The Integumentary System
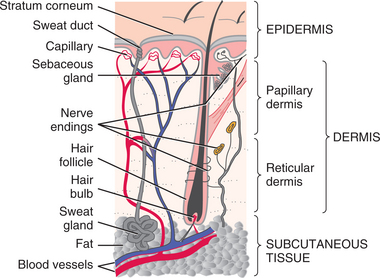
Skin is the largest body organ, constituting 15% to 20% of the body weight and consisting of three primary layers (Fig. 10-1). The dermis is more distinctly divided into two separate layers referred to as the papillary dermis and reticular dermis. The structures included in each layer are listed in Table 10-1.
Table 10-1
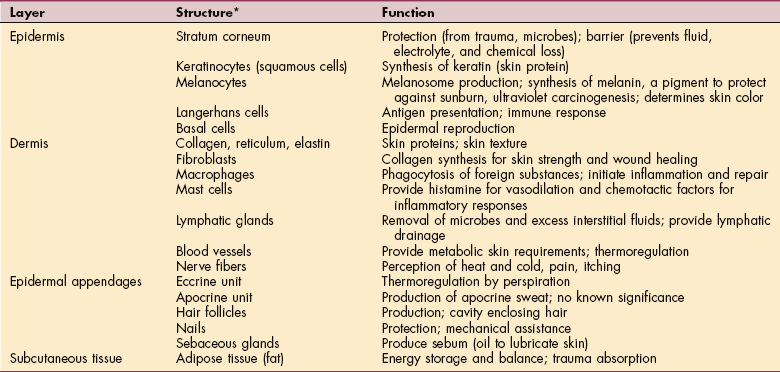
*Understanding the structure of the integument is important in wound management. Knowing why a wound closes the way it does is an essential assessment tool.
Modified from Nicol NH: Structure and function: assessment of clients with integumentary disorders. In Black JM, Matassarin-Jacobs E, eds: Medical-surgical nursing, ed 5, Philadelphia, 1997, Saunders, p 2176.
The skin differs anatomically and physiologically in different areas of the body, but the overall primary function of the skin is to protect underlying structures from external injury and harmful substances. The skin is primarily an insulator, not an organ of exchange.
It has many other different functions, including holding the organs together, sensory perception, contributing to fluid balance, controlling temperature, absorbing ultraviolet (UV) radiation, metabolizing vitamin D, and synthesizing epidermal lipids.
SKIN LESIONS
Approximately one in every four people who consult a physician has a skin disorder. Skin lesions can occur as a result of a wide variety of etiologic factors (Box 10-1). Lesions of the skin or skin manifestations of systemic disorders can be classified as primary or secondary lesions.
The primary lesion is the first lesion to appear on the skin and has a visually recognizable structure (e.g., macule, papule, plaque, nodule, tumor, wheal, vesicle, pustule). When changes occur in the primary lesion, it becomes a secondary lesion (e.g., scale, crust, thickening, erosion, ulcer, scar, excoriation, fissure, atrophy). These changes may result from many factors, including scratching, rubbing, medication, natural disease progression, or processes of healing.
Birthmarks, commonly caused by a nevus (pl., nevi), may involve an overgrowth of one or more of any of the normal components of skin, such as pigment cells, blood vessels, and lymph vessels. Birthmarks may be classified as pigment cell (e.g., mongolian spot, café au lait spot), vascular (e.g., port-wine stain, strawberry hemangioma), epidermal (e.g., epidermal nevus, nevus sebaceus), or connective tissue (e.g., juvenile elastoma, collagenoma) birthmarks.
Most birthmarks do not require treatment. Vascular birthmarks may be removed with laser therapy for cosmetic reasons. The presence of six or more café au lait spots over 5 cm in length requires medical investigation, because these may be diagnostic of neurofibromatosis or Albright’s syndrome. Mongolian spots (blue-black macules) are found over the lumbosacral area in 90% of Native American, African American, and Asian infants and can easily be mistaken for a large bruise by uninformed individuals (Fig. 10-2).

Figure 10-2 Mongolian spots (congenital dermal melanocytosis). Mongolian spots are common among people of Asian, East Indian, Native American, Alaskan American, African, and Latino or Hispanic heritage. They are also present in about 1 in 10 fair-skinned infants. Bluish grey to deep brown to black skin markings, they often appear on the base of the spine, on the buttocks and back, and even sometimes on the shoulders, ankles, or wrists. Mongolian spots may cover a large area of the back. When the melanocytes are close to the surface, they look deep brown. The deeper they are in the skin, the more bluish they look, often mistaken for signs of child abuse. These spots “fade” with age as the child grows and usually disappear by age 5. (Courtesy Dr. Dubin Pavel, 2004.)
SIGNS AND SYMPTOMS OF SKIN DISEASE
Pruritus (itching) is one of the most common manifestations of dermatologic disease and a symptom of underlying systemic disease in up to 50% of people with generalized itching, especially among the chronically ill and older populations.133 It can lead to damage if scratching injures the skin’s protective barrier, possibly resulting in increased inflammation, infection, and scarring. Many systemic disorders may cause pruritus, most commonly diabetes mellitus, drug hypersensitivity, and hyperthyroidism (Box 10-2).
Urticaria, more commonly known as hives, is a vascular reaction of the skin marked by the appearance of smooth, slightly elevated patches (wheals). These are redder or paler than the surrounding skin and are often accompanied by severe itching. These eruptions are usually an allergic response to drugs or infection and rarely last longer than 2 days but may exist in a chronic form, lasting more than 3 weeks and, rarely, months to years. There is approximately a 50% reduction in numbers of mast cells responsible for urticaria in intrinsically aged skin. This explains the relative rarity of urticaria in the older adult population.
Rash is a generalized term for an eruption on the skin, most often on the face, trunk, axilla, and groin, and is often accompanied by itching. As such, a rash can present as a continuum anywhere from erythema, to macular lesions, to a raised papular appearance. Rashes typically occur as a secondary response to some primary agent, such as exposure to the sun, allergens, irritants, or medications or in association with systemic disease.
The most common rashes are diaper rash, drug rash, heat rash, and butterfly rash (a cutaneous reaction across the nose and adjacent areas of the cheeks in the pattern of a butterfly, most often encountered in systemic lupus erythematosus; see Fig. 10-22). Rash appearing on the breast, especially a rash on the areola or nipple with or without accompanying symptoms of itching, soreness, or burning, may be a sign of Paget’s disease of the nipple, a rare form of breast cancer.
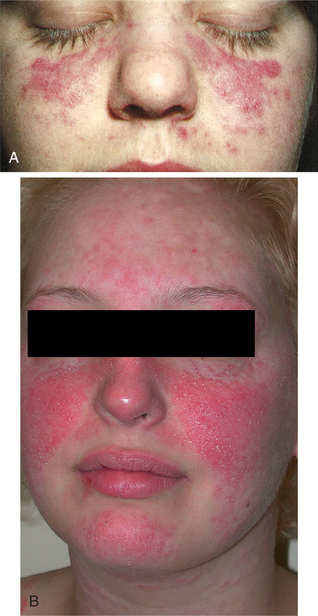
Figure 10-22 A, Butterfly rash of systemic lupus erythematosus across the bridge of the nose and the cheeks. B, In some cases the rash covers a larger portion of the face, including the lips and chin. (A, From Goldstein BJ, Goldstein AO: Practical dermatology, ed 2, St Louis, 1997, Mosby. Courtesy Department of Dermatology, University of North Carolina at Chapel Hill. Used with permission. B, From Bolognia JL, Jorizzo JL, Rapini RP: Dermatology, 2 volume set, St Louis, 2003, Mosby.)
Blisters (vesicle or bulla) are fluid-containing elevated lesions of the skin with clear watery or bloody contents. They can occur as a manifestation of a wide variety of diseases. Blisters may be primarily associated with diseases of a genetic or autoimmune origin or may be secondary to viral or bacterial infections of the skin (e.g., herpes simplex, impetigo), local injury to the skin (e.g., burns, ischemia, pressure, dermatitis), or drug-induced (e.g., penicillamine, captopril).29 Blisters associated with underlying neoplasm, called paraneoplastic pemphigus, may be the first sign of underlying malignancy.
Xeroderma is a mild form of ichthyosis or excessive dryness of the skin characterized by dry, rough, discolored skin with the formation of scaly desquamation (shedding of the epithelium in small sheets). This problem is accentuated by the use of drying skin cleansers, soaps, disinfectants, and solvents, and by dry climates.
Other symptoms, such as unusual spots, moles, cysts, fibromas, nodules, swelling, or changes in nail beds, may be observed frequently, since more than half of all people have some basic skin problem at some point in their lives (Box 10-3). Any unusual spot that has appeared recently or changed since its initial appearance should be documented and brought to the physician’s attention. On the legs, varicosities and stasis changes from poor venous return may be signaled by changes in skin pigmentation, skin turgor (see Fig. 5-7), and skin texture. Edema of the lower extremities can be a sign of multiple systemic illnesses, such as heart, kidney, or liver disease.
AGING AND THE INTEGUMENTARY SYSTEM
The skin undergoes numerous changes that can be seen and felt throughout the lifespan. The most obvious changes occur first during puberty and again during older adulthood. Hormone changes during puberty stimulate the maturation of hair follicles, sebaceous glands, and apocrine and eccrine units in certain body areas. Mild acne, perspiration and body odor, freckles (promoted by sun exposure), and pigmented nevi (moles) are common occurrences.
During adolescence and adulthood, the use of birth control pills or pregnancy may result in temporary changes in hair growth patterns or hyperpigmentation of the cheeks and forehead known as melasma or pregnancy mask. Other hormonal abnormalities may result in excessive facial and body hair in women (androgen-related). Hormonal and genetic changes also produce male-pattern baldness (alopecia). Smoking is an independent causative factor of facial wrinkles.43
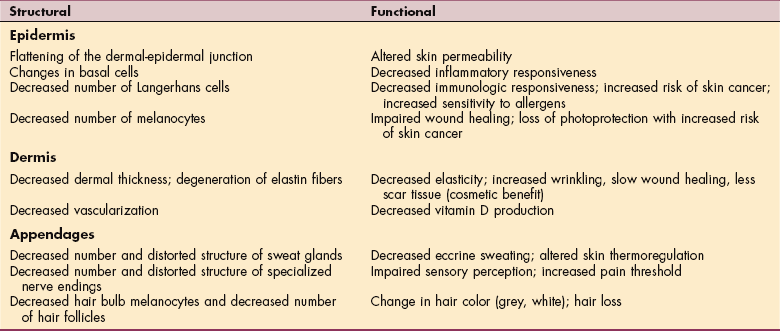
The skin exhibits changes that denote the onset of senescence (the process or condition of growing old). These changes may be due to the aging process itself (intrinsic aging), to the cumulative effects of exposure to sunlight (photoaging), or to environmental factors (extrinsic aging). As aging occurs, both structural and functional changes occur in the skin (Table 10-2), resulting clinically in diminished pain perception, increased vulnerability to injury, decreased vascularity, and a weakened inflammatory response.
Visible indications of skin changes associated with aging include grey hair, balding and loss of secondary sexual hair, and increased facial hair. For women, excessive facial hair may occur along the upper lip and around the chin. Women may also experience balding after menopause. Men frequently develop increased facial hair in the nares, eyebrows, and helix of the ear.
Other common age-related integumentary changes include lax skin, vascular changes (e.g., decreased elasticity of blood vessel walls; angiomas) (Fig. 10-3), dermal or epidermal degenerative changes, and wrinkling. Wrinkling signifies loss of elastin fibers, weakened collagen, and decreased subcutaneous fat and is accelerated by smoking and excessive sun exposure.
