Chapter 5 Observation
Symmetry and Posture
Assessments of symmetry and posture are important aspects of a lameness examination. Comparison between the normal and abnormal sides facilitates identification of abnormalities, unless the condition is bilateral so that no recognizable differences exist between the left and right limbs. The horse should be standing squarely on a flat surface in a quiet, insect-free environment. Horses with severe lameness often are reluctant to stand correctly, but information gained about symmetry and posture of severely lame horses is valuable. The veterinarian should look carefully at size, shape, contour, heights, and widths and compare with the opposite side.
Forelimb Symmetry
Muscle Atrophy
The symmetry of skeletal muscle in the forearm, pectoral, and cervical areas should be assessed. Muscle atrophy that occurs in horses with chronic lameness conditions is called disuse atrophy and in those with neurological disease is called neurogenic atrophy. Horses with muscle atrophy and lower motor neuron disease (see Chapter 11) may be lame, sometimes as a result of muscle pain or nerve root pain, complicating differentiation between these causes of muscle atrophy. In most but not all horses with neurogenic atrophy, other clinical signs suggestive of neurological disease may be present. Horses with disuse atrophy resulting from chronic lameness usually have generalized atrophy of the ipsilateral forelimb. Muscle loss usually is not pronounced but involves the forearm (extensors are most commonly affected), triceps, and shoulder muscles. Shoulder muscle atrophy involving the infraspinatus and supraspinatus muscles generally is not pronounced, and lateral subluxation of the shoulder joint during weight bearing is not present (see Chapter 40).
Development of disuse atrophy resulting from chronic lameness generally takes weeks to months unless severe lameness exists. In horses with severe or non–weight-bearing lameness, atrophy may develop within 10 to 14 days. In horses with severe forelimb lameness, carpal contraction (flexural deformity of the carpus) may occur simultaneously with muscle atrophy. The most common causes of carpal contraction because of ipsilateral forelimb lameness are olecranon fracture and other elbow lameness, but carpal contraction may occur in horses with severe shoulder or even lower limb lameness. Atrophy of the triceps muscles usually is recognized before other muscle atrophy in severely lame horses.
Horses with neurogenic atrophy may have profound atrophy of one or more muscles in the forearm, pectoral, or cervical regions. Atrophy often is much more pronounced than expected based on the degree of lameness, prompting suspicion of neurological disease. Pronounced, unilateral pectoral or triceps atrophy with mild atrophy of the forearm muscles suggests neurological disease. Severe atrophy localized to the infraspinatus or supraspinatus muscles without subluxation of the shoulder joint usually results from injury of the suprascapular nerve caused by external trauma. Atrophy and subluxation of the shoulder joint is associated with injury of the brachial plexus or nerve roots. Other muscles may also show atrophy.
Localized muscle atrophy or fibrosis occurs in horses with previous injury and subsequent scar tissue formation within muscle bellies. This condition is more common in the hindlimb but occasionally occurs in the forelimb.
Swelling
Swelling, a common sign of inflammation, often causes asymmetry. The presence of swelling and heat should alert the lameness diagnostician to the possibility of an infectious process and may lead to additional examinations such as assessment of body temperature and the acquisition of laboratory data. Swelling within a joint capsule caused by excess joint fluid, effusion, is a general reaction of the joint to several traumatic or degenerative processes. Edema, cellulitis (lymphangitis), bleeding, and fibrosis can cause soft tissue swelling. Underlying bony enlargement can mimic soft tissue swelling, particularly in older horses with advanced osteoarthritis. Some swellings are clinically innocuous, such as mild distention of a digital flexor tendon sheath (so-called “windgalls” or “wind puffs”), but a recent change in size, local heat, or marked left-right asymmetry should alert the clinician to a possible problem. Occasionally a well-circumscribed tense spherical swelling is seen palmar to the neurovascular bundle on the side of the fetlock. These synovium-filled masses are usually incidental findings of no clinical significance. Edema usually signals acute inflammation, and pits (a distinct impression is visible) when compressed by digital palpation (pitting edema). Horses develop edema around and often distal to the site of inflammation. In some horses, especially racehorses left unbandaged when accustomed to being bandaged, benign mild-to-moderate edema of the distal extremities develops. This process is called “stocking-up” and should not be misinterpreted as a pathological process. In these horses the edematous area is not painful and usually does not pit, and the horse is not lame. Edema in these horses can complicate lameness examination because it is sometimes difficult to palpate underlying structures and to perform diagnostic analgesia.
Cellulitis describes infection within the tissue planes of the distal extremities (see Chapter 14) and is sometimes called lymphangitis. Lymphangitis, by definition, is inflammation of the lymphatic circulation of the limb, but the conditions are similar and the terms are used interchangeably. Swelling is firm, warm, and painful, and lameness is often pronounced. “Stovepipe” swelling describes this condition (“the horse is all stoved-up”). Horses generally show systemic signs such as fever and elevated white blood cell count. Cellulitis usually results from small puncture wounds that may be difficult to discover or occurs after articular, periarticular, or subcutaneous injections. Infection develops in subcutaneous tissues or deeper in the dense fascial planes and can be difficult to eradicate.
