Nutrition in Exercise and Sports Performance
Successful athletic performance is a combination of favorable genetics, desire, proper training, and a sensible approach to nutrition. Whether an athlete is recreational or elite, young or mature, the importance of nutrition as a contributing factor to success in training and competition has been recognized for decades. Athletes attempting to gain a competitive edge will try almost any dietary regimen or artificial means, including nutritional supplements and oral or injectable medications, in the hope of reaching a new level of wellness or physical performance. Unfortunately, there is a plethora of misinformation on the topic of sports nutrition. Among college athletes, men are more likely than women to rely on strength coaches for supplement information. Athletes rely on trainers (71%), coaches (60%), and physicians (41%); they also refer to the Internet (79%), magazines (68%), and television (52%) for guidance (Malinauskas et al., 2007). Athletes can benefit from nutrition education and intervention by nutrition experts—increasing knowledge, self-efficacy, and dietary improvement.
Energy Production
The human body must be supplied continuously with energy to perform its many complex functions. As a person’s energy demands increase with exercise, the body must provide additional energy, or the exercise will cease. Two metabolic systems supply energy for the body: one dependent on oxygen (aerobic metabolism), and the other independent of oxygen (anaerobic metabolism). The use of one system over the other depends on the duration, intensity, and type of physical activity.
Adenosine Triphosphate
The body obtains its continuous supply of fuel through adenosine triphosphate (ATP), found within the cells of the body. ATP is the energy currency of the cell. The energy produced from the breakdown of ATP provides the fuel that activates muscle contraction. The energy from ATP is transferred to the contractile filaments (myosin and actin) in the muscle, which form an attachment of actin to the cross-bridges on the myosin molecule, thus forming actomyosin. Once activated the myofibrils slide past each other and cause the muscle to contract.
Resynthesizing Adenosine Triphosphate
Although ATP is the main currency for energy in the body, it is stored in limited amounts. In fact, only approximately 3 oz of ATP is stored in the body at any one time. This provides only enough energy for several seconds of exercise. ATP must continually be resynthesized to provide a constant energy source during exercise. When ATP loses a phosphate, thus releasing energy, the resulting adenosine diphosphate (ADP) is enzymatically combined with another high-energy phosphate from creatine phosphate (CP) to resynthesize ATP. The concentration of high-energy CP in the muscle is five times that of ATP.
Creatine kinase is the enzyme that catalyzes the reaction of CP with ADP and inorganic phosphate. It is the fastest and most immediate means of replenishing ATP, and it does so without the use of oxygen (anaerobic). Although this system has great power, it is time-limited because of the concentration of CP found in the muscles (see “Creatine” later in the chapter).
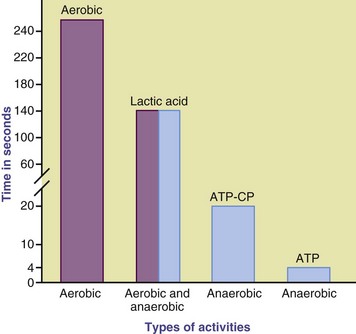
The energy released from this ATP-CP system will only support an all-out exercise effort of a few seconds, such as in a power lift, tennis serve, or sprint. If the all-out effort continues for longer than 8 seconds or if moderate exercise is to proceed for longer periods, an additional source of energy must be provided for the resynthesis of ATP (Figure 24-1). The production of ATP carries on within the muscle cells through either the anaerobic or aerobic pathways.
Anaerobic or Lactic Acid Pathway
The next energy pathway for supplying ATP for more than 8 seconds of physical activity is the process of anaerobic glycolysis. In this pathway the energy in glucose is released without the presence of oxygen. Lactic acid is the end product of anaerobic glycolysis. Without the production of lactic acid, glycolysis would shut down. The coenzyme called nicotinic acid dehydrogenase (NAD) is in limited supply in this pathway. When NAD is limited, the glycolytic pathway cannot provide constant energy. By converting pyruvic acid to lactic acid, NAD is freed to participate in further ATP synthesis. The amount of ATP furnished is relatively small (the process is only 30% efficient). This pathway contributes energy during an all-out effort lasting up to 60 to 120 seconds. Examples are a 440-yard sprint and many sprint-swimming events.
Although this process provides immediate protection from the consequences of insufficient oxygen, it cannot continue indefinitely. When exercise continues at intensities beyond the body’s ability to supply oxygen and convert lactic acid to fuel, lactic acid accumulates in the blood, lowers the pH to a level that interferes with enzymatic action, and causes fatigue. Lactic acid can be removed from the muscle; transported into the bloodstream; and converted to energy in muscle, liver, or brain. Otherwise, it is converted to glycogen. Conversion to glycogen occurs in the liver and to some extent in muscle, particularly among trained athletes.
The amount of ATP produced through glycolysis is small compared with that available through aerobic pathways. Substrate for this reaction is limited to glucose from blood sugar or the glycogen stored in the muscle. Liver glycogen contributes but is limited.
Aerobic Pathway
Production of ATP in amounts sufficient to support continued muscle activity for longer than 90 to 120 seconds requires oxygen. If sufficient oxygen is not present to combine with hydrogen in the electron transport chain, no further ATP is made. Thus the oxygen furnished through respiration is of vital importance. Here, glucose can be broken down far more efficiently for energy, producing 18 to 19 times more ATP. In the presence of oxygen, pyruvate is converted to acetyl coenzyme A (CoA), which enters the mitochondria. In the mitochondria acetyl CoA goes through the Krebs cycle, which generates 36 to 38 ATP per molecule of glucose (Figure 24-2).
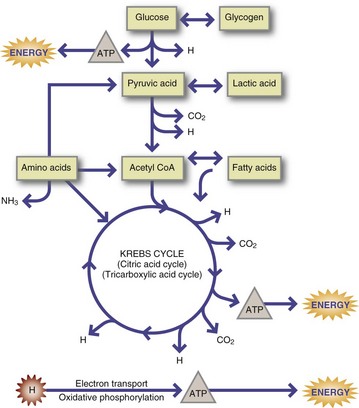
FIGURE 24-2 Pathways of energy production. ATP, Adenosine triphosphate; CoA, coenzyme A; H, hydrogen atoms.
Aerobic metabolism is limited by the availability of substrate, a continuous and adequate supply of oxygen, and the availability of coenzymes. At the onset of exercise and with the increase in exercise intensity, the capability of the cardiovascular system to supply adequate oxygen is a limiting factor, and this is largely due to the level of conditioning. The aerobic pathway can also provide ATP by metabolizing fats and proteins. A large amount of acetyl CoA, which enters the Krebs cycle and provides enormous amounts of ATP, is provided by β-oxidation of fatty acids. Proteins may be catabolized into acetyl CoA or Krebs cycle intermediates, or they may be directly oxidized as another source of ATP.
Energy Continuum
A person who is exercising may use one or more energy pathways. For example, at the beginning of any physical activity, ATP is produced anaerobically. As exercise continues, the lactic acid system produces ATP for exercise. If the person continues to exercise and does so at a moderate intensity for a prolonged period, the aerobic pathway will become the dominant pathway for fuel. On the other hand, the anaerobic pathway provides most of the energy for short-duration, high-intensity exercise such as sprinting; the 200-meter swim; or high-power, high-intensity moves in basketball, football, or soccer.
The production of ATP for exercise is on a continuum that depends on the availability of oxygen. Other factors that influence oxygen capabilities, and thus energy pathways, are the capacity for intense exercise and its duration. These two factors are inversely related. For example, an athlete cannot perform high-power, high-intensity moves over a prolonged period. To do this, he or she would have to decrease the intensity of the exercise to increase its duration (Figure 24-3).
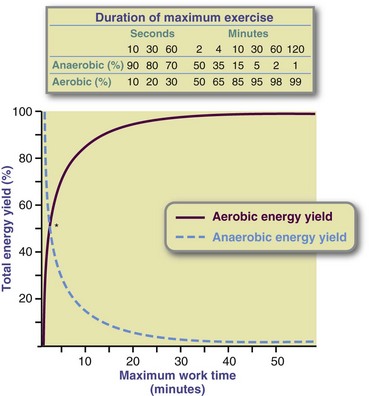
FIGURE 24-3 Relative contribution of aerobic and anaerobic energy during maximum physical activity of various durations. Note that 90 to 120 seconds of maximum effort requires 50% of the energy from each of the aerobic and anaerobic processes. This is also the point at which the lactic acid pathway for energy production is at its maximum.
The aerobic pathway cannot tolerate the same level of intensity as duration increases because of the decreased availability of oxygen and accumulation of lactic acid. As the duration of exercise increases, power output decreases. The contribution of energy-yielding nutrients must be considered also. As the duration of exercise lengthens, fats contribute more as an energy source. The opposite is true for high-intensity exercise; when intensity increases, the body relies increasingly on carbohydrates as substrate.
Fuels for Contracting Muscles
Protein, fat, and carbohydrate are all possible sources of fuel for muscle contraction. The glycolytic pathway is restricted to glucose, which can originate in dietary carbohydrates or stored glycogen, or it can be synthesized from the carbon skeletons of certain amino acids through the process of gluconeogenesis. The Krebs cycle is fueled by three-carbon fragments of glucose; two-carbon fragments of fatty acids; and carbon skeletons of specific amino acids, primarily alanine and the branched-chain amino acids. All these substrates can be used during exercise; however, the intensity and duration of the exercise determine the relative rates of substrate use.
Intensity
The intensity of the exercise is important in determining what fuel will be used by contracting muscles. High-intensity, short-duration exercise has to rely on anaerobic production of ATP. Because oxygen is not available for anaerobic pathways, only glucose and glycogen can be broken down anaerobically for fuel. When glycogen is broken down anaerobically, it is used 18 to 19 times faster than when glucose is broken down aerobically. Persons who are performing in high-intensity workouts or competitive races may run the risk of running out of muscle glycogen before the event or exercise is done as a result of its high use.
Sports that use both the anaerobic and aerobic pathways also have a higher glycogen use rate and, like anaerobic athletes, athletes in these sports also run the risk of running out of fuel before the race or exercise is finished. Sports such as basketball, football, soccer, and swimming are good examples; glycogen usage is high because of the intermittent bursts of high-intensity sprints and running drills. In moderate-intensity sports or exercise such as jogging, hiking, aerobic dance, gymnastics, cycling, and recreational swimming, approximately half of the energy for these activities comes from the aerobic breakdown of muscle glycogen, whereas the other half comes from circulating blood glucose and fatty acids.
Moderate- to low-intensity exercise such as walking is fueled entirely by the aerobic pathway; thus a greater proportion of fat can be used to create ATP for energy. Fatty acids cannot supply ATP during high-intensity exercise because fat cannot be broken down fast enough to provide the energy. Also, fat provides less energy per liter of oxygen consumed than does glucose (4.65 kcal/L of O2 versus 5.01 kcal/L of O2). Therefore when less oxygen is available in high-intensity activities, there is a definite advantage for the muscles to be able to use glycogen because less oxygen is required (Figure 24-4).

FIGURE 24-4 Running is a high-intensity exercise in which both carbohydrates and fat are used as fuels, depending on the speed and length of the event. (Courtesy Richard Andrews, Titusville, Fl.)