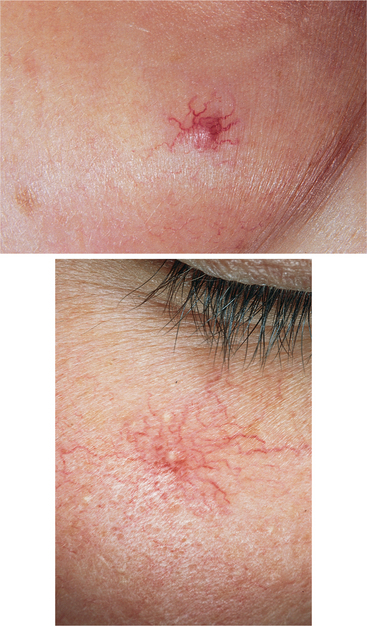
Figure 10-3 Spider angioma (arterial spider, spider telangiectasia, vascular spider) is so called because it consists of a central arteriole, radiating from which are numerous small vessels resembling a spider’s legs (ranging from pinhead size to 0.5 cm in diameter). Common sites are the necklace area, face, forearms, and dorsum of the hand; may be associated with rosacea, basal cell carcinoma, scleroderma, pregnancy, liver disease, or estrogen therapy or may occur by itself. (From Habif T: Clinical dermatology, ed 4, St Louis, 2004, Elsevier, Figs. 23-20, 23-21, p 830.)
Blood vessels within the reticular dermis are reduced in number, and the walls are thinned. This compromises blood flow and appears physiologically as pale skin and an impaired capacity to thermoregulate, a possible contributing factor to the increased susceptibility of older individuals to hypothermia and hyperthermia. Many other benign changes may occur, including seborrheic keratoses (raised brown or black wartlike growths), lentigines (liver spots, unrelated to the liver but rather sec- ondary to sun exposure), and skin tags (small flesh-colored papules).
A primary factor in the loss of protective functions of the skin is the diminished barrier function of the stratum corneum (outermost layer of the epidermis; see Fig. 10-1). As this layer becomes thinner, the skin becomes translucent and paper-thin, reacting more readily to minor changes in humidity, temperature, and other irritants. There are fewer melanocytes, with decreased protection against UV radiation.
A significant decrease in the number of Langerhans cells occurs, so that by the time a person reaches 70 years of age there is only half the number of Langerhans cells compared to the number in early adulthood. A reduction in Langerhans cell number represents a loss of immune surveillance and an increased risk of skin cancer.55
The epidermis is also one of the body’s principal suppliers of vitamin D, which is produced when a hormone, 7-dehydrocholesterol, is exposed to sunlight. At 65 years of age, the levels of that hormone are only about 25% of what they were in youth, contributing to vitamin D deficiency and, because vitamin D plays a vital role in building bone, to osteoporosis as well.
It is generally agreed that one of the major and important contributions to skin aging, skin disorders, and skin diseases is the oxidative damage that occurs to the skin as a result of environmental exposures and endogenous (within the skin itself) factors.
The skin is rich in lipids, proteins, and deoxyribonucleic acid (DNA), all of which are extremely sensitive to the oxidation process. Scientists are striving to understand the mechanisms involved in skin oxidation and the skin defense systems in order to understand skin aging and the mechanisms involved in various pathologic processes of the skin.77
COMMON SKIN DISORDERS
Definition and Incidence
Atopic dermatitis (AD) is a chronic inflammatory skin disease. It is the most common type of eczema, frequently already present during the first year of life and affecting more than 10% of children.
AD is considered an early manifestation of atopy that appears before the development of allergic rhinitis or asthma. The word atopic (from atopy) refers to a group of three associated allergic disorders: asthma, allergic rhinitis (hay fever), and AD. There is usually a personal or family history of allergic disorders present, and AD is often associated with food allergies as well.
Etiologic and Risk Factors and Pathogenesis
The exact cause of AD is unknown, although recent studies have demonstrated the complex interrelationship of genetic, physical environment, skin barrier, pharmacologic, psychologic, and immunologic etiologic factors that contribute to the development and severity of AD.85,159
The pathomechanisms associated with AD are also unknown but most likely include both immediate and cellular immune responses. Two possibilities include the release of inflammatory mediators by autoallergens and the release of proinflammatory cytokines by autoreactive T cells in response to autoallergens mediated by immunoglobulin E (IgE).155
AD is often associated with increased levels of serum IgE and with sensitization to food allergens.139 Some foods may be responsible for exacerbations of skin inflammation, but their pathogenic role must be clinically assessed before an avoidance diet is recommended.68 Xerosis (abnormal dryness) associated with AD is usually worse during periods of low humidity and over the winter months in northern latitudes.
The underlying biochemical abnormality in xerosis is unknown, and the pathologic findings may be a result of the dry skin rather than the cause of the drying effects of this condition. Compared with normal skin, the dry skin of AD has a reduced water-binding capacity, a higher transepidermal water loss, and a decreased water content. Rubbing and scratching of itchy skin are responsible for many of the clinical changes seen in the skin. Hands frequently in and out of water make the condition worse.
Clinical Manifestations
AD begins in many people during infancy in the form of a red, oozing, crusting rash classified as acute dermatitis (Fig. 10-4). As the child grows, the chronic form of dermatitis results in skin that is dry, thickened, and brownish-grey in color (lichenified). The rash tends to become localized to the large folds of the extremities as the person becomes older. It is found mainly on flexor surfaces such as the elbows and knees, neck, sides of the face, eyelids, and the backs of hands and feet. Hand and foot dermatitis can become a significant problem for some people.

Figure 10-4 Infantile atopic dermatitis with oozing and crusting lesions. (From Paller A, Mancini A: Hurwitz clinical pediatric dermatology: a textbook of skin disorders of childhood and adolescence, ed 3, Philadelphia, 2006, Saunders.)
Xerosis and pruritus are the major symptoms of AD and cause the greatest morbidity with severely excoriated lesions, infection, and scarring. Viral, bacterial, and fungal secondary skin infections may cause further changes in the skin. Staphylococcus aureus is the most common bacte- rial infection, resulting in extensive crusting with serous weeping, folliculitis (inflammation of hair follicles), pyoderma (pus), and furunculosis (boils).
MEDICAL MANAGEMENT
DIAGNOSIS, TREATMENT, AND PROGNOSIS.
Although no cure exists, AD often resolves spontaneously, and more than 90% of cases of AD can be effectively controlled through proper management. The goal of medical therapy is to break the inflammatory cycle that causes excess drying, cracking, itching, and scratching.
Personal hygiene, moisturizing the skin, avoidance of irritants, topical pharmacology, and systemic medications (e.g., antibiotics, antihistamines, and rarely, systemic corticosteroids) are treatment techniques currently available. S. aureus, known to colonize the skin of people with AD, may exacerbate skin lesions and needs to be treated with antibiotics. Advancing knowledge in understanding the immunologic basis of this disease will continue to result in effective new local and systemic treatments in the decade to come.104,140
Contact Dermatitis
Etiologic Factors, Incidence, and Pathogenesis
Contact dermatitis can be an acute or chronic skin inflammation caused by exposure to a chemical, mechanical, physical, or biologic agent. It is one of the most common environmental skin diseases occurring at any age. As people age, they may develop delayed cell-mediated hypersensitivity to a variety of substances that come in contact with the skin.
Common sensitizers include nickel (found in jewelry and many common foods), chromates (used in tanning leathers), wool fats (particularly lanolin found in moisturizers and skin creams), rubber additives (see the section on Latex Rubber Allergy in Chapter 4), topical antibiotics (typically neomycin and bacitracin),32 and topical anesthetics, such as benzocaine or lidocaine.57 Dermatitis of unknown cause is more commonly diagnosed in the older population.
A small percentage of the population is allergic to silicone. The therapist is most likely to see this reaction in a sensitized person with an amputation using a silicone type of interface in a prosthetic device (designed to reduce shear, decrease repetitive stress, and absorb shock). Silicone sheets used for scar reduction in the postburn population may also result in an episode of contact dermatitis.
Clinical Manifestations
Intense pruritus (itching), erythema (redness), and edema of the skin occur 1 to 2 days after exposure in previously sensitized persons. Clinical manifestations begin at the site of exposure but then extend to more distant sites. These conditions may progress to vesiculation, oozing (watery discharges), crusting, and scaling (Fig. 10-5). If these symptoms persist, the skin becomes thickened, with prominent skin markings and pigmentation changes. Older people have a less pronounced inflammatory response to standard irritants than do younger persons.

Figure 10-5 Primary contact dermatitis, a local inflammatory reaction, can occur in response to an irritant in the environment or an allergy. Characteristic location of lesions often gives a clue to the cause. Erythema occurs first, followed by swelling, wheals or urticaria, or maculopapular vesicles accompanied by intense pruritus. The example shown here is a result of contact with poison ivy. (From Paller A, Mancini A: Hurwitz clinical pediatric dermatology: a textbook of skin disorders of childhood and adolescence, ed 3, Philadelphia, 2006, Saunders.)
MEDICAL MANAGEMENT
DIAGNOSIS, TREATMENT, AND PROGNOSIS.
If contact dermatitis is suspected, the client should be referred to a physician. A detailed history and careful examination are frequently all that are needed to make the diagnosis. It may be necessary to perform patch testing to identify the causative agent.
Primary treatment is removal of the offending agent; treatment of the skin is secondary. The client should be instructed to avoid contact with strong soaps, detergents, solvents, bleaches, and other strong chemicals. The involved skin should be lubricated frequently with emollients. Topical anesthetics or steroids (topical or sometimes systemic) or both may be prescribed. For those people unable to avoid known allergens, immunosuppressant therapies (including phototherapy) can be helpful.8
Acute lesions usually resolve in 3 weeks; chronic lesions persist until the causative agent has been removed.
Eczema and Dermatitis
Eczema and dermatitis are terms that are often used interchangeably to describe a group of disorders with a characteristic appearance. Eczema or dermatitis is a superficial inflammation of the skin caused by irritant exposure, allergic sensitization (delayed hypersensitivity), or genetically determined idiopathic factors.
Many types of dermatitis are represented according to these major etiologic categories (e.g., allergic dermatitis, irritant dermatitis, seborrheic dermatitis, nummular eczema, AD, stasis dermatitis).
Eczema or dermatitis has three primary stages. This condition can manifest in any one of the three stages, or the three stages may coexist. Acute dermatitis is characterized by extensive erosions with serous exudate or by intensely pruritic, erythematous papules and vesicles on a background of erythema.
Subacute dermatitis is characterized by erythematous, excoriated (scratched or abraded), scaling papules or plaques that are either grouped or scattered over erythematous skin. Often the scaling is so fine and diffuse the skin acquires a silvery sheen.
Chronic dermatitis is characterized by thickened skin and increased skin marking (called lichenification) secondary to rubbing and scratching; excoriated papules, fibrotic papules, and nodules (prurigo nodularis); and postinflammatory hyperpigmentation and hypopigmentation.
Incidence and Etiologic Factors
Dermatitis is a common skin disorder in older people. It may be caused by hypoproteinemia, venous insufficiency, allergens, irritants, or underlying malignancy, such as leukemia or lymphoma. Because older people often take multiple medications, dermatitis from drug-drug interaction can occur. The normal aging process with the flattened epidermal-dermal junction and loss of dermis results in skin fragility, which contributes to the development of skin tears and dermatitis.
Stasis Dermatitis
Stasis dermatitis is the development of areas of very dry, thin skin and sometimes shallow ulcers of the lower legs primarily as a result of venous insufficiency. The client commonly has a history of varicose veins or deep vein thrombosis (see also the section on Venous Diseases in Chapter 12).
The process of stasis dermatitis begins with edema of the leg as a result of slowed venous return. As the venous insufficiency continues, the tissue becomes hypoxic from inadequate blood supply. This poorly nourished tissue begins to necrose.
The clinical manifestations include itching, a feeling of heaviness in the legs, brown-stained skin, and open shallow lesions (Fig. 10-6). The lesions are very slow to heal because of a lack of oxygenated blood. Gait training is an important part of compression, the gold standard, in the treatment of stasis dermatitis. Compression hose work well in the recumbent position, but ambulation with the muscular contract-relax cycle pushes the venous return within the compressive field.

Figure 10-6 Stasis dermatitis secondary to venous insufficiency. Hemosiderin staining (dark pigmentation) indicative of venous insufficiency is evident. This staining is caused by the leakage of hemosiderin (an iron-rich pigment, the product of red cell hemolysis) as a result of blood that cannot return due to valvular incompetence. (Courtesy Harriett B. Loehne, PT, DPT, CWS, FCCWS, Archbold Center for Wound Management, Thomasville, GA, 2006. Used with permission)
Environmental Dermatoses
It is well documented that exposure to various environmental chemicals and to physical stimuli (Box 10-6) is capable of inducing adverse cutaneous responses. Common environmental skin diseases seen in a therapy practice may include irritant and allergic dermatitis, acne lesions, pigmentary changes (hyperpigmentation, hypopigmentation, absence of pigment), photosensitivity reactions, scleroderma, infectious disorders, and cutaneous malignancy. Each of these environmentally induced skin conditions is discussed separately in this chapter (see also Chapter 4).
