive motions. The prevalence of computers in modern society’s workplace and leisure activities has also contributed to the increase in the “weekend warrior syndrome,” or injuries to sedentary workers who go out on a weekend (or on an occasional basis during free time) and participate in sports or other strenuous physical activities. Overuse injuries and muscle strains are common, especially in the middle-aged and older adult. Activities, such as gardening, hiking, or household repairs, can be more strenuous than they seem in these age groups.77
Faster travel for business or pleasure in smaller spaces for long periods of time may also be contributing to an increase in injuries, deep vein thrombosis (DVT), or neck and back strain. Some individuals are at increased risk for these problems. For example, people are more prone to DVT if they have had a previous history of DVT, stroke, heart disease, or cancer. Anyone who has a neurologic disorder, lower extremity impairment, or mobility impairments may be at risk for DVT under these circumstances.77
Healthy People 2010 continues to maintain and work toward the goal of preventing injuries and illnesses by identifying risk factors, providing education, and developing effective safety strategies, including public health surveillance programs. Data collected and reported from death certificates, cancer registries, and hospital discharge data are occupational health indicators (OHI) used to identify risk factors and populations at risk. Worker’s compensation programs, the Bureau of Labor Statistics, and the U.S. Census provide additional information used in statistical analysis.
Risk Factors for Occupational Injury
Risk factors for musculoskeletal occupational injury have been identified by OSHA. If workers are exposed to two or more of these factors (Box 4-2) during their shift, they are at increased risk and require preventive intervention. Additionally, in April 2000, Congress adopted the Senior Citizens’ Freedom to Work Act that allows retired seniors to continue working without losing their Social Security benefits. The growing silver collar work force (adults of the baby boomer generation working past the age of 65) may represent a unique risk factor, since aging is associated with a progressive decrement in various components of physical work capacity, including aerobic power and capacity, muscular strength and endurance, flexibility and coordination, and the tolerance of thermal stress.142 Aging may thus contribute to additional workplace injuries and accidents.
Other risk factors in the general population may include psychosocial stress, gender, and personality. For example, psychosocial stress increases the physical demands of lifting for people with certain personality traits, making those people more susceptible to spine-loading increases and suspected low-back disorder risk.89
Obesity may also be a co-risk factor for the development of occupational asthma and cardiovascular disease that may modify the worker’s response to occupational stress, immune response to chemical exposures, and risk of disease from occupational neurotoxins. The interrelationship of work, obesity, and occupational safety and health is under further investigation.137
Ergonomics
Derived from the Greek terms ergon, meaning work, and nomos, meaning law, ergonomics is the study of work and of the relationship between humans and their working and physical environment. Over the last two decades, ergonomics has become a branch of industrial engineering that seeks to maximize productivity by minimizing worker discomfort and fatigue. Ergonomics is the science of fitting the task or the job to the worker.
Ergonomics is an interdisciplinary field of study that integrates engineering, medicine, and physical and behavioral management sciences and addresses issues arising from the interaction of humans in an increasingly technologic society. As a field of study, ergonomics deals with job design, work performance, health and safety, stress, posture, body mechanics, biomechanics, anthropometry (measurement of body size, weight, and proportions in relation to the task requirements), manual material handling, equipment design, quality control, environment, workers’ education and training, and employment testing.
The goal is to provide an environment that allows the individual to adequately absorb and dissipate forces placed on the body. Fitting the work to the worker makes it possible to enhance productivity while controlling errors and reducing musculoskeletal strain and fatigue. Ergonomics reduces risk factors known to contribute to occupational ergonomic-related injuries.
Humans have limitations arising from factors such as gender differences; differences in size, weight, and body proportions; aging; physical fitness and lifestyle choices; diet; stress; and pain and injury. Our abilities (and limitations), combined with the necessary acquired skills, determine how well we perform our daily tasks. Ergonomics helps people recognize their abilities and limitations for safe and effective performance within the environment. Work environments are often designed without adequate consideration for the people who will use them. Inadequate workplace design can contribute to stress, injury, pain, job-related impairments, disabilities, and subsequently, lost productivity. If products are designed without considering the human factor, health and safety hazards can occur.
A substantial body of validated scientific research and other evidence (epidemiologic, biomechanical, pathophysiologic studies) support the positive outcomes of ergonomic programs.103,107 The evidence strongly supports two basic conclusions: (1) a consistent relationship exists between musculoskeletal disorders and certain workplace factors, especially at higher exposure levels; and (2) specific ergonomic interventions (e.g., proper equipment, postural education, and use of correct body mechanics) can reduce these injuries and illnesses.
A new branch of ergonomists, rehabilitation ergonomists, are health care professionals who, in addition to functioning as an ergonomist practitioner, also use knowledge of the relationship between pathology and work to match the demands of the job to the capacity of the worker. Rehabilitation ergonomists work with people who do not fit the normal standards but require modification to safely and productively perform their job or task. Concentrating on improved safety focuses on physiologic improvement, which in turn increases productivity.
Ergonomic Certification
Certification as an ergonomist practitioner is available through two national boards: the Board of Certified Professional Ergonomists (BCPE) and the Oxford Research Institute (ORI). The ORI and BCPE are nonprofit board certification programs that are nationally and internationally recognized. Competency is demonstrated through experience, work samples, and a passing grade on a board examination. Previously, board certification in professional ergonomics accredited engineering ergonomists through a certification examination. Today, psychologists, therapists, and others have joined engineers in the pursuit of ergonomics as a career.
A wide range of private certification programs are available to the health care professional seeking training and certification as an ergonomist. The Occupational Injury Prevention and Rehabilitation Society (OIPRS) supports the accreditation of therapists through the BCPE and ORI but recognizes other programs that meet the minimum criteria for certification as an ergonomist. These criteria and a listing of ergonomic certification options for therapists are available.13,68 The orthopedic section of the American Physical Therapy Association (APTA) also has an occupational health special-interest group (SIG) with plans for credentialing occupational health physical therapists (Certification as an Occupational Health Specialist).
Occupational Injuries
The most common occupational injuries, referred to as musculoskeletal disorders (MSDs), involve cumulative trauma disorders caused by prolonged static positioning while using force (e.g., exerting constant force with the thumb pressed in while holding a computer mouse or constant gripping of tools or handles) and forceful repetition of work (repetitive strain injury) while using incorrect muscle groups or posture (e.g., keyboarding, meat cutting, or repetitive lifting and turning). The use of the term strain may be a misnomer because the symptoms occur in response to static muscle overload or maintenance of constrained postures rather than repetitive or dynamic muscle load.
Back injuries account for 60% of all work-related cases, and upper extremity injuries account for a majority of the remaining percentage. Seventy percent of the repeated trauma cases are in manufacturing industries.27 The shift in the U.S. economy to service industries, such as nursing homes and other long-term care facilities, in which staff members are required to perform heavy lifting, has contributed significantly to the number of back injuries.83 Other commonly sustained workplace injuries include eye injuries, hearing impairment, fractures, amputations, and lacerations severe enough to require medical intervention.
Musculoskeletal Disorders
MSDs encompass both cumulative trauma disorders (CTDs) and repetitive strain injuries (RSIs) and are more accepted terminology in the fields of ergonomics and occupational medicine, although the use of CTD and RSI is still often used in the literature. Work-related MSDs (WMSDs) are defined as an injury or disorder of the muscles, tendons, ligaments, cartilage, or spinal disks as diagnosed by a health care professional, resulting in a positive physical finding sufficient to require medical intervention and/or days away from work or assignment (i.e., an “OSHA-recordable” injury).113
MSDs do not include injuries resulting from slips, trips, falls, or accidents. The disorder must be directly related to the employee’s job and specifically connected to activities that form the core or a significant part of the job (e.g., a poultry processor might report tendinitis, but a back injury while occasionally changing the water bottle would not be covered).113
WMSDs account for more than one-third of all occupational injuries that are serious enough to result in days away from work. Back injuries and carpal tunnel syndrome (CTS) are the most prevalent, most expensive, and most preventable MSDs. Each year more than 100,000 women experience work-related back injuries that cause them to miss work. It is estimated that 300,000 injuries and $9 billion in worker’s compensation can be saved with improved industry safety and ergonomic practices.
