Unwarranted Withholding of Opioids
Long-Term Opioid Use in Patients with Persistent Noncancer Pain
Ability to Drive and Engage in Other Activities
Opioid-Induced Hyperalgesia (OIH)
Opioid Safety Regulations: Risk Evaluation and Mitigation Strategy (REMS)
Withholding Opioids from Patients with Addictive Disease
Patients with Pain and Active Addictive Disease
Patients in Recovery from Addictive Disease
Comments on the Treatment of Pain in Patients with Addictive Disease
Opioid Use During Breast-Feeding
Opioid Use in the Critically Ill
THIS chapter discusses pain management for patients in whom opioid analgesics are sometimes withheld. It will discuss the controversies, correct any misconceptions, and provide recommendations for pain treatment in these patients. (See also Chapter 13, p. 339 for care of the patient with sickle cell disease and p. 331 for care of the patient post craniotomy.)
Long-Term Opioid Use in Patients with Persistent Noncancer Pain
Of all the types of pain experienced by patients, the use of opioids is the most controversial in patients with persistent noncancer pain. Opioids are recognized as the mainstay of treatment for moderate to severe acute pain and moderate to severe cancer pain (American Pain Society [APS], 2003). Length of time on opioids seems to be the key issue. Acute pain is defined as being brief, subsiding as healing takes place. Cancer pain, on the other hand, is known to be both acute and persistent, lasting months. However, with newer cancer treatments, pain may last up to one or two years, even longer. The patients who may live the longest are those with persistent noncancer pain, and sadly, this is the group that may be denied pain relief if opioids are needed. Some patients with persistent noncancer pain who cannot obtain needed opioids have been known to say they wished they had terminal cancer so that they would be afforded pain relief.
Is withholding of opioids from patients with persistent noncancer pain warranted? Multiple reasons have been given for withholding opioids from this group of patients, including, fear of addiction, tolerance, limitations on activity such as driving, opioid-induced hyperalgesia, harm to the immune system, and opioid-induced hypogonadism. As will be seen in the discussion that follows, evidence does not support using these reasons for denying opioids to patients with persistent noncancer pain. Rather, the decision to implement a trial of long-term opioid therapy should be based on a careful assessment of potential benefits and burdens (Chou, Fanciullo, Fine, et al., 2009).
Addiction
The likelihood of a patient developing addictive disease as a result of being treated with opioids has already been discussed in Chapter 11. The risk of iatrogenic addiction after short-term exposure for postoperative pain is known to be less than 1%. The risk during long-term treatment is not clear, and is likely to be related to risk factors, the most important of which—a personal history of drug or alcohol abuse, or a family history of drug or alcohol abuse—underscore the importance of a genetic determinant for the disease of addiction.
A review of definitions related to conditions often confused with addiction will clarify some of the confusion about addiction. Following are the definitions proposed by the American Academy of Pain Medicine (AAPM), the APS, and the American Society of Addiction Medicine (ASAM) (2001):
• Physical dependence is a normal response that occurs with repeated administration of the opioid for more than 2 weeks and cannot be equated with addictive disease. It is manifested by the occurrence of withdrawal symptoms when the opioid is suddenly stopped or rapidly reduced or an antagonist such as naloxone (Narcan) is given. Withdrawal symptoms may be suppressed by the natural, gradual reduction of the opioid as pain decreases or by gradual, systematic reduction, referred to as tapering.
• Tolerance is also a normal response that occurs with regular administration of an opioid and consists of a decrease in one or more effects of the opioid (e.g., decreased analgesia, sedation, or respiratory depression). It cannot be equated with addictive disease. Tolerance to analgesia usually occurs in the first days to 2 weeks of opioid therapy but is uncommon after that. It may be treated with increases in dose. However, disease progression, not tolerance to analgesia, appears to be the reason for most dose escalations. Stable pain usually results in stable doses. Thus tolerance poses very few clinical problems.
• Opioid addiction, or addictive disease, is a chronic neurologic and biologic disease. Its development and manifestations are influenced by genetic, psychosocial, and environmental factors. No single cause of addiction, such as taking an opioid for pain relief, has been found. It is characterized by behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving.
In addressing the relationship between addictive disease and the use of opioids for persistent noncancer pain, the following two questions need to be considered:
• How many patients who are receiving opioids for persistent pain also have addictive disease? This is prevalence data. Based on their review of the literature, Nicholson and Passik (2007) found that some studies indicate that the rate of addiction to illicit drugs, prescribed opioids, and alcohol in this population is approximately the same as in the general population, which ranges from 6% to 10% (Savage, 2002).
• How many patients who receive opioids for persistent pain become addicted? This is a causal relationship and cannot be answered by prevalence data.
Very few studies have been conducted to examine the latter question. The appropriate research needs to start with patients who do not already have addictive disease and find out how many become addicted as a result of long-term use of opioids for pain. In a review of all available studies on the development of abuse, addiction, and aberrant drug-related behaviors in patients with persistent pain of noncancer origin who received opioids for pain, only four studies preselected patients for no previous or current history of abuse or addiction (Fishbain, Cole, Lewis, et al., 2008). In these studies, the percentage of patients who became addicted was calculated at 0.19%. A more recent registry study of patients who participated in controlled trials and therefore represented a population from which patients with a history of drug abuse were excluded demonstrated an incidence of 2.6% of drug misuse and no addiction during 3 years of follow-up (Portenoy, Farrar, Backonja, et al., 2007). These data suggest that patients who do not develop a pattern of misuse of psychoactive drugs are at very low risk of developing prescription drug abuse later. None of these data provide insight into the true risk of opioid addiction or abuse among the large population that has a history, or a family history, of alcohol or drug abuse and later receives an opioid for persistent pain.
Ability to Drive and Engage in Other Activities
The effect of opioids on performance of normal activities is sometimes given as reason for withholding opioids. Sometimes employers will not allow patients on opioids to continue their employment. Some prescribers have asked patients to sign agreements that stipulate “no driving” if opioids are taken on a long-term basis (Fishman, Bandman, Edwards, et al., 1999). These outcomes reduce the likelihood that a patient will agree to a trial of this treatment.
According to the opioid treatment guidelines developed by a panel for the APS and the AAPM, the evidence does not support universal prohibition of driving for patients on long-term opioid therapy (Chou, Fanciullo, Fine, et al., 2009). The ability to drive should be assessed in each patient and not prevented in all patients. This is discussed earlier in Chapter 19. Highlights of this discussion are repeated here, and the reader is referred to the earlier discussion for details.
In one study with findings similar to other research, driving tests based on German national recommendations were conducted on 90 healthy controls and 21 patients with noncancer pain who had been treated with transdermal fentanyl for at least 4 weeks without a dose change in the last 12 days (Sabatowski, Schwalen, Rettig, et al., 2003). The median dose of transdermal fentanyl was 50 mcg/h, with a range of 25 to 400 mcg/h. Based on test results, the authors concluded that patients with noncancer pain on stable doses of transdermal fentanyl do not have any clinically significant impairment of psychomotor or cognitive function that would prevent them from driving a car. These results suggest that patients on long-term opioid therapy are probably also able to continue with many other activities. In fact, other drugs such as diphenhydramine (Benadryl) may impair persons more than opioids (Weiler, Bloomfield, Woodworth, et al., 2000).
Whether or not a patient taking opioid analgesics can drive or perform other activities must be decided on an individual basis. Some patients will be able to drive safely, but others may be impaired by opioids. Impairment usually is transient and occurs only at the beginning of opioid therapy or following significant increases in dose, but the reality that some patients have persistent problems requires a careful assessment on a case-by-case basis. Patients who report mental clouding or sedation, or who have signs of impairment on exam should be considered for a change in opioid. It seems prudent to warn all patients that driving ability may be compromised and not to drive if they feel drowsy, dizzy, or impaired in any way, and to advise them of the current literature on driving while taking opioids. In addition, some clinicians advocate asking patients on long-term opioid therapy to obey certain rules if they decide to drive. These rules and a consent form are discussed earlier in Chapter 19 and Box 19-3 on p. 508.
Opioid-Induced Hyperalgesia (OIH)
Hyperalgesia means increased sensitivity to pain. In opioid-induced hyperalgesia (OIH) increasing doses of opioid result in increasing sensitivity to pain (Compton, 2008). OIH has only recently been identified as a clinical reality (Mitra, 2008), but the extent to which it compromises treatment is unknown (Angst, Clark, 2006; Chu, Angst, Clark, 2008). OIH is discussed in more detail in Chapter 11, and the highlights of this discussion are repeated here.
OIH is suspected when increasing doses (usually high, rapidly escalating doses) of opioid fail to relieve pain and actually make pain worse at the original site of pain or at other sites (Chu, Angst, Clark, 2008; Mitra, 2008). OIH may involve unexplained pain, diffuse pain (even the whole body), and diffuse allodynia (Compton, 2008; Chu, Angst, Clark, 2008; Mitra, 2008). To assess the possible presence of OIH, other reasons for failure of the opioid to relieve pain must be ruled out. These include increase in pain pathology, opioid tolerance, opioid withdrawal, pseudoaddiction, and opioid addiction (Compton, 2008). Only when these are ruled out can a diagnosis of OIH be entertained. Table 11-3 (p. 296) gives a brief description of these conditions compared with OIH and suggests some distinguishing characteristics.
Treatment strategies may include opioid dose reduction, opioid rotation, use of N-methyl-d-aspartate (NMDA) receptor antagonists, and continued use of a COX-2 selective NSAID in persistent pain. Once OIH is established, the current opioid dose should be reduced, but the patient is also usually treated with other pain relief strategies as well.
Research has begun to identify potential approaches to preventing OIH. These include proper timing of COX-2 selective NSAIDs in postoperative patients, NMDA antagonists, opioid dose-sparing medications such as certain adjuvants, and avoidance of rapid opioid dose escalation when possible. Theoretically, continued use of COX-2 selective NSAIDs in persistent pain is not only opioid dose-sparing but also may help prevent OIH because these medications reduce the spinal release of excitatory neurotransmitters (Mitra, 2008).
Knowing that long-term opioid therapy, especially if doses escalate rapidly, might actually worsen pain for selected patients adds to the list of reasons to be cautious about this use of opioids. At present, the importance of this outcome is unknown, however, and its reality calls only for careful assessment of patients who do not appear to be improving when an opioid is prescribed.
Other Concerns
Many other concerns about using long-term opioid therapy for patients with persistent noncancer pain exist but are beyond the scope of this book. However, two others deserve at least brief mention: opioid effects on the immune system and opioid effects on the endocrine system in the form of opioid-induced hypogonadism.
A review of the literature by Page (2005) points out that the effect of opioids on immune function has been studied in animals and in humans in the absence of pain and found to suppress immune function. But, in the presence of acute pain, opioid administration in analgesic doses seems to be protective. However, much less is known about the effect on the immune system of prolonged opioid administration in the presence of persistent pain. To date, one small study of 10 patients with persistent pain receiving oral modified-release morphine for 12 weeks indicates that morphine does not influence immune function (Palm, Lehzen, Mignat, et al., 1998). The conclusion was that, at this point in our evidence, concern about opioid effect on immune function is not a reason to withhold opioids from patients with persistent pain. Page (2005) reasons that since it is well known that pain itself suppresses immune function, opioids in analgesic doses could provide relief of pain and thereby provide some relief of the immune suppression of pain.
Negative effects of opioids on the endocrine system have been known for years, but little is written about this. Most of the literature concerns opioid-induced hypogonadism, which is probably common in both male and female patients on long-term opioid therapy (Katz, Mazer, 2009). No standards for laboratory monitoring exist, but recommendations include testing for total and free testosterone (especially in men) and monitoring bone density. Symptoms include decreased libido, erectile dysfunction in men, depression, anxiety, and fatigue. Of course, these symptoms may be due to many other causes such as pain itself. Treatment considerations include opioid rotation and testosterone supplementation. Based on available information, it is not reasonable to withhold opioid therapy because of concerns about endocrine effects of long-term opioid use. These can be monitored and treated.
Treatment Guidelines
The first treatment guidelines developed by professional organizations and designed specifically for the use of long-term opioid therapy for persistent noncancer pain were published in 2009 by a panel convened by the APS and the AAPM (Chou, Fanciullo, Fine, et al., 2009). By contrast, treatment guidelines for cancer pain were published by the World Health Organization (WHO) in the 1980s (WHO, 1986), quickly followed by the APS (APS, 1987) guidelines for acute pain and cancer pain but not for persistent noncancer pain. The Agency for Health Care Policy and Research (AHCPR) then developed guidelines for acute pain (Acute Pain Management Guideline Panel, 1992) and cancer pain (Jacox, Carr, Payne, et al., 1994) but again, not for persistent noncancer pain. Notably, it was approximately 2 decades between the development of guidelines for acute and cancer pain and guidelines for the pharmacologic treatment of persistent noncancer pain. During those years and up to the present time, considerable controversy exists about the long-term use of opioids for persistent noncancer pain.
Despite this controversy, the use of opioids for persistent noncancer pain has increased considerably. Although evidence is limited, the APS-AAPM panel concluded that long-term opioid therapy can be effective with carefully selected patients with persistent noncancer pain. The guideline includes, among other things, a discussion of informed consent and opioid management plans, initiation and titration of long-term opioid therapy, and monitoring of patients.
This guideline is a step in the right direction but has been subject to some criticism, making it important to remember that guidelines are not rules—they are simply guides. Some recommendations are considered questionable since they were presented as “strong recommendation, low-quality evidence” (Leavitt, 2009).
Another criticism is related to a previously registered serious objection to the Washington State Agency Medical Directors’ Group (2007) recommendation in their guidelines that doses greater than 120 mg/day of oral morphine or equivalents should rarely be given and only prescribed after consultation with a pain management expert (Fishman, Webster, 2009). Yet, based on low-level evidence, the APS-AAPM defined a “high” dose of opioid as greater than 200 mg/day of oral morphine or its equivalent and stated that such doses require more intense monitoring.
Another guideline from the American Geriatrics Society (AGS) addresses the pharmacologic treatment of persistent noncancer pain in people 75 years or older (AGS, 2009). Previously, NSAIDs were recommended if acetaminophen did not relieve pain. However, new evidence has drawn attention to the dangerous adverse effects of NSAIDs, such as cardiovascular risk, nephrotoxicity, and gastrointestinal (GI) toxicity (see Section III). Since NSAIDs may result in life-threatening problems, opioids are suggested as a safer alternative in many older adults (AGS, 2009).
Regulatory Issues
The APS-AAPM panel points out that surveys show that prescribers have limited understanding of the laws, policies, and other matters that govern the prescribing of opioids, and that this may have an impact on the care patients receive (Chou, Fanciullo, Fine, et al., 2009). Our impression is that fear of regulatory scrutiny causes prescribers to be fearful of long-term prescribing of opioids and in turn causes them to be overly cautious of prescribing opioids. For their own protection and the patient’s benefit, prescribers should find out about the numerous policy changes that have occurred in recent years. The Pain and Policy Studies Group, University of Wisconsin Database, provides information on state laws, regulations, and other official government policies, and is available at www.painpolicy.wisc.edu/matrix.htm.
Opioid Safety Regulations: Risk Evaluation and Mitigation Strategy (REMS)
A defining consideration in the approval of any drug by the United States Food and Drug Administration (U.S. FDA) is that the benefit of the drug must outweigh its risks. In the case of opioids, abuse potential and the consequent concerns for public health are receiving increasing attention in the review process for new drugs, while new regulations are being considered for some drugs already marketed.
In February of 2008, a new federal law gave the U.S. FDA expanded powers to regulate both new and established medications. One of the provisions authorizes the U.S. FDA to require that a drug manufacturer submit a Risk Evaluation and Mitigation Strategy (REMS). REMS typically include patient and prescriber education. Some may require restricted distribution through specified pharmacies and registries of approved patients, prescribers, and pharmacists. The most restrictive REMS requires that a courier deliver the prescription to the approved pharmacy and also deliver the medication to the patient (Biodelivery Sciences International, 2009) (See U.S. FDA, 2010 for approved REMS).
Manufacturers of methadone and all modified-release opioids were informed in early 2009 that they would be required to develop a REMS for each of their products. A “Draft Guidance” document for opioid REMS has been published (U.S. FDA, 2009d) but a final rule is unlikely before 2011. In the meantime, individual product REMS will be required for any newly approved opioid analgesic.
The REMS approach for opioid analgesics is controversial. Patient advocacy groups and professional societies have endorsed the goals of safe use and avoidance of abuse and diversion. However, they have expressed concerns about the potential unintended consequence of decreased access to appropriately prescribed opioids (American Pain Foundation, 2009;American Pharmacists Association, 2009; Inturrisi, 2009; Shane, 2010). There is broad consensus that patient and public safety must be considered at all levels of opioid development, approval, and clinical use. It will be some time before either positive or negative outcomes of opioid REMS are known.
Withholding Opioids from Patients with Addictive Disease
Opioids, if they are appropriate, should not be withheld from patients with pain who also have addictive disease. Unfortunately, when persons with addictive disease come to health care providers for help with their painful conditions, they may encounter disrespect and poor pain management. Abundant evidence suggests that pain in persons with addictive disease is undertreated (Iocolano, 2000; Nichols, 2003).
Clinicians often fear that by providing opioids for pain they are “feeding the addiction.” No research shows that providing opioid analgesics to this person will worsen the disease. Conversely, there is no research to show that withholding opioid analgesics when needed will increase the likelihood of recovery (Compton, 1999; McCaffery, Vourakis, 1992). In fact, withholding opioids in this situation may cause significant pain, which can increase the patient’s level of stress and lead to increased craving for drugs of abuse. The patient may make efforts to obtain the drug that has been abused, or a patient in recovery may relapse. In the inpatient setting, the patient may make efforts to bring in illicit drugs. Clearly, on many levels, providing pain relief to the patient with addictive disease, even when it includes opioids, is preferable to withholding opioids.
Nevertheless, persons with addictive disease and pain often encounter many biases in the health care system. In addition to the problem of inappropriately withholding opioids because of misguided information, the disease of addiction is often misdiagnosed. Section II on assessment discusses the definition of addictive disease, misconceptions that result in a “label” (not a diagnosis) of addiction, and a warning about the use of the term drug seeking, which often erroneously implies addictive disease (see Chapter 2). The reader is asked to review this information. Many behaviors suggestive of addiction may be “pseudoaddiction,” a situation of undertreated pain. When pain is adequately treated, the behaviors that suggested addiction subside.
Care of patients with addictive disease and pain is complex and ideally would be undertaken in a multidisciplinary manner, but this is not always possible. Since these patients may present in almost any clinical setting, all clinicians are encouraged to learn how to treat pain in actively using and recovering patients. Before attempting to manage pain in these patients, clinicians need to acknowledge their own biases about addictive disease and attempt to prevent them from interfering with their care of the patient. Rather than understanding that addiction is a chronic, neurobiologic disease, some clinicians may believe that addiction reflects a moral weakness, blaming the patient for not just stopping their drug use. In their eyes, the patient does not deserve care, or worse, is someone who should be punished. This often poses an ongoing challenge for clinicians. Openly discussing these attitudes with staff may assist all of those caring for the patient with addictive disease to more comfortably provide appropriate pain management.
An excellent guide to pain management in the patient with pain and addictive disease was developed by the American Society for Pain Management Nursing (ASPMN) in 2002. It is titled, “ASPMN Position Statement: Pain Management in Patients with Addictive Disease,” available at http://www.aspmn.org/Organization/documents/addictions_9pt.pdf. It covers patients actively using alcohol or other drugs, patients in recovery, and those receiving methadone maintenance therapy (MMT) for opioid addictive disease. All of these conditions will be discussed briefly here.
The first sentence of the ASPMN paper states a belief that is crucial for clinicians to adopt, “…patients with addictive disease and pain have the right to be treated with dignity, respect, and the same quality of pain assessment and management as all other patients” (p. 1). It is a quote worth posting for all to see, including clinicians, patients, and families.
Patients with Pain and Active Addictive Disease
Patients who are actively using alcohol and other drugs may come to the inpatient or outpatient health care setting under the influence of these drugs. Treatment of pain may be difficult if the patient is unable to give consistent answers to questions about the pain or the drugs he or she has taken, sometimes causing a delay in treating pain. However, pain treatment should begin as soon as possible. If the patient is too sedated to safely receive opioids, the use of NSAIDs, regional anesthetic techniques, adjuvant analgesics, or nonpharmacologic methods of pain control is recommended.
If the patient has been using opioids, naloxone or other opioid antagonists should not be administered for the purpose of decreasing the opioid’s effect unless the patient’s life is in danger. Opioid antagonists could increase the patient’s pain and throw the patient into withdrawal.
As soon as possible, obtain information from the patient and family about which drugs the patient has been abusing and all medications that have been prescribed. Become familiar with signs of withdrawal from each of the drugs and how to minimize withdrawal symptoms, such as by an appropriate tapering of the drug or an appropriate substitute. Obtain protocols for assessing and treating withdrawal from opioids, other drugs, and alcohol (e.g., to assess symptoms of alcohol withdrawal, obtain a protocol from http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.table.4060; for clinical detoxification protocols, also see http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat5.table.4060. Withdrawal from alcohol can be life-threatening if not assessed and treated properly.
Box 20-1 presents general guidelines for treating patients with addictive disease and pain in all clinical settings, and more specific guidelines for treating patients in the inpatient setting and in the outpatient setting.
Patients in Recovery from Addictive Disease
Most clinicians, persons with addictive disease, and their families expect complete abstinence from the drug of abuse and other drugs with abuse potential. However, it is not realistic to expect all patients recovering from addictive disease to be totally abstinent (Passik, Kirsh, 2004). Harm reduction may be a more realistic goal and should not be considered a failure. Some patients may find it possible to cut down on their drugs of abuse or find a less harmful way to consume the drug, such as smoking heroin instead of sharing needles to give it IV. Others may need medically prescribed medications, such as opioids or benzodiazepines.
Alcoholics Anonymous (AA) published a pamphlet in 1984 to address the use of medications and other drugs while in recovery from alcoholism. They point out that while some members of AA believe that no one in AA should take any medication, this can be disastrous for some people. Those with depression, schizophrenia, manic depression, epilepsy, and others requiring medication may meet with serious consequences, such as suicide or seizures, if they do not take their prescribed medications, some of which admittedly carry the potential for abuse. This pamphlet may be ordered by writing AA World Services, Inc., Box 459, New York, NY 10163 or by contacting AA at 212-870-3400. Having this available is often reassuring and informative for staff as well as patients with addictive disease and their families. Nonetheless, whether or not to take opioids for pain relief is the patient’s decision, not the clinician’s.
Patients who are in recovery and are totally abstinent are often fearful of relapse, and clinicians should discuss any intent or recommendation to use opioids or other psychoactive medications in their treatment. Establish from the beginning that the patient can make the final decision about the use of opioids or other drugs. In the past, clinicians used to make this decision for the patient and simply withhold opioids. Assure the patient that this will not happen. Discuss alternative options, such as nonopioids (NSAIDs and acetaminophen), regional anesthetic techniques, adjuvant analgesics, and nonpharmacologic methods, with those who do not want to take an opioid for pain relief.
