Health Promotion of the School-Age Child and Family
On completion of this chapter the reader will be able to:
 Describe the physical, cognitive, and moral changes that take place during the middle childhood years.
Describe the physical, cognitive, and moral changes that take place during the middle childhood years.
Describe ways to help a child develop a sense of accomplishment.
Demonstrate an understanding of the changing interpersonal relationships of school-age children.
Discuss the role of the peer group in the socialization of the school-age child.
Discuss the role of schools in the development and socialization of the school-age child.
Outline an appropriate health teaching plan for the school-age child.
Plan a sex education session for a group of school-age children.
Identify the causes and discuss the preventive aspects of injury in middle childhood.
RELATED TOPICS and ADDITIONAL RESOURCES
 IN TEXT
IN TEXTChildhood Mortality, Ch. 1
Dental Health, Ch. 12
Eating Disorders, Ch. 17
Growth and Development, Ch. 5
Health Problems of School-Age Children and Adolescents, Ch. 17
Immunizations, Ch. 10
Physical and Developmental Assessment of the Child, Ch. 5 and Ch. 6
Psychosocial History, Ch. 6
Limit Setting and Discipline, Ch. 3
Traumatic Injury, Ch. 31
PROMOTING OPTIMAL GROWTH AND DEVELOPMENT
The segment of the life span that extends from age 6 to approximately age 12 has a variety of labels, each of which describes an important characteristic of the period. These middle years are most often referred to as school-age or the school years. This period begins with entrance into the school environment, which has a significant impact on development and relationships.
Physiologically the middle years begin with the shedding of the first deciduous tooth and end at puberty with the acquisition of the final permanent teeth (with the exception of the wisdom teeth). Before 5 or 6 years of age, children have progressed from helpless infants to sturdy, complicated individuals with an ability to communicate, conceptualize in a limited way, and become involved in complex social and motor behaviors. Physical growth is also rapid during the preschool-age years. In contrast, the period of middle childhood, between the rapid growth of early childhood and the prepubescent growth spurt, is a time of gradual growth and development with more even progress in both physical and emotional aspects.
BIOLOGIC DEVELOPMENT
During middle childhood, growth in height and weight assumes a slower but steady pace as compared with the earlier years. Between ages 6 and 12, children will grow an average of 5 cm (2 inches) per year to gain 30 to 60 cm (1 to 2 feet) in height and will almost double their weight, increasing 2 to 3 kg (4.5 to 6.5 pounds) per year. The average 6-year-old child is about 116 cm (45.7 inches) tall and weighs about 21 kg (46 pounds); the average 12-year-old child is about 150 cm (59 inches) tall and weighs approximately 40 kg (88 pounds). During this period, girls and boys differ little in size, although boys tend to be slightly taller and somewhat heavier than girls. Toward the end of the school-age years, both boys and girls begin to increase in size, although most girls begin to surpass boys in both height and weight, to the acute discomfort of both girls and boys.
Proportional Changes
School-age children are more graceful than they were as preschoolers, and they are steadier on their feet. Their body proportions take on a slimmer look, with longer legs, varying body proportion, and a lower center of gravity. Posture improves over that of the preschool period to facilitate locomotion and efficiency in using the arms and trunk. These proportions make climbing, bicycle riding, and other activities easier. Fat gradually diminishes, and its distribution patterns change, contributing to the thinner appearance of the child during the middle years.
Accompanying the skeletal lengthening and fat diminution is an increase in the percentage of body weight represented by muscle tissue. By the end of this age period, both boys and girls double their strength and physical capabilities, and their steady and relatively consistent development of coordination increases their poise and skill. However, this increased strength can be misleading. Although strength increases, muscles are still functionally immature when compared with those of the adolescent, and they are more readily damaged by muscular injury caused by overuse.
The most pronounced changes that indicate increasing maturity in children are a decrease in head circumference in relation to standing height, a decrease in waist circumference in relation to height, and an increase in leg length in relation to height. These observations often provide a clue to a child’s degree of physical maturity and have proved useful in predicting readiness for meeting the demands of school. There appears to be a correlation between physical indications of maturity and success in school.
Specific physiologic and anatomic characteristics are typical of children in middle childhood. Facial proportions change as the face grows faster in relation to the remainder of the cranium. The skull and brain grow very slowly during this period and increase little in size. Because all of the primary (deciduous) teeth are lost during this age span, middle childhood is sometimes known as the age of the loose tooth (Fig. 15-1). The early years of middle childhood, when the new secondary (permanent) teeth appear too large for the face, are known as the ugly duckling stage.

Maturation of Systems
Maturity of the gastrointestinal system is reflected in fewer stomach upsets, better maintenance of blood glucose levels, and an increased stomach capacity, which permits retention of food for longer periods. The school-age child does not need to be fed as carefully, as promptly, or as frequently as the preschool-age child. Caloric needs are less than they were in the preschool years.
Physical maturation is evident in other body tissues and organs. Bladder capacity, although differing widely among individual children, is generally greater in girls than in boys. The heart grows more slowly during the middle years and is smaller in relation to the rest of the body than at any other period of life. Heart and respiratory rates steadily decrease and blood pressure increases from ages 6 to 12 (see inside back cover).
The immune system becomes more competent in its ability to localize infections and to produce an antibody-antigen response. However, children have several infections in the first 1 to 2 years of school because of increased exposure to other children.
Bones continue to ossify throughout childhood but yield to pressure and muscle pulls more readily than with mature bones. Children need ample opportunity to move around, but they should observe caution in carrying heavy loads. For example, they should shift books or tote bags from one arm to the other. Backpacks distribute weight more evenly than tote bags.
Wider differences between children are observed at the end of middle childhood than at the beginning. These differences become increasingly apparent and, if they are extreme or unique, may create emotional problems. The associated characteristics of height and weight relationships, rapid or slow growth, and other important features of development should be explained to children and their families. Physical maturity is not necessarily correlated with emotional and social maturity. Seven-year-old children who look like 10-year-old children will, in fact, think and act like 7-year-old children. To expect behaviors appropriate for the older age is unrealistic and can be detrimental to their development of competence and self-esteem. Conversely, to treat 10-year-old children who look young physically as though they were younger is an equal disservice to them.
Prepubescence
Preadolescence is the period of approximately 2 years that begins at the end of middle childhood and ends with the thirteenth birthday. Because puberty signals the beginning of the development of secondary sex characteristics, prepubescence typically occurs during preadolescence.
Toward the end of middle childhood the discrepancies in growth and maturation between boys and girls become apparent. On the average, there is a difference of approximately 2 years between girls and boys in the age of onset of pubescence. This is a period of rapid growth in height and weight, especially for girls.
There is no universal age at which children assume the characteristics of prepubescence. The first physiologic signs appear at about 9 years of age (particularly in girls) and are usually clearly evident in 11- to 12-year-old children. Although preadolescent children do not want to be different, variability in physical growth and physiologic changes between children of the same sex and between the two sexes is often striking at this time. This variability, especially in relation to the onset of secondary sexual characteristics, is of great concern to the preadolescent. Either early or late appearance of these characteristics is a source of embarrassment and uneasiness to both sexes.
Preadolescence is a period of considerable overlapping of developmental characteristics of both middle childhood and early adolescence. However, several unique characteristics set this period apart from others. Generally, puberty begins at 10 years in girls and 12 years in boys, but can be normal for either sex after the age of 8 years. Boys experience little visible sexual maturation during preadolescence.
PSYCHOSOCIAL DEVELOPMENT: DEVELOPING A SENSE OF INDUSTRY (ERIKSON)
Freud described middle childhood as the latency period, a time of tranquility between the Oedipal phase of early childhood and the eroticism of adolescence. During this time children experience relationships with same-sex peers following the indifference of earlier years and preceding the heterosexual fascination that occurs for most boys and girls in puberty.
Successful mastery of Erikson’s first three stages of psychosocial development is important in terms of development of a healthy personality. Successful completion of these stages requires a loving environment within a stable family unit. These experiences prepare the child to engage in experiences and relationships beyond the intimate family group.
A sense of industry, or a stage of accomplishment, is achieved somewhere between age 6 and adolescence. School-age children are eager to develop skills and participate in meaningful and socially useful work. They acquire a sense of personal and interpersonal competence; receive the systematic instruction prescribed by their individual cultures; and develop the skills needed to become useful, contributing members of their social communities.
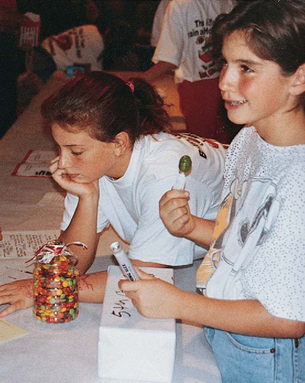
Interests expand in the middle years, and with a growing sense of independence, children want to engage in tasks that can be carried through to completion (Fig. 15-2). They gain satisfaction from independent behavior in exploring and manipulating their environment and from interaction with peers. Often the acquisition of skills provides a way to achieve success in social activities. Reinforcement in the form of grades, material rewards, additional privileges, and recognition provides encouragement and stimulation.

A sense of accomplishment also involves the ability to cooperate, to compete with others, and to cope effectively with people. Middle childhood is the time when children learn the value of doing things with others and the benefits derived from division of labor in the accomplishment of goals. Peer approval is a strong motivating power.
The danger inherent in this period of development is the occurrence of situations that might result in a sense of inferiority. Children with physical and mental limitations may be at a disadvantage in the acquisition of certain skills. When the reward structure is based on evidence of mastery, children who are incapable of developing these skills risk feeling inadequate and inferior. Even children without chronic disabilities may experience feelings of inadequacy in some areas. No child is able to do everything well, and children must learn that they will not be able to master every skill they attempt. All children, even children who usually have positive attitudes toward work and their own abilities, will feel some degree of inferiority when they encounter specific skills that they cannot master.