Etiology and Risk Factors
Risk factors for MSDs are divided into four major categories: genetic, morphologic, biomechanical, and psychosocial. Among the various biomechanical risk factors, exposure to repetitive, static, and vibratory activities is known to result in MSDs.80 Differences in physical, occupational, and physiologic factors may contribute to MSDs. For example, CTS is associated with pregnancy, as well as rheumatoid arthritis, which is a condition that affects women more often than men. Women comprise 70% of the CTS cases and 62% of tendinitis cases that are serious enough to warrant time off work.112
CTS accounts for more days away from work than any other workplace injury. In addition to workers who spend hours at the computer, CTS has been reported in meat packers, assembly line workers, jackhammer operators, athletes, physical and occupational therapists, and homemakers. In both genders, CTS can be associated with other medical conditions, such as thyroid problems, liver disease, multiple myeloma, and diabetes, as well as with other musculoskeletal disorders that may or may not be work-related (see Box 39-1). For all work-related CTS, poor worksite design, poor posture and body mechanics, and industrial equipment and computers that take out the automatic pauses of work must be evaluated as possible contributors. An in-depth discussion of CTS is included in Chapter 39.
Pathogenesis
The exact pathomechanisms of MSDs remain obscured because of the difficulty of analyzing tissues of individuals in the early stages of work-related MSDs. Tissue injury caused by repeated motion may involve an inflammatory response, but why one worker develops symptoms while others doing the same task do not remains unknown and a topic of discussion and study. The relationship between repetition rate, forcefulness of tasks, cellular responses to these activities, number of strains, and inflammatory response is under investigation. The role of genetics and psychosocial factors is also being considered.9,10,153
It is likely that the development of MSDs is multifactorial, with variations in individual tissue tolerances. Each individual may have his or her own threshold below which tissue integrity is preserved and above which injury results. It is possible that the combined and/or accumulative effects of risk factors for MSD can exceed tissue tolerance capacity and cause injury. When continued task performance is superimposed on injured and inflamed tissues, a cycle of injury, inflammation, and motor dysfunction occurs.9,10
MSDs in the lumbar spine may have a different mechanism. Static lumbar loading applied to ligaments results in creep (e.g., stretch of viscoelastic tissue over time that is not fully restored immediately after load removal). In theory, ligaments that remain stretched beyond their resting length may result in increased laxity of intervertebral joints and risk of instability and injury. In the spine, ligaments have a secondary role in maintaining intervertebral stability.150
Static lumbar flexion under constant load results in long-lasting viscoelastic creep that does not fully recover after 7 hours of rest. The creep developed gives rise to a neuromuscular disorder with reduced reflexive muscle activity, muscle spasms during flexion, and hyperexcitability of muscle activity during rest that may last 24 hours or more. The viscoelastic creep and associated neuromuscular disorder can occur even with low loads, which may help explain how cumulative low back problems develop.150
Clinical Manifestations
Workers suffering from MSDs, especially upper extremity MSDs (UEMSDs), may experience decreased grip strength and range of motion, impaired muscle function, and inability to complete activities of daily living (ADLs). Symptoms are persistent (although intermittent, they return and progress over time) and most commonly include pain (e.g., headache, neck, back, shoulder, wrist, hip, or knee); burning sensation, numbness, and/or tingling (hands or feet); Raynaud’s phenomenon; and myalgias and arthralgias with spasm, stiffness, swelling, or inflammation.
Neural tissues at the cervical spine, carpal tunnel, cubital tunnel, or thoracic outlet can be compressed as a result of the swelling associated with the biomechanical microtrauma. The individual may perceive weakness and drop objects or have difficulty with handwriting. Common MSDs/UEMSDs are listed in Box 4-3.
A predictable sequence of events leads up to MSDs of a repetitive nature or those caused by static postures (e.g., some tasks such as prolonged writing or typing at a keyboard require co-contraction of the agonists and antagonists). Fatigue and the inability to recover from fatigue brought on by additional hours and pressured deadlines, combined with emotional stress and improper posture, improper use of tools, or an ergonomically inadequate workstation, result in muscle soreness.
Over time and without intervention or a change in the contributing factors, the body strains to keep up and pain develops, followed by injury or trauma. In the case of tendinitis or focal hand dystonia, it is possible that a sensory problem rather than just a motor problem occurs and is caused by a dysfunction in cortical sensory processing.29 Evidence suggests that aggressive sensory discriminative training complemented by traditional exercises to facilitate musculoskeletal health can improve sensory processing and motor control.28
Occupational Burns
Of the more than one million firefighters employed in the United States, 300,000 are career firefighters. The rate of injury and death occurring on the fire ground or while responding to or returning from an incident has declined since the late 1980s with the mandatory use of gloves, self-contained breathing apparatus (SCBA), and full personal protective clothing. National trends for firefighter injuries are sprain/strain-and stress-related injuries. Over 50% of all injuries involve overexertion, lifting, pulling, or carrying hose and equipment. Studies support the long-standing assertion that the number of firefighters responding to a fire is a factor that affects injuries.167
Aside from the acute injurious effects of fire, clinicians must be alert to the pathophysiologic changes associated with exposure to heat and smoke and to the chronic sequelae, both physical and psychologic (Table 4-3). In addition to the management of burns and trauma, it is necessary to evaluate clients for all acute systemic effects of exposure to smoke, heat, or toxic substances; recognize toxic effects that may be obscured by more serious traumatic effects; be alert for delayed consequences; and recognize acute and chronic exposure and health effects as a result of toxic chemicals in smoke, especially among firefighters.
Table 4-3
Types of Fire-and-Rescue–Related Acute and Chronic Injury
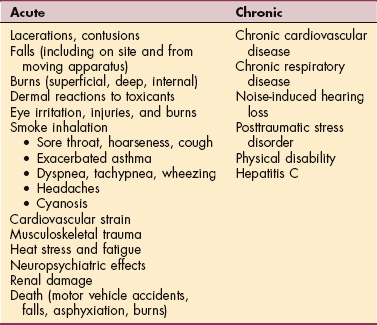
Modified from NIOSH Fire Fighter Fatality/Injury Investigation Reports (http://www.cdc.gov/niosh/firehome.html, 2001).
Carbon monoxide is always present at fires. Smoldering fires with incomplete combustion of burning material can lead to significant levels of CO. For this reason, firefighters are required to wear SCBA at every incident. Respiratory responses of firefighters while wearing SCBA will reduce their breathlessness during exercise (exertion on the job).43
Occupational Pulmonary Diseases
Materials inhaled in the workplace can lead to all the major chronic lung diseases, except those as a result of vascular disease. Exposure in office buildings and hospitals is now included as a known workplace-related cause of disease. As new industries are developed, new problems are reported. For example, obstructive lung disease has been reported in workers in the microwave popcorn and flavor-manufacturing business who have not been adequately protected from chemical exposures.91
Identifying the source of illness is important because it can lead to cure and prevention for others.15 Disorders caused by chemical agents are classified as (1) pneumoconioses, (2) hypersensitivity pneumonitis, (3) obstructive airway disorders, (4) toxic lung injury, (5) lung cancer, and (6) pleural diseases. These conditions are discussed more fully in Chapter 15.
Asbestos and other silicates, such as kaolin, mica, and vermiculite, can cause pneumoconiosis. Asbestos-induced diseases cause lung inflammation and fibrosis as a result of activation of alveolar macrophages. Coal worker’s pneumoconiosis is another parenchymal lung disease caused by inhalation of coal dust.
Hypersensitivity pneumonitis has many other names, such as extrinsic allergic alveolitis, farmer’s lung, and detergent worker’s lung, and is characterized by a granulomatous inflammatory reaction in the pulmonary alveolar and interstitial spaces. Silicosis is a parenchymal toxic lung disease caused by inhalation of crystalline silica, a component of rock and sand. Workers at risk include miners, tunnelers, quarry workers, stonecutters, sandblasters, foundry workers, glass blowers, and ceramic workers.
The pathogenesis of these occupational lung diseases varies among different pneumoconioses, but the bottom line is that cilia and mucus-secreting cells are absent in the small bronchioles and alveoli. The body depends on macrophages to remove any of the tiny particles that lodge in these areas. The macrophages then carry them to the mucociliary elevator or dump them into the lymphatics. The process is often sabotaged because substances, such as silica dust, can destroy the macrophages. In the process, substances are released that trigger inflammation and pulmonary fibrosis. See Chapter 15 for more details about these diseases.