Rosacea
Rosacea* is a chronic facial disorder of middle-aged and older people. Although it is a form of acne, it is differentiated by age, the presence of a large vascular component (erythema, telangiectasis), and usually the absence of comedones.
An acneiform rosacea can occur with papules, pustules, and oily skin. No known cause or factor has been identified to explain the pathogenesis of this disorder. A statistically significant incidence of migraine headaches accompanying rosacea has been reported.
Rosacea has often been linked with gastrointestinal (GI) disturbances, and a causal relationship between Helicobacter pylori (a bacterium that causes gastritis) and rosacea was reported in the early 1990s. Many studies linking rosacea to H. pylori infection were uncontrolled and were performed in areas where the endemic rates of both H. pylori infection and rosacea are high.149 A study done in Iran in 2003, where prevalence is low, also supported some form of relationship between rosacea and H. pylori infection.167 Continued investigation of this issue is required before a causal relationship can be confirmed.
Clinically, the cheeks, nose, and chin (sometimes the entire face) may have a rosy appearance marked by reddened skin. This benign but obvious condition is most common in people with fair skin who flush easily. Sun, hot weather, and humidity can all trigger flare-ups; the condition is worse in the summer.
The affected person reports burning or stinging with episodes of flushing that come and go, but the condition may worsen over time, causing lasting redness, pimples, telangiectasias, or nasal hypertrophy (rhinophyma). Inflammatory papules are prominent, and there may be pustules. It is not uncommon to have associated ophthalmic disease, including blepharitis and keratitis.
Medical management aimed at the inflammatory papules, pustules, and surrounding erythema may include topical or systemic therapy. Rosacea tends to be a persistent condition that can be controlled with drugs. Chronic rosacea has long been treated by pulsed dye lasers. A newer system, the Intense Pulsed Light (IPL) system, allows deeper and wider area treatments.132
Rosacea associated with H. pylori–induced gastritis can be effectively treated by addressing the underlying problem. Although therapists do not treat this condition, clients with other diagnoses often present with this condition also. Clients with this condition should see a physician for adequate medical treatment.
SKIN INFECTIONS
Many bacterial, viral, fungal, and other parasitic skin infections encountered by the therapist are not the primary focus of intervention but rather occur in clients who are hospitalized or being treated for some other condition. Many of these skin disorders are contagious (Table 10-3) and require careful handling by all health care professionals to avoid spreading the infection and becoming contaminated themselves.
Table 10-3
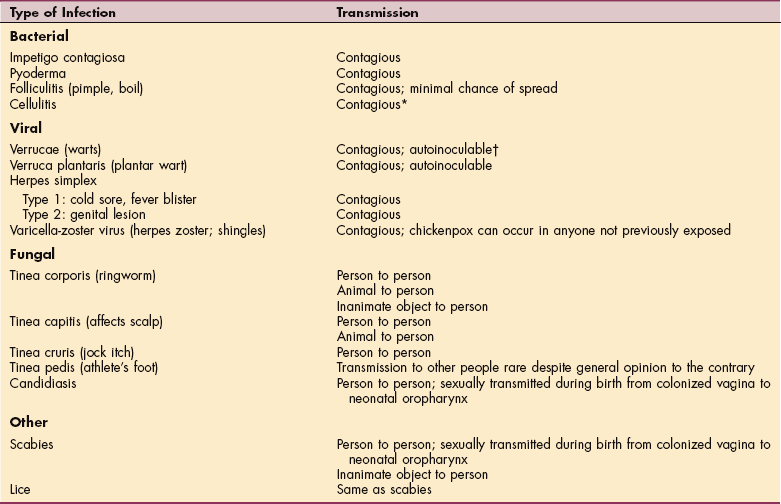
*Technically, cellulitis is contagious, but from a practical point of view the chances of this spreading are very low and would require a susceptible host, for example, an open cut on the therapist’s hand coming in contact with blood or pus from the client’s open wound.
†Capable of spreading infection from one’s own body by scratching.
Sources of infection differ depending on the disease and mode of transmission (see also Chapter 7). Predisposing factors to skin infections include decreased resistance, dehydrated skin, burns or pressure ulcers, decreased blood flow, contamination from nasal discharge, poor hygiene, and crowded living conditions. Only the most common skin infections encountered in the therapy or rehabilitation setting are discussed further in this section.
Bacterial Infections
Normally the skin harbors a variety of bacterial flora, including the major pathogenic varieties of staphylococci and streptococci. The degree of their pathogenicity depends on the invasiveness and toxigenicity of the specific organisms, the integrity of the skin, the barrier of the host, and the immune and cellular defenses of the host. Organisms usually enter the skin through abrasions or puncture wounds of the hands.
In the therapist’s practice, periwound care requires cleaning away from the wound opening to avoid introducing bacteria from the surrounding skin into the wound. Clinical infection develops 3 to 7 days after inoculation. Septicemia can develop if treatment is not provided or if the person is immunocompromised.
People at risk for the development of bacterial infections include children and adults who are immunocompromised, such as occurs with acquired or inherited immunodeficiency; anyone in a debilitated physical condition; those receiving immunosuppressive therapy; and those with a generalized malignancy, such as leukemia or lymphoma.
All these factors emphasize the importance of careful handwashing and cleanliness to prevent spread of infection before and after caring for infected people and their lesions.
Some conditions (e.g., impetigo) are easily spread by self-inoculation; therefore the affected person must be cautioned to avoid touching the involved area. Follicular lesions should not be squeezed because this will not hasten the resolution of the infection and may increase the risk of making the lesion worse or spreading the infection.
Impetigo
Definition and Overview.: Impetigo is a superficial skin infection commonly caused by staphylococci or streptococci. It is most commonly found in infants, young children 2 to 5 years of age, and older people. Predisposing factors include close contact in schools, overcrowded living quarters, poor skin hygiene, anemia, malnutrition, and minor skin trauma. It can be spread by direct contact, environmental contamination, or an arthropod vector. Impetigo often occurs as a secondary infection in conditions characterized by a cutaneous barrier broken to microbes, such as eczema or herpes zoster excoriations.
Clinical Manifestations.: Small macules (flat spots) rapidly develop into vesicles (small blisters) that become pustular (pus-filled). When the vesicle breaks, a thick yellow crust forms from the exudate, causing pain, surrounding erythema, regional adenitis (inflammation of gland), cellulitis (inflammation of tissue), and itching.
Scratching spreads infection, a process called autoinoculation. Lesions frequently affect the face, heal slowly, and leave depigmented areas. If the infection is extensive, malaise, fever, and lymphadenopathy may also be present. A less common presentation occurs with few isolated bullae.
MEDICAL MANAGEMENT
Single small lesions can often be managed by soaking them for 10 minutes with drying agents (Burow’s solution). Oral antibiotics are regularly used to treat impetigo. Rarely, extensive lesions require systemic antibiotics to reduce the risk of glomerulonephritis and to prevent this contagious condition from spreading. A skin swab culture may be necessary to determine the contaminating organism.
Cellulitis
Cellulitis is a rapidly spreading acute inflammation with infection of the skin and subcutaneous tissue that spreads widely through tissue spaces. Streptococcus pyogenes or Staphylococcus is the usual cause of this infection in adults and Haemophilus influenzae type b in children, although other pathogens may be responsible. Clients at increased risk for cellulitis include older adults and people with lowered resistance from diabetes, malnutrition, steroid therapy, and the presence of wounds or ulcers.
Other predisposing factors include the presence of edema or other cutaneous inflammation or wounds (e.g., tinea, eczema, burns, trauma). Venous insufficiency or stasis, thrombophlebitis, surgery, substance abuse, immunocompromise (e.g., HIV infection, chemotherapy, autoimmune diseases, chronic use of immunosuppressants), and lymphedema also predispose individuals to this condition. There is a tendency for recurrence, especially at sites of lymphatic obstruction. See also the sections on Streptococcal Cellulitis in Chapter 8 and Lymphangitis in Chapter 13.
Cellulitis of the breast can occur following breast conservation therapy for breast cancer. Although only a minority of women who undergo this therapy will develop breast cellulitis, the therapist may be the first to observe signs of this disorder. A definitive pathogen has not been identified, and recurrent breast cellulitis is possible months to years after the procedure is completed. Local breast findings include the skin changes typical of cellulitis with or without fever.5
Cellulitis usually occurs in the loose tissue beneath the skin, but it may also occur in tissues beneath mucous membranes or around muscle bundles. The skin is erythematous, edematous, tender, and sometimes nodular. It can develop under the skin anywhere but affects the extremities most often.
Erysipelas, a surface cellulitis of the skin, affects the upper dermis and is characterized by patches of skin that are red and painful with sharply defined borders and that feel hot to the touch. Red streaks extending from the patch indicate that the lymph vessels have been infected. Facial cellulitis involves the face, especially the cheek or periorbital or orbital tissues; the neck may also be affected. Pelvic cellulitis involves the tissues surrounding the uterus and is called parametritis.
Intravenous (IV) antibiotic infusion is the primary treatment. Good nutrition and hydration are advised to help fight infection, repair tissue, and remove bacteria and their by-products. Extensive cellulitis requires surgical debridement of the necrotic tissue. Lymphangitis may occur if cellulitis is untreated, and gangrene, metastatic abscesses, and sepsis can result.
Viral Infections
Viruses are intracellular parasites that produce their effect by using the intracellular substances of the host cells. Viruses are composed only of DNA or ribonucleic acid (RNA), not both, usually enclosed in a protein shell, and are unable to provide for their own metabolic needs or to reproduce themselves.
After a virus penetrates a cell of the host organism, it sheds the outer shell and disappears within the cell, where the nucleic acid core stimulates the host cell to form more virus material from its own intracellular substance. In a viral infection the epidermal cells react with inflammation and vesiculation (as in herpes zoster) or by proliferating to form growths (warts).
Herpes Zoster
Definition, Incidence, and Risk Factors.: Herpes zoster, or shingles, is a local disease brought about by the reactivation of the same virus, varicella-zoster virus (VZV), that causes a systemic disease called varicella (chickenpox). The initial infection with varicella-zoster virus is common during childhood. Shingles may occur and recur at any age, although peak incidence occurs between ages 50 and 70 years.
An estimated 300,000 episodes of zoster occur annually. Of these episodes, 95% are first occurrences and 5% are recurrences. By age 80 years, almost 15% of persons will have experienced at least one episode of zoster.4 The disease is usually brought on by an immunocompromised state, such as occurs with stress, advancing age, underlying malignancy, organ transplantation, or acquired immunodeficiency syndrome (AIDS).
Pathogenesis.: Herpes zoster results from reactivation of varicella virus that has been dormant in the cerebral ganglia (extramedullary ganglia of the cranial nerves) or the ganglia of posterior nerve roots from a previous episode of chickenpox.
The immunologic mechanism that controls latency of VZV is not well understood. One explanation is that the virus multiplies as it is reactivated and that it is neutralized by antibodies remaining from the initial infection. If effective antibodies are not present, the virus continues to multiply in the ganglia, destroying the host neuron and spreading down the sensory nerves to the skin. Factors associated with recurrent disease include aging, immunosuppression, intrauterine exposure to VZV, and varicella at a young age (less than 18 months).4
Clinical Manifestations.: The vesicular eruption of zoster generally occurs unilaterally in the distribution of a specific dermatome supplied by a dorsal root or extramedullary cranial nerve sensory ganglion. Most often, this involves the trunk or the area of the fifth cranial nerve. Two to four days before the eruption the affected person may have some warning (prodromal symptoms) that the virus has become reactivated, especially in repeat incidences.
Early symptoms of pain and tingling along the affected spinal or cranial nerve dermatome are usually accompanied by fever, chills, malaise, and GI disturbances. One to three days later red papules are seen along a dermatome (Fig. 10-7). The lesions most commonly spread unilaterally around the thorax or vertically over the arms or legs.
