Congenital heart disease in adults
Jo Ann Nieves and Susan M. Fernandes
Pearls
• An estimated 90% of patients born with congenital heart disease today are expected to reach adulthood.
• Adult survivors with congenital heart lesions outnumber affected children.
• Few congenital heart lesions are “cured.” Most patients have ongoing risk of sequelae or complications unique to each type of congenital heart defect. These patients require lifelong follow-up by specialists in congenital heart disease.
• Transition of the adolescent into adult clinic requires a planned, progressive change resulting in an adult who can manage all aspects of care.
• Most adults with congenital heart disease are “lost to follow-up” care. Reasons include insufficient patient and family instruction regarding lifelong follow-up needs and loss of insurance coverage.
Etiology/Epidemiology
Improved surgical techniques and medical therapies for pediatric patients with congenital heart disease have made survival into adulthood an expectation, but lifelong medical surveillance is necessary to maintain optimal health. Adults with congenital heart disease (ACHD) now outnumber the population of children with congenital heart disease, with greater than 1 million adult survivors.946 An estimated 90% of patients with congenital heart disease who receive treatment are expected to reach adulthood.215 The population of ACHD patients is increasing at a rate of 5%/year.107 The patients who survived complex neonatal interventions (arterial switch, Ross, Norwood, tetralogy of Fallot repairs) from the 1980s are now adults with emerging issues. An estimated half of these survivors have moderate to complex disease, requiring lifelong, continuous care from ACHD specialists for optimal management.383,926 The most complex ACHD patients will need lifelong followup at a minimum of every 6 to 12 months at a regional ACHD program with expertise in adult CHD care.926
Unfortunately, noncompliance in follow-up may be an issue for many adolescents and adults. Many patients present after gaps in care (often >10 years) during late adolescence and early adulthood; such gaps are associated with increased morbidity and mortality.402,728,915,945 The inability to achieve continuity of care is likely multifactorial, with forces including limitations in the patient's and family's understanding of the illness and care required, limitations in health insurance, and adolescent rebellion.131,625,943 Access to adult congenital heart clinics remains limited; families report difficulty finding specialists to care for the adult patient with congenital heart disease.
Many ACHD patients “feel well” and seek follow-up only after they become ill. They can mistakenly believe they are “cured” and may not understand their lesion or potential consequences such as a ventricular dysfunction, thrombosis, arrhythmias, or pulmonary hypertension. The patient may seek medical care only when symptoms of significant sequelae have developed.
Transitioning (self-care management) programs, even when limited in scope, are thought to improve patient knowledge and compliance with medical management and follow-up.953 Given the significant risk of morbidity and mortality in patients with complex congenital heart disease without adequate follow-up, some form of transitioning (self-care management) education is imperative to improve patient outcomes.
Transitioning and Transfer
Transitioning is defined by Blum and colleagues as, “the purposeful, planned movement of adolescents and young adults with chronic physical and medical conditions from child-centered to adult-oriented healthcare systems.”87 This notion has been publicly and academically discussed since 1984 (with the national Minnesota “Youth with Disability: The Transition Years” conference), with recommendations from several related conferences and publications.87,744
The patient with congenital heart disease shares many of the same general issues as other patients with chronic diseases (struggle for independence, personal risk-taking, noncompliance with medical therapy, participation in unprotected sexual behavior, and increased personal emotional exposure and tendency for depression).66,110,834
Patients with congenital heart disease do have many things in common with other patients with chronic disease, yet each patient with congenital heart disease is unique, given the wide spectrum of disease and variable physical, medical, and intellectual impact on any given patient. In addition, the management of the adult with congenital heart disease requires specialized training that few providers can offer. In light of these observations, Knauth and colleagues482 specified that transitioning should exclude transferring of care. They defined transitioning as a process by which adolescents and young adults with chronic childhood illnesses are prepared to take charge of their lives and their health in adulthood. It is an individualized educational process that ideally begins before children reach adolescence and continues until they are capable of assuming full responsibility for their care485 and is recommended to begin by age 12 years.926
In the ideal environment, once a patient successfully transitioned he or she would be transferred to an adult-oriented healthcare system able to care for the cardiac, other medical, and psychosocial issues. Until resources are available to supply this level of care, we must provide all patients with the necessary skills to take responsibility for their health regardless of where or by whom care is provided.