Children need and want real achievement. Children achieve a sense of industry when they have access to tasks that need to be done and they are able to complete the tasks well despite individual differences in their innate capacities and emotional development.
COGNITIVE DEVELOPMENT (PIAGET)
When children enter the school years, they begin to acquire the ability to relate a series of events to mental representations that can be expressed both verbally and symbolically. This is the stage Piaget describes as concrete operations, when children are able to use thought processes to experience events and actions. The rigid, egocentric view of the preschool years is replaced by mental processes that allow children to see things from another’s point of view.
During this stage, children develop an understanding of relationships between things and ideas. They progress from making judgments based on what they see (perceptual thinking) to making judgments based on what they reason (conceptual thinking). They are able to master symbols and to use their memories of past experiences to evaluate and interpret the present.
One cognitive task of school-age children is mastering the concept of conservation (Fig. 15-3). At an early age (about 5 to 7 years), children grasp the concept of reversibility of numbers as a basis for simple mathematics problems (e.g., 2 + 4 = 6 and 6 − 4 = 2). They learn that simply altering their arrangement in space does not change certain properties of the environment, and they are able to resist perceptual cues that suggest alterations in the physical state of an object. For example, they recognize that changing the shape of a substance such as a lump of clay does not alter its total mass. They no longer perceive a tall, thin glass of water as containing a greater volume than a short, wide glass; they can distinguish between the weight of items regardless of their size. They recognize that size is not necessarily related to weight or volume. There is a developmental sequence in children’s capacity to conserve matter. Conservation of mass usually is accomplished first, weight some time later, and volume last.
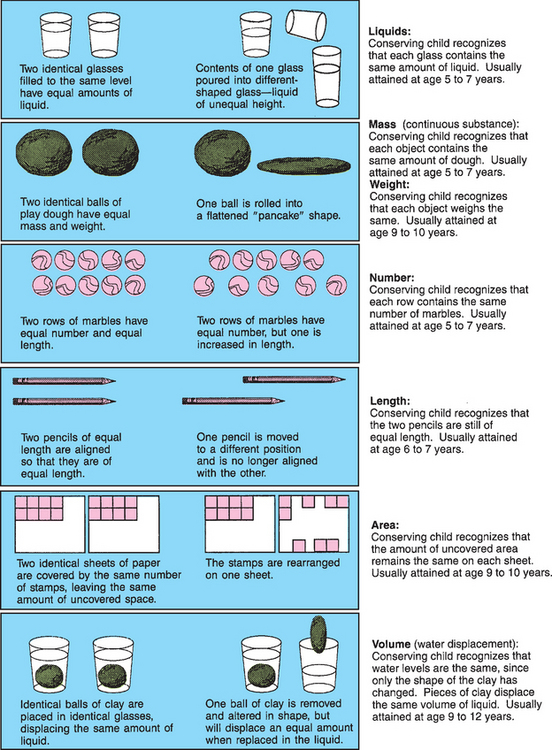
FIG. 15-3 Common examples that demonstrate the child’s ability to conserve (ages are only approximate).
School-age children also develop classification skills. They can group and sort objects according to the attributes they share, place things in a sensible and logical order, and hold a concept in mind while making decisions based on that concept. Another characteristic of middle childhood is that children derive enjoyment from classifying and ordering their environment. They become occupied with collections of objects, such as stickers, shells, dolls, cars, cards, and stuffed animals. They may even begin to order friends and relationships (e.g., best friend, second best friend).
They develop the ability to understand relational terms and concepts, such as bigger and smaller; darker and paler; heavier and lighter; to the right of and to the left of; first, last, and intermediate relationships; and more than and less than. They view family relationships in terms of reciprocal roles (e.g., to be a brother, one must have a sibling).
School-age children learn the alphabet and the world of symbols called words, which can be arranged in terms of structure and their relationship to the alphabet. They learn to tell time, to see the relationship of events in time (history) and places in space (geography), and to combine time and space relationships (geology and astronomy).
The ability to read is acquired during the school years and becomes the most significant and valuable tool for independent inquiry. Children’s capacity to explore, imagine, and expand their knowledge is enhanced by reading.
MORAL DEVELOPMENT (KOHLBERG)
As children move from egocentrism to more logical patterns of thought, they also move through stages in the development of conscience and moral standards. Young children do not believe that standards of behavior come from within themselves but that rules are established and set down by others. During the preschool years children adopt and internalize the moral values of their parents. They learn standards for acceptable behavior, act according to these standards, and feel guilty when they violate them. Although children 6 or 7 years of age know the rules and behaviors expected of them, they do not understand the reasons behind them. Rewards and punishments guide their judgment; a “bad act” is one that breaks a rule or causes harm. Young children believe that what other people tell them to do is right and that what they themselves think is wrong. Consequently, children 6 or 7 years old may interpret accidents or misfortunes as punishment for “bad” acts.
Older school-age children are able to judge an act by the intentions that prompted it rather than just its consequences. Rules and judgments become less absolute and authoritarian, and begin to be founded on the needs and desires of others. For older children, a rule violation is likely to be viewed in relation to the total context in which it appears. The situation, as well as the morality of the rule itself, influences reactions. Although younger children judge an act only according to whether it is right or wrong, older children take into account a different point of view. They are able to understand and accept the concept of treating others as they would like to be treated.
SPIRITUAL DEVELOPMENT
Children at this age think in concrete terms, but are avid learners and have a great desire to learn about their God. They picture God as human and use adjectives such as “loving” and “helping” to describe their deity. They are fascinated by the concepts of hell and heaven, with a developing conscience and concern about rules. They may fear going to hell for misbehavior. School-age children want and expect to be punished for misbehavior and, when given the option, tend to choose a punishment that “fits the crime.” However, they may view illness or injury as a punishment for a real or imagined misdeed. The beliefs and ideals of family and religious persons are more influential than those of their peers in matters of faith.
 CULTURAL AWARENESS
CULTURAL AWARENESSMany schools and communities have a Judeo-Christian orientation toward prayer, holidays, and values. This may result in conflict and discomfort for children of other religious or ethnic groups. Sensitivity must be exercised so as not to offend and confuse children from other religious backgrounds, such as the Buddhist, Hindu, and Muslim faiths, and those with no religious backgrounds.
School-age children begin to learn the difference between the natural and the supernatural but have difficulty understanding symbols. Consequently, religious concepts must be presented to them in concrete terms. Prayer or other religious rituals comfort them, and if these activities are a part of their daily lives, they can help them cope with threatening situations. Their petitions to their God in prayers tend to be for tangible rewards. Although younger children expect their prayers to be answered, as they get older, they begin to recognize that this does not always occur and become less concerned when prayers are not answered. They are able to discuss their feelings about their faith and how it relates to their lives (see Cultural Awareness box).
SOCIAL DEVELOPMENT
One of the most important socializing agents in the school-age years is the peer group. In addition to parents and the schools, the peer group conveys a substantial amount of information to its members. Peer groups have a culture of their own, with secrets, traditions, and codes of ethics that promote feelings of solidarity and detachment from adults. Through peer relationships, children learn how to deal with dominance and hostility, how to relate to persons in positions of leadership and authority, and how to explore ideas and the physical environment.
Peer group identification is an important factor in gaining independence from parents. The aid and support of the group provide the child with enough security to risk the moderate parental rejection brought about by small victories in the development of independence.
A child’s concept of the appropriate sex role is also influenced by relationships with peers. During the early school years few gender differences exist in the play experiences of children. Both girls and boys share games and other activities. However, in the later school years the differences in the play of boys and girls becomes more marked.
Social Relationships and Cooperation
Daily relationships with peers provide important social interactions for school-age children. For the first time, children join group activities with unrestrained enthusiasm and steady participation. Previous interactions were limited to short periods under considerable adult supervision. With increased skills and wider opportunities, children become involved with one or more peer groups in which they can gain status as respected members.
Valuable lessons are learned from daily interaction with age-mates. First, children learn to appreciate the numerous and varied points of view that are represented in the peer group. As children interact with peers who see the world in ways that are somewhat different from their own, they become aware of the limits of their own point of view. Because age-mates are peers and are not forced to accept each other’s ideas as they are expected to accept those of adults, other children have a significant influence on decreasing the egocentric outlook of the child. Consequently, children learn to argue, persuade, bargain, cooperate, and compromise to maintain friendships.
Second, children become increasingly sensitive to the social norms and pressures of the peer group. The peer group establishes standards for acceptance and rejection, and children are often willing to modify their behavior to be accepted by the group. The need for peer approval becomes a powerful influence toward conformity. Children learn to dress, talk, and behave in a manner acceptable to the group. A variety of roles, such as class joker or class hero, may be assumed by individual children to gain approval from the group.
Third, the interaction among peers leads to the formation of intimate friendships between same-sex peers. The school-age period is the time when children have “best friends” with whom they share secrets, private jokes, and adventures; they come to one another’s aid in times of trouble. In the course of these friendships children also fight, threaten each other, break up, and reunite. These relationships, in which the child experiences love and closeness for a peer, may be important as a foundation for relationships in adulthood (Fig. 15-4).
