The Child with Cerebral Dysfunction
On completion of this chapter the reader will be able to:
 Describe the various modalities for assessment of cerebral function.
Describe the various modalities for assessment of cerebral function.
Differentiate between the stages of consciousness.
Formulate a care plan for the unconscious child.
Distinguish between the types of head injuries and the serious complications.
Describe the nursing care of a child with a tumor of the central nervous system.
Outline a care plan for the child with bacterial meningitis.
Differentiate between the various types of seizure disorders.
Demonstrate an understanding of the manifestations of a seizure disorder and the management of a child with such a disorder.
Describe the preoperative and postoperative care of a child with hydrocephalus.
RELATED TOPICS and ADDITIONAL RESOURCES
 IN TEXT
IN TEXTAdministration of Medication, Ch. 22
Childhood Mortality, Ch. 1
Family-Centered Care of the Child During Illness and Hospitalization, Ch. 21
Family-Centered Home Care, Ch. 20
Immunizations, Ch. 10
Impact of Chronic Illness or Disability on the Child, Ch. 18
Infection Control, Ch. 22
Maintaining Healthy Skin, Ch. 22
Neurologic Assessment, Ch. 6
Pain Assessment; Pain Management, Ch. 7
Preparation for Diagnostic and Therapeutic Procedures, Ch. 22
CEREBRAL DYSFUNCTION
Most of the information about the status of the brain is obtained by indirect measurements. Some of these measurements are discussed elsewhere in relation to numerous aspects of childcare (e.g., as part of assessments of health [Chapter 6], newborn status [Chapter 8], intellectual disability [Chapter 19], hypoxic injury [cerebral palsy, Chapter 32], and attainment of developmental milestones at each stage of development). Since increased intracranial pressure (ICP) and altered states of consciousness have such prominent places in neurologic dysfunction, they are described here, followed by techniques for neurologic assessment and diagnostic tests.
GENERAL ASPECTS
Children younger than 2 years of age require special evaluation, since they are unable to respond to directions designed to elicit specific neurologic responses. Early neurologic responses in infants are primarily reflexive; these responses are gradually replaced by meaningful movement in the characteristic cephalocaudal direction of development. This evidence of progressive maturation reflects more extensive myelinization and changes in neurochemical and electrophysiologic properties.
Most information about infants and small children is gained by observing their spontaneous and elicited reflex responses as they develop increasingly complex locomotor and fine motor skills and by eliciting progressively sophisticated communicative and adaptive behaviors. Delay or deviation from expected milestones helps identify high-risk children. Persistence or reappearance of reflexes that normally disappear indicates a pathologic condition. In evaluating the infant or young child, it is also important to obtain the pregnancy and delivery history to determine the possible impact of intrauterine environmental influences known to affect the orderly maturation of the central nervous system (CNS). These influences include maternal infections, chemicals, trauma, and metabolic insults.
General aspects of assessment that provide clues to the etiology of dysfunction include:
Family history—Sometimes offers clues regarding possible genetic disorders with neurologic manifestations
Health history—May provide valuable clues regarding the cause of dysfunction (e.g., an injury, short febrile illness, encounter with an animal or insect, ingestion of neurotoxic substances, inhalation of chemicals, a past illness, or known diabetes mellitus)
Physical evaluation of infants—Includes observation of:
Spontaneous activity and postural reflex activity
Attitude—normal flexed posture, extreme extension, opisthotonos, hypotonia
Symmetry in movement of extremities
Excessive tremulousness or frequent twitching movements
Altered expiratory cycle—prolonged apnea, ataxic breathing, paradoxic chest movement, and hyperventilation
Asymmetric contraction of facial muscles
Yawning (may indicate cranial nerve involvement)
INCREASED INTRACRANIAL PRESSURE
The brain, tightly enclosed in the solid bony cranium, is well protected but highly vulnerable to pressure that may accumulate within the enclosure. The cranium’s total volume—brain (80%), cerebrospinal fluid (CSF) (10%), and blood (10%)–must remain approximately the same at all times. A change in the proportional volume of one of these components (e.g., increase or decrease in intracranial blood) must be accompanied by a compensatory change in another. In this way the volume and pressure normally remain constant. Examples of compensatory changes are reduction in blood volume, decrease in CSF production, increase in CSF absorption, or shrinkage of brain mass by displacement of intracellular and extracellular fluid. Children with open fontanels compensate by skull expansion and widened sutures. However, at any age the capacity for spatial compensation is limited. An increase in ICP may be caused by tumors or other space-occupying lesions, accumulation of fluid within the ventricular system, bleeding, or edema of cerebral tissues. Once compensation is exhausted, any further increase in volume will result in a rapid rise in ICP.
Early signs and symptoms of increased ICP are often subtle and assume many patterns (Box 28-1). As pressure increases, signs and symptoms become more pronounced and the level of consciousness (LOC) deteriorates.
ALTERED STATES OF CONSCIOUSNESS
Consciousness implies awareness—the ability to respond to sensory stimuli and have subjective experiences. There are two components of consciousness: alertness, an arousal-waking state, including the ability to respond to stimuli; and cognitive power, including the ability to process stimuli and produce verbal and motor responses.
An altered state of consciousness usually refers to varying states of unconsciousness that may be momentary or may extend for hours, for days, or indefinitely. Unconsciousness is depressed cerebral function—the inability to respond to sensory stimuli and have subjective experiences. Coma is defined as a state of unconsciousness from which the patient cannot be aroused even with powerful stimuli.
Levels of Consciousness
Assessment of LOC remains the earliest indicator of improvement or deterioration in neurologic status. LOC is determined by observations of the child’s responses to the environment. Other diagnostic tests, such as motor activity, reflexes, and vital signs, are more variable and do not necessarily directly parallel the depth of the comatose state. The most consistently used terms are described in Box 28-2.
Coma Assessment
Several scales have been devised in an attempt to standardize the description and interpretation of the degree of depressed consciousness. The most popular of these is the Glasgow Coma Scale (GCS), which consists of a three-part assessment: eye opening, verbal response, and motor response (Fig. 28-1). When LOC is being assessed in young children, it is often useful to have a parent present to help elicit a desired response. An infant or child may not respond in an unfamiliar environment or to unfamiliar voices. Children older than 3 years of age should be able to give their name, although they may not be cognizant of place or time.
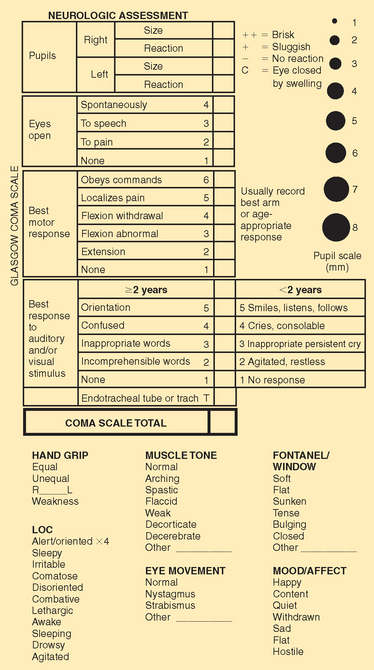
Numeric values of 1 through 5 are assigned to the levels of response in each category. The sum of these numeric values provides an objective measure of the patient’s LOC. The lower the score, the deeper the coma. A person with an unaltered LOC would score the highest, 15; a score of 8 or below is generally accepted as a definition of coma; the lowest score, 3, indicates deep coma. The Task Force for the Determination of Brain Death in Children has established physical examination criteria for cases of irreversible coma (1987).
NEUROLOGIC EXAMINATION
The purpose of the neurologic examination is to establish an accurate, objective baseline of neurologic information. It is essential that the neurologic examination be documented in a fashion that is able to be reproduced by others. This allows for a comparison of the findings so the observer can detect subtle changes in the neurologic status that might not otherwise be evident. Descriptions of behaviors should be simple, objective, and easily interpreted: “Drowsy but awake and conversationally rational/oriented”; “Sleepy but arousable with vigorous physical stimuli. Pressure to nail base of right hand results in upper extremity flexion/lower extremity extension.”
Vital Signs
Pulse, respiration, and blood pressure provide information regarding the adequacy of circulation and the possible underlying cause of altered consciousness. Autonomic activity is most intensively disturbed in cases of deep coma or brainstem lesions.
Body temperature is often elevated, and sometimes the elevation may be extreme. High temperature is most frequently a sign of an acute infectious process or heat stroke but may be caused by ingestion of some drugs (especially salicylates, alcohol, and barbiturates) or by intracranial bleeding, especially subarachnoid hemorrhage. Hypothalamic involvement may cause elevated or decreased temperature. Coma of a toxic origin may produce hypothermia.
The pulse is variable and may be rapid, slow and bounding, or feeble. Blood pressure may be normal, elevated, or at shock levels. The Cushing reflex, or pressor response, which causes a slowing of the pulse and an increase in blood pressure, is uncommon in children; when it occurs, it is a very late sign of ICP. Vital signs are also affected by medications. For assessment purposes, actual changes in pulse and blood pressure are more important than the direction of the change.
Respirations are often slow, deep, and irregular. Slow, deep breathing is often seen in the heavy sleep caused by sedatives, after seizures, or in cerebral infections. Slow, shallow breathing may result from sedatives or opioids (narcotics). Hyperventilation (deep and rapid respirations) is usually a result of metabolic acidosis or abnormal stimulation of the respiratory center in the medulla caused by salicylate poisoning, hepatic coma, or Reye syndrome (RS).
Breathing patterns have been described with a number of terms (e.g., apneustic, cluster, ataxic, Cheyne-Stokes). However, it is better to describe what is being observed rather than placing a label on it because the traditional terms are often used and interpreted incorrectly. Periodic or irregular breathing is an ominous sign of brainstem (especially medullary) dysfunction that often precedes complete apnea. The odor of the breath may provide additional clues (e.g., the fruity, acetone odor of ketosis; the foul odor of uremia; the fetid odor of hepatic failure; or the odor of alcohol).
Skin
The skin may offer clues to the cause of unconsciousness. The body surface should be examined for signs of injury, needle marks, petechiae, bites, and ticks. Evidence of toxic substances may be found on the hands, face, mouth, and clothing—especially in small children.
Eyes
Pupil size and reactivity are assessed (Fig. 28-2; see also Fig. 28-1). Pinpoint pupils are commonly observed in poisoning, such as opiate or barbiturate poisoning, or in brainstem dysfunction. Widely dilated and reactive pupils are often seen after seizures and may involve only one side. Dilated pupils may also be caused by eye trauma. Widely dilated and fixed pupils suggest paralysis of cranial nerve III secondary to pressure from herniation of the brain through the tentorium. A unilateral fixed pupil usually suggests a lesion on the same side. If pupils are fixed bilaterally for more than 5 minutes, brainstem damage is usually implied. Dilated and nonreactive pupils are also seen in hypothermia, anoxia, ischemia, poisoning with atropine-like substances, or prior instillation of mydriatic drugs.
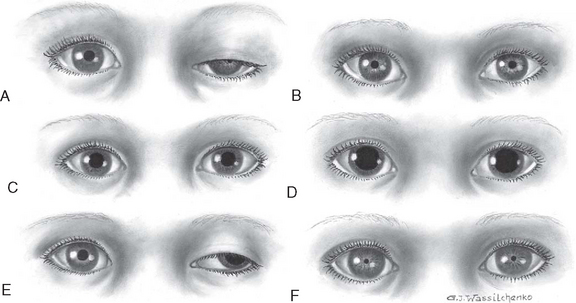
FIG. 28-2 Variations in pupil size with altered states of consciousness. A, Ipsilateral pupillary constriction with slight ptosis. B, Bilateral small pupils. C, Midposition, light fixed to all stimuli. D, Bilateral dilated and fixed pupils. E, Dilated pupils, left eye abducted with ptosis. F, Pinpoint pupils.
The description of eye movements should indicate whether one or both eyes are involved and how the reaction was elicited. The parents should be asked about preexisting strabismus, which will cause the eyes to appear normal under compromise. Posttraumatic strabismus indicates cranial nerve VI damage.
Special tests, usually performed by qualified persons, include:
Doll’s head maneuver—Elicited by rotating the child’s head quickly to one side and then to the other. Conjugate (paired or working together) movement of the eyes in the direction opposite to the head rotation is normal. Absence of this response suggests dysfunction of the brainstem or oculomotor nerve (cranial nerve III).
Caloric test, or oculovestibular response—Elicited with the child’s head up (head of bed is elevated 30 degrees) by irrigating the external auditory canal with 10 ml of ice water for 20 seconds, which normally causes conjugate movement of the eyes toward the side of stimulation. This movement is lost when the pontine centers are impaired, thus providing important information in assessment of the comatose patient.
Funduscopic examination—Reveals additional clues. Papilledema will not be evident early in the course of unconsciousness because it takes 24 to 48 hours to develop, if it develops at all. Papilledema is characterized by optic disc swelling, indistinct optic disc margins, hemorrhage, tortuosity of vessels, and absence of venous pulsations. The presence of preretinal (subhyaloid) hemorrhages in children is almost invariably a result of acute trauma with intracranial bleeding, usually subarachnoid or subdural hemorrhage.
Motor Function
Observing spontaneous activity, posture, and response to painful stimuli provides clues to the location and extent of cerebral dysfunction. Even subtle movements (e.g., the outward rotation of a hip) should be noted and the child observed for other signs. Asymmetric movements of the limbs or absence of movement suggests paralysis. In hemiplegia the affected limb lies in external rotation and will fall uncontrollably when lifted and allowed to drop. These observations should be described rather than labeled.
In the deeper comatose states there is little or no spontaneous movement, and the musculature tends to be flaccid. There is considerable variability in the motor behavior in lesser degrees of coma. For example, the child may be relatively immobile or restless and hyperkinetic; muscle tone may be increased or decreased. Tremors, twitching, and spasms of muscles are common observations. The patient may display purposeless plucking or tossing movements. Combative or negativistic behavior is not uncommon. Hyperactivity is more common in acute febrile and toxic states than in cases of increased ICP. Seizures are common in children and may be present in coma from any cause. Any repetitive or seizure movements should be described.