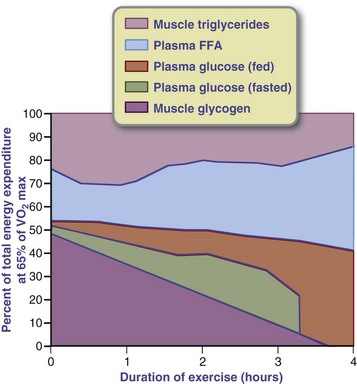
In general, both glucose and fatty acids provide fuel for exercise in proportions depending on the intensity and duration of the exercise and the fitness of the athlete. Exertion of extremely high intensity and short duration draws primarily on reserves of ATP and CP. High-intensity exercise that continues for more than a few seconds depends on anaerobic glycolysis. During exercise of low-to-moderate intensity (60% of maximum oxygen uptake [VO2max]), energy is derived mainly from fatty acids. Carbohydrate becomes a larger fraction of the energy source as intensity increases until, at an intensity level of 85% to 90% VO2max, carbohydrates from glycogen is the principal energy source, and the duration of activity is limited (Figure 24-5).
Duration
The duration of a training session determines the substrate used during the exercise bout. For example, the longer the time spent exercising, the greater the contribution of fat as the fuel. Fat can supply up to 60% to 70% of the energy needed for ultra-endurance events lasting 6 to 10 hours. As the duration of exercise increases, the reliance on aerobic metabolism becomes greater, and a greater amount of ATP can be produced from fatty acids. However, fat cannot be metabolized unless a continuous stream of some carbohydrates is also available through the energy pathways. Therefore muscle glycogen and blood glucose are the limiting factors in human performance of any type of intensity or duration.
Effect of Training
The length of time an athlete can oxidize fatty acids as a fuel source is related to the athlete’s conditioning, as well as the exercise intensity. In addition to improving cardiovascular systems involved in oxygen delivery, training increases the number of mitochondria and the levels of enzymes involved in the aerobic synthesis of ATP, thus increasing the capacity for fatty acid metabolism. Increases in mitochondria with aerobic training are seen mainly in the type IIA (intermediate fast-twitch) muscle fibers. These fibers however quickly lose their aerobic capacity with the cessation of aerobic training, reverting to the genetic baseline.
These changes from training result in a lower respiratory exchange ratio (RER), the amount of CO2 produced divided by the amount of O2 consumed, lower blood lactate and catecholamine levels, and a lower net muscle glycogen breakdown at a specific power output. These metabolic adaptations enhance the ability of muscle to oxidize all fuels, especially fat.
Nutritional Requirements of Exercise
The most important component of successful sport training and performance is to ensure adequate calorie intake to support energy expenditure and maintain strength, endurance, muscle mass and overall health. Energy and nutrient requirements vary with weight, height, age, sex, and metabolic rate (see Chapter 2) as well as the type, frequency, intensity, and duration of training and performance.
Individuals who participate in an overall fitness program (i.e., 30 to 40 min/day, three times per week) can generally meet their daily nutritional needs by following a normal diet providing 25 to 35 kcal/kg/day or roughly 1800 to 2400 calories a day. However, the 50-kg athlete engaging in more intense training of 2 to 3 hours/day five to six times a week or high-volume training of 3 to 6 hours in one to two workouts per day 5 to 6 days a week may expend up to an additional 600 to 1200 calories a day, thus requiring 50 to 80 kcal/kg/day or roughly 2500 to 4000 kcal/day. For elite athletes or heavier athletes, daily calorie needs can reach 150 to 200 kcal/kg, or roughly 7500 to 10,000 calories a day, depending on the volume and intensity of different training phases.
Meeting caloric needs for many fitness-minded and or elite, intensely training individuals can be a challenge. For working individuals, balancing daily training schedules with work and family responsibilities can compromise the quantity, quality, and timing of meals, which can greatly affect energy, strength levels, and overall health. In the elite athlete, consuming enough food at regular intervals without compromising performance is challenging, particularly for the collegiate athlete. School schedules, budgets, cafeteria schedules, travel requirements, and a varying appetite can further complicate the situation.
Meeting the daily energy needs and the appropriate macronutrient distribution for active individuals may necessitate the use of sports bars, drinks, and convenience foods and snacks in addition to whole foods and meals. Dietitians need to be flexible in accommodating lifestyles and eating behaviors when designing meal plans for maximum sport performance.
Sports Supplements
Sports supplements include the easy-to-carry, easy-to-consume, and easy-to-digest meal-replacement powders, ready-to-drink supplements, energy bars, and energy gels. This group represents 50% to 70% of the industry’s sales. These products are typically fortified with 33% to 100% of the recommended dietary allowances (RDAs) for vitamins and minerals; provide varying amounts and types of carbohydrates, protein, and fat; and are ideal for athletes on the run. They provide a portable, easy-to-consume food that can be used pericompetitively; while traveling; at work; in the car; or throughout the day at a multievent meet such as in track and field, swimming, diving, or gymnastics.
Many fitness-minded and athletic individuals use these products as a convenient way to enhance their current diet. These products are generally regarded as safe. However, if they are substituted in the place of whole foods on a regular basis, they can deprive the athlete of a well-balanced diet. They may also contain excesses of sugars, fats, and protein and banned substances such as caffeine, Ephedra, and other botanicals. See Table 24-1.
TABLE 24-1
Comparison of the Electrolyte Content between Standard Sport Drinks and Endurance-Specific Sport Drinks
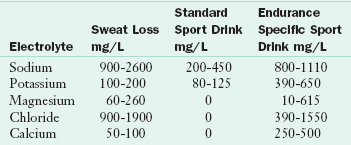
Source: First endurance. Accessed 14 July 2010 from http://blog.firstendurance.com/tag/electrolytes/.
Weight Management
In efforts to maximize performance, many athletes alter normal energy intake to either gain or lose weight. Although such efforts are sometimes appropriate, weight-reduction programs may involve elements of risk. For some young athletes achievement of an unrealistically light weight can jeopardize growth and development. Chronic dieting by female athletes can lead to eating disorders, delayed menarche, amenorrhea, and potential osteoporosis (see Chapters 23 and 25).
The goal weight of an athlete should be based on body fatness. Adequate time should be allowed for a slow, steady weight loss of approximately 1 to 2 lb each week over several weeks. Weight loss should be achieved before the competitive season begins to ensure maximum strength. In addition, the exercise should be of moderate intensity because at this level a greater proportion of energy is derived from fat than carbohydrate and the exercise can be sustained longer. When planned school-based activity programs are in effect, up to a 50% reduction in the incidence of overweight is feasible (Foster et al., 2008). Appropriate programs for weight management are discussed in Chapter 22.
Weight gain should be achieved through a gradual increase in energy intake combined with a strength training program to maximize muscle weight gain over fat gain. A realistic goal is  to 1 lb weekly. Fat intake should not exceed 30% of kilocalories from fat, and protein should be 1 to 1.5 g/kg of body weight. The professional working with an elite athlete must remember the tremendous motivation that comes from a desire to perform well in the sport.
to 1 lb weekly. Fat intake should not exceed 30% of kilocalories from fat, and protein should be 1 to 1.5 g/kg of body weight. The professional working with an elite athlete must remember the tremendous motivation that comes from a desire to perform well in the sport.
Macronutrients
Individuals engaging in a general fitness program can typically meet their macronutrient needs by consuming a normal diet of 45% to 55% of calories from carbohydrates (3 to 5 g/kg/day), 10% to 15% from protein (0.8 to 1 g/kg/day) and 25% to 35% from fat (0.5 to 1.5 g/kg/day). Athletes involved in moderate- to high-volume training need greater amounts of carbohydrates and protein to meet macronutrient needs. An intake of at 60% to 70% of total calories (5 to 8 g/kg/day or 250 to 1200 g/day for 50- to 150-kg athletes) should be met by carbohydrates. The remaining calories should be obtained from protein and fat. These percentages are only guidelines for estimating macronutrient requirements
Specific macronutrient recommendations should be used when counseling an active individual or athlete. When energy intake is high (more than 4500 calories/day), even a diet containing only 50% of the calories from carbohydrates would provide 500 g of carbohydrates, which is sufficient to maintain muscle glycogen stores. Similarly, if protein intake in this high-calorie diet were low, at 10% of calories, absolute protein intake would still exceed the recommendation for a 70-kg athlete. Thus specific recommendations should be based on an individual’s body size, body composition, sport, and gender. Calories and nutrients should come from a wide variety of foods on a daily basis.
Carbohydrate
The first source of glucose for the exercising muscle is its own glycogen store. When this is depleted, glycogenolysis and then gluconeogenesis (both in the liver) maintain the glucose supply (see Chapter 3). During endurance exercise that exceeds 90 minutes, such as marathon running, muscle glycogen stores become progressively lower. When they drop to critically low levels, high-intensity exercise cannot be maintained. In practical terms the athlete is exhausted and must either stop exercising or drastically reduce the pace. Athletes often refer to this as “hitting the wall.”
Glycogen depletion may also be a gradual process, occurring over repeated days of heavy training, in which muscle glycogen breakdown exceeds its replacement, as well as during high-intensity exercise that is repeated several times during competition or training. For example, a distance runner who averages 10 miles per day but does not take the time to consume enough carbohydrates in his or her diet, or the swimmer who completes several interval sets at maximum oxygen consumption within hours can deplete glycogen stores rapidly. A high-carbohydrate or glycogen loading (glycogen supercompensation) diet can help athletes maximize glycogen stores and be able to continue endurance performance.
The amount of carbohydrate required depends on the athlete’s total daily energy expenditure, type of sport, gender, and environmental conditions. Recommendations should provide for daily carbohydrate intake in grams relative to body mass, and allow flexibility for the athlete to meet these targets within the context of their energy needs and other dietary goals. Carbohydrate intake of 5 to 7 g/kg/day can meet general training needs, and 7 to 10 g/kg/day will suffice for endurance athletes. For example, a 70-kg (154-lb) athlete would consume 350 to 700 g of carbohydrate daily (see Table 24-1).
Types of Carbohydrate
Even though the effects of different sugars on performance, substrate use, and recovery has been studied extensively, the optimal type of carbohydrate for the athlete is debatable. The glycemic index represents the ratio of the area under the blood glucose curve resulting from the ingestion of a given quantity of carbohydrate and the area under the glucose curve resulting from the ingestion of the same quantity of white bread or glucose (see Chapter 31 and Appendix 43). Studies concerning whether the glycemic index of carbohydrate in the preexercise meal affects performance are inconclusive (Lin-Wu and Williams, 2006; Wong et al., 2009).
Carbohydrate Intake Before Exercise
The preevent or pretraining meal serves two purposes: (1) it keeps the athlete from feeling hungry before and during the exercise and (2) it maintains optimal levels of blood glucose for the exercising muscles. A preexercise meal can improve performance compared with exercising in a fasted state. Athletes who train early in the morning before eating or drinking risk developing low liver glycogen stores that can impair performance, particularly if the exercise regimen involves endurance training. Preexercise sports drinks (PRXs) are commonly used in athletic competitions requiring aerobic power. PRX (containing 14 g/serving of fructose, medium-chain triglycerides, and amino acids mixed with 8 oz of water) given 30 minutes prior to performing enhances indices of aerobic performance, specifically VO2max, time to exhaustion, and percentage of nonprotein fat substrate use (Byars et al., 2010).
