The Respiratory System
OVERVIEW
Anatomically, the respiratory system can be divided into three main portions: the upper airway, the lower airway, and the terminal alveoli (Fig. 15-1). The upper airway consists of the nasal cavities, sinuses, pharynx, tonsils, and larynx. The lower airway consists of the conducting airways, including the trachea, bronchi, and bronchioles (Fig. 15-2). The alveoli, or air sacs, at the end of the conducting airways in the lower respiratory tract are the primary lobules, sometimes called the acini, of the lung.
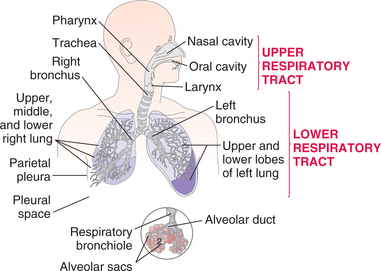
Figure 15-1 Structures of the upper and lower respiratory tracts. The upper respiratory tract consists of the nasal cavity, pharynx, and larynx; the lower respiratory tract includes the trachea, bronchi, and lungs. The circle shows the acinus, the terminal respiratory unit, which consists of the respiratory bronchioles, alveolar ducts, and alveolar sacs. This is the portion of the lungs where oxygen and carbon dioxide are exchanged.
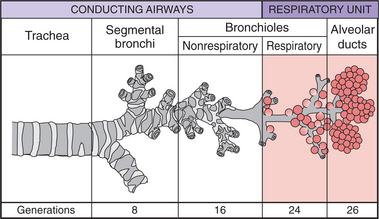
Figure 15-2 Structures of the lower airway. The first 16 generations of the airways branching in human lungs are purely conducting; transitional airways lead into the final respiratory zone consisting of alveoli where gas exchange takes place.
Physiologically, lung function is comprised of ventilation and respiration. Ventilation is the ability to move the air in and out of the lungs via a pressure gradient. Respiration is the gas exchange that supplies oxygen to the blood and body tissues and removes carbon dioxide. Pathology or impairment of the airways, lungs, chest wall, and diaphragm will affect ventilation. Pathology of the lungs and cardiovascular system, as well as peripheral tissues, will affect respiration.
Major Sequela of Pulmonary Disease or Injury
Hypoxemia is the most common condition caused by pulmonary disease or injury. Hypoxemia, deficient oxygenation of arterial blood, may lead to hypoxia, a broad term meaning diminished availability of oxygen to the body tissues. Prolonged hypoxia will cause tissue damage or death. Hypoxemia is caused by respiratory alterations (Table 15-1) or cardiovascular compromise, whereas hypoxia may occur anywhere in the body caused by alterations of other systems and may not be related to changes in the pulmonary system.
Table 15-1
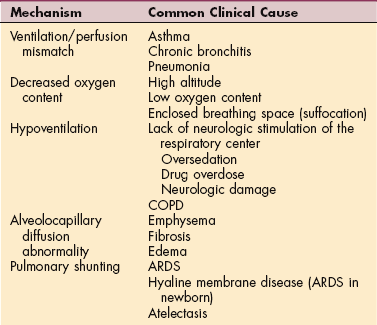
COPD, Chronic obstructive pulmonary disease; ARDS, acute respiratory distress syndrome.
Modified from McCance KL, Huether SE, eds: Pathophysiology: the biologic basis for disease in adults and children, ed 3, St Louis, 1998, Mosby-Year Book.
Signs and symptoms of hypoxemia vary, depending on the level of oxygenation in the blood (Table 15-2). Exercise testing may be performed to determine the degree of oxygen desaturation and/or hypoxemia that occurs on exertion. This testing requires analysis of arterial blood samples drawn with the subject at rest and at peak exercise. Continuous noninvasive measurement of arterial oxyhemoglobin saturation is usually determined by pulse oximetry.
Table 15-2
Signs and Symptoms of Hypoxemia
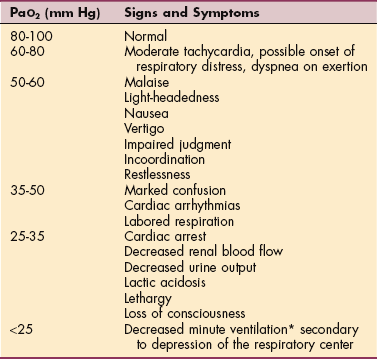
PaO2, Partial pressure of arterial oxygen.
*The total expired volume of air per minute.
Modified from Frownfelter DL, Dean E: Principles and practice of cardiopulmonary physical therapy, ed 4, St Louis, 2006, Mosby-Year Book.
Oxygen Transport Deficits in Systemic Disease
Although this chapter focuses on primary pulmonary impairment, pathologic conditions of every major organ system can have secondary effects on pulmonary function and on the oxygen transport pathway (which includes the cardiovascular system). Such effects are of considerable clinical significance given that they can be life-threatening and that therapy interventions usually put additional demands on the oxygen transport system. The resulting secondary effect may include a large range of pulmonary impairments such as altered ventilation, perfusion, and ventilation/perfusion matching; reduced lung volumes, capacities, and flow rates; atelectasis; reduced surfactant production and distribution; impaired mucociliary transport; secretion accumulation; pulmonary aspiration; impaired lymphatic drainage; pulmonary edema; impaired coughing; and respiratory muscle weakness or fatigue.111
When assessing signs and symptoms of pulmonary disease, the therapist must consider the possibility that these are secondary effects and should investigate the nature of the underlying etiologic factors. Making as specific a physical therapy diagnosis as possible enables the therapist to identify and implement the most effective interventions.
Signs and Symptoms of Pulmonary Disease
Pulmonary disease is often classified as acute or chronic, obstructive or restrictive, or infectious or noninfectious and is associated with many common signs and symptoms. The most common of these are cough and dyspnea. Other manifestations include chest pain, abnormal sputum, hemoptysis, cyanosis, digital clubbing, and altered breathing patterns (Box 15-1 and Table 15-3).
Table 15-3
Descriptions of Altered Breathing Patterns and Sounds
| Breathing Pattern or Sound | Description |
| Apneustic | Gasping inspiration followed by short expiration. |
| Biot’s respiration (ataxia) | An irregular pattern of deep and shallow breaths; fast, deep breaths interspersed with abrupt pauses in breathing. |
| Cheyne-Stokes respiration | Repeated cycle of deep breathing followed by shallow breaths or cessation of breathing. |
| Crackles/rales | Discontinuous, low-pitched sounds predominantly heard during inspiration that indicate secretions in the peripheral airways.140 |
| Hyperventilation | Abnormally prolonged and deep breathing. |
| Hypoventilation | Reduction in the amount of air entering the pulmonary alveoli, which causes an increase in the arterial CO2 level. |
| Kussmaul’s respiration | A distressing dyspnea characterized by increased respiratory rate (>20/min), increased depth of respiration, panting, and labored respiration typical of air hunger. |
| Lateral-costal breathing | Chest becomes flattened anteriorly with excessive flaring of the lower ribs (supine position); minimal to no upper chest expansion or accessory muscle involvement with outward flaring of the lower rib cage instead; the person breathes into the lateral plane of respiration (gravity eliminated) because the weakened diaphragm and intercostal muscles cannot effectively oppose the force of gravity in the anterior plane; used to focus expansion in areas of the chest wall that have decreased expansion (e.g., spinal cord injury with atelectasis or pneumonia, asymmetric chest expansion with scoliosis).* |
| Paradoxical breathing (sometimes referred to as reverse breathing) | All or part of the chest wall falls in during inspiration; may be abdominal expansion during exhalation; can lead to a flattened anterior chest wall or pectus excavatum. |
| Stridor | A shrill, harsh sound heard during inspiration in the presence of laryngeal obstruction. |
| Wheezing | High-pitched, continuous whistling sound, usually with expiration and related to bronchospasm or other constriction of the airways. |
Cough
As a physiologic response, cough occurs frequently in healthy people, but a persistent dry cough may be caused by a tumor, congestion, or hypersensitive airways (allergies). A productive cough with purulent sputum may indicate infection, whereas a productive cough with nonpurulent sputum is nonspecific and indicates airway irritation. Hemoptysis (coughing and spitting blood) indicates a pathologic condition—infection, inflammation, abscess, tumor, or infarction.
Dyspnea
Shortness of breath (SOB), or dyspnea, usually indicates hypoxemia but can be associated with emotional states, particularly fear and anxiety. Dyspnea is usually caused by diffuse and extensive rather than focal pulmonary disease, pulmonary embolism being the exception. Factors contributing to the sensation of dyspnea include increased work of breathing (WOB), respiratory muscle fatigue, increased systemic metabolic demands, and decreased respiratory reserve capacity. Dyspnea when the person is lying down is called orthopnea and is caused by redistribution of body water. Fluid shift leads to increased fluid in the lung, which interferes with gas exchange and leads to orthopnea. In supine and prone, the abdominal contents also exert pressure on the diaphragm, increasing the WOB and often limiting vital capacity.
Chest Pain
Pulmonary pain patterns are usually localized in the substernal or chest region over involved lung fields, including the anterior aspect of the chest, side, or back. However, pulmonary pain can radiate to the neck, upper trapezius, costal margins, thoracic area of the back, scapulae, or shoulder. Shoulder pain caused by pulmonary involvement may radiate along the medial aspect of the arm, mimicking other neuromuscular causes of neck or shoulder pain. Musculoskeletal causes of chest (wall) pain must be differentiated from pain of cardiac, pulmonary, epigastric, and breast origins.
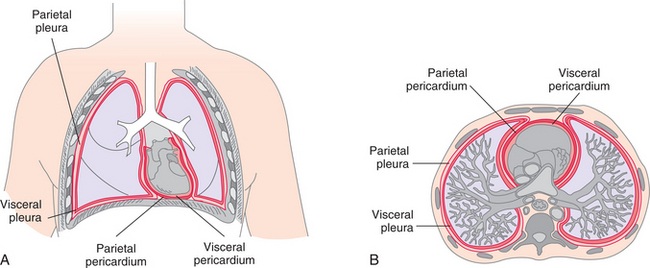
Extensive disease may occur in the lung without occurrence of pain until the process extends to the parietal pleura (Fig. 15-3). Pleural irritation then results in sharp, localized pain that is aggravated by any respiratory movement. Clients usually note that the pain is alleviated by autosplinting, that is, lying on the affected side, which diminishes the movement of that side of the chest.375,392
Cyanosis
The presence of cyanosis, a bluish color of the skin and mucous membranes, depends on the oxygen saturation of arterial blood and the total amount of circulating hemoglobin. It is further differentiated as central or peripheral. Central cyanosis is best observed as a bluish discoloration in the oral mucous membranes, lips, and conjunctivae (i.e., the warmer, more central areas) and is most often associated with cardiac right-to-left shunts and pulmonary disease. Peripheral cyanosis is associated with decreased perfusion to the extremities, nail beds, and nose (i.e., the cooler, exposed areas) and is commonly caused by cold external temperature, anxiety, heart failure, or shock.
Clinically detectable cyanosis depends not only on oxygen saturation but also on the total amount of circulating hemoglobin that is bound to oxygen. For example, a child with severe anemia may not be cyanotic because all available hemoglobin is fully saturated with oxygen. However, a child with polycythemia may demonstrate signs of cyanosis because the overproduction of red blood cells (RBCs) results in increased amounts of hemoglobin that are not fully saturated with oxygen. In some instances, however, such as in carbon monoxide poisoning, hemoglobin is bound with a substance other than oxygen. Cyanosis is not present since the hemoglobin is fully bound, but since the hemoglobin is not bound to oxygen, there is inadequate tissue oxygenation and potential tissue death.
Arterial saturation in central cyanosis is usually decreased, whereas arterial saturation may be normal in peripheral cyanosis. In the case of peripheral cyanosis, vasoconstriction with decreased blood supply and perfusion rather than unsaturated blood is the underlying cause of symptoms.
Clubbing
Thickening and widening of the terminal phalanges of the fingers and toes result in a painless clublike appearance recognized by the loss of the angle between the nail and the nail bed (Fig. 15-4). Conditions that chronically interfere with tissue perfusion and nutrition may cause clubbing, including cystic fibrosis (CF), chronic obstructive pulmonary disease (COPD), lung cancer, bronchiectasis, pulmonary fibrosis, congenital heart disease, and lung abscess. Although 75% to 85% of clubbing is due to pulmonary disease and resultant hypoxia (diminished availability of blood to the body tissues), clubbing does not always indicate lung disease. It is sometimes present in heart disease, peripheral vascular disease, and disorders of the liver and gastrointestinal tract.
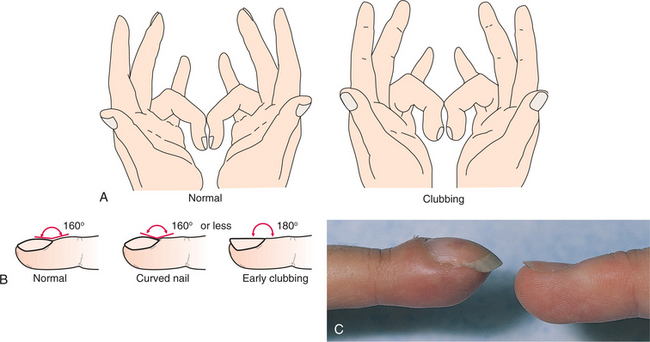
Figure 15-4 A, Assessment of clubbing by the Schamrath method. The client places the fingernails of opposite fingers together and holds them up to a light. If a diamond shape can be seen between the nails, there is no clubbing. B, The profile of the index finger is examined, and the angle of the nail base is noted; it should be about 160 degrees. The nail base is firm to palpation. Curved nails are a variation of normal with a convex profile and may look like clubbed nails, but the angle between the nail base and the nail is 160 degrees or less. In early clubbing, the angle straightens out to 180 degrees and the nail base feels spongy to palpation. C, Photograph of advanced clubbing of the finger (left) compared with normal finger (right). (A and B, from Swartz MH: Textbook of physical diagnosis: history and examination, Philadelphia, 1989, WB Saunders; C, from Swartz MH: Textbook of physical diagnosis: history and examination, ed 5, Philadelphia, 2006, WB Saunders
Altered Breathing Patterns
Changes in the rate, depth, regularity, and effort of breathing occur in response to any condition affecting the pulmonary system (see Table 15-3). Breathing patterns can vary, depending on the neuromuscular or neurologic disease or trauma (Box 15-2).
In a large cross-section of people and clinical disorders, hypoventilation is one of the most common changes in breathing patterns observed. Anything that can cause hypoxemia (e.g., fever, malnutrition, metabolic disturbance, loss of blood or blood flow, or availability of oxygen) reduces energy supplies and results in respiratory muscle dysfunction and altered breathing patterns. When hypoxemia is accompanied by skeletal muscle atonia associated with any neuromuscular cause, hypoventilation may further jeopardize the ventilatory pump.
Breathing pattern abnormalities seen with head trauma, brain abscess, diaphragmatic paralysis of chest wall muscles and thorax (e.g., generalized myopathy or neuropathy), heat stroke, spinal meningitis, and encephalitis can include apneustic breathing, ataxic breathing, or Cheyne-Stokes respiration (CSR). Apneustic breathing localizes damage to the midpons and is most commonly a result of a basilar artery infarct. Ataxic, or Biot’s, breathing is caused by disruption of the respiratory rhythm generator in the medulla. CSR may be evident in the well older adult, as well as in compromised clients. The most common cause of CSR is severe congestive heart failure, but it can also occur with renal failure, meningitis, drug overdose, and increased intracranial pressure. It may be a normal breathing pattern in infants and older persons during sleep.
Spinal cord injuries above C3 result in loss of phrenic nerve innervation, necessitating a tracheostomy and ventilatory support. Ventilatory support is used to refer to a variety of interventions, including mechanical ventilation via endotracheal intubation, noninvasive ventilatory support with continuous positive airway pressure (CPAP), positive end-expiratory pressure (PEEP), and bilevel positive airway pressure (BiPAP). See reference 140 for a complete description of the various means of ventilatory support.