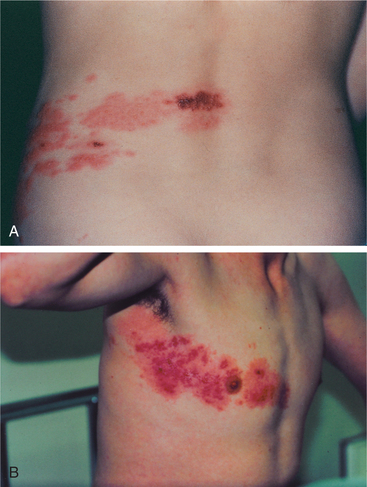
Figure 10-7 Herpes zoster (shingles). A, Lesions appear unilaterally along the path of a spinal nerve. B, Eruptions involving the T4 dermatome. (A, From Callen J, Greer K, Hood H, et al: Color atlas of dermatology, Philadelphia, 1993, Saunders. B, From Marx J, Hockberger R, Walls R: Rosen’s emergency medicine: concepts and clinical practice, ed 6, St Louis, 2006, Mosby.)
Herpes papules rapidly develop into vesicles that vary in size and may be filled with clear fluid or pus. The vesicles are confined to the distribution of the infected nerve root and begin to dry 5 days after eruption with gradual, progressive healing over the next 2 to 4 weeks.
Postherpetic neuralgia, or pain in the area of the recurrence that persists after the lesions have resolved, is a distressing complication of zoster with no adequate therapy currently available. Incidence of postherpetic neuralgia increases sharply in people over the age of 60 years and may last as long as 1 year after the episode of zoster. Children are unaffected by postherpetic pain.
In the adult, severe neuralgic pain can occur in peripheral areas innervated by the nerves arising in the inflamed root ganglia. The pain may be constant or intermittent and vary from light burning to a deep visceral sensation. The cause of postherpetic neuralgia is not fully understood. Scarring and degenerative changes involving the nerve trunks, ganglia, and skin may be important factors. The incidence of scarring and hyperpigmentation is much higher in older adults.
Occasionally herpes zoster involves the cranial nerves, especially the trigeminal and geniculate ganglia or the oculomotor nerve. Geniculate zoster may cause vesicle formation in the external auditory canal, ipsilateral facial palsy, hearing loss, dizziness, and loss of taste. Trigeminal ganglion involvement causes eye pain and possibly corneal and scleral damage with loss of vision.
In rare cases, herpes zoster leads to generalized central nervous system (CNS) infection, muscle atrophy, motor paralysis (usually transient), acute transverse myelitis, and ascending myelitis. More often, generalized infection causes acute retention of urine and unilateral paralysis of the diaphragm.
MEDICAL MANAGEMENT
Diagnosis is usually based on clinical examination and recognition of the skin lesions with accompanying systemic signs of infection. Laboratory diagnosis may include culture and histologic examination of a skin biopsy specimen.
Differentiation of herpes zoster from localized herpes simplex requires staining of antibodies from vesicular fluid and identification using a fluorescent monoclonal antibody test that is very sensitive and specific. For those individuals who are uncertain whether they have had childhood varicella, a variety of serologic tests for the varicella antibody are available.
TREATMENT.
There is no curative agent for shingles, but supportive treatment to relieve itching and neuralgic pain is provided. The use of systemic corticosteroids within the first week of eruption may abort the attack and appears to reduce both the acute symptoms and the risk of postherpetic neuralgia in older persons.
Acyclovir (Zovirax) seems to stop the progression of the rash and prevents visceral complications. Famciclovir, an oral drug, is comparable to acyclovir in effectiveness but has a longer duration of action and requires less frequent dosing. Valacyclovir (Valtrex) is dosed only three times daily and has been shown in studies to decrease postherpetic neuralgia and shorten duration of symptoms.
Hospitalized clients with varicella-zoster should be placed in isolation rooms, and personnel entering the room should wear gowns, gloves, and masks. Eye involvement in zoster requires ophthalmologic evaluation and treatment.
A live varicella virus vaccine (Varivax) is available for use in persons 12 months of age or older who have not had varicella. The Advisory Committee on Immunization Practices (ACIP) also recommends the vaccine for use in susceptible persons following exposure to varicella. Data from the United States and Japan collected in a variety of settings indicate that varicella vaccine is effective in preventing illness or modifying the severity of illness if used within 3 days, and possibly up to 5 days, of exposure.4
The vaccine provides long-lasting (but not lifelong) immunity with an 80% to 85% efficacy. Vaccine breakthrough cases are common but mild. Persons present with fewer lesions (usually less than 50) and lack systemic symptoms (such as fever).
The first shingles vaccine (Zostavax; zoster vaccine live) has been approved for adults age 60 and older. Zostavax has been shown to reduce the incidence of shingles by 51% and the incidence of postherpetic neuralgia by 67% in adults age 60 and older. Among people who get shingles despite being vaccinated, it can reduce its severity. Approval of this drug for use in adults ages 50 to 59 is pending more evidence to support its safety and effectiveness in this age group.111
PROGNOSIS.
Overall prognosis is good unless the infection spreads to the brain (rare). Most people recover completely, with the possible exception of scarring and, with corneal damage, visual impairment. Occasionally, intractable pain associated with neuralgia may persist for months or years. Those persons who develop postherpetic neuralgia may require further medical intervention.
Warts (Verrucae)
Warts are common, benign viral infections of the skin and adjacent mucous membranes caused by human papillomaviruses (HPVs). There are more than 50 different varieties of these viruses depending on their location on the skin. The incidence of warts is highest in children and young adults, but warts can occur at any age. Transmission is probably through direct contact, but autoinoculation is possible.
Warts may appear singly or as multiple lesions with thick white surfaces containing many pointed projections. Clinical manifestations depend on the type of wart and its location. The most common wart (verruca vulgaris) is referred to as such and appears as a rough, elevated, round surface most frequently on the extremities, especially the hands and fingers. Plantar warts are slightly elevated or flat, occurring singly or in large clusters referred to as mosaic warts, primarily at pressure points of the feet.
MEDICAL MANAGEMENT
Diagnosis is usually made on the basis of visual examination. Plantar warts can be differentiated from corns and calluses by certain distinguishing features. Plantar warts obliterate natural lines of the skin, may contain red or black capillary dots that are easily discernible if the surface of the wart is shaved down with a scalpel, and are painful on application of pressure. Both plantar warts and corns have a soft, pulpy core surrounded by a thick callous ring; plantar warts and calluses are flush with the skin surface.
TREATMENT.
Some warts respond to simple treatment, and some disappear spontaneously. Warts can be chronic or recurrent. Many treatment regimens are available. The specific choice of treatment method is influenced by the location of the wart or warts, size and number of warts, presence of secondary infection, amount of tenderness present on palpation, age and gender of the client, history of previous treatment, and individual compliance with treatment. Over-the-counter salicylic acid preparations (e.g., DuoFilm, Wart-Off, Clear Away, or other wart-removing compounds) applied topically may be used to induce peeling of the skin.
Cryotherapy is performed with either liquid nitrogen or solid carbon dioxide. This procedure is widely used as the cosmetically preferred treatment choice, but it is painful. The procedure causes epidermal necrosis; the area dries and peels off together with the wart.
Acids in liquid form or as a paste (salicylic acid, lactic acid) can be painted on warts daily, removed after 24 hours, and reapplied. This treatment choice is not recommended for areas where perspiration is heavy, for areas likely to get wet, or for exposed body parts where patches are cosmetically undesirable. Acid therapy requires a commitment from the client or family to perform it on a daily basis.
Electrodesiccation and curettage of warts are widely used for common warts and occasionally for plantar warts. High-frequency electric current destroys the wart and is followed by surgical removal of dead tissue at the base with application of an antibiotic ointment and bandage for 48 hours. Atrophic scarring may occur, and the recurrence rate is 20% to 40%.
The use of mechanical (nonthermal) ultrasound has been advocated by some in the treatment of plantar warts, but this has not been widely accepted by the medical community.
Fungal Infections (Dermatophytoses)
Fungal infections such as ringworm are caused by a group of fungi that invade the stratum corneum, hair, and nails.57 These are superficial infections by fungi that live on, not in, the skin and are confined to the dead keratin layers, unable to survive in the deeper layers. Since the keratin is being shed (desquamated) constantly, the fungus must multiply at a rate that equals the rate of keratin production to maintain itself; otherwise the organisms would be shed with the discarded skin cells.
Fungal infections will spread without treatment; antifungal creams are available over the counter, but diagnosis is required to identify the skin lesion.
Ringworm (Tinea Corporis)
Dermatophytoses, or fungal infections of the hair, skin, or nails, are designated by the Latin word tinea, with further designation related to the affected area of the body (see Table 10-3). Tinea corporis, or ringworm, has no association with worms but rather is marked by the formation of ring-shaped pigmented patches covered with vesicles or scales that often become itchy (Fig. 10-8). Transmission can occur directly through contact with infected lesions or indirectly through contact with contaminated objects, such as shoes, towels, or shower stalls.
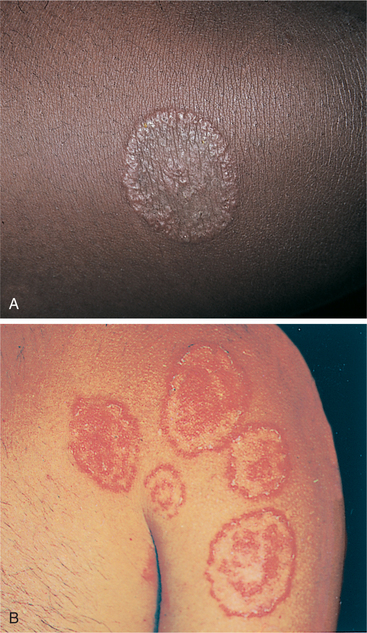
Figure 10-8 Tinea corporis (ringworm). A, Scales forming circular lesions with clear centers are characteristic of tinea corporis (ringworm). B, Most adults or children present with multiple lesions that are hyperpigmented in Caucasians and depigmented in dark-skinned people. The lesions occur most often on the face, chest, abdomen, and back of arms. (A, From Zitelli BJ, Davis HW: Atlas of pediatric physical diagnosis, St Louis, 2002, Mosby. B, From Habif T: Clinical dermatology, ed 4, St Louis, 2004, Elsevier.)
Diagnosis can be made through laboratory examination of the affected skin. Treatment for any type of ringworm requires maintaining clean, dry skin and applying antifungal powder or topical agent as prescribed.
Treatment with the drug griseofulvin may take weeks to months to complete and should be continued throughout the prescribed dosage schedule even if symptoms subside. Possible side effects of this agent include headache, GI upset, fatigue, insomnia, and photosensitivity. Prolonged use of this drug requires monitoring of liver function. Oral medication is reserved for clients with more involved cases.
Occasionally an obese client with tinea corporis is referred to therapy for wound care secondary to skin breakdown. Advanced wound dressings may be applied to areas of moist, denuded skin to optimize healing.
Athlete’s Foot (Tinea Pedis)
Tinea pedis, or athlete’s foot, causes erythema, skin peeling, and pruritus between the toes that may spread from the interdigital spaces to the sole. Severe infection may result in inflammation, with severe itching and pain on walking. Some individuals develop a strong foot odor as well.
Clean, dry socks and adequate footwear (well-ventilated, properly fitting) are important. After washing the feet and drying thoroughly between the toes, antifungal cream or powder (the latter to absorb perspiration and prevent excoriation) can be applied.
A history of antibiotic use, yeast infections (candidiasis, including intestinal yeast), and other risk factors for candidiasis may contribute to athlete’s foot. If symptomatic treatment including topical preparations does not eradicate the problem, treatment of intestinal yeast may be required.
Other Parasitic Infections
Some parasitic infections of the skin are caused by insect and animal contacts. Contact with insects that puncture the skin for the purpose of sucking blood, injecting venom, or laying their eggs is relatively common. Substances deposited by insects are considered foreign to the host and may create an allergic sensitivity in that individual and produce pruritus, urticaria, or systemic reactions of a greater or lesser degree, depending on the individual’s sensitivity.
Scabies
Definition.: Scabies (mites) is a highly contagious skin eruption caused by a mite, Sarcoptes scabiei. It is a common public health problem with an estimated prevalence of 300 million cases worldwide. The female mite burrows into the skin and deposits eggs that hatch into larvae in a few days.