Posturing
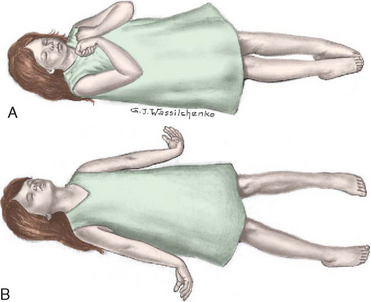
Primitive postural reflexes emerge as cortical control over motor function is lost in brain dysfunction. These reflexes are evident in posturing and motor movements directly related to the area of the brain involved. Posturing reflects a balance between the lower exciting and the higher inhibiting influences, and strong muscles overcome weaker ones. Flexion posturing (Fig. 28-3, A) is seen with severe dysfunction of the cerebral cortex or with lesions to corticospinal tracts above the brainstem. Typical flexion posturing includes rigid flexion, with arms held tightly to the body; flexed elbows, wrists, and fingers; plantar flexed feet; legs extended and internally rotated; and possibly presence of fine tremors or intense stiffness. Extension posturing (see Fig. 28-3, B) is a sign of dysfunction at the level of the midbrain or lesions to the brainstem. It is characterized by rigid extension and pronation of the arms and legs, flexed wrists and fingers, clenched jaw, extended neck, and possibly an arched back. Unilateral extension posturing is often caused by tentorial herniation.
Posturing may not be evident when the child is quiet but can usually be elicited by applying painful stimuli, such as a blunt object pressed on the base of the nail. Nurses should avoid applying thumb pressure to the supraorbital region of the frontal bone (risk of orbital damage). Noxious stimuli (e.g., suctioning) will elicit a response, as may turning or touching. When the nurse is describing posturing, the stimulus needed to provoke the response is as important as the reaction.
Reflexes
Testing of some reflexes may be of limited value. In general, the corneal, pupillary, muscle-stretch, superficial, and plantar reflexes tend to be absent in deep coma. The state of reflexes is variable in lighter grades of unconsciousness and depends on the underlying pathologic process and the location of the lesion. Absence of corneal reflexes and presence of a tonic neck reflex are associated with severe brain damage. The Babinski reflex (see Extremities, Chapter 6) may be of value if it is found to be present consistently in children older than 18 months. A positive Babinski reflex is significant in assessment of pyramidal tract lesions when it is unilateral and associated with other pyramidal signs.
SPECIAL DIAGNOSTIC PROCEDURES
Numerous diagnostic procedures are used for assessment of cerebral function. Laboratory tests that may help delineate the cause of unconsciousness include blood glucose, urea nitrogen, and electrolyte (pH, sodium, potassium, chloride, calcium, and bicarbonate) tests; clotting studies, hematocrit, and a complete blood count; liver function tests; blood cultures if there is fever; and sometimes studies to detect lead or other toxic substances, such as drugs.
An electroencephalogram (EEG) may provide important information. For example, generalized random, slow activity suggests suppressed cortical function, and localized slow activity suggests a space-occupying lesion. A flat tracing is one of the criteria used as evidence of brain death.
Examination of spinal fluid is carried out when toxic encephalopathy or infection is suspected. Lumbar puncture is ordinarily delayed if intracranial hemorrhage is suspected and is contraindicated in the presence of ICP because of the potential for tentorial herniation.
Auditory and visual evoked potentials are sometimes used in neurologic evaluation of very young children. Brainstem auditory evoked potentials are useful for evaluating the continuity of brainstem auditory tracts and are particularly useful for detecting demyelinating disease and neoplasms of the brainstem and distinguishing between brainstem and cortical lesions. For example, a normal evoked potential in a comatose patient suggests involvement of the cerebral hemispheres.
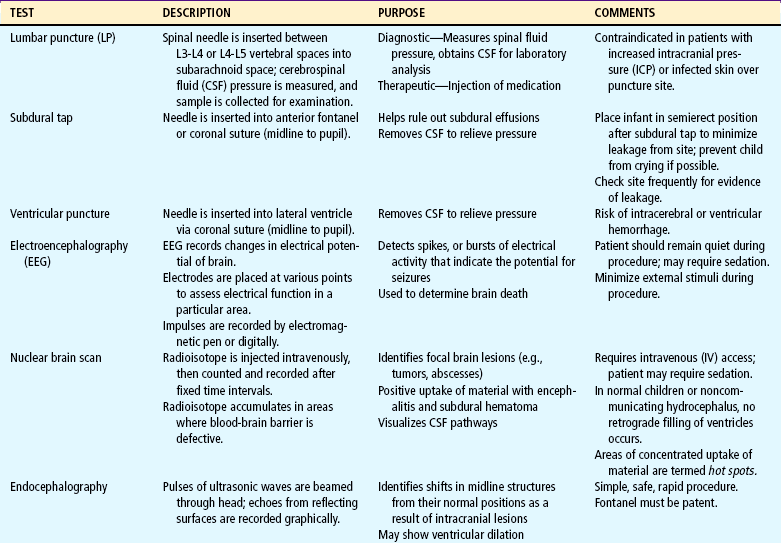
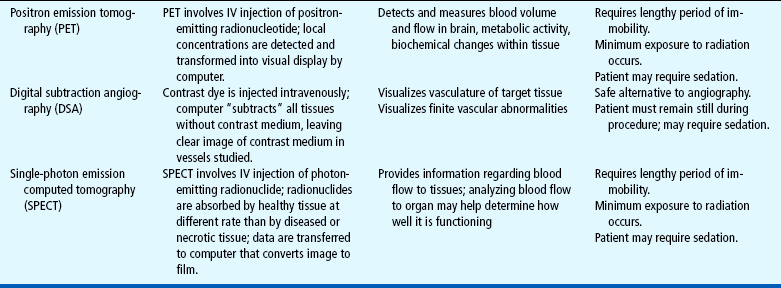
Highly sophisticated tests are carried out with specialized equipment. Two imaging techniques, computed tomography (CT) and magnetic resonance imaging (MRI), assist in diagnosis by scanning both soft tissues and solid matter. Most of these tests are outlined in Table 28-1. Because such tests can be threatening to children, the nurse needs to prepare patients for the tests and provide support and reassurance during the tests (see Preparation for Diagnostic and Therapeutic Procedures, Chapter 22). Children who are old enough to understand require careful explanation of the procedure, why it is being done, what they will experience, and how they can help. School-age children usually appreciate a more detailed description of why contrast material is injected. The importance of lying still for tests, particularly CT, needs to be stressed. Children unfamiliar with the machines can be shown a picture beforehand. Although radiographic examinations are not painful, the machinery is often so frightening in appearance that the child protests because of anxiety.
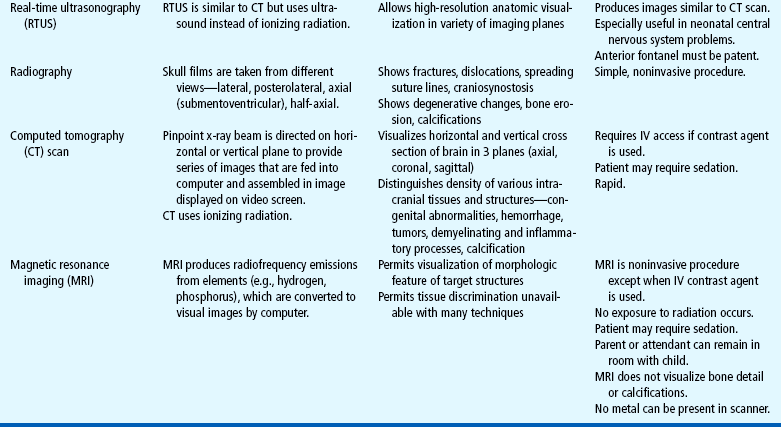
This is especially true of CT and MRI, both of which require that the child’s head be placed within a special immobilizing device. Chin and cheek pads are sometimes used to prevent the slightest head movement, and straps are applied to the body to prevent a slight change in body position. The nurse can explain these events to a frightened child by comparing them to an astronaut’s preparation for a space flight. It is important to emphasize to the child that at no time is the procedure painful.
The nurse should not expect cooperation from a young child. Sedation may be required. Many different agents are currently used for sedation of children undergoing neurologic diagnostic procedures. Chloral hydrate or benzodiazepines have been used for decades as short-term sedative agents and remain safe methods of pediatric outpatient sedation (Kao, Adamson, Tatman, and others, 1999; Wetzell, 2007). Chloral hydrate is used alone for sedating children for procedures such as MRI. In recent years other sedative agents have been used safely, alone and in combination, for children in the outpatient setting. These include intravenous (IV) sodium pentobarbital (Nembutal), IV fentanyl (Sublimaze), IV midazolam (Versed) (Wetzell, 2007), and intranasal midazolam (Ljungman, Kreuger, Andreasson, and others, 2000; Lloyd, Alredy, and Lloyd, 2000). (See Pain Management, Chapter 7.)
Physical preparation for the diagnostic test may involve administration of a sedative. If so, children should be helped through the preparation and administration and assured that someone will remain with them (if possible). Children need continual support and reinforcement during procedures in which they remain conscious. Vital signs and physiologic responses to the procedure are monitored throughout. Many diagnostic procedures performed on an outpatient basis require sedation, and children need recovery time and observation. The nurse should review written instructions with parents if the child is discharged after a procedure. Children who have undergone a procedure with a general anesthetic require postanesthesia care, including positioning to prevent aspiration of secretions and frequent assessment of the vital signs and LOC. In addition, other neurologic functions such as pupillary responses, motor strength, and movement are tested at regular intervals. Any surgical wound resulting from the test is checked for bleeding, CSF leakage, and other complications. Children who undergo repeated subdural taps should have their hematocrit monitored to detect excessive blood loss from the procedure.
NURSING CARE OF THE UNCONSCIOUS CHILD
The unconscious child requires nursing attendance, with observation, recording, and evaluation of changes in objective signs. These observations provide valuable information regarding the patient’s progress. Often they serve as a guide to diagnosis and treatment. Therefore careful and detailed observations are essential for the patient’s welfare. In addition, vital functions must be maintained and complications prevented through conscientious and meticulous nursing care. The outcome of unconsciousness may be early and complete recovery, death within a few hours or days, persistent and permanent unconsciousness, or recovery with varying degrees of residual mental or physical disability. The outcome and recovery of the unconscious child may depend on the level of nursing care and observational skills.
Emergency measures are directed toward ensuring a patent airway, treatment of shock, and reduction of ICP (if it is increased). Delayed treatment often leads to increased damage. As soon as emergency measures have been implemented—and in many cases concurrently—therapies for specific causes are begun. Because nursing care is closely related to medical management, both are considered here.
Continual observation of LOC, pupillary reaction, and vital signs is essential to manage CNS disorders. Regular assessment of neurologic signs is a vital part of nursing comatose children. Vital signs are measured and recorded regularly. The frequency depends on the cause of coma, the status, and the progression of cerebral involvement. Intervals may be as short as every 15 minutes or as long as every 2 hours. Significant alterations are reported immediately. Temperature is taken every 2 to 4 hours, depending on the patient’s condition.
An elevated temperature may occur in children with CNS dysfunction; therefore a light covering is sufficient. Vigorous efforts, such as tepid sponge baths or application of a hypothermia blanket, are needed to prevent brain damage if temperature exceeds 40° C (104° F) rectally.
The LOC is assessed periodically, including size, equality, and reaction of pupils to light. Signs of meningeal irritation such as nuchal rigidity are also assessed. Other aspects of LOC assessment include response to vocal commands, spontaneous behavior, resistance to care, and response to painful stimuli. Motions of any type, changes in muscle tone or strength, and body position are noted. Seizure activity is described according to the type and length of seizure and body areas involved. An antiepileptic drug such as phenytoin (Dilantin) or phenobarbital is ordered for control of seizure activity.
Pain management for the comatose child requires astute nursing observation and management. Signs of pain include changes in behavior (e.g., increased agitation and rigidity, alterations in physiologic parameters); increased heart rate, respiratory rate, and blood pressure; and decreased oxygen saturation. Since these findings are not specific for pain, the nurse should observe for their appearance during times of induced or suspected pain and their disappearance after the end of the inciting procedure or the administration of analgesia. A pain assessment record should be used to document indications of pain and the effectiveness of interventions (see Pain Assessment, Chapter 7).
The use of opioids, such as morphine, to relieve pain is controversial because they may mask signs of altered consciousness or depress respirations. However, unrelieved pain activates the stress response, which can elevate ICP. To block the stress response, some authorities advocate the use of analgesics, sedatives, and, in some cases such as head injury, paralyzing agents via continuous IV infusion. A frequently used combination is fentanyl, midazolam, and vecuronium (Norcuron). If there are concerns about assessing the LOC or respiratory depression, naloxone (Narcan) can be used to reverse the opioid effects. Acetaminophen and codeine may also be effective analgesics for mild to moderate pain. Regardless of which drugs are used, adequate dosage and regular administration are essential to provide optimal pain relief (see Pain Management, Chapter 7).
Other measures to relieve discomfort include providing a quiet, dimly lit environment; limiting visitors; preventing any sudden, jarring movement, such as banging into the bed; and preventing an increase in ICP. The last is most effectively achieved by proper positioning and prevention of straining, such as during coughing, vomiting, or defecating.
RESPIRATORY MANAGEMENT
Respiratory effectiveness is the primary concern in the care of the unconscious child, and establishment of an adequate airway is always the first priority. Carbon dioxide has a potent vasodilating effect and will increase cerebral blood flow (CBF) and ICP. Cerebral hypoxia that lasts longer than 4 minutes nearly always causes irreversible brain damage.
