Communication and Physical Assessment of the Child
GUIDELINES FOR COMMUNICATION AND INTERVIEWING
GENERAL APPROACHES TOWARD EXAMINING THE CHILD
On completion of this chapter the reader will be able to:
 Identify communication strategies for interviewing parents.
Identify communication strategies for interviewing parents.
Formulate guidelines for using an interpreter.
Identify communication strategies for communicating with children of different age-groups.
Describe four communication techniques that are useful with children.
State the components of a complete health history.
List three areas that are evaluated as part of nutritional assessment.
Prepare a child for a physical examination based on his or her developmental needs.
Perform a comprehensive physical examination in a sequence appropriate to the child’s age.
Recognize expected normal findings for children at various ages.
Record the physical examination according to the head-to-toe format.
RELATED TOPICS and ADDITIONAL RESOURCES
 IN TEXT
IN TEXTAltered States of Consciousness, Ch. 28
Assessment of Cardiac Function, Ch. 25
Biologic Development (Adolescents), Ch. 16
Dental Problems, Ch. 15
Family Structure and Function, Ch. 3
Hearing Impairment; Visual Impairment, Ch. 19
Idiopathic Scoliosis, Ch. 31
Immunizations, Ch. 10
Neurologic Examination, Ch. 28
Pain Assessment, Ch. 7
Physical Assessment (Newborn), Ch. 8
Preparation for Diagnostic and Therapeutic Procedures, Ch. 22
Sex Education: Preschooler, Ch. 13; School-Age Child, Ch. 15; Adolescent, Ch. 16
Sexually Transmitted Diseases, Ch. 17
Skin Lesions, Ch. 30
Social, Cultural, and Religious Influences on Child Health Promotion, Ch. 4
Systemic Hypertension, Ch. 25
Use of Play in Procedures, Ch. 22
GUIDELINES FOR COMMUNICATION AND INTERVIEWING
The most widely used method of communicating with parents on a professional basis is the interview process. Unlike social conversation, interviewing is a specific form of goal-directed communication. As nurses converse with children and adults, they focus on the individuals to determine the kind of persons they are, their usual mode of handling problems, whether help is needed, and the way they react to counseling. Developing interviewing skills requires time and practice, but following some guiding principles can facilitate this process. An organized approach is most effective when using interviewing skills in patient teaching.
ESTABLISHING A SETTING FOR COMMUNICATION
Introduce yourself to, and ask the name of, each family member who is present. Address parents or other adults by their appropriate titles, such as “Mr.” and “Mrs.,” unless they specify a preferred name. Record the preferred name on the medical record. Using formal address or their preferred names, rather than using first names or “mother” or “father,” conveys respect and regard for the parents or other caregivers (Seidel, Ball, Dains, and others, 2003).
At the beginning of the visit, include children in the interaction by asking them their name, age, and other information. Nurses often direct all questions to adults, even when children are old enough to speak for themselves. This serves to terminate one extremely valuable source of information: the patient. When the child is included, follow the general rules for communicating with children given in the Nursing Care Guidelines box on p. 103.
Explain to interpreter the reason for the interview and the type of questions that will be asked.
Clarify whether a detailed or brief answer is required and whether the translated response can be general or literal.
Introduce interpreter to family and allow some time before the interview for them to become acquainted.
Communicate directly with family members when asking questions to reinforce interest in them and to observe nonverbal expressions, but do not ignore interpreter.
Pose questions to elicit only one answer at a time, such as ‘Do you have pain?’ rather than ‘Do you have any pain, tiredness, or loss of appetite?’
Refrain from interrupting family member and interpreter while they are conversing.
Avoid commenting to interpreter about family members, since they may understand some English.
Be aware that some medical words, such as allergy, may have no similar word in another language; avoid medical jargon whenever possible.
Be aware that cultural differences may exist regarding views on sex, marriage, or pregnancy.
Allow time after the interview for interpreter to share something that he or she thought could not be said earlier; ask about the interpreter’s impression of nonverbal clues to communication and family members’ reliability or ease in revealing information.
Arrange for family to speak with same interpreter on subsequent visits whenever possible.
Assurance of Privacy and Confidentiality
The place where the interview is conducted is almost as important as the interview itself. The physical environment should allow for as much privacy as possible, with distractions, such as interruptions, noise, or other visible activity, kept to a minimum. At times it is necessary to turn off a television or radio. The environment should also have some play provision for young children to keep them occupied during the parent-nurse interview (Fig. 6-1). Parents who are constantly interrupted by their children are unable to concentrate fully and tend to give brief answers to finish the interview as quickly as possible.

Confidentiality is another essential component of the initial phase of the interview. Since the interview is usually shared with other members of the health team care or the teacher (in the case of students), be certain to inform the family of the limits regarding confidentiality. If confidentiality is a concern in a particular situation, such as when talking to a parent suspected of child abuse or a teenager contemplating suicide, deal with this directly and inform the person that in such instances confidentiality cannot be ensured. However, the nurse judiciously protects information of a confidential nature (Sullivan, 1997).
COMPUTER PRIVACY AND APPLICATIONS IN NURSING
The use of computer technology to store and retrieve health information has become widespread. The privacy and security of this health information has generated a growing concern throughout the health care community. Any person accessing confidential health information is charged with managing safeguards for disclosure, since violations might incur civil damages.
In 1994 a committee of the Institute of Medicine recommended a national code of fair health information practices. It suggested that health data organizations establish data protection units to develop privacy policies and security practices for manual and automated data processing systems. Technologic safeguards, such as encryption and managerial security procedures, can be applied to computer hardware across a network to ensure protection of individual patient privacy.
Many institutions use computer and information applications in nursing (nursing informatics), such as electronic medical records, to record care and access information. Two important health care applications are record transmission, including facsimile (fax), electronic mail (e-mail), and telemedicine. The telemedicine application is capable of two-way video conferencing, transmission of radiographs, and clinical consultation between remote sites and centralized resources.*
TELEPHONE TRIAGE AND COUNSELING
Nurses are increasingly responsible for assessment of children’s symptoms and clinical judgment for further medical care (triage) via telephone report. Most often, health problems are assessed and prioritized according to urgency, and treatment is judiciously provided via telephone services. Successful outcomes are based on the consistency and accuracy of the information provided, and parents are empowered to participate in their child’s medical care. Telephone triage care management has increased access to high-quality health care services, and patient satisfaction has significantly improved. Unnecessary emergency department and clinic visits have decreased, saving medical costs and time (with less absence from work) for families in need of health care. The most common telephone triage call is for a fever. Approximately 37% of the triage calls related to fever require emergency care, and nearly 50% benefit from home management (Deadrick and Boggess, 1996).
A well-designed telephone triage program is essential for safe, prompt, and consistent-quality health care (Rutenberg, 2000). Telephone triage is more than ‘just a phone call,’ since a child’s life is a high price to pay for poorly managed or incompetent telephone assessment skills. Typically, guidelines for telephone triage include asking screening questions; determining when to immediately refer to emergency medical services (dial 911); and determining when to refer to same-day appointments, appointments in 24 to 72 hours, appointments in 4 days or more, or home care (Box 6-1).
COMMUNICATING WITH FAMILIES
Although the parent and child are separate and distinct individuals, the nurse’s relationship with the child is frequently mediated by the parent, particularly in the case of younger children. For the most part, information about the child is acquired by direct observation or is communicated to the nurse by the parents. Usually it can be assumed that because of the close contact with the child, the parent gives reliable information. Making an assessment of the child requires input from the child (verbal and nonverbal), information from the parent, and the nurse’s own observations of the child and interpretation of the relationship between the child and the parent. Counseling and guidance must be directed to the care giver of infants and small children; when children are old enough to be active participants in their own health maintenance, the parent becomes a collaborator in health care.
Encouraging the Parent to Talk
Interviewing parents not only offers the opportunity to determine the child’s health and developmental status, but also offers information about factors that influence the child’s life. Whatever the parent sees as a problem should be a concern of the nurse. These problems are not always easy to identify. Nurses need to be alert for clues and signals by which a parent communicates worries and anxieties. Careful phrasing with broad, open-ended questions such as “What is Jimmy eating now?” provides more information than several single-answer questions, such as “Is Jimmy eating what the rest of the family eats?”