Clients with generalized weakness, as in the Guillain-Barré syndrome, some myopathies or neuropathies, or incomplete spinal cord injuries, may show a tendency toward a specific breathing pattern called lateral-costal breathing (see Table 15-3).
15-1 SPECIAL IMPLICATIONS FOR THE THERAPIST
Signs and Symptoms of Pulmonary Disease
Many people with neuromusculoskeletal conditions, as well as people with primary or secondary pulmonary pathology, have the potential for oxygen trans- port deficits (and their sequelae discussed previuosly), impaired ventilation, and altered breathing patterns. For each type of condition, the therapist must identify those steps in the oxygen transport pathway that are affected so that intervention targets the specific underlying problem as much as possible.
Monitoring the cardiopulmonary status is important because many of the interventions provided by a therapist elicit an exercise stimulus and stress the oxygen transport system. Because impairment can result from diseases other than cardiopulmonary conditions, therapists in all settings need expertise in anticipating and detecting pulmonary dysfunction in the absence of primary pulmonary disease.111,140
Recognizing abnormal responses to interventions is important in identifying the client who needs additional intervention or who needs to be referred to another health care professional. For an excellent review of the oxygen transport deficits concept and more detailed implications by system, see reference 111.
Clinical observation of the client as he or she breathes is important (Box 15-3) and can alert the therapist to respiratory pathologic conditions. Assessment of the muscle groups (abdominal and intercostal muscles, accessory muscles, and the diaphragm) involved in normal ventilatory function may be required. Techniques to improve ventilation can enhance motor performance and improve a client’s functional level. The reader is referred to more specific texts for information about intervention techniques.140,198
High blood pressure in the pulmonary circulation (pulmonary hypertension) can cause pain during exercise that is often mistaken for cardiac pain (angina pectoris). For the therapist, musculoskeletal causes of chest pain must be differentiated from pain of cardiac, pulmonary, epigastric, and breast origins before treatment intervention begins.172 The therapist involved in performing airway clearance techniques and pulmonary rehabilitation must recognize precautions for and contraindications to therapy interventions in the medical client (Table 15-4).
Table 15-4
Considerations for and Contraindications to Airway Clearance Techniques in the Medical Client
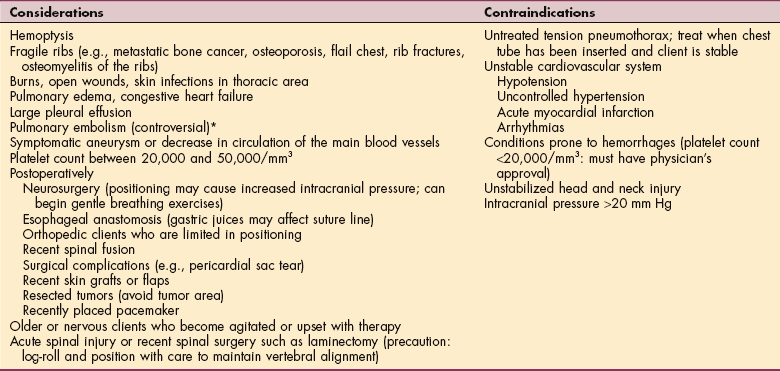
*A question remains whether there may be a recurrence (repeat emboli in the medically unstable client, i.e., one whose blood level of anticoagulants is not yet adequate to prevent a possible second embolus from dislodging) with movement in positioning the client for airway clearance techniques. However, allowing the client to lie still can contribute to the development of further venous stasis.
AGING AND THE PULMONARY SYSTEM
Aging affects not only the physiologic functions of the lungs (ventilation and respiration) but also the ability of the respiratory system to defend itself. More than any other organ, the lung is susceptible to infectious processes and environmental and occupational pollutants (see the section on Environmental and Occupational Diseases in this chapter). These factors, combined with the normal aging process, contribute to the decline of lung function.
Age-related alterations in the respiratory system are based on structural changes that lead to functional impairment of gas exchange.399,463 Chest wall compliance decreases with aging because of changes in joints of the ribs and spine, as well as alterations in collagen. This increased stiffness affects the volume of air moved and the WOB. Elastic recoil also is decreased by intermolecu- lar collagen crosslinks. Alveolar walls flatten, surface area is reduced, and the small airways more readily collapse and trap air, reducing the capacity for gas exchange.140,218 Thus diminished gas exchange is primarily due to increased physiologic dead space.
Many changes that occur with aging affect the lower airway, but in the upper airway the movement of the cilia slows and becomes less effective in sweeping away mucus and debris. This reduced ciliary action combined with the other changes noted predisposes the older client to increased respiratory infections.
Reduction in respiratory muscle strength and endurance and subsequent increase in WOB requiring greater muscle oxygen consumption at any workload are observed with increasing age.52,140 Respiratory muscle strength is measured by maximum inspiratory pressure and maximum expiratory pressure. These measurements have been correlated with spirometry, nutritional status, and grip strength. Loss of respiratory muscle strength can lead to dyspnea and ultimately to ventilatory pump failure.
Normal minute ventilation of older adults is comparable to that of younger people, although tidal volumes are smaller and rate is higher. There is a significant blunting of response to hypoxia and hypercapnia from both the respiratory and cardiovascular systems, particularly at rest. The hypercapnia response during exercise is greater in older adults, contributing to more dyspnea for a given workload even in the absence of oxygen desaturation or metabolic acidosis.
Most adults attain maximal lung function (as measured by forced expiratory volume [FEV]) during their early twenties, but with increasing age, especially after age 55 years, there is an overall decrease in the functional ability of the lungs to move air in and out. This decline peaks by age 75 years, falling to about 70% of our maximum. Aging reduces the reserve capacity of virtually all pulmonary functions regardless of lifestyle, although a sedentary lifestyle accelerates the decline in functional capacity.249
All of these changes contribute to the increased WOB, meaning that the older adult works harder for the same air exchange as the younger person. These changes are influenced by lifestyle and environmental factors, respiratory disease, and body size. The effects of age are not nearly as influential as the effects of smoking in causing a premature decline in lung function and in limiting the ability to exercise.
Pulmonary complications during anesthesia and the postoperative period are significantly increased in older adults with preexisting diseases. Loss of an effective cough reflex contributes to an increased susceptibility to pneumonia and postoperative atelectasis in the older population. Other contributing factors to the loss of an effective cough reflex include conditions more common in older age such as reduced consciousness, use of sedatives, impaired esophageal motility, dysphagia, and neurologic diseases.
INFECTIOUS AND INFLAMMATORY DISEASES
Overview and Etiologic Factors
Pneumonia is an inflammation affecting the parenchyma of the lungs and can be caused by (1) a bacterial, viral, fungal, or mycoplasmal infection (organisms that have both viral and bacterial characteristics); (2) inhalation of toxic or caustic chemicals, smoke, dusts, or gases; or (3) aspiration of food, fluids, or vomitus. It may be primary or secondary, and it often follows influenza. The common feature of all types of pneumonia is an inflammatory pulmonary response to the offending organism or agent. This response may involve one or both lungs at the level of the lobe (lobar pneumonia) or more distally at the bronchioles and alveoli (bronchopneumonia).
Routes of Infection
The major routes of infection are airborne pathogens, circulation, sinus or contiguous infection, and aspiration. Nosocomial infections have twice the mortality and morbidity of non–hospital-acquired infections.318
Incidence
Pneumonia is a commonly encountered disease with more than 4 million cases diagnosed each year. Combined cost of pneumonia and influenza to the U.S. economy was $37.5 billion in 2004.344 It is a leading cause of death in the United States, claiming the lives of approximately 65,000 Americans annually. Approximately 30% of pneumonias are bacterial and especially prevalent in the older adult. Viral pneumonia, accounting for nearly one-half of all cases, is not usually life-threatening except in the immunocompromised person. The remaining 20% of all cases are caused by mycoplasma.
Risk Factors
Infectious agents responsible for pneumonia are typically present in the upper respiratory tract and cause no harm unless resistance is lowered by some other factor. Many host conditions promote the growth of pathogenic organisms, but cigarette smoking (more than 20 cigarettes/day) is highly correlated with community-acquired pneumonia.10 Pneumonia is also a frequent complication of acute respiratory infections such as influenza and sinusitis.
Other risk factors include chronic bronchitis, poorly controlled diabetes mellitus, uremia, dehydration, malnutrition, and prior existing critical illnesses such as chronic renal failure, chronic lung disease, or acquired immunodeficiency syndrome (AIDS). In addition, the stress of hospitalization, confinement to an extended care facility or intensive care unit, surgery, tracheal intubation, treatment with antineoplastic chemotherapy or immunosuppressive drugs, and urinary incontinence promotes rapid colonization of pathogenic organisms.
Infants, older adults, people with profound disabilities or who are bedridden, and persons with altered consciousness (e.g., caused by alcoholic stupor, head injury, seizure disorder, drug overdose, or general anesthesia) are most vulnerable. Inactivity and immobility cause pooling of normal secretions in the airways that creates an environment promoting bacterial growth. People with severe periodontal disease, those who have difficulty swallowing, those who have an inability to take oral medications, or those whose cough reflexes are impaired by drugs, alcohol, or neuromuscular disease are at increased risk for the development of pneumonia as a result of aspiration.
Pathogenesis
Although a common disease, pneumonia is relatively rare in healthy people because of the effectiveness of the respiratory host defense system and the fact that healthy lungs are generally kept sterile below the first major bronchial divisions. In the compromised person, the normal release of biochemical mediators by alveolar macrophages as part of the inflammatory response does not eliminate invading pathogens. The multiplying microorganisms release damaging toxins stimulating full-scale inflammatory and immune responses with damaging side effects.
Endotoxins released by some microorganisms damage bronchial mucous and alveolocapillary membranes. Inflammation and edema cause the acini and terminal bronchioles to fill with infectious debris and exudate so that air cannot enter the alveoli and gas exhange is impaired, leading to ventilation/perfusion abnormalities and dyspnea. With the appearance of an inflammatory response, clinical illness usually occurs. Production of interleukin-1 (IL-1) and tumor necrosis factor (TNF) by alveolar macrophages can contribute to many of the systemic effects of pneumonia such as fever, chills, malaise, and myalgias.
Resolution of the infection with eventual healing occurs with successful containment of the pathogenic microorganisms. However, little is known about the actual processes that halt the acute inflammatory reaction in pneumonia and initiate recovery.
Aspiration Pneumonia.: The risk of aspiration pneumonia occurs when anatomic defense mechanisms are impaired such as occurs with seizures; a depressed central nervous system (CNS) inhibiting the cough reflex; recurrent gastroesophageal reflux; neuromuscular disorders, especially with suck-swallow dysfunction; anatomic abnormalities (laryngeal cleft or tracheoesophageal fistula); and debilitating illnesses. Chronic aspiration often causes recurrent bouts of acute febrile pneumonia. Although any region may be affected, the right side, especially the right upper lobe in the supine person, is commonly affected because of the anatomic configuration of the right main-stem bronchus.
Fungal Pneumonia.: Pneumonia caused by fungi may present with mild symptoms, though some people become very ill. The three most common types, histoplasmosis, coccidioidomycosis, and blastomycosis, are generally specific to a limited geographic area. Other fungal lung infections primarily affect people with compromised immune systems. Diagnosis is made by culturing sputum samples.
Viral Pneumonia.: Viral pneumonia is usually mild and self-limiting, often bilateral and panlobular but confined to the septa rather than the intraalveolar spaces as is more likely with bacterial pneumonia. Viral pneumonia can be a primary infection creating an ideal environment for a secondary bacterial infection, or it can be a complication of another viral illness such as measles or chickenpox. The virus destroys ciliated epithelial cells and invades goblet cells and bronchial mucous glands. Bronchial walls become edematous and infiltrated with leukocytes. The destroyed bronchial epithelium sloughs throughout the respiratory tract, preventing mucociliary clearance.
Bacterial Pneumonia.: Destruction of the respiratory epithelium by infection with the influenza virus may be one mechanism whereby influenza predisposes people to bacterial pneumonia. The lung parenchyma, especially the alveoli in the lower lobes, is the most common site of bacterial pneumonia. When bacteria reach the alveolar surfaces, most are rapidly ingested by phagocytes.
Once phagocytosis has occurred, intracellular lysis proceeds but at a slower rate for bacteria than for other particles. As the condition resolves, neutrophils degenerate and macrophages appear in the alveolar spaces, which ingest the fibrin threads, and the remaining bacteria in the respiratory bronchioles are then transported by lung lymphatics to regional lymph nodes. The infection is usually limited to one or two lobes.
Clinical Manifestations
Most cases of bacterial pneumonia are preceded by an upper respiratory infection (URI), frequently viral. Signs and symptoms of pneumonia include sudden and sharp pleuritic chest pain aggravated by chest movement and accompanied by a hacking, productive cough with rust-colored or green purulent sputum. Other symptoms include dyspnea, tachypnea accompanied by decreased chest excursion on the affected side, cyanosis, headache, fatigue, fever and chills, and generalized aches and myalgias that may extend to the thighs and calves. Older adults with bronchopneumonia have fewer symptoms than younger people, and 25% remain afebrile because of the changes in temperature regulation as part of the normal aging process. Associated changes in gas exchange (hypoxia and hypercapnia) may result in altered mental status (e.g., confusion) or loss of balance and may lead to falls.
Most cases of pneumonia are relatively mild and resolve within 1 to 2 weeks, although symptoms may linger for 1 or 2 more weeks (more typical of viral or mycoplasma pneumonia). If the infection develops slowly with a fever so low as to be unnoticeable, the person may have what is referred to as “walking pneumonia.” This form tends to last longer than any other form of pneumonia. Complications of pneumonia can include pleural effusion (fluid around the lung), empyema (pus in the pleural cavity), and more rarely, lung abscess.
MEDICAL MANAGEMENT
The clinical presentations of pneumonias caused by different pathogenic microorganisms overlap considerably, requiring microscopic examination of respiratory secretions in making a differential diagnosis. Gram stain, color, odor, and cultures are part of the sputum analysis. A blood culture may help identify the bacteria, but bacterial counts are only positive in approximately 10% of bacterial pneumonias; 90% of bacterial pneumonias do not show a positive bacterial count.
The U.S. Food and Drug Administration (FDA) has approved a simple, quick urine test (urinary antigen testing) for detecting Streptococcus pneumoniae that provides results in 15 minutes. Immediate test results allow specific treatment to begin right away, thus controlling antibiotic overuse and antibiotic resistance with cost-effective targeted antibiotics. Results of the urine test should be confirmed with a culture. Research continues to develop new diagnostic techniques (e.g., polymerase chain reaction testing) to determine the microbiologic etiology of pneumonia.
Other diagnostic procedures may include chest films showing infiltrates that may involve a single lobe (lobar pneumonia from staphylococci) or may be more diffuse as in the case of bronchopneumonia (usually streptococci). Physical examination, including percussion and auscultation of the chest, may reveal signs of lung consolidation such as dullness, inspiratory crackles, or bronchial breath sounds.
TREATMENT.
The primary treatment for bacterial and mycoplasmic forms of pneumonia is antibiotic therapy along with rest and fluids. Treatment with specific antibiotics is based on the history; whether the pneumonia was community-acquired, hospital-acquired, or extended care facility–acquired; and on the medical status and overall condition of the client (e.g., otherwise healthy or debilitated). Airway clearance techniques (formerly, chest physical therapy, pulmonary physical therapy, and pulmonary hygiene) may aid in clearing purulent sputum.
Fungal pneumonia is treated with antifungal drugs such as itraconazole or amphotericin B. Viral pneumonia is treated symptomatically unless secondary bacterial pneumonia develops. Hospitalization may be required for the immunocompromised client.