Children in lighter states of coma may be able to cough and swallow, but those in deeper states are unable to handle secretions, which tend to pool in the throat and pharynx. Dysfunction of cranial nerves IX and X places the child at risk for aspiration and cardiac arrest; therefore the child is positioned to prevent aspiration of secretions, and the stomach is emptied to reduce the likelihood of vomiting. In infants, blockage of air passages from secretions can happen in seconds. In addition, upper airway obstruction from laryngospasm is a frequent complication in comatose children.
An oral airway can be used for the child who is suffering a temporary loss of consciousness, such as after a contusion, seizure, or anesthesia. For children who remain unconscious for a longer time, a nasotracheal or orotracheal tube is inserted to maintain the open airway and facilitate removal of secretions. A tracheostomy is performed in cases in which laryngoscopy for introduction of an endotracheal tube would be difficult or dangerous. Suctioning is used only as needed to clear the airway, exerting care to prevent increasing ICP. Respiratory status is observed and evaluated regularly. Signs of respiratory embarrassment may be an indication for ventilatory assistance.
When the respiratory center is involved, mechanical ventilation is usually indicated (see Chapter 22). Blood gas analysis is performed regularly, and oxygen is administered when indicated. Moderately severe hypoxia and respiratory acidosis are often present but are not always evident from clinical manifestations. Hyperventilation frequently accompanies unconsciousness and may lead to respiratory alkalosis, or it may represent the body’s attempt to compensate for metabolic acidosis. Therefore blood gas and pH determinations are essential guides for electrolyte therapy. Chest physiotherapy is carried out on a regular basis, and the child’s position is changed at least every 2 hours to prevent pulmonary complications.
INTRACRANIAL PRESSURE MONITORING
Management of the child with increased ICP is possibly the most formidable task and the most controversial subject in pediatric critical care. It appears that the outcome in pediatric neurologic injury may reflect the initial cerebral damage more than the subsequent intracranial hypertension. Of note, ICP gives little indication of the severity of the initial insult (Bayir, Kochanek, and Clark, 2003).
When increased ICP is a result of accumulation of CSF from obstruction of CSF flow, a ventricular tap will provide relief quickly and effectively. Evacuation of a hematoma reduces pressure from this source. Indications for inserting an ICP monitor are as follows:
GCS evaluation of less than 8 with respiratory assistance
Subjective judgment regarding clinical appearance and response
Four major types of ICP monitors are
1. Intraventricular catheter with fibroscopic sensors attached to a monitoring system
Transducers for both ventricular and subarachnoid monitoring should be set up without the use of a flush device. Direct ventricular pressure measurement remains the gold standard of ICP monitoring.
The catheter method involves introduction of a catheter into the lateral ventricle on the nondominant side, if known, or placement in the subdural space. The catheter has the advantage of providing a means of extraventricular (or continuous) drainage to reduce pressure. A drainage bag attached to the system is kept at the level of the ventricles and can be lowered to decrease ICP (see Critical Thinking Exercise).
With the bolt method the end of the bolt is placed into the subarachnoid space. The bolt cannot be adequately secured in a small child’s pliant skull, although special modifications have been developed for children younger than 6 years of age.
The placement of the bolt is not adjusted by anyone except the neurosurgeon who placed the device. The neurosurgeon is notified if a satisfactory waveform is not observed.
An epidural sensor can be placed between the dura and the skull through a burr hole and connected to a stopcock assembly and a transducer, which provides a readout of the pressure. Correlation of pressure readings is less invasive but may be inconsistent. In infants a fontanel transducer can be used to detect impulses from a pressure sensor and convert them to electrical energy. The electrical energy is then converted to visible waves or numeric readings on an oscilloscope. ICP measurement from the anterior fontanel is noninvasive but may prove to be inaccurate if the equipment is poorly placed or inconsistently recalibrated. The intraparenchymal pressure monitoring device (e.g., Camino) is a result of fiberoptic technology and performs reliably.
ICP can be increased by instillation of solutions; therefore antibiotics are administered systemically if a positive CSF culture is obtained. However, IV ICP monitoring rarely causes infection. Since CSF is a body fluid, standard precautions are implemented according to hospital policy (see Infection Control, Chapter 22).
Nurses caring for patients with intracranial monitoring devices must be acquainted with the system, assist with insertion, interpret the monitor readings, and be able to distinguish between danger signals and mechanical dysfunction.
 CRITICAL THINKING EXERCISE
CRITICAL THINKING EXERCISEThree-year-old Emma is 5 days postoperative for removal of a posterior fossa tumor. Although an external ventricular drain (EVD) was placed to treat her hydrocephalus, she continues to demonstrate signs of increased intracranial pressure (ICP), including holding the back of her head, anorexia, crying when moved or when strangers enter the room, and intermittent lethargy. On examination, fluid drainage is noted on the mother’s clothes, and Emma is experiencing repetitive, rapid eyelid blinking.
1. Evidence—Is there sufficient evidence to draw conclusions about Emma’s behavior, physical assessment findings, and ICP?
2. Assumptions—Describe any underlying assumption about each of the following:
a. A preschool-age child who had a posterior fossa tumor removed 5 days ago
b. A preschool-age child who has an EVD placed to treat the hydrocephalus
c. A preschool-age child with an EVD who continues to demonstrate physical signs associated with increased ICP after recent surgery
3. What priorities for nursing care should be established?
For increased ICP resulting from cerebral edema, several medical measures are available. Osmotic diuretics may provide rapid relief in emergency situations. Although their effect is transient, lasting only about 6 hours, they can be lifesaving in emergencies. These substances are rapidly excreted by the kidneys and carry with them large quantities of sodium and water. Mannitol (or sometimes urea) administered intravenously is the drug most frequently used for rapid reduction. The infusion is generally given slowly but may be pushed rapidly in cases of herniation or impending herniation. Because of the profound diuretic effect of the drug, an indwelling catheter is inserted to ensure bladder emptying. Adrenocorticosteroids are not recommended for cerebral edema secondary to head trauma. Paco2 should be maintained at 25 to 30 mm Hg to produce vasoconstriction, which reduces CSF, thereby decreasing ICP.
Nursing Activities
In cases of high levels of increased ICP, nursing procedures tend to trigger reactive pressure waves in many patients. For example, increased intrathoracic or abdominal pressure will be transmitted to the cranium. Particular care should be taken in positioning these patients to avoid neck vein compression, which may further increase ICP by interfering with venous return.
The child can be propped to one side or the other, and the use of an alternating-pressure mattress reduces the chance of prolonged pressure to vulnerable areas. Frequent clinical assessment of the child cannot be replaced by an ICP monitoring device.
It is important to avoid activities that may increase ICP by causing pain or emotional stress. Gentle range-of-motion exercises can be carried out but should not be performed vigorously. Nontherapeutic touch can cause an increase in ICP. Any disturbing procedures to be performed should be scheduled to take advantage of therapies that reduce ICP, such as osmotherapy and sedation. Efforts are taken to minimize or eliminate environmental noise. Assessment and intervention to relieve pain are important nursing functions to decrease ICP. Individualizing nursing activities and minimizing environmental stimuli by decreasing noxious procedures help control ICP (El Bashir, Laundy, and Booy, 2003; Vernon-Levett, 1998).
Suctioning
Suctioning and percussion are poorly tolerated and are therefore contraindicated unless concurrent respiratory problems exist. Hypoxia and the Valsalva maneuver associated with cough both acutely elevate ICP. Vibration, which does not increase ICP, accomplishes excellent results and should be tried first if treatment is needed. If suctioning is necessary, it should be brief and preceded by hyperventilation with 100% oxygen, which can be monitored during suctioning with a pulse oxygen sensor reading to determine oxygen saturation.
NUTRITION AND HYDRATION
Fluids and calories are supplied initially by the IV route (see Chapter 22). An IV infusion is started early, and the type of fluid administered is determined by the patient’s general condition. Fluid therapy requires careful monitoring and adjustment based on neurologic signs and electrolyte determinations. Often, comatose children are unable to cope with the same amounts of fluid they could tolerate at other times, and overhydration must be avoided to prevent fatal cerebral edema.
Hydration is maintained in the same manner (initially by IV and later by feeding tube). When cerebral edema is a threat, fluids may be restricted to reduce the chance of fluid overload. Skin and mucous membranes are examined for signs of dehydration. Observation for signs of altered fluid balance related to abnormal pituitary secretions is a part of nursing care.
Altered Pituitary Secretion
An altered ability to handle fluid loads is attributed in part to the syndrome of inappropriate antidiuretic hormone secretion (SIADH) and diabetes insipidus (DI) resulting from hypothalamic dysfunction (see Chapter 29). SIADH frequently accompanies CNS diseases such as head injury, meningitis, encephalitis, brain abscess, brain tumor, and subarachnoid hemorrhage. In the patient with SIADH, scant quantities of urine are excreted, electrolyte analysis reveals hyponatremia and hyposmolality, and manifestations of overhydration are evident. It is important to evaluate all parameters, since the reduced urinary output might be erroneously interpreted as a sign of dehydration.
The treatment of SIADH consists of restriction of fluids until serum electrolytes and osmolality return to normal levels. Since SIADH frequently occurs with meningitis in children, fluid restriction is often prescribed. Likewise, DI may occur after intracranial trauma. There is increased urine volume and the accompanying danger of dehydration. Adequate replacement of fluids is essential, and observation of electrolyte balance is necessary to detect signs of hypernatremia and hyperosmolality. Exogenous vasopressin may be administered.
MEDICATIONS
The cause of unconsciousness determines specific drug therapies. Children with infectious processes are given antibiotics appropriate to the disease and the infecting organism, and corticosteroids are prescribed for inflammatory conditions and edema. Cerebral edema is an indication for osmotherapy with osmotic diuretics. Sedatives or antiepileptics are prescribed for seizure activity (see p. 1008). Sedation in the combative child provides amnesic and anxiolytic properties in conjunction with a paralytic agent. The combination decreases ICP and allows treatment of cerebral edema. Usual drugs include morphine, midazolam, and pancuronium (Pavulon). Midazolam is attractive because of its short half-life.
Deep coma, induced by administration of barbiturates, is controversial in the management of ICP. Barbiturates are currently reserved for the reduction of increased ICP when all else has failed. Barbiturates decrease the cerebral metabolic rate for oxygen and protect the brain during times of reduced cerebral perfusion pressure. Barbiturate coma requires extensive monitoring, cardiovascular and respiratory support, and ICP monitoring to assess response to therapy. Paralyzing agents such as pancuronium also may be needed to aid in performing diagnostic tests, improving effectiveness of therapy, and reducing risks of secondary complications. Elevation of ICP and/or heart rate of patients who are being given paralyzing agents or are under sedation may indicate the need for another dose of either or both medications.
THERMOREGULATION
Hyperthermia often accompanies cerebral dysfunction; if it is present, measures are implemented to reduce the temperature to prevent brain damage and to reduce metabolic demands generated by the increased body temperature. Medically induced hypothermia assists in controlling ICP and may result in an improved outcome (Palmer, 2000). Antipyretics are the method of choice for fever reduction; cooling devices are used to induce hypothermia. Laboratory tests and other methods are used in an attempt to determine the cause, if any, of the hyperthermia.
ELIMINATION
A retention catheter is usually inserted in the acute phase, although diapers may be used and weighed to record urinary output. The child who formerly had bowel and bladder control is generally incontinent. If the child remains comatose for a long period, the indwelling catheter may be removed and periodic bladder emptying accomplished by intermittent catheterization. Stool softeners are usually sufficient to maintain bowel function, but suppositories or enemas may be needed occasionally for adequate elimination and to prevent an impaction. The passage of liquid stool after a period of no bowel activity is usually a sign of an impaction. To avoid this preventable problem, daily recording of bowel activity is essential.
HYGIENIC CARE
Routine measures for cleansing and maintaining skin integrity are an integral part of nursing care of the unconscious child (see Maintaining Healthy Skin, Chapter 22).
Mouth care is performed at least twice daily, since the mouth tends to become dry or coated with mucus. The teeth are carefully brushed with a soft toothbrush or cleaned with gauze saturated with saline. Commercially prepared cleansing devices, such as Toothettes, are convenient for cleansing the mouth and teeth. Lips are coated with ointment or other preparations to protect them from drying, cracking, or blistering.
The deeply comatose child is also prone to eye irritation. The corneal reflexes are absent; therefore the eyes are easily irritated or damaged by linen, dust, or other substances that may come in contact with them. There is excessive dryness as a result of incomplete closure of the eyes and/or decreased secretions, especially if the child is undergoing osmotherapy to reduce or prevent brain edema.
POSITIONING AND EXERCISE
The unconscious child is positioned to prevent aspiration of saliva, nasogastric secretions, and vomitus and to minimize ICP. The head of the bed is elevated, and the child is placed in a side-lying or semiprone position. A small, firm pillow is placed under the head, and the uppermost limbs are flexed and supported with pillows. The weight of the body should not rest on the dependent arm. In the semiprone position the child lies with the dependent arm at the side behind the body, the opposite side supported on pillows, and the uppermost arm and leg flexed and resting on the pillows. This position prevents undue pressure on the dependent extremities. The dependent position of the face encourages drainage of secretions and prevents the flaccid tongue from obstructing the airway.
Normal range-of-motion exercises help maintain function and prevent contractures of joints. Exercises should be done gently and with full range of motion. A small rolled pad can be placed in the palms to help maintain proper position of fingers; footboards or boots can be used to help prevent footdrop; and splinting may be needed to prevent severe contractures of the wrist, knee, or ankle in decerebrate children.
STIMULATION
Sensory stimulation is important in the care of the unconscious child, just as it is in the care of the alert child. For the temporarily unconscious or semiconscious child, sensory stimulation helps arouse the child to the conscious state and orient the child in terms of time and place. Auditory and tactile stimulation are especially valuable. Tactile stimulation is not appropriate for the child in whom it may elicit an undesirable response. However, for other children tactile contact often has a relaxing and calming effect. When the child’s condition permits, holding or rocking has a soothing effect and provides the body contact needed by young children.
