Health Promotion of the Adolescent and Family
On completion of this chapter the reader will be able to:
 Describe the physical changes that occur at puberty.
Describe the physical changes that occur at puberty.
Discuss the reactions of the adolescent to physical changes that take place at puberty.
Demonstrate an understanding of the processes by which the adolescent develops a sense of identity.
Discuss the significance of the changing interpersonal relationships and the role of the peer group during adolescence.
Outline a health teaching plan for adolescents.
Plan a sexuality education session for a group of adolescents.
Identify the causes and discuss the preventive aspects of injuries during adolescence.
RELATED TOPICS and ADDITIONAL RESOURCES
 IN TEXT
IN TEXTAcne, Ch. 30
Adolescent Pregnancy, Ch. 17
Altered Growth and Maturation, Ch. 17
Dental Health: Toddler, Ch. 12; School-Age Child, Ch. 15
Disorders Related to the Reproductive System, Ch. 17
Growth and Development, Ch. 5
Health Problems of School-Age Children and Adolescents, Ch. 17
Injury Prevention, Ch. 15
Traumatic Injury, Ch. 31
PROMOTING OPTIMAL GROWTH AND DEVELOPMENT
Adolescence is a period of transition between childhood and adulthood—a time of rapid physical, cognitive, social, and emotional maturation as the boy prepares for manhood and the girl prepares for womanhood (see Cultural Awareness box). The precise boundaries of adolescence are difficult to define, but this period is customarily viewed as beginning with the gradual appearance of secondary sex characteristics at about 11 or 12 years of age and ending with cessation of body growth at 18 to 20 years.
Several terms are used to refer to this stage of growth and development. Puberty refers to the maturational, hormonal, and growth process that occurs when the reproductive organs begin to function and the secondary sex characteristics develop. This process is sometimes divided into three stages: prepubescence, the period of about 2 years immediately before puberty when the child is developing preliminary physical changes that herald sexual maturity; puberty, the point at which sexual maturity is achieved, marked by the first menstrual flow in girls but by less obvious indications in boys; and postpubescence, a 1- to 2-year period following puberty during which skeletal growth is completed and reproductive functions become fairly well established. Adolescence, which literally means, “to grow into maturity,” is generally regarded as the psychologic, social, and maturational process initiated by the pubertal changes. It involves three distinct subphases: early adolescence (ages 11 to 14), middle adolescence (ages 15 to 17), and late adolescence (ages 18 to 20). The term teenage years is used synonymously with adolescence to describe ages 13 through 19.
BIOLOGIC DEVELOPMENT
The physical changes of puberty are primarily the result of hormonal activity under the influence of the central nervous system, although all aspects of physiologic functioning are mutually interacting. The obvious physical changes are noted in increased physical growth and in the appearance and development of secondary sex characteristics; less obvious are physiologic alterations and neurogonadal maturity, accompanied by the ability to procreate. Physical distinction between the sexes is made on the basis of distinguishing characteristics. Primary sex characteristics are the external and internal organs that carry out the reproductive functions (e.g., ovaries, uterus, breasts, penis). Secondary sex characteristics are the changes that occur throughout the body as a result of hormonal changes (e.g., voice alterations, development of facial and pubertal hair, fat deposits), but that play no direct part in reproduction.
 CULTURAL AWARENESS
CULTURAL AWARENESSOther societies in which adolescence is seen as part of the life cycle may have ideas very different from those of American culture about how the adolescent years are to be spent. For example, some societies discourage contact between adolescent males and females. Sexual experimentation is outlawed, and all grown children, males and females, remain in their parents’ home until they wed. In the United States we tend to believe that the way our culture is organized is the way all cultures are or should be organized, but of course this is not so. Each society is unique. The way we describe adolescence, the way we experience it, and the predisposition of our adolescents toward violence are peculiar to our American culture.
Modified from Prothrow-Stith D: Deadly consequences: how violence is destroying our teenage population and a plan to begin solving the problem, New York, 1993, HarperCollins.
Hormonal Changes of Puberty
The events of puberty are caused by hormonal influences and controlled by the anterior pituitary (adenohypophysis) in response to a stimulus from the hypothalamus. Stimulation of the gonads has a dual function:
1. Production and release of gametes—production of sperm in the male and maturation and release of ova in the female
2. Secretion of sex-appropriate hormones—estrogen and progesterone from the ovaries (female) and testosterone from the testes (male)
The ovaries, testes, and adrenals secrete sex hormones. These hormones are produced in varying amounts by both sexes throughout the life span. The adrenal cortex is responsible for the small amounts secreted before the pubescent years, but the sex hormone production that accompanies maturation of the gonads is responsible for the biologic changes observed during puberty.
Estrogen, the feminizing hormone, is found in low quantities during childhood. This hormone is secreted in slowly increasing amounts until about age 11 years. In males this gradual increase continues through maturation. In females the onset of estrogen production in the ovary causes a pronounced increase that continues until about 3 years after the onset of menstruation, at which time it reaches a maximum level that continues throughout the reproductive life of the female.
Androgens, the masculinizing hormones, are also secreted in small and gradually increasing amounts up to about 7 or 9 years of age, at which time there is a more rapid increase in both sexes, especially boys, until about age 15 years. These hormones appear to be responsible for most of the rapid growth changes of early adolescence. With the onset of testicular function, the level of androgens (principally testosterone) in males increases over that in females and continues to increase until a maximum is attained at maturity.
Sexual Maturation
The visible evidence of sexual maturation is achieved in an orderly sequence, and the state of maturity can be estimated on the basis of the appearance of these external manifestations. The age at which these changes are observed and the time required to progress from one stage to another may vary among children. The time from the appearance of breast buds to full maturity may be 1½ to 6 years for adolescent girls. It may take 2 to 5 years for male genitalia to reach adult size. The stages of development of secondary sex characteristics and genital development have been defined as a guide for estimating sexual maturity and are referred to as the Tanner stages. The usual sequence of appearance of maturational changes is presented in Box 16-1.
Sexual Maturation in Girls.: In most girls the initial indication of puberty is the appearance of breast buds, an event known as thelarche, which occurs between 9 and 13½ years of age (Fig. 16-1). This is followed in approximately 2 to 6 months by growth of pubic hair on the mons pubis, known as adrenarche (Fig. 16-2). In a minority of normally developing girls, however, pubic hair may precede breast development.
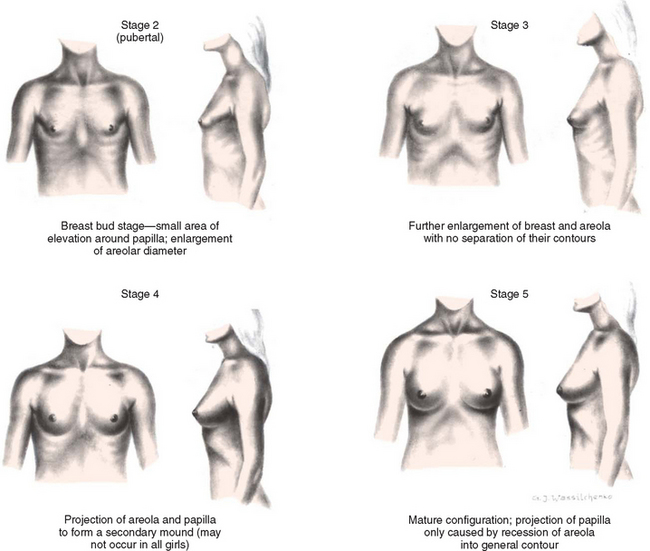
FIG. 16-1 Development of breasts in girls—average age span, 9 to 13½ years. Stage 1 (prepubertal—elevation of papilla only) is not shown.(Modified from Marshall WA, Tanner JM: Variations in pattern of pubertal changes in girls, Arch Dis Child 44(235):291-303, 1969; and Daniel WA, Paulshock BZ: A physician’s guide to sexual maturity, Patient Care 13:122-124, 1979.)
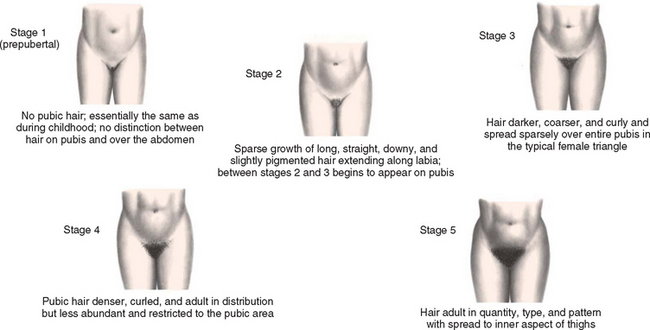
FIG. 16-2 Growth in pubic hair in girls—average age span for stages 2 through 5: 9 to 13½ years. (Modified from Marshall WA, Tanner JM: Variations in pattern of pubertal changes in girls, Arch Dis Child 44(235):291-303, 1969; and Daniel WA, Paulshock BZ: A physician’s guide to sexual maturity, Patient Care 13:122-124, 1979.)
The initial appearance of menstruation, or menarche, occurs about 2 years after the appearance of the first pubescent changes, approximately 9 months after attainment of peak height velocity, and 3 months after attainment of peak weight velocity. Menarche has been related to a critical gain in body fat content (more fat content, earlier menarche), although this is controversial. The normal age range of menarche is usually 10½ to 15 years, with the average age being 12 years, 9½ months for North American girls. Ovulation and regular menstrual periods usually occur 6 to 14 months after menarche. Girls may be considered to have pubertal delay if breast development has not occurred by age 13 or if menarche has not occurred within 4 years of the onset of breast development.
Sexual Maturation in Boys.: The first pubescent changes in boys are testicular enlargement accompanied by thinning, reddening, and increased looseness of the scrotum (Fig. 16-3). These events usually occur between 9½ and 14 years of age. Early puberty is also characterized by the initial appearance of pubic hair. Penile enlargement begins, and testicular enlargement and pubic hair growth continue throughout midpuberty. During this period there is also increasing muscularity, early voice changes, and development of early facial hair. Temporary breast enlargement and tenderness, gynecomastia, are common during midpuberty, occurring in up to one third of boys. The spurts in height and weight occur concurrently toward the end of midpuberty. For most boys, breast enlargement disappears within 2 years. By late puberty there is a definite increase in the length and width of the penis, testicular enlargement continues, and first ejaculation occurs. Axillary hair develops, and facial hair extends to cover the anterior neck. Final voice changes occur secondary to the growth of the larynx. Concerns about pubertal delay should be considered for boys who exhibit no enlargement of the testes or scrotal changes by 13½ to 14 years of age, or if genital growth is not complete 4 years after the testicles begin to enlarge.
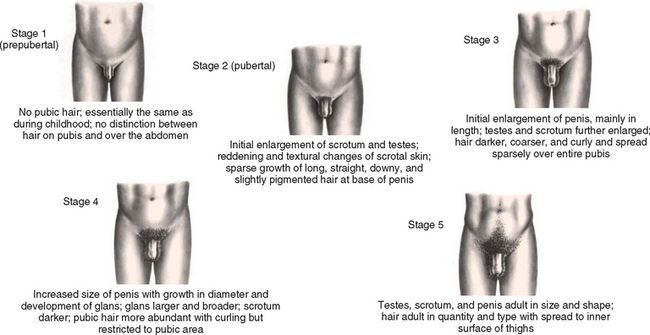
FIG. 16-3 Developmental stages of secondary sex characteristics and genital development in boys—average age span, 9½ to 14 years. (Modified from Marshall WA, Tanner JM: Variations in pattern of pubertal changes in girls, Arch Dis Child 44(235):291-303, 1969; and Daniel WA, Paulshock BZ: A physician’s guide to sexual maturity, Patient Care 13:122-124, 1979.)
