Developmental Influences on Child Health Promotion
Foundations of Growth and Development
DEVELOPMENT OF PERSONALITY AND MENTAL FUNCTION
Theoretic Foundations of Personality Development
SELECTED FACTORS THAT INFLUENCE DEVELOPMENT
On completion of this chapter the reader will be able to:
 Describe major trends in growth and development.
Describe major trends in growth and development.
Explain the alterations in the major body systems that take place during the process of growth and development.
Discuss the development and relationships of personality, cognition, language, morality, spirituality, and self-concept.
Describe the role of play in the growth and development of children.
Demonstrate an understanding of the role of innate and environmental factors in the physical and emotional development of children.
RELATED TOPICS and ADDITIONAL RESOURCES
 IN TEXT
IN TEXTGrowth Failure (Failure to Thrive), Ch. 11
Health Promotion of the Adolescent and Family, Ch. 16
Health Promotion of the Infant and Family, Ch. 10
Health Promotion of the Preschooler and Family, Ch. 13
Health Promotion of the School-Age Child and Family, Ch. 15
Health Promotion of the Toddler and Family, Ch. 12
Providing Opportunities for Play and Expressive Activities, Ch. 21
Use of Play in Procedures, Ch. 22
GROWTH AND DEVELOPMENT
FOUNDATIONS OF GROWTH AND DEVELOPMENT
Growth and development, usually referred to as a unit, express the sum of the numerous changes that take place during the lifetime of an individual. The entire course is a dynamic process that encompasses several interrelated dimensions:
Growth—an increase in number and size of cells as they divide and synthesize new proteins; results in increased size and weight of the whole or any of its parts
Development—a gradual change and expansion; advancement from lower to more advanced stages of complexity; the emerging and expanding of the individual’s capacities through growth, maturation, and learning
Maturation—an increase in competence and adaptability; aging; usually used to describe a qualitative change; a change in the complexity of a structure that makes it possible for that structure to begin functioning; to function at a higher level
Differentiation—processes by which early cells and structures are systematically modified and altered to achieve specific and characteristic physical and chemical properties; sometimes used to describe the trend of mass to specific; development from simple to more complex activities and functions
All these processes are interrelated, simultaneous, and ongoing; none occurs apart from the others. The processes depend on a sequence of endocrine, genetic, constitutional, environmental, and nutritional influences (Seidel, Ball, Dains, and others, 2007). The child’s body becomes larger and more complex; the personality simultaneously expands in scope and complexity. Very simply, growth can be viewed as a quantitative change, and development as a qualitative change.
Stages of Development
Most authorities in the field of child development conveniently categorize child growth and behavior into approximate age stages or in terms that describe the features of an age-group. The age ranges of these stages are admittedly arbitrary and, because they do not take into account individual differences, cannot be applied to all children with any degree of precision. However, categorization affords a convenient means to describe the characteristics associated with the majority of children at periods when distinctive developmental changes appear and specific developmental tasks must be accomplished. (A developmental task is a set of skills and competencies peculiar to each developmental stage that children must accomplish or master to deal effectively with their environment.) It is also significant for nurses to know that there are characteristic health problems peculiar to each major phase of development. The sequence of descriptive age periods and subperiods that are used here and elaborated in subsequent chapters is listed in Box 5-1.
Patterns of Growth and Development
There are definite and predictable patterns in growth and development that are continuous, orderly, and progressive. These patterns, or trends, are universal and basic to all human beings, but each human being accomplishes these in a manner and time unique to that individual.
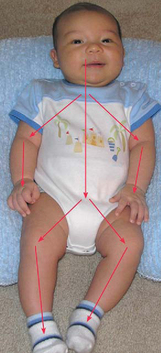
Directional Trends.: Growth and development proceed in regular, related directions or gradients and reflect the physical development and maturation of neuromuscular functions (Fig. 5-1). The first pattern is the cephalocaudal, or head-to-tail, direction. The head end of the organism develops first and is large and complex, whereas the lower end is small and simple and takes shape at a later period. The physical evidence of this trend is most apparent during the period before birth, but it also applies to postnatal behavior development. Infants achieve structural control of the head before they have control of the trunk and extremities, hold their back erect before they stand, use their eyes before their hands, and gain control of their hands before they have control of their feet.
Second, the proximodistal, or near-to-far, trend applies to the midline-to-peripheral concept. A conspicuous illustration is the early embryonic development of limb buds, which is followed by rudimentary fingers and toes. In the infant, shoulder control precedes mastery of the hands, the whole hand is used as a unit before the fingers can be manipulated, and the central nervous system develops more rapidly than the peripheral nervous system.
These trends or patterns are bilateral and appear symmetric—each side develops in the same direction and at the same rate as the other. For some of the neurologic functions, this symmetry is only external because of unilateral differentiation of function at an early stage of postnatal development. For example, by the age of approximately 5 years the child has demonstrated a decided preference for the use of one hand over the other, although previously either one had been used.
The third trend, differentiation, describes development from simple operations to more complex activities and functions. From broad, global patterns of behavior, more specific, refined patterns emerge. All areas of development (physical, mental, social, and emotional) proceed in this direction. Through the process of development and differentiation, early embryonal cells with vague, undifferentiated functions progress to an immensely complex organism composed of highly specialized and diversified cells, tissues, and organs. Generalized development precedes specific or specialized development; gross, random muscle movements take place before fine muscle control.
Sequential Trends.: In all dimensions of growth and development there is a definite, predictable sequence, with each child normally passing through every stage. Children crawl before they creep, creep before they stand, and stand before they walk. Later facets of the personality are built on the early foundation of trust. The child babbles, then forms words and, finally, sentences; writing emerges from scribbling.
Developmental Pace.: Although development has a fixed, precise order, it does not progress at the same rate or pace. There are periods of accelerated growth and periods of decelerated growth in both total body growth and the growth of subsystems. Not all areas of development occur at the same pace. When a spurt occurs in one area such as gross motor, minimal advances may take place in language, fine motor, or social skills. Once the gross motor skill has been achieved, then development focus will shift to another area. The rapid growth before and after birth gradually levels off throughout early childhood. Growth is relatively slow during middle childhood, markedly increases at the beginning of adolescence, and levels off in early adulthood. Each child grows at his or her own pace. Distinct differences are observed between children as they reach developmental milestones.
Sensitive Periods.: There are limited times during the process of growth when the organism will interact with a particular environment in a specific manner. Periods termed critical, sensitive, vulnerable, and optimal are those times in the lifetime of an organism when it is more susceptible to positive or negative influences.
The quality of interactions during these sensitive periods determines whether the effects on the organism will be beneficial or harmful. For example, physiologic maturation of the central nervous system is influenced by adequacy and timing of contributions from the environment such as stimulation and nutrition. The first 3 months of prenatal life are sensitive periods for physical growth of the fetus.
Psychologic development also appears to have sensitive periods, when an environmental event has maximal influence on the developing personality. For example, primary socialization occurs during the first year when the infant makes the initial social attachments and establishes a basic trust in the world. A warm relationship with a parent figure is fundamental to a healthy personality. The same concept might be applied to readiness for learning skills such as toilet training or reading. In these instances there appears to be an opportune time when the skill is best learned.
Individual Differences
Each child grows in his or her own unique and personal way. Great individual variation exists in the age at which developmental milestones are reached. The sequence is predictable; the exact timing is not. Rates of growth vary, and measurements are defined in terms of ranges to allow for individual differences. Some children are fast growers, others are moderate, and some are slower to reach maturity. Periods of fast growth, such as the pubescent growth spurt, may begin earlier or later in some children than in others. Children may grow fast or slowly during the spurt and may finish sooner or later than other children. Gender is an influential factor because girls seem to be more advanced in physiologic growth at all ages.
BIOLOGIC GROWTH AND PHYSICAL DEVELOPMENT
As children grow, their external dimensions change. These changes are accompanied by corresponding alterations in structure and function of internal organs and tissues that reflect the gradual acquisition of physiologic competence. Each part has its own rate of growth, which may be directly related to alterations in the size of the child (e.g., the heart rate). Skeletal muscle growth approximates whole body growth; brain, lymphoid, adrenal, and reproductive tissues follow distinct and individual patterns (Fig. 5-2). When growth deficiency has a secondary cause, such as severe illness or acute malnutrition, recovery from the illness or the establishment of an adequate diet will produce a dramatic acceleration of the growth rate that usually continues until the child’s individual growth pattern is resumed.
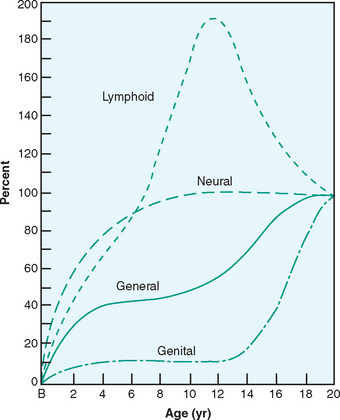
FIG. 5-2 Growth rates for the body as a whole and three types of tissues. Lymphoid: thymus, lymph nodes, and intestinal lymph masses. Neural: brain, dura, spinal cord, optic apparatus, and head dimensions. General: body as a whole; external dimension; and respiratory, digestive, renal, circulatory, and musculoskeletal systems. (From Jackson JA, Patterson DG, and Harris RE: The measurement of man, Minneapolis, 1930, University of Minnesota Press.) University of Minnesota Press
External Proportions
Variations in the growth rate of different tissues and organ systems produce significant changes in body proportions during childhood. The cephalocaudal trend of development is most evident in total body growth as indicated by these changes. During fetal development the head is the fastest-growing body part, and at 2 months of gestation the head constitutes 50% of total body length. During infancy growth of the trunk predominates; the legs are the most rapidly growing part during childhood; in adolescence, the trunk once again elongates. In the newborn infant the lower limbs are one third the total body length but only 15% of the total body weight; in the adult the lower limbs constitute one half of the total body height and 30% or more of the total body weight. As growth proceeds, the midpoint in head-to-toe measurements gradually descends from a level even with the umbilicus at birth to the level of the symphysis pubis at maturity.
Biologic Determinants of Growth and Development
The most prominent feature of childhood and adolescence is physical growth (Fig. 5-3). Throughout development various tissues in the body undergo changes in growth, composition, and structure. In some tissues the changes are continuous (e.g., bone growth and dentition); in others, significant alterations occur at specific stages (e.g., appearance of secondary sex characteristics). When these measurements are compared with standardized norms, a child’s developmental progress can be determined with a high degree of confidence (Table 5-1). Growth in children with Down syndrome differs from that in other children. They have slower growth velocity between 6 months and 3 years and then again in adolescence. Puberty occurs earlier, and they achieve shorter stature. This population of patients are frequent users of the health care system, often with multiple providers, and benefit from the use of the Down syndrome growth chart to monitor their growth (Cronk, Crocker, Pueschel, and others, 1988; Myrelid, Gustafsson, Ollars, and others, 2002).
TABLE 5-1
General Trends in Height and Weight Gain During Childhood
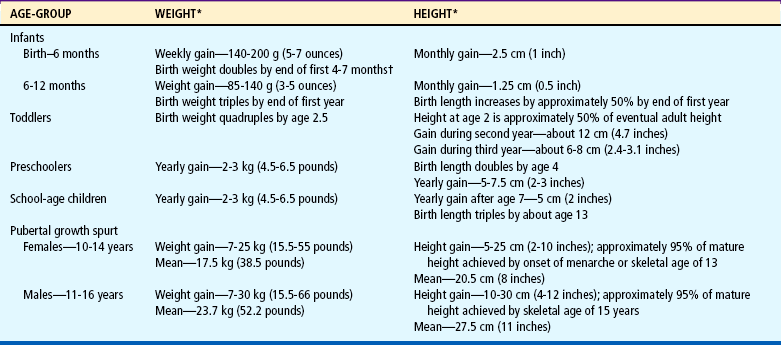
*Yearly height and weight gains for each age-group represent averaged estimates from a variety of sources.
†Jung FE, Czajka-Narins DM: Birth weight doubling and tripling times: an updated look at the effects of birth weight, sex, race, and type of feeding, Am J Clin Nutr 42:182-189, 1985.

Linear growth, or height, occurs almost entirely as a result of skeletal growth and is considered a stable measurement of general growth. Growth in height is not uniform throughout life but ceases when maturation of the skeleton is complete. The maximum rate of growth in length occurs before birth, but the newborn continues to grow at a rapid, though slower, rate.
At birth, weight is more variable than height and is, to a greater extent, a reflection of the intrauterine environment. The average newborn weighs from 3175 to 3400 g (7 to 7.5 pounds). In general, the birth weight doubles by 4 to 7 months of age and triples by the end of the first year. By the age of 2 to 2½ years the birth weight usually quadruples. After this point the “normal” rate of weight gain, just as the growth in height, assumes a steady annual increase of approximately 2 to 2.75 kg (4.4 to 6 pounds) per year until the adolescent growth spurt.
Both bone age determinants and state of dentition are used as indicators of development. Because both are discussed elsewhere, neither is elaborated here (see next section for bone age; see also Chapters 10 and 12 for dentition).