Address fear of relapse by encouraging patients to continue and increase their activities with their recovery program. Remember to include the patient’s family in these discussions because they may be equally or even more fearful of relapse.
Some patients recovering from addiction to opioids may be receiving opioid agonist therapy with either methadone or buprenorphine. These patients are likely to be undertreated for acute pain due to several misconceptions (Alford, Compton, Samet, 2006). Some clinicians erroneously believe that the maintenance opioid dose will suffice to relieve pain, and, therefore, fail to take additional action to provide pain relief. Other misconceptions are that adding another opioid analgesic may result in addiction relapse or cause respiratory depression. If these misconceptions are not corrected, the patient with acute pain will likely suffer, and the patient’s reports of pain may be seen as manipulation to obtain more opioids.
If the patient is receiving methadone maintenance therapy (MMT) a common approach is to continue the methadone maintenance dose and add short-acting opioids, titrating the dose upward until pain relief is achieved (Alford, Compton, Samet, 2006). MMT has been used for decades, but buprenorphine maintenance therapy was only approved in the United States in 2004. Research and clinical experience have not yet identified the most effective approach for relieving pain in buprenorphine-maintained patients. Four options were suggested by Alford, Compton, and Samet (2006). The simplest one consisted of continuing the buprenorphine maintenance therapy and titrating a short-acting opioid analgesic to a dose that relieves the pain. A similar approach was suggested by other researchers in which the maintenance dose is given in divided doses and an additional opioid agonist such as morphine is added and titrated to effect (Vadivelu, Hines, 2007). In a study of managing acute postpartum pain in one group of patients on MMT (N = 10) and the other maintained on buprenorphine (N = 8), ibuprofen was used along with adding an opioid agonist for both groups and appeared to be beneficial in relieving pain (Jones, O’Grady, Johnson, et al., 2009). Patients on either form of maintenance therapy are likely to require higher doses of opioid for pain relief than the usual opioid-naïve patient. Box 20-2 presents guidelines for the management of pain in the patient recovering from addictive disease.
Comments on the Treatment of Pain in Patients with Addictive Disease
This aspect of patient care, relieving pain when the patient has addictive disease, especially the active addict, is one of the most challenging situations clinicians encounter. Knowledge of pain, addictive disease, and regulations governing the prescribing of controlled substances are required. It takes courage—the clinician’s fear of endangering his or her license is not unfounded. Extensive experience and considerable self-awareness are always helpful. And the clinician needs to be willing to spend the extra time these patients usually require. Too often patients recovering from addictive disease are dismissed from practice when any suggestion of relapse or abuse occurs, and this is understandable in view of the above demands on the clinician. Hopefully, such patients are referred to others who are more prepared or willing to care for these patients. Unfortunately, an appropriate referral cannot always be made. So, who is going to be responsible for the care of these patients? This question has yet to be answered. Following is one response.
A pain specialist speaking about addictive disease to an audience of other pain specialists received this comment from a member of the audience, “These patients are too difficult, take up too much time, and put me in legal jeopardy. I simply have to discharge them from my practice.” To this the speaker replied, “If we, the pain specialists, don’t treat them, who will?”
Opioid Use During Pregnancy
Opioids have a long history of safely relieving pain during pregnancy, such as following surgery, traumatic injury, or painful conditions associated with the pregnancy itself. For example, pelvic girdle pain is common during pregnancy; 10% of women with this condition experience severe pain, and a large number of these have persistent pain and disability (Hess, Aleshi, 2008). Some pregnant women have chronic conditions, such as sickle cell disease or rheumatoid arthritis, for which they take regular doses of opioid analgesics. The mu opioid agonists, such as morphine, hydromorphone, fentanyl, oxycodone, hydrocodone, and methadone, are recommended when an opioid is needed during pregnancy. Meperidine is often prescribed for pregnant women, but this is discouraged. Meperidine is not recommended for any type of pain because of its toxic metabolite, normeperidine (see Chapter 13).
Research conducted over the years has looked at the incidence of teratogenic effects in babies born to mothers who took opioids during pregnancy. One large collaborative study found no congenital anomalies in infants whose mothers took hydrocodone, meperidine, methadone, morphine, or oxycodone during pregnancy (Heinomen, Slone, Shapiro, 1977). Anomalies were observed in the offspring of those who took codeine or propoxyphene, but with the exception of respiratory malformation associated with codeine use, the incidence was not statistically greater than in the general population (Viscomi, Rathmell, 1998). A more recent retrospective review of the data of 15 parturients with persistent pain who received regular doses of opioid analgesics during pregnancy revealed that opioids were safe in both the mothers and infants (Hadi, da Silva, Natale, et al., 2006).
There is surprisingly little research on the use of opioids during pregnancy. A Cochrane Collaboration Review searched for randomized controlled trials that enrolled “opiate-dependent pregnant women” and revealed just three studies. These were in women who took long-acting opioids for treatment of addictive disease: two studies compared methadone with buprenorphine, and one compared methadone with modified-release morphine (Minozzi, Amato, Vecchi, et al., 2008). The researchers could find no significant difference between the opioids in terms of abstinence from the use of heroin but underscored the urgent need for more randomized controlled trials with large numbers of patients to draw sound conclusions. They cited a number of benefits of treatment of addiction with the long-acting opioids, including prevention of repeated episodes of opioid withdrawal in the fetus, reduction in maternal illicit drug use, improved compliance with obstetric care, and improved infant birth weight. Other studies have demonstrated less prematurity, higher birth weights, and a lower rate of stillbirth in infants born of women with addictive disease who were maintained in addiction treatment programs compared with women who were not (Fajemirokun-Odudeyi, Sinha, Tutty, et al., 2006; Little, Snell, Van Beveren, et al., 2003). One study found no difference in the Apgar scores of infants of mothers in addiction treatment programs who took methadone, buprenorphine, or modified-release morphine during pregnancy and those who were not addicted and did not take any opioids (Ebner, Rohrmeister, Winklbauer, et al., 2007). The researchers observed that this finding is consistent with other research.
An interesting case report described a woman who had been taking transdermal fentanyl (25 mcg/h) for 2 years for systemic lupus erythematosus and fibromyalgia prior to becoming pregnant and who delivered a healthy baby with an Apgar score of 9 and who nursed readily after birth (Einarson, Bozzo, Taguchi, 2009). The infant required no special observation or treatment and was roomed in with his mother who monitored the baby for withdrawal symptoms (see the following paragraphs), which were not observed. Follow-up visits with the pediatrician revealed the baby to be healthy and achieving all developmental milestones.
Neonatal Abstinence Syndrome
Physical dependence can occur in an infant whose mother took opioids during pregnancy, and abrupt discontinuation of the opioid can result in withdrawal symptoms after birth. These symptoms are collectively called neonatal abstinence syndrome and are characterized by neuralgic excitability (e.g., tremor, irritability, hypertonicity, abnormal crying, insomnia, and rarely seizures); GI dysfunction (e.g., nausea, vomiting, diarrhea); and autonomic dysfunction (e.g., fever, chills, nasal congestion). It is important to understand that physical dependence is not addiction. Addiction implies the psychological dependence on a particular drug and a cause-and-effect mode of thinking. Infants are incapable of this higher-level cognitive recognition and therefore cannot become addicted (Stevens, 1999). (See Chapter 11 for the difference between addiction and physical dependence.)
Not all infants born of mothers who take opioids during pregnancy will exhibit neonatal abstinence syndrome, as noted in the case study described earlier (Einarson, Bozzo, Taguchi, 2009). Studies have consistently shown that approximately 40% of infants will not develop symptoms (Berghella, Lim, Hill, et al., 2003; Ebner, Rohrmeister, Winklbaur, et al., 2007). Research is conflicting regarding whether or not the dose of opioid the mother takes influences the severity of symptoms. Whereas one retrospective review showed that the higher the methadone dose the more likely it was that the infant would have withdrawal symptoms and the longer the duration of treatment (Lim, Prasad, Samuels, et al., 2009), another retrospective review showed no correlation between methadone dose and severity or duration of neonatal abstinence syndrome (Berghella, Lim, Hill, et al., 2003).
Expecting a newborn to endure neonatal abstinence syndrome without appropriate treatment is unethical, dangerous, and not recommended. Rather, symptoms are prevented with the administration and gradual tapering of a mu opioid over several days; oral morphine or tincture of opium is usually used for this purpose (Stevens, 1999). A Cochrane Collaboration Review found that opioids and supportive care compared with supportive care only for the treatment of neonatal abstinence syndrome reduced the time to regain birth weight and the duration of supportive care (Osborn, Jeffery, Cole, 2005a). Length of hospitalization was longer in those who were treated with morphine, but it was not clear if this was related to infant status. The review also revealed that oral morphine was associated with better outcomes than diazepam and prevented seizures better than phenobarbital. Another Cochrane Collaboration Review found that phenobarbital was more effective than diazepam for neonatal abstinence syndrome (Osborn, Jeffery, Cole, 2005b). Phenobarbital was associated with shorter hospital stays than oral morphine, but the researchers observed that this may have been related to the willingness of health care providers to discharge an infant with a prescription for phenobarbital but not with one for morphine (Osborn, Jeffery, Cole, 2005b). A study of the babies of women who attended an addiction treatment clinic found that oral morphine (0.05 to 0.1 mg/kg/dose PRN) was more effective than phenobarbital (5 to 10 mg/kg/day) for the treatment of neonatal abstinence syndrome, and unlike the previously mentioned study, found that morphine was associated with a significantly shorter treatment time (Ebner, Rohrmeister, Winklbaur, et al., 2007).
In summary, the current research suggests that oral morphine is the preferred drug for the prevention and treatment of neonatal abstinence syndrome. During administration, infants should be monitored closely, and other comfort measures, such as swaddling, massage, relaxation bathing, waterbeds, and pacifiers, should be provided (Osborn, Jeffery, Cole, 2005a).
Opioid Use During Breast-Feeding
Opioids taken by breast-feeding women are secreted in the breast milk, ingested by the nursing baby, and undergo hepatic metabolism. It is quite common for women to require an opioid during lactation, and guidelines and other publications have listed opioids as compatible with breast-feeding for several years (American Academy of Pediatrics, 2001; Dillon, Wagner, Wiest, et al., 1997). A case report described safe and successful breast-feeding of an infant born to a mother who took transdermal fentanyl (100 mcg/h) throughout pregnancy and lactation (Cohen, 2009). The baby’s blood fentanyl levels were undetectable.
An exception to this is meperidine, which is associated with sedation, poor suckling, and neurobehavioral delay in the nursing baby (Bar-Oz, Bulkowstein, Benyamini, et al., 2003; Wilbeck, Schorn, Daley, 2008; Wittels, Glosten, Faure, et al., 1997). The U.S. FDA issued a warning that nursing mothers who are ultra-rapid metabolizers of codeine can transfer sufficient morphine to their breast-feeding infants to cause life-threatening or fatal adverse effects, so this drug should be avoided during breast-feeding as well, especially since few women know whether or not they are an ultra-rapid metabolizer of codeine (U.S. FDA, 2007a) (see Chapter 13 for more on codeine metabolism). A better choice would be oxycodone.
To minimize sedation during exposure to opioids in breast-feeding infants, mothers who are receiving IV PCA can be encouraged to self-administer a dose just after nursing. Intraspinal analgesia typically administers very low doses of opioid, and drug exposure is minimal (Rathmell, Viscomi, Ashburn, 1997).
The impact of labor epidural analgesia on breast-feeding has been studied and shown to have an opioid dose-dependent effect. Laboring women (N = 177) who had previous experience with breast-feeding a child and were recruited in the prenatal period were randomized to receive epidural analgesia with no fentanyl, intermediate-dose fentanyl (1 to 150 mcg), or high-dose fentanyl (more than 150 mcg) (plus 0.0625% to 0.125% bupivacaine in all groups) (Beilin, Bodian, Weiser, et al., 2005). On postpartum day 1, twice as many women who received high-dose fentanyl (N = 12) reported difficulty breast-feeding than those who received intermediate-dose fentanyl (N = 6) or no fentanyl (N = 6), although this number did not reach statistical significance. There were no significant differences among the groups based on the lactation consultant’s evaluation. Neurobehavior scores were lowest in infants whose mothers received more than 150 mcg of fentanyl. An interesting finding was that at 6 weeks, significantly more women in the high-dose group (N = 10) had stopped breast-feeding than in the intermediate-dose fentanyl (N = 3) and no fentanyl (N = 1) groups. A randomized controlled trial evaluated women who received epidural fentanyl analgesia or no epidural analgesia during labor and found a similar rate of initiation and duration of breast-feeding among the groups (Wilson, MacArthur, Cooper, et al., 2010). It is important to note that numerous factors influence a woman’s decision and ability to breast-feed.
Opioid Use in the Critically Ill
Patient surveys indicate that the critically ill experience a high level of pain and other discomforts associated with underlying pathology and care activities while in the ICU (Nelson, Meier, Oei, et al., 2001; Puntillo, Pasero, Li, et al., 2009). This population is at particularly high risk for undertreated pain because many are unable to report their pain and discomforts using customary methods, such as the 0-to-10 numerical pain rating scale (Puntillo, Pasero, Li, et al., 2009) (see Section II).
Opioids have a long history as first-line analgesics for the management of pain in the critically ill and should be started before or concomitantly with sedatives (Erstad, Puntillo, Gilbert, et al., 2009). The recommended treatment approach in critically ill patients who cannot report their pain is to administer opioid analgesics based on the assumption that their underlying condition or disease process is associated with significant pain (see Section II).
Opioids are warranted also because tracheal intubation, mechanical ventilation, and the aftermath of care, such as chest physiotherapy and suctioning, are known to be extremely painful (Pasero, McCaffery, 2002). A multicenter study supported by the American Society of Critical Care Nurses of over 6000 acutely or critically ill patients ranging from the age of 4 to 97 years old evaluated pain and distress associated with six common procedures these patients would experience: turning, wound drain removal, tracheal suctioning, femoral catheter removal, placement of central venous catheter, and changing of non-burn wound dressing (Puntillo, White, Morris, et al., 2001). Simple turning was identified as the most painful and distressing of the procedures in adults ages 18 and older. Other research confirmed a high incidence of pain in 30 traumatically injured patients in the ICU; 96% reported pain in injured areas of their bodies, and 36% reported pain related to devices and tubings, such as chest tubes, Foley catheters, wound drains, and orthopedic fixation devices (Stanik-Hutt, Soeken, Belcher, et al., 2001). Again, turning was found to be very painful; resting pain intensity scores (mean 26.5) nearly doubled after turning (mean, 48.1).
These studies underscore the high prevalence of pain in the critically ill and the need for an aggressive approach to managing it. Mu agonist opioids are first-line analgesics in a multimodal treatment plan. The risk of adverse effects of the nonopioid and adjuvant analgesics must be carefully considered in the critical care population (Erstad, Puntillo, Gilbert, et al., 2009), but unless contraindicated, nonopioids (e.g., acetaminophen and an NSAID) and appropriate adjuvant analgesics (e.g., anticonvulsants for neuropathic pain, if thought to be likely), are added. Local anesthetics applied topically or given by continuous peripheral nerve block (e.g., for some orthopedic surgeries) or added to opioids for epidural administration (e.g., thoracotomy) should be considered in some patients. The reader is referred to a series of articles focusing on various aspects of pain in the critically ill published in the Postgraduate Corner of the journal of Chest (see volume 135, issues 4 to 6, 2009).
Selection of Opioid Doses in Patients Unable to Report Pain
Nurses often ask how to select a starting opioid dose and how to know if that dose is effective in patients who cannot report their pain. Chapter 16 discusses in detail the method used to determine opioid doses, and this method is applicable to patients who cannot report pain. In most cases, pain is assumed to be severe in critically ill patients based on the presence of significant pathology (Puntillo, Pasero, Li, et al., 2009), and doses are selected accordingly (e.g., 2.5 mg/h IV morphine or equivalent starting dose in an opioid-naïve adult; higher doses will be required for opioid tolerant patients). As in patients who can report pain, pain is also prevented prior to painful procedures with IV opioid bolus doses (e.g., 1 to 2 mg). If present, changes in behaviors after an opioid dose is administered or an opioid infusion is initiated are used to evaluate analgesic effectiveness. In patients who are unresponsive, no change in behavior will be evident to guide assessment of analgesic effectiveness; therefore, the optimized opioid dose is continued (Pasero, 2009a).
Weaning from the Mechanical Ventilator
When critically ill patients show improvement, they are weaned from mechanical ventilation. Often opioids are discontinued before beginning the weaning process out of a fear that opioids will produce adverse respiratory effects and impede weaning. However, the fear of respiratory depression, cited as the main reason for stopping opioids before weaning, usually is unfounded in critically ill patients. Most critically ill patients will receive opioids long enough for some tolerance to develop, and tolerance to respiratory depression develops relatively rapidly within days of regular dosing. Therefore, fear of respiratory depression should not be a barrier to continuing opioids for patients who have been receiving them for several days or longer (APS, 2003).
In addition, loss of pain control can cause ventilator weaning to fail. Unrelieved pain can contribute to pulmonary dysfunction (Ghori, Zhang, Sinatra, 2009; Jacobi, Fraser, Coursin, et al., 2002). Even when the source of pain is remote from the thoracic and abdominal region, respiratory dysfunction can occur. Involuntary responses to pain cause reflex muscle spasm at the site of tissue damage and in muscle groups above and below the site. Patients with pain also voluntarily limit their thoracic and abdominal muscle movement in an effort to reduce the pain they are experiencing.
The measurable respiratory effects of severe pain are small tidal volumes and high inspiratory and expiratory pressures, as well as decreases in vital capacity, functional residual capacity, and alveolar ventilation (Ghori, Zhang, Sinatra, 2009). If adequate pain relief is not provided, these effects can progress to significant pulmonary complications, such as atelectasis and pneumonia.
Abrupt discontinuation of opioids can have other undesirable consequences besides loss of pain control. At the time of weaning, many critically ill patients have been receiving opioids long enough to have developed physical dependence. If the opioid is stopped abruptly for weaning, physically dependent patients will experience withdrawal syndrome. Signs of withdrawal include restlessness and agitation and may be confused with failed weaning or “ICU psychosis.” The practice of abrupt discontinuation of opioids can result in inaccurate assessment of the patient’s response and inappropriate treatment (e.g., benzodiazepines to sedate the patient).
If a reduced opioid dose is required for successful weaning, using a multimodal analgesic approach may make it easier to do so without compromising good pain control. If an NSAID is not contraindicated and is not being administered around the clock (ATC) already, one can be added before weaning to allow a reduced opioid dose. Acetaminophen can be given rectally for additional analgesia. Anticonvulsants, such as gabapentin, can be added to treat neuropathic pain and prevent the development of persistent pain. Other appropriate nonsedating adjuvants, such as local anesthetics via continuous peripheral nerve block or added to epidural opioids, should be considered.
The lack of a respiratory depressant effect with dexmedetomidine (Precedex) has implications for its use during weaning from mechanical ventilation and extubation. A study of patients who had failed previous attempts at ventilator weaning secondary to agitation unresponsive to traditional sedatives described successful extubation of 14 of the 20 patients who were given dexmedetomidine (Arpino, Klafatas, Thompson, 2008). Other positive results were a reduction in concomitant sedative and analgesic use and minimal adverse effects. Dexmedetomidine has also been reported to facilitate terminal weaning and withdrawal of ventilatory support at end of life in palliative care (Kent, Kaufman, Lowy, 2005) (see Section V for more on dexmedetomidine).
The intraspinal routes are frequently used to deliver opioids to the critically ill. One of the benefits of intraspinal analgesia in mechanically ventilated patients is excellent analgesia with lower opioid doses and less threat of respiratory depression during weaning. In addition, a number of studies have demonstrated improved pulmonary function with intraspinal analgesia (see Chapter 15 for research and detailed discussion of intraspinal analgesia). Continuous peripheral nerve blocks, which rely on local anesthetics for analgesia, may be ideal for some patients in the ICU (see Section V).
Managing Pain in the Terminally Ill
The American Nurses Association’s 2003 position statement on Pain Management and Control of Distressing Symptoms in Dying Patients states:
“In the context of the caring relationship, nurses perform a primary role in the assessment and management of pain and other distressing symptoms in dying patients. Therefore, nurses must use effective doses of medications prescribed for symptom control and nurses have a moral obligation to advocate on behalf of the patient when prescribed medication is insufficiently managing pain and other distressing symptoms. The increasing titration of medication to achieve adequate symptom control is ethically justified.” (p. 1, American Nurses Association, 2003)
The American Medical Association (AMA) maintains its stand taken in a 1992 position paper stating that “the administration of a drug necessary to ease the pain of a patient who is terminally ill and suffering excruciating pain may be appropriate medical treatment even though the effect of the drug may shorten life” (AMA, 1992).
Despite these standards, pain in the terminally ill continues to be undertreated. The 1995 publication of a disturbing study of more than 9000 terminally ill hospitalized patients revealed that 50% of conscious seriously ill patients who died in the hospital experienced moderate to severe pain at least half of the time (SUPPORT, 1995). Four in 10 experienced severe pain; 59% preferred a treatment plan that focused on comfort, but 10% received care contrary to this (Lynn, Teno, Phillips, 1997). The SUPPORT publication spurred a number of initiatives, and one of the most notable was the Robert Wood Johnson Foundation Last Acts national campaign to promote improvements in care and caring near the end of life. In 2002, Last Acts conducted the first ever state-by-state evaluation of end-of-life care and found that, despite years of research, educational, and grass roots efforts, and millions of dollars of private philanthropy “… care for dying Americans is no better than mediocre.” The entire Last Acts analysis can be found in the publication: Means to a Better End. A Report on Dying in America Today at http://www.rwjf.org/files/publications/other/meansbetterend.pdf. Last Acts completed its work in 2005. In response to its Report on Dying, many states initiated comprehensive educational efforts to improve their performance (Virani, Malloy, Ferrell, et al., 2008) (also see ELNEC later in the chapter).
The underdosing of opioids in terminally ill patients is particularly tragic because it is usually based on the unfounded fear that the opioid will produce adverse respiratory effects and hasten death. However, most terminally ill patients have been receiving opioids long enough to have developed tolerance to the opioid’s respiratory depressant effects. In fact, in an early study of patients from whom life support had been withdrawn or withheld, those who received analgesics and sedatives lived longer (2.2 hours) than those who did not receive analgesics and sedatives (Wilson, Smedira, Fink, et al., 1992). More recent research reports similar findings. A case note review of 238 consecutive patients who died in a palliative care unit observed that there were no significant differences in survival from admission or frequency of unexpected death between those who received a marked increase in opioids at end of life and those who needed no increase (Thorns, Sykes, 2000). A study of the use of sedatives at end of life also demonstrated that increased doses of sedatives in the last hours of life were not associated with shortened survival (Sykes, Thorns, 2003a). Another study found no evidence that opioids or benzodiazepines hastened death in critically ill patients after withdrawal of life support; in fact, for every 1 mg/h increase in benzodiazepine dose, time to death was increased by 13 minutes (Chan, Treece, Engelberg, et al., 2004). The same was found in terminally ill cancer patients (Morita, Tsunoda, Inoue, et al., 2001). A more recent multicenter, observational, prospective study evaluated overall survival in two cohorts of hospice patients, one submitted to palliative sedation (sedatives and analgesics) and the other managed by routine hospice practice (Maltoni, Pittureri, Scarpi et al., 2009). The median survival was 12 days and 9 days for those who received palliative sedation and those who received routine hospice care, respectively, which led the researchers to conclude that palliative sedation therapy does not shorten life when used to treat refractory symptoms. These studies suggest that the underlying disease, not the analgesics and sedatives, usually determines death (Brody, Campbell, Faber-Langendoen, et al., 1997).