Blunt trauma or fractures may cause bleeding within tissue planes. Severe lameness and swelling accompany fractures of the scapula and humerus, because large vessels are nearby. Bleeding may be severe and cause a decrease in plasma protein and packed blood cell volume values. In horses with fractures located more distally in the limb, swelling is less pronounced but still prominent. The most likely location of injury is the swollen area, but swelling may occur distal to the site of injury because of venous and lymphatic congestion.
Fibrosis or scar tissue formation as the result of previous cellulitis or trauma causes asymmetry of the distal extremities but may not be the source of the current lameness. The veterinarian should avoid overinterpreting areas of scar tissue formation unless evidence of recrudescent inflammation exists. Horses may have scars caused by previous application of counterirritants or from healed wounds, leaving large, painless, and thus benign blemishes. Scars from previous surgical procedures, sometimes recognized by small areas of white hair accumulation, should be noted but may have no bearing on the current problem. Previous scars may have more relevance during prepurchase examinations.
Bony swelling is a common cause of asymmetry. Proliferative change results in periosteal or periarticular new bone formation and accompanies myriad problems in the distal extremities. Bony changes may be active, causing the current lameness problem, or old and inactive, causing few or no clinical signs. For example, old inactive bony swelling of the shin or osselets (bony and fibrous swelling of the fetlock joint) may be prominent in ex-racehorses but may have little to no relevance to current lameness.
Angular Deformity
Angular limb deformities in young horses are common, are sometimes associated with lameness or other developmental orthopedic disease, and are discussed elsewhere (see Chapter 58). Abnormalities of conformation should be noted but may have little relevance to the current lameness problem (see Chapter 4). Horses younger than 2 years of age with severe forelimb lameness of several months’ duration may develop contralateral varus deformity originating from the carpus or elbow joints.
Horses with severe lameness usually caused by trauma may have luxation or subluxation of joints as a result of collateral ligament injury or fractures and may have an acute change in limb angulation. Angular deviations of limbs are unusual in older horses and generally signal severe injury. Visual examination should be followed by careful palpation during which varus and valgus stress is applied to joints. Stress radiographs can be useful to determine collateral ligament integrity.
Foot Size
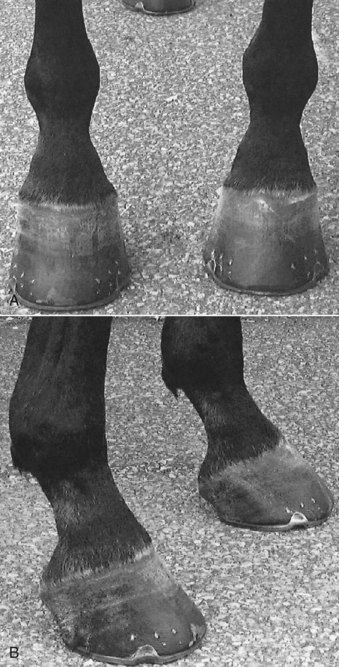
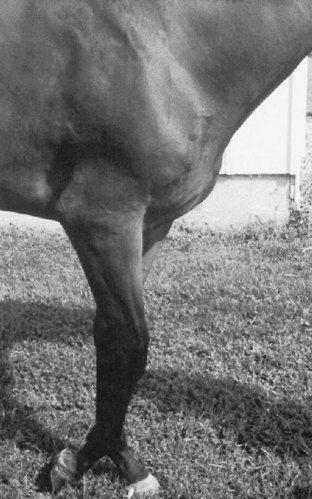
Ideally both front feet should be identical in size and shape, or nearly so, and any asymmetry should be noted. Horses with chronic lameness may have disparity in foot size, usually with the smaller foot being ipsilateral to lameness. The small foot often is contracted and more upright (Figure 5-1). Chronic reduction in weight bearing results in foot size disparity in some, but not all, horses. Mild disparity in foot size is a normal finding in some horses. Mild clubfoot conformation, acquired from previous flexural deformity, may be present incidentally in adult horses. Previous lameness may have caused contraction of the foot but has since resolved, resulting in disparity in foot size and shape but no residual lameness. In these horses it would be a mistake to assume current lameness is originating from the foot without confirmation using diagnostic analgesia. Clubfoot conformation appears to be better tolerated in Thoroughbred (TB) than in Standardbred (STB) racehorses.