Carbohydrate feedings before exercise can enhance liver glycogen stores. Although allowing for personal preferences and psychological factors, the preevent meal should be high in carbohydrates, nongreasy, and readily digested. Fat should be limited because it delays gastric emptying time and takes longer to digest. A meal eaten 3.5 to 4 hours before competition should be limited to 25% of the kilocalories from fat. Closer to the event, the fat content should be less than 25% (Box 24-1).
BOX 24-1 Examples of Pre-event Meals
For athletes who compete in events such as track or swimming meets or soccer, basketball, volleyball, and wrestling tournaments, nutritious, easy-to-digest food and fluid choices require attention. The athlete should consider the amount of time between eating and performance when choosing foods during these all-day events. Suggested precompetition menus include the following:
 plain bagel or English muffin
plain bagel or English muffin2 to 3 Hours Before Competition—Approximately 300-400 kcal
One of these choices:
 of turkey sandwich on white bread with baked chips
of turkey sandwich on white bread with baked chips bagel with low sugar jelly and 1 banana
bagel with low sugar jelly and 1 banana3 to 4 Hours Before Competition—Approximately 700 kcal
One of these selections:
Scrambled egg whites with white toast with low-sugar jam and banana
1 bagel with fat-free or low-fat cream cheese and low-sugar jelly and 1 banana
1 6-in turkey sub on Italian bread with lettuce, tomato, and mustard
1 3-oz grilled chicken breast with small baked potato, roll, and water
2 cups plain pasta with 1 plain roll
1 can of low fat sport shake with no more than 25 g protein, 1 sports bar, 1 banana, water
Exercising with a full stomach may cause indigestion, nausea, and vomiting. Thus the pregame meal should be eaten 3 to 4 hours before an event and should provide 200 to 350 g of carbohydrates (4 g/kg). Allowing time for partial digestion and absorption provides a final addition to muscle glycogen, additional blood sugar, and also relatively complete emptying of the stomach. To avoid gastrointestinal (GI) distress, the carbohydrate content of the meal should be reduced when the meal is close to the exercise time. For example, 4 hours before the event it is suggested that the athlete consume 4 g of carbohydrate per kilogram of body weight, whereas 1 hour before the competition the athlete would consume 1 g of carbohydrate per kilogram of body weight.
Commercial liquid formulas providing an easily digested high-carbohydrate fluid are popular with athletes and probably leave the stomach faster. Foods high in fiber, fat, and lactose will cause GI distress for some (e.g., bloating, gas, or diarrhea) and should be avoided before competition. Athletes should always use what works best for them by experimenting with foods and beverages during practice sessions and planning ahead to ensure that they have these foods available when they compete.
Carbohydrate Intake During Exercise
Carbohydrate consumed during endurance exercise lasting longer than 1 hour ensures the availability of sufficient amounts of energy during the later stages of exercise, improves performance, and enhances feeling of pleasure during and following exercise (Backhouse et al., 2005). Carbohydrate feeding does not prevent fatigue; rather, it simply delays it. During the final minutes of exercise, when muscle glycogen is low and athletes rely heavily on blood glucose for energy, their muscles feel heavy, and they must concentrate to maintain exercise at intensities that are ordinarily not stressful when muscle glycogen stores are full. Glucose ingestion during exercise has also been shown to spare endogenous protein and carbohydrates in fed cyclists without glycogen depletion (van Hamont et al., 2005). Thus consuming an exogenous carbohydrate during endurance exercise helps to maintain blood glucose and improve performance.
The form of carbohydrate does not seem to matter physiologically. Some athletes prefer to use a sports drink, whereas others prefer to eat a solid or gel and consume water. If a sports drink with carbohydrates is consumed during exercise, the rate of carbohydrate ingestion should be approximately 26 to 30 g every 30 minutes, an amount equivalent to 1 cup of a 6% to 8% carbohydrate solution taken every 15 to 20 minutes. This ensures that 1 g of carbohydrate will be delivered to the tissues per minute at the time fatigue sets in. It is unlikely that a carbohydrate concentration of less than 5% is enough to help performance, but solutions with a concentration greater than 10% are often associated with abdominal cramps, nausea, and diarrhea.
Combining protein and carbohydrates in a sport fluid or snack may also improve performance, muscle protein synthesis and net balance, and recovery. A small amount of amino acids ingested in small amounts alone or in conjunction with carbohydrates before or after exercise appears to improve net protein balance and may stimulate protein synthesis and improve net protein balance at rest during exercise and postexercise recovery (Millard-Stafford et al., 2005).
Carbohydrate Intake After Exercise
On average, only 5% of the muscle glycogen used during exercise is resynthesized each hour following exercise. Accordingly, at least 20 hours will be required for complete restoration after exhaustive exercise, provided approximately 600 g of carbohydrates are consumed. The highest muscle glycogen synthesis rates have been reported when large amounts of carbohydrates—1 to 1.85 g/kg/hr—are consumed immediately after exercise and at 15- to 60-minute intervals thereafter for up to 5 hours after exercise. Delaying carbohydrate intake for too long after exercise reduces muscle glycogen resynthesis.
It also appears that the consumption of carbohydrates with a high glycemic index results in higher muscle glycogen levels 24 hours after exercise compared with the same amount of carbohydrates provided as foods with a low glycemic index (Wilson M et al., 2009). Adding approximately 5 to 9 g of protein with every 100 g of carbohydrate eaten after exercise may further increase glycogen resynthesis rate, provide amino acids for muscle repair and promote a more anabolic hormonal profile (Millard-Stafford et al., 2005).
Many athletes find it difficult to consume food immediately after exercise. Usually when body or core temperature is elevated, appetite is depressed, and it is difficult to consume carbohydrate-rich foods. Many athletes find it easier and simpler to drink their carbohydrate or to consume easy-to-eat, carbohydrate-rich foods such as fruit pops, bananas, oranges, melon, or apple slices.
Protein
There has been considerable debate regarding the protein needs of athletes. The current RDA is 0.8 g/kg bodyweight and the acceptable macronutrient distribution range for protein for 18 years and older is 10% to 35% of total calories. Factors affecting the protein needs of athletes include age, gender, mass, fitness level, regimen, and phase of training. Nitrogen balance studies in endurance athletes suggest a range of 1.2 g/kg to 1.4 g/kg/day, and for strength athletes 1.2 to 1.7 g/kg/day with the higher end of the range recommended in early season (Rodriguez et al., 2009).
Reports of food intake in athletes and nonathletes consistently indicate that protein represents from 12% to 20% of total energy intake or 1.2 to 2 g of protein per kilogram of body weight daily. The exception to the rule is small, active women who may consume a low-energy intake in conjunction with an exercise or training program. Although these women may consume close to the RDA for protein in conjunction with the restricted energy intake, it may be inadequate to maintain lean body mass.
Intermittent bouts of high-intensity interval training (HIIT) depletes energy substrates and allows for metabolite accumulation. Studies suggest that supplementation with beta-alanine may improve endurance performance as well as lean body mass (Smith et al., 2009). However, the need for protein during exercise is just slightly elevated above that for sedentary persons. Consuming more protein than the body can use is not necessary and should be avoided.
When athletes consume diets that are high in protein, they compromise their carbohydrate status, which may affect their ability to train and compete at peak levels. High protein intakes can also result in diuresis and potential dehydration. Protein foods are often also high in fat, and consumption of excess protein can create difficulty in maintaining a low-fat diet.
Protein Needs for Resistance Exercise
Protein needs for resistance exercise involve maintenance (minimum protein required to accomplish nitrogen equilibrium), and the need for increasing lean tissue (positive nitrogen balance). For bodybuilders or persons interested in increasing body mass, the mythology of increased protein need is rampant. Strategies to increase the concentration and availability of amino acids after resistance exercise such as timing of snacks and meals have become an area of interest. See Clinical Insight: How Does Type, Timing, and Amount of Protein Affect Muscle Hypertrophy?
 Clinical Insight
Clinical Insight
How Does Type, Timing, and Amount of Protein Affect Muscle Hypertrophy?
Although many factors appear to contribute to overall muscle hypertrophy, nutritional factors that control protein synthesis during exercise are not well understood, leaving experts in discord about the type, amount, and timing of meals to enhance protein synthesis and muscle hypertrophy (Pennings, 2010). Resistance training and diet consistently appear to play a role in postworkout muscle protein synthesis. Many studies support supplementation of free-form amino acids or whole protein to enhance training. A 2005 study with resistance-trained participants for 14 weeks demonstrated that the administration of a protein supplement resulted in greater increases in cross-sectional muscle size of types I and II fibers and greater increase in squat height (Anderson et al., 2005). In another study, a postexercise trial, including a mixture of carbohydrate and whey protein consumed 1 hour after exercise resulted in a more immediate and overall greater protein synthesis response, whereas the addition of free essential amino acids before and after exercise also was shown to cause a rapid increase in protein synthesis and balance (Kerksick and Leutholtz, 2005). This higher rate of protein synthesis after exercise has been shown to occur in both young and elderly men (Pennings, 2010).
Although the optimal amount of amino acids to ingest for maximum protein synthesis is not known, a study examined the effect of 25 g of whey and casein protein solution before and after a strength-training session (STS). When consumed 30 minutes before an STS, there were significant increases in growth hormone, testosterone, free fatty acids, and serum insulin, and significantly increased postexercise oxygen consumption and respiratory exchange ratio during the 2 hours after exercise; hence there was a more anabolic environment for muscle growth (Hulmi et al., 2005).
For athletes interested in muscle hypertrophy, it appears that the neither the type nor the amount of protein matters if the day’s total amount is within the recommended range for resistance-training athletes of 1.2 to 2 g of protein per kilogram of body weight per day. Sports nutrition professionals can use these data to construct pre- and postworkout formulas to enhance the resistance training sessions of their clients.
Fat
Even though maximum performance is impossible without muscle glycogen, fat also provides energy for exercise. Fat is the most concentrated source of food energy, supplying 9 kcal/g. Essential fatty acids are necessary for cell membranes, skin, hormones, and transport of fat-soluble vitamins. The body has total glycogen stores (both muscle and liver) equaling approximately 2600 calories, whereas each pound of body fat supplies 3500 calories. This means that an athlete weighing 74 kg (163 lb) with 10% body fat has 16.3 lb of fat, which equals 57,000 calories.
Fat is the major, if not most important, fuel for light- to moderate-intensity exercise. Although fat is a valuable metabolic fuel for muscle activity during longer aerobic exercise and performs many important functions in the body, more than the usual recommended amount of fat is not indicated. In addition, athletes who consume a high-fat diet typically consume fewer calories from carbohydrate.
The diet content also determines which substrate is used during an exercise bout. If an athlete is consuming a high-carbohydrate diet, he or she will use more glycogen as fuel for the exercise. If the diet is high in fat, more fat will be oxidized as a fuel source. Fat oxidation rates decline after the ingestion of high-fat diets, partly because of adaptations at the muscle level and decreased glycogen stores. Fasting longer than 6 hours optimizes fat oxidation; however, the ingestion of carbohydrates in the hours before or at the beginning of an exercise session augments the rate of fat oxidation significantly when compared with fasting (Achten and Jeukendrup, 2004).