Skeletal Growth and Maturation
The most accurate measure of general development is skeletal or bone age, the radiologic determination of osseous maturation. Skeletal age appears to correlate more closely with other measures of physiologic maturity (such as onset of menarche) than with chronologic age or height. Bone age is determined by comparing the mineralization of ossification centers and advancing bony form to age-related standards.
Bone formation begins during the second month of fetal life when calcium salts are deposited in the intercellular substance (matrix) to form calcified cartilage first and then true bone. Bone formation exhibits some differences. In small bones the bone continues to form in the center and cartilage continues to be laid down on the surfaces. In long bones the ossification begins in the diaphysis (the long central portion of the bone) and continues in the epiphysis (the end portions of the bone). Between the diaphysis and the epiphysis, an epiphyseal cartilage plate (or growth plate) unites with the diaphysis by columns of spongy tissue, the metaphysis. Active growth in length takes place in the epiphyseal growth plate. Interference with this growth site by trauma or infection can result in deformity.
The first centers of ossification appear in the 2-month-old embryo, and at birth the number is approximately 400, about half the number at maturity. New centers appear at regular intervals during the growth period and provide the basis for assessment of bone age. Postnatally the earliest centers to appear (at 5 to 6 months of age) are those of the capitate and hamate bones in the wrist. Therefore radiographs of the hand and wrist provide the most useful areas for screening to determine skeletal age, especially before age 6 years. These centers appear earlier in girls than in boys.
Nurses must understand that the growing bones of children possess many unique characteristics. Bone fractures occurring at the growth plate may be difficult to discover and may significantly affect subsequent growth and development (Urbanski and Hanlon, 1996). Factors that may influence skeletal muscle injury rates and types in children and adolescents include (Kaczander, 1997; Caine, DiFiori, and Maffulli; 2006):
Less protective sports equipment for children
Less emphasis on conditioning, especially flexibility
In adolescents, fractures that are more common than ligamentous ruptures because of the rapid growth rate of the physeal (segment of tubular bone that is concerned mainly with growth) zone of hypertrophy
Neurologic Maturation
In contrast to other body tissues, which grow rapidly after birth, the nervous system grows proportionately more rapidly before birth. Two periods of rapid brain cell growth occur during fetal life: a dramatic increase in the number of neurons between 15 and 20 weeks of gestation and another increase at 30 weeks, which extends to 1 year of age. The rapid growth of infancy continues during early childhood and then slows to a more gradual rate during later childhood and adolescence.
Postnatal growth consists of increasing the amount of cytoplasm around the nuclei of existing cells, increasing the number and intricacy of communications with other cells, and advancing their peripheral axons to keep pace with expanding body dimensions. This allows for increasingly complex movement and behavior. Neurophysiologic changes also provide the foundation for language, learning, and behavior development. Neurologic or electroencephalographic development is sometimes used as an indicator of maturational age in the early weeks of life.
Lymphoid Tissues
Lymphoid tissues contained in the lymph nodes, thymus, spleen, tonsils, adenoids, and blood lymphocytes follow a growth pattern unlike that of other body tissues. These tissues are small in relation to total body size, but they are well developed at birth. They increase rapidly to reach adult dimensions by 6 years of age and continue to grow. At about age 10 to 12 years they reach a maximum development that is approximately twice their adult size. This is followed by a rapid decline to stable adult dimensions by the end of adolescence.
Development of Organ Systems
All tissues and organ systems undergo changes during development. Some are striking; others are subtle. Many have implications for assessment and care. Because the major importance of these changes relates to their dysfunction, the developmental characteristics of various systems and organs are discussed throughout the book as they relate to these areas. Physical characteristics and physiologic changes that vary with age are included in age-group descriptions.
PHYSIOLOGIC CHANGES
Physiologic changes that take place in all organs and systems are discussed as they relate to dysfunction. Other changes such as pulse and respiratory rates and blood pressure are an integral part of physical assessment (see Chapter 6). In addition, there are changes in basic functions, including metabolism, temperature, and patterns of sleep and rest.
Metabolism
The rate of metabolism when the body is at rest (basal metabolic rate, or BMR)demonstrates a distinctive change throughout childhood. Highest in the newborn infant, the BMR closely relates to the proportion of surface area to body mass, which changes as the body increases in size. In both sexes the proportion decreases progressively to maturity. The BMR is slightly higher in boys at all ages and further increases during pubescence over that in girls.
The rate of metabolism determines the caloric requirements of the child. The basal energy requirement of infants is about 108 kcal/kg of body weight and decreases to 40 to 45 kcal/kg at maturity (Table 5-2). Water requirements throughout life remain at approximately 1.5 ml/calorie of energy expended. Children’s energy needs vary considerably at different ages and with changing circumstances. The energy requirement to build tissue steadily decreases with age, following the general growth curve; however, energy needs vary with the individual child and may be considerably higher. For short periods (e.g., during strenuous exercise) and more prolonged periods (e.g., illness), the needs can be very high.
TABLE 5-2
Dietary Reference Intake for Calories and Protein Throughout Adolescence*
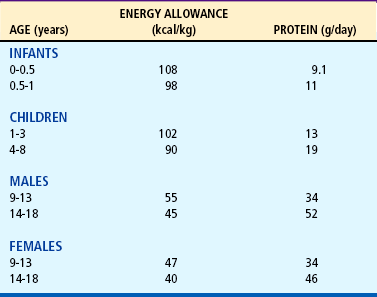
*According to the American Academy of Pediatrics, energy and protein needs during adolescence should be based on height rather than weight.
Data from Otten JJ, Hellwig J P, Meyers LD, editors: Dietary reference intakes: the essential guide to nutrient requirements, Washington, DC, 2006, National Academies Press. National Academies Press
Temperature
Body temperature, reflecting metabolism, decreases over the course of development (see inside back cover). Thermoregulation is one of the most important adaptation responses of the infant during the transition from intrauterine to extrauterine life. In the healthy neonate hypothermia can result in several negative metabolic consequences such as hypoglycemia, elevated bilirubin levels, and metabolic acidosis. Skin-to-skin care, also referred to as kangaroo care, is an effective way to prevent neonatal hypothermia in infants. Unclothed, diapered infants are placed on the parent’s bare chest after birth, promoting thermoregulation and attachment (Galligan, 2006). After the unstable regulatory ability in the neonatal period, heat production steadily declines as the infant grows into childhood. Individual differences of 0.5° to 1° F are normal, and occasionally a child normally displays an unusually high or low temperature. Beginning at approximately 12 years of age, girls display a temperature that remains relatively stable, whereas the temperature in boys continues to fall for a few more years. Females maintain a temperature slightly above that of males throughout life.
Even with improved temperature regulation, infants and young children are highly susceptible to temperature fluctuations. Body temperature responds to changes in environmental temperature and is increased with active exercise, crying, and emotional stress. Infections can cause a higher and more rapid temperature increase in infants and young children than in older children. In relation to body weight, an infant produces more heat per unit than adolescents. Consequently, during active play or when heavily clothed, an infant or small child is likely to become overheated.
Sleep and Rest
Sleep, a protective function in all organisms, allows for repair and recovery of tissues after activity. As in most aspects of development, there is wide variation among individual children in the amount and distribution of sleep at various ages. As children mature, there is a change in the total time they spend in sleep and the amount of time they spend in deep sleep.
Newborn infants sleep much of the time that is not occupied with feeding and other aspects of their care. As infants grow older, the total time spent in sleep gradually decreases, they remain awake for longer periods, and they sleep longer at night. For example, the length of a sleep cycle increases from approximately 50 to 60 minutes in the newborn infant to approximately 90 minutes in adolescence (Anders, Sadeh, and Appareddy, 2005). During the latter part of the first year, most children sleep through the night and take one or two naps during the day. By the time they are 12 to 18 months old, most children have eliminated the second nap. After age 3 years the child has usually given up daytime naps, except in cultures in which an afternoon nap or siesta is customary. Sleep time declines slightly from ages 4 to 10 and then increases somewhat during the pubertal growth spurt.
The quality of sleep changes as children mature. As children develop through adolescence, their need for sleep does not decline, but their opportunity for sleep may be affected by social, activity, and academic schedules. The time spent in deep, restful sleep increases from 50% in infancy to 80% in the older child.
TEMPERAMENT
Temperament is defined as “the manner of thinking, behaving, or reacting characteristic of an individual” (Chess and Thomas, 1999) and refers to the way in which a person deals with life. From the time of birth, children exhibit marked individual differences in the way they respond to their environment and the way others, particularly the parents, respond to them and their needs. A genetic basis has been suggested for some differences in temperament. Nine characteristics of temperament have been identified through interviews with parents (Box 5-2). Temperament refers to behavioral tendencies, not to discrete behavioral acts. There are no implications of good or bad. Most children can be placed into one of three common categories based on their overall pattern of temperamental attributes:
The easy child—Easy-going children are even tempered, are regular and predictable in their habits, and have a positive approach to new stimuli. They are open and adaptable to change and display a mild to moderately intense mood that is typically positive. Approximately 40% of children fall into this category.
The difficult child—Difficult children are highly active, irritable, and irregular in their habits. Negative withdrawal responses are typical, and they require a more structured environment. These children adapt slowly to new routines, people, or situations. Mood expressions are usually intense and primarily negative. They exhibit frequent periods of crying, and frustration often produces violent tantrums. This group represents about 10% of children.
The slow-to-warm-up child—Slow-to-warm-up children typically react negatively and with mild intensity to new stimuli and, unless pressured, adapt slowly with repeated contact. They respond with only mild but passive resistance to novelty or changes in routine. They are inactive and moody but show only moderate irregularity in functions. Fifteen percent of children demonstrate this temperament pattern.
Thirty-five percent of children either have some, but not all, of the characteristics of one of the categories or are inconsistent in their behavioral responses. Many normal children demonstrate this wide range of behavioral patterns.
Significance of Temperament
Observations indicate that children who display the difficult or slow-to-warm-up patterns of behavior are more vulnerable to the development of behavior problems in early and middle childhood. Any child can develop behavior problems if there is dissonance between the child’s temperament and the environment. Demands for change and adaptation that are in conflict with the child’s capacities can become excessively stressful. However, authorities emphasize that it is not the temperament patterns of children that place them at risk; it is the degree of fit between children and their environment, specifically their parents, that determines the degree of vulnerability. The potential for optimum development exists when environmental expectations and demands fit with the individual’s style of behavior and the parents’ ability to navigate this period (Chess and Thomas, 1999) (see Growth Failure [Failure to Thrive], Chapter 11).
Early identification of temperament provides a useful tool for caregivers in anticipating probable areas of difficulty or risk associated with development. For example, “difficult” children may be prone to colic in infancy, active children require more vigilance to prevent injury, and school entry requires different approaches for children with different temperaments.
Research indicates that irritable and unadaptable infants can raise doubts in mothers about their competence (Beck, 1996). Additional research indicates that a child’s temperament can affect parent-child interactions and can influence the parents’ self-esteem, marital harmony, mood, and overall satisfaction as parents (Carey, 1998). Studies on the relationship between temperament and the ability to perform a task successfully (mastery motivation) have found that infants with high mastery are more cooperative and less difficult (Morrow and Camp, 1996). Principles that can be used by nurses in direct patient care and in providing anticipatory guidance are listed in Box 5-3.
BOX 5-3 Activities to Promote Mastery Motivation
Encourage unobtrusive assistance during play.
Share pleasure with infant in accomplishments.
Don’t give immediate assistance during tasks.
Don’t interrupt infant during tasks.
Let infant initiate activities.
Limit controlling feedback during play.
Provide audio and visually responsive toys.
Provide early kinesthetic stimulation (picking up, rocking).
From Morrow JD, Camp BW: Mastery motivation and temperament of 7-month-old infants, Pediatr Nurs 22(3):211-217, 1996.
DEVELOPMENT OF PERSONALITY AND MENTAL FUNCTION
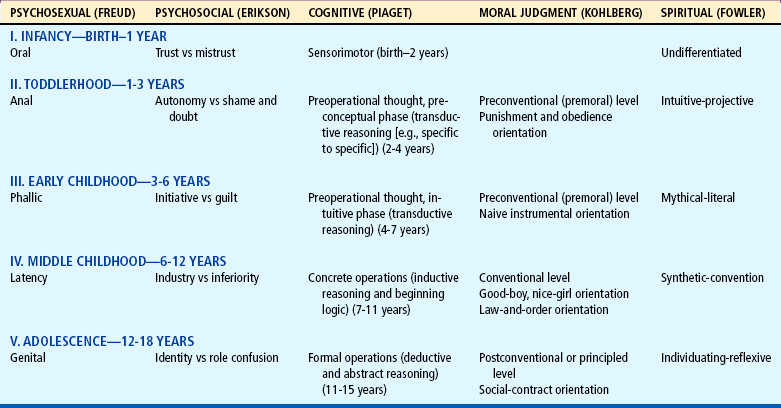
Personality and cognitive skills develop in much the same manner as biologic growth—new accomplishments build on previously mastered skills. Many aspects depend on physical growth and maturation. This is not a comprehensive account of the multiple facets of personality and behavior development. Many aspects are integrated with the child’s emotional and social development in later discussion of various age-groups. Table 5-3 summarizes some of the developmental theories.