A vaccine is recommended for everyone age 65 years or older; for people with chronic disorders of the lungs, heart, liver, or kidneys; for individuals with poorly controlled diabetes mellitus; and for those with a compromised immune system or confined to a long-term care facility. Immunization can provide protection from pneumococcal disease for a period of 3 to 5 years in over 80% of vaccinated persons. A pneumococcal conjugate vaccine for routine use in infants and in high-risk children effective against invasive pneumococcal disease and to a lesser degree against otitis media and pneumonia has been licensed for use in the United States.314,386
The pneumonia vaccine has been successful in reducing penicillin-resistant S. pneumoniae by 81% in infants and 49% in the elderly between 1999 and 2004. Because pneumonia is a common complication of the flu, the U.S. Centers for Disease Control and Prevention (CDC) recommends annual flu vaccinations as well.
PROGNOSIS.
Community-acquired pneumonia remains a common and serious clinical problem despite the availability of potent antibiotics and aggressive supportive measures. Hospital-acquired pneumonia (HAP) has an even higher mortality rate. Pneumonia ranks seventh among the causes of death in the United States and currently accounts for almost 40% of hospital deaths; 90% of those fatalities occur in people over age 65 years, largely a result of coexisting medical problems that weaken the immune system.
Highly effective prevention and treatment methods can improve survival and reduce the likelihood of developing pneumonia, but one-half of older adults do not get vaccinations that could cut the death rate in one-half. The Healthy People 2010 Objective 1-9c is to reduce hospitalization for immunization-preventable pneumonia to 8 per 10,000 in persons aged 65 years or older.
Pneumocystis Carinii Pneumonia
Definition, Etiology, and Risk Factors
Pneumocystis carinii pneumonia (PCP) is a progressive often fatal pneumonia. The origin of the organism is unknown. It is possibly acquired from the environment; infected humans; or animals, fungi, or protozoa. Other people at risk for the development of PCP include anyone who is immunosuppressed for organ transplantation, by chemotherapy for lymphoma or leukemia, by steroid therapy, or by malnutrition.
Previously, the majority of people with AIDS developed PCP during the course of their illness, but this is much less common now with pharmacologic prophylaxis. PCP has been shown to be the first indicator of conversion from human immunodeficiency virus (HIV) infection to the designation of AIDS. In a retrospective 10-year analysis of people with PCP, 6 out of 18 patients were HIV positive.208
Pathogenesis and Clinical Manifestations
Infection begins with the attachment of the Pneumocystis trophozoite (the feeding stage of a sporozoan parasite) to the alveolar lining cell. The trophozoite feeds on the host cell, enlarges, and transforms into the cyst form that ruptures to release new trophozoites, repeating the cycle. If the process is uninterrupted by the immune system or antibiotic therapy, the affected alveoli progressively fill with organisms and proteinaceous fluid until consolidation disrupts gas exchange, slowly causing hypoxia and death.
The physiologic response to PCP includes fever, impaired gas exchange, and altered respiratory function. Symptoms of PCP develop slowly and present as fever and progressive dyspnea, accompanied by a nonproductive cough. Fatigue, tachypnea, weight loss, and other manifestations of underlying immunosuppressive disease may be present and worsened as a result of the increased metabolic demands.
MEDICAL MANAGEMENT
DIAGNOSIS, TREATMENT, AND PROGNOSIS.
Molecular techniques in the laboratory play an essential role in the microbiologic diagnosis of pneumonia in the immunocompromised person. Other diagnostic tools may include fiberoptic bronchoscopy to obtain respiratory specimens for testing and chest radiograph. Diagnosis is important because effective pharmacologic treatment is available. Thanks to a worldwide collaborative effort among health care providers, academia, governments, and industry, our knowledge about and treatment of infection caused by HIV have evolved from palliative care to the use of a chronic disease model where survival is measured by decades, not months or years.197
Although pulmonary disease remains a major problem for people with HIV, prophylaxis against opportunistic infection in people with HIV has cut morbidity and mortality rates by 80%.21 The increasing seroprevalence of HIV among women of reproductive age, the risks of vertical transmission of HIV, and the fact that PCP is the most common infection seen in people progressing to AIDS have led to recommendations for routine prenatal HIV infection counseling and testing.
Pulmonary Tuberculosis
Tuberculosis (TB), formerly known as consumption, is an infectious, inflammatory systemic disease that affects the lungs and may disseminate to involve lymph nodes and other organs. TB is caused by infection with Mycobacterium tuberculosis and is characterized by granulomas, caseous (resembling cheese) necrosis, and subsequent cavity formation. Latent infection is defined as harboring M. tuberculosis without evidence of active infection; active infection is based on the presence of clinical and laboratory findings.
Overview
TB may be primary or secondary. The first or primary infection with the tubercle bacillus is usually asymptomatic and almost always (99%) remains quiet after the development of a hypersensitivity to the microorganism. The primary infection usually involves the middle or lower lung area with lesions consisting of exudation in the lung parenchyma. These lesions quickly become caseous and spread to the bronchopulmonary lymph nodes, where they gain access to the bloodstream and predispose the person to the subsequent development of chronic pulmonary and extrapulmonary TB at a later time.
Secondary TB develops as a result of either endogenous or exogenous reinfection by the tubercle bacillus. This is the most common form of clinical TB. Reactivated TB usually causes abnormalities in the upper lobes of one or both lungs. In the United States, development of secondary TB is almost always the result of endogenous reinfection that occurs when the primary lesion becomes active as a result of debilitation or lowered resistance.
Incidence
Despite improved methods of detection and treatment, TB remains a global health problem with the highest rates in Southeast Asia, sub-Saharan Africa, and eastern Europe (new cases 200 to 400 per 100,000).82 Before the development of anti-TB drugs in the late 1940s, TB was the leading cause of death in the United States. Drug therapy, along with improvements in public health and general living standards, resulted in a marked decline in incidence. However, recent influxes of immigrants from developing third world nations, rising homeless populations, prolonged lifespans, and the emergence of HIV led to an increase in reported cases in the mid1980s, reversing a 40-year period of decline.
Overall, between 1985 and 1992 there was a 20% increase in new TB cases in the United States. Now, after years of rising TB infection rates, the United States has started to see a decrease in the annual number of cases (current incidence is 4.8 cases per 100,000 U.S-born individuals, which is a 3.8% decline, and the incidence among foreign-born persons has not risen.93,221 Cases of multidrug-resistant TB have continued to rise annually, and there remains a huge reservoir of individuals who are infected.
Multidrug-resistant TB has emerged as a major infectious disease problem throughout the world. The infected individual begins taking the prescribed medication, feels better, and discontinues taking the drugs that are normally required to be taken 6 to 9 months. The disease flares up months later and is now resistant to the medications, and the infected person passes it along as a new drug-resistant strain characterized by mutations in existing genes.139
The AIDS pandemic, the increased incidence of TB in populations without easy access to anti-TB medications (e.g., homeless people and economically disadvantaged people), the deterioration of the public health infrastructure, interruptions in the drug supply, and inadequate training of health care providers in the epidemiology of TB are some factors contributing to the increased incidence of multidrug-resistant TB.
Risk Factors
Although TB can affect anyone, certain segments of the population have an increased risk of contracting the disease, particularly those with HIV infection and people age 65 years and older. The latter constitute nearly one-half of the newly diagnosed cases of TB in the United States and most cases of reactivation of dormant mycobacteria.
Other groups at risk include (1) economically disadvantaged or homeless people living in overcrowded conditions, frequently ethnic groups such as Hispanics, Native Americans, and Asian/Pacific Islanders; (2) immigrants from Southeast Asia, Africa (high HIV incidence), Eastern Europe, Mexico, and Latin America; (3) clients dependent on injection drugs, alcohol, or other drugs associated with malnutrition, debilitation, and poor health; (4) infants and children under the age of 5 years; (5) current or past prison inmates; (6) people with diabetes mellitus; (7) people with end-stage renal disease; and (8) others who are immunocompromised (not only those who are HIV infected but also those who are malnourished, organ transplant recipients, anyone receiving cancer chemotherapy or prolonged corticosteroid therapy).
The Institute of Medicine (IOM) estimates that more than one-half of all TB cases in the United States are attributable to foreign-born residents. The IOM has published a report calling for TB screening of all U.S. immigrants to prevent a predicted resurgence of the disease in the United States.212
Limited access to health care because of socioeconomic status or illegal alien status and sociocultural differences contribute to delays in seeking care and influence adherence to treatment, contributing to the rise in TB among ethnic groups, especially along the U.S.-Mexican border.304
Risk associated with processing contaminated medical waste has been reported,227 and the first documented case of cadaver-to-embalmer (mortician) TB has occurred, possibly by exposure to infectious aerosols generated during the aspiration of blood and other body fluids from the cadaver.400
Staff members of laboratories and necropsy rooms are estimated to be between 100 and 200 times more likely than the general public to develop TB by the inhalation of the bacilli in aerosols or dried material, by injuries (e.g., cuts and accidental inoculations with infected instruments), and by contact with infected materials and surfaces. Necropsies on individuals who had undiagnosed TB while alive present a potential hazard to pathologists, technicians, and medical students involved in postmortem examinations.92
Environmental factors that enhance transmission include contact between susceptible persons and an infectious person in relatively small, enclosed spaces (e.g., evidence of limited transmission during extended airline, train, or bus travel has been documented)239; inadequate ventilation that results in insufficient dilution or removal of infectious droplet nuclei (e.g., older buildings such as hospitals, prisons, government buildings, universities); and recirculation of air containing infectious droplet nuclei. Adequate ventilation is the most important measure to reduce the infectiousness of the environment. Mycobacteria are susceptible to ultraviolet irradiation (i.e., sunshine), so outdoor transmission of infection rarely occurs.
Etiologic Factors
The causative agent is the tubercle bacillus (Fig. 15-5), commonly transmitted in the United States by inhalation of infected airborne particles, known as droplet nuclei, which are produced when the infected persons sneeze, laugh, speak, sing, or cough.
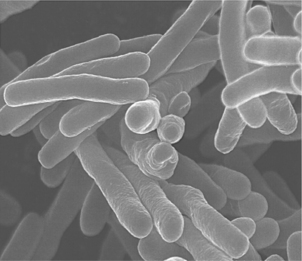
Figure 15-5 Tuberculosis (TB) bacteria. (Courtesy National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD, 2001.)
Casual contact or brief exposure to a few bacilli will not result in transmission of sufficient bacilli to infect a person. Rather, prolonged exposure in an enclosed space is required for transmission. Genetic factors determining susceptibility and resistance to the infection are suspected but have not been proven. In some other parts of the world, bovine TB carried by unpasteurized milk and other dairy products from tuberculous cattle is more prevalent.
The tubercle bacillus is capable of surviving for months in sputum that is not exposed to sunlight. Within the body it becomes encapsulated and can lie dormant for decades and then become reactivated years after an initial infection. This secondary TB infection (endogenous reinfection) can occur at any time the person’s resistance is lowered (e.g., alcoholism, immunosuppression, silicosis, advancing age, or cancer).
The older people of today were children when transmission of tubercle bacilli occurred more often. Now, reactivation of the disease is developing in their later years because an increasing portion of older adults who were previously not infected are acquiring new infections in extended care facilities.
Pathogenesis
Once a susceptible person inhales droplet nuclei containing M. tuberculosis and bacilli become established in the alveoli of the lungs, a proliferation of epithelial cells surrounds and encapsulates the multiplying bacilli in an attempt to wall off the invading organisms, thus forming a typical tubercle.
Two to ten weeks after initial human infection with the bacilli, acquired cell-mediated immunity usually limits further multiplication and spread of the TB bacilli. Although the TB bacilli are walled off inside a tubercle, the bacilli are not necessarily destroyed; they can remain alive but dormant inside the structure.
No one yet knows how the TB bacterium does its damage. M. tuberculosis has no known endotoxins or exotoxins so there is no immediate host response to the infection. The organisms grow for 2 to 12 weeks until they reach a number sufficient to elicit a cellular immune response that can be detected by a reaction to the tuberculin skin test.
The organisms tend to be localized or focused at sites of infection. In persons with intact cell-mediated immunity, collections of activated T cells and macrophages form granulomas that limit multiplication and spread of the organism, rendering the infection inactive, or latent. The tubercles stay intact as long as the immune system is maintained.
For the majority of individuals with an intact immune system, latent infection is clinically and radiographically undetected; a positive tuberculin (protein purified derivative [PPD]) skin test result is the only indication that infection has taken place. Individuals with latent TB infection but not active disease are not infectious and cannot transmit the organism. When residual lesions are visible on chest radiograph these sites remain potential lesions for reactivation.
If, however, the infection is not controlled by the immune defenses, the person develops symptoms of progressive primary TB. The granulomas become necrotic in the center and eventually produce fibrosis and calcification of the tissues.
Tubercle bacilli can spread to other parts of the body by way of the lymphatics to the hilar lymph nodes and then through the bloodstream to more distant sites, producing a condition called miliary (evenly distributed small nodules) TB, most common in people 50 years or older and in very young children with unstable or underdeveloped immune systems.
Erosion of blood vessels by the primary lesion can cause a large number of bacilli to enter the circulatory system, where they are carried to all areas of the body and may lodge in any organ, especially the lymph system, spine and weight-bearing joints, urogenital system, and meninges. Untreated, these tiny lesions spread and produce large areas of infection (e.g., TB pneumonia, tubercular meningitis). The same pharmacologic treatment is used for extrapulmonary and pulmonary TB, though the duration may be extended for some neurologic or skeletal infections.166
Researchers have identified a segment of deoxyribonucleic acid (DNA) that allows the TB organism to invade macrophages, where they lie dormant for years before leaving the macrophage cells to invade the lungs or other parts of the body. Finding this genetic fragment may provide information needed to block the microorganisms from entering human cells. The DNA fingerprint identified probably represents only one of several mechanisms that permit the TB transmission and invasion.193 Using DNA, scientists are developing faster and more accurate diagnostic tests for TB. Earlier detection improves treatment effectiveness.225
Clinical Manifestations
Most symptoms associated with TB do not appear in the early, most curable stage of the disease, although a skin test administered would be positive. Often symptoms are delayed until 1 year or more after initial exposure to the bacilli. Symptoms suggestive of TB include productive cough of more than 3 weeks’ duration, especially when accompanied by other symptoms such as weight loss, fever, night sweats, fatigue, malaise, and anorexia. Rales may be heard in the area of lung involvement, as well as bronchial breath sounds, if there is lung consolidation.
Complications associated with TB can include bronchopleural fistulae, esophagopleural fistulae, pleurisy with effusion, tuberculous pneumonia or laryngitis, and sudden lung atelectasis, indicating that a deep tuberculous cavity in the lung has perforated or created an opening into the pleural cavity, allowing air and infected material to flow to it (Fig. 15-6).
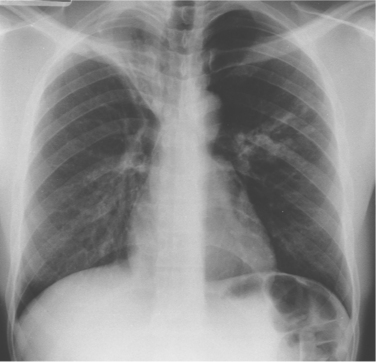
Figure 15-6 Segmental consolidation in tuberculous bronchopneumonia. The right upper lobe is grossly collapsed, scarred, and bronchiectatic. It had remained stable for many years until segmental nodular and linear consolidation appeared in the left mid zone, signaling reactivation. The segmental lesion was thought to be secondary to aspiration of bacteria from the right upper lobe. (From Grainger RG, Allison D: Grainger and Allison’s diagnostic radiology: a textbook of medical imaging, ed 4, Philadelphia, 2001, Churchill Livingstone. Used with permission.)
Extrapulmonary involvement (e.g., abdominal, pericardial, genitourinary, lymph node, central nervous system, or skeletal TB) increases in frequency in the presence of declining immunocompetency. Extrapulmonary TB occurs alone (i.e., without pulmonary involvement) in one-third of HIV-infected persons and in another one-third of HIV-infected persons with pulmonary involvement.12
Tuberculous involvement of the brain and spinal cord (extrapulmonary TB) is a common neurologic disorder in developing countries and has recently shown resurgence when associated with HIV. In tuberculous meningitis the process is located primarily at the base of the brain, and symptoms include those related to cranial nerve involvement, as well as headache, decreased level of consciousness, and neck stiffness. Tuberculous meningitis is associated with high morbidity and mortality. Tuberculous spondylitis (Pott’s disease), a rare complication of extrapulmonary TB, is discussed in Chapter 25.