Scabies is easily transmitted by skin-to-skin contact or by contact with contaminated objects, such as linens or shared inanimate objects. Infections with human T-cell leukemia/lymphoma virus 1 (HTLV-1) and HIV are associated with scabies.29 Mites can spread rapidly between members of the same household, nursing home, or institution, but the inflammatory response and itching do not occur until approximately 30 to 60 days after initial contact.
Clinical Manifestations.: The symptoms include intense pruritus (worse at night), usually excoriated skin, and the burrow, which is a linear ridge with a vesicle at one end. The mite is usually found in the burrow, commonly in the interdigital web spaces, flexor aspects of the wrist (volar surface), axillae, waistline, nipples in females, genitalia in males, and the umbilicus. Intense scratching can lead to severe excoriation and secondary bacterial infection. Itching can become generalized secondary to sensitization.
MEDICAL MANAGEMENT
The mite can be excavated from one end of a burrow with a needle or a scalpel blade and examined under a microscope. In longstanding cases, a mite may not be found. At that point treatment is based on a presumptive diagnosis.
Treatment has traditionally been with a scabicide, usually a lotion or cream containing permethrin or lindane, applied to the entire body from the neck down. Single oral-dose therapy of ivermectin (Stromectol) is an effective treatment for this infestation. Permethrin is generally the treatment of choice for head lice and scabies because of its residual effect and because toxicity and absorption are minimal. Ivermectin may be reserved for cases where permethrin fails39; further research is advocated regarding the safety and effectiveness of ivermectin.
10-7 SPECIAL IMPLICATIONS FOR THE THERAPIST
Impaired Integumentary Integrity Associated with Superficial Skin Involvement
If a hospitalized person has scabies, prevent transmission to self and others by practicing good handwashing technique and by wearing gloves when touching the affected person and a gown when in close contact. Observe wound and skin precautions for 24 hours after treatment of scabies. Gas-autoclave blood pressure cuffs or other equipment used with the affected person before using them on other people. All linens and toweling used must be isolated after use until the person is noninfectious. If the person is treated anywhere outside the hospital room (e.g., on a plinth or treatment mat), the area must be thoroughly disinfected after each session.
In using a scabicide, the individual must understand that NO area can be missed. After 24 hours, the affected person should bathe. All bed linens and clothes must be laundered in hot water or dry-cleaned. Other household members and those in close contact with the affected person should be treated. A second application of the cream or lotion may need to be applied 7 days later. The same procedure is followed.
Itching may persist for 1 to 2 weeks after treatment until the stratum corneum is replaced, but lesions on the forearms or legs can be occluded with Unna’s boots to eliminate the scratch-itch cycle (Fig. 10-9). Widespread bacterial infections require additional treatment with systemic antibiotics.
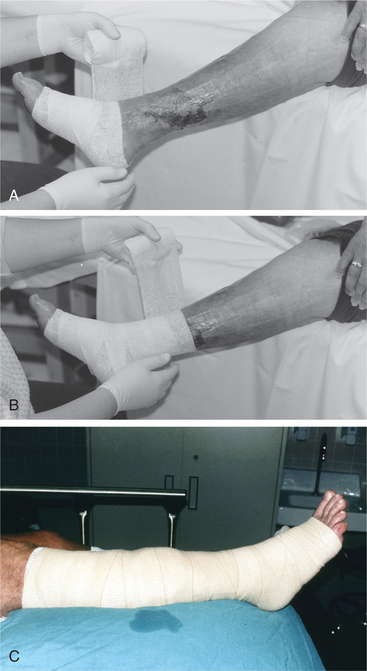
Figure 10-9 A, Unna’s boots. Although most often used in cases of venous insufficiency (the client must be ambulatory to enlist the calf muscle pump), the application of Unna’s boot to the forearms or legs can be used with a variety of skin lesions to eliminate the scratch-itch cycle. Unna’s boot is a dressing made of gauze impregnated with gelatin, zinc oxide, calamine, and glycerin. B, The bandage is applied in a spiral fashion and allowed to dry, forming a semi-rigid dressing. This dressing can be allowed to stay intact for 7 days. C, A four-layer gradient compression wrap (Profore) provides sustained compression for up to 1 week, for both ambulatory and nonambulatory clients. (A and B, Courtesy Pam Unger, PT, Community General Hospital, Center for Wound Management, Reading, PA, 1995. C, Courtesy Harriett B. Loehne, PT, DPT, CWS, FCCWS, Archbold Center for Wound Management, Thomasville, GA, 2006. Used with permission.)
Pediculosis (Lousiness)
Pediculosis is an infestation by Pediculus humanus, a very common parasite infecting the head, body, and genital area. Transmission is from one person to another, usually on shared personal items, such as combs, lockers, clothes, or furniture. Lice are not carried or transmitted by pets. School-age children are easily infected as are people who live in overcrowded surroundings and those older adults who have poor personal hygiene, depend on others for care, or live in a nursing home.
Pediculus humanus var. capitis, the head louse, is transmitted through personal contact or through shared hairbrushes or shared head wear. Severe itching accompanied by secondary eczematous changes develops, and small greyish or white nits (eggs) are usually seen attached to the base of the hair shafts.
Pediculus corporis, the body or clothes louse, produces intense itching, which in turn results in severe excoriations from scratching and possible secondary bacterial infections. The lice or nits are generally found in the seams of the affected individual’s clothing.
Pediculus pubis (Phthirus pubis), the pubic or crab louse, is usually transmitted by sexual contact but can be transferred on clothing or towels. The lice and nits are usually found at the base of the pubic hairs. Sometimes dark brown particles (louse excreta) may be seen on underclothes.
MEDICAL MANAGEMENT
Traditional treatment has been with the appropriate cleaning solution (e.g., shampoo or soap containing permethrin) specific to the type of louse present. As with scabies, single oral-dose therapy of ivermectin (Stromectol) is an effective treatment for this infestation (see previous section on Scabies).
SKIN CANCER
The American Cancer Society (ACS) estimates that skin cancers are the most prevalent form of cancer, eventually affecting nearly all Caucasian people older than 65 years of age. Skin cancer is the most rapidly increasing cancer in the United States, with over 1 million new cases of nonmelanoma (i.e., basal and squamous cell) skin cancer diagnosed annually in the United States. There is no evidence that this epidemic has peaked.70,141
Solar radiation (exposure to midrange-wavelength ultraviolet B [UVB] radiation) causes most skin cancers, and protection from the sun during the first two decades of life significantly reduces the risk of skin cancer (Box 10-7). The melanoma rate is rising most rapidly in persons younger than 40 years of age and is now the most common cancer in women between the ages of 25 and 29 years and second only to breast cancer in the age group from 30 to 34 years.
In this chapter, skin cancer is discussed in three broad categories: benign, premalignant, and malignant (Box 10-8). Malignant lesions of the skin are considered as either melanoma or nonmelanoma. Kaposi’s sarcoma, which occurs in the skin, is not included in these categories and is discussed separately in this chapter.

Benign skin lesions, such as seborrheic keratosis or nevi (moles), do not usually undergo transition to malignant melanoma and do not usually require treatment. Although most moles remain benign skin lesions, when malignant melanoma does occur, it often arises from a preexisting mole, derived from pigment cells (melanocytes) of the skin.
Keratoacanthomas do require treatment. Precancerous lesions, such as actinic keratosis or Bowen’s disease, may progress to malignancy and must be carefully evaluated. The most common types of (nonmelanoma) malignant skin cancer are basal call carcinoma and squamous cell carcinoma.
These carcinomas occur twice as often in Caucasian men as in Caucasian women, and the incidence increases steadily with age. A third type of malignant skin cancer (also affecting Caucasian men more than Caucasian women), malignant melanoma, is the most serious skin cancer, resulting in early metastasis and possible death.
Benign Tumors
Seborrheic keratosis is a hereditary benign proliferation of basal cells occurring most frequently after middle age and presenting as multiple lesions on the chest, back, and face. The lesions also often appear following hormonal therapy or inflammatory dermatoses. The areas are waxy, smooth, or raised lesions that vary in color from yellow to flesh tones to dark brown or black. Their size varies from barely palpable to large verrucous (wartlike) plaques. These tumors are usually left untreated unless they itch or cause pain. Otherwise, cryotherapy with liquid nitrogen is an effective treatment.
Nevi (Moles)
Nevi are pigmented or nonpigmented lesions that form from aggregations of melanocytes beginning early in life. Most moles are brown, black, or flesh-colored and may appear on any part of the skin. They vary in size and thickness, occurring in groups or singly.
Nevi seldom undergo transition to malignant melanoma, but as previously mentioned, when malignant melanoma does occur, it often arises from a preexisting mole; the chances of cancerous transformation are increased as a result of constant irritation. Any change in size, color, or texture of a mole; bleeding; or any excessive itching should be reported to a physician.
Precancerous Conditions
There are two common premalignant skin lesions: actinic keratosis and Bowen’s disease.
Actinic Keratosis
Actinic keratosis (also known as solar keratosis) is a skin disease resulting from many years of exposure to the sun’s UV rays. The damage caused by overexposure to sunlight results in abnormal cell growth, causing a well-defined, crusty, or sandpaper-like patch or bump that appears on chronically sun-exposed areas of the body (e.g., face, ears, lower lip, bald scalp, dorsa of hands and forearms).
The base may be light or dark, tan, pink, red, or a combination of these, or it may be the same color as the skin. The scale or crust is horny, dry, and rough; it is often recognized by touch rather than sight. Occasionally it itches or produces a pricking or tender sensation. The skin abnormality or lesion develops slowly to reach a size that is most often 3 to 6 mm. It may disappear only to reappear later. Often there are several actinic keratoses present at one time.
Actinic keratosis affects nearly 100% of the older Caucasian population. It is most common in fair-complexioned, blue-or green-eyed, middle-aged men with a history of sun exposure (solar radiation). The number of lesions that develops is directly related to heredity and lifetime exposure to the sun.
There is a known risk of malignant degeneration and subsequent metastatic potential in neglected lesions. Almost half of the estimated 5 million current cases of skin cancer began as actinic keratosis lesions. It is important that this condition be diagnosed properly, because it is often difficult to distinguish a large or hypertrophic actinic keratosis from a squamous cell carcinoma. A biopsy may be indicated.
Not all keratoses need to be removed. The decision about treatment protocol is based on the nature of the lesion, the number of lesions, and the age and health of the affected person. Treatment may be with 5-fluorouracil (5-FU, Efudex), a topical antimetabolite that inhibits cell division, or masoprocol cream; cryosurgery using liquid nitrogen; or curettage by electrodesiccation (superficial tissue destruction through the use of bursts of electrical current).
These clients should be advised to avoid sun exposure and use a high-potency (sun protection factor [SPF] 15) sunscreen 30 to 60 minutes before going outside. SPF 30 is recommended for people of fair complexion. Sunscreens are not recommended for infants under 6 months of age. Infants should be kept out of the sun or shaded from it. Fabric with a tight weave, such as cotton, is suggested.
Some conditions call for more invasive treatments, such as laser resurfacing (outer layers of the skin are vaporized) or chemical peels (outer layers are burned off via chemical solution). In June 2000 the U.S. Food and Drug Administration (FDA) approved the use of photodynamic treatment of actinic keratosis of the face and scalp using a topical application (Levulan Kerastick) followed by exposure to a nonlaser blue light source. This is a painful and involved treatment requiring application of Levulan 16 hours prior to exposure to the light source.
Bowen’s Disease
Bowen’s disease can occur anywhere on the skin (exposed and unexposed areas) or mucous membranes (especially the glans penis in uncircumcised males). It presents as a persistent, brown to reddish brown, scaly plaque with well-defined margins. Often the person has a history of arsenic exposure in youth. Multiple lesions have been associated with an increased number of internal malignancies and therefore require close follow-up. Treatment is with surgical excision and topical 5-FU.
Malignant Neoplasms
Definition and Overview.: Basal cell carcinoma is a slow-growing surface epithelial skin tumor originating from undifferentiated basal cells contained in the epidermis. This type of carcinoma rarely metastasizes beyond the skin and does not invade blood or lymph vessels but can cause significant local destruction.