Clubs and Peer Groups.: One of the outstanding characteristics of middle childhood is the formation of formalized groups, or clubs. A prominent feature of these groups is the rigid rules imposed on the members. There is exclusiveness in the selection of persons who have the privilege of joining. Acceptance in the group is often determined on a pass-fail basis according to social or behavioral criteria. Conformity is the core of the group structure. There are often secret codes, shared interests, and special modes of dress, and each child must abide by a standard of behavior established by the members. Conforming to the rules provides children with feelings of security and relieves them of the responsibility of making decisions. By merging their identities with those of their peers, children are able to move from the family group to an outside group as a step toward seeking further independence. Peer groups and clubs allow children to substitute conformity to a peer group for conformity to a family at a time when children are still too insecure to function independently.
During the early school years, groups are usually small and loosely organized, with changing membership and no formal structure. The clubs and groups usually do not display elements of cooperation and order that are seen in groups of older children. In general, girls’ groups are less formalized than boys’ are, and although there may be a mixture of both sexes in the early school years, the groups of later school years are composed predominantly of children of the same sex. Common interests are the basis around which the group is structured.
Peer-group identification and association are essential to a child’s socialization. Poor relationships with peers and a lack of group identification can contribute to bullying. Bullying is any recurring activity that is intended to harm or bother someone where there is a perceived imbalance of power between the aggressor(s) and the victim (Glew, Fan, Katon, and others, 2005). Bullying occurs most frequently at school during unstructured times, with recess being the most common opportunity for bullying, followed by gym classes, lunchrooms, hallways, and buses (Glew, Fan, Katon, and others, 2005). Bullies may be from any ethnic, racial, or socioeconomic group. They are generally defiant toward adults, antisocial, and likely to break school rules. They have little anxiety, strong self-esteem, and dominant personalities; may come from homes where parental involvement and nurturing are lacking; and may experience or witness violence or abuse at home (Lyznicki, McCaffree, and Robinowitz, 2004). Boys who bully tend to use physical force, whereas girls who bully employ psychologic methods such as ostracism or rumors. Bullying by boys is more common than by girls. Children who are targeted for bullying often have characteristics different from the group norm (i.e., children who are short or obese; have facial deformities; or have attention deficit hyperactivity disorder, mental retardation, or other developmental disabilities) (Vessey, Carlson, and David, 2003).
The long-term consequences of bullying are significant. Chronic bullies seem to continue their behaviors into adulthood, negatively influencing their ability to develop and maintain relationships. Victims of bullying often feel socially rejected and can fear school, which can develop into school phobia or long-term problems of depression and low self-esteem (Vreeman and Carroll, 2007). School personnel play an important role in implementing antibullying interventions in the elementary schools before bullying becomes a part of the school culture (Glew, Fan, Katon, and others, 2005).
There are also dangers in peer-group attachments that are too strong. Peer pressures force some children to take risks or engage in behaviors that are against their better judgment. A child’s membership in a gang is associated with marked increases in serious delinquent behavior (Dishion, Nelson, and Yasui, 2005). Peer-group activities that result in unlawful or criminal gang violence are increasing in the United States. An integration of family-centered and school-based programs is needed to reduce the influences for children to become affiliated with gangs (Dishion, Nelson, and Yasui, 2005).
Relationships with Families
Although the peer group is influential and necessary to normal child development, parents are the primary influence in shaping the child’s personality, setting standards for behavior, and establishing value systems. Family values usually take precedence over peer value systems. Although children may appear to reject parental values while testing the new values of the peer group, ultimately they retain and incorporate into their own value systems the parental values they have found to be of worth.
In the middle school years, children want to spend more time in the company of peers and they often prefer peer-group activities to family activities. This can be disturbing to parents. Children become intolerant and critical of their parents, especially when their parents’ ways deviate from those of the group. They discover that parents can be wrong, and they begin to question the knowledge and authority of their parents who were previously considered to be all-knowing and all-powerful.
Although increased independence is the goal of middle childhood, children are not prepared to abandon all parental control. They need and want restrictions placed on their behavior, and they are not prepared to cope with all the problems of their expanding environment. They feel more secure knowing there is an authority figure to implement controls and restrictions. Children may complain loudly about restrictions and try to break down parental barriers, but they are uneasy if they succeed in doing so. They respect adults who prevent them from acting on every urge. Children view this behavior as an expression of love and concern for their welfare.
Children also need their parents as adults, not as friends. Sometimes parents, hurt by their children’s rejection, attempt to maintain their love and gratitude by assuming the role of “pals.” Children need the stable, secure strength provided by mature adults to whom they can turn during troubled relationships with peers or stressful changes in their world. With a secure base in a loving family, children are able to develop the self-confidence and maturity needed to break loose from the group and stand independently.
Play
Play takes on new dimensions that reflect a new stage of development in the school years. Play involves increased physical skill, intellectual ability, and fantasy. In addition, children develop a sense of belonging to a team or club by forming groups and cliques.
Rules and Rituals.: The need for conformity in middle childhood is strongly manifested in the activities and games of school-age children. In the preschool years, children’s games were either invented for them or played in the company of a friend or an adult. Now children begin to see the need for rules, and their games have fixed and unvarying rules that may be bizarre and extraordinarily rigid. Part of the enjoyment of the game is knowing the rules because knowing means belonging. Conformity and ritual permeate their play and are also evident in their behavior and language. Childhood is full of chants and taunts, such as “Eeeny, meeny, miney, mo,” “Last one is a rotten egg,” and “Step on a crack, break your mother’s back.” Children derive a sense of pleasure and power from such sayings, which have been handed down with few changes through generations.
Team Play.: A more complex form of play that evolves from the need for peer interaction is team games and sports. A referee, umpire, or person of authority may be required so that the rules can be followed more accurately. Team play teaches children to modify or exchange personal goals for goals of the group; it also teaches them that division of labor is an effective strategy for attaining a goal. Children learn about competition and the importance of winning—an attribute highly valued in the United States.
Team play can also contribute to children’s social, intellectual, and skill growth. Children work hard to develop the skills needed to become team members, to improve their contribution to the group, and to anticipate the consequences of their behavior for the group. Team play helps stimulate cognitive growth because children are called on to learn many complex rules, make judgments about those rules, plan strategies, and assess the strengths and weaknesses of members of their own team and members of the opposing team.
Quiet Games and Activities.: Although play at this age is highly active, school-age children also enjoy quiet and solitary activities. The middle years are the time for collections, which constitute another ritual. Young school-age children’s collections are an odd assortment of unrelated objects in messy, disorganized piles. Collections of later school years are more orderly; selective; and organized in scrapbooks, on shelves, or in boxes.
School-age children become fascinated with complex board, card, or computer games that they can play alone, with a best friend, or with a group. As in all games, adherence to the rules is fanatic. Disagreements over rules can cause much discussion and argument, but are easily resolved by reading the rules of the game.
The newly acquired skill of reading becomes increasingly satisfying as school-age children expand their knowledge of the world through books (Fig. 15-5). School-age children never tire of stories and, as with preschool children, love to have stories read aloud. Sewing, cooking, carpentry, gardening, and creative activities such as painting are other activities enjoyed. Many creative skills such as music and art, as well as athletic skills such as swimming, karate, dancing, and skating, are learned during these years and continue to be enjoyed into adolescence and adulthood (Fig. 15-6).

Ego Mastery.: Play affords children the means to acquire mastery over themselves, their environment, and others. Through play, children can feel as big, as powerful, and as skillful as their imaginations will allow. They can also feel in control and attain vicarious mastery and power over whomever and whatever they choose. School-age children still need the opportunity to use large muscles in exuberant outdoor play and the freedom to exert their newfound autonomy and initiative. They need space in which to exercise large muscles and to deal with tensions, frustrations, and hostility. Physical skills practiced and mastered in play help them develop a feeling of personal competence, which contributes to a sense of accomplishment and provides status in their peer group.
DEVELOPING A SELF-CONCEPT
The term self-concept refers to a conscious awareness of self-perceptions, such as one’s physical characteristics, abilities, values, self-ideals and expectancy, and idea of self in relation to others. It also includes one’s body image, sexuality, and self-esteem. Although primary caregivers continue to exert influence on children’s self-evaluation, the opinions of peers and teachers provide valuable input during middle childhood. With the emphasis on skill building and broadened social relationships, children are continually engaged in the process of self-evaluation.
Significant adults can often manage to unobtrusively manipulate the environment so that children experience success. Each small success increases a child’s self-image. The more positive children feel about themselves, the more confident they will be in trying for success in the future. All children profit from feeling that they are in some way special to a significant adult. A positive self-concept makes children feel likeable, worthwhile, and capable of significant contributions. These feelings lead to self-respect, self-confidence, and happiness. Negative feelings lead to self-doubt.
Developing a Body Image
School-age children have a relatively accurate and positive perception of their physical selves, but in general they like their physical selves less as they grow older. The head appears to be the most important part of the school-age child’s perceived image of self, with hair and eye color the characteristics used most frequently to describe the physical self.
Body image is influenced, but not solely determined, by significant others. The number of significant others influencing one’s perception of the physical self increases with age. Children are acutely aware of their own body, the bodies of their peers, and those of adults. They are also aware of deviations from the norm. It is important that children learn about bodily functions and that adults provide correct information.
Physical impairments, such as hearing or visual defects, ears that “stick out,” or birthmarks, assume great importance. Increasing awareness of these differences, especially when accompanied by unkind comments and taunts from others, may cause a child to feel inferior and less desirable. This is especially true if the defect interferes with the child’s ability to participate in games and activities.