Exposure to allergens and irritants has resulted in the recognition of a new disease called work-related upper airway disease or united airway disease, which although not life-threatening, has been reported to cause sufferers to experience reduced quality of life. Occupational allergens identified are many and varied, including plants (e.g., tobacco leaf dust, grapes, asparagus, or flowers), insects (e.g., bees or locusts), powder paints, and others. Reports of upper airway disease in various occupational groups involved in rescue, recovery, and cleanup at the World Trade Center identified a new work hazard from irritants.169
Health problems caused by these irritants range from runny nose to full-blown allergic rhinitis. Up to 40% of individuals in the workplace with allergic rhinitis also have asthma. The link between rhinitis and asthma is the presence of inflammation of the nasal and bronchial mucosae.169
Occupational asthma or work-related asthma (WRA) (airway obstruction) is asthma that is attributable to or is made worse by environmental exposures (e.g., inhaled gases, dusts, fumes, or vapors) in the workplace. The air in health care institutions may contain irritating and sensitizing chemicals and particles that can aggravate asthma (Box 4-4).
WRA has become the most prevalent occupational lung disease in developed countries, is more common than is generally recognized, and can be severe and disabling. The reactions can be immediate or delayed, sometimes hours after leaving the workplace. Identification of workplace exposures causing and/or aggravating the asthma and appropriate control or cessation of these exposures can often lead to reduction or even complete elimination of symptoms and disability.55
OSHA requires employers to provide a safe and healthy work environment free from recognized hazards. In addition, the Americans with Disabilities Act of 1990 requires employers to accommodate workers with asthma. Suspected episodes of WRA should be documented, including symptoms, suspected exposures, visits to health services, and similar symptoms reported by other employees. Many effective and appropriate substitutions and controls are available that can be incorporated to eliminate or prevent airborne and topical exposures.7
Occupational Cancer
Despite increased knowledge of occupational risk for cancer, it is estimated that 30% to 40% of the population in the industrialized world will develop malignant disease during their lifetime. Changes in wood processing and decreased duration of occupational exposure because of more frequent job changes may have altered the picture somewhat.
Studies continue to provide evidence that cancer in humans has environmental causes (e.g., exposure to arsenic is associated with increased risk of skin, urinary bladder, and respiratory tract cancers; chronic exposure to ultraviolet light is associated with skin cancer; vinyl chloride is associated with liver cancer; dry cleaning solvents are associated with kidney and liver cancer and non-Hodgkin’s lymphoma). Research is ongoing to assess combined genetic and environmental contributions to risk.44,69,131
Alteration or mutation in the genetic material (deoxyribonucleic acid [DNA]) may occur as a result of exposure to carcinogenic chemicals or radiation. Both experimental animal models of cancer and the study of human cancers with known causes have revealed the existence of a significant interval between first exposure to the responsible agent and the first manifestation of a tumor. This period is referred to as the induction period, latency period, or induction-latency period.
For humans, the length of the induction-latency period varies from a minimum of 4 to 6 years for radiation-induced leukemias to 40 or more years for some cases of asbestos-induced mesotheliomas. For most tumors, the interval ranges from 12 to 25 years; such a long period may easily obscure the relationship between a remote exposure and a newly discovered tumor.
In the future, individuals with a high environmental risk of developing cancer may benefit from immune stimulation as a means of cancer prevention by inducing specific immunity through the use of vaccines.52 Individual cancers and their treatment are discussed in organ-specific chapters in this text; see also Chapter 9.
Acute Radiation Syndrome
Acute radiation syndrome is caused by brief but heavy exposure of all or part of the body to ionizing radiation. The radiation disrupts chemical bonds, which causes molecular excitation and free radical formation. Highly reactive free radicals react with other essential molecules, such as nucleic acids and enzymes, and this in turn disrupts cellular function.
The clinical presentation and severity of illness depend on many factors, including volume of tissue treated, the dosage (fractionation), and other independent variables. Tissues with the most rapid cellular turnover are the most radiosensitive and include reproductive, hematopoietic, and gastrointestinal tissues. See the section on Physical Agents in this chapter and also the section on Radiation Injuries in Chapter 5.
Occupational Infections
Occupational infections are diseases caused by work-associated exposure to microbial agents, including bacteria, viruses, fungi, and protozoa. Occupational infections are distinguished by the fact that some aspect of the work involves contact with a biologically active organism. Occupational infection can occur after contact with infected people, as in the case of health care workers; infected animal or human tissue, secretions, or excretions, as in laboratory workers; asymptomatic or unknown contagious humans, as happens during business travel; or infected animals, as in agriculture (e.g., brucellosis). Tuberculosis, herpes simplex and herpes zoster (shingles), hepatitis, and AIDS are the most likely occupational infections encountered in a therapy practice.
Occupational Skin Disorders
Accounting for 20% of all cases of occupational disease in the United States, 61,000 new cases of occupational skin disease are reported each year. It is likely that many cases of work-related skin disorders are underreported, since it is often not a life-threatening condition and never diagnosed or treated. The health care industry reports 4000 cases of skin illness each year, but the highest rates are in agriculture and manufacturing.
Dermatoses are more prevalent in some states such as California and Florida; contact dermatitis from plants, especially in combination with sunlight, and chemicals, such as pesticides or fertilizers, is common among agricultural workers. Contact dermatitis (acute, chronic, or allergic) is the most common of occupational skin disorders, but other types include contact urticaria, psoriasis, scleroderma, vitiligo (areas of depigmentation), chloracne (see Fig. 4-1), actinic skin damage known as farmer’s skin or sailor’s skin, cutaneous malignancy, and cutaneous infections.
Other agents in the workplace include irritating chemicals such as solvents, cutting oils, detergents, alkalis, and acids. Arsenic and tar products can increase the risk of cancer either alone or in combination with sunlight. Skin cancer is an important occupational illness and is most often the result of excessive exposure to ultraviolet light; farmers, fishermen, roofers, and road workers who continuously work in the sun are at greatest risk. For further discussion of specific skin disorders, see Chapter 10.
Rubber Latex Allergy
During the recent past, the incidence of natural rubber latex allergy (LA) has dramatically increased not only among the general population but also among health care workers, the latter because of repeated contact as a result of standard precautions and subsequent increased occupational exposure.
LA occurs predominantly in certain high-risk groups (Box 4-5); the estimated prevalence in health care workers varies widely (2.8% to 18%), and studies do not always distinguish between those who are positive in an assay for latex-specific immunoglobulin E (IgE) and those with clinical allergy.120 The prevalence of LA in the general population ranges from 0.1% to 1.0%, compared with as high as 60% for those with spina bifida or other chronic medical conditions associated with repeated exposure to latex.102
This occupational sensitivity to natural rubber latex (NRL) (i.e., latex proteins and in some cases the associated cornstarch glove powder serve as a carrier for the allergenic proteins from the NRL) has resulted in the following three types of reactions:
• Immediate hypersensitivity (type I hypersensitivity; IgE-mediated) with urticaria (hives), watery eyes, rhinitis, respiratory distress, and asthma or skin rash, which can spread from the hands, up the arms, and to the face (it can also cause swelling of the lips, eyes, ears, and larynx [laryngeal edema can prevent the person from speaking]).
• Irritation or irritant contact dermatitis manifested as dry, crusty, hard bumps; sores; and horizontal cracks on the skin (Fig. 4-4)
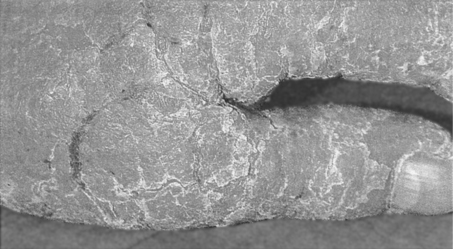
Figure 4-4 Rubber glove dermatitis. (From Raffle PAB, Adams PH: Hunter’s diseases of occupations, ed 8, London, 1994, Edward Arnold.) Edward Arnold
• Mild-to-severe allergic contact dermatitis (delayed type IV hypersensitivity; cell-mediated) (Fig. 4-5)
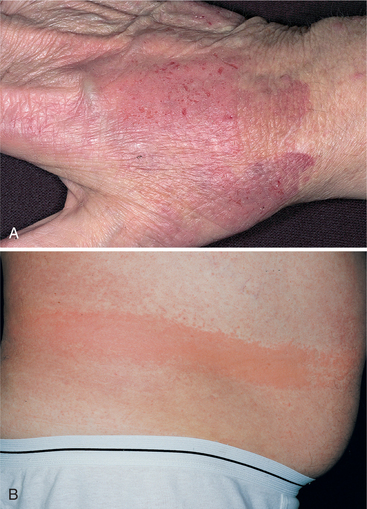
Figure 4-5 Latex allergy dermatitis. A, Latex glove allergy should be suspected in health care workers who present with eczema, blistering, or skin peeling anywhere on the hands. B, Allergy to the rubber band of underwear. Washing clothes with bleach may make the rubber allergenic. Similar skin reactions can be seen in women across the midback under the bra strap (not shown). (From Habif TP: Clinical dermatolog y, ed 4, St Louis, 2004, Mosby.)