Until recently, this tumor rarely appeared before age 40 years and was more prevalent in blond, fair-skinned males. In the age group under 30 years, more women than men develop skin cancer associated with the use of indoor tanning booths with concentrated doses of UV radiation. It is the most common malignant tumor affecting Caucasians, with a reported 100,000 new cases each year; African Americans and Asians are rarely affected.
Etiologic and Risk Factors.: Prolonged sun exposure and intermittent sun exposure are the most common causes of basal cell carcinoma; but immunosuppression (e.g., organ transplant recipients, individuals who are HIV positive), genetic predisposition, and rarely, the site of vaccinations are other possible causes. Immunosuppressed organ transplant recipients are more likely to develop squamous cell carcinoma, whereas HIV-infected adults are far more likely to have basal cell carcinoma.
These lesions are seen most frequently in geographic regions with intense sunlight in people with outdoor occupations and on those areas most exposed, the face and neck. Dark-skinned people are rarely affected because their basal cells contain the pigment melanin, a protective factor against sun exposure. Anyone who has had one basal cell carcinoma is at increased risk of developing others. Recurrences of previously treated lesions are possible, usually within the first 2 years after initial treatment.
Pathogenesis.: The pathogenesis of basal cell tumors remains uncertain, and basal cell carcinoma is considered biologically unusual. It is a stable growth characterized by monotonous structure (the same in small as well as large tumors), the absence of progression to metastasis, and a small amount of chromosomal damage (as compared with moderate chromosomal damage associated with squamous cell carcinoma).
To the dismay of investigators seeking to design experiments, basal cell carcinomas are very seldom seen in animals and not found in laboratory rodents at all. Whereas squamous cell carcinoma is often preceded by a precursor (actinic keratosis), there are no known precursors to basal cell carcinoma. This fact suggests that basal cell carcinoma tumors need only a few mutations to induce malignant transformation.114
One theory suggests that these tumors arise as a result of a defect that prevents the cells from being shed by the normal keratinization process. The process of epidermal cell maturation is called keratinization because the cells synthesize a fibrous protein called keratin. Basal cells that lack the normal keratin proteins form basal cell tumors. Another hypothesis is that undifferentiated basal cells become carcinomatous instead of differentiating into sweat glands, sebum, and hair. See also the section on Squamous Cell Carcinoma: Pathogenesis.
Clinical Manifestations.: Basal cell carcinoma (Fig. 10-10) typically has a pearly or ivory appearance, has rolled edges, and is slightly elevated above the skin surface, with small blood vessels on the surface (telangiectasia) (see Fig. 10-3).
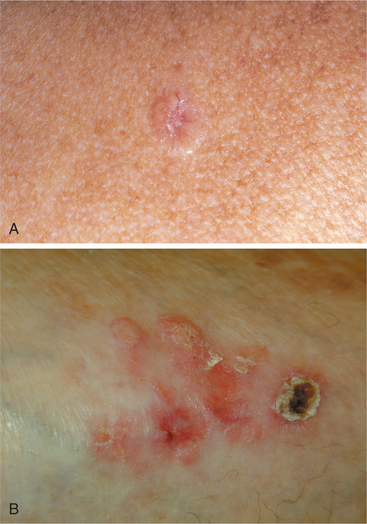
Figure 10-10 Basal cell carcinoma. A, Skin cancer in the form of basal cell carcinoma can appear as a shiny, pearly, or translucent pink, red, or white bump. There may be a rolled border with an indented center. B, This type of skin cancer may also present as a red patch; a crusty, open sore that will not heal; or a scarlike area. (A, From Lookingbill D, Marks J: Principles of dermatology, ed 3, Philadelphia, 2000, Saunders. B, From Townsend C, Beauchamp RD, Evers BM, Mattox K: Sabiston textbook of surgery, ed 17, Philadelphia, 2004, Saunders.)
The nodule is usually painless and slowly increases in size and may ulcerate centrally. More than 65% of basal cell carcinomas are found on the head and neck. Other locations are the trunk, especially the upper back and chest.
They also can appear similar to Bowen’s disease, chronic venous ulcer (Fig. 10-11), or squamous cell carcinoma in a flatter, scaling lesion, usually on the trunk or extremities.

Figure 10-11 Chronic venous ulcer. Basal cell carcinoma can also mimic a chronic venous ulcer potentially causing a delay in diagnosis. Biopsy is required to make the definitive medical diagnosis. (Courtesy Harriett B. Loehne, PT, DPT, CWS, FCCWS, Archbold Center for Wound Management, Thomasville, GA, 2006. Used with permission.)
MEDICAL MANAGEMENT
Diagnosis by clinical examination of appearance must be confirmed via biopsy and histologic study. Treatment depends on the size, location, and depth of the lesion and may include curettage and electrodesiccation, chemotherapy, surgical excision, and irradiation.
Mohs’ micrographic surgery is the gold standard treatment in which the specimen is excised, frozen-sectioned, and examined for positive margins while the client waits, thus ensuring clean margins before complex repairs are performed. Irradiation is used if the tumor location requires it and in older or debilitated people who cannot tolerate surgery.
Radiation therapy is generally contraindicated in persons less than 50 years of age because of the risk of recurrence and the development of secondary radiation-induced tumors of the skin. Radiotherapy can be followed by chronic skin ulcers that are difficult to close, much less heal. Some radiation-induced ulcers open on and off for years, and some just develop 10 to 20 years after the radiation therapy.136
If the tumor is identified and treated early, local excision or even nonexcisional destruction is usually curative. Skin grafting may be required in cases where large areas of tissue have been removed. A new experimental treatment called photodynamic therapy (PDT) is being investigated in the treatment of superficial nonmelanoma skin cancers. This technique requires the administration of a drug that induces photosensitivity, followed in 48 to 72 hours by exposure to light that helps outline the tumor. The tumor cells concentrate this drug so as to allow selective destruction of the cancer cells when exposed to a laser light of 630 nm.75,150
Clinical trials are under way investigating the use of chemopreventive agents, such as vitamin A analogues called retinoids. These topical agents may potentially complement sunscreens and result in decreased incidence, morbidity, and mortality of skin cancer.145
Tretinoin has proven effective in preventing UV-induced lesions and can be considered for high-risk basal or squamous cell carcinoma patients, as well as those with actinic keratosis, realizing that it is off-label use.131 Topical imiquimod was approved by the FDA in 2004 for individuals who have superficial basal cell carcinoma.49
Cytokine therapy, including interferon and interleukin, is a type of systemic immunotherapy used to treat skin cancer. Both cytokines mentioned here have been FDA approved for metastatic melanoma.128
PROGNOSIS.
If left untreated, basal cell lesions slowly invade surrounding tissues over months and years, destroying local tissues such as bone and cartilage, especially around the eyes, ears, and nose.
Squamous Cell Carcinoma
Definition and Overview.: Squamous cell carcinoma is the second most common skin cancer in whites, usually arising in sun-damaged skin, such as the rim of the ear, the face, the lips and mouth, and the dorsa of the hands (Fig. 10-12). It is a tumor of the epidermal keratinocytes and rarely occurs in dark-skinned people.

Figure 10-12 Squamous cell carcinoma can take the form of a persistent scaly, red patch that sometimes crusts or bleeds or an open sore that does not heal. This type of skin cancer may also present as a raised or wartlike growth that may bleed. (From Goldman L: Cecil textbook of medicine, ed 22, Philadelphia, 2004, Saunders.)
Squamous cell tumors may be one of two types: in situ (confined to the site of origin) and invasive (infiltrate surrounding tissue). In situ squamous cell carcinoma is usually confined to the epidermis but may extend into the dermis. Common premalignant skin lesions associated with in situ carcinomas are actinic keratosis and Bowen’s disease (see earlier section).
Invasive squamous cell carcinoma can arise from premalignant lesions of the skin, including sun-damaged skin, actinic dermatitis, scars, whitish discolored areas (leukoplakia), radiation-induced keratosis, tar and oil keratosis, and chronic ulcers and sinuses.
Incidence.: As with basal cell carcinoma, fair-skinned people have a higher incidence of squamous cell carci- noma. This particular type of tumor has a peak incidence at 60 years of age and affects men more than women.
Etiologic and Risk Factors.: Predisposing factors associated with squamous cell carcinoma include cumulative overexposure to UV radiation (e.g., outdoor employment or residence in a warm, sunny climate), burns, presence of premalignant lesions such as actinic keratosis or Bowen’s disease, radiation therapy, ingestion of herbicides containing arsenic, chronic skin irritation and inflammation, exposure to local carcinogens (tar, oil), and hereditary disease such as xeroderma pigmentosum and albinism.
Organ transplant recipients who are chronically immunosuppressed are at risk for the development of recurring squamous cell carcinoma. Rarely, squamous cell carcinoma may develop on the site of a smallpox vaccination, psoriasis, or chronic discoid lupus erythematosus.
Pathogenesis.: UV radiation continues to be one of the most important causes of skin cancer, because the sun’s UV rays damage the DNA inside the nuclei of the epidermal cells, triggering enzymes to repair the damage. We differ in our ability to produce repair enzymes, which may explain our differences in tanning ability as well as susceptibility to skin cancer. Not all DNA lesions are properly repaired, increasing the risk of skin cancer.
Newer studies show that when DNA damage occurs, a cell surface molecule (Fas ligand; FasL) belonging to the tumor necrosis factor family binds to its receptor Fas and attaches to the damaged cells, inducing them to die by apoptosis (i.e., programmed cell death).
These suicidal cells known as keratinocytes take themselves out of action, and the less damaged ones repair themselves. After many years of cumulative sun exposure, keratinocytes can become malignant. But even then, the cancers (either basal or squamous cell) grow slowly and do not spread easily.
On the other hand, melanocytes, the cells that give rise to melanomas, seem highly resistant to self-destruction. After a person gets badly sunburned, damaged melanocytes continue to replicate, increasing the chance that some will turn malignant. These studies suggest that Fas ligand is a critical defense against the accumulation of mutations caused by sunlight exposure. Its absence or inactivation may be key to the development of skin cancer.67,110
Clinical Manifestations.: Squamous cell lesions are more difficult to characterize than basal cell tumors. The squamous cell tumor has poorly defined margins, since the edge blends into the surrounding sun-damaged skin.
This type of carcinoma can present as an ulcer, a flat red area, a cutaneous horn, an indurated plaque, or a nodule. It may be red to flesh-colored and surrounded by scaly tissue. More than 80% of squamous cell carcinomas occur in the head and neck region.
Malignant transformation of any chronic wound can occur (Fig. 10-13). Marjolin’s ulcer is the term given to aggressive epidermoid tumors that arise from areas of chronic injury and form squamous cell carcinomas. Healed burn wounds are common sites, but any chronic wound can transform into a malignancy. Dr. Jean Nicolas Marjolin first described the occurrence of ulcerating lesions within scar tissue in 1828. If these lesions are not detected and treated early, they may invade deep tissues and ulcerate (see Prognosis).

Figure 10-13 Marjolin’s ulcer. This large lesion constitutes a Marjolin’s ulcer. The client had a history of venous ulcers and had been treated for many months by home health nurses with no improvement. She was seen at the Archbold Center for Wound Management; a biopsy was done immediately with a fresh-frozen section, and a diagnosis of Marjolin’s was made. The cancer had metastasized to the bone, and a below-knee amputation was required. It was never clear whether the cancer began in a new ulcer or in scar tissue from a previous ulcer. (Courtesy Harriett B. Loehne, PT, DPT, CWS, FCCWS, Archbold Center for Wound Management, Thomasville, GA, 2006. Used with permission.)
Usually lesions on unexposed skin tend to be more invasive and more likely to metastasize, with the exception of lesions on the lower lip and ears. These sites tend to metastasize early, beginning with the process of indu- ration and inflammation of the lesion. Metastasis can occur to the regional lymph nodes, producing characteristic systemic symptoms of pain, malaise, fatigue, weakness, and anorexia.
MEDICAL MANAGEMENT
DIAGNOSIS, TREATMENT, AND PROGNOSIS.
An excisional biopsy provides definitive diagnosis and staging (Table 10-4) of squamous cell carcinoma. Other laboratory tests may be appropriate depending on the presence of systemic symptoms. The size, shape, location, and invasiveness of a squamous cell tumor and the condition of the underlying tissue determine the treatment method selected (see the section on Basal Cell Carcinoma; see also Box 10-7). A deeply invasive tumor may require a combination of techniques. As with all benign, premalignant, or malignant skin lesions, sun protection is vitally important (see Box 10-4).