Exercise intensity and duration are important determinants of fat oxidation. Fat oxidation rates decrease when exercise intensity becomes high. A high-fat diet has been shown to compromise high-intensity performance even when a high-fat diet regimen is followed by carbohydrate loading before high-intensity performance (Havemann et al., 2005). The mode and duration of exercise can also affect fat oxidation; running increases fat oxidation more than cycling (Achten and Jeukendrup, 2004).
Fats, Inflammation and Sports Injury
When players get injured, they want to heal and get back on the field as soon as possible. Specific foods at the right time can help to provide energy for rehabilitation, rebuild strength, and ensure a complete, healthy, and faster recovery.
Stress to muscle leads to inflammation, bruising and tissue breakdown. Failure to decrease inflammation can lead to scar tissue, poor mobility, and delayed recovery times. The inflammatory stage is impacted by foods, especially the types of dietary fat consumed. A diet high in trans fats, saturated fats, and some ω-6 vegetable oils has been shown to promote inflammation while a diet high in monounsaturated fat and essential ω-3 fats has been shown to be anti-inflammatory. Monounsaturated fats like olive, peanut, canola, and sesame oils as well as avocado also inhibit and reduce inflammation by interfering with pro-inflammatory compounds such as leukotrienes, which are produced naturally by the body. Diets high in ω-3s have been shown to increase collagen deposition and promote healing. New research also suggests that ω-3s may impact healing from concussions.
Supplemental ω-3 fat has been recommended during the inflammation stage especially when the diet is deficient. However, there are also concerns regarding the usual source of ω-3 fats and fish oils since some have been found to be contaminated with mercury and polychlorinated biphenyls (PCBs), toxins dangerous to humans.
Fruits and vegetables are also good sources of alpha linolenic acid, an ω-3. See Appendix 40. However, the conversion to the more active forms of ω-3s, DHA and EPA, in the body is very low. Plant-based foods rich in ALA include: kidney beans, navy beans, tofu, winter and summer squash, certain berries such as raspberries and strawberries, broccoli, cauliflower, green beans, romaine lettuce, and collard greens. Wheat germ and free-range beef and poultry are also good sources of ω-3 fats since they are fed with ω-3 rich food.
Vitamins and Minerals
Unless an individual is deficient in a given nutrient, supplementation with that nutrient does not have a major effect on performance. Several nutrients are of concern for athletes. A daily intake of less than one third of the RDA for thiamin, riboflavin, B6, and vitamin C, even when other vitamins are supplemented, may lead to a significant decrease in VO2max and the anaerobic threshold in less than 4 weeks. Iron and calcium are the two minerals most likely to be low in the diet of young athletes.
Training and work schedules, low-nutrient snacks, infrequent nutrient-dense meals, and overall low calorie intakes may cause inadequate intakes of vitamins and minerals. Because many women athletes are also vegetarians, zinc, iron, and vitamin B12 may be of concern. In one study, female athletes failed to meet the estimated average requirement for folate in 48% of cases, calcium (24%), magnesium (19%), and iron (4%) (Heaney et al., 2010).
When limited to 100% of the dietary reference intakes (DRIs), vitamin supplementation is generally regarded as safe. Excess amounts may contribute to health problems; athletes need to understand that more is not always better. The DRIs for vitamins and minerals are the guide for determining nutritional needs, and upper levels have been established (see Chapter 12 and inside front cover).
B Vitamins
Increased energy metabolism creates a need for more of the B vitamins that serve as part of coenzymes involved in the energy cycles. Studies have shown that athletes can become depleted in some B vitamins, and in these athletes dietary change or supplementation improves exercise performance. For some athletes such as wrestlers, gymnasts, or rowers who consume low-calorie diets for long periods, a B-vitamin supplement to meet the RDA may be appropriate. There is no evidence that supplementing the well-nourished athlete with more B vitamins will increase performance
A deficiency of vitamin B12 could develop in a vegetarian athlete after several years of a strict vegan intake; thus a vitamin B12 supplement is warranted. There is a possibility of altered B12 metabolism based on serum homocysteine concentrations. The intake of folic acid is marginal for a large portion of the U.S. population and could be low in an athlete whose consumption of whole fruits and vegetables is low. A folate supplement to meet the RDA plus wheat, grain, and fortified products can be suggested to boost dietary intake of folate.
Antioxidants
Antioxidants have been studied individually and collectively for their potential to enhance exercise performance or to prevent exercise-induced muscle tissue damage. Cells continuously produce free radicals and reactive oxygen species (ROS) as a part of metabolic processes. The rate of whole-body oxygen consumption during exercise may increase 10- to 15-fold, or as much as 100-fold in active peripheral skeletal muscles. Oxidative stress increases the generation of lipid peroxides and free radicals. The magnitude of stress depends on the ability of the body’s tissues to detoxify ROS.
Free radicals are neutralized by antioxidant defense systems that protect the cell membrane from oxidative damage. These systems include catalase; superoxide dismutase; glutathione peroxidase; antioxidant vitamins A, E, and C; selenium; and phytonutrients such as carotenoids (see Focus On: Eating to Detoxify in Chapter 20).
Whether exercise increases the need for additional antioxidants in the diet is unclear. Watson and colleagues (2005) compared antioxidant-restricted diets and high-antioxidant diets of trained athletes running for 40 minutes (acute high-intensity exercise); they found an increased rate of perceived exertion, significantly higher levels of oxidative stress markers, and up to 1 hour of recovery in those with antioxidant-deficient diets. In a more recent study, for the first time the antioxidant status of athletes was changed by live-high-train-low (LHTL) conditioning or acute hypoxic exposure, and remained impaired after 14 days of recovery (Pialoux et al., 2010).
Vitamins with antioxidant activity neutralize free radicals. The question is whether they enhance recovery from exercise. Susceptibility to oxidative stress appears to vary from person to person and the effect varies by diet, lifestyle, environmental factors, and training (Pialoux et al., 2009). Antioxidant nutrients may enhance recovery from exercise, maintaining optimal immune response, and lowering lipid peroxidation after exercise.
Evidence suggests that the antioxidant compounds found in tart cherry juice can help to reduce inflammation, muscle damage and oxidative stress following marathon running. An unexpected effect of tart cherry juice is that it may also have beneficial effect on sleep which has been attributed to the high melatonin content of tart cherries and its impact on sleep quality (Howatson et al., 2010; Kuehl et al., 2010; Pigeon et al., 2010). A diet rich in fruits and vegetables can ensure an adequate intake of antioxidants and prudent use of an antioxidant supplement may provide insurance against a suboptimal diet and the increased stress from exercise.
Vitamin C
Vitamin C is involved in a number of important biochemical pathways that are important to exercise metabolism and the health of athletes. The effect of vitamin C supplementation on performance has received considerable attention, mainly because athletes consume vitamin C in large quantities, generally because of the volume of food they consume. In studies in which athletes were deficient in vitamin C, supplementation improved physical performance, but a thorough analysis of these studies supports the general conclusion that vitamin C supplementation does not increase physical performance capacity in subjects with normal body levels of vitamin C. On the other hand, because exercise is a stressor to the body, some nutritionists recommend that the active individual may need more vitamin C than the DRI.
Vitamin E
Vitamin E is used widely as a supplement by athletes who hope to improve performance. Vitamin E may protect against exercise-induced oxidative injury and acute immune response changes. Over the course of an exercise season with intense workouts and competition, vitamin E supplementation of 200 to 450 IU daily may prevent oxidative injury; further studies are recommended.
Vitamin D
Research has shown that up to 77% of athletes who live in northern climates with little winter sunlight may be affected by deficiencies of vitamin D (Cannell et al., 2009).
Athletes who are at risk for Vitamin D deficiency include those who:
are lactose intolerant and avoid milk and dairy
live in colder, less sunny climates
have darker skin, like African-Americans, even if they live and train in sunny climates
use sun block on exposed areas or wear extensive clothing (Cannell et al., 2009; Larson-Meyer and Willis, 2010)
Blood tests can determine deficiency states. A measurement of 25-(OH) vitamin D levels of 50 ng/mL or less may be cause for concern. The most improvement with supplementation will be for those with a value of 15 to 30 ng/mL, followed by those with 30 to 50 ng/mL (Cannell et al., 2009).
Although the specific amount of vitamin D needed to reverse deficiency states has not been determined, partly because it is dependent on the extent of deficiency, athletes should be tested and guided by a health professional if diagnosed with a deficiency. The RDA for males and females under age 70 is 600 IU and for those 70 and over, 800 IU/day. The tolerable upper intake level (UL) is 4000 IU/day for all individuals age 9 and older (IOM, 2011).
Iron
Iron is critical for sport performance. As a component of hemoglobin, it is instrumental in transporting oxygen from the lungs to the tissues. It performs a similar role in myoglobin, which acts within the muscle as an oxygen acceptor to hold a supply of oxygen readily available for use by the mitochondria. Iron is also a vital component of the cytochrome enzymes involved in the production of ATP. Thus it follows that iron-deficiency anemia limits aerobic endurance and the capacity for work. Even partial depletion of iron stores in the liver, spleen, and bone marrow, as evidenced by low serum ferritin levels, can have a detrimental effect on exercise performance, even when anemia is not present (see Chapters 8 and 33).
Although iron-deficiency anemia is not frequent in athletes, suboptimal serum ferritin levels are relatively common (Sinclair and Hinton, 2005). Athletes at risk are the rapidly growing male adolescent; the female athlete with heavy menstrual losses; the athlete with an energy-restricted diet; distance runners who may have increased GI iron loss, hematuria, hemolysis caused by foot impact, and myoglobin leakage; and those training heavily in hot climates with heavy sweating. All athletes, especially female long-distance runners and vegetarians, should be screened periodically to assess their iron status.
Heavy training can also cause a transient decrease in serum ferritin and hemoglobin that may be experienced by some athletes. This was once called sports anemia, but erythrocyte morphology remains normal, and performance does not appear to deteriorate. These decreases in serum ferritin and hemoglobin are a result of an increase in plasma volume, which causes a hemodilution and appears to have no effect on performance (see Chapter 33).
Some athletes, especially long-distance runners, experience GI bleeding. Iron loss through GI bleeding can be detected by fecal hemoglobin assays. GI bleeding is related to the intensity and duration of the exercise, the ability of the athlete to stay hydrated, how well the athlete is trained, and whether he or she has taken ibuprofen before the competition.
The iron concentration in sweat is lower in a hot environment. Iron supplementation can be beneficial in improving iron stores of athletes who are iron depleted, but the effects on aerobic performance of nonanemic athletes are equivocal. Because large doses of iron (75 mg/day) may be toxic in persons with the genetic disorder hemochromatosis (see Chapter 33), such supplements should be used only by those diagnosed as iron depleted or anemic.
If true iron depletion is present, iron supplementation along with vitamin C to enhance its absorption is appropriate. Oral iron therapy is effective and maintains performance in runners who are deficient in iron but not anemic (see Chapter 33). Some athletes experience iron deficiency without anemia, a condition with normal hemoglobin levels but reduced levels of serum ferritin (20 to 30 ng/mL; see Chapter 8). Iron supplementation may restore serum ferritin to normal; it may not have an effect on performance (Williams, 2005).