An extensive analysis of data derived from the National Hospice Outcomes Project (Connor, Horn, Smout, et al., 2005) appropriately concluded that concern about hastening death does not justify withholding opioid therapy at end of life (Portenoy, Sibirceva, Smout, et al., 2006). Nevertheless, research shows that clinicians continue to be apprehensive about using high doses of analgesics and sedatives in the terminally ill even when deemed necessary and appropriate (Bendiane, Bouhnik, Favre, et al., 2007; Bilsen, Norup, Deliens, et al., 2006; Rocker, Heyland, Cook, et al., 2004; Sykes, Thorns, 2003a,b; Thorns, Sykes, 2000).
The enormous tolerance that patients develop to the respiratory depressant effects of opioids is illustrated by numerous accounts of opioid doses that have escalated over time. One of the earliest studies on pain and other symptoms in patients with advanced cancer reported that all 90 of the patients reviewed had pain, and almost 40% required increases in their opioid requirements by 25% during the last 4 weeks of life (Coyle, Adelhardt, Foley, et al., 1990). Total daily opioid doses in these patients ranged from 7 to 35,164 mg parenteral morphine equivalents. Five percent used an opioid dose of more than 900 mg parenteral morphine equivalents per day 4 weeks before death, and within 24 hours of death, this proportion increased to 9%. Even patients receiving the highest doses were titrated in the home setting. These findings reinforce that “high” doses of opioids are both appropriate and safe in terminally ill patients with pain.
Other recent research has shown similar findings. A retrospective medical record review of 661 home-care hospice patients noted that 66% received morphine for pain relief and that 91% of these received a dose of between 5 and 299 mg/day and 1.6% received doses of more than 600 mg/day (Bercovitch, Adunksy, 2004). A prospective Canadian study observed that morphine was the most commonly administered drug at end of life in critically ill patients, and the dose ranged from 2 to 450 mg; midazolam was the second most common with a range of 2 to 380 mg (Rocker, Heyland, Cook, et al., 2004). This study also surveyed the families of the patients and reported strong evidence of the staff’s ability to convey a caring attitude; 92.3% of surveyed family members reported feeling “supported” or “very supported” by the health care team during their loved ones’ dying process. This type of positive experience is not always the case (Teno, Clarridge, Casey, et al., 2004). The health care team often misses opportunities to facilitate family interactions and improve the family’s involvement in decision making and understanding of the comprehensive treatment plan (Mularski, Puntillo, Varkey, et al., 2009).
Research shows that there is wide variation in the treatment of pain and other discomforts during withdrawal of life support in the ICU; the use of standardized protocols and guidelines are recommended as a way to improve the health care team’s decision making and ultimately patient outcomes at end of life (Mularski, Puntillo, Varkey, et al., 2009). The implementation of a standardized order form for the withdrawal of life support in the ICU resulted in an increase in total doses of opioids and benzodiazepines, and there was no change in the median time from ventilator withdrawal pre- and post-implementation of the form (Treece, Engelberg, Crowley, et al., 2004).
Most patients with advanced illness lose the ability to communicate during the final days of life. This loss of communication should not be interpreted as loss of pain. As described above, higher doses at end of life suggest that pain often increases as death approaches. Patients who are confused, grimacing, moaning, agitated, or restless most likely are experiencing unrelieved pain and require an increase in the opioid dose (see Section II). Opioids should be continued at the optimized dose in patients who lose consciousness at the end of life.
Treatment of Dyspnea
Dyspnea is a very distressing symptom that can occur in both opioid-naïve and opioid-tolerant patients (Bruera, Currow, 2009). It is a common symptom in many cancer and noncancer-related chronic illnesses (Newton, Davidson, Macdonald, et al., 2008). It is often present at end of life and is an independent predictor for shorter survival among cancer patients (Bruera, Currow, 2009). An early prospective study of hospice patients in the last 6 weeks of life found that as many as 70% suffered from the condition (Reuben, Mor, 1986). There is no consensus on how to measure breathlessness (Bruera, Currow, 2009). Patients’ subjective descriptions of dyspnea vary widely, for example, “difficult, labored, uncomfortable breathing” and “the sensation of breathlessness or air hunger” (American Thoracic Society, 1999). The condition is associated with significant patient distress and poor quality of life (Edmonds, Higginson, Altmann, et al., 2000). It often coexists with fatigue, depression, and anxiety (Bruera, Currow, 2009).
Clinical assessment of dyspnea is described as having four components: (1) obtaining a comprehensive history about onset and exacerbating and relieving factors; (2) performing a physical examination for causes; (3) assessing the intensity of unpleasantness of breathlessness with a scale (e.g., 0-to-10) to establish a baseline; and (4) tracking dyspnea along with other symptoms to evaluate its impact on quality of life (Bruera, Currow, 2009). A variety of medications and routes of administration have been used to treat dyspnea, although opioids have been the mainstay for treatment of dyspnea for many years (Pasero, Portenoy, McCaffery, 1999). A Cochrane Collaboration Review concluded that there was evidence to support the use of systemic (oral, parenteral) but not nebulized opioids to treat dyspnea (Jennings, Davies, Higgins, et al., 2001). The researchers encouraged more research with larger numbers of patients, the use of standardized protocols, and evaluation of quality of life measures. A later review of 20 articles with evaluable evidence reached similar conclusions (Joyce, McSweeney, Carrieri-Kohlman, et al., 2004). In their evidence-based guidelines on interventions to improve the palliative care of pain, dyspnea, and depression, the American College of Physicians recommended the use of opioids for both pain and dyspnea based on a history of proven effectiveness (Qaseem, Snow, Shekelle, et al., 2008).
Oxygen has been used for treatment of dyspnea, but a prospective study (N = 46) found no correlation between intensity of dyspnea and oxygen saturation in either hypoxic or nonhypoxic palliative care patients who received -oxygen (4 L/min) by nasal cannulation; opioids on the other hand, significantly reduced the intensity of the patients’ dyspnea (Clemens, Quednau, Klaschik, 2009). A small randomized controlled, double-blind, crossover trial (N = 9) administered placebo or 5 mg of subcutaneous morphine to 7 opioid-naïve older adults and 3.5 mg of subcutaneous morphine in addition to their usual oral morphine doses to 2 older adults (all patients had cancer) and found that the subcutaneous morphine significantly improved the symptoms of dyspnea and did so without compromising respiratory effort or oxygen saturation (Mazzocato, Buclin, Rapin, 1999). Another small study (N = 6) found similar results in patients with terminal amyotrophic lateral sclerosis (Clemens, Klaschik, 2008a).
Clinicians are sometimes reluctant to use opioids to treat dyspnea, citing concern that adding another or more opioid to the opioid a patient is already receiving for analgesia, or starting an opioid in an opioid-naïve patient, increases the risk of opioid-induced sedation or respiratory depression. Studies have not confirmed this fear.
A randomized, double blind, placebo-controlled cross-over trial found that oral modified-release morphine (20 mg) provided significant improvement in refractory dyspnea in 48 opioid-naïve patients (Abernethy, Currow, Frith, et al., 2003). Treatment was tolerated well with minimal adverse effects, and patients cited improved sleep as a major benefit of treatment. Hydromorphone has also been used for dyspnea. A small prospective study demonstrated that titrated doses of oral hydromorphone produced considerable and sustained improvement of moderate or severe dyspnea during both rest and mild activity in 14 palliative care patients (Clemens, Klaschik, 2008b). The mean single dose of hydromorphone was 2.5 mg (0.5 to 6.0 mg range). Half of the patients were opioid-naïve. An important finding was that there were no significant increases in carbon dioxide (CO2) or decreases in oxygen (O2) saturation. Treatment with hydromorphone was continued in all patients after the study was completed.
As mentioned earlier in the chapter, more well-controlled research is needed on the use of nebulized opioids (see Chapter 14). Nevertheless, morphine by this route has been used for many years to treat dyspnea. A prospective, nonrandomized study (N = 46) used transcutaneous CO2 measurement and pulse oximetry (O2 saturation) and found that there was no higher risk of respiratory depression in opioid-naïve compared with opioid-tolerant palliative patients treated with nebulized morphine (Clemens, Quednau, Klaschik, 2008). The patients experienced a significant decrease in the intensity of dyspnea and respiratory rate. These studies and clinical experience support the recommendation that carefully titrated doses of opioids for treatment of dyspnea should be administered to patients who are suffering from the distress of having to fight to breathe.
End-of-Life Nursing Education Consortium (ELNEC)
There have been numerous educational efforts directed toward improving the nurse’s ability to manage pain and the other symptoms patients experience at the end of life. One of the most successful efforts is the End-of-Life Nursing Education Consortium (ELNEC), which began in 2000 and was funded initially by the Robert Wood Johnson Foundation and administered by the American Association of Colleges of Nursing (AACN) and the City of Hope in Duarte, California. Partnerships have developed with other organizations, such as the Oncology Nursing Society, Sigma Theta Tau International, and the National Cancer Institute, among many others, to fund and provide training (Malloy, Paice, Virani, et al., 2008). By the summer of 2009, almost 9000 nurses representing all 50 states in America had received ELNEC training through national courses and, as instructors, had extended that knowledge to countless other nurses and members of the health care team (AACN, 2009). There are international ELNEC courses as well. One oncology training program reported that participants had educated 26,000 nurses after attending the course (Coyne, Paice, Ferrell, et al., 2007). The ELNEC educational modules focus on palliative care in advanced practice nursing; pain and symptom management; communication; ethical issues; final hours of life; loss, grief, and bereavement; and achieving quality care at the end of life (Malloy, Paice, Virani, et al., 2008). Follow-up evaluation of ELNEC seminars reveal many successes as well as ongoing challenges, such as a lack of funds and minimal institutional support for educational efforts (Ferrell, Virani, Paice, et al., 2009). For information on ELNEC training, the reader is referred to the AACN website http://www.aacn.nche.edu/ELNEC/. For information on international ELNEC training, see http://www.aacn.nche.edu/elnec.
Conclusion
The undertreatment of pain as a result of the unwarranted withholding of opioids is particularly disturbing. Among the many patients at risk for this are those with persistent noncancer pain, individuals with addictive disease, women during pregnancy and breast-feeding, the critically ill, and individuals at the end of life.
Section IV Conclusion
OPIOID analgesics remain first-line agents for the treatment of moderate-to-severe acute pain, persistent cancer pain, and some persistent noncancer pain states. For many patients with pain, particularly those in the palliative care settings, opioid drugs continue to be the mainstay of analgesia. Pain control is improved and adverse effects are reduced when they are given in combination with nonopioids and adjuvant analgesics as part of a multimodal pain treatment plan.
Documenting Pain Management
Documentation is a means for communicating pain assessments (e.g., pain ratings), interventions to manage the pain, and the patient’s response (e.g., pain ratings and adverse effects). The more severe the pain, the more often it is assessed and documented. The use of opioid analgesics requires documentation, not only as an intervention but also for substance control purposes. When invasive therapies are used, such as epidural analgesia and PCA, special flow sheets are useful for ensuring that the patient’s pain assessments, adverse effects, and use of opioids during therapy are documented. Use of a flow sheet helps to centralize and standardize documentation, avoid duplication of documentation, save time, meet substance control requirements, and provide an overall picture of the patient’s pain experience during treatment. The reader is referred to Section II for a detailed discussion of documentation of pain and examples of a variety of flow sheets.
Patient Education
As discussed in Chapter 12, adherence to the pain treatment plan helps to ensure optimal pain control. A review of the literature revealed numerous reasons why patients do not adhere to a variety of medications prescribed for pain (Monsivais, McNeil, 2007). In addition to an introductory review of the literature, these authors examined 42 abstracts and 17 full-text articles. Some of the concerns revealed are pertinent to opioid analgesics and may be diminished by providing the patient with both verbal and written information about their medications. (See Patient Medication Education Forms for selected medications on pp. 547-579 at the end of this section.) A common reason for nonadherence was high levels of concern about the medication, such as adverse effects, “dependency,” and questions about the real need for the medication. Patients also had misconceptions about how long it should take for the drug to be effective, and they would stop taking it if no benefits occurred by the expected time. Patients also feared tolerance, that is, that the medication might cease to work if taken on a regular basis.
An excellent synthesis of quantitative and qualitative research on the use of morphine for cancer pain treatment revealed key social, contextual, and physical concerns held by patients, caregivers, and health care professionals (Flemming, 2010). The synthesis showed that patients commonly perceive that the use of morphine is a balancing act and a trade-off between pain relief and adverse effects. For example, there is evidence that patients struggle with wanting pain relief but fearing that adverse effects would prevent them from maintaining functionality. Deep-seated concerns about the symbolism of morphine, addiction, and tolerance held by patients, caregivers, and health care professionals were shown to affect prescription, dispensation, and use of opioids. For many of the patients, the use of morphine was considered a “last resort” or “death sentence.”
A superb qualitative study of the perspectives of patients receiving long-term opioid treatment for persistent noncancer pain revealed that desperation, humiliation, and thoughts of suicide were common before opioid treatment (Vallerand, Nowak, 2009). After treatment was initiated, patients described the challenge of maintaining a balance between pain, pain relief, and functionality as well as having to live a “secret life” (hiding medications) for fear that others would misunderstand the need for opioid treatment. An overriding theme of this research was the anticipation or dread of losing their treatment regimen and returning to a life of pain.
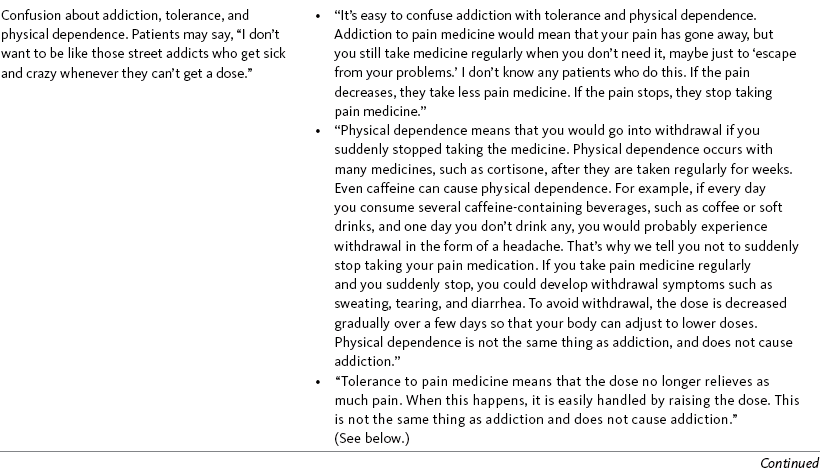
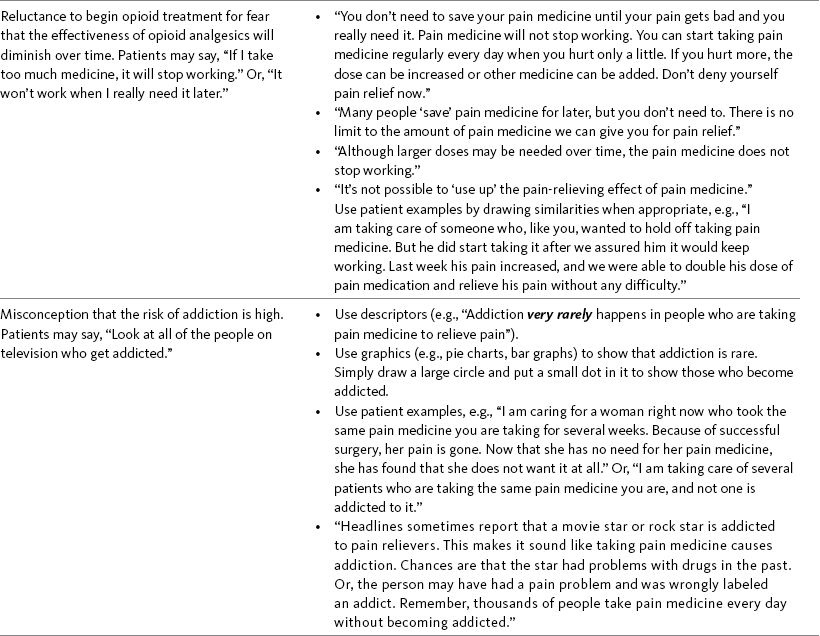
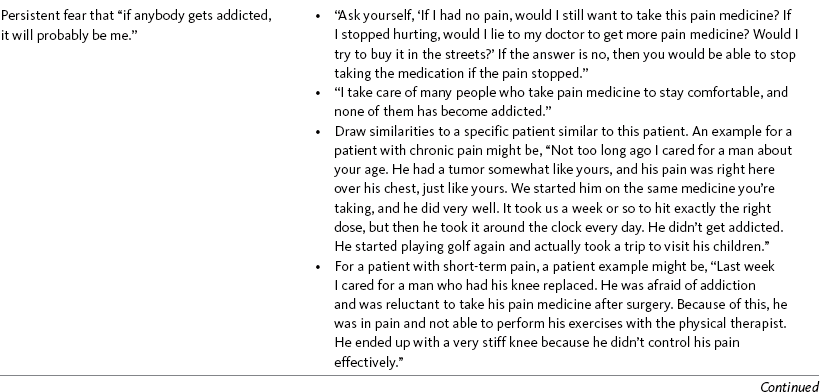
All of this research underscores the importance of initial and ongoing discussion about pain and opioid use with patients and their families and caregivers to ensure such fears and barriers are adequately addressed. It should be assumed that all patients share at least some of the feelings described in the research, so such discussion should be an integral part of care. Ensuring that patients obtain the maximum benefit from opioid analgesics requires education of the patient and family/caregiver. Teaching patients and families about addiction, tolerance, and physical dependence often fails to allay fears and change attitudes. Efforts to present the facts about such emotionally charged issues frequently are overshadowed by fiercely held beliefs. No proven method exists for breaking down such strong barriers to achieving effective pain control. Where one method may work with 1 patient, it may fail with another. Giving consistent and confident explanations about addiction and repeating information frequently provides reassurance for patients and their families. Table IV-1 provides considerations and examples of responses to the concerns patients and families often express about addiction. Using a variety of these approaches is recommended at the start and periodically during the course of treatment.
Table IV-1
Talking with Patients and Families about Addiction
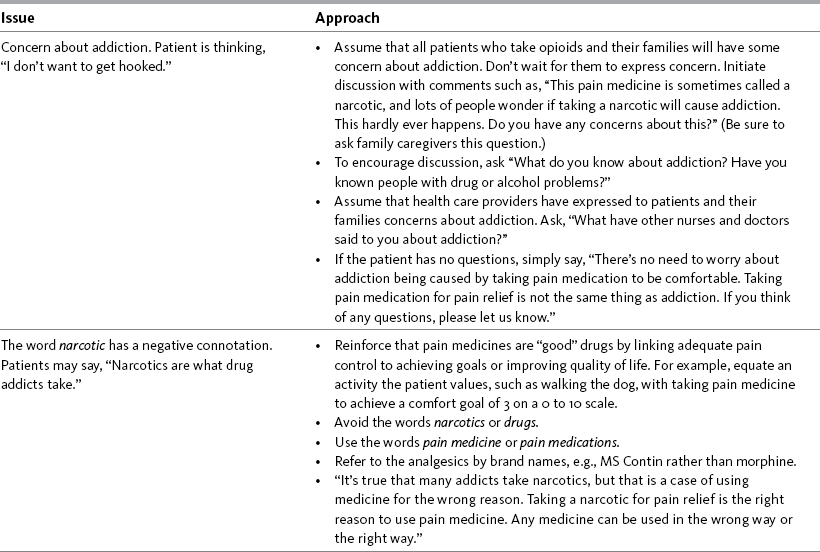
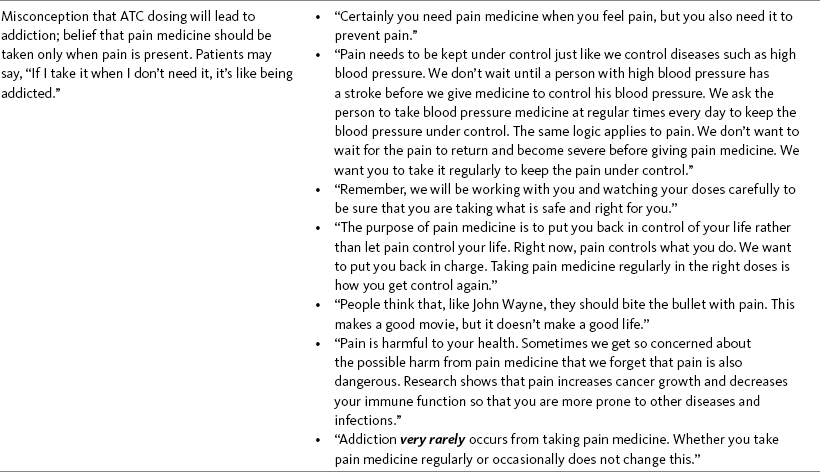
From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 539-541, St. Louis, Mosby. Data from Jacox, A., Carr, D. B., Payne, R., et al. (1994). Managing cancer pain: Consumer version. Clinical practice guideline No. 9. AHCPR Publication No. 94-0595, Rockville, MD, U.S. Public Health Service, AHCPR, March 1994; Lang, S. L., & Patt, R. B. (1994). You don’t have to suffer, New York, Oxford University Press. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
In addition to verbal explanations, providing written information reinforces explanations about method of opioid delivery, dose, dosing schedules, and other important points that the patient and family will need to remember. The information in the “Patient Medication Information” forms that follow is based on content from this section and the following five references:
1. Clinical Pharmacology Online. Gold Standard, Inc. Available at http://clinicalpharmacology.com.
2. Drug inserts, available online for each medication.
3. Fox Chase Cancer Center/Pain Management. Patient Education Forms, Philadelphia. (Codeine plus acetaminophen, 2007; Darvocet, 2007; extended-released morphine, 2008; fentanyl patch, 2008; hydrocodone, 2007; morphine concentrate, 2007; morphine sulfate tablets or capsules, 2007; oral transmucosal fentanyl citrate, 2007; oxycodone, 2007; oxycodone HCL modified-release tablets, 2008; oxycodone plus acetaminophen, 2008; time-released morphine, 2007; Tylenol with codeine, 2007.)
4. Clinical Pharmacology Online. Gold Standard, Inc. Available at http://clinicalpharmacology.com.
5. Lacy, C. F., Armstrong, L. L., Goldman, M. P., et al. (Eds.). (2009-2010). Drug information handbook, ed 18, Hudson, OH, American Pharmacists Association, Lexi-Comp.