Table 10-4
Staging of Squamous Cell Carcinoma (Skin)
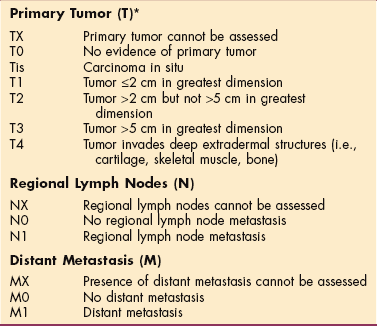
*In the case of multiple simultaneous tumors, the tumor with the highest T category will be classified and the number of separate tumors will be indicated in parentheses, for example, T2 (5).
Used with permission of the American Joint Committee on Cancer (AJCC), Chicago. AJCC handbook for staging of cancer, ed 6, New York, 2002, Springer-Verlag.
All the major treatment methods have excellent rates of cure; generally, the prognosis is better with a well-differentiated lesion in an unusual location.
Malignant Melanoma
Malignant melanoma is a neoplasm of the skin originating from melanocytes or cells that synthesize the pigment melanin. The melanomas occur most frequently in the skin but can also be found in the oral cavity, esophagus, anal canal, vagina, or meninges or within the eye. The clinical varieties of cutaneous melanoma are classified into four types (Fig. 10-14)15:
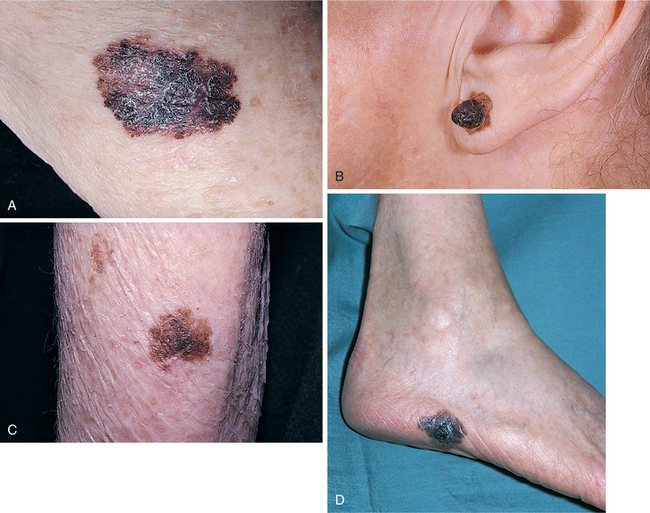
Figure 10-14 A, Superficial spreading melanoma. An irregular margin with multiple colors of black, blue, pale red, and white may be seen. B, Nodular lesion of melanoma. This lesion developed on top of a benign compound nevus. C, Lentigo maligna. If left alone, progression to lentigo maligna melanoma occurs. D, Acral lentiginous melanoma. This brown to black, flat lesion has irregular borders and variable pigmentation. (From Callen JP, Greer K, Paller A, Swinyer L: Color atlas of dermatology, ed 2, Philadelphia, 2000, Saunders. D, Courtesy Dr. Neil A. Fenske, Tampa.)
1. Superficial spreading melanoma (SSM) is the most common type of melanoma and accounts for 75% of cutaneous melanomas. SSM can occur on any part of the body, especially in areas of chronic irritation, the legs of females between the knees and ankles, or the upper back in both genders. SSM is usually diagnosed in people between 20 and 60 years of age. It usually arises in a preexisting mole and presents as a brown or black, raised patch with an irregular border and variable pigmentation (red, white, and blue; brown-black; black-blue). It is usually asymptomatic. With advanced lesions, itching and bleeding may occur.
2. Nodular melanoma can be found on any part of the body with no specific site preference. Men between 20 and 60 years of age are affected more often than women. It is often described as a small, suddenly appearing but quickly enlarging, uniformly and darkly pigmented papule (may be greyish) and accounts for approximately 12% of cutaneous melanomas. This type invades the dermis and metastasizes early.
3. Lentigo maligna melanoma (LMM) is a less common type of lesion occurring predominantly on sun-exposed areas, especially the head, neck, and dorsa of hands or under the fingernails, in the 50-to 80-year-old age group, accounting for 6% to 10% of cutaneous melanomas. This lesion looks like a large (3-to 6-cm), flat freckle with an irregular border containing varied pigmentation of brown, black, blue-black, red, and white found in a single lesion. These lesions enlarge and become progressively irregularly pigmented over time. Approximately one third develop into malignant melanoma and therefore bear careful watching.
4. Acral lentiginous melanoma (ALM) is a relatively uncommon form of melanoma accounting for 5% of all cutaneous melanomas. It is the most common form of melanoma in dark-skinned people (e.g., Africans, Asians). These lesions usually have flat, dark brown portions with raised bumpy areas that are predominantly brown-black or blue-black. Most common areas include low-pigment sites where hair is absent, such as the palms of the hands, soles of the feet, nail beds of fingers and toes, and mucous membranes.
Incidence
Malignant melanoma accounts for up to 5% of all cancers, currently affecting 1 in 75 people in the course of a lifetime. This has increased dramatically from a 1 in 1500 risk of developing melanoma in the 1930s.
Epidemiologists, who report that the incidence of melanoma is doubling every 10 to 20 years, call this a melanoma epidemic. The ACS estimates 62,190 new cases of malignant melanoma in 2006,70 accounting for 7910 deaths, more than from any other skin disorder. The peak incidence is between 40 and 60 years; women are affected more than men but the mortality rate is greater among men. The incidence is rising in younger age groups, but the disorder remains rare in children before adolescence.
Etiologic and Risk Factors
Most people who develop melanoma have blond or red hair, fair skin, and blue eyes; are prone to sunburn; and are of Celtic or Scandinavian ancestry (Box 10-9). These risk factors are believed to be linked to variations in a gene called MC1R that assists in producing melanin pigment to help protect the skin against UV rays.61,123 Not all UVB radiation (280 to 320 nm) but all UVA radiation (320 to 400 nm), the type produced by sun lamps, may promote skin cancer. For these reasons, tanning parlors should also be considered a significant risk factor for the development of skin cancer.
Melanomas appear to be more prevalent among Caucasians of high socioeconomic status who work indoors and tend to take short vacations with intense sun exposure than in people who are at risk of chronic sun exposure. This correlation appears to be related to education, not income.60
Melanoma occurs more often within families and among people who have dysplastic nevus syndrome, also known as the atypical mole syndrome. This is a familial disorder that results in a large number of irregular moles that have an almost 50% chance of developing into melanoma during the person’s lifetime. Puberty and pregnancy may enhance growth. Previous history of melanoma places the individual at greater risk of developing a second melanoma.
Other risk factors include excessive exposure to UV radiation through sunlight or tanning booths, especially intense intermittent exposure, and immune suppression from chemotherapy. There are some reports that airline pilots and flight crews exposed to ionizing radiation of cosmic origin have increased rates of malignant melanoma.13,83,118
Increased cancer risk among all flight personnel has been previously noted, including breast cancer among flight attendants and acute myeloid leukemia among pilots. Further studies are needed to identify specific and potentially preventable risk factors.7,42
Although the evidence is clear that flight personnel have the highest incidence ratio of skin cancer, whether this is a result of excessive exposure to cosmic and UV radiation (which can easily penetrate the cockpit), from flying over multiple time zones (disturbance of circadian rhythm), or from factors related to lifestyle (excessive sunbathing) rather than work conditions remains inconclusive.58,119 Supportive research shows that an 8% to 10% increase in UVB radiation occurs for every 1000 feet of elevation, suggesting a higher incidence of skin cancer at higher elevations.128
Pathogenesis
See the section on Squamous Cell Carcinoma: Pathogenesis.
The majority of malignant melanomas appear to be associated with the intensity rather than the duration of sunlight exposure; that is, most people who develop melanoma work indoors and have intense but limited exposure to the sun on weekends or vacations. This accounts for the location of melanomas most commonly on skin that is covered most of the year.
Clinical Manifestations
Melanoma can appear anywhere on the body, not just on sun-exposed areas. Common sites are the head and neck in men, the legs in women, and the backs of people exposed to excessive UV radiation. Up to 70% arise from a preexisting nevus. Any change in a skin lesion or nevus (increased size or elevation; bleeding; soreness or inflammation; changes in color, pigmentation, or texture) must be examined for melanoma (Fig. 10-15).
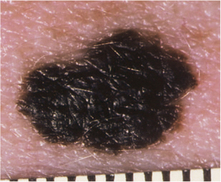
Figure 10-15 Malignant melanoma. Warning signs of malignant melanoma include asymmetry, irregular border, two or more shades of color, and diameter as outlined in Box 10-10. Any other changes in moles or skin lesions (e.g., itchiness, tenderness, swelling, redness, softening, or hardening) should be evaluated by a physician. (From Goldman L: Cecil textbook of medicine, ed 22, Philadelphia, 2004, Saunders.)
MEDICAL MANAGEMENT
Early recognition of cutaneous melanomas can have a major impact on the surgical cure of this disease. The ACS suggests a monthly self-examination. A skin biopsy with histologic examination can distinguish malignant melanoma from other lesions, determine tumor thickness, and provide staging.
There are several techniques for staging skin cancer. The Breslow method measures the thickness of the melanoma; the thinner the melanoma, the better the prognosis. Generally, melanomas less than 1 mm in depth have a very small chance of spreading. A second system (Clark’s levels) used to determine the appropriate stage evaluates the layers of skin that are invaded by the melanoma (Fig. 10-16).
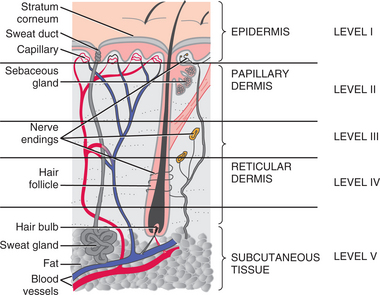
Figure 10-16 Clark’s levels, a system of classifying tumor progression according to skin layer penetration. Level I involves only the epidermis, level II has spread to the dermis, level III involves most of the upper dermis, level IV has spread to the lower dermis, and level V indicates the cancer has spread to the subcutis. The higher the level, the greater the chance that metastasis has occurred.
A third method of staging, TNM, combines both previously described methods (Table 10-5). Depending on the depth of the tumor invasion and metastatic spread, other testing procedures may be used, including baseline laboratory studies, a bone scan for metastasis, or computed tomographic (CT) scan for metastasis to the chest, abdomen, CNS, and brain.
Table 10-5
Staging of Malignant Melanoma*
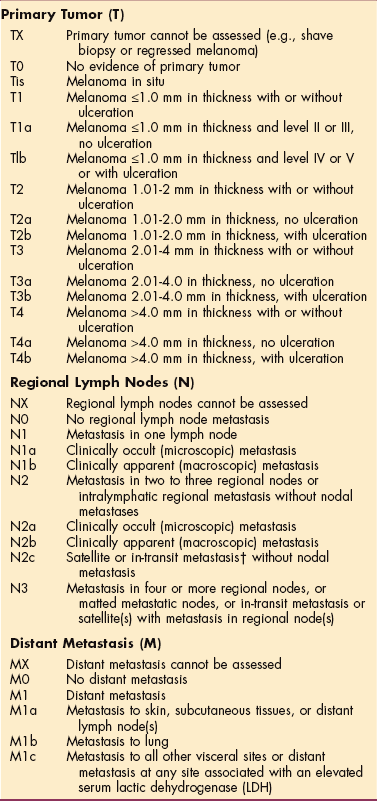
*Several systems exist for staging malignant melanoma, including the TNM (tumor, node, metastasis) system, developed by the American Joint Committee on Cancer, and Clark’s system, which classifies tumor progression according to skin layer penetration (see Fig. 10-16).
†In-transit metastasis involves skin or subcutaneous tissue more than 2 cm from the tumor but not beyond the regional lymph nodes.