To address specific needs in congenital heart disease, the American College of Cardiology, 32nd Bethesda Conference outlined recommendations for transition and transfer of care.171,273,513,925
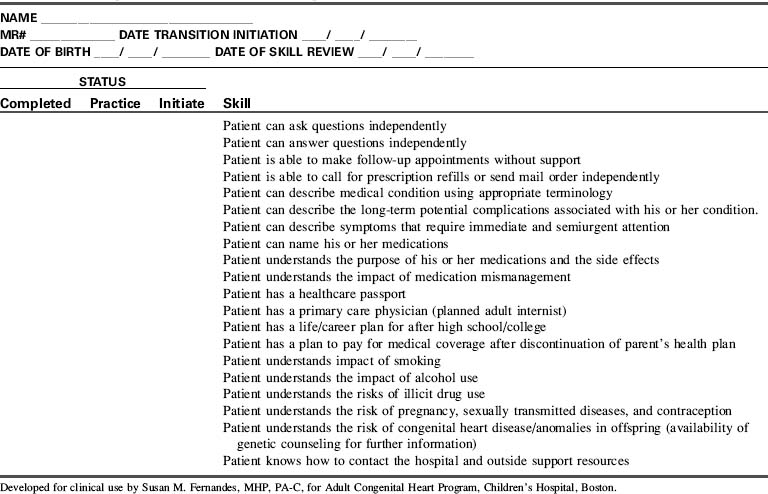
Although the optimal approach to provide transitioning (self-care management) education to adult patients with congenital heart disease has not yet been established, experts in the field proposed a life span model that focused on developmental issues faced by these patients. The areas of concentration included physical development, social and family relations, emotional health, medical issues, health behaviors, screening and prevention, and treatment issues. Using this information, many centers have developed checklists covering several of these areas to ensure that the patient has acquired the necessary skills before transfer of care. An example of such a checklist is provided in Table 8-20. In addition, either electronic or paper complete medical healthcare passports should be carried by patients with details of current and past history specifics, as well as contact information for immediate access to their ACHD healthcare providers.926
Patients who have undergone early childhood total surgical correction for patent ductus arteriosus, atrial septal defect, small ventricular defect, and mild pulmonary stenosis typically have few if any hemodynamic residua and therefore require infrequent evaluation and treatment.215 Most other patients have some form of residua or sequelae of their disease or the treatment and will require lifelong care by ACHD specialists.926
Most patients with ACHD are palliated, not “repaired” or “fixed,” and they require lifelong care.196 Complications of the defect or treatment can include arrhythmias, thrombosis, sudden death, ventricular or valvular dysfunction, pulmonary hypertension, and endocarditis.946 Additional problems can result from residual shunts, valvar disease, ventricular dysfunction, and arterial pathology. These issues may require further surgical or cardiac catheter-based interventions.215 Approximately 50% of adult patients with CHD face additional surgery, arrhythmias, complications, heart failure or, if inappropriately managed, premature death.301,304,305 Late complications increase in frequency over time, typically developing in the second, third, or fourth decade of life; they can be irreversible and potentially fatal.
Occasionally, a congenital heart defect is not diagnosed until adult years; this may be the result of widespread availability of echocardiography.510 A new diagnosis in the adult can include simple lesions, such as an atrial septal defect or a bicuspid aortic valve, to complex lesions, such as L-transposition of the great arteries diagnosed at the age 60 to 70 years,331 with the new development of symptoms, cardiac rhythm disturbances, or congestive heart failure. In some lesions, late diagnosis is complicated by the presence of pulmonary hypertension.
Cardiac catheterization based interventional procedures can be used to treat a variety of adult lesions. Interventions can include balloon dilation, stent placement, occlusion by devices, valve replacement (pulmonary or aortic), valve intervention, and therapeutic arrhythmia procedures (see Cardiac Catheterization).
ACHD survivors require appropriate testing and follow-up for likely residuae and sequelae. Echocardiograms are used but may not be optimal because of poor echocardiographic “windows” (sites to enable visualization of specific cardiac structures). Cardiac MRI (magnetic resonance imaging) is an increasingly important tool for the complete evaluation of complex congenital anatomy and surgical interventions in the adolescent and adult.197 The MRI studies can identify and follow important residual problems, and enable calculation of chamber volumes, quantify valve regurgitation, and enable evaluation of ventricular function, baffle leaks, patency of Fontan pathways, aortic arch status, residual lesions, and flow characteristics. (For additional information, see the MRI section at the end of this chapter.).197,215,314 Cardiac catheterization is used most frequently for interventions.215
Residuae and Sequelae of Congenital Heart Disease
Anticipatory management and ongoing care are critically important and must take place in a center with expertise in complex ACHD care. These patients require expert care for the complications associated with congenital heart interventions and aging. The goal is to monitor for and detect sequelae and provide timely treatment with regular follow-up care. Required management can include simple to complex imaging, cardiac catheter interventions, medications, cardiac pacing or defibrillator implantation, surgery, or cardiac transplantation. Development or progression of symptoms to report is summarized in Box 8-14.215
Box 8-14 Adult Congenital Heart Disease: Symptoms to Report215
If cyanotic, also report hemoptysis, joint pain, headache, epistaxis, or myalgia.
Lesion-specific guidelines and recommendations for the management of adults with congenital heart disease were published in December, 2008, by the American College of Cardiology and the American Heart Association.927 Lesion-specific pathways have also been developed for testing and follow-up of congenital heart lesions in the adult; these are covered extensively by Daniels,215,216 Gatzoulis and Webb,304 and Deanfield et al,227 It is important to note that each patient requires a unique plan for lifelong management; patients with identical original defects may have vastly different presentations in adult years. For example, patients with coarctation may have different ages at intervention, unique forms of surgery or catheterization intervention, specific associated lesions, and unique aortic arch anatomy.215 Each patient also has unique risk factors for acquired coronary artery disease, such as potential obesity, tobacco use, hypertension, diabetes mellitus, hyperlipidemia, or family history of coronary artery disease.215 Many patients do not report the symptoms that they are experiencing that might suggest an increased risk of heart failure and arrhythmias.215 Protocols for routine diagnostic testing can monitor for the development of known lesion-specific significant long-term complications and may enable prevention of serious, potentially irreversible disability.
Heart failure can be right- or left-sided, and related to systolic or diastolic dysfunction or pulmonary hypertension. Structurally significant lesions (whether unoperated or residual lesions) may be treated in selected cases by cardiac catheter interventional procedure or, when applicable, surgery.510 Ventricular dysfunction and heart failure are treated primarily with drug therapy, and treatment of pulmonary hypertension as needed (see section, Pulmonary Hypertension).