Patient Information Brochure: Patient-Controlled Epidural Analgesia (PCEA)
• When you are injured, pain warns you to protect yourself and avoid further injury. However, unrelieved pain can be harmful, especially when you are sick or after surgery. Pain can make it difficult to take a deep breath and interferes with your ability to move and walk. This can result in complications and a long stay in the hospital.
How will others know how much pain I have?
• Your nurses will check you often while you are receiving PCEA. They will ask you to rate your pain on a 0 to 10 scale. A rating of 0 means you feel no pain at all, 5 means you feel a moderate (medium) amount of pain, and 10 means you feel the worst pain you can imagine.

• Your comfort-function goal is _________________________________________. If you are unable to maintain this level of comfort, especially during activities such as physical therapy, let your nurse know. The dose of pain medicine usually can be increased to keep you as comfortable as possible.
• Pain medicine will be given by a small pump through an epidural catheter, which is a tiny tube that will be put in your back before surgery.
• The pump will give you a small amount of pain medicine continuously.
• You also will have a PCEA button that is attached to the pump. You can press the PCEA button to give yourself a dose of pain medicine when you hurt.
• The recovery room nurse will manage your pain for you when you arrive in the recovery room, then give you the PCEA button as soon as you are awake enough to manage the pain yourself.
• It is difficult to treat pain when it is severe, so it is important to “stay on top” of your pain. When you begin to feel some discomfort, press the PCEA button, and then wait a few minutes to see if the dose helped to relieve the pain. If the pain has not been relieved, press the PCEA button again.
How is the epidural catheter placed?
• You will be positioned on your side or sitting up with your back arched out to the anesthesiologist.
• Your back will be washed with a cool soap solution.
• The anesthesiologist will inject local anesthetic to numb the area where the catheter will go. This will sting like a bee bite.
• You will feel pressure against your back while the anesthesiologist finds the epidural space.
• A very small catheter will be inserted through the needle into the epidural space, and then the needle will be removed.
• The catheter will be taped to your back and up to your shoulder where it will be connected to the pump.
• While the catheter is in place, you may lie on your back, turn, walk, and perform any activities your physician or nurse approves.
• The pump will be programmed to give you an amount of pain medicine that is typically safe for someone your sex, size, age, and diagnosis or type of surgery. If this is too much, the dose of the pain medicine can be reduced.
• The pump will be set with a safe time between doses so you cannot give yourself too much pain medicine too often.
• PATIENT-ONLY USE! You are the only person who will know when you are hurting and when it is necessary and safe to have a dose of pain medicine. Therefore you are the only person who should press the PCEA button. Your family, visitors, physicians, and hospital personnel are not to press the PCEA button. If you or they are concerned about your pain, let the nurse know.
• Let the nurse know before you take any other medicines, including the ones you usually take at home.
What are the side effects of PCEA?
• Itching is not an allergic reaction but is a fairly common adverse effect of pain medicine. Ask the nurse for medicine to relieve the itching when necessary.
• Nausea can occur from pain medicine, and it also can be treated with medicine that has been prescribed.
• Some patients have difficulty urinating while taking pain medicine. Reducing the dose of pain medicine helps relieve this adverse effect, and it usually resolves on its own within 48 hours.
• Pain medicine slows the bowel and can cause constipation. If your condition allows, the nurse will give you medicine to prevent constipation.
• Excessive drowsiness and respiratory depression are the most serious but least common adverse effects of pain medicine. It is rare for patients to experience these effects. These effects develop slowly, and nurses will be checking your sedation and breathing frequently. If these occur, both are easily treated and corrected by decreasing the dose of pain medicine. Let the nurse know if you feel too sleepy.
• Numbness and tingling from the epidural local anesthetic is normal in and around the surgery incision area. Let your nurse know if numbness or tingling occurs in other areas. If you have difficulty feeling or moving your legs, stay in bed and call your nurse. This usually can be corrected by reducing the dose of pain medicine. Be sure to ask someone to help you up the first few times you walk.
• As your condition improves, your pain will decrease. You will find that you need to press the PCEA button less often as you improve.
• The dose of pain medicine will be decreased gradually until the pump is no longer necessary and you are able to use a different method for taking pain medicine.
• Your nurse will remove the epidural catheter. This is a simple and painless procedure.
In addition to talking with patients about opioids and their adverse effects, providing written information reinforces explanations about the method of opioid delivery and other important points the patient will need to remember. This box provides an example of a patient information brochure on PCEA.
From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 542-543, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
Patient Information Brochure: Intravenous Patient-Controlled Analgesia (IV PCA)
• When you are injured, pain warns you to protect yourself and avoid further injury. However, unrelieved pain can be harmful, especially when you are sick or after surgery. Pain can make it difficult to take a deep breath and interferes with your ability to move and walk. This can result in complications and a long stay in the hospital.
How will others know how much pain I have?
• Your nurses will check you often while you are receiving IV PCA. They will ask you to rate your pain on a 0 to 10 scale. A rating of 0 means you feel no pain at all, 5 means you feel a moderate (medium) amount of pain, and 10 means you feel the worst pain you can imagine.

• Your comfort-function goal is __________. If you are unable to maintain this level of comfort, especially during activities such as physical therapy, let your nurse know. The dose of pain medicine usually can be increased to keep you as comfortable as possible.
• Pain medicine will be given by a small pump through your IV line. If you have surgery, this will be attached to your IV in the recovery room.
• You will have a PCA button that is attached to the pump. You can press the button to give yourself a dose of pain medicine when you hurt.
• The recovery room nurse will manage your pain for you when you arrive in the recovery room, then give you the PCA button as soon as you are awake enough to manage the pain yourself.
• It is difficult to treat pain when it is severe, so it is important to “stay on top” of your pain. When you begin to feel some discomfort, press the PCA button, and then wait a few minutes to see if the dose helped to relieve the pain. If the pain has not been relieved, press the PCA button again.
• If you have any trouble controlling your pain, let your nurse know. The dose of pain medicine may need to be increased, or you may be given oral pain medicine.
• The pump will be programmed to give you an amount of pain medicine that is typically safe for someone your sex, size, age, and diagnosis or type of surgery. If this is too much, the dose of the pain medicine can be reduced.
• The pump will be set with a safe time between doses so you cannot give yourself too much pain medicine too often.
• PATIENT-ONLY USE! You are the only person who will know when you are hurting and when it is necessary and safe to have a dose of pain medicine. Therefore you are the only person who should press the PCA button. Your family, visitors, physicians, and hospital personnel are not to press the PCA button. If you or they are concerned about your pain, let the nurse know.
• Let the nurse know before you take any other medicines, including the ones you usually take at home.
What are the side effects of IV PCA?
• Itching is not an allergic reaction but is a fairly common adverse effect of pain medicine. Ask the nurse for medicine to relieve the itching when necessary.
• Nausea can occur from pain medicine, and it also can be treated with medicine that has been prescribed.
• Some patients have difficulty urinating while taking pain medicine. Reducing the dose of pain medicine helps relieve this adverse effect, and it usually resolves on its own within 48 hours.
• Pain medicine slows the bowel and can cause constipation. If your condition allows, the nurse will give you medicine to prevent constipation.
• Excessive drowsiness and respiratory depression are the most serious but least common adverse effects of pain medicine. It is rare for patients to experience these effects. These effects develop slowly, and nurses will be checking your sedation and breathing frequently. If these occur, both are easily treated and corrected by decreasing the dose of pain medicine. Let the nurse know if you feel too sleepy.
• As your condition improves, your pain will decrease. You will find that you need to press the PCA button less often as you improve.
• The dose of pain medicine will be decreased gradually until the pump is no longer necessary and you are able to use a different method for taking pain medicine.
In addition to talking with patients about opioids and their adverse effects, providing written information reinforces explanations about the method of opioid delivery and other important points the patient will need to remember. This box provides an example of a patient information brochure on IV PCA.
From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 544-545, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
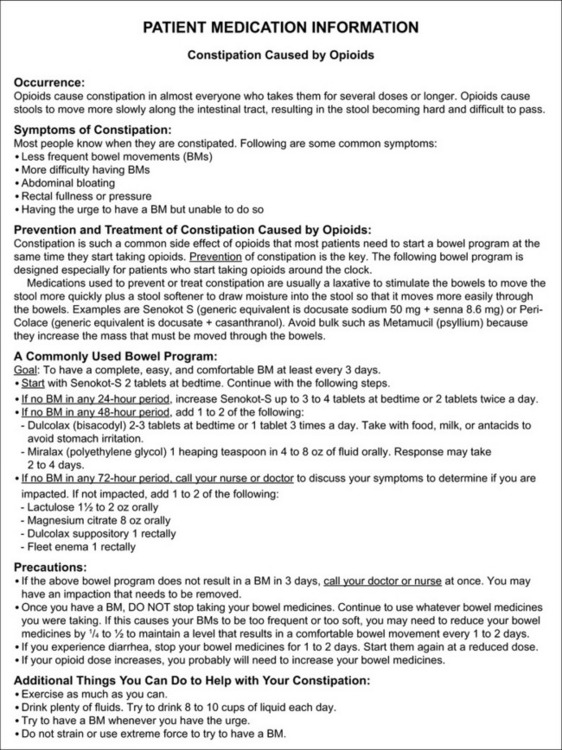
Form IV-1 Constipation caused by opioids: patient information. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 546, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
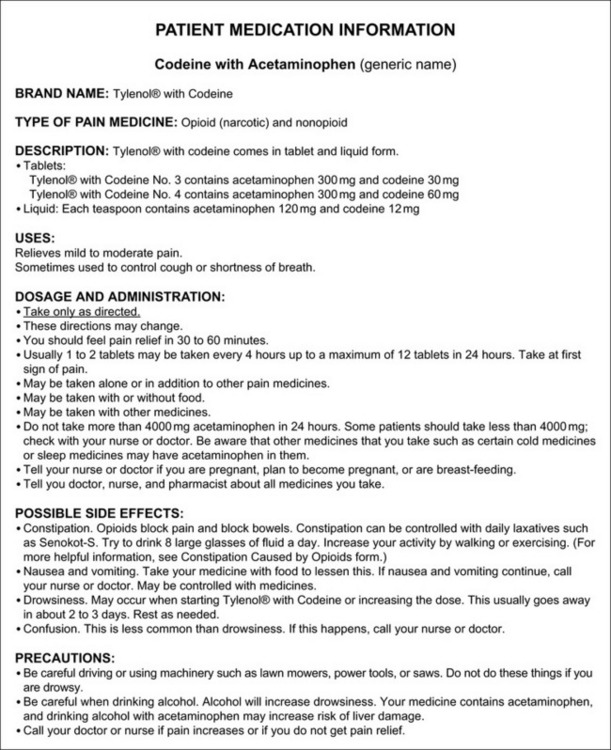
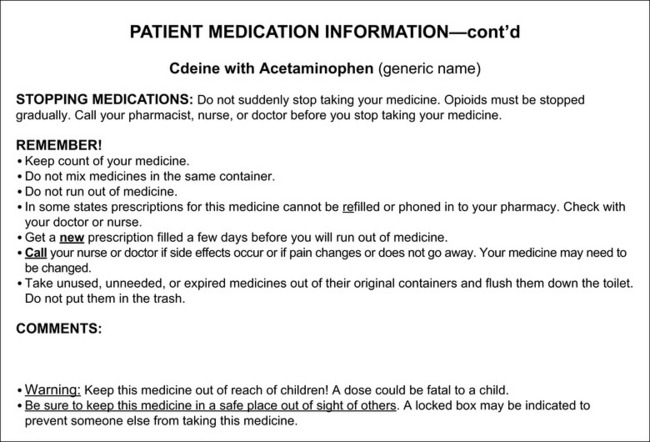
Form IV-2 Patient medication information: codeine with acetaminophen. As appears in Pasero, C., & McCaffery, M. (2011). Pain assessment and pharmacologic management, pp. 547-548, St. Louis, Mosby. Modified from Fox Chase Cancer Center/Pain Management, Philadelphia, 2007. May be duplicated for use in clinical practice.
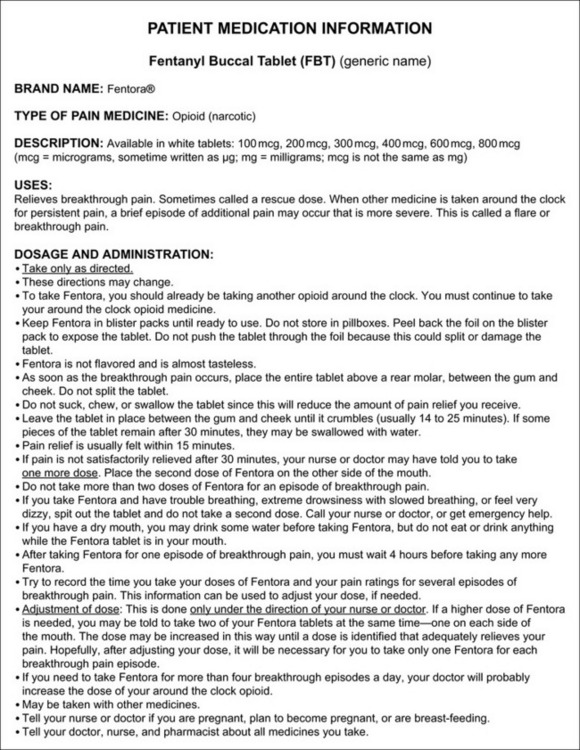
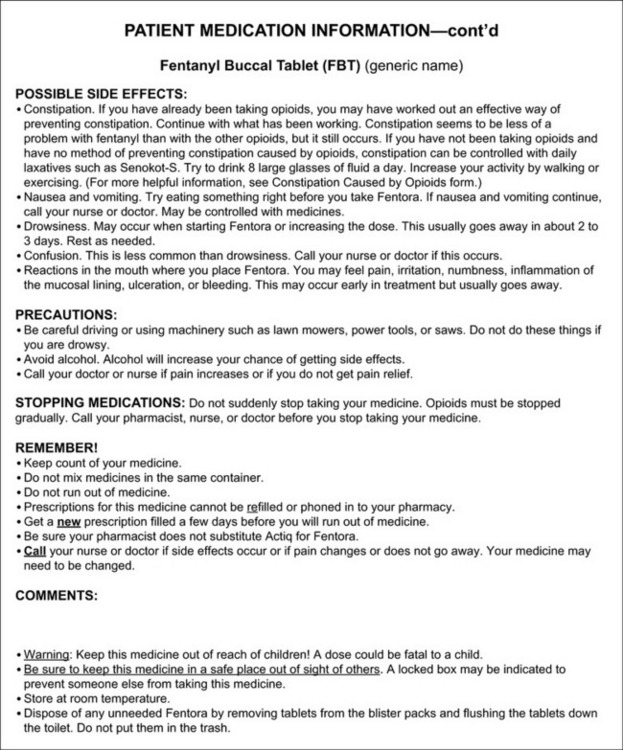
Form IV-3 Patient medication information: fentanyl buccal tablet. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 549-550, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
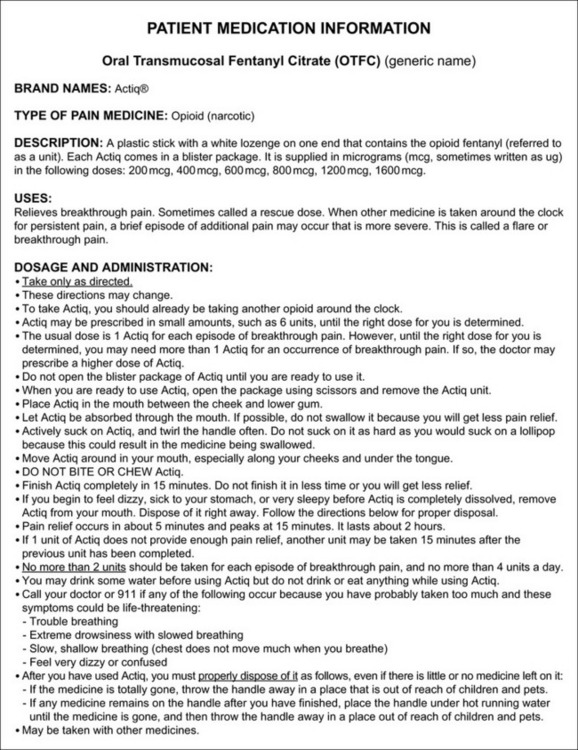

Form IV-4 Patient medication information: oral transmucosal fentanyl citrate. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 551-552, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
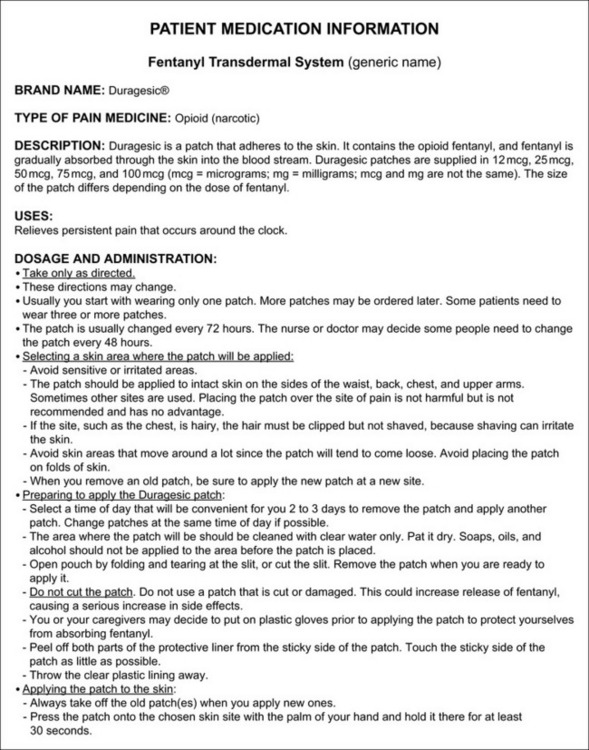
Form IV-5 Patient medication information: fentanyl transdermal system. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 553-555, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
Form IV-6 Patient medication information: hydrocodone with acetaminophen. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 556-557, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
Form IV-7 Patient medication information: hydromorphone. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 558-559, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
Form IV-8 Patient medication information: methadone. As appears in Pasero, C., & McCaffery, M. (2011). Pain assessment and pharmacologic management, pp. 560-561, St. Louis, Mosby. From Leavitt, S. B. (2008). Methadone safety handout for patients. Pain Treatment Topics. Available at http://pain-topics.org/pdf/MethadoneHandout.pdf. Accessed Sept. 30, 2009.
Form IV-9 Patient medication information: morphine sulfate, short-acting. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 562-563, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
Form IV-10 Patient medication information: morphine sulfate, modified-release, 12-hour dosing. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 564-565, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
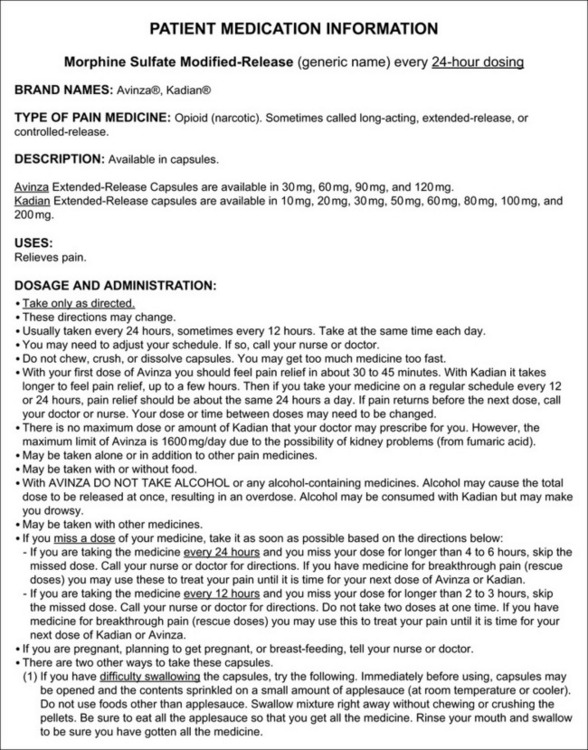
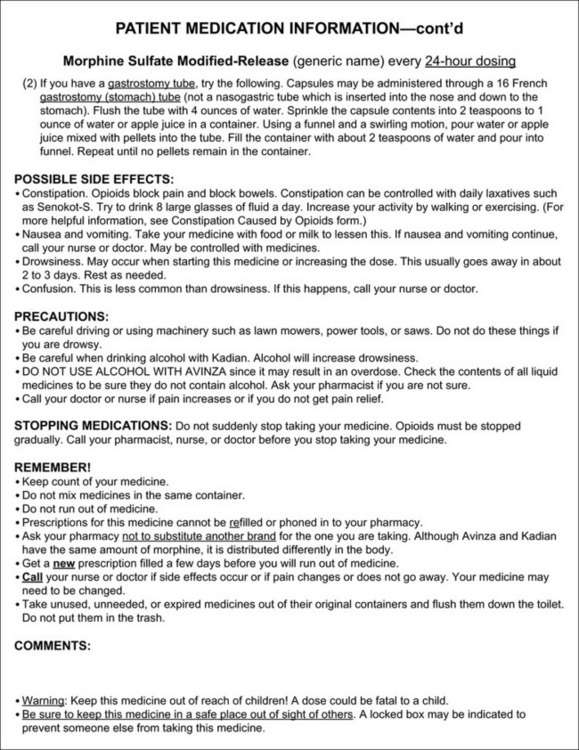
Form IV-11 Patient medication information: morphine sulfate, modified-release, 24-hour dosing. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 566-567, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
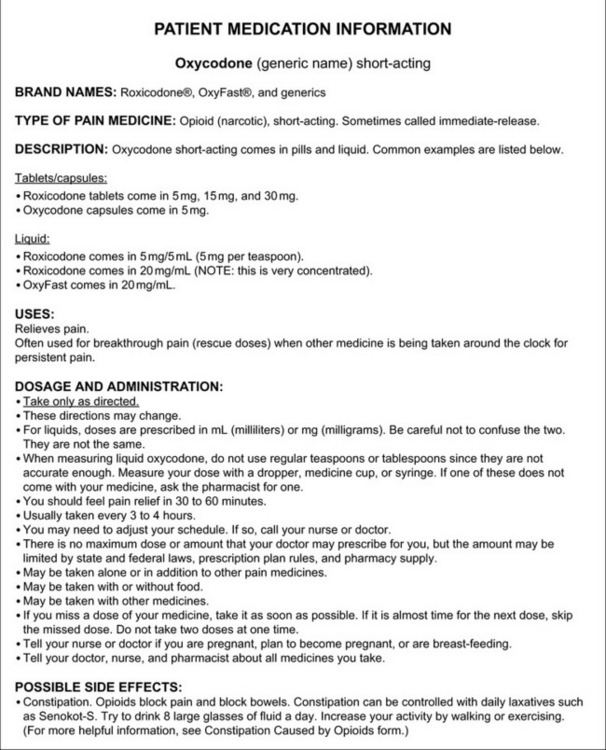
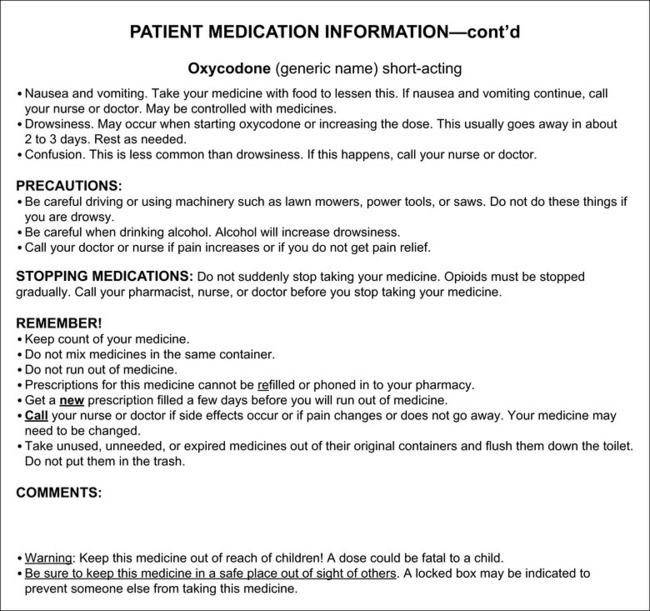
Form IV-12 Patient medication information: oxycodone, short-acting. As appears in Pasero, C., & McCaffery, M. (2011). Pain assessment and pharmacologic management, pp. 568-569, St. Louis, Mosby. Modified from Fox Chase Cancer Center/Pain Management, Philadelphia, 2007. May be duplicated for use in clinical practice.