MEDICAL MANAGEMENT
Preventing the transmission of TB is essential and can be done by using such simple measures as covering the mouth and nose with a tissue when coughing and sneezing, reducing the number of organisms excreted into the air. However, preventive and therapeutic interventions must address not only the bacillus but also the financial, nutritional, and employment status of those people at risk.
Adequate room ventilation and preventing overcrowding such as in homeless shelters and prisons are well-known preventive measures, but preventing this infection in many high-risk groups is complicated. For example, should control efforts among the poor emphasize the amelioration of social problems or merely the ingestion of appropriate dose and duration of antibiotic therapy?
Involuntary isolation is no longer acceptable, and directly observed therapy (i.e., the client receives the antibiotics under the supervision of an outreach worker) may be a violation of civil rights. How are individuals’ civil liberties and the public health best balanced? How should health professionals address the problem of the noncompliant individual? The complex issues surrounding TB in the United States remain an unresolved challenge at this time.*
The term preventive drug therapy has been changed to treatment of latent TB infection (LTBI). The failure of vaccination with bacille Calmette-Guérin (BCG), a freeze-dried preparation of a live, attenuated strain of M. bovis, to control the global TB epidemic and the spread of multidrug resistance has resulted in renewed research efforts to develop a better vaccine. New vaccines that could boost BCG could be soon available, and live vaccines are currently being tested.279
DIAGNOSIS.
Recent advances in DNA molecular techniques for the diagnosis of TB have improved the accuracy and speed of laboratory diagnosis in symptomatic people. Fortunately, some of these improved tools are appropriate for low-income settings and may help integrate new diagnostic tools into national TB control programs.331,224
Diagnostic measures for identifying TB currently include history, physical examination, tuberculin skin test, chest radiograph, and microscopic examination and culture of sputum. The tuberculin skin test determines whether the body’s immune response has been activated by the presence of the bacillus. The skin and other tissue become sensitized to the protein part of the tubercle bacilli. A positive reaction causes a swelling or hardness at the site of infection and develops 3 to 10 weeks after the initial infection. A positive skin test reaction indicates the presence of a TB infection but does not show whether the infection is dormant or is causing a clinical illness. Other diagnostic methods, such as sputum analysis, bronchoscopy, or biopsy, may be indicated in some cases.
Because of the dormant properties of the tubercle bacillus, anyone infected with TB should have periodic TB testing performed. In the case of someone with known TB, the skin test will always be positive, requiring periodic screening with chest x-ray studies. Previously an annual examination was recommended, but currently, screening is based on symptomatic presentation (if asymptomatic, testing is not required) and job exposure (i.e., those health care workers treating persons with active TB or AIDS or HIV infection are at increased risk of exposure).
The tuberculin skin test is the most common method currently used that demonstrates infection with M. tuberculosis in the absence of active TB, although newer methods, including a blood test, QuantiFeron-TB Gold test (QFT-G), have been approved by the FDA. The test detects the release of interferon-γ (IFN-γ) in fresh heparinized whole blood from sensitized persons when it is incubated with two synthetic peptides that simulate two proteins present in M. tuberculosis.62,225,331
The new test has higher sensitivity and specificity (fewer false negative and false positive tests) than the old TB PPD skin test and the former QFT test, which used PPD as the incubating agent. The peptide-sensitizing agents used in the test are absent from all BCG vaccine strains and most commonly encountered non-TB mycobacteria. The client only needs one appointment for the test. Nucleic acid amplification techniques are under development.225,331
TREATMENT.
The American Thoracic Society and the CDC13 have published guidelines for the treatment of TB infection. These guidelines should contribute to improved TB control worldwide and to TB elimination in the United States. Once diagnosed, all cases of active disease are treated, and certain cases of inactive disease are treated prophylactically, although it is unclear that preventive treatment is helpful in people with latent TB.138 Treatment may be initiated with only a positive skin test even if chest film and sputum analyses show no evidence of the disease. In this way, the disease is less likely to reactivate later in life when the immune system is more likely to be compromised.
Pharmacologic treatment through medication is the primary treatment of choice and renders the infection noncontagious and nonsymptomatic. These agents work by inhibiting cell wall biosynthesis, but the intracellular response that occurs is complex and poorly understood at this time.
Drug treatments now include combinations of all primary anti-TB medications (e.g., rifampin; isoniazid; pyrazinamide [Rifater]; and ethambutol) taken in one dose to replace the traditional treatment requiring multiple drugs daily. Treatment is problematic with homeless people and people who abuse alcohol and use injection drugs because this population is often noncompliant with the recommended 6-to 9-month treatment regimen. Children are usually treated with isoniazid and rifampin for 6 months. Multidrug-resistant TB has further complicated treatment. Treatment of resistant mycobacteria or the complications of TB frequently requires pneumonectomy.
Chemotherapy using a variety of chemical agents may be used, and often two or more drugs are used simultaneously to prevent the emergence of drug-resistant mutants. Immune amplifiers, such as IFN-γ, IL-2, and IL-12, are being tested as possible treatment alternatives. Treatment regimens do not differ for pulmonary and extrapulmonary TB.
PROGNOSIS.
Pulmonary TB is a major cause of morbidity and mortality worldwide, resulting in the greatest number of deaths from any one single infectious agent. This trend is due in part to increasing numbers of individuals infected with both HIV and TB. Untreated, TB is 50% to 80% fatal, and the median time period to death is 2½ years. HIV-related death from TB represents 12% of all adult AIDS-related deaths.93 Noncompletion of treatment (especially among inner city residents and homeless people) is the primary factor in multidrug-resistant TB. Mortality from multidrug-resistant TB is high in both persons infected with HIV and persons free of HIV.
Lung Abscess
Described as a localized accumulation of purulent exudate within the lung, an abscess usually develops as a complication of pneumonia, especially aspiration and staphylococcal pneumonia. This can occur when bacteria are aspirated from the oropharynx along with foreign material or vomitus, or it can occur from septic embolus from a heart valve. Septic pulmonary emboli from staphylococcal endocarditis of the tricuspid or pulmonary valves are most often a complication of the use of illicit injection drugs. An abscess may also form when a neoplasm becomes necrotic and contains purulent material that does not drain from the area because of partial or complete obstruction.
Risk Factors
Aspiration associated with alcoholism is the single most common condition predisposing to lung abscess. Other predisposed persons include those with altered levels of consciousness because of drug or alcohol use as mentioned, seizures, general anesthesia, lung cancer, or CNS disease; impaired gag reflex as a result of esophageal disease or neurologic disorders; poor dentition and periodontal care; and tracheal or nasogastric tubes, which disrupt the mechanical defenses of the airways.
Pathogenesis and Clinical Manifestations
As with all abscesses, a lung abscess is a natural defense mechanism in which the body attempts to localize an infection and wall off the microorganisms so these cannot spread throughout the body. As the microorganisms destroy the local parenchymal tissue (including alveoli, airways, and blood vessels), an inflammatory process causes alveoli to fill with fluid, pus, and microorganisms (consolidation). Death and decay of consolidated tissue may progress proximally until the abscess drains into the bronchus, spreading the infection to other parts of the lung and forming cavities (cavitation).
Clinical signs and symptoms of abscess formation almost always include cough productive of foul-smelling sputum and persistent fever. Other characteristic features include chills, dyspnea, pleuritic chest pain, cyanosis, and clubbing of fingernails, which can develop over a short period of time. Cavitation causes severe cough with copious amounts of purulent sputum and sometimes hemoptysis.
MEDICAL MANAGEMENT
The radiographic appearance of a thick-walled solitary cavity surrounded by consolidation suggests lung abscess but must be differentiated from other possible lesions. Cavitary lesions in the apex of the upper lobes are frequently caused by TB rather than bacterial abscess. Sputum analysis and culture, bronchoscopy, or ultrasound-guided transthoracic needle biopsy may be diagnostic; the latter diagnostic procedure also permits successful drainage of pulmonary abscesses.
TREATMENT AND PROGNOSIS.
Treatment includes specific antibiotics and good nutrition. Airway clearance techniques may be helpful if the abscess communicates with the main-stem bronchi; percussion helps promote drainage of associated secretions. Other measures are similar to the treatment of pneumonia. Bronchoscopy may be used to drain the abscess. Percutaneous drainage has also been deemed to be effective and safe for refractory lung abcess.437
Prognosis is good if antibiotics can treat the underlying cause, leaving only a residual lung scar. However, mortality remains in the range of 5% to 10% and is influenced by the severity of the primary disease that initially caused consolidation, the client’s general state of health, and the promptness of treatment.316b
Pneumonitis
Pneumonitis, an acute inflammation of lung tissue usually caused by infections, is discussed in this chapter (see section in this chapter on Environmental and Occupational Diseases) under its most common presentation as hypersensitivity pneumonitis. Other causes of pneumonitis include lupus pneumonitis associated with systemic lupus erythematosus (SLE), aspiration pneumonitis associated with inspiration of acidic gastric fluid, obstructive pneumonitis associated with lung cancer, and interstitial pneumonitis associated with AIDS. Consolidation with impaired gas exchange may occur in the involved lung tissue, but with successful inactivation of the infecting agent, resolution occurs with restoration of normal lung structure.
Acute Bronchitis
Acute bronchitis is an inflammation of the trachea and bronchi (tracheobronchial tree) that is of short duration (1 to 3 weeks) and self-limiting with few pulmonary signs. It may result from chemical irritation, such as smoke, fumes, or gas, or it may occur with viral infections such as influenza, measles, chickenpox, or whooping cough. These predisposing conditions may become apparent during the therapist’s interview with the client.
Symptoms of acute bronchitis include the early symptoms of an URI or a common cold, which progress to fever; a dry, irritating cough caused by transient hyperresponsiveness; sore throat; possible laryngitis; and chest pain from the effort of coughing. Later, the cough becomes more productive of purulent sputum, followed by wheezing. There may be constitutional symptoms, including moderate fever with accompanying chills, back pain, muscle pain and soreness, and headache.
Clients with viral bronchitis present with a nonproductive cough that frequently occurs in paroxysms and is aggravated by cold, dry, or dusty air. Bacterial bronchitis (common in clients with COPD) causes retrosternal (behind the sternum) pain that is aggravated by coughing.
Acute bronchitis should be differentiated from chronic bronchitis, pneumonia, whooping cough, rhinosinus conditions, and gastrointestinal reflux disease before treatment begins.57 Treatment is conservative and symptomatic with cough suppressants, rest, humidity, and nutrition and hydration.
Seasonal vaccination of people with recurrent bouts of bronchitis reduces the number and severity of exacerbations over the winter months.137 Bronchodilators are not indicated and the use of antibiotics for acute bronchitis is not recommended.57,442
Prognosis is usually good with treatment, and although acute bronchitis is usually mild, it can become complicated in people with chronic lung or heart disease and in older adults because they are more susceptible to secondary infections. Pneumonia is a critical complication.
OBSTRUCTIVE DISEASES
Chronic Obstructive Pulmonary Disease
Definition
COPD, also called chronic obstructive lung disease, refers to chronic airflow limitation that is not fully reversible. Chronic bronchitis, obstructive bronchiolitis,411 and emphysema are three forms of pathology that manifest as COPD. Chronic, unremitting asthma may be indistinguishable from COPD.79 Although these diseases share a common obstructive component and can occur independently, they most commonly coexist, requiring differing treatment and having different prognoses. COPD has also been divided into septic (bronchiectasis) and nonseptic (emphysema) categories to help guide treatment.118
Incidence and Risk Factors
COPD is second only to heart disease as a cause of disability in adults under 65 years of age. It is the fourth leading cause of death in the United States, predicted to be the third leading cause of death by 2020. Nearly 12 million people in the United States were diagnosed with COPD in 2000, but the prevalence is much higher (nearly 24 million adults have documented lung impairment). There were approximately 119,000 deaths from COPD in 2000. The estimated cost of COPD was $32.1 billion in 2002.
COPD is almost always caused by exposure to environmental irritants, especially smoking, which is the most common cause of COPD; this condition rarely occurs in nonsmokers. As with all chronic diseases, the prevalence of COPD is strongly associated with age and usually presents at age 55 to 60 years. More men are affected than women, but the incidence in women is increasing with the concomitant increase in smoking by women. Because smoking is the major cause of both emphysema and chronic bronchitis, these two conditions often occur together.
Morbidity and mortality rates for COPD increase with the effects of repeated or chronic exposure to irritating gases, dusts, or allergens; chronic irritation; and pollution in urban environments. Other contributing factors include chronic respiratory infections (e.g., sinusitis), periodontal disease,374 the aging process, heredity, and genetic predisposition.
Pathogenesis and Clinical Manifestations
The pathogenesis and clinical manifestations of each component of COPD are discussed separately in their respective sections. A broad overview of COPD is shown in Fig. 15-7. The person with COPD often develops a characteristic look with shoulders raised and muscles tensed from SOB and the increased WOB (Fig. 15-8).
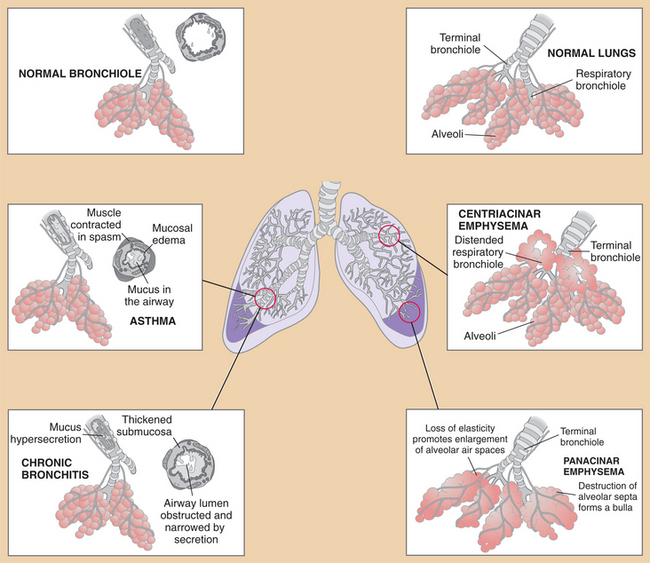

Figure 15-8 Characteristic look of chronic obstructive pulmonary disease (COPD) with shoulders raised and muscles tensed from shortness of breath (SOB) and the increased work of breathing (WOB). This gentleman had a 30-year history of smoking 1.5 packs/day combined with asthma eventually leading to stage IV emphysema and COPD. The effects of asthma and emphysema weakened the heart, resulting in congestive heart failure. Symptoms of SOB, productive cough, fatigue, dizziness, and muscular pain (caused by lack of oxygen) result in disability and reduced quality of life. Use of portable oxygen is required at all times. (Courtesy William T. Cannon, Missoula, MT. Used with permission.)
MEDICAL MANAGEMENT
At least two sets of guidelines for diagnosis and management of COPD are available.165 One set of guidelines was developed by the Global Initiative for Chronic Obstructive Lung Disease (GOLD), a joint project of the National Heart, Lung, and Blood Institute and the World Health Organization. Guidelines were also developed jointly by the American Thoracic Society and European Respiratory Society. These groups have set standards and made recommendations for management and future research of COPD.
DIAGNOSIS.
Physical examination and air-flow limitation on pulmonary function testing (see Table 40-22) are assessment tools in determining the presence and extent of COPD. A simple and inexpensive portable spirometer permits such testing in the outpatient setting but may also be conducted in a respiratory laboratory with a computerized spirometer; the results should not be used interchangeably.
Spirometry is the most basic and frequently performed test of pulmonary (lung) function. The spirometer mea- sures how much air the lungs can hold and how well the respiratory system is able to move air into and out of the lungs. Because spirometry is based on a maximal forced exhalation, the accuracy of its results are highly dependent on the person’s understanding, cooperation, and best efforts. Spirometry differs from peak flow readings in that spirometry records the entire forced breathing capacity against time, and peak flow records the largest breathing flow that can be sustained for 10 ms. Both are often used to assess results in the management of asthma.