THEORETIC FOUNDATIONS OF PERSONALITY DEVELOPMENT
Psychosexual Development (Freud)
According to Freud, all human behavior is energized by psychodynamic forces, and this psychic energy is divided among three components of personality: the id, the ego, and the superego. The id, the unconscious mind, is the inborn component that is driven by instincts. The id obeys the pleasure principle of immediate gratification of needs, regardless of whether the object or action can actually do so. The ego, the conscious mind, serves the reality principle. It functions as the conscious or controlling self that is able to find realistic means for gratifying the instincts while blocking the irrational thinking of the id. The superego, the conscience, functions as the moral arbitrator and represents the ideal. It is the mechanism that prevents individuals from expressing undesirable instincts that might threaten the social order.
Freud considered the sexual instincts to be significant in the development of the personality. However, he used the term psychosexual to describe any sensual pleasure. During childhood certain regions of the body assume a prominent psychologic significance as the source of new pleasures and new conflicts gradually shifts from one part of the body to another at particular stages of development:
Oral stage (birth to 1 year)—During infancy the major source of pleasure seeking is centered on oral activities such as sucking, biting, chewing, and vocalizing. Children may prefer one of these over the others, and the preferred method of oral gratification can provide some indication of the personality they develop.
Anal stage (1 to 3 years)—Interest during the second year of life centers in the anal region as sphincter muscles develop and children are able to withhold or expel fecal material at will. At this stage the climate surrounding toilet training can have lasting effects on children’s personalities.
Phallic stage (3 to 6 years)—During the phallic stage the genitalia become an interesting and sensitive area of the body. Children recognize differences between the sexes and become curious about the dissimilarities. This is the period around which the controversial issues of the Oedipus and Electra complexes, penis envy, and castration anxiety are centered.
Latency period (6 to 12 years)—During the latency period children elaborate on previously acquired traits and skills. Physical and psychic energy are channeled into acquisition of knowledge and vigorous play.
Genital stage (age 12 and older)—The last significant stage begins at puberty with maturation of the reproductive system and production of sex hormones. The genital organs become the major source of sexual tensions and pleasures, but energies are also invested in forming friendships and preparing for marriage.
Psychosocial Development (Erikson)
The most widely accepted theory of personality development is that advanced by Erikson (1963). Although built on Freudian theory, it is known as psychosocial development and emphasizes a healthy personality as opposed to a pathologic approach. Erikson also uses the biologic concepts of critical periods and epigenesis, describing key conflicts or core problems that the individual strives to master during critical periods in personality development. Successful completion or mastery of each of these core conflicts is built on the satisfactory completion or mastery of the previous stage.
Each psychosocial stage has two components—the favorable and the unfavorable aspects of the core conflict—and progress to the next stage depend on resolution of this conflict. No core conflict is ever mastered completely but remains a recurrent problem throughout life. No life situation is ever secure. Each new situation presents the conflict in a new form. For example, when children who have satisfactorily achieved a sense of trust encounter a new experience (e.g., hospitalization), they must again develop a sense of trust in those responsible for their care in order to master the situation. Erikson’s life-span approach to personality development consists of eight stages; however, only the first five relating to childhood are included here:
Trust vs mistrust (birth to 1 year)—The first and most important attribute to develop for a healthy personality is basic trust. Establishment of basic trust dominates the first year of life and describes all of the child’s satisfying experiences at this age. Corresponding to Freud’s oral stage, it is a time of “getting” and “taking in” through all the senses. It exists only in relation to something or someone; therefore consistent, loving care by a mothering person is essential for development of trust. Mistrust develops when trust-promoting experiences are deficient or lacking or when basic needs are inconsistently or inadequately met. Although shreds of mistrust are sprinkled throughout the personality, from a basic trust in parents stems trust in the world, other people, and oneself. The result is faith and optimism.
Autonomy vs shame and doubt (1 to 3 years)—Corresponding to Freud’s anal stage, the problem of autonomy can be symbolized by the holding on and letting go of the sphincter muscles. The development of autonomy during the toddler period is centered on children’s increasing ability to control their bodies, themselves, and their environment. They want to do things for themselves, using their newly acquired motor skills of walking, climbing, and manipulating and their mental powers of selecting and decision making. Much of their learning is acquired by imitating the activities and behavior of others. Negative feelings of doubt and shame arise when children are made to feel small and self-conscious, when their choices are disastrous, when others shame them, or when they are forced to be dependent in areas in which they are capable of assuming control. The favorable outcomes are self-control and willpower.
Initiative vs guilt (3 to 6 years)—The stage of initiative corresponds to Freud’s phallic stage and is characterized by vigorous, intrusive behavior; enterprise; and a strong imagination. Children explore the physical world with all their senses and powers (Fig. 5-4). They develop a conscience. No longer guided only by outsiders, they have an inner voice that warns and threatens. Children sometimes undertake goals or activities that are in conflict with those of parents or others, and being made to feel that their activities or imaginings are bad produces a sense of guilt. Children must learn to retain a sense of initiative without impinging on the rights and privileges of others. The lasting outcomes are direction and purpose.

FIG. 5-4 The stage of initiative is characterized by physical activity and imagination while children explore the physical world around them.
Industry vs inferiority (6 to 12 years)—The stage of industry is the latency period of Freud. Having achieved the more crucial stages in personality development, children are ready to be workers and producers. They want to engage in tasks and activities that they can carry through to completion; they need and want real achievement. Children learn to compete and cooperate with others, and they learn the rules. It is a decisive period in their social relationships with others. Feelings of inadequacy and inferiority may develop if too much is expected of them or if they believe that they cannot measure up to the standards set for them by others. The ego quality developed from a sense of industry is competence.
Identity vs role confusion (12 to 18 years)—Corresponding to Freud’s genital period, the development of identity is characterized by rapid and marked physical changes. Previous trust in their bodies is shaken, and children become overly preoccupied with the way they appear in the eyes of others as compared with their own self-concept. Adolescents struggle to fit the roles they have played and those they hope to play with the current roles and fashions adopted by their peers, to integrate their concepts and values with those of society, and to come to a decision regarding an occupation. Inability to solve the core conflict results in role confusion. The outcome of successful mastery is devotion and fidelity to others and to values and ideologies.
THEORETIC FOUNDATIONS OF MENTAL DEVELOPMENT
The term cognition refers to the process by which developing individuals become acquainted with the world and the objects it contains. Children are born with inherited potentials for intellectual growth, but they must develop that potential through interaction with the environment. By assimilating information through the senses, processing it, and acting on it, they come to understand relationships between objects and between themselves and their world. With cognitive development, children acquire the ability to reason abstractly, to think in a logical manner, and to organize intellectual functions or performances into higher-order structures. Language, morals, and spiritual development emerge as cognitive abilities advance.
Cognitive Development (Piaget)
Cognitive development consists of age-related changes that occur in mental activities. The best-known theory regarding children’s thinking, and a more comprehensive developmental theory than those already described, was developed by the Swiss psychologist Jean Piaget (1969). According to Piaget, intelligence enables individuals to make adaptations to the environment that increase the probability of survival, and through their behavior individuals establish and maintain equilibrium with the environment.
Piaget (1969) proposed three stages of reasoning: (1) intuitive, (2) concrete operational, and (3) formal operational. When they enter the stage of concrete logical thought at about age 7 years, children are able to make logical inferences, classify, and deal with quantitative relationships about concrete things. Not until adolescence are they able to reason abstractly with any degree of competence. Each stage is derived from and builds on the accomplishments of the previous stage in a continuous, orderly process. The course of intellectual development is both maturational and invariant and is divided into the following stages (ages are approximate):
Sensorimotor (birth to 2 years)—The sensorimotor stage of intellectual development consists of six substages (see pp. 327 and 412) that are governed by sensations in which simple learning takes place. Children progress from reflex activity through simple repetitive behaviors to imitative behavior. They develop a sense of cause and effect as they direct behavior toward objects. Problem solving is primarily by trial and error. They display a high level of curiosity, experimentation, and enjoyment of novelty and begin to develop a sense of self as they are able to differentiate themselves from their environment. They become aware that objects have permanence—that an object exists even though it is no longer visible. Toward the end of the sensorimotor period, children begin to use language and representational thought.
Preoperational (2 to 7 years)—The predominant characteristic of the preoperational stage of intellectual development is egocentrism, which in this sense does not mean selfishness or self-centeredness, but the inability to put oneself in the place of another. Children interpret objects and events not in terms of general properties, but in terms of their relationships or their use to them. They are unable to see things from any perspective other than their own; they cannot see another’s point of view, nor can they see any reason to do so (see Cognitive Development, Chapter 13).
Preoperational thinking is concrete and tangible. Children cannot reason beyond the observable, and they lack the ability to make deductions or generalizations. Thought is dominated by what they see, hear, or otherwise experience. However, they are increasingly able to use language and symbols to represent objects in their environment. Through imaginative play, questioning, and other interactions, they begin to elaborate concepts and to make simple associations between ideas. In the latter stage of this period their reasoning is intuitive (e.g., the stars have to go to bed just as they do), and they are only beginning to deal with problems of weight, length, size, and time. Reasoning is also transductive—because two events occur together, they cause each other, or knowledge of one characteristic is transferred to another (e.g., all women with big bellies have babies).
Concrete operations (7 to 11 years)—At this age thought becomes increasingly logical and coherent. Children are able to classify, sort, order, and otherwise organize facts about the world to use in problem solving. They develop a new concept of permanence’ conservation (see Cognitive Development [Piaget], Chapter 16); that is, they realize that physical factors such as volume, weight, and number remain the same even though outward appearances are changed. They are able to deal with a number of different aspects of a situation simultaneously. They do not have the capacity to deal in abstraction; they solve problems in a concrete, systematic fashion based on what they can perceive. Reasoning is inductive. Through progressive changes in thought processes and relationships with others, thought becomes less self-centered. They can consider points of view other than their own. Thinking has become socialized.
Formal operations (11 to 15 years)—Formal operational thought is characterized by adaptability and flexibility. Adolescents can think in abstract terms, use abstract symbols, and draw logical conclusions from a set of observations. For example, they can solve the following question: If A is larger than B, and B is larger than C, which symbol is the largest? (The answer is A.) They can make hypotheses and test them; they can consider abstract, theoretic, and philosophic matters. Although they may confuse the ideal with the practical, most contradictions in the world can be dealt with and resolved.
Language Development
Children are born with the mechanism and capacity to develop speech and language skills. However, they do not speak spontaneously. The environment must provide a means for them to acquire these skills. Speech requires intact physiologic structure and function (including respiratory, auditory, and cerebral) plus intelligence, a need to communicate, and stimulation.
The rate of speech development varies from child to child and is directly related to neurologic competence and cognitive development. Gesture precedes speech, and in this way a small child communicates satisfactorily. As speech develops, gesture recedes but never disappears entirely. Research suggests that infants can learn sign language before vocal language and that it may enhance the development of vocal language (Thompson, Cotner-Bichelman, McKerchar, and others, 2007). At all stages of language development, children’s comprehension vocabulary (what they understand) is greater than their expressed vocabulary (what they can say), and this development reflects a continuing process of modification that involves both the acquisition of new words and the expanding and refining of word meanings previously learned. By the time they begin to walk, children are able to attach a name to objects and persons.
The first parts of speech used are nouns, sometimes verbs (e.g., “go”), and combination words (such as “bye-bye”). Responses are usually structurally incomplete during the toddler period, although the meaning is clear. Next they begin to use adjectives and adverbs to qualify nouns, followed by adverbs to qualify nouns and verbs. Later, pronouns and gender words are added (such as “he” and “she”). By the time children enter school, they are able to use simple, structurally complete sentences that average five to seven words.
Moral Development (Kohlberg)
Children also acquire moral reasoning in a developmental sequence. Moral development, as described by Kohlberg (1968), is based on cognitive developmental theory and consists of the following three major levels, each of which has two stages:
Preconventional level—The preconventional level of moral development parallels the preoperational level of cognitive development and intuitive thought. Culturally oriented to the labels of good/bad and right/wrong, children integrate these in terms of the physical or pleasurable consequences of their actions. At first children determine the goodness or badness of an action in terms of its consequences. They avoid punishment and obey without question those who have the power to determine and enforce the rules and labels. They have no concept of the basic moral order that supports these consequences. Later, children determine that the right behavior consists of that which satisfies their own needs (and sometimes the needs of others). Although elements of fairness, give and take, and equal sharing are evident, they are interpreted in a practical, concrete manner without loyalty, gratitude, or justice.
Conventional level—At the conventional stage children are concerned with conformity and loyalty. They value the maintenance of family, group, or national expectations regardless of consequences. Behavior that meets with approval and pleases or helps others is considered good. One earns approval by being “nice.” Obeying the rules, doing one’s duty, showing respect for authority, and maintaining the social order are the correct behaviors. This level is correlated with the stage of concrete operations in cognitive development.