Physical Growth
A constant phenomenon associated with sexual maturation is a dramatic increase in growth. The final 20% to 25% of height is achieved during puberty, and most of this growth occurs during a 24- to 36-month period—the adolescent growth spurt. This accelerated growth occurs in all children but, as in other areas of development, is highly variable in age of onset, duration, and extent. The growth spurt begins earlier in girls, usually between ages 9½ and 14½ years; on average it begins between ages 10½ and 16 years in boys. During this period, the average boy gains 10 to 30 cm (4 to 12 inches) in height and 7 to 30 kg (15.5 to 66 pounds) in weight. The average girl, in whom the growth spurt is slower and less extensive, gains 5 to 20 cm (2 to 8 inches) in height and 7 to 25 kg (15.5 to 55 pounds) in weight. Growth in height typically ceases 2 to 2½ years after menarche in girls and at age 18 to 20 years in boys.
This increase in size is acquired in a characteristic sequence. Growth in length of the extremities and neck precedes growth in other areas, and because these parts are the first to reach adult length, the hands and feet appear larger than normal during adolescence. Increases in hip and chest breadth take place in a few months, followed several months later by an increase in shoulder width. These changes are followed by increases in length of the trunk and depth of the chest. This sequence of changes is responsible for the characteristic long-legged, gawky appearance of the early adolescent child.
Sex Differences in General Growth Patterns.: Sex differences in general growth and distribution patterns are apparent in skeletal growth, muscle mass, adipose tissue, and skin. Skeletal growth differences between boys and girls are apparently a function of hormonal effects at puberty and are evident primarily in limb length. The earlier cessation of growth in girls is caused by epiphyseal unity under the potent effect of estrogen secretion, and the hormonal effect on female bone growth is much stronger than the similar effect of testosterone in boys. In boys the prolonged growth period before puberty and the less rapid epiphyseal closure are reflected in their greater overall height and longer arms and legs. Other skeletal differences are increased shoulder width in boys and broader hip development in girls.
Hypertrophy of the laryngeal mucosa and enlargement of the larynx and vocal cords occur in both boys and girls to produce voice changes. Girls’ voices become slightly deeper and considerably fuller, but the effect in boys is striking. The change in the voice of adolescent boys occurs between Tanner stages 3 and 4, with the voice often shifting uncontrollably from deep to high tones in the middle of a sentence. The average lengthening of the vocal cords is 10.9 mm (0.4 inch) for boys and 4.2 mm (0.17 inch) for girls.
Growth of lean body mass, principally muscle, which tends to occur after the bone growth spurt, takes place steadily during adolescence. Lean body mass is both quantitatively and qualitatively greater in boys than in girls at comparable stages of pubertal development. Muscle development, under the influence of androgenic hormones, increases steadily. Muscles become remarkably well developed in boys, whereas in girls, muscle mass increase is proportionate to general tissue growth.
Nonlean body mass, primarily fat, is also increased but follows a less orderly pattern. There may be a transient increase in subcutaneous fat just before the skeletal growth spurt, especially in boys. This is followed 1 to 2 years later by a modest to marked decrease, which is again more marked in boys. Later, variable amounts of fat are deposited to fill out and contour the mature physique in patterns characteristic of the adolescent’s sex, particularly in the regions over the thighs, hips, and buttocks and around the breast tissue. It should be noted, however, that pediatric obesity is steadily on the increase in the United States, and obesity can change the timing and sequence of puberty. Girls with thelarche as the first sign of puberty have earlier menarche and greater body fat and body mass index (BMI) at menarche than girls with adrenarche as the first pubertal sign. This may have long-term effects for increased risk of adult adiposity and obesity (Biro, Lucky, Simbarti, and others, 2003).
Hormonal influences during puberty cause acceleration in growth and maturation of the skin and its structural appendages. Sebaceous glands become extremely active at this time, especially those on the genitalia and in the “flush areas” of the body (i.e., face, neck, shoulders, upper back, and chest). This increased activity and the structural nature of the glands are extremely important in the pathogenesis of a common problem of puberty: acne (see Chapter 30). The eccrine sweat glands, present almost everywhere on the human skin, become fully functional and respond to emotional as well as thermal stimulation. Heavy sweating appears to be more pronounced in boys than in girls. The apocrine sweat glands, nonfunctional in childhood, reach secretory capacity during puberty. Unlike the eccrine sweat glands, the apocrine glands are limited in distribution and grow in conjunction with hair follicles in the axillae, around the areola of the breast, around the umbilicus, on the external auditory canal, and in the genital and anal regions. Apocrine glands secrete a thick substance as a result of emotional stimulation that, when acted on by surface bacteria, becomes highly odoriferous.
Body hair assumes characteristic distribution patterns and changes texture during puberty. Under the influence of gonadal and adrenal androgens, hair coarsens, darkens, and lengthens at sites related to secondary sex characteristics. Pubic and axillary hair appears in both sexes, although pubic hair is more extensive in males than in females. Beard, mustache, and body hair on the chest, upward along the linea alba, and sometimes on other areas (e.g., back and shoulders) appears in males and is androgen dependent. Extremity hair appears in varying amounts in both males and females but is also more prolific in the male.
Physiologic Changes
A number of physiologic functions are altered in response to some of the pubertal changes. The size and strength of the heart, blood volume, and systolic blood pressure increase, whereas the pulse rate and basal heat production decrease (see inside back cover). Blood volume, which has increased steadily during childhood, reaches a higher value in boys than in girls, a fact that may be related to the increased muscle mass in pubertal boys. Adult values are reached for all formed elements of the blood. Respiratory rate and basal metabolic rate, decreasing steadily throughout childhood, reach the adult rate in adolescence. Respiratory volume and vital capacity are increased, and to a far greater extent in males than in females. During this period, physiologic responses to exercise change drastically: performance improves, especially in boys, and the body is able to make the physiologic adjustments needed for normal functioning after exercise is completed. These capabilities are a result of the increased size and strength of muscles and the increased level of cardiac, respiratory, and metabolic functioning.
PSYCHOSOCIAL DEVELOPMENT: DEVELOPING A SENSE OF IDENTITY (ERIKSON)
Traditional psychosocial theory holds that the developmental crisis of adolescence leads to the formation of a sense of identity. Throughout childhood, individuals have been going through the process of identification as they concentrate on various parts of the body at specific times. During infancy children identify themselves as being separate from the mother, during early childhood they establish gender-role identification with the appropriate-sex parent, and in later childhood they establish who they are in relation to others. In adolescence they come to see themselves as distinct individuals, somehow unique and separate from every other individual.
Adolescence begins with the onset of puberty and extends to relative physical and emotional stability at or near graduation from high school. During this time the adolescent is faced with the crisis of group identity vs alienation. In the period that follows, the individual strives to attain autonomy from the family and develop a sense of personal identity as opposed to role diffusion. A sense of group identity appears to be essential to the development of a personal identity. Young adolescents must resolve questions concerning relationships with a peer group before they are able to resolve questions about who they are in relation to family and society.
Group Identity.: During the early stage of adolescence, pressure to belong to a group is intensified. Teenagers find it essential to belong to a group from which they can derive status. Belonging to a crowd helps adolescents establish the differences between themselves and their parents. They dress as the group dresses and wear makeup and hairstyles according to group criteria, all of which are different from those of the parental generation. Language, music, and dancing reflect a culture that is exclusive to the adolescent. When adults begin to emulate these fashions and interests, the style changes immediately. The evidence of adolescent conformity to the peer group and nonconformity to the adult group provides teenagers with a frame of reference for self-assertion and rejection of the identity of their parents’ generation. To be different is to be unaccepted and alienated from the group.
Individual Identity.: The quest for personal identity is part of the ongoing identification process. As adolescents establish identity within a group, they also attempt to incorporate multiple body changes into a concept of the self. Body awareness is part of self-awareness. In their search for identity, adolescents consider the relationships that have developed between themselves and others in the past, as well as the directions they hope to take in the future.
Significant others hold expectations for the behavior of the adolescent. Often these expectations or demands are persistent enough that individuals make certain decisions that they would not make if they were solely responsible for identity formation. Adolescents may find it too easy to slip into the roles expected by others without incorporating personal goals or questioning decisions. Thus individuals may become what parents or others wish them to be based on these premature decisions. Young persons might form a negative identity when society or their culture provides them with a self-image that is contrary to the values of the community. Labels such as “juvenile delinquent,” “hoodlum,” or “failure” are applied to certain adolescents, who then accept and live up to these labels with behaviors that validate and strengthen them.
Jeremy, age 17, will be graduating from high school in the spring. His mother, a single parent, tells you that she is concerned because graduation is quickly approaching and Jeremy has made no plans for what he will do with his life after graduation. Whenever Jeremy mentions the topic, his mother tells him, “This is what you must do,” and begins to outline the steps he must take. Jeremy just walks away. She asks, “What should I do?” What advice should you give Jeremy’s mother?
1. Evidence—Is there sufficient evidence to draw any conclusions about what advice to give Jeremy’s mother?
2. Assumptions—Describe an underlying assumption about each of the following issues:
a. Adolescents and the search for personal identity
b. The influence of others on the adolescent’s search for personal identity
3. What implications and priorities for nursing care can be drawn at this time?
4. Does the evidence objectively support your argument (conclusion)?
5. Are there alternative perspectives to your arguments? What are they?
The process of evolving a personal identity is time-consuming and fraught with periods of confusion, depression, and discouragement. Determining an identity and a place in the world is a critical and perilous feature of adolescence (see Critical Thinking Exercise). However, as the pieces gradually shift and settle into place, a positive identity emerges. Role diffusion results when the individual is unable to formulate a satisfactory identity from the multiplicity of aspirations, roles, and identifications.
Sex-Role Identity.: Adolescence is the time for consolidation of a sex-role identity. During early adolescence the peer group begins to communicate expectations regarding heterosexual relationships, and as development progresses, adolescents encounter expectations for mature sex-role behavior from both peers and adults. Expectations vary from culture to culture, among geographic areas, and among socioeconomic groups.
Emotionality.: Adolescents vacillate in their emotional states between considerable maturity and childlike behavior. One minute they are exuberant and enthusiastic; the next minute they are depressed and withdrawn. Unpredictable but essentially normal, mood swings are common during this time. As the tension is relieved, emotion is brought under control and individuals retreat to review what has happened, to attempt to master their anger, and to grow in their ability to control their emotions and gain from the new experience. Because of these mood swings, adolescents are frequently labeled as unstable, inconsistent, and unpredictable. Little things can cause an emotional upheaval and, depending on the teenager’s interpretation, can mean a great deal.
Teenagers are better able to control their emotions in later adolescence. They can approach problems more calmly and rationally, and although they are still subject to periods of sadness, their feelings are less vulnerable and they begin to demonstrate the more mature emotions of later adolescence. Whereas early adolescents react immediately and emotionally, older adolescents can control their emotions until socially acceptable times and places for expression present themselves. They are still subject to heightened emotion, and when it is expressed, their behavior reflects feelings of insecurity, tension, and indecision.
COGNITIVE DEVELOPMENT (PIAGET)
Cognitive thinking culminates with the capacity for abstract thinking. This stage, the period of formal operations, is Piaget’s fourth and last stage. Adolescents are no longer restricted to the real and actual, which was typical of the period of concrete thought; now they are also concerned with the possible. They think beyond the present. Without having to center attention on the immediate situation, they can imagine a sequence of events that might occur, such as college and occupational possibilities; how things might change in the future, such as relationships with parents; and the consequences of their actions, such as dropping out of school. At this time their thoughts can be influenced by logical principles rather than just their own perceptions and experiences. They become increasingly capable of scientific reasoning and formal logic.