Calcium
Osteoporosis is a major health concern, especially for women. Although the disease has been regarded as a problem of older women, young women, especially those who have had interrupted menstrual function, may be at risk for decreased bone mass.
The female athlete triad is a disturbing pattern in women’s athletics (see Chapter 23). Strategies to promote the resumption of menses include estrogen replacement therapy, weight gain, and reduced training. Regardless of menstrual history, most female athletes need to increase their calcium and vitamin D3 intake, as well as magnesium. Low-fat and nonfat dairy products, calcium-fortified fruit juices, calcium-fortified soy milk, and tofu made with calcium sulfate are all good sources.
Fluid
Maintaining fluid balance requires the constant integration of input from hypothalamic osmoreceptors and vascular baroreceptors so that fluid intake matches or modestly exceeds fluid loss (Murray, 2006). Proper fluid balance maintains blood volume, which in turn supplies blood to the skin for body temperature regulation. Because exercise produces heat, which must be eliminated from the body to maintain appropriate temperatures, regular fluid intake is essential. Any fluid deficit that is incurred during an exercise session can potentially compromise the subsequent exercise bout.
The body maintains appropriate temperatures by thermoregulation. As heat is generated in the muscles during exercise, it is transferred via the blood to the body’s core. Increased core temperature results in increased blood flow to the skin; in cool to moderate ambient temperatures, heat is then transferred to the environment by convection, radiation, and evaporation.
Environmental conditions have a large effect on thermoregulation. When ambient temperatures range from warm to hot, the body must dissipate the heat generated from exercise, as well as the heat absorbed from the environment. When this occurs, the body relies solely on the evaporation of sweat to maintain appropriate body temperatures. Thus maintaining hydration becomes crucial when ambient temperatures reach or exceed 36° C (96.8° F). The hotter the temperature, the more important sweating is for body-heat dissipation. Exercise in the heat also affects blood flow and alters the stress response, with modest changes in circulating leukocytes and cytokines. A critical threshold for elevation of body temperature is 6° F (3.5° C), above which the systemic inflammatory response leads to heatstroke (Peake, 2010).
Humidity affects the body’s ability to dissipate heat to a greater extent than air temperatures. As humidity increases, the rate at which sweat evaporates decreases, which means more sweat drips off the body without transferring heat from the body to the environment. Combining the effects of a hot, humid environment with a large metabolic heat load produced during exercise taxes the thermoregulatory system to its maximum. Ensuring proper and adequate fluid intake is key to reducing the risk of heat stress.
Fluid Balance
Body fluid balance is regulated by mechanisms that reduce urinary water and sodium excretion, stimulate thirst, and control the intake and output of both water and electrolytes. In response to dehydration, antidiuretic hormone (ADH or vasopressin) and the renin-angiotensin II–aldosterone system increase water and sodium retention by the kidneys and provoke an increase in thirst. These hormones maintain the osmolality, sodium content, and volume of extracellular fluids and play a major role in the regulation of fluid balance (see Chapter 7).
Water losses throughout the course of the day include those from sweat and the respiratory tract, plus losses from the kidneys and GI tract. When fluid is lost from the body in the form of sweat, plasma volume decreases and plasma osmolality increases. The kidneys, under hormonal control, regulate water and solute excretion in excess of the obligatory urine loss. However, when the body is subjected to hot environments, hormonal adjustments occur to maintain body function. Some of these adjustments include the body’s conservation of water and sodium and the release of ADH by the pituitary gland to increase water absorption from the kidneys. These changes cause the urine to become more concentrated, thus conserving fluid and making the urine a dark gold color. This feedback process helps to conserve body water and blood volume.
At the same time, aldosterone is released from the adrenal cortex and acts on the renal tubules to increase the resorption of sodium, which helps maintain the correct osmotic pressure. These reactions also activate thirst mechanisms in the body. However, in situations in which water losses are increased acutely such as in athletic workouts or competition, the thirst response can be delayed, making it difficult for athletes to trust their thirst to ingest enough fluid to offset the volume of fluid lost during training and competition. A loss of 1.5 to 2 L of fluid is necessary before the thirst mechanism kicks in, and this level of water loss already has a serious effect on temperature control. Athletes need to rehydrate on a timed basis rather than as a reaction to thirst, and it should be enough to maintain the preexercise weight.
Daily Fluid Needs
Daily fluid intake recommendations for sedentary individuals vary greatly because of the wide disparity in daily fluid needs created by body size, physical activity, and environmental conditions. The DRI for water and electrolytes identify the adequate intake for water to be 3.7 L/day in men (130 oz/day, 16 cups of fluid/day) and 2.7 L/day for women (95 oz/day, approximately 12 cups/day) (Institute of Medicine, 2004). Approximately 20% of the daily water need comes from water found in fruits and vegetables; the remaining 80% is provided by beverages, including water, juice, milk, coffee, tea, soup, sports drinks, and soft drinks.
When individuals work, train, and compete in warm environments, their fluid needs can increase to more than 10 L/day. The water required to excrete the urea from protein metabolism and excess electrolyte intake adds to the daily needs. However, for active individuals this volume is relatively small (130 mL/1000 kcal) and inconsequential because usually they are consuming more than 2 L each day (Murray, 2006).
Fluid Replacement
Several opinions are published by a variety of professional organizations that address fluid and electrolyte replacement before, during, and after exercise. A summary of these recommendations can be found in Box 24-2. The groups that developed these statements include the American College of Sports Medicine, the National Athletic Trainers Association, the American Academy of Pediatrics, the American Dietetic Association and the Dietitians of Canada, the International Marathon Directors Association, the Inter-Association Task Force on External Heat Illnesses, and USA Track and Field.
When possible, fluid should be consumed at rates that closely match sweating rate. It appears that plain water is not the best beverage to consume following exercise to replace the water lost as sweat (Murray, 2006). Although specific recommendations differ slightly, the intent is to keep athletes well hydrated.
Electrolytes
The replacement of electrolytes as well as water is essential for complete rehydration (see Table 24-1).
Sodium
It is important to include sodium in fluid-replacement solutions, especially with excessive intake of plain water (Hew, 2005; Noakes et al., 2005). For events lasting more than 2 hours, sodium should be added to the fluid to replace losses and to prevent hyponatremia. Rehydration with water alone dilutes the blood rapidly, increases its volume, and stimulates urine output. Blood dilution lowers both sodium and the volume-dependent part of the thirst drive, thus removing much of the drive to drink and replace fluid losses.
The potential benefits of temporary hyperhydration with sodium salts is important. Sodium losses can contribute to heat cramping, especially among football players (Stofan et al., 2005). Besides individual variations, the intensity and duration of workouts appear to play a role in the amount of sodium lost.
Water-soluble electrolytes such as sodium can move rapidly across the proximal intestines. During prolonged exercise lasting more than 4 to 5 hours, including sodium in replacement fluids increases palatability and facilitates fluid uptake in the intestines. Both sodium and carbohydrate are actively transported from the lumen to the bloodstream.
Water replacement in the absence of supplemental sodium can lead to decreased plasma sodium concentrations. As plasma sodium levels fall below 130 mEq/L, symptoms can include lethargy, confusion, seizures, or loss of consciousness. Exercise-induced hyponatremia may result from fluid overloading during prolonged exercise over 4 hours. Hyponatremia is associated with individuals who drink plain water in excess of their sweat losses or who are less physically conditioned and produce a saltier sweat.
Potassium
As the major electrolyte inside the body’s cells, potassium works in close association with sodium and chloride in maintaining body fluids, as well as generating electrical impulses in the nerves, muscles, and heart. Potassium balance is regulated by aldosterone and regulation is precise. Although aldosterone acts on sweat glands to increase the resorption of sodium, potassium secretion is unaffected. Loss of potassium from skeletal muscle has been implicated in fatigue during athletic events. There is little loss of potassium through sweat; loss of 32 to 48 mEq/day does not appear to be significant and is easily replaced by diet.
Fluid Absorption
The speed at which fluid is absorbed depends on a number of different factors, including the amount, type, temperature, and osmolality of the fluid consumed and the rate of gastric emptying. Because glucose is actively absorbed in the intestines, it can markedly increase both sodium and water absorption. A carbohydrate-electrolyte solution enhances exercise capacity by elevating blood sugar, maintaining high rates of carbohydrate oxidation, preventing central fatigue, and reducing perceived exertion (Byrne et al., 2005).
Early studies indicate that water absorption is maximized when luminal glucose concentrations range from 1% to 3% (55 to 140 mM); however, most sports drinks contain two to three times this quantity without causing adverse GI symptoms. To determine the concentration of carbohydrate in a sports drink, the grams of carbohydrate or sugar in a serving are divided by the weight of a serving of the drink, which is usually 240 g, the approximate weight of 1 cup of water. A 6% carbohydrate drink contains 14 to 16 g of carbohydrate per 8 oz (1 cup).
Cold water is preferable to warm water because it attenuates changes in core temperature and peripheral blood flow, decreases sweat rate, speeds up gastric emptying, and is absorbed more quickly.
Children
Because young children are likely to participate in physical activities less than 60 minutes in duration there is often little attention to their hydration. Children do not drink enough when offered fluids freely during exercise in hot and humid climates. But children differ from adults in that, for any given level of dehydration, their core temperatures rise faster than those of adults, putting them at far greater risk for heat stress. Children who participate in sports activities must be taught to prevent dehydration by drinking above and beyond thirst and at frequent intervals, such as every 20 minutes.
A rule of thumb is that a child 10 years of age or younger should drink until he or she does not feel thirsty and then should drink an additional half a glass ( to
to  cup). Older children and adolescents should follow the same guidelines; however, they should consume an additional cup of fluid (8 oz). When relevant, regulations for competition should be modified to allow children to leave the playing field periodically to drink. One of the hurdles to getting children to consume fluids is to provide fluids they like. Providing a sports drink that will maintain the drive to drink and rehydrate them is the key.
cup). Older children and adolescents should follow the same guidelines; however, they should consume an additional cup of fluid (8 oz). When relevant, regulations for competition should be modified to allow children to leave the playing field periodically to drink. One of the hurdles to getting children to consume fluids is to provide fluids they like. Providing a sports drink that will maintain the drive to drink and rehydrate them is the key.
Older Athletes
Older, mature, or masters-level athletes are also at risk for dehydration and need to take precautions when exercising or staying fit. Hypohydration (water loss exceeding water intake with a body water deficit) in older individuals can affect circulatory and thermoregulatory function to a greater extent and may be caused by the lower skin blood flow, causing core temperature to rise. Because the thirst drive is reduced in older adults, they need to drink adequately before exercise, well before they become thirsty. Women athletes need to drink more than men during interval exercise in the heat. Fluid balance is maintained better when palatable carbohydrate and electrolyte solutions are offered (Baker et al., 2005).
Hydration at High Altitudes
Unacclimated individuals undergo a plasma volume contraction when acutely exposed to moderately high altitude. This is the result of increased renal sodium and water excretion and decreased voluntary sodium and water intake. Respiratory losses are increased by high ventilatory rates and typically dry air. The result is an increase in serum hematocrit and hemoglobin, which increases the oxygen-carrying capacity of the blood, but at the cost of reduced blood volume, stroke volume, and cardiac output. Fluid requirements increase as a result. With acclimation, red blood cell production increases and plasma and blood volume return to pre–high altitude levels.