Postconventional, autonomous, or principled level—At the postconventional level the individual has reached the cognitive stage of formal operations. Correct behavior tends to be defined in terms of general individual rights and standards that have been examined and agreed on by the entire society. Although procedural rules for reaching consensus become important, with emphasis on the legal point of view, there is also emphasis on the possibility for changing law in terms of societal needs and rational considerations.
The most advanced level of moral development is one in which self-chosen ethical principles guide decisions of conscience. These are abstract and ethical but universal principles of justice and human rights with respect for the dignity of persons as individuals. It is believed that few persons reach this stage of moral reasoning.
Spiritual Development (Fowler)
Spiritual beliefs are closely related to the moral and ethical portion of the child’s self-concept and, as such, must be considered as part of the child’s basic needs assessment. Children need to have meaning, purpose, and hope in their lives. Also, the need for confession and forgiveness is present, even in very young children. Extending beyond religion (an organized set of beliefs and practices), spirituality affects the whole person: mind, body, and spirit. Fowler (1981) has identified seven stages in the development of faith, four of which are closely associated with and parallel cognitive and psychosocial development in childhood:
Stage 0: Undifferentiated—This stage of development encompasses the period of infancy during which children have no concept of right or wrong, no beliefs, and no convictions to guide their behavior. However, the beginnings of a faith are established with the development of basic trust through their relationships with the primary caregiver.
Stage 1: Intuitive-projective—Toddlerhood is primarily a time of imitating the behavior of others. Children imitate the religious gestures and behaviors of others without comprehending any meaning or significance to the activities. During the preschool years children assimilate some of the values and beliefs of their parents. Parental attitudes toward moral codes and religious beliefs convey to children what they consider to be good and bad. Children still imitate behavior at this age and follow parental beliefs as part of their daily lives rather than through an understanding of their basic concepts.
Stage 2: Mythical-literal—Through the school-age years, spiritual development parallels cognitive development and is closely related to children’s experiences and social interaction. Most have a strong interest in religion during the school-age years. They accept the existence of a deity, and petitions to an omnipotent being are important and expected to be answered; good behavior is rewarded, and bad behavior is punished. Their developing conscience bothers them when they disobey. They have a reverence for thoughts and matters and are able to articulate their faith. They may even question its validity.
Stage 3: Synthetic-convention—As children approach adolescence, however, they become increasingly aware of spiritual disappointments. They recognize that prayers are not always answered (at least on their own terms) and may begin to abandon or modify some religious practices. They begin to reason, to question some of the established parental religious standards, and to drop or modify some religious practices.
Stage 4: Individuating-reflexive—Adolescents become more skeptical and begin to compare the religious standards of their parents with those of others. They attempt to determine which to adopt and incorporate into their own set of values. They also begin to compare religious standards with the scientific viewpoint. It is a time of searching rather than reaching. Adolescents are uncertain about many religious ideas but will not achieve profound insights until late adolescence or early adulthood.
DEVELOPMENT OF SELF-CONCEPT
Self-concept is how an individual describes himself or herself. The term self-concept includes all the notions, beliefs, and convictions that constitute an individual’s self-knowledge and that influence that individual’s relationships with others. It is not present at birth but develops gradually as a result of unique experiences within the self, with significant others, and with the realities of the world. However, an individual’s self-concept may or may not reflect reality.
In infancy the self-concept is primarily an awareness of one’s independent existence learned in part as a result of social contacts and experiences with others. The process becomes more active during toddlerhood as children explore the limits of their capacities and the nature of their impact on others. School-age children are more aware of differences among people, are more sensitive to social pressures, and become more preoccupied with issues of self-criticism and self-evaluation. During early adolescence children focus more on physical and emotional changes taking place and on peer acceptance. Self-concept is crystallized during later adolescence as young people organize their self-concept around a set of values, goals, and competencies acquired throughout childhood.
Body Image
A vital component of self-concept, body image refers to the subjective concepts and attitudes that individuals have toward their own bodies. It consists of the physiologic (the perception of one’s physical characteristics), psychologic (values and attitudes toward the body, abilities, and ideals), and social nature of one’s image of self (the self in relation to others). All three of the components interrelate with one another. Body image is a complex phenomenon that evolves and changes during the process of growth and development. Any actual or perceived deviation from the “norm” (no matter how this is interpreted) is cause for concern. The extent to which a characteristic, defect, or disease affects children’s body image is influenced by the attitudes and behavior of those around them.
The significant others in their lives exert the most important and meaningful impact on children’s body image. Labels that are attached to them (such as “skinny,” “pretty,” or “fat”) or body parts (such as “ugly mole,” “bug eyes,” or “yucky skin”) are incorporated into the body image. Because they lack the understanding of deviations from the physical standard or norm, children notice prominent differences in others and unwittingly make rude or cruel remarks about such minor deviations as large or widely spaced front teeth, large or small eyes, moles, or extreme variations in height.
Infants receive input about their bodies through self-exploration and sensory stimulation from others. As they begin to manipulate their environment, they become aware of their bodies as separate from others. Toddlers learn to identify the various parts of their bodies and are able to use symbols to represent objects. Preschoolers become aware of the wholeness of their bodies and discover the genitalia. Exploration of the genitalia and the discovery of differences between the sexes become important. There is only a vague concept of internal organs and function (Stuart and Laraia, 2000).
School-age children begin to learn about internal body structure and function and become aware of differences in body size and configuration. They are highly influenced by the cultural norms of society and current fads. Children whose bodies deviate from the norm are often criticized or ridiculed. Adolescence is the age when children become most concerned about the physical self. The unfamiliar body changes, and the new physical self must be integrated into the self-concept. Adolescents face conflicts over what they see and what they visualize as the ideal body structure. Body image formation during adolescence is a crucial element in the shaping of identity, the psychosocial crisis of adolescence.
Self-Esteem
Self-esteem is the value that an individual places on oneself and refers to an overall evaluation of oneself (Willoughby, King, and Polatajko, 1996). Self-esteem is described as the affective component of the self, whereas self-concept is the cognitive component; however, the two terms are almost indistinguishable and are often used interchangeably.
The term self-esteem refers to a personal, subjective judgment of one’s worthiness derived from and influenced by the social groups in the immediate environment and individuals’ perceptions of how they are valued by others. Self-esteem changes with development. Highly egocentric toddlers are unaware of any difference between competence and social approval. On the other hand, preschool and early school-age children are increasingly aware of the discrepancy between their competencies and the abilities of more advanced children. Being accepted by adults and peers outside the family group becomes more important to them. Positive feedback enhances their self-esteem; they are vulnerable to feelings of worthlessness and are anxious about failure.
As children’s competencies increase and they develop meaningful relationships, their self-esteem rises. Their self-esteem is again at risk during early adolescence when they are defining an identity and sense of self in the context of their peer group. Unless children are continually made to feel incompetent and of little worth, a decrease in self-esteem during vulnerable times is only temporary. Children assess the following aspects of themselves in forming an overall evaluation of their self-esteem (Sieving and Zirbel-Donisch, 1990):
Competence—How adequate are my cognitive, physical, and social skills?
Sense of control—How well can I complete tasks needed to produce desired actions? Is someone or something specific vs luck or chance responsible for my successes and failures?
Moral worth—How closely do my actions and behaviors meet moral standards that have been set?
Worthiness of love and acceptance—How worthy am I of love and acceptance from parents, other significant adults, siblings, and peers?
Factors that influence the formation of a child’s self-esteem include (1) the child’s temperament and personality, (2) abilities and opportunities available to accomplish age-appropriate developmental tasks, (3) how significant others interact with the child, and (4) social roles assumed and the expectations of these roles (see also Psychosocial History, Chapter 6).
ROLE OF PLAY IN DEVELOPMENT
Through the universal medium of play, children learn what no one can teach them. They learn about their world and how to deal with this environment of objects, time, space, structure, and people. They learn about themselves operating within that environment—what they can do, how to relate to things and situations, and how to adapt themselves to the demands society makes on them. Play is the work of the child. In play, children continually practice the complicated, stressful processes of living, communicating, and achieving satisfactory relationships with other people.
CLASSIFICATION OF PLAY
From a developmental point of view, patterns of children’s play can be categorized according to content and social character. In both there is an additive effect; each builds on past accomplishments, and some element of each is maintained throughout life. At each stage in development the new predominates.
CONTENT OF PLAY
The content of play involves primarily the physical aspects of play, although social relationships cannot be ignored. The content of play follows the directional trend of the simple to the complex:
Social-affective play—Play begins with social-affective play, wherein infants take pleasure in relationships with people. As adults talk, touch, nuzzle, and in various ways elicit a response from an infant, the infant soon learns to provoke parental emotions and responses with such behaviors as smiling, cooing, or initiating games and activities. The type and intensity of the adult behavior with children vary among cultures.
Sense-pleasure play—Sense-pleasure play is a nonsocial stimulating experience that originates from without. Objects in the environment—light and color, tastes and odors, textures and consistencies—attract children’s attention, stimulate their senses, and give pleasure. Pleasurable experiences are derived from handling raw materials (water, sand, food), from body motion (swinging, bouncing, rocking), and from other uses of senses and abilities (smelling, humming) (Fig. 5-5).

Skill play—After infants have developed the ability to grasp and manipulate, they persistently demonstrate and exercise their newly acquired abilities through skill play, repeating an action over and over again. The element of sense-pleasure play is often evident in the practicing of a new ability, but all too frequently the determination to conquer the elusive skill produces pain and frustration (e.g., learning to get into a play car) (Fig. 5-6).

FIG. 5-6 After infants develop new skills to grasp and manipulate, they begin to conquer new abilities such as getting on a play motorcycle.
Unoccupied behavior—In unoccupied behavior children are not playful but focusing their attention momentarily on anything that strikes their interest. Children daydream, fiddle with clothes or other objects, or walk aimlessly. This role differs from that of onlookers, who actively observe the activity of others.
Dramatic, or pretend, play—One of the vital elements in children’s process of identification is dramatic play, also known as symbolic or pretend play. It begins in late infancy (11 to 13 months) and is the predominant form of play in the preschool child. After children begin to invest situations and people with meanings and to attribute affective significance to the world, they can pretend and fantasize almost anything. By acting out events of daily life, children learn and practice the roles and identities modeled by the members of their family and society. Children’s toys, replicas of the tools of society, provide a medium for learning about adult roles and activities that may be puzzling and frustrating to them. Interacting with the world is one way children get to know it. The simple, imitative, dramatic play of the toddler, such as using the telephone, driving a car, or rocking a doll, evolves into more complex, sustained dramas of the preschooler, which extend beyond common domestic matters to the wider aspects of the world and the society, such as playing police officer, storekeeper, teacher, or nurse. Older children work out elaborate themes, act out stories, and compose plays.
Games—Children in all cultures engage in games alone and with others. Solitary activity involving games begins as very small children participate in repetitive activities and progress to more complicated games that challenge their independent skills such as puzzles, solitaire, and computer or video games. Very young children participate in simple, imitative games such as pat-a-cake and peek-a-boo. Preschool children learn and enjoy formal games, beginning with ritualistic, self-sustaining games such as ring-around-a-rosy and London Bridge. With the exception of some simple board games, preschool children do not engage in competitive games. Preschoolers hate to lose and will try to cheat, want to change rules, or demand exceptions and opportunities to change their moves. School-age children and adolescents enjoy competitive games, including cards, checkers, and chess, and physically active games such as baseball.
SOCIAL CHARACTER OF PLAY
The play interactions of infancy are between the child and an adult. Children continue to enjoy the company of an adult but are increasingly able to play alone. As age advances, interaction with age-mates increases in importance and becomes an essential part of the socialization process. Through interaction, highly egocentric infants, unable to tolerate delay or interference, ultimately acquire concern for others and the ability to delay gratification or even to reject gratification at the expense of another. A pair of toddlers will engage in considerable combat because their personal needs cannot tolerate delay or compromise. By the time they reach age 5 or 6 years, children are able to arrive at a compromise or make use of arbitration, usually after they have attempted but failed to gain their own way. Through continued interaction with peers and the growth of conceptual abilities and social skills, children are able to increase participation with others in the following types of play:
Onlooker play—During onlooker play, children watch what other children are doing but make no attempt to enter into the play activity. There is an active interest in observing the interaction of others but no movement toward participating. Watching an older sibling bounce a ball is a common example of the onlooker role.
Solitary play—During solitary play, children play alone with toys different from those used by other children in the same area. They enjoy the presence of other children but make no effort to get close to or speak to them. Their interest is centered on their own activity, which they pursue with no reference to the activities of the others.
Parallel play—During parallel activities children play independently but among other children. They play with toys like those the children around them are using, but as each child sees fit, neither influencing nor being influenced by the other children. Each plays beside, but not with, other children (Fig. 5-7). There is no group association. Parallel play is the characteristic play of toddlers, but it may also occur in other groups of any age. Individuals who are involved in a creative craft with each person separately working on an individual project are engaged in parallel play.