Adolescents are capable of mentally manipulating more than two categories of variables at the same time. For example, they can consider the relationship between speed, distance, and time in planning a trip. They can detect logical consistency or inconsistency in a set of statements and evaluate a system or set of values in a more analytic manner. For instance, they question the parent who insists on honesty in the youngster but at the same time cheats on an income tax report or expense account.
In adolescence, young people begin to consider both their own thinking and the thinking of others. They wonder what opinion others have of them, and they are able to imagine the thoughts of others. With this capacity comes the ability to differentiate between others’ thoughts and their own and to interpret the thoughts of others more accurately. They are able to understand that few concepts are absolute or independent of other influencing factors. As they become aware that other cultures and communities have different norms and standards from their own, it becomes easier for them to accept members of these other cultures, and the decision to behave in their own culture in an accepted manner becomes a more conscious commitment.
MORAL DEVELOPMENT (KOHLBERG)
Although younger children merely accept the decisions or point of view of adults, adolescents, to gain autonomy from adults, must substitute their own set of morals and values. When old principles are challenged but new independent values have not yet emerged to take their place, young people search for a moral code that preserves their personal integrity and guides their behavior, especially in the face of strong pressure to violate the old beliefs. Their decisions involving moral dilemmas must be based on an internalized set of moral principles that provides them with the resources to evaluate the demands of the situation and to plan actions that are consistent with their ideals.
Late adolescence is characterized by serious questioning of existing moral values and their relevance to society and the individual. Adolescents can easily take the role of another. They understand duty and obligation based on reciprocal rights of others and the concept of justice that is founded on making amends for misdeeds and repairing or replacing what has been spoiled by wrongdoing. However, they seriously question established moral codes, often as a result of observing that adults verbally ascribe to a code but do not adhere to it.
SPIRITUAL DEVELOPMENT
As adolescents move toward independence from parents and other authorities, some begin to question the values and ideals of their families. Others cling to these values as a stable element in their lives as they struggle with the conflicts of this turbulent period. Adolescents need to work out these conflicts for themselves, but they also need support from authority figures or peers for their resolution.
Adolescents are capable of understanding abstract concepts and of interpreting analogies and symbols. They are able to empathize, philosophize, and think logically. Most teens search for ideals and speculate about illogical statements and conflicting ideologies. Their tendency toward introspection and emotional intensity often makes it difficult for others to know what they are thinking. They tend to keep their thoughts private, fearing that no one will understand these feelings that they perceive to be unique and special. However, they may reveal deep spiritual concerns. They need support and encouragement in their struggle for understanding and the freedom to question without censure.
Greater levels of religiosity and spirituality are associated with fewer high-risk behaviors and more health-promoting behaviors (Brown, 2001). Nurses play an important role for teens by providing an opportunity to discuss issues regarding spirituality.
SOCIAL DEVELOPMENT
To achieve full maturity, adolescents must free themselves from family domination and define an identity independent of parental authority. However, this process is fraught with ambivalence on the part of both teenagers and their parents. Adolescents want to grow up and to be free of parental restraints, but they are fearful as they try to comprehend the responsibilities that are linked with independence. Feelings of immortality and exemption from the consequences of risk-taking behavior, although viewed as negative, can serve an important developmental function at this time. These feelings give adolescents the courage to separate from their parents and become independent. Part of this emancipation involves developing social relationships outside the family that help teenagers identify their role in society. Adolescence is a time of intense sociability and often a time of equally intense loneliness. Acceptance by peers, a few close friends, and the secure love of a supportive family are requisites for interpersonal maturation.
Relationships with Parents
During adolescence the parent-child relationship changes from one of protection-dependency to one of mutual affection and equality. The process of achieving independence often involves turmoil and ambiguity as both parent and adolescent learn to play new roles and work toward this end while, at the same time, resolving the often painful series of rifts essential to establishing the ultimate relationship.
Most behavior observed in the adolescent is related to the struggle for independence and the external restrictions and checks that are placed on this spontaneous maturation process. On the one hand, adolescents are accepted as maturing preadults. They are allowed privileges heretofore denied, and they are provided with increasing responsibilities. On the other hand, because of their unpredictability and insecurity in evaluating situations and making sound judgments, they must conform to regulations and restrictions set by adults. This state of affairs is particularly exemplified by the struggle between parents and adolescents concerning the nightly curfew.
As teenagers assert their rights for grown-up privileges, they frequently create tensions within the home. They resist parental control, and conflicts can arise from almost any situation or any subject. Favorite topics of dispute include use of the home telephone, Internet use, the need for a personal cellular telephone, manners, dress, chores and duties, homework, disrespectful behavior, friendships, dating and relationships, money, automobiles, alcohol and other substance abuse, and time schedules. Present in these areas of conflict are the overriding arguments that “Everyone else has one” or is allowed the desired item or privilege and the ever-present assertions that “You don’t understand me or trust me” and “You always treat me like a baby.” Spoken or unspoken, parents’ reactions consist of “Is this all the thanks I get for what I have done for you?”
Teenagers’ earliest attempts to achieve emancipation from parental controls are manifested in a period of rejection of the parents. They absent themselves from home and family activities and spend an increasing amount of time with the peer group. They confide less in their parents, but parents continue to play an important role in the personal and health-related decision making of adolescents.
With advancing adolescence, teenagers become more competent, and with this competence comes a need for more autonomy. Although they may be psychologically prepared for independence, they are often thwarted in their efforts by lack of money or other parental barriers. Conflict arises in relation to the teenager’s outside activities and the elements of privacy and trust. Parental monitoring remains important throughout adolescence and may have a direct influence on adolescent sexual and substance use behavior. Parents should be guided toward an authoritative style of parenting in which authority is used to guide the adolescent while allowing developmentally appropriate levels of freedom and providing clear, consistent messages regarding expectations. Authoritative style of parenting has been shown to have both immediate and long-term protective effects toward adolescent risk reduction (DeVore and Ginsburg, 2005). However, to gain the trust of adolescents, parents must respect their adolescent’s privacy and show an honest and sincere interest in what the adolescent believes and feels (see Family Focus box).
Relationships with Peers
Although parents remain the primary influence in their lives, for the majority of teenagers, peers assume a more significant role in adolescence than they did during childhood. The peer group serves as a strong support to teenagers, individually and collectively, providing them with a sense of belonging and a feeling of strength and power. The peer group forms the transitional world between dependence and autonomy.
 FAMILY FOCUS
FAMILY FOCUSCommunication with Adolescents: The Art of Listening
Conflicts between parents and their adolescents are often a result of a natural characteristic of parenthood: the desire to protect one’s offspring—from harm or from simply doing something “stupid” or embarrassing or something they may later regret. Teenagers sometimes “bounce” their thoughts and ideas off adults. At times they really want some feedback; at other times they simply want to elicit a reaction.
I found it easy to listen openly, thoughtfully, and without interrupting when my teenagers’ friends discussed troublesome topics. However, one day, when one of my own teenagers had a similar conversation with me, the parent part kicked in. I felt responsible and spoke my piece on the spot.
This brought communication to a halt and resulted in defensiveness. It was a long time before my child tried to talk to me about anything controversial again.
The next time one of my teenagers started a similar conversation, I decided to try to trick myself. Throughout the entire conversation, I told myself over and over again to act as if this were not my teenager, but rather someone else’s child. I found this actually worked quite well, and I was able to listen without interrupting. I continue to use the system, sometimes with more success than at other times.
Peer Group.: Adolescents are usually social, gregarious, and group minded. Thus the peer group has an intense influence on adolescents’ self-evaluation and behavior. To gain acceptance by a group, younger teenagers tend to conform completely in such things as mode of dress, hairstyle, taste in music, and vocabulary. Teenagers use the peer group as a yardstick of what is normal.
The school is psychologically important to adolescents as a focus of social life. Teenagers usually distribute themselves into a relatively predictable social hierarchy. They know to which groups they and others belong. A sense of school connectedness and optimal social connectedness is associated with positive outcomes for school completion, positive mood, and decreased high-risk behavior in adolescents (Bond, Butler, Thomas, and others, 2007). School connectedness is correlated with caring teachers and the absence of prejudice or discrimination from peers. A sense of school connectedness is less dependent on class size, attendance, academic preparation, and parental involvement (Maes and Lievens, 2003).
Within the larger groups are smaller, distinct, and exclusive crowds or cliques of selected close friends who are emotionally attached to one another. The selection is based on common tastes, interests, and background. Although cliques may become formalized, most remain informal and small. However, each has an identifying feature that proclaims its difference from others and its solidarity within itself, in much the same manner as the adolescent generation as a whole sets itself apart from the adult generation. Cliques are usually made up of one sex, and girls tend to be more cliquish than boys and to have a greater need for close friendships (Fig. 16-4). Within the intimacy of the group, adolescents gain support in learning about themselves, consideration for the feelings of others, and increased ego development and self-reliance.

To belong is of utmost importance; thus adolescents behave in a way that will ensure their establishment in a group. Adolescents are highly susceptible to social approval, acceptance, and demands. To be ignored or criticized by peers creates feelings of inferiority, inadequacy, and incompetence.
Best Friends.: Personal friendships of the one-on-one variety usually develop between same-sex adolescents. This relationship is closer and more stable than it is in middle childhood, and it is important in the quest for identity. A best friend is the best audience on whom to try out possible roles and identities that an adolescent wants to test. Best friends may try a role together, each providing support for the other. Each cares about what the other thinks and feels. Because a sense of intimacy grows within a permanent relationship, the stability of this same-sex friendship is an important link in the progress toward an intimate relationship in young adulthood.
Interests and Activities
Adolescents spend a large amount of time engaging in leisure-time activities. As teenagers progress through the developmental stages of adolescence, these leisure-time activities move from being family centered to being peer centered. In addition to providing teenagers with fun and enjoyment, leisure-time activities assist in the development of social, physical, and cognitive skills. Leisure-time activities also allow teenagers the opportunity to learn to set priorities and structure their time (Fig. 16-5).

Today, many adolescents must learn to juggle their time between school, activities, and the responsibilities of a job. Adolescent work experiences provide many benefits, including time management, teamwork skills, and increased income. However, many jobs available to teenagers do not provide opportunities to apply the skills they learn in school, and jobs often have high demands for quick work with low rewards. Few apprentice opportunities are available for teenagers. It is generally recommended that adolescents limit their work to no more than 20 hours per week during the school year.
ADOLESCENT SEXUALITY
Sexual activity rates have been decreasing for teens since the 1990s, including a decline in the rate among early adolescents (Santelli, Lindberg, Finer, and others, 2007). Among teenagers who have initiated sexual intercourse at an age younger than 14 years, the incidence of sexual abuse is high. In 2002 about half of all teenagers had had sexual intercourse at least once (Abma, Martinez, Mosher, and others, 2004). Teens engage in a wide range of sexual activity, including kissing and petting (fondling), oral sex, and vaginal and rectal sex. Data indicate that adolescents are engaging in sexual activity such as oral sex and delaying vaginal intercourse (Mosher, Chandra, and Jones, 2005); whether this is intended to preserve female virginity or to presumably avoid sexually transmitted disease or pregnancy is not known.