Form IV-13 Patient medication information: oxycodone, modified-release. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 570-571, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.

Form IV-14 Patient medication information: oxycodone with acetaminophen. As appears in Pasero, C., & McCaffery, M. (2011). Pain assessment and pharmacologic management, pp. 572-573, St. Louis, Mosby. Modified from Fox Chase Cancer Center/Pain Management, Philadelphia, 2008. May be duplicated for use in clinical practice.

Form IV-15 Patient medication information: oxymorphone. From Pasero, C., & McCaffery, M. Pain assessment and pharmacologic management, pp. 574-575, St. Louis, Mosby. McCaffery M, Pasero C. May be duplicated for use in clinical practice.
References
Abd-El-Maeboud, K.H, Ghazy, A.A., Nadeem, A.A, et al. Effect of vaginal pH on the efficacy of vaginal misoprostol for induction of midtrimester abortion. The Journal of Obstetrics and Gynaecology Research. 2008;34(1):78–84.
Abnerthy, A.P., Currow, D.C., Frith, P., et al. Randomised, double blind, placebo controlled crossover trial of sustained release morphine for the management of refractory dyspnea. BMJ (Clinical Research Ed.). 2003;327(7414):523–528.
Abou hammoud, H., Simon, N., Urien, S., et al. Intravenous morphine titration in immediate postoperative pain management: Population kinetic-pharmacodynamic and logistic regression analysis. Pain. 2009;144(1–2):139–146.
Acute Pain Management Guideline Panel. AHCPR Pub. No. 92-0032. Acute pain management: Operative or medical procedures and trauma. Agency for Health Care Policy and Research (AHCPR), Public Health Service, U.S. Department of Health and Human Services, 1992.
Adams, E.H., Chwiecko, P., Ace-Wagoner, Y., et al. A study of Avinza (morphine sulfate extended-release capsules) for chronic moderate-to-severe noncancer pain conducted under real-world treatment conditions – the ACCPT study. Pain Practice. 2006;6(4):254.
Adams, M., Pieniaszek, H.J., Jr., Gammaitoni, A.R., et al. Oxymorphone extended release does not affect CYP2C9 or CYP3A4 metabolic pathways. Journal of Clinical Pharmacology. 2005;45(3):337–345.
Agarwal, A., Gautam, S., Nath, S.S., et al. Comparison of the incidence and severity of cough induced by sufentanil and fentanyl: A prospective, randomised, double-blind study. Anaesthesia. 2007;62(12):1230–1232.
Agarwal, S., Polydefkis, M., Block, B., et al. Transdermal fentanyl reduces pain and improves functional activity in neuropathic pain states. Pain Medicine. 2007;8(7):554–562.
Agashe, G.S., Coakley, J., Mannheimer, P.D. Forehead pulse oximetry: Headband use helps alleviate false low readings likely related to venous pulsation artifact. Anesthesiology. 2006;105(6):1111–1116.
Ahdieh, H., Ma, T., Babul, N., et al. Efficacy of oxymorphone extended release in postsurgical pain: A randomized clinical trial in knee arthroplasty. Journal of Clinical Pharmacology. 2004;44(7):767–776.
Alcoholics Anonymous (AA) World Services, Inc. The A.A. Member – Medications and Other Drugs. New York, NY: AA, 1984.
Alemdar, M., Pekdemir, M., Selekler, H.M. Single-dose intravenous tramadol for acute migraine pain in adults: A single-blind, prospective, randomized, placebo-controlled clinical trial. Clinical Therapeutics. 2007;29(7):1441–1447.
Alford, D.P., Compton, P., Samet, J.H. Acute pain management for patients receiving maintenance methadone or buprenorphine therapy. Annals of Internal Medicine. 2006;144(2):127–134.
Alkhazrajy, W.K., Macintyre, P.E., Upton, R.N., et al. An audit of the safety and effectiveness of an alfentanil:morphine mixture in the postanaesthesia care unit. Acute Pain. 2007;9(1):13–19.
Allan, L., Hays, H., Jensen, N.H., et al. Randomised crossover trial of transdermal fentanyl and sustained release oral morphine for treating chronic noncancer pain. BMJ (Clinical Research Ed.). 2001;322(7295):1154–1158.
Allan, L., Richarz, U., Simpson, K., et al. Transdermal fentanyl versus sustained release oral morphine in strong-opioid naïve patients with chronic low back pain. Spine. 2005;30(22):2484–2490.
Allegri, M., Baldi, C., Pitino, E., et al. An accidental intravenous infusion of ropivacaine without any adverse effects. Journal of Clinical Anesthesia. 2009;21(4):312–313.
Allen, L.V., Stiles, M.L., Tu, Y.H. Stability of fentanyl citrate in 0.9% sodium chloride solution in portable infusion pumps. American Journal of Hospital Pharmacy. 1990;47(7):1572–1573.
Allen, L.V., Stiles, M.L., Wang, D.P. Stability of bupivacaine hydrochloride, epinephrine hydrochlorid, and fentanyl citrate in portable infusion-pump reservoirs. American Journal of Hospital Pharmacy. 1993;50(4):714–715.
Alpharma Pharmaceuticals. Kadian prescribing information. Elizabeth, NJ: Alpharma Pharmaceuticals; 2008 Available at http://www.kadian.com/pages/getfile.aspx?id=1C6197AB-8F83-43E7-B239-D4615293989B [Accessed April 17, 2008].
Alsahaf, M.H., Stockwell, M. Respiratory failure due to the combined effects of transdermal fentanyl and epidural bupivacaine/diamorphine following radical nephrectomy. Journal of Pain and Symptom Management. 2000;20(3):210–213.
Alvarez, J.C., de Mazancourt, P., Chartier-Kastler, E., et al. Drug stability testing to support clinical feasibility investigations for intrathecal baclofen-clonidine admixture. Journal of Pain and Symptom Management. 2004;28(3):268–272.
Amabile, C.M., Bowman, B.J. Overview of oral modified-release opioid products for the management of chronic pain. The Annals of Pharmacotherapy. 2006;40(7/8):1327–1335.
Amador, L.F., Goodwin, J.S. Postoperative delirium in the older patient. Journal of the American College of Surgeons. 2005;200(5):767–773.
American Academy of Pain Medicine (AAPM), American Pain Society (APS), American Society of Addiction Medicine (ASAM) Definitions related to the use of opioids for the treatment of pain, 2001. Available at http://www.painmed.org/pdf/definition.pdf [Accessed July 28, 2009].
American Academy of Pediatrics (AAP), The transfer of drugs and other chemicals into human milk. Pediatrics, 2001;108(3):776–789. Available at http://aappolicy.aappublications.org/cgi/content/full/pediatrics%3b108/3/776 [Accessed November 21, 2008].
American Association of Colleges of Nursing (AACN) End of Life Nursing Education Consortium (ELNEC). American Association of Colleges of Nursing (AACN), 2009. Available at http://www.aacn.nche.edu/ELNEC/factsheet.htm [Accessed September 1, 2009].
American Geriatrics Society (AGS). The management of persistent pain in older persons. Journal of the American Geriatrics Society. 2002;50(1):S205–S224.
American Geriatrics Society (AGS). Panel on Pharmacological Management of Persistent Pain in the Older Persons. Journal of the American Geriatrics Society. 2009;57(8):1331–1346.
American Medical Association (AMA) Council on Ethical and Judicial Affairs. Decisions near the end of life. JAMA: The Journal of the American Medical Association. 1992;267(16):2229–2233.
American Nurses Association (ANA) Pain management and control of distressing symptoms in dying patients, 2003. Available at http://www.nursingworld.org/MainMenuCategories/HealthcareandPolicyIssues/ANAPositionStatements/EthicsandHumanRights.aspx [Accessed September 28, 2009].
American Pain Foundation American Pain Foundation endorses opioid class REMS recommendations to FDA, 2009. Available at http://www.painfoundation.org/newsroom/position-statements/rems-recommendations.pdf. [Accessed March 16, 2010].
American Pain Society (APS). Principles of analgesic use in the treatment of acute pain and chronic cancer pain. Washington DC: APS, 1987.
American Pain Society (APS). Principles of analgesic use in the treatment of acute and cancer pain, 5th ed. Glenview, IL: APS, 2003.
American Pharmacists Association. White paper on designing a risk evaluation and mitigation strategies (REMS) system to optimize the balance of patient access, medication safety, and impact on the health care system. J Am Pharm Assoc. 2009;49(6):729–743.
American Psychiatric Association. text revised. Diagnostic and statistical manual of mental disorders. 4th ed. Washington DC: American Psychiatric Association; 2000.
American Society for Pain Management Nursing (ASPMN). The use of “as needed” range orders for opioid analgesics in the management of acute pain: A consensus statement of the American Society for Pain Management Nursing and the American Pain Society. Lenexa, KS: ASPMN, 2004.
American Society of Addiction Medicine (ASAM) Definitions related to the use of opioids for the treatment of pain: Consensus Statement of the American Academy of Pain Medicine, the American Pain Society, and the American Society of Addiction Medicine, 2001. Available at http://www.asam.org/DefinitionsRelatedtoUseofOpioidsforTreatmentofPain.html [Accessed March 22, 2009].
American Society of Anesthesiologists (ASA). Practice guidelines for acute pain management in the perioperative setting: An updated report. Anesthesiology. 2004;100(6):1573–1581.
American Society of Anesthesiologists (ASA). Practice guidelines for the perioperative management of patients with obstructive sleep apnea. Anesthesiology. 2006;104(5):1081–1093.
American Society of Anesthesiologists Task Force on Neuraxial Opioids. Practice guidelines for the prevention, detection, and management of respiratory depression associated with neuraxial opioid administration. Anesthesiology. 2009;110(2):218–230.
American Society of PeriAnesthesia Nurses (ASPAN). ASPAN’s evidence-based clinical practice guideline for the prevention and/or management of PONV/PDNV. J Perianesthesia Nursing. 2006;21(4):230–250.
American Thoracic Society. Dyspnea. Mechanisms, assessment, and management: A consensus statement. American Journal of Respiratory and Critical Care Medicine. 1999;159(1):321–340.
Andersen, G., Christrup, L., Sjøgren, P. Relationships among morphine metabolism, pain and side effects during long-term treatment: An update. Journal of Pain and Symptom Management. 2003;25(1):74–91.
Anderson, S.L., Shreve, S.T. Continuous subcutaneous infusion of opiates at end-of-life. The Annals of Pharmacotherapy. 2004;38(6):1015–1023.
Andrieu, G., Roth, B., Ousmane, L., et al. The efficacy of intrathecal morphine with or without clonidine for postoperative analgesia after radical prostatectomy. Anesthesia and Analgesia. 2009;108(6):1954–1957.
Anghelescu, D.L., Burgoyne, L.L., Oakes, L.L., et al. The safety of patient-controlled analgesia by proxy in pediatric oncology patients. Anesthesia and Analgesia. 2005;101(6):1623–1627.
Angst, M.S., Chu, L.F., Tingle, M.S., et al. No evidence for the development of acute tolerance to analgesic, respiratory depessant and sedative opioid effects in humans. Pain. 2009;142(1–2):17–26.
Angst, M.S., Clark, D. Opioid-induced hyperalgesia. Anesthesiology. 2006;104(3):570–587.
Angst, M.S., Koppert, W., Pahl, I., et al. Short-term infusion of the mu-opioid agonist remifentanil in humans causes hyperalgesia during withdrawal. Pain. 2003;106(1–2):49–57.
Angst, M.S., Ramaswamy, B., Riley, E.T., et al. Lumbar epidural morphine in humans and supraspinal analgesia to experimental heat pain. Anesthesiology. 2000;92(2):312–324.
Antonopolous, J., Bollinger, K., Goshman, L. Guidelines for use of meperidine. Drug Policy Perspect. 1996;2(3):25–27.
Anwari, JS, Iqbal, S. Antihistamines and potentiation of opioid induced sedation and respiratory depression. Anaesthesia. 2003;58(5):494–495.
Apfel, C.C., Korttila, K., Abdalla, M., et al. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. The New England Journal of Medicine. 2004;350(24):2441–2451.
Apfel, C.C., Kranke, P., Eberhart, L.H.J., et al. Comparison of predictive models for postoperative nausea and vomting. British Journal of Anaesthesia. 2002;88(2):234–240.
Apfel, C.C., Laara, E., Koivuranta, M., et al. A simplified risk score for predicting postoperative nausea and vomiting. Anesthesiology. 1999;91(3):693–700.
Apolone, G., Corli, O., Negri, E., et al. Effects of transdermal buprenorphine on patients-reported outcomes in cancer patients. The Clinical Journal of Pain. 2009;25(8):671–682.
Aqua, K., Gimbel, J.S., Singla, N., et al. Efficacy and tolerability of oxymorphone immediate release for acute postoperative pain after abdominal surgery: A randomized, double-blind, active- and placebo-controlled, parallel-group trial. Clinical Therapeutics. 2007;29(6):1000–1012.
Ardery, G., Herr, K., Hannon, B.J., et al. Lack of opioid administration in older hip fracture patients. Geriatric Nursing (New York, N.Y.). 2003;24(6):353–360.
Argoff, C.E., Tailoring chronic pain treatment to the patient: Long-acting, short-acting, and rapid-onset opioids. Medscape Neurology Neurosurgery 2007. Available at http://www.medscape.com/viewarticle/554015 [Accessed April 6, 2007].
Argoff, C.E. Clinical implications of opioid pharmacogenetics. The Clinical Journal of Pain. 2010;26(Suppl. 1):S16–S20.
Argoff, C.E., Albrecht, P., Irving, G., et al. Multimodal analgesia for chronic pain: Rationale and future directions. Pain Medicine (Malden, Mass.). 2009;10(Suppl. 2):S53–S66.
Argoff, C.E., Backonja, M.M., Belgrade, M.J., et al. Consensus guidelines: Treatment and planning. Mayo Clinic Proceedings. 2006;81(Suppl. 4):S12–S25.
Armstrong, P.J., Morton, C.P., Nimmo, A.F. Pethidine has local anesthetic action on peripheral nerves in vivo. Anaesthesia. 1993;48(5):382–386.
Armstrong, S.C., Cozza, K.L., Sandson, N.B. Six patterns of drug-drug interactions. Psychosomatics. 2003;44(3):255–258.
Armstrong, S.C., Wynn, G.H., Sandson, N.B. Pharmacokinetic drug interactions of synthetic opiate analgesics. Psychosomatics. 2009;50(2):169–176.
Arpino, P.A., Klafatas, K., Thompson, B.T. Feasibility of dexmedetomidine in facilitating extubation in the intensive care unit. Journal of Clinical Pharmacy Therapeutics. 2008;33(1):25–30.
Arsenjo, J.F., Brecht, K.M. Opioids: Other routes for use in recovery room. Current Drug Targets. 2005;6(7):773–779.
Asao, T., Kuwano, H., Nakamura, J., et al. Gum chewing enhances early recovery from postoperative ileus after laparoscopic colectomy. Journal of the American College of Surgeons. 2002;195(1):30–32.
Ashburn, M.A., Caplan, R.A., Carr, D.B., et al. Practice guidelines for acute pain management in the perioperative setting. An updated report by the American Society of Anesthesiologists task force on acute pain management. Anesthesiology. 2004;100(6):1573–1581.
Ashburn, M.A., Fine, P.G., Stanley, T.H. Oral transmucosal fentanyl citrate for the treatment of breakthrough cancer pain: A case report. Anesthesiology. 1989;71(4):615–617.
Ashburn, M.A., Love, G., Pace, N.L. Respiratory-related critical events with intravenous patient-controlled analgesia. The Clinical Journal of Pain. 1994;10(1):52–56.
Ashburn, M.A., Ogden, L.L., Zhang, J., et al. The pharmacokinetics of transdermal fentanyl delivered with and without controlled heat. The Journal of Pain. 2003;4(6):291–297.
Aubrun, F., Bunge, D., Langeron, O., et al. Postoperative morphine consumption in the elderly patient. Anesthesiology. 2003;99(1):160–165.
Aubrun, F., Langeron, O., Quesnel, C., et al. Relationships between measurement of pain using visual analog score and morphine requirements during postoperative intravenous morphine titration. Anesthesiology. 2003;98(6):1415–1421.
Aubrun, F., Marmion, F. The elderly patient and postoperative pain treatment. Best Practice & Research Clinical Anaesthesiology. 2007;21(1):109–127.
Aubrun, F., Monsel, S., Langeron, O., et al. Postoperative titration of intravenous morphine. European Journal of Anaesthesiology. 2001;18(3):159–165.
Aubrun, F., Monsel, S., Langeron, O., et al. Postoperative titration of intravenous morphine in the elderly patient. Anesthesiology. 2002;96(1):17–23.
Aubrun, F., Riou, B. In reply to correspondence. Anesthesiology. 2004;100(3):745.
Aubrun, F., Salvi, N., Coriat, P., et al. Sex- and age-related differences in morphine requirements for postoperative pain relief. Anesthesiology. 2005;105(1):156–160.
Austin, K.L., Stapleton, J.V., Mather, L.E. Relationship between blood meperidine concentrations and analgesic response: A preliminary report. Anesthesiology. 1980;53(6):460–466.
Austin, K.L., Stapleton, J.V., Mather, L.E. Multiple intramuscular injections: A major source of variability in analgesic response to meperidine. Pain. 1980;8:47–62.
Ayonrinde, O.T., Bridge, D.T. The rediscovery of methadone for cancer pain management. The Medical Journal of Australia. 2000;173(10):536–540.
Bach, S., Noreng, M.J., Tjellden, N.U. Phantom pain in amputees during the first 12 months following limb amputation, after preoperative lumbar epidural blockade. Pain. 1988;33(3):297–301.
Badner, N.H., Doyle, J.A., Smith, M.H., et al. Effect of varying intravenous patient-controlled analgesia dose and lockout intervals while maintaining a constant hourly maximum dose. Journal of Clinical Anesthesia. 1996;8(5):382–385.
Bagri, A.S., Rico, A., Ruiz, J.G. Evaluation and management of the elderly patient at risk for postoperative delirium. Clinics in Geriatric Medicine. 2008;24(4):667–686.
Bailie, G.R., Johnson, C.A. Safety of propoxyphene in dialysis patients. Seminars in Dialysis. 2002;15(5):375.
Bainbridge, D., Martin, J.E., Cheng, D.C. Patient-controlled versus nurse-controlled analgesia after cardiac surgery—a meta-analysis. Canadian Journal of Anaesthesia. 2006;53(5):492–499.
Baker, R.A., Zeller, R.A., Klein, R.I., et al. Burn wound itch control using H1 and H2 antagonists. The Journal of Burn Care & Rehabilitation. 2001;22(4):263–268.
Ballantyne, J.C. Does epidural analgesia improve surgical outcome? (Editorial). British Journal of Anaesthesia. 2004;92(1):4–6.
Ballantyne, J.C., Carwood, C. Comparative efficacy of epidural, subarachnoid, and intracerebroventricular opioids in patients with pain due to cancer. Cochrane Database of Systematic Reviews (Online). (1):2005. [CD005178].
Ballas, S.K., Viscusi, E.R., Epstein, K.R. Management of acute chest wall sickle cell pain with nebulized morphine. American Journal of Hematology. 2004;76(2):190–191.
Baltali, S., Turkoz, A., Bozdogan, N., et al. The efficacy of intravenous patient-controlled remifentanil versus morphine anesthesia after coronary artery surgery. Journal of Cardiothoracic and Vascular Anesthesia. 2009;23(2):170–174.
Barkin, R.L., Barkin, S.J., Barkin, D.S. Propoxyphene (dextropropoxyphene): A critical review of a weak opioid analgesic that should remain in antiquity. American Journal of Therapeutics. 2006;13(6):534–542.
Barkin, R.L., Lubenow, T.R., Bruehl, S., et al. Management of chronic pain. Disease-A-Month. 1996;42(7):389–454.
Barnhill, B.J., Holbert, M.D., Jackson, N.M., et al. Using pressure to decrease the pain of intramuscular injections. Journal of Pain and Symptom Management. 1996;12(1):52–58.
Bar-Oz, B., Bulkowstein, M., Benyamini, L., et al. Use of antibiotic and analgesic drugs during lactation. Drug Safety: An International Journal of Medical Toxicology and Drug Experience. 2003;26(13):925–935.
Basse, L., Billesbolle, P., Kehlet, H. Early recovery after abdominal rectopexy with multimodal rehabilitation. Diseases of the Colon and Rectum. 2002;45(2):195–199.
Basse, L., Hjort Jakobsen, D., Billesbolle, P., et al. A clinical pathway to accelerate recovery after colonic surgery. Annals of Surgery. 2000;232(1):51–57.
Basse, L., Raskov, H.H., Hjort Jakobsen, D., et al. Accelerated postoperative recovery programme after colonic resection improves physical performance, pulmonary function, and body composition. The British Journal of Surgery. 2002;89(4):446–453.
Basse, L., Werner, M., Kehlet, H. Is urinary drainage necessary during continuous epidural analgesia after colonic resection? Regional Anesthesia and Pain Medicine. 2000;25(5):498–501.
Bateman, D.N., Eddleston, M. Clinical pharmacology: The basics. The Foundation Years. 2007;3(6):235–239.
Bates, J.J., Foss, J.F., Murphy, D.B. Are peripheral opioid antagonists the solution to opioid side effects? Anesthesia and Analgesia. 2004;98(1):116–122.