The auditory sense is often present in a state of coma. Hearing is the last sense to be lost and the first one to be regained; therefore the child should be spoken to as any other child. Conversation around the child should not include thoughtless or derogatory remarks. A radio playing soft music or a music box or CD player is frequently used to provide auditory stimulation. Singing the child’s favorite songs or reading a favorite story is a tactic used to maintain the child’s contact with a familiar world. Playing songs or stories recorded in the parents’ voices can provide a continuous source of familiar stimulation.
Regaining Consciousness
Awakening from a coma is a gradual process; however, sometimes children regain consciousness within a short time. Regaining orientation involves knowing person, place, and time, in that order.
Certain behaviors have been observed when children awaken from the unconscious state. The stress and anxiety they appear to feel in a strange and unfamiliar environment are consistently expressed in silent and withdrawn behavior. Children respond to basic questioning but usually do not display their prehospitalization personality and social behavior until they are transferred from the critical care area.
FAMILY SUPPORT
Helping parents of an unconscious child cope with the situation is especially difficult. They may demonstrate all the guilt, fear, hostility, and anxiety of any parent of a seriously ill child (see Chapter 18). In addition, these parents are faced with the uncertain outcome of the cerebral dysfunction. The fear of death, intellectual disability, or other permanent disability is present. Nursing intervention with parents depends on the nature of the pathologic condition, the parents’ personality, and the parent-child relationship before the injury or illness.
If there is little or no residual effect, the child will be dismissed to home care fairly soon. The parents need the most intensive nursing intervention during the period of crisis and uncertainty. During the recovery phase they are given information, information is clarified, and they are encouraged to become involved in the child’s care. Often the child’s hospitalization is brief; however, some children require extended hospitalization for intensive therapy and rehabilitation.
Like parents who lose a child through death, the parents of the child lost to their world attempt to reconstitute a representation of the child. They bring items that belong to the child, such as favorite toys, music, and other objects cherished by the child. This is interpreted as an attempt to provide stimulation for the child in the hope of eliciting a response, to let the hospital staff know the child as the unique individual he or she was so that the parents’ distress can be better appreciated, and to reconstitute an image of the child “lost” to them and for whom they mourn. An awareness of these behaviors and coping mechanisms provides nurses with the understanding that helps them support the parents in their grief process.
Superimposed on the process of grieving for the “lost” child, parents may be faced with difficult decisions. When the child’s brain is so severely damaged that vital functions must be maintained by artificial means, the parents must make the final decision of whether to remove life-support systems. Since the decision is so difficult for parents, the practitioner is frequently placed in a position of making the decision indirectly. After providing the parents with all of the information, the practitioner will suggest that the child be removed from the life support to “see if the child can make it without help.” The approach relieves the parents of the decision and can be effective, but it is based on an evaluation of the parents’ intellectual level and emotional state. Sometimes parents may even choose to refuse treatment if they believe it to be best for the child and the family (informed dissent). At other times parents request that “everything possible” be done for the child.
When the child has survived the cerebral insult and is not comatose, but physical and/or mental capacity is limited, either minimally or severely, families must cope with the long and tedious rehabilitation process and the uncertain outcome. The drain on financial, emotional, and social resources can be enormous.
For parents who choose to care for their child at home, planning for home care begins early in the recovery process. The family should become involved with the child’s care as soon as they indicate an interest and ability to do so. They need education and support in learning to care for the child, regular follow-up observation and assessment of the home management, and planning for some respite care of the child. Parents need to understand that it is important to plan for periodic relief from the continual care of the child (see Preparing for Discharge and Home Care, Chapter 21; and Family-Centered Home Care, Chapter 20).
CEREBRAL TRAUMA
Head injury is a pathologic process involving the scalp, skull, meninges, or brain as a result of mechanical force. According to national statistics and Safe Kids Worldwide,* injuries are the number one health risk for children and the leading cause of death in children older than 1 year of age. Yearly, one in four children in the United States will suffer an injury serious enough to require medical attention. Tragically, 8000 children are killed every year by injuries. It has been estimated that 300 per 100,000 children per year have a traumatic brain injury and that 10 per 100,000 children per year die as a result of the brain injury. Studies indicate that as many as three fourths of the childhood deaths caused by mechanical trauma are the direct result of a brain injury. There is evidence to demonstrate that a previous head injury increases a child’s risk of having a subsequent head injury (Swaine, Tremblay, Platt, and others, 2007).
Etiology
The three major causes of brain damage in childhood, in order of importance, are falls, motor vehicle injuries, and bicycle injuries. Neurologic injury accounts for the highest mortality rate, with boys affected twice as often as girls. In motor vehicle accidents children younger than 2 years of age are almost exclusively injured as passengers, whereas older children may also be injured as pedestrians or cyclists. The majority of deaths from brain trauma caused by bicycle injuries occur between the ages of 5 and 19 years. Bicycle helmet laws have been effective in reducing the risk of head injury by 85% and brain injury by 88% (Rivara and Grossman, 2007).
The exposed nature of the head renders it particularly vulnerable to external violence, and many of the physical characteristics of children predispose them to craniocerebral trauma. For example, infants are frequently left unattended on beds, in high chairs, and in other places from which they can fall. Because the head of an infant or toddler is proportionately larger and heavier in relation to other body parts, it is the most likely to be injured. Incomplete motor development contributes to falls at young ages, and the natural curiosity and exuberance of children also increase their risk of injury.
Pathophysiology
The pathology of brain injury is directly related to the force of impact. Intracranial contents (brain, blood, CSF) are damaged because the force is too great to be absorbed by the skull and musculoligamentous support of the head. The elastic, pliable skull of the infant and young child absorbs much of the direct energy of physical impact to the head and affords some protection to intracranial structures. Although nervous tissue is delicate, it usually requires a severe blow to cause significant damage.
A child’s response to head injury is different from that of an adult. The larger head size and insufficient musculoskeletal support render the very young child particularly vulnerable to acceleration-deceleration injuries.
Primary head injuries are those that occur at the time of trauma and include skull fracture, contusions, intracranial hematoma, and diffuse injury. Subsequent complications include hypoxic brain damage, increased ICP, infection, and cerebral edema. The predominant feature of a child’s brain injury is the amount of diffuse swelling that occurs. Hypoxia and hypercapnia threaten the energy requirements of the brain and increase CBF. The added volume across the blood-brain barrier, along with the loss of autoregulation, exacerbates cerebral edema. Pressure inside the skull that is greater than arterial pressure results in inadequate perfusion.
Cerebral hyperemia occurs more often in children than adults, and this volume expansion may account for their tendency to develop intracranial hypertension. However, because the cranium of very young children has the ability to expand and the thin skull is more compliant, they may tolerate increases in ICP better than older children and adults do. Children have a significantly higher percentage of good outcomes, a lower mortality rate, and a lower incidence of surgical mass lesions after severe head trauma. However, their thinner, softer skull may sustain greater long-term damage than previously suggested.
Physical forces act on the head through acceleration, deceleration, or deformation. Acceleration or deceleration is more descriptive of the circumstances responsible for most head injuries. When the stationary head receives a blow, the sudden acceleration causes deformation of the skull and mass movement of the brain. Continued movement of the intracranial contents allows the brain to strike parts of the skull (e.g., the sharp edges of the sphenoid or the irregular surface of the anterior fossa) or the edges of the tentorium.
Although the brain volume remains unchanged, significant distortion takes place as the brain changes shape in response to the force of impact to the skull. This movement can cause bruising at the point of impact (coup) and/or at a distance as the brain collides with the unyielding surfaces far removed from the point of impact (contrecoup) (Fig. 28-4). Thus a blow to the occipital region can cause severe injury to the frontal and temporal areas of the brain. Sudden deceleration, such as takes place during a fall, causes the greatest cerebral injury at the point of impact. Children with an acceleration-deceleration injury demonstrate diffuse generalized cerebral swelling produced by increased blood volume or a redistribution of cerebral blood volume (cerebral hyperemia) rather than by increased water content (edema), as seen in adults.
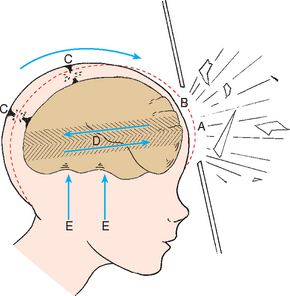
FIG. 28-4 Mechanical distortion of cranium during closed head injury. A, Preinjury contour of skull. B, Immediate postinjury contour of skull. C, Torn subdural vessels. D, Shearing forces. E, Trauma from contact with floor of cranium. (Redrawn from Grubb RL, Coxe WS: Central nervous system trauma: cranial. In Eliasson SG, Presky AL, Hardin Jr WB, editors: Neurological pathophysiology, New York, 1974, Oxford University Press.) Oxford University Press
Another effect of brain movement is shearing stresses, which may tear small arteries and cause subdural hemorrhages. Damage can also occur when severe compression of the skull causes the brain to be forced through the tentorial opening. This can produce irreparable damage to the brainstem (Fig. 28-5).
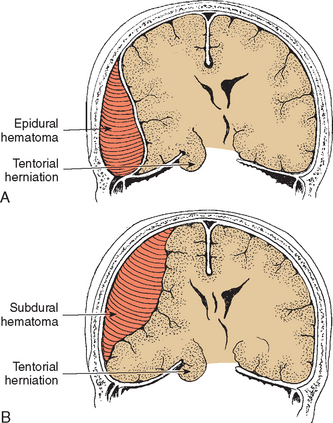
FIG. 28-5 A, Epidural (extradural) hematoma and compression of temporal lobe through tentorial hiatus. B, Subdural hematoma.
Concussion.: The most common head injury is concussion, a transient and reversible neuronal dysfunction, with instantaneous loss of awareness and responsiveness, that results from trauma to the head and persists for a relatively short time, usually minutes or hours. It is generally followed by amnesia for the moment of the injury and a variable period after the injury. The common misconception that loss of consciousness is the hallmark of concussion is not true, especially for children. Concussion is correctly defined as a traumatically induced alteration in mental status. Confusion and amnesia following head injury are the hallmarks of concussion.
The pathogenesis of concussion is still unclear but may be a result of shearing forces that cause stretching, compression, and tearing of nerve fibers, particularly in the area of the central brainstem, the seat of the reticular activating system. It has also been suggested that the anatomic alterations of nerve fibers cause the release of large quantities of acetylcholine into the CSF and a reduction in oxygen consumption with increased lactate production.
Contusion and Laceration.: The terms contusion and laceration are used to describe visible bruising and tearing of cerebral tissue. Contusions represent petechial hemorrhages along the superficial aspects of the brain at the site of impact (coup injury) or a lesion remote from the site of direct trauma (contrecoup injury). In serious accidents there may be multiple sites of injury.
The major areas of the brain susceptible to contusion or laceration are the occipital, frontal, and temporal lobes. Also, the irregular surfaces of the anterior and middle fossae at the base of the skull are capable of producing bruises or lacerations on forceful impact. Contusions may cause focal disturbances in strength, sensation, or visual awareness. The degree of brain damage in the contused areas varies according to the extent of vascular injury. Signs will vary from mild, transient weakness of a limb to prolonged unconsciousness and paralysis. However, the signs and symptoms may be clinically indistinguishable from those of concussion.
The lower incidence of cerebral contusion in infancy has been attributed to the infant’s pliable skull with less convolutional markings of the inner space between brain tissue and bone. In addition, the infant’s brain tissue has a softer consistency, which also reduces surface injury. However, infants who are roughly shaken (shaken baby syndrome) can sustain profound neurologic impairment, seizures, retinal hemorrhages, and intracranial subarachnoid or subdural hemorrhages. In addition to these classic injuries, high cervical spinal cord hemorrhages and contusions can occur.
Cerebral lacerations are generally associated with penetrating or depressed skull fractures. However, they may occur without fracture in small children. When brain tissue is actually torn, with bleeding into and around the tear, usually more severe and prolonged unconsciousness and paralysis occur, leaving permanent scarring and some degree of disability.
Fractures.: Because of its flexibility, the immature skull is able to sustain a greater degree of deformation than the adult skull before it incurs a fracture. A great deal of force is required to produce a fracture in an infant’s skull. However, the undersurface of the skull contains grooves in which the meningeal arteries lie. A fracture that runs through one of these grooves may tear the artery and produce severe and damaging hemorrhage. Hypovolemic hypotension can occur in infants with skull fractures.
The types of fractures that occur are as follows:
Linear fractures are those in which the lines of the fracture are predetermined by the site and velocity of the impact, as well as by the strength of the bone. These are uncommon before 2 to 3 years of age but constitute the majority of childhood skull fractures. Most linear skull fractures are associated with an overlying hematoma or soft-tissue swelling (Schutzman and Greenes, 2001).
Depressed fractures are those in which the bone is locally broken, usually into several irregular fragments that are pushed inward, causing pressure on the brain. The inner portion of the bone is more extensively fragmented than the outer portion, which almost invariably produces tears in the dura. These are uncommon before 2 to 3 years of age. In infants and very young children, the soft, malleable bone may become dented in a peculiar rounded or “Ping-Pong ball” depression, without laceration of either skin or dura.
Comminuted fractures consist of multiple associated linear fractures. They usually result from intense impact. These types of fractures often result from repeated blows against an object and may suggest child abuse.
Basilar fractures involve the basilar portion of the frontal, ethmoid, sphenoid, temporal, or occipital bones. Because of the proximity of the fracture line to structures surrounding the brainstem, this is a serious head injury. Approximately 80% of the cases may include clinical features such as subcutaneous bleeding in the posterior neck area and over the mastoid process (battle sign). Bleeding around the eyes (raccoon eyes) or bleeding behind the tympanic membrane (hemotympanum) may occur.