Fetlock Height
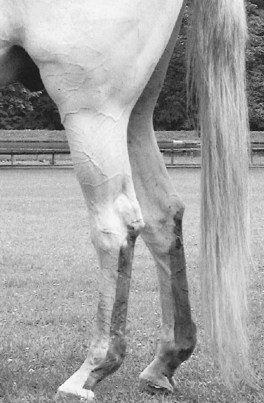
Fetlock position should be assessed in the standing horse and during movement. In a standing horse, fetlock height should be symmetrical, assuming the horse is loading the limbs equally. Horses with severe lameness commonly “point” or hold the limb in front of the opposite forelimb, thus taking weight off the limb. This standing posture obviously causes disparity in fetlock height but should be carefully interpreted. Loss of support of a fetlock in the standing horse causes the affected fetlock to drop and occurs most commonly with acute, traumatic disruption of the suspensory apparatus in racehorses but also appears with chronic, active desmitis (Figure 5-2). Severe superficial digital flexor tendonitis or lacerations resulting in fiber damage of the deep or superficial digital flexor tendons can cause similar clinical signs.

Fig. 5-2 Standardbred racehorse with severe suspensory desmitis and a “dropped fetlock.” The level of the right front fetlock joint is lower than that of the left front, caused by chronic, severe desmitis. Similar clinical signs and severe lameness appear in horses with acute traumatic disruption of the suspensory apparatus.
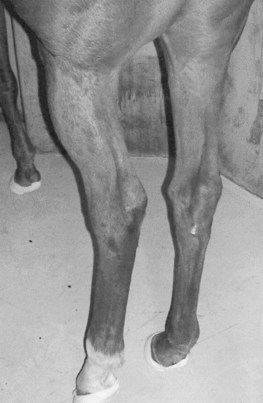
In horses with mild flexural deformity of the metacarpophalangeal joint, dynamic knuckling (buckling forward, flexion) of the fetlock joint may occur in the standing position (Figure 5-3). Joint position usually returns to normal during movement. In horses with severe flexural deformity, normal fetlock position is never achieved. Knuckling of the fetlock also may result from desmitis of the accessory ligament of the deep digital flexor tendon.

Fig. 5-3 Knuckling forward of the right front fetlock joint occurs in a standing position in this horse with mild flexural deformity of the metacarpophalangeal joint. This dynamic instability abates somewhat when the horse moves, but the left front fetlock also is straight, indicating the presence of bilateral flexural deformity.
Scapular Height
Disparity in scapular height is a rare clinical sign in a lame horse. The veterinarian must stand behind and above the horse to observe scapular height. The horse’s mane may obscure observation from a distance, requiring closer examination by palpation. Traumatic or neurological conditions affect scapular height, causing either injury or dysfunction of the serratus ventralis muscle, respectively. With both conditions the dorsal aspect of the scapula is higher on the affected side. The veterinarian may place pieces of white tape or other suitable markers on both sides of the horse and stand back to compare height or may use two assistants to point to the locations. Horses may have disparity in scapular height unrelated to the current lameness condition if there has been resolution of the original injury or neurological problem. Care must be taken to differentiate between genuine differences in the height of each scapula and asymmetrical musculature, which occurs much more commonly and may be an incidental observation. Horses with disparity in scapular height or asymmetrical muscle development may have problems with saddle fit.
Hindlimb Symmetry
Muscle Atrophy
Asymmetry of bone and muscle mass in the hindlimbs and pelvis is a common clinical sign but must be differentiated carefully. The horse should stand squarely on a flat, even surface. The clinician must determine whether asymmetry exists, and if so, if the problem involves muscle, bone, or a combination of the tissues. Muscle atrophy is most common and, if unilateral muscle atrophy exists, easily can be confused with bony asymmetry caused by pelvic fractures or asymmetry of the tubera sacrale.
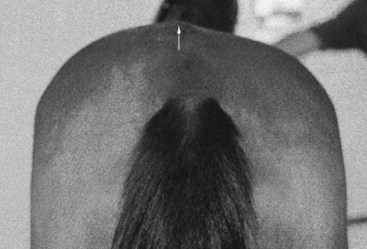
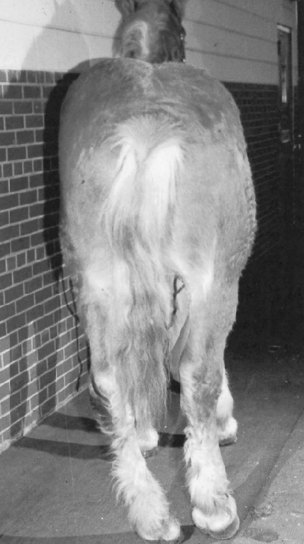
Disuse and neurogenic muscle atrophy occur in the hindlimb. Horses with chronic hindlimb lameness develop ipsilateral gluteal muscle atrophy, but asymmetry may be subtle. Mild muscle atrophy usually first appears just lateral to a tuber sacrale. The veterinarian should differentiate muscle atrophy from disparity in height of the tubera sacrale (Figure 5-4). Recognition of muscle atrophy helps determine the lame leg and provides some information about the duration of the problem. Severe muscle atrophy develops in horses with long-standing, severe lameness or in those with neurological disease (Figure 5-5).