Bauer, C., Hentz, J.G., Ducrocq, X., et al. Lung function after lobectomy: A randomized, double-blinded trial comparing thoracic epidural ropivacaine/sufentanil and intravenous morphine for patient-controlled analgesia. Anesthesia and Analgesia. 2007;105(1):238–244.
Beattie, W.S., Badner, N.H., Choi, P. Epidural analgesia reduces postoperative myocardia infarction: A meta-analysis. Anesthesia and Analgesia. 2001;93(4):853–858.
Beaulé, P.E., Smith, M.I., Nguyen, V.N. Meperidine-induced seizure after revision hip arthroplasty. Journal of Arthroplasty. 2004;19(4):516–519.
Beaver, W.T., Frise, G.A. A comparison of the analgesic effect of oxymorphone by rectal suppository and intramuscular injection in patients with postoperative pain. Journal of Clinical Pharmacology. 1977;17(5–6):276–291.
Becker, G., Blum, H.E. Novel opioid antagonists for opioid-induced bowel dysfunction and postoperative ileus. Lancet. 2009;373(9670):1198–1206.
Becker, G., Galandi, D., Blum, H.E. Peripherally acting opioid antagonists in the treatment of opioid-related constipation: A systematic review. Journal of Pain and Symptom Management. 2007;35(5):547–565.
Bedder, M.D., Burchiel, K., Larson, A. Cost analysis of two implantable narcotic delivery systems. Journal of Pain and Symptom Management. 1991;6(3):368–373.
Beers, M.H. Explicit criteria for determining potentially inappropriate medication use by the elderly. An update. Archives of Internal Medicine. 1997;157(14):1531–1536.
Beers, M.H., Ouslander, J.G., Rollingher, I., et al. Explicit criteria for determining inappropriate medication use in nursing home residents. Archives of Internal Medicine. 1991;151(9):1825–1832.
Beers, R., Camporesi, E. Remifentanil update: Clinical science and utility. CNS Drugs. 2004;18(15):1085–1104.
Beilin, Y., Bernstein, H.H., Zucker-Pinchoff, B., et al. Subhypnotic doses of propofol do not relieve pruritus induced by intrathecal morphine after cesarean section. Anesthesia and Analgesia. 1998;86(2):310–313.
Beilin, Y., Bodian, C.A., Weiser, J., et al. Effect of labor epidural analgesia with and without fentanyl on infant breast-feeding. Anesthesiology. 2005;103(6):1211–1217.
Bell, J.G., Shaffer, L.E., Schrickel-Feller, T. Randomized trial comparing 3 methods of postoperative analgesia in gynecology patients: Patient-controlled intravenous, scheduled intravenous, and scheduled subcutaneous. American Journal of Obsetetrics and Gynecology. 2007;197(5):e1–e7. [472].
Beloeil, H., Corsia, G., Coriat, P., et al. Remifentanil compared with sufentanil during extra-corporeal shock wave lithotripsy with spontaneous ventilation: A double-blind, randomized study. British Journal of Anaesthesia. 2002;89(4):567–570.
Ben-David, B., Frankel, R., Arzumonov, T., et al. Minidose bupivacaine-fentanyl spinal anesthesia for surgical repair of hip fracture in the aged. Anesthesiology. 2000;92(1):6–10.
Bendiane, M.K., Bouhnik, A.D., Favre, R., et al. Morphine prescription in end-of-life care and euthanasia: French home nurses’ opinions. Journal of Opioid Management. 2007;3(1):21–26.
Benítez-Rosario, M.A., Salinas-Martín, A., Aguirre-Jaime, A., et al. Morphine-methadone opioid rotation in cancer patients: Analysis of dose ratio predicting factors. Journal of Pain and Symptom Management. 2009;37(6):1061–1068.
Bennett, D., Burton, A.W., Fishman, S., et al. Consensus panel recommendations for the assessment and management of breakthrough pain. Part I Assessment. Pharmacology & Therapeutics. 2005;30(5):296–301.
Bennett, D., Burton, A.W., Fishman, S., et al. Consensus Panel Recommendations for the Assessment and Management of Breakthrough Pain. Part II Management. Pharmacology & Therapeutics. 2005;30(6):354–361.
Bennett, G., Burchiel, K., Buchser, E., et al. Clinical guidelines for intraspinal infusion: Report of an expert panel. Journal of Pain and Symptom Management. 2000;20(2):S37–S43.
Bennett, G., Serafini, M., Burchiel, K., et al. Evidence-based review of the literature on intrathecal delivery of pain medication. Journal of Pain and Symptom Management. 2000;20(2):S12–S36.
Bennett, J.A., Abrams, J.T., Van Riper, D.F., et al. Difficult or impossible ventilation after sufentanil-induced anesthesia is caused primarily by vocal cord closure. Anesthesiology. 1997;87(5):1070–1074.
Bercovitch, M., Adunsky, A. Patterns of high-dose morphine use in a home-care hospice serve: Should we be afraid of it? Cancer. 2004;101(6):1473–1477.
Berde, C.B., Brennan, T.J., Raja, S.N. Opioids: More to learn, improvements to be made. (Editorial). Anesthesiology. 2003;98(6):1309–1312.
Berdine, H.J., Nesbit, S.A. Equianalgesic dosing of opioids. Journal of Pain & Palliative Care Pharmacotherapy. 2006;20(4):79–84.
Berghella, V., Lim, P.J., Hill, M.K., et al. Material methadone dose and neonatal withdrawal. American Journal of Obstetrics and Gynecology. 2003;189(2):312–317.
Berliner, M.N., Giesecke, T., Bornhovd, K.D. Impact of transdermal fentanyl on quality of life in rheumatoid arthritis. The Clinical Journal of Pain. 2007;23(6):530–534.
Bernards, C.M. Rostral spread of epidural morphine. (Editorial). Anesthesiology. 2000;92(2):299–301.
Berntzen, D., Gotestam, K.G. Effects of on-demand versus fixed-interval schedules in the treatment of chronic pain with analgesic compounds. Journal of Consulting and Clinical Psychology. 1987;55(2):213–217.
Beyea, S.C., Nicoll, L.H. Back to basics: Administering IM injections the right way. The American Journal of Nursing. 1996;96(1):34–35.
Bhatnagar, S., Mishra, S., Srikanti, M., et al. Cancer pain management at a tertiary care cancer center in India—a retrospective analysis of 3238 patients. Journal of Opioid Management. 2008;46(6):361–368.
Bhimji, K. Opioid rotation from methadone: Fraught with difficulties. Journal of Pain and Symptom Management. 2005;29(4):334–335.
Bignami, E., Landoni, G., Biondi-Zoccai, G.G.L., et al. Epidural analgesia improves outcome in cardiac surgery: A meta-analysis of randomized controlled trials. Journal of Cardiothoracic and Vascular Anesthesia. 2010. [in press. doi:10.1053/j.jvca.2009.09.015].
Bijur, P.E., Kenny, M.K., Gallagher, E.J. Intravenous morphine at 0.1 mg/kg is not effective for controlling severe acute pain in the majority of patients. Annals of Emergency Medicine. 2005;46(4):362–367.
Bilsen, J., Norup, M., Deliens, L., et al. Drugs used to alleviate symptoms with life shortening as a possible side effect: End-of-life care in six European countries. Journal of Pain and Symptom Management. 2006;31(2):111–121.
BioDelivery Sciences International, Inc Risk Evaluation and Mitigation Strategy (REMS): FOCUS™ Program for Onsolis™, 2009. Available at http://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM187537.pdf [Accessed March 16, 2010].
Birnbach, D.J., Browne, I.M., Anesthesia for Obstetrics. Miller, R.D., eds. Miller’s anesthesia, 6th ed, vol. 2. St. Louis: Churchill Livingstone, 2005;2307–2344.
Birnbaum, A., Esses, D., Bijur, P.E., et al. Randomized double-blind placebo-controlled trial of two intravenous morphine dosages (0.10 mg/kg and 0.15 mg/kg) in emergency department patients with moderate to severe acute pain. Annals of Emergency Medicine. 2007;49(4):445–453.
Blackburn, D., Somerville, Squire, J. Methadone: An alternative conversion regime. Eur J Palliat Care. 2002;9(3):92–96.
Blair, J.M., Hill, D.A., Fee, J.P.H. Patient-controlled analgesia for labour using remifentanil: A feasibility study. British Journal of Anaesthesia. 2001;87(3):415–420.
Blaylock, V., Brinkman, M., Carver, S., et al. Comparison of finger and forehead oximetry sensors in postanesthesia care patients. Journal of Perianesthesia Nursing. 2008;23(6):379–386.
Blick, S.K., Wagstaff, A.J. Fentanyl buccal tablet: In breakthrough pain in opioid-tolerant patients with cancer. Drugs. 2006;66(18):2387–2393.
Blum, D., Breithaupt, I., Hackett, S., et al. The safety of BEMA (BioErodible MucoAdhesive) fentanyl for breakthrough pain (BTP) in cancer patients. Journal of Clinical Oncology. 26(May 20 Suppl.), 2008. [abstract 20486].
Blum, D., Finn, A. Lack of adverse events affecting the mouth in three clinical trials of BEMA (BioErodible MucoAdhesive) fentanyl. The Journal of Pain. 2008;9(4, Suppl. 1):P24.
Blumenthal, S., Min, K., Marquardt, M., et al. Postoperative intravenous morphine consumption, pain scores, and side effects with perioperative oral controlled-release oxycodone after lumbar discectomy. Anesthesia and Analgesia. 2007;105(1):233–237.
Blumstein, H.A., Moore, D. Visual analog pain scores do not define desire for analgesia in paitents with acute pain. Academic Emergency Medicine. 2003;10(3):211–214.
Boitquin, L., Hecq, J.D., Evrard, J.M., et al. Long-term stability of sufentanil citrate with levobupivacaine hydrochloride in 0.9% sodium chloride infusion pvc bags at 4° C. Journal of Pain and Symptom Management. 2004;28(1):4–6.
Booth, J.V., Lindsay, D.R., Olufolabi, A.J., et al. Subarachnoid meperidine (pethidine) causes significant nausea and vomiting during labor. Anesthesiology. 2000;93(2):418–421.
Borgbjerg, F.M., Nielsen, K., Franks, J. Experimental pain stimulates respiration and attenuates morphine-induced respiratory depression: A controlled study in human volunteers. Pain. 1996;64(1):123–128.
Borgeat, A., Ekatodramis, G., Schenker, C.A. Postoperative nausea and vomiting in regional anesthesia. Anesthesiology. 2003;98(2):530–547.
Borgeat, A., Wilder-Smith, O., Saiah, M., et al. Subhypnotic doses of propofol relieves pruritus induced by epidural and intrathecal morphine. Anesthesiology. 1992;76(4):510–512.
Borland, M.L., Bergesio, R., Pascoe, E.M., et al. Intranasal fentanyl is an equivalent analgesic to oral morphine in paediatric burns patients for dressing changes: A randomised double blind crossover study. Burns: Journal of the International Society for Burn Injuries. 2005;31(7):831–837.
Bostrom, E., Hammarlund-Udenaes, M., Simonsson, U.S. Blood-brain barrier transport helps to explain discrepancies in in vivo potency between oxycodone and morphine. Anesthesiology. 2008;108(3):495–505.
Bounes, V., Ducasse, J.L., Bona, A.M., et al. Nebulized morphine for analgesia in an emergency setting. Journal of Opioid Management. 2009;5(1):23–26.
Bourdeanu, L., Loseth, D.B., Funk, M. Management of opioid-induced sedation in patients with cancer. Clinical Journal of Oncology Nursing. 2005;9(6):705–711.
Bowdle, T.A., Camporesi, E.M., Maysick, L., et al. A multi-center evaluation of remifentanil for early postoperative analgesia. Anesthesia and Analgesia. 1996;83(6):1292–1297.
Bracco, D., Hemmerling, T.M. Thoracic epidural analgesia in cardiac surgery: Impact on postoperative morbidity. Techniques Reg Anesth Pain Manage. 2008;12(1):32–40.
Bradshaw, A., Price, L. Rectal suppository insertion: The reliability of the evidence as a basis for nursing practice. Journal of Clinical Nursing. 2007;16(1):98–103.
Brandman, J.F. Cancer patients, opioids, and driving. Journal of Supportive Oncology. 2005;3(4):317–320.
Brandsborg, B., Dueholm, M., Nikolajsen, L., et al. A prospective study of risk factors for pain persisting 4 months after hysterectomy. The Clinical Journal of Pain. 2009;25(4):263–268.
Breitbart, W., Chandler, S., Eagel, B., et al. An alternative algorithm for dosing transdermal fentanyl for cancer-related pain. Oncology. 2000;14(5):695–705. [See discussion in same issue, pages 705, 709–710, 712, 717].
Brennan, M.J. Summary of short-term and long-term oxymorphone efficacy (pain) studies in low back pain, cancer pain, osteoarthritis, and neuropathic pain. Pain Medicine (Malden, Mass.). 2009;10(1 Suppl.):S11–S19.
Bridges, D., Thompson, S.W.N., Rice, A.S.C. Mechanisms of neuropathic pain. British Journal of Anaesthesia. 2001;87(1):12–26.
Brimacombe, J., Archdeacon, J., Newell, S., et al. Two cases of naloxone-induced pulmonary oedema: The possible use of phentolamine in management. Anesthesia Intens Care. 1991;19(4):578–580.
Brodner, G., Van Aken, H., Hertle, L., et al. Multimodal perioperative management—combining thoracic epidural analgesia, forced mobilization, and oral nutrition—reduces hormonal and metabolic stress and improves convalescence after major urologic surgery. Anesthesia and Analgesia. 2001;92(6):1595–1600.
Brody, H., Campbell, M.L., Faber-Langendoen, K., et al. Withdrawing intensive life-sustaining treatment: Recommendations for compassionate clinical management. (Sounding Board). The New England Journal of Medicine. 1997;336(9):652–657.
Bromley, L. Pre-emptive analgesia and protective premedication. What is the difference? Biomedicine & Pharmacotherapy. 2006;60(7):336–340.
Brooks, K., Pasero, C., Hubbard, L., et al. The risk of infection associated with epidural analgesia. Infection Contol and Hospital Epidemiology. 1995;16(12):725–726.
Brown, D.L., Spinal, epidural, and caudal anesthesia. Miller, R.D., eds. Miller’s anesthesia, 6th ed., vol. 2. Philadelphia: Elsevier, 2005;1653–1683.
Brown, D.R., Hofer, R.E., Patterson, D.E., et al. Intrathecal anesthesia and recovery from radical prostatectomy. Anesthesiology. 2004;100(4):926–934.
Brownridge, P., Cohen, S.E., Ward, M.E. Neural blockade for obstetrics and gynecologic surgery. In: Cousins M.J., Bridenbaugh P.O., eds. Neural blockade in clinical anesthesia and management of pain. 3rd ed. Philadelphia: Lippincott-Raven; 1998:557–604.
Bruce, J., Drury, N., Poobalan, A.S., et al. The prevalence of chronic chest and leg pain following cardiac surgery: A historical cohort study. Pain. 2003;104(1–2):265–273.
Bruce, R.D., Altice, F.L., Gourevitch, M.N., et al. Pharmacokinetic drug interactions between opioid agonist therapy and antiretroviral medications: Implications and management for clinical practice. Journal of Acquired Immune Deficiency Syndromes. 2006;41(5):563–572.
Bruera, E., Brennels, C., Michaud, M., et al. Continuous SC infusion of narcotics using a portable disposable device in patients with advanced cancer. Cancer Treatment Rep. 1987;71(6):635–637.
Bruera, E., Currow, D. Strategies for the palliation of dyspnea in cancer. HIV/AIDS Cancer Pain Release. 2009;22(1–2):1–5.
Bruera, E., Macmillan, K., Hanson, J., et al. The cognitive effects of the administration of narcotic analgesics in patients with cancer pain. Pain. 1989;39(1):13–16.
Bruera, E., Palmer, J.L., Bosnjak, S., et al. Methadone versus morphine as a first-line strong opioid for cancer pain: A randomized, double-blind study. Journal of Clinical Oncology. 2004;22(1):185–192.
Bruera, E., Sweeney, C. Methadone use in cancer patients with pain: A review. Journal of Palliative Medicine. 2002;5(1):127–138.
Buck, M.L., Naloxone for reversal of opioid adverse effects. Pediatric Pharmacology (New York, N. Y.), 2002;8(8):5–10. http://www.medscape.com/viewarticle/441915. [Accessed February 8, 2007].
Buggy, D.J., Doherty, W.L., Hart, E.M., et al. Postoperative wound oxygen tension with epidural or intravenous analgesia. Anesthesiology. 2002;97(4):952–958.
Buntin-Mushock, C., Phillip, L., Moriyana, K., et al. Age-dependent opioid escalation in chronic pain patients. Anesthesia and Analgesia. 2005;100(6):1740–1745.
Burlacu, C.L., Buggy, D.L. Update on local anesthetics: Focus on levobupivacaine. Therap Clin Risk Manage. 2008;4(2):381–392.
Burnham, R., McNeil, S., Hegedus, C., et al. Fibrous myopathy as a complication of repeated intramuscular injection for chronic headache. Pain Research and Management. 2006;11(4):249–252.
Burns, J.W., Hodsman, N.B.A., McLintock, T.T.C., et al. The influence of patient characteristics on the requirements for postoperative analgesia. Anaesthesia. 1989;44(1):2–6.
Burns, S.M., Cowan, C.M., Barclay, P.M., et al. Intrapartum epidural catheter migration: A comparative study of three dressing applications. British Journal of Anaesthesia. 2001;86(4):565–567.
Burton, A.W., Driver, L.C., Mendoza, T.R., et al. Oral transmucosal fentanyl citrate in the outpatient management of severe cancer pain crises: A retrospective case series. The Clinical Journal of Pain. 2004;20(3):195–197.
Busch, C.A., Shore, B.J., Bhandari, R., et al. Efficacy of periarticular multimodal drug injection in total knee Arthroplasty. Journal of Bone and Joint Surgery. 2006;88a(5):959–963.
Bussink, M., Gramke, H.F., van Kleef, M., et al. Bacterial meningitis ten days after spinal anesthesia. (Letter). Regional Anesthesia and Pain Medicine. 2005;30(2):210–211.
Butterworth, J., Douglas-Akinwande, A. Lower extremity paralysis after thoracotomy or thoracic epidural: Image first, ask questions later. Anesthesia and Analgesia. 2007;104(1):201–203.
Buxton, I.L.O. Pharmacokinetics and pharmacodynamics. The dynamics of drug absorption, distribution, action, and elimination. In: Brunton L.L., Lazo J.S., Parker K.L., eds. Goodman, Gilman’s the pharmacological basis of therapeutics. 11th ed. New York: McGraw-Hill; 2006:1–39.
Buyse, I., Stockman, W., Columb, M., et al. Effect of sufentanil on minimum local analgesic concentrations of epidural bupivacaine, ropivacaine, and levobupivacaine in nullipara in early labour. International Journal of Obstetric Anesthesia. 2007;16(1):22–28.
Cai, Q., Huang, H., Sun, X., et al. Efficacy and safety of transdermal fentanyl for treatment of oral mucositis pain caused by chemotherapy. Expert Opinion on Pharmacotherapy. 2008;9(18):3137–3144.
Calderon, E., Pernia, A., De Antonio, P., et al. A comparison of two constant-dose continuous infusions of remifentanil for severe postoperative pain. Anesthesia and Analgesia. 2001;92(3):715–719.
Caldwell, J.R., Rapoport, R.J., Davis, J.C., et al. Efficacy and safety of a once-daily morphine formulation in chronic, moderate-to-severe osteoarthritis pain: Results from a randomized, placebo-controlled, double-blind trial and an open-label extension trial. Journal of Pain and Symptom Management. 2002;23(4):278–291.
Cameron, C.M., Scott, D.A., McDonald, W., et al. A review of neuraxial epidural morbidity. Anesthesiology. 2007;106(5):997–1002.
Candido, K.D., Franco, C.D., Khan, M.A., et al. Buprenorphine added to local anesthetic for brachial plexus block to provide postoperative analgesia in outpatients. Regional Anesthesia and Pain Medicine. 2001;26(4):352–356.
Candido, K.D., Winnie, A.P., Ghaleb, A.H., et al. Buprenorphine added to the local anesthetic for axillary brachial plexus block prolongs postoperative analgesia. Regional Anesthesia and Pain Medicine. 2002;27(2):162–167.
Candiotti, K.A., Kovac, A.L., Melson, T.I., et al. A randomized, double-blind study to evaluate the efficacy and safety of three different doses of palonosetron versus placebo for preventing postoperative nausea and vomiting. Anesthesia and Analgesia. 2008;107(2):445–451.
Caraceni, A., Martini, C., Zecca, E., et al. Working Group of an IASP Task Force on Cancer Pain. Breakthrough pain characteristics and syndromes in patients with cancer pain. An international survey. Palliative Medicine. 2004;18(3):177–183.
Carli, F., Mayo, N., Klubien, K., et al. Epidural analgesia enhances functional exercise capacity and health-related quality of life after colonic surgery. Anesthesiology. 2002;97(3):540–549.
Carli, F., Trudel, J.L., Belliveau, P. The effect of intraoperative thoracic epidural anesthesia and postoperative analgesia on bowel function after colorectal surgery. Diseases of the Colon and Rectum. 2005;44(8):1083–1089.
Carlisle, J., Stevenson, C.A. Drugs for preventing postoperative nausea and vomiting. Cochrane Database of Systematic Reviews (Online). (3):2006. [CD004125].
Carr, D.B., Goudas, L.C. The Brietbart, et al article reviewed. Oncology. 2000;14(5):712. [717].
Carroll, I.R., Angst, M.S., Clark, J.F. Management of perioperative pain in patients chronically consuming opioids. Regional Anesthesia and Pain Med. 2004;29(6):576–591.
Carvalho, B., Riley, E., Cohen, S.E., et al. Single-dose, sustained-release epidural morphine in the management of postoperative pain after elective cesarean delivery: Results of a multicenter randomized controlled study. Anesthesia and Analgesia. 2005;100(4):1150–1158.
Casarett, D.J., Inouye, S.K. Diagnosis and management of delirium near the end of life. Annals of Internal Medicine. 2001;135(1):32–40.
Cashman, J. Patient-controlled analgesia. In: Shorten G., Carr D.B., Harmon D., Puig M.M., Browne J., eds. Postoperative pain management: An evidence-based guide to practice. Philadelphia: Saunders; 2006:148–153.
Cashman, J. Routes of administration. In: Macintyre P.E., Walker S.M., Rowbotham D.J., eds. Acute pain. 2nd ed. London, UK: Hodder Arnold; 2008:201–216.
Cashman, J.N., Dolin, S.J. Respiratory and haemodynamic effects of acute postoperative pain management: Evidence from published data. British Journal of Anaesthesia. 2004;93(2):212–223.
Cassinelli, E.H., Dean, C.L., Garcia, R.M., et al. Ketorolac use for postoperative pain management following lumbar decompression surgery: A prospective, randomized, double-blinded, placebo-controlled trial. Spine. 2008;33(12):1313–1317.