Open fractures cause communication between the skull and the scalp or the surfaces of the upper respiratory tract. Open fractures increase the risk of CNS infection. They may have an overlying laceration called a compound fracture. Open fractures can also create an opening in the paranasal sinuses or middle ear that can lead to CSF rhinorrhea or otorrhea. Facial paralysis, vertigo, tinnitus, or hearing loss may develop.
Diastatic fractures are traumatic separations of the cranial sutures. These most frequently affect the lambdoid suture and are rarely seen beyond the first 3 years of life. They require no specific treatment but should be observed for “growing fractures.” Growing fractures are skull fractures associated with an underlying dural tear that may be caused by a leptomeningeal cyst, dilated ventricles, or a herniated brain. Neurologic symptoms include headache, seizures, and asymmetric cranial growth (Schutzman and Greenes, 2001). Infants and young children who have isolated skull fractures should be evaluated for growing skull fractures from 1 to 2 months after the injury (Schutzman and Greenes, 2001).
Complications
The major complications of trauma to the head are hemorrhage, infection, edema, and herniation through the tentorium. Infection is always a hazard in open injuries, and edema is related to tissue trauma. Vascular rupture may occur even in minor head injuries, causing hemorrhage between the skull and cerebral surfaces. Compression of the underlying brain produces effects that can be rapidly fatal or insidiously progressive.
Epidural Hemorrhage.: The blood accumulates between the dura and the skull to form a hematoma, which, because of the difficulty with which dura is stripped from bone, forces the underlying brain contents downward and inward as the brain expands (see Fig. 28-5, A). Since bleeding is generally arterial, brain compression occurs rapidly. Most often the expanding hematoma is located in the parietotemporal region, forcing the medial portion of the temporal lobe under the edge of the tentorium, where it causes pressure on nerves and blood vessels. The lower incidence of epidural hematoma in childhood has been attributed to the fact that the middle meningeal artery is not embedded in the bone surface of the skull until approximately 2 years of age. Therefore a fracture of the temporal bone is less likely to lacerate the artery. Second, the dura closely adheres to the inner table of the skull, especially at the level of the sutures, making separation from bleeding less likely. However, a child’s skull can be indented with sufficient force to tear the middle meningeal artery and rebound intact without causing a fracture. Hemorrhage can also derive from dural veins or the dural sinuses, especially in infants and small children, in whom fracture is less likely to occur. In 20% to 40% of children a skull fracture is not detectable. The classic clinical picture of epidural hemorrhage (momentary unconsciousness followed by a normal period, then lethargy or coma) is seldom evident in children (see Box 28-3 for clinical manifestations). The period of impaired consciousness is frequently lacking, and the symptom-free period is atypical because of nonspecific complaints such as irritability, headache, and vomiting. When it does occur, the symptom-free period frequently lasts longer than 48 hours.
Clinically significant epidural hematomas are uncommon in children younger than 4 years of age. These differences may be caused by the decreased tendency of the resilient skull to fracture; the ability of blood to escape through widened sutures, an open fontanel, or a fracture; bleeding from smaller vessels with less rapid and massive bleeding; lower systolic blood pressure in children; and possibly the decreased susceptibility of the child’s brain to pressure changes.
Subdural Hemorrhage.: A subdural hemorrhage is bleeding between the dura and the cerebrum, usually as a result of rupture of cortical veins that bridge the subdural space (see Fig. 28-5, B). Subdural hematomas are 10 times more frequent than epidural hematomas, occurring most often in infancy, with a peak incidence at 6 months.
Unlike epidural hemorrhage, which develops inwardly against the less resistant brain tissue, subdural hemorrhage tends to develop more slowly and spreads thinly and widely until it is limited by the dural barriers—the falx and tentorium. Subdural hematoma is fairly common in infants, frequently as a result of birth trauma, falls, assaults, or violent shaking. The small subdural space and dura firmly attached to the skull in this area are highly vulnerable to increased ICP.
Repeated subdural taps often provide relief in the infant, as revealed by follow-up CT scans, improved neurologic status, and a flat anterior fontanel. Surgical evacuation of the hematoma is the treatment of choice in the older child and is frequently required in infants.
Cerebral Edema.: Some degree of brain edema is expected, especially 24 to 72 hours after craniocerebral trauma. Cerebral edema caused by direct cellular injury or vascular injury induces vascular stasis, anoxia, and further vasodilation. If the progression continues unchecked, ICP exceeds arterial pressure and fatal anoxia ensues, and/or the pressure causes herniation of a portion of the brain over the edge of the tentorium, compressing the brainstem and occluding the posterior cerebral arteries. Diffuse cerebral swelling and changes in CBF are common patterns after head injury in children.
Diagnostic Evaluation
A detailed history, especially a health history, both past and present, is essential in evaluating the child with a craniocerebral trauma. Certain disorders, such as drug allergies, hemophilia, diabetes mellitus, or epilepsy, may produce similar symptoms. Furthermore, even minor traumatic injury can aggravate a preexisting disease process. Events surrounding the injury often supply significant data. It must be determined whether the infant or child exhibited alterations in consciousness; any other signs and behaviors exhibited by the child must be noted. Since head injuries are frequently accompanied by injuries in other areas, the examination is performed with care to avoid further damage.
Initial Assessment.: Priorities in the initial stabilization phase of a child with a head injury include assessment of the ABCs (airway, breathing, circulation); evaluation for shock; a neurologic examination, especially LOC; assessment of pupillary symmetry and response to light; and observation for seizures (Bayir, Kochanek, and Clark, 2003). The assessment is carried out quickly in relation to vital signs (see Emergency Treatment box). Excited and irritable children may have a rapid pulse, hyperventilate, appear pale, and feel clammy shortly after an injury.
Ocular signs such as fixed and dilated pupils, fixed and constricted pupils, and pupils that are poorly reactive or nonreactive to light and accommodation indicate increased ICP or brainstem involvement. It is important to remain with the child who demonstrates fixed and dilated pupils, since these are ominous signs, with the probability of respiratory arrest. Dilated, nonpulsating blood vessels indicate increased ICP before the appearance of papilledema. Retinal hemorrhages are seen in acute head injuries.
Less urgent but important additional assessments include examination of the scalp for lacerations and palpation for other abnormalities. A significant amount of blood loss can occur from scalp lacerations.
An accurate assessment of clinical signs provides baseline information. Serial evaluations, preferably by a single observer, help to detect changes in the neurologic status. Alterations in mental status, evidenced by increased difficulty in rousing the child, mounting agitation, development of focal lateral neurologic signs, or marked changes in vital signs, usually indicate extension or progression of the basic pathologic process.
Assess child:
Clean any abrasions with soap and water.
Keep NPO (nothing by mouth) until instructed otherwise.
Assess pain, but do not give analgesics or sedatives.
Check pupil reaction every 4 hours (including twice during night) for 48 hours.
Awaken twice during the night to check level of consciousness.
Seek medical attention if any of the following apply:
– At high speed (e.g., automobile)
– Fall from a significant distance (e.g., roof, tree, or height greater than that of the child)
Discomfort (crying) more than 10 minutes after injury
Headache that is severe, worsening, interferes with sleep
Swelling in front of or above earlobe or increased swelling
Confusion or not behaving normally
Difficult to arouse from sleep
Blurred vision or seeing double
Pupils dilated, unequal, or fixed
Special Tests.: After a thorough clinical examination, a variety of diagnostic tests are helpful in providing a more definitive diagnosis of the type and extent of the trauma. The severity of a head injury may not be apparent on clinical examination of a child, but it will be detectable on a CT scan. Whenever the child has a history consistent with a serious head injury (unrestrained occupant in a severe motor vehicle accident or a fall from a significant height), it is important that a scan be performed even if the child initially appears alert and oriented. All children with head injuries who have any alteration of consciousness, headache, vomiting, skull fracture, seizure, or a predisposing medical condition should also undergo CT scanning.
MRI and neurobehavioral assessment following early head injury may be useful in documenting cognitive impairment in relation to structural alterations in the young brain. MRI provides details of soft tissues better than any other noninvasive device. Electroencephalography is not particularly helpful for early diagnosis but is useful for defining seizure activity or focal destructive lesions after the acute phase of illness. Lumbar puncture is rarely used in craniocerebral trauma and is contraindicated in the presence of increased ICP because of the possibility of herniation. In some centers monitoring ICP is part of the assessment.
Posttraumatic Syndromes.: Posttraumatic syndromes can be clinically manifested because of structural complications resulting from a head injury and through the signs and symptoms demonstrated by the child. Structural complications can include hydrocephalus and focal deficits such as optic atrophy, cranial nerve palsies, motor deficits, DI, aphasia, and seizures. Behavioral disturbances include sleep disturbances, phobias, emotional lability, altered school performance, and changes related to aggressiveness or withdrawal. Postconcussion syndrome is a common sequela to brain injury and can occur within minutes to an hour after a head injury. The manifestations vary with the child’s age. The syndrome occurs frequently in children younger than 1 year of age. The syndrome in adolescents is similar to that in adults. The duration of manifestations can vary from several days to several months. Death from concussion is preventable unless overwhelming secondary brain injury has occurred (Durkin, Olsen, Barlow, and others, 1998; Gennarelli, 1999).
Posttraumatic seizures occur in a number of children who survive a head injury and are more common in children than in adults. Seizures are more likely to occur within the first few days of the head injury (Chiaretti, De Benedictis, Polidori, and others, 2000). Structural complications (e.g., hydrocephalus) may occur after a head injury. The type of residual effect depends on the location and nature of the disorder. True intellectual disability occurs only after severe injuries.
Therapeutic Management
The majority of children with mild to moderate concussion who have not lost consciousness can be cared for and observed at home after careful examination reveals no serious intracranial injury. Nurses should provide parents with clear explanations and instructions and should encourage them to ask questions both before and after leaving the medical facility if clarification is needed (see Family Focus box).
The parents are instructed to check the child every 2 hours to determine any changes in responsiveness. The sleeping child should be wakened to see if he or she can be roused normally. Parents are advised to maintain contact with the health professional, who usually wishes to examine the child again in 1 or 2 days. The manifestations of epidural hematoma in children do not generally appear until 24 hours or more after injury.
Children with severe injuries, those who have lost consciousness for more than a few minutes, and those with prolonged and continued seizures or other focal or diffuse neurologic signs must be hospitalized until their condition is stable and their neurologic signs have diminished.
The child is maintained on nothing by mouth (NPO) or restricted to clear liquids, if able to take fluids by mouth, until it is determined that vomiting will not occur. IV fluids are indicated in the child who is comatose or displays dulled sensorium and in the child with persistent vomiting. Fluid balance is closely monitored by daily weights; accurate intake and output measurements; and serum osmolality to detect early signs of water retention, excessive dehydration, and states of hypertonicity or hypotonicity.
Maintaining contact with parents for continued observation and reevaluation of the child, when indicated, facilitates early diagnosis and treatment of possible complications from head injury, such as hematoma, hydrocephalus, cysts, and posttraumatic seizures. Children are generally hospitalized for 24 to 48 hours’ observation if their family lives far from medical facilities or lacks transportation or a telephone that would provide access to immediate help. Other circumstances such as language or other communication barriers, or even emotional trauma, may hinder learning and make it difficult for families to feel confident in caring for their child at home.
The volume of IV fluid is carefully monitored to avoid aggravating any cerebral edema and to minimize the possibility of overhydration in case of SIADH. However, damage to the hypothalamus or pituitary gland may produce DI with its accompanying hypertonicity and dehydration.
Restlessness can be satisfactorily managed, if necessary, with mild sedation, and headache is usually controlled with acetaminophen (Tylenol). Antiepileptics are used for seizure control and frequently in cases of suspected contusion or laceration. Antibiotics may be administered if lacerations, CSF leakage, or excessive cerebral tissue damage is present. Prophylactic tetanus toxoid is given as appropriate. Cerebral edema is managed as described for the unconscious child. Hyperthermia is controlled with tepid sponges or a hypothermia blanket.
Surgical Therapy.: Scalp lacerations are sutured after the underlying bone is carefully examined. Depressed fractures require surgical reduction and removal of bone fragments. Torn dura is sutured. Ping-Pong ball skull fractures in very young infants ordinarily correct themselves within a few weeks and do not require specific treatment, although they can be reduced by pressure against the bone.
Prognosis.: The outcome of craniocerebral trauma depends on the extent of injury and complications. However, the outlook is generally more favorable for children than for adults (Faillace, 2002; Masson, Thicoipe, Mokni, and others, 2003). More than 90% of children with concussions or simple linear fractures recover without symptoms after the initial period. The incidence of fatalities and neurologic sequelae is lower in children than in adults, even in those with severe head injuries. The prognosis for recovery is primarily related to the duration of coma and the degree of injury. The combination of impaired consciousness and skull fracture carries the highest risk of complication.
The concern regarding outcome is increasingly focused on cognitive, emotional, and mental problems. Children experience a higher frequency of psychologic disturbances after head injury, whereas adults are more prone to physical complaints. Children may be more vulnerable than adults to long-term cognitive and behavioral dysfunction after diffuse brain injury. Even with recovery, the effects of brain injury on a child’s potential can never be known.
True coma (not obeying commands, eyes closed, and not speaking) usually does not last more than 2 weeks. A child’s eventual outcome can range from brain death to a persistent vegetative state to complete recovery. However, even the best recovery may be associated with personality changes, including mood lability and loss of confidence; impaired short-term memory; headaches; and subtle cognitive impairments. Many children are left with significant disabilities after head injury that appear months later as learning difficulties, behavioral changes, or emotional disturbances (Faillace, 2002). Generally, within 6 months to 1 year after the injury, 90% of the long-term neurologic outcome has been achieved.
Nursing Care Management
The hospitalized child requires careful neurologic assessment and evaluation (including vital signs) repeated at frequent intervals to provide information needed to establish a correct diagnosis, reveal signs and symptoms of increased ICP, determine clinical management, prevent many complications, and provide support to the child and family during the recovery phases.