The spirometer measures the expired air-flow rate and volume in a specific time period. More than a 10% difference measured before and after activity or before and after medication (a bronchodilator) is considered diagnostic for a reactive airway disease component of COPD. Predicted values based on age, height, gender, and body weight are compared to actual values to determine the numeric (%) comparison (Table 15-5).77
Table 15-5
Spirometric Classification of Chronic Obstructive Pulmonary Disease (COPD)*
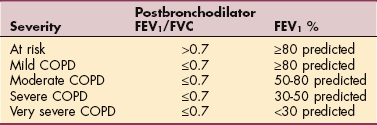
FEV1, Forced expiratory volume in 1 second (volume of air expelled in the first second of forced expiration); FVC, forced vital capacity (the maximum volume of air that can be forcibly and rapidly exhaled).
*The diagnosis of COPD should be considered in anyone who has chronic cough, sputum production, dyspnea, or history of risk factors for COPD. Spirometry is required in making the diagnosis: airflow limitation that is not reversible is indicated by a postbronchodilator FEV1/FVC ratio of ≤0.7
Data from Celli BR, MacNee W: STS/ERS Task Force Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper, Eur Respir J 23(6):932-946, 2004.
Spirometry results are expressed as a percentage and are considered abnormal if they are less than 80% of the normal predicted value. An abnormal result usually indicates the presence of some degree of obstructive lung disease. FEV in 1 second (FEV1) values (percentage of predicted) can be used to classify the obstruction that may occur as mild to very severe.
History, clinical examination, x-ray studies, and laboratory findings usually enable the physician to distinguish COPD from other obstructive pulmonary disorders, such as bronchiectasis, adult CF, and central airway obstruction. High-resolution computed tomography (CT) scan is used to diagnose and quantify emphysema. Most cases of emphysema involve a history of cigarette smoking, chronic cough and sputum production, and dyspnea.
Laboratory analysis may include blood gas measurements and blood pH to indicate the presence of hypoxemia or hypercapnia (excess carbon dioxide in blood) and acid-base balance, sputum culture, or presence of immunoglobulin E (IgE) antibodies against specific allergens. Skin testing for allergens that trigger attacks is most useful in young clients with extrinsic allergic asthma.
TREATMENT.
The successful management of COPD requires a multifaceted approach that includes smoking cessation, pharmacologic management, airway clearance as needed, exercise (aerobic, strength, flexibility, posture, and breathing), control of complications, avoiding irritants, psychologic support, and dietary management.
The main goals for the client with COPD are to improve oxygenation and decrease carbon dioxide retention. These are accomplished by (1) reducing airway edema secondary to inflammation and bronchospasm (asthma) through the use of bronchodilator medication, (2) facilitating the elimination of bronchial secretions, (3) preventing and treating respiratory infection, (4) increasing exercise tolerance, (5) controlling complications, (6) avoiding airway irritants and allergens, (7) relieving anxiety and treating depression, which often accompany COPD, and (8) exercise to improve muscle oxidative capacity.
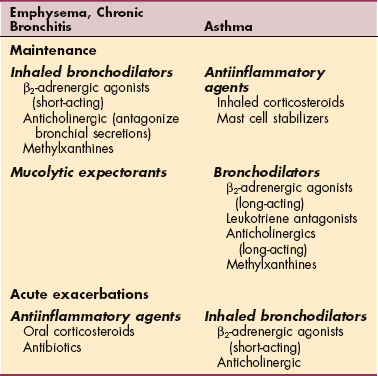
Common classifications of medications used in the treatment of COPD include oral or inhaled bronchodilators, antiinflammatory agents, antibiotics, mucolytic expectorants, mast cell membrane stabilizers, and antihistamines (Table 15-6). Combining bronchodilators improves effectiveness in reducing exacerbations and improves lung function.123 Systemic corticosteroids are of some help in acute exacerbations of COPD but have some side effects, including hyperglycemia,454 and do not produce any long-term benefits.320
Table 15-6
Pharmacotherapy for Chronic Obstructive Pulmonary Disease (COPD)
Courtesy Susan Queen, PT, PhD, University of New Mexico, Albuquerque, NM.
The benefits of pneumococcal vaccine have been proved (decreased mortality and hospitalization), and vaccination is recommended for all people with COPD. Annual prophylactic vaccination against influenza is also recommended.
Narcotics, tranquilizers, and sedatives are used with caution because these depress the respiratory center. Pharmacologic research includes investigation of multiple mediator antagonists, antiinflammatories with better delivery of the medication and lower side effects, induced repair of alveolar tissue, and effects of drug combinations.131,123
Long-term oxygen treatment (LTOT) reduces morbidity and extends life in clients with hypoxemia.99 People with PaO2 of 55 to 59 mm Hg or less (determined by arterial blood gases [ABGs]) with signs of tissue hypoxemia (see Table 15-2) are considered for long-term oxygen therapy. Oxygen therapy is also considered for those who desaturate during sleep or exercise. The National Heart, Lung, and Blood Institute in collaboration with the Centers for Medicare and Medicaid Services has identified areas of future research to improve care and/or reduce cost of care.99
Surgical treatment for COPD remains controversial, but lung-volume reduction surgery (LVRS), which is bilateral pneumectomy or removal of large bullae that compress the lung and add to dead space, has been shown to reduce the lung volume, relieve thoracic distention, and improve respiratory mechanics and reduce morbidity.78,199 LVRS may be an alternative treatment to lung transplantation for selected individuals with end-stage disease.
A multicenter, prospective, randomized study, called the National Emphysema Treatment Trial, was established by the National Heart, Lung, and Blood Institute to study the medical management, including pulmonary rehabilitation, in COPD. Confirming previous research, no change in lung function occurred with rehabilitation, but significant changes were seen in exercise tolerance, dyspnea, and quality of life. Pulmonary rehabilitation is considered important in selecting surgical candidates and preparing them for surgery.355
Lung transplantation, both single and double, are appropriate for clients with COPD when FEV1 is less than 24% predicted and/or the partial pressure of arterial carbon dioxide (PaCO2) is equal to or greater than 55 mm Hg. Survival rates are approximately 80% at year 1, 50% at year 5, and 35% at year 10.69,281
PROGNOSIS.
The prognosis for chronic bronchitis and emphysema is poor because these are chronic, progressive, and debilitating diseases. The death rate from COPD has increased 22% in the last decade, especially among older men, and the mortality rate 10 years after diagnosis is greater than 50%. COPD is largely preventable, and many believe that early recognition of small airway obstruction with appropriate treatment and cessation of smoking may prevent relentless progression of this disease. Early treatment of airway infections and vaccination against influenza and pneumococcal disease have an effect on morbidity and mortality of individuals with COPD.
There is no cure for COPD, but smoking cessation and oxygen therapy have been shown to increase the survival rate. Pulmonary rehabilitation has also been shown to improve quality of life, decrease hospitalizations, and decrease incidence of COPD exacerbations.53,382
Chronic Bronchitis
Chronic bronchitis is clinically defined as a condition of productive cough lasting for at least 3 months (usually the winter months) per year for 2 consecutive years. If obstructive lung disease characterized by a decreased FEV1/FVC ratio* less than 75% is combined with chronic cough, chronic bronchitis is diagnosed. Initially, only the larger bronchi are involved, but eventually all airways become obstructed, especially during expiration.
Risk Factors and Pathogenesis
Chronic bronchitis is characterized by inflammation and scarring of the bronchial lining. This inflammation obstructs air flow to and from the lungs and increases mucus production. Irritants, such as cigarette smoke, long-term dust inhalation, or air pollution, cause mucus hypersecretion and hypertrophy (increased number and size) of mucus-producing glands in the large bronchi. Epithelial atrophy, changes in squamous cells, and hypertrophy of smooth muscle cells occur.411
The swollen mucous membrane and thick sputum obstruct the airways, causing wheezing and a subsequent cough as the person tries to clear the airways. In addition, impaired ciliary function reduces mucous clearance and increases client susceptibility to infection. Infection results in even more mucus production with bronchial wall inflammation and thickening. As airways collapse, air is trapped in the distal portion of the lung, causing reduced alveolar ventilation, hypoxia, and acidosis. This downward spiral continues since the client now has an abnormal ventilation/perfusion (V/Q) ratio and resultant decreased PaO2.
As compensation for the hypoxemia, polycythemia (overproduction of erythrocytes) occurs. Cyanosis results from insufficient arterial oxygenation and peripheral edema from ventricular failure. Pulmonary vascular resistance caused by inflammation and loss of capillary beds will lead to cor pulmonale (right-sided congestive heart failure).
Clinical Manifestations
The symptoms of chronic bronchitis are persistent cough and sputum production (worse in the morning and evening than at midday). The increased secretion from the bronchial mucosa and obstruction of the respiratory passages interfere with the flow of air to and from the lungs. The result is SOB, prolonged expiration, persistent coughing with expectoration, and recurrent infection. Infection may be accompanied by fever and malaise.
Over time, reduced chest expansion, wheezing, cyanosis, and decreased exercise tolerance develop. In addition, the obstruction present results in decreased alveolar ventilation and increased PaCO2. Hypoxemia (deficient oxygenation of the blood) leads to polycythemia (overproduction of erythrocytes) and cyanosis. If not reversed, pulmonary hypertension leads to cor pulmonale. Severe disability or death is the final clinical picture.
MEDICAL MANAGEMENT
In stable conditions, reducing irritants and using a combination of bronchodilators is effective. There is no evidence for use of antibiotics, oral corticosteroids, expectorants or postural drainage. In acute exacerbations of chronic bronchitis, antibiotics and oral or IV corticosteroids can be effective.58 See also Medical Management and Special Implications for the Therapist: Chronic Obstructive Pulmonary Disease in the previous section in this chapter.
Emphysema
Emphysema is defined as a pathologic accumulation of air in tissues, particularly in the lungs, and is found in the lungs of most people with COPD. There are three types of emphysema (see Fig. 15-7). Centrilobular emphysema, the most common type, produces destruction in the bronchioles, usually in the upper lung regions. Inflammation develops in the bronchioles, but usually the alveolar sac (distal to respiratory bronchioles) remains intact.
Panlobular emphysema destroys the air spaces of the entire acinus and most commonly involves the lower lung. These two forms of emphysema, collectively called centriacinar emphysema, occur most often in smokers. Paraseptal (panacinar) emphysema destroys the alveoli in the lower lobes of the lungs, resulting in isolated blebs along the lung periphery. Paraseptal emphysema is believed to be the likely cause of spontaneous pneumothorax.
Etiologic Factors
Cigarette smoking is the major etiologic factor in the development of emphysema and has been shown to increase the numbers of alveolar macrophages and neutrophils in the lung,* enhance protease release,† and impair the activity of antiproteases. However, other factors, such as heredity, must determine susceptibility to emphysema because less than 10% to 15% of people who smoke develop clinical evidence of airway obstruction.
In many cases, emphysema occurs as a result of prolonged respiratory difficulties, such as chronic bronchitis that has caused partial obstruction of the smaller divisions of the bronchi. Emphysema can also occur without serious preceding respiratory problems as in the case of a defect in the elastic tissue of the lungs or in older persons whose lungs have lost their natural elasticity.
A number of clients with early onset of COPD have an inherited deficiency of (low levels or absent) AAT, a protective protein. AAT is made in the liver but circulates in the blood to protect the tissues in the body, including the lungs. Epidemiologists report approximately 100,000 people with this disorder; 20 million more may be undiagnosed asymptomatic carriers. AAT deficiency is suspected in smokers who develop emphysema before age 40 years and in nonsmokers who develop emphysema; symptoms may not develop until affected individuals are in their seventies. Progressive liver (cirrhosis) and lung disease (panlobular emphysema) occur when AAT is absent.404
Pathogenesis
Emphysema is a disorder in which destruction of elastin protein in the lung that normally maintains the strength of the alveolar walls leads to permanent enlargement of the acini. It is suspected that an interaction of accelerated cellular apoptosis, inflammation, and proteolysis causes the tissue destruction associated with emphysema.411
Eventually the loss of elasticity in the lung tissue causes narrowing or collapse of the bronchioles so that inspired air becomes trapped in the lungs, making breathing difficult, especially during the expiratory phase. Obstruction results from changes in lung tissues, rather than from mucus production and swelling as in chronic bronchitis (which is why steroids are usually not helpful in this condition).
The permanent overdistention of the air spaces with destruction of the walls (septa) between the alveoli is accompanied by partial airway collapse and loss of elastic recoil. Pockets of air form between the alveolar spaces (blebs) and within the lung parenchyma (bullae). This process leads to increased ventilatory dead space, or areas that do not participate in gas or blood exchange (Fig. 15-9).
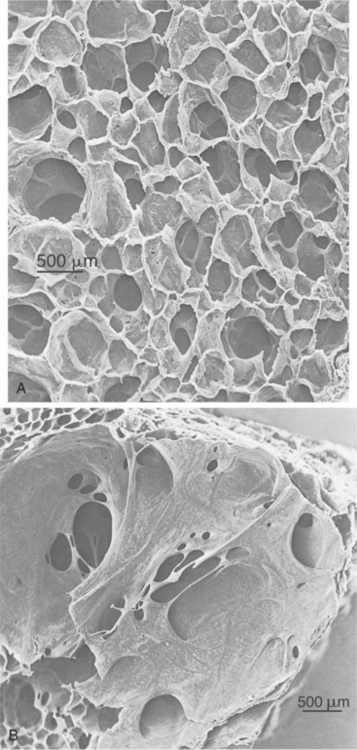
Figure 15-9 Effects of emphysema seen in these scanning electron micrographs of lung tissue. A, Normal lung with many small alveoli. B, Lung tissue affected by emphysema. Notice that the alveoli have merged into larger air spaces, reducing the surface area for gas exchange. (From Thibodeau GA, Patton KT: Structure and function of the body, ed 11, St Louis, 2000, Mosby. Used with permission.)
The WOB is increased as a result of ventilatory drive from hypoxemia and hypercapnia, increased effort during exhalation (normally passive recoil), and flattening of the diaphragm caused by hyperinflation. As the disease progresses, there is increasing dyspnea and pulmonary infection. Pulmonary hypertension develops from capillary loss and vessel intimal thickening, and this eventually leads to cor pulmonale (right-sided congestive heart failure).
In centrilobular emphysema the destruction of the lung is uneven and originates around the airways. The membranous bronchioles are thicker, narrower, and more reactive than in panlobular emphysema. Lung com- pliance is low or normal and does not relate to the extent of the emphysema (i.e., not to the losses of elastic recoil), but rather the decrease in airflow is related mainly to the degree of airway abnormality.
In contrast, panlobular emphysema is characterized by even destruction of the lung and the small airways appear less narrowed and less inflamed than in centrilobular emphysema. Lung compliance is increased and is related to the extent of the emphysema; the decrease in airflow is primarily associated with the loss of elastic recoil rather than with the abnormalities in the airways.95
At the molecular and microvascular levels, protease-antiprotease (associated with AATD emphysema) and oxidant-antioxidant theories continue under investigation as theories relate to impaired reparative mechanisms in the causation of emphysema. Oxidative damage by free radicals, which is the basis for the free radical theory of aging (see discussion in Chapter 6), identifies cigarette smoke as the main source of oxidants contributing to epithelial damage associated with smoking-induced emphysema. Determining the mechanisms regulating the antioxidant responses is critical to understanding the role of oxidants in the pathogenesis of smoking-induced lung disease and to developing future strategies for antioxidant therapy.382
Muscle wasting in emphysema and COPD is linked to increased TNF-α production. Respiratory muscle atrophy can lead to deterioration of lung function and increased WOB.411
Clinical Manifestations
At first, symptoms may be apparent only during physical exertion, but eventually marked exertional dyspnea progresses to dyspnea at rest. This occurs as a result of the irreversible destruction reducing elasticity of the lungs and increasing the effort to exhale trapped air. Cough is uncommon, with little sputum production. The client is often thin, has tachypnea with prolonged expiration, and must use accessory muscles for ventilation. To increase lung capacity and use of accessory muscles, the client often leans forward with arms braced on the knees supporting the shoulders and chest. The combined effects of trapped air and alveolar distention change the size and shape of the client’s chest, causing a barrel chest and increased expiratory effort. The normal arterial oxygen levels and dyspnea give clients a classic appearance (Fig. 15-10).