Castillo, R.C., MacKenzie, E.J., Wegener, S.T., et al. Prevalence of chronic pain seven years following limb threatening lower extremity trauma. Pain. 2006;124(3):321–329.
Cata, J.P., Noguera, E.M., Parke, E., et al. Patient-controlled epidural analgesia (PCEA) for postoperative pain control after lumbar spine surgery. Journal of Neurosurgical Anesthesiology. 2008;20(4):256–260.
Centeno, C., Vara, F. Intermittent subcutaneous methadone administration in the management of cancer pain. Journal of Pain & Palliative Care Pharmacotherapy. 2005;19(2):7–12.
Center for Drug Evaluation and Research (CDER) Drug Information: Subutex (buprenorphine hydrochloride) and Suboxone tablets (buprenorphine hydrochloride and naloxone hydrochloride), 2002. Available at http://www.fda.gov/cder/drug/infopage/subutex_suboxone/default.htm [Accessed Feb 29, 2008].
Cepeda, M.S., Camargo, F., Zea, C., et al. Tramadol for osteoarthritis. Cochrane Database of Systematic Reviews (Online). (3):2006. [CD005522].
Cepeda, M.S., Camargo, F., Zea, C., et al. Tramadol for osteoarthritis: A systematic review and metaanalysis. The Journal of Rheumatology. 2007;34(3):543–555.
Cephalon Actiq prescribing information. Frazer, PA: Cephalon Inc; 2007 Available at http://www.actiq.com/pdf/actiq_package_insert_4_5_07.pdf [Accessed April 13, 2008].
Cephalon Fentora prescribing information. Frazer, PA: Cephalon Inc; 2008 Available at http://www.fda.gov/cder/foi/label/2008/021947s006lbl.pdf [Accessed April 13, 2008].
Chabbouh, T., Lentschener, C., Zuber, M., et al. Persistent cauda equine syndrome with no identifiable facilitating condition after uneventful single spinal administration of 0.5% hyperbaric bupivacaine. Anesthesia and Analgesia. 2005;101(6):1847–1848.
Chamberlin, B.H., Cross, K., Winston, J.L., et al. Methylnaltrexone treatment of opioid-induced constipation in patients with advanced illness. Journal of Pain and Symptom Management. 2009;38(5):683–690.
Chamberlin, K.W., Cottle, M., Neville, R., et al. Oral oxymorphone for pain management. The Annals of Pharmacotherapy. 2007;41(7):1144–1152.
Chan, J.D., Treece, P.D., Engelberg, R.A., et al. Narcotic and benzodiazepine use after withdrawal of life support. Chest. 2004;126(1):286–293.
Chandler, S. Nebulized opioids to treat dyspnea. The American Journal of Hospice & Palliative Care. 1999;16(1):418–422.
Chaney, M.A., Furry, P.A., Fluder, E.M., et al. Intrathecal morphine for coronary artery bypass grafting and early extubation. Anesthesia and Analgesia. 1997;84(2):241–248.
Chang, A., Emmel, D.W., Rossi, G.C., et al. Methadone analgesia in morphine-insensitive CXBK mice. European Journal of Pharmacology. 1998;351(2):189–191.
Chang, A.K., Bijur, P.E., Campbell, C.M., et al. Safety and efficacy of rapid titration using 1- mg doses of intravenous hydromorphone in emergency department patients with acute severe pain: The “1 +1” protocol. Annals of Emergency Medicine. 2009;54(2):221–225.
Chang, A.K., Bijur, P.E., Davitt, M., et al, Randomized clinical trial comparing a patient-driven titration protocol of intravenous hydromorphone with traditional physician-driven management of emergency department patients with acute severe pain. Annals of Emergency Medicine, 2009;4:561.e2. [567.e2].
Chang, A.K., Bijur, P.E., Meyer, R.H., et al. Safety and efficacy of hydromorphone as an analgesic alternative to morphine in acute pain: A randomized clinical trial. Annals of Emergency Medicine. 2006;48(2):164–172.
Chang, A.K., Bijur, P.E., Napolitano, A., et al. Two milligrams IV hydromorphone is efficacious for treating pain but is associated with oxygen desaturation. Journal of Opioid Management. 2009;5(2):75–80.
Chang, K.Y., Dai, C.Y., Ger, L.P., et al. Determinants of patient-controlled epidural analgesia requirements. A prospective analysis of 1753 patients. The Clinical Journal of Pain. 2006;22(9):751–756.
Chao, J. Retrospective analysis of Kadian (morphine sulfate sustained-release capsules) in patients with chronic, nonmalignant pain. Pain Medicine (Malden, Mass.). 2005;6(3):262–265.
Chapalain-Pargade, S., Laville, I., Paci, A., et al. Microbiological and physicochemical stability of fentanyl and sufentanil solutions for patient-controlled delivery systems. Journal of Pain and Symptom Management. 2006;32(1):90–97.
Chapman, S., Byas-Smith, M.G., Reed, B.A. Effects of intermediate- and long-term use of opioids on cognition in patients with chronic pain. The Clinical Journal of Pain. 2002;18:S83–S90.
Charlton, S.T., Davis, S.S., Illum, L. Evaluation of bioadhesive polymers as delivery systems for nose to brain delivery: In vitro characterisation studies. Journal of Controlled Release. 2007;118(2):225–234.
Charoenkwan, K., Phillipson, G., Vutyavanich, T. Early versus delayed oral fluids and food for reducing complications after major abdominal gynaecologic surgery. Cochrane Database of Systematic Reviews (Online). (4):2007. [CD004508].
Charuluxananan, S., Kyokong, O., Somboonviboon, W., et al. Nalbuphine versus ondansetron for prevention of intrathecal morphine-induced pruritus after cesarean delivery. Anesthesia and Analgesia. 2003;96(6):1789–1793.
Charuluxananan, S., Somboonviboon, W., Kyokong, O., et al. Ondansetron for treatment of intrathecal morphine-induced pruritus after cesarean delivery. Regional Anesthesia and Pain Medicine. 2000;25(5):535–539.
Chelly, J.E., Greger, J., Gebhard, R., et al. Continuous femoral nerve blocks improve recovery and outcome of patients undergoing total knee arthroplasty. The Journal of Arthroplasty. 2001;16(4):436–445.
Chen, J., Hillman, K., Bellomo, R., et al. The impact of introducing medical emergency team system on the documentations of vital signs. Resuscitation. 2009;80(1):35–43.
Chen, P.P., Cheam, E.W., Ma, M., et al. Patient-controlled pethidine after major upper abdominal surgery: Comparison of the epidural and intravenous routes. Anaesthesia. 2001;56(1):1090–1115.
Chen, X., Qian, X., Fu, F., et al. Intrathecal sufentanil decreases the median effective dose (ED50) of intrathecal hyperbaric ropivacaine for caesarean delivery. Acta Anesthesiologica Scandinavica. 2009. [10.1111/j.1399-6576.2009.02051.x].
Cheng, D.C.H., Newman, M.F., Duke, P., et al. The efficacy and resource utilization of remifentanil and fentanyl in fast-track coronary artery bypass graft surgery: A prospective randomized, double-blinded controlled, multi-center trial. Anesthesia and Analgesia. 2001;92(5):1094–1102.
Cherny, N., Ripamonti, C., Pereira, J., et al. Strategies to manage the adverse effects of oral morphine: An evidence-based report. Journal of Clinical Oncology. 2001;19(9):2542–2554.
Cherrier, M.M., Amory, J.K., Ersek, M., et al. Comparative cognitive and subjective side effects of immediate-release oxycodone in healthy middle-aged and older adults. The Journal of Pain. 2009;10(10):1038–1050.
Cheville, A., Chen, A., Oster, G., et al. A randomized trial of controlled-release oxycodone during inpatient rehabilitation following unilateral total knee arthroplasty. Journal of Bone and Joint Surgery. 2001;83A(4):572–576.
Chia, Y.Y., Kuo, M.C., Liu, K., et al. Does postoperative pain induce emesis? The Clinical Journal of Pain. 2002;18(5):317–323.
Chia, Y.Y., Wei, R.J., Chang, H.C., et al. Optimal duration of urinary catheterization after thoractomy in patients under postoperative patient-controlled epidural analgesia. Acta Anaesthesiologica Taiwan. 2009;47(4):173–179.
Choi, P., Bhandari, M., Scott, J., et al. Epidural analgesia for pain relief following hip or knee replacement. Cochrane Database of Systematic Reviews (Online). (3):2003. [CD003071].
Choi, S.H., Koo, B.N., Nam, S.H., et al. Comparison of remifentanil and fentanyl for postoperative pain control after abdominal hysterectomy. Yonsei Medical Journal. 2008;49(2):204–210.
Chou, R., Fanciullo, G.J., Fine, P., et al. Opioid treatment guidelines: Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. The Journal of Pain. 2009;10(2):113–130.
Chou, W.Y., Wang, C.H., Liu, C.C., et al. Human opioid receptor A118G polymorphism affects intravenous patient-controlled analgesia morphine consumption after total abdominal hysterectomy. Anesthesiology. 2006;105(2):334–337.
Christensen, K.S., Cohen, A.E., Mermelstein, F.H., et al. The analgesic efficacy and safety of a novel intranasal morphine formulation (morphine plus chitosan), immediate release oral morphine, intravenous morphine, and placebo in a postsurgical dental pain model. Anesthesia and Analgesia. 2008;107(6):2018–2024.
Christie, I.W., McCabe, S. Major complications of epidural analgesia after surgery: Results of a six-year survey. Anaesthesia. 2007;62(4):334–341.
Chu, C.C., Shieh, J.P., Tzeng, J.I., et al. The prophylactic effect of haloperidol plus dexamethasone on postoperative nausea and vomiting in patients undergoing laparoscopically assisted vaginal hysterectomy. Anesthesia and Analgesia. 2008;106(5):1402–1406.
Chu, L.F., Angst, M.S., Clark, D. Opioid-induced hperalgesia in humans: Molecular mechanisms and clinical considerations. The Clinical Journal of Pain. 2008;24(6):479–496.
Chu, L.F., Clark, K.J., Angst, M.S. Opioid tolerance and hyperalgesia in chronic pain patients after one month of oral morphine therapy: A preliminary prospective study. The Journal of Pain. 2006;7:43–48.
Classen, A.M., Wimbish, G.H., Kupiec, T.C. Stability of admixture containing morphine sulfate, bupivacaine hydrochloride, and clonidine hydrochloride in an implantable infusion system. Journal of Pain and Symptom Management. 2004;28(6):603–611.
Claxton, A.R., McGuire, G., Chung, F., et al. Evaluation of morphine versus fentanyl for postoperative analgesia after ambulatory surgical procedures. Anesthesia and Analgesia. 1997;84(3):509–514.
Clemens, K.E., Klaschik, E. Morphine in the management of dyspnoea in ALS. A pilot study. European Journal of Neurology. 2008;15(5):445–450.
Clemens, K.E., Klaschik, E. Effect of hydromorphone on ventilation in palliative care patients with dyspnea. Supportive Care in Cancer. 2008;16(1):93–99.
Clemens, K.E., Quednau, I., Klaschik, E. Is there a higher risk of respiratory depression in opioid-naïve palliative care patients during symptomatic therapy of dyspnea with strong opioids? Journal of Palliative Medicine. 2008;11(2):204–216.
Clemens, K.E., Quednau, I., Klaschik, E. Use of oxygen and opioids in the palliation of dyspnoea in hypoxic and non-hypoxic palliative care patients: A prospective study. Supportive Care in Cancer. 2009;17(4):367–377.
Coda, B.A. Opioids. In Barash P.G., Cullen B.F., Stoelting R.K., eds.: Clinical anesthesia, 5th ed., Philadelphia: Lippincott, Williams, Wilkins, 2006.
Coddings, C., Levinsky, D., Hale, M., et al. Analgesic efficacy and safety of controlled-release hydrocodone and acetaminophen tablets, dosed twice daily for moderate-to-severe mechanical chronic low back pain: A randomized, double-blind, placebo-controlled withdrawal trial, 2008. [Paper presented at American Pain Society Annual Meeting, Tampa, Florida, May 8–10].
Coelho, J.C.U., Runkel, N., Herfarth, C., et al. Effect of analgesic drugs on electromyographic activity of the gastrointestinal tract and sphincter of Oddi and on biliary pressure. Annals of Surgery. 1986;204(1):53–58.
Cohen, M.R., Smetzer, J. Patient-controlled analgesia safety issues. Journal of Pain & Palliative Care Pharmacotherapy. 2005;19(1):45–50.
Cohen, R.S. Fentanyl transdermal analgesia during pregnancy and lactation. Journal of Human Lactation. 2009;25(3):359–361.
Collado, F., Torres, L.M. Association of transdermal fentanyl and oral transmucosal fentanyl citrate in the treatment of opioid naïve patients with severe chronic noncancer pain. Journal of Opioid Management. 2008;4(2):111–115.
Coloma, M., White, P.F., Markowitz, S.D., et al. Dexamethasone in combination with dolasetron for prophylaxis in the ambulatory setting. Anesthesiology. 2002;96(6):1346–1350.
Coloma, M., White, P.F., Ogunnaike, B.O., et al. Comparison of acustimulation and ondansetron for the treatment of established postoperative nausea and vomiting. Anesthesiology. 2002;97(6):1387–1392.
Coluzzi, P.H., Schwartzberg, L., Conroy, J.D., et al. Breakthrough cancer pain: A randomized trial comparing oral transmucosal fentanyl citrate (OTFC) and morphine sulfate immediate release (MSIR). Pain. 2001;91(1–2):123–130.
Committee on the Safety of Medicines of the UK. Overdose risk prompts UK withdrawal of propoxyphene combination. Journal of Pain & Palliative Care Pharmacotherapy. 2006;20(4):49–50.
Compton, P. Substance abuse. In: McCaffery M., Pasero C., eds. Pain: Clinical manual. 2nd ed. St. Louis: Mosby; 1999:429–466.
Compton, P., The OIH paradox: Can opioids make pain worse? Pain Treatment Topics 2008. Available at http://pain- topics.org/pdf/Compton-OIH-Paradox.pdf [Accessed Feb. 16, 2009].
Connelly, N.R., Parker, R.K., Rahimi, A., et al. Sumatriptan in patients with postdural puncture headache. Headache. 2000;40(4):316–319.
Connor, S.R., Horn, S.D., Smout, R.J., et al. The National Hospice Outcomes Project (NHOP): Development and implementation of a multi-site hospice outcomes study. Journal of Pain and Symptom Management. 2005;29(3):286–296.
Cook, D.J., Rooke, G.A. Priorities in perioperative geriatrics. Anesthesia and Analgesia. 2003;96(6):1823–1836.
Correll, D.J., Viscusi, E.R., Grunwald, Z., et al. Epidural analgesia compared with intravenous morphine patient-controlled analgesia: Postoperative outcome measures after mastectomy with immediate TRAM flap breast reconstruction. Regional Anesthesia and Pain Medicine. 2001;26(5):444–449.
Cortinez, L.I., Munoz, H.R., De al Fuente, R., et al. Target-controlled infusión of remifentanil or fentanyl Turing extra-corporeal shock-wave lithotripsy. European Journal of Anaesthsiology. 2005;22(1):56–61.
Cousins, M.J. Advances in the long-term management of chronic pain: Recent evidence with OROS hydromorphone, a novel, once-daily, long-acting opioid analgesic. Journal of Pain and Symptom Management. 2007;33(Suppl. 2):S1–S3.
Cousins, M.J., Umedaly, H.S. Postoperative pain management in the neurosurgical patient. International Anesthesiology Clinics. 1996;34(4):179–193.
Cousins, M.J., Veering, B.T. Epidural neural blockade. In: Cousins M.J., Bridenbaugh P.O., eds. Neural blockade in clinical anesthesia and management of pain. Philadelphia: Lippincott-Raven Publishers; 1998:243–321.
Covino, B.G., Wildsmith, J.A.W. Clinical pharmacology of local anesthetic agents. In: Cousins M.J., Bridenbaugh P.O., eds. Neural blockade in clinical anesthesia and management of pain. Philadelphia: Lippincott; 1998:97–128.
Coyle, N. Cancer patients and subcutaneous infusions. The American Journal of Nursing. 1996;96(3):61.
Coyle, N., Adelhardt, J., Foley, K.M., et al. Character of terminal illness in the advanced cancer patient: Pain and other symptoms during the last four weeks of life. Journal of Pain and Symptom Management. 1990;5(2):83–93.
Coyle, N., Cherny, N., Portenoy, R.K. Pharmacologic management of cancer pain. In: McGuire D., Yarbro C.H., Ferrell B.R., eds. Cancer pain management. 2nd ed. Boston: Jones, Bartlett Publishers; 1995:89–130.
Coyle, N., Mauskop, A., Maggard, J., et al. Continuous subcutaneous infusions of opiates in cancer patients with pain. Oncology Nursing Forum. 1986;13(4):53–57.
Coyle, N., Portenoy, R.K. Pharmacologic management of cancer pain. In Cancer Nursing, 2nd ed., Philadelphia: WB Saunders; 1996:1035–1055.
Coyne, P.J., Paice, J.A., Ferrell, B.R., et al. Oncology End-of-Life Nursing Education Consortium training program: Improving palliative care in cancer. Oncology Nursing Forum. 2007;34(4):801–807.
Coyne, P.J., Viswanathan, R., Smith, T.J. Nebulized fentanyl citrate improves patients’ perception of breathing, respiratory rate, and oxygen saturation in dyspnea. Journal of Pain and Symptom Management. 2002;23(2):157–160.
Cretikos, M.A., Bellomo, R., Hillman, K., et al. Respiratory rate: The neglected vital sign. MJA. 2008;188(11):657–659.
Cruciani, R.A. Methadone: To ECG or not to ECG…That is still the question. Journal of Pain and Symptom Management. 2008;36(5):545–552.
Currow, D.C., Plummer, J.L., Cooney, N.J., et al. A randomized, double-blind, multi-site, crossover, placebo-controlled equivalence study of morning versus evening once-daily sustained-release morphine sulfate in people with pain from advanced cancer. Journal of Pain and Symptom Management. 2007;34(1):17–23.
Curry, C.E., Butler, D.M. Constipation. In Berardi R.R., Kroon A.L., McDermott J.H., et al, eds.: Handbook of nonprescription drugs. An interactive approach to self care, ed 15, Washington DC: American Pharmacists Association, 2006.
Cywinski, J.B., Parker, B.M., Xu, M., et al. A comparison of postoperative pain control in patients after right lobe donor hepatectomy and major hepatic resection for tumor. Anesthesia and Analgesia. 2004;99(6):1747–1752.
Czarnecki, M.L., Ferrise, A.S., Jastrowski Mano, K.E., et al. Parent/nurse-controlled analgesia for children with developmental delay. The Clinical Journal of Pain. 2008;24(9):817–824.
Dabu-Bondoc, S., Franco, S.A., Sinatra, R.S. Neuraxial analgesia with hydromorphone, morphine, and fentanyl: Dosing and safety guidelines. In: Sinatra R.S., de Leon-Casasola O.A., Ginsberg B., Viscusi E.R., eds. Acute pain management. Cambridge, New York: Cambridge University Press; 2009:230–244.
Daeninck, P.J., Bruera, E. Reduction in constipation and laxative requirements following opioid rotation to methadone: A report of four cases. Journal of Pain and Symptom Management. 1999;18(4):303–309.
Dahaba, A.A., Grabner, T., Rehak, P.H., et al. Remifentanil versus morphine analgesia and sedation for mechanically ventilated critically ill patients. Anesthesiology. 2004;101(3):640–646.
Dahan, A., Aarts, L., Smith, T.W. Incidence, reversal, and prevention of opioid-induced respiratory depression. Anesthesiology. 2010;112(1):226–238.
Dahan, A., van Dorp, E., Smith, T., et al. Morphine-6-glucuronide (M6G) for postoperative pain relief. European Journal of Pain (London, England). 2008;12(4):403–411.
Dahan, A., Yassen, A., Bijl, H., et al. Comparison of the respiratory effects of intravenous buprenorphine and fentanyl in humans and rats. British Journal of Anaesthesia. 2005;94(6):325–334.
Dahan, A., Yassen, A., Romberg, R., et al. Buprenorphine induces ceiling in respiratory depression but no in analgesia. British Journal of Anaesthesia. 2006;96(5):627–632.
Dahl, J.B., Moiniche, S. Pre-emptive analgesia. British Medical Bulletin. 2004;71(1):13–27.
Dahmani, S., Dupont, H., Mantz, J., et al. Predictive factors of early morphine requirements in the post-anaesthesia care unit (PACU). British Journal of Anaesthesia. 2001;87(3):385–389.
Dal, D., Canbak, M., Cagler, M., et al. A background infusion of morphine does not enhance postoperative analgesia after cardiac surgery. Canadian Journal of Anesthesia. 2003;50(3):476–479.
Dale, O., Hjortkjær, R., Kharasch, E.D. Nasal administration of opioids for pain management in adults. Acta Anaesthesiologica Scandinavica. 2002;46(7):759–770.
Dale, O., Hoffer, C., Sheffels, P., et al. Disposition of nasal, intravenous, and oral methadone in healthy volunteers. Clinical Pharmacology and Therapeutics. 2002;72(5):536–545.
Dale, O., Piribauer, M., Kaasa, S., et al. A double-blind, randomized, crossover comparison between single-dose and double-dose immediate-release oral morphine at bedtime in cancer patients. Journal of Pain and Symptom Management. 2009;37(1):68–76.
Dale, O., Sheffels, P., Kharasch, E.D. Bioavailabilities of rectal and oral methadone in healthy subjects. British Journal of Clinical Pharmacology. 2004;58(2):156–162.
Daniels, S., Casson, E., Stegmann, J.U., et al. A randomized, double-blind, placebo-controlled phase 3 study of the relative efficacy and tolerability of tapentadol IR and oxycodone IR for acute pain. Current Medical Research and Opinion. 2009;25(6):1551–1556.
Darwish, M., Kirby, M., Jiang, J.G., et al. Bioequivalence following buccal and sublingual placement of fentanyl buccal tablet 400 microg in healthy subjects. Clinical Drug Investigation. 2008;28(1):1–7.
Darwish, M., Kirby, M., Robertson, P., Jr., et al. Absolute and relative bioavailability of fentanyl buccal tablet and oral transmucosal fentanyl citrate. Journal of Clinical Pharmacology. 2007;47(3):343–350.
Davies, A.N., Vriens, J., Kennett, A., et al. An observational study of oncology patients’ utilization of breakthrough pain medication. Journal of Pain and Symptom Management. 2008;35(4):406–411.
Davis, G.A., Rudy, A.C., Archer, S.M., et al. Bioavailability and pharmacokinetics of intranasal hydromorphone in patients experiencing vasomotor rhinitis. Clinical Drug Investigation. 2004;24(11):633–639.
Davis, G.A., Rudy, A.I.A., Archer, S.M., et al. Bioavailability of intranasal butorphanol administered from a single-dose sprayer. American Journal of Health-System Pharmacy: AJHP. 2005;62(1):48–53.