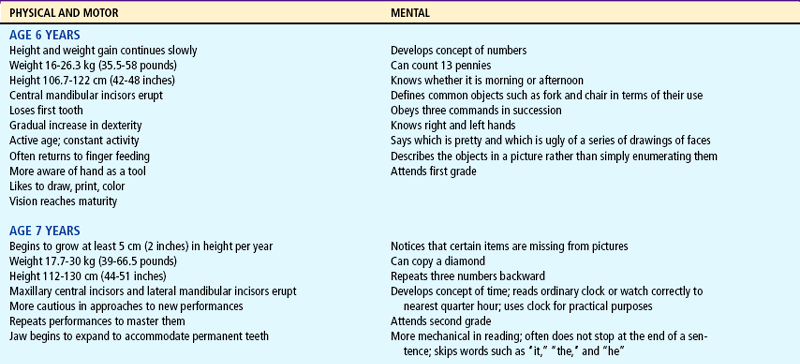
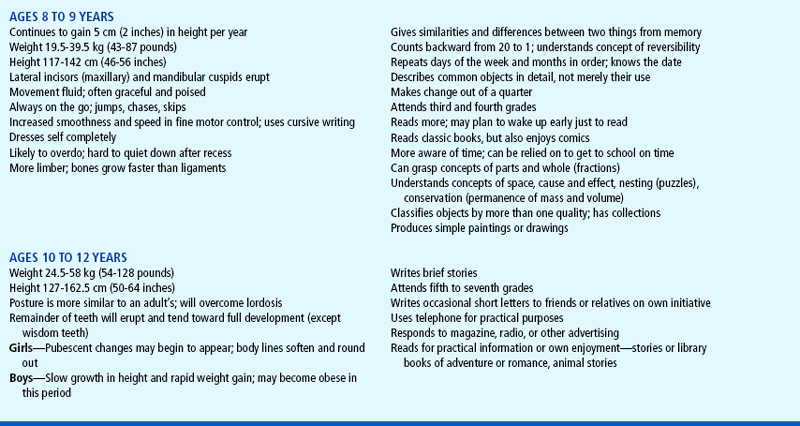
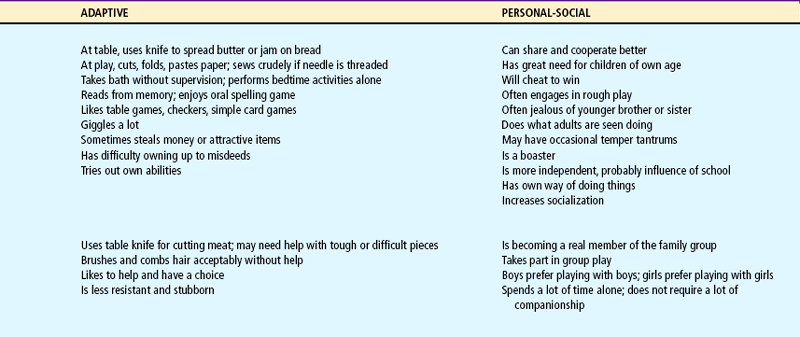
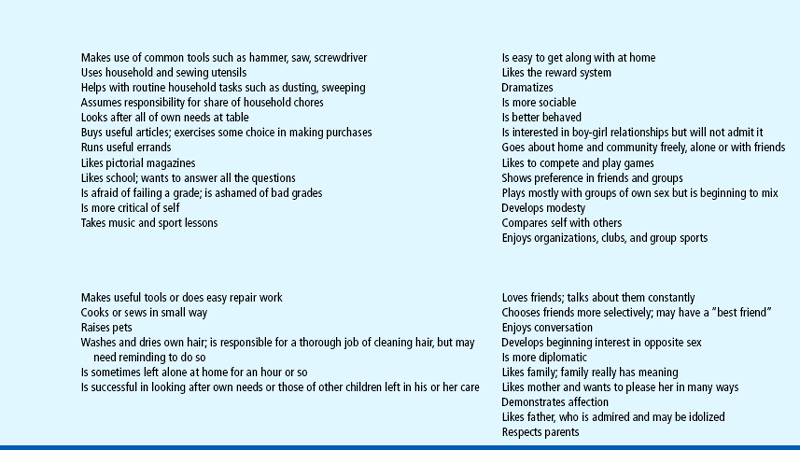
Table 15-1 summarizes the major developmental achievements of the school-age years.
COPING WITH CONCERNS RELATED TO NORMAL GROWTH AND DEVELOPMENT
School serves as the agent for transmitting the values of society to each succeeding generation of children. School is also the setting for relationships with peers. After the family, schools are the second most important socializing agent in the lives of children.
Entrance into school causes a sharp break in the structure of the child’s world. For many children it is their first experience in conforming to a group pattern imposed by an adult who is not a parent and who has responsibility for too many children to be constantly aware of each child as an individual. Children want to go to school and usually adapt to the new conditions with little difficulty. Successful adjustment is related to the child’s physical and emotional maturity and the parent’s readiness to accept the separation associated with school entrance. Unfortunately, some parents express their unconscious attempts to delay the child’s maturity by clinging behavior, particularly with their youngest child.
By the time they enter school, most children have a fairly realistic concept of what school involves. They receive information regarding the role of a student from parents, siblings, playmates, and the media. In addition, most children have had some experience with daycare, preschool, or kindergarten. Middle-class children have fewer adjustments to make and less to learn about expected behavior, since schools tend to reflect dominant middle-class customs and values. If the child has attended a preschool program, the focus of the preschool program also affects the child’s adjustment. Some preschool programs provide custodial care only, whereas others emphasize emotional, social, and intellectual development.
Classmates have a significant impact on the socialization of children. School is the first time that most children become members of a large group of individuals their own age. Peer relationships become increasingly important and influential as children proceed through school. The specific influence exerted by the peer group depends on the background, interests, and abilities of the individual child.
Teachers.: Children respond best to teachers who possess the characteristics of a warm, loving parent. Teachers in the early grades perform many of the activities formerly assumed by the parent, such as recognizing the child’s personal needs (e.g., the need to go to the bathroom, need for help with clothing) and helping to develop their social behavior (e.g., manners).
Teachers, like parents, are concerned about the child’s psychologic and emotional welfare. Although the functions of teachers and parents differ, both place constraints on behavior and both are in a position to enforce standards of conduct. However, the teacher’s primary responsibility involves stimulating and guiding children’s intellectual development, as opposed to providing for their physical welfare beyond the school setting.
Teachers serve as models that children try to emulate. Children seek their teachers’ approval and avoid their disapproval. The teacher is a significant person in the life of the early schoolchild, and hero worship of a teacher may extend into late childhood and preadolescence. Teachers who make supportive statements that reassure or commend children, use accepting and clarifying statements that help children refine ideas and feelings, and provide assistance that aids children with their own problem solving contribute to the development of a positive self-concept in the school-age child.
Parents.: Parents share responsibility for helping children achieve their maximum potential. Parents can supplement the school program in numerous ways (see Family-Centered Care box). Cultivating responsibility is the goal of parental assistance. Being responsible for schoolwork helps children learn to keep promises, meet deadlines, and succeed at their jobs as adults. Responsible children may occasionally ask for help (e.g., with a spelling list), but usually they prefer to think through their work by themselves. Excessive pressure or lack of encouragement from parents may inhibit the development of these desirable traits.
Latchkey Children
The term latchkey children is used to describe children in elementary school who are left to care for themselves before or after school without the supervision of an adult. The increasing numbers of single-parent families and working mothers, together with the lack of available child care, have created a stress-provoking situation for many school-age children. Some of these children may have a chronic illness as well.
 FAMILY-CENTERED CARE
FAMILY-CENTERED CAREBe supportive—provide companionship; share ideas and thoughts.
Be positive—every child should experience some success each day.
Share an interest in reading—use the library; discuss books they are reading.
Support and encourage activity rather than passivity.
Encourage originality—help children make their own projects from discarded articles or other available materials.
Foster the development of hobbies and collections.
Encourage children to wonder and reflect during free time.
Encourage family experiences and trips to places of interest.
Encourage questions—help children discover sources for information or places to explore and investigate.
Stimulate creative thinking and problem solving—help children try out new solutions to problems without fear of making mistakes.
Meet the teacher at the beginning of school and plan to visit the school to see what is taught and expected.
Send the child to school every day. Teachers are concerned when parents make other plans for their children; it conveys the impression that school is unimportant.
Demonstrate an interest in what the child is learning.
Demonstrate an interest in content and growth more than in grades.
Make it clear to the child that schoolwork is between the child and the teacher; teacher and child should set goals for better school performance to allow the child to feel responsible for school successes and failures.
Take advantage of situations that support and reinforce school learning.
Share information with teachers that will help them understand the child better.
Communicate with the teacher if there appears to be a problem; avoid waiting for a scheduled conference.
Provide a quiet, well-lit area for study that is safe from interruption; do not allow television or radio.
Avoid dictating a study time, but do enforce rules, such as no television until homework is done; accept the child’s word that work is complete.
Help with homework should focus on explaining the question, not giving the answer.
Teach the child to break large tasks (e.g., a report) into smaller, manageable tasks spread over the allotted time rather than attempt the entire project the night before it is to be completed.
Limit home tutoring to special circumstances, such as when the teacher requests parental assistance after a child’s prolonged absence.
Request special help for children with learning problems.
Support the school staff by showing respect for both the school system and the teacher, at least in the child’s presence.
Inadequate adult supervision after school leaves children at greater risk for injury and delinquent behavior. In some instances outside activities are curtailed and relationships with peers may be significantly diminished. Latchkey children may feel more lonely, isolated, and fearful than children who have someone to care for them. To cope with their fears and anxieties while alone, these children may devise strategies such as hiding, playing the television at loud volume, or using pets for comfort.