Associative play—In associative play, children play together and are engaged in a similar or even identical activity, but there is no organization, division of labor, leadership assignment, or mutual goal. Children borrow and lend play materials, follow each other with wagons and tricycles, and sometimes attempt to control who may or may not play in the group. Each child acts according to his or her own wishes; there is no group goal (Fig. 5-8). For example, two children play with dolls, borrowing articles of clothing from each other and engaging in similar conversation, but neither directs the other’s actions or establishes rules regarding the limits of the play session. There is a great deal of behavioral contagion: when one child initiates an activity, the entire group follows the example.

Cooperative play—Cooperative play is organized, and children play in a group with other children (Fig. 5-9). They discuss and plan activities for the purposes of accomplishing an end—to make something, to attain a competitive goal, to dramatize situations of adult or group life, or to play formal games. The group is loosely formed, but there is a marked sense of belonging or not belonging. The goal and its attainment require organization of activities, division of labor, and role playing. The leader-follower relationship is definitely established, and the activity is controlled by one or two members who assign roles and direct the activity of the others. The activity is organized to allow one child to supplement another’s function to complete the goal.

FUNCTIONS OF PLAY
Sensorimotor activity is a major component of play at all ages and is the predominant form of play in infancy. Active play is essential for muscle development and serves a useful purpose as a release for surplus energy. Through sensorimotor play, children explore the nature of the physical world. Infants gain impressions of themselves and their world through tactile, auditory, visual, and kinesthetic stimulation. Toddlers and preschoolers revel in body movement and exploration of objects in space. With increasing maturity, sensorimotor play becomes more differentiated and involved. Whereas very young children run for the sheer joy of body movement, older children incorporate or modify the motions into increasingly complex and coordinated activities such as races, games, roller skating, and bicycle riding.
Intellectual Development
Through exploration and manipulation children learn colors, shapes, sizes, textures, and the significance of objects. They learn the significance of numbers and how to use them; they learn to associate words with objects; and they develop an understanding of abstract concepts and spatial relationships, such as up, down, under, and over. Activities such as puzzles and games help them develop problem-solving skills. Books, stories, films, and collections expand knowledge and provide enjoyment as well. Play provides a means to practice and expand language skills. Through play, children continually rehearse past experiences to assimilate them into new perceptions and relationships. Play helps children comprehend the world in which they live and distinguish between fantasy and reality.
Socialization
From very early infancy children show interest and pleasure in the company of others. Their initial social contact is with the mothering person, but through play with other children they learn to establish social relationships and solve the problems associated with these relationships. They learn to give and take, which is more readily learned from critical peers than from the more tolerant adults. They learn the sex role that society expects them to fulfill, as well as approved patterns of behavior and deportment. Closely associated with socialization is development of moral values and ethics. Children learn right from wrong, the standards of the society, and to assume responsibility for their actions.
Creativity
In no other situation is there more opportunity to be creative than in play. Children can experiment and try out their ideas in play through every medium at their disposal, including raw materials, fantasy, and exploration. Creativity is stifled by pressure toward conformity; therefore striving for peer approval may inhibit creative endeavors in the school-age or adolescent child. Creativity is primarily a product of solitary activity, yet creative thinking is often enhanced in group settings where listening to others’ ideas stimulates further exploration of one’s own ideas. After children feel the satisfaction of creating something new and different, they transfer this creative interest to situations outside the world of play.
Self-Awareness
Beginning with active explorations of their bodies and awareness of themselves as separate from the mother, the process of developing a self-identity is facilitated through play activities. Children learn who they are and their place in the world. They become increasingly able to regulate their own behavior, to learn what their abilities are, and to compare their abilities with those of others. Through play, children are able to test their abilities, to assume and try out various roles, and to learn the effect their behavior has on others. They learn the sex role that society expects them to fulfill, as well as approved patterns of behavior and deportment.
Therapeutic Value
Play is therapeutic at any age (Fig. 5-10). In play, children can express emotions and release unacceptable impulses in a socially acceptable fashion. Children are able to experiment and test fearful situations and can assume and vicariously master the roles and positions that they are unable to perform in the world of reality. Children reveal much about themselves in play. Through play, children are able to communicate to the alert observer the needs, fears, and desires that they are unable to express with their limited language skills. Throughout their play, children need the acceptance of adults and their presence to help them control aggression and to channel their destructive tendencies.

Moral Value
Although children learn at home and at school those behaviors considered right and wrong in the culture, the interaction with peers during play contributes significantly to their moral training. Nowhere is the enforcement of moral standards as rigid as in the play situation. If they are to be acceptable members of the group, children must adhere to the accepted codes of behavior of the culture (e.g., fairness, honesty, self-control, consideration for others). Children soon learn that their peers are less tolerant of violations than are adults and that to maintain a place in the play group, they must conform to the standards of the group.
TOYS
The type of toys chosen by or provided for children can support and enhance the child’s development in the areas just described. Although no scientific evidence shows that any toy is necessary for optimal learning, toys offer an opportunity to bring the child and parent together. Research has indicated that a positive parent-child interaction can enhance early childhood brain development (American Academy of Pediatric, 2003). Toys that are small replicas of the culture and its tools help children assimilate into their culture. Toys that require pushing, pulling, rolling, and manipulating teach them about physical properties of the items and help develop muscles and coordination. Rules and the basic elements of cooperation and organization are learned through board games.
Because they can be used in a variety of ways, raw materials with which children can exercise their own creativity and imaginations are sometimes superior to ready-made items. For example, building blocks can be used to construct a variety of structures, to count, and to learn shapes and sizes.
Toy Safety
Selection of toys and play equipment is a joint effort between parents and children, but evaluation of their safety is the responsibility of the adult. Government agencies do not inspect and police all toys on the market. Therefore adults who purchase, supervise purchases, or allow children to use play equipment need to evaluate such equipment for its safety and age appropriateness. This includes toys that are gifts or those that are purchased by the children themselves (see Family-Centered Care box). A choke tube tester, about the same diameter as a child’s windpipe, can be used to determine whether a toy is small enough to be a choking hazard. Parents should also be alert to notices of toys determined to be defective and recalled by the manufacturers. Parents and health workers can obtain information on a variety of recalled products and can report potentially dangerous toys and child products to the U.S. Consumer Product Safety Commission (CPSC) * or, in Canada, the Canadian Toy Testing Council. †
SELECTED FACTORS THAT INFLUENCE DEVELOPMENT
Inherited characteristics have a profound influence on development. The sex of the child, determined by random selection at the time of conception, directs both the pattern of growth and the behavior of others toward the child. In all cultures, attitudes and expectations are shaped by the sex of the child. Sex and other hereditary determinants strongly affect the end result of growth and the rate of progress toward it. There is a high correlation between parent and child with regard to traits such as height, weight, and rate of growth. Most physical characteristics, including shape and form of features, body build, and physical peculiarities, are inherited and can influence the way in which children grow and interact with their environment. Many dimensions of personality, such as temperament, activity level, responsiveness, and a tendency toward shyness, are believed to be inherited.
Differences in health and vigor of children may be attributed to hereditary traits. An inherited physical or mental disorder will alter or modify a child’s physical or emotional growth and interactions. The extent to which disabling conditions interfere with the child’s growth and well-being is considered in relation to numerous disabilities throughout the remainder of the book.
NEUROENDOCRINE FACTORS
The hypothalamic-pituitary axis produces a number of releasing and inhibitory hormones that influence growth. There is evidence, based on observations of denervated skeletal muscles, that the peripheral nervous system may influence growth, since muscles deprived of nerve supply degenerate. Many of these effects are not sufficiently explained by disuse or diminished blood supply.
Probably all hormones affect growth in some fashion. Three hormones—growth hormone, thyroid hormone, and androgens—when given to persons deficient in these hormones, stimulate protein anabolism and thereby produce retention of elements essential for building protoplasm and bony tissue. It appears that each of the hormones that has a significant influence on growth manifests its major effect at a different period of growth (see Chapter 29).
 FAMILY-CENTERED CARE
FAMILY-CENTERED CAREToy Safety*
Select toys that suit the skills, abilities, and interests of children.
Select toys that are safe for the specific child; look for a label that indicates the intended age-group. Toys that are safe for one age may not be safe for another.
For infants, toddlers, and all children who still mouth objects, avoid toys with small parts that may pose a fatal choking or aspiration hazard. Toys in this category are usually labeled, “Not recommended for children under 3 years.”
For infants avoid toys with strings or cords that are 7 inches or longer because they may cause strangulation.
For all children younger than 8 years avoid electric toys with heating elements.
For children younger than 5 years avoid arrows or darts.
Check for safety labels such as “flame retardant” or “flame resistant.” Select toys durable enough to survive rough play; look for sturdy
construction such as tightly secured eyes, nose, or any small parts. Select toys light enough that they will not cause harm if one falls on a child.
Look for toys with smooth, rounded edges. Avoid toys with sharp edges that can cut or that have sharp points. Points on the inside of the toy can puncture the skin if the toy is broken.
Avoid toys with any shooting or throwing objects that can injure eyes. This includes toys with which other missiles such as sticks or pebbles might be used as substitutes for the intended projectiles.
Arrows and darts used by children should have blunt tips and be manufactured from resilient materials; make certain the tips are securely attached.
Make certain that materials in toys are nontoxic by checking where the toy is manufactured, looking for recalls on toys, and checking the news.
Avoid toys that make loud noises that might damage a child’s hearing. Even some squeaking toys are too loud when held close to the ear.
If selecting caps for cap guns, look for the label required by federal law to be on boxes or packages of caps, which states: “Warning–Do not fire closer than 1 foot to the ear. Do not use indoors.”
If selecting a toy gun, be certain that the barrel or the entire gun is brightly colored to avoid being mistaken for a real gun.
BB guns or pellet rifles should not be given to children under the age of 16.
Electric toys should be labeled UL, which means they have met the safety standards of the Underwriters Laboratories.
Check toy instructions for clarity. They should be clear to an adult and, when appropriate, to the child.
Maintain a safe play environment.
Remove and discard plastic wrappings on toys immediately; they could suffocate a child.
Remove large toys, bumper pads, and boxes from playpens; an adventuresome child can use such items as a means of climbing or falling out.
Supervise young children closely during play. Teach children how to use toys properly and safely.
Instruct older children to keep their toys away from younger brothers, sisters, and friends.
Keep children who are playing with riding toys away from stairs, hills, traffic, and swimming pools.
Establish and enforce rules regarding protective gear.
Insist that children wear helmets when using bicycles, skateboards, or in-line skates.
Insist that children wear gloves and wrist, elbow, and knee pads when using skateboards or in-line skates.
Instruct children on electrical safety.
Teach children the proper way to unplug an electric toy–pull on the plug, not the cord.
Teach children to beware of electrical appliances and even electrically operated playthings; often children are unfamiliar with the hazards of electricity in association with water.
Teach children the safe use of utensils that under certain circumstances can cause injury–scissors, knives, needles, heating elements, loops, long string, or cord.
Inspect old and new toys regularly for breakage, loose parts, and other potential hazards.
Look for jagged or sharp edges or broken parts that might constitute a choking hazard.
Check movable parts to make certain they are attached securely to the toys; sometimes pieces that are safe when attached to the toy become a danger when detached.
Examine all outdoor toys regularly for rust and weak or sharp parts that could become a danger to a child.
Check electrical cords and plugs for cracked or fraying parts.
Maintain toys in good repair, without signs of possible hazards such as sharp edges, splinters, weak seams, or rust.
Make repairs immediately, or discard out of reach of children.
Sand sharp wooden toys or splintered surfaces so they are smooth.
Use only paint labeled “nontoxic” to repaint toys, toy boxes, or children’s furniture.
Provide a safe place for children to store toys, and teach them how to store toys safely to prevent accidental injury from stepping, tripping, or falling on a toy.
Select a toy chest or toy box that is ventilated, is free of self-locking devices that could trap a child inside, and has a lid designed not to pinch a child’s fingers or fall on a child’s head.
To avoid entrapment and suffocation, containers other than toy chests used for storage purposes should be fitted with spring-loaded support devices if they have a hinged lid.
Playthings meant for older children and adults should be safely stowed away on high shelves, in locked closets, or in other areas unavailable to younger children.
*Another helpful resource is Toy safety: guidelines for parents from American Academy of Pediatrics, Division of Publications, 141 Northwest Point Blvd., Elk Grove Village, IL 60007-1098; http://www.aap.org.
 COMMUNITY FOCUS
COMMUNITY FOCUSCurrent research indicates that new lower-fat recipes in school lunch programs are well accepted by children (Matvienko, 2007). However, less-healthy foods are still more readily available than more-healthy foods in our nation’s schools (Delva, O’Malley, Johnston, 2007).
NUTRITION
Nutrition is probably the single most important influence on growth. Dietary factors regulate growth at all stages of development, and their effects are exerted in numerous and complex ways. During the rapid prenatal growth period, poor nutrition may influence development from the time of implantation of the ovum until birth. During infancy and childhood the demand for calories is relatively great, as evidenced by the rapid increase in both height and weight. At this time protein and caloric requirements are higher than at almost any period of postnatal development. As the growth rate slows, with its concomitant decrease in metabolism, there is a corresponding reduction in caloric and protein requirements (see Table 5-2).