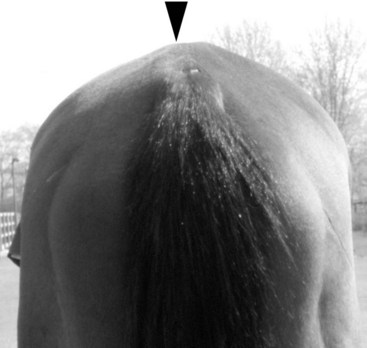
Fig. 5-4 Three-year-old Thoroughbred filly with subtle disparity in tubera sacrale height. The left tuber sacrale is slightly lower (arrow) than the right, caused by a fracture at the base of the tuber sacrale. This clinical finding can easily be missed or confused with mild muscle atrophy.
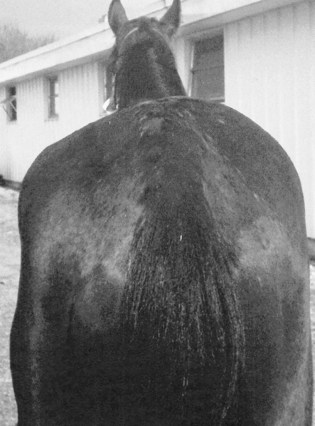
Fig. 5-5 A 4-year-old Standardbred with severe left gluteal atrophy caused by neurological disease. The presumptive clinical diagnosis was equine protozoal myelitis.
In horses with neurogenic atrophy of the gluteal muscles the degree of muscle loss is inappropriately severe compared with observed lameness. Neurological signs such as weakness and proprioceptive deficits usually appear in horses with neurogenic atrophy, but early in the course of diseases such as equine protozoal myelitis (EPM) the only observable signs may be muscle atrophy and mild lameness.
Selective atrophy of individual muscles or muscle groups occurs in horses with neurological disease or injuries causing focal muscle loss and scarring. Horses with trauma involving fracture of the tubera ischii may develop focal muscle loss of the semitendinosus or semimembranosus muscles. A depression, sometimes subtle, resulting from localized muscle atrophy replaces initial swelling of the point of the rump. Horses with fibrotic myopathy, which in most horses is believed to result from injury and scarring of the semitendinosus muscle, usually have palpable scars or defects of the caudal thigh muscles. Degenerative neuropathy of the nerves supplying the distal aspect of the semitendinosus muscle also may cause fibrotic myopathy1 (see Chapter 48).
Swelling
Swelling is especially important in horses with acute, severe lameness when the clinician must differentiate between catastrophic injury, such as pelvic or long bone fracture, and more common conditions, such as cellulitis. Horses with pelvic fractures may develop mild swelling in the thigh, but swelling is not prominent in most horses. In horses with fracture of a tuber coxae or ilial wing or shaft, mild swelling may develop distally but usually is not prominent. Inappropriate lameness and lack of swelling should prompt the clinician to perform a rectal examination, checking for internal asymmetry or crepitus. Horses with femoral fractures develop acute, severe swelling of the thigh, accompanied by severe lameness, instability, and often crepitus (Figure 5-6). Horses may develop severe swelling of the stifle and thigh resulting from trauma and secondary bleeding. Large stifle hematomas resemble the swelling in horses with femoral fractures, and in some horses hematomas can be confused with severe femoropatellar effusion (Figure 5-7). Excessive bleeding from subcutaneous vessels also may involve the ventral, lateral abdominal region. In horses with stifle hematoma, lameness may not be as prominent as expected, and swelling fluctuates, which is useful in differentiating this cause of lameness from femoral fractures. Generalized, diffuse soft tissue swelling appears in horses with cellulitis or lymphangitis in the hindlimb (Figure 5-8). Horses that negotiate fences such as event and timber horses are at risk for stifle-region trauma and swelling.

Fig. 5-6 A Thoroughbred broodmare with severe lameness and swelling of the left thigh caused by a comminuted femoral fracture.

Bony Asymmetry
Comparison of the height of the tubera coxae is important to determine the nature and extent of pelvic bony injury (Figure 5-9). Two assistants, one on each side of the horse, may point to the dorsal aspect of the tubera coxae, or the veterinarian may use temporary markers to compare the height. Determining the height of the tubera sacrale may be difficult and requires careful palpation to differentiate bone, ligament, and muscle asymmetry. Accurate determination may be possible only by ultrasonography. Estimating the midline-to-lateral pelvic width also aids in diagnosing acute or chronic pelvic fractures.