Davis, J.J., Johnson, K.B., Egan, T.D., et al. Preoperative fentanyl infusion with pharmacokinetic simulation for anesthetic and perioperative management of an opioid-tolerant patient. Anesthesia and Analgesia. 2003;97(6):1661–1662.
Davis, K.M., Esposito, M.A., Meyer, B.A. Oral analgesia compared with intravenous patient-controlled analgesia for pain after cesarean delivery: A randomized controlled trial. American Journal of Obstetrics and Gynecology. 2006;194(4):967–971.
Davis, M.P. Acute pain in advanced cancer: An opioid dosing strategy and illustration. The American Journal of Hospice & Palliative Care. 2004;21(1):47–140.
Davis, M.P. Buprenorphine in cancer pain. Supportive Care in Cancer. 2005;13(11):878–887.
Davis, M.P., Varga, J., Dickerson, D., et al. Normal-release and controlled-release oxycodone: Pharmacokinetics, pharmacodynamics, and controversy. Supportive Care in Cancer. 2003;11(2):84–92.
Davis, M.P., Walsh, D. Methadone for relief of cancer pain: A review of pharmacokinetics, pharmacodynamics, drug interactions and protocols of administration. Supportive Care in Cancer. 2001;9(2):73–83.
Davis, M.P., Walsh, D., LeGrand, S.B., et al. Symptom control in cancer patients: The clinical pharmacology and therapeutic role of suppositories and rectal suspensions. Supportive Care in Cancer. 2002;10(2):117–138.
Dawn, A.G., Yosipovitch, G. Butorphanol for treatment of intractable pruritus. Journal of the American Academy of Dermatology. 2006;54(3):527–531.
Dawson, P., Rosenfeld, J.V., Murphy, M.A., et al. Epidural abscess associated with postoperative epidural analgesia. Anaesthesia and Intensive Care. 1991;19(4):569–572.
Dean, M. Opioids in renal failure and dialysis patients. Journal of Pain and Symptom Management. 2004;28(5):497–504.
De Beer Jde, V., Winemaker, M.J., Donnelly, G.A.E., et al. Efficacy and safety of controlled-release oxycodone and standard therapies for postoperative pain after knee or hip replacement. Canadian Journal of Surgery. 2005;48(4):277–283.
De Cicco, M., Matovic, M., Castellani, G.T., et al. Time-dependent efficacy of bacterial filters and infection risk in long-term epidural catheterization. Anesthesiology. 1995;82(3):765–771.
De Cosmo, G., Congedo, E., Lai, C., et al. Ropivacaine vs. levobupivacaine combined with sufentanil for epidural analgesia after lung surgery. European Journal of Anaesethesiology. 2008;25(12):1020–1025.
Deer, T., Krames, E.S., Hassenbusch, S.J., et al. Polyanalgesic consensus conference: Recommendations for the management of pain by intrathecal (intraspinal) drug delivery; report of an interdisciplinary expert panel. Neuromodulation. 2007;10(4):300–328.
De Kock, M., Lavand’homme, P., Waterloos, H. The short-lasting analgesia and long-term antihyperalgesic effect of intrathecal clonidine in patients undergoing colonic surgery. Anesthesia and Analgesia. 2005;101(2):566–572.
de Leon-Casasola, O.A. Current developments in opioid therapy for management of cancer pain. The Clinical Journal of Pain. 2008;24(4):S3–S7.
Delvecchio, L., Bettinelli, S., Klersy, C., et al. Comparing the efficacy and safety of continuous epidural analgesia in abdominal and urological surgery between two opioids with different kinetic properties: Morphine and sufentanyl. Minerva Anestesiologica. 2008;74(3):69–76.
Demeure, M.J., Fain, M.J. The elderly surgical patient and postoperative delirium. Journal of the American College of Surgeons. 2006;203(5):752–757.
Dempsey, S.J., Davidson, J., Cahill, D., et al. Selection of a sedation assessment scale for clinical practice: Inter-rater reliability, ease of use, and applicability testing of the Richmond-Agitation-Sedation and Pasero Opioid-induced Sedation Scale, 2008. [Poster presentation, National Association of Orthopedic Nurses Congress, Tampa, FL, May 6–10].
De Pinto, M., Dunbar, P.J., Edwards, W.T. Pain management. Anesthesiology Clin N Am. 2006;24(1):19–37.
Dershwitz, M., Landow, L., Joshi-Ryzewicz, W. Anesthesia for bedside procedures. In: Irwin R.S., Rippe J.M., eds. Irwin, Rippe’s intensive care medicine. Philadelphia: Lippincott Williams, Wilkins, 2003.
Devulder, J., Jacobs, A., Richarz, U., et al. Impact of opioid rescue medication for breakthrough pain on the efficacy and tolerability of long-acting opioids in patients with chronic non-malignant pain. British Journal of Anaesthesia. 2009;103(4):576–585.
Dewachter, P., Lefebvre, D., Kalaboka, S., et al. An anaphylactic reaction to transdermal delivered fentanyl. Acta Anaesthesiologica Scandinavica. 2009;53(8):1092–1093.
Dillon, A.E., Wagner, C.L., Wiest, D., et al. Drug therapy in the nursing mother. Obstetrics and Gynecology Clinics of North America. 1997;24(3):675–696.
Dix, P., Sandhar, B., Murdoch, J., et al. Pain on medical wards in a district general hospital. British Journal of Anaesthesia. 2004;92(2):235–237.
D’Onofrio, P., Novelli, A.M.M., Mecacci, F., et al. The efficacy and safety of continuous intravenous administration of remifentanil for birth pain relief: An open study of 205 parturients. Anesthesia and Analgesia. 2009;109(6):1922–1924.
Dole, V., Nyswander, M.E. A medical treatment for diacetylmorphine (heroin) addiction. J Am Med Assoc. 1965;193:646–650.
Dolin, S.J., Cashman, J.N. Tolerability of acute postoperative pain management: Nausea, vomiting, sedation, pruritus, and urinary retention. Evidence from published data. British Journal of Anaesthesia. 2005;95(5):584–591.
Donnelly, S., Davis, M.P., Walsh, D., et al. Morphine in cancer pain management: A practical guide. Supportive Care in Cancer. 2002;10(1):13–35.
Donner, B., Zenz, M., Tryba, M., et al. Direct conversion from oral morphine to transdermal fentanyl: A multicenter study in patients with cancer pain. Pain. 1996;64(3):527–534.
Donshik, P.C., Pearlman, D., Pinnas, J., et al. Efficacy and safety of ketorolac tromethamine 0.5% and levocabastin 0.05%: A multicenter comparison in patients with seasonal allergic conjunctivitis. Advances in Therapy. 2000;17(2):94–102.
Dorr, L.D., Raya, J., Long, W.T., et al. Multimodal analgesia without parenteral narcotics for total knee arthroscopy. The Journal of Arthroplasty. 2008;23(4):502–508.
Dosa, D.M., Dore, D.D., Mor, V., et al. Frequency of long-acting opioid analgesic initiation in opioid-naive nursing home residents. Journal of Pain and Symptom Management. 2009;38(4):515–521.
Doss, N.W., Ipe, J., Crimi, T., et al. Continuous thoracic epidural anesthesia with 0.2% ropivacaine versus general anesthesia for perioperative management of modified radical mastectomy. Anesthesia and Analgesia. 2001;92(6):1552–1557.
Douma, M.R., Verwey, R.A., Kam-Endtz, C.E., et al. Obstetric analgesia: A comparison of patient-controlled meperidine, remifentanil, and fentanyl in labour. British Journal of Anaesthesia. 2010;104(2):209–215.
Doverty, M., White, J.M., Somogyi, A.A., et al. Hyperalgesic responses in methadone maintenance patients. Pain. 2001;90(1–2):91–96.
Downing, G.M., Kuziemsky, C., Lesperance, M., et al. Development and reliability testing of the Victoria Bowel Performance Scale (BPS). Journal of Pain and Symptom Management. 2007;34(5):513–522.
Drug Enforcement Administration Drugs and chemicals of concern, 2008. Available at http://www.deadiversion.usdoj.gov/drugs_concern/tramadol.htm [Accessed June 30, 2009].
Drug Topics Top 200 drugs, 2008. Available at http://drugtopics.modernmedicine.com/drugtopics/data/articlestandard/drugtopics/222009/599844/article.pdf [Accessed 9 June 2008].
Duggleby, W., Lander, J. Cognitive status and postoperative pain: older adults. Journal of Pain and Symptom Management. 1994;9(1):19–27.
Dunbar, P.J., Chapman, C.R., Buckley, F.P., et al. Clinical analgesic equivalence for morphine and hydromorphone with prolonged PCA. Pain. 1996;68(2–3):265–270.
Duncan, A. The use of fentanyl and alfentanil sprays for episodic pain. Palliative Medicine. 2002;16(6):550.
Dunteman, E., Karanikolas, M., Filos, K.S. Transnasal butorphanol for the treatment of opioid-induced pruritus unresponsive to antihistamines. Journal of Pain and Symptom Management. 1996;12(4):255–260.
DuPen, A., Shen, D., Ersek, M. Mechanisms of opioid-induced tolerance and hyperalgesia. Pain Management Nursing. 2007;8(3):113–121.
DuPen, S., DuPen, A., Hillyer, J. Intrathecal hydromorphone for intractable nonmalignant pain: A retrospective study. Pain Medicine (Malden Mass.). 2006;7(1):10–15.
DuPen, S.L., DuPen, A.R. Spinal analgesia. In: Ashburn M.A., Rice L.J., eds. The management of pain. New York: Churchill Livingstone; 1998:171–186.
Dworkin, R.H., Barbano, R.L., Tyring, S.K., et al. A randomized, placebo-controlled trial of oxycodone and of gabapentin for acute pain in herpes zoster. Pain. 2009;142(3):209–217.
Dworkin, R.H., O’Connor, A.B., Backonja, M., et al. Pharmacologic management of neuropathic pain: Evidence-based recommendations. Pain. 2007;132(3):237–251.
Eberhart, L.H., Mauch, M., Morin, A.M., et al. Impact of a multimodal anti-emetic prophylaxis on patient satisfaction in high-risk patients for postoperative nausea and vomting. Anaesthesia. 2002;57(10):1022–1027.
Ebner, N., Rohrmeister, K., Winklbaur, B., et al. Management of neonatal abstinence syndrome in neonates born to opioid maintained women. Drug and Alcohol Dependence. 2007;87(2–3):131–138.
Edmonds, P., Higginson, I., Altmann, D., et al. Is the presence of dyspnea a risk factor for morbidity in cancer patients? Journal of Pain and Symptom Management. 2000;19(1):15–22.
Edwards, J.E., McQuay, H.J., Moore, R.A. Single dose oral dihydrocodeine for acute postoperative pain. Cochrane Database of Systematic Reviews (Online). (4):2004. [D002760].
Edwards, S.M., Murdin, L. Respiratory rate – an under-documented clinical assessment. Clinical Medicine (London, England). 2001;1(1):85.
Egan, T.D., Huizinga, B., Gupta, S.K., et al. Remifentanil pharmcokinetics in obese versus lean patients. Anesthesiology. 1998;89(3):562–573.
Egan, T.D., Kern, S.E., Muir, K.T., et al. Remifentanil by bolus injection: A safety pharmacokinetic, pharmacodynamic, and age effect investigation in human volunteers. British Journal of Anaesthesia. 2004;92(3):335–343.
Egan, T.D., Sharma, A., Ashburn, M.A., et al. Multiple dose pharmacokinetics of oral transmucosal fentanyl citrate in healthy volunteers. Anesthesiology. 2000;92(3):665–673.
Egbert, A.M., Parks, L.H., Short, L.M., et al. Randomized trial postoperative patient-controlled analgesia vs. Intramuscular narcotics in frail elderly men. Archives of Internal Medicine. 1990;150:1897–1903.
Einarson, A., Bozzo, P., Taguchi, N. Use of fentanyl patch throughout pregnancy. (Letter). Journal of Obstet Gynecol Can. 2009;31(1):20.
Eisenberg, E., Berkey, C.S., Carr, D.B., et al. Efficacy and safety of nonsteroidal antiinflammatory drugs for cancer pain: A meta-analysis. Journal of Clinical Oncology. 1994;12(12):2756–2765.
Eisenberg, E., Marinangeli, F., Birkhahn, J., et al. Time to modify the WHO analgesic ladder? Pain. Clinical Updates. IASP. 2005;13(5):1–4.
Eisenberg, E., McNicol, E.D., Carr, D.B. Efficacy of mu-opioid agonists in the treatment of evoked neuropathic pain: Systematic review of randomized controlled trials. European Journal of Pain (London, England). 2006;10(8):667–676.
Eisenkraft, J.B. Forehead pulse oximetry. Friend and foe. (Editorial). Anesthesiology. 2006;105(6):1075–1077.
Elia, N., Culebras, X., Mazza, C., et al. Clonidine as an adjuvant to intrathecal local anesthetics for surgery: Systematic review of randomized trials. Regional Anesthesia and Pain Medicine. 2008;33(2):159–167.
Eliot, L., Geiser, R., Loewen, G. Steady-state pharmacokinetic comparison of a new, once-daily, extended-release morphine formulation (Morphelan) and OxyContin twice daily. Journal of Oncology Pharmacy Practice. 2001;7(1):1–8.
Elliott, P., O’Hare, R., Bill, K.M., et al. Severe cardiovascular depression with remifentanil. Anesthesia and Analgesia. 2000;91(1):58–61.
Ely, E.W., Truman, B., Shintani, A., et al. Monitoring sedation status over time in ICU patients. JAMA: The Journal of the American Medical Association. 2003;289(22):2983–2991.
Endo Opana prescribing information. Chadds Ford, PA: Endo Pharmaceuticals; 2006 Available at http://www.endo.com/pdf/Opana_IR_PI.pdf [Accessed April 17, 2008].
Engoren, M., Luther, G., Fenn-Buderer, N. A comparison of fentanyl, sufentanil, and remifentanil for fast-track cardiac anesthesia. Anesthesia and Analgesia. 2001;93(4):859–864.
Ernst, A.A., Weiss, S.J., Park, S., et al. Prochlorperazine versus promethazine for uncomplicated nausea and vomiting in the emergency department: A randomized, double-blind clinical trial. Annals of Emergency Medicine. 2000;36(2):89–94.
Erstad, B.L., Puntillo, K., Gilbert, H.C., et al. Pain management principles in the critically ill. Chest. 2009;135(4):1075–1086.
Estfan, B., Mahmoud, F., Shaheen, P., et al. Respiratory function during parenteral opioid titration for cancer pain. Palliative Medicine. 2007;21(1):81–86.
Etches, R.C. Respiratory depression associated with patient-controlled analgesia: A review of eight cases. Canadian Journal of Anaesthesia. 1994;41:125–132.
Etches, R.C., Gammer, T.-L., Cornish, R. Patient-controlled epidural analgesia after thoracotomy: A comparison of meperidine with and without bupivacaine. Anesthesia and Analgesia. 1996;83(1):81–86.
Ethuin, F., Boudaoud, S., Leblanc, I., et al. Pharmacokinetics of long-term sufentanil infusion for sedation in ICU patients. Intensive Care Medicine. 2003;29(11):1916–1920.
Etropolski, M., Rauschkolb-Loffler, C., Shapiro, D., et al. A randomized, double-blind, placebo- and active-controlled phase III study of tapentadol ER for chronic low back pain: Analysis of efficacy endpoint sensitivity. (Abstract). The Journal of Pain: Official Journal of the American Pain Society. 2009;10(Suppl. 4):S51.
Evans, T.N., Park, G.R. Remifentanil in the critically ill. Anaesthesia. 1997;52(8):797–811.
Evron, S., Glezerman, M., Sadan, O., et al. Remifentanil: A novel systemic analgesic for labor pain. Anesthesia and Analgesia. 2005;100(1):233–238.
Evron, S., Sessler, D., Sadan, O., et al. Identification of the epidural space: Loss of resistance with air, lidocaine, or the combination of air and lidocaine. Anesthesia and Analgesia. 2004;99(1):245–250.
Ewalenko, P., Janny, S., Dejonckheere, M., et al. Antiemetic effect of subhypnotic doses of propofol after thyroidectomy. British Journal of Anaesthesia. 1996;77(4):463–467.
Ezri, T., Lurie, S., Stein, A., et al. Postoperative nausea and vomiting: Comparison of the effect of postoperative meperidine or morphine in gynecologic surgery patients. Journal of Clinical Anesthesia. 2002;14(4):262–266.
Fairlie, F.M., Marshall, L., Walker, J.J., et al. Intramuscular opioids for maternal pain relief in labor: A randomized controlled trial comparing pethidine with diamorphine. Britsh Journal of Obstetrics and Gynaecology Research. 1999;106(11):1181–1187.
Fajemirokun-Odudeyi, O., Sinha, C., Tutty, S., et al. Pregnancy outcome in women who use opiates. European Journal of Obstetrics Gynecology and Reproductive Biology. 2006;126(2):170–175.
Fakuda, K., Intravenous opioid anesthetics. Miller, R.D., eds. Miller’s anesthesia, 6th ed., vol. 1. Philadelphia: Elsevier, 2005;379–437.
Farragher, R.A., Laffey, J.G. Postoperative pain management after cesarean section. In: Shorten G., Carr D.B., Harmon D., Puig M.M., Browne J., eds. Postoperative pain management: An evidence-based guide to practice. Philadelphia: Saunders; 2006:225–238.
Ferrell, B.R., Griffith, H. Cost issues related to pain management: Report from the cancer pain panel of the Agency for Health Care Policy and Research. Journal of Pain and Symptom Management. 1994;9(4):221–234.
Ferrell, B.R., Virani, R., Paice, J.A., et al. Evaluation of palliative care nursing education seminars. European Journal of Oncology Nursing. 2009. [doi: 10.1016/j.ejon.2009.08.004].
Fick, D.M., Cooper, J.W., Wade, W.E., et al. Updating the Beers criteria for potentially inappropriate medication use in older adults: Results of a US consensus panel of experts. Archives of Internal Medicine. 2003;163(22):2716–2724.
Filitz, J., Ihmsen, H., Gunther, W., et al. Supra-additive effects of tramadol and acetaminophen in a human pain model. Pain. 2008;136(3):262–270.
Fillingim, R.B. Individual differences in pain responses. Current Rheumatology Reports. 2005;7(5):342–347.
Fine, P.G., Mahajan, G., McPherson, M.L. Long-acting opioids and short-acting opioids: Appropriate use in chronic pain management. Pain Medicine (Malden, Mass.). 2009;10(Suppl 2):S79–S88.
Fine, P.G., Portenoy, R.K. A clinical guide to opioid analgesia. New York: Vendome Group, LLC, 2007.
Fine, P.G., Portenoy, R.K., Ad Hoc Expert Panel on Evidence Review and Guidelines for Opioid Rotation. Establishing “Best practices” for opioid rotation: Conclusions of an expert panel. Journal of Pain and Symptom Management. 2009;38(3):418–425.
Finn, J., Wright, J., Fong, J., et al. A randomised crossover trial of patient controlled intranasal fentanyl and oral morphine for procedural wound care in adult patients with burns. Burns: Journal of the International Society for Burn Injuries. 2004;30(3):262–268.
Finnerup, N.B., Otto, M., McQuay, H.J., et al. Algorithm for neuropathic pain treatment: An evidence-based proposal. Pain. 2005;118(3):289–305.
Finucane, B.T., Ganapathy, S., Carli, F., et al. Prolonged epidural infusions of ropivacaine (2 mg/mL) after colonic surgery: The impact of adding fentanyl. Anesthesia and Analgesia. 2001;92(5):1276–1285.
Fishbain, D.A. Oxymorphone status. Pain Medicine (Malden, Mass.). 2009;10(Suppl. 1):S1–S2.
Fishbain, D.A., Cole, B., Lewis, J., et al. What percentage of chronic nonmalignant pain patients exposed to chronic opioid analgesic therapy develop abuse/addiction and/or aberrant drug-related behaviors? A structured evidence-based review. Pain Medicine (Malden, Mass.). 2008;9(4):444–459.
Fishbain, D.A., Cutler, R.B., Rosomoff, H.L., et al. Can patients taking opioids drive safely? A structured evidence-based review. Journal Pain Palliative Care Pharmacotherapy. 2002;16(1):9–28.
Fishbain, D.A., Cutler, R.B., Rosomoff, H.L., et al. Are opioid-dependent/tolerant patients impaired in driving-related skills? A structured evidence-based review. Journal of Pain and Symptom Management. 2003;25(6):559–577.
Fishbain, D.A., Lewis, J.E., Cole, B., et al. Medicolegal rounds: Medicolegal issues and alleged breaches of standards of medical care in a patient motor vehicle accident allegedly related to chronic opioid analgesic therapy. Journal of Opioid Management. 2007;3(1):16–20.
Fisher, K., Stiles, C., Hagen, N.A. Characterization of the early pharmacodynamic profile of oral methadone for cancer-related breakthrough pain: A pilot study. Journal of Pain and Symptom Management. 2004;28(6):619–625.
Fisher, K., Stiles, C., Heim, B., et al. Can fentanyl be systemically absorbed when administered vaginally? A feasibility study. Journal of Palliative care. 2006;22(1):54–56.
Fishman, S.M., Bandman, T.B., Edwards, A., et al. The opioid contract in the management of chronic pain. Journal of Pain and Symptom Management. 1999;18(1):27–37.
Fishman, S.M., Webster, L.R. Unintended harm from opioid prescribing guidelines. Pain Medicine (Malden, Mass.). 2009;10(2):285–286.
Fitzgibbon, D., Morgan, D., Dockter, D., et al. Initial pharmacokinetic, safety and efficacy evaluation of nasal morphine gluconate for breakthrough pain in cancer patients. Pain. 2003;106(3):309–315.
Fleming, A., Noonan, P., Wheeler, A., et al. Abuse-deterrent properties and pharmacokinetics of a novel sustained release formulation of oxycodone for the treatment of moderate to severe pain. The Journal of Pain. 2008;9(4, Suppl. 1):P46.
Flemming, K. The use of morphine to treat cancer-related pain: A synthesis of quantitative and qualitative research. Journal of Pain and Symptom Management. 2010;39(1):139–154.
Flisberg, P., Rudin, A., Linner, R., et al. Pain relief and safety after major surgery. A prospective study of epidural and intravenous analgesia in 2696 patients. Acta Anaesthesiologica Scandinavica. 2003;47(4):457–465.
Foley, K.M. Opioids. Neurologic Clinics. 1993;11(3):503–522.
Foley, K.M. Misconceptions and controversies regarding the use of opioids in cancer pain. Anti-Cancer Drugs. 1995;6(Suppl 3):4–13.
Foley, K.M. Acute and chronic cancer pain syndromes. In: Doyle D., Hanks G., Cherny N.I., Calman K., eds. Oxford textbook of palliative medicine. 3rd ed. New York: Oxford Press; 2004:298–316.
Foley, K.M., Houde, R.W. Methadone in cancer pain management: Individualize dose and titrate to effect. Journal of Clinical Oncology. 1998;16(10):3213–3215.