Used with permission of the American Joint Committee on Cancer (AJCC), Chicago. AJCC andbook for staging of cancer, ed 6, New York, 2002, Springer-Verlag. Used with permission of the American Joint Committee on Cancer (AJCC), Chicago. AJCC handbook for staging of cancer, ed 6, New York, 2002, Springer-Verlag. Springer-Verlag
Diagnostic accuracy will continue to improve as digitalized images of lesions can be analyzed, enabling the physician to determine whether a biopsy is needed. Computer-aided microscopic examination of biopsy slides may lead to better diagnosis, and teledermatology will add additional assistance in melanoma diagnosis. This technology makes it possible to compress digital images of suspicious lesions and transmit them electronically anywhere in the world, making consultation easier.127
Scientists are continuing to seek complementary ways of predicting metastatic potential so that preventive therapies can be initiated earlier. Tests that can detect submicroscopic melanoma cells circulating in the blood vessels and lymphatics could prove invaluable, since melanoma generally metastasizes via these systems.
The recently developed reverse transcriptase polymerase chain reaction (RT-PCR) assay designed to detect genetic markers or indicators of potential metastatic melanoma in the blood has been seriously hampered by false-negative reports. A study in 2005 concluded that RT-PCR does not correlate with traditional indicators for prognosis of melanoma.121,156
Additional assays that make use of multiple melanoma markers are being investigated.36,52 Adhesion markers have proven valuable112 as well as microtubule-associated protein 2 (MAP2), a marker of neuronal differentiation that induces mitotic defects, inhibits growth of melanoma cells, and predicts metastatic potential of cutaneous melanoma.142
TREATMENT.
Neither cryosurgery with liquid nitrogen nor electrodesiccation is used to treat melanoma, although they are among the acceptable procedures for squamous cell and basal cell tumors. The treatment of choice for melanoma without evidence of distant metastatic spread is surgical excision. Surgery is combined with postoperative adjuvant radiation therapy and/or chemotherapy when there is evidence of regional spread. Surgery is not usually recommended for tumors that have metastasized to distant sites.100
Previously, surgical excision of the primary lesion site may have been accompanied by removal of regional lymph nodes (regional lymphadenectomy), but sentinel node biopsy (see Chapter 9) has been shown to be a reliable diagnostic tool for selecting individuals to be submitted to lymph node dissection, thereby reducing the extent of surgery for those who do not need this procedure.20,101
There is considerable debate about the use of sentinel node biopsy in staging melanoma at this time. Some studies report that this type of biopsy is highly reliable in experienced hands but a low-yield procedure in most thin melanomas,24,162 whereas others argue against its use except in clinical trials151 and claim that there is not enough evidence to support the current combined use of sentinel node biopsy and systemic interferon (IFN) for melanoma.109
In 2005 a study indicated that children with high-risk melanoma could be treated with sentinel lymph node biopsy and IFN-alfa-2b with tolerable toxicity.103 A more recent study of sentinel lymph node biopsy histology in melanomas less than or equal to 1.0 mm in depth suggests it is a significant predictor of outcome and should be considered for individuals with melanomas 0.75 to 1.0 mm in depth.120
Surgeons are now able to use aggressive surgical approaches on a more selective basis and therefore decrease treatment-related complications and disfigurement without compromising surgical goals. This change in treatment approach came as a result of the knowledge that the recurrence rate for people with melanoma clinically localized to the skin correlates directly with tumor thickness or depth of invasion, whereas the prognosis for people whose disease has spread to the regional lymph nodes depends primarily on the number of nodes that have tumors.129
Deep primary lesions may warrant adjuvant chemotherapy and biotherapy to eliminate or reduce the number of tumor cells, but there is no role at present for chemotherapy or radiation therapy as the initial treatment. Radiation therapy is used for metastatic disease to reduce tumor size and provide palliative relief from painful symptoms; it does not prolong survival time.
Ongoing research to develop immunomodulation therapy remains a large area of study. In addition to immunotherapy to stimulate the immune system, research to treat people with a vaccine made from their own cancer cells is under way. This antimelanoma immunization is currently undergoing multiple clinical trials and has shown evidence of clinical effectiveness with minimal side effects.16,99,152
Long-term effectiveness remains unknown. Other more investigational techniques include incorporating Fas ligands (a protein found to provide defense against the accumulation of mutations caused by sun exposure) into short-acting drugs or mixing them into sunscreens to boost people’s natural resistance to skin cancer.
PROGNOSIS.
Malignant melanoma is a more serious problem than other skin cancers because it can spread quickly and insidiously, becoming life-threatening at an earlier stage of development. However, it is essentially 100% curable if detected early.
The prognosis for all types of melanoma depends primarily on the tumor’s thickness and depth of invasion, not on the histologic type. The more superficial or thin the tumor, the better the prognosis. For example, melanoma lesions less than 0.76 mm deep have an excellent prognosis (5-year survival rate is 90%), whereas deeper lesions (more than 0.76 mm) carry the risk for metastasis (5-year survival rate is 65% with local metastasis; 30% to 35% when distant metastases are present). Metastases to the brain, lungs, bones, liver, and CNS are universally fatal, usually within 1 year.
Prognosis is better for a tumor on an extremity that is drained by one lymphatic network than for one on the head, neck, or trunk drained by several lymphatic networks. Tumors can recur more than 5 years after primary surgery, requiring close long-term medical follow-up. Local recurrence without metastases may not represent a poor prognosis if the recurrence is simply an outgrowth of residual undetected microscopic cells from the previously excised primary tumor.17,168 Education on the effects of UVB exposure can dramatically reduce the incidence and recurrence of skin cancer.
Kaposi’s Sarcoma
Kaposi’s sarcoma (KS) is a malignancy of vascular tissue that presents as a skin disorder. Until recently, this tumor was most commonly seen in older men of Mediterranean or Eastern European origin, especially men of Jewish or Italian ancestry (now referred to as classic KS).
The sudden emergence of this malignancy in the Western world is directly related to AIDS-associated immunodeficiency, and the incidence has risen dramatically along with the incidence of AIDS (epidemic KS). KS may also occur in kidney transplant recipients taking immunosuppressive drugs.
Etiologic Factors and Incidence
Research in the mid-1990s confirmed that KS is caused by a herpesvirus infection. The human herpesvirus 8 (HHV-8) or Kaposi’s sarcoma–associated herpesvirus (KSHV) is present in all AIDS-related KS and has been linked to all four forms of KS (classic, iatrogenic, endemic [African], HIV associated); however, only iatrogenic KS and HIV-associated KS have been shown to be linked to impairment of the host immune response. This universal detection of KSHV/HHV-8 suggests a central role for the virus in the development of KS and common etiologic factors for all KS types.69 Genetic or hereditary predisposition may be a factor in the classic form.
Epidemiologic surveys indicate that the seroprevalence for HHV-8 parallels the risk of developing KS—5% to 10% in the general population of the Western world but ranging up to 20% to 70% in homosexual HIV-infected clients. Among the people who develop AIDS, KS is seen almost exclusively among homosexual or bisexual men, with the probability of HHV-8 seropositivity directly proportional to the number of previous male sex partners. If a person contracts AIDS as a result of IV drug use or from a transfusion, the chance of developing KS is less than 2%.
Rates are lower (10%) among HIV-infected women, people with hemophilia, and injection drug users. Overall incidence has been reduced among adults with AIDS associated with the use of antiretroviral therapy to control HIV replication and limit the associated immunodeficiency.24,53
Pathogenesis
Although HHV-8 is detectable in saliva and semen, the exact mechanism of transmission is not known and the details of the pathogenesis remain unknown. KS is an angioproliferative tumor. It is suspected that endogenous substances produced by HIV-infected cells and/or a viral-induced tumorigenesis may promote angiogenesis and the growth of KS.1,97
Studies have demonstrated the role of vascular endothelial growth factor A (VEGF-A) and its receptors in the pathogenesis of KS.3 VEGF-A is needed in the pathogenesis of KSHV, due to its ability to mediate angiogenesis.2 In Kaposi’s sarcoma, VEGF was also increased in cells from lesions as a result of organ transplants and even more so in normal cells around the Kaposi’s sarcoma’s lesion.143
Clinical Manifestations
This neoplasm involves the skin and mucous membranes as well as other organs and can lead to tumor-associated edema and ulcerations. Classic KS occurs commonly on the lower extremities, and the affected areas are red, purple, or dark blue macules (Fig. 10-17) that slowly enlarge to become nodules or ulcers. Itching and pain in the lesions that impinge on nerves or organs may occur; and as the sarcoma progresses, causing lymphatic obstruction, the legs become edematous. The lesions may spread by metastasis through the upper body to the face and oral mucosa.
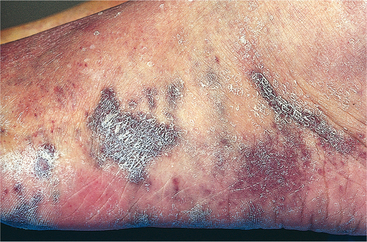
Figure 10-17 Classic Kaposi’s sarcoma is present as typical nodular lesions on this ankle and foot. (From Kumar V, Abbas AK, Fausto M: Robbins and Cotran pathologic basis of disease, ed 7, Philadelphia, 2005, Saunders.)
Unlike classic forms of the disease, AIDS-associated KS is a multicentric entity that appears on the upper body (including face, chest, and neck) but can occur on the legs. It frequently involves lymph nodes, lung, and the GI tract; it may be the first manifestation of AIDS (Fig. 10-18; see also Fig. 7-18).
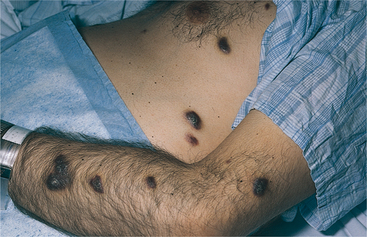
Figure 10-18 Epidemic Kaposi’s sarcoma in the plaque stage. Evolving lesions develop into raised papules or thickened plaques that are oval in shape and vary in color from red to brown. (From Swartz MH: Textbook of physical diagnosis, ed 5, Philadelphia, 2006, Saunders.)
Early lesions are faint pink and can easily be mistaken for bruises or nevi and be ignored. Systemic involvement may present with one or more signs and symptoms, including weight loss (10% of body weight), fever of unknown origin that exceeds 100° F (37.8° C) for more than 2 weeks, chills, night sweats, lethargy, anorexia, and diarrhea. Pulmonary involvement may be characterized by dyspnea, cough, chest pain, and hemoptysis (in order of prevalence).
MEDICAL MANAGEMENT
DIAGNOSIS, TREATMENT, AND PROGNOSIS.
Diagnosis is by skin biopsy using a highly sensitive and specific test for this neoplasm. A CT scan may be performed to detect and evaluate possible metastasis. Dermatologic manifestations of KS can be alarming, but it is visceral involvement associated with AIDS KS that is most lifethreatening.
However, new antiretroviral therapies, in particular the protease inhibitors, appear to be changing the clinical course of KS. It is now possible to see a complete resolution and control of KS with the use of these new agents. As researchers continue to unravel the pathogenesis of KS, new treatment modalities will target its pathogenic pathways.
Chemotherapy remains an integral part of treatment, and new agents are becoming available. Experimental therapies being evaluated in ongoing clinical trials include angiogenesis inhibitors, pregnancy hormone (human chorionic gonadotropin), photodynamic therapy, isotretinoin, antiviral medications ganciclovir and foscarnet, retinoic acid derivatives, and immune modulators, such as interleukin-12.48,98,164 See discussion of AIDS in Chapter 7.
SKIN DISORDERS ASSOCIATED WITH IMMUNE DYSFUNCTION
Definition and Incidence
Psoriasis is a chronic, inherited, recurrent inflammatory but noninfectious dermatosis characterized by well-defined erythematous plaques covered with a silvery scale (Fig. 10-19). There are several types of psoriasis, including plaque, guttate, erythrodermic, and pustular psoriasis.

Figure 10-19 Deforming arthritis of the hands in a person with psoriasis (psoriatic arthritis). (From Callen JP, Greer K, Paller A, Swinyer L: Color atlas of dermatology, ed 2, Philadelphia, 2000, Saunders.)
Psoriasis occurs equally in both genders and most commonly in young adults (mean age of onset is 27 years of age) but can occur at any point in a person’s life and, once present, becomes a chronic condition that may go in and out of remission. Although psoriasis can occur in infancy, it is uncommon in children under the age of 6 years. It is uncommon among blacks but affects 1% to 2% of the white population; more than 6 million Americans are affected, with more than 100,000 classified as severe cases.