The first two reactions are related to mechanical and chemical exposure, whereas LA is caused by sensitization to the proteins in NRL. These responses occur when items containing latex touch the skin, mucous membranes (eyes, mouth, nose, genitals, bladder, or rectum), or open areas.
Latex exposure has become one of the leading causes of occupational asthma. Once sensitized, some health care workers are at risk for severe systemic allergic reactions, which can be fatal in some cases. In susceptible individuals, airways react to low levels of a variety of sensitizers and irritants in the environment. The two major routes of exposure include dermal exposure and inhalation exposure. NRL protein absorption is enhanced when perspiration collects under latex clothing articles (e.g., elastic waistbands and leg bands in underwear). However, the elimination of wearing latex gloves has not been successful in eliminating latex sensitization, since latex allergens are airborne.
Exposure by the respiratory route occurs when the NRL protein becomes airborne, especially since glove powder becomes airborne, acting as a carrier for the NRL protein when gloves are donned or removed.
Latex-induced rhinitis and occupational asthma are new forms of occupational illness secondary to airborne latex allergens in operating rooms, intensive care units, and dental suites. Anyone with latex allergies should be treated as the first case of the day, whether in the operating room or in a therapy department, to avoid latex in the air and to avoid introducing any latex from clothes or materials from previous contacts.
4-3 SPECIAL IMPLICATIONS FOR THE THERAPIST
Possible patterns related to latex-induced asthma:
6B, 6C, 6F, 6G, 6H, or 6I
All clients should be screened for known LA or risk factors on admission. It is not enough to ask if someone is allergic to latex; risk factors and past medical history must be assessed. This is especially important because anaphylaxis could be the first sign of LA. If anyone in the rehabilitation or therapy department develops symptoms in association with the use of latex gloves, emergency medical care may be required. The presence of hives, perioral itching, respiratory distress, watery eyes, and facial swelling may indicate a type I hypersensitivity response and requires immediate medical attention. In a hospital setting, a physician can be paged immediately; other locations may require an emergency medical team (calling 911 or an emergency medical service). Check with the facility for incident report requirements.
For the health care worker with a known sensitivity, a medical-alert bracelet should be worn, and the individual should have autoinjectable epinephrine (EpiPen) for use if another reaction occurs. Anyone experiencing the first reaction should not ignore the symptoms; further episodes must be avoided by developing a latex-safe environment and using nonlatex products.
All clients with myelomeningocele are to be treated as if latex allergic. The therapist, family members, and caregivers must avoid using toys, feeding utensils, pacifiers, nipples, or other items made of latex that the infant or child might put in the mouth. Clothes and shoes with elastic anywhere must be avoided. Parents must be advised to read all labels and avoid all items containing latex. If no indication of latex content is evident, the manufacturer should be contacted for verification before purchase or use of the item. More information on this topic is available at the web site Exceptional Parent (http://www.eparent.com/toys/latex.htm) or the American Latex Allergy Association (www.latexallergyresources.org).
A latex-safe environment may be required for complete recovery for people with LA and is essential for all pediatric cases and anyone with known LA. A latex-safe environment, including the operating room, is described as one in which no latex gloves are used by any personnel, no direct client contact with latex devices (e.g., catheters, condoms, diaphragms, adhesives, tourniquets, rubber backing on bath mats or other materials, hot water bottles, or anesthetic equipment) occurs; and all medical and patient/client care items have been assessed for latex and labeled.
Handwashing before donning and after removing gloves must be carried out at all times with special care given to using a pH-balanced soap and rinsing well to remove all residue. All medical products containing NRL that could come in contact with clients must be labeled. Keep in mind that many latex-free supplies have packaging that contains latex (glue), and those workers in the production or packaging of these products may have worn latex gloves.
No latex balloons or toys containing latex should be allowed in health care facilities; crash carts should be latex free. Personnel in the therapy department must be aware of the many items in the department that contain latex and replace these with latex-free products or a latex-free barrier (Table 4-4). Almost all equipment, supplies, and personal protective equipment is available in latex-free form, although not by all manufacturers. Complete guidelines for prevention and protection are available through the American Nurses Association at (800) 274-4ANA.
Table 4-4
Potential Sources of Latex in a Rehabilitation Department*
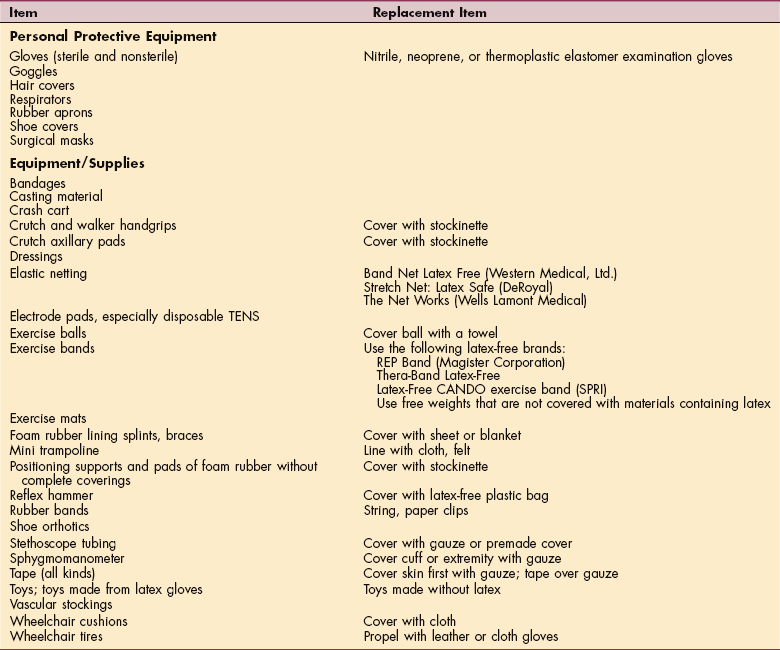
TENS, Transcutaneous electrical nerve stimulation.
*Many manufacturers now make latex-free items. Any medical supply with latex must be so marked.
Courtesy Harriett B. Loehne, PT, DPT, CWS, FCCWS.
Several potential sources of powder-free, natural hypoallergenic latex gloves may be tolerated by latex-sensitive individuals, but no single replacement glove has been found for all people affected. Cotton liners or barrier creams can be effective interventions. Vinyl gloves are generally less protective than latex and more prone to tearing. Some of the new synthetic materials, such as nitrile, neoprene, and thermoplastic elastomer, offer equal or superior barrier protection and durability and are a reasonable alternative to latex or vinyl, offer better protection than latex types when handling lipid-soluble substances and chemicals, and are reasonably priced.128
However, like latex, synthetic glove products can cause allergic reactions because they may contain chemical additives similar to those found in latex and both are manufactured using the same process, called vulcanization. Additionally, synthetic gloves also provide a poorer fit than their latex counterpart and come with environmental concerns (e.g., the production and disposal of vinyl gloves releases toxic substances, such as dioxins, into the environment).