Growth is uneven during the periods of childhood between infancy and adolescence, when there are plateaus and small growth spurts. The child’s appetite fluctuates in response to these variations until the turbulent growth spurt of adolescence, when adequate nutrition is extremely important but may be subjected to numerous emotional influences. Adequate nutrition is closely related to good health throughout life, and an overall improvement in nourishment is evidenced by the gradual increase in size and early maturation of children in this century (see Community Focus box).
INTERPERSONAL RELATIONSHIPS
Relationships with significant others play a critical role in development, particularly in emotional, intellectual, and personality development. Not only do the quality and quantity of contacts with other persons exert an influence on the growing child, but the widening range of contacts is essential to learning and developing a healthy personality.
The mothering person is unquestionably the single most influential person during early infancy. This person is the one who meets the infant’s basic needs of food, warmth, comfort, and love. He or she provides stimulation for the child’s senses and facilitates his or her expanding capacities. Through this person the child learns to trust the world and feel secure to venture in increasingly wider relationships.
It is generally the parents who are most influential in helping the child to assume sex-role identification. Parents define and reinforce acceptable sex-role behavior and provide sex-appropriate role models for the child. In the absence of a sex-role model in the family setting, the child may adopt some characteristics of the opposite-sex parent or sibling. Frequently the child identifies with a teacher or other significant person of the same sex.
Siblings are children’s first peers, and the way in which they learn to relate to each other affects later interactions with peers outside the family group. The sphere of persons from whom children seek approval widens to include other members of their family, their peers, and, to a lesser extent, other authority figures (e.g., teachers). The increasing importance of the peer group in determining the behavior of school-age children and adolescents is well documented (Fig. 5-11).

FIG. 5-11 Peers become increasingly important as children develop friendships outside the family group.
When children fail to have high-quality interpersonal relationships with mothering persons, they experience emotional deprivation. The most prominent feature of emotional deprivation, particularly during the first year, is developmental delays. Much of the information regarding the adverse effects of interpersonal influences on development has been acquired through retrospective studies of gross deprivation and trauma. The most notable instances involved homeless infants who were placed in institutions for care. Those infants who did not receive consistent mothering care failed to gain weight even with an adequate diet; were pale, listless, and immobile; and were unresponsive to stimuli such as smiling or cooing that usually elicit a response from the normal infant. If emotional deprivation continues for a sufficient length of time, the child may not survive infancy.
Although the most remarkable examples of emotional deprivation were first recognized among infants in institutions, the term masked deprivation has been used to describe children reared in homes in which there is a distorted parent-child relationship or otherwise disordered home environment. Infants do not thrive if the caregiving person is hostile, fearful of handling them, or indifferent to them and their needs. Such children exhibit poor growth even though they are apparently free of physical disease. Growth delays in these children are believed to be caused by a psychologically induced endocrine imbalance that interferes with growth. These same infants and children display “catch-up” growth in a changed environment (see Growth Failure [Failure to Thrive], Chapter 11).
SOCIOECONOMIC LEVEL
Evidence indicates that the socioeconomic level of children’s families has a significant impact on growth and development. At all ages, children from upper- and middle-class families are taller than comparative children of families in the lower socioeconomic strata. The cause of these differences is less definite, although the poorer health and nutrition of lower socioeconomic levels are probably significant factors. Nutritious food sources (especially proteins) are scarce, and other factors (e.g., larger family size and irregularity in eating, sleeping, and exercise) may play a role.
Families from lower socioeconomic groups may lack the knowledge or resources needed to provide the safe, stimulating, and enriched environment that fosters optimum development for children. They may be unable to move from unsafe neighborhoods where drug traffic and drive-by shootings are the norm. The effects on the emotional development of children living under these conditions have been compared with those experienced by children living in war zones.
DISEASE
Altered growth and development are one of the clinical manifestations in a number of hereditary disorders. Growth impairment is particularly marked in skeletal disorders, such as the various forms of dwarfism and at least one of the chromosomal anomalies (Turner syndrome). Many of the disorders of metabolism, such as vitamin D—resistant rickets, the mucopolysaccharidoses, and the numerous endocrine disorders, interfere with the normal growth pattern. In other disorders the tendency is toward the upper percentile of height (e.g., Klinefelter and Marfan syndromes).
Many chronic illnesses that are associated with varying degrees of growth failure are congenital cardiac anomalies and respiratory disorders such as cystic fibrosis. Any disorder characterized by the inability to digest and absorb body nutrients will have an adverse effect on growth and development.
ENVIRONMENTAL HAZARDS
Hazards in the environment are a source of concern to health care providers and others interested in health and safety. Physical injuries are the most prevalent consequences of environmental dangers, and these are discussed extensively throughout the book in relation to age, specific hazards, and selected physical disabilities.
Children are at a high risk for harm resulting from the chemical residues of modern life present in the environment. The hazards of these chemical residues relate to their potential carcinogenicity, enzymatic effects, and accumulation (Baum and Shannon, 1995) (see Community Focus box). The harmful agents most often associated with health risks are chemicals and radiation. Water, air, and food contamination from a variety of sources are well documented. Significant causes of exposure are substances in the immediate environment such as lead and asbestos, chemicals secreted in breast milk (especially prescribed drugs and nicotine), and contamination within well-insulated homes (especially from disinfectants or burning of substances that produce toxic fumes). Passive inhalation of tobacco smoke by infants and children is a hazard at all stages of development. The harmful effects of large doses of radiation are unquestioned, although the effects of low-dose or short-term radiation are debatable, as are the safe vs harmful dosage levels.
Skin cancer is increasing in children, accounting for about 4% of pediatric malignancies. Each Global Solar UV Index level has associated precautions, including sunglasses, sunscreens, sun protective clothing, and sun avoidance.
Children’s sunglasses must absorb at least 99% of ultraviolet radiation (UV). Choose sunglasses with the label “Blocks 99% of UV rays,” “UV absorption up to 400 nm,” “Special purpose,” or “Meets American National Standards Institute (ANSI) requirements.”
Allow children to choose their sunglasses. A child who wears prescription glasses should also wear prescription sunglasses.
Avoid sun exposure between 10 Am and 2 Pm. High altitude, sand, concrete, snow, and water increase UV exposure.
Wear wide-brim hats and sun protective clothing.
Apply an adequate layer of sunscreen, preferably waterproof or water resistant, and reapply at regular intervals.
From Maguire-Eisen M, Rothman K, Demierre M: The ABC’s of sun protection, Dermatol Nurs 17(6):419-433, 2005.
STRESS IN CHILDHOOD
Defined from both a physiologic and an emotional point of view, essentially stress is “an imbalance between environmental demands and a person’s coping resources that … disrupts the equilibrium of the person” (Masten, Garmezy, Tellegen, and others, 1988).
Although all children experience stress, some youngsters appear to be more vulnerable than others. Children’s age, temperament, life situation, and state of health affect their vulnerability, reactions, and ability to handle stress. Also, the responses to a stressor can be behavioral, psychologic, or physiologic. It is impossible and undesirable to protect children from stress, but providing them with interpersonal security helps them develop coping strategies for dealing with stress. The concept of an emotional bank, in which deposits and withdrawals can be made, can help parents and caregivers maintain a proper perspective regarding the effects of stress and coping. Children with a good, positive balance in the account can tolerate significant withdrawal experiences. For children with a low balance, even a minor withdrawal may bankrupt the account, causing it to be overdrawn.
Parents and other caregivers can try to recognize signs of stress to help children deal with stressors before they become overwhelming. Signs of stress take many forms but are typically the same ones seen in children who are abused (see Chapter 14) or depressed (see Chapter 17). If a number of stressors are imposed on children at the same time, the children are more vulnerable. When a succession of stressors produces an excessive stress load, children may experience a serious change in health or behavior.
It is important that parents and persons working with children understand the nature of childhood stress and ways it can be recognized or anticipated. Caregivers must listen to children so they are aware of children’s fears and concerns and must let them know that they are important and that what they say matters. Physical contact is comforting and reassuring to children. Simply holding, touching, or hugging children is both relaxing and comforting and facilitates communication. Spending unhurried time with children, taking family outings or vacations, and exposing children to positive influences help build children’s strength and security. Supportive interpersonal relationships are essential to the psychologic well-being of children.
Coping
Coping refers to a special class of individual reactions to stressors—specifically, a reaction to a stressor that resolves, reduces, or replaces the affective state classified as stressful. Coping strategies are the specific ways in which children cope with stressors, as distinguished from coping styles, which are relatively unchanging personality characteristics or outcomes of coping (Wachs, 2006). Research indicates that, as children age, they tend toward a more internal locus of control and use more vigilant modes of coping (LaMontagne, Hepworth, Johnson, and others, 1996). Children, like adults, respond to everyday stress by trying to change the circumstances or trying to adjust to circumstances the way they are. Any strategy that provides relaxation is effective in reducing stress, and most children have their own natural methods such as withdrawal, physical activity, reading, listening to music, working on a project, or taking a nap. Some turn to parents to solve their problems, or they may develop socially unacceptable strategies, such as cheating, stealing, or lying.
Children can be taught stress-reduction techniques to use in coping. First, they must be helped to recognize signs of tension in themselves and then taught any of a variety of appropriate strategies—special exercises, relaxation and breathing, mental imagery, and numerous other simple activities. Also, parents and other caregivers can anticipate possible stress-provoking events and prepare children for coping by role playing a scenario or “talking it through” beforehand. Probably the most useful tool that children can learn is how to solve problems. When children can view any new situation as a problem to be solved and an opportunity to learn, they are not vulnerable to the control of others. It provides them with a sense of mastery over their own lives and reinforces the fact that they have within themselves the ability and information to handle whatever comes their way. Problem-solving skill gives them the confidence to know where and how to seek help when they need it.
INFLUENCE OF THE MASS MEDIA
Media can have an enormous influence on the developing child. There is no doubt that the media provide children with a means for extending their knowledge about the world in which they live and have helped narrow the differences between classes. However, there is growing concern regarding the enormous influence the media can have on the developing child because of the large number of hours spent watching television. The images of risky behavior presented by the media may serve to establish or reinforce teenagers’ perceptions of their social environment. Children may identify closely with people or characters portrayed in reading materials, movies, video games, and television programs and commercials.
Today, children tend to select media and sports figures as their ideal role models, whereas in the past the majority of children chose their parents or parent surrogates as the people they most wanted to be like (Duck, 1990). This trend can be viewed as a grave concern or a magnificent opportunity to promote positive role models.
Reading Materials
Books, newspapers, and magazines are the oldest form of mass media. They contribute to children’s competence in almost every respect and also provide enjoyment. Recognition of the impact that reading matter used in the schools has on the value system and socialization processes has prompted reevaluation of the content of textbooks in terms of the biased presentation of male and female role models, the sugar-coated view of life situations, and the biased history of minority groups.
Fairy tales, for generations the mainstay of young children’s literature, for a time were condemned for being sexist; violent; and riddled with unfavorable stereotypes, such as the wicked stepmother, dwarfs, and physical unattractiveness associated with evil. They are now believed to provide an excellent medium for explaining puzzling and important topics such as death, stepparents, and inner feelings and turmoil. Although they do not provide solutions, fairy tales confront children with emotional predicaments and offer suggestions for dealing with them.
Comic books and other pulp reading material have been popular in every generation, usually at the expense of literature provided by schools, libraries, and parents. Many children have nothing else to read. The easy reading, quick action, and adventure in brief episodes seem to fulfill a need for children who are striving to understand both aggression in others and their own impulses. Reading ability, intelligence, and school adjustment apparently have no relationship to the number and type of comic books read. Most comic books appear to be relatively harmless to the majority of children and may be beneficial. Comic books seem to have only a minor influence on acquisition of beliefs, values, and behaviors. The popularity of this medium has prompted some educators to encourage translations of literature into comic book form to stimulate students’ interest in the classics.
Movies
Movies that are not closely bound to reality and often portray an assortment of socially approved behaviors may contribute to children’s value systems and provide opportunities for desirable social learning. On the other hand, children, especially adolescents, flock to the “macho” movies and those whose heroes resort to violent resolution of problems, such as karate and wild automobile chases. The carryover of these influences into daily life and relationships may account in part for the increase in violent behavior of young persons.
Another concern is the plethora of “slasher” and R-rated movies available to children and teenagers in theaters and through cable television and videocassettes. The content of movies has changed markedly during the past few decades, with violence and mutilation being major themes. To children who are unable to distinguish between reality and fantasy, these films play on their deepest fears and result in bedtime fears, nightmares, and a fearful view of the world.
Young children can be frightened by some of the movies considered safe for family viewing. For example, Bambi can frighten young children, and the villainous witches in Snow White and the Wizard of Oz are terrifying figures. Also, certain classic children’s movies, such as Snow White and Cinderella, depict stepmothers as evil, destructive persons; such portrayals can have a deleterious effect on children-stepmother relationships or can be confusing to children who have developed a positive relationship with a stepmother.