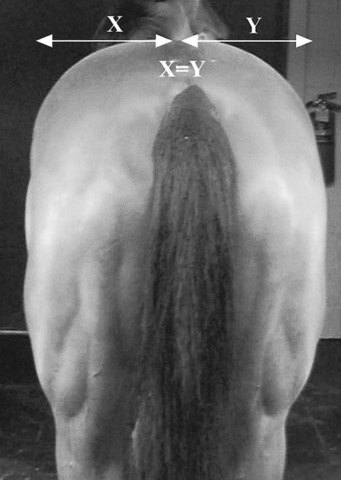
Fig. 5-9 A horse that is well positioned for determination of tubera coxae height and the midline-to-lateral pelvic width (X, Y). In a normal horse, X = Y.
Tubera Coxae
Asymmetry in height of the tubera coxae accompanies many different pelvic fractures. The most common fracture involves the tuber coxae itself, often called knocked-down hip. Marked ventral and medial displacement of the fracture fragment occurs because of muscle attachment to the bony prominence. The veterinarian also must palpate the actual shape of the tuber coxae, because ventral displacement occurs with other pelvic injuries. Displacement and rotation occur in horses with fracture of the wing of the ilium caudal to the tuber coxae without an obvious change in size or shape of the tuber coxae. However, with a partial fracture of the ventral aspect of the tuber coxae, there is a change in its shape without displacement of the dorsal aspect of the bone.
Tubera Sacrale
The term hunter’s bump describes the prominence of the tubera sacrale. This finding may reflect the horse’s conformation, poorly developed surrounding musculature, or a change in position of one or both tubera sacrale. Increase or decrease in size of the overlying dorsal sacroiliac ligament also results in apparent asymmetry. Many clinically normal horses have slight apparent asymmetry of the tubera sacrale. Asymmetry in height of the tubera sacrale occurs in horses with acute or chronic sacroiliac joint disruption (Figure 5-10). In horses with acute fractures of the base of the tubera sacrale, the affected side is lower2 (see Chapters 49 and 50). Ultrasonography and nuclear scintigraphy may help identify the cause of asymmetry.
Midline-to-Lateral Pelvic Width
A change in the relative width of each hemipelvis is a subtle but important clinical sign of pelvic injury. In most horses with pelvic fractures, the injured side is narrower than the normal side. Overriding and displacement of fracture fragments result in compression on the injured side.
Swelling over the Greater Trochanter
Mild swelling over the lateral aspect of the coxofemoral joint may be a subtle clinical sign of acetabular or proximal femoral fractures. When standing behind the horse, the veterinarian should carefully observe for enlargement over the affected hip joint. This clinical sign usually is not noticeable initially, but soft tissue enlargement is visible within 2 to 3 weeks after intraarticular fracture. The groove between the greater trochanter and the biceps femoris muscle should be compared carefully; usually a slight bulge or subtle enlargement on the affected side is visible.
Crepitus
Bone-on-bone grating is a valuable clinical sign, particularly in horses with pelvic injury. Crepitus can be heard (with or without a stethoscope) or felt (external or rectal palpation) and most often is caused by movement of bone fragments in horses with displaced fractures (see Chapter 6). In horses with pelvic fractures, crepitus usually is not observed for several days to weeks after injury because muscle tone and fracture hematoma apparently stabilize fracture fragments and delay onset. Crepitus also can be felt or heard in horses with end-stage osteoarthritis.
Calcaneus
The points of the hock should be of equal height when observed from the side or from behind. There is dramatic lowering of the point of the hock with complete disruption of the common calcaneal tendon or gastrocnemius tendon alone. Partial injury of the gastrocnemius muscle origin, the musculotendonous junction, or the tendon itself causes varying degrees of asymmetry in height of the point of the hock, both in a standing horse and during movement.3 Other gait abnormalities such as unusual rotation or instability of the limb usually are present (Figure 5-11).

Fig. 5-11 A horse with partial disruption of the left gastrocnemius. An injury to the origin of the lateral head of the gastrocnemius muscle in this horse caused an unusual gait deficit, lameness, and mild distal displacement (drop) of the hock and fetlock.
The point of the hock is elevated in horses with severe pelvic fractures involving the acetabulum, luxation of the coxofemoral joint, and some femoral fractures (Figure 5-12). Evaluating elevation is difficult because horses with severe lameness usually cannot bear weight, causing a dramatic alteration in limb position. However, in horses with true elevation in the point of the hock, the hock is extended, whereas with most non–weight-bearing conditions, the hock is flexed.
Fetlock Height
Assessment of fetlock position is as important in the hindlimb as in the forelimb. Horses with excessively straight hindlimb conformation (straight hocks) may have more obvious excursion of the fetlock (fetlock drop) while moving or shifting position during standing. Pathological fetlock drop generally accompanies suspensory desmitis (Figure 5-13) but also occurs with partial disruption of the gastrocnemius and other ligamentous and tendonous injuries.
Posture
Body posture provides important clues to the source of lameness, but some abnormalities may be missed unless the horse is observed over long periods. Normal horses tend to rest one hindlimb and may alternate between limbs. Resting a forelimb is uncommon but does occur. Distractions in the environment may make a horse stand normally despite pain. However, abnormal posture because of mechanical or neurological dysfunction usually is evident.