Glove specifications (e.g., leak defect rate; American Society for Testing and Materials [ASTM] specifications for length, width, tensile strength, thickness; powder particulate weight per glove; and protein levels) are available and should be examined by each health care provider according to facility or client-based use.172 For more information, see NIOSH Alert: Preventing Allergic Reactions to Natural Rubber Latex in the Workplace (800-35-NIOSH) or OSHA: Technical Information Bulletin—Potential for Allergy to Natural Rubber Latex Gloves and Other Natural Rubber Products (http://www.osha.gov/dts/tib/tib_data/tib19990412.html)
Military-Related Diseases
Seven diseases (asthma, laryngitis, chronic bronchitis, emphysema, and three eye ailments) have been identified by the Department of Veterans Affairs for compensation as a result of exposure to toxic chemicals during World War II.
Survivors of the Vietnam War who have been exposed to a dioxin (2,3,7,8-tetrachlorodibenzo-para-dioxin [TCDD]) contained in the herbicide mixture Agent Orange (sprayed from the air, by boat, and on the ground in Vietnam to defoliate jungles from 1962 to 1971) are known to be at risk for diabetes and chronic lymphocytic leukemia. The risk for other types of cancer has never been conclusively proven, but as Vietnam veterans continue to age, additional research will yield more information about cancer risk.56
There has been concern about reproductive effects of Agent Orange such as birth defects in the children of exposed veterans. Neural tube defects, neurotoxicity, neuropsychiatric dysfunction, deficits in motor function, and peripheral neuropathy may be linked to Agent Orange exposure but considerable uncertainty exists about these associations.56
More recently, a group of symptoms presented by participants in the Gulf War have been identified. ALS, or Lou Gehrig’s disease, has been identified among these military personnel. The U.S. government confirmed this link in December 2001. Anyone seeking more information about either Agent Orange or the Gulf War Syndrome can contact the Gulf War/Agent Orange Helpline at (800) PGW-VETS.
Gulf War Syndrome
Overview.: Regardless of whether an actual Gulf War syndrome (GWS) exists, it remains a hotly debated topic. According to the Centers for Disease Control and Prevention (CDC), Americans who served in the Persian Gulf War are significantly more likely than others to experience more than a dozen disorders known generically as GWS. The CDC does not term this phenomenon GWS but reports that people who went to the Persian Gulf are experiencing problems (referred to as Persian Gulf illness [PGI]) that those who did not go are not experiencing. However, the Department of Defense does not support the existence of this illness, reporting only that the results of medical examinations of 10,000 veterans and family members affected revealed multiple illnesses with overlapping symptoms.78
Incidence and Clinical Manifestations.: Of the 700,000 troops dispatched to the Persian Gulf between August 1990 and June 1991, as of January 2007, more than 100,000 veterans have filed with the federal registry reports of symptoms that include (in order of frequency) fatigue, skin rash, headache, muscle and joint pain, memory loss, shortness of breath, sleep disturbances, diarrhea and other gastrointestinal symptoms, and depression. CDC data show that GWS affects 27% of veterans compared with 2% of nonveterans. Fatigue has been reported to affect 54% of Gulf War veterans compared with 16% of non–Gulf War veterans.
Etiologic Factors.: No single cause has been identified, but possible factors include chemical or biologic weapons used on allied forces, insecticides, oil well fires in Kuwait, nerve agents from the demolition of Iraqi chemical weapons, parasites, pills protecting against nerve gas, and inoculations against petrochemical exposure administered by the military that had unexpected side effects or reacted with one another to create adverse symptoms.
In 1993, the Birmingham, Alabama Veterans Administration Center was designated as a national pilot center to study the possible neurologic effects of exposure to environmental agents in the Persian Gulf. Other designated environmental hazards research centers are located in Boston; East Orange, NJ; and Portland, OR.
Pathogenesis.: The pathogenesis for GWS remains unknown but researchers are investigating the similarities between the underlying mechanisms of chronic fatigue syndrome, fibromyalgia, migraine headaches, and GWS. MRI studies of veterans with different GWS have biochemical evidence of neuronal damage in different distributions in the basal ganglia and brainstem, supporting the theory of neurologic toxicity related to chemically induced injury to dopaminergic neurons in the basal ganglia.65,66
A new theory, referred to as toxicant-induced loss of tolerance (TILT), has been suggested. Drug addiction and multiple chemical intolerance (“abdiction”) appear to be polar opposites (addiction is characterized by craving and dependency, abdiction is characterized by aversion); however, when compared side-by-side, common underlying mechanisms are observed.
Both addiction and chemical intolerance involve a fundamental breakdown in innate tolerance, resulting in an amplification of various biologic effects, particularly withdrawal symptoms. Although addicts seek further exposures to avoid unpleasant withdrawal symptoms, chemically intolerant individuals avoid exposure to reduce unpleasant symptoms. The question of whether addictive drugs and environmental pollutants initiate an identical pathogenic process with triggered symptoms and cravings remains under investigation.96
MEDICAL MANAGEMENT
No specific intervention beyond management and symptomatic measures exists for PGI. Focusing on triggering events rarely helps define treatment for people with syndromes such as GWS. Understanding the entire spectrum of illnesses from chronic fatigue syndrome to fibromyalgia to GWS in light of treatment must be the means to developing multidisciplinary treatment programs for affected people that includes allopathic, naturopathic, and alternative treatment.
Iraqi War
Veterans of Operations Enduring Freedom and Iraqi Freedom (OEF/OIF) have endured high combat stress and are at risk for posttraumatic stress disorder (PTSD) and psychosocial problems.139 During deployment, there were reports of heat illness despite predeployment efforts to prepare soldiers. Extreme temperatures averaging 46° C still resulted in a heat illness rate of 50/1000 during the first 10 to 14 days of deployment.20 There have been no reports of long-term results from this problem.
References
1. Abelsohn, A. Identifying and managing adverse environmental effects: outdoor air pollution. CMAJ. 2002;166(9):1161–1165.
2. Adir, Y, et al. Effects of exposure to low concentrations of carbon monoxide on exercise performance and myocardial perfusion in young healthy men. Occup Environ Med. 56(8), 1999. [535-535].
3. Alarcon, WA. Acute illnesses associated with pesticide exposure at schools. JAMA. 2005;294(4):455–465.
4. Alfred, EN. Short-term effects of carbon monoxide exposure on the exercise performance of subjects with coronary artery disease. N Engl J Med. 1989;321:1426.
5. Altenkirch, H. Multiple chemical sensitivity (MCS)-differential diagnosis in clinical neurotoxicology: a German perspective. Neurotoxicology. 2000;21(4):589–597.
6. American Physical Therapy Association (APTA) Occupational Health Guidelines 2007. Available on-line at http://www.apta.org Accessed April 23, 2007.
7. Bain, EI. Perils in the air: avoiding occupational asthma triggers in the workplace. AJN. 2000;100(6):88.
8. Bainbridge, D. OSHA standards call for ergonomics in the workplace. PT Magazine. 2001;9(1):61.
9. Barr, AE, Barbe, MF. Inflammation reduces physiological tissue tolerance in the development of work-related musculoskeletal disorders. J Electromyogr Kinesiol. 2004;14(1):77–85.
10. Barr, AE, Barbe, MF. Pathophysiological tissue changes associated with repetitive movement: a review of the evidence. Phys Ther. 2002;82(2):173–187.
11. Barr, DB. Biologic monitoring of exposure to environmental chemicals throughout the life stages: requirements and issues for consideration for the National Children’s Study. Environ Health Perspect. 2005;113(8):1083–1091.
12. Barwick, RS, et al. Surveillance for waterborne-disease outbreaks-United States, 1997-1998. MMWR. 2000;49(4):1–21.
13. Bassett, J, Ergonomics, to the letter. ADVANCE Physical Therap PT Assist. 2004;15(7):37–38. Available on-line at http://www.advanceweb.com. Accessed April 23 2007.
14. Bassett, J. Silver collar workers seek silver dollar paychecks. ADVANCE Physical Therap PT Assist. 2001;12(2):9–10.
15. Beckett, WS. Occupational respiratory diseases. N Engl J Med. 2000;342(6):406–413.
16. Bertam, JS. The molecular biology of cancer. Mol Aspects Med. 2000;21(6):167–223.
17. Bertin, G, Averbeck, D. Cadmium: cellular effects, modifications of biomolecules, modulations of DNA repair and genotoxic consequences (a review). Biochimie. 2006;88(11):1549–1559.
18. Betts, GA, et al. Neck muscle vibration alters visually-perceived roll after unilateral vestibular loss. Neuroreport. 2000;11(12):2659–2662.