The details of a patient's surgical history is important, given the wide variation of surgical technique and the clinical implications. As an example, a Fontan procedure may have been performed with a right atrium to pulmonary artery anastomosis, a lateral tunnel, an extracardiac conduit, or a modification of any one of those. Even less complex lesions such as a coarctation repair can have numerous variations including an end-to-end anastomosis, an interposition graft or a left subclavian flap plasty, which interrupts normal arterial flow to the arm. This along with original versions of the Blalock Taussig shunt may lead to future inaccurate upper extremity blood pressures, which could have significant implications if not noted.
Arrhythmias
Arrhythmias are the most common cause of sudden cardiac death in ACHD,352 and affect up to 50% of adults with congenital heart disease.946 Patients with uncorrected and corrected congenital heart disease may present with arrhythmias. For example, patients with uncorrected atrial septal defect may develop atrial fibrillation or flutter. Ninety percent of patients with late sudden cardiac death related to arrhythmias have tetralogy of Fallot, D-transposition of the great arteries, coarctation of the aorta, or aortic stenosis.352 Antiarrhythmic therapy can be used to treat specific rhythms, but proarrhythmic effects must be monitored. Therapies are detailed by Harris.352 Treatments can include medications, cardiac pacing, implantation of cardiac defibrillators, or surgical interventions such as the Maze procedure46 in the management of patients' status post right atria to pulmonary artery Fontan procedure with subsequent development of atrial re-entry tachycardia or atrial fibrillation.864 The Maze procedure or Cox-Maze III procedure involves cryoablation (−160 °C) as well as surgical atrial incisions of the abnormal conduction pathways during open heart surgery.864
Cyanosis
Cyanosis can affect patients with uncorrected cyanotic lesions, those with uncorrected shunt lesions and Eisenmenger syndrome, those with cyanotic heart defects and palliative procedures (e.g., systemic artery to pulmonary artery shunts, systemic vein to pulmonary artery shunts, central aorta to pulmonary artery shunts [e.g., Waterston, Potts shunt]), Fontan-type procedures with fenestrations, or complex surgical repairs where atrial fenestration remains.
Polycythemia with hematocrit rising to 60% or above may produce symptoms of headache, dizziness, dyspnea, fatigue, and neurologic changes.215 Dehydration must be avoided because of hyperviscosity and risk for stroke or emboli. All intravenous systems require meticulous removal of any air or clots because of risk of paradoxic emboli to the brain, kidney, or heart.215 Thrombocytopenia and coagulopathies are common (see Hypoxemia Caused by Congenital Heart Disease).
Phlebotomy is not routinely performed unless the patient becomes symptomatic. An equal volume of whole blood may be removed and replaced with saline or albumin. Potential complications of phlebotomy include stroke, seizures, and death.864
If the cyanosis is associated with pulmonary hypertension (e.g., Eisenmenger syndrome), the patient requires pulmonary hypertensive care precautions. In addition, medical management is required (see the following).
Cyanotic adults may also develop hyperuricemia, gouty arthritis, and altered renal function requiring treatment with allopurinol or colchicines.864 Hypoperfusion and chronic hypoxia also lead to renal disease.215
Pulmonary Hypertension
Pulmonary hypertension can develop as a consequence of congenital heart disease in 15% to 30% of patients,511 those repaired at a later age, or those with significant unrepaired left-to-right shunts.215 Patients with single ventricle with Glenn and Fontan palliations or staged correction require the lowest possible pulmonary resistance for survival.511 Evaluation of the status of the pulmonary vascular bed may include cardiac catheterization with measurement of the reactivity to pulmonary vasodilator therapy (see Common Diagnostic Tests, Cardiac Catheterization).
Patients may demonstrate hypoxemia as a result of pulmonary hypertension and progression to Eisenmenger syndrome with reversal of the intracardiac shunt. This pulmonary hypertension is typically unresponsive to oxygen.926 Pulmonary vasodilator treatments include oxygen therapy to treat hypoxemia (particularly at night),215 inhaled nitric oxide or epoprostenol,511 prostacyclines, endothelin receptor antagonists (Bosentan),912 and phosphodiesterase five inhibitors (Sildenafil).511
Pulmonary hypertensive precautions are vital during periods of illness or procedures requiring anesthesia because these situations include risk for conditions such as acidosis, alveolar hypoxia, pain, agitation, and hypoventilation that may provoke pulmonary vasoconstriction. Goals of care will include lowering PAP, decreasing PVR and RV afterload while maximizing RV function, ultimately improving cardiac output. Nursing care will focus on optimizing ventilation, improving RV function, providing adequate sedation, treating pain, avoiding metabolic and respiratory acidosis, avoiding atelectasis, avoiding anemia, and minimizing energy expenditure needs.511 In the immediate cardiac surgery postoperative period, reactivity of the pulmonary vascular bed is heightened.511 Support of systemic blood pressure may be required with use of agents such as norepinephrine to maintain coronary perfusion.511
Adequate hydration is essential, and hypotension must be avoided.215 Strategies for care attempt to decrease pulmonary artery pressure, enhance right ventricular function, and avoid development of pulmonary hypertensive events or crises with subsequent right ventricular failure (see Sectons “Pulmonary Hypertension” and “Management”).