The horse has a well-developed stay apparatus in both the forelimbs and hindlimbs.4 It is assumed that the main purpose of the stay apparatus is to allow the horse to remain standing for long periods. The stay apparatus in the hindlimbs is better developed than in the forelimbs and includes ligamentous and tendonous structures dictating predictable movement of joints in the limb. If intact, the hindlimb stay apparatus demands reciprocal movement of the hock and stifle and often is called the reciprocal apparatus. A change in posture usually means a part of the reciprocal apparatus is broken.
Forelimb Posture
Pointing
Horses that are severely lame often point or hold the affected forelimb ahead of the unaffected forelimb, or the least affected forelimb in horses with bilateral pain. These horses usually are severely lame at a walk. Horses with severe, bilateral forelimb lameness caused by laminitis may stand camped out in front, attempting to point with both forelimbs simultaneously. However, pointing is not synonymous with the presence of pain or lameness or its degree. Some horses prefer to point one forelimb or another and walk and trot normally. In general, pointing is unusual and often signals resting pain or subtle pain relieved by adopting this posture. Some horses stack bedding under the heel of one or both front feet to stand in a toe-down position, indicating a degree of unilateral or bilateral foot pain. These horses often are not as lame as expected based on the degree of postural change seen at rest. Alternatively a horse may stand with its hindquarters “sitting” on a manger partially to unload the front feet.
Treading
Constant shifting of weight from one forelimb to the other may indicate bilateral forelimb lameness. Laminitis, severe soft tissue injuries such as tendonitis or suspensory desmitis, or severe osteoarthritis may cause treading. Horses with chronic, severe unilateral forelimb lameness often stand with little weight on the affected limb, overload the unaffected limb, and seldom tread. The development of treading in such circumstances is an ominous sign because the horse now is trying to shift weight from the previously unaffected limb, probably because of laminitis.
Buckling Forward at the Knee
Horses with bucked-knee or over-at-the-knee conformation may buckle forward at the knee while standing. In clinically normal older field hunters or other heavily used riding horses with bilateral over-at-the-knee conformation, this may be particularly obvious. The carpus is locked in extension primarily by the action of the extensor muscles. Neurological disease (e.g., EPM) affecting forelimb extensor muscles is a rare cause of buckling forward at the knee, both at rest and during movement. Specific injury of the distal aspect of the radial nerve causes similar clinical signs. In foals, rupture of the common digital extensor tendon or other extensor tendons may cause this posture (see Chapters 77 and 128).
Dropped Elbow
A dropped elbow results from failure of the triceps apparatus to maintain elbow extension (Figure 5-14) and usually results from fracture of the olecranon process. It also may result from injury to the radial nerve or brachial plexus. Similar clinical signs appear in horses with lesions of the nerve roots (neuritis, radiculopathy) or nerve cell bodies in the cervical intumescence, usually the result of lower motor neuron disease. A most unusual cause of this posture appears in horses with root signature (see the section on neck pain).
Severe Lameness of the Shoulder Region
Horses with severe shoulder pain may stand with the affected limb more caudal than usual (Figure 5-15) and often drag the limb with even the slightest movement. This posture is similar to dropped-elbow posture, but in horses with a dropped elbow the limb is held at, or even slightly cranial to, the expected position.

Fig. 5-15 Forelimb posture in a foal with osteomyelitis (scapula) and infectious arthritis (shoulder joint). With severe lameness of the shoulder or bicipital bursa, horses are reluctant to stand or move normally and often hold the limb caudally. This posture may be difficult to differentiate from that seen with loss of the triceps apparatus (see Figure 5-14).
Neck Pain
Horses with neck pain often hold the head and neck lower than expected, at a level equal to or slightly lower than the withers (Figure 5-16). Historically some horses may be observed to get caught in this position. In horses with severe pain, muscle tremors or spasms are visible, especially when one approaches the horse or the horse moves; the horse may stand in a guarded position. The horse may be reluctant to turn or move and may be unable or unwilling to eat food from either the ground or an elevated position. An unusual but characteristic sign of neck pain is posturing of a single forelimb, usually on the side of the lesion. The limb is held extended or pointed in front of the other forelimb; rarely the limb is held in slight flexion (see Figure 53-10, A). This sign appears in dogs with cervical pain, most commonly from intervertebral disk disease, and is termed root signature.5,6 Pain associated with the nerve roots supplying the brachial plexus may be the cause. Such a posture has also been seen in a horse with a mediastinal abscess. Some horses with cervical pain also have unilateral forelimb lameness.7

Hindlimb Posture
Resting a Hindlimb
Normally a horse rests one hindlimb or another, but immediate resting of a hindlimb after work, or a combination of resting of the hindlimb and trembling in the flank or stifle region, may indicate lameness. Resting of the hindlimb, particularly with trembling of the quadriceps muscles, often prompts handlers to erroneously assume the horse has stifle region pain. Horses with hindlimb pain from other locations will often assume this posture.