Many communities and persons concerned about the welfare of latchkey children are trying to help these children and their parents deal with this potentially serious problem. Some communities and employers have implemented after-school programs or telephone “hotlines” that provide check-in and reassurance for children. Nurses should be aware of these community services and encourage parents to teach self-help skills to these children.
Limit Setting and Discipline
Many factors influence the amount and manner of discipline and limit setting imposed on school-age children. Some of these factors are the parents’ psychosocial maturity, the parents’ childhood and childrearing experiences, the children’s temperament, the context of the children’s misconduct, and the children’s response to rewards and punishments. When children develop an ability to see a situation from another’s point of view, they are also able to understand the effects of their reactions on others and themselves.
Discipline should take place in a positive, supportive environment with the use of strategies to instruct and guide desired behaviors and eliminate undesired behaviors (Ateah, 2003). Reasoning is an effective technique for middle school—age children. With advancing cognitive skills, they are able to benefit from more complex disciplinary strategies. For example, withholding privileges, requiring compensation, imposing penalties, and contracting can be used with great success. Problem solving is the best approach to limit setting, and children themselves can be included in the process of determining appropriate disciplinary measures.
Dishonest Behavior
During middle childhood, children may engage in what is considered to be antisocial behavior. Previously well-behaved children may engage in lying, stealing, and cheating. Such behaviors are disturbing and challenging to parents.
Lying can occur for a number of reasons. By the time children enter school, they still “tell stories,” often exaggerating a story or situation as a means of impressing their family or friends. However, during middle childhood, children become able to distinguish between fact and fantasy. If children do not develop this characteristic, parents need to teach them what is real and what is make-believe.
Young children may lie to escape punishment or to get out of some difficulty even when their misbehavior is evident. Older children may lie to meet expectations set by others to which they have been unable to measure up. However, most children know that lying and cheating are wrong, and they are concerned when it is observed in their friends. They are quick to tell on others when they detect cheating.
Parents need to be reassured that all children lie occasionally and that sometimes children may have difficulty separating fantasy from reality. Parents should be helped to understand the importance of being truthful in their relationships with children.
Cheating is most common in young children 5 to 6 years of age. They find it difficult to lose at a game or contest, so they may cheat to win. They have not yet realized that this behavior is wrong, and they do it almost automatically. This behavior usually disappears as they mature. However, because children model observed behaviors, parents need to be aware of their own behavior. When parents set examples of honesty, children are more likely to conform to these standards.
As with other ethically related behavior, stealing is not unexpected in the younger child. Between 5 and 8 years of age, children’s sense of property rights is limited, and they tend to take something simply because they are attracted to it or to take money for what it will buy. They are equally likely to give away something valuable that belongs to them. When young children are caught and punished, they are penitent—they “didn’t mean to” and “promise to never do it again”–but they are likely to repeat the performance the following day. Often they not only steal but also lie about their behavior or attempt to justify it with excuses. It is seldom helpful to trap children into admission by asking directly if they committed the offense. Children do not take responsibility for these behaviors until the end of middle childhood.
Children steal for several reasons. Young children may lack a sense of property rights, attempt to acquire a specific object to bribe favors from other children, have a strong desire to own a coveted item, or have a desire for revenge to “get back at someone” (usually a parent for unfair treatment). Older children may steal to supplement an inadequate allowance. Stealing can be an indication that something is seriously wrong or lacking in the child’s life. For example, children may steal to make up for love or another satisfaction that they feel is lacking. In most situations it is wise not to attempt to attach a hidden or deep meaning to the stealing. An admonition, together with an appropriate and reasonable punishment, such as having the older child pay back the money or return the stolen items, takes care of most cases. Most children can be taught to respect the property rights of others with little difficulty despite numerous temptations and opportunities. If children’s personal rights are respected, they are likely to respect the rights of others. Some children simply need more time to learn the rules regarding private property.
Stress and Fear
Children today experience significant amounts of stress, which can cause long-term adjustment and health problems. Stress in childhood comes from a variety of sources such as conflict within the family, interpersonal relationships, poverty, and chronic illness. The school environment and participation in multiple organized activities can be additional sources of stress. The demands from coaches and parents, in addition to school requirements and pressure from teachers to do well on proficiency testing, can cause unrealistic expectations on the school-age child (Ryan-Wenger, Sharrer, and Campbell, 2005). In addition, with the increased exposure to sexuality and provocative clothing and behaviors, children of this age-group may feel pressured to have a girlfriend or boyfriend, which their maturity level cannot handle and which causes additional stress (Ryan-Wenger, Sharrer, and Campbell, 2005).
The increasing violence in society has also spilled over into the school setting. In the present information age, in which tragedy is broadcast daily in the media, children come to school knowing more about the latest world events than any previous generation of children. In addition, today’s children are often personally aware of violence in their families or communities. Many children know other children who have been killed or children who have brought weapons to school. School-age children can be victims of teasing, bullying, and physical abuse in the school environment (Nansel, Overpeck, Haynie, and others, 2003).
To help children cope with stress, parents, teachers, and health care providers need to frequently reassure children that they are safe, have honest and open communication, encourage children to express their feelings, and promote a daily routine (Nansel, Overpeck, Haynie, and others, 2003). Adults must recognize signs that indicate a child is undergoing stress, identify the source of the stress promptly, and refer those children who need specialized treatment.
The nurse who observes the following signs of stress in a child should explore the situation further:
Children 7 to 12 years of age are capable of identifying their own physiologic responses to stress with terms that have meaning to them. Some words or phrases used by children to describe their body’s reaction to stress include tight muscles, hot or red in the face, tingling, chills or goose bumps, shakiness, heart beating fast, headache, and stomachache (Sharrer and Ryan-Wenger, 2002). Children should be taught to recognize these signs as indicators of stress and to use techniques to manage their stress. Children can learn relaxation techniques such as deep-breathing exercises, progressive relaxation of muscle groups, and positive imagery to immediately reduce stress (Mortweet and Christophersen, 2004). Encouraging them to “blow off steam” through physical activity reduces tension and anxiety. Children can be encouraged to observe effective coping strategies in others and adopt them for their own use (Mortweet and Christophersen, 2004). When an effective strategy has been developed for one situation, parents can show the child how to transfer the coping strategy or technique to other situations.
In addition to stress, school-age children experience a wide variety of fears, including fear of the dark, excessive worry about past behavior, self-consciousness, social withdrawal, and an excessive need for reassurance. These fears are considered normal for children this age. During the middle-school years, children become less fearful of body safety than they were as preschoolers, but they still fear being hurt, being kidnapped, or having to undergo surgery. They also fear death and are fascinated by all the aspects of death and dying. The fears of noises, darkness, storms, and dogs lessen, but new fears related predominantly to school and family bother children during this time.
PROMOTING OPTIMAL HEALTH DURING THE SCHOOL YEARS
Although caloric needs are diminished in relation to body size during middle childhood, resources are being laid down at this time for the increased growth needs of adolescence. Parents and children need to be aware of the value of a balanced diet to promote growth because children usually eat what their family members eat. The quality of the child’s diet depends on the family’s pattern of eating.
Likes and dislikes established at an early age continue in middle childhood, although preferences for single foods subside, and children develop a taste for a variety of foods. However, the easy availability of fast-food restaurants, the influence of the mass media, and the temptation of “junk food” make it easy for children to fill up on empty calories. Foods that do not promote growth, such as sugars, starches, and excess fats, are common in the school-age child’s diet. The easy availability of high-calorie foods, combined with the tendency toward more sedentary activities, has also contributed to an epidemic of childhood obesity. This problem is discussed further in Chapter 17.
Parents are unable to monitor what their children eat when they are away from home. A parent may pack a lunch for school but be unaware of how much is eaten, traded, sold, or thrown away. Nutrition education can and should be integrated in the curriculum throughout the school years. Important aspects of nutrition education include the U.S. Food and Drug Administration’s MyPyramid; elements of a wholesome diet; and how food products are grown, processed, and prepared. However, the school cafeteria may not always provide healthy, nutritious meals. The school nurse can take an active role in nutrition education by working with teachers to plan and implement units on nutrition instruction and by working with parents and children to give nutritional guidance.
SLEEP AND REST
The amount of sleep and rest required during middle childhood is highly individualized. The amount of sleep depends on the child’s age, activity level, and state of health. The growth rate slows in the school-age years, and less energy is expended in growth than during preceding years.
School-age children usually do not require a nap, and they sleep approximately 11 hours at age 5 years and 9.25 hours at age 12 years during the night (Carno, Hoffman, Carcillo, and others, 2003). Although fewer bedtime problems occur during these years, occasional difficulties are still associated with the bedtime ritual. Usually children 6 or 7 years old exhibit few bedtime problems, and encouraging quiet activity before bedtime, such as coloring or reading, facilitates the task of going to bed. However, most children in middle childhood must be reminded frequently to go to bed; 8- to 9-year-old children and 11-year-old children are particularly resistant. Often these children are unaware that they are tired; if they are allowed to remain up later than usual, they are fatigued the following day. Sometimes, bedtime resistance can be resolved by allowing a later bedtime as the child gets older. Twelve-year-old children usually offer no resistance at bedtime; some even retire early to read a book or listen to music.
EXERCISE AND ACTIVITY
The improved capabilities and adaptability of the school-age child permit greater speed and effort in motor activities. Larger, stronger muscles permit longer and increasingly strenuous play without exhaustion. School-age children acquire the coordination, timing, and concentration that are required to participate in adult-type activities, but they may lack the strength, stamina, and control of the adolescent and adult. They can engage in a greater amount of physical activity during the school years. However, parents, teachers, and coaches must remember that, although children this age are large and appear strong, they may not be ready for strenuous competitive athletics.