19. Binkley, HM. National Athletic Trainers’ Association Position Statement: Exertional heat illnesses. J Athletic Trng. 2002;37(3):329–343.
20. Bolton, JP. Heat illness on Operation Telic in summer 2003: the experience of the Heat illness treatment unit in northern Kuwait. JR Army Med Corps. 2006;152(3):148–155.
21. Bolton, JP. Magnetic fields and mammary cancer in rodents: a critical review and evaluation of published literature. Radiat Res. 2000;153(5 Pt 2):617–626.
22. Bork, BE. Work-related musculoskeletal disorders among physical therapists. Phys Ther. 1996;76:642–652.
23. Bosco, C, et al. Hormonal responses to whole-body vibration in men. Europ J Appl Physiol. 2000;81(6):449–454.
24. Brook, RD. Air pollution and cardiovascular disease: a statement for healthcare professionals from the expert panel on population and prevention science of the American Heart Association. Circulation. 2004;109(21):2655–2671.
25. Brook, RD. You are what you breathe: evidence linking air pollution and blood pressure. Curr Hypertens Rep. 2005;7(6):427–434.
26. Brutsaert, TD, et al. Higher arterial oxygen saturation during submaximal exercise in Bolivian amara compared to Europeans born and raised at high altitude. Am J Phys Anthropol. 2000;113(2):169–181.
27. Bureau of Labor Statistics (BLS) Injuries, illnesses, and fatalities 2005. Available on-line at http://stats.bls.gov/ Accessed April 23, 2007.
28. Byl, NN. A primate model for studying focal dystonia and repetitive strain injury: effects on the primary somatosensory cortex. Phys Ther. 1997;77(3):269–284.
29. Byl, NN, McKenzie, A. Treatment effectiveness for patients with a history of repetitive hand use and focal hand dystonia: a planned, prospective follow-up study. J Hand Ther. 2000;13(4):289–301.
30. Calafat, AM. Serum concentrations of 11 polyfluoroalkyl compounds in the U.S. population: data from the national health and nutrition examination survey (NHANES). Environ Sci Technol. 2007;41(7):2237–2242.
31. Calvert, GM. Acute pesticide poisoning in the U.S. retail industry. Public Health Rep. 2007;122(2):232–244.
32. Calvert, GM. Lead exposure among females of childbearing age in the United States. MMWR. 2007;56(16):397–400.
33. Canfield, RL. Intellectual impairment in children with blood lead concentrations below 10 micrograms. N Engl J Med. 2003;348(16):1517–1526.
34. Centers for Disease Control and Prevention (CDC) Extreme heat: a prevention guide to promote your personal health and safety. Available on-line at http://www.bt.cdc.gov/disasters/extremeheat/heat_guide.asp Accessed April 21, 2007.
35. Clark, JI, Muchowski, PJ. Small heat-shock proteins and their potential role in human disease. Curr Opin Struct Biol. 2000;10(1):52–59.
36. Cohen, JT, Graham, JD. A revised economic analysis of restrictions on the use of cell phones while driving. Risk Anal. 2003;23(1):5–17.
37. Consensus Statement. Multiple chemical sensitivity: a 1999 consensus. Arch Environ Health. 1999;54(3):147–149.
38. Cromie, JE. Work-related musculoskeletal disorders and the culture of physical therapy. Phys Ther. 2002;82(5):459–472.
39. Cromie, JE, Robertson, VJ, Best, MO. Work-related musculoskeletal disorders in physical therapists: prevalence, severity, risks, and responses. Phys Ther. 2000;80(4):336–351.
40. Davis, S, Mirick, DK. Residential magnetic fields, medication use, and the risk of breast cancer. Epidemiology. 2007;18(2):266–269.
41. Degen, GH, Bolt, HM. Endocrine disruptors: update on xenoestrogens. Int Arch Occup Environ Health. 2000;73(7):433–441.
42. Derk, SJ. Nonfatal occupational injuries and illnesses in the United States. MMWR. 2007;56(16):393–397.
43. Donovan, KJ, McConnell, AK. Do fire-fighters develop specific ventilatory responses in order to cope with exercise whilst wearing self-contained breathing apparatus? Eur J Appl Physiol Occup Physiol. 1999;80(2):107–112.
44. Dooley, MA. Epidemiology and health services: year in review. Curr Opin Rheumatol. 2007;19(2):118–121.
45. Eis, D. Clinical ecology-an unproved approach in the context of environmental medicine. Zentralbl Hyg Umweltmed. 1999;202:291–330.
46. Environmental Protection Agency (EPA) Categories of released chemicals reported to the toxic release inventory, 2006. Available on-line at http://www.epa.gov Accessed April 23, 2007.
47. Environmental Protection Agency (EPA) Mercury (2007). Available on-line at http://www.epa.gov/mercury/data.htm Accessed April 19, 2007.
48. Environmental Protection Agency (EPA) Toxic release inventory (TRI). Available on-line at http://www.epa.gov/tri/ Accessed April 19, 2007.
49. Fan, LK. Hsp72 induction: a potential molecular mediator of the delay phenomenon. Ann Plast Surg. 2000;44(1):65–71.
50. Fenety, A, Walker, JM. Short-term effects of workstation exercises on musculoskeletal discomfort and postural changes in seated video display unit workers. Phys Ther. 2002;82(6):578–589.
51. Finkelstein, EA. Economic burden of injuries in the United States. New York: Oxford Press, 2006.
52. Forni, G. Immunoprevention of cancer: is the time ripe? Cancer Res. 2000;60(10):2571–2575.
53. Foster, WM. Bronchial reactivity of healthy subjects: 18-20 h postexposure to ozone. J Appl Physiol. 2000;89(5):1804–1819.
54. Frazer, L. The trickle-down theory of cleaner air. Environ Health Perspect. 2000;108(4):178–180.
55. Friedman-Jimenez, G. Clinical evaluation, management, and prevention of work-related asthma. Am J Ind Med. 2000;37(1):121–141.
56. Frumkin, H. Agent orange and cancer: an overview for clinicians. CA Cancer J Clin. 2003;53(4):245–255.
57. Gangi, S, Johansson, O. A theoretical model based upon mast cells and histamine to explain the recently proclaimed sensitivity to electric and/or magnetic fields in humans. Med Hypotheses. 2000;54(4):663–671.
58. Goehring, M, Older does not equal obsolete. Rehab Manag. 2002;15(6):24–26. Available on-line at http://www.rehabpub.com. Accessed April 3, 2007.
59. Gold, DR, et al. Ambient pollution and heart rate variability. Circulation. 2000;101(11):1267–1273.
60. Goodman, CC, Snyder, TE. Differential diagnosis for physical therapists: screening for referral, ed 4. Philadelphia: WB Saunders, 2007.
61. Green, H. Human skeletal muscle exercise metabolism following an expedition to Mount Denali. Am J Physiol Regul Integr Comp Physiol. 2000;279(5):R1872–1879.
62. Griefahn, B, Brode, P, Jaschinski, W. Contrast thresholds and fixation disparity during 5-Hz sinusoidal single-and dual-axis (vertical and lateral) whole-body vibration. Ergonomics. 2000;43(3):317–332.
63. Grigor’ev, IuG. Delayed biological effect of electromagnetic fields action. Radiats Biol Radioecol. 2000;40(2):217–225.
64. Gwynn, RC, Burnett, RT, Thurston, GD. A time-series analysis of acidic particulate matter and daily mortality and morbidity in the Buffalo, New York region. Environ Health Perspect. 2000;108(2):125–133.
65. Haley, RW. Brain abnormalities in Gulf War syndrome: evaluation with 1H MR spectroscopy. Radiology. 2000;215(3):807–817.
66. Haley, RW. Effect of basal ganglia injury on central dopamine activity in Gulf War syndrome. Arch Neurol. 2000;57(9):1280–1285.
67. Healthcare Without Harm Available on-line at http://www.noharm.org Accessed April 19, 2007.
68. Heller, A. Becoming a board certified ergonomist. ADVANCE Phys Therap PT Assist. 2000;11-12:26. [Reprints available at (800) 355-5627 (ext 446)].
69. Hemminiki, K. The balance between heritable and environmental aetiology of human disease. Nat Rev Genet. 2006;7(12):958–965.
70. Herbert, R, et al. Occupational coronary heart disease among bridge and tunnel officers. Arch Environ Health. 2000;55(3):152–163.