Other Considerations
Alcohol is a central nervous system depressant. Pure alcohol supplies 7 kcal/g and is a source of energy that is metabolized more like fat. For alcohol to be used by muscle, it must first be metabolized in the liver. Alcohol consumption immediately before or during exercise has a detrimental effect on athletic performance, even though, by reducing feelings of insecurity, tension, and discomfort, it may cause the athlete to believe that he or she is performing better. Some athletes incorrectly believe that because alcohol contains carbohydrates, they can load up on beer to improve their performance. Perceptual motor performance, gross motor skills, balance, and coordination are affected by alcohol consumption.
Alcohol may cause reduced glucose secretion from the liver, which may lead to hypoglycemia and early fatigue during endurance exercise. Alcohol may also be a contributing factor to hypothermia if consumed during exercise in cold weather. Alcohol should not be used to replace fluids immediately after exercise because of its diuretic effect and adverse effects on blood glucose and glycogen levels. Chronic alcohol use causes the loss of many nutrients important for performance and health, including thiamin, vitamin B6, and calcium.
Caffeine
Caffeine contributes to endurance performance, apparently because of its ability to enhance mobilization of fatty acids and thus conserve glycogen stores. Caffeine may also directly affect muscle contractility, possibly by facilitating calcium transport. It could reduce fatigue as well by reducing plasma potassium accumulation, which contributes to fatigue. Probably some ergogenic effects occur at doses of 6.5 mg/kg of body weight when taken before endurance exercise, however, caffeine does not seem to offer any benefits before high-intensity exercise.
Because of this potential ergogenic effect, caffeine is banned by the International Olympic Committee (IOC), although the banned level is much higher than that needed to enhance performance. An energy-enhancing effect is seen with only 1.5 to 3 mg of caffeine per pound (3.3 to 6.6 mg/kg). For a 150-lb man this is equivalent to only one 10-oz cup of coffee. As fluid-replacement beverages, tea, iced tea, coffee, cola, caffeinated water, and some of the new caffeine-containing energy drinks are poor choices because of their diuretic effect and variable carbohydrate content. The diuretic action of caffeine could have negative consequences for athletes with excessive water needs or for those participating in long-distance events who do not want to have to urinate during the event. As a restricted drug by the IOC, caffeine is considered a doping agent if the intake results in urine caffeine concentrations of more than 12 mg/L.
Ergogenic Aids
Ergogenic aids include any training technique, mechanical device, nutrition practice, pharmacologic method, or physiologic technique that can improve exercise performance capacity and training adaptations. The use of ergogenic aids in the form of dietary supplements is widespread in all sports. Many athletes, whether recreational, elite, or professional, use some form of dietary supplementation (e.g., substances obtainable by prescription or by illegal means or others marked as supplements, vitamins, or minerals) to improve athletic performance or to assist with weight loss (Dhar et al., 2005). Research suggests that 50% to 98.6% of university athletes use some form of supplements as ergogenic aids (Kristiansen et al., 2005; Neiper, 2005).
Reasons for supplement use differ between genders. Women athletes reported taking supplements for their health or to overcome an inadequate diet, whereas men may take supplements to improve speed, agility, strength, and power. Health reasons (45%), immune system enhancement (40%), and performance improvement (25%) have also been cited as reasons for supplement use (Neiper, 2005). Performance enhancement supplements are pills, drinks, bars, or gels that improve speed, strength, or performance, or minimize or delay fatigue (Bishop, 2010). Supplements used to help build body mass and reduce weight or excess body fat may also enhance exercise performance. The most common supplements used by athletes are described in Tables 24-2 and 24-3.
TABLE 24-2
Recommendations for Use of Sport Foods and Drinks

CHO, Carbohydrate; DV, daily value; RDA, recommended dietary allowance.
Modified from Gatorade Sports Science Institute.
TABLE 24-3
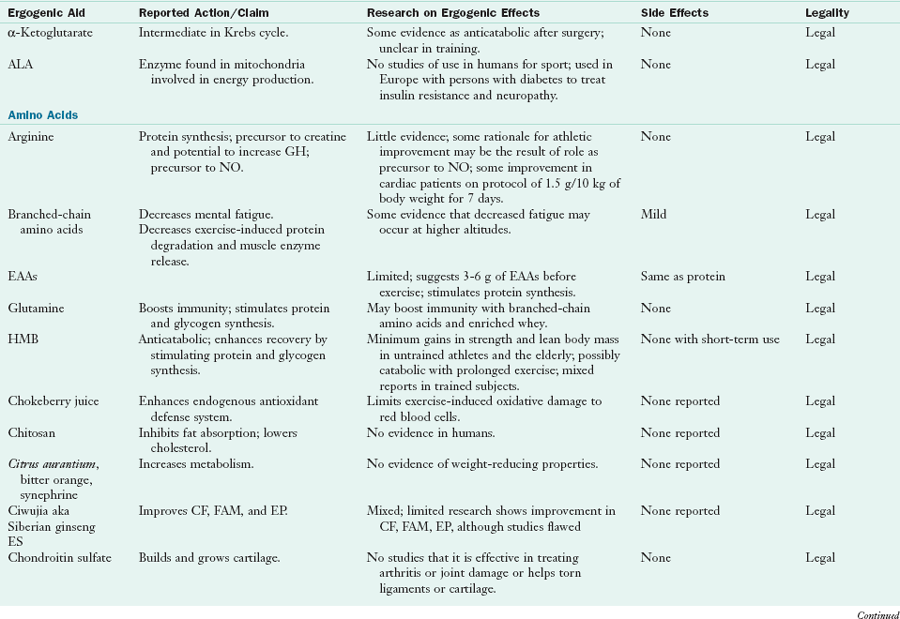
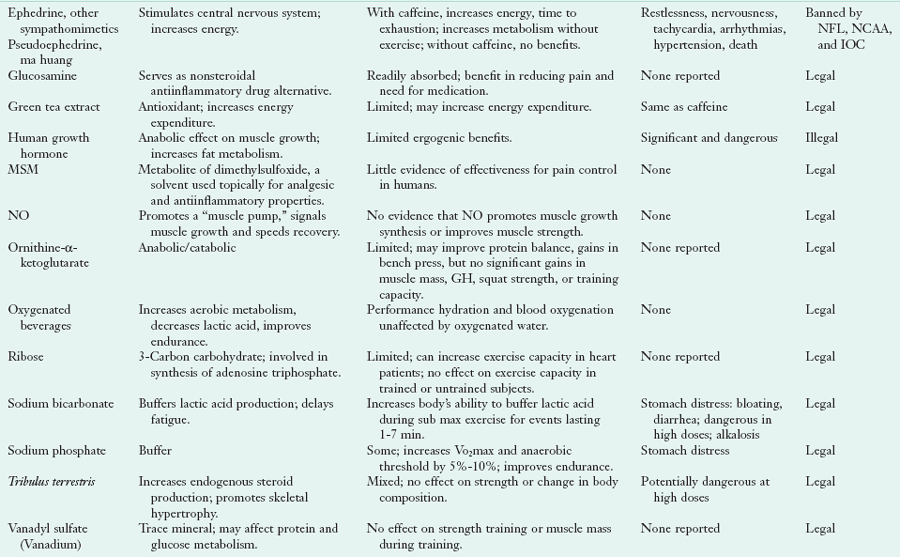
For additional information go to http://gssiweb.org/Article_Detail.aspx?articleid=704&level=3&topic=9.
ALA, α-Lipoic acid; CF, cardiorespiratory fitness; EAA, essential amino acid; EP, endurance performance; ES, Eleutherococcus senticosus; FAM, fat metabolism; GH, growth hormone; HMB, β-hydroxy-β-methylbutyrate; IOC, International Olympic Committee; MSM, methylsulfonylmethane; NCAA, National Collegiate Athletic Association; NFL, National Football League; NO, nitric oxide.
Athletes are bombarded with advertisements and testimonials from other athletes and coaches about the effects of dietary supplements on performance. The Dietary Supplement Health and Education Act (DSHEA) protects dietary supplements from being required to demonstrate proof of efficacy or safety (see Chapter 13). Under this act the Food and Drug Administration no longer has regulatory control of supplements and they are now classified as foods. Manufacturers are allowed to publish limited information about the benefits of dietary supplements in the form of statements of support, as well as so-called structure and function claims. This results in a great deal of printed material that can be confusing to athletes at the point of sale of nutritional products.
Research suggests that the Internet, family members, friends, physicians, or pharmacists guide supplement choices for women athletes; whereas the store nutritionist, fellow athletes, friends, or coaches, advise on supplement decisions for men athletes (Kristiansen et al., 2005). Many believe that ergogenic aids will improve their performance and assist in recovery. As in the past and probably in the future, many of these ergogenic aids are not supported by scientific studies. In fact, many act only as placebos (Figure 24-6).
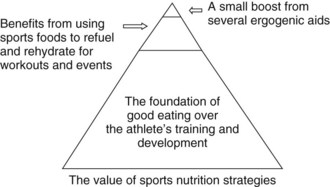
FIGURE 24-6 The value of sports nutrition strategies versus sports drinks and ergogenic aids. (From Australia Sports. Accessed 14 July 2010 at http://fulltext.ausport.gov.au/fulltext/2001/ascpub/images/FactSupp2.gif.)
Many of these supplements confer no performance or health benefit, and some may actually be detrimental to both performance and health when taken for prolonged periods. They may contain excessive doses of potentially toxic ingredients or contain significant amounts of ingredients not approved by the IOC, the World Anti-Doping Agency, the National Collegiate Athletic Association (NCAA), Major League Baseball, and the National Football League (NFL) (Maughan, 2005).
Sports nutritionists need to know how to evaluate the scientific merit of articles and advertisements about exercise and nutrition products so they can separate marketing hype from scientifically based training and nutrition practices. Performance-enhancing substances such as anabolic-androgenic steroids, tetrahydrogestrinone, and androstenedione (andro); stimulants such as ephedra; and nonsteroidal agents such as recombinant human erythropoietin (EPO), human growth hormone (HGH), creatine, and β-hydroxy-β-methylbutyrate (HMB) may cause serious side effects, including adverse cardiovascular changes and sudden death (Dhar et al., 2005).
Muscle-Building Supplements
Muscle-building supplements include amino acids, HMB, creatine, prohormones, glutamine, protein, high-calorie powders, protein-fortified beverages and bars, and other compounds listed in Table 24-2.
Amino Acids
Protein or amino acid supplementation in the form of powders or pills is not necessary and should be discouraged. Taking large amounts of protein or amino acid supplements can lead to dehydration, hypercalciuria, weight gain, and stress on the kidney and liver. Taking single amino acids or in combination, such as arginine and lysine, may interfere with the absorption of certain other essential amino acids. An additional concern is that substituting amino acid supplements for food may cause deficiencies of other nutrients found in protein-rich foods such as iron, zinc, niacin, and thiamin. Athletes and coaches need to realize that amino acid supplements taken in large doses have not been tested in human subjects, and no margin of safety is available. It is important for the health professional to develop a strategy to approach and discuss this supplement use effectively with both athletes and coaches.