The child is placed on bed rest, usually with the head of the bed elevated slightly. Appropriate safety measures, such as side rails kept up and seizure precautions for children of all ages, are implemented. For the extremely restless child, hard surfaces may have to be padded and restraint used to prevent the possibility of further injury. Care is individualized according to the child’s specific needs. The unconscious child is managed as described in the previous section, but most childhood head injuries are those causing momentary stunning or temporary unconsciousness. Children may be restless and irritable, but more often their reaction is to fall asleep when left undisturbed. A quiet environment helps reduce restlessness and irritability. Shining bright lights directly into the child’s face is irritating and often aggravates the child, making assessment of ocular responses difficult.
Frequent examinations of vital signs, neurologic signs, and LOC are extremely important nursing observations. When possible, they should be performed by a single observer to better detect subtle changes that may indicate worsening neurologic status. Pupils are checked for size, equality, reaction to light, and accommodation. After the initial elevations usually seen following injury, the vital signs generally return to normal unless there is brainstem involvement. An axillary measurement of temperature is the safest method, since seizures are not uncommon and vomiting is a frequent response in children, especially when the child is disturbed.
The most important nursing observation is assessment of the child’s LOC. Alterations in consciousness appear earlier in the progression of an injury than alterations of vital signs or focal neurologic signs. Some expected responses may be misinterpreted as deviations from the normal. Frequent examinations of alertness are fatiguing to the child; therefore the child often desires to fall asleep, which may be confused with depressed consciousness. When left alone, the child goes to sleep. It is not uncommon to observe ocular divergence through the partially closed eyelids.
A key nursing role is to provide sedation and analgesia for the child. The conflict between the need to promote comfort and relieve anxiety in the child vs the need to assess for neurologic changes presents a dilemma. However, both goals can be achieved with close observation of the child’s LOC and response to analgesics, use of a pain assessment record, and effective communication with the practitioner. To differentiate between sedation from an opioid and sedation from the injury, naloxone can be given slowly to reverse the opioid’s sedative effect. Decreasing restlessness after administration of an analgesic most likely reflects pain control rather than a declining LOC.
Observations of position and movement provide additional information. Any abnormal posturing is noted, as well as whether it occurs continuously or intermittently. Are the child’s handgrips strong and equal in strength? Are there any signs of flexion or extension posturing? What is the child’s response to stimulation? Is movement purposeful, random, or absent? Are movement and sensation equal on both sides or restricted to one side only?
The child may complain of headache or other discomfort. The child who is too young to describe a headache will be fussy and resist being handled. The child who suffers from vertigo will often assume a position of comfort and vigorously resist efforts to be moved. Forcible movement causes the child to vomit and display spontaneous nystagmus. Seizures, relatively common in children with craniocerebral trauma, may be of any type but are more often generalized, regardless of the type of injury. Any seizure activity should be carefully observed and described in detail. Children in postictal (postseizure) states are lethargic, with sluggish pupils.
Drainage from any orifice is noted. Bleeding from the ear suggests the possibility of a basal skull fracture. The amount and characteristics of the drainage are observed, and since the auditory canal may be a source of infection, dry, sterile cotton can be placed loosely at the orifice and changed when soiled.
Head trauma is frequently accompanied by other undetected injuries; therefore any bruises, lacerations, or evidence of internal injuries or fractures of the extremities are noted and reported. Associated injuries are evaluated and treated appropriately.
The child with normal LOC is usually allowed clear liquids unless fluid is restricted. If the child has an IV infusion, it is maintained as prescribed. The diet is advanced to that appropriate for the child’s age as soon as the condition permits. Intake and output are measured and recorded, and any incontinence of bowel or bladder is noted in the child who has been toilet trained.
The child should be observed for any unusual behavior, but behavior should be interpreted in relation to the child’s normal behavior. For example, urinary incontinence during sleep would be of no consequence in a child who routinely wets the bed but would be highly significant for one who is always dry. In addition, a child who is subject to nightmares might cry out and demonstrate agitated behavior at night. There would be less concern about a child who falls asleep several times during the day if this were consistent with the child’s usual behavior. Parents are valuable resources. Information obtained from parents at or shortly after admission is helpful in evaluating the child’s behavior (e.g., the ease with which the child is roused normally, the usual sleeping position, how much the child sleeps during the day, motor activity the child is capable of [rolling over, sitting up, climbing], hearing and visual acuity, appetite, and manner of eating [spoon, bottle, cup]).
Family Support.: The emotional and educational support of the family of children who have suffered head injury presents a formidable, challenging aspect to nursing care. Witnessing the parents’ ordeal of grief and helplessness on seeing their child in an altered state, connected to monitoring equipment in an intensive care unit, evokes empathy. The nurse can encourage the family to be involved in the child’s care, to bring in familiar belongings, or to make a tape recording of familiar voices and sounds. Parents may need a demonstration on how to touch or cuddle their child and may want to talk about their grief. The nurse can listen attentively, reinforce what is being done to assist the child, and direct parents toward signs and symptoms of recovery to instill hope without promises. A common phenomenon is for families to seek information from all health care providers, asking, “What will she be like? What do you know?” as they search for some clue that the child is recovering. Honesty and kindness, along with competent care, distinguish excellent nursing abilities.
When the child is discharged, the parents are advised of probable posttraumatic symptoms that may be expected, such as behavioral changes, sleep disturbances, phobias, and seizures. They should understand observations they need to make and how to contact the physician, nurse, or health facility in case the child develops any unusual signs or symptoms. The importance of follow-up evaluation should be emphasized. It is often advisable to refer the family to a public health agency for home follow-through to be certain that the child receives posthospital evaluation.
Rehabilitation.: The rehabilitation and management of the child with permanent brain injury are essential aspects of care. Rehabilitation of brain-injured children is begun as soon as feasible and usually involves the family and a rehabilitation team. Careful assessment of the child’s capabilities, limitations, and probable potential is made as early as possible, and appropriate interventions are implemented to maximize the residual capacities. The Brain Injury Association of America* provides information and listings of rehabilitation services and support groups throughout the country.
Pediatric trauma rehabilitation is a national concern. Coordinating care and services for early rehabilitation involves identifying the child’s and family’s response to the traumatic injury and disability, securing available resources, and recognizing the parental role in the process.
The child with a disability resulting from head trauma requires assessment on a physical, cognitive, emotional, and social level. The child has experienced separation, pain, sensory deprivation and overload, changes in circadian cycle, and fear of the unknown. Recovery and transition require new coping strategies at the same time that regressive and acting-out behavior may start. Parents and children need honest communication for decision making. A rehabilitation facility or home rehabilitation is advocated when the child has progressed beyond what can be provided in a hospital setting. The Rancho Los Amigos Scale provides a systematic assessment of the possible progress a child may achieve following a severe head injury.
Prevention.: Tremendous strides have been taken in the prevention of cerebral damage after head injury in children. New developments requiring research point to the prevention of cellular injury or the primary insult. However, the greatest benefit lies in prevention of head injuries. Nurses can exert a valuable influence on behalf of children through education. The reason injuries remain preventable is that unnecessary risks go unchecked. Inadequate supervision combined with a child’s natural sense of indestructibility and exploration can lead to lethal results. Nurses are in the unique position of influencing caregivers in terms of growth and development. Banning the use of infant walkers is an example. This equipment does not help develop motor skills and places infants at risk for head and neck injuries from falls, especially down steps. Public education, coupled with legislative support, can prevent childhood injuries. (For extensive discussions of childhood injuries and prevention, see Chapters 10, 12, 13, 15, and 16. See also Childhood Mortality, Chapter 1.)
NEAR-DROWNING
Drowning is a major cause of accidental death in children over 1 year of age. Most cases of drowning are accidental, usually involving the following individuals:
Children who are helpless in water, such as inadequately attended children in or near swimming pools or infants in bathtubs
Small children who fall into ponds, streams, and flooded excavations, usually near home
Occupants of pleasure boats who fail to wear life preservers
Children who have diving accidents
Children who are able to swim but overestimate their endurance
Accidental drowning occurs five times more often in boys than in girls; almost 40% of children are younger than age 5, and 90% of cases occur in private swimming pools (Kallas, 2004). Drowning can take place in any body of water, including such unlikely ones as a pail of water. Top-heavy toddlers fall head first into a pail of water, their arms become trapped, and they are unable to free themselves. Hot tubs and whirlpool spas have been implicated in childhood drowning injury. The suction created at the outlet is strong enough to trap even larger children underwater. Drowning as a form of fatal child abuse has also been recognized as a problem. Homicidal drownings are unwitnessed, they usually occur in the home, and the victims are either infants or toddlers. With expeditious treatment many children are being saved.
For purposes of this discussion, two terms need clarification:
Drowning—Death from asphyxia while submerged, regardless of whether fluid has entered the lungs
Near-drowning—Survival at least 24 hours after submersion in a fluid medium
Pathophysiology
The major pulmonary changes that occur in drowning are directly related to the length of submersion (regardless of the type and amount of fluid aspirated), the victim’s physiologic response, and the development and degree of immersion hypothermia. In addition, cerebral recovery depends on the effectiveness of initial resuscitation and subsequent critical care measures to support cerebral salvage.
Physiologic factors that influence the extent of damage from immersion include resistance to asphyxia and anoxia, which shows some individual variation. There is greater resistance with diminishing age; young children can withstand longer periods of submersion. More important is the drowning, or diving, reflex. This neurologic response is triggered by immersion of the face in cold water. Blood is shunted away from the periphery, and the flow is concentrated in the brain and heart predominantly.
The problems created by near-drowning are (1) hypoxia and asphyxiation, (2) aspiration, and (3) hypothermia (except near-drowning in hot tubs). Cardiopulmonary arrest is secondary to asphyxiation.
Hypoxia is the primary problem because it results in global cell damage, and different cells tolerate variable lengths of anoxia. Neurons, especially cerebral cells, sustain irreversible damage after 4 to 6 minutes of submersion. The heart and lungs can survive up to 30 minutes. Regardless of the amount of water aspirated, there is arterial hypoxemia (resulting from atelectasis with shunting of blood through the nonventilated alveoli) and a combined respiratory acidosis (resulting from retained carbon dioxide) and metabolic acidosis (caused by buildup of acid metabolites from anaerobic metabolism). The pathologic events are directly related to the duration of submersion. The major difficulty is acute ventilatory insufficiency. Approximately 10% of drowning victims die without aspirating fluid but succumb from acute asphyxia as a result of prolonged reflex laryngospasm.
Aspiration of fluid occurs in the majority of drownings. The aspirated fluid results in pulmonary edema, atelectasis, airway spasm, and pneumonitis, which aggravates the hypoxia. It was previously thought that submersion in salt water vs fresh water altered the physiologic response to near-drowning. However, there is no clinically significant difference in the response of human survivors, and the type of water does not alter the therapy or outcome.
Hypothermia occurs rapidly in infants and children, partly because of their large surface area relative to body mass and partly as a result of the cold water itself. Water is an excellent heat conductor, and contact with the skin is increased by struggling. Hypothermia may make resumption or maintenance of cardiac function possible if body temperature is less than 30° C (86° F). Profound hypothermia is usually evidence of lengthy submersion.
Therapeutic Management
Resuscitative measures should begin at the scene of a drowning, and the victim should be transported to the hospital with maximal ventilatory and circulatory support. Many victims need care for some time after aspiration of fluid. In the hospital, intensive pulmonary care is implemented and continued according to the patient’s needs.
In general, the management of the near-drowning victim is based on the degree of cerebral insult (Box 28-4). The first priority is to restore oxygen delivery to the cells and prevent further hypoxic damage. A spontaneously breathing child will do well in an oxygen-enriched atmosphere; the more severely affected child will require endotracheal intubation and mechanical ventilation. Blood gases and pH are monitored frequently as a guide to oxygen, fluid, and electrolyte therapies.
Aspiration pneumonia is a frequent complication that occurs about 48 to 72 hours after the episode. Bronchospasm, alveolocapillary membrane damage, atelectasis, abscess formation, and acute respiratory distress syndrome are other complications that occur after aspiration of fluid.
Prognosis.: Studies report that the best predictors of a good outcome were length of submersion in nonicy water (> 5° C [41° F]) for less than 5 minutes and the presence of sinus rhythm, reactive pupils, and neurologic responsiveness at the scene. The worst prognoses—for death or severe neurologic impairment—were in children submerged for more than 10 minutes and not responding to advanced life support within 25 minutes. All children without spontaneous, purposeful movement and normal brainstem function 24 hours after near-drowning suffered severe neurologic deficits or death (Zuckerman, Gregory, and Santos-Damiani, 1998; Kallas, 2004). (See Nursing Care Guidelines box.)
Nursing Care Management
Nursing care depends on the child’s condition. A child who survives may need intensive respiratory nursing care with attention to vital signs, mechanical ventilation and/or tracheostomy, blood gas determination, chest therapy, and IV infusion. Frequently the child is comatose for an indefinite period and requires the same care as an unconscious child. A difficult aspect in the care of the child victim of near-drowning is helping the parents cope with severe guilt reactions. The magnitude of the event is so great that efforts to provide comfort and support are of only limited success. Parents need to hear that everything possible is being done to treat the child, and this message needs to be repeated often.
The parents of the child who is saved from death are also faced with the anxiety of not knowing what the outcome will be. The situation generates such intense feelings of loneliness, it is important for families to know that they are not alone. They need to be reminded frequently that there are caring people to assist them both during the crisis and later. Additional sources of support that can be recommended are psychiatric and social work consultants, community services, and religious support. Self-help groups are excellent if these are available in the community.
Nurses often have difficulty relating to the parents if obvious neglect has precipitated the accident and subsequent problems; therefore it is important for those who care for these children and their families to assess their own feelings about the situation, as well as the family’s coping abilities and resources. Caring for near-drowning victims and their families requires nurses to be sensitive to the needs of the child and family and to recognize their own reactions and emotions.