71. Holder, NL. Cause, prevalence, and response to occupational musculoskeletal injuries by physical therapists and physical therapists assistants. Phys Ther. 1999;79:642–652.
72. Hospitals for a healthy environment Available on-line at http://www.h2eonline.org Accessed April 19, 2007.
73. Houlihan, J. & Kropp, T. Body burden-the pollution in newborns. Environmental Working Group, 2005. Available on-line at http://www.ewg.org Accessed April 19, 2007.
74. Huang, YC. Intrabreath analysis of carbon monoxide uptake during exercise in patients at risk for lung injury. Respir Med. 2006;100(7):1226–1233.
75. Hultgren, HN. High-altitude medical problems. In: Rubenstein E, Federman D, eds. Scientific American medicine. New York: Scientific American, 1992.
76. Ingelido, AM. Polychlorinated biphenyls (PCBs) and polybrominated diphenyl ethers (PBDEs) in milk from Italian women living in Rome and Venice. Chemosphere. 2007;67(9):S301–306.
77. Johnson, LH. The challenges of modern society. PT Magazine. 2002;10(10):40–45.
78. Joseph, S. No unique illness afflicts Gulf veterans (news release), Washington, DC, August 2, 1995.
79. Kahan, ES. Chronic cough and dyspnea in ice hockey players after an acute exposure to combustion products of a faulty ice resurfacer. Lung. 2007;185(1):47–54.
80. Kumar, S. Theories of musculoskeletal injury causation. Ergonomics. 2001;44:17–47.
81. Labarge, XS, McCaffrey, RJ. Multiple chemical sensitivity: a review of the theoretical and research literature. Neuropsychol Rev. 2000;10(4):183–211.
82. Larsen, JC, Farland, W, Winters, D. Current risk assessment approaches in different countries. Food Addit Contam. 2000;17(4):359–369.
83. Lavelle, M. Burdened by old age: the hazards of toiling in the service economy. US News World Rep. 1999;126(19):69.
84. Lee, ME. Radon-smoking synergy: a population-based behavioral risk reduction approach. Prev Med. 1999;29(3):222–227.
85. Lewis, PG. Occupational and environmental medicine: moving the factory fence or hedging our bets? Occup Med (London). 2000;50(4):217–220.
86. Lönn, S. Long-term mobile phone use and brain tumor risk. Am J Epidem. 2005;161(6):526–535.
87. Marcus, M. Video display terminals and miscarriage. J Am Med Wom Assoc. 2000;55(2):84–88. [105].
88. Marklin, RW, Simoneau, GG. Design features of alternative computer keyboards: a review of experimental data. J Orthop Sports Phys Ther. 2004;34(10):638–649.
89. Marras, WS. The influence of psychosocial stress, gender, and personality on mechanical loading of the lumbar spine. Spine. 2000;25(23):3045–3054.
90. Marshall, L, Identifying and managing adverse environmental health effects: taking an exposure history. CMAJ. 2002;266(8):1049–1055. Available on-line at http://www.cmaj.ca/cgi/reprint/166/8/1049.pdf Accessed April 19, 2007.
91. Materna, B. Fixed obstructive lung disease among workers in the flavor-manufacturing industry. MMWR. 2007;56(16):389–393.
92. Matheson, LN. Work hardening for patients with back pain. J Musculoskel Med. 1993;10:53–63.
93. McElroy, JA. Occupational exposure to electromagnetic field and breast cancer risk in a large, population-based, case-control study in the United States. J Occup Environ Med. 2007;49(3):266–274.
94. Menegaus, F. Household exposure to pesticides and the risk of childhood acute leukemia. Occup Environ Med. 2006;63(2):131–134.
95. Mester, J, Spitzenfeil, P, Schwarzer, J. Biological reaction to vibration-implications for sport. J Sci Med Sport. 1999;2(3):211–226.
96. Miller, CS. Toxicant-induced loss of tolerance. Addiction. 2001;96(1):115–137.
97. Moller, P. The alkaline comet assay: towards validation in biomonitoring of DNA damaging exposures. Basic Clin Pharmacol Toxicol. 2006;98(4):336–345.
98. Morbidity Mortality Weekly Report (MMWR). Blood and hair mercury levels in young children and women of childbearing age. MMWR. 2004;53(43):1010–1020.
99. Morbidity and Mortality Weekly Report (MMWR). Childhood lead poisoning from commercially manufactured ceramic dinnerware. MMWR. 2004;53(26):584–586.
100. Morbidity Mortality Weekly Report (MMWR). Radon testing in households with a residential smoker-United States, 1993-1994. MMWR. 1999;48(31):683–686.
101. Morgan, BJ. The patient with coronary heart disease at altitude: observations during acute exposure to 3100 meters. J Wilderness Med. 1990;1:147.
102. Nakamura, CT, et al. Latex allergy in children on home mechanical ventilation. Chest. 2000;118(4):1000–1003.
103. National Academy of Sciences. Work-related musculoskeletal disorders: the research base. Washington, DC: The Academy, 1998.
104. National Athletic Trainers’ Association (NATA) Inter-association task force on exertional heat illnesses. Available on-line at http://www.nata.org/consumer/heatillness/index.htm Accessed April 20, 2007.
105. National Children’s Study (NCS) Health, growth, environment. Available on-line at http://www.nationalchildrensstudy.gov/ Accessed April 19, 2007.
106. National Health and Nutrition Examination Survey (NHANES)Third national health and examination survey public use data files. Available on-line at http://www.cdc.gov/nchs/products/elec_prods/subject/nhanes3.htm Accessed May 1, 2007.
107. National Institute of Occupational Safety and HealthErgonomics: effective workplace practices and programs, Washington DC, 1997. Available on-line at http://www.osha.gov
108. Newman, LS. Occupational illness. N Engl J Med. 1995;333:1128–1134.
109. Nriagu, JO, Kim, MJ. Emissions of lead and zinc from candles with metal-core wicks. Sci Total Environ. 2000;250(1-3):37–41.
110. O’Brien, M. Making better environmental decisions: an alternative to risk assessment. Cambridge, MA: MIT Press, 2000.
111. Occupational Safety and Health Administration (OSHA)Comprehensive Plan 2002. Available on-line at http://www.osha.gov Accessed April 23, 2007.
112. Occupational Safety and Health Administration (OSHA)One size doesn’t fit all approach (OSHA national news release), USDL 99-333, November 22, 1999. Available on-line at http://www.osha.gov/media/oshnew
113. Occupational Safety and Health Administration (OSHA)Preventing work-related musculoskeletal disorders, Month 2006. Available on-line at http://www.osha.gov Accessed April 24, 2007.
114. O’Leary, ES. Shift work, light at work, and breast cancer on Long Island, New York. Am J Epidemiol. 2006;164(4):358–366.
115. Olsen, GW. Preliminary evidence of a decline in perfluorooctanoic sulfonate (PFOS) and perfluorooctanoic (PFOA) concentrations in American Red Cross blood donors. Chemosphere. 2007;68(1):105–111.
116. Patel, M. Recognition of illness associated with exposure to chemical agents. MMWR. 2003;52(39):938–940.
117. Piantadosi, CA. Physical, chemical, and aspiration injuries of the lung. In Goldman L, Bennett JC, Cecil RL, eds.: Cecil textbook of medicine, ed 22, Philadelphia: WB Saunders, 2004.
118. Pinksi, SL, Trohman, RG. Interference with cardiac pacing. Cardiol Clin. 2000;18(1):219–239.
119. Pope, MH, Wilder, DG, Magnusson, ML. A review of studies on seated whole-body vibration and low-back pain. Proc Inst Mech Eng. 1999;213(6):435–446.
120. Pridgeon, C. Assessment of latex allergy in a health care population: are the available tests valid? Clin Exp Allergy. 2000;30(10):1444–1449.
121. Proctor, SP. Chemical sensitivity and gulf war veterans’ illnesses. Occup Med. 2000;15(3):587–599.
122. Pyne, DB. Training strategies to maintain immunocompetence in athletes. Int J Sports Med 21 Suppl. 2000;1(6):S51–S60.