Adolescence represents a critical time in the development of sexuality. Hormonal, physical, cognitive, and social changes that occur during adolescence all have an impact on sexual development. Of all the developmental changes that affect adolescent sexuality, none is more obvious than the impact of puberty. Adolescents must come to terms with hormonal influences, physiologic manifestations such as menstruation and ejaculation, and physical changes such as breast and genital development. All these changes have a profound impact on the way teenagers perceive their bodies (i.e., body image). In addition to transitions in body image, increasing levels of pubertal hormones contribute to increased levels of sexual motivation among both boys and girls.
Changes in sexual motivations and feelings, happening at the same time as shifts in cognitive skills, contribute to painful conjectures (“Is what I’m feeling normal?”), self-conscious concern (“Am I good-looking enough?”), and hypothetical thinking (“What if she wants to have sex?”). The emergence of formal operational thinking also increases adolescents’ decision-making capabilities concerning sexual issues. As they mature, teenagers become better able to think through potential risks and benefits of sexual behaviors before they engage in any behavior. Older adolescents may also be able to conceptualize more long-term consequences of present behaviors. One of the important tasks of adolescence is to incorporate sexuality successfully into close, intimate relationships. This task is made possible by the advanced cognitive abilities that emerge over the course of adolescence.
Part of adolescent identity formation involves the development of sexual identity. As they begin to integrate changes involved with puberty, young adolescents also develop emotional and social identities separate from their family’s. For young adolescents, the process of sexual identity development usually involves forming close friendships with same-sex peers, with whom they may experiment sexually, often to satisfy curiosity. Sexual activity among young teenagers varies by gender. Masturbation provides an opportunity for sexual self-exploration; participation in this behavior is influenced by learned cultural attitudes and sex-role expectations.
Many teenagers begin to make a shift from relationships with same-sex peers to intimate relationships with members of the opposite sex during middle adolescence (Fig. 16-6). Opposite-sex relationships typically begin with peer activities involving both boys and girls. Pairing off as couples becomes more common as middle adolescence progresses. The type and degree of seriousness of partner relationships vary. Initial relationships are usually noncommittal, extremely mobile, and seldom characterized by any deep romantic attachments. Sexual activity becomes more common during middle adolescence. The relationship between love and sexual expression is brought into focus during middle adolescence. Most young people oppose exploitation, pressure, or force in sex as well as sex solely for the sake of physical enjoyment without a personal relationship. Adolescents find it hard to believe that sex can exist without love; therefore they view each relationship as real love.

An integrated sexual identity often emerges during late adolescence as individuals incorporate sexual experiences, feelings, and knowledge. For most, this identity is consistent with their own physical and mental capacities and with societal limits and expectations. Most older adolescents identify themselves as being predominantly heterosexual or bisexual, with a smaller number self-identifying as homosexual and an even smaller group still unsure of their sexual orientation, although this varies somewhat by ethnicity (Saewyc, Bearinger, Heinz, and others, 1998; Russell, Seif, and Truong, 2001). Whatever their sexual orientation, most older teenagers possess the capacity to have intimate relationships that satisfy the emotional and sexual needs of both partners.
Sexual orientation is an important aspect of sexual identity. Sexual orientation is defined as a pattern of sexual arousal or romantic attraction toward persons of the opposite gender (heterosexual), of the same gender (homosexual, often called gay or lesbian), or of both genders (bisexual). Sexual orientation encompasses several dimensions, including attraction, fantasy, actual sexual behavior, and self-labeling or group affiliation. In individuals the direction and intensity of each dimension are not necessarily consistent with any of the others. For example, individuals may be attracted most strongly to their same gender, fantasize about both genders, have sexual activity only with the opposite gender, and identify as gay or lesbian. Other individuals may engage in same-gender sexual behavior, fantasize about both genders, but identify as heterosexual. As with all aspects of sexual identity, the dimensions of sexual orientation are influenced by cultural meaning and expectation, by gender, by peer groups, and by other environmental contexts.
Adolescence is the period during which individuals commonly begin to identify their sexual orientation as part of their developing sexual identity. However, this identification process can be profoundly influenced by cultural beliefs and values, by societal and family pressures, or by a lack of similar peers. The majority of adolescents eventually report an orientation toward exclusively heterosexual relationships. For adolescents whose orientation encompasses any same-gender dimensions, the identity process during adolescence can be complicated, especially when community norms disapprove of orientations other than heterosexual. Adolescents who have witnessed harassment or violence directed at gay, lesbian, and bisexual people, for example, may be reluctant to self-identify, even when their attractions and behaviors are exclusively same-gender or bisexual.
The development of sexual orientation as part of sexual identity includes several developmental milestones during late childhood and throughout adolescence. These milestones do not necessarily occur in the same order for everyone, nor are they completed in the same amount of time. They include (1) the realization of romantic or erotic attraction to people of one (or both) genders; (2) erotic daydreaming about one or both genders; (3) romantic partners or dates without sexual activity; (4) sexual activity with people of the preferred gender or genders (also, for some teens, sexual activity with a nonpreferred gender, out of curiosity or through social pressure); (5) self-identification of the orientation that best fits one’s current circumstances and understanding; (6) publicly self-identifying that orientation, usually to intimate friends and family first, then the wider social group; and (7) an intimate, committed sexual relationship with a person of the gender appropriate to one’s orientation.
Discussing Sexual Orientation with Adolescents
John, a 17-year-old adolescent, comes into the school-based clinic and tells the nurse practitioner that he thinks he is homosexual. What is the most appropriate response for the nurse practitioner?
1. Evidence—Is there sufficient evidence to draw any conclusions about John’s sexual orientation at this time?
2. Assumptions—Describe an underlying assumption about each of the following issues:
3. What implications and priorities for nursing care can be drawn at this time?
4. Does the evidence support your argument (conclusion)?
5. Are there alternative perspectives to your arguments? What are they?
There is no evidence that gay, lesbian, or bisexual adults are more or less likely to create long-term, stable relationships than are heterosexual couples. It should be noted that bisexual adolescents and adults do not generally engage in sexual relationships with both genders concurrently; self-identification as bisexual usually refers to the ability to be attracted to either gender but does not imply that such a person requires partners of both genders, or that one must be equally attracted to and have sexual experience with both genders in order to be bisexual.
Although the order of these milestones varies greatly among adolescents, adolescents who identify as gay, lesbian, or bisexual tend to publicly self-identify later than heterosexual peers. Without positive gay, lesbian, or bisexual role models or a supportive peer group, sexual-minority teens can feel isolated, and they may not share their orientation with anyone for fear of rejection or violence. (See Critical Thinking Exercise.) When adolescents who would otherwise identify as bisexual can only find a peer group of gay and lesbian teens, they may focus on their same-gender dimensions of orientation and adopt the label of lesbian or gay; later, they may self-label as bisexual. Likewise, some gay and lesbian adolescents may first identify as heterosexual, then bisexual, before identifying as gay or lesbian.
DEVELOPMENT OF SELF-CONCEPT AND BODY IMAGE
The sudden growth that takes place in early adolescence creates feelings of confusion for adolescents. They have lost the security of a familiar body and feel uncomfortable with their altered body. Consequently, they may try to either hide their body or advertise it, or they may alternate between the two extremes. Teenagers are acutely aware of their appearance as they begin to acquire images of themselves as adults, but they see discrepancies between their ideal and actual skills and abilities.
Adolescents are continually comparing themselves with their peers and making judgments about their own normality based on these observations. Pubertal children feel most comfortable when they are just like their friends and age-mates. Perceived defects or deviations from the group average are threatening to their idealized image. Any blemish is likely to be magnified out of proportion, and any delay of the visible evidence of maturity is cause for worry. Unfortunately, this is also the time when the hormonal effect of the sebaceous glands produces acne, which creates problems for many adolescents. To the adolescent, even the most insignificant pimple may be viewed as a gross disfigurement. The advent of chronic disease or a permanent physical disability has special significance during adolescence and creates additional stresses for both adolescents with the condition and health care providers.
Experts have determined that the body image established during adolescence is the one that individuals retain throughout life. Much of adolescents’ search for identity takes place before a mirror as they try to read from the reflected features just who they are and what they look like to other people. Adolescents practice facial expressions and postures, try out hair arrangements, worry about a pimple, and in other ways attempt to assess the best means to achieve a maximum effect—to reveal the “true self.”
The self-concept becomes more differentiated as adolescents acquire a more complex picture of themselves, one that takes situational factors into account. The self-concept gradually becomes more individualized and more distinct from the concepts of others. Although younger teenagers describe themselves in terms of similarities with peers, as adolescence advances, young people describe themselves in terms of their special characteristics.
Responses to Puberty
The response to the physical changes of pubertal growth and development differs depending on the stage of development. Young adolescents become preoccupied with the rapid changes in their body and are interested in the anatomy, physiology, and function of their sexual organs. Boys must also confront the sexual feelings and tensions that accompany puberty, and the appearance of nocturnal emissions may be puzzling, troublesome, or embarrassing events. Unless the boy has been prepared in advance, he may find it difficult to discuss his feelings with his parents and may turn to his friends for information and guidance. Many girls also are concerned over the rapid changes in their body. Some girls perceive the increase in weight and associated fat deposition as evidence of obesity and may indulge in fad diets. Although many girls look forward to menstruation and take this event in stride, others may find the first menstrual period a distressing and frightening event. All teenagers, regardless of gender, are concerned with the question, “Am I normal?” To answer this question, they compare their body with the bodies of their peers and with images in the media. This leads to a great deal of uncertainty about their appearance and attractiveness.
If an adolescent does not enter puberty at the same time as his or her peers, considerable inner conflict may occur. Early-maturing girls and boys have higher rates of sexual risk-taking behaviors, delinquency, and substance abuse than their on-time peers (Costello, Sung, Worthman, and others, 2007; Lynne, Graber, Nichols, and others, 2007). Nurses who work with adolescents must provide teaching and health care interventions that are appropriate for the chronologic and cognitive development of the adolescent rather than the stage of physical maturation.
As growth and development proceed through middle adolescence, the rapid body changes diminish, and the adolescent has time to try to make the body more attractive. Adolescents strive to achieve the perfect body within their own cultural norms. The “right” clothes and hairstyle become very important. By late adolescence the heightened concern with body image has ended and is replaced with a general comfort with the body.
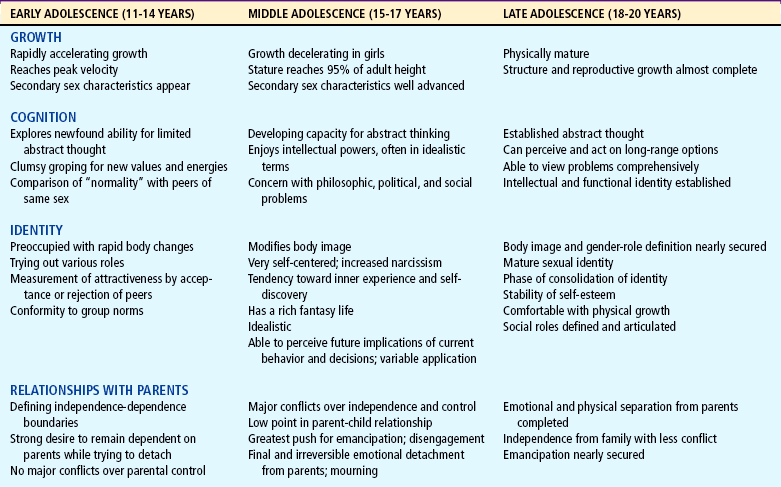
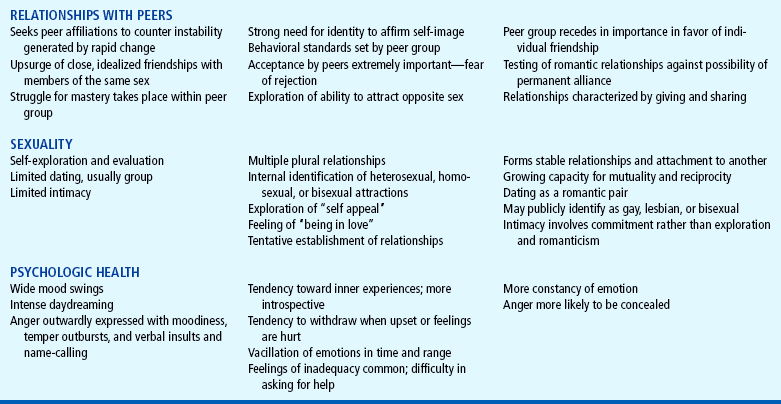
The changes that occur during the early, middle, and late phases of adolescence are summarized in Table 16-1.