All growing children need regular exercise and opportunities for satisfying experiences consistent with individual likes and dislikes. Appropriate activities during the school-age years include running, jumping rope, swimming, roller skating, ice skating, dancing, and bicycle riding. Positive reinforcement achieved by experiencing increasingly smooth, rhythmic, and efficient use of the body conditions the child toward regular physical activity. Exercise is essential for muscle development and tone, refinement of balance and coordination, increased strength and endurance, and stimulation of body functions and metabolic processes. Children need ample space to run, jump, skip, and climb, in addition to safe indoor and outdoor facilities and equipment. Most children have abundant energy and need little encouragement to engage in physical activity. Children with disabling conditions or those who hesitate to become involved in active play (such as obese children) require special assessment and help so that activities appeal to them and are compatible with their limitations while also meeting their developmental needs.
Sports
Considerable controversy surrounds the trend toward early participation in competitive athletics and the amount and type of competitive sports that are appropriate for children in the elementary grades. The current view is that virtually every child is suited for some sport, and authorities do not discourage participation if children are matched to the type of sport appropriate to their abilities and to their physical and emotional constitution. School-age children enjoy competition (Fig. 15-7). However, teachers and coaches must understand the physical limitations of children this age and teach them the proper techniques and safety measures needed to avoid injuries. A safe and appropriate sport can be identified for even the most unskilled and uncompetitive child, including children with chronic illnesses and mental retardation. Common activities for school-age children include baseball, soccer, gymnastics, and swimming. Equipment must be maintained in safe condition, and protective apparatus should be worn to prevent serious injury (see Traumatic Injury, Chapter 31).

FIG. 15-7 The activities engaged in by school-age children vary according to interest and opportunity. A, Little League competitors. B, Playing tug-of-war.
During the school-age years girls have the same basic body structure as boys and have a similar response to systematic exercise training. However, at puberty, boys become larger and have more muscle mass, and at this stage, it is usually recommended that girls compete only against other girls. Before puberty there is no essential difference in strength and size between girls and boys, making these precautions unnecessary.
Preadolescence is a time to teach fundamental motor skills; develop fitness in a practical, safe, and gradual manner; and promote healthy attitudes and values. Activities should include both practice sessions and unstructured play; the actual game or event should be managed in a manner that stresses mastery of the sport and enhancement of self-image rather than winning or pleasing others. All children should have an opportunity to participate, and special ceremonies should recognize all participants, not just individuals who excel in sports or athletics.
Acquisition of Skills
School-age children demonstrate increasing fine motor abilities and complex artistic skills. Handedness is well established by the beginning of the school years, and children make great strides in writing and drawing during this period. It is a time of energetic and vibrant creative productivity. With the tools of language and reading, children create poems, stories, and plays. With more advanced fine motor skills, they are able to master an unlimited variety of handicrafts, such as ceramics, needlework, wood carving, and beadwork. They avidly pursue these skills in solitude; with a friend; or through organized groups such as boys’ or girls’ clubs or special interest groups that use crafts or other activities as a means to occupy, entertain, and educate children.
School-age children are capable of assuming responsibility for their own needs, although their distaste for soap and water and “dress” clothes is legendary. School-age children can and want to assume their share of household tasks, which usually are related to the male and female roles that have been defined by their culture. Many children also assume responsibility for tasks outside the home, such as baby-sitting, mowing lawns, or paper routes.
DENTAL HEALTH
The first permanent (secondary) teeth erupt at about 6 years of age, beginning with the 6-year molar, which erupts posterior to the deciduous molars. Other permanent teeth appear in approximately the same order as eruption of the primary teeth (see Teething, Chapter 10) and follow shedding of the deciduous teeth (Fig. 15-8). With the appearance of the second permanent (12-year) molar, most permanent teeth are present. Permanent dentition is more advanced in girls than in boys.
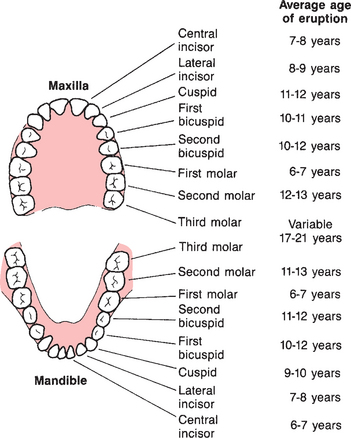
FIG. 15-8 Sequence of eruption of secondary teeth. (Data from McDonald RE, Avery DR: Dentistry for the child and adolescent, ed 6, St Louis, 1994, Mosby.)
Because the permanent teeth erupt during the school-age years, dental hygiene and regular attention to dental caries are important parts of health supervision during this period (see Dental Health, Chapter 12). Correct brushing techniques should be taught or reinforced, and the role that fermentable carbohydrates play in production of dental caries should be emphasized. It is important to be alert to possible malocclusion problems that may result from irregular eruption of permanent teeth and that may impair function. Regular dental supervision and continued fluoride supplementation are integral parts of the health maintenance program.
The most effective means of preventing dental caries is proper oral hygiene. Children should be taught to perform their own dental care with the supervision and guidance of the parents. Parents should learn the correct brushing technique with their children, and they should monitor their child’s efforts until the child can assume full responsibility.
Teeth should be brushed after meals, after snacks, and at bedtime. Children who brush their teeth frequently and become accustomed to the feel of a clean mouth at an early age usually maintain the habit throughout life. For the school-age child with mixed and permanent dentition, the best toothbrush is one with soft nylon bristles and an overall length of about 21 cm (6 inches). Several methods of brushing have been described and recommended for children, but there is no conclusive evidence that one method is superior to another. Thorough cleaning is more important than the specific technique used. The dentist should assess factors such as the manipulative skills and special needs of the child, and suggest the most appropriate brushing technique and regimen. Flossing follows brushing. Parents should perform the flossing until children acquire the manual dexterity required (usually at about 8 or 9 years of age).
Dental Problems
Limited or inadequate dental care results in the most common dental problems: dental caries, malocclusion, and periodontal disease. Trauma, especially tooth avulsion, is another important dental problem. All of these conditions benefit from early intervention to prevent tooth loss.
Dental caries (cavities) is the principal oral problem in children and adolescents. Reducing the incidence and consequences of dental caries is extremely important in childhood. If untreated, dental caries can result in total destruction of the involved teeth. The prevalence rate of caries increases steadily across the life span; 18% of children ages 2 to 4 years have caries, whereas 52% of children ages 6 to 8 years have caries (American Academy of Pediatrics, 2000).
Dental caries is a multifactorial disease involving susceptible teeth, cariogenic microflora, and an appropriate oral environment. The incidence of lesions and the likelihood of progressive invasion vary considerably and depend on a number of factors being present in the right combination. Because many children are exposed to health care but not dental care, oral inspection is an integral part of the physical assessment of every child. If there is any evidence of dental caries or other unhealthy dental state, the child should be referred for dental services. An alarming number of children do not receive regular dental supervision, and a significant number reach adulthood without dental examinations or treatment by a dentist.
Periodontal disease, an inflammatory and degenerative condition involving the gums and tissues supporting the teeth, often begins in childhood and accounts for a significant amount of tooth loss in adulthood. The more common periodontal problems are gingivitis (simple inflammation of the gums) and periodontitis (inflammation of the gums and loss of connective tissue and bone in the supporting structures of the teeth).
Gingivitis, the most prevalent periodontal disease, is a reversible inflammatory disease that can begin in early childhood and is most often associated with the buildup of plaque on the teeth. Changes take place in the plaque bacteria, in both the type and number of organisms, causing them to release destructive exotoxins, enzymes, and other noxious agents. These substances produce an inflammatory reaction in the gingival tissues, causing the gums to become red, edematous, tender, and subject to bleeding at the slightest irritation. Management is directed toward prevention by conscientious brushing and flossing, including the use of fluoride. The child should see the dentist at any signs of inflammation or irritation.
Malocclusion occurs when teeth of the upper and lower dental arches do not approximate in the proper relationships. As a result, the physiologic function of chewing is less effective and the cosmetic effect is displeasing. Teeth that are uneven, crowded, or overlapping are unable to meet their counterparts in the opposite jaw in the appropriate relationships and may be predisposed to disease in later years.
Orthodontic treatment is most successful when it is started in the late school-age or early teenage years, after the last primary teeth have been shed and before growth ceases. However, referral should be made as soon as malocclusion is evident, since some deformities can be corrected at an earlier age.
Dental injury may occur in childhood and includes fractures of varying degrees of severity, chipping, dislocation, or avulsion. All tooth injuries require prompt treatment by a competent dentist to prevent permanent displacement or loss. Delayed examination and diagnosis of tooth damage can result in infection or pulp involvement. Because it can affect the remaining teeth, replacement of the lost tooth is needed to maintain normal alignment and position of the other teeth.
A tooth that is avulsed (exarticulated, or “knocked out”) should be replanted by the child, parent, or nurse and stabilized as soon as possible so that the blood supply to the tooth can be reestablished and the tooth kept alive (see Emergency Treatment box). A tooth that is replanted within 15 minutes has a 98% survival rate (Krause-Parello, 2005). Avulsed primary teeth are usually not reimplanted.
As with all injuries to the mouth, an avulsed tooth causes a large amount of bleeding, which is frightening to children and their families; therefore the nurse or anyone faced with dental trauma should be prepared to provide support and reassurance during the dental trauma.
SEX EDUCATION
Many children experience some form of sex play during or before preadolescence as a response to normal curiosity, not as a result of love or sexual urges. Children are experimentalists by nature, and sex play is incidental and transitory. Any adverse emotional consequences or guilt feelings depend on how the behavior is managed by the parents, if it is discovered, or whether children view their actions as wrong in the eyes of significant persons, particularly the parents.