Sometimes the parent will take the lead without prompting. At other times it may be necessary to direct another question on the basis of an observation, such as “Connie seems unhappy today” or “How do you feel when David cries?” If the parent appears to be tired or distraught, consider asking, “What do you do to relax?” or “What help do you have with the children?” A comment such as “You handle the baby very well. What kinds of experience have you had with babies?” to new parents who appear comfortable with their first child gives positive reinforcement and provides an opening for any questions they might have regarding the infant’s care. Often all that is required to keep parents talking is a nod or saying “yes” or “uh-huh.”
When attempting to elicit feelings and covert problem areas, avoid closed-ended questions that begin with “Does …,” “Did …,” or “Is …,” which usually require only a single response. In addition, asking questions such as “Does your son have any problems at school?” subtly implies a lack of parental skills and evokes defensiveness. Instead, say, “What …,” “How …,” “Tell me about …” and encourage elaboration with “You were saying …” or “You say that …,” or by reflecting back a key word. Open-ended questions are nonthreatening and encourage description.
Directing the Focus
The ability to direct the focus of the interview while allowing for maximum freedom of expression is one of the most difficult goals in effective communication. One approach is the use of open-ended or broad questions, followed by guiding statements. For example, if the parent proceeds to list the other children by name, say, “Tell me their ages, too.” If the parent continues to describe each child in depth, which is not the purpose of the interview, redirect the focus by stating, “Let’s talk about the other children later. You were beginning to tell me about Paul’s activities at school.” This approach conveys interest in the other children but focuses the assessment on the patient.
If a parent suggests that a problem exists with one of the other children, reintroduce this subject at the end of the interview to assess the need for further family follow-up. Saying to the parent, “Before, you mentioned that your older son is having trouble in school. Tell me what you see as the problem,” reintroduces this subject but only in terms of the possible problem.
Listening and Cultural Awareness
Listening is the most important component of effective communication. When listening is truly aimed at understanding the client, it is an active process that requires concentration and attention to all aspects of the conversation—verbal, nonverbal, and abstract. Major blocks to listening are environmental distraction and premature judgment.
The nurse’s attitudes and feelings are easily injected into an interview. Often nurses’ perceptions of a parent’s behavior are influenced by their own perceptions, prejudices, and assumptions, which may include racial, religious, and cultural stereotypes. What may be interpreted as passive hostility or a lack of interest in a parent may be shyness or an expression of anxiety. For example, in Western cultures eye contact and directness are signs of paying attention. However, in many non-Western cultures, including that of Native Americans, directness, such as looking someone in the eye, is considered rude. Children are taught to avert their gaze and to look down when being addressed by an adult, especially one with authority (Seidel, Ball, Dains, and others, 2003). Therefore judgments about “listening,” as well as verbal interactions, need to be made with an appreciation of cultural differences (see Nursing Care Guidelines box, p. 62, and Chapter 3).
Although it is necessary to make some preliminary judgments, listen with as much objectivity as possible by clarifying meanings and attempting to see the situation from the parent’s point of view. Effective interviewers consciously control their reactions, responses, and the techniques they use.
Minimum verbal activity with active listening facilitates parent involvement. It is tempting to spend time explaining, describing, and interpreting health information when the op portunity presents itself. However, it is possible to provide effective health education by timing the information properly and presenting only as much as is necessary at the moment.
Careful listening facilitates the use of clues, verbal leads, or signals from the interviewee to move the interview along. Frequent references to an area of concern, repetition of certain key words, or a special emphasis on something or someone serves as cues to the interviewer for the direction of inquiry. Concerns and anxieties are often mentioned in a casual, off hand manner. Even though they are casual, they are important and deserve careful scrutiny to identify problem areas. For example, a parent who is concerned about a child’s habit of bed-wetting may casually mention that the child’s bed was “wet this morning.”
Listening is also helpful in assessing reliability. For example, the answers elicited at the beginning of the interview may differ from those at the end, when the parent feels more confident in revealing problems. It is important to identify any discrepancies and reintroduce those topics for further investigation.
Using Silence
Silence as a response is often one of the most difficult interviewing techniques to learn. It requires a sense of confidence and comfort on the part of the interviewer to allow the interviewee space in which to think without interruptions. Silence permits the interviewee to sort out thoughts and feelings and search for responses to questions. Silence can also be a cue for the interviewer to go more slowly, reexamine the approach, and not push too hard (Seidel, Ball, Dains, and others, 2003).
Sometimes it is necessary to break the silence and reopen communication. Do this in a way that encourages the person to continue talking about what is considered important. Breaking a silence by introducing a new topic or by prolonged talking essentially terminates the interviewee’s opportunity to use the silence. Suggestions for breaking the silence include statements such as “Is there anything else you wish to say?” “I see you find it difficult to continue; how may I help?” or “I don’t know what this silence means. Perhaps there is something you would like to put into words but find difficult to say.”
Being Empathic
Empathy is the capacity to understand what another person is experiencing from within that person’s frame of reference; it is often described as the ability to put oneself in another’s shoes. The essence of empathic interaction is accurate understanding of another’s feelings (Price and Archbold, 1997; White, 1997; Reynolds, Scott, and Jessiman, 1999). Empathy differs from sympathy, which is having feelings or emotions in common with another person, rather than understanding those feelings. Sympathy is not therapeutic in the helping relationship because it leads to overinvolvement emotionally and potentially to professional burnout (Yegdich, 1999).
Providing Anticipatory Guidance
The ideal way to handle a situation is to deal with it before it becomes a problem. The best preventive measure is anticipatory guidance. Traditionally, anticipatory guidance has focused on providing families information on normal growth and development, as well as nurturing childrearing practices. For example, one of the most significant areas in pediatrics is injury prevention. Beginning prenatally, parents need specific instructions on home safety. Because of the child’s maturing developmental skills, home safety changes must be implemented early to minimize risks to the child.
Many normal developmental changes can disturb unprepared parents, such as a toddler’s diminished appetite, negativism, altered sleeping patterns, and anxiety toward strangers. Such topics are discussed in the chapters on health promotion to provide the nurse with information for counseling parents.
However, anticipatory guidance should extend beyond giving information to empowering families to use the information as a means of building competence in their parenting abilities. To achieve this level of anticipatory guidance (Desselle and Pearlmutter, 1997), the nurse should:
Avoiding Blocks to Communication
A number of blocks to communication can adversely affect the quality of the helping relationship. Many of these blocks are initiated by the interviewer, such as giving unrestricted advice or forming prejudged conclusions. Another type of block occurs primarily with the interviewees and concerns information overload. When individuals are presented with too much information or information that is overwhelming, they will often demonstrate signs of increasing anxiety or decreasing attention. Such signals should alert the interviewer to give less information or to clarify what has been said. Some of the more common blocks to communication, including signs of information overload, are listed in Box 6-2.
Communication blocks can be corrected by careful analysis of the interview process. One of the best methods for improving interviewing skills is audiotape or videotape feedback. With supervision and guidance, the interviewer can recognize the blocks and consciously avoid them.
Communicating with Families Through an Interpreter
Sometimes communication is impossible because two people speak different languages. In this case it is necessary to obtain information through a third party, the interpreter. When an interpreter is used, the same interviewing guidelines apply. Specific guidelines for using an adult interpreter are presented in the Nursing Care Guidelines box.
Communicating with families through an interpreter requires sensitivity to cultural, legal, and ethical considerations. For example, in some cultures using a child as an interpreter is considered an insult to an adult because children are expected to show respect by not questioning their elders. In some cultures class differences between the interpreter and the family may cause the family to feel intimidated and less inclined to offer information. Therefore it is important to choose the translator carefully and provide time for the interpreter and family to establish rapport.
Issues of legal and ethical concerns may also arise. For example, in obtaining informed consent through an interpreter, it is important that the family be fully informed of all aspects of the particular procedure to which they are consenting. Issues of confidentiality may arise when family members related to another patient are asked to interpret for the family, thus revealing sensitive information that may be shared with other families on the unit. With increased sensitivity toward patient rights and confidentiality, many institutions now require consent forms to be produced in the patient’s primary language.
When no one else is available to translate, children within the family are often asked to assume this role. In this situation it is important to stress literal translation of parent responses. To ensure correct translations, it may be necessary to interrupt the parent and ask the child to translate every few sentences. When using children as interpreters, ask questions directed at specific answers and assess the interpreted translation in terms of nonverbal expressions of communication. It should be noted that some institutions prohibit or discourage the use of children as interpreter; check institutional policy for compliance.
COMMUNICATING WITH CHILDREN
Although the greatest amount of verbal communication is usually carried out with the parent, do not exclude the child during the interview. Pay attention to infants and younger children through play or by occasionally directing questions or remarks to them. Include older children as active participants.