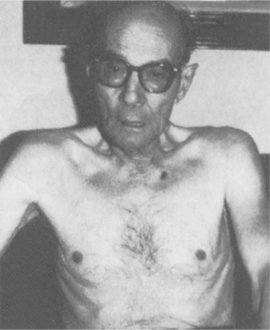
Figure 15-10 The person with emphysema presents with classic findings. Use of respiratory accessory (intercostal, neck, shoulder) muscles and cachectic appearance (wasting caused by ill health) reflect two factors: (1) shortness of breath (SOB), the most disturbing symptom, and (2) the tremendous increased work of breathing (WOB) necessary to increase ventilation and maintain normal arterial blood gases (ABGs). (From Kersten LD: Comprehensive respiratory nursing, Philadelphia, 1989, WB Saunders.)
Persons with emphysema have three times the rate of anxiety as the general public. This anxiety is associated with dyspnea or fear of dyspnea. Antianxiety medications, particularly selective serotonin reuptake inhibitors (SSRIs), and cognitive behavioral therapy have been shown to be helpful, although more research is needed.60
The most common signs and symptoms of AATD include dyspnea, wheezing, cough, chronic allergies (year round), asthma that does not respond to treatment, and liver problems. A high prevalence of wheezing to allergen and irritant exposures with symptoms of atopy suggests that asthma is common in AATD but is usually associated with COPD. Individuals with AATD who are susceptible to asthma require allergy evaluation and aggressive antiinflammatory management.125
MEDICAL MANAGEMENT
Diagnosis is made on the basis of history (usually cigarette smoking), physical examination, chest film, and pulmonary function tests. The most important factor in the treatment of emphy- sema is cessation of smoking. Human lungs benefit no matter when someone quits smoking (see Table 3-4); quitting smoking is the most effective way of preventing lung function decline caused by emphysema (and chronic bronchitis).
Pursed-lip breathing causes resistance to outflow at the lips, which in turn maintains intrabronchial pressure and improves the mixture of gases in the lungs. This type of breathing should be encouraged to help the client get rid of the stale air trapped in the lungs. However, this type of breathing pattern has been found to be ineffective for some people; methods to examine diaphragmatic movement and the potential for success with diaphragmatic breathing are available.70 Pulmonary rehabilitation and supplemental oxygen are critical aspects of management of COPD.78
In the case of AATD, serum testing to measure the levels of AAT is required to identify this problem. Underrecognition of AATD is common with diagnostic and treatment delays documented.403 AATD is treated with weekly intravenous augmentation therapy to slow down or halt the destruction of lung tissue. Home infusion is available for some people.
Infusion of purified AAT from pooled human plasma raises the concentration in serum and epithelial-lining fluid above the protective threshold. Although evidence suggests this treatment slows the decline of lung function and may reduce infection rates while enhancing survival, the cost-effectiveness has been questioned.402 Only nonsmokers can benefit from this treatment regimen; smoking increases neutrophils, which in turn inhibit AAT.
PROGNOSIS.
Prognosis for individuals with symptomatic AATD is poor with a high incidence of transplantation for liver and lung disease and even more on a transplant waiting list.405 Lung volume reduction surgery (surgically removing damaged areas of the lung) may help improve breathing and ventilation. Studies have not been able to predict who can benefit the most from this treatment approach. See also the section in this chapter on Medical Management under Chronic Obstructive Pulmonary Disease and Special Implications for the Therapist: Chronic Obstructive Pulmonary Disease.
Asthma
Asthma is defined as a reversible obstructive lung disease characterized by inflammation and increased smooth muscle reaction of the airways to various stimuli. It is a chronic condition with acute exacerbations and characterized as a complex disorder involving biochemical, autonomic, immunologic, infectious, endocrine, and psychologic factors in varying degrees in different individuals. This condition can be divided into two main types according to causative factors: extrinsic (allergic) and intrinsic (nonallergic), but other recognized categories include adult-onset, exercise-induced, aspirinsensitive, Aspergillus-hypersensitive, and occupational asthma (Table 15-7).
Table 15-7
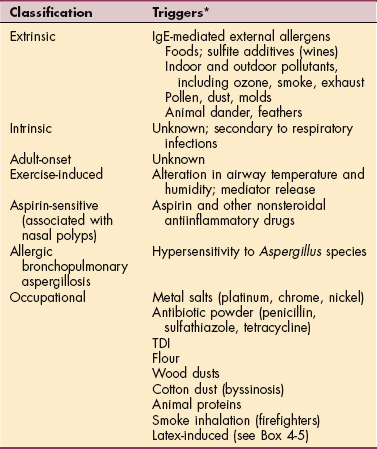
IgE, Immunoglobulin E; TDI, toluene diisocyanate.
*Emotional stress can be a trigger for anyone with asthma.
Incidence
Asthma, as one component of COPD, is the most common chronic disease in adults (11.9% incidence) and children (7% to 9% incidence), and the prevalence, morbidity, and mortality of asthma are increasing in the United States. Puerto Ricans have the highest incidence, followed by non-Hispanic Blacks and Native Americans.
The incidence of asthma cases and asthma deaths is increasing nationwide, but the reason for the increase is unknown. Explanations include increased accuracy of medical diagnosis and increased chart documentation among physicians, as well as increased prevalence as average life expectancy increases.
Risk Factors
The environment, including air pollution and exposure to other environmental toxins (including pesticides),205,157 homes that are airtight, exposure to pets, and windowless offices may also be risk factors contributing to the significant rise in incidence. The hygiene hypothesis blames lack of exposure to stimulants or overexposure to cleaning agents.277,368
Large families, early exposure to pets, early infections, and attending daycare may protect against allergic sensitization.426 Adults with asthma are 12 times more likely to develop COPD,181 and there are more than 4500 deaths from asthma each year in the United States.
Asthma can occur at any age, although it is more likely to occur for the first time before the age of 5 years. Antibiotic exposure during infancy appears to be a risk factor for developing childhood asthma. In childhood, it is three times more common and more severe in boys; however, after puberty, the incidence in the genders is equal, although monthly variations in asthma episodes seem to be correlated with estrogen levels for women.119
Children with lower birth weight (less than 5½ lb at birth) and prematurity (more than 3 weeks premature) are more susceptible to the effects of ozone (air pollution) compared with children who are born full term or full weight.311 It is estimated that asthma goes unrecognized as an adverse factor affecting performance in 1 in 10 adolescent athletes.
Asthma is found most often in urban, industrialized settings; in colder climates; and among the urban disadvantaged population (areas of poverty). Asthma is more prevalent and more severe among black children, but this may not be a result of race or low income per se but rather of demographic location because all children living in an urban setting are at increased risk for asthma.9 The number of African-American boys with asthma increased in 2001 to 2004, whereas the incidence remained stable for African-American girls and white children of both sexes.278
Overcrowded living conditions with repeated exposure to cigarette smoke, dust, cockroaches, and mold and where the use of a gas stove or oven is used for heat may be contributing factors.257 Alcoholic drinks, particularly wines, appear to be important triggers for asthmatic responses. Sensitivity to the sulfite additives and salicy lates present in wine seems likely to play an important role in these reactions.427
There is a relationship between obesity and asthma. Data from the Nurses Health Study II show that obesity increases women’s risk of developing adult-onset asthma possibly as a result of estrogen stored in lipids. The higher the body mass index (BMI), the greater the risk of developing asthma.72 One study demonstrated reduced respiratory function in 32% of obese children and only 3% of children with a normal BMI.425
Inflammatory mediators are produced by adipose tissue and may represent an immunologic connection between asthma and obesity. Increased leptin secretion may enhance airway inflammation while reduced adiponectin (an antiinflammatory agent) secretion affects modulation of inflammation. Comorbidity of asthma and obesity may complicate the treatment of either condition and appropriate asthma treatment may help with exercise and weight loss. Prevention of obesity and/or weight loss should be encouraged for all persons with asthma.349
Etiologic Factors
Asthma occurs in families, which indicates that it is an inherited disorder. Asthma is influenced by two genetic tendencies: one associated with the capacity to develop allergies (atopy) and the other with the tendency to develop hyperresponsiveness of the airways independent of atopy. Eighty percent of individuals with asthma report allergic rhinitis. Studies have shown that stimulation of the nasal mucosa causes bronchi to react.336 Environmental factors interact with inherited factors to cause attacks of bronchospasm. Asthma can develop when predisposed persons are infected by viruses or exposed to allergens or pollutants.
Extrinsic asthma, also known as atopic or allergic asthma, is the result of an allergy to specific triggers; usually the offending allergens are foods or environmental antigens suspended in the air in the form of pollen, dust, molds, smoke, automobile exhaust, and animal dander. In this type of asthma, mast cells, sensitized by IgE antibodies, degranulate and release bronchoactive mediators after exposure to a specific antigen. More than one-half of the cases of asthma in children and young adults are of this type.
Intrinsic asthma, or nonallergic asthma, has no known allergic cause or trigger, has an adult onset (usually over 40 years of age), and is most often secondary to chronic or recurrent infections of the bronchi, sinuses, or tonsils and adenoids. This type of asthma may develop from a hypersensitivity to the bacteria, or more commonly, viruses causing the infection. Other factors precipitating intrinsic asthma include drugs (aspirin and β-adrenergic antagonists), environmental irritants (occupational chemicals and air pollution), cold dry air, exercise, and emotional stress.
Occupational asthma is defined as variable narrowing of airways, causally related to exposure in the working environment to specific airborne dusts, gases, acids, molds, dyes, vapors, or fumes. Many of these substances are very common and not ordinarily considered hazardous. Only a small proportion of exposed workers develop occupational asthma, but it has received considerable attention recently as the most frequent occupational lung disease worldwide.
New substances and processes involving new chemicals have increased dramatically in the last 2 decades, and there is little information about “safe” levels of exposure that protect all workers.27 High-risk occupations for asthma include farmers, animal handlers, and agricultural workers; painters; plastics and rubber workers; cleaners and homemakers (especially if cooking is done with a gas stove); textile workers; metal workers; and bakers, millers, and other food processors. Exposure to biologic dusts and gases and fumes can cause a 30% to 50% increased risk of asthma.
Pathogenesis
The airways are the site of an inflammatory response consisting of cellular infiltration, epithelial disruption, mucosal edema, and mucous plugging (Fig. 15-11). The release of inflammatory mediators produces bronchial smooth muscle spasm; vascular congestion; increased vascular permeability; edema formation; production of thick, tenacious mucus; and impaired mucociliary function.
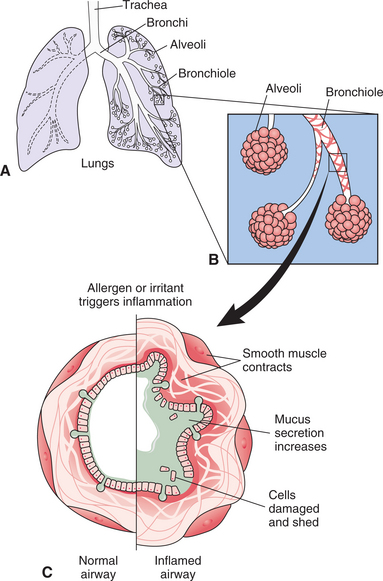
Figure 15-11 Bronchiole response in asthma. A, Air is distributed throughout the lungs via small airways called bronchioles. B, Healthy bronchioles accommodate a constant flow of air when open and relaxed. C, In asthma, exposure to an allergen or irritant triggers inflammation, causing constriction of the smooth muscle surrounding the bronchus (bronchospasm). The airway tissue swells; this edema of the mucous membrane further narrows airways with production of excess mucus also interfering with breathing
Several mediators also cause thickening of airway walls and increased contractile response of bronchial smooth muscles. These changes in the bronchial musculature, combined with the epithelial cell damage caused by eosinophil infiltration, result in the airway hyperresponsiveness characteristic of asthma.
Once the airway is in spasm and airways are swollen, mucus plugs the airway, trapping distal air. V/Q mismatch, hypoxemia, obstructed expiratory flow, and increased workload of breathing follow. Most attacks of asthmatic bronchospasm are short-lived, with freedom from symptoms between episodes, although airway inflammation is present, even in people who are asymptomatic.
Excessive airway narrowing occurs when the smooth muscle shortens (not necessarily to an abnormal degree). The relationship between the mechanical and contractile properties of smooth muscle and lung volume and how these interact to determine smooth muscle length are the subject of new research. The relative importance of smooth muscle area and mechanical properties, altered airway structure, and airway inflammation in asthma is not yet determined.216
Although definitive causes of asthma have not been determined, there is much known about the immune system mechanisms that lead to allergic airway obstruction. T-helper cells secrete cytokine, which contribute to inflammation that is mediated by IgE. IgE is present on mast cells and other airway cells. After repeated contact with antigens, these cells break down and release toxins, particularly leukotrienes, which cause bronchospasm and hypersecretions.30
Researchers are also investigating the possibility of underlying neurogenic mechanisms that may contribute to the pathogenesis and pathophysiology of asthma.88,361,336 Investigations include determination of the linkages among psychosocial factors and behavioral, neural, endocrine, and immune processes in the role of asthma. It has been shown that health-related behaviors, demographic factors, and psychosocial factors influence susceptibility to and severity of exacerbation of asthma.240,390
Clinical Manifestations
Clinical signs and symptoms of asthma differ in presentation (Box 15-6), degree (Table 15-8), and frequency among clients, and although current symptoms are the most important concern of affected people, they reflect the current level of asthma control more than underlying disease severity.327
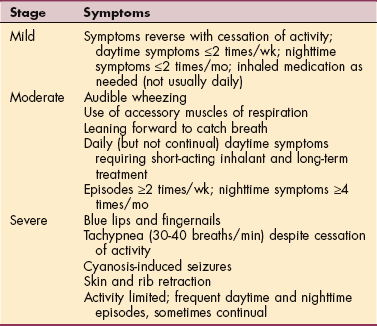
During full remission, clients are asymptomatic and pulmonary function tests are normal. Over time, repeated attacks cause airway remodeling, chronic air trapping, proliferation of submucosal glands, and hypertrophied smooth muscle. This may progress to irreversible changes and COPD.
At the beginning of an attack, there is a sensation of chest constriction, inspiratory and expiratory wheezing, nonproductive coughing, prolonged expiration, tachycardia, and tachypnea. Secondary bronchospasm is marked by recurrent attacks of dyspnea, with wheezing caused by the spasmodic constriction of the bronchi. Other symptoms may include fatigue, a tickle in the back of the throat accompanied by a cough in an attempt to clear the airways, and nostril flaring (advanced).
The person usually assumes a classic sitting or squatting position to reduce venous return, leaning forward so as to use all the accessory muscles of respiration. The skin is usually pale and moist with perspiration, but in a severe attack there may be cyanosis of the lips and nail beds. In the early stages of the attack coughing may be dry, but as the attack progresses, the cough becomes more productive of a thick, tenacious mucoid sputum. The nocturnal worsening of asthma is a common feature of this disease and may affect daytime alertness, even in children.116 Rhinitis, chronic cough, snoring, and apnea may be responsible for sleep disturbance.
An acute attack that cannot be altered with routine care is called status asthmaticus. This is a medical emergency requiring more vigorous pharmacologic and support measures. Despite appropriate treatment, this condition can be fatal. With severe bronchospasm, the workload of breathing increases 5 to 10 times, which can lead to acute cor pulmonale.
When air is trapped, a severe paradoxical pulse develops as venous return is obstructed; blood pressure drops over 10 mm Hg during inspiration. Pneumothorax occasionally develops. If status asthmaticus continues, hypoxemia worsens and acidosis begins. If the condition is untreated or not reversed, respiratory or cardiac arrest will occur.