Selected Eisenmenger syndrome patients may require phlebotomy because of symptomatic hyperviscosity, with specific guidelines to avoid acute adverse reactions and even death. For further information, see Daniels215 and Warnes et al.926
Conduit Obstruction
Extracardiac conduits and baffles can develop obstruction over time, requiring reintervention. The conduits connect the subpulmonary ventricle to the pulmonary arteries in tetralogy of Fallot and other complex congenital heart disease.398 Treatments include cardiac catheterization intervention (balloon angioplasty or stent implantation).
Conduit replacement is possible with early low mortality; of patients reoperated at a mean age of 9.6 years, 55% were free from conduit reoperation at 10 years, and 31.9% at 20 years.228 Developments in percutaneous pulmonary valve replacement have resulted in avoiding surgical revisions in many of the cases treated550 and are FDA approved since 2009.598 Patients with conduits require lifelong periodic reevaluation526 in adult CHD clinics.215,926
Adult Cardiovascular Problems
Additional impacts on cardiac health related to adult lifestyle and hereditary issues include smoking, obesity, hypertension, hypercholesterolemia, and coronary artery disease. Healthy adults (18 to 65 years old) should ideally complete at least 30 minutes of regular physical activity per day, 5 days a week,354 yet many adult patients with congenital heart disease are uncertain of their specific goals and limits, requiring additional assessment from their cardiology team and education about the benefits of exercise.246 (See http://www.heart.org/HEARTORG/Conditions/CongenitalHeartDefects/CareTreatmentfor CongenitalHeartDefects/Congenital-Heart-Defects-and-Physical-Activity_UCM_307738_Article.jsp). Aerobic functional capacity compared with healthy adults has been found to be diminished in patients with congenital heart disease, and significantly lower than normal.280 Typical low-intensity exercises such as walking, casual swimming, and dancing are encouraged. Individualized instructions are recommended (see http://www.americanheart.org/presenter.jhtml?identifier=11081).
Atherosclerotic heart disease is a major cause of morbidity and mortality in adults in the United States and many countries.369 Atherosclerotic heart disease begins to develop in early childhood, even in the patient with congenital heart disease,578 and guidelines for primary prevention in children have been identified.369
Lifestyle choices and modifiable risk factors can have a major impact on morbidity and mortality of patients with congenital heart disease. Minimizing cardiovascular risk factors, and following a healthy lifestyle can minimize the risks of complications related to coronary artery disease. Strategies include management of diet, regular exercise, and avoiding cigarette smoking.186 Obesity is a common finding in children with congenital heart disease.703 A known independent risk factor for type 2 diabetes and heart disease is obesity,683 which should be avoided. (See http://www.heart.org/HEARTORG/Conditions/CongenitalHeartDefects/CareTreatmentforCongenitalHeartDefects/Recommendations-for-Heart-Health_UCM_307739_Article.jsp).
Long-Term Outcomes of Specific Defects
As patients age following surgical intervention for congenital heart disease, information is accumulating regarding long-term outcomes.
Bicuspid Aortic Valve
Bicuspid aortic valve is the most common congenital lesion, present in about 1% to 2% of the population.215,926 The lesion can progress over time, requiring patients to be monitored for potential development of aortic valve calcification, regurgitation, and stenosis. Aortic root dilation and dissection may also develop.926
When indicated, therapeutic interventions may include interventional catheterization balloon valvuloplasty, or surgery for aortic valve intervention or replacement, or a Ross procedure (see section, Specific Diseases, Aortic Stenosis).
Coarctation of the Aorta
Coarctation of the aorta may be diagnosed late in life, and the patient may present with upper extremity hypertension with decreased lower extremity pulses and blood pressures. Late complications of repair include recoarctation, aortic aneurysm or dissection, and sudden death. Systemic hypertension has been reported in up to 70% of patients after coarctation repair,427 and must be differentiated from hypertension caused by recoarctation through use of physical exam (arm and leg blood pressure gradients) and diagnostic studies. Systemic hypertension may occur during rest or activity, and may require medical therapy.215,926 Blood pressures may be decreased in the left arm if a left subclavian artery flap was used in the original repair. The cause of the high risk of hypertension and aortic dissection is unknown.215
Recoarctation incidence is 8% to 54% and in selected cases may be treated with transcatheter therapy (stent, angioplasty).215 An aortic aneurysm may form in the left subclavian flap or patch aortoplasty repair site.197 Bicuspid aortic valve is present in about half of patients with coarctation of the aorta.527a These bicuspid valves can develop significant stenosis or regurgitation.196
Atrial Septal Defect
The adult with an undiagnosed atrial septal defect may present with a cerebrovascular accident or transient ischemic attack following a paradoxic embolism across the atrial septal defect.215 Factors leading to arrhythmia development include chronic right heart volume overload, ventricular dysfunction,926 late date at operation, or the presence of pulmonary hypertension.352 About 50% of those patients with preoperative atrial arrhythmias have postoperative arrhythmias, particularly if they are 40 years old or older at the time of surgery. The presence of atrial arrhythmias can result in need for anticoagulation.352 Transcatheter device closure is possible for many with secundum type lesions (see Specific Defects, Atrial Septal Defect).