Prevention.: Most drownings, particularly of infants or small children, can be prevented with adequate supervision. Water safety and survival training should be required for all school-age children, and nurses can be active advocates in their communities. Nurses are also in a position to emphasize the importance of adequate adult supervision when children are in the water. Aquatic programs for infants and toddlers do not decrease the risk of drowning; young children should never be left unattended when in or near the water (American Academy of Pediatrics, 2000b; Kallas, 2004). Parents with pools should know cardiopulmonary resuscitation techniques. (See also Injury Prevention, Chapters 10, 12, 13, 15, and 16.)
NERVOUS SYSTEM TUMORS
Brain tumor and neuroblastoma are two major forms of childhood cancer derived from neural tissue. CNS tumors account for approximately 20% of all childhood cancers, and approximately 3.3 cases per 100,000 occur in children under 15 years of age (Blaney, Kun, Hunter, and others, 2006). Both of these tumors are difficult to treat and have not demonstrated the dramatic improvements in survival seen in other forms of childhood cancer.
BRAIN TUMORS
Brain tumors are the most common solid tumors in children and are the second most common childhood cancer. The majority of tumors (about 60%) are infratentorial (below the tentorium cerebelli), which means that they occur in the posterior third of the brain, primarily in the cerebellum or brainstem. This anatomic distribution accounts for the frequency of symptoms resulting from increased ICP. The other tumors are supratentorial, or within the anterior two thirds of the brain, mainly the cerebrum.
Brain tumors, whether benign or malignant, can arise from any cell within the cranium. Consequently, the cranial cells’ origin provides a histologic classification for major tumors. For instance, astrocytes (cells that form the supportive tissue for neurons) may form a common glial tumor called an astrocytoma. The major infratentorial tumors are medulloblastomas, cerebellar astrocytomas, brainstem gliomas, and ependymomas, and the major supratentorial tumors are astrocytomas, hypothalamic tumors, optic pathway tumors, and craniopharyngiomas.
Diagnostic Evaluation
The signs and symptoms of brain tumors are directly related to their anatomic location and size and, to some extent, the child’s age. In infants, whose cranial sutures are still open, virtually no early detectable symptoms develop. It is not until spinal fluid obstruction causes markedly increased head size that a lesion may be suspected. Even in older children, clinical manifestations are nonspecific. However, the most common symptoms are headache, especially on awakening, and vomiting that is not related to feeding. Vomiting occurs from increased ICP that compresses the brainstem, directly stimulating the vomiting center in the medulla (Blaney, Kun, Hunter, and others, 2006).
Diagnosis of a brain tumor is based subjectively on presenting clinical signs and objectively on neurologic tests and histologic diagnosis via surgery. Because the signs and symptoms are vague and easily overlooked, early diagnosis relies on a high index of suspicion during history taking. A number of tests may be used in the neurologic evaluation, but the most common diagnostic procedure is MRI, which determines the location and extent of the tumor. Other tests that may be used include CT, angiography, electroencephalography, and lumbar puncture. Lumbar puncture is dangerous in the presence of increased ICP because of the possibility of brainstem herniation following a sudden release of pressure. The definitive diagnosis is based on brain tissue specimens obtained during surgery.
Therapeutic Management
Treatment may involve the use of surgery, radiotherapy, and chemotherapy. All three may be used, depending on the type of tumor. The treatment of choice is total removal of the tumor without residual neurologic damage. Patients with the most complete tumor removal have the greatest chance of survival. Radiotherapy is used to treat most tumors and to shrink the size of the tumor before attempting surgical removal. Chemotherapy has emerged in the past decade to delay radiation in children younger than 3 years of age because of the rapid brain development occurring in the first 3 years of life (Blaney, Kun, Hunter, and others, 2006; Murray-Ryan and Petriccione, 2002). Chemotherapy is also used as adjunct therapy for residual tumor, nonresectable tumor, or recurrent tumor. Water-soluble agents are able to penetrate the disrupted blood-brain barrier and attack brain tumor cells (Blaney, Kun, Hunter, and others, 2006; Murray-Ryan and Petriccione, 2002). Typically, the most commonly used chemotherapy agents are cisplatin, carboplatin, vincristine, cyclophosphamide, lomustine, carmustine, etoposide, ifosfamide, and topotecan. Surgery (biopsy, resection, laser, or stereotactic), radiotherapy (hyperfractionated, fractionated, or stereotactic), and multiagent chemotherapy are all instrumental in the treatment of brain tumors.
Prognosis.: The prognosis for the child with a brain tumor depends on the type of brain tumor, the tumor’s size, the extent of the disease, and the child’s age. Problems associated with treatment and a relatively poor prognosis, primarily in infants and young children, are compounded by serious late effects of therapy. A decline in incidence of children with medulloblastoma has been significantly linked with a protective effect of maternal folate, iron, and multivitamin supplementation. Along with the recent advances in surgical instrumentation allowing aggressive surgical intervention (e.g., stereotactic surgery, radiosurgery), modifications in radiation (e.g., hyperfractionation, brain mapping) and use of chemotherapy (e.g., intrathecal, intratumoral) have increased the long-term survival rates for many children with brain tumors (Blaney, Kun, Hunter, and others, 2006; Alston, Newton, Kelsey, and others, 2003; Gupta and Berger, 2003; Murray-Ryan and Petriccione, 2002).
Nursing Care Management
A brain tumor is often suspected in a child admitted to the hospital with neurologic dysfunction, although the actual diagnosis may not yet be confirmed. Establishing a baseline of data with which to compare preoperative and postoperative changes is an essential step toward planning physical care and preventing complications. It also allows the nurse to assess the degree of physical incapacity and the family’s emotional reaction to the diagnosis.
Vital signs, including blood pressure and pulse pressure (the difference between systolic and diastolic pressures), are taken routinely and more often when any change is noted. Any sudden variations are reported immediately. It is especially important to note a change in vital signs during or after diagnostic procedures. A routine neurologic assessment is also performed at the same time as vital signs, and head circumference is measured on infants and very young children.
The child is observed for evidence of headache, vomiting, and any seizure activity. The location, severity, and duration of the headache are noted, as well as its relationship to activity and time of day. Behaviors such as lying flat and facing away from light or refusing to engage in play are clues to discomfort in the nonverbal child. The child’s gait is observed at least once daily. Head tilt and other changes in posturing are always noted.
Prevent Postoperative Complications.: Usually the surgeon will prescribe specific orders for vital signs, neurologic checks, positioning, fluid regulation, and medication. These vary somewhat, depending on the location of the craniotomy. The following are general principles of care for infratentorial or supratentorial surgery. Additional aspects of care that are discussed elsewhere may include care of the child with seizures and neurologic assessment of the unconscious child.
Vital signs are taken as frequently as every 15 to 30 minutes until the child is stable. Temperature measurement is particularly important because of hyperthermia resulting from surgical intervention in the hypothalamus or brainstem and from some types of general anesthesia. To prepare for this reaction, a cooling blanket should be placed on the bed before the child returns to the unit so that it is ready for use when needed. The temperature is monitored carefully when any cooling measures are taken because hypothermia can occur suddenly. Recognizing signs of other complications such as increased ICP, meningitis, and respiratory tract infection is imperative.
Neurologic checks are an essential aspect of care and include pupillary reaction to light, LOC, sleep patterns, and response to stimuli. Although children may be comatose for a few days, once they regain consciousness, there should be a steady increase in alertness. Regression to a lethargic, irritable state indicates increasing pressure, possibly caused by meningitis or cerebral edema.
Observations for function are not instituted until the child regains consciousness. However, as soon as possible the nurse should begin testing reflexes, handgrip, and functioning of the cranial nerves. Muscle strength is usually diminished as a result of general weakness after surgery but should improve daily. Ataxia may be significantly worse with cerebellar intervention, but it will slowly improve. Edema near the cranial nerves may depress important functions such as the gag, blink, or swallowing reflex.
Dressings are observed for evidence of drainage. If soiled, the dressing is not removed but is reinforced with dry sterile gauze. The approximate amount of drainage is estimated and recorded. A drain may be placed in the operative site.
Correct positioning after surgery is critical to prevent pressure against the operative site, reduce ICP, and avoid the danger of aspiration. If a large tumor was removed, the child is not placed on the operative side, since the brain may suddenly shift to that cavity, causing trauma to the blood vessels, linings, and the brain itself. The nurse confers with the surgeon to be certain of the correct position, including degree of neck flexion. The first 24 to 48 hours after brain surgery are critical. If the child’s position is restricted, notice of this is posted above the head of the bed. When the child is turned, every precaution is used to prevent jarring or malalignment to prevent undue strain on the sutures. Two nurses are needed—one supporting the head and the other supporting the body. The use of a turning sheet may facilitate turning a heavy child.
The child with an infratentorial procedure is usually positioned on either side with the bed flat. When a supratentorial craniotomy is performed, the head of bed is elevated 20 to 30 degrees with the child on either side or on the back. In a supratentorial craniotomy the head elevation facilitates CSF drainage and decreases excessive blood flow to the brain to prevent hemorrhage. Pillows should be placed against the child’s back, not head, to maintain the desired position. Ordinarily the head and neck are kept in midline with the body and the neck should not be flexed (Curley and Moloney-Harmon, 2001).
With an infratentorial craniotomy the child is allowed nothing by mouth for at least 24 hours, or longer if the gag and swallowing reflexes are depressed or the child is comatose. With a supratentorial operation, clear fluids may be resumed soon after the child is alert, sometimes within 24 hours. If the child vomits, oral liquids are stopped. Vomiting not only predisposes the child to aspiration, but also increases ICP and the potential for incisional rupture.
The child should be fed to conserve energy and minimize movement. If there is any sign of facial paralysis, the child is fed slowly to prevent choking or aspiration. Sometimes gavage feeding is necessary when body functions are too depressed to permit safe oral feedings or when the child refuses to eat or drink. IV fluids are continued until oral fluids are well tolerated. Because of the postoperative cerebral edema and danger of increased ICP, fluids are carefully monitored.
Headache may be severe and is largely a result of cerebral edema. Measures to relieve some of the discomfort include providing a quiet, dimly lit environment; restricting visitors; preventing any sudden jarring movement, such as banging into the bed; and preventing an increase in ICP. Avoiding increased ICP is most effectively achieved by proper positioning and prevention of straining, such as during coughing, vomiting, or defecating. The use of opioids, such as morphine, to relieve pain is controversial because it is thought that they may mask signs of altered consciousness or depress respirations. However, they can be given safely, since naloxone can be used to reverse opioid effects, such as sedation or respiratory depression. Acetaminophen and codeine are also effective analgesics for mild to moderate pain. Regardless of the drugs used, adequate dosage and regular administration are essential to providing optimal pain relief (see also Pain Assessment; Pain Management, Chapter 7). Placing an ice bag on the forehead may also provide some headache relief, especially if facial edema is severe.
Support Child and Family.: The family’s emotional needs are immense when the diagnosis is a brain tumor, and feelings are influenced by the extent of surgery, any neurologic deficits, the expected prognosis, and additional therapy.* Since few definitive answers can be given before surgery, the surgeon’s report is a significant finding that can vary from a completely benign, resected neoplasm to a highly malignant, invasive, and only partially removed tumor. Although parents try to prepare themselves for a potentially fatal diagnosis, it is a shock for them.
Parents should be encouraged to verbalize their feelings about the diagnosis. Often they express tremendous guilt for viewing the insidious onset of symptoms, such as ataxia, visual difficulty, or headache, as “minor complaints” by the child. Any comments that insinuate that the parents should have sought medical advice sooner are avoided, since such remarks only add to the parents’ guilt feelings.
During this period the nurse should also discuss with parents what they plan to tell the child. If the child was prepared honestly, the diagnosis can be expressed in a similar manner. During recovery the child will need additional explanation about the treatment and the reason for any residual neurologic effects, such as ataxia or blindness.
NEUROBLASTOMA
Neuroblastomas are the most common malignant extracranial solid tumors in children, accounting for 8% to 10% of all childhood cancers (Brodeur and Maris, 2006). They occur in about 1 per 10,000 live births, with a slightly higher incidence in boys. The majority of children with neuroblastoma manifest the disease before 10 years of age, with the median age of occurrence at 22 months (Brodeur and Maris, 2006). These tumors originate from embryonic neural crest cells that normally give rise to the adrenal medulla and the sympathetic ganglia. Consequently, the majority of tumors develop in the adrenal gland or the retroperitoneal sympathetic chain. Other sites may be in the head, neck, chest, or pelvis.
Neuroblastoma is a “silent” tumor. In more than 70% of cases, diagnosis is made after metastasis occurs, with the first signs caused by involvement in the nonprimary site, usually the lymph nodes, bone marrow, skeletal system, skin, or liver.
Diagnostic Evaluation
The objective of diagnosis is to locate the primary site and areas of metastasis. The signs and symptoms of neuroblastoma depend on the location and stage of the disease. Most presenting signs are caused by compression of adjacent structures. Skeletal survey; skull, neck, chest, abdominal, and bone CT scans; and bilateral bone marrow aspirations and biopsies are used to locate a tumor mass and metastasis. A metaiodobenzylguanidine (MIBG) scan is used to determine involvement of bone or tissue; however, it is only available at certain centers.
Urinary excretion of catecholamines is detected in approximately 95% of children with adrenal or sympathetic tumors. Analyzing the breakdown products excreted in the urine, namely vanillylmandelic acid (VMA), homovanillic acid (HVA), dopamine, and norepinephrine, permits detection of suspected tumor before and after medical-surgical intervention (Kline and Sevier, 2003; Brodeur and Maris, 2006). Amplification of proto-oncogene, known as the N-myc gene, and chromosomal abnormalities correlates strongly with advanced-stage disease, rapid tumor progression, and a poor prognosis (Brodeur and Maris, 2006).