MEDICAL MANAGEMENT
Heavier emphasis on teaching selfmanagement and especially prevention for anyone with asthma is recommended by the American Academy of Allergy, Asthma, and Immunology. An excellent daily asthma management plan is available.11 Healthy People 2010 has identified 11 objectives specifically related to this condition, including increasing the proportion of people with asthma who receive formal education as part of their management program (see Healthy People 2010: http://health.gov/healthypeople/).
DIAGNOSIS.
Pulse oximetry, pulmonary function studies, bronchial challenge test with methacholine, skin prick tests, ABG analysis, serum IgE and blood eosinophil counts, induced sputum cell counts, exhaled nitric oxide (marker for eosinophilic inflammation),419 questionnaires, and chest films may be used in assessing for both the presence and the severity of asthma (see Chapter 40 for a description of and reference values for these tests). The methacholine challenge test is a valuable diagnostic measure. There are strong correlations with this test and some symptoms.462 Inexpensive but reliable spirometer testing can be used to obtain evidence of the bronchial hyperreactivity associated with asthma.
Diagnosis may be delayed in older clients who have other illnesses that cause similar symptoms or who attribute their breathlessness to the effects of aging and respond to the onset of asthma by limiting their activities to avoid eliciting symptoms. The diagnosis of occupational asthma is usually based on history of a temporal association between exposure and the onset of symptoms and objective evidence that these symptoms are related to airflow limitation. Sputum induction and analysis may be helpful in confirming occupational asthma.159
TREATMENT.
Identifying specific allergens for each individual and avoidance of asthma triggers, combined with the use of two classes of medications (bronchodilators and antiinflammatory agents; see Table 15-6), has been recommended in the management of asthma. In the past, asthma was thought to be caused by spasms of the muscles surrounding the airways between the trachea and lungs and therefore treated first with bronchodilator drugs to widen the constricted airways and ease symptoms. It is now clear that asthma attacks are actually episodic flareups of chronic inflammation in the lining of the airways necessitating the use of inhaled antiinflammatories to suppress the underlying inflammation and allow the airways to heal.
Most people require bronchodilator therapy to control symptoms by activating β-agonist receptors on smooth muscle cells in the respiratory tract, thereby relaxing the bronchial muscle and opening the airways; those with mild symptoms may use metered-dose inhaler (MDI) devices to administer sympathomimetic bronchodilators on an as-needed basis.
People who experience moderate-to-severe asthma may require daily administration of antiinflammatory agents, such as corticosteroids, to prevent asthma attacks. Corticosteroids dampen the entire immune system response. Antiinflammatory drugs have a preventive action by interrupting the development of bronchial inflammation. They may also modify or terminate ongoing inflammatory reactions in the airways.
It is important that people with asthma know the difference between medications that must be taken daily to prevent asthma symptoms and medications that relieve symptoms once they begin. Low-dose corticosteroid inhalants are recommended to reduce the risk of side effects (e.g., psychiatric problems, reduced growth in children, ocular effects, death, osteoporosis, or alopecia and hirsutism) from prolonged use.117,407 Leukotriene- receptor antagonists inhibit inflammation and have been shown to be safe and effective in adults with asthma and allergic rhinitis434 (see further discussion in Chapter 6).
Oxygen metabolites (free radicals) may play a direct or indirect role in the modulation of airway inflammation. Excessive superoxide and hydroxyl radical production accompanied by significantly lower free radical scavengers in asthma (the latter even during rest) endorses the correlation between disease severity and oxygen radical production in people with asthma.383
Low dietary intake and blood levels of vitamins C and E, selenium, and flavonoids are seen in people with asthma.302,337,384 Although some researchers suggest that antioxidant nutrients (especially obtained from food sources such as fruits and vegetables) appear helpful in asthma treatment,288,300,317,337 others report that people with asthma may have a diminished capacity to restore the antioxidant defenses, making the use of supplemental antioxidants questionable in this population.341
Many complementary treatments have been used to ameliorate asthma symptoms though there has been minimal research to validate most of these claims. There is minimal but growing evidence to support the use of acupuncture.266 Spinal manipulation and other manual therapy have been deemed to be ineffective in the treatment of asthma.128,203 In one study of 65 people, yoga was found to have no effect on asthma.370 Complementary treatments are still being studied for benefits and adverse affects.42b
Genetic treatment is under investigation. For example, gene transfer into the airway cells to block mediator proteins (signal transducer activator of transcription [STAT]) from setting off an immune response or too strong an immune response in the asthma pathway is the subject of several studies.129,372 A recombinant monoclonal antibody (Omalizumab) was approved by the FDA in 2003. This antibody prevents IgE from binding to mast cells and other effector cells, preventing inflammation.438
PROGNOSIS.
The outlook for clients with bronchial asthma is excellent despite the recent increase in the death rate. Childhood asthma may disappear, but only about one-quarter of the children with asthma become symptom-free when their airways reach adult size. Factors that predict adult asthma include gender (males are more likely to outgrow asthma), smoking, allergy to dust mites, degree of airway hyperresponsiveness, and early age of onset.379,418 Adults with asthma are 12 times more likely to progress to COPD, but studies indicate that the majority of people with asthma do not experience a decline in pulmonary mechanics or appear to be at risk for reduced life expectancy.181,290
Attention to general health measures and use of pharmacologic agents permit control of symptoms in nearly all cases. The risk of lung cancer is two times greater in people with asthma compared with those who do not have a history of asthma.66
Status asthmaticus can result in respiratory or cardiac arrest and possible death (see previous discussion). If ventilation becomes necessary, prognosis for recovery is poor.
15-7 SPECIAL IMPLICATIONS FOR THE THERAPIST
Impaired Ventilation, Respiration/Gas Exchange, and Aerobic Capacity/Endurance Associated with Airway Clearance Dysfunction
Impaired Ventilation and Respiration/Gas Exchange Associated with Ventilatory Pump Dysfunction or Failure
Impaired Ventilation and Respiration/Gas Exchange Associated with Respiratory Failure
Many people with asthma do not even know they have the disease. Some think they simply have chronic bronchitis, colds, or allergies. Anyone who reports coughing or a feeling of tightness in the chest when others smoke nearby and especially anyone who gasps for breath after exercise should be referred to a physician for evaluation of these symptoms.
Exercise-induced bronchospasm (EIB), or exercise-induced asthma (EIA), does not represent a unique syndrome but rather an example of the airway hyperactivity common to all persons with asthma. EIA is an acute, reversible, usually self-terminating airway obstruction that develops 5 to 15 minutes after strenuous exercise when the person no longer breathes through the nose, warming and humidifying the air, but opens the mouth. Breathing cold, dry air through the mouth degranulates mast cells that release bronchoconstrictive mediators inducing EIB. EIB/EIA lasts 15 to 60 minutes after the onset.
Because physical therapists prescribe and observe exercise, they may be the first to recognize symptoms of undiagnosed asthma. Coughing is the most common symptom of EIA, but other symptoms include chest tightness, wheezing, and SOB. The affected (but undiagnosed) individual may comment, “I am more out of shape than I thought.” This should be a red flag for the therapist to consider the possibility of asthma and need for medical diagnosis and intervention.
If an asthma attack should occur during therapy, first assess the severity of the attack. Place the person in the high Fowler’s position and encourage diaphragmatic and pursed-lip breathing. If the client has an inhaler available, provide whatever assistance is necessary for that person to self-administer the medication. Help the person relax while assessing the person’s response to the medication.
Usually the episode subsides spontaneously in 30 to 60 minutes. The severity of an attack increases as the exercise becomes increasingly strenuous. Warmup exercise can ameliorate the inflammatory process by affecting platelet-eosinophil/neutrophil reactions.439 The problem is rare in activities that require only short bursts of energy (e.g., baseball, sprints, gymnastics, or skiing) compared with those that involve endurance exercise (e.g., soccer, basketball, distance running, or biking).
Swimming, even long-distance swimming, is well tolerated by people with EIA, partly because they are breathing air fully saturated with moisture, but the type of breathing required may also play a role. Exhaling under water, which is essentially pursed-lip breathing, is beneficial because it prolongs each expiration and increases the end-expiratory pressure within the respiratory tree.
There are many barriers to exercise for people with asthma, including lack of motivation, time constraints, weather conditions, and belief that exercise is not good for this condition.273 To prevent secondary complication of a sedentary lifestyle and because obesity can contribute to the inflammatory process associated with asthma, exercise and education about exercise should be part of any treatment program.
There is strong evidence to support physical training for cardiovascular training in this population.351 There is inadequate evidence for a positive effect of breathing exercises and inspiratory muscle training in individuals who have asthma.202,352
Bronchospasm can occur during exercise (especially in EIA) if the person with asthma has a low blood oxygen level before exercise. For this reason, it is helpful to take bronchodilators by MDI 20 to 30 minutes before exercise, performing mild stretching and warmup exercises during that time period to avoid bronchospasm with higher workload exercise. Increased exercise should be accompanied by good bronchodilator coverage to promote bronchodilation and improve alveolar ventilation and oxygenation. Exercise guidelines for adults with asthma can be modified from recommendations for children with asthma (Table 15-9).
Table 15-9
Exercise Guidelines for Children With Asthma
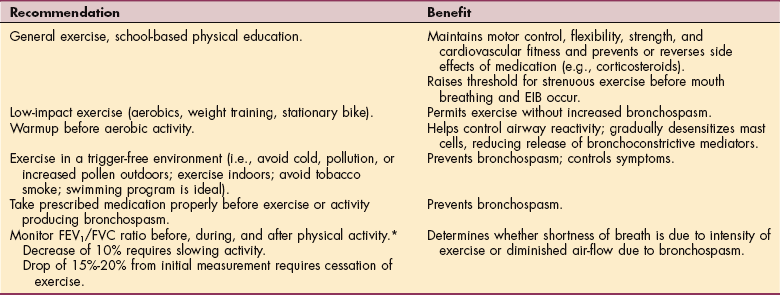
EIB, Exercise-induced bronchospasm; FEV1/FVC, ratio of forced expiratory volume in 1 sec to forced vital capacity.
*Peak flowmeters can be used to obtain this information. Determine the child’s normal range of lung function by having the child blow in the meter in the morning and evening for 1 week. The average level measured varies from person to person and is influenced by gender and height. Testing should establish a peak flow protocol against which lung function can be compared to determine if deterioration has occurred.
Many clients have found that using their inhalers in this way before exercise permits them to exercise without onset of symptoms. Proper administration of an MDI is essential (see Box 15-5). The first dose induces dilation of the larger, central bronchial tubes, relaxing smooth muscles in the airways; the second dose dilates the bronchioles (smaller airways).
Metabolism of certain drugs administered can be altered by exercise, tobacco, marijuana, or phenobarbital (all of which increase drug metabolism). Cimetidine (Tagamet), erythromycin, or the presence of a viral infection may decrease drug metabolism.
If a client develops signs of asthma or any bronchial reactivity during exercise, the physician must be informed. Medication dosage can then be altered to maintain optimal physical performance. Excessive use of inhaled β-adrenergic agents (using three or more full canisters monthly) requires physician referral for further evaluation.
Common manifestations of drug-induced (theophylline) toxicity include nausea, vomiting, tremors, anxiety, tachycardia and arrhythmias, and hypotension. The use of nonsteroidal antiinflammatory drugs (NSAIDs), including aspirin, in older people with asthma should be avoided if possible because the drug interactions can cause increased bronchospasm in susceptible individuals.
Some athletes do not achieve the control needed for the performance demands of competition. The effectiveness of short-acting medications and medications in general for asthma varies widely among people with asthma while exercising. The preventive benefits of each medication dose may wane after taking a new drug for several weeks. Any athlete with asthma who cannot perform at the levels desired or expected because of asthma symptoms should be advised to review medications and medication use with the physician.
Long-term use of inhaled corticosteroids in the management of moderate-to-severe asthma is associated with decreased bone mineral density (BMD) and associated increased risk of fractures and a high occurrence of asymptomatic vertebral fractures, particularly in high-risk postmenopausal women (i.e., those not receiving hormone replacement therapy).15,364,451 African-American children may be afforded some protection from osteoporosis as compared to Caucasian children using high-dose inhaled corticosteroids.176
All people receiving glucocorticoid therapy (e.g., prednisolone) at doses of 7.5 mg/day or more for 6 months or longer should discuss with their physician the use of low-dose inhaled corticosteroids, assessment of BMD, and preventive therapies (e.g., bisphosphonates, calcium supplementation, or vitamin D).321 The physical therapist can be very instrumental in providing education for the prevention and intervention for the treatment of osteopenia and osteoporosis. See the section on Osteoporosis in Chapter 24.
Monitoring vital signs can alert the therapist to important changes in bronchopulmonary function. Developing or increasing tachypnea may indicate worsening asthma or drug toxicity. Other signs of toxicity, such as diarrhea, headache, and vomiting, may be misinterpreted as influenza. Hypertensive blood pressure readings may indicate asthma-related hypoxemia.
Auscultate the lungs frequently, noting breath sounds including the degree of wheezing and the quality of air movement. In this way, any change in respiratory status will be more readily perceived. If the client does not have a productive cough in the presence of rhonchi (dry rattling in the bronchial tube), teach effective coughing techniques.
Therapy can augment the medical management of the client with status asthmaticus. In coordination with the individual’s medications, the therapist helps to remove secretions; promotes relaxed, more efficient breathing; enhances V/Q matching; reduces hypoxemia; and teaches the client to coordinate relaxed breathing with general body movement.
Caution needs to be observed to avoid stimuli that bring on bronchospasm and deterioration (e.g., aggressive percussion, forced expiration maneuvers, aggressive bag ventilation, or manual hyperinflation with an intubated individual). Certain body positions may have to be avoided because of client intolerance or exacerbation of symptoms in those positions.111
Immediate medical care is recommended for anyone with asthma who is struggling to breathe with no improvement in 15 to 20 minutes after initial treatment with medications or who is hunched over and unable to straighten up or resume activity after medication dosage. The presence of blue or gray lips or nail beds is another indication of the need for immediate medical attention.
Bronchiectasis
Bronchiectasis is a progressive form of obstructive lung disease characterized by irreversible destruction and dilation of airways generally associated with chronic bacterial infections. Clinically, it is considered an extreme form of bronchitis and no longer considered part of COPD. Abnormal and permanent dilation of the bronchi and bronchioles develops when the supporting structures (bronchial walls) are weakened by chronic inflammatory changes associated with secondary infection.
Incidence and Etiologic and Risk Factors
The incidence of bronchiectasis is low in the United States because of improved control of bronchopulmonary infections. However, any condition producing a narrowing of the lumen of the bronchioles may create bronchiectasis, including TB, adenoviral infections, and pneumonia. Bronchiectasis also develops in people with immunodeficiencies involving humoral immunity, recurrent aspiration, and abnormal mucociliary clearance (immotile cilia syndromes).
CF causes about one-half of all cases of bronchiectasis. Sinusitis, dextrocardia (heart located on right side of chest), Kartagener’s syndrome (alterations in ciliary activity), defective development of bronchial cartilage (Williams-Campbell syndrome), and endobronchial tumor predispose a person to bronchiectasis.
Pathogenesis
Although bronchiectasis has been viewed as a progressive disease of destruction and dilation of the medium and large airways, there is now evidence of the importance of the small airways in the pathogenesis of this condition. Chronic inflammation of the bronchial wall by mononuclear cells is common to all types of bronchiectasis. Abnormal bronchial dilation characteristic of bronchiectasis is accompanied by accumulation of wet secretions that plug the airway and cause bronchospasm, producing even more mucus. A vicious cycle of bacteria-provoked inflammatory lung damage occurs with irreversible destruction or fragmentation of the bronchial wall and resultant fibrosis further obstructing and obliterating the bronchial lumen (Fig. 15-12).