Movie rating categories are available on the Motion Picture Association of America website.*
Television
The medium with the most impact on children in North America today is television, which has become one of the most significant socializing agents in the lives of young children. The content of programs and commercials provides multiple sources for acquiring information, modeling behaviors, and observing value orientations. Besides producing a leveling effect on class differences in general information and vocabulary, television exposes children to a wider variety of topics and events than they encounter in day-to-day life. Television always has time to talk to children and is a form of access to the adult world.
Television viewing has a direct impact on child development and behavior. Several studies have found that violence on television and the mass media in general can have a negative influence on the development of unhealthy behaviors and violence in children (Earles, Alexander, Johnson, and others, 2002; Monsen, 2002; Brown and Witherspoon, 2002). Several factors encourage the learning or performing of television-influenced behaviors (Box 5-4).
Most researchers have concluded that protracted television viewing can have detrimental effects on children. For example, in one study, television viewing was implicated as contributing to irregular sleep schedules in children under 3 years of age (Thompson and Christakis, 2005). Recognizing the negative effects of television viewing, the American Academy of Pediatrics has recommended that children older than age 2 watch less than 2 hours of high-quality television a day and that children younger than 2 years watch no television (American Academy of Pediatrics, 2001a; Certain and Kahn, 2002). However, this warning has not been heeded, with approximately 40% of infants already watching by 3 months of age and the number increasing to 90% by 24 months. Parents reported the three primary reasons they allowed their infants to watch television was because they thought it was educational for them, they thought it was entertaining, and they needed time to get other things done. Parents did watch television with their infants more than half the time (Zimmerman, Christakis, and Meltzoff, 2007).
The passive activity associated with television viewing is frequently accompanied by eating—in many cases, high-calorie snacks. Furthermore, children may expend tremendous mental energy processing the audiovisual messages from television, which may be exhausting and make them less likely to engage in physical activity later. Andersen, Crespo, Bartlett, and others (1998) found that the incidence of body fat increased in direct proportion to the amount of hours of television watched by children in the United States; as the number of hours of television viewing increased, children were less likely to participate in vigorous physical activities.
In a study to identify children at risk for heart disease, researchers found that more than half of the children with high cholesterol levels watched at least 2 hours of television each day. Using a family history of heart disease or high cholesterol as the screening indicator for cholesterol testing in children, researchers identified three out of four children with high cholesterol levels. When these families were also questioned about the time their children spent watching television, investigators were able to identify 90% of the children with high cholesterol levels by using 2 or more viewing hours as the risk factor (Goldsmith, 1990).
Television programs and commercials, like movies, contain many implicit and explicit messages that promote alcohol consumption, smoking, violence, and promiscuous or unsafe sexual activity. An area of increasing concern is media violence, especially in programs featuring heavy metal rock groups, whose lyrics and videos sensationalize violent sex, suicide, and satanism. There is now clear evidence documenting a relationship between television viewing and the use of alcohol or tobacco, violence and aggressive behavior, the use of guns to commit violent acts, and early sexual activity (American Academy of Pediatrics, 2001a; Strasburger and Donnerstein, 1999).
Parents can help children evaluate television violence by pointing out the subtleties children miss, such as the aggressor’s motives and intentions and the unpleasant consequences the perpetrators suffer as a result of their aggressive acts. Often the consequence is separated from the act by a commercial, and therefore children cannot make the correlation. Parents need to point out that conflicts can be resolved without resorting to violent behavior. They can also stress the purpose of the programs—primarily entertainment—and explain why they like or dislike something on television (e.g., “This show is trying to tell you that crime does not pay and that if one does wrong, one will go to jail”). Explanations and discussions can take place between shows (with the volume turned down), and young children can learn from both older children and adults. These discussions can be effective when begun early and carried out consistently.
It is especially important to identify at-risk children and control their viewing. House rules that specify the type and amount of television help children understand limits, and video-recorded selections of appropriate programs can be substituted for less desirable offerings. Parents need to carefully monitor cable and other pay-television programming because these popular options present more uncensored programming. Locked boxes, V-chips, and blocking devices are available for cable receivers to prevent children from viewing programs when unsupervised. Vessey, Yim-Chiplis, MacKenzie, and others (1998) suggest that parental role modeling may have a more positive influence on the child’s behavior than television programming. They further recommend that parents watch television with children and help children understand the difference between their life and habits and those of persons represented on television.
Television is the medium by which most children learn of a natural disaster or act of terrorism. Research on the effects of September 11, 2001, and the Oklahoma City bombing suggests that posttraumatic stress reactions increase with increased exposure to media coverage. Reading, rather than watching the event on television, may lead to better retention of the experience (Pfefferbaum, Seale, Brandt, and others, 2003). After September 11, 2001, 85% of children in one study reported concerns for their safety and security (Phillips, Prince, and Schiebelhut, 2004). More than half of the children in this study coped by volunteering their time or donating materials for relief teams. In addition, parents should limit the exposure to media coverage of traumatic events, talk to their child about the event, and maintain routines as much as possible.
On the positive side, television has been shown to be a positive influence on children’s abilities to deal with a variety of social issues such as divorce, the arrival of a new baby, discrimination, honesty, and helpfulness. Children who view educational programming (such as “Mister Rogers’ Neighborhood” and “Sesame Street”) for a long period become more affectionate, considerate, cooperative, and helpful toward their playmates. A systematic review of preschoolers and television found that educational viewing can increase their knowledge, affect their racial attitudes, and increase their imaginative behavior (Thakkar, Garrison, and Christakis, 2006). The ways that minority and ethnic characters are portrayed on television can have an impact on the way the majority culture views minority persons and on the self-image of minority children.
Parents need to supervise the amount and type of television programs their children watch and to teach their children how to watch television (Box 5-5 and Family-Centered Care box).
Nurses and parents can be powerful forces in influencing the media. They can watch closely for an increase in violence and other undesirable programming and complain to sponsors and television stations if they believe it is not appropriate. Good programming can be both educational and entertaining.
Video Games
With the popularity of home gaming systems, children are spending increased hours playing video games. Unfortunately, many of the video games available are violent, portraying virtual crimes and violence against others, particularly women. Video games allow the player to be the aggressor, making an ideal environment for a child to learn violent behavior (American Academy of Pediatrics, 2001b). Although video games come with violence and age ratings, many parents are not aware of or choose to ignore the rating appropriate for their child. The American Academy of Pediatrics (2001b) recommends that health care providers encourage parents to adhere to the game ratings and limit the amount of time spent playing games and watching television to less than 2 hours a day combined. Video games have two ratings criteria. The front cover has the rating symbol for age appropriateness, and the back cover has a descriptor indicating the elements of the game. The ratings can be found on the Entertainment Software Rating Board website.*
Provide a positive role model by developing television substitutes such as reading, athletics, physical conditioning, and hobbies.
Construct a time chart of child’s activities (homework, television viewing, scheduled outside activities, playing with a friend).
Discuss with child what you both believe to be a balanced set of activities.
At the beginning of each week, select appropriate programs from television schedules.
Allow child to select programs from this approved list.
Limit child’s viewing to 2 hours or less per day.
Rule out television at specific times (e.g., before breakfast or on school nights).
Leave the television off at mealtimes.
Make a list of alternative activities (e.g., riding a bicycle, reading a book, or working on a hobby).
Require that child choose to do something from this list before watching television.
Discuss program and commercial content with child:
Distinguish between the real and the unreal.
Correlate consequences with actions.
Explore alternatives to aggressive conflict resolution.
Turn the television off after the selected program is over.
Remove televisions from children’s bedrooms.
Monitor cable and pay television selections; use a lockbox if necessary.
Limit use of television as a safe distraction to potentially stressful times (e.g., keeping the children occupied while the parent gets organized after a difficult day).
Internet
The use of computers in both the classroom and household has affected childhood learning and development. Schools offer a wide variety of computer programs that enable children of all ages to broaden their world views. Computers offer the advantage of interactive learning and improved hand-eye co–ordination. Parents have a wide variety of computer software choices for learning and gaming.
Although computer technology has enhanced many forms of learning and recreation, there are potential dangers to children. The Internet and e-mail have made correspondence and information available to children from around the world in minutes. Social networking sites (e.g., MySpace, FaceBook) provide opportunities for children and adolescents to express themselves through blogs, music, pictures, and videos. Although the site owner can accept new friends, many experts are concerned that on-line friendships do not have the same depth as in-person relationships and that security filters are inadequate to protect vulnerable teenagers. Some activities such as “cybersex” and “kiddie porn,” as well as some “chat rooms,” may expose children to individuals who may attempt to take advantage of the child’s naïveté for illicit purposes. Government officials are working to curb illegal activities on the Internet that involve children, yet at the same time maintain freedom of speech. Filtered Internet service providers are available that may serve to protect children from objectionable sites. Nurses must be involved in encouraging parents to be knowledgeable of their children’s Internet activities while providing appropriate learning activities unique to computers. One helpful strategy is to locate the computer in a public area of the home such as the kitchen or family room to enable parents to easily monitor its use.
DEVELOPMENTAL ASSESSMENT
One of the most essential components of a complete health appraisal is assessment of developmental function. Screening procedures are designed to identify quickly and reliably those children whose developmental level is below normal for their age and who therefore require further investigation. They also provide a means of recording objective measurements of present developmental function for future reference. Since the passage of Public Law 99-457, the Education of the Handicapped Act Amendments of 1986, much greater emphasis is placed on developmental assessment of children with disabilities, and nurses can play a vital role in providing this service. It is estimated that 16% of children are affected by developmental disabilities, but fewer than 30% of these children are identified before kindergarten (Wagner, Jenkins, and Smith, 2006). All the procedures discussed in this section can be administered in a variety of settings: home, school, daycare center, hospital, practitioner’s office, or clinic.
DENVER II
The most widely used developmental screening tests for young children are the series of tests developed by William Frankenburg and his colleagues (1994a). The oldest and best known—the Denver Developmental Screening Test (DDST) and its revision, the DDST-R—have been revised, restandardized, and renamed the Denver II. Before administering the Denver II, the examiner should be trained by, and receive certification from, a master instructor who has been trained by the Denver faculty.* The Denver II differs from the DDST in items, test form, interpretation, and referral (see Appendix A). The previous total of 105 items has been increased to 125, including an increase from 21 DDST to 39 Denver II language items. Previous items that were difficult to administer or interpret have been either modified or eliminated. Many items that were previously tested by parental report now require observation by the examiner.
Each item was evaluated to determine whether significant differences exist on the basis of sex, ethnic group, maternal education, and place of residence. Items for which clinically significant differences exist were replaced or, if retained, are discussed in the technical manual. When evaluating children delayed on one of these items, the examiner can look up norms for the subpopulations to consider whether the delay may be caused by sociocultural or environmental differences.
The items on the test form are arranged in the same format as the DDST-R. The norms for the distribution bars were updated with the new standardization data but retain the 25th, 50th, 75th, and 90th percentile divisions. The test form contains a place to rate the child’s behavioral characteristics (compliance, interest in surroundings, fearfulness, and attention span).
To determine relative areas of advancement and delay, enough items should be administered to establish the basal and ceiling levels in each sector. By scoring appropriate items as “pass,” “fail,” “refusal,” or “no opportunity” and relating such scores to the child’s age, the examiner can interpret each item as described in Box 5-6. To identify “cautions,” all items intersected by the age line are administered. To screen solely for developmental delays, only the items located totally to the left of the child’s age line are administered. Criteria for referral are based on the availability of resources in the community.
Research on the Denver II’s validity and accuracy continues. One study found that it identified most children with even subtle developmental problems. However, almost half the children without developmental problems received suspect scores, resulting in a high rate of overreferrals (Glascoe, Byrne, Ashford, and others, 1992). To minimize overreferrals, a decision for referral depends not only on the results of the Denver II, but also on the practitioner’s clinical judgment after considering the child’s developmental history; general health status; social, cultural, and emotional environment; and the availability of local resources for diagnosis and treatment (Frankenburg, 1994a, 1994b).
Although it is not the purpose of this discussion to detail the instruction manual, some points concerning preparation, administration, and interpretation of the Denver II are important to stress. Before beginning the screening, ask whether the child was born preterm and correctly calculate the adjusted age. Up to 24 months of age, allowances are made for preterm infants by subtracting the number of weeks of missed gestation from their present age and testing them at the adjusted age. For example, a 16-week-old infant who was born 4 weeks early is tested at a 12-week adjusted age level.
Explain to the parents and child, if appropriate, that the screenings are not intelligence tests but rather are a method of showing what the child can do at a particular age. Emphasize that the child is not expected to perform each item on the test. Tell the parent before the screening begins that the results of the child’s performance will be explained after all the items have been concluded. It is the nurse’s responsibility to properly inform parents of any testing or screening procedure before its administration so that they are fully aware of its purpose and intent.