PROMOTING OPTIMAL HEALTH DURING ADOLESCENCE
The major causes of morbidity and mortality in adolescence are not diseases, but health-damaging behaviors. New sources of morbidity in adolescence include injury, depression, violence, sexually transmitted diseases, and pregnancy; obesity may begin in childhood or adolescence, but the health consequences are more evident in early and middle adulthood. Health promotion for this age-group consists mainly of teaching and guidance to avoid risk-taking activities and health-damaging behaviors. Adolescence provides an opportunity for teenagers to incorporate healthy lifestyle behaviors that will benefit them not only during the teenage years, but also throughout the life span.
Effective health education for adolescents should incorporate a developmentally appropriate, multifaceted approach. Motivational interviewing has been shown to improve adherence to health care advice by using a collaborative approach (Gance-Cleveland, 2007). Education alone is not enough to change behavior. Effective programs must include opportunities to improve communication skills and enhance their social network to make more positive connections (Tuttle, Campbell-Heider, and David, 2006).
As adolescents develop, they are able to assume additional responsibility for their own health, including maintaining health practices, taking prescribed medications, keeping appointments, and performing procedures when necessary. Health professionals who work with adolescents should consider their increasing independence and responsibility while maintaining privacy and ensuring confidentiality (see Nursing Care Guidelines box and Critical Thinking Exercise). Parents should also respect their teenager’s independence and move toward the role of consultant about health issues while maintaining some level of involvement throughout adolescence.
In response to changes in adolescent morbidity and mortality, the American Medical Association (1997) developed the Guidelines for Adolescent Preventive Services (GAPS), which provide a framework for health care providers to use in their clinical practice. The following discussion provides information on specific GAPS topics and recommendations related to screening, guidance, and immunizations.
Ensure confidentiality and privacy; interview adolescent without parents.
Show concern for adolescent’s perspective: “First, I’d like to talk about your main concerns” and “I’d like to know what you think is happening.”
Offer a nonthreatening explanation for the questions you ask: “I’m going to ask a number of questions to help me better understand your health.”
Maintain objectivity; avoid assumptions, judgments, and lectures.
Ask open-ended questions when possible; move to more directive questions if necessary.
Begin with less sensitive issues and proceed to more sensitive ones.
Use language that both the adolescent and you understand. Clarify terms, such as “having sex.”
Restate: reflect back to adolescents what they have said, along with feelings that may be associated with their descriptions.
Jamie, a 17-year-old girl, arrives at the adolescent clinic with her mother, Mrs. S., for a routine history and physical examination with the nurse practitioner. As the nurse practitioner walks with Jamie to an examination room, Mrs. S. whispers to the nurse practitioner, “I need to speak with you in private.” How should the nurse practitioner respond to Mrs. S.’s request?
1. Evidence—Is there sufficient evidence to formulate a response to Jamie’s mother?
2. Assumptions—Describe an underlying assumption about each of the following topics:
a. The role of the adolescent in health care
b. The role of the parents in the health of their adolescent
3. What priorities or implications for nursing care should be established at this time?
4. Does the evidence support your conclusion?
5. Are there alternative perspectives that you should consider? What are they?
IMMUNIZATIONS
An immunization update is an important part of adolescent preventive care. Obtaining a record of the teenager’s prior immunizations is important. Adolescents 11 to 18 years of age should receive a single tetanus-diphtheria—acellular pertussis (Tdap) vaccine if they have received the recommended childhood series of DTaP immunizations. This vaccine is now recommended because of the increased incidence of pertussis seen in adolescents and adults who were immunized with the DTaP series as young children. The adolescent who has received Td but not Tdap vaccine should also receive a single dose of the Tdap vaccine provided 5 years have elapsed between the Td and Tdap vaccination (American Academy of Pediatrics, 2006). Meningococcal vaccine (MCV4) should be given to adolescents 11 to 12 years of age or at 15 years of age if previous immunization with MPSV4 occurred in childhood and at least 3 to 5 years have passed since primary immunization. The MCV4 vaccine is now preferred over the MPSV4 vaccine (American Academy of Pediatrics, 2008).
The human papillomavirus (HPV) vaccine series is recommended only for girls based on research results at this time. Additional recommendations may be made for boys if it is determined to be safe and effective. The series may be started as early as 9 years of age, with the second and third doses at 2 months and 6 months, respectively.
With the exception of pregnant teenagers, all adolescents should receive a second measles-mumps-rubella (MMR) vaccine unless they have documentation of two MMR vaccinations during childhood.
All adolescents who have not previously received three doses of hepatitis B vaccine should be vaccinated against hepatitis B virus. The hepatitis A vaccine should be given to all adolescents as part of the routine immunization schedule; the two-dose series may be completed in childhood, and a catch-up schedule for those who have not been previously immunized is recommended. Annual influenza vaccination with either the live attenuated influenza vaccine or trivalent influenza vaccine is now encouraged for all children and adolescents. All adolescents should also be assessed for previous history of varicella infection or vaccination. Vaccination with the varicella vaccine is recommended for those with no previous history; for those with no previous infection or history, the varicella vaccine may be given in two doses 4 or more weeks apart to adolescents 13 years or older (American Academy of Pediatrics, 2008). (See also Immunizations, Chapter 10.)
NUTRITION
The rapid and extensive increase in height, weight, muscle mass, and sexual maturity of adolescence is accompanied by increased nutritional requirements. Because nutritional needs are closely related to the increase in body mass, the peak requirements occur in the years of maximum growth, during which the body mass almost doubles. The caloric and protein requirements during this time are higher than at almost any other time of life. As a result of this increased anabolic need, the adolescent is highly sensitive to caloric restrictions.
Current guidelines for caloric intake are provided by a number of sources. The Dietary Reference Intakes (DRIs) provide age-specific guidelines for nutrients (see Chapter 6). Another guideline, which was recently developed by the American Heart Association (2005), aims at promoting balanced nutrient intake in children and adolescents with an overall decrease in fat intake and discretionary calories or snacks that increase the propensity for obesity and cardiovascular disease. Caloric intake can be tailored to meet the adolescent’s increased growth needs as well as activity level such as involvement in sports. The guidelines also encourage limiting sweetened beverage consumption and moderating caloric intake to activity levels.
Adolescents usually have sufficient intake of protein to meet their needs, except for those who limit their food intake because of economic problems or in an attempt to lose weight. There is a substantial increase in the need for the minerals calcium, iron, and zinc during periods of rapid growth: calcium for skeletal growth, iron for expansion of muscle mass and blood volume, and zinc for the generation of both skeletal and bone tissue. Girls with heavy or frequent menses may be especially susceptible to iron deficiency resulting from blood loss. Calcium intake from food sources is essential during adolescence to assist in the prevention of osteoporosis. Eventual bone mass is a balance between the amount of bone laid down during adolescence and the amount later lost with aging. Overall, osteoporosis is a result of polygenic and multiple environmental factors such as nutrition, economics, and exercise (Ongphiphadhanakul, 2007). Dietary intervention should promote the regular consumption of breakfast and a balanced intake of a variety of foods.
Eating Habits and Behavior
Eating and attitudes toward food are primarily family centered during early and middle childhood, and food habits are largely related to cultural and individual family preferences and patterns. With adolescence and the move toward independence, family influences on the child diminish. Children’s interests, attitudes, and routines are altered as an increasing number of meals are eaten away from home. These changes are largely a result of the high value that teenagers place on peer acceptability and sociability. Their peers easily influence their eating habits.
Pressure for time and commitments to activities adversely affect the teenager’s eating habits. Omitting breakfast or eating a breakfast that is nutritionally poor in quality is frequently a problem. Snacks, usually selected on the basis of accessibility rather than nutritional merit, become more and more a part of the habitual eating pattern during adolescence (Fig. 16-7). Excess intake of calories, sugar, fat, cholesterol, and sodium is common among adolescents and is found in all income and racial or ethnic groups and both genders. Inadequate intake of certain vitamins (folic acid, vitamin B6, vitamin A) and minerals (iron, calcium, zinc) is also evident, particularly among girls and teenagers of low socioeconomic status. In combination with other factors, these dietary patterns could result in increased risk for obesity and chronic diseases such as heart disease, osteoporosis, and some types of cancer later in life. Girls, in particular, may be susceptible to iron deficiency at menarche. Maximum bone mass is also acquired during adolescence; therefore the calcium deposited during these years determines the risk of osteoporosis. Milk is usually passed over in favor of soft drinks.
Overeating or undereating during adolescence presents special problems. When they experience the normal increase in weight and fat deposition of the growth spurt, teenage girls often resort to dieting. The desire for a slim figure and a fear of becoming “fat” prompt teenage girls to embark on nutritionally inadequate reducing regimens that drain their energy and deprive their growing bodies of essential nutrients. They resort to diets on their own or with peers in an effort to conform. Many adopt current fad diets and are victims of food misinformation. Boys are less inclined to undereat. They are more concerned about gaining size and strength. However, they tend to eat foods high in calories but low in other essential nutrients.
Obesity is increasing among both children and adolescents in the United States. The obesity currently seen is not a result of metabolic disturbances, but of poor dietary habits and increasingly sedentary lifestyles. Childhood obesity often results in obesity in adulthood. Adolescent obesity poses both immediate and long-term problems for adolescents. Obesity is directly linked to the development of cardiovascular disease and other chronic illnesses such as diabetes. Anorexia nervosa and bulimia nervosa also commonly occur during the adolescent and young adult years. If left untreated, these disorders, like obesity, can lead to considerable morbidity and mortality. The past two decades have revealed an increase in the overall portion size of foods. The largest portions for most foods are found at fast-food restaurants. However, portion sizes for desserts and hamburgers are the largest at home (Nielsen and Popkin, 2003). Lifestyle changes necessary for adolescents to lose weight require the involvement of family members who provide support and encourage active participation.
Nursing Care Management
Adolescents should receive at a minimum an annual assessment of weight, height, and BMI for age, plotted on a standard growth chart. Healthy dietary habits should be discussed with all adolescents. The frequency of eating at fast-food and other restaurants, consumption of sweetened beverages, and consumption of excessive portion sizes should be identified. In addition to food intake, the nurse should assess the level of physical activity and sedentary behaviors. Readiness to change; environmental supports and barriers; and family history of diabetes, heart disease, and early stroke must be considered when planning nutritional education and guidance. Nurses in the school setting can assist in advocating for comprehensive nutritional services for preschool through grade 12 students. Comprehensive nutrition education with access to nutritious meals and snacks and physical activity at school will begin to reverse the trend of childhood obesity (Briggs, Safaii, and Beall, 2003).
To help teenagers select a nutritious diet, it is best to begin with their present diet and actively involve them in the process. Adolescents do not respond well to judgmental attitudes and dislike lectures, but they do respond when their independence is respected and they are given the opportunity to make their own decisions regarding food choices.