The child’s attitude toward sex is acquired indirectly at an early age. Initial curiosity about differences in body structure between boys and girls and between children and adults arises in the preschool years. Middle childhood is an ideal time for formal sex education, and many authorities believe that the topic is best presented from a life span approach. Information about sexual maturation and the process of reproduction minimizes the child’s uncertainty, embarrassment, and feelings of isolation that often accompany puberty.
An important component of ongoing sex education is effective communication with parents. If parents either repress the child’s sexual curiosity or avoid dealing with it, the sexual information that the child receives may be acquired almost entirely from peers. When peers are the primary source of sexual information, it is transmitted and exchanged in secret conversation and contains a large amount of misinformation.
Nurse’s Role in Sex Education
No matter where nurses practice, they can provide information on human sexuality to both parents and children. To discuss the topic adequately, nurses must have an understanding of the physiologic aspects of sexuality; knowledge of the cultural and societal values; and an awareness of their own attitudes, feelings, and biases about sexuality.
When presenting sexual information to school-age children, nurses should treat sex as a normal part of growth and development. Questions should be answered honestly, matter-of-factly, and to the same extent as questions about other topics. Answers should be at the child’s level of understanding. There may be times when boys and girls should be taught content separately.
Children need help to differentiate sex and sexuality. Exercises on clarifying values, identifying role models, engaging in problem-solving skills, and practicing responsibility are important to prepare children for early adolescence and puberty. In addition, children need explanations of sexual information that is provided via the media or jokes. Information concerning pregnancy; contraceptives; and sexually transmitted diseases, including human immunodeficiency virus and human papillomavirus, should be presented in simple, accurate terms.
Preadolescents need precise and concrete information that will allow them to answer questions such as “What if I start my period in the middle of class?” or “How can I keep people from telling I have an erection?” It is important to tell children what they want to know and what they can expect to happen as they become mature sexually.
During encounters with parents, nurses can be open and available for questions and discussion. They can set an example by the language they use in discussing body parts and their function and by the way in which they deal with problems that have emotional overtones, such as exploratory sex play and masturbation. Parents need help to understand normal behaviors and to view sexual curiosity in their children as a part of the developmental process. Assessing the parents’ level of knowledge and understanding of sexuality provides cues to their need for supplemental information that will prepare them for the increasingly complex explanations they will need to provide as their children grow older.
SCHOOL HEALTH
Child health maintenance is ultimately the responsibility of the parents; however, the public schools and health departments in the United States have contributed to the improvement of child health by providing a healthful school environment, health services, and health education that emphasize sound health practices. Most of these functions constitute major components of community health services and involve large amounts of public funds and large numbers of health professionals, including nurses.
A school health program is involved in ongoing health maintenance through assessment, screening, and referral activities. Routine health services provided by most schools include health appraisal, emergency care, safety education, communicable disease control, counseling, and follow-up care. Health education of school-age children is directed toward providing knowledge of health and influencing habits, attitudes, and conduct in relation to health and injury prevention.
Traditionally, school nurses were viewed as the individuals who detected diseases in the school, applied bandages, and cared for students who were ill or injured. Although these functions remain important parts of the school nurse’s job, the role has expanded considerably in recent years. Today, school nurses manage and coordinate all the care required by regular students and students with special health care needs. In many settings, school health services have enlarged into family health centers that meet the needs of not only school-age children, but also their families and the community. In these settings, school nurse practitioners provide health care that includes assessment of physical, psychomedical, psychoeducational, behavioral, and learning problems, as well as comprehensive well-child care (Hackbarth and Gall, 2005).
The passage of the Education for All Handicapped Children Act and its amendments (Public Laws 94-142 and 99-457) mandated the integration of children with chronic illness or disability into the least restrictive environments, including regular classrooms whenever possible. School nurses are responsible for the medical and nursing needs of these children while they are in the school setting. School nurses develop, implement, and evaluate individualized health care plans for these children. Unfortunately, not all schools have a school nurse, and the use of unlicensed assistive personnel (UAP) is increasing. In many schools, nurses are faced with the task of delegating to and supervising UAP (Potter and Grant, 2004). Delegation and supervision of UAP requires skillful nursing assessment, effective communication, and professional judgment.
INJURY PREVENTION
Because school-age children have developed more refined muscular coordination and control and can apply their cognitive capacities to their behavior, the number of injuries in middle childhood is diminished compared with the number in early childhood. The most common cause of severe injury and death in school-age children is motor vehicle accidents—either as a pedestrian or passenger (Schnitzer, 2006). It is important that nurses continue to emphasize three automobile safety measures that have been found to reduce the severity of injuries: effective car restraint systems, door-lock mechanisms, and appropriate passenger-seating locations in the motor vehicle. The American Academy of Pediatrics advises health professionals and parents that the rear vehicle seat is the safest place for children under the age of 13 years (Durbin, Chen, Smith, and others, 2005).
The school-age child’s desire for riding bicycles increases the risk of injury on streets. Other serious injuries include accidents on skateboards, roller skates, in-line skates, scooters, and other sports equipment. All-terrain vehicles (ATVs), popular with children younger than 16 years of age, are unstable, difficult to handle, and responsible for an increasing number of childhood injuries. The Consumer Product Safety Commission has outlined ATV recommendations that include free driver training, no passengers, use of helmets, no roadway traveling, and adult supervision for children under the age of 16 years (Humphries, Stone, Stapczynski, and others, 2006).
Most injuries occur in or near the home or school. The most effective means of prevention is education of the child and family regarding the hazards of risk taking and the improper use of equipment. Safety helmets, protective eye and mouth shields, and protective padding are strongly recommended for children engaging in active sports, even though they may not be required equipment. Falls from bicycles, ATVs, and skating devices are the cause of a significant number of head injuries in school-age children. Because head injury is the major cause of bicycle-related fatalities, the most important aspect of bicycle safety is to encourage the rider to wear a protective helmet (Fig. 15-9) (Khambalia, MacArthur, and Parkin, 2005).

FIG. 15-9 The right size bike is important; the child should be able to sit on the bike and place the balls of both feet on the ground. The foot should comfortably reach and manipulate the pedal in the down position. Wearing a protective helmet is mandatory. The helmet should be positioned so it sits low on the forehead and parallel to the ground when the head is held upright. It should not rock back and forth or shift from side to side. The strap should fasten securely under the chin.
Always wear a properly fitted bicycle helmet that is approved by the U.S. Consumer Product Safety Commission (CPSC); encourage parents to look for the CPSC approval sticker on the inside liner of the helmet.
Replace a helmet every 5 years or sooner if manufacturer recommends it. Never use a damaged or outgrown helmet.
Ride bicycles with traffic and away from parked cars.
Walk bicycles through busy intersections only at crosswalks.
Give hand signals well in advance of turning or stopping.
Keep as close to the curb as practical.
Watch for drain grates, potholes, soft shoulders, loose dirt, or gravel.
Keep both hands on handlebars, except with signaling.
Never ride double on a bicycle.
Do not carry packages that interfere with vision or control; do not drag objects behind bike.
Watch for and yield to pedestrians.
Watch for cars backing up or pulling out of driveways; be especially careful at intersections.
Look left, right, then left before turning into traffic or roadway.
Never hitch a ride on a truck or other vehicle.
Learn rules of the road and respect for traffic officers.
Wear shoes that fit securely while riding.
Wear light colors at night and attach fluorescent material to clothing and bicycle.
Equip bicycle with proper lights and reflectors.
Be certain the bicycle is the correct size for rider (see Fig. 15-9).
Have bicycle inspected to ensure good mechanical condition.
Children riding as passengers must wear appropriate-size helmets and sit in specially designed protective seats.
Modified from American Academy of Pediatrics, Committee on Injury and Poison Prevention: Bicycle helmets, Pediatrics 108(4):1030-1032, 2001.
Physically active school-age children are also highly susceptible to cuts and abrasions, and the incidence of childhood fractures, strains, and sprains is high. Trampoline injuries are highest in children 5 through 14 years and account for numerous fractures, sprains, and head injuries. Trampolines in the home environment, routine physical education classes, or outdoor playgrounds are not recommended for children of any age (Nysted and Drogset, 2006). Serious injuries are discussed elsewhere in the book: burns (Chapter 30), eye trauma (Chapter 19), near-drowning (Chapter 28), and head injuries (Chapter 28). The prevalence of injuries depends on the dangers present in the environment, the protection offered by adults, and the behavior patterns of the children. Table 15-2 lists characteristics of the school-age child that make them prone to injury and suggestions for injury prevention. Family-Centered Care boxes provide guidelines for bicycle, skateboard, and in-line skate safety and guidance during the school years.