Adult patients presenting with sinus venosus or primum defects require surgical repair.802 Pulmonary hypertension may be present in the unrepaired adult. Atrial septal defects repaired early in life are typically symptom free, but atrial arrhythmias (fibrillation or flutter) may develop in the operated608,926 and the unoperated patient.352,926
Tetralogy of Fallot
Tetralogy of Fallot is the most common complex defect with the longest survival history.946 Most adult patients have undergone surgical repair in childhood or even adolescence,352 and some have undergone initial palliative shunt procedure. Some patients may have a right ventriculotomy with a patch or a valved conduit between the right ventricle and pulmonary artery, whereas others have surgical removal of the pulmonary valve with a transannular patch and resultant free pulmonary regurgitation.
If the pulmonary valve is present, it may become insufficient or stenotic and the distal pulmonary arteries obstructed. Postoperative patients may develop arrhythmias. Atrial arrhythmias (flutter, fibrillation or supraventricular tachycardia) develop in up to one third of patients.743 Ventricular tachycardia and sudden cardiac death are known complications.215,926 By 35 years after surgery, the estimated risk for sustained ventricular tachycardia is 11.9%, and for sudden death is 8.3%.302
RV size correlates with QRS duration. The combination of older age at correction and QRS duration of 180 ms or longer, as well as older age at initial repair352 predict risk of sustained ventricular arrhythmias and sudden cardiac death.303 Right bundle branch block (RBBB) is a common finding in patients who had surgical correction many years ago, but in itself is not predictive of a worse prognosis (although RBBB with QRS 180 ms or higher is).352
The most common problem following surgical correction of tetralogy of Fallot is pulmonary regurgitation, which causes chronic right ventricular volume overload and may progress to right ventricular enlargement and systolic dysfunction.215,926 Severe right ventricular dilation and mild global right ventricular systolic dysfunction are associated with higher risk for adverse clinical outcomes in patients with repaired tetralogy of Fallot.482 Progressive aortic root dilation and potential for aortic dissection may also develop.215 Pulmonary regurgitation is the most common reason for late reoperation.946
Tetralogy of Fallot survivors require lifelong monitoring, including regular evaluation with MRI,482,926 for each of these potential complications and to avoid progression of decreased cardiac function. Surveillance for potential arrhythmias is required. Treatment for arrhythmias includes cardiac pacing, use of implantable cardioverter/defibrillators, antiarrhythmic therapy or radiofrequency ablation, or arrhythmia intervention during reoperation352 for pulmonary valve replacement. Selected cases may undergo transcatheter pulmonary valve replacement via cardiac catheterization.598 Long-term survival at 32 years is 86%.641 Tetralogy of Fallot is the most common diagnosis for patients with implantable cardioverter defibrillators.467
Transposition of the Great Arteries
Atrial switch for d-transposition of the great artery (Mustard or Senning procedure) requires extensive atrial incisions and suture lines.352 As a result, patients who undergo these procedures require lifelong regular monitoring215,926 for development of arrhythmias (atrial tachycardia, sick sinus syndrome) and are at risk for sudden cardiac death. Loss of sinus rhythm is common, with only 18%950 to 40%310 of survivors in sinus rhythm 15 to 20 years after surgery. Pacemaker implantation is anticipated in about one-fifth of adults with long-term followup after a Mustard procedure.352
Pacemakers can be used to treat bradyarrhythmias or tachyarrhythmias,352 and radiofrequency ablation or medications can be used to treat tachyarrhythmias.215 Despite close followup, about 7% of patients have sudden cardiac death after atrial switch.950
After an atrial switch procedure for d-transposition of the great arteries, the right ventricle is the systemic ventricle (pump) for life and progressive dysfunction develops by the second or third decade of life in about 15% of postoperative patients,950 with progression to ventricular arrhythmias in the failing ventricle.352 The tricuspid valve, exposed to systemic pressures, can become dysfunctional. Narrowing in the left ventricular outflow area can also develop.
Reconstruction of the atrial flow pathways can rarely result in the serious complication of baffle obstruction of pulmonic or systemic venous return.215 Baffle leaks causing atrial shunting are common but they are often small.215 If despite optimal medical management the ventricular dysfunction becomes severe, either staged surgical anatomic correction (arterial switch procedure) or cardiac transplant may be planned. Patients with d-TGA, VSD, and pulmonary stenosis repair will have undergone a Rastelli procedure with a conduit between the right ventricle and pulmonary artery, that will require continued surveillance.