In general, adolescents are body conscious and concerned about their appearance. Concrete messages about the relationship between an attractive appearance and the benefits of a healthy lifestyle are most effective. However, helping young persons arrive at a decision for change is more difficult than providing information. They respond best when the counselor provides straightforward information, uses instructional methods that actively involve them, talks with them and not at them, and listens to what they have to say.
SLEEP AND REST
Teenagers vary in their need for sleep and rest. Rapid physical growth, the tendency toward overexertion, and the overall increased activity of this age contribute to fatigue in adolescents. During growth spurts the need for sleep is increased. Their propensity for staying up late makes it difficult to arise in the morning, and they may sleep late at every opportunity. Adequate sleep and rest at this time are important to a total health regimen.
EXERCISE AND ACTIVITY
Although today’s youth are less fit than children 20 years ago, adolescents probably spend more time and energy practicing and participating in sports activities than members of any other age-group. Many adolescents participate in sports within school settings (Fig. 16-8). School-based, health-oriented physical education may provide both immediate effects of the activity and sustained effects through encouragement of lifelong activity patterns. High schools continue to cut physical education classes, with only half of high school students attending physical education classes in 2005. Less than half of students attended these classes daily, and the majority of classes included only 20 minutes of exercise (Centers for Disease Control and Prevention, 2006a). To improve health outcomes, school-age children and adolescents should engage in 60 minutes or more of moderate to vigorous physical activity daily (Strong, Malina, Blimkie, and others, 2005).

FIG. 16-8 Adolescents should be encouraged to participate in activities that contribute to lifelong physical fitness.
The practice of sports, games, and even dancing contributes significantly to growth and development, the education process, and better health. These activities provide exercise for growing muscles, interactions with peers, and a socially acceptable means of enjoying stimulation and conflict. In addition, competitive activities help the teenager in the process of self-appraisal and the development of self-respect and concern for others. Because physical fitness appears to be a major influence on one’s lifelong health status, children should be encouraged to participate in activities that contribute to lifelong physical fitness. Nurses can encourage participation as a way to promote health and build self-esteem. However, adolescents should not be encouraged to engage in physical activities that are beyond their physical or emotional capacity (see Health Problems Related to Sports Participation, Chapter 17).
DENTAL HEALTH
Dental health should not be neglected during adolescence, although the rate of caries formation is not as great as in childhood. Dental care is an aspect of preventive care that is not received by substantial proportions of children in the United States. Pit and fissure sealants are a safe and effective technique for dental caries prevention. Early adolescence is usually when corrective orthodontic appliances are worn, and these are frequently a source of embarrassment and concern to the youngster. Reassurance regarding the temporary nature of the annoyance and anticipation of an improved appearance help adolescents tolerate the inconvenience. It is also important to reinforce the orthodontist’s directions regarding use and care of the appliances and to emphasize careful attention to toothbrushing during this time (see also Chapters 12 and 15).
PERSONAL CARE
The body-conscious teenager is highly amenable to discussion and counseling about personal care and hygiene. Body changes associated with puberty bring special needs for cleanliness. The hyperactive sebaceous glands and newly functioning apocrine glands make frequent bathing or showering a necessity, and underarm deodorants assume an important place in personal care. The adolescent discovers that hair requires more frequent shampooing, and girls often have questions about hair removal, use of cosmetics, and menstrual hygiene. Peer group discussions center on the advantages of particular products or methods. Adolescents are continually bombarded with messages from the media regarding the best way to enhance their popularity and attractiveness. Nurses are in a position to help them evaluate the relative merits of commercial products.
Vision
Regular vision testing is an important part of health care and supervision during adolescence. During adolescence, visual refractive difficulties reach a peak that is not exceeded until the fifth decade of life. The increased demands of schoolwork make adequate vision essential for academic success. Consequently, teenagers are more likely to be referred for visual evaluation. The need for corrective lenses can create psychologic problems for teenagers if they believe that glasses spoil their appearance or do not fit their body image. Contact lenses may be a preferred solution; a variety of lenses are now available at fairly reasonable prices. For some, the impact of a visual defect, no matter how slight, may be stressful.
Hearing
Considerable concern has focused on current teenage practices that cause hearing damage. Cochlear damage from relatively continuous exposure to the loud sound levels of rock music has been documented. The popularity of personal music players with lightweight earphones that are inserted into the ear canal is of particular concern to health care professionals. When these units are used for extended periods, permanent hearing loss can occur. Although appeals for more judicious use are not always successful, teenagers should be informed of the risk. Efforts directed toward legislating legal limits to the noise exposure that can be achieved through the sets may be another possible solution. (See Chapter 19 for a discussion of noise-related hearing loss.)
Posture
Many adolescents demonstrate altered posture. Rapid skeletal growth is often associated with slower muscular growth, and as a result, some teenagers may appear awkward or slump and fail to stand or sit upright. However, some postural defects of adolescence require early medical intervention. Scoliosis is a defect of the spine that occurs frequently in adolescence and is more common in girls than in boys (see Idiopathic Scoliosis, Chapter 31). The majority of the cases are idiopathic, and the defect manifests as a painless curvature of the spine. Fortunately, most of these spinal curvatures will not require treatment. However, because there is no way to predict which curvatures will progress, all curvatures of the spine should be referred for further evaluation.
Body Art
Body art (piercing and tattooing) is an aspect of adolescent identity formation. The skin has become the latest source of parent-adolescent conflict. The adolescent often seeks body art as an expression of his or her personal identity and style. Tattoos may mark significant life events such as new relationships, births, and deaths. Piercing the ear, nose, nipple, eyebrow, navel, penis, or tongue may sometimes create a health problem. It is a nursing responsibility to caution girls and boys against having piercing performed by friends, parents, or themselves. Although in most cases piercings have few if any serious side effects, there is always a danger of complications such as infection, cyst or keloid formation, bleeding, dermatitis, or metal allergy. Using the same unsterilized needle to pierce body parts of multiple teenagers presents the same risk of human immunodeficiency virus (HIV), hepatitis C, and hepatitis B virus transmission as occurs with other needle-sharing activities.
A qualified operator using proper sterile technique should perform the procedure. This is especially important if a youngster has a history of diabetes, allergies, or skin disorders. Adolescents should be informed about the approximate time for healing after body piercing and the care of the pierced area during and after healing. Some body sites need extra precautions. For example, cartilage (ear, nose) has a poor blood supply and heals slowly and scars easily; nipple piercing puts the adolescent at risk for breast abscess. Finally, migration of the piercing is common with naval and other flat skin surface piercing. Piercing guns should not be used for piercing anything other than the earlobe because guns place the piercing too deeply.
It is estimated that 3% to 5% of people in Western society have a tattoo and that 13% of the population in the United States has at least one tattoo. Studies of distinct populations of young adults and adolescents report body art rates as high as 23% (Braverman, 2006). Professionals as well as amateur artists administer tattoos. The risk to the adolescent receiving a tattoo is low. The greatest risk is for the tattoo artist who comes in contact with the client’s blood. Adolescents who are amateur tattoo artists benefit from discussions about standard precautions and the hepatitis B vaccination. Many states either have no regulations or do not enforce existing regulations of piercing and tattooing facilities. The local health department is a source of information about local regulatory requirements. The Centers for Disease Control and Prevention has an excellent website that outlines safety concerns for persons performing and receiving body art. *
Tanning
The quest for an attractive appearance leads many teenagers to excessive sunbathing and artificial means for tanning. However, this practice has serious long-term risks, and the adolescent should be educated regarding the detrimental effects of sunlight on the skin (see Sunburn, Chapter 30). Long-term effects include premature aging of the skin, increased risk of skin cancer, and, in susceptible individuals, phototoxic reactions.
The increasing popularity of artificial tanning has prompted concern from health professionals regarding the use of sunlamps and tanning machines. The long-term effects of tanning machines are similar to those of the sun; dermatologists do not recommend suntanning by this means. Those who insist on using tanning equipment should be warned that goggles must be worn in tanning booths to prevent serious corneal burning. Education on the use of sunscreens, including hypoallergenic products, with a sun protective factor (SPF) of at least 15 and a nonalcohol base without lanolin, parabens, or fragrance, is important. Broad-spectrum sunscreens that protect against both ultraviolet A and B (UV-A and UV-B) are the most effective. Self-tanning creams safely stimulate the appearance of a tan; however, teens using these products should be cautioned that sun protection is still required. Targeting health education messages to adolescents and incorporating educational components relating to sun protection behaviors in school health curricula and in health care visits will increase adolescent knowledge and awareness.
STRESS REDUCTION
The multiple changes occurring in adolescence can result in great stress (Fig. 16-9 and Box 16-2). Adolescents are faced with pressures from peers that often involve taking serious health risks, including pressures for sexual experimentation; use of drugs, alcohol, and cigarettes; and potentially dangerous physical activities.

FIG. 16-9 Adolescents use being alone as a method of coping with stress. Health care professionals need to assess whether this indicates clinical depression.
Early-maturing girls and late-maturing children are especially sensitive to the stresses of being different from their peers. Many feel intense anxiety over their identity. Both early- and late-maturing children feel out of place among their classmates, but slow-maturing children appear to suffer the most pronounced inner turmoil and may be hesitant to voice their concerns. Slow-maturing adolescents need support and reassurance that they are not abnormal and need only be patient until the time comes when they, too, will mature physically.
SEXUALITY EDUCATION AND GUIDANCE
Contemporary adolescents are constantly exposed to sexual symbolism and erotic stimulation from the mass media. At the same time, the development of primary and secondary sex characteristics and the increased sensitivity of the genitalia produce thoughts and fantasies about sexual relationships. Sexual aspects of interpersonal relationships become particularly important. Societal expectations push adolescents toward dating, and their own inner sex drive urges them toward exploration.
Our society continues to do a poor job of educating adolescents about pubertal growth and development. Omar, McElderry, and Zakharia (2003) found that 36% of boys and 2% of girls had never been spoken to about pubertal development or sexuality issues. Girls received education at a mean age of 13 years and boys at an average age of 15 years. A large portion of their knowledge relating to sex is acquired from peers, television, movies, and magazines. In addition, some information obtained from their parents may be inaccurate. As a result, the information they accumulate may be incomplete, inaccurate, riddled with cultural and moral judgments, and not very helpful.
The responsibility for providing sexuality education has been assumed by parents, schools, churches, community agencies such as Planned Parenthood Federation of America, Inc.,* and health professionals, especially nurses. Many adolescents perceive nurses, especially school nurses, as individuals who possess important information and who are willing to discuss sex with them. To be able to discuss the topic adequately, nurses must have not only an understanding of the physiologic aspects of sexuality and a knowledge of cultural and societal values, but also an awareness of their own attitudes, feelings, and biases about sexuality.
Comprehensive information about sexuality education is offered by the Sexuality Information and Education Council of the United States (SIECUS)† and the Sex Information and Education Council of Canada.‡ SIECUS maintains that every sexuality education program should present the topic from six aspects: biologic, social, health, personal adjustments and attitudes, interpersonal associations, and the establishment of values.
Whether nurses counsel young people on an individual basis, in mixed groups, or in groups segregated by gender makes little difference. Ideally, boys and girls should be able to discuss sexuality objectively with one another and in groups, but this is not always possible. The differences in the rate of maturation between boys and girls and between different members of the same sex often make it desirable to discuss certain aspects of sexuality in segregated groups. As a rule, the need for separate discussion groups diminishes as young people mature.