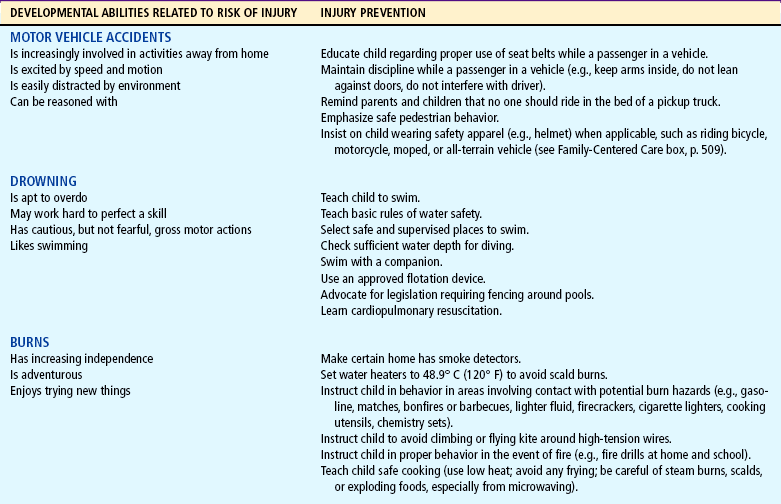
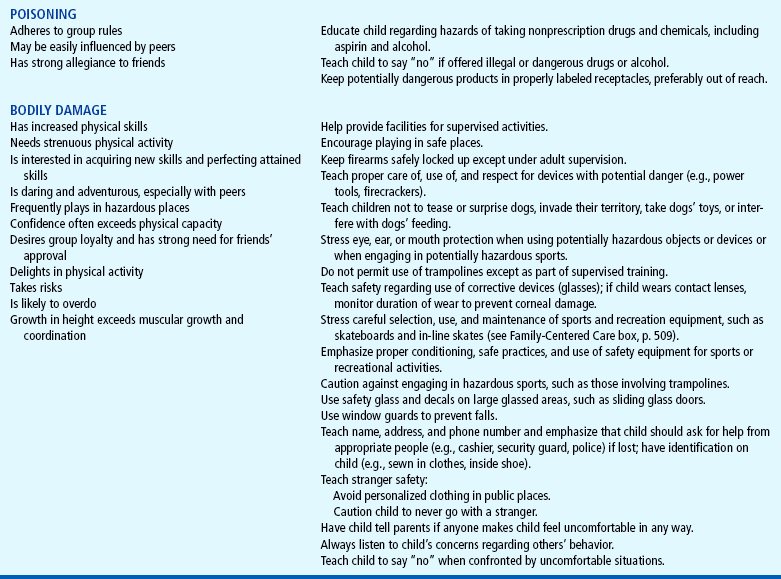
ANTICIPATORY GUIDANCE—CARE OF FAMILIES
Parents of the school-age child must share their child’s time with the increasingly important peer group. Experiences with the peer group prepare school-age children for the broader world of relationships and increased independence from their parents. Parents must learn to provide support as unobtrusively as possible without feeling rejected, hurt, or angry. The nurse can help parents of the school-age child by providing anticipatory guidance and reassurance throughout this period (see Family-Centered Care box).
Skateboard and In-Line Skate Safety
Children younger than 5 years of age should not use skateboards or in-line skates because they are not developmentally prepared to protect themselves from injury. Children ages 6 to 10 years should use these only with close adult supervision.
Children who ride skateboards or in-line skates should wear helmets and other protective equipment, especially on knees, wrists, and elbows, to prevent injury.
Skateboards and in-line skates should never be used near traffic. Their use should be prohibited on streets and highways. Activities that bring skateboards together (e.g., “catching a ride”) are especially dangerous.
Some types of use, such as riding homemade ramps on hard surfaces, may be particularly hazardous.
Data from American Academy of Pediatrics, Committee on Injury and Poison Prevention: Skateboard injuries, Pediatrics 109(3):542-543, 2002; and American Academy of Pediatrics, Committee on Injury and Poison Prevention: In-line skating injuries in children and adolescents, Pediatrics 117(5):1846-1847, 2006.
Prepare parents to expect strong food preferences and frequent refusal of specific food items.
Prepare parents to expect increasingly ravenous appetite.
Prepare parents for emotionality as child experiences erratic mood changes.
Help parents anticipate continued susceptibility to illness.
Teach injury prevention and safety, especially bicycle safety.
Encourage parents to respect child’s need for privacy and to provide a separate bedroom for child, if possible.
Prepare parents for child’s increasing interests outside the home.
Help parents understand the need to encourage child’s interactions with peers.
Prepare parents to expect improvement in health with fewer illnesses, but warn them that allergies may increase or become apparent.
Prepare parents to expect an increase in minor injuries.
Emphasize caution in selecting and maintaining sports equipment and reemphasize safety.
Prepare parents to expect increased involvement with peers and interest in activities outside the home.
Emphasize the need to encourage independence while maintaining limit setting and discipline.
Prepare mothers to expect more demands at 8 years.
Prepare fathers to expect increasing admiration at 10 years; encourage father-child activities.
Help parents prepare child for body changes of pubescence.
Prepare parents to expect a growth spurt in girls.
Make certain child’s sex education is adequate with accurate information.
Prepare parents to expect energetic but stormy behavior at 11 years, becoming more even-tempered at 12 years.
Encourage parents to support child’s desire to “grow up” but to allow regressive behavior when needed.
Prepare parents to expect an increase in child’s masturbation.
Instruct parents that the amount of rest the child needs may increase.
Help parents educate child regarding experimentation with potentially harmful activities.
Help parents understand the importance of regular health and dental care for the child.
Encourage parents to teach and model sound health practices, including diet, rest, activity, and exercise.
Stress the need to encourage children to engage in appropriate physical activities.
Emphasize providing a safe physical and emotional environment.
Middle childhood, also known as the school years, is the period of life that extends from 6 to 12 years of age.
Although growth is slower than in previous years, there is a steady gain in height and weight, with maturation of body systems; primary teeth are lost and replaced by permanent teeth.
A major task during the middle school years is developing a sense of industry or accomplishment (Erikson).
Piaget’s period of concrete operations refers to the school-age period, when children are able to use their thought processes to experience events and actions and make judgments based on reasoning.
The child develops a conscience and is able to understand and adhere to rules and standards set by others.
Entertaining different points of view, becoming sensitive to social norms, and forming peer friendships are important features of social development during the school years.
Cooperative play, team activities, and the acquisition of skills are prime elements of play during the school years; rules and rituals assume greater importance.
Parental concerns during middle childhood include lying, cheating, stealing, and school achievement.
The availability of junk foods, irregular family meals, and schedules of working parents often interfere with optimal nutrition.
Dental care is important during this time; potential dental problems include caries, periodontal disease, malocclusion, and dental injury.
Increased socialization and media exposure make the school years an ideal time for sex education.
School health programs ideally include health appraisal, emergency care, safety education, communicable disease control, counseling, guidance, and health education with adjustment to individual student needs.
Injury prevention is directed toward safety education, provision of safe play areas and equipment, and well-supervised sports activities.
References
American Academy of Pediatrics, Pediatrics Collaborative Care Program. Oral health risk assessment training for pediatricians and other child health professionals. Rockville, Md: National Institutes of Health, 2000.
Ateah, CA. Disciplinary practices with children: parental sources of information, attitudes, and educational needs. Issues Compr Pediatr Nurs. 2003;26:89–101.
Carno, MA, Hoffman, LA, Carcillo, JA, et al. Developmental stages of sleep from birth to adolescence, common childhood sleep disorders: overview and nursing implications. J Pediatr Nurs. 2003;18(4):274–283.
Dishion, TJ, Nelson, SE, Yasui, M. Predicting early adolescent gang involvement from middle school adaptation. J Clin Child Adolesc Psychol. 2005;34(1):62–73.
Durbin, DR, Chen, I, Smith, R, et al. Effects of seating position and appropriate restraint use on the risk of injury to children in motor vehicle crashes. Pediatrics. 2005;115(3):305–309.
Glew, GM, Fan, MY, Katon, W, et al. Bullying, psychosocial adjustment, and academic performance in elementary school. Arch Pediatr Adolesc Med. 2005;159:1026–1031.
Hackbarth, D, Gall, GB. Evaluation of school-based health center programs and services: the whys and hows of demonstrating program effectiveness. Nurs Clin North Am. 2005;40(4):711–724.
Humphries, RL, Stone, CK, Stapczynski, JS, et al. An assessment of pediatric all-terrain vehicle injuries. Pediatr Emerg Care. 2006;22(7):491–494.
Khambalia, A, MacArthur, C, Parkin, PC. Peer and adult companion helmet use is associated with bicycle helmet use by children. Pediatrics. 2005;116(4):939–942.
Krause-Parello, CA. Tooth avulsion in the school setting. J School Nurs. 2005;21(5):279–282.
Lyznicki, JM, McCaffree, MA, Robinowitz, CB. Childhood bullying: implications for physicians. Am Fam Physician. 2004;70(9):1723–1728.
Mortweet, SL, Christophersen, E. Coping skills for the angry/impatient/clamorous child: a home/office practicum. Contemp Pediatr. 2004;21(6):43–45.
Nansel, TR, Overpeck, MD, Haynie, DL, et al. Relationships between bullying and violence among US youth. Arch Pediatr Adolesc Med. 2003;157(4):348–353.
Nysted, M, Drogset, JO. Trampoline injuries. Br J Sports Med. 2006;40:984–987.
Potter, P, Grant, E. Understanding RN and unlicensed assistive personnel working relationships in designing care delivery strategies. J Nurs Admin. 2004;34(1):19–24.
Ryan-Wenger, NA, Sharrer, VW, Campbell, KK. Changes in children’s stressors over the past 30 years. Pediatr Nurs. 2005;31(4):282–288.
Schnitzer, PG. Prevention of unintentional childhood injuries. Am Fam Physician. 2006;74(11):1864–1869.
Sharrer, VW, Ryan-Wenger, NA. School-age children’s self-reported stress symptoms. Pediatr Nurs. 2002;28(1):21–27.
Vessey, JA, Carlson, K, David, J. Helping children who are being teased and bullied. Nurs Spectrum. 2003;13:16–18.
Vreeman, RC, Carroll, AE. A systematic review of school-based interventions to prevent bullying. Arch Pediatr Adolesc Med. 2007;161(1):78–88.