Arterial switch became the treatment of choice for transposition of the great arteries in the 1980s. Follow-up shows good systemic ventricular function and sinus rhythm,946 although the patients having additional VSD repair are reported at higher risk for arrhythmias.359 Potential long-term issues include the need for serial assessment of ventricular function and surveillance for the development of arrhythmias, stenosis at the great vessel suture sites,946 neo-aortic root dilation, and development of valvar regurgitation.186
Coronary artery lesions, found in 5% of patients following the arterial switch operation, are progressive and can be treated by coronary angioplasty or surgery.719 Coronary atherosclerosis remains a concern and requires careful followup.692 The progression of coronary artery disease after the arterial switch procedure is unknown. The most common cause for reoperation is pulmonic stenosis.547 Survival at 15 years after the initial operation is 88%,547 but long-term outcome is unknown.186,215,926
Single Ventricle
Although it is a rare condition, patients with a single ventricle account for a disproportionate share of the morbidity and mortality found in adults with congenital heart disease.946 Single ventricle includes diagnoses of tricuspid atresia, mitral atresia, double inlet LV, hypoplastic right or left ventricle, or single ventricle. These patients will remain cyanotic until they undergo Fontan-type correction. The first patients with a Fontan-type staged palliation and correction are now in their fourth decade of followup.466 Young adults with a univentricular heart who are unrepaired have a poor prognosis.215
The original Fontan procedures (1970s) connected the right atrium directly to the pulmonary arteries, or connected the right atrium to the right ventricle, exposing the right atrium to high systemic venous pressure.352 Over time elevated right atrial pressure can lead to right atrial enlargement, hypertrophy, and slowed atrial conduction.352 A severely enlarged right atrium is often seen in patients with a classic Fontan procedure and a failing Fontan circuit, which contributes to development of medically resistant complex atrial arrhythmias.926 Atrial distension and surgical incisions with subsequent scarring also contribute to arrhythmia formation.352 Atrial tachycardia and sick sinus syndrome may be observed, particularly in those patients with the right atrium included within the Fontan pathway.352 Atrial tachycardia can develop in up to 50% of adults with Fontan procedure,226,926 and sinus bradycardia or junctional escape rhythm has been reported in up to 15% of patients.352 Sustained atrial arrhythmias may cause patients to present with congestive heart failure, low cardiac output, and can lead to development of atrial thrombi.352 Anticoagulation therapy is often required in the presence of sustained atrial arrhythmias.352 Therapy for arrhythmias can include antiarrhythmic therapy, pacemaker (typically epicardial if ventricular), radiofrequency ablation, or arrhythmia intervention during reoperation.352
Many long-term complications have been reported following single ventricle palliations. Outcomes have improved, but systemic ventricle dysfunction may develop, particularly with a right ventricular systemic pump.311 The less efficient right atrium to pulmonary artery Fontan type surgical procedure has become obsolete,311 replaced by the total cavopulmonary artery connections (superior vena cava to pulmonary artery shunt plus intraatrial lateral tunnel or extracardiac conduit).467 The use of external conduits from the inferior vena cava to the pulmonary artery results in a sutureless right atrium, and potentially may decrease incidence of postoperative atrial arrhythmias.311 Some patients may have a lateral tunnel connecting the inferior vena cava to an intraatrial tunnel, then the pulmonary arteries. Long-term data are not yet available to define long-term outcomes of these two procedures.311
Pulmonary vein compression, pulmonary artery stenosis, Fontan pathway obstruction, atrioventricular valve insufficiency, arrhythmias, hepatic dysfunction, hepatic fibrosis, and cirrhosis may each develop after the Fontan procedure.47,215,926 Protein losing enteropathy is reported in 3.7% of patients following Fontan-type correction and is associated with a poor clinical course,311 with a 50% 5-year mortality after the diagnosis.612,926
The function of the single systemic ventricle and atrioventricular valve can deteriorate, and must be monitored closely, particularly in those patients with a right ventricle performing a lifetime of systemic work. Heart failure risk in Fontan patients is reported to be higher in those patients with the (single) morphologic right ventricle functioning as the systemic ventricle.944 Currently, many patients with the Fontan operation have hypoplastic left heart syndrome, with a resultant systemic right ventricle, creating concerns regarding long-term right ventricle status.311
Arterial oxygen saturations will be monitored for the potential late development of cyanosis caused by fenestration of the Fontan or the development of pulmonary arteriovenous malformations (AVM), systemic venous collaterals, or baffle leaks.215 Patients developing cyanosis215 or residual stenosis may require diagnostic or therapeutic cardiac catheterization. Cardiac magnetic resonance imaging (MRI) cannot be completed if the patient has a cardiac pacemaker.
The failing Fontan circuit may require surgical revision with conversion to an extracardiac Fontan and a form of the Maze procedure for treatment of intractable atrial tachycardia.926 Recent reported perioperative mortality is 1%,46,226 and late mortality is 5%.46
Survival at 25 years after Fontan-type correction has been reported at 70%.467 The most frequent causes of late death in Fontan patients are sudden death (9.2%), thromboembolism (7.9%), and heart failure (6.7%), with an arrhythmic origin presumed for the sudden deaths.467 Absence of aspirin or warfarin therapy is a predictor of death caused by thromboembolic event.467 The risk for thromboembolic death increases sharply 15 years after Fontan surgery.467 All single ventricle patients require continuous lifelong care in a center with expertise in ACHD care. In the presence of single ventricle dysfunction or protein-losing enteropathy, a heart transplant may be beneficial.926 More information is needed regarding long-term outcome of these patients.
Reproductive Health in Women with Congenital Heart Disease
Women with congenital heart disease appear to have similar sexual activity and fertility rates as their healthy peers.137,245,609,729 Pregnancy planning in this patient population is required to reduce maternal and/or fetal morbidity. Yet, few patients seek advice regarding birth control and family planning.428,738,835 It is imperative, therefore, that the healthcare team caring for these patients maximize opportunities to discuss pregnancy prevention and planning. Detailed information regarding pregnancy, contraception, and delivery for patients with congenital heart disease is included in the Chapter 8 Supplement, section, Adults with Congenital Heart Disease, on the Evolve Website.