Sexuality education should consist of instruction concerning normal body functions and should be presented in a straightforward manner using correct terminology. When discussing sex and sexual activities, nurses should use simple but correct language, not street language, highly scientific terminology, or evasive jargon. Once they understand the meaning of biologic terms such as uterus, testicles, and vagina, most teenagers prefer to use them in their discussions.
Many girls arrive at menarche with ambivalent attitudes, myths, and illogical beliefs. Even girls adequately prepared for menstruation do not always understand its relationship to the total process of reproduction. Many are under the incorrect impression that the “safe” time for sexual intercourse is midway between menstrual periods.
Teenagers’ curiosity and desire for information extend beyond the need for anatomic and physiologic knowledge. They need to know more than the mechanics of conception, pregnancy, and birth. Adolescents, girls in particular, want answers to questions such as “What is it like?” “Does it hurt?” “What happens when … ?” and “Is it all right if you … ?” Boys are often concerned about the fallacy that a relationship exists between penis size and sexual function. They need reassurance that masturbation is a normal and common practice, that some degree of homosexuality in early adolescence is not unusual, and that oral-genital relations can be normal substitutes for intercourse.
Teenagers need to discuss intercourse, alternative methods of sexual satisfaction, and how to resist peer pressure. With the increased incidence of sexually transmitted diseases, especially HIV infection, the topic of “safe sex,” especially abstinence or the use of condoms, is essential. Role-playing can help teenagers learn effective approaches to dealing with difficult situations. Sex and sexuality cannot be taught without discussions of mature decision making, sexual responsibility, and values clarification. Adolescents may receive inaccurate and ambiguous messages regarding sexual behavior; for example, an adolescent may be told that abstinence from vaginal intercourse will prevent transmission of a sexually transmitted disease. Accurate and unbiased information regarding sexual practices should be provided in a setting wherein the adolescent feels comfortable asking questions without being degraded or made to feel uncomfortable for seeking information.
Adolescents need role models and life experiences with delayed gratification. Most important, they need problem-solving experience and decision-making skills so that they can anticipate the positive and negative outcomes of a decision. With this type of assistance, teenagers can become sexually responsible young adults.
INJURY PREVENTION
Physical injuries are the greatest single cause of death in the adolescent age-group and claim more lives than all other causes combined. The most vulnerable ages are the years 15 to 24, when accidental injuries account for about 60% of deaths in boys and 40% of deaths in girls. These figures remain fairly constant from year to year and are significant because almost all fatal injuries are preventable.
During adolescence, peak physical, sensory, and psychomotor function gives teenagers a feeling of strength and confidence that they have never experienced before, and the physiologic changes of puberty give impetus to many basic instinctual forces. One manifestation of this is an increase in energy that simply must be discharged through action, often at the expense of logical thinking and other control mechanisms. Their propensity for risk-taking behavior plus feelings of indestructibility makes adolescents especially prone to injuries. Some of the developmental characteristics of teenagers and injury prevention suggestions are outlined in Box 16-3.
BOX 16-3 Injury Prevention During Adolescence
DEVELOPMENTAL ABILITIES RELATED TO RISK OF INJURY
Need for independence and freedom
Age permitted to drive a motor vehicle (varies from state to state)
Need for discharging energy, often at expense of logical thinking and other control mechanisms
Peak incidence for practice and participation in sports
Pedestrian—Emphasize and encourage safe pedestrian behavior.
Passenger—Promote appropriate behavior while riding in a motor vehicle. Refuse to ride with an impaired person or one who is driving recklessly.
Driver—Provide competent driver education; encourage judicious use of vehicle; discourage drag racing or “playing chicken”; maintain vehicle in proper condition (brakes, tires, etc.).
Teach and promote safety and maintenance of two- and three-wheeled vehicles.
Promote and encourage wearing of safety apparel such as helmet, long trousers.
Reinforce the dangers of drugs, including alcohol, when operating a motor vehicle.
Promote acquisition of proper instruction in sports and use of sports equipment.
Instruct in safe use of and respect for firearms and other devices with potential danger (e.g., power tools, firecrackers).
Provide and encourage use of protective equipment when using potentially hazardous devices.
Promote access to or provision of safe sports and recreational facilities.
Be alert for signs of depression (potential suicide).
Discourage use of hazardous sports equipment (e.g., trampoline, surfboards).
Instruct regarding proper use of corrective devices (e.g., glasses, contact lenses, hearing aids).
Encourage and foster judicious application of safety principles and prevention.
Motor Vehicle—Related Injuries
The adolescent’s newly acquired ability to drive and the normal developmental need for independence and freedom make the automobile an attractive part of an adolescent’s life. Thirty-six percent of all teen deaths in the United States are the result of motor vehicle crashes (Centers for Disease Control and Prevention, 2006b). Many factors contribute to the higher rate of crashes among teen drivers, including lacking driving experience and maturity, following too closely, driving too fast, having other teen passengers in the car, and using alcohol (Williams and Ferguson, 2002). Because of the significant increase in the number of accidents when adolescents drive at night, many states have effectively enacted driving curfews, decreasing fatal crashes by 38% and crashes involving injury by 40% for adolescents (Baker, Chen, and Li, 2007).
Nurses should educate teenagers and their parents about the risk of driving while drinking alcohol or of riding in an automobile with a drunk driver. Many families arrange a no-questions-asked ride home to prevent an adolescent from riding with a drunk driver. Families should also require adolescents to log several hours of supervised practice driving before taking the car out alone. The major risk for death in a motor vehicle accident is failure to use a safety restraint. Teenage seatbelt use, especially among boys, is lower than adult seat belt use. Belt use as a passenger is low for adolescents even when the driver is an adult. Continued efforts to ensure teenage seat belt use should be focused at the individual educational level and through tough enforcement laws (Williams, McCartt, and Geary, 2003).
Other Vehicle Injuries.: The increasing use of motorcycles, all-terrain vehicles (ATVs), jet skis, and snowmobiles has caused an increase in injuries among young people who are below the legal age for driving automobiles. Many adolescents ride bicycles without helmets and without lights at night, and the overwhelming majority of deaths from bicycle injuries (primarily head injuries) involve teenagers.
Firearms
Firearms are the major cause of intentional fatal injuries in the United States. Adolescence is the peak age for being either a victim or an offender in an injury involving a firearm. Gun carrying among adolescents is on the rise and is not limited to the stereotypic inner-city youth. Family members and acquaintances are a common source of guns for young people. Gun availability in the home is strongly linked to unintentional death and injury to children (Glatt, 2005). In addition, the presence of a gun in the home increases the risk of adolescent suicide and homicide. All families should be assessed for the presence of a gun in the home and informed of this risk. They must take preventive action to ensure that the guns are never loaded, that they are locked up in a safe place, and that ammunition is stored and locked up separately in a location accessible only to appropriate adults.
Nonpowder Firearms.: Guns that do not use powder (e.g., air rifles, BB guns), although viewed as toys by many, account for almost as many injuries as powder guns. The regulations regarding nonpowder guns are relaxed; they can be purchased legally by adolescents and are labeled as suitable for children as young as 8 years of age. Few states regulate their use. Nurses should act as child advocates and urge passage of laws to regulate the sale of these potentially dangerous “toys.”
Sports Injuries
Because the degree of physical maturation, size, coordination, and endurance varies greatly among adolescents of the same age, sports competition between young people who differ greatly in strength and agility is unfair and hazardous. Matching candidates for sports should be done relative to physical maturity, height, weight, and physical fitness and skills, particularly in a sport involving rigorous body contact. Age is a less important consideration.
Every sport has some potential for injury, whether one participates in serious competition or engages in the activity for pure enjoyment. Overuse injuries are common in adolescents and result in more time missed from the activity than fractures. A large number of severe or fatal injuries occur to youths who are not physically prepared for the activity. The increase in strength and vigor in adolescence may tempt adolescents to overextend themselves, especially boys who are urged on by teammates or are stimulated by the admiration of female observers. Injuries sustained in sports or recreational activities can involve any part of the body and range from relatively minor cuts, bruises, and abrasions to totally incapacitating central nervous system injuries or death. The leading cause of serious sports injuries among boys is participation in football, whereas most girls are injured while participating in gymnastics.
Nursing Care Management
Injury prevention is an ongoing part of nursing responsibility throughout the childhood years. Anticipatory guidance to parents and children regarding the expected problems and hazards related to growth and development does not end as children approach maturity. They need education in basic safety precautions, instruction in skills required in the performance of activities such as sports, instruction in handling motor vehicles, and information about using proper protective equipment and properly maintaining equipment. During adolescence, however, health and safety education and guidance are more effective when the young people are involved directly. Parents and health professionals can emphasize the importance of safety during performance of activities and the proper conditioning and preparation for sports.
Prevention can occur on a variety of levels. Safety advocacy, public policy changes, and legislation can curtail injuries. Examples of such approaches are laws that mandate wearing seat belts, using helmets while driving moving vehicles other than automobiles, keeping the legal drinking age at 21 years, and instituting curfews for teen drivers. In addition to improvements in the environment, health education for teenagers and significant adults is essential. Helping adolescents understand their need for engaging in risky behavior, exploring possible negative outcomes, and weighing possible alternatives are critical components of injury prevention.
ANTICIPATORY GUIDANCE—CARE OF FAMILIES
Both adolescents and their parents are often confused and perplexed about the changes and behavior of this stage of development. Parents need support and guidance to help them through this trying time. They need to understand the changes taking place and to accept the expected behaviors that accompany the process of detachment. Parents may need help to “let go” and to promote the changed relationship from one of dependence to one of mutuality (see Family-Centered Care and Family Focus boxes).
 FAMILY-CENTERED CARE
FAMILY-CENTERED CAREAccept adolescent as a unique individual.
Respect adolescent’s ideas, likes and dislikes, and wishes.
Be involved with school functions and attend adolescent’s performances, whether it be a sporting event or a school play.
Listen and try to be open to teenager’s views, even when they disagree with parental views.
Avoid criticism about no-win topics.
Provide opportunity for choosing options and accept natural consequences of these choices.
Allow young persons to learn by doing, even when choices and methods differ from those of adults.
Provide adolescent with clear, reasonable limits.
Clarify house rules and consequences for breaking them. Adhere to the rules (even though it hurts!!).
Let society’s rules and consequences teach responsibility outside the home.
Allow increasing independence within limitations of safety and well-being.
Be available but avoid pressing teenager too far.
Try to share adolescent’s feelings of joy or sorrow.
Respond to feelings, as well as words.
Be available to answer questions, give information, and provide companionship.
Try to make communication clear.
Avoid comparisons with siblings.
Assist adolescent in selecting appropriate career goals and preparing for adult role.
Welcome adolescent’s friends into the home and treat them with respect.
U.S. society does little to help adolescents mature and separate. Americans have remarkably few rites of passage that mark the stages of life. Few ceremonies and tests are practiced to determine eligibility for specific adult privileges. Obtaining a driver’s license, graduating from high school, and reaching legal age for drinking are among the few milestones that exist. U.S. society also does not have many generally agreed-on social dictums. When is the right age to begin dating? What is a reasonable curfew? Should an 18-year-old be allowed to stay out all night? There are few areas of general agreement. Every family makes up its own rules, influenced, but uninstructed, by the society at large. Many families have great difficulty with this process.
Modified from Prothrow-Stith D: Deadly consequences: how violence is destroying our teenage population and a plan to begin solving the problem, New York, 1993, HarperCollins. HarperCollins
Adolescence is considered as beginning with the gradual appearance of secondary sex characteristics at about 11 or 12 years of age and ending with cessation of body growth at 18 to 20 years.