Branched-chain amino acids
The BCAAs include leucine, isoleucine, and valine and they make up 35% to 40% of the essential amino acids (EAAs) in the body’s protein and 14% of the total AAs in muscle. In order to get energy, the body can break down muscle to get the BCAAs. During times of stress, BCAAs are required more than any other EAA.
BCAAs consumed before and after training have been shown to increase protein synthesis and muscle gains beyond normal adaptation. They have been reported to decrease exercise-induced protein breakdown and muscle enzyme release, which is a sign of muscle damage. Some research suggests that 14 grams of BCAAs during eight weeks of weight training can produce a significantly greater weight gain in lean mass.
Dairy products and red meat contain the greatest amounts of BCAAs. Whey protein and egg protein supplements are also good sources.
| Branched-chain amino acid | Food sources |
| Leucine | meats, dairy, nuts, beans, brown rice, soy, and whole wheat |
| Isoleucine | meats, chicken, eggs, fish, almonds, chickpeas, soy protein, and most seeds |
| Valine | meat, dairy, soy protein, grains, peanuts, and mushrooms |
Leucine is the most readily oxidized BCAA and is most effective at causing insulin secretion from the pancreas. It lowers elevated blood sugar levels and aids in growth hormone production. Leucine works in conjunction with isoleucine and valine to protect muscle and act as fuel for the body. Doses of up to 2 grams (2000 mg) post workout have been suggested by some experts for accelerating muscle repair and recovery.
β-Hydroxy-β-Methylbutyrate
HMB is an important compound made in the body and a metabolite of the essential amino acid leucine. In humans oral administration of HMB has been associated with increased body mass across the young, elderly, untrained, trained, and clinically cachexic (Wilson JM et al., 2009). The effects of HMB supplementation in trained athletes is not clear, with most studies reporting nonsignificant gains in muscle mass (Palisin and Stacy, 2005). Regarding HMB supplementation and exercise recovery, several studies have found that subjects supplemented with HMB may have less stress-induced muscle protein breakdown. Recent research suggests that both acute and chronic administration of HMB are associated with less exercise-induced muscle damage and soreness (Wilson JM et al., 2009), Additional research is necessary to determine the effectiveness of this supplement both as an ergogenic and recovery aid for athletes.
Creatine
Creatine is an amino acid normally produced in the body from arginine, glycine, and methionine. Most dietary creatine comes from meat, but half is manufactured in the liver and kidneys. For meat eaters, dietary intake of creatine is approximately 1 g daily. The body also synthesizes approximately 1 g of creatine per day, for a total production of approximately 2 g daily.
In normal healthy persons approximately 40% of muscle creatine exists as free creatine; the remainder combines with phosphate to form CP. Approximately 2% of the body’s creatine is broken down daily to creatinine before excretion by the kidneys. The normal daily excretion of creatinine is approximately 2 g for most persons. Those with lower levels of intramuscular creatine such as vegetarians may respond to creatine supplementation (Williams, 2006).
Creatine is one of the most researched and popular sports supplements. It supplies most of the energy for short-term, maximum exercise such as weight lifting, running a 100-m sprint, swinging a bat, or punting a football. Supplementation elevates muscle creatine levels and facilitates the regeneration of CP, which helps to regenerate ATP. When creatine stores in the muscles are depleted, ATP synthesis is prevented and energy can no longer be supplied at the rate required by the working muscle. Improved athletic performance has been attributed to this ATP resynthesis.
Creatine supplementation increases body mass or muscle mass during training; short-term gains may be primarily water, whereas long-term gains along with resistance training are muscle mass (Williams, 2006). Studies suggest that creatine does not enhance exercise and events lasting more than 90 seconds (Astorino et al., 2005). However, creatine supplementation may improve submaximal exercise performance for HIIT, which promotes fitness similar to endurance training (Graef et al., 2009).
Creatine absorption appears to be stimulated by insulin. Therefore ingesting creatine supplements in combination with carbohydrate, amino acid, or protein can increase muscle creatine concentrations (Buford TW, 2007). Once creatine is taken up by the muscles, it is trapped within the muscle tissue. It is estimated that muscle creatine stores decline slowly and will still be elevated 2 to 3 months after ingestion of 20 g of creatine for 5 days.
Current thought is to consume creatine at a dose of 2 to 5 g daily. Human muscle appears to have an upper limit of creatine storage; thus excess creatine presumably will be of little benefit. Few data exist on the long-term benefits and risks of creatine supplementation. There have been anecdotal descriptions of athletes who have had muscle strains and tears, dehydration, and kidney damage (Rodriquez et al., 2009). Thus the American College of Sports Medicine advises against taking creatine for youth 18 years old and younger.
Peptide Hormones
Erythropoietin: EPO is commonly used to keep up the body’s production of red blood cells in patients with bone marrow suppression such as patients with leukemia, those who are receiving chemotherapy, or those with renal failure (see Chapter 36). In athletes, injections increase the serum hematocrit and oxygen-carrying capacity of the blood and thus enhance VO2max and endurance. EPO use as an ergogenic aid is difficult to detect because it is a hormone produced by the kidneys, although newer blood tests can detect its use. Typically, athletes with elevated hematocrit have been banned from endurance sports for suspected EPO misuse; however, despite its ban by the IOC, it is still commonly abused. Drastically high hematocrit combined with exercise-induced dehydration can lead to thick or viscous blood, which can lead to coronary or cerebral vascular occlusions, heart attack, or stroke. EPO can also cause elevated blood pressure or elevated potassium levels.
Human growth hormone (HGH) has many functions in the body, and it is produced naturally throughout life. It stimulates protein synthesis, enhances carbohydrate and fat metabolism, helps to maintain sodium balance, and stimulates bone and connective tissue turnover. HGH production decreases with age after the peak growth years. The amount secreted is affected by diet, stress, exercise, nutrition, and medications. HGH is banned by the IOC; however, it continues to be abused by athletes. Potential side effects can include skin changes, darkening of moles, an adverse effect on glucose metabolism and on the lipid profile, and growth of bones as evidenced by a protruding jaw and boxy forehead.
Prohormones and Steroids
Prohormones are popular among bodybuilders, many of whom believe that these prohormones are natural boosters of anabolic hormones. Androstenedione, 4-androstenediol, 19-nor-4-androstenedione, 19-nor-4-androstenediol, 7-keto dehydroepiandrosterone (DHEA) and 7-keto DHEA are naturally derived precursors to testosterone and other anabolic steroids. Androstenedione is an anabolic androgenic steroid used to increase blood testosterone levels for the purpose of increasing strength and lean body mass, although there is no research that it has that effect in humans. Although theoretically prohormones may increase testosterone levels, there is no evidence that these compounds affect training adaptations in younger men with normal hormone levels. They may even increase estrogen levels and low-density lipoprotein cholesterol levels and reduce high-density lipoprotein (HDL) cholesterol.
Androstenedione: Androstenedione (andro) is a prehormone, an inactive precursor to both female estrogen and male testosterone. It has about one seventh of the activity of testosterone and is a precursor that directly converts to testosterone by a single reaction. It is naturally produced in the body from either DHEA or 17-α-hydroxyprogesterone. Some researchers have found that taking andro elevates testosterone more than DHEA does; however, the induced increase lasts only several hours and remains at peak levels for just a few minutes. Acute or long-term administration of testosterone precursors does not effectively increase serum testosterone levels and fails to produce any significant changes in lean body mass, muscle strength, or performance improvement (Smurawa and Congeni, 2007).
Adverse reactions occur in male and female athletes, including muscle tightness and cramps, increased body weight, acne, GI problems, changes in libido, amenorrhea, liver damage, and stunted growth in adolescents. Consumption of a prohormone supplement can alter a patient’s hypothalamic-pituitary-gonadal axis. Andro-related hormones may abnormally elevate estrogen-related hormones and alter elevations of serum estrogen, which is thought to increase the risk for developing prostate or pancreatic cancers. A significant decline in HDLs occur, leading to an increased cardiovascular disease risk (Dhar et al., 2005). Therefore taking androstenedione may be irresponsible because of the potential risks associated with long-term use. Until there is scientific support for its use, andro should not be sold under the assumption that it is either an effective or a safe athletic ergogenic aid. Clearly adolescents and women of childbearing age should not use it. In 1998 andro was added to the list of banned substances by the IOC and several amateur and professional organizations, including the NFL and the NCAA.
Dehydroepiandrosterone (DHEA) is a weak androgen and product of dehydroandrosterone-3-sulfate (DHEA-S) and is used to elevate testosterone levels. It is a precursor to more potent testosterone and dihydrotestosterone. Although DHEA-S is the most abundant circulating adrenal hormone in humans, its physiologic role is poorly understood. DHEA has been labeled the “fountain of youth” hormone because its levels peak during early adulthood. The decline with aging has been associated with increased fat accumulation and risk of heart disease. Several studies have suggested a positive correlation between increased plasma levels of DHEA and improved vigor, health, and well-being in persons who range in age from 40 to 80 years. By decreasing cortisol output from the liver by 50%, DHEA could have an anabolic effect. If this were to occur in muscle tissue as well, the anabolic effect would be comparable to that of anabolic steroids; however, no proof of this currently exists.
DHEA supplementation does not increase testosterone levels or increase strength in men, but it may increase testosterone levels in women with a virilizing effect. Because DHEA can take several different hormonal pathways, the one that it follows depends on several factors, including existing levels of other hormones. It can take several routes in the body and interact with certain enzymes along the sex-steroid pathway. Thus it can turn into less desirable byproducts of testosterone, including dihydrotestosterone, which is associated with male-pattern baldness, prostate enlargement, and acne.
Until recently DHEA was a prescription drug, but it is now sold over the counter. Analysis of DHEA products on the market shows a dramatic difference between the amount stated on the label and the actual amount in the product.
The benefits of taking DHEA for sports performance have not been clearly established, and the effects of chronic DHEA ingestion are not known. Long-term safety has not been established, and there are concerns that chronic use in men may worsen prostate hyperplasia or even promote prostate cancer. DHEA is not recommended for athletic use because it can alter the testosterone-epitestosterone ratio so that it exceeds the 6 : 1 limit set by the IOC, the U.S. Olympic Committee, the NFL, and the NCAA.
Steroids: Androgenic-anabolic steroids (AASs) categorize all male sex steroid hormones, their synthetic derivatives, and their active metabolites used to enhance athletic performance and appearance (DiLuigi et al., 2005). AAS use was reported in the 1950 Olympics and was banned in 1976. Steroids may be used in oral or intramuscular preparations.
The legal and illegal use of these drugs is increasing as a result of society’s preoccupation with increasing muscle strength, size, and libido. Originally designed for therapeutic uses to provide enhanced anabolic potency, nontherapeutic use of AAS is increasing among adolescents and females (DiLuigi et al., 2005). Anecdotal evidence suggests widespread use of anabolic steroids among athletes (20% to 90%), especially at the professional and elite amateur levels. Use among high school boys is approximately 5% to 10%; rates among college athletes are slightly higher. Use of multiple steroids simultaneously in excess of therapeutic doses by 10-fold to 100-fold is known as “stacking” (Trenton and Currier, 2005). See Box 24-3 for a list of commonly abused steroids.