Medical and surgical advances have made survival into adulthood an expectation for patients with congenital heart disease. With these advances have come an influx of women with moderate and complex congenital heart disease who desire pregnancy. Although pregnancy and delivery are associated with significant hemodynamic changes such as increased blood volume, increased stroke volume, increased cardiac output, and decreased systemic vascular resistance, most women with repaired congenital heart disease appear to tolerate pregnancy and delivery with only minimal risk.809
The majority of women with congenital heart disease tolerate pregnancy and delivery without significant risk, although there are many obstetric, cardiac, anesthesia, genetic, and psychosocial factors to consider. In patients with more than simple disease, a multidisciplinary approach in a regional center is essential to optimize maternal and fetal outcomes.
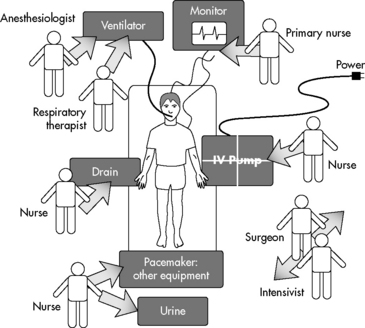
Perioperative Care for the Patient with Adult CHD
Perioperative care for the patient with ACHD for minor (elective noncardiac procedures) and major procedures, as well as emergency admissions426 requires comprehensive medical, surgical, and nursing management. The team must be knowledgeable about the cardiac anesthesia requirements, the potentially complex hemodynamics, any residual structural abnormalities, anticoagulation needs, and physiologic abnormalities related to each congenital heart lesion. Adults with important co-morbidities such as coronary artery disease or renal failure may require postprocedure recovery in an adult cardiac critical care unit with the consultation of the required adult subspecialists. Adults without significant comorbidities may be treated in a section of the pediatric cardiac critical care unit. Communication among the congenital surgical, interventional cardiology, and adult medical subspecialists is essential to provide optimal care, involving nursing education regarding the defect pathophysiology, hemodynamics, surgical intervention, and likely postoperative complications. The healthcare team must continue to monitor for and document long-term outcomes.
Procedures
Cardiac catheterization may be required in adults with CHD for hemodynamic assessments. Interventions are commonly performed for complex pulmonary artery stenosis, baffle stenosis, or residual aortic narrowing. Shunting defects, including fenestrations, may be sealed with devices (see Common Diagnostic Tests, Cardiac Catheterization). Pulmonary valves and aortic valves are now replaced by transcatheter interventions in selected cases. Pediatric electrophysiology studies to detect and treat atrial or ventricular arrhythmias may include implantation of a cardiac pacemaker with possible cardioverter defibrillator.388
Postoperative Care
Comprehensive guidelines are available for the perioperative assessment and management of patients with adult congenital heart disease undergoing noncardiac surgery.196 When cardiovascular surgery is required, reoperations are the most common type of surgery needed.802 High-risk patients require close postoperative surveillance in a critical care or coronary care unit, particularly patients with cyanosis, pulmonary hypertension, ventricular dysfunction, or single ventricle.196
The most common reported complication in the postoperative cardiac surgery adult (occurring in 10.8% of patients) is atrial arrhythmias.1 The postoperative team must carefully monitor the patient's volume status, hemodynamics, and electrolyte balance, and be observant for evidence of hypoxemic pulmonary hypertensive episodes or crisis and be aware of all drug therapies required. Each cardiac lesion carries risks of particular rhythm disturbances, and unexpected arrhythmias may occur at any time.
Conduction anomalies are common in adults with uncorrected cyanotic CHD,802 including ventricular or supraventricular ectopy. Perioperative development of arrhythmias can lead to sudden, severe low cardiac output. Immediate evaluation and prompt treatment are required.802 Monitoring for development of cardiac ischemia includes monitoring for ST segment changes and ventricular ectopy. Atrial and ventricular pacing wires can assist in management (see Arrhythmia Detection and Management).
Bleeding is a potential risk following reoperation, particularly in the patient with longstanding cyanosis.802 Reoperation requires incisions through vascular scar tissue and chronic hypoxemia is associated with thrombocytopenia and thrombocytopathia. In addition, patients with chronic hypoxemia may demonstrate a decrease in vitamin K-dependent clotting factors. For these reasons, bleeding should be anticipated and plenty of blood should be available for postoperative blood replacement.
Cardiac reserve may be limited in many cyanotic patients, and excessive blood loss can rapidly cause hemodynamic instability. Target hemoglobin values and plans for coagulation factor replacement are individualized based on the specific congenital lesion, operative interventions, and associated risk factors. A patient with expected residual cyanosis cannot tolerate anemia, because it decreases oxygen-carrying capacity and reduces oxygen content and likely oxygen delivery.
The risk of perioperative low cardiac output is increased in the presence of chronic hypoxemia, ventricular hypertrophy, chronic volume or pressure overload, ventricular dysfunction, and arrhythmias. In the postoperative period, reactivity of the pulmonary vascular bed is heightened,511 so pulmonary hypertension precautions are vital (see section, Pulmonary Hypertension).
Pulmonary hemorrhage may develop with interventions that increase pulmonary blood flow, particularly after interventional cardiac catheterization. Mechanical ventilation and pulmonary support are required. Development of pneumonia, infection, fever, thrombosis, or pulmonary edema can seriously destabilize the patient with ACHD, even after a minor procedure. Supplementary oxygen can help to decrease the pulmonary vascular resistance, although if cyanotic heart disease is present it may not increase the arterial oxygen saturation.196 Parameters for acceptable and expected oxygen saturation levels and PaO2 are required.