Abnormal Tail Position
Horses may carry the tail in an abnormal position during movement, often alerting an observer to possible hindlimb pain. The tail usually is carried away from the lame limb, but this finding is inconsistent. Horses seldom have an abnormal tail posture at rest unless the tail has been traumatized or set or there is severe hindlimb lameness.
External Rotation of the Hindlimb
Cow-hocked conformation is common, but unilateral external rotation may reflect pelvic injury (Figure 5-17). The veterinarian should verify this change in posture by moving and reevaluating the horse. Horses with pronounced unilateral external rotation usually have fractures of the acetabulum or the proximal aspect of the femur but may have nonarticular ilial shaft or wing fractures.
Hindlimb Varus Posture
Horses with chronic, severe unilateral hindlimb lameness may develop varus conformation of the contralateral limb (see Figure 5-17). This posture most often appears in foals and may develop 7 to 10 days after onset of lameness.
Treading
Constant shifting of weight between the hindlimbs, or treading, is an unusual clinical sign and usually indicates pronounced bilateral lameness. Horses with bilateral hindlimb laminitis or severe osteoarthritis of any joint may tread. Horses with chronic, severe unilateral hindlimb lameness can endure 4 to 6 weeks or more of weight bearing on the contralateral limb, but treading may be the earliest sign of traumatic laminitis in the supporting limb.
Camped Under
Camped under appears only in horses with bilateral hindlimb laminitis and is rare. Horses often tread and exhibit an unusual hindlimb gait (shortened caudal phase of the stride) when moved at a walk in hand. Pain arising from the thoracolumbar region may also result in a camped under posture.
Soft Tissue Injuries Altering Hindlimb Posture 
Upward fixation of the patella causes rigid extension of all hindlimb joints in a standing horse (Figure 5-18). Patellar dysfunction resulting in fixed extension of the stifle also causes extension of the tarsus and lower limb joints because of the hindlimb reciprocal apparatus. The horse may maintain this posture during movement, or the posture may be intermittent and resolve when the horse is moved. Occasionally a horse with severe hindlimb lameness assumes a similar posture, apparently hanging the limb, but the limb is not locked in extension (Figure 5-19). Normal horses simply resting a hindlimb, or those with severe lameness, usually keep the sole facing the ground.

Fig. 5-18 A horse with the classic posture seen with upward fixation of the patella. All joints are held in rigid extension, and the horse is forced to rest or bear weight on the dorsal aspect of the hoof wall.
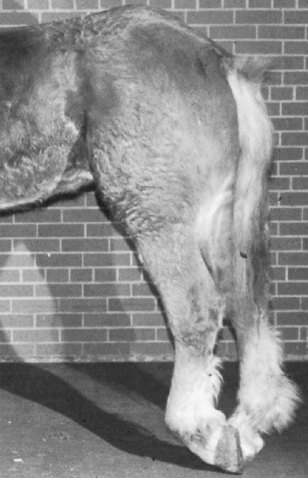
Fig. 5-19 Belgian gelding shown in Figure 5-17. This horse occasionally rested the left hindlimb in this extended position, similar to that of upward fixation of the patella. Most normal horses, or those with severe lameness, prefer to rest the limb with the sole facing the ground.
Foals with unilateral or bilateral lateral patellar luxation have an unusual crouched hindlimb posture similar to femoral nerve paresis. The foal may have difficulty in rising if the condition is bilateral and severe or long-standing.
Disruption of fibularis (peroneus) tertius allows the hock to extend abnormally during weight bearing. Foals occasionally stand excessively straight in the hock (extended) in the affected hindlimb. In foals the injury usually causes tearing at the origin of fibularis tertius from the distal aspect of the femur, but in adults injury may occur in the crus or at the distal aspect of the ligament as it courses over the hock. Swelling and excessive hock extension may occur with the latter injury (Figure 5-20). The diagnosis is confirmed by manipulation: the hock can be extended while the stifle is flexed.
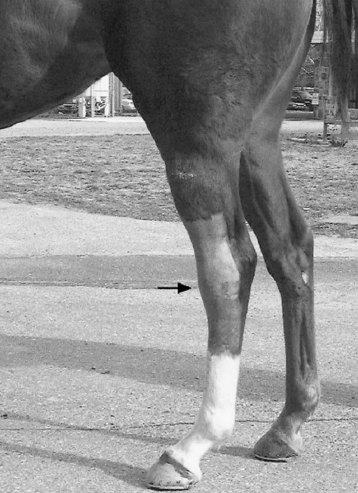
Fig. 5-20 This Thoroughbred racehorse with fibularis tertius injury has swelling over the dorsal aspect of the hock (arrow) and straight-in-the-hock conformation.
Rupture of the gastrocnemius tendon, or severe injury at any level of the muscle-tendon unit, causes mild or severe hindlimb postural change. During weight bearing, the hock flexes excessively as the stifle is held in extension, so the point of the hock drops. This injury is called disruption of the caudal component of the reciprocal apparatus.8,9
Peripheral Nerve Deficits (see Chapter 11)
Sciatic nerve damage is rare. It occurs in foals as a result of injections into the thigh or rump or may occur transiently after injection of local anesthetic solution caudal to the coxofemoral joint. Horses with sciatic nerve damage support weight but appear to be crouched behind, because innervation to the gastrocnemius, flexor, and extensor muscles causes the hock to drop and fetlock to knuckle forward. Careful observation of stifle action and the ability to support weight are useful for attempting to differentiate this deficit from femoral nerve paresis.
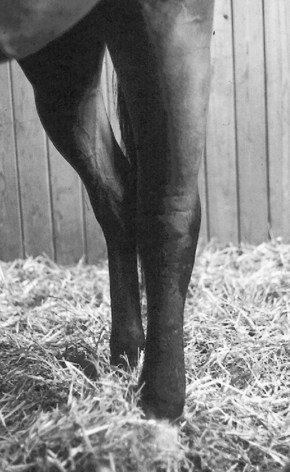
Horses with femoral nerve paresis also assume a crouched hindlimb posture but are unable to bear weight, and the stifle drops substantially (Figure 5-21). Because the reciprocal apparatus is intact, the inability to fix the stifle leads to hock flexion and knuckling (flexion) of the fetlock joint. If the condition is bilateral, the horse is unable to rise for more than a few seconds. Femoral nerve paresis may occur unilaterally or bilaterally after general anesthesia or may result from lower motor neuron disease or injury.
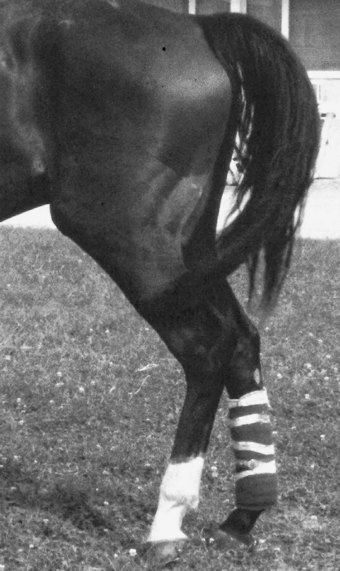
Fig. 5-21 Thoroughbred with transient, postanesthesia, unilateral (left hindlimb) femoral nerve paresis. The crouched posture of the left hindlimb includes flexion (knuckling) of the fetlock joint.
Solitary tibial nerve injury is rare. Fibular (peroneal) nerve injury usually is recognized after general anesthesia and causes characteristic knuckling of the fetlock joint. Tibial nerve injury is differentiated from sciatic injury by lack of involvement of the fibular nerve, and thus normal positioning of the hock, and from femoral nerve injury, because horses are able to support weight and fix the stifle.
A rare polyneuropathy in Norwegian horses caused unilateral or bilateral knuckling of the hindlimbs, and in some horses paraplegia occurred as a result of peripheral injury of the sciatic nerves.10 A common epidemiological factor in all horses was the feeding of big bale silage or hay of poor quality.10 I have seen similar clinical signs in a Warmblood gelding, which developed acute, severe, bilateral hindlimb knuckling (at the fetlock) that resolved completely several days after onset. The cause in this horse was not determined.
Other Unusual Leg Positions
Horses with severe lameness occasionally rest a hindlimb back, forward, or abducted. Often these positions also are maintained during movement. Horses with caudal thigh or pelvic pain prefer to keep the affected hindlimb back, behind the unaffected limb. Horses with shivers may stand with the limb slightly abducted and more caudal than expected, with elevation of the tail head (see Chapter 48).
Stance in Horses with Pelvic Fractures and Conditions Affecting the Coxofemoral Region
Horses with pelvic fractures, in particular those involving the acetabulum, or other severe conditions involving the coxofemoral joint often stand with the limb slightly forward and often are reluctant to place the limb behind the unaffected limb, thus reducing the caudal phase of the stride at the walk. In addition, horses will often stand with the limb externally rotated, and in the rare instance there is coxofemoral luxation, the point of the hock of the affected limb will be slightly proximal to the contralateral point of the hock (see Figure 5-17). I find it interesting that children with infectious arthritis of the coxofemoral joint will often hold the affected hip in flexion, abduction, and external rotation,11,12 remarkably similar to those clinical signs seen in the horse. Horses with pain in the medial thigh and groin area stand with the limb abducted and may travel in this manner. Adductor muscle damage, medial thigh abscessation, and scirrhous cord or other inguinal problems also cause this posture.