Short-term administration of these drugs by athletes can increase strength and body weight. Anabolic effects include increased muscle mass; increased bone mineral density; increased blood cell production; decreased body fat; increased heart, liver, and kidney size; vocal cord changes; and increased libido. Anabolic steroids increase protein synthesis in skeletal muscles and reverse catabolic processes; however, increased muscle mass and strength are observed only in athletes who maintain a high-protein, high-calorie diet during steroid administration. Androgenic effects are the development of secondary sexual characteristics in men, changes in genital size and function, and growth of auxiliary pubic and facial hair (Trenton and Currier, 2005). Some adverse effects associated with steroid use are irreversible, especially in women (Table 24-4).
TABLE 24-4
Effects of Androgenic Anabolic Steroids in Athletes
| Children | Premature closing of growth plates |
| Males | Increase sex drive, acne vulgaris, enlarged breasts, testicular hypotrophy, infertility |
| Females | Clitoris enlargement, excessive body hair |
| Athletic performance | Increased strength and lean body mass; no increase in endurance performance |
| Cardiovascular system | Increased blood pressure, depression of HDL, HDL2, and HDL3 cholesterol |
| Hormonal changes | Disturbance in endocrine and immune function |
| Hepatic system | Peliosis (purpura), hepatitis, increased liver enzymes, jaundice, cancer |
| Immune compromised—those with HIV, AIDS, hepatitis | Infections from injectable forms |
| Mental health | Increase in aggressive behavior, mood disturbances (e.g., depression, hypomania, psychosis, homicidal rage, mania, delusions) |
| Metabolic changes | Changes in hemostatic system and urogenital tract, altered glucose metabolism, immune system suppression, low thyroid hormone levels |
| Physical | Short stature, tendon rupture |
| Skin | Acne, cysts, oily scalp |
AIDS, Acquired immune deficiency syndrome; HDL, high-density lipoprotein; HIV, human immunodeficiency virus.
 Clinical Scenario
Clinical Scenario
Ben is a 21-year-old active college student who is interested in building muscle mass and losing body fat. His height is 5 ft 8 in, and his weight is 160 lb. Ben says that, although he is very disciplined, he has weekend splurges of a pizza and a six-pack of beer, as well as chips, ribs, and nuts during football, basketball, and baseball season. He does not work out on the weekends. He cannot understand why he is not losing body fat because he works out twice a day, includes resistance training and cardiovascular exercise, and eats the following:
 chicken, string beans, and a lettuce salad with olive oil
chicken, string beans, and a lettuce salad with olive oil{kind=link}
Nutrition Diagnostic Statement
Excessive protein intake related to frequent intake of protein bars and supplemental beverages, as evidenced by an intake of 265 g of protein per day from these products compared with a recommended dietary allowance (RDA) of 55 to 75 g/day for normal growth and development.
1. How many grams of protein is Ben consuming? What is his protein per kilogram of body weight consumption? Can this be a contributing factor to his difficulty with losing body fat?
2. What level of protein intake would you recommend for him? Is this different from the RDA for normal growth and development? Are there healthier sources of protein that he can consume?
3. What is the calorie cost of his weekend splurges? Are they in excess of his calorie needs? And if so, by how much? What type of recovery beverages and protein dosages may be more suitable for Ben to consume? What additional questions would you ask Ben about his bars and supplements?
4. What nutrients are in deficient amounts in Ben’s diet? Including what foods in his diet would be beneficial?
5. What are other changes Ben can make on the weekends? What foods and exercise will help him reduce his body fat and manage his weight better?
References
Achten, J, Jeukendrup, AE. Optimizing fat oxidation through exercise and diet. Nutrition. 2004;20:716.
Anderson, LL, et al. Effect of resistance training and combined with timed ingestion of protein muscle fiber size and muscle strength. Metabolism. 2005;54:151.
Astorino, T, et al. Is running performance enhanced with creatine serum ingestion? J Strength Cond Res. 2005;19:730.
Backhouse, SH, et al. Effect of carbohydrate and prolonged exercise on affect and perceived exertion. Med Sci Sports Exerc. 2005;37:1768.
Baker, LB, et al. Sex differences in voluntary fluid intake by older adults during exercise. Med Sci Sports Exerc. 2005;37:789.
Bishop, D. Dietary supplements and team-sport performance. Sports Med. 2010;40:995.
Buford, TW, et al. International Society of Sports Nutrition position stand: creatine supplementation and exercise. Int Soc Sports Nutr. 2007;30:4.
Byars, A, et al. The influence of a pre-exercise sports drink (PRX) on factors related to maximal aerobic performance. J Int Soc Sports Nutr. 2010;7:12.
Byrne, C, et al. Water versus carbohydrate electrolyte replacement during loaded marching under heat stress. Mil Med. 2005;170:715.
Cannell, JJ, et al. Athletic performance and vitamin D. Med Sci Sports Exerc. 2009;41:1102.
Dhar, R, et al. Cardiovascular toxicities of performance-enhancing substances in sports. Mayo Clin Proc. 2005;80:1307.
DiLuigi, L, et al. Androgenic-anabolic steroids abuse in males. J Endocrinol Invest. 2005;28:81S.
Foster, GD, et al. A policy-based school intervention to prevent overweight and obesity. Pediatrics. 2008;121:e794.
Graef, JL, et al. The effects of four weeks of creatine supplementation and high-intensity interval training on cardiorespiratory fitness: a randomized controlled trial. J Int Soc Sports Nutr. 2009;6:18.
Havemann, L, et al. Fat adaptation followed by carbohydrate loading compromises high intensity sprint performance. J Appl Physiol. 2005;100:194.
Heaney, S, et al. Comparison of strategies for assessing nutritional adequacy in elite female athletes’ dietary intake. Int J Sport Nutr Exerc Metab. 2010;20:245.
Hew, TD. Women hydrate more during a marathon race: hyponatremia in the Houston Marathon: a report on 60 cases. Clin J Sport Med. 2005;15:148.
Howatson, G, et al. Influence of tart cherry juice on indices of recovery following marathon running. Scand J Med Sci Sports. 2010;37:843.
Hulmi, JJ, et al. Protein ingestion prior to strength exercise affects blood hormones and metabolism. Med Sci Sports Exerc. 2005;37:1990.
Institute of Medicine (IOM), Food and Nutrition Board. Dietary reference intakes (DRIs) for water, potassium, sodium and chloride and sulfate. Washington, DC: National Academies Press; 2004.
Institute of Medicine (IOM), Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academies Press; 2011.
Kerksick, C, Leutholz, B. Nutrient administration and resistance training. J Int Soc Sports Nutr. 2005;2:50.
Kristiansen, M, et al. Dietary supplement use by university athletes at a Canadian university. Int J Sports Nutr Exerc Metab. 2005;15:195.
Kuehl, KS, Perrier, ET, Elliot, DL, Chesnutt, JC. Efficacy of tart cherry juice in reducing muscle pain during running a randomized controlled trial. J Int Soc Sports Nutr. 2010;7:17.
Larson-Meyer, DE, Willis, KS. Vitamin D and athletes. Curr Sports Med Rep. 2010;9:220.
Lin-Wu, CL, Williams, C. A low glycemic index meal before exercise improves endurance running capacity in men. Int J Sport Nutr Exerc Metab. 2006;16:510.
Malinauskas, BM, et al. Supplements of interest for sport-related injury and sources of supplement information among college athletes. Adv Med Sci. 2007;52:50.
Maughan, RJ. Contamination of dietary supplements and positive drug tests in sport. J Sports Sci. 2005;23:883.
Millard-Stafford, M, et al. Recovery from run training: efficacy of a carbohydrate-protein beverage? Int J Sport Nutr Exerc Metab. 2005;15:610.
Murray, R. Fluids, electrolytes, and exercise. In Danford M, ed.: Sports nutrition: a practice manual for professionals, ed 4, Washington, DC: American Dietetic Association, 2006.
Neiper, A. Nutritional supplement practices in UK junior national track and field athletes. Br J Sports Med. 2005;39:645.
Noakes, TD, et al. Three independent biological mechanisms cause exercise-associated hyponatremia: evidence from 2,135 weighed competitive performances. Proc Natl Acad Sci. 2005;102:18550.
Palisin, T, Stacy, JJ. Beta-hydroxy-methylbutyrate and its use in athletics. Curr Sports Med Rep. 2005;4:220.
Peake, J. Heat, athletes and immunity. Am J Lifestyle Med. 2010;4:320.
Pennings, B, et al. Exercising before protein intake allows for greater use of dietary protein—derived amino acids for de novo muscle protein synthesis in both young and elderly men. Am J Clin Nutr. 2010;93(2):322.
Pialoux, V, et al. Effects of acute hypoxic exposure on prooxidant/antioxidant balance in elite endurance athletes. Int J Sports Med. 2009;30:87.
Pialoux, V, et al. Antioxidant status of elite athletes remains impaired 2 weeks after a simulated altitude training camp. Eur J Nutr. 2010;49:285.
Pigeon, WR, et al. Effects of a tart cherry juice beverage on the sleep of older adults with insomnia: a pilot study. J Med Food. 2010;13:579.
Rodriguez, NR, et al. Position of the American Dietetic Association, Dietitians of Canada, and the American College of Sports Medicine: nutrition and athletic performance. J Am Diet Assoc. 2009;109:509.
Sinclair, L, Hinton, P. Prevalence of iron deficiency with and without anemia in recreationally active men and women. J Am Diet Assoc. 2005;105:975.
Smith, AE, et al. Effects of beta-alanine supplementation and high-intensity interval training on endurance performance and body composition in men: a double-blind trial. J Int Soc Sports Nutr. 2009;6:5.
Smurawa, TM, Congeni, JA. Testosterone precursors: use and abuse in pediatric athletes. Pediatr Clin North Am. 2007;54:787.
Stofan, J, et al. Sweat and sodium losses in NCAA football players: a precursor to heat cramps? J Sport Nutr Exerc Metabol. 2005;15:641.
Trenton, AJ, Currier, GW. Behavioral manifestations of anabolic steroid use. CNS Drugs. 2005;19:571.
Van Hamont, D, et al. Reduction in muscle glycogen and protein utilization with glucose feeding during exercise. Int J Sport Nutr Exerc Metabol. 2005;15:350.
Watson, TA, et al. Antioxidant restriction and oxidative stress in short-duration exhaustive exercise. Med Sci Sports Exerc. 2005;37:63.
Williams, M. Dietary supplements and sports performance: metabolites, constituents, and extracts. J Int Soc Sports Nutr. 2006;3:1.
Williams, M. Dietary supplements and sport performance: minerals. J Int Soc Sports Nutr. 2005;2(1):43.
Wilson, JM, et al. Acute and timing effects of beta-hydroxy-beta-methylbutyrate (HMB) on indirect markers of skeletal muscle damage. Nutr Metab. 2009;6:6.
Wilson, M, et al. Effect of glycemic index meals on recovery and subsequent endurance capacity. Int J Sports Med. 2009;30:898.
Wong, SH, et al. Effect of preexercise glycemic-index meal on running when CHO-electrolyte solution is consumed during exercise. Int J Sport Nutr Exerc Metab. 2009;19:222.