Smoking can compromise pulmonary function preoperatively and postoperatively. Encourage pulmonary toilet hourly while awake with incentive spirometry, and encourage the patient to get out of bed and walk or at least sit in a chair as soon as possible. Intermittent pneumatic compression or the use of antiembolism stockings should be used to reduce the risk of deep vein thrombosis (DVT).196
Risk of DVT is increased with prolonged bedrest, neuromuscular blockade, and limited range of motion. Early ambulation is optimal. Monitor for signs of DVT, including redness or pain in the leg calves. Signs of pulmonary embolus include sudden dyspnea, tachypnea, increased oxygen requirement, and rales. An arterial blood gas will not establish the diagnosis. Massive pulmonary embolism can result in acute right ventricular failure, low cardiac output, and myocardial ischemia with ST segment changes. Diagnosis is confirmed by lung perfusion scan or pulmonary angiogram. Treatment includes immediate, heparinization, and hemodynamic supportive care. In acute situations, fibrinolytics (recombinant tissue plasminogen activator or rTPA) are administered. Cardiopulmonary bypass may be employed to remove the embolus (pulmonary embolectomy).
Renal dysfunction is a known risk in patients with chronical cyanotic hypoxemia.802 Cardiopulmonary bypass can further exacerbate renal dysfunction. Perioperative care includes maintaining optimal cardiac output with careful fluid balance and support of systemic perfusion. Volume replacement requires normal saline infusions typically of 500 cc or more (10 cc/kg), administered as a bolus to optimize cardiac filling pressures. Infusion by syringe injections (often used for pediatric patients) does not allow administration of sufficiently large volumes when resuscitation is required.
Relative hypovolemia can result from rewarming and vasodilation, fever, increased capillary permeability, and use of vasodilators. Signs can include sinus tachycardia, decreased central venous or intracardiac pressures, and signs of decreased perfusion.
Standard medication doses for adults are used, including doses for resuscitation drugs, antiarrhythmic therapy, and antibiotics. Intravenous drug infusions in the adult can be specifically concentrated by the clinical pharmacist to avoid excessive fluid volume administration. Doses must be titrated individually with consideration of any renal or hepatic dysfunction.
Cyanotic patients are at greater risk of postural hypotension because of a greater right-to-left shunt.196 Changes in movement should be gradual.
Effective pain management is essential to minimize catecholamine surges.196 The patient with ACHD may have sensitization to and greater fear of painful procedures because of a previous history of inadequately managed pain during prior surgeries or hospitalization.707 Discussion of plans for pain control and patient-controlled analgesia help to control potential anxiety. Patients with preoperative history of illegal drug use or preoperative prescription narcotics typically require higher doses of analgesia postoperatively. Inadequate analgesia can lead to decreased chest physiotherapy and ambulation.
Many adult survivors of congenital heart disease have unique alterations in neurologic status related to the presence of genetic syndromes (Down, DiGeorge, Williams) or previous neurologic alterations leading to developmental delays and increased dependence on family involvement in care. Rest and privacy are essential. The adult's bedtime ritual can be assessed. Some may use prescriptions, rituals, or over-the-counter medications to promote sleep.
Unique developmental needs and degree of family involvement may be present in the patient with ACHD. Some may rely heavily on a parent and/or significant other for making decisions and daily activities. Survivors require guidance in terms of educational and vocation choices. Some of the survivors of complex congenital heart disease management are at risk for inattention, hyperactivity, and developmental disabilities, and require remedial school services.798
Issues with independence and interdependence may exist, as well as other psychological challenges found in patients with chronic illness, as detailed in Claessens et al180 and Tong et al.867 Providers should assess the patient's knowledge and independence in areas of self-care.
Transitioning to Adult Specialist Care
The transitioning process from pediatric to adult-focused CHD care is life-altering for patients, parents, and staff. The act of transfer may be a substantial source of stress for the patient, parent, and longtime caregiver. Therefore all involved parties should be involved in the transitioning process. The concept of transitioning should be discussed early, around age 12 if the patient is emotionally and intellectually ready, and should continue until the patient demonstrates the ability to take responsibility for self-care. It is essential to provide adequate resources for support of the family at this time, including both in-hospital resources and outside patient support resources. The Adult Congenital Heart Association (ACHA) and American College of Cardiology developed a “Passport” document to allow patients to concisely identify their specific cardiac health needs and endocarditis prophylaxis requirements. The healthcare team can provide lesion specific identification of patient conditions, therapies, and the suggested guidelines for ACHD care. A clinic resource list now identifies ACHD clinics nationwide, and is available on the ACHA web site (www.achaheart.org).
Education with respect to employment, insurance needs, and social service resources are also required by many. Continued monitoring and instruction regarding management of noncardiac surgical procedure care and required collaboration with the adult CHD team are essential to optimize care and safety, and minimize morbidity and mortality risks.
Ultimate goals are to optimize ACHD survival and maximize quality of life. It is clear that all patients with congenital heart disease require lifelong collaborative care from pediatric and adult specialists who will provide ongoing screening for known complications and potentially unexpected sequelae of the defect and therapies. These complex patients face potential long-term and possible life-threatening complications. Transition from the pediatric into the ACHD clinic is a vital priority.
Resources for Healthcare Professionals and Families
• Adult Congenital Heart Association (ACHA): www.achaheart.org
“Passports” for CHD, extensive patient education materials, pamphlets available
• American Heart Association: http://www.heart.org/HEARTORG
• International Society of Adult Congenital Cardiac Disease (ISAACD): http://www.isaccd.org/