123. Risom, L. Oxidative stress-induced DNA damage by particulate air pollution. Mutat Res. 2005;592(1-2):119–137.
124. Rittweger, J, Beller, G, Felsenberg, D. Acute physiologic effects of exhaustive whole-body vibration exercise in man. Clin Physiol. 2000;20(2):134–142.
125. Ritz, B. Air pollution and infant death in southern California, 1989-2000. Pediatrics. 2006;118(2):493–502.
126. Rogan, WJ, Ware, JH. Exposure to lead in children-how low is low enough? NEJM. 2003;348(16):1515–1516.
127. Roosli, M. Cellular telephone use and time trends in brain tumour mortality in Switzerland from 1969-2002. Eur J Cancer Prev. 2007;16(1):77–82.
128. Russell-Fell, RW. Avoiding problems: evidence-based selection of medical gloves. Br J Nurs. 2000;9(3):139–146.
129. Salvi, S. Acute inflammatory responses in the airways and peripheral blood after short-term exposure to diesel exhaust in healthy human volunteers. Am J Respir Crit Care Med. 1999;159(3):702–709.
130. Sanborn, MD. Identifying and managing adverse environmental health effects. CMAJ. 2002;166(11):1431–1436.
131. Sander, M. The twenty-first Aspen cancer conference: mechanisms of toxicity, carcinogenesis, cancer prevention, and cancer therapy. Mol Carcinog. 2007;46:415–435.
132. Schlenk, D. In vivo bioassay-guided fractionation of marine sediment extracts from the Southern California Bight, USA, for estrogenic activity. Environ Toxicol Chem. 2005;24(11):2820–2826.
133. Schneider, A. Peripheral arterial vascular function at altitude: sea-level natives versus Himalayan high-altitude natives. J Hypertens. 2001;19(2):213–222.
134. Schreinemachers, DM. Birth malformations and other adverse perinatal outcomes in four U.S. wheat-producing states. Environ Health Perspect. 2003;111(9):1259–1264.
135. Schreinemachers, DM. Cancer mortality in four northern wheat-producing states. Environ Health Perspect. 2000;108(9):873–881.
136. Schreinemachers, DM. Mortality from ischemic heart disease and diabetes mellitus (type 2) in four U.S. wheat-producing states: a hypothesis-generating study. Environ Health Perspect. 2006;114(2):186–193.
137. Schulte, PA. Work, obesity, and occupational safety and health. Am J Public Health. 2007;97(3):428–436.
138. Schuz, J. Cellular telephone use and cancer risk: update of a nationwide Danish cohort. J Natl Cancer Inst. 2006;98(23):1707–1713.
139. Seal, KH. Bringing the war back home: mental health disorders among 103,788 US veterans returning from Iraq and Afghanistan seen at Department of Veterans Affairs facilities. Arch Intern Med. 2007;167(5):476–482.
140. Selevan, SG. Blood lead concentrations and delayed puberty in girls. N Engl J Med. 2003;348(16):1527–1536.
141. She, J. Polybrominated diphenyl ethers (PBDEs) and polychlorinated biphenyls (PCBs) in breast milk from the Pacific Northwest. Chemosphere. 2007;67(9):S307–S317.
142. Shephard, RJ. Age and physical work capacity. Exp Aging Res. 1999;25(4):331–343.
143. Sheps, DS. Production of arrhythmias by elevated carboxyhemoglobin in patients with coronary artery disease. Ann Intern Med. 1990;113:343.
144. Sher, L. The effects of natural and man-made electromagnetic fields on mood and behavior: the role of sleep disturbances. Med Hypotheses. 2000;54(4):630–633.
145. Simeonova, PP, Luster, MI. Arsenic and atherosclerosis. Toxicol Appl Pharmacol. 2004;198(3):444–449.
146. Simeonova, PP, Luster, MI. Mechanisms of arsenic carcinogenicity: genetic or epigenetic mechanisms? J Environ Pathol Toxicol Oncol. 2000;19(3):281–286.
147. Singh, R, Kaur, B, Kalina, I, et al. Effects of environmental air pollution on endogenous oxidative DNA damage in humans. Mutat Res. 2007;620(1-2):71–82.
148. Sliwinska-Kowalska, M. Environmental exposure to electromagnetic fields and the risk of cancer. Med Pr. 1999;50(6):581–591.
149. Sobel, HL, Lurie, P, Wolfe, SM. Lead exposure from candles. JAMA. 2000;284(2):180.
150. Solomonow, M. Biomechanics and electromyography of a common idiopathic low back disorder. Spine. 2003;28(12):1235–1248.
151. Spengler, JD, et al. Health effects of acid aerosols on North American children: air pollution exposures. Environ Health Perspect. 1996;104(5):492–499.
152. Sram, RJ, Binkova, B. Molecular epidemiology studies on occupational and environmental exposure to mutagens and carcinogens. Environ Health Perspect. 2000;108(Suppl 1):57–70. [(1)].
153. Stauber, WT. Factors involved in strain-induced injury in skeletal muscles and outcomes of prolonged exposures. J Electromyogr Kinesiol. 2004;14(1):61–70.
154. Staudenmayer, H. Psychological treatment of psychogenic idiopathic environmental intolerance. Occup Med. 2000;15(3):627–646.
155. Story, DA, Thistlewaite, P, Bellomo, R. The effect of PVC packaging on the acidity of 0.9% saline. Anaesth Intensive Care. 2000;28(3):287–292.
156. Taioli, E, Sram, RJ, Garte, S, et al. Effects of polycyclic aromatic hydrocarbons (PAHs) in environmental pollution on exogenous and oxidative DNA damage (EXPAH project). Mutat Res. 2007;620(1-2):1–6.
157. Thomas, HV. Systematic review of multi-symptom conditions in Gulf War veterans. Psychol Med. 2006;36(6):735–747.
158. Thomas, PK, King, RH, Feng, SF. Neurological manifestations in chronic mountain sickness: the burning feet-burning hands syndrome. J Neurol Neurosurg Psychiatry. 2000;69(4):447–452.
159. Thomsen, C. Indicators for occupational health surveillance. MMWR. 2007;56(RR01):1–7.
160. Tickner, JA. Health risks posed by use of Di-2-ethylhexyl phthalate (DEHP) in PVC medical devices: a critical review. Am J Ind Med. 2001;39(1):100–111.
161. Toms, LM, Harden, FA, Symons, RK. Polybrominated diphenyl ethers (PBDEs) in human milk from Australia. Chemosphere. 2007;68(5):797–803.
162. Tri, JL. Cellular phone interferes with external cardiopulmonary monitoring devices. Mayo Clin Proc. 2001;76(1):11–15.
163. Trosko, JE. Human health consequences of environmentally-modulated gene expression: potential roles of ELF-EMF induced epigenetic versus mutagenic mechanisms of disease. Bioelectromagnetics. 2000;21(5):402–406.
164. Tsutsumi, O. Assessment of human contamination of estrogenic-endocrine-disrupting chemicals and their risk for human reproduction. J Steroid Biochem Mol Biol. 2005;93(2-5):325–330.
165. U.S. Environmental Protection AgencyAir & Radiation-National ambient air quality standards (NAAQS). Available on-line at http://www.epa.gov/air/criteria.html Accessed April 21, 2007.
166. van der Heide, S, van Aalderen, WM, Kauffman, HF. Clinical effects of air cleaners in homes of asthmatic children sensitized to pet allergens. J Allergy Clin Immunol. 1999;104(2 Pt 1):447–451.
167. Vatter, MJ, The impact of staffing levels and fire severity on injuries. Fire Engin. 1999;152(8). Available on-line at http://www.fe.pennwellnet.com.
168. Waldrop, S. Work-related injuries: preventing the PT from becoming the patient. PT Magazine. 2004;12(2):34–41.
169. Walusiak, J. Occupational upper airway disease. Curr Opin Allergy Clin Immunol. 2006;6(1):1–6.
170. Walvekar, RR. Chronic arsenic poisoning: a global health issue-a report of multiple primary cancers. J Cutan Pathol. 2007;34(2):203–206.
171. Weigl, E. Heat shock proteins in immune reactions. Folia Microbiol. 1999;44(5):561–566.
172. Worthington, K. Seeking the perfect fit: alternatives to latex gloves. AJN. 2000;100(8):88.
173. Zuurbier, M. Children’s exposure to polybrominated diphenyl ethers. Acta Paediatr Suppl. 2006;95(453):65–70.