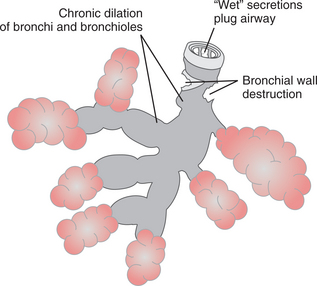
In response to these changes, large anastomoses develop between the bronchial and pulmonary blood vessels to increase the blood flow through the bronchial circulation. V/Q mismatch causes hypoxia and hypercapnia. Damage to these anastomoses is responsible for the hemoptysis present in persons with bronchiectasis.
Clinical Manifestations
The most immediate symptom of bronchiectasis is persistent coughing, with large amounts of purulent sputum production (worse in the morning). Rhinosinusitis, dyspnea, and fatigue are also strongly related to bronchiectasis. For those without other significant disease, most report chronic childhood respiratory problems.242
Weight loss, anemia, and other systemic manifestations, such as low-grade fever, hemoptysis, and weakness, are also common. Clubbing may occur, and the breath and sputum may become foul-smelling with advanced disease. Heart failure may occur due to the vascular fibrosis. There is a known correlation between bronchiectasis and rheumatoid arthritis, but the exact mechanism remains unknown.
MEDICAL MANAGEMENT
Imaging studies (e.g., high-resolution CT scan) have become increasingly accurate in depicting the features of early bronchiectasis. Ultrafast and multislice CT scans have increased the value of CT as a diagnostic tool by reducing the need for sedation or anesthesia. Other diagnostic tests include radiographic studies, laboratory tests including sweat chloride test for CF, electron microscopy of bronchial biopsy for immotile cilia, and sputum culture analyses.
TREATMENT.
The goals of treatment are removal of secretions and prevention of infection. The principal treatment is airway clearance techniques, bronchodilators, and antibiotics selected on the basis of sputum smears and cultures. A recent study demonstrated that use of inhaled corticosteroids improved quality of life for people with steady-state bronchiectasis.282 Hydration is important, and oxygen may be administered. Surgical resection is reserved for the few clients with localized bronchiectasis and adequate pulmonary function who fail to respond to conservative management or for the person with massive hemoptysis. Long-term care is the same as for any person with COPD.
PROGNOSIS.
The morbidity and mortality associated with bronchiectasis have declined markedly in industrialized nations, but prevalence remains high in Pacific and Asian countries. The overall prognosis is often poor, and although bronchiectasis is usually localized to a lung lobe or segment, persistent, nonresolving infection may cause the disorder to spread to other parts of the same lung. Complications of bronchiectasis include recurrent pneumonia, lung abscesses, metastatic infections in other organs (e.g., brain abscess), and cardiac and respiratory failure. Good pulmonary hygiene and avoidance of infectious complications in the involved areas may reverse some cases of bronchiectasis.
Bronchiolitis
Bronchiolitis refers to several morphologically distinct pathologic conditions that involve the small airways. Acute bronchiolitis is a commonly occurring, diffuse, and often severe inflammation of the lower airways (bronchioles) in children under 2 years caused by a viral infection. Acute adult onset is related to asthma, aspiration, or bronchiectasis.
Bronchiolitis was once classified as a type of chronic interstitial pneumonia and referred to as small airways disease; progress in pathology has provided more specific etiology-directed diagnoses that reflect the individual reaction patterns observed. Constrictive bronchiolitis, diffuse panbronchiolitis, and airway-centered fibrosis are also forms of bronchiolitis.
Bronchiolitis obliterans in the adult is now considered acute or chronic with identification of these special forms (e.g., obliterative, eosinophilic bronchiolitis in asthma, necrotizing bronchiolitis in viral infection, or toxic fume bronchiolitis after exposure to noxious gases and the development of chemical pneumonitis).346,435 Bronchiolitis obliterans is the most important clinical complication in heart-lung and lung transplant recipients and may represent a form of allograft rejection; it is a rare complication of allogeneic (human-to-human) bone marrow transplantation. Circulating fibroblast precursors from bone marrow may be implicated in transplant recipients with bronchiolitis.63
Bronchiolitis obliterans may occur in association with rheumatoid arthritis, polymyositis, and dermatomyositis. Penicillamine therapy has been implicated as a possible cause of bronchiolitis obliterans in clients with rheumatoid arthritis.
Incidence and Etiologic Factors
Bronchiolitis obliterans in adults usually occurs with chronic bronchitis; bronchiolitis in children is associated with pulmonary infections, such as respiratory syncytial virus (RSV), parainfluenza viruses, adenoviruses, or pertussis (whooping cough), or associated with measles. Primarily present in winter and spring, it is easily spread by hand-to-nose or nose-to-eye transmission. Exudative bronchiolitis, which is inflammation of the bronchioles with exudation of grey tenacious sputum, is often associated with asthma.
Pathogenesis and Clinical Manifestations
Variable degrees of obstruction occur in response to infection as the bronchiolar mucosa swells and the lumina fill with mucus and exudate. Depending on the type, these changes occur as the walls of the bronchi and bronchioles are infiltrated with inflammatory cells, increased goblet cells, and fibroblasts.
Bronchiolitis obliterans is usually confined to one lobe and its airways, showing dense collagen but no proliferation of fibroblasts. In contrast, constrictive bronchiolitis is characterized by fibrosis of the submucosa and peribronchial tissues.
Chronic bronchiolitis with fibrosis (airway centered fibrosis) presents with epithelial hyperplasia and goblet cell and squamous metaplasia.435 Hyperinflation, obstructive emphysema from partial obstruction, and patchy areas of atelectasis may occur distal to the inflammatory lesion as the disease progresses.
Cough, respiratory distress, and cyanosis occur initially, followed by a brief period of improvement. Dyspnea, paroxysmal cough, sputum production, and wheezing with marked use of accessory muscles follow as the disease progresses. Apnea may be the first indicator of RSV infection in very young infants. Severe disease may be followed by a rise in PaCO2 (hypercapnia), leading to respiratory acidosis and hypoxemia.
MEDICAL MANAGEMENT
Currently there is no vaccine for RSV. The outcome of infection depends on host and viral genetics. A better understanding of RSV molecular biology and pathogenesis will help facilitate an effective vaccine and molecular targets for new drug treatment. Understanding RSV disease mechanisms in order to develop a vaccine is difficult because there is a wide range of RSV disease phenotypes in humans and disparities in RSV disease phenotypes among the animal models used in research.308
Frequent handwashing and not sharing items, such as cups, glasses, and utensils, with persons who have RSV illness can decrease the spread of virus to others. Excluding children with colds or other respiratory illnesses (without fever) who are well enough to attend childcare or school settings may not decrease the transmission of RSV, since it is often spread in the early stages of illness. In a hospital setting, RSV transmission can and should be prevented by strict attention to contact precautions such as handwashing and wearing gowns and gloves.
DIAGNOSIS AND TREATMENT.
Diagnosis is made on the basis of clinical findings, age, the season, and the epidemiology of the community. On chest radiographs, this condition is difficult to differentiate from bacterial pneumonia. RSV can be positively identified using an enzyme-linked immunosorbent assay (ELISA) from direct aspiration of nasal secretions. Early diagnosis in transplant recipients may be facilitated by using CT.112
There is no specific treatment for bronchiolitis, and medical therapy is controversial. Treatment modalities may include steroids, humidified air, hydration, and airway clearance techniques such as postural drainage, coughing, and deep-breathing exercises. Antibiotics may be used initially when a bacterial cause of illness has not been ruled out or for secondary infections. Mist therapy combined with oxygen by hood or tent to alleviate dyspnea and hypoxia may be used with children.
Corticosteroids should be used with caution because there is a relationship between levels of cortisol and severity of the disease.343 Recently, heliox therapy (combination of oxygen and helium) has been shown to have a positive effect on wheezing and respiratory distress.73 In another study, the use of hypertonic saline with epinephrine also improved respiratory status and decreased hospital length of stay of infants.414
PROGNOSIS.
The acute disease lasts about 3 to 10 days, and the majority of cases can be managed at home with a good prognosis. Hospitalization may be necessary for anyone with complicating conditions such as underlying lung or heart disease, associated debilitated states, poor hydration, or questionable care at home. Some children deteriorate rapidly and die within weeks; others may follow a more long-term course. Onset before the age of 1 may be related to allergies or asthma, but there appear to be adverse long-term pulmonary consequences.412 In the adult, the acute form usually has a good prognosis, but the prognosis for chronic bronchiolitis obliterans is poor.
Sleep-Disordered Breathing
Sleep-disordered breathing comprises a collection of syndromes characterized by breathing abnormalities during sleep that result in intermittently disrupted gas exchange and in sleep interruption. Sleep-disordered breathing includes CSR, hypoventilation syndromes with and without chronic lung disease, heavy snoring with daytime sleepiness (upper airway resistance syndrome), and sleep apnea. The most common and only one discussed here, sleep apnea syndrome, is defined as significant daytime symptoms (e.g., sleepiness) in conjunction with evidence of sleep-related upper airway obstruction and sleep disturbance.41
There are three types of sleep apnea: central, obstructive, and mixed. Central sleep apnea is caused by altered chemosensitivity and cerebral respiratory control. In this type of apnea, the brain fails to send the appropriate signals to the respiratory muscles to initiate breathing and there is no diaphragmatic movement and no airflow. This is seen in infants less than 40 weeks’ conceptual age and in people with neurologic disorders (e.g., tumors, brain infarcts, diffuse encephalopathies).
The most dramatic presentation is the person with repetitive apneas during sleep, accompanied by extreme daytime sleepiness. Obstructive sleep apnea (OSA), the most commonly diagnosed form of sleep apnea, is characterized by respiratory effort without airflow because of upper airway obstruction. Mixed sleep apnea is a central apnea that is immediately followed by an obstructive event.
Incidence
Depending on geographic area, prevalence of OSA ranges from 2% to 58% in men and 10% to 37% in women.349 Gender differences in upper airway collapse have not been observed, although there appears to be a relationship to testosterone levels.366,465,466 Forty percent of obese people have OSA, and 70% of people with sleep apnea are obese. OSA in children without neurologic impairment is most commonly caused by adenotonsillar hypertrophy, although obesity is positively correlated with this disorder in children also.18 Children with Down syndrome are particularly vulnerable to OSA and should be tested at age 3 to 4 years.387
Etiologic and Risk Factors
OSA is due to partial or complete pharyngeal collapse during sleep, leading to either reduction (hypopnea) or cessation (apnea) of breathing. The main cause in adults is upper body obesity, especially a large neck circumfer ence. A neck circumference greater than 16 inches for a woman or greater than 17 inches in a man correlates with an increased risk for this disorder.432
People with anatomically narrowed upper airways, such as occur in micrognathia; macroglossia (large tongue); and adenoid, uvula, elongated soft palate, or tonsillar hypertrophy, are predisposed to the development of OSA. Fat deposits or swelling in any or all of these tissues causes further obstruction. Other risk factors include increasing age; genetic factors (sleep-disordered breathing clusters in families); neurologic disorders; smoking; and cardiopulmonary dysfunctions such as hypertension, moderate-to-severe heart failure (including cor pulmonale), calcification of carotid arteries, chronic bronchitis, or cardiac dysrhythmia. Alcohol or sedatives before sleeping may precipitate or worsen the condition.
Pathogenesis
There are several hypotheses as to the pathogenesis of sleep apnea syndrome. Collapse or obstruction of the airway may occur with the inhibition of muscle tone that characterizes rapid eye movement (REM) sleep. When loss of normal pharyngeal muscle tone allows the larynx to collapse passively during inspiration, upper airway obstruction occurs and prevents effective ventilation.
By definition, apnea is a complete cessation of ventilation and therefore is precipitated by complete pharyngeal collapse, whereas hypopnea results from partial pharyngeal closure and is manifested by a substantial reduction in, but not a cessation of, breathing. Both conditions can lead to substantial hypoxia and hypercapnia with arousal from sleep required to reestablish airway patency and a resumption of ventilation. This cycle of recurrent pharyngeal collapse with subsequent arousal from sleep leads to the primary symptoms of daytime somnolence.135 Enlarged tonsils or adenoids are the primary cause of sleep apnea in children.353
Clinical Manifestations
The frequent interruptions of deep, restorative sleep often lead to daytime (including morning) sluggishness and headaches, daytime fatigue, excessive daytime sleepiness, cognitive impairment, recent weight gain, and sexual impotence. Bed partners usually report loud cyclic snoring with periods of silence (breath cessation), restlessness, frequent episodes of waking up gasping, and often thrashing movements of the extremities during sleep.
Neurocognitive effects may include personality changes; irritability, hyperactivity, and depression; judgment impairment or poor school performance; domestic, work-related, or automobile accidents; memory loss; and difficulty concentrating.
Neurocognitive effects of apnea may also cause a mood disorder leading to an erroneous diagnosis of dysthymia; treatment with standard antidepressant medications may exacerbate the condition.235 Anyone with acquired or congenital neurologic disorders, such as tetraplegia, stroke, and Down syndrome, is susceptible to sleep disorders.387,401
Fragmented sleep with its repetitive cycles of snoring, airway collapse, and arousal may cause hypertension in some people. Sleep-disordered breathing may be a risk factor for cardiovascular involvement, including angina pectoris, acute myocardial infarction, cardiac arrhythmias, and ischemic stroke.64,65,338 The exact mechanisms for this are yet unknown, but there is an association with inflammation and prothrombic factors, as well as CNS effects.237 Risk for stroke is independent of other risk factors, including obesity and hypertension.457
MEDICAL MANAGEMENT
Diagnosis may be made using sleep monitoring devices, radiologic imaging, laboratory assays, questionnaires, and clinical signs and symptoms, but the most reliable test to confirm the diagnosis is overnight polysomnography (i.e., monitoring the subject during sleep for periods of apnea and lowered blood oxygen saturation).
The physician must differentiate sleep apnea syndrome from seizure disorder, narcolepsy, or psychiatric depression. A hemoglobin level is obtained, and thyroid function tests are performed. Several clinical diagnostic predictive formulas are being studied.332 Diagnosis criteria for children have not been standardized, although it is recognized that they should be different from adult criteria.353 The primary symptom in children is hyperactivity, not daytime somnolence.
TREATMENT.
Obstructive and mixed types of sleep apnea syndrome can be treated. Since many clients with sleep apnea are overweight, weight loss is recommended. Weight loss may be curative, but only a small percentage of people maintain their weight loss and symptoms return with weight gain. Therefore alternative interventions have been developed, and the most common treatment for OSA is CPAP used during sleep. The positive pressure from the CPAP pumps open the airway and prevents it from obstructing, but this treatment technique may not be tolerated by some people and adherence to its use is only about 40%.264 Adherence level is demonstrated in the first 2 weeks, but there may be increased compliance after 2 years because the perceived benefits outweigh the barriers such as noise and discomfort.151,406
BiPAP and automatic self-adjusting CPAP have also been used, but their effectiveness is not known at this time.252 One study has evaluated adherence and effectiveness of CPAP in children. CPAP was effective in improving oxygen saturation and the average nightly use was 5.3 hours (a time markedly overestimated by parents).276
In adults, CPAP is more effective than no treatment and treatment with oral appliances (OA) in reducing apnea, decreasing blood pressure, and improving quality of life.155 Guidelines for use of CPAP are published.252 OA may be inserted into the mouth at bedtime and used to hold the jaw forward, thus preventing pharyngeal occlusion. Such devices are regulated by the FDA. There is evidence that OA reduces sleepiness and disordered breathing when compared to control but that CPAP is more effective overall. It is recommended that OA be used for mild sleep disorders or when the person does not tolerate CPAP.261
Surgery is recommended if an airway obstruction can be determined as the cause of the sleep apnea. Neuro genic causes of sleep apnea are more difficult to control. There is insufficient evidence to draw any conclusions about the effectiveness of medication. Medication has been directed at improving tone in the upper airway, increasing ventilatory drive, reducing REM sleep, and reducing airway resistance or surface tension.390 Alcohol and hypnotic medications should be avoided. In children, tonsillectomy/adenoidectomy has been shown be effective in a majority of cases.353,385