Prepare toddlers and preschoolers for the procedure by presenting it as a game. Frequently, the Denver II is an excellent way to begin a health appraisal because it is nonthreatening, requires no painful or unfamiliar procedures, and capitalizes on the child’s natural activity of play. Because children are easily distracted, perform each item quickly and present only one toy from the kit at a time. After that toy’s purpose is concluded, such as building a tower of blocks or identifying its color, replace the toy in the bag and take out another one. Temporary factors that may interfere with the child’s performance include fatigue, illness, fear, hospitalization, separation from the parent, or general unwillingness to perform the activities. In addition, undiagnosed mental retardation, hearing loss, vision loss, or neurologic impairment or a familial pattern of slow development greatly influences the child’s performance.
After completion of the Denver II, ask the parent whether the child’s performance was typical of behavior at other times. If the parent replies affirmatively and the child’s cooperation was satisfactory, explain the results, emphasizing all successful items first, then those items the child failed but was not expected to pass, and finally those items that represent delays. If the parent replies that the child’s performance was not typical of usual behavior, it is best to defer any scoring or discussion of results, especially if the refusals yield a suspect score. In this situation reschedule testing for a time when the child is more likely to cooperate.
In explaining a normal score, focus on how well the child performed and reinforce the parents’ efforts in satisfactorily stimulating their child. In addition to assessing the child’s present developmental level, the Denver II can be used to guide parents toward those activities that are appropriate, although not necessarily expected, for the child’s age. By testing for items to the right of the age line (ones the child is not expected to perform), the examiner can identify children with advanced development, who may be gifted.
In explaining delays, carefully note the parent’s response, especially casual acceptance such as “He’ll catch up” or questions such as “Does this mean my child is retarded?” Be aware of personal anxieties during these situations and refrain from giving glib reassurances such as “I’m sure he will do better next time.” Rather, respond honestly to parents’ questions, yet with appropriate flexibility and concern, stressing the need for further developmental testing.
DENVER II PRESCREENING DEVELOPMENTAL QUESTIONNAIRE
The Prescreening Developmental Questionnaire (PDQ II) is a further revision of the PDQ and the R-PDQ. This version uses the norms (90th and 75th percentiles) from the Denver II. The PDQ II is a parent-answered prescreen consisting of 91 questions from the Denver II, although only a subset of questions is asked for each age-group. The form may need to be read to parents and caregivers who are less educated.
Four different forms are available and are selected based on age: orange (0 to 9 months), purple (9 to 24 months), cream (2 to 4 years), and white (4 to 6 years). The caregiver answers questions until (1) three “nos” are circled (they do not have to be consecutive) or (2) all the questions on both sides of the form have been answered. Scoring is based on the number of delays or cautions (see Box 5-6). Children who have no delays or cautions are considered to be developing normally. If a child has one delay or two cautions, the caregiver is provided with age-appropriate developmental activities to pursue with the child, and a rescreen with the PDQ II is done 1 month later. If on rescreening the child has one or more delays, the Denver II is administered as soon as possible. If a child has two or more delays or three or more cautions on the first screening with the PDQ II, the Denver II is administered as soon as possible.
Several additional parent report developmental screening tools meet the standards for screening test accuracy. Some of the most common include the Ages and Stages Questionnaires (ASQ), Parents’ Evaluation of Developmental Status (PEDS), Child Development Inventory, and the Pediatric Symptom Checklist. Although it is beyond the scope of this chapter to describe each screening tool, using a tool can aid the nurse in providing anticipatory guidance and appropriate referral (Wagner, Jenkins, and Smith, 2006).
KEY POINTS
Growth describes a change in quantity and occurs when cells divide and synthesize new proteins.
Maturation, a qualitative change, describes the aging process or an increase in competence and adaptability.
Differentiation refers to a biologic description of the processes by which early cells and structures are modified and altered to achieve specific and characteristic physical and chemical properties.
Development involves change from a lower to a more advanced stage of complexity.
The five major developmental periods are prenatal, infancy, early childhood, middle childhood, and later childhood (pubescence and adolescence).
Growth and development proceed in predictable patterns of direction, sequence, and pace.
The directional trends in growth and development are cephalocaudal, proximodistal, and mass to specific.
Physical development includes increase in height and weight and changes in body proportion, dentition, and some body tissues.
The three broad classifications of child temperament are the easy child, the difficult child, and the slow-to-warm-up child.
The developmental theories most widely used in explaining child growth and development are Freud’s psychosexual stages, Erikson’s stages of psychosocial development, Piaget’s stages of cognitive development, Kohlberg’s stages of moral development, and Fowler’s stages of spiritual development.
To develop a positive self-concept, children need recognition for their achievements and the approval of others.
Through play, children learn about their world and how to relate to objects, people, and situations.
Play provides a means of development in the areas of sensorimotor and intellectual progress, socialization, creativity, self-awareness, and moral behavior; it serves as a means for release of tension and expression of emotions.
Growth and development are affected by a variety of conditions and circumstances, including heredity, physiologic function, gender, disease, physical environment, nutrition, and interpersonal relationships.
Children’s vulnerability and reaction to stress depend to a large extent on their age, coping behaviors, and support systems.
The mass media can be influential in children’s learning and behavior.
Developmental screening tools are valuable in identifying infants and children who are at risk for developmental delays.
REFERENCES
American Academy of Pediatrics, Committee on Early Childhood, Adoption, and Dependent Care. Selecting appropriate toys for young children: the pediatrician’s role. Pediatrics. 2003;111(4):911–913.
American Academy of Pediatrics, Committee on Public Education. Children, adolescents, and television. Pediatrics. 2001;107(2):423–426.
American Academy of Pediatrics, Committee on Public Education. Media violence. Pediatrics. 2001;108(5):1222–1226.
Anders, TF, Sadeh, A, Appareddy, V. Normal sleep in neonates and children. In: Sheldon S, Ferber R, Kryger M, eds. Principles and practice of sleep medicine in the child. Philadelphia: Saunders, 2005.
Andersen, RE, Crespo, CJ, Bartlett, SJ, et al. Relationship of physical activity and television watching with body weight and level of fatness among children. JAMA. 1998;279(12):938–943.
Baum, C, Shannon, M. Environmental toxins: cutting the risks. Contemp Pediatr. 1995;12(7):20–43.
Beck, CT. A meta-analysis of the relationship between postpartum depression and infant temperament. Nurs Res. 1996;45(4):225–230.
Brown, JD, Witherspoon, EM. The mass media and American adolescents’ health. J Adolesc Health. 2002;31(6S):153–170.
Caine, D, DiFiori, J, Maffulli, N. Physeal injuries in children’s and youth sports: reasons for concern? Br J Sports Med. 2006;40(9):749–760.
Carey, WB. Teaching parents about infant temperament. Pediatrics. 1998;102(5 Suppl E):1311–1316.
Certain, LK, Kahn, RS. Prevalence, correlates, and trajectory of television viewing among infants and toddlers. Pediatrics. 2002;109(4):634–642.
Chess, S, Thomas, A. Goodness of fit: clinical applications from infancy through adult life. London: Routledge, 1999.
Cronk, C, Crocker, AC, Pueschel, SM, et al. Growth charts for children with Down syndrome: 1 month to 18 years of age. Pediatrics. 1988;81(1):102–110.
Delva, J, O’Malley, PM, Johnston, LD. Availability of more-healthy and less-healthy food choices in American schools: a national study of grade, racial/ethnic, and socioeconomic differences. Am J Prev Med. 2007;33(4 Suppl):S226–S239.
Duck, J. Children’s ideals: the role of real-life versus media figures. Aust J Psychol. 1990;42:19–29.
Earles, KA, Alexander, R, Johnson, M, et al. Media influences on children and adolescents: violence and sex. J Natl Med Assoc. 2002;94(9):797–801.
Erikson, EH. Childhood and society, ed 2. New York: Norton, 1963.
Fowler, J. Stages of faith: the psychology of human development and the quest for meaning. New York: HarperCollins, 1981.
Frankenburg, WK. Preventing developmental delays: is developmental screening sufficient? I. Developmental screening and the Denver II. Pediatrics. 1994;93(4):586–589.
Frankenburg, WK. Preventing developmental delays: is developmental screening sufficient? II. Partners in health care. Pediatrics. 1994;93(4):589–593.
Galligan, M. Proposed guidelines for skin to skin treatment of neonatal hypothermia. MCN. 2006;31(5):298–304.
Gentile, D, Oberg, C, Sherwood, N, et al. Well-child visits in the video age: pediatricians and the American Academy of Pediatrics guidelines for children’s media use. Pediatrics. 2004;114(5):1235–1241.
Glascoe, FP, Byrne, KE, Ashford, LG, et al. Accuracy of the Denver-II in developmental screening. Pediatrics. 1992;89(6 Pt 2):1221–1225.
Goldsmith, M. Youngsters dialing up cholesterol levels? JAMA. 1990;264(23):2976.
Kaczander, BI. Pediatric sports medicine: a unique perspective. Podiatr Manage. 1997;16(2):53–60.
Kohlberg, L. Moral development. In: Sills DL, ed. International encyclopedia of the social sciences. New York: Macmillan, 1968.
LaMontagne, LL, Hepworth, JT, Johnson, BD, et al. Children’s preoperative coping and its effects on postoperative anxiety and return to normal activity. Nurs Res. 1996;45(3):141–147.
Lampl, M, Thompson, A, Frongillo, EA. Sex differences in the relationships among weight gain, subcutaneous skinfold tissue and salutatory length growth spurts in infancy. Pediatr Res. 2005;58(6):1238–1242.
Lampl, M, Johnson, ML, Frongillo, EA. Mixed distribution analysis identifies saltation and stasis growth. Ann Hum Biol. 2001;28(4):403–411.
Masten, AS, Garmezy, N, Tellegen, A, et al. Competence and stress in school children: moderating effects of individual and family qualities. J Child Psychol Psychiatry. 1988;29:747–764.
Matvienko, O. Impact of a nutrition education curriculum on snack choices of children ages six and seven years. J Nutr Educ Behav. 2007;39(5):281–285.
Monsen, RB. Children and the media. J Pediatr Nurs. 2002;17(4):309–310.
Morrow, JD, Camp, BW. Mastery motivation and temperament of 7-month-old infants. Pediatr Nurs. 1996;22(3):211–217.
Myrelid, A, Gustafsson, J, Ollars, B, et al. Growth charts for Down’s syndrome from birth to 18 years of age. Arch Dis Child. 2002;87(2):97–103.
Pfefferbaum, B, Seale, T, Brandt, E, et al. Media exposure in children 100 miles from a terrorist bombing. Ann Clin Psychiatry. 2003;15(1):1–8.
Phillips, D, Prince, S, Schiebelhut, L. Elementary school children’s responses 3 months after the September 11 terrorist attacks: a study in Washington, DC. Am J Orthopsych. 2004;75(4):509–528.
Piaget, J. The theory of stages in cognitive development. New York: McGraw-Hill, 1969.
Seidel, HM, Ball, JW, Dains, JE, et al. Mosby’s guide to physical examination, ed 6. St Louis: Mosby, 2007.
Sieving, RE, Zirbel-Donisch, ST. Development and enhancement of self-esteem in children. J Pediatr Health Care. 1990;4(6):290–296.
Strasburger, VC, Donnerstein, E. Children, adolescents, and the media: issues and solution. Pediatrics. 1999;103(1):129–139.
Stuart, GW, Laraia, MT. Principles and practice of psychiatric nursing, ed 7. St Louis: Mosby, 2000.
Thakkar, R, Garrison, M, Christakis, D. A systematic review for the effects of television viewing by infants and preschoolers. Pediatrics. 2006;118(5):2025–2031.
Thompson, DA, Christakis, DA. The association between television viewing and irregular sleep schedules among children less than 3 years of age. Pediatrics. 2005;116(4):851–856.
Thompson, R, Cotner-Bichelman, N, McKerchar, P, et al. Enhancing early communication through infant sign training. J Appl Behav Anal. 2007;40(1):15–23.
Urbanski, LF, Hanlon, DP. Pediatric orthopedics. Top Emerg Med. 1996;18(2):73–90.
Vessey, JA, Yim-Chiplis, PK, MacKenzie, NR. Effects of television viewing on children’s development. Pediatr Nurs. 1998;23(5):483–486.
Wachs, T. Contributions of temperament to buffering and sensitization processes in children’s development. Ann NY Acad Sci. 2006;1094:28–30.
Wagner, J, Jenkins, B, Smith, J. Nurses’ utilization of parent questionnaires for developmental screening. Pediatr Nurs. 2006;32(5):409–412.
Willoughby, C, King, G, Polatajko, H. A therapist’s guide to children’s self-esteem. Am J Occup Ther. 1996;50(2):124–132.
Zimmerman, F, Christakis, D, Meltzoff, A. Television and DVD/video viewing in children younger than 2 years. Arch Pediatr Adolesc Med. 2007;161:473–479.
*CPSC hotline: (800) 638-2772; http://www.cpsc.gov (assistance is also available in Spanish).
†1973 Baseline Road, Ottawa ON K2C 0C7, Canada; (613) 228-3155; fax: (613) 228-3242; http://www.toy-testing.org.
*Forms and complete instructions are available from Denver Developmental Materials, PO box 371075, Denver, CO 80237-5075; (800) 419-4729; http://www.denverii.com. The DDST and DDST-R are no longer available.