Biologic development during puberty is characterized by increased activity of the pituitary gland, which results in sexual maturity and the appearance of secondary sex characteristics.
According to Erikson, the major developmental crisis of adolescence is establishing a sense of identity.
Cognitive development in adolescence includes abstract thought, thinking beyond the present, logical reasoning, and a sense of idealism.
Development of body image is closely tied to body changes and social interactions.
According to Kohlberg’s theory of moral development, adolescents begin to question existing moral values and learn to make choices.
Spiritual development is characterized by the questioning of family values and ideals, a move to more philosophic thinking, and emphasis on personal religion.
Adolescent relationships with parents may be strained, whereas the influence of the peer group increases and intimate relationships assume importance.
Teenagers demonstrate a wide variety of interests, and their increased physical and cognitive skills allow them to engage in increasingly difficult and complex activities.
Adolescents’ emotions fluctuate.
Nutritional needs, especially for calcium, zinc, and iron, may not be met by teenagers’ eating habits, such as snacking and irregular mealtimes.
Motor vehicle injuries are the primary cause of death from injury in the adolescent years.
 answers to CRITICAL THINKING EXERCISE
answers to CRITICAL THINKING EXERCISE
1. Yes, there is sufficient information to arrive at a conclusion about what advice to give Jeremy’s mother.
a. During adolescence, teens consider all their past relationships as they attempt to form their own personal identity. They attempt to formulate a satisfactory identity from a multiplicity of roles, aspirations, and identifications. The process of developing this identity is time-consuming and can be associated with confusion and discouragement.
b. If significant others are too persistent and demand that adolescents make specific decisions or behave in definite ways, adolescents often make premature decisions and accept roles that do not incorporate their own personal goals or aspirations.
c. Parents who communicate well with their teens have an open, nonjudgmental, nondictatorial manner. They demonstrate that they are available and willing to listen to their teenagers. However, they also wait until the teenager opens the discussion, and then they listen attentively and allow the teen to explore issues.
3. The nursing priority in this situation is to have the mother become more aware that Jeremy is not likely to discuss his concerns on a timetable, and that it is important for her to respect his point of view. Although Jeremy wants his mother’s guidance and support, he does not want to be told what to do, and he needs an opportunity to express his own feelings and views. An example of appropriate advice to give Jeremy’s mother might be: “Be open and available to Jeremy. Tell him what you think, but not what to do.”
4. Yes, the information about how teens formulate a personal identity and the principles of effective parent communication allow the nurse to formulate this response.
5. If Jeremy’s mother changes her behavior and Jeremy still does not want to communicate and continues to withdraw from conversation, after a significant time the nurse might explore the possibility of counseling for Jeremy and his mother. Jeremy could be suffering from depression or some other condition that causes him to withdraw from conversation and interaction with his mother.
DISCUSSING SEXUAL ORIENTATION WITH ADOLESCENTS
1. No, there are insufficient data to arrive at a conclusion about John’s sexual orientation. Further discussion with him is necessary before making any assumptions.
a. Studies of gay men and lesbians indicate that adolescence is the time when individuals become aware of same-sex attraction. Homosexual and bisexual youths are at risk for health-damaging behaviors such as early initiation of sexual behavior, substance abuse, suicide, and running away from home.
b. Homosexual and bisexual youths are often confronted with the antihomosexual attitudes and values of society. It is this reaction of society that makes it difficult for homosexual and bisexual youths to grow up and become healthy physically and mentally.
c. Health professionals who work with adolescents should consider the adolescent’s increasing independence and responsibility while ensuring confidentiality.
3. The nurse’s first priority in this situation is to give John permission to discuss his feelings about this topic. He has come to the nurse practitioner to discuss this matter, and he probably feels comfortable sharing this information with her. The nurse practitioner needs to be open and nonjudgmental in her interactions with John. He needs to know that the nurse practitioner will maintain confidentiality, appreciate his feelings, and remain sensitive to his need to talk about this topic. An example of an appropriate response for the nurse practitioner might be: “John, tell me more about how you came to this conclusion.”
4. Yes, the information about sexual orientation in adolescence and the role of the health care professional support this conclusion.
5. It might be appropriate for the nurse to gather information about John’s support system and to determine the attitudes and values of John’s family and peer group toward homosexuality. In addition to establishing a trusting relationship and effective communications with John, the nurse practitioner should make certain that John has a safe environment.
1. Yes, there is sufficient evidence for the nurse to formulate a response to Jamie’s mother.
a. As teenagers progress through adolescence, they are able to assume more responsibility for their own health. They can take prescribed medications, keep health care appointments, and discuss their care with health care professionals.
b. Parents of adolescents should respect their teenager’s independence while maintaining some level of involvement with their child. However, in matters of health care, they should gradually assume the role of a consultant and allow their child to take an increasingly active role in relating to health professionals.
c. Health professionals who work with adolescents must consider the adolescent’s increasing independence and responsibility while also maintaining privacy and ensuring confidentiality. In most adolescent clinics, health care professionals meet with the adolescent and the parent together, followed by individual time with both the adolescent and the parent.
3. The first priority for nursing care at this point is to reassure both Jamie and her mother that they will each have an opportunity to express their concerns to the nurse practitioner. Because Jamie is the nurse practitioner’s patient and the setting is an adolescent clinic, the nurse practitioner should speak with Jamie first, after he or she has met briefly with Jamie and her mother together. An appropriate response by the nurse practitioner might be: “I would like to begin by speaking with both of you together, then spend some time with just you, Jamie, then with just you, Mrs. S.” Knowing that her mother will also have an opportunity to express concerns, Jamie will likely be more open and may even say, “I know what my mother will tell you,” and address the issue herself. This response will also demonstrate to Jamie that the nurse practitioner respects her privacy and will maintain confidentiality. If the nurse speaks with Jamie first, Jamie might think that her privacy is being violated and become distrustful of both the nurse practitioner and her mother. In addition, if the nurse practitioner speaks with Mrs. S. first, Jamie is likely to become defensive and spend her time trying to draw from the nurse practitioner what her mother said.
4. Yes, the information about adolescent growth and development and the roles of adolescents, their parents, and the health care professional support this conclusion.
5. The nurse practitioner should remember the circumstances under which she or he would not be able to maintain confidentiality. For example, if either Jamie or her mother share information indicating that Jamie is at risk for either self-destructive behavior (e.g., a suicide attempt) or maltreatment by others (child abuse), the nurse practitioner would not be able to maintain confidentiality. However, this does not seem to be the case based on the evidence presented at this point.
References
Abma, JC, Martinez, GM, Mosher, WE, et al. Teenagers in the United States: sexual activity, contraceptive use, and childbearing, 2002. Vital Health Stats. 2004;23(24):1–48.
American Academy of Pediatrics, Committee on Infectious Diseases. Recommended immunization schedules for children and adolescents—United States, 2008. Pediatrics. 2008;121(1):219–220.
American Academy of Pediatrics, Committee on Infectious Diseases, Pickering L, eds. Red book: 2006 report of the Committee on Infectious Diseases, ed 27, Elk Grove Village, Ill: The Academy, 2006.
American Heart Association. Dietary recommendations for children and adolescents. http://www.americanheart.org/presenter.jhtml?identifier=53033999, 2005. [retrieved Jan 24, 2008, from].
American Medical Association. Guidelines for Adolescent Preventive Services (GAPS). Chicago: The Association, 1997.
Baker, SP, Chen, L, Li, G. Nationwide review of graduated driver licensing. Washington, DC: AAA Foundation for Traffic Safety, 2007.
Biro, FM, Lucky, AW, Simbarti, LA, et al. Pubertal maturation in girls and the relationship to anthropometric changes: pathways through puberty. J Pediatr. 2003;142(6):643–646.
Bond, L, Butler, H, Thomas, L, et al. Social and school connectedness in early secondary school as predictors of late teenage substance use, mental health, and academic outcomes. J Adolesc Health. 2007;40(4):357.e9–357.e18.
Braverman, PK. Body art: piercing, tattooing, and scarification. Adolesc Med. 2006;17:505–519.
Briggs, M, Safaii, S, Beall, DL. Nutrition services: an essential component of comprehensive school health programs. J Am Diet Assoc. 2003;103(4):505–514.
Brown, J. Body and spirit: religion, spirituality and health among adolescents. Adolesc Med. 2001;12(3):509–523.
Centers for Disease Control and Prevention. Welcome to WISQARS. http://www.cdc.gov/ncipc/wisqars, 2006. [retrieved Jan 24, 2008, from].
Centers for Disease Control and Prevention. Youth risk behavior surveillance—United States, 2005. MMWR. 2006;55(SS-5):1–108.
Costello, EJ, Sung, M, Worthman, C, et al. Pubertal maturation and the development of alcohol use and abuse. Drug Alcohol Depend. 2007;88(4 Suppl 1):S50–S59.
DeVore, ER, Ginsburg, KR. The protective effects of good parenting on adolescents. Curr Opin Pediatr. 2005;17(4):460–465.
Gance-Cleveland, B. Motivational interviewing: improving patient education. J Pediatr Health. 2007;21(2):81–88.
Glatt, K. Child-to-child unintentional injury and death from firearms in the United States: what can be done? J Pediatr Nurs. 2005;10(6):448–452.
Lynne, SD, Graber, JA, Nichols, TR, et al. Links between pubertal timing, peer influences and externalizing behaviors among urban students followed through middle school. J Adolesc Health. 2007;40(2):181–213.
Maes, L, Lievens, J. Can the school make a difference? A multilevel analysis of adolescent risk and health behaviour. Soc Sci Med. 2003;56(3):517–529.
Mosher, WD, Chandra, A, Jones, J. Sexual behavior and selected health measures: men and women 15-44 years of age, United States, 2002. Adv Data, Sep. 2005;15(362):1–55.
Nielsen, SJ, Popkin, BM. Patterns and trends in food portion sizes, 1977-1998. JAMA. 2003;289(4):450–453.
Omar, H, McElderry, D, Zakharia, R. Educating adolescents about puberty: what are we missing? Int J Adolesc Med Health. 2003;15(1):79–83.
Ongphiphadhanakul, B. Osteoporosis: the role of genetics and the environment. Forum Nutr. 2007;60:158–167.
Saewyc, EM, Bearinger, LH, Heinz, PA, et al. Gender differences in health and risk behaviors among bisexual and homosexual adolescents. J Adolesc Health. 1998;23(3):181–188.
Santelli, JS, Lindberg, LD, Finer, LB, et al. Explaining recent declines in adolescent pregnancy in the United States: the contribution of abstinence and improved contraceptive use. Am J Pub Health. 2007;97(1):150–156.
Strong, WB, Malina, RM, Blimkie, CJ, et al. Evidence based physical activity for school-aged youth. J Pediatr. 2005;146:732–737.
Tuttle, J, Campbell-Heider, N, David, TM. Positive adolescent life skills training for high-risk teens: results of a group intervention study. J Pediatr Health. 2006;20(3):184–191.
Williams, AF, Ferguson, SA. Rationale for graduated licensing and the risks it should address. Inj Prevent. 2002;6:9–16.
Williams, AF, McCartt, AF, Geary, L. Seatbelt use by high school students. Inj Prevent. 2003;9:25–28.
*http://www.cdc.gov/Features/BodyArt.
*434 West 33rd St., New York, NY 10001; (212) 541-7800; http://www.plannedparenthood.org.
†130 West 42nd St., Suite 350, New York, NY 10036; (212) 819-9770; http://www.siecus.org.
‡850 Coxwell Ave., Toronto, Ontario M4C 5R1; (416) 466-5304; http://www.sieccan.org.