In communication with children of all ages, the nonverbal components of the communication process convey the most significant messages. It is difficult to disguise feelings, attitudes, and anxiety when relating to children. They are alert to surroundings and attach meaning to every gesture and move that is made; this is particularly true of very young children.
Active attempts to make friends with children before they have had an opportunity to evaluate an unfamiliar person tend to increase their anxiety. It is helpful to continue to talk to the child and parent but go about activities that do not involve the child directly, thus allowing the child to observe from a safe position. If the child has a special toy or doll, “talk” to the doll first. Ask simple questions such as “Does your teddy bear have a name?” to ease the child into conversation. Other guidelines for communicating with children are presented in the Nursing Care Guidelines box. Specific guidelines for preparing children for procedures, a common nursing function, are discussed in Chapter 22.
Communication Related to Development of Thought Processes
The normal development of language and thought offers a frame of reference for communicating with children. Thought processes progress from sensorimotor to perceptual to concrete and finally to abstract, formal operations. The early social communicative development of children has been divided into three stages: (1) perlocutionary stage—unintentional communication behavior; (2) illocutionary stage—true intent in communication efforts; and (3) locutionary stage—intentional communication behaviors and use of symbols (Hoge and Parette, 1995). An understanding of the typical characteristics of these stages provides the nurse with a framework to facilitate social communication (Box 6-3).
Infancy.: Because they are unable to use words, infants primarily use and understand nonverbal communication. Infants communicate their needs and feelings through nonverbal behaviors and vocalizations that can be interpreted by someone who is around them for a sufficient time. Infants smile and coo when content and cry when distressed. Crying is provoked by unpleasant stimuli from inside or outside, such as hunger, pain, body restraint, or loneliness. Adults interpret this to mean that an infant needs something and consequently try to alleviate the discomfort and reduce tension. Crying (or the desire to cry) persists as a part of everyone’s communication repertoire.
Infants respond to adults’ nonverbal behaviors. They become quiet when they are cuddled, are patted, or receive other forms of gentle physical contact. They derive comfort from the sound of a voice, even though they do not understand the words that are spoken. Until infants reach the age at which they experience stranger anxiety, they readily respond to any firm, gentle handling and quiet, calm speech. Loud, harsh sounds and sudden movements are frightening.
Older infants’ attention is centered on themselves and their parents; therefore any stranger is a potential threat until proved otherwise. Holding out the hands and asking the child to “come” is seldom successful, especially if the infant is with the parent. If infants must be handled, simply pick them up firmly without gestures. Observe the position in which the parent holds the infant. Most infants learn to prefer a particular position and manner of handling. In general, infants are more at ease upright than horizontal. Also, hold infants so they can see their parents. Until they develop the understanding that an object (in this case the parent) removed from sight can still be present, they have no way of knowing the object is still there.
Early Childhood.: Children younger than 5 years of age are egocentric. They see things only in relation to themselves and from their point of view. Therefore, focus communication on them. Tell them what they can do or how they will feel. Experiences of others are of no interest to them. It is futile to use another child’s experience in an attempt to gain the cooperation of small children. Allow them to touch and examine articles that will come in contact with them. A stethoscope bell will feel cold; palpating a neck might tickle. Although they have not yet acquired sufficient language skills to express their feelings and wants, toddlers are able to communicate effectively with their hands to transmit ideas without words. They push an unwanted object away, pull another person to show them something, point, and cover the mouth that is saying something they do not wish to hear.
Everything is direct and concrete to small children. They are unable to work with abstractions and interpret words literally. Analogies escape them because they are unable to separate fact from fantasy. For example, they attach literal meaning to such common phrases as “two-faced,” “sticky fingers,” or “coughing your head off.” Children who are told they will get “a little stick in the arm” may not be able to envision an injection (Fig. 6-3). Therefore, avoid using a phrase that might be misinterpreted by a small child (see Nursing Care Guidelines box, Chapter 22, p. 693).
Allow children time to feel comfortable.
Avoid sudden or rapid advances, broad smiles, extended eye contact, or other gestures that may be seen as threatening.
Talk to the parent if child is initially shy.
Communicate through transition objects such as dolls, puppets, and stuffed animals before questioning a young child directly.
Give older children the opportunity to talk without the parents present.
Assume a position that is at eye level with child (Fig. 6-2).

Speak in a quiet, unhurried, and confident voice.
Speak clearly, be specific, and use simple words and short sentences.
State directions and suggestions positively.
Offer a choice only when one exists.

Young children assign human attributes to inanimate objects. Consequently they fear that objects may jump, bite, cut, or pinch all by themselves. Children do not know that these devices are unable to perform without human direction. To minimize their fear, keep unfamiliar equipment out of view until it is needed.
School-Age Years.: Younger school-age children rely less on what they see and more on what they know when faced with new problems. They want explanations and reasons for everything but require no verification beyond that. They are interested in the functional aspect of all procedures, objects, and activities. They want to know why an object exists, why it is used, how it works, and the intent and purpose of its user. They need to know what is going to take place and why it is being done to them specifically. For example, to explain a procedure such as taking blood pressure, show the child how squeezing the bulb pushes air into the cuff and makes the “silver” in the tube go up. Let the child operate the bulb. An explanation for the procedure might be as simple as, “I want to see how far the silver goes up when the cuff squeezes your arm.” Consequently, the child becomes an enthusiastic participant.
School-age children have a heightened concern about body integrity. Because of the special importance they place on their body, they are sensitive to anything that constitutes a threat or suggestion of injury to it. This concern extends to their possessions, so that they may appear to overreact to loss or threatened loss of treasured objects. Helping children voice their concerns enables the nurse to provide reassurance and to implement activities that reduce their anxiety. For example, if a shy child dislikes being the center of attention, ignore that particular child by talking and relating to other children in the family or group. When children feel more comfortable, they will usually interject personal ideas, feelings, and interpretations of events.
Older children have an adequate and satisfactory use of language. They still require relatively simple explanations, but their ability to think concretely can facilitate communication and explanation. Commonly, they have sufficient experience with health and health care workers to understand what is transpiring and what is generally expected of them.
Adolescence.: As children move into adolescence, they fluctuate between child and adult thinking and behavior. They are riding a current that is moving them rapidly toward a maturity that may be beyond their coping ability. Therefore, when tensions rise, they may seek the security of the more familiar and comfortable expectations of childhood. Anticipating these shifts in identity allows the nurse to adjust the course of interaction to meet the needs of the moment. No single approach can be relied on consistently, and encountering cooperation, hostility, anger, bravado, and a variety of other behaviors and attitudes can be expected. It is as much a mistake to regard the adolescent as an adult with an adult’s wisdom and control as it is to assume that the teenager has the concerns and expectations of a child.
Frequently adolescents are more willing to discuss their concerns with an adult outside the family, and they often welcome the opportunity to interact with a nurse outside the presence of their parents. They are accepting of anyone who displays a genuine interest in them. However, adolescents are quick to reject persons who attempt to impose their values on them, whose interest is feigned, or who appear to have little respect for who they are and what they think or say.
Interviewing the adolescent presents some special issues. The first may be whether to talk with the adolescent alone or with the adolescent and parents together. Of course, if the parent is not there, the only question is whether to suggest to the teenager that the parents be interviewed at another time. If the parents and teenager are together, talking with the adolescent first has the advantage of immediately identifying with the young person, thus fostering the interpersonal relationship. However, talking with the parents initially may provide insight into the family relationship. In either case, give both parties an opportunity to be included in the interview. If time constraints are important, such as during history taking, clarify these at the onset to avoid appearing to “take sides” by talking more with one person than with the other.
Confidentiality is of great importance when interviewing adolescents. Explain to parents and teenagers the limits of confidentiality, specifically that young persons’ disclosures will not be shared unless they indicate a need for intervention, as in the case of suicidal behavior.
Another dilemma in interviewing adolescents is that two views of a problem frequently exist–the teenager’s and the parents’. Clarification of the problem is a major task. However, providing both parties an opportunity to discuss their perceptions in an open and unbiased atmosphere can, by itself, be therapeutic. Demonstrating positive communication skills can help families communicate more effectively (see Nursing Care Guidelines box).
COMMUNICATION TECHNIQUES
In addition to such conventional interviewing methods as reflection and open-ended questions, a number of techniques encourage family members to express their thoughts and feelings in a less directive and confrontational manner. Several approaches are projective—they present nonspecific material that enables individuals to externalize or project inner aspects of themselves to others.
A variety of verbal techniques can be used to encourage communication. Some of these techniques can be used to pose questions or explore concerns in a less threatening manner. Others can be presented as “word games,” which are often well received by children. However, for many children and adults, talking about feelings is difficult, and verbal communication may be more stressful than supportive. In such instances several nonverbal techniques can be used to encourage communication.
Both verbal and nonverbal techniques are described in Box 6-4. Because of the importance of play in communicating with children, play is discussed more extensively below. Any of the verbal or nonverbal techniques can give rise to strong feelings that surface unexpectedly. Be prepared to handle them or to recognize when issues go beyond your ability to deal with them. At that point, consider an appropriate referral.
BOX 6-4 Creative Communication Techniques with Children
Relate a feeling about a behavior in terms of “I.”
Describe effect behavior had on the person.
Express a feeling in terms of a third person (“he,” “she,” “they”). This is less threatening than directly asking children how they feel because it gives them an opportunity to agree or disagree without being defensive.
Example—“Sometimes when a person is sick a lot, he feels angry and sad because he cannot do what others can.” Either wait silently for a response or encourage a reply with a statement such as “Did you ever feel that way?”
Approach allows children three choices: (1) to agree and, one hopes, express how they feel; (2) to disagree; or (3) to remain silent, which means they probably have such feelings but are unable to express them at this time.
Listen carefully and reflect back to patients the feelings and content of their statements.
Responses are empathic and nonjudgmental and legitimize the person’s feelings.
Formula for facilitative responses: “You feel ____________ because ____________.”
Use the language of children to probe into areas of their thinking while bypassing conscious inhibitions or fears.
The simplest technique is asking children to relate a story about an event, such as “being in the hospital.”
Reveal child’s thinking and attempt to change child’s perceptions or fears by retelling a somewhat different story (more therapeutic approach than storytelling).
Begin by asking child to tell a story about something, then tell another story that is similar to child’s tale but with differences that help child in problem areas.
Example—Child’s story is about going to the hospital and never seeing his or her parents again. Nurse’s story is also about a child (using different names but similar circumstances) in a hospital whose parents visit every day, but in the evening after work, until the child is better and goes home with them.
Use books in a therapeutic and supportive process.
Provide children with an opportunity to explore an event that is similar to their own but sufficiently different to allow them to distance themselves from it and remain in control.
General guidelines for using bibliotherapy are:
1. Assess child’s emotional and cognitive development in terms of readiness to understand the book’s message.
2. Be familiar with the book’s content (intended message or purpose) and the age for which it is written.
3. Read the book to the child if child is unable to read.
4. Explore the meaning of the book with the child by having child:
Dreams often reveal unconscious and repressed thoughts and feelings.
Ask, “If you could have any three things in the world, what would they be?”
If child answers, “That all my wishes come true,” ask child for specific wishes.
State key words and ask children to say the first word they think of when they hear the word.
Start with neutral words and then introduce more anxiety-producing words, such as “illness,” “needles,” “hospitals,” and “operation.”
Select key words that relate to some relevant event in the child’s life.
Present a partial statement and have the child complete it. Some sample statements are:
The thing I like best (least) about school is _________.
The best (worst) age to be is _________.
The most (least) fun thing I ever did was ___________.
The thing I like most (least) about my parents is _________.
The one thing I would change about my family is __________.
Writing is an alternative communication approach for older children and adults.
Write down feelings or thoughts that are difficult to express.
Write “letters” that are never mailed (a variation is making up a “pen pal” to write to).
Keep an account of child’s progress from both a physical and an emotional viewpoint.
Drawing is one of the most valuable forms of communication—both nonverbal (from looking at the drawing) and verbal (from child’s story of the picture).
Children’s drawings tell a great deal about them because they are projections of their inner selves.
Spontaneous drawing involves giving child a variety of art supplies and providing the opportunity to draw.
Directed drawing involves a more specific direction, such as “draw a person” or the “three themes” approach (state three things about child and ask child to choose one and draw a picture).
Guidelines for Evaluating Drawings
Use spontaneous drawings and evaluate more than one drawing whenever possible.
Interpret drawings in light of other available information about child and family, including the child’s age and stage of development.
Interpret drawings as a whole rather than focusing on specific details of the drawing.
Consider individual elements of the drawing that may be significant:
Sex of figure drawn first—Usually relates to child’s perception of own sex role.
Size of individual figures—Expresses importance, power, or authority.
Order in which figures are drawn—Expresses priority in terms of importance.
Child’s position in relation to other family members—Expresses feelings of status or alliance.
Exclusion of a member—May denote feeling of not belonging or desire to eliminate.
Accentuated parts—Usually express concern for areas of special importance (e.g., large hands may be a sign of aggression).
Absence of or rudimentary arms and hands—Suggest timidity, passivity, or intellectual immaturity; tiny, unstable feet may express insecurity, and hidden hands may mean guilt feelings.
Placement of drawing on the page and type of stroke—Free use of paper and firm, continuous strokes express security, whereas drawings restricted to a small area and lightly drawn in broken or wavering lines may be a sign of insecurity.
Erasures, shading, or cross-hatching—Expresses ambivalence, concern, or anxiety with a particular area.
Use simple magic tricks to help establish rapport with child, encourage compliance with health interventions, and provide effective distraction during painful procedures.
Although the “magician” talks, no verbal response from child is required.
Play is the universal language and “work” of children.
It tells a great deal about children because they project their inner selves through the activity.
Spontaneous play involves giving child a variety of play materials and providing the opportunity to play.
Directed play involves a more specific direction, such as providing medical equipment or a dollhouse for focused reasons, such as exploring child’s fear of injections or exploring family relationships.
Play
Play is a universal language of children. It is one of the most important forms of communication and can be an effective technique in relating to them. Clues about physical, intellectual, and social developmental progress can often be gleaned from the form and complexity of a child’s play behaviors. Play requires minimum equipment or none at all. Therapeutic play is often used to reduce the trauma of illness and hospitalization (see Chapter 21) and to prepare children for therapeutic procedures (see Chapter 22).
Because their ability to perceive precedes their ability to transmit, infants respond to activities that register on their senses. Patting, stroking, and other skin play conveys messages. Repetitive actions, such as stretching infants’ arms out to the side while they are lying on their back and then folding the arms across the chest or raising and revolving the legs in a bicycling motion, will elicit pleasurable sounds. Colorful items to catch the eye or interesting sounds, such as a ticking clock, chimes, bells, or singing, can be used to attract children’s attention.
Older infants respond to simple games. The old game of peek-a-boo is an excellent means of initiating communication with infants while maintaining a “safe,” nonthreatening distance. After this intermittent eye contact, the nurse is no longer viewed as a stranger but as a friend. This can be followed by touch games. Clapping an infant’s hands together for pat-a-cake or wiggling the toes for “this little piggy” delights an infant or small child. Talking to a foot or other part of the child’s body is another effective tactic. Much of the nursing assessment can be carried out with the use of games and simple play equipment while the infant remains in the safety of the parent’s arms or lap.
The nurse can capitalize on the natural curiosity of small children by playing games such as “Which hand do you take?” and “Guess what I have in my hand” or by manipulating items such as a flashlight or stethoscope. Finger games are useful. More elaborate materials, such as puppets and replicas of familiar or unfamiliar items, serve as excellent means of communicating with small children. The variety and extent are limited only by the nurse’s imagination.
Through play, children reveal their perceptions of interpersonal relationships with their family, friends, or hospital personnel. Children may also reveal the wide scope of knowledge they have acquired from listening to others around them. For example, through needle play, children may disclose how carefully they have watched each procedure by precisely duplicating the technical skills. They may also reveal how well they remember those who performed procedures. One child who painstakingly reenacted every detail of a tedious medical procedure also played the role of the physician who had repeatedly shouted at her to be still for the long ordeal. Her anger at him was most evident during the play session and revealed the cause for her abrupt withdrawal and passive hostility toward the medical and nursing staff after the test.
Play sessions serve not only as assessment tools for determining children’s awareness and perception of their illness, but also as methods of intervention and evaluation. In the previous example, when the child revealed anger toward the physician, the nurse acted the part of the patient but this time did not accept the physician’s harsh commands to stay still. Instead, the nurse said to the physician all the things the child had wished she could say.
HISTORY TAKING
The format used for history taking may be (1) direct, where the nurse asks for information via direct interview with the informant; or (2) indirect, where the informant supplies the information by completing some type of questionnaire. The direct method is superior to the indirect approach or a combination of both. However, in view of time constraints, the direct approach is not always practical. If the direct approach cannot be used, review parents’ written responses and question them regarding any unusual answers. The categories listed in Box 6-5 encompass children’s current and past health status and information about their psychosocial environment.
Identifying Information
Much of the identifying information may already be available from other recorded sources. However, if the parent and youngster seem anxious, use this opportunity to ask about such information to help them feel more comfortable.
Informant.: One of the important elements of identifying information is the informant, the person(s) who furnish the information. Record (1) who the person is (child, parent, or other), (2) an impression of reliability and willingness to communicate, and (3) any special circumstances such as the use of an interpreter or conflicting answers by more than one person.
Chief Complaint
The chief complaint is the specific reason for the child’s visit to the clinic, office, or hospital. It may be viewed as the theme, with the present illness viewed as the description of the problem. The chief complaint is elicited by asking open-ended, neutral questions such as “What seems to be the matter?” “How may I help you?” or “Why did you come here today?” Avoid labeling-type questions such as “How are you sick?” or “What is the problem?”; it is possible that the reason for the visit is not an illness or problem.
Occasionally, it is difficult to isolate one symptom or problem as the chief complaint because the parent may identifymany. In this situation be as specific as possible when asking questions. For example, asking informants to state which one problem or symptom prompted them to seek help now may help them focus on the most immediate concern.
Present Illness
The history of the present illness* is a narrative of the chief complaint from its earliest onset through its progression to the present. Its four major components are (1) the details of onset, (2) a complete interval history, (3) the present status, and (4) the reason for seeking help now. The focus of the present illness is on all factors relevant to the main problem, even if they have disappeared or changed during the onset, interval, and present.
Analyzing a Symptom.: Because pain is often the most characteristic symptom denoting the onset of a physical problem, it is used as an example for analysis of a symptom. Assessment includes (1) type, (2) location, (3) severity, (4) duration, and (5) influencing factors (see Nursing Care Guidelines box; see also Pain Assessment, Chapter 7).
History
The history contains information relating to all previous aspects of the child’s health status and concentrates on several areas that are ordinarily passed over in the history of an adult, such as birth history, detailed feeding history, immunizations, and growth and development. Since a great deal of information is included in this section, use a combination of open-ended and fact-finding questions. For example, begin interviewing for each section with an open-ended statement such as “Tell me about your child’s birth” to provide the informants with the opportunity to relate what they think is most important. Ask fact-finding questions related to specific details whenever necessary to focus the interview on certain topics.
Birth History.: The birth history includes all data concerning (1) the mother’s health during pregnancy, (2) the labor and delivery, and (3) the infant’s condition immediately after birth. Since prenatal influences have significant effects on a child’s physical and emotional development, a thorough investigation of the birth history is essential. Because parents may question what relevance pregnancy and birth have on the child’s present condition, particularly if the child is past infancy, explain why such questions are included. An appropriate statement may be, “I will be asking you some questions about your pregnancy and ____’s [refer to child by name] birth. Your answers will give me a more complete picture of his [or her] overall health.”
Because emotional factors also affect the outcome of pregnancy and the subsequent parent-child relationship, investigate (1) concurrent crises during pregnancy and (2) prenatal attitudes toward the fetus. It is best to approach the topic of parental acceptance of pregnancy through indirect questioning. Asking parents if the pregnancy was planned is a leading statement because they may respond affirmatively for fear of criticism if the pregnancy was unexpected. Rather, encourage parents to disclose their true reactions by referring to specific facts relating to the pregnancy, such as the spacing between offspring, an extended or short interval between marriage and conception, or the concurrent experience of pregnancy and adolescence. The parent can choose to explore such statements with further explanations or, for the moment, may not be able to reveal such feelings. If the parent remains silent, return to this topic later in the interview.
Dietary History.: Because parental concerns are common and nursing interventions are important in ensuring optimum nutrition, the dietary history is discussed in detail later in this chapter under Nutritional Assessment.
Previous Illnesses, Injuries, and Operations.: When inquiring about past illnesses, begin with a general statement such as “What other illnesses has your child had?” Since parents are most likely to recall serious health problems, ask specifically about colds; earaches; and childhood diseases such as measles, rubella (German measles), chickenpox, mumps, pertussis (whooping cough), diphtheria, tuberculosis, scarlet fever, strep throat, tonsillitis, or allergic manifestations.
In addition to illnesses, ask about injuries that required medical intervention, operations, and any other reason for hospitalization, including the dates of each incident. It is important to focus on injuries such as accidental falls, poisoning, choking, or burns, since these may be potential areas for parental guidance.
Allergies.: Ask about commonly known allergic disorders such as hay fever and asthma; unusual reactions to drugs, food, or latex products; and reactions to other contact agents such as poisonous plants, animals, household products, or fabrics. If asked appropriate questions, most people can give reliable information about drug reactions (see Nursing Care Guidelines box).
Has your child ever taken any drugs or tablets that have disagreed with him or her or caused an allergy? If yes, can you remember the name(s) of these drugs?
Can you describe the reaction?
Was the drug taken by mouth (as a tablet or syrup), or was it an injection?
How soon after starting the drug did the reaction happen?
Did anyone tell you it was an allergic reaction, or did you decide for yourself?
Has your child ever taken this drug, or a similar one, again? If yes, did your child experience the same problems?
Have you told the doctors or nurses about your child’s reaction or allergy?
Modified from Cantrill JA, Cottrell WN: Accuracy of drug allergy documentation, Am J Health Syst Pharm 54:1627-1629, 1997.
Current Medications.: Inquire about current drug regimens, including vitamins, antipyretics (especially aspirin), antibiotics, antihistamines, decongestants, or antitussives. List all medications, including name, dose, schedule, duration, and reason for administration. Often parents are unaware of the drug’s actual name. Whenever possible, ask parents to bring the containers with them to the next visit, or ask for the name of the pharmacy and call for a list of all the child’s recent prescription medications. However, this list will not include over-the-counter medications, which are important to know.
Immunizations.: A record of all immunizations is essential. Since many parents are unaware of the exact name and date of each immunization, the most reliable source of information is a hospital, clinic, or private practitioner’s record. All immunizations and “boosters” are listed, stating (1) the name of the specific disease, (2) the number of injections, (3) the dosage (sometimes lesser amounts are given if a reaction is anticipated), (4) the ages when administered, and (5) the occurrence of any reaction following the immunization.
Growth and Development.: The most important previous growth patterns to record are:
Approximate weight at 6 months, 1 year, 2 years, and 5 years of age
Approximate length at ages 1 and 4 years
Dentition, including age of onset, number of teeth, and symptoms during teething
Developmental milestones include:
Age of holding up head steadily
Age of sitting alone without support
Age of walking without assistance
Use specific and detailed questions when inquiring about each developmental milestone. For example, “sitting up” can mean many different activities, such as sitting propped up, sitting in someone’s lap, sitting with support, sitting up alone but in a hyperflexed position for assisted balance, or sitting up unsupported with the back slightly rounded. A clue to misunderstanding of the requested activity may be an unusually early age of achievement (see Developmental Assessment, p. 93).
Habits.: Habits are an important area to explore (Box 6-6). Parents frequently express concerns during this part of the history. Encourage their input by saying, “Please tell me any concerns you have about your child’s habits, activities, or development.” Investigate further any concerns that are expressed.
BOX 6-6 Habits to Explore During a Health Interview
Behavior patterns such as nail biting, thumb sucking, pica (habitual ingestion of nonfood substances), rituals (‘security’ blanket or toy), and unusual movements (head banging, rocking, overt masturbation, walking on toes)
Activities of daily living, such as hour of sleep and arising, duration of nighttime sleep and naps, type and duration of exercise, regularity of stools and urination, age of toilet training, and daytime or nighttime bed-wetting
One of the most common concerns relates to sleep. Many children develop a normal sleep pattern, and all that is required during the assessment is a general overview of nighttime sleep and nap schedules. However, a number of children also develop sleep problems (see Sleep Problems, Chapters 10 and 13). When sleep problems occur, a more detailed sleep history is required to guide appropriate interventions.*
Habits related to use of chemicals apply primarily to older children and adolescents. If a youngster admits to smoking, drinking, or drug use, ask about the quantity and frequency. Questions such as “Have you ever had a drinking or drug problem?” or “When was the last time you had a drink or took drugs?” may yield more reliable data than questions such as “How much do you drink?” or “How often do you drink or take drugs?” Clarify that “drinking” includes all types of alcohol, such as beer and wine. When quantities such as a “glass” of wine or a “can” of beer are given, ask about the size of the container.
If older children deny use of chemical substances, inquire about past experimentation. Asking, “You mean you never tried to smoke or drink?” implies that the nurse expects some such activity, and the youngster may be more inclined to answer truthfully. Be aware of the confidential nature of such questioning, the adverse effect that the parents’ presence may have on the adolescent’s willingness to answer, and the fact that self-reporting may not be an accurate account of chemical abuse.
Sexual History
The sexual history is an essential component of adolescents’ health assessment. The history uncovers areas of concern related to sexual activity; alerts the nurse to circumstances that may indicate screening for sexually transmitted diseases or testing for pregnancy; and provides information related to the need for sexual counseling, such as safe sex practices. Guidelines for anticipatory guidance topics for parents and adolescents are found in Box 6-7.
One approach to initiating a conversation about sexual concerns is to begin with a history of peer interactions. Open-ended statements such as “Tell me about your social life” or “Who are your closest friends?” generally lead into a discussion of dating and sexual issues. To probe further, include questions about the adolescent’s attitudes on such topics as sex education, “going steady,” “living together,” and premarital sex. Phrase questions to reflect concern rather than judgment or criticism of sexual practices.
In any conversation regarding sexual history, be aware of the language that is used in either eliciting or conveying sexual information. For example, avoid asking if the adolescent is “sexually active,” because this term is broadly defined. “Are you having sex with anyone?” is probably the most direct and best understood question. Since same-sex experimentation may occur, refer to all sexual contacts in nongender terms, such as “anyone” or “partners,” rather than “girlfriends” or “boyfriends.”
A detailed account of sexual partners is needed if the patient has a history of, displays any symptoms of, or asks for treatment of a sexually transmitted disease. A difficult but necessary part of the interview is to determine the sites of possible infection. Since sexual diseases can be contracted in any of the body orifices, inform the adolescent that a sexually transmitted disease can be acquired without visible signs of disease at nongenital sites.
Family Medical History
The family medical history is used primarily for the purpose of discovering the potential existence of hereditary or familial diseases in the parents and child. In general, it is confined to first-degree relatives (parents, siblings, grandparents, and immediate aunts and uncles). Information for each family member includes age, marital status, state of health if living, cause of death if deceased, and any evidence of the following conditions: heart disease, hypertension, cancer, diabetes mellitus, obesity, congenital anomalies, allergy, asthma, seizures, tuberculosis, sickle cell disease, mental retardation, mental disorders such as depression or psychosis, emotional problems, syphilis, or rheumatic fever. Confirm the accuracy of the reported disorders by inquiring about the symptoms, course, treatment, and sequelae of each diagnosis.
Geographic Location.: One of the important areas to explore when assessing the family health history is geographic location, including the birthplace and travel to different areas in or outside of the country, for identification of possible exposure to endemic diseases. Although the primary interest focuses on the child’s temporary residence in various localities, also inquire about close family members’ travel, especially during tours of military service or business trips. Children are especially susceptible to parasitic infestation in areas of poor sanitary conditions and to vector-borne diseases, such as those from mosquitoes or ticks in warm and humid or heavily wooded regions.
Family Structure
Assessment of the family, both its structure and function, is an important component of the history-taking process. Because the quality of the functional relationship between the child and family members is a major factor in emotional and physical health, family assessment is discussed separately and in greater detail apart from the more traditional health history.
Family assessment is the collection of data about the composition of the family and the relationships among its members. In its broadest sense, family refers to all those individuals who are considered by the family member to be significant to the nuclear unit, including relatives, friends, and social groups such as the school and church. Although family assessment is not family therapy, it can and frequently is therapeutic. Involving family members in discussing family characteristics and activities can provide insight into family dynamics and relationships.
Because of the time involved in performing an in-depth family assessment as presented here, be selective in deciding when knowledge of family function may facilitate nursing care (see Nursing Care Guidelines box). During brief contacts with families, a full assessment is not appropriate, and screening with one or two questions from each category may reflect the health of the family system or the need for additional assessment.
Initiating a Comprehensive Family Assessment
Perform a comprehensive assessment on:
Children receiving comprehensive well-child care
Children experiencing major stressful life events (e.g., chronic illness, disability, parental divorce, death of a family member)
Children requiring extensive home care
Children with developmental delays
Children with repeated accidental injuries and those with suspected child abuse
Children with behavioral or physical problems that could be caused by family dysfunction
Modified from Cantrill JA, Cottrell WN: Accuracy of drug allergy documentation, Am J Health Syst Pharm 54:1627-1629, 1997.
Family structure refers to the composition of the family—;who lives in the home and those social, cultural, religious, and economic characteristics that influence the child’s and family’s overall psychobiologic health (see also Chapters 3 and 4). Since the information elicited in this part of the history is often the most personal and confidential, include it toward the end of the interview when rapport is well established.
The most common method of eliciting information on the family structure is to interview family members. The principal areas of concern (Box 6-8) are (1) family composition, (2) home and community environment, (3) occupation and education of family members, and (4) cultural and religious traditions.
BOX 6-8 Family Assessment Interview
Schedule the interview with the family at a time that is most convenient for all parties; include as many family members as possible; clearly state the purpose of the interview.
Begin the interview by asking each person’s name and their relationship to one another.
Restate the purpose of the interview and the objective.
Keep the initial conversation general to put members at ease and to learn the ‘big picture’ of the family.
Identify major concerns and reflect these back to the family to be certain that all parties receive the same message.
Terminate the interview with a summary of what was discussed and a plan for additional sessions if needed.
Immediate members of the household (names, ages, and relationships)
Significant extended family members
Previous marriages, separations, death of spouses, or divorces
Home and Community Environment
Type of dwelling, number of rooms, occupants
Number of floors, accessibility of stairs and elevators
Safety features (fire escape, smoke and carbon monoxide detectors, guardrails on windows, use of car restraint)
Environmental hazards (e.g., chipped paint, poor sanitation, pollution, heavy street traffic)
Availability and location of health care facilities, schools, play areas
Occupation and Education of Family Members
Types of employment
Exposure to environmental or industrial hazards
Sources of income and adequacy
Cultural and Religious Traditions
Religious beliefs and practices
Cultural and ethnic beliefs and practices
Does the family identify with a particular religious or ethnic group? Are both parents from that group?
How is religious or ethnic background part of family life?
What special religious or cultural traditions are practiced in the home (e.g., food choices and preparation)?
Where were family members born, and how long have they lived in this country?
What language does the family speak most frequently?
Do they speak and understand English?
What do they believe causes health or illness?
What religious or ethnic beliefs influence the family’s perception of illness and its treatment?
What methods are used to prevent or treat illness?
How does the family know when a health problem needs medical attention?
Whom does the family contact when a member is ill?
Does the family rely on cultural or religious healers or remedies? If so, ask them to describe the type of healer or remedy.
Whom does the family go to for support (clergy, medical healer, relatives)?
Does the family experience discrimination because of their race, beliefs, or practices? Ask them to describe.
Interactions refer to ways family members relate to each other.
Chief concern is the amount of intimacy and closeness among the members, especially spouses.
Roles refer to behaviors of people as they assume a different status or position.
Family members’ responses to each other (cordial, hostile, cool, loving, patient, short tempered)
What activities does the family perform together?
Whom do family members talk to when something is bothering them?
What are members’ household chores?
Who usually oversees what is happening with the children, such as at school or health care?
How easy or difficult is it for the family to change or accept new responsibilities for household tasks?
Power, Decision Making, and Problem Solving
Power refers to individual member’s control over others in family; it is manifested through family decision making and problem solving.
Chief concern is clarity of boundaries of power between parents and children.
One method of assessment involves offering a hypothetical conflict or problem, such as a child failing school, and asking family how they would handle this situation.
Communication is concerned with clarity and directness of communication patterns.
Further assessment includes periodically asking family members if they understood what was just said and to repeat the message.
Expression of Feelings and Individuality
Expressions are concerned with personal space and freedom to grow with limits and structure needed for guidance.
Observing patterns of communication offers clues to how freely feelings are expressed.
Is it OK for family members to get angry or sad?
Who gets angry most of the time? What do they do?
If someone is upset, how do other family members try to comfort this person?
Who comforts specific family members?
When someone wants to do something, such as try out for a new sport or get a job, what is the family’s response (offer assistance, discouragement, or no advice)?
Psychosocial History
The traditional medical history includes a personal and social section that concentrates on children’s personal status, such as school adjustment and any unusual habits, and the family and home environment. Since several personal aspects are covered under development and habits, only those issues related to children’s ability to cope and their self-concept are presented here.
Through observation, obtain a general idea of how children handle themselves in terms of confidence in dealing with others, answering questions, and coping with new situations. Observe the parent-child relationship for the types of messages sent to children about their coping skills and self-worth. Do the parents treat the child with respect, focusing on strengths, or is the interaction one of constant reprimands, with emphasis on weaknesses and faults? Do the parents help the child learn new coping strategies or support the ones the child uses?
Messages about body image are also conveyed through the parent-child interaction. Do the parents label the child and body parts, such as “bad boy,” “skinny legs,” or “ugly scar”? Do the parents handle the child gently, using soothing touch to calm an anxious child, or do they treat the child roughly, using slaps or restraint to force compliance? If the child touches certain parts of the body, such as the genitalia, do the parents make comments that suggest a negative connotation?
With older children many of the communication strategies discussed earlier in the chapter are useful in eliciting more definitive information about their coping and self-concept. Children can write down five things they like and dislike about themselves. The nurse can use sentence completion statements, such as “The thing I like best (or worst) about myself is ____________,” “If I could change one thing about myself, it would be ____________,” or “When I am scared, I ____________.”
Review of Systems
The review of systems is a specific review of each body system, following an order similar to that of the physical examination (see Nursing Care Guidelines box). Often the history of the present illness provides a complete review of the system involved in the chief complaint. Since asking questions about other body systems may appear unrelated and irrelevant to the parents or child, precede the questioning with an explanation of why the data are needed (similar to the explanation concerning the relevance of the birth history) and reassure the parents that the child’s main problem has not been forgotten.
Begin the review of a specific system with a broad statement such as “How has your child’s general health been?” or “Has your child had any problems with his eyes?” If the parent states that the child has had problems with some body function, pursue this with an encouraging statement such as “Tell me more about that.” If the parent denies any problems, query for specific symptoms (e.g., “No headaches, bumping into objects, or squinting?”). If the parent reconfirms the absence of such symptoms, record positive statements in the history, such as “Mother denies headaches, bumping into objects, or squinting.” In this way, anyone who reviews the health history is aware of exactly what symptoms were investigated.
NUTRITIONAL ASSESSMENT
Food consumption patterns of children have changed over the past 30 years (Nicklas, Demory-Luce, Yang, and others, 2004). The prevalence of overweight and obesity among children and adolescents has significantly increased (Hedley, Ogden, Johnson, and others, 2004). Knowledge of the child’s dietary intake is an essential component of a nutritional assessment. However, it is also one of the most difficult factors to assess. Individuals’ recall of food consumption, especially amounts eaten, is frequently unreliable. The food intake history of children and adolescents is prone to reporting error, mostly in the form of underreporting (Livingstone, Robson, and Wallace, 2004). People from different cultures may have difficulty adequately describing the types of food they eat. Despite these obstacles, a dietary evaluation is an important component of the child’s assessment.
The dietary reference intakes (DRIs) are a set of four nutrient-based reference values that provide quantitative estimates of nutrient intake for use in assessing and planning dietary intake (American Academy of Pediatrics, 2004; Murphy and Poos, 2002). The specific DRIs include:
Estimated average requirement (EAR)—Nutrient intake estimated to meet the requirement of half the healthy individuals (50%) for a specific age and gender group. Used to examine the possibility of inadequacy.
Recommended dietary allowance (RDA)—Average daily dietary intake sufficient to meet the nutrient requirement of nearly all (97% to 98%) of healthy individuals for a specific age and gender group. Dietary intake at or above this level usually has a low probability of inadequacy.
Adequate intake (AI)—Recommended intake level based on estimates of nutrient intake by healthy groups of individuals. Dietary intake at or above this level usually has a low probability of inadequacy.
Tolerable upper intake level (UL)—Highest average daily nutrient intake level likely to pose no risk of adverse health effects. As intake increases above the UL, risk of adverse effects increases. Dietary intake above this level usually places an individual at risk of adverse effects from excessive nutrient intake.
MyPyramid for Kids describes dietary intake in children (see Fig. 11-1). Specific questions used to conduct a nutritional assessment are also included in Box 6-9. Every nutritional assessment should begin with a dietary history. The exact questions used to elicit a dietary history vary with the child’s age. In general, the younger the child, the more specific and detailed the history should be.
What are the family’s usual mealtimes?
Do family members eat together or at separate times?
Who does the family grocery shopping and meal preparation?
How much money is spent to buy food each week?
How are most foods prepared—baked, broiled, fried, other?
How often does the family or your child eat out?
What kinds of restaurants do you go to?
What kinds of food does your child typically eat at restaurants?
Does your child eat breakfast regularly?
Where does your child eat lunch?
What are your child’s favorite foods, beverages, and snacks?
What are the average amounts eaten per day?
What foods are artificially sweetened?
What are your child’s snacking habits?
What special cultural practices are followed? What ethnic foods are eaten?
What foods and beverages does your child dislike?
How would you describe your child’s usual appetite (hearty eater, picky eater)?
What are your child’s feeding habits (breast, bottle, cup, spoon, eats by self, needs assistance, any special devices)?
Does your child take vitamins or other supplements? Do they contain iron or fluoride?
Does your child have any known or suspected food allergies? Is your child on a special diet?
Has your child lost or gained weight recently?
Are there any feeding problems (excessive fussiness, spitting up, colic, difficulty sucking or swallowing)? Are there any dental problems or appliances, such as braces, that affect eating?
What types of exercise does your child do regularly?
Is there a family history of cancer, diabetes, heart disease, high blood pressure, or obesity?
ADDITIONAL QUESTIONS FOR INFANTS
What was the infant’s birth weight? When did it double? Triple?
Are you breastfeeding or have you breast-fed your infant? For how long?
If you use a formula, what is the brand?
Are you giving the infant cow’s milk (whole, low fat, skim)?
Do you give your infant extra fluids (water, juice)?
If the infant takes a bottle to bed at nap or nighttime, what is in the bottle?
At what age did the child start on cereal, vegetables, meat or other protein sources, fruit or juice, finger food, table food?
Do you make your own baby food or use commercial foods, such as infant cereal?
Does the infant take a vitamin or mineral supplement? If so, what type?
Has the infant had an allergic reaction to any food(s)? If so, list the foods and describe the reaction.
Does the infant spit up frequently; have unusually loose stools; or have hard, dry stools? If so, how often?
Modified from Murphy SP, Poos MI: Dietary reference intakes: summary of applications in dietary assessment, Pub Health Nutr 5(6A):843-849, 2002.
The overview elicited from the dietary history can be helpful in evaluating food frequency records. The history is also concerned with financial and cultural factors that influence food selection and preparation (see Cultural Awareness box).
 CULTURAL AWARENESS
CULTURAL AWARENESSBecause cultural practices are prevalent in food preparation, consider carefully the kinds of questions that are asked and the judgments made during counseling. For example, some cultures, such as Hispanic, African American, and Native American, include many vegetables, legumes, and starches in their diet that together provide sufficient essential amino acids, even though the actual amount of meat or dairy protein is low. (See Food Customs, Chapter 4.)
The most common and probably easiest method of assessing daily intake is the 24-hour recall. The child or parent recalls every item eaten in the past 24 hours and the approximate amounts. The 24-hour recall is most beneficial when it represents a typical day’s intake. Some of the difficulties with a daily recall are the family’s inability to remember exactly what was eaten and inaccurate estimation of portion size. To increase accuracy of reporting portion sizes, the use of food models and additional questioning are recommended. In general, this method is most useful in providing qualitative information about the child’s diet.
To improve the reliability of the daily recall, the family can complete a food diary by recording every food and liquid consumed for a certain number of days. A 3-day record consisting of 2 weekdays and 1 weekend day is representative for most people. Providing specific charts to record intake can improve compliance. The family should record items immediately after eating.
A food frequency questionnaire or record provides information about the number of times in a day, week, or month a child consumes items from the different food groups. In general, it provides a qualitative overview but has the advantage of avoiding recall based on a “typical” day. It can be especially useful when verifying a food history or diary.
CLINICAL EXAMINATION
A significant amount of information regarding nutritional deficiencies is elicited from a clinical examination, especially from assessing the skin, hair, teeth, gums, lips, tongue, and eyes. Hair, skin, and mouth are vulnerable because of the rapid turnover of epithelial and mucosal tissue. Table 6-1 summarizes clinical signs of possible nutritional deficiency or excess. Few are diagnostic for a specific nutrient, and if suspicious signs are found, they must be confirmed with dietary and biochemical data. Generally, the clinical examination does not reveal children at risk for a deficiency or excess.
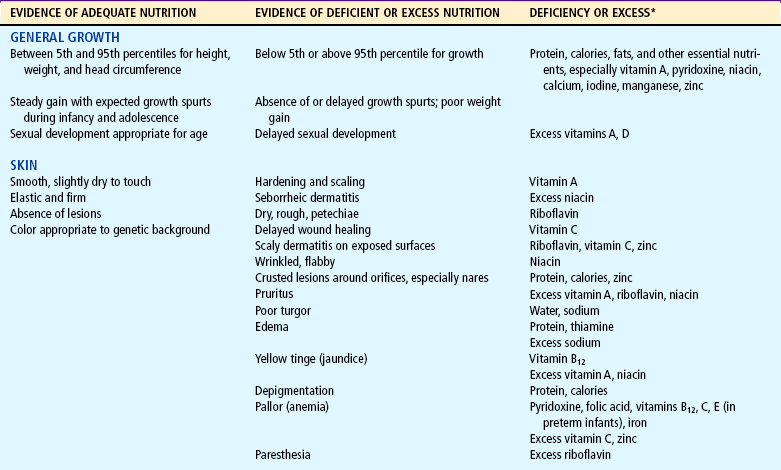
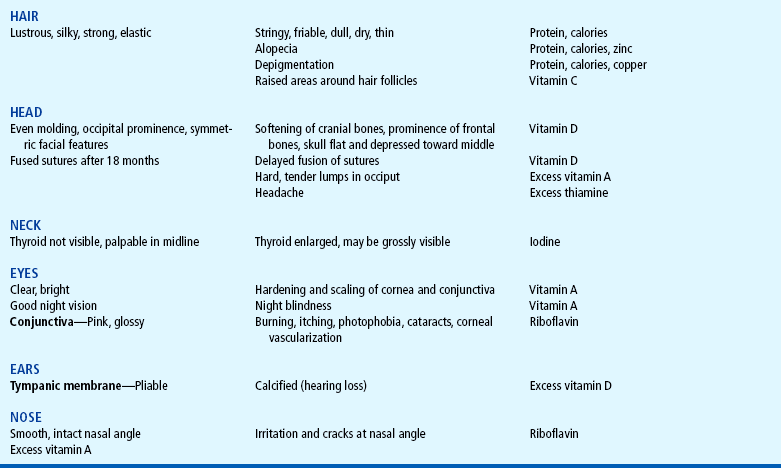
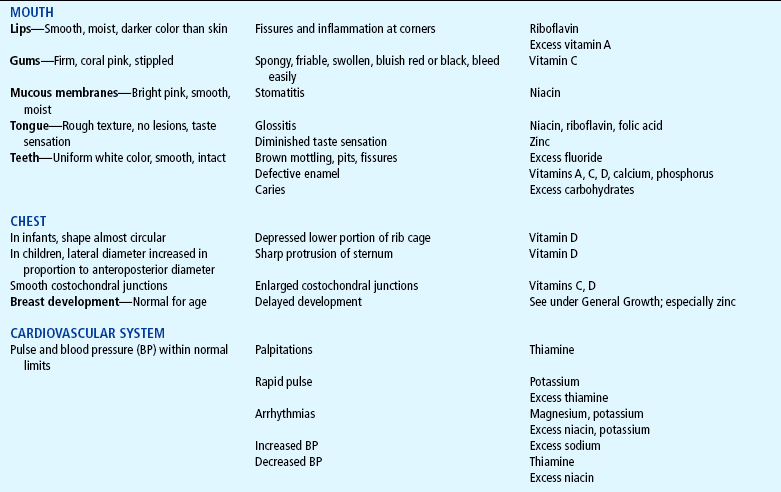
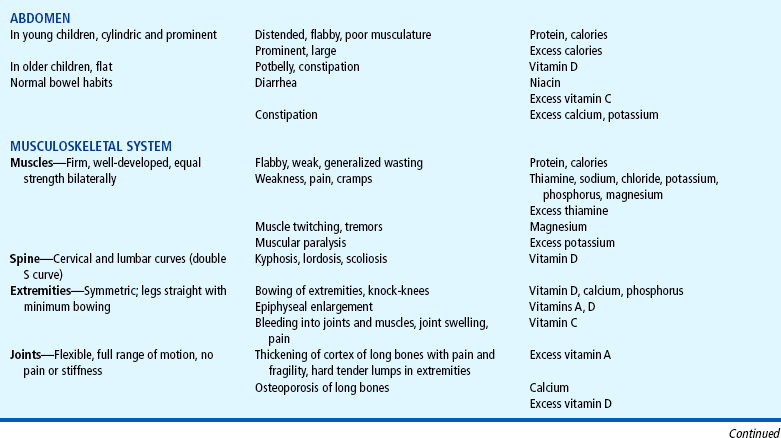
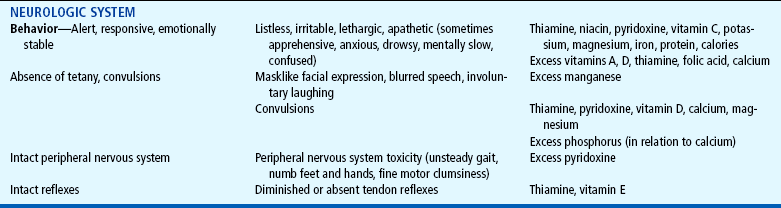
Anthropometry, an essential parameter of nutritional status, is the measurement of height, weight, head circumference, proportions, skinfold thickness, and arm circumference in young children. Height and head circumference reflect past nutrition, whereas weight, skinfold thickness, and arm circumference reflect present nutritional status, especially of protein and fat reserves. Skinfold thickness is a measurement of the body’s fat content because approximately half the body’s total fat stores are directly beneath the skin. The upper arm muscle circumference is correlated with measurements of total muscle mass. Since muscle serves as the body’s major protein reserve, this measurement is considered an index of the body’s protein stores. Ideally, growth measurements are recorded over time, and comparisons are made regarding the velocity of growth based on previous and present values. Numerous biochemical tests are available for assessing nutritional status and include analysis of plasma; blood cells; urine; and tissues from liver, bone, hair, and fingernails. Many of these tests are complicated and are not performed routinely. Common laboratory procedures for nutritional status include measurement of hemoglobin, hematocrit, transferrin, albumin, creatinine, and nitrogen. Laboratory values for these tests and more specific nutrient measurements are given in Appendix C.
EVALUATION OF NUTRITIONAL ASSESSMENT
After collecting the data needed for a thorough nutritional assessment, evaluate the findings to plan appropriate counseling. From the data, assess whether the child is (1) malnourished, (2) at risk for becoming malnourished, or (3) well nourished with adequate reserves.
Analyze the daily food diary for the variety and amounts of foods suggested in MyPyramid (see Fig. 11-1). For example, if the list includes no vegetables, inquire about this rather than assuming that the child dislikes vegetables, since it could be that none were served that day. Also, evaluate the information in terms of the family’s ethnic practices and financial resources. Encouraging increased protein intake with additional meat may be unfeasible for families on a limited budget or in conflict with food practices that use meat sparingly, such as in Asian meal preparation.
GENERAL APPROACHES TOWARD EXAMINING THE CHILD
Ordinarily, the sequence for examining patients follows a head-to-toe direction. The main function of such a systematic approach is to provide a general guideline for assessment of each body area to avoid omitting segments of the examination. The standard recording of data also facilitates exchange of information among different professionals. The typical organization of a physical examination is indicated in the chapter outline. In examining children, this orderly sequence is frequently altered to accommodate the child’s developmental needs, although the examination is recorded following the head-to-toe model. Using developmental and chronologic age as the main criteria for assessing each body system accomplishes several goals:
Minimizes stress and anxiety associated with assessment of various body parts
Fosters a trusting nurse-child-parent relationship
Allows for maximum preparation of the child
Preserves the essential security of the parent-child relationship, especially with young children
Maximizes the accuracy and reliability of assessment findings