Therapeutic Management
Accurate clinical staging is important for establishing initial treatment. Therefore surgery is used both to remove as much of the tumor as possible and to obtain biopsies. In early stages, complete surgical removal of the tumor is the treatment of choice. If the tumor is large, partial resection is attempted, with a course of irradiation postoperatively to shrink the tumor in the hope of complete removal at a later date. Surgery is usually limited to biopsy in stages III and IV because of the extensive metastasis, although the use of additional surgery to assess tumor regression or remove a regressed tumor is not unlikely.
Radiotherapy provides emergency management of a massive neuroblastoma that is causing spinal cord compression (Kline and Sevier, 2003; Nguyen, Sallah, Ludin, and others, 2000). Radiotherapy also offers palliation for metastatic lesions in the bones, lung, liver, or brain.
Chemotherapy is the mainstay of therapy for extensive local or disseminated disease. Agents used in various combinations include cyclophosphamide, doxorubicin, cisplatin, etoposide, vincristine, ifosfamide, carboplatin, topotecan, and teniposide. In children with high-risk disease or recurrent disease, retinoic acid, radiotherapy, and myeloablative chemotherapy with peripheral stem cell rescue may be used to obtain a longer remission, even though a poor overall survival rate is seen (Kline and Sevier, 2003; Brodeur and Maris, 2006).
Prognosis.: If all stages are grouped together, the 5-year disease-free survival rates range from 88% to 90% for children in the low-risk stage, and from 22% to 30% in children in the high-risk stage (Brodeur and Maris, 2006). Generally, the younger the child at diagnosis (especially younger than 1 year of age), the better the survival rate. Neuroblastoma is one of the few tumors that demonstrate spontaneous regression (especially stage IV-S), possibly as a result of maturity of the embryonic cell or the development of an active immune system.
Nursing Care Management
Nursing considerations are similar to those discussed for leukemia and brain tumors, including psychologic and physical preparation for diagnostic and operative procedures; prevention of postoperative complications for abdominal, thoracic, or cranial surgery; and explanation of chemotherapy, radiotherapy, and their side effects.
Since this tumor carries a poor prognosis for many children, every consideration must be given the family in terms of coping with a life-threatening illness (see Chapter 18). Because of the high degree of metastasis at the time of diagnosis, many parents suffer substantial guilt for not having recognized signs earlier. Parents need much support in dealing with these feelings and expressing them to the appropriate people.
INTRACRANIAL INFECTIONS
The nervous system is subject to infection by the same organisms that affect other organs of the body. However, the nervous system is limited in the ways in which it responds to injury. Laboratory studies are needed to identify the causative agent. The inflammatory process can affect the meninges (meningitis) or brain (encephalitis).
Meningitis can be caused by a variety of organisms, but the three main types are (1) bacterial, or pyogenic, caused by pus-forming bacteria, especially meningococci, pneumococci, and Haemophilus organisms; (2) viral, or aseptic, caused by a wide variety of viral agents; and (3) tuberculous, caused by the tuberculin bacillus. The majority of children with acute febrile encephalopathy have either bacterial meningitis or viral meningitis as the underlying cause.
BACTERIAL MENINGITIS
Bacterial meningitis is an acute inflammation of the meninges and CSF. The advent of antimicrobial therapy has had a marked effect on the course and prognosis, although the introduction of conjugate vaccines against Haemophilus influenzae type b (Hib vaccine) in 1990 has led to the most dramatic change in the epidemiology of bacterial meningitis (Centers for Disease Control and Prevention, 2002; Prober, 2007; Scheifele, Halperin, Law, and others, 2005) (see Evidence-Based Practice box). In 1993 the incidence of H. influenzae was two cases per 100,000 children younger than 5 years, whereas in 1987 the incidence was 41 per 100,000 (Centers for Disease Control and Prevention, 2002). Today, H. influenzae type b infection has been virtually eradicated among young children in areas in the world where the Hib vaccine is administered routinely (Centers for Disease Control and Prevention, 2002; Yogev and Guzman-Cottrill, 2005). Routine use of the conjugated pneumococcal vaccine introduced in 2000 may lead to world trends in young children similar to those experienced with the Hib vaccine (Yogev and Guzman-Cottrill, 2005). Practitioners are optimistic that the use of the new pneumococcal conjugate vaccine will produce a rapid and adequate antibody response in young children. Bacterial meningitis from Streptococcus pneumoniae will soon be on the decline (Prober, 2007).
Bacterial meningitis remains a significant cause of illness in the pediatric age-groups because of the residual damage caused by undiagnosed and untreated or inadequately treated cases. The majority of reported cases occur in children between 1 month and 5 years of age, with an increased mortality risk in the adolescent and young adult (Saez-Llorens and McCracken, 2003; Sotir, Ahrabi-Fard, Croft, and others, 2005).
Bacterial meningitis can be caused by a variety of bacterial agents. Currently H. influenzae type b, S. pneumoniae, and Neisseria meningitidis (meningococcus) are responsible for bacterial meningitis in 95% of children older than 2 months.
Other organisms are β-hemolytic streptococci, Staphylococcus aureus, and Escherichia coli. The leading causes of neonatal meningitis are group B streptococci, E. coli, and Listeria monocytogenes. E. coli infection is seldom seen beyond infancy. Meningococcal meningitis occurs in epidemic form and is the only type readily transmitted by droplet infection from nasopharyngeal secretions. Although this condition may develop at any age, the risk of meningococcal infection increases with the number of contacts; therefore it occurs predominantly in school-age children and adolescents.
There appear to be some seasonal variations. Meningitis caused by H. influenzae primarily occurs in autumn or early winter. Pneumococcal and meningococcal infections can occur at any time but are more common in later winter or early spring.
Pathophysiology
The most common route of infection is vascular dissemination from a focus of infection elsewhere. For example, organisms from the nasopharynx invade the underlying blood vessels and enter the cerebral blood supply or form local thromboemboli that release septic emboli into the bloodstream. Invasion by direct extension from infections in the paranasal and mastoid sinuses is less common. Organisms also gain entry by direct implantation after penetrating wounds, skull fractures that provide an opening into the skin or sinuses, lumbar puncture or surgical procedures, anatomic abnormalities such as spina bifida, or foreign bodies such as an internal ventricular shunt or an external ventricular device. Once implanted, the organisms spread into the CSF, by which the infection spreads throughout the subarachnoid space.
The infective process is like that seen in any bacterial infection: inflammation, exudation, white blood cell accumulation, and varying degrees of tissue damage. The brain becomes hyperemic and edematous, and the entire surface of the brain is covered by a layer of purulent exudate that varies with the type of organism. For example, meningococcal exudate is most marked over the parietal, occipital, and cerebellar regions; the thick, fibrinous exudate of pneumococcal infection is confined chiefly to the surface of the brain, particularly the anterior lobes; and the exudate of streptococcal infections is similar to that of pneumococcal infections, but thinner.
As infection extends to the ventricles, thick pus, fibrin, or adhesions may occlude the narrow passages and obstruct the flow of CSF.
Clinical Manifestations
The clinical manifestations of acute bacterial meningitis depend to a large extent on the child’s age. The picture is also influenced to some degree by the type of organism, the effectiveness of therapy for antecedent illness, and whether it occurs as an isolated entity or as a complication of another illness or injury. The onset of illness is likely to be abrupt, with fever, chills, headache, and vomiting that are associated with or quickly followed by alterations in sensorium. See Box 28-5 for clinical manifestations of bacterial meningitis.
BOX 28-5 Clinical Manifestations of Bacterial Meningitis
Usually abrupt onset
Seizures (often the initial sign)
Positive Kernig and Brudzinski signs
Classic picture (above) rarely seen in children between 3 months and 2 years of age
Frequent seizures (often accompanied by a high-pitched cry)
Nuchal rigidity (may or may not be present)
Brudzinski and Kernig signs not helpful in diagnosis
Children with Bacterial Meningitis and Preventive Vaccines
In children and adolescents with bacterial meningitis, has the administration of Haemophilus influenzae type b (Hib), pneumococcal, and meningococcal preventive vaccines reduced the incidence and mortality associated with bacterial meningitis?
CRITICALLY ANALYZE THE EVIDENCE
Laval, Pimenta, de Andrade, and others (2003) conducted a systematic review of several studies done in developed and developing countries that compared the effect of the conjugate of the Hib vaccine in the early 1990s to the more recent use of the heptavalent pneumococcal and the serogroup C meningococcal vaccines of today. The researchers concluded that all the vaccines mentioned have contributed directly to the decline in acute bacterial meningitis.
Data trends on Streptococcus pneumoniae infections from the Bacterial Core Surveillance of the Centers for Disease Control and Prevention were evaluated during 1998 to 2001. After being licensed in early 2000, the pneumococcal conjugate vaccine significantly reduced the number of invasive pneumococcal cases, with the largest decline in young children less than 2 years of age (Whitney, Farley, Hadler, and others, 2003).
Haddy, Perry, Chacko, and others (2005) compared the incidence of S. pneumoniae disease before and after the introduction of conjugated pneumococcal vaccine from 1999 to 2002. The trend in the rates of invasive pneumococcal disease cases showed significant declines during the study period for all ages after the introduction of the heptavalent S. pneumoniae protein conjugate vaccine.
Children’s Hospital of Pittsburgh reported the occurrence of bacterial meningitis before and after the licensure of the Hib conjugate vaccine. Two hundred and twenty-one children, ages 1 month to 18 years, diagnosed with bacterial meningitis were identified from 1988 to 1998. H. influenzae was the organism responsible for approximately 58% of cases of bacterial meningitis. The absolute number of cases of bacterial meningitis caused by H. influenzae declined to 2.5 cases per year after the introduction of the Hib conjugate vaccine (Neuman and Wald, 2001).
Data from an outbreak of meningococcal disease in northern Ghana in 1997 was used to assess the potential effect of different vaccination strategies. Vaccination conducted between February and April covered 72% of the high-risk population and prevented approximately 23% of the meningitis cases and 18% of the deaths related to meningitis. Routine childhood and adult immunization would have prevented 61% of cases had this same rate of vaccine coverage been achieved and maintained before the epidemic. This study suggests that the prevention of the meningococcal disease epidemic in West Africa will be difficult unless long-lasting conjugate meningococcal vaccines are incorporated into routine infant immunization schedules (Woods, Armstrong, Sackey, and others, 2000).
A double-blind randomized trial in Gambia was conducted to assess the efficacy of an Hib conjugate vaccine for the prevention of meningitis, pneumonia, and other invasive diseases caused by H. influenzae. From March 1993 to October 1995, 42,848 infants were randomly administered the conjugate vaccine Hib polysaccharide tetanus protein (PRP-T) mixed with diphtheria-tetanus-pertussis vaccine (DTP), or DTP alone at age 2 months, 3 months, and 4 months. Three doses of the vaccine were 95% effective in the prevention of meningitis and pneumonia caused by H. influenzae in the group of infants receiving the Hib vaccine (Mulholland, Hilton, Adegbola, and others, 1997).
APPLY THE EVIDENCE: NURSING IMPLICATIONS
The epidemiologic studies strongly suggest that all children should be immunized against the most common organisms responsible for bacterial meningitis (i.e., H. influenzae type b, S. pneumoniae, and N. meningitidis) as preventive vaccines to decrease the incidence of bacterial meningitis. The nurse should stress to the parents, children, adolescents, and young adults the importance of adhering to the immunization schedule to protect the child against serious childhood diseases.
REFERENCES
Haddy, RI, Perry, K, Chacko, CE, et al. Comparison of incidence in invasive Streptococcus pneumoniae disease among children before and after introduction of conjugated pneumococcal vaccine. Pediatr Infect Dis J. 2005;24(4):320–330.
Laval, CA, Pimenta, FC, de Andrade, JG, et al. Progress towards meningitis prevention in the conjugate vaccines era. Braz J Infect Dis. 2003;7(5):315–324.
Mulholland, K, Hilton, S, Adegbola, R, et al. Randomised trial of Haemophilus influenzae type-b tetanus protein conjugate for prevention of pneumonia and meningitis in Gambian infants. Lancet. 1997;349(9060):1191–1197.
Neuman, HB, Wald, ER. Bacterial meningitis in childhood at the Children’s Hospital of Pittsburgh: 1988-1998. Clin Pediatr (Phila). 2001;40(11):595–600.
Whitney, CG, Farley, MM, Hadler, J, et al. Decline in invasive pneumococcal disease after the introduction of protein—polysaccharide conjugate vaccine. N Engl J Med. 2003;348(18):1737–1746.
Woods, CW, Armstrong, G, Sackey, SO, et al. Emergency vaccination against epidemic meningitis in Ghana: implications for the control of meningococcal disease in West Africa. Lancet. 2000;355(9197):30–33.
Diagnostic Evaluation
A lumbar puncture is the definitive diagnostic test. The fluid pressure is measured, and samples are obtained for culture, Gram stain, blood cell count, and determination of glucose and protein content. The findings are usually diagnostic. Culture and sensitivity testing are needed to identify the causative organism. Spinal fluid pressure is usually elevated, but interpretation is often difficult when the child is crying. Sedation with fentanyl and midazolam can alleviate the child’s pain and fear associated with this procedure. If there is evidence or suspicion of increased ICP (papilledema, focal neurologic deficits, bulging fontanel), a CT scan of the head may be warranted before the procedure.
The patient generally has an elevated white blood cell count, often predominantly polymorphonuclear leukocytes. The glucose level is reduced, generally in proportion to the duration and severity of the infection. The relationship between the CSF glucose and serum glucose levels is important in evaluating the glucose content of CSF; therefore a serum glucose sample is drawn approximately one half hour before the lumbar puncture. Protein concentration is usually increased.
A blood culture is advisable for all children suspected of having meningitis and occasionally will be positive when CSF culture is negative. Nose and throat cultures may